UPDATE: COMMUNITY HEALTH IMPROVEMENT PLAN … 21/CHIP and... · Agree on the process for gathering documentation ... PHAB has shared comments from many of the first 11 Public Health
15
UPDATE: COMMUNITY HEALTH IMPROVEMENT PLAN AND PUBLIC HEALTH ACCREDITATION Presentation to the Health Commission, May 21, 2013 Colleen Chawla, Deputy Director of Health, Director of Policy & Planning Karen Pierce, Accreditation Coordinator
UPDATE: COMMUNITY HEALTH IMPROVEMENT PLAN AND PUBLIC HEALTH ACCREDITATION Presentation to the Health Commission, May 21, 2013
Colleen Chawla, Deputy Director of Health, Director of Policy & Planning
Karen Pierce, Accreditation Coordinator
CHIP UPDATE: ALIGNING FOR COMMUNITY HEALTH IMPROVEMENT Expanding the San Francisco Health Improvement Partnership (SF HIP)
2
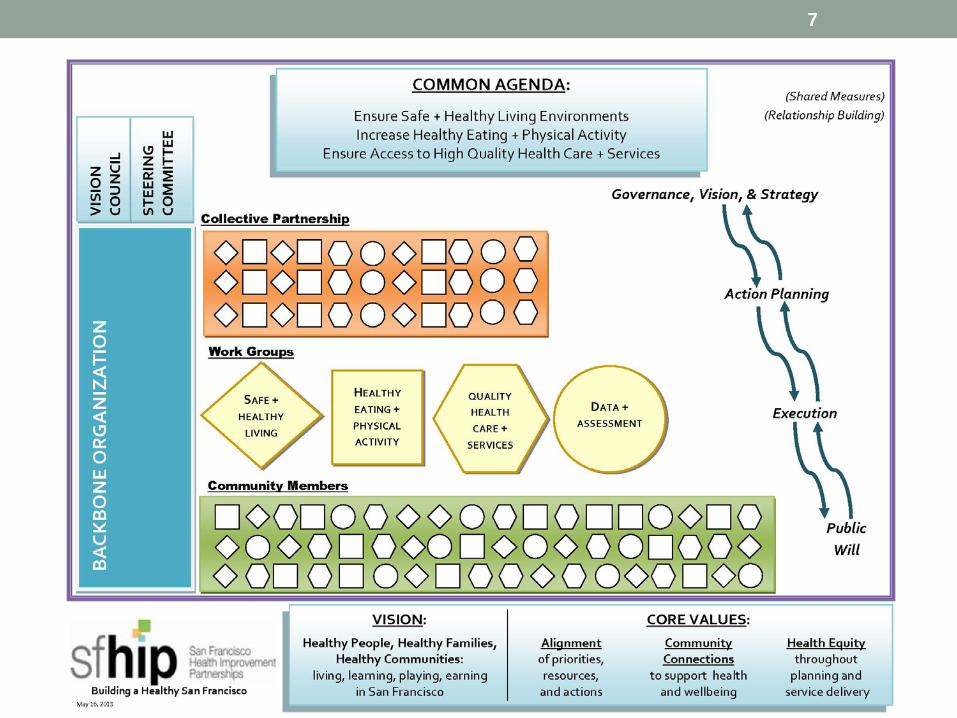
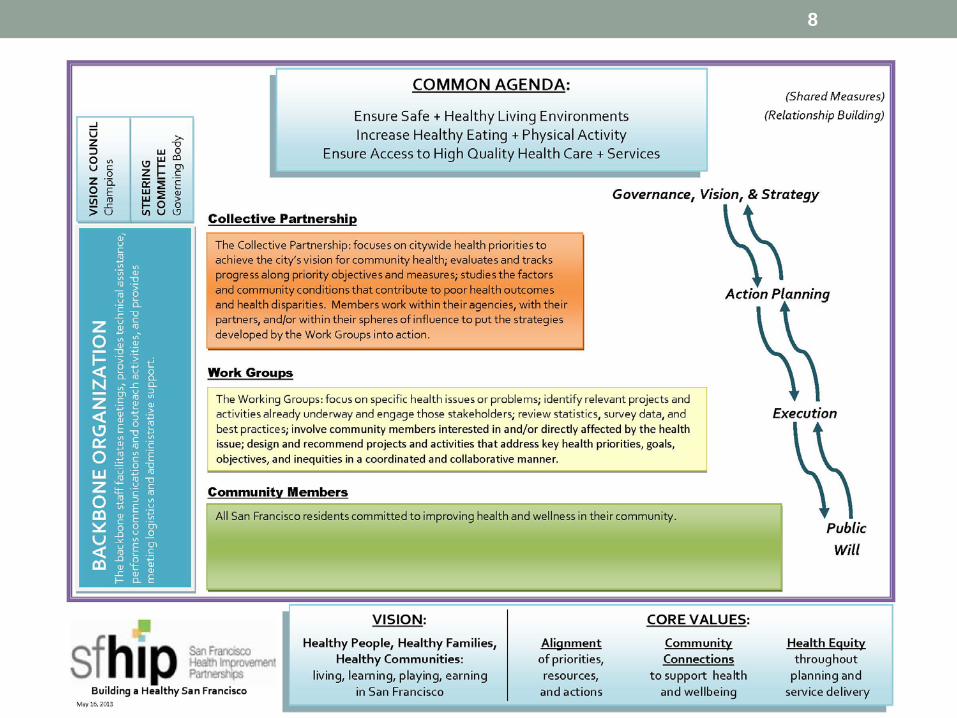
Community Health Improvement Plan – Three Core Values
Alignment of priorities, resources, and actions
Health Equity throughout
planning and service delivery
Draft - for review and discussion by the Planning Team
3
Community Connections
to support health and well being
“During the CHA/CHIP process, many residents and service providers expressed the need for greater alignment of efforts in order to have the greatest impact on health.”
Current Efforts Include
Collaboratives
• Building a Healthier San Francisco (BHSF)
• Community Benefits Partnership (CBP)
• San Francisco Health Improvement Partnerships (SFHIP)
• Community Transformation Initiative (CTI)
Projects • BHSF tri-annual community
health needs assessment (CHNA) • Community Vital Signs • HealthMattersinSF.org
• SF HIP Partnership Working Groups
• SF Department of Public Health Accreditation • Community Health Assessment
(CHA) • Community Health Improvement
Plan (CHIP) • Health Care Services Master
Plan
Draft - for review and discussion by the Planning Team
4
Presenter
Presentation Notes
Major efforts, sample of things happening, but this is hardly an exhaustive list.
Partners Have a Long History of Collaboration for Community Health Improvement
BHSF Created
BHSF completes first CHNA
Health Matters in
SF website design begins
CBP Created
Health
Matters in SF
launched
Community Vital Signs released
SF HIP Created
Community Vital Signs Moving the
Needle effort
launched
SF awarded Community Transformation Initiative
SF HIP formed
Partnership Working Groups
5
