unraveling the molecular basis of cancer · unraveling the molecular basis of cancer hai t. tran,...
TRANSCRIPT
Unraveling the MolecularUnraveling the MolecularBasis of CancerBasis of Cancer
Hai T. Tran, Hai T. Tran, PharmDPharmD
Assistant ProfessorAssistant Professor
Pharmacology Pharmacology –– Research ResearchCancer Medicine and PharmacyCancer Medicine and Pharmacy
The University of TexasThe University of Texas
M. D. Anderson Cancer CenterM. D. Anderson Cancer Center
Houston, TexasHouston, Texas

Molecular Basis of CancerMolecular Basis of Cancer
Understand the complexity of cancer andUnderstand the complexity of cancer andappropriately identify potential targets forappropriately identify potential targets for
therapeutic interventiontherapeutic intervention
Causes of cancerCauses of cancer
Process of malignant transformationProcess of malignant transformation
Cell cycle controlCell cycle control
Roles of angiogenesis and growth factorsRoles of angiogenesis and growth factors
Effects of tyrosine kinase inhibitionEffects of tyrosine kinase inhibition
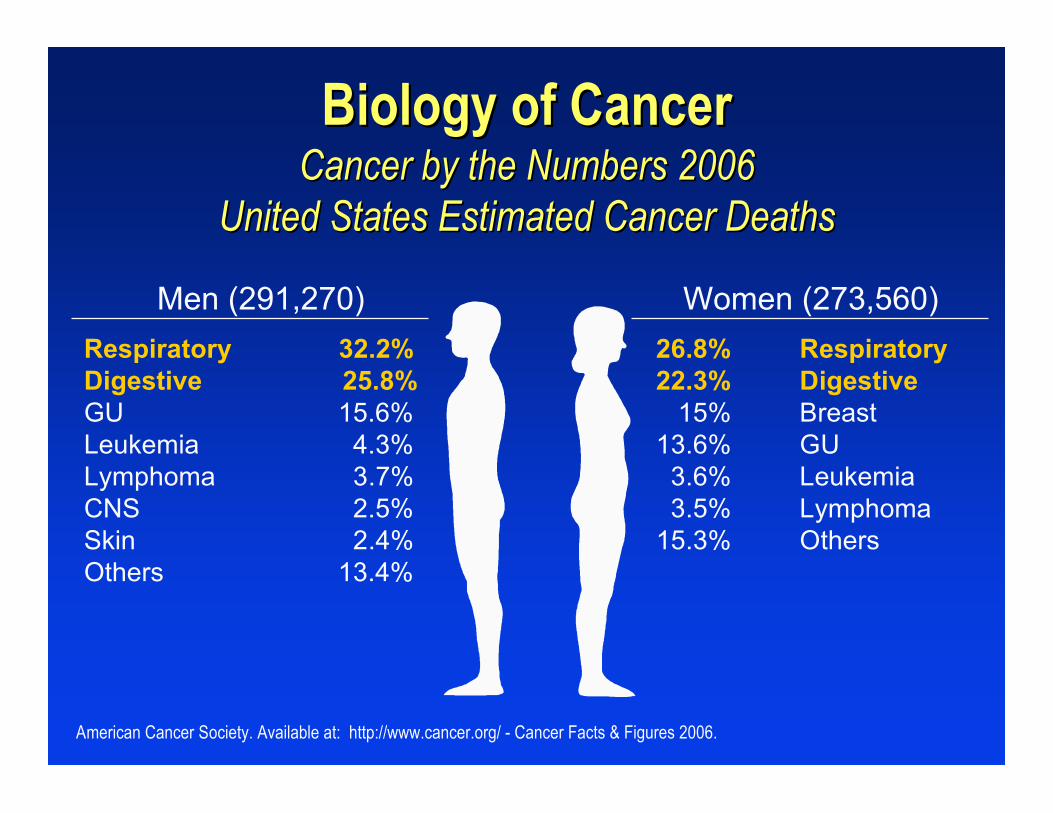
Biology of CancerBiology of CancerCancer by the Numbers 2006Cancer by the Numbers 2006
United States Estimated Cancer DeathsUnited States Estimated Cancer Deaths
Men (291,270) Women (273,560)26.8% Respiratory22.3% Digestive 15% Breast13.6% GU 3.6% Leukemia 3.5% Lymphoma15.3% Others
Respiratory 32.2%Digestive 25.8%GU 15.6%Leukemia 4.3%Lymphoma 3.7%CNS 2.5%Skin 2.4%Others 13.4%
American Cancer Society. Available at: http://www.cancer.org/ - Cancer Facts & Figures 2006.

Weinberg RA. The Biology of Cancer. 2007. Garland Science, Taylor & Francis Group, LLC, New York, NY, USA.
Biology of CancerBiology of CancerAbbreviated List of the Usual SuspectsAbbreviated List of the Usual Suspects
ChemicalsChemicals–– Hydrocarbons: Hydrocarbons: benzopyrenebenzopyrene, benzene, benzene
compounds, 2-napthylaminecompounds, 2-napthylamine–– Asbestos & tobacco exposuresAsbestos & tobacco exposures
Radiation exposureRadiation exposure Tumor virusesTumor viruses
–– DNA: HBV, SV40/polyoma, HPV16, HAV5, HSV-DNA: HBV, SV40/polyoma, HPV16, HAV5, HSV-8, 8, Shope fibroma Shope fibroma virusvirus
–– RNA: RSV, HTLV-1RNA: RSV, HTLV-1 Cellular Cellular oncogenesoncogenes
–– mycmyc, , erbBerbB, int-1,2,3; p53, GM-CSF, IL-2, IL-3,, int-1,2,3; p53, GM-CSF, IL-2, IL-3,k-rask-ras, Cyc-D1 & D2, Cyc-D1 & D2

Biology of CancerBiology of CancerA Learning Curve That Never PlateausA Learning Curve That Never Plateaus
Process of malignant transformationProcess of malignant transformation–– Accumulation of multiple genetic alterationsAccumulation of multiple genetic alterations
Escape from normal growth controlEscape from normal growth control Evade from apoptotic programEvade from apoptotic program Induction of sustained angiogenesisInduction of sustained angiogenesis Enhanced ability to metastasizeEnhanced ability to metastasize Ability to invade healthy tissuesAbility to invade healthy tissues
Identification of more than 300 cancer genesIdentification of more than 300 cancer genes–– Signal transduction, cell cycle progression, apoptosis,Signal transduction, cell cycle progression, apoptosis,
angiogenesis and invasionangiogenesis and invasion A very complex systemA very complex system
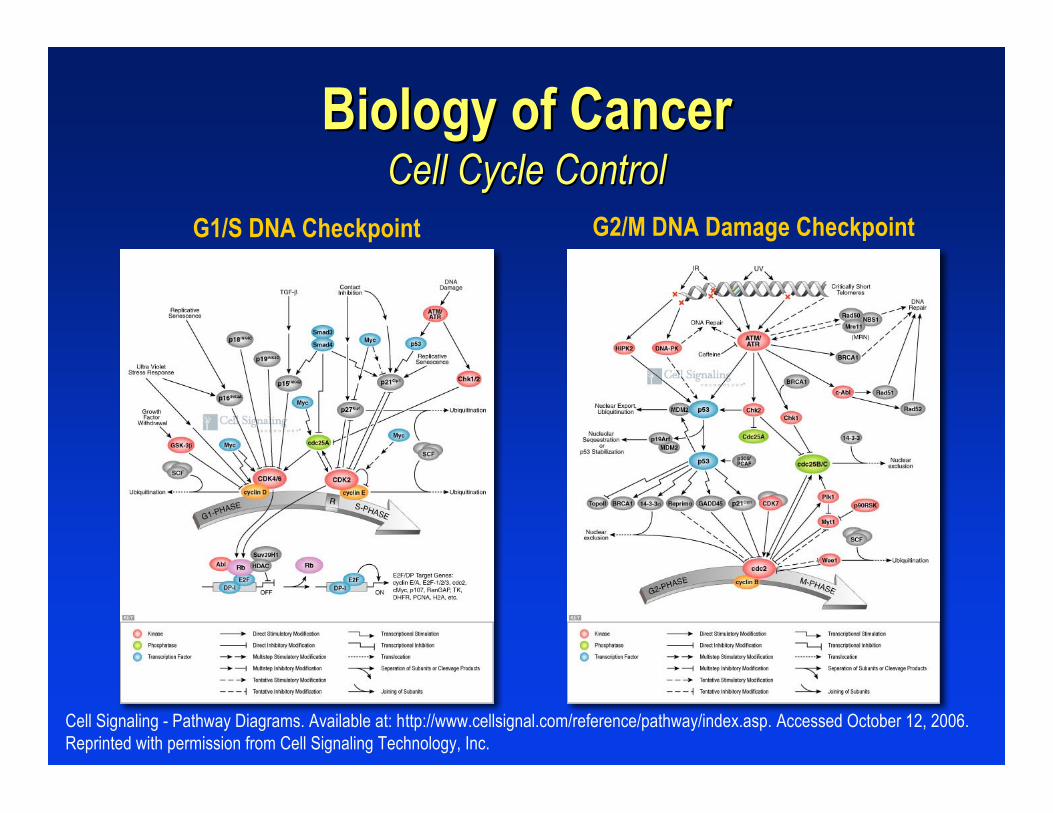
Biology of CancerBiology of CancerCell Cycle ControlCell Cycle Control
G2/M DNA Damage CheckpointG1/S DNA Checkpoint
Cell Signaling - Pathway Diagrams. Available at: http://www.cellsignal.com/reference/pathway/index.asp. Accessed October 12, 2006.Reprinted with permission from Cell Signaling Technology, Inc.

Biology of CancerBiology of Cancer p53 and Cell Deathp53 and Cell Death
Transcriptionblockage
Hypoxia Oncogene RadiationMissing
nucleotides
p53
DNArepair
Inhibition ofangiogenesis
ApoptosisCell cycle
arrest
Proliferation Senescence
Courtesy of Dr. H. Tran.

1. Hanahan D, Weinberg RA. Cell. 2000;100:57.2. Dvorak HF. N Engl J Med. 1986;315:1650.3. Folkman J. N Engl J Med. 1971;285:1182.4. Folkman J, et al. J Exp Med. 1971;133:275.
Biology of CancerBiology of CancerAngiogenesisAngiogenesis
Angiogenesis: formation of new blood vesselsAngiogenesis: formation of new blood vessels Heterotypic signaling and interactionsHeterotypic signaling and interactions11
–– Mitogenic Mitogenic growth factors: HGD, TGF-a, PDGFgrowth factors: HGD, TGF-a, PDGF–– Growth-inhibitory signals: TGF-bGrowth-inhibitory signals: TGF-b–– Trophic Trophic factors: IGF-1 & -2factors: IGF-1 & -2
Tumor Tumor —— ““a wound that never healsa wound that never heals””22
Observation: cancer cells located > 0.2 mm fromObservation: cancer cells located > 0.2 mm fromcapillaries stop growing and become apoptotic orcapillaries stop growing and become apoptotic ornecroticnecrotic3,43,4

Biology of Cancer Biology of Cancer —— Invasion and Metastasis Invasion and MetastasisThe The Angiogenic Angiogenic SwitchSwitch
• Tumor secretion of angiogenic factors stimulates angiogenesis• Neovascularization
– Makes rapid tumor growth possible by supplying oxygenand nutrients and removing waste
– Facilitates metastasis
Ferrara, N. The Oncologist. 2004;9:2. Reprinted with permission.

Biology of CancerBiology of CancerErbB/HER ErbB/HER Receptor Tyrosine Receptor Tyrosine KinasesKinases
Cell Signaling. ErbB/HER Signaling. Available at: http://www.cellsignal.com/reference/pathway/erbB.asp. Accessed October 12, 2006.Copyright 2005 - Cell Signaling Technology, Inc. Reprinted with permission.

