university of tennessee 6.doc · web viewhealth science center. doctoring: recognizing signs and...
TRANSCRIPT
UNIVERSITY OF TENNESSEEHEALTH SCIENCE CENTER
Doctoring: Recognizing Signs and Symptoms
(DRS)
Topics:
Neurologic SystemMental Status Evaluation
Chapter 6August 13-17, 2007

DRS M-2 Grading System for 2007-2008
Chapter 6 August 13-17, 2007 Topics: Neurologic exam Mini-mental statusMonday Checklist 2%Preceptor 2%Master Clinicians 2%Standardized Patient Encounter and Documentation (SPED) 8%
14%
Chapter 7 September 17-21, 2007 Topics: Skin and lymph, Sexual historyMonday Checklist 2%Preceptor 2%Master Clinicians 2%SOAP note assignment 8%
14%
Chapter 8 October 22-26, 2007 Topics: Heart ProfessionalismMonday Checklist 2%Preceptor 3%Master Clinicians 2%Professionalism Assignment 1%SOAP note assignment 8%
16%
Chapter 9 February 4-8, 2008 Topics: EyeMonday Checklist 2%Preceptor 3%Master Clinicians 2%Rounding 1%SPED 8%
16%
Week 10 March 17-20, 2008
End-Of- Year Assessment 40%40%
2

M-2 DRS Student Evaluation Policy
The M-2 DRS is a graded 4 credit hour course.
The major goal of the course is to provide a basic foundation of clinical skills and knowledge that you will draw upon throughout your professional career. Grade determinants for the course are outlined below.
FoundationsProfessionalism Criteria for building this foundation are explained in the document entitled “Code
of Professional Conduct” which can be accessed in the Course Overview section of the Class of 2010 DRS Blackboard site.
Non-adherent students will be counseled. Chronically non-adherent students will have their overall course grade lowered and may not pass the course.
Participation All graded/non-graded assignments and surveys/evaluations must be turned in by
the due dates indicated in the course materials. Participation in ALL M-2 DRS learning activities.
Non-adherent students will be counseled. Chronically non-adherent students will have their overall course grade lowered and may not pass the course.
Attendance Students are expected to attend ALL scheduled M-2 DRS sessions including all
lectures, small group sessions, and sessions with the community preceptor. Non-adherent students will be counseled. Chronically non-adherent students will
have their overall course grade lowered and may not pass the course.Determinants
M-2 DRS grades will be determined on the basis on 100 total percentage points as follows:
End of Year Assessment 40Graded Assignments 34Community Preceptor Visits 10Monday & Thursday Small Groups 16
TOTAL 100 Points
The End of the Year Assessment is an observed clinical examination and post-encounter written test covering the skills presented in M-2 DRS chapters 1-10. This is a comprehensive assessment.
The M-2 DRS letter grade will be assigned as follows:
Points Letter grade90-100 A79-89 B68-78 C< 67 F
3
CLASS SCHEDULEAugust 11-15, 2008
DRS2 Chapter 6
Date Time Event Presenter(s)Monday, 1:00-1:30p Overview of M2 DRS Dr. Beeman8/11/08 1:30-3:00p Neurological Examination Dr. Pulsinelli
*Sign-up for SPED Encounter (Tuesday & Wednesday) after lecture3:00-5:00p Clinical Practice Sessions M-4s
Tuesday, 8:00-5:00p Community Preceptor or8/12/08 SPED
Wednesday, 8:00-5:00p Community Preceptor or8/13/08 SPED
Thursday, 8:00-10:00a Small Groups Master Clinicians8/14/08 10:00-12:00p Mini Mental Status Exam Dr. Alex Auchus
Orientation to SOAP Note Assignment Dr. Beeman12:00-1:00p BREAK1:00-5:00p Community Preceptor
Friday, 8:00-5:00p Community Preceptor8/15/08
DRSChapter 6
Monday,August 11
Tuesday,August 12
Wednesday,August 13
Thursday,August 14
Friday,August 15
8-12 AM [PCC class time] DRS Option CP or SPED*
[PCC self-study]
DRS Options CP or SPED*
[PCC self-study]
Small groups in GEB then entire class in A103
DRS OptionsCP*
[PCC small groups]
Break1-5 PM DRS Class
Entire class in A103. Then small groups at 920 Madison, 7th Floor.
DRS OptionCP or SPED*
[PCC self-study]
DRS OptionsCP or SPED*
[PCC self-study]
DRS OptionsCP*
[PCC self-study]
DRS OptionsCP*
[PCC small groups]
Community Preceptor (CP) – required for TWO of the DRS Option boxes. Logs turned in by 8/22.
*Standardized Patient Encounter and Documentation (SPED) assignment for two hours at assigned time on Tuesday or Wednesday at 920 Madison, 7th floor. Check Blackboard for scheduling of SPED times and partners.
4

CHAPTER 6ASSIGNMENTS, DUE DATES, AND GRADES
Assignment : Clinical Practice Sessions Checklist and Documentation – Attendance and participation in these small groups led by Senior Medical Students includes performing the examination skills according to a checklist and documenting the skills presented during the week.Due Date: Monday afternoon –August 13, 2007Grade: 2 points of 100.
Assignment : Standardized Patient Encounter and Documentation (SPED) August 14-15, 2007
Interview and examine a standardized patient during first the hour. Document the encounter during the second hour. This is an open book assignment.Due Date: As scheduled – Tuesday or Wednesday of Chapter 6. Sign-up for this will be after the neurology lecture on Monday, August 13, 2007.Grade: 8 points of 100. Grades will be recorded on Blackboard by August 31, 2007. Feedback on the assignment will be given during the next week.
Assignment : Discussion about Patients with Master Clinicians - Attendance and participation in these small groups led by the Master Clinicians includes role-playing the written cases and orally communicating patient information.Due Date: Thursday morning-August 16, 2007. Grade: 2 points of 100.
Assignment : Community Preceptor Log - The Preceptor log includes information in the “box”, patient examination documentation, and the list of patients seen. Logs should be signed by the preceptor and placed in the Preceptor Log Box in the Madison Building.Due Date: Chapter 6 log is due by August 24, 2007. Grade: 2 points of 100. Make-up sessions are required if sessions are missed for any reason.
Posting of gradesThe grades are posted on the Blackboard Grade Book by the beginning of the following DRS week. It is your responsibility to check your own grades and if you have any problems or questions regarding these, contact Michael Holliday at [email protected].
5

Topics: NEUROLOGICAL EXAMINATION AND MENTAL STATUS EXAM
Reading for the week:Coulehan and Block, 5th edition: Chapter 11 pages 218-227Swartz, 5th edition: Chapter 21 pages 650-710
PREPARATION:NEURO 212 Integrated Neurosciences Course (2007-08). Go to Course Documents and open folder “Neurologic Exam:. The “Synopsis of a Normal Neurological Exam” is a written form of the neuron exam and then you can view the exam by opening the “Neurologic Exam Video”.
Bring your stethoscope. (Tongue blades, cotton balls and ear specula will be provided). Dress appropriately for practicing the physical examination on each other to include review of the skills learned from Chapters 1-5.