1994 1996 2005 2007 2010 2011 2011-13
Presenter
Presentation Notes
BHSF 1994: Community Needs Assessment required of private, non-profit hospitals every 3 years. (SB697) 1995: BHSF founded – a collaborative of hospitals, foundations, health/human service providers, CBOs to respond to SB697. 1996: BHSF developed first needs assessment. (BHSF produced 6 reports since 1996.) 2005: Health Matters in San Francisco website began development. (Website launched in ‘07.) CBP 2007: CBP created to serve a broader mission and larger cross-section of partners. 2009: Identified 10 priority health goals. 2010: Developed and launched Community Vital Signs, a dynamic web portal to the priority health issues. Established 34 indicators (engaging over 600 stakeholders and content experts). 2011: “Moving the Needle” meeting series and identified 24 “Champions,” assigned to an indicator. SF Health Improvement Partnerships (SF HIP) (2010): Convened as a “partnership [academic + nonprofit + civic representatives] to collaboratively plan, implement, and evaluate systematic, well-coordinated interventions to make a measurable impact on the health of SF and reduce health disparities.” Assessed local health reports. Assigned navigation staff. Formative evaluation began. 2011 through 2013: Formed Partnership Working Groups and continued process evaluation. To improve local community health the Partnership Working Groups bring together many different professionals and community stakeholders. They developed their list of priorities that has very much overlapped with the other goals and lists that have been developed. Their topics include: Physical activity and nutrition (CHIP = Increase Healthy Eating and Physical Activity) Alcohol Violence and its impact on youth mental health Hepatitis B HIV Tobacco Early childhood caries Environmental threats to health (CHIP = Ensure Safe & Healthy Living Environments) Cardiovascular disease Healthy child development in a family context CHIP = Increase Access to Quality Health Care and Services – fits into many of these. The Community Transformation Initiative 2011: Grant funded through the Patient Protection & Affordable Care Act – Prevention & Public Health Fund was awarded to San Francisco. Grant will run through 2016. Focus is to transform and integrate prevention approaches. Priority areas: Tobacco-free living Healthy eating/active living Quality clinical preventive services.