Tumor
Inhibitor Angiogenic Inhibition VEGFR Inhibition
Mechanism Inhibits tumor cell growthand blocks synthesis ofangiogenic proteins (eg,EGFR, bFGF, VEGF,TGF-α) by tumor cells
Inhibits endothelial cellsfrom responding to theangiogenic protein VEGF
bFGFVEGFTGF-α
Endothelial cells
Sandler A, Herbst RS. Clin Cancer Res. 2006;12:4421s. Adapted from Herbst RS, et al. J Clin Oncol. 2005;23:2544. Reprintedwith permission from the American Society of Clinical Oncology.
Rationale for Combining Inhibitors of EGFR and VEGFRRationale for Combining Inhibitors of EGFR and VEGFRTargeting Both the Targeting Both the Tumor Tumor and Endothelial Cellsand Endothelial Cells

Biology of CancerBiology of CancerSignaling Control & NetworkingSignaling Control & Networking
Hanahan D, Weinberg RA. Cell. 2000;100:57. Reprinted with permission.
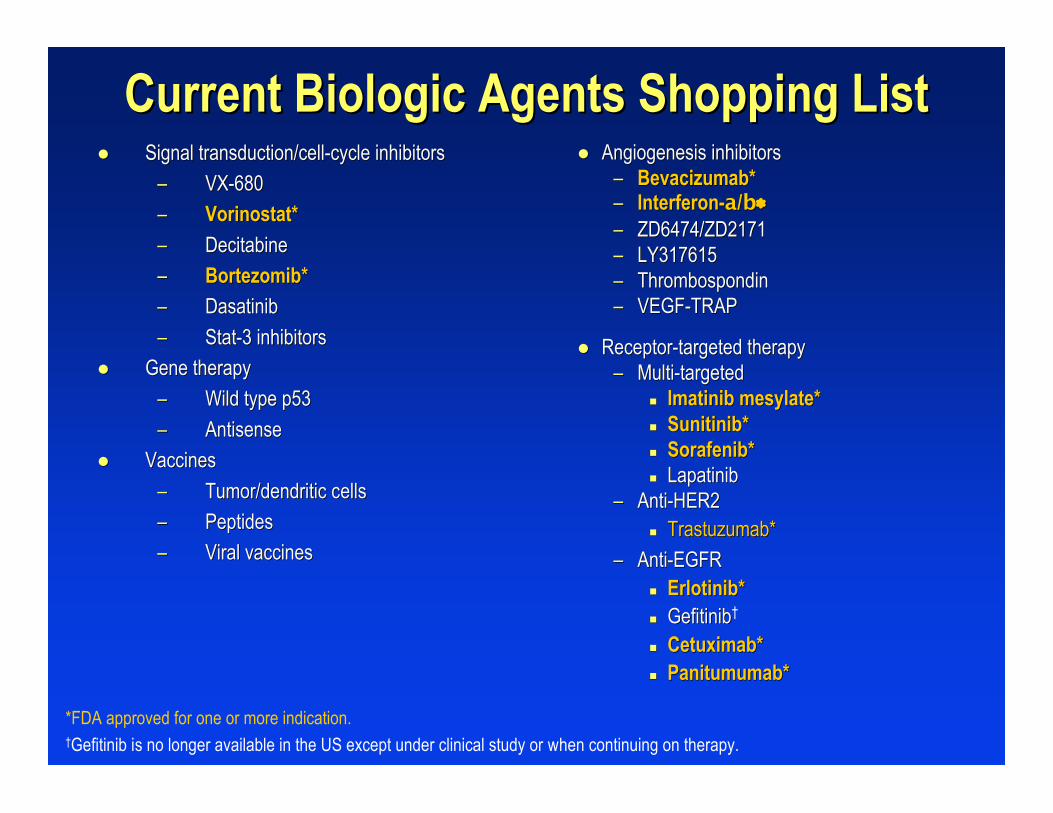
Angiogenesis inhibitorsAngiogenesis inhibitors–– Bevacizumab*Bevacizumab*–– Interferon-Interferon-aa//bb∗∗–– ZD6474/ZD2171ZD6474/ZD2171–– LY317615LY317615–– ThrombospondinThrombospondin–– VEGF-TRAPVEGF-TRAP
Receptor-targeted therapyReceptor-targeted therapy–– Multi-targetedMulti-targeted
Imatinib mesylateImatinib mesylate** SunitinibSunitinib** SorafenibSorafenib** LapatinibLapatinib
–– Anti-HER2Anti-HER2 TrastuzumabTrastuzumab**
–– Anti-EGFRAnti-EGFR Erlotinib*Erlotinib* GefitinibGefitinib†
CetuximabCetuximab** PanitumumabPanitumumab**
*FDA approved for one or more indication.†Gefitinib is no longer available in the US except under clinical study or when continuing on therapy.
Current Biologic Agents Shopping ListCurrent Biologic Agents Shopping List Signal transduction/cell-cycle inhibitorsSignal transduction/cell-cycle inhibitors
–– VX-680VX-680
–– VorinostatVorinostat**
–– DecitabineDecitabine
–– BortezomibBortezomib**
–– DasatinibDasatinib
–– Stat-3 inhibitorsStat-3 inhibitors
Gene therapyGene therapy
–– Wild type p53Wild type p53
–– AntisenseAntisense
VaccinesVaccines
–– Tumor/dendritic Tumor/dendritic cellscells
–– PeptidesPeptides
–– Viral vaccinesViral vaccines

Targeted Therapies in CancerTargeted Therapies in CancerParadigm Shift?Paradigm Shift?
Not a new concept
“Cytostatic vs Cytotoxic”
Modest response rates with single agents
Combination with cytotoxics?
Now with survival data
Who should receive (“Individualized”)?
Where is the best setting (early, sequential)?
Cancer is a “Chronic Disease”
Courtesy of Dr. H. Tran.
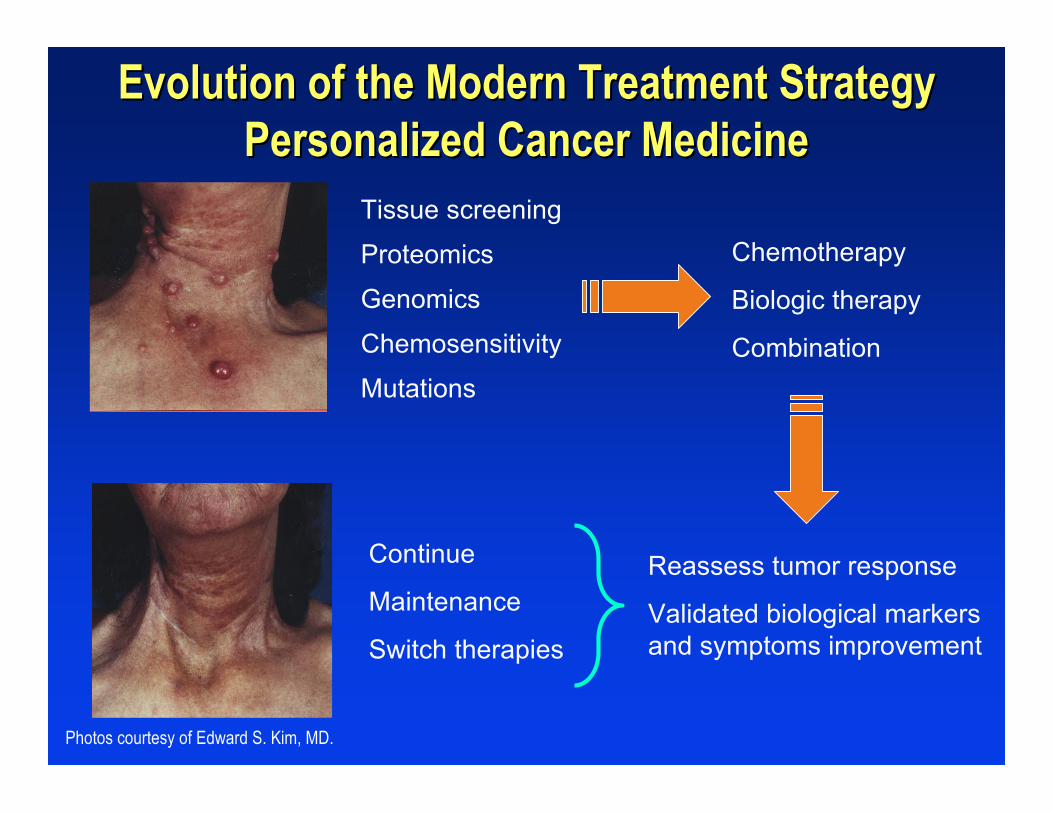
Tissue screening
Proteomics
Genomics
Chemosensitivity
Mutations
Chemotherapy
Biologic therapy
Combination
Reassess tumor response
Validated biological markersand symptoms improvement
Continue
Maintenance
Switch therapies
Evolution of the Modern Treatment StrategyEvolution of the Modern Treatment StrategyPersonalized Cancer MedicinePersonalized Cancer Medicine
Photos courtesy of Edward S. Kim, MD.
How Do TargetedHow Do TargetedTherapies Work?Therapies Work?
Jon D. Herrington, Jon D. Herrington, PharmDPharmD, BCPS, BCOP, BCPS, BCOPHematology/Oncology Clinical SpecialistHematology/Oncology Clinical Specialist
Department of PharmacyDepartment of Pharmacy
Scott & White Memorial HospitalScott & White Memorial Hospital
Temple, TexasTemple, Texas

Purine synthesis Pyrimidine synthesis
Ribonucleotides
Deoxyribonucleotides
DNA
RNA
Proteins
MicrotubulesEnzymes, etc
Etoposide, teniposide
Irinotecan, topotecan
Tyrosine kinase inhibitors
Bortezomib
Monoclonal antibodies
Cytarabine, gemcitabine
Fluorouracil
Fludarabine, cladribine
Chabner BA, et al. Antineoplastic agents. In: Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 11th ed. 2006.Reprinted with permission from the McGraw Hill Companies.
Traditional Chemotherapy TargetsTraditional Chemotherapy Targets
Mercaptopurine
MethotrexateHydroxyurea
Alkylating agents
Anthracyclines
L-asparaginase
Vinca alkaloids
Taxanes
Traditional Chemotherapy AgentsTraditional Chemotherapy Agents
AdvantageAdvantage
–– Activity in certain malignanciesActivity in certain malignancies
DisadvantagesDisadvantages
–– SelectivitySelectivity
Target rapidly dividing cellsTarget rapidly dividing cells
Minimal efficacy in advanced diseaseMinimal efficacy in advanced disease
–– ToxicitiesToxicities

Targeted TherapiesTargeted Therapies
AdvantagesAdvantages–– SelectivitySelectivity
Molecular targetsMolecular targets–– ToxicitiesToxicities
Decreased normal cell destructionDecreased normal cell destruction DisadvantagesDisadvantages
–– UnknownUnknown CombinationsCombinations Dosing regimensDosing regimens
–– Long-termLong-term–– CostCost
Types of Targeted TherapiesTypes of Targeted Therapies
Monoclonal antibodies (Monoclonal antibodies (MoAbsMoAbs))–– Engineered murine/human Engineered murine/human MoAbsMoAbs
that interact with a certain targetthat interact with a certain target MurineMurine ChimericChimeric HumanizedHumanized HumanHuman
Tyrosine kinase inhibitors (Tyrosine kinase inhibitors (TKIsTKIs))–– Small molecule inhibitors that interfereSmall molecule inhibitors that interfere
with TK activationwith TK activation Single inhibitorSingle inhibitor Multitargeted inhibitorMultitargeted inhibitor

TargetsTargets
Circulating targetsCirculating targets
–– egeg, VEGF, VEGF
Transmembrane targetsTransmembrane targets
–– egeg, EGFR, PDGFR, EGFR, PDGFR
Cell-membrane bound targetsCell-membrane bound targets
–– egeg, CD20, CD33, CD20, CD33

Targets for Available AgentsTargets for Available AgentsMonoclonal AntibodiesMonoclonal Antibodies
EGFR/HER1EGFR/HER1PanitumumabPanitumumab77
CD33CD33Gemtuzumab Gemtuzumab ozogamicinozogamicin44
CD52CD52AlemtuzumabAlemtuzumab55
VEGFVEGFBevacizumabBevacizumab99
HER2HER2TrastuzumabTrastuzumab88
EGFR/HER1EGFR/HER1CetuximabCetuximab66
CD20CD20RituximabRituximab11
Ibritumomab Ibritumomab tiuxetantiuxetan22
TositumomabTositumomab, iodine I-131, iodine I-13133
TargetTargetDrugDrug
Rituxan® [PI]. San Francisco, CA: Genentech, Inc; 2006. 2. Zevalin® [PI]. San Francisco, CA: Biogen Idec Inc and Genentech, Inc; 2005. 3. Bexxar® [PI].Research Triangle Park, NC: GlaxoSmithKline; 2005. 4. Mylotarg® [PI]. Philadelphia, PA: Wyeth Pharmaceuticals Inc; 2006. 5. Campath® [PI]. CambridgeMA : Genzyme Corporation; 2005. 6. Erbitux® [PI]. Branchburg, NJ, Princeton, NJ : Imclone Systems Inc and Bristol-Myers Squibb Company; 2006. 7.Vectibix TM [PI]. Thousand Oaks, CA,: Amgen Inc; 2006. 8. Herceptin® [PI]. San Francisco, CA: Genentech, Inc; 2005. 9. Avastin® [PI]. San Francisco, CA:Genentech, Inc; 2006.Courtesy of Dr. J. Herrington.