SYNOPSIS:A guiding lecture is followed by small group practice and review sessions. The first session follows the lecture and emphasizes the physical examination skills. Other opportunities for practicing skills include encounters with patients in the community preceptors’ office and with a standardized patient. The second small group session on Thursday morning with the Master Clinician emphasizes medical interviewing, communication issues, and pathophysiology. A lecture on Mental Status Exam and Orientation to Chapter 8 Assignments are scheduled for Thursday morning after Master Clinician sessions.
OBJECTIVES:
By the end of these sessions you will be able to:
Perform an examination of the neurological system. Perform a Folstein mini-mental status exam. With a focus on the complaints of headache and dementia,
- identify attributes of symptoms of neurologic origin.- correlate the presence of abnormal physical findings of the neurologic system with these illnesses.
Document/communicate the findings of the physical examination of the neurologic system.
6

Nervous System Physical Examination Checklist:Cranial Nerves Please circle one:Pupillary constriction (II, III) Done Not DoneExtra ocular movements (EOM) (III, IV, VI) Done Not Done
Up and down Done Not DoneLaterally and medially Done Not DoneOblique Done Not Done
Pupillary accommodation (III) Done Not DoneCorneal reflex (V, VII) Done Not DoneSensory of the face (V) Done Not Done
Above and below the eyes Done Not DoneBilaterally Done Not Done
Mastication (bite down) (V) Done Not DoneFacial expression (VII) Done Not Done
Eyes closed tightly Done Not DoneRaise eyebrows Done Not DoneSmile Done Not DonePuffy cheeks Done Not Done
Weber, Rinne (VIII) Done Not DoneGag (IX) Done Not Done
Use the “Say Ah” method for each other and all standardized patients (IX, X)Turn head against resistance (XI) Done Not Done
Bilaterally Done Not DoneShoulder Shrug (XI) Done Not DoneTongue movement (XII) Done Not Done• Motor Function StrengthUpper extremity, bilaterally Done Not DoneAbduction Done Not DoneFlexion Done Not DoneExtension Done Not DoneFlexion of wrist Done Not DoneExtension of wrist Done Not DoneAdduction/abduction of fingers Done Not DoneThumb adduction Done Not DoneLower extremity, bilaterally Done Not DoneHip flexion Done Not DoneKnee flexion Done Not DoneKnee extension Done Not DoneAnkle dorsiflexion Done Not DoneAnkle plantar flexion Done Not DoneGreat toe dorsiflexion Done Not DoneGreat toe plantar flexion Done Not DoneToneUpper extremity Done Not DoneLower extremity Done Not DoneBilaterally Done Not Done• Deep Tendon Reflexes (DTR)Mandibular (not in Swartz) Done Not DoneEach of the following bilaterally: Normal reflexesBiceps Done Not DoneBrachioradialis Done Not DoneTriceps Done Not DonePatella Done Not DoneAchilles Done Not Done
7
Abnormal reflexesBabinski Done Not DoneChaddocks (optional) Done Not DoneOppenheims (optional) Done Not Done• Sensory FunctionPain Done Not Done
Sharp or dull Done Not DoneDistally to proximally Done Not DoneBilaterally Done Not DoneUpper and lower extremities Done Not Done
Temperature (not in Swarts) Done Not DoneDistally to proximally Done Not DoneBilaterally Done Not DoneUpper and lower extremities Done Not Done
