university of medicine and pharmacy ”gr t. … doctorat...dysfunctional response of the response...
TRANSCRIPT

UNIVERSITY OF MEDICINE AND PHARMACY”GRIGORE T. POPA” IAŞIFACULTY OF MEDICINE
MEDICAL BRANCH
ABSTRACT OF THE DOCTORAL THESIS
Mălina CIUMAŞU-RÎMBUOccupational Health Physician
Management of occupational stress in the military.The possibilities of evaluation and therapeutics
Scientific advisorProf. Dr. CARMEN VULPOI
IASI2012

Key words:Occupational stress
MilitaryEvaluation
Therapeutics
TABLE OF CONTENTSINTRODUCTION.............................................................................1
Relevance of the research subject................................................1Chapter I............................................................................................2
OCCUPATIONAL STRESS FROM PSYCHO-NEURO-ENDOCRINOLOGY’S ANGLE .....................................................2
I.1. Concept of stress and homeostasis ...........................................2I.2. Mediators of homeostasis and stress system ............................4I.3. Occupational stress important part of modern stress..............10
I.3.1. Socio-economic impact of occupational stress.Quantification and management ...............................................10I.3.2. Occupational stress in the military ..................................13I.3.3. Occupational stress management programs in modernmilitary forces ...........................................................................16
Chapter II ........................................................................................18ADAPTOGENS AS HOMEOSTATIC MODULATORS...........18
II.1. Adaptogens- concept and criteria ..........................................18II.2.General Adaptation Syndrome. Adaptogen Conceptualization.......................................................................................................19II.3. The biochemical, molecular and phytochemical action ofadaptogens.....................................................................................23II.4. Adaptogens used in the research study..................................27
Chapter III......................................................................................32DYSFUNCTION OF STRESSOR RESPONSE AND UTILITY
OF ADAPTOGENS IN THEIR MODULATION .......................32III.1. Dysfunctional response of the response system in acute andchronic stress.................................................................................32III.2. Adaptogens’ role in regulating acute and chronic stressresponse dysfunctions ...................................................................35
PERSONAL CONTRIBUTIONS..................................................47Chapter IV......................................................................................47STUDY OF ASSESSMENT AND THERAPEUTIC OPTIONS
OF OCCUPATIONAL STRESS IN THE MILITARY FIELD .47IV.1 Motivation for choosing the topic.........................................47IV.2. Research hypothesis.............................................................48IV.3. Objectives ............................................................................48IV.4. Materials and methods .........................................................49

IV.4.1. Patients..........................................................................50IV.4.2. Method ..........................................................................53
IV. 5. Statistical data processing and analysis ..............................56IV.6.RESULTS .............................................................................56
IV.6.1. Study 1- evaluation of the occupational stress level andcomponents through validated simple questionnaires ..............56IV.6.2. Study 2- identification of the cardiac stress typology inemployees with predominantly desk work and highresponsibility...........................................................................123IV.6.3. Study 3- dishomeostatic response of the autonomicnervous system and of the HPA axis measured bycardiometabolic dysfunctions and implementation of apreventive pillar 2 scheme in employees exposed to multipletasking and extended working hours.......................................143IV.6.4. Study 4- identification of the typology vulnerable toalternating shift work in employees exposed to a sudden changein work schedule .....................................................................202IV.6.5. Study 5- dishomeostatic response of the autonomicnervous system and of the HPA axis measured bycardiometabolic dysfunctions and implementation of apreventive pillar 2 scheme in employees exposed to alternatingshift work and extended working hours..................................203IV.6.6. Study 6- exaggerated response alarm in employeesexposed to chronic occupational stress and implementation of apreventive pillar 2 scheme ......................................................211
IV. 7. Discussions .......................................................................220Chapter V .....................................................................................230
FINAL CONCLUSIONS OF THE RESEARCH.......................230REFFERENCES ...........................................................................232PUBLISHED WORKS .................................................................249
1
CURRENT STATE OF KNOWLEDGE
INTRODUCTION
Relevance of the research subjectContemporary socioeconomic status has influence on health
care strategies towards prevention.Optimum basal activity and reactivity to stress is vital for the
sense of wellbeing, succesfull complying with work assignments andproper social integration . Excessive or improper basal activity andreactivity to stress relates with behavioural and somatic dysfunctions.
Military environment associates well with a variety ofpsycological, physical, chemical and biological stressors whichmigth overburden the homeostatic mechanisms of the militaryemployee.
Best preventive interventions are made before military unitsare involved in high risk, high stress operations.
Finding individual stress reactive patterns during ordinaryoccupational health check might bring useful information on possibledysfunctions of the homeostatic mechanisms facing major stressorsin field operations, thus letting us aplly primary preventive measures.
Early treatment of dishomeostatic reactions as secondarypreventive measure implies efficient rehabilitation of the militaryemployee before this affects his collective assignment.
Tertiary preventive measures might rehabilitate entirely orpartially a well qualified key employee with stress pathology.
In our reaserch we propose to underline destinctive featuresof military organisation and find possibilities of occupational stressevaluation and therapeutics.
2
Chapter I
OCCUPATIONAL STRESS FROM PSYCHO-NEURO-ENDOCRINOLOGY’S ANGLE
I.1. Concept of stress and homeostasisAll organisms must mantain a complex, dynamic equilibrium,
or homeostasis, which is constantly challenged by internal orexternal adverse forces termed stressors. Thus, stress is defined as astate in which homeostasis is actually threatened or perceived to beso; homeostasis is re established by a complex repertoire ofbehavioral and physiological adaptive responses of the organism.
Stressors comprise a long list of potentially adverse forces,which can be emotional or physical. Both the magnitude andchronicity of stressors are important. When any stressor exceeds acertain severity or temporal threshold, the adaptive homeostaticsystems of the organism activate compensatory responses thatfunctionally correspond to the stressor.
The stress system has a major role in coordination of thisprocess through its central and peripheral functions.
I.2. Mediators of homeostasis and stress systemThe principal, greatly interconnected CNS effectors of the
stress system, include the hypothalamic hormones argininevasopressin (AvP), corticotropin releasing hormone (CRH), theproopiomelanocortinderived peptides αmelanocytestimulatinghormone and βendorphin, and norepinephrine produced in theA1/A2 centers of the brainstem’s locus ceruleus and in the central,autonomic nervous system. Serotonergic pathways that originatefrom the nuclei raphe and the posterior hypothalamic histaminergicsystems, accompany the locus ceruleus derived norepinephrinecentral stress response through secretion of 5 hydroxytryptamine andhistamine, respectively.
The principal peripheral effectors are glucocorticoids, whichare regulated by the hypothalamic–pituitary–adrenal axis, and thecatecholamines norepinephrine and epinephrine, which are regulated

3
by the systemic and adrenomedullary sympathetic nervous systems.Postganglionic sympathetic nerve fibers also secrete CRH, amongother substances, whereas both catecholamines stimulate interleukin(Il ) 6 release by immune cells and other peripheral cells viaβadrenergic receptors.
The targets of all these stress mediators include the executiveand/or cognitive, the fear/anger and reward systems, the wake–sleepcenters of the brain, the growth, reproductive and thyroid hormoneaxes, as well as the gastrointestinal, cardiorespiratory, metabolic, andimmune systems.
I.3. Occupational stress important part of modern stress
I.3.1. Socio-economic impact of occupational stress.Quantification and management
Modern societies are plagued by clusters of the so calledmultifactorial polygenic disorders (e.g. obesity, the metabolicsyndrome and type 2 diabetes mellitus).
Socioeconomical impact of occupational stress is huge: 300 billion dollars in work productivity and occupational
handicap 50% more costs for the healthcare system, 80 % of workers declare they are stressed at workplace, 50% need assistance in occupational stress management
Stress is ubiquitous and universally pervasive, however, itsobjective quantification has not been easy. International
study initiave (Collaborative International Study of ManagerialStress, 2002) involving institutions from 24 countries used twoinstruments of stress quantification: OSI-2 (occupational stressindicator) questionnaires with 90 indicators (e.g. occupationalstressors, stress sources, personality types - A and B, stressadaptability) or WHOQOL-100 Instrument – mesuing the qualityof life. The study founded in the first four places as occupationalstressors: overworking, loss of equilibrium between work andhome, negative workplace relationships and need ofresponsability.