EGFR/HER1, HER2Lapatinib – investigational3
PDGFRα and β, VEGFR1, 2 and 3, Kit,Flt3, CSF-1R, Ret
Sunitinib7
PDGFRβ, VEGFR 2 and 3, Kit, Flt3, RafSorafenib6
Bcr-abl, Kit, Src family, Epha2, PDGFRβDasatinib5
Bcr-abl, Kit, PDGFRImatinib4
EGFR/HER1Erlotinib2
EGFR/HER1Gefitinib1
TargetDrug
EGFR = epidermal growth factor receptor; HER = human epidermal growth factor receptor; Kit = stem cell factor receptor; PDGFR = platelet derived growth factorreceptor; VEGFR = vascular endothelial growth factor receptors; Flt3 = Fms-like tyrosine kinase-3; CSF-1R = colony stimulating factor receptor Type 1; Ret =glial cell-line derived neutrophic factor receptor.
Iressa® [PI]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2005. 2. Tarceva® [PI]. Melv ille, NY and San Francisco, CA: OSI Pharmaceuticals, Inc andGenentech Inc; 2005. 3. Burris HA, et al. J Clin Oncol. 2005;23:5305. 4. Gleevec® [PI]. East Hanover, NJ: Novartis Pharmaceutical Corporation; 2005. 5.SprycelTM [PI]. Princeton, NJ: Bristol-Myers Squibb Company; 2006. 6. Nexavar® [PI]. West Haven, CT and Emeryv ille, CA: Bayer PharmaceuticalCorporation and Onyx Pharmaceuticals: 2006. 7. Sutent® [PI]. New York, NY: Pfizer Labs; 2006.
Courtesy of Dr. J. Herrington.
Tyrosine Tyrosine Kinase Kinase Inhibitors Molecular TargetsInhibitors Molecular Targets

Baselga J. Science. 2006;312:1175. Reprinted with permission from AAAS.
TrastuzumabHER2Breast cancer
ErlotinibGefitinib
EGFRLung cancer
ImatinibKIT
PDGFRGastrointestinalstromal tumors
ImatinibBCR-ABLChronic myelogenousleukemia
First-GenerationInhibitor
Tyrosine KinaseTargetCancer Type
First-Generation First-Generation TKIs TKIs and and MoAbsMoAbs

Cell Signaling. ErbB/HER Signaling. Available at: http://www.cellsignal.com/reference/pathway/erbB.asp. Accessed October 12, 2006.Copyright 2005 - Cell Signaling Technology, Inc. Reprinted with permission.
ErbB/HER/EGFR ErbB/HER/EGFR Signaling PathwaySignaling Pathway

Reprinted with permission from Krause DS, Van Etten RA. N Engl J Med. 2005;353:172. Copyright 2005 Massachusetts MedicalSociety. All rights reserved.
EGFR = epidermal growth factor receptor; TKI = tyrosine kinase inhibitors.
Targeting TK Receptors andTargeting TK Receptors andTheir Ligands for Cancer TherapeuticsTheir Ligands for Cancer Therapeutics
Overexpression of a normal receptor TK (EGFR), its ligand, or both. TK receptorsand their ligands can be specifically targeted extracellularly by monoclonal antibodiesand intracellularly by TKIs.
Mendelsohn J, Baselga J. Semin Oncol. 2006;33:369.;33;369.
Expected Results from Selective Expected Results from Selective MoAbsMoAbsand and TKIsTKIs
Cell cycle arrestCell cycle arrest
Apoptosis potentiationApoptosis potentiation
Angiogenesis inhibitionAngiogenesis inhibition
Inhibition of tumor cell invasion and metastasisInhibition of tumor cell invasion and metastasis
Chemotherapy and radiotherapy augmentationChemotherapy and radiotherapy augmentation

Gerber H-P, Ferrara N. Cancer Res. 2005;65:671. Reprinted with permission.
Hypothetical Model for Synergism BetweenHypothetical Model for Synergism BetweenCytotoxic Compounds and BevacizumabCytotoxic Compounds and Bevacizumab

Reprinted with permission from Krause DS, Van Etten RA. N Engl J Med. 2005;353:172.Copyright 2005 Massachusetts Medical Society. All rights reserved.
Mechanisms of Resistance to Mechanisms of Resistance to TKIsTKIs

Baselga J. Science. 2006;312:1175. Reprinted with permission from AAAS.
ErlotinibGefitinib
Trastuzumab
Imatinib
Imatinib
First-GenerationInhibitor
LapatinibHER2Breast cancer
IrreversibleInhibitors(EKB569)
EGFRLung cancer
SunitinibKIT
PDGFRGastrointestinalstromal tumors
DasatinibBCR-ABLChronicmyelogenousleukemia
Second-Generation
InhibitorTyrosine Kinase
TargetCancer Type
Second-Generation Second-Generation TKIsTKIs

ConclusionsConclusions
Targeted therapies have revolutionized theTargeted therapies have revolutionized thetreatment of malignanciestreatment of malignancies
Unique mechanisms will allow for future useUnique mechanisms will allow for future usein combination therapiesin combination therapies

Clinical Update: Efficacy and SafetyClinical Update: Efficacy and Safetyof Targeted Therapiesof Targeted Therapies
Cathy Eng, MDCathy Eng, MDAssistant ProfessorAssistant Professor
Department of Gastrointestinal Medical OncologyDepartment of Gastrointestinal Medical Oncology
The University of TexasThe University of Texas
M. D. Anderson Cancer CenterM. D. Anderson Cancer Center
Houston, TexasHouston, Texas

OverviewOverview
Discuss the role of targeted therapies in solid tumorsDiscuss the role of targeted therapies in solid tumors Discuss on-label FDA-approved agents in variousDiscuss on-label FDA-approved agents in various
malignanciesmalignancies–– ColorectalColorectal–– LungLung–– RenalRenal–– Breast cancerBreast cancer
Side effectsSide effects FutureFuture
–– Drugs of interestDrugs of interest

Treatment of Metastatic ColorectalTreatment of Metastatic ColorectalCancer (MCRC):Cancer (MCRC):
anti-VEGF and EGFR Inhibitionanti-VEGF and EGFR Inhibition

Efficacy of Bevacizumab (B)and Cetuximab (C) in MCRC
Phase III Pivotal Trial Results
Cunningham (prior irinotecanexposure)‡
Second-line: Giantonio(bevacizumab-naive)†
First-line: Hurwitz*
Trial
6.9
8.6
1.5
4.1
11
23
Cetuximab
Irinotecan + C
10.8
12.9
4.8
7.2
9
22
FOLFOX
FOLFOX + B
15.6
20.3
6.2
10.6
35
45
IFL
IFL+B
Median OS (mo)Median PFS or
TTP (mo)RR (%)Regimen
Hurwitz HI, et al. N Engl J Med. 2004;350:2335. Giantonio BJ, et al. 41st ASCO; May 13-17, 2005. Abstract 2.Cunningham D, et al. N Engl J Med. 2004;351:337.
*RR comparison, P = .0024; PFS comparison, P < .001; OS comparison, P < .001.†RR comparison, P = <.0001; PFS comparison, P < .05; OS comparison, P < .05.‡RR comparison, P = .007; PFS comparison, P < .001; OS comparison, P = .48.RR = response rate; PFS = progression-free survival; TTP = time to progression; OS = overall survival; IFL = irinotecan + bolus5-fluorouracil/leucovorin; FOLFOX = infusional 5-fluorouracil/leucovorin + oxaliplatin.