Vibratory Done Not DoneDistally to proximally Done Not DoneBilaterally Done Not DoneUpper and lower extremities Done Not Done
Proprioreception Done Not DoneFingers Done Not DoneToes Done Not DoneHold laterally Done Not DoneBilaterally Done Not Done
Tactile localization Done Not DoneDouble simultaneous stimulation X 2 Done Not Done
Graphesthesia Done Not DoneNumbers on palms Done Not DoneBilaterally Done Not DoneRight side up for patient Done Not Done
• Cerebellar FunctionFinger to nose Done Not Done
Bilaterally Done Not DoneHeel to knee Done Not Done
Move heel distally Done Not DoneBilaterally Done Not Done
Rapid alternating movements Done Not DonePronate/supinate Done Not DoneThumb to fingers Done Not DoneBilaterally Done Not Done
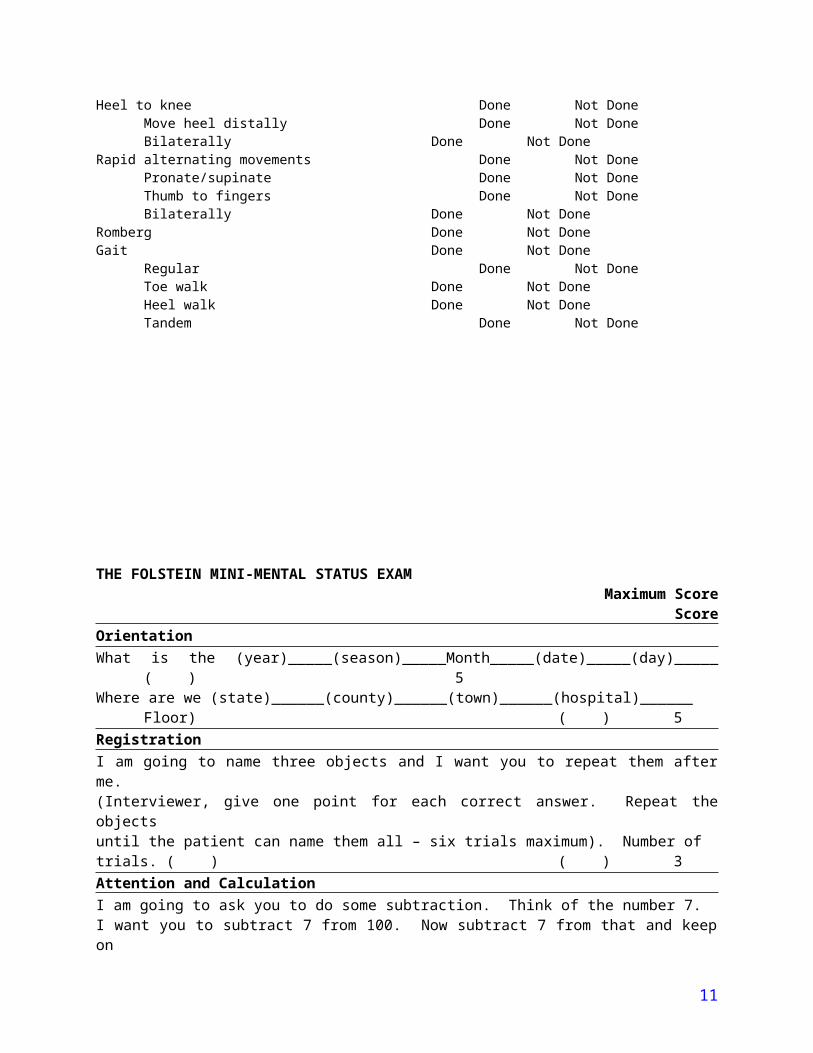
Romberg Done Not DoneGait Done Not Done
Regular Done Not DoneToe walk Done Not DoneHeel walk Done Not DoneTandem Done Not Done
8

THE FOLSTEIN MINI-MENTAL STATUS EXAMMaximum Score
ScoreOrientationWhat is the (year)_____(season)_____Month_____(date)_____(day)_____ ( ) 5Where are we (state)______(county)______(town)______(hospital)______
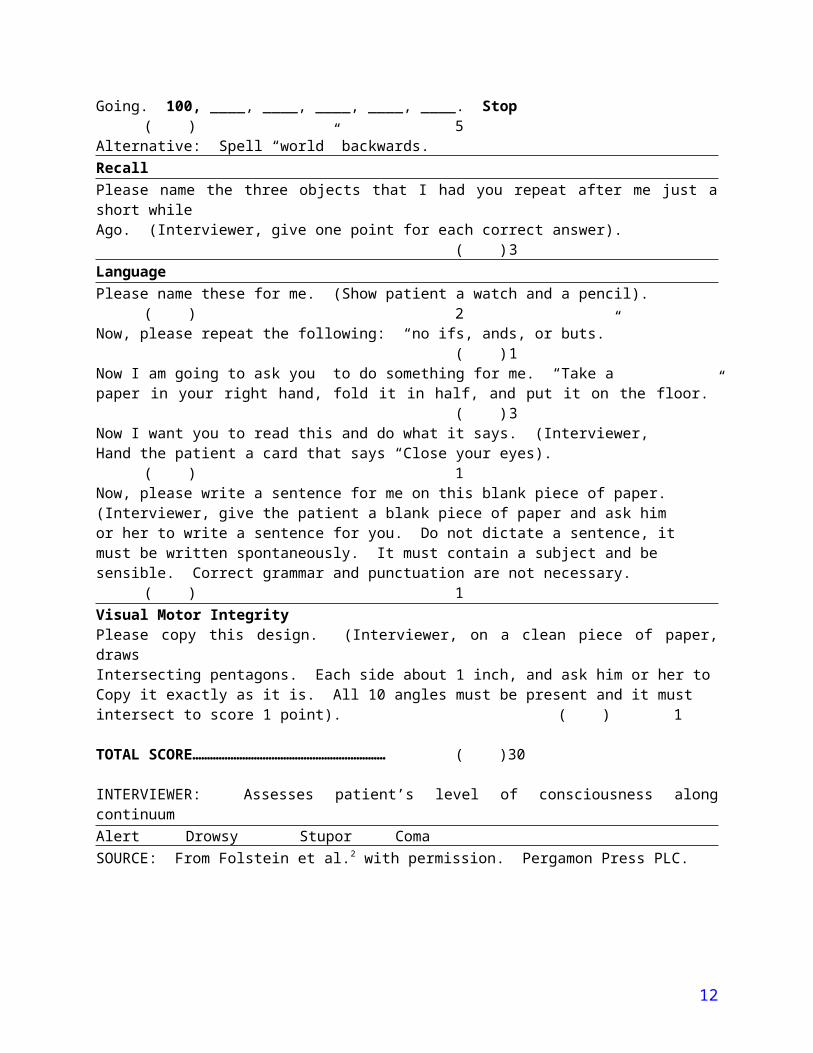
Floor) ( ) 5RegistrationI am going to name three objects and I want you to repeat them after me.(Interviewer, give one point for each correct answer. Repeat the objectsuntil the patient can name them all – six trials maximum). Number oftrials. ( ) ( ) 3Attention and CalculationI am going to ask you to do some subtraction. Think of the number 7.I want you to subtract 7 from 100. Now subtract 7 from that and keep onGoing. 100, ____, ____, ____, ____, ____. Stop ( ) 5Alternative: Spell “world” backwards.RecallPlease name the three objects that I had you repeat after me just a short whileAgo. (Interviewer, give one point for each correct answer). ( ) 3LanguagePlease name these for me. (Show patient a watch and a pencil). ( ) 2Now, please repeat the following: “no ifs, ands, or buts.” ( ) 1Now I am going to ask you to do something for me. “Take apaper in your right hand, fold it in half, and put it on the floor.” ( ) 3Now I want you to read this and do what it says. (Interviewer,Hand the patient a card that says “Close your eyes). ( ) 1Now, please write a sentence for me on this blank piece of paper.(Interviewer, give the patient a blank piece of paper and ask himor her to write a sentence for you. Do not dictate a sentence, it must be written spontaneously. It must contain a subject and be sensible. Correct grammar and punctuation are not necessary. ( ) 1Visual Motor IntegrityPlease copy this design. (Interviewer, on a clean piece of paper, draws Intersecting pentagons. Each side about 1 inch, and ask him or her to Copy it exactly as it is. All 10 angles must be present and it must intersect to score 1 point). ( ) 1
TOTAL SCORE………………………………………………………… ( ) 30
INTERVIEWER: Assesses patient’s level of consciousness along continuumAlert Drowsy Stupor ComaSOURCE: From Folstein et al.2 with permission. Pergamon Press PLC.
9
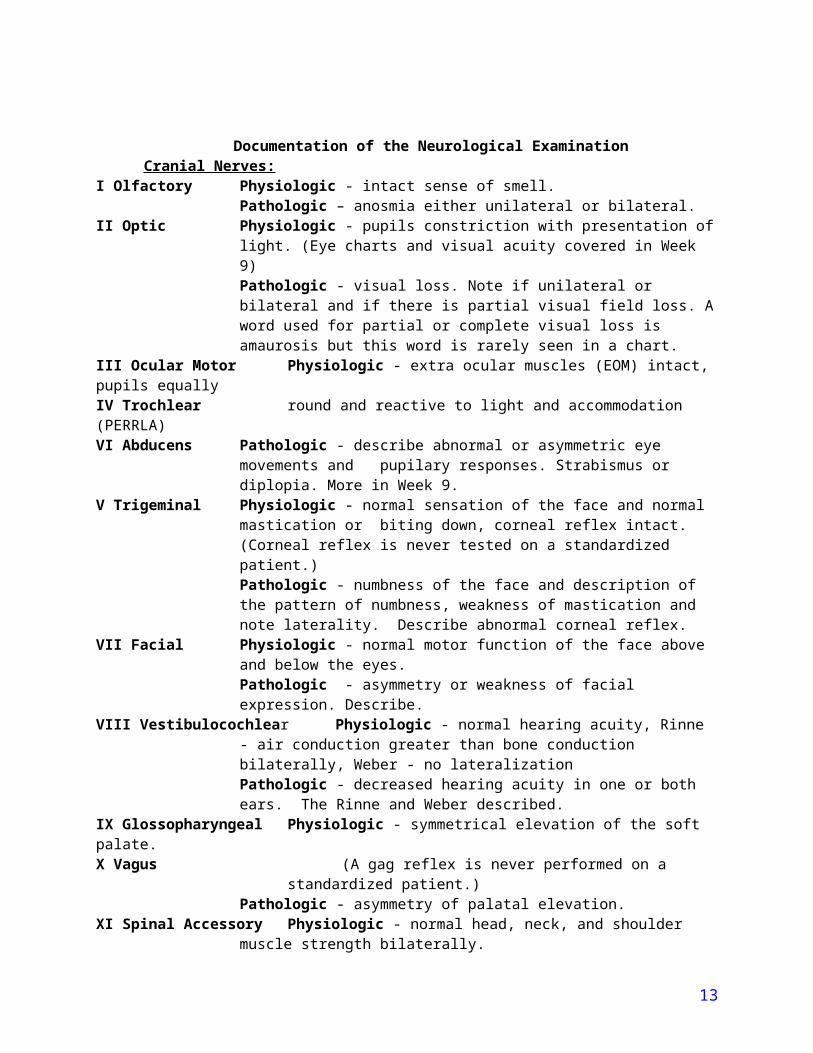
Documentation of the Neurological ExaminationCranial Nerves:
I Olfactory Physiologic - intact sense of smell. Pathologic – anosmia either unilateral or bilateral.