Uniting and Aligning Efforts
• Embracing the Collective Impact* model: • The commitment of a group of actors from different sectors to a
common agenda for solving a complex social problem • Isolated impact v. collective impact
• The Five Conditions of Collective Impact Success • Common Agenda • Shared Measurement • Mutually Reinforcing Activities • Continuous Communication • Backbone Organization
Draft - for review and discussion by the Planning Team
6
*John Kania and Mark Kramer, “Collective Impact,” Stanford Social Innovation Review, Winter 2011.
Presenter
Presentation Notes
Collective Impact is the commitment of a group of actors from different sectors to a common agenda for solving a complex social problem. In order to create lasting solutions to social problems on a large-scale, organizations — including those in government, civil society, and the business sector — need to coordinate their efforts and work together around a clearly defined goal. Collective Impact is a significant shift from the social sector’s current paradigm of "isolated impact," because the underlying premise of Collective Impact is that no single organization can create large-scale, lasting social change alone. There is no "silver bullet" solution to systemic social problems, and these problems cannot be solved by simply scaling or replicating one organization or program. Strong organizations are necessary but not sufficient for large-scale social change. The Five Conditions of Collective Impact Success Collective Impact is more rigorous and specific than collaboration among organizations. There are five conditions that, together, lead to meaningful results from Collective Impact: Common Agenda: All participants have a shared vision for change including a common understanding of the problem and a joint approach to solving it through agreed upon actions Shared Measurement: Collecting data and measuring results consistently across all participants ensures efforts remain aligned and participants hold each other accountable Mutually Reinforcing Activities: Participant activities must be differentiated while still being coordinated through a mutually reinforcing plan of action Continuous Communication: Consistent and open communication is needed across the many players to build trust, assure mutual objectives, and appreciate common motivation Backbone Organization: Creating and managing collective impact requires a separate organization(s) with staff and a specific set of skills to serve as the backbone for the entire initiative and coordinate participating organizations and agencies
7
8
“Collective impact is not merely a new process that supports the same social sector solutions, but an entirely different model of social progress. The power of collective impact lies in the heightened vigilance that comes from multiple organizations looking for resources and innovations through the same lens, the rapid learning that comes from continuous feedback loops, and the immediacy of action that comes from a unified and simultaneous response among all participants.”
--John Kania and Mark Kramer, ‘Embracing Emergence: How Collective Impact Addresses Complexity,’ Stanford Social Innovation Review, p.2
5/10/13
Draft - for review and discussion by the Planning Team
9
PUBLIC HEALTH ACCREDITATION UPDATE
10
Coordination and Support • The Backbone:
• Project Sponsors: Barbara Garcia and Tomás Aragón
• Project Lead: Israel Nieves-Rivera, PHD Director of Public Health Accreditation, Equity and Quality Improvement Branch • Project Manager: Karen Pierce, Accreditation Coordinator • Accreditation Leadership Team
11
Accreditation Leadership Team • Domain 1: Megan Gaydos Domain 7: Susan Philip • Domain 2: Rajiv Bhatia Domain 8: Jonathan Fuchs • Domains 3&4 : Tracey Packer Domain 9: Priscilla Chu • Domain 5: Israel Nieves Domain 10: Kyle Bernstein • Domains 6&12: Tomás Aragón Domain 11: Christine Siador
• Colleen Chawla • Frances Culp • Karen Pierce
12
Action Planning and Execution • Kickoff meeting of the Leadership Team will be in June
when we will collectively: • Develop the Work Plan and Timeline • Design a Communications Plan • Set meeting Schedules • Agree on the process for gathering documentation • Set group expectations and collaborative agreements
13
PHD Milestones • California Department of Health initiate a monthly webinar
with a focus on Quality Improvement and Performance Management
• Priscilla Chu and Karen Pierce are participating
• PHD Branch Managers completed workshop on alignment of the Strategic Map with Public Health Accreditation
14
Presenter
Presentation Notes
Updates: PHAB has shared comments from many of the first 11 Public Health Departments to achieve accreditation and some common themes include experiencing successful team building throughout the various Departments, a feeling of accomplishment shared by the full staff, recognition of a level of excellence by other agencies and a sense that it was well worth the effort spent.