4
I.3.2. Occupational stress in the militaryOccupational stress is a significant stressor in the military
profession. A 2002 study on 472 employees working on a USAmilitary base reports that 26% of participants suffer from intenseoccupational stress, 15% of participants suffer from significantemotional distress caused by occupational stress and 8% ofparticipants have health issues caused by it.
Military environment involves a great variety ofoccupational stressors like psychological, physical, chemical andbiological stressors.
The majority of studies concentrate on occupationalpsychosocial stressors, their relation with field operations andtheir dishomeostatic effect from psychological and psychiatricalpoint of view.
Field operation occupational stress it is not the only face ofstress at work in the military. Chronic occupational stress can becaused by multiple tasks, long working hours, ambiguity ofoccupational role, inadequat administrative support, low jobcontrol, tasks that do not match with employee’s potential beingover or undersolicitating, sudden coming and interfering withdaily work, responsability not equal with independence ofdecision, penury of positive feedback on efficacity of workperformance, tense occupational relationships, insufficientfinancial retribution.
Need for efficiency and performance of military personnelhas been recognized as a military research priority. If army wantsto remain a well rated employer it is obvious that our efforts andresources should be targeted towards the human resource andimplementation of good programs of occupational stressmanagement.
I.3.3. Occupational stress management programs in modernmilitary forces
In american army occupational stress control and preventivemedicine are recognized as independent and important functional

5
medical areas, part of „Force Health Protection” operational systemin field operations.
Occupational stress control it is applied according to thefollowing principle: „ Best preventive interventions are made beforeunits are involved in major risk operations”and targeted to all threelevels of prevention: primary, secondary and tertiary.
In canadian army forces the program of occcupational stressmanagement concentrates on first level of prevention takingmeasures on improving work environment, relationships inside theoccupational group ant its cohesion and efficient stress reactionstrategies to operational or daily,chronic stressors.
In indian military forces the program of occupational stressmanagement addresses to first two levels of prevention throughpromoting traditional relaxing tecniques like Yoganidra as dailytraining routine.
These programs were presented in order to underline thatoccupational military stress it is a major problem recognized by allmilitary systems and that there is a necessity to implement efficientand active management programs.
Chapter II
ADAPTOGENS AS HOMEOSTATIC MODULATORS
II.1. Adaptogens- concept and criteriaThe concept of adaptogens was introduced by russian
pharmacologist N.V.Lazarev whose 10 year studies concentrated onsintetic derivatives of bensimidasole starting from registered markdibasole.
Brekhman, student and disciple of Lazarev, moved totraditional phytotherapics used as tonics and suspected that thesesubstances had adaptogenic properties.
Differential criteria between adaptogens and tonics are asfollows:
1. An adaptogen should be completely harmless in itsaction, should have a wide therapeutic spectrum, a minum or none
6
effect on physiological functions and manifest its adaptogenicquality only facing adequate stressors;
2. Adaptogenic action should be non-specific anddefined as the capacitaty of rising resistance to a wide spectrum ofstressors;
3. Adaptogen should have a regulatory action no matterthe direction of the stressor.
From a large variety of tonics, Brekhman selectedaccording to above criteria only 4 adaptogens: Eleuterococcussenticosus (ES), Panax ginseng, Raponticum carthamoides şiRhodiola Rosea (RR) and observed that:
1. Raw plant modifies biochemical and anatomicalmanifestations of alarm phase and injuries associated with thisphase were no longer present..
2. Adaptogens convey to the organism a state of non-specific resistance to stressors and lesser alarm phase ordinaryinjuries.
3. Adaptogenic effect becomes obvious whenorganisms are overstressed otherwise they didnt prove that effect.
4. Adaptogens act on celular şi physiological level.Cells treated with adaptogens presented stimulation of proteicsynthesis and DNA replication. They also work as antioxidants.
5. Adaptogenic activity dues its characteristics at leastto the presence of saponines in its composition with differentlevels of intensity on their adaptogenic action.
Definition of adaptogens was reestablished byPanossian et al in 1999 as being a new class of metabolicregulators which had the ability to rise the adaptability of theorganism to environmental stressors and protect it from theirdamage. Today the concept of adaptogens is unanimouslyaccepted in scientific world.
Our studies introduce a new class of adaptogens thatis meristematic vegetal tissue which contains abscisic acid used byplant to adapt to different stressors.
7
II.2.General Adaptation Syndrome. AdaptogenConceptualization
Sensory adaptation is defined as the change in theresponsiveness of a sensory organ during a constant stimulus,resulting in the need of some increasing intensity stimuli toproduce the same answer. Physiological adaptation is defined as abiochemical change arising from the interaction of stressors andinvolves a more effective response to them. Such adaptivechanges lead the body from the previous homeostatic status to ahigher level of dynamic equilibrium (heterostasis) or the so-calledstate of non-specific resistance.
Regardless of the stressor’s nature the animal's response tostress involves every major system of the body. Selye called this"general adaptation syndrome (GAS): The sum of all nonspecificsystemic reactions of the body as a result of long-term chronicexposure to stress."
SGA is an intrinsic mechanism of resistance that enables thebody to react to stress factors. Selye discovered that SGA hasthree distinct and sequential stages: the alarm stage (AS) theresistance stage (RS) and the exhaustion stage (ES).
The alarm stage "all nonspecific phenomena that occur afterexposure to a stressor factor" is made of two stages: shock andcounter-shock.
The resistance stage occurs if exposure to the harmful actionof the stress factor continues for several days. Selye defined thisstage as "the sum of all nonspecific systemic reactions caused byprolonged exposure to the stressors to which the body becameresistant."
If the exposure to the stressor factor continues, the resistancestage shifts to the exhaustion stage. Selye defined this stage as"the sum of all nonspecific reactions that develop as a result of theexposure to the stressor factor to which adaptation was obtained,but can no longer be sustained."

8
In the mid-1900’s it was suggested that the state ofnonspecific resistance can be achieved either by graduallytraining the body to resist to the stress factor or by usingsubstances which may change the biological response and thedirect placement of the body in the heterostasis stage,pharmacologically active substances which have beensubsequently called adaptogens.
II.3. The biochemical, molecular and phytochemical action ofadaptogens
The stress protective activity of adaptogens is associated tothe activity of HPA axis and to the regulation of some keymediators of stress response, common to all cells, such as: Hsp 70and Hsp 16 heat shock protein, JNK 1 protein kinase, DAF-16FoxO transcription factor, mediators of HPA axis includingcortisol and glucocorticoid receptors, beta-endorphin, nitric oxide,ATP.
From the phytochemical point of view adaptogens arephenolic complexes or tetracyclic triterpenes / steroids. Phenoliccompounds are structurally similar to the catecholamines involvedin the initial stages of stress response. Triterpene compounds arestructurally similar to the corticosteroids involved in theprotective inactivation of the stress response system.
Meristematic tissues of plants contain plant hormones suchas auxins to stimulate cell growth and promote increased diseaseresistance, giberelines which stimulate protein synthesis andribonucleic acid, cytokines with protective role in cell mitosis,abscisic acid with adaptogen role to external or internal agents andethylene involved in maturation, growth inhibition and aging.
II.4. Adaptogens used in the research studyEleuterococcus senticosus - animal studies can determine
the possible mobilizing energetic impact by increasing the glucoseconsumption, the protective stress effect by changing the centralnervous, hormonal regulation. Military studies have focused onthe effects of ES on air and sea crews in extreme conditions