Avastin® [PI]. San Francisco, CA: Genentech, Inc; 2006.
FDA June 2006FDA June 2006BevacizumabBevacizumab
Combination with intravenous 5-FUCombination with intravenous 5-FU––based chemotherapy, isbased chemotherapy, isadministered as an intravenous infusion (5 mg/kg or 10 mg/kg)administered as an intravenous infusion (5 mg/kg or 10 mg/kg)every 14 days until disease progressionevery 14 days until disease progression
The recommended dose of bevacizumab when used inThe recommended dose of bevacizumab when used incombination with bolus-IFL is 5 mg/kgcombination with bolus-IFL is 5 mg/kg
The recommended dose of bevacizumab when used inThe recommended dose of bevacizumab when used incombination with FOLFOX-4 is 10 mg/kgcombination with FOLFOX-4 is 10 mg/kg
This announcement does not take into account the dose to beThis announcement does not take into account the dose to beused with FOLFIRI and modified schedules of used with FOLFIRI and modified schedules of FOLFOXFOLFOX——ieie,,FOLFOX6 or FOLFOX7FOLFOX6 or FOLFOX7
IFL = irinotecan + bolus 5-fluorouracil/leucovorin; FOLFOX = infusional 5-fluorouracil/leucovorin + oxaliplatin; FOLFIRI = 5-fluorouracil/leucovorin + irinotecan
Facts of Approved BiologicsMetastatic Colorectal Cancer
CetuximabCetuximab22
–– Acne-type rashAcne-type rash
–– Paronychial Paronychial infectionsinfections
–– Electrolyte imbalance: Mg, CaElectrolyte imbalance: Mg, Ca
–– Hypersensitivity reactionHypersensitivity reaction
–– Weekly administrationWeekly administration
–– Approved for patients whoApproved for patients whohave progressed onhave progressed onirinotecan or irinotecanirinotecan or irinotecanintolerantintolerant
BevacizumabBevacizumab11
–– HypertensionHypertension–– Remote risk of GI perforationRemote risk of GI perforation–– ReversibleReversible
leukoencephalopathyleukoencephalopathysyndromesyndrome
–– Patients with history of Patients with history of ATEsATEsare at higher risk of recurrentare at higher risk of recurrenteventevent
–– q2wk or q3wkq2wk or q3wk–– Approved for front-line orApproved for front-line or
bevacizumab naivebevacizumab naive
1. Avastin® [PI]. San Francisco, CA: Genentech, Inc; 2006.2. Erbitux® [PI]. Branchburg, NJ and Princeton, NJ: Imclone Systems Incorporated and Bristol-Myers Squibb Company; 2006.
GI = gastrointestinal; ATEs = arterial thromboembolic events.
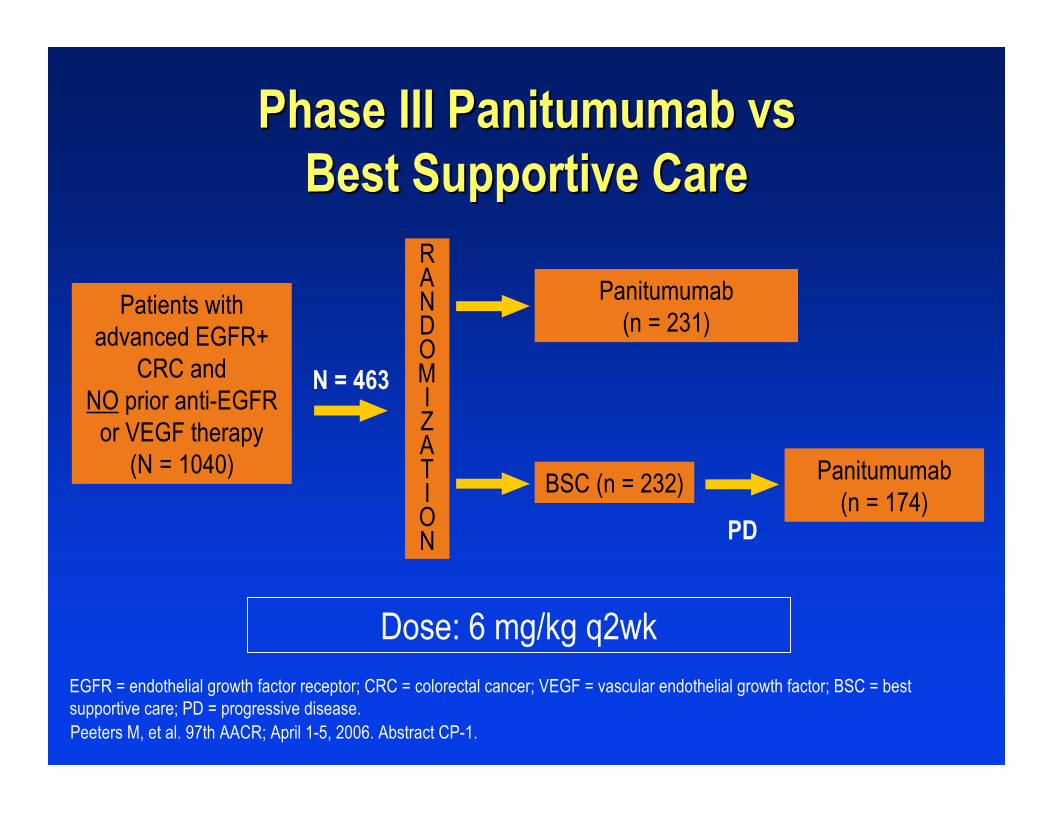
PD
Peeters M, et al. 97th AACR; April 1-5, 2006. Abstract CP-1.
Patients withadvanced EGFR+
CRC andNO prior anti-EGFR
or VEGF therapy(N = 1040)
Panitumumab(n = 231)
BSC (n = 232) Panitumumab(n = 174)
RANDOMIZATION
N = 463
Dose: 6 mg/kg q2wk
Phase III Phase III Panitumumab vsPanitumumab vsBest Supportive CareBest Supportive Care
EGFR = endothelial growth factor receptor; CRC = colorectal cancer; VEGF = vascular endothelial growth factor; BSC = bestsupportive care; PD = progressive disease.

Even
t-Fre
e Pr
obab
ility
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Weeks from Randomization0 8 16 24 32 40 48 56
Hazard ratio = 0.54 (95% CI: 0.44, 0.66)
Stratified log-rank testP < .000000001
Panitumumab
Best Supportive Care (BSC)
Patients at risk:PanitumumabBSC
231 118 49 31 13 5 1232 75 17 7 3 1 1
Panitumumab Panitumumab vs vs Best Supportive CareBest Supportive CareProgression-Free SurvivalProgression-Free Survival
Peeters M, et al. 97th AACR; April 1-5, 2006. Abstract CP-1. Reprinted with permission from Dr. Peeters.

Summary for FDA-Approved Drugs inSummary for FDA-Approved Drugs inMetastatic Colorectal Cancer (MCRC)Metastatic Colorectal Cancer (MCRC)
IFL has been replaced by its infusional counterpart (FOLFIRI)IFL has been replaced by its infusional counterpart (FOLFIRI) Front-line MCRC: bevacizumab + 5-FU based chemotherapyFront-line MCRC: bevacizumab + 5-FU based chemotherapy
(FOLFOX, FOLFIRI, or 5-FU)(FOLFOX, FOLFIRI, or 5-FU) The benefits of continuing bevacizumab following progression areThe benefits of continuing bevacizumab following progression are
unknown. Given the lack of data, its use cannot be advocatedunknown. Given the lack of data, its use cannot be advocatedfollowing progressionfollowing progression
Cetuximab is approved in combination with irinotecan followingCetuximab is approved in combination with irinotecan followingprogression on irinotecan or as a single agent if intolerant toprogression on irinotecan or as a single agent if intolerant toirinotecanirinotecan
Panitumumab was recently approved for the treatment of MCRCPanitumumab was recently approved for the treatment of MCRC(trials compared (trials compared panitumumab vs panitumumab vs BSC)BSC)
Biologics in Lung CancerBiologics in Lung Cancer

NSArm 1: 9.9 moArm 2: 10.1 mo
1) gemcitabine/cisplatin x 6 cycles + erlotinib (150 mg daily)2) gemcitabine/cisplatin
1172TALENT3
NSArm 1: 10.6 moArm 2: 10.5 mo
1) carboplatin/paclitaxel x 6 cycles+ erlotinib (150 mg daily)2) carboplatin/paclitaxel
1059TRIBUTE4
NSArm 1: 8.7 moArm 2: 9.8 moArm 3: 9.9 mo
Carboplatin/paclitaxel x 6 cycles +1) gefinitib 500 mg daily2) gefinitib 250 mg daily3) placebo
1037INTACT 22
NSArms 1&2: 9.9 moArm 3: 10.9 mo
Gemcitabine/cisplatin x 6 cycles +1) gefinitib 500 mg daily2) gefinitib 250 mg daily3) placebo
1093INTACT 11
P-valueMedian OSTreatmentN
1. Giaccone G, et al. J Clin Oncol. 2004;22:777. 2. Herbst RS, et al. J Clin Oncol. 2004;22:785. 3. Gatzemeier U, et al. 40thASCO; June 5-8, 2004. Abstract 7010. 4. Herbst RS, et al, J Clin Oncol. 2005;23:5892.
The Role of Small MoleculeThe Role of Small MoleculeAnti-EGFR Anti-EGFR TKIs TKIs in NSCLCin NSCLC
0 5 10 15 20 25
ErlotinibPlacebo
0
0.2
0.4
0.6
0.8
1.0
0
0.2
0.4
0.6
0.81.0
0 5 10 15 20 25Months on Study
Surv
ival
Rat
e
Months on Study
ErlotinibPlacebo
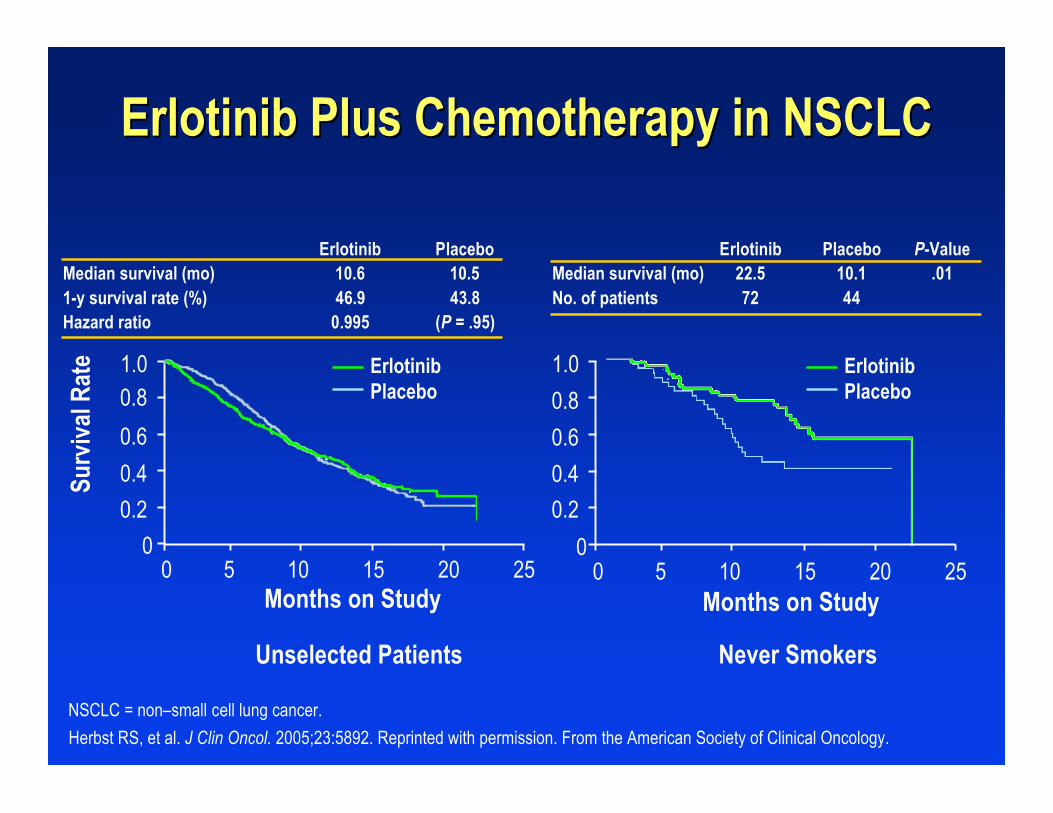
Herbst RS, et al. J Clin Oncol. 2005;23:5892. Reprinted with permission. From the American Society of Clinical Oncology.
Unselected Patients Never Smokers
Erlotinib Plus Chemotherapy in NSCLCErlotinib Plus Chemotherapy in NSCLC
Erlotinib PlaceboMedian survival (mo) 10.6 10.51-y survival rate (%) 46.9 43.8Hazard ratio 0.995 (P = .95)
Erlotinib Placebo P-ValueMedian survival (mo) 22.5 10.1 .01No. of patients 72 44
NSCLC = non–small cell lung cancer.

Sandler AB, et al. 41st ASCO; May 13-17, 2005. Abstract LB4.
• Treatment-naivestage IIIB or IVNSCLC
• No history ofhemoptysis
• No CNSmetastases
• ECOG PS 0–1
Carboplatin (C) AUC = 6 Paclitaxel(P) 200 mg/m2 and
q3wk for 6 cycles withBevacizumab (B) 15 mg/kg
(n = 434)
Carboplatin (C) AUC = 6 Paclitaxel(P) 200 mg/m2 and q3wk for 6 cycles
(n = 444)
RANDOMIZATION
Primary endpoint: OS
6.4 mo vs 4.5 mo(HR = 0.62, 95% CI: 0.53,
0.72, P < .0001)
Median PFS
12.5 mo vs 10.2 mo(HR = 0.77, 95% CI: 0.65, 0.93,
P = .007)27% vs 10% (P < .0001)
Median OSRR
E4599E4599 Phase III Trial of Paclitaxel + CarboplatinPhase III Trial of Paclitaxel + Carboplatin
+/- Bevacizumab in Advanced NSCLC+/- Bevacizumab in Advanced NSCLC

Summary of Biologic Agents in NSCLCSummary of Biologic Agents in NSCLC
4 large phase III studies failed to demonstrate a benefit in4 large phase III studies failed to demonstrate a benefit inoverall survival (OS) with the addition of overall survival (OS) with the addition of gefinitib gefinitib or erlotinib toor erlotinib tostandard chemotherapystandard chemotherapy–– Subset analysis revealed that patients who areSubset analysis revealed that patients who are
nonsmokers and Asians fared betternonsmokers and Asians fared better1,21,2
–– Patients with a mutation in the TK domain of the EGFRPatients with a mutation in the TK domain of the EGFRreceptor have improved OSreceptor have improved OS3-53-5
Exons Exons 18-2118-21–– Erlotinib is currently approved for use in surgicallyErlotinib is currently approved for use in surgically
unresectable NSCLC patientsunresectable NSCLC patients Bevacizumab in combination with Bevacizumab in combination with paclitaxel paclitaxel and and carboplatincarboplatin,,
was approved by the FDA (10/12/06) as first-line therapy forwas approved by the FDA (10/12/06) as first-line therapy forNSCLCNSCLC
1. Thomas SK, et al. Clin Lung Cancer. 2006;7:326. 2. Lim ST, et al. Br J Cancer. 2005;93:23. 3. Riely GJ, et al. Clin Cancer Res.2006;12:839. 4. Takano T, et al. J Clin Oncol. 2005;23:6829. 5. Tsao MS, et al. N Engl J Med. 2005;353:133.