II Optic Physiologic - pupils constriction with presentation of light. (Eye charts and visual acuity covered in Week 9)Pathologic - visual loss. Note if unilateral or bilateral and if there is partial visual field loss. A word used for partial or complete visual loss is amaurosis but this word is rarely seen in a chart.
III Ocular Motor Physiologic - extra ocular muscles (EOM) intact, pupils equally IV Trochlear round and reactive to light and accommodation (PERRLA)VI Abducens Pathologic - describe abnormal or asymmetric eye movements and pupilary
responses. Strabismus or diplopia. More in Week 9.V Trigeminal Physiologic - normal sensation of the face and normal mastication or biting
down, corneal reflex intact. (Corneal reflex is never tested on a standardized patient.)Pathologic - numbness of the face and description of the pattern of numbness, weakness of mastication and note laterality. Describe abnormal corneal reflex.
VII Facial Physiologic - normal motor function of the face above and below the eyes. Pathologic - asymmetry or weakness of facial expression. Describe.
VIII Vestibulocochlear Physiologic - normal hearing acuity, Rinne - air conduction greater than bone conduction bilaterally, Weber - no lateralizationPathologic - decreased hearing acuity in one or both ears. The Rinne and Weber described.
IX Glossopharyngeal Physiologic - symmetrical elevation of the soft palate.X Vagus (A gag reflex is never performed on a standardized patient.)
Pathologic - asymmetry of palatal elevation.XI Spinal Accessory Physiologic - normal head, neck, and shoulder muscle strength bilaterally.
Pathologic - weakness of head, neck, and shoulder muscles. Describe.XII Hypoglossal Physiologic - normal tongue movements.
Pathologic - weakness and wasting of the tongue musculature. Motor:
Comments on muscle strength and muscle tone should be included in this section. Muscle strength is generally noted on a scale of 1 to 5.
0 - absent, no contraction whatsoever. 1 - a trace or a person can slightly contract muscles. 2 - weak, some movement with gravity. 3 - fair movement against gravity only so one can lift own arm but not against resistance. 4 - good movement against gravity with some resistance from the examiner. 5 - normal movement against gravity with full resistance.
Note anatomical location of tested muscles.
Physiologic- muscle strength 5 on above scale bilaterally, note areas tested. Muscle tone - appropriate resistance to passive movement and note of location tested.
Pathologic - note location of muscle weakness on scale above. For muscle tone, note increases (spasticity and rigidity) and decreases (flaccidity). Loss of muscle bulk and facsiculations may also be noted.
Deep Tendon Reflexes:
10
Note which reflexes were tested - biceps, triceps, brachoradialis, patellar, or Achilles. Note bilaterally. Again, there is a number system used for reflexes and it is different from the muscle strength scale.
0 – no response1+ - diminished2+ - normal3+ - increased 4+ - hyperactive (induces clonus)
Many people draw a little stick person and note the reflex scores and locations.Physiologic - DTR 2+ in all locations bilaterally, plantar flexionPathologic - note location and score of DTR, Babinski present or plantar dorsiflexion
Sensory: Note pain, temperature, vibratory, proprioreception, tactile localization and graphesthesia. Physiologic - intact sensory function in anatomical areas tested and types of sensation. Pathologic - note deficits by type of sensation and bodily location.
Cerebellar: Physiologic - Normal finger-to-nose, heel-to-knee, and rapid alternating movements, Romberg and gait are intactPathologic - Past pointing, tremor, disdiadochokinesis, sway or pronator drift, describe abnormal gait - ataxic, foot drop, etc. (p 630 Swartz)
Mental Status Exam: Physiologic - Folstein Mini Mental Status Exam 25-30/30. Pathologic - Folstein Mini Mental Status Exam 0-24/30.
Signs and Symptoms of Common Neurological Conditions:Headaches
Symptoms Risks Signs CauseRecurrent, severe, unilateral frontal parietal areas, triggers (food, menstrual periods), aura, nausea and vomiting
Young adult, more often female, positive family history for migraine headaches
Photophobia, possible transient focal neurological deficits (aura) precede or accompany headache
Migraine
Occipital or frontal, builds up as day wears on, evening time, dull, non pulsatile
Female, stress Normal neurological exam, may have muscle tenderness in occipital or TMJ area
Tension
Headaches occurred for less than 2 months, duration, worse on awakening in the morning
Hypertension, papilledema,focal neurological findings
Brain Tumor
DementiaAcquired and persistent impairment of long and short term memory, and other
disturbances such as language, concentration, visuospatial abilities, emotions, and personality despite a clear consciousness. Score on mini-mental exam < 25/30.
Symptoms Risks Signs CauseGradual onset, progressive
Old age, positive family history, certain genes
No sensorimotor deficits. Often well-kempt appearance.
Alzheimers
Sudden onset Age greater than 60 years, diabetes, hypertension, hyper-lipidemia, smoking
Upper motor neuron abnormalities (paresis and spasticity)
Stroke (multi-infarct)
11
Urinary urgency/incontinence
History of traumatic head injury, intercranial hemorrhage or infection (may be subtle)
Apraxic or magnetic, ataxic gait. Less well-kempt
Hydrocephalic
MONDAYAugust 13, 2007
LECTURE SERIES ON CLINICAL SKILLS
Participating Faculty: Gail Beeman, MD., M.H.P.E.1:00-1:30 PM GEB A103
Topic: Overview of M-2 DRS
Participating Faculty: Dr. William Pulsinelli1:30-2:30 PM GEB A103
Topic: Neurologic System
The Monday afternoon lecture will present the techniques for examining the neurologic system. Common symptoms and illnesses associated with pathology of the neurologic system will also be discussed.
Please review the Video of the physical exam of the NeurologicalSystem as described on Page 6
CLINICAL PRACTICE SESSIONS
Educational Activities: Guided by the lectures, reading assignments, checklists, and an upperclassman, practice physical
examination and documentation of the nervous system. Review the physical examination of the chest, abdomen, ears, nose, oral cavity, and pharynx,
musculoskeletal, skin, lymph, peripheral vascular system, and vital signs. Organize the format for case discussions on Thursday, August 17, 2006.
Room Assignments Please report directly to the Kaplan Clinical Skills Center. If you are female report at 3:00 PM or directly after the lecture. If you are male report at 4:00 PM. (During the next week we will switch times.)
Turn in your checklist and documentation assignment to your M-4BEFORE you leave.
TUESDAY or WEDNESDAYAugust 14-15, 2007
SPED ASSIGNMENT(8pts)
The main purpose of this experience is to see a standardized patient to complete a medical history and physical exam with the patient. You are required to document the patient’s medical history and physical to turn in for a grade. Use a composite of the checklists and the following guidelines to complete your document of the patient’s medical history and physical. You have one hour to examine the patient and one hour to complete the write up after examining the patient. You have an outline to write on. Do NOT write on the back of the paper that is blank. Please write legibly. This is an open book assignment. An example of the format needed for this assignment starts on page 867 of Swartz, 5 th edition. Remember this assignment focuses on the neurologic exam and requires much more detail than this example has under the heading “Neurologic”.