9
(tropical, arctic area) to demonstrate the recovery stimulationeffects (3 h vs. 1 day), against fatigue, antidepressants, anti-excitators, which regulate sleep disorders (aprox.700 participants).The studies performed on aprox.1500 athletes have shown theeffects ES has in increasing endurance, decreasing the recoveryperiod. The ES capacity to stimulate the auditory and visualacuity, the cognitive functions and reduce the overall incidence ofthe disease by 35% was also demonstrated.
Rhodiola rosea - Clinical studies have focused on the effectsof standardized extract to rosavin in chronic stress, resulting in theimprovement of mental fatigue, of sleep quality and quantity,emotional stability, motivation, psychomotor functions, mental,physical performances, decreased appetite, irritability,hypertension, headaches and leading to the improvement ofresistance to biological stressors.
Schisandra chinensis (SC) – the mechanisms of action aredue to the stimulation of Hsp 70 expression at the cellular levelwith neuroprotective role in the physical, intellectual stressors andinduction of the activity of P450 cytochrome withhepatoprotective role in the chemical stressor.
Crataegus monogyna şi oxyacantha (CMO) - pharmacologicaland clinical studies have demonstrated its heart function modulatoreffects, positive inotropic and chronotropic, antispasmodic, coronarydilator, antioxidant, anxiolytic, anti-inflammatory, antiviral,cholesterol lowering effect.
Olea europaea (OE) - pharmacological and clinical studies havedemonstrated its role of decreasing total cholesterol and overallhyper-lipidemia, hyper-beta-lipoproteinemia, normalizing hyper-beta-phospholipidemia and regulating total phospholipids,hypoglycemic and antioxidant role reducing cardiovascular andantiasthenic risks – strong effect on a pre-existing fatigue status.

10
Chapter III
DYSFUNCTION OF STRESSOR RESPONSE AND UTILITYOF ADAPTOGENS IN THEIR MODULATION
III.1. Dysfunctional response of the response system in acute andchronic stress
Acute stress can cause allergic symptoms such as asthma,eczema, nettle rash, angiokinetic phenomena: migraine,hypertension or hypotension outbursts, various types of aches:headaches, abdominal pains, pelvic pains, back pains,gastrointestinal symptoms: indigestion, diarrhea, constipation,panic attacks and psychotic episodes.
Pathogenesis of chronic stress-related disorders is explainedby excessive and sustained secretion, and thus long-term effects ofstress system mediators which influence various homeostaticsystems leading to behavioral and somatic disorders: essentialhypertension, visceral fat accumulation, reactive insulin hypersecretion, decreased glucose tolerance, 2nd type diabetes, hyposecretion of growth hormone, hypogonadism, sarcopenia,osteopenia, osteoporosis, dyslipidemia and last but not leastacceleration of atherosclerosis, with its suite of cardiovascular andneurovascular after effects.
III.2. Adaptogens’ role in regulating acute and chronic stressresponse dysfunctions
Table 1. Adaptogens - pharmacological profilesAdaptogens pharmacological effects RR ES SCCNS stimulation: increases the physical andcognitive performance (learning and memory)
+ + +
Neuroprotective + +Hepatoprotective + + +Cardioprotective + +Gastroprotective + +Antioxidant and radioprotective + + +Anti-atherosclerotic + +
11
Vasodilatator/hypotensive +Gluco-regulatory +Anti-inflammatory/anti-allergic + + +Immunotropic + + +Anti-depressive +Tranquilizer + +
The most convincing studies are those that show theeffectiveness of adaptogens in terms of neuro-protective effectsand of cognitive and mental performance functions in fatigue, inasthenia and depression. A very recent study (Panossian 2012)shows that a standardized combination of adaptogens exercise itsstress protective effect by stimulating the NPY expression andrelease from the neuroglial cells into the systemic circulation as adefense intrinsic response providing thus the practical tools for theNPY expression positive regulation theory as the basis of asuccessful behavioral adjustment to stress which has beenpreviously postulated by Thorsel and Heilig.
PERSONAL CONTRIBUTIONS
Chapter IV
STUDY OF ASSESSMENT AND THERAPEUTIC OPTIONSOF OCCUPATIONAL STRESS IN THE MILITARY FIELD
IV.1 Motivation for choosing the topicOccupational stress is a significant risk factor affecting a
significant segment of the military population and causing importantconsequences on the health and performance of job duties.
In the military field homeostatic dysfunctions caused byoccupational stress do not necessarily occur as a result of anincreased occupational stress level, but rather as an erosion ofindividual adaptability. They may result in organizational andindividual repercussions on the health of the employee in the short or

12
long term and may adversely affect military missions in times ofpeace or war.
The need to maintain the performance and efficiency ofmilitary staff has been recognized as a military research priority.
Occupational stress management programs running onmodern armed forces focus mainly on measures related to pillar 1and 2, primary and secondary prevention, with positive changes inthe working environment, education for the increase of the individualsystem resistance to the stressors, relaxation techniques. Militaryoccupational stress is a significant issue which applies to all systemsthat require the implementation of efficient and active managementprograms.
IV.2. Research hypothesisResearch hypotheses are related to the peculiarities of
occupational stress in the military field and the prevention and / ortreatment possibilities. We assume that:
- The level of chronic military occupational stress issignificant; there are parts of the work process influencing thestress level. The occupational stress is an important component ofthe daily stress compared to the extra-occupational one, there arefactors outside the work environment, with a cumulative ordeterminant role in overload and facilitating individual structuralresorts
- There stressful typologies: personality structures moreprone to dyshomeostatic response to occupational stress factors,unhealthy behavioral attitudes with favoring or cumulative roleand occupational features with a high risk potential.
- The significant occupational stress level causesdysfunctions of the autonomic nervous system and hypothalamic-pituitary-adrenal axis early measurable by cardiometabolicparameters and, in particular, because military chronic stresscauses an early measurable exaggerated alarm reaction in thecardiovascular parameters of an employee exposed to a newstressor which can be readjusted using adaptogenic substances.
13
- The introduction of adaptogens as substances mediatingstress response acts in addition to preventive standard programs ofoccupational risk management in the military field.
IV.3. ObjectivesThis paper is circumscribed to the military priority research
direction that focuses on improving the performance andefficiency of military employee who works in a complex anddiverse environment in terms of occupational stressors. Thestudies carried out in the occupational medicine room within theMilitary Hospital Iasi focus on occupational stress componentsspecific to the military organization: heavy workload, long hoursand alternating shift work identify early homeostatic dysfunctionof the autonomic nervous system and hypothalamic-pituitaryadrenal axis and propose a solution suitable for the specific of theRomanian forces: using phytoadaptogens as homeostaticmodulators.
The main objective of the research is to create a pilotmodel for the prevention of adverse effects of occupationalstress which applies in the occupational medicine routine.
To achieve the main objective secondary endpoints wereestablished per stage as follows:
► assessment of occupational stress in the military field,► identify the components of military occupational stress,► identify the dominant personality profile of the target
population vulnerable to a specific component of occupationalstress,
► identify the effects of the occupational component onthe target population,
► propose, organize and implement effective preventiveand practical schemes to improve the standard of preventionprograms for pillar 1 and 2, using adaptogenic substances.
The purpose of research is to implement these schemes inthe daily, routine practice from any occupational medicine room,the occupational physician being an important pillar in screeningthe population involved in the work processes, both in terms of
14
possible pathologies caused by occupational stress and in primary,secondary and tertiary prevention of the above mentionedpathology.
IV.4. Materials and methodsThis paper consists of 6 studies that derive from each other
in order to assess occupational stress (ESO), identify the targetpopulation vulnerable to a specific component of occupationalstress, and indentify the effects of the occupational component onthe target population, proposing, organizing and implementingearly prevention schemes.
The 1st Study is a cross-section study, a survey typequestionnaire (Ilie 2004) and consists in assessing the level ofoccupational stress and its components in the military field. So weproceeded to design useful questionnaires serving this goal byadjusting some validated questionnaires used for this purpose bythe Department of Teacher Training within "Gh Asachi"Technical University to the military occupational specificcharacter. The questionnaires thus elaborated were applied on asample of 145 subjects from the military population andunderwent the validation process within the same department.
The next stage of the research sought to identify the targetpopulation vulnerable to a specific component of occupationalstress and potential dyshomeostatic effects of this component onthe target population:
The 2nd study is a prospective study conducted on a groupof soldiers carrying mostly office activities, but with highresponsibility, selected from the 145 subjects who have completedthe first stage of the research process.
The aim of the study is circumscribed within the militarypriority research direction and Pillar 1 and 2 of occupational stressmanagement program, namely primary prevention by identifyinga stress typology, of some unhealthy attitudes and of someoccupational characteristics of a high risk potential andsecondary prevention by identifying reversible dysfunctions of
15
the autonomic nervous system, essential component of the stressresponse system.
Of items followed during the first stage were mention: theranking of the subjective perception of specific militaryoccupational stress on a 1-10 scale, the single or multiple causalitythereof, the predominance of one or more components ingenerating stress levels and individual adjustment strategies used,namely substance use potentially modifying the autonomicnervous system. In selecting the group, it has been consideredoccupational characteristics of high cardiovascular risk withcumulative value for the dysfunctions noticed.
The third stage of the research process aimed to propose,organize and implement early preventive schemes:
The 3rd study is a randomized open-label study made on agroup of soldiers with different responsibilities and roles in theorganization which were selected from the 145 subjects who haveundergone the first stage of the research process in order toconfirm the conclusions of the 2nd study on an expanded groupand generate early prevention schemes for the modifications of theautonomic nervous system of the military personnel examinedcaused by chronic occupational stress during routine occupationalmedical assessments.
Applying the research pattern of the 1st, 2nd and 3rd studies inthe following two studies we noticed another feature of the militaryoccupational stress: the quick adjustment to a spontaneous change inthe work scheme in a group of soldiers with alternating shift work andovertime work. The change consisted in reducing the number ofemployees and redistribution of the same tasks to the employeesavailable.
The 4th study is a prospective study on a group of soldierswhich has a particular employment situation, with a total of 50 hoursof work per week, alternating shifts of 24 hours with a reducedrecovery period (24h) due to downsizing. Soldiers underwent aprocess of rapid, potentially dyshomeostatic adaptation. The aim ofthe study was to identify the target population vulnerable to