Renal Cell CarcinomaRenal Cell CarcinomaMultitargeted Multitargeted Oral AgentsOral Agents
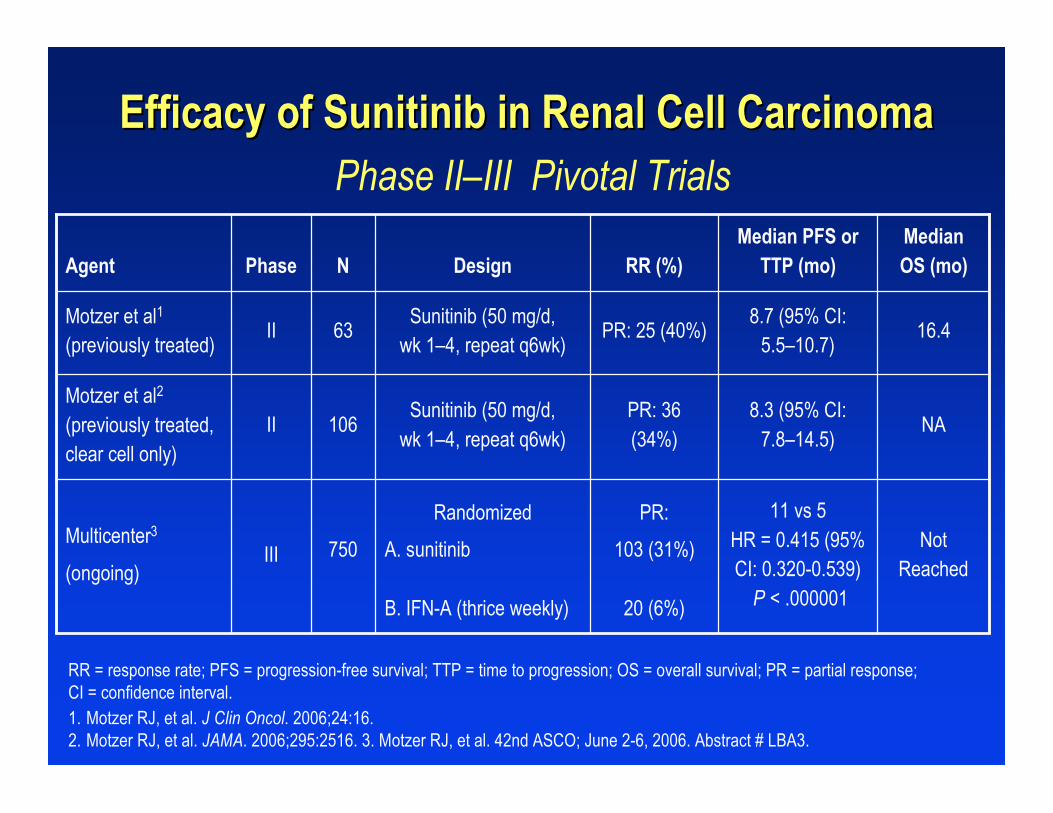
20 (6%)B. IFN-A (thrice weekly)
750
106
63
N
NotReached
11 vs 5HR = 0.415 (95%CI: 0.320-0.539)
P < .000001
PR:
103 (31%)
Randomized
A. sunitinibIIIMulticenter3
(ongoing)
NA8.3 (95% CI:
7.8–14.5)PR: 36(34%)
Sunitinib (50 mg/d,wk 1–4, repeat q6wk)
IIMotzer et al2
(previously treated,clear cell only)
II
Phase
Motzer et al1
(previously treated)
Agent
16.48.7 (95% CI:
5.5–10.7)PR: 25 (40%)
Sunitinib (50 mg/d,wk 1–4, repeat q6wk)
MedianOS (mo)
Median PFS orTTP (mo)RR (%)Design
1. Motzer RJ, et al. J Clin Oncol. 2006;24:16.2. Motzer RJ, et al. JAMA. 2006;295:2516. 3. Motzer RJ, et al. 42nd ASCO; June 2-6, 2006. Abstract # LBA3.
Efficacy of Sunitinib in Renal Cell CarcinomaEfficacy of Sunitinib in Renal Cell Carcinoma Phase II–III Pivotal Trials
RR = response rate; PFS = progression-free survival; TTP = time to progression; OS = overall survival; PR = partial response;CI = confidence interval.

PD
Eisen T, et al. 42nd ASCO; June 2-6, 2006. Abstract 4524.
Clear cell cancer patients,failed 1 prior therapy
< 8 mo prior,ECOG PS 0–1
Sorafenib 400 mg PO BID(n = 451)
Placebo(n = 452)
Sorafenib(n = 200)
RANDOMIZATION
Primary endpoint: OS
19.3 vs 15.9 moHR = 0.77
(95% CI: 0.63–0.95)P = .015
Median OS (mo):6-mo Postcrossover
19.3 vs 14.3 moHR = 0.74
(95% CI: 0.58–0.93)P = .01
24 wk vs 12 wkHR = 0.44
(95% CI = 0.35–0.55)P < .000001
Median OS (mo): with CensoredPlacebo Arm
Median PFS or TTP (mo)
Efficacy of Sorafenib in Renal Cell CarcinomaEfficacy of Sorafenib in Renal Cell Carcinoma Pivotal Phase III Trial (TARGET)Pivotal Phase III Trial (TARGET)
SunitinibSunitinib11
NauseaNausea
DiarrheaDiarrhea
StomatitisStomatitis
HyperlipasemiaHyperlipasemia
NeutropeniaNeutropenia
FatigueFatigue
Decrease in LVEFDecrease in LVEF(rare)(rare)
SorafenibSorafenib22
RashRash
FatigueFatigue
DyspneaDyspnea
HypertensionHypertension
1. Sutent® PI, Pfizer Labs, New York, NY, February 2006.2. Nexavar® PI, Bayer Pharmaceutical Corporation, West Haven, CT, Onyx Pharmaceuticals, Emeryville, CA, August 2006.
Associated Side EffectsAssociated Side EffectsSunitinib and SorafenibSunitinib and Sorafenib

Summary of Biologic AgentsSummary of Biologic Agentsin Metastatic Renal Cell Cancerin Metastatic Renal Cell Cancer
Both sunitinib and sorafenib clearly have a roleBoth sunitinib and sorafenib clearly have a rolein previously treated renal cell cancer and arein previously treated renal cell cancer and arecurrently FDA approvedcurrently FDA approved
Additional biologic agents are currently beingAdditional biologic agents are currently beingevaluated and have demonstrated promisingevaluated and have demonstrated promisingactivityactivity

Biologics in Breast CancerBiologics in Breast Cancer

Miller KD, et al. 41st ASCO; May 13-17, 2005. Late-breaking session.
RANDOMIZATION
Paclitaxel 90 mg/m2 d 1, 8, 15of 28-d cycle
Paclitaxel 90 mg/m2
d 1, 8,15 of 28-d cycle +Bevacizumab 10 mg/kg d 1, 15
715 recurrent/metastatic breastcancer patients
E2100E2100Phase III Trial of Paclitaxel +/- Bevacizumab as First-LinePhase III Trial of Paclitaxel +/- Bevacizumab as First-Line
Therapy in Recurrent or Metastatic Breast CancerTherapy in Recurrent or Metastatic Breast Cancer
28%14%Response rate
11 months6 monthsOverall survival
(n = 330)(n = 316)
Paclitaxel + BevacizumabPaclitaxel

RANDOMIZATION
Capecitabine (2000 mg/m2/d) + lapatinib(1250 mg/d), d 1–14, repeat q21d
315 locally advanced ormetastatic Her 2+
cancer patients withrecurrent disease
Capecitabine (2500 mg/m2/d)d 1–14, repeat q21d
P = .00016
P-value
36.9 weeks vs 19.7 weeks
Median TTP
Geyer CE, et al. ASCO 2006. Abstract, SPS23.
EGF 100151EGF 100151Phase III Trial of Capecitabine +/- Lapatinib as Second-Phase III Trial of Capecitabine +/- Lapatinib as Second-Line Therapy in Recurrent or Metastatic Breast CancerLine Therapy in Recurrent or Metastatic Breast Cancer
TTP = time to tumor progression.

Geyer CE, et al. ASCO 2006. Abstract, SPS23.
Side Effects of LapatinibSide Effects of Lapatinib
DiarrheaDiarrhea
Palmar-plantar erythrodysesthesiaPalmar-plantar erythrodysesthesia
RashRash
Decreased left ventricular ejectionDecreased left ventricular ejectionfractionfraction

Summary of Biologic AgentsSummary of Biologic Agentsin Metastatic Breast Cancerin Metastatic Breast Cancer
Both bevacizumab and lapatinib haveBoth bevacizumab and lapatinib havedemonstrated advantages in metastatic anddemonstrated advantages in metastatic andrecurrent breast carcinomarecurrent breast carcinoma
Final data have yet to be reported on both ofFinal data have yet to be reported on both ofthese studiesthese studies
Neither bevacizumab nor lapatinib is currentlyNeither bevacizumab nor lapatinib is currentlyFDA approved for this indicationFDA approved for this indication

IIIAZD 2171, GW783034
(pazopanib)VEGFR 1-3
IIIAG-013736 (axitinib)VEGFR 1-3, PDGFR,
c-Kit
IIIZD6474 (vandetanib)EGFR/VEGFR-2
IIVEGF TrapVEGF-A, B, PIGF
Phase of DevelopmentName of DrugMolecular Target
CCI-779 (temsirolimus),RAD001 (everolimus)
Dasatinib, AZD0530
IIImTOR
II Src Kinase
New Agents on the HorizonNew Agents on the Horizonin Solid Tumorsin Solid Tumors
Courtesy of Dr. C. Eng.

Present and Future Role of TargetedPresent and Future Role of TargetedTherapies in Cancer CareTherapies in Cancer Care
Tarek MekhailTarek Mekhail, , MD, MD, MScMSc, FRCSI, , FRCSI, FRCSEdFRCSEd
Director, Lung Cancer Medical Oncology ProgramDirector, Lung Cancer Medical Oncology Program
Hematology/Medical OncologyHematology/Medical Oncology
The Cleveland ClinicThe Cleveland Clinic
Cleveland,Cleveland, OhioOhio

Drug Development ParadigmDrug Development Paradigm
Identifying a therapeutic targetIdentifying a therapeutic target
Preclinical activityPreclinical activity
Clinical drug developmentClinical drug development

Targeted TherapyTargeted Therapy
Anti-EGFRblocking
antibodies
Antiligandblocking
antibodies
Tyrosinekinase
inhibitors Ligand-toxin
conjugates
HER dimerizationinhibitors
TOXIN
Adapted from Noonberg SB, Benz CC. Drugs. 2000;59:753, with permission.