12
You will meet the criteria of excellence for this assignment if you do the following:
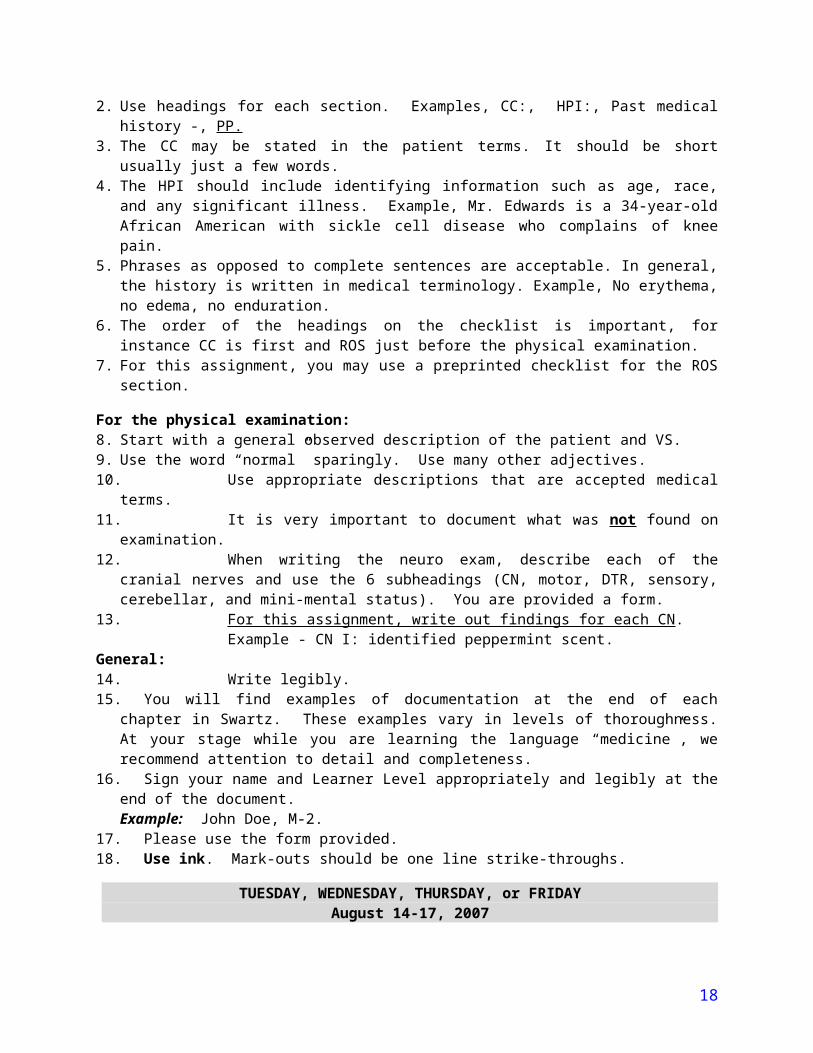
For the medical history,1. Start off with the patient’s name, who gave the history, how reliable it is.2. Use headings for each section. Examples, CC:, HPI:, Past medical history -, PP.3. The CC may be stated in the patient terms. It should be short usually just a few words. 4. The HPI should include identifying information such as age, race, and any significant illness.
Example, Mr. Edwards is a 34-year-old African American with sickle cell disease who complains of knee pain.
5. Phrases as opposed to complete sentences are acceptable. In general, the history is written in medical terminology. Example, No erythema, no edema, no enduration.
6. The order of the headings on the checklist is important, for instance CC is first and ROS just before the physical examination.
7. For this assignment, you may use a preprinted checklist for the ROS section.
For the physical examination:8. Start with a general observed description of the patient and VS.9. Use the word “normal” sparingly. Use many other adjectives.10. Use appropriate descriptions that are accepted medical terms.11. It is very important to document what was not found on examination.12. When writing the neuro exam, describe each of the cranial nerves and use the 6 subheadings (CN,
motor, DTR, sensory, cerebellar, and mini-mental status). You are provided a form.13. For this assignment, write out findings for each CN .
Example - CN I: identified peppermint scent.General:14. Write legibly.15. You will find examples of documentation at the end of each chapter in Swartz. These examples vary
in levels of thoroughness. At your stage while you are learning the language “medicine”, we recommend attention to detail and completeness.
16. Sign your name and Learner Level appropriately and legibly at the end of the document.Example: John Doe, M-2.
17. Please use the form provided.18. Use ink. Mark-outs should be one line strike-throughs.
TUESDAY, WEDNESDAY, THURSDAY, or FRIDAYAugust 14-17, 2007
ACTIVITIES WITH THE COMMUNITY PRECEPTORS
Participating Faculty: Community Preceptors Practice the organ system of the week. The organ system is the nervous system. As usual, the
checklist for examining the organ system of the week is included in the syllabus. Review the following skills when the opportunity arises - vital signs, ears, nose, oral cavity, and
pharynx, chest, abdomen, musculoskeletal, and the complete medical history including chief complaint, history of present illness, past medical history, family history, patient profile and habit history.
You are required to meet for at least three hours on TWO sessions for this DRS week. If you do not attend your preceptor sessions, Michael Holliday and the preceptor’s office must be notified as soon as possible.1. Observe the circumstances when a neurological exam is performed on patients in the office.2. Fill out the Community Preceptor Log and have it signed.
13

Please note: The course director understands that the opportunity to perform complete neurological exams may not arise during the time you spend with your preceptor. Roommates, spouses, friends and relatives are usually curious enough to allow you to practice your new expertise. When you are with your preceptor, be assertive in your willingness to interview and examine patients. Once your preceptor knows of your interests, more opportunities are likely to come up.
Guidelines for A Successful Professional Relationship With Your Preceptor
1. You should know how to contact your preceptor and the preceptor’s office. They should know how to contact you. You should recognize the office personnel and they should recognize you.
2. It should be clear to you and the preceptor and the office personnel what times you are to come. These plans may vary from week to week, but they should be planned. Never just show up expecting to stay for the session.
3. Bring with you the activities for the week, the list from the syllabus. Do not interpret the preceptor’s inability to find a copy of this list as a sign of disinterest in you and your learning.
4. Try to find a time to reflect upon this list of activities with your preceptor. Five minutes of planning and reflection may make a big difference in how the session goes.
5. Try to attend the beginning and/or the end of each session. Coming and going during the session will make it difficult to pause for planning and reflection with your preceptor. Sessions should last at least 3 hours, but may be longer.
6. Help out if things get hectic. Making a telephone call, walking for a chart, helping a patient through the waiting room are all part of patient care.
If you have any questions regarding this course please feel free to contact:Michael Holliday [email protected] - 448-4530
THURSDAYAugust 16, 2007
PATIENT DISCUSSIONS WITH MASTER CLINICAN8:00-10:00 AM GEB A103
Check BLACKBOARD for Group Assignments
Role play the patient dialogues and discuss the questions at the end of each case. Since you have a written assignment to document, a complete patient history, and physical, please review documentation format and content.
Discuss differential diagnosis for CC - HeadacheAbnormal mental status
You have two patients today:Nancy Ledbetter, a 51 year old, complaining of severe headache.Mildred Farmer, 62 year old, having arm problems
Mrs. Nancy LedbetterStudent DoctorNancy Ledbetter, fifty-one year old female
14

Setting: Your preceptor’s office. The patient has been sent in by her primary physician for a primary evaluation of a severe headache. Student notices a portly woman who seems mildly uncomfortable.