16
alternating shift work and long hours, by quantifying cardiometabolicdisorders in the inadequate process of rapid adaptation.
The 5th study is an open label randomized study conducted inorder to generate early prevention schemes for the employees in theprevious target group (study 4) who underwent dysfunctions of thestress response system, manifesting a reduced tolerance to alternatingshift work and overtime.
Based on the research pattern established in the first threestudies, the latest study aims the peculiarity of exaggerated alarmreaction in the military employees with chronic occupational stressexposed to a new stressor. This simulates the adaptation of a militarypresenting chronic barracks stress who has to do with new, heavystressors in the theater of operations:
The 6th Study is an open label randomized study conducted ona group of soldiers with chronic occupational stress and exposed to anew low intensity stressor: routine occupational medical assessment.The cardiovascular dysfunctions measured were considered theexpression of a typical exaggerated alarm reaction and anxiousbehavior of the subject with chronic exposure to occupational stressand dysfunctions of the NPY system that causes him to be hyperreactive to new stimuli. The study aims to generate an earlyprevention scheme applicable on employees with exaggerated alarmreaction before they are involved in large-scale activities in thetheatres of operations.
IV.4.1. PatientsResearch was conducted over a period of about three years
(2009-2012) in the occupational medicine room within theMilitary Hospital Iasi. Patients were recruited from among theemployees who were performing routine occupational medicalassessment.
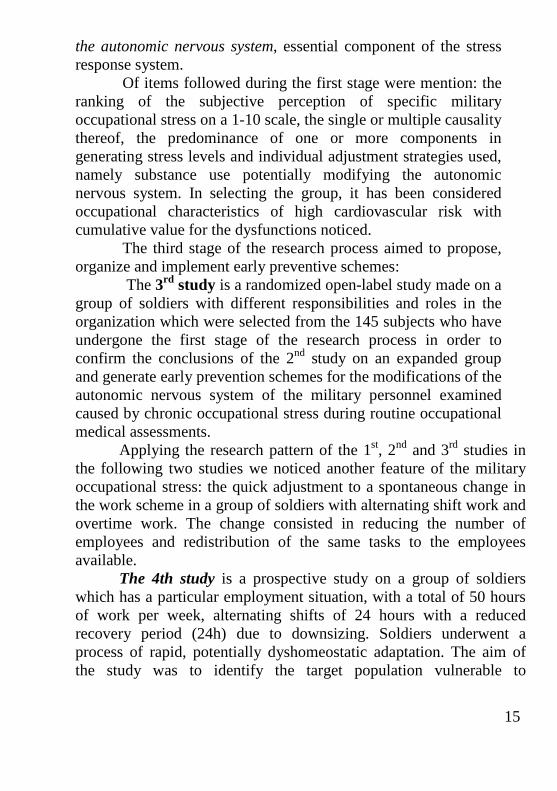
Of the total 9500 patients assessed during this period in theoccupational medicine room a total of 221 subjects (Fig. 1) wereselected according to the following criteria:► Criteria for inclusion1. aged 25-53 years
17
2 employees who subjectively perceived the change of the newwork scheme (only for the 4th study) with long hours, alternatingshift work and reduced recovery time as the main reason ofoccupational stress3. desk work with high responsibility4. apparently healthy status5. no significant heredo-collateral history6. Average arterial blood pressure ≥ 140/80 mmHg7. resting heart rate ≥ 80 beats / minute8. signed and dated consent► Exclusion criteria1. cardiovascular disease2. endocrine disorders3. neurological disorders4. normal cardiovascular parameters (studies 3, 5, 6)
The studied population did not include subjects withchronic debilitating diseases or psychiatric disorders.
All patients signed the consent form.
Figure 1. Schematic representation of the groups per studies

18
Legend:* inclusion and exclusion criteria1st Study – questionnaire type survey, assessing the occupational stresslevel by ESO questionnaire on 145 patients;2nd Study – prospective type, identify the types of reaction to cardiacstressors in the employees with desk work and high responsibility, cardiacstressor study group (blood pressure ≥ 140/80 mm Hg, resting heart rate ≥80 beats / minute); non cardiac stressors witness group (blood pressure<140/80 mm Hg, resting heart rate <80 beats / minute);3rd Study - open label, randomized type checking cardiac stressors’typology on an extended group (114 patients) and implementation of ascheme for the prevention of pillar 2 (27 patients) for cardiac stressors;the study group received adaptogen and lifestyle counselling, the controlgroup received only counselling;4th Study - prospective type; identifying vulnerable typology for thealternating shift work and overtime, study group - patients withcardiometabolic disorders arising from unexpected change of workschedule, the control group - patients without cadiometabolicdysfunctions;Study 5 - open label, randomized type, implementing a pillar 2 preventionscheme to the employees with cardiometabolic dysfunctions from the 4th
study, study group received adaptogen and counselling on lifestyle,control group received only counselling;Study 6 - open label, randomized type; assessing exaggerated alarmresponse for an employee with chronic stress exposed to a new mildstressor and implementing new, pillar 2 schemes for prevention; studygroup - received adaptogen and counselling on the harmful lifestyle,control group –only counselling.
IV.4.2. MethodIn the 1st study in order to assess occupational stress and
stress component at the work place we adjusted a questionnairealready used by the Department of Teacher Training within "GhAsachi" Technical University by adding 2 items specific to themilitary field. The final version of the questionnaire has a numberof 136 variables and 22 items of which 10 variables concern theformal identity of the subject, 90 opinion variables and 36occupational/professional stress assessment variables (SOIP),including control items of answer truthfulness.
The opinion variables provide information regarding:
19
► measures to increase work capacity, the degree andextent of use of the methods to improve performances, about thechoice of medical or psychological services in case of overload,the significance of one’s workplace success, the influence ofcompetition between co-employees, relaxation, sleep, sources ofincome, expenses, degree of desire to change performances, orderof acceptance of the requests from the organization on a regularbasis, in the situation of risking to lose one’s job and in theconditions of promotion and about peer relationships, namely withthe higher structures/managers.
The questionnaire was applied to 145 subjects, who filledit out on paper, without a time limit, in a separate space forperforming the clinical examination. The subject’s identity wasprotected given the specific organization and we remind thatbefore filling out, the subject signed the informed consent (Annex1). The completed questionnaires were then subjected to avalidation process. The validation procedure was to establish thevalidity through factorial analysis and its fidelity through theanalysis of its internal consistency, namely the Cronbach’s Alphaindex and it was done by the Department for Teacher Training,“Gh.Asachi” Technical University, Iaşi.
In study 2, the 31 military employees with administrativeactivities and high responsibilities who had previously filled outthe validated questionnaires for the evaluation of occupationaldemand (Annex 2), underwent a clinical examination,measurement of the cardiovascular parameters: systolic anddiastolic blood pressure and resting heart rate.
The evaluation questionnaire mainly focused on theclassification of the occupational stress level on a scale from 1 to10, its singular or multiple causality and the predominance of oneor more descriptive items of the causality in perceiving the degreeof damage.
Also, information was retained about the strategies toadapt to occupational stress, that is those with cardiovasculardishomeostatic potential, nicotine and caffeine, and characteristics