*Day 1 of treatment defined as tumor size 5–6 mm (3–5 days postimplantation).
Adapted from Sirotnak FM, et al. Clin Cancer Res. 2000;6:4885, with permission.
Control
Paclitaxel 25 mg/kgGefitinib 50 mg/kg
Gefitinib + paclitaxel
0
200
400
600
800
1000
1200
0 4 8 12 16 20 24 28 32 36Days Postimplantation
Tum
or V
olum
e (m
m3 )
Gefitinib + PaclitaxelGefitinib + PaclitaxelResponse in LX-1 Lung Tumor Xenografts withResponse in LX-1 Lung Tumor Xenografts with
Low Expression of Wild-Type HER1/EGFRLow Expression of Wild-Type HER1/EGFRP = paclitaxel d 1, 4, 8, and 11*
G = gefitinib d 1–5 and 8–12*
P P P P
G
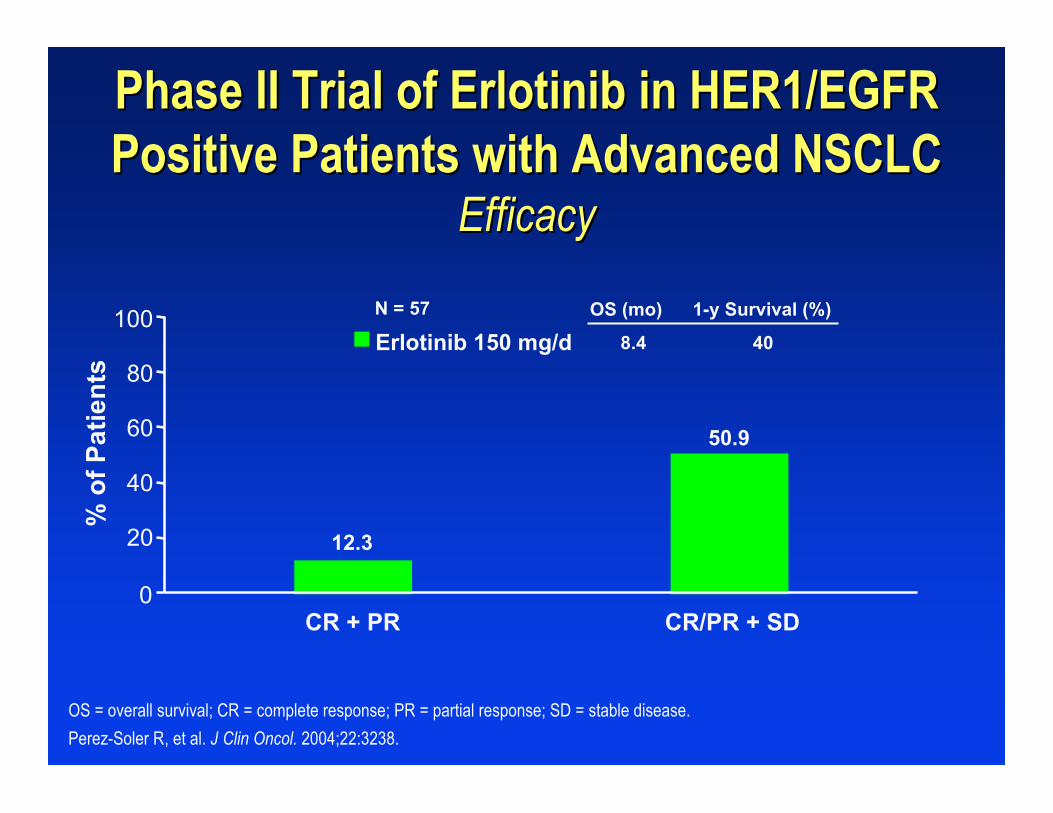
Erlotinib 150 mg/d
CR + PR CR/PR + SD
% o
f Pat
ient
s
100
80
60
40
20
0
8.4 40
OS (mo) 1-y Survival (%)
Phase II Trial of Erlotinib in HER1/EGFRPhase II Trial of Erlotinib in HER1/EGFRPositive Patients with Advanced NSCLCPositive Patients with Advanced NSCLC
EfficacyEfficacy
OS = overall survival; CR = complete response; PR = partial response; SD = stable disease.
Perez-Soler R, et al. J Clin Oncol. 2004;22:3238.
N = 57
12.3
50.9

BR.21BR.21Phase III Trial of Phase III Trial of Erlotinib Erlotinib for Advanced for Advanced NSCLCNSCLC——SchemaSchema
End PointsPrimary: overall survivalSecondary: progression-free survival, overall response rate, duration of response, quality of life, safety
Erlotinib 150 mg/dn = 488
Placebon = 243
RANDOMIZE
*2:1 randomization to the experimental arm.PS = performance status; CR = complete response; PR = partial response; SD = stable disease;PD = progressive disease.
Shepherd FA, et al. N Engl J Med. 2005;353:123.
Locally advanced or metastatic NSCLCPS 0–3≥1 failed prior chemotherapy regimenNo prior malignancies or uncontrolled CNS metastases except basal cell skin cancersStratified by
• Center• PS (0/1 vs 2/3)• Response to prior therapy
(CR/PR:SD:PD)• Prior regimens (1 vs 3)• Prior platinum (yes vs no)
N = 731*

HR = hazard ratio.
Adapted from Shepherd FA, et al. N Engl J Med. 2005;353:123, with permission from the Massachusetts Medical Society.Copyright 2005. All rights reserved.
BR.21BR.21Phase III Trial of Phase III Trial of Erlotinib Erlotinib for Advancedfor Advanced
NSCLCNSCLC——Overall Overall SurvivalSurvival
MedianSurvival (mo)
1-YearSurvival (%)
6.7 31
4.7 22
Erlotinib
Placebo
Months
0 6 12 18 24 30
100
80
60
40
0
20
Ove
rall
Su
rviv
al (
% P
atie
nts
)
HR = 0.70, P < .001

Ran
dom
izat
ion
Docetaxel + cetuximab
Pemetrexed
2nd- or 3rd-line therapyfor NSCLC
No priorEGFR,
docetaxel, orpemetrexed
Multicenter StudyN = 800Open
Primary Endpoint = Response
Pemetrexed + cetuximab
Docetaxel
http://clinicaltrials.gov
Phase III NSCLC Registration TrialPhase III NSCLC Registration TrialDocetaxel Docetaxel or or Pemetrexed Pemetrexed +/- +/- CetuximabCetuximab
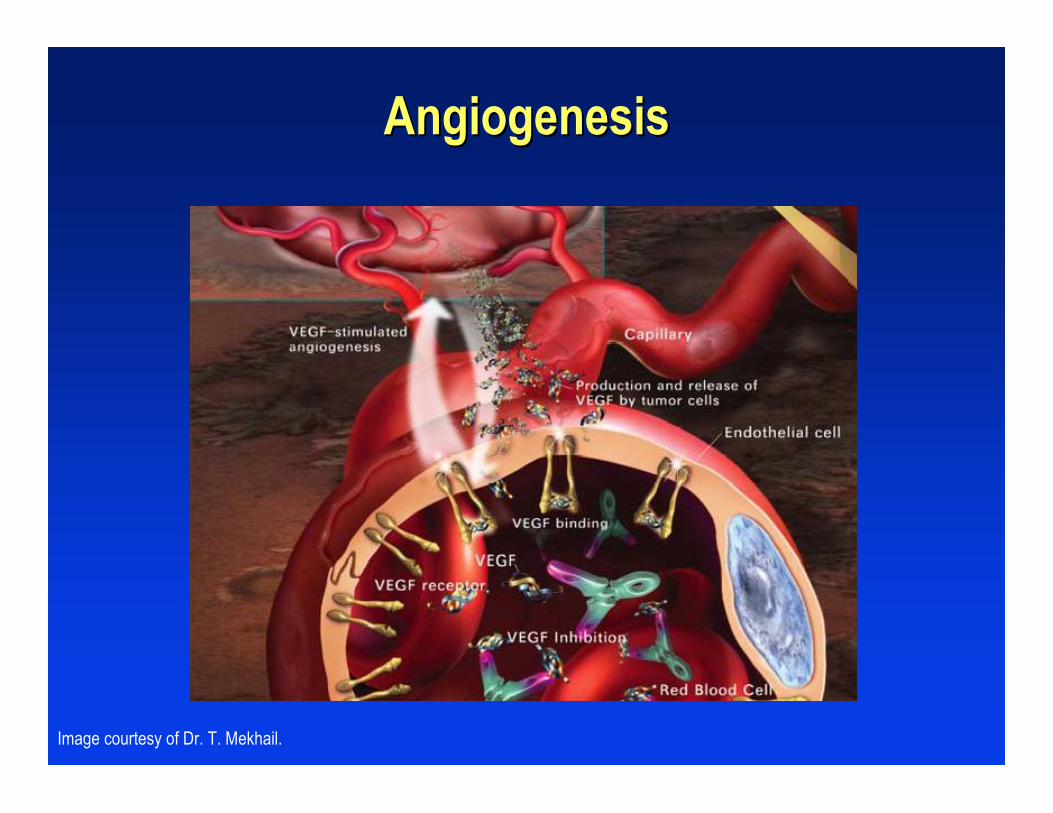
Image courtesy of Dr. T. Mekhail.
AngiogenesisAngiogenesis

The Angiogenic Switch Is a Key Step forThe Angiogenic Switch Is a Key Step forTumor Growth and Risk of MetastasisTumor Growth and Risk of Metastasis
Angiogenicswitch
100 µm
Small tumor Nonvascular “Dormant”
Larger tumor Vascular Metastatic potential
Adapted from Ferrara, N. The Oncologist. 2004;9:2. Reprinted with permission.
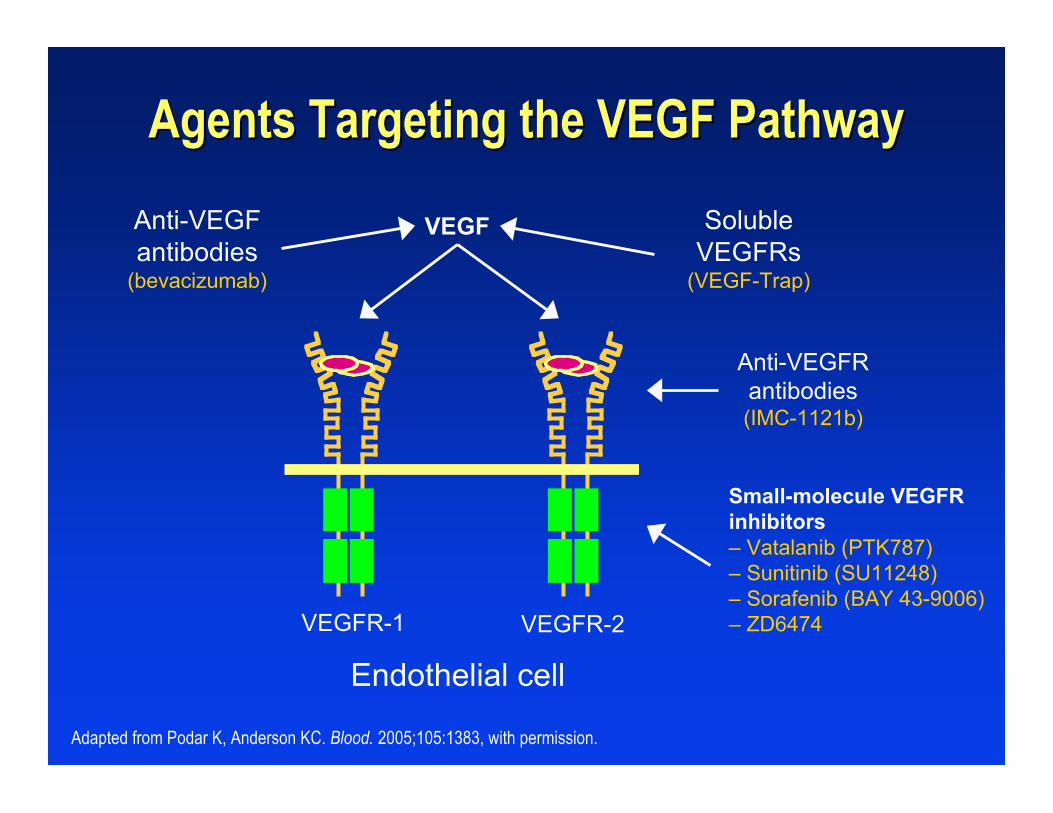
Agents Targeting the VEGF PathwayAgents Targeting the VEGF Pathway
VEGFR-2VEGFR-1
Endothelial cell
Small-molecule VEGFRinhibitors– Vatalanib (PTK787)– Sunitinib (SU11248)– Sorafenib (BAY 43-9006)– ZD6474
Anti-VEGFRantibodies(IMC-1121b)
VEGFAnti-VEGFantibodies
(bevacizumab)
SolubleVEGFRs
(VEGF-Trap)
Adapted from Podar K, Anderson KC. Blood. 2005;105:1383, with permission.