Student: Hello, my name is _________ _________, student doctor. I'm here to ask you some questions and do a physical examination. My attending will be along a little later.
Mrs. Ledbetter: Um….., OK.
Student: It's noted here that your primary physician sent you in for evaluation today, what would that be about?
Mrs. Ledbetter: I have this awful headache.
Student: How long have you had the headache?
Mrs. Ledbetter: Since Monday evening.
Student: Where does it hurt?
Mrs. Ledbetter: There's a throbbing inside my head above my eyes.
Student: Oh, so you've had this headache since yesterday and it's throbbing in front.
Mrs. Ledbetter: Yes.
Student: How bad is the headache?
Mrs. Ledbetter: Terrible, and it's getting worse.
Student: Have you had anything like this before?
Mrs. Ledbetter: Yes, twice before. Last month and about a year ago.
Student: Were those times just like this one?
Mrs. Ledbetter: Yes, but not so bad, I just took 2 extra strength Tylenol, kinda sat down and closed my eyes. It went away and then came back the next day, but then I just took some more Tylenol and rested up.
Student: Anything bring your headaches on?
Mrs. Ledbetter: Well, a year ago I was on vacation, but I wasn't really relaxing. I had drunk a bit of wine and I thought that was the problem. Last month I was really tired.
Student: Are you tired now?
Mrs. Ledbetter: Yes, my oldest daughter is getting married and my youngest daughter is learning how to drive. They just drive me crazy! (Mrs. Ledbetter laughs at her pun.) My crazy mother-in-law is so pompous about this wedding. It just doesn't make sense to her that the bridesmaids' dresses are black. I think they're beautiful, and if Carol wants them black, it is her decision, not Mrs. Ledbetter's.
Student: Sounds like a lot is going on right now. Have you tried the Tylenol for this headache?
15

Mrs. Ledbetter: Yes, and Aleve and Nutrin or Nuprin and Anacin and a nap and a steamy shower and even Feverfew, an herb that my neighbor gave me. It works for her and her cousin's migraines! I also took an extra Vitamin tablet. I read that B vitamins might help.
Student: Did you drink wine this time?
Mrs. Ledbetter: Just a little to calm me down after the "Margaret Ledbetter Show."
Student: Your mother-in-law? Mrs. Ledbetter: Yes, the bridesmaids' black dresses.
Student: Do you think you drink too much?
Mrs. Ledbetter: Oh, no. I wasn't really drunk.
Student: What I mean is, do you feel like you need to cut down on your drinking?
Mrs. Ledbetter: No, not at all.
Student: Do people criticize you for your drinking?
Mrs. Ledbetter: No! Not even my mother-in-law.
Student: Have you ever felt guilty about your drinking?
Mrs. Ledbetter: No, I don't think so.
Student: Have you ever taken a drink for an "eye opener," like a Bloody Mary, first thing in the morning for a hangover?
Mrs. Ledbetter: Well, I'll have to admit, I did try that this time since I did have such a terrible headache the next morning after I drank that little bit of wine.
Student: Mrs. Ledbetter, do you have any other medical problems that I need to know about?
Mrs. Ledbetter: Well, I have had diabetes for several years. I don't take insulin, but I do take a pill for my sugars. My sugars do usually run a little high and I know, I know, I need to lose weight. I really want to lose weight for this wedding. I'd like to lose about fifty pounds. I…
Student: (Interrupting) Any problems except headache and diabetes?
Mrs. Ledbetter: I don't think so.
Student: What kind of work do you do?
Mrs. Ledbetter: I'm an assistant manager at a Honey Baked Ham store. This season is "hell," pardon my French. If your heart is beating, you're hired to cut those hams. Lines out the door for those hams. Those people are nuts sometimes. Drive me crazy. Don't you have a bigger ham? Man, that's expensive! Pay me with a hot check! (Getting louder and louder.) Bring in ham bones and say the ham wasn't worth eating. It’s not worth eating, but we had to eat something. This side dish is frozen! I didn’t have time to . . .
Student: Wow, no wonder you have a headache!
16

Mrs. Ledbetter: I am…(Stops in mid-sentence, frowns, puts her hand on her forehead and sighs.)
Student: Let's do the PE.
Physical Examination:
The medical student notices that the nurses have documented a temperature of 98.6ºF, respiratory rate of 20, heart rate of 90, and blood pressure of 135/88.
The student doctor proceeds with a neurological examination. Starts off with cranial nerves The pupillary constriction, extraocular movements, pupillary accommodation, corneal reflexes optional, sensory of the face, mastication, strength, facial expression, Weber, Rinne, the modified gag, turning head against resistance, the shoulder shrug, checking the tongue's movement. Motor is checked for by strength in both upper and lower extremities. Also, the upper and lower extremities are checked for muscle tone. The deep tendon reflexes are checked, the mandibular reflex and the normal reflexes of the biceps, brachioradialis, triceps, patellar, Achilles. Abnormal reflexes, Babinski's, Chaddock's and Oppenheim's are checked. Sensory function is tested by checking for pain with sharps and dulls going distally to proximally bilaterally over the upper and lower extremities. Temperature is checked distally to proximally and bilaterally over the upper and lower extremities using the cold tuning fork. Vibratory sense is checked as well as proprioreception, tactile localization, and graphesthesia.
Cerebellar function is tested by using finger-to-nose, heel-to-knee, rapid alternating movements, pronating and supernating thumb-to-fingers. The Romberg is checked and, also, the gait.
The student who is playing Mrs. Ledbetter should demonstrate the following abnormal findings:1. The Achilles reflexes are decreased.2. During the sensory testing on the distal extremities, there should be absent pin prick (pain) sensation bilaterally in the distal lower extremities.3. The perception of vibration is decreased bilaterally in the distal lower extremities.4. Proprioreception in the toes is also difficult for Mrs. Ledbetter.5. Mrs. Ledbetter's gait is also abnormal.
Questions:1. What type of gait would you speculate Mrs. Ledbetter would have, and why?2. What do the physical examination findings mean? Why?3. What type of headache would you speculate Mrs. Ledbetter has?4. Discuss Mrs. Ledbetter's use of alternative medicine.5. Discuss the process of the interview.
Did the HPI proceed from open to closed-ended questions? How many attributes were obtained?How do you feel about the way the student handled the patient's tangents?Were the CAGE questions appropriate? Why or why not?Did the student express empathy? Were there missed opportunities to express understanding? Explain.
Mrs. Mildred FarmerStudent DoctorMildred Farmer, a sixty-two year old femaleRobert Farmer, Mildred’s forty year old son
17
Setting: The examination room of your preceptor’s primary care clinic. The student has been sent in first to talk with the patient and perform an exam, as needed.
Student: Hello Ms. Farmer I’m student doctor, ______________. Dr. Hunt sent me totalk with you and perform an examination. He’ll join us right after I finish.
Robert Farmer: Can I see you outside just a moment, Dr. __________? Mother, excuse us just a moment. We’ll be right back.
(Robert and Student move into the hallway to talk privately.)
Robert Farmer: I live in Phoenix and only return to Memphis about once every other year. I am very concerned about my mother. She’s confused and she doesn’t seem to be using her right arm very well. My grandparents had Alzheimer’s disease, and mother is behaving a lot like my grandparents. I think she may need to be put in a nursing home.