20
of the work process were taken into consideration, which have acumulative role in the observed dysfunctions of the autonomousnervous system: the prolonged sitting position, the sedentaryoffice work.
The results were communicated to the command segmentwith the intention of its active involvement in taking preventivemeasures given that the primary responsibility rests with it to a largeextent.
In study 3, done in order to generate some early preventionschemes of the autonomous nervous system changes and toconfirm the conclusions of study 2 in what concerns the existenceof the cardio-stressing typology; all subjects involved in the studywho had already filled out the evaluation questionnaires (114)underwent a clinical examination, measurement of thecardiovascular parameters, systolic and diastolic blood pressureand heart rate.
In the next phase, the 27 employees with a cardio-stressingtypology (changed cardio-vascular parameters) an additionalDECAS personality inventory-questionnaire was applied, basedon the structure of the Big Five personality model (Annex 3). Theinterpretation and use of these licensed questionnaires waspossible due to the collaboration with the Department for TeacherTraining, „Gheorghe Asachi” Technical University, Iaşi. Thequestionnaire contains 90 items and 8 raw scores.
The items address the 5 personality dimensions describedby the concepts of openness, extraversion, conscientiousness,agreeableness and stability.
The results are interpreted from a quantitative standpointthrough two types of standard scores, T quotas and percentiles.The instrument also contains possibilities to appreciate the degreeof reliability in the results, implicitly of the distorted answersbecause of social desirability, approval or random answers.
Also, the 27 employees were drawn blood in order to measureglycaemia, total cholesterol and serous triglycerides, the metabolicparameters considered suggestive for the dyshomeostasis of thehypothalamic-pituitary-adrenal axis. Blood was drawn in basic
21
conditions, on empty stomach, 12 h from the last meal, in themorning between 7 and 9 through a vacutainer-type closed system,Beckson-Dickinson tubes. The blood was submitted to centrifugationand the serum was separated. 4-5 ml of blood were used from eachpatient and the sample analysis was done in the Medical AnalysisLaboratory from the Iaşi Military Hospital through thespectrophotometric (enzymatic-colorimetric) method. The normalvalues used as standard for the measured values were the following:
► Glycaemia- 70-106 mg/dl► Total cholesterol - optimum < 200 mg/dl► Serous triglycerides - optimum < 150 mg/dl
Of the items of the demand evaluation questionnaire, thefollowing were retained: the subjective perception of occupationalstress, noted on a scale from 1 to 10, 10 being the maximum levelof intensity of the felt stress, the specified occupational stressfactors which determine the inclusion in the aforementioned scale:multiple tasking, responsibilities, relations with the managers,subordinates or peers, order contradictory-ambiguous, workconditions and other unmentioned stress factors with thepossibility of multiple answers and harmful means of coping withthe stress factor – use of disturbing potential on the autonomousnervous system and with cardio-vascular risk: nicotine andcaffeine.
In the next phase of research, the study group received astandard adaptogen substance from embryonic plant tissues(Corphyt-Plantextrakt Cluj) 2 ml twice a day, morning andevening, 3 months, and they were advised regarding the change ofharmful eating habits and the use of potentially dysfunctionalsubstances upon the autonomous nervous system, while thewitness-groups did not receive the adaptogen substance, howeverit was advised regarding the changes of the harmful eating habitsand the used of potentially dysfunctional substances upon theautonomous nervous system. After 3 months, the subjects were re-assessed through a clinical examination and their cardio-vascular
22
and metabolic parameters were measured: glycaemia, totalcholesterol, serous triglycerides in the conditions described abovein the preceding phase.
The plant embryonic tissues of Corphyt: Crataegusmonogyna, oxyacantha, Olea europaea, are obtained through astandard method. The chosen vegetal embryonic tissues containboth abscisic acid used by the young tissue for adapting toenvironmental stress factors and present only at this level ofresearch, as well as cardio-metabolic regulating propertiesdetailed in the theoretical part and present in the young and adultplant. The detailed phytochemical studies in order to identify theclasses of active compounds require modern analytical methods,such as cromatography and spectrophotometry. Corphyt isstandardized in hyperoside minimum 2% mg/ml.
In study 4, the hypothesis considered the possibility ofgenerating cardio-metabolic dysfunctions as a result of the stressfulchanges in the daily occupational routine through the mechanism ofdesynchronization of the physiological systems rhythmicality in thetarget group with low tolerance for work in shifts (MSA) and longhours (OP).
The 36 military men working long hours and in shifts, factorswhose characteristics had recently changed following the reductionof the number of employees and the redistribution of the same tasksto available employees, underwent a clinical examination with themeasurement of their cardio-vascular parameters: blood pressure,resting heart rate.
The employees filled out the questionnaires to evaluate thelevel of occupational stress. The subjective perception, causality andstrategies to adapt to stress were the retained items.
Also, the 36 employees were drawn blood in order to measureglycaemia, total cholesterol and serous triglycerides, the metabolicparameters considered suggestive for the dyshomeostasis of thehypothalamic-pituitary-adrenal axis. Information connected to blooddraw, analysis and normal values are detailed in study 3.
The values resulted following the measurements werestatistically evaluated between the 2 batches and for the additional