BevacizumabBevacizumab
Recombinant humanizedRecombinant humanizedmonoclonal IgGmonoclonal IgG11 antibody antibody11
Recognizes all isoforms ofRecognizes all isoforms ofVEGF-AVEGF-A22
Estimated half-lifeEstimated half-lifeis approximately 20 daysis approximately 20 days(range, 11(range, 11––50)50)11
1Avastin [package insert] San Francisco, CA: Genentech; 2006.2Presta JL, et al. Cancer Res. 1997;57:4593.Image courtesy of Dr. T. Mekhail.
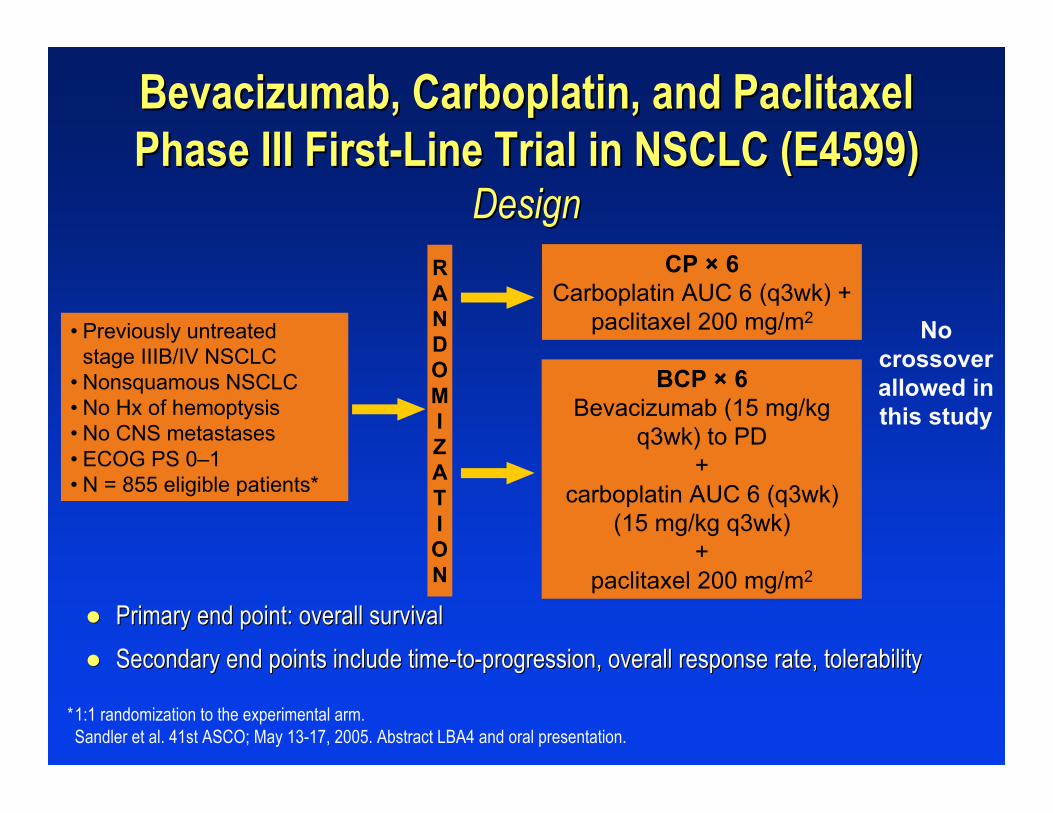
Bevacizumab, Carboplatin, and PaclitaxelBevacizumab, Carboplatin, and PaclitaxelPhase III First-Line Trial in NSCLC (E4599)Phase III First-Line Trial in NSCLC (E4599)
DesignDesignCP × 6
Carboplatin AUC 6 (q3wk) +paclitaxel 200 mg/m2
BCP × 6Bevacizumab (15 mg/kg
q3wk) to PD+
carboplatin AUC 6 (q3wk)(15 mg/kg q3wk)
+paclitaxel 200 mg/m2
Nocrossoverallowed inthis study
Primary end point: overall survivalPrimary end point: overall survival
Secondary end points include time-to-progression, overall response rate, tolerabilitySecondary end points include time-to-progression, overall response rate, tolerability
*1:1 randomization to the experimental arm.Sandler et al. 41st ASCO; May 13-17, 2005. Abstract LBA4 and oral presentation.
RANDOMIZATION
• Previously untreatedstage IIIB/IV NSCLC
• Nonsquamous NSCLC• No Hx of hemoptysis• No CNS metastases• ECOG PS 0–1• N = 855 eligible patients*

0 6 12 18 24 30 36
Months
Medians: 10.2, 12.5
12 mo 24 mo 43.7% 16.9% 51.9% 22.1%
HR = 0.77 (0.65, 0.93)
P = .007
0
0.2
0.4
0.6
0.8
1.0
Prob
abili
ty
CPBCP
Bevacizumab, Carboplatin, and PaclitaxelBevacizumab, Carboplatin, and PaclitaxelPhase III First-Line Trial in NSCLC (E4599)Phase III First-Line Trial in NSCLC (E4599)
Overall SurvivalOverall Survival
Sandler AB, et al. 41st ASCO; May 13-17, 2005. Abstract LBA4 and oral presentation. Reprinted with permission from the AmericanSociety of Clinical Oncology.

The FutureThe Future
Combination therapyCombination therapy
Multitargeted Multitargeted agentsagents
Clinical markers for responseClinical markers for response
Molecular markers for responseMolecular markers for response

Bevacizumab + ErlotinibBevacizumab + ErlotinibPhase I/II Trial in Recurrent NSCLC (OSI2486)Phase I/II Trial in Recurrent NSCLC (OSI2486)
Overall Overall Antitumor Antitumor Activity*Activity*
*By RECIST criteria (N = 40).† Total population.
Herbst RS, et al. J Clin Oncol. 2005;23:2544. Reprinted with permission from the American Society of Clinical Oncology.
26 (65)SD
8 (20)PR
6 (15)PD
0CR
No. of Patients (%)Best Response (N = 40†)

Phase I/II Trial of Phase I/II Trial of Bevacizumab Bevacizumab + + ErlotinibErlotinibin Recurrent NSCLCin Recurrent NSCLCCase History (Phase I)Case History (Phase I)
Pretreatment with Bevacizumab + Erlotinib
Posttreatment with Bevacizumab + Erlotinib
48-year-old African-American male with stage IIIB adenocarcinoma with pleural effusion CT scans at baseline and following 2 cycles of therapy (dose level I)
Herbst RS, et al. J Clin Oncol. 2005;23:2544. Reprinted with permission from the American Society of Clinical Oncology.

Heymach JV, et al. J Clin Oncol. 2005;23:3025.
Multitargeted Multitargeted ApproachesApproachesZD6474 in Advanced NSCLCZD6474 in Advanced NSCLC
Orally available inhibitor of 2 key pathways in tumor growthOrally available inhibitor of 2 key pathways in tumor growth
–– VEGFR-dependent tumor angiogenesisVEGFR-dependent tumor angiogenesis
–– EGFR-dependent tumor cell proliferation and survivalEGFR-dependent tumor cell proliferation and survival
Number of randomized phase II trials ongoing/completedNumber of randomized phase II trials ongoing/completed
–– ZD6474 vs gefitinibZD6474 vs gefitinib
–– Docetaxel +/- ZD6474Docetaxel +/- ZD6474
–– 3 arms: ZD6474 alone vs paclitaxel/carboplatin +3 arms: ZD6474 alone vs paclitaxel/carboplatin +ZD6474 or placeboZD6474 or placebo

Clinical Markers for Response BR.21Clinical Markers for Response BR.21Exploratory AnalysisExploratory Analysis——Survival by Smoking HistorySurvival by Smoking History
Never Smoked Current and Ex-smokers
HR = 0.42 (95% CI, 0.28–0.64)ORR = 24.7%
HR = 0.87 (95% CI, 0.71–1.05)ORR = 3.9%
Months0 5 10 15 20 25
Months
% S
urv
ival
0 5 10 15 20 25
100
80
60
40
0
20
100
80
60
40
0
20
Placebo(n = 42)
Erlotinib(n = 104)
Placebo(n = 187)
Erlotinib(n = 358)
% S
urv
ival
HR = hazard ratio; CI = confidence interval; ORR = overall response rate.
Reprinted from Clin Lung Cancer, 7, Clark GM, et al, Smoking History and Epidermal Growth Factor Receptor Expression asPredictors of Survival Benefit from Erlotinib for Patients with Non-Small-Cell Lung Cancer in the National Cancer Institute of CanadaClinical Trials Study BR.21, pp 389-394, Copyright © 2006, with permission from Cancer Information Group.
Molecular Markers for ResponseMolecular Markers for Response
EGFR mutation status by gene sequencingEGFR mutation status by gene sequencing
EGFR gene copy number by fluorescenceEGFR gene copy number by fluorescencein situ hybridizationin situ hybridization
EGFR protein expression byEGFR protein expression byimmunohistochemistryimmunohistochemistry

b pVHL HIF=a
VEGFR EGFRPDGFR
Sunitinib, Sorafenib,AG-013736
Sorafenib
Bevacizumab
RAF
Erlotinib
Kaelin WG. Nat Rev Cancer. 2002;2:673. Reprinted with permission.
Renal Cell CarcinomaRenal Cell CarcinomaTargets of Single AgentsTargets of Single Agents
VEGF TGF-aPDGF
RAFSorafenib