Student: I’ll talk with your mother and examine her, and then Dr. Hunt can help us with that decision. (They return to room). Mrs. Farmer, what’s the reason that your son has brought you to see us today?
Mrs. Farmer: Oh, I’ve been doing pretty well. My son thinks there is something terribly wrong with me but I don’t feel bad at all. I live by myself and I’m doing just fine.
Student: Is anything bothering you?
Mrs. Farmer: Oh my right arm is a little weak but I think that’s because I fell a week or two ago and it just hasn’t felt right since.
Student: Did you injure your arm when you fell?
Mrs. Farmer: I think so. It didn’t bring the blood.
Student: How did you happen to fall?
Mrs. Farmer: Oh, I just happen to stumble on my front steps going to pick up some trash in the yard. I didn’t fall completely. I caught myself against one of the columns on our front porch.
Student: Did you hit your head?
Mrs. Farmer: No.
Student: Is anything else bothering you?
Mrs. Farmer: Nothing at all?
Robert Farmer: Mother, please tell Dr. ___________ about how forgetful you’ve become. Remember that cake you tried to make two days ago? You left the eggs out of it.
Mrs. Farmer: Oh, I’m not really having any trouble.
Robert Farmer: Well, actually Dr, my mother is having lots of problems. When I last visited a couple of years ago, she was doing great. She was able to have friends over for dinner. She was able to prepare a six course meal without problems. Now, she is extremely forgetful. I’m really
18
worried about her because I saw her turn on the oven’s gas jets and then forgets to light them. She sometimes forgets the names of the neighbors and isn’t as careful now about her physical appearance. Just yesterday she got all dressed up because she thought it was Sunday but it wasn’t, it was Tuesday.
Mrs. Farmer: Oh, I’m getting just a little forgetful; it’s nothing at all.
Student: Has she had any other weakness?
Mrs. Farmer: No.
Student: Have you had any headaches or fever?
Mrs. Farmer: No, I did have a cold a week or two ago but that’s gone.
Student: What medications are you on?
Mrs. Farmer: The names are hard to remember but I do take two or three pills a day.(She shuffles in her purse).
Robert Farmer: I’m afraid sometimes, she may not be taking her medicines. I made a list of them and they are Procardia XL 30 mg a day, Esidrix 25 mg per day and her multi-vitamin. Dr. Hunt said that she needed to stay on these medicines because of her high blood pressure.
Student: What other illness does Mrs. Farmer have?
Mrs. Farmer: I’m in good health. There is nothing else wrong with me.
Robert Farmer: Well, mother is a borderline diabetic and has to watch her diet. She is suppose to not have much salt in her diet too, but I found potato chips in the pantry yesterday. I’m really concerned she is not eating the right foods and sometimes skipping meals all together.
Student: What about any other serious illnesses you’ve had in the past. Any hospitalizations or operations?
Mrs. Farmer: Well when I was a little girl, they took my appendix out. My tonsils too. In fact, my whole family had their tonsils taken out. Have you ever had your tonsils taken out?
Student: No! Did you have any other hospitalizations or operations?
Mrs. Farmer: I had Bobby in a hospital. They had to cut me open to get him out. I had his older sister there too. She’s dead now you know. She died in a car wreck.
Student: Is there anything you are allergic to?
Mrs. Farmer: Penicillin gives me a rash.
Student: Tell me more about that.
Mrs. Farmer: Oh, I don’t remember.
Student: Are there any illnesses that run in your family.
Mrs. Farmer: My brother couldn’t take penicillin either. He swelled up.
19

Student: Mrs. Farmer are there any illnesses that run in your family like high blood pressure, diabetes, heart disease or cancer.
Mrs. Farmer: Cancer you say. You don’t think I’ve got cancer do you?
Student: No Mrs. Farmer. Are there any blood relatives who have illnesses like cancer, heart trouble, diabetes, or high blood pressure?
Mrs. Farmer: Well, my father had high blood pressure and my mother had diabetes.Nobody had cancer.
Student: Now, I’d like to ask you some questions about your body in general. Have you had any fever or chills lately?
Mrs. Farmer: No.
Student: Any problems with headaches or dizziness?
Mrs. Farmer: Oh, I get dizzy sometimes.
Student: Tell me more about that?
Mrs. Farmer: Oh, I don’t know. I just think every now and then, I am a little dizzy.
Student: What do you mean by dizzy? Does your head spin or do you feel lightheaded or what?
Mrs. Farmer: No, just dizzy.
Student: Do you have any ringing in your ears or do you get sick to your stomach?
Mrs. Farmer: No.
Student: Any trouble with your bones or joints?
Mrs. Farmer: No.
Student: Any changes in your weight.
Mrs. Farmer: No. I’m fine.
Robert Farmer: Mother, I’m sure you have lost at least twenty pounds since I washere two years ago. Your clothes look like they are just hanging on you.
Mrs. Farmer: I feel fine.
Student: Have you had any difficulty in swallowing or any problems with your mouth?
Mrs. Farmer: No.
Student: Have you had any chest pain or shortness of breath?
Mrs. Farmer: No.
20
Student: Have you had any wheezing or any cough?
Mrs. Farmer: No.
Student: Any swelling of your feet?
Mrs. Farmer: No.
Student: Are you able to sleep flat on your back at night or does it take several pillows?
Mrs. Farmer: I sleep fine.
Student: Do you have any irregularity of your heart?
Mrs. Farmer: No.
Student: Have you had any problems with your stomach or your digestive system.
Mrs. Farmer: No.
Robert Farmer: Now, mother you were just telling me yesterday how bad your constipation was and how you were having to take laxatives to have a bowel movement.
Student: Mr. Farmer, is there anything else your mother has complained of to you?
Robert Farmer: No, not that I could think of.
Student: Has she complained of any numbness or tingling anywhere.
Robert Farmer: No.
Student: What about either alcohol or tobacco use.
Mrs. Farmer: No, I’ve never done either.
Robert Farmer: That’s correct.
Student: So you live by yourself?
Mrs. Farmer: Yes, I do pretty well. I’ve got a neighbor that takes me to the store twice a week.
Robert Farmer: The neighbors are very helpful. I’m worried though because I don’t think my mother is eating three meals a day. I’m also worried because she seems to be wandering a little bit at night. I’m afraid that she’s going to fall.
Student: I can understand your concern. I’m going to go ahead and perform a physical examination at this time. Mr. Farmer if I can ask you to step out of the room for a few minutes but I’ll need you back in when Dr. Hunt comes to see your mother.
Physical Examination:
Vital signs: Pulse 80 and irregular Temperature: 98.7 BP: 165/103 R: 15
21

Skin: No rashes, petechiae, or telangiectasias. Specifically no ecchymoses over the right arm where the patient said that she fell.HEENT: PERRL, Fundai with mild arteriolar narrowing and nicking no hemorrhages or exudates. TMS and canals –normal. Normal molds and nasal mecosa. Normal mouth and oropharynx. Unremarkable except for a hyperactive gag reflexCarotids 2+ on the right. Left carotid barely palpable with a loud bruitThyroid palpable Chest-clear. Heart: irregularly, irregular rhythm. Variable S1. Normal S-2 No murmurs, rubs, or gallops. Breasts: Without masses or discharge. Lymph Nodes-non palpable Abdomen: Normal bowel sounds no masses, megaly tendencies or bruits. Femoral 2+ bruits. Extremities: no edemaInterosseus wasting and Pulse 2+.Neurologic-cranial nerves II-XII revealed a right homonymous hemiaopsia, right central VII facial palsy, a right hyperactive gag reflex but other cranial nerves intact. Strength-3/5 in , right upper extremity and 4/5 in right lower extremity; otherwise normal. Reflexes 3+ on the right side, 2 + on the left. There is a Babinski on the right. Sensor examination appears to be normal to pinprick position and touch. Mental status:Demonstrate the following areas using the Folstein Mini-mental Status Examination.