23
study batch were compared with the ones already existing in the database from the occupational medical check-up prior to the newlycreated situation.
All employees included in the study worked more than 50hours a week and in long shifts with a reduced recovery period (24hours) because of the personnel reduction. The previous work schemein shifts required a 48 to 72 hours rest period after the 24 hour shiftand the results shall be presented below.
In study 5, done in order to evaluate a prevention scheme foremployees in the previous target group, with low tolerance for MSAand OP and cardio-metabolic dysfunctions, employed from the studybatch received a standardized adaptogen substance (Eleuterococcussenticosus - Alevia, Fălticeni) - in eleuteroside 0.4%, tablets of 250mg in a multi-dose scheme, 1 tablet twice a day, for 3 weeks and wereadvised regarding the change of harmful behavioral patterns: use ofcaffeine, nicotine, disorganized diet and the employees in the witnessbatch received only counselling. After 3 weeks, the patients were re-assessed through a clinical examination and their blood pressure andmetabolic parameters were measured: glycaemia, cholesterol andtriglycerides and the results are presented in the next chapter.
In study 6, done in order to assess the exaggerated alarmreaction to new stress factors, the employees exposed to a chronicoccupational stress, we considered the routine occupational medicalevaluation as a new stress factor, of low intensity and measuredcardio-vascular dysfunctions (blood pressure ≥ 140/80 mmHg andcardiac frequency >80 beats/minute) as an exaggerated alarm reactionand anxious behaviour typical to the subject chronically exposed tooccupational stress and dysfunctions of the NPY system which makeshim be hyper-active to new stimuli. The study batch received thestandard protocol for preventing occupational stress: counselling for ahealthy lifestyle and an additional standard combination (eleuteroside0.4%, schizandrine 2% rosavine 5%) of adaptogen substances -Adaptonic- Eleutherococcus senticosus extract (root), Schizandrachinensis (fruit) and Rhodiola Rosea (root), made by Alevia,Fălticeni, in a multi-dose scheme 1 tablet twice a day for 30 days. Thewitness-batch received only the standard prevention protocol:
24
counselling for a healthy lifestyle. Our research hypothesis is that theNPY stimulation through Adaptonic will improve tolerance to newstress factors of subjects chronically exposed to occupational stress.The employees were re-evaluated after 30 days and were re-exposedto the same stress factor of low intensity, observing the alarm reactionby measuring their cardio-vascular parameters.
ES, RR and SC were chosen for their adaptogen propertiesdetailed in the theoretic part and argued by numerous and solidstudies.
IV. 5. Statistical data processing and analysisThe data statistical processing was done by computer using
SPSS 11.0, for both validating occupational demand evaluationquestionnaires in the Department for Teacher Training at the„Gheorghe Asachi” Technical University, Iaşi, and the rest of thedata. Descriptive statistics tests were used: average, standard, mediandeviation and those for inferential statistics were used according to thedata supplied by the distribution tests, as follows: parametric- onesample t-test, paired sample t-test, ANOVA and non-parametric: chi-test. The Pearson, namely Spearman correlation was used. Thegraphic representation were histograms, pie, line, scatter, Excell 2007being used beside SPSS 11.0 due to its programme graphic design.The eigen-value coefficients, Catell’s scree test, the Varimax rotationmethod and the internal consistency analysis method were also usedfor validation.
IV.6.RESULTS
IV.6.1. Study 1- evaluation of the occupational stress level andcomponents through validated simple questionnaires
All employees are military men aged between 20 and 53. Thissection has two distinctive parts: the validation and the statisticinterpretation of the questionnaires applied on a sample of 145 malemilitary employees exposed to occupational chronic stress.
25
The validation of the questionnaires was conducted by theTeachers’ Training Department within „Gheorghe Asachi” TechnicalUniversity of Iasi.
For validity, the factorial analysis was performed on the maincomponents based on the correlations between 34 variables. Initially,12 factors were extracted that had coefficients eigen value greaterthan or equal to 1, with a total variance of 62.216%. This value ishigher than 40%, thus showing a satisfactory validity. The evaluationof the indices eigen value and of the chart resulted after Catell’sScree test indicates a clear break after the third component and,therefore, suggests grouping the variables into three categories offactors.
The Varimax rotation method was used for the calculation ofthe items’ saturation in each factor. We specify that the saturationvalues below 0,30 have led us to remove five items of the statisticalprocessing.
To verify the fidelity of the instrument, we used the internalconsistency analysis method by calculating the coefficient Alpha.The 29 items retained from the factor analysis were subjected tostatistical calculations using SPSS 11 for Windows. We have a goodinternal consistency of the scale since Cronbach’s Alpha reached.6644. For each factor, Alpha index is: Fl =.6708; F2 = .6800; F3=.5803
The results of the statistical processing of the validatedquestionnaires:
For the studied cases, the subjective perception of theoccupational solicitation was registered to reach in average 6.04 ±1.67 and based on the stress level the most stressful features seem tobe multitasking work and interpersonal relations.

26
Fig.2. Average values of the scores for the most stressful dutyfeatures
In order to increase work capacity, most frequently employeesmade use of the rationalization of the working time and itsprolongation. Also, in order to improve performance, most frequentlyparticipants chose to practice sport and consume coffee, chocolate,nicotine, energy drinks and less food supplements.
Under over-stress, among the physician’s proposals, theypreferred changing their lifestyle, including diet control; among thepsychologist’s proposals, they preferred the diagnosis of the potentialstaff of emotional and intellectual effort.
It is noted that individual therapy correlates directly with thelevel of stress (r = 0,293) and that group therapy correlates with thediagnosis of the potential staff of intellectual and emotional effort (r= 0,228).
For the studied cases, it is noted that the use of herbalmedicines is correlated directly with the level of stress (r = 0,201),diet control (r = 0,363), Yoga initiation (r = 0,313), food supplementsconsumption (r = 0,702) and supportive drug therapy (r = 0,388).
The most common solicitations from the institution usuallyhave been additional work assignments (80,7%) and long workinghours (74,5%) that were accepted by employees.
27
Additional work assignments directly correlate withpsychological counselling acceptance (r = 0,165), medical adviceacceptance (r = 0,229), use of stimulant medications available overthe counter in pharmacies (r = 0,297) and acceptance of gymnasticsat work (r = 0,238).
Extending working hours significantly correlated withacceptance of gymnastics at work (r = 0,204).
The most common solicitation from the institution at risk wereadditional work assignments (99,3%) and long working hours(76,6%) that were accepted by employees.
Additional work assignments directly correlate with medicaladvice acceptance (r = 0,242) and consumption of food supplements(r = 0,200).
Extending working hours significantly correlated withpsychological counselling acceptance (r = 0,172), medical adviceacceptance (r = 0,202), food supplements consumption (r = 0,365)and use of stimulant medications available over the counter inpharmacies (r = 0,287).
The most common solicitations from the institution to promoteworkplace were additional work assignments (95,2%) and longworking hours (75,2%) that were accepted by employees.
Additional work assignments directly correlate with extendingworking hours (r = 0,293), use of new drugs in order to test them (r =0,167) and Yoga initiation (r = 0,214).
Extending working hours significantly correlated withgymnastics performance at work (r = 0,230).
Medical counselling significantly correlated with foodsupplements consumption (r = 0,297) and gymnastics at work (r =0,204).
11.7% of the subjects from the study group are not influencedby competition between colleagues; nonetheless, for these subjects, itcan be noted a stress level with scores ranging between 2 and 8, theaverage value being 5,71, whereas 2,1% of the subjects declaredthemselves inhibited by the competition between colleagues, with alevel of stress placed in the range 5-10 and an average score of 8.The remaining subjects (86,2%) consider competition between

28
colleagues stimulating, but the average value of the stress level was6,05.
The feeling that the image was improved among colleagues andbefore leaders was significantly increased as compared to theimprovement of the image among friends.
For the studied cases, the material benefits are more popular ascompared to chances of promotion in schools or companies ratedhigher.
Occupational stress level is increased in subjects preoccupiedby the improvement of the image in society (r = -0,166).
An improved image in the eyes of colleagues directly correlateswith an improved image in society (r = 0,190), but also with materialbenefits (r = 0,189).
For the studied cases, mean scores of the relation with theinstitution, managers or administrative board highlighted that fairplay was assessed against the criteria and evaluation measures andtransparency of the promotion opportunities.
Occupational over-stress directly correlate to the materialitythreshold of 95%, with family solicitation (r = 0,177).
It appears that subjects are working daily between 8 and 16hours, most commonly 8 hours (44.8%), yet 14.5% of the subjectsexceed 12 working hours per day.
Based on the main expenditure other than food and housing,most commonly are noted rates with a frequency of 66.9%.
Occupational stress level has not showed significant correlationwith parameters such as: attention, memory, fatigue, efficiency,correlation of information, flexibility, focus, judgment, cooperation,sociability.
It should be noted that the desire to be more understanding withthe others is lower in subjects with high occupational stress level (r =-0,214, p = 0,01), the correlation being indirect, statisticallysignificant.
The occupational stress level did not present any significantdifferences neither in terms of environment of origin (p = 0,274) noras regards the current residing place (p = 0,217), most participantsliving in the urban area.
29
IV.6.2. Study 2- identification of the cardiac stress typology inemployees with predominantly desk work and high responsibility
Of the 31 military men performing mostly office work of highresponsibility, aged 25-53 (40,51 ± 5.9) years, 19 (61.29%) hadaverage blood pressure (TAm) ≥ 140/80mm Hg: TAsm (averagesystolic blood pressure) -144.10 ± 10,5 mm Hg, TAdm (averagediastolic blood pressure) -82.78 ± 6.8 mm Hg and resting heart rate ≥80 beats/ minute (FCr - resting heart rate - 83.26 ± 8, 9 beats/minute), being included in the group of cardiac-stressors (CS). The12 subjects whose cardiovascular parameters were within normallimits (TAm <140/80mmHg, FCr <80/min) constituted the controlgroup of non-cardiac-stressors (nCS) with TAsm-122.08 ± 8.38mmHg, TAdm- 72.08 ± 6.89 mm Hg and FCr- 71.25 ± 5.47 FCR beats/minute. There were statistically significant differences between the 2groups’ parameter diastolic blood pressure (p-0,0001) andstatistically insignificant differences in what concerns TAsparameters (p-3.1) and FCr (p-3.5), except that for the last 2parameters, the average values were higher in cardiac stressors.
It is noted that the average level of occupational stress in thegeneral group is 7.19 (Table 2) with 7.21 for CS as opposed to 7.16for nCS.
Table 2. Descriptive statistical analysis for the cases of exposureto occupational stress for the general group- by level of
occupational stressVariable Indicators Statistics (years) Standard error
No. of casesMedia
Age Reliability range Inf. limitfor the average of 95% Sup. limit
VariationStandard deviation (+/-)MinimumMaximum
317, 19356,54147,8457
3,1611,778005,0010,00
,31934

30
High work volume/ multitasking was the most frequentlyincriminated occupational factor, followed by the specificresponsibilities and restrictions of the military system.
The higher the age, the higher the level of occupationalsolicitation felt by a subject. It was noted that there is no correlationbetween occupational composition and age (p = 0,848).
Occupational stress is associated with an increasedconsumption of substances potentially disturbing for the autonomicnervous system. There is a direct, weak, significant correlationbetween the caffeine consumption and stress level at work;nonetheless, there is no statistical correlation between theconsumption of nicotine and occupational stress level. Also, there isno correlation between stress coping strategies and cardiovascularparameters or occupational components.
There is a direct, weak, significant correlation between theoccupational stress level and body weight (p = 0,027), 10,52% (BMI31.5 ± 0,9) of the cardiac stressor lot of subjects and 16.66% (BMI30,27 ± 0,12) of the control group subjects were diagnosed withgrade I obesity (p 0,05).
IV.6.3. Study 3- dishomeostatic response of the autonomicnervous system and of the HPA axis measured by
cardiometabolic dysfunctions and implementation of apreventive pillar 2 scheme in employees exposed to multiple
tasking and extended working hours
The average age of subjects did not differ statistically betweenthe analyzed groups (p = 0,825), the age reaching the average valueof 35 years, varying between 24 and 45 years. Depending on theoccupational stress level values, there were not significantdifferences between the investigated groups (χ2=0,64; df=3;p=0,887).
There were significant differences in all parameters in thestudy group that received adaptogens and the parameters of diastolicblood pressure as well as the metabolic ones in the control group (p<0,05). Statistically insignificant differences were recorded for

31
systolic blood pressure parameters (p-0, 516) and the resting heartrate (p-0, 318) in the control group. We note that even for thesignificant differences, these were higher in the study group.
Coping strategies did not differ significantly between the 2groups. Depending on personality, stand distributions of theoccupational stress level with strong differences statistically speaking(p = 0,000): the highest average values of the occupational stresslevel are found in type N subjects in which emotional stability isessential (8.71 ± 0,91); with variations between 6 and 7, in subjectswith agreeable personality, there is an average value of occupationalstress of 6.33 ± 0,52; in subjects with open profile, extraversion andconscientiousness, the average value of the occupational stress levelwas 5, without changes of the series of values.
Fig. 3. Average values of the level of occupational stressdepending on personality
Of the monitored parameters, only systolic blood pressureshowed significant differences depending on personality: TAS wassignificantly higher in subjects with altered emotional stability (p =0,000).
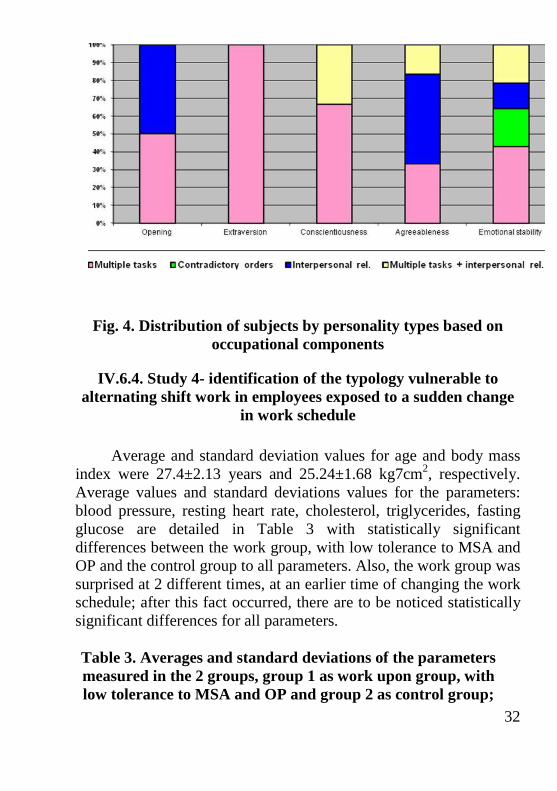
Frequency distribution of subjects according to the personalityand the occupational component was statistically significant(χ2=8,407; df=4; p=0,038).
32
Fig. 4. Distribution of subjects by personality types based onoccupational components
IV.6.4. Study 4- identification of the typology vulnerable toalternating shift work in employees exposed to a sudden change
in work schedule
Average and standard deviation values for age and body massindex were 27.4±2.13 years and 25.24±1.68 kg7cm2, respectively.Average values and standard deviations values for the parameters:blood pressure, resting heart rate, cholesterol, triglycerides, fastingglucose are detailed in Table 3 with statistically significantdifferences between the work group, with low tolerance to MSA andOP and the control group to all parameters. Also, the work group wassurprised at 2 different times, at an earlier time of changing the workschedule; after this fact occurred, there are to be noticed statisticallysignificant differences for all parameters.
Table 3. Averages and standard deviations of the parametersmeasured in the 2 groups, group 1 as work upon group, withlow tolerance to MSA and OP and group 2 as control group;

33
tas,tad,fcr,col,trg,gb are blood parameters representingsystolic, respectively diastolic blood pressure, resting heart
rate, cholesterol, triglycerides and fasting glucose; p-p value<0,05-statistical threshold, prm-parameter
Prm Group 1 Group2 Ptas 161±10,58 122.18±9.65 1.97x10-13
tad 94.75±4.43 74.37±5.43 4.41x10-13
fcr 98.4±8.65 69.31±6.62 3.62x10-12
col 271.6±37.5 159.81±18.61 0,45x10-12
trg 200±47.31 85.62±20,64 1.22x10-10
gb 117.2±8.03 84.25±5.4 2.44x10-16
IV.6.5. Study 5- dishomeostatic response of the autonomic nervoussystem and of the HPA axis measured by cardiometabolic
dysfunctions and implementation of a preventive pillar 2 scheme inemployees exposed to alternating shift work and extended working
hours
Cardio-metabolic parameters values decreased significantly inboth groups except that the diastolic blood pressure increasedsignificantly in the control group. It has to be noted that for the studygroup that received adaptogens, differences were higher.
IV.6.6. Study 6- exaggerated response alarm in employees exposedto chronic occupational stress and implementation of a preventive
pillar 2 scheme
The average age of subjects did not differ statisticallybetween the analyzed groups (p = 0,888), reaching the average valueof 36 years, with variations between 24 and 50 years.
Cardiovascular parameter values declined significantly in thestudy group; for the control group, significant differences wererecorded only for the diastolic blood pressure parameter (p <0,05).

34
IV. 7. Discussions
Study 1- evaluation of the occupational stress level andcomponents through validated simple questionnaires
The validation process consisted of two stages: establishing thevalidity by factor analysis and establishing the accuracy by analyzingthe internal consistency of the scale and items. The total variableparameter over 40% showed a satisfying validity and the Crombach’sAlpha parameter of 0,6644 indicates that we have demonstrated agood internal consistency, thus a satisfactory accuracy. TheOccupational Evaluation Questionnaire applied in the military fieldwas concluded to be a useful tool to guide the process of monitoringthe health of personnel subjected to occupational chronic stress; theemployee identified through this questionnaire will be subsequentlysubmitted to more complex procedures of diagnosis and possiblyspecialized therapy.
The evaluation of the results of the validated questionnaireprovide us information about the subjective perception ofoccupational solicitation, above average (6.04 ± 1.67), as well asabout psychosocial characteristics of the military organization: thecompetitive environment (86.2% consider competition asstimulating), in which the image of the individual within the workgroup prevails to the family, with a significant percentage of type Apersonalities, career oriented and thus prone to occupational strain (r= 0,321).
It can be noticed a strong constant choice to increase workcapacity or improve performance and acceptance as well as therequest preferred from the institution under normal conditions,instability of employment or promotion: multitasking and extendedtime (80,7% and 74.5%). This component has been shown to be themost stressful occupational one, beside the interpersonal relations(Fig. 2).
Adaptation strategies to occupational overstress can be groupedinto benefices: increased physical effort at work (r = 0,238), medicaladvice for lifestyle changes, including diet (r = 0,229) and
35
psychological counselling to improve knowledge of the individualemotional and intellectual potential (r = 0,165) and strategiespotentially harmful cumulative as effect on health in the short or longrun: consumption of substances with dishomeostatic potential such ascaffeine, nicotine, energy drinks. The higher the occupational stresslevel, the more the military employee is willing to accede also tosupportive medication: food supplements (r = 0,365), herbal drugssuch as stimulants (r = 0,287) or symptomatic: drug type medicationsthrough pharmaceutical network.
The employee found in the position of promotion is anemployee willing to undertake new tasks and new medicines orunfamiliar Yoga relaxation techniques enter into this equation.
The Occupational Evaluation Questionnaire solicitation helpsus to focus on the subjective perception of stress at work and inimproving prevention programs as to increase employee’scooperation in their implementation, using even the solutionspreferred by the employee.
Study 2- identification of the cardiac stress typology inemployees with predominantly desk work and high responsibility
For the studied cases, the occupational stress level was aboutevenly between the two groups, above average (7.19) in relativelyyoung employees. The military organization by nature and specificitygenerates occupational stress; most soldiers accept stress as a normalfeature of the soldierly activity. Problems arise when the effects ofstress go beyond the resilience and adaptive capacity of theindividual. The results of the study confirmed the findings from thespecialty literature, the differences between groups being notsignificant in terms of subjective perceptions of stress; only slightlyhigher score of the cardiac stressors have been recorded. Groupspresented the level of the occupational stress over the average, thestudy group being represented by those employees whose adaptivecapacity was exceeded and who revealed changes in thecardiovascular profile. High work volume/ multitasking was the mostfrequently incriminated occupational factor in both groups and this is
36
correlated with the most intense level of occupational stress andrestrictions followed by the specific responsibility of the militarysystem. Other stress factors namely contradictory orders,interpersonal relations or working conditions as a human resource,financial and technical enough had less weight. There have beenemployees who said they perceive a higher level of the occupationalstress than the average, but these cannot highlight a dominantstressor factor. Data fall into the specific organizational framementioned in specialty literature, attention being drawn to the needfor a better ranking of the work scheme and distribution tasks. Thehigher the age, the higher is the perception of the occupational stresslevel, probably due to the decrease of adaptability under theconditions of combined dyshomeostasis effects of variousoccupational stressors. The correlation is stronger in the group ofnon-cardiac stressors, this suggesting that not the level of solicitationfelt makes the difference but the typology of stress response. It wasnoted that there is not a correlation between the occupationalcomponent and age, so the latter does not make an individual to bemore sensitive to a component or another of the occupational stressand the cause of this difference must be sought elsewhere, perhaps inthe individual way of networking the various components, modeinvestigated by applying „Big Five” personality questionnaires in thefollowing study. Occupational stress is associated with an increasedconsumption of substances potentially disturbing for the autonomicnervous system. There is a direct, weak, significant correlationbetween caffeine consumption and stress levels at work; nonetheless,between the consumption of nicotine and the occupational stresslevel, there is no statistical correlation, caffeine being actually aneffective strategy to adapt to stress with favorable role in generatingthe dysfunction of the autonomic nervous system in employeesundergoing important occupational stress level while nicotine is notan effective adaptation strategy being purely additive. There is nocorrelation between coping strategies to stress and cardiovascularparameters, fact suggesting that these strategies do not influencedirectly the dyshomeostasis of the autonomic nervous system, havinga cumulatively role, respectively favourable. The absence of a

37
statistical correlation between the occupational component and stresscoping strategies suggests that their initiation is a matter of strictindividuality. The level of the occupational level is related to bodymass index; this correlation could be explained by the link:neuropeptide Y, under stress, promotes food consumption and fatdeposition. The results obtained in evaluating cardiovascularparameters in the two groups confirm data from the specialtyliterature, this suggesting that the diastolic blood pressure parameteris an early marker, specific to the homeostatic disorders caused byoccupational stress, its measure being introduced as a means ofscreening in prevention schemes, part of stress managementprograms in the workplace. Occupational stress is associated with anincreased consumption of substances potentially disturbing for theautonomic nervous system, essential component of the stressresponse system. The role of nicotine as a cardiovascular risk factoris recognized in the specialty literature, the differences betweengroups not being statistically significant in this regard; this suggeststhat dysfunction detected in cardiac stressors are not due to smoking,this habit having at most a cumulative role. Caffeine has a favorablerole in generating the autonomic nervous system dysfunction inemployees subjected to an important occupational stress level. Thesignificant differences between the 2 groups in terms of regularconsumption of caffeine, with a high percentage registered in cardiacstressors requires consideration of this factor in the equationgenerating autonomic nervous system dysfunction with specificoccupational stress factors and prevention schemes. In terms of therelation between body mass index, occupational stress andcardiovascular risk, the insignificant differences between the 2groups suggest that obesity as a cardiovascular risk factor may haveat most a cumulative role, among the occupational stress factors inhomeostatic dysfunctions generated by them.
Study 3- dishomeostatic response of the autonomic nervoussystem and of the HPA axis measured by cardiometabolicdysfunctions and implementation of a preventive pillar 2 scheme inemployees exposed to multiple tasking and extended working hours
38
Study 3 shall constitute a natural consequence of Study 1,which identifies the target population, cardiovascular dysfunctionfollowing exposure to chronic occupational stress levels aboveaverage and indicates the role of stress coping strategies ingenerating disorders.
Study 3 is based on the findings of the proof-of-conceptStudy 1, checking them on a large group and on a wider range ofroles in the military organization; it identifies personality relatedtype to a cardiovascular hyper reactivity to chronic occupationalstress; also, the study quantifies associated metabolic dysfunctionsand proposes a management model of the dishomeostatic responseof the autonomic nervous system and HPA axis in employeesexposed to multiple tasking and extended schedule by usingadditional adaptogens in addition to the classic preventionprogram: advice on unhealthy lifestyles.
The identification of the personality type was made usingquestionnaires - DECAS personality inventory based on Big Fivepersonality model structure. Big Five personality model proposesan integrative descriptive model for research studies of personalityand is the theory with the highest level of spread and scientificvalidation. Researchers have determined that there are fivepersonality dimensions; these can be described by the followingconcepts: openness, extraversion, conscientiousness,agreeableness and emotional stability/ neuroticism. The resultsobtained are interpreted by two types of standard scores: T ratesand percentiles. These are obtained by relating the evaluatedperson to a reference sample.
DECAS personality inventory is based on Big Five modeland was used in the study for the correlation of the dimension ofpersonality with the typology of response to occupational stressfactors and implicitly, precocity of appearance of thecardiometabolic dysfunctional status in employees exposed to anoccupational stress level above average.
The personality type provides information on reactivity tostress factors. Type N of personality in its unbalanced part is
39
related to hyper reactivity to stress. Other 2 types of personalitiespredisposed to dysfunctional reactions to stress are types C and Abut the mechanisms are different. This knowledge helps us toidentify the personality structures arranged as dishomeostaticresponse and helps us guiding an early prevention program. Forthe cases studied, the first three places are held in order bypersonalities type N, A and C, according to the specialty literature.Occupational stress level significantly correlated with N typology,fact suggesting that