1. Nexavar® [package insert]. West Haven, CT: Bayer Pharmaceuticals Corporation; and Emeryville, CA: Onyx Pharmaceuticals;2006. 2. Sutent [package insert]. New London, CT: Pfizer Labs; 2006. 3. Rugo HS, et al. J Clin Oncol. 2005;23:5474. 4. Avastin[package insert]. San Francisco, CA: Genentech Inc, 2006. 5. Atkins MB, et al. J Clin Oncol. 2004;22:909.
Molecular Targeted Therapies for RCCMolecular Targeted Therapies for RCCTarget InhibitionTarget Inhibition
SorafenibSorafenib11
–– VEGFR, PDGFR, RAFVEGFR, PDGFR, RAF SunitinibSunitinib22
–– VEGFR, PDGFRVEGFR, PDGFR AG-013736AG-01373633
–– VEGFR, PDGFRVEGFR, PDGFR BevacizumabBevacizumab44
–– VEGFVEGF Temsirolimus Temsirolimus (CCI-779)(CCI-779)55
–– mTORmTOR
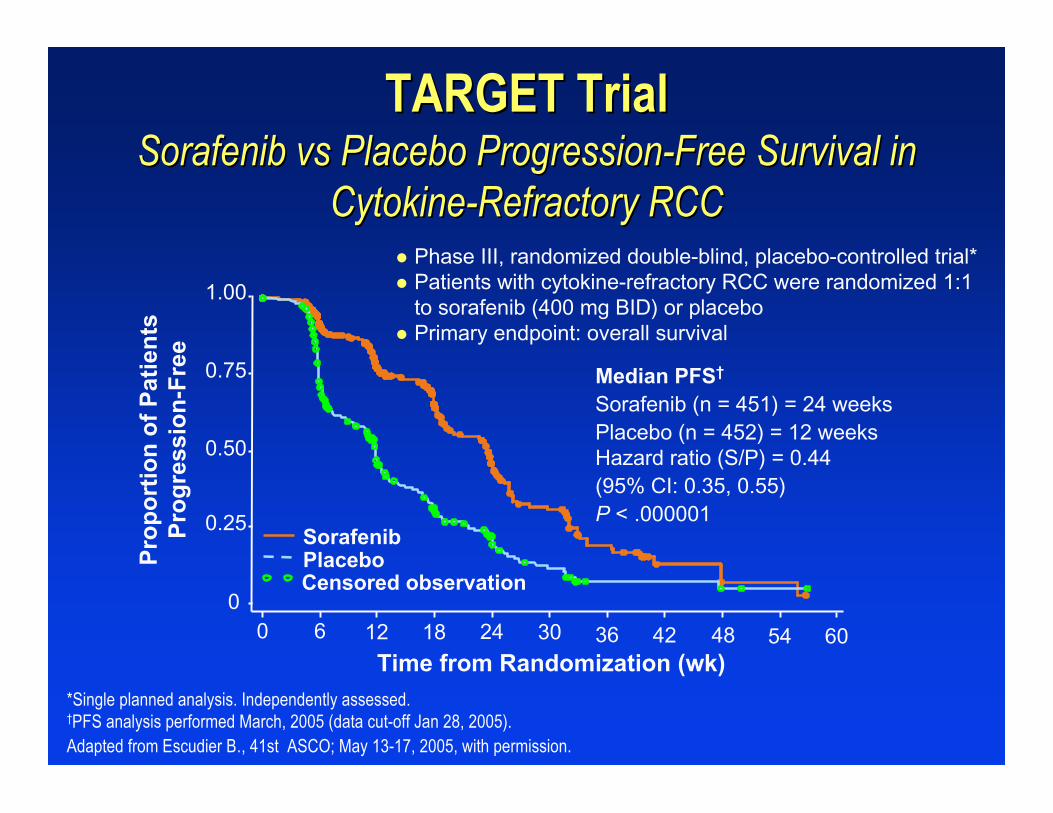
*Single planned analysis. Independently assessed.†PFS analysis performed March, 2005 (data cut-off Jan 28, 2005).Adapted from Escudier B., 41st ASCO; May 13-17, 2005, with permission.
Pro
po
rtio
n o
f P
atie
nts
Pro
gre
ssio
n-F
ree
0
0.25
0.50
0.75
1.00
Median PFS†
Sorafenib (n = 451) = 24 weeksPlacebo (n = 452) = 12 weeksHazard ratio (S/P) = 0.44(95% CI: 0.35, 0.55)P < .000001
0 6054484236302418126
Time from Randomization (wk)
PlaceboSorafenib
Censored observation
Phase III, randomized double-blind, placebo-controlled trial* Patients with cytokine-refractory RCC were randomized 1:1
to sorafenib (400 mg BID) or placebo Primary endpoint: overall survival
TARGET TrialTARGET TrialSorafenib Sorafenib vs vs Placebo Progression-Free Survival inPlacebo Progression-Free Survival in
Cytokine-Refractory RCCCytokine-Refractory RCC

21 June 2005 17 October 2005
Escudier B, et al. Eur J Cancer Suppl. 2005;3:226 (abstract 794). Reprinted with permission.
TARGET TrialTARGET TrialTumor ResponseTumor Response
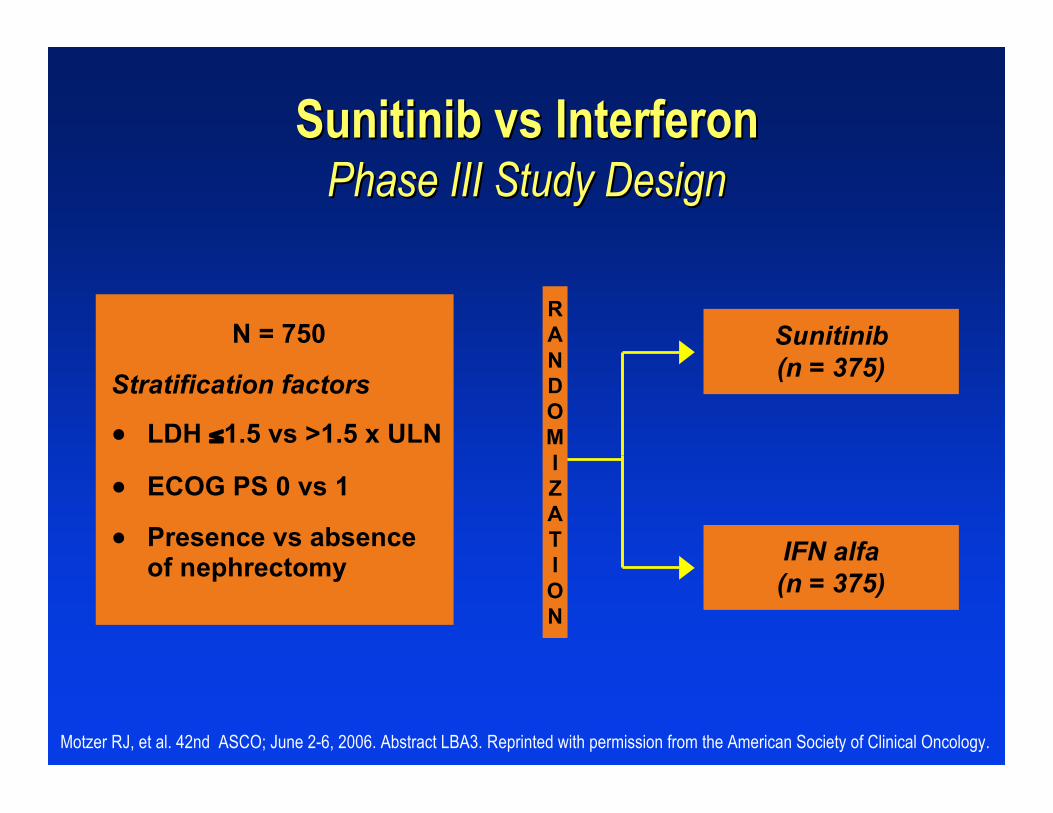
Sunitinib Sunitinib vs vs InterferonInterferonPhase III Study DesignPhase III Study Design
N = 750
Stratification factors
● LDH ≤1.5 vs >1.5 x ULN
● ECOG PS 0 vs 1
● Presence vs absenceof nephrectomy
Sunitinib(n = 375)
IFN alfa(n = 375)
Motzer RJ, et al. 42nd ASCO; June 2-6, 2006. Abstract LBA3. Reprinted with permission from the American Society of Clinical Oncology.
RANDOMIZATION
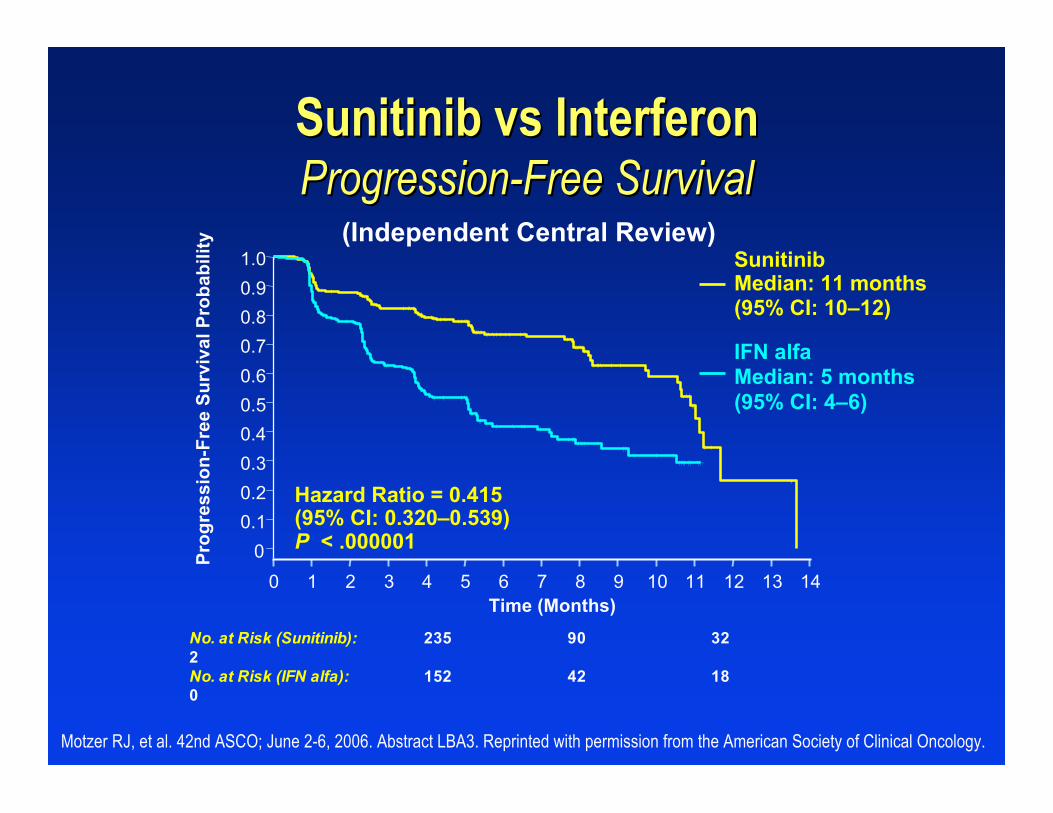
Sunitinib Sunitinib vs vs InterferonInterferonProgression-Free SurvivalProgression-Free Survival
Motzer RJ, et al. 42nd ASCO; June 2-6, 2006. Abstract LBA3. Reprinted with permission from the American Society of Clinical Oncology.
No. at Risk (Sunitinib): 235 90 322No. at Risk (IFN alfa): 152 42 180
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14Time (Months)
00.10.20.30.40.50.60.70.80.91.0
Prog
ress
ion-
Free
Sur
viva
l Pro
babi
lity
SunitinibMedian: 11 months(95% CI: 10–12)
IFN alfa Median: 5 months(95% CI: 4–6)
Hazard Ratio = 0.415(95% CI: 0.320–0.539)P < .000001
(Independent Central Review)

Most Common SideMost Common Side Effects AssociatedEffects Associatedwith Marketed Targeted Agentswith Marketed Targeted Agents
Diarrhea, hypertension, bleeding, mucositis, skin abnormalities,altered taste
Sunitinib6
Rash, diarrhea, hand-foot skin reaction, fatigue, hypertension,alopecia
Sorafenib5
Diarrhea, rash, acne, dry skin, nausea, vomitingGefitinib4
Rash, diarrhea, anorexia, fatigue, dyspnea, coughErlotinib3
Acneform rash, asthenia/malaise, diarrhea, nausea, abdominalpain, vomiting
Cetuximab2
Asthenia, pain, abdominal pain, headache, hypertension,diarrhea, nausea, vomiting
Bevacizumab1
Most Common ToxicitiesAgent
1. Avastin [package insert] San Francisco, CA: Genentech; 2006. 2. Erbitux® [package insert]. Branchburg, NJ: Imclone SystemsIncorporated; and Princeton, NJ: Bristol-Myers Squibb Company; 2006. 3. Tarceva™ [package insert]. Melville, NY: OSIPharmaceuticals Inc, and Genentech, Inc; 2005. 4. Iressa [package insert]. Wilmington, DE: AstraZeneca; 2005. 5. Nexavar®
[package insert]. West Haven, CT: Bayer Pharmaceuticals Corporation; and Emeryville, CA: Onyx Pharmaceuticals; 2006.6. Sutent [package insert]. New London, CT: Pfizer Labs; 2006.
Raising The BarRaising The BarToxicity ProfileToxicity Profile
Absence of traditional side effectsAbsence of traditional side effects
Manageable toxicityManageable toxicity

The FutureThe Future
Overcoming evolving resistanceOvercoming evolving resistance
Combination with other agentsCombination with other agents
Treatment of earlier stage of the diseaseTreatment of earlier stage of the disease
Individualizing treatmentIndividualizing treatment
Cure!Cure!