Orientation RecallRegistration LanguageAttention and Calculation Visual-Motor Integrity
Mental status examination score of only 22. The patient was not able to identify specifically the day, month, and year. She could not recall three objects, nor could she complete serials 7’s.
Questions:1. Based on the history and physical examination, what is most likely wrong with this patient?2. Do you think this patient is mentally competent? Why or why not?3. Would this patient be able to provide informed consent for medical evaluation work-up possibly including a cerebral arteriogram?4. If Dr. Hunt feels that the patient needs nursing home placement but the patient is adamant about staying at home, what can be done?
THURSDAYAugust 16, 2007
Participating Faculty: Dr. Alex Auchus10:00-11:00 AM GEB A103
Topic: Review Min-Mental and Neuro Exam
Participating Faculty: Gail Beeman, MD., M.H.P.E.11:00-12:00 PM GEB A103
Topic: SOAP Note Assignment Orientation
SOAP NOTE ASSIGNMENT DESCRIPTION
You will be assigned to a patient to perform a pertinent history and physical examination. The patient’s chief complaint will be a common one from the organ systems that have been covered so far in the
22
course. The role play case discussions and the common signs and symptoms chart in your syllabi will help you prepare for this assignment.
Timing and activities for the assignment are as follows: 15 minutes to perform the pertinent history and physical
10 minutes and desk space to complete a SOAP note 2 minutes to orally present the patients findings and your assessment and plan to the observer After the oral presentation, you will turn your paper in for grading and receive feedback
according to the form included in this folder.
A learner-of-medicine senior to you will observe you during the patient encounter and the oral presentation. The observer will fill out a checklist, grade your note and presentation, and then give you oral and written feedback. Written comments from the Standardized Patient will be included in the feedback. The observer will assign a pass or fail to your performance. If a pass is assigned, then you will be awarded the maximum number of points for this assignment. If a fail is assigned, remedial work is required.
Reviewing the sample notes and patient encounters on the USMLE web site should give you an idea of the nature of this experience. USMLE.org and to Step 2 CS. This assignment will last about 45 minutes. Your time is posted on Blackboard and should reflect the half-day you signed up for earlier in the academic year.
Instructions for Oral PresentationsDoctor-to-Doctor Communication
1. Appropriate identifying statement about this patient.“Mr. G is a 40-year-old man who works as a house painter.”
2. State the symptom that is the chief complaint. Note: this can be in medical terms or in the patient’s words.“He comes in today with the complaint of shortness of breath.”
3. The HPI is a narrative; you are telling a story. Give all the attributes that you have. It usually takes at least four to make a diagnosis.
Bodily location Setting (context)Quality (or character) Aggravating factorsQuantity (or intensity or severity) Alleviating factorsChronology (onset, duration, frequency) Associated manifestations
“He complained of this symptom for two weeks and it seems to be increasing in severity. He has a nighttime non-productive cough. He tried some over-the-counter remedies which did not work. I think they were antihistamines.”
State pertinent positives and negatives. Sometimes absence of an attribute of a symptom has more diagnostic value than the presence of a symptom. As you know more pathophysiology you will use pertinent negatives more. This is not a review of systems (ROS). This is diagnostically pertinent information.
“He does not complain of chest pain. He does not have a runny nose. He has not had fever.”4. Summarize the important parts of patient’s past medical history (PMH), family history (FH), patient
profile (PP), habit history, and review of systems (ROS).“Mr. G has a history of multiple admissions during the last decade for pneumonia. The last one was one month ago. He was treated with broad-spectrum antibiotics and was symptom-free prior to the current illness. The others were also acute illnesses from which he fully recovered. He has not been diagnosed with asthma. There is no related family history. His father who was a smoker died of lung cancer at age 50. Mr. G. does not smoke. As I mentioned earlier, he does breathe paint fumes on the
23

job. Mr. G. is recently divorced. He was married for five years to a high school teacher. Prior to his divorce he was drinking heavily and lost his job as a salesman.”
5. Objective, observed physical examination findings follow the history. Start with a general observed description of the patient.“Mr. G. looks healthy and appears normal weight. However, he has increased effort to breathe today.”
6. Report the physical findings both pertinent normal and abnormal in order – VS and BMI first followed by a head-to-toe description by organ systems.“Mr. G’s respiratory rate is 30 per minute which is rapid. His other VS are within the normal ranges. Tympanic membranes are pearly gray bilaterally. Nose exam does not reveal any secretions. Lung findings show decreased breath sounds in the lower left lung field bilaterally. I do not appreciate any crackles or wheezes. Heart has regular rhythm and rate, no murmurs appreciated. PMI is at the 5 th
intercostals space mid-clavicular line. Distal extremities show strong pulses and no edema.”7. Report available and pending pertinent laboratory and imaging studies. Be sure you know
which tests are normal and which are abnormal.“The O2 sat is 95%. So he doesn’t need O2 and is presently on his way down to X-ray for a PA and lateral chest film.”
8. Assess the patient. For now the assessment may be a summary of findings and/or a list of possible diagnoses.“Mr. G. has an acute illness involving the respiratory system. This seems to be a reoccurrence of a similar illness suffered a few times over the last decade. Risk factors include inhaled paint fumes. I think he has either community acquired pneumonia or some kind of chemical pneumonitis.”
9. Later you will state a plan of action to include ordered studies, medication, referrals, etc,
Note: Be enthusiastic. Make it interesting. Your interpretations are important, but when describing personal information about the patient, be descriptive not judgmental. Timing of onset of various symptoms and events of the illness is important. Be sure you include this information in the presentation like you would tell a story.
SOAP Note Assignment Feedback
M-2 Name: ________________________________________ Date: ____________
Overall: ___ Pass (8 points) ___ Fail (remedial work required)
15 MINUTES IN THE EXAMINATION ROOM Outstanding Clear Pass Borderline Clear Fail
History takingContent of the medical history was satisfactory with the following comments:Attributes of the chief complaint, pertinent positives and negatives, identifying risks
Physical examinationThe physical examination was complete with the following comments:
The techniques of the physical examination were satisfactory with the following comments:
Standardized Patient comments
24
ORAL PRESENTATIONOutstanding Clear Pass Borderline Clear Fail
Timing, content, presentation, organization:
SOAP NOTE DOCUMENTATIONOutstanding Clear Pass Borderline Clear Fail
Subjective: The document portrays what was communicated in the examination room with the following comments: (ID information, CC, attributes, sequence of events, pertinent + and -, risks)
Objective: ____ VS ____ General appearanceThe document portrays what was performed in the examination room with the following comments:
Assessment and Plan: (Identified organ system; binary characteristics, acute vs. chronic, mild vs. severe, etc.; risk factors to make some diagnoses more likely.)
The above was discussed with the student named aboveInitial ___________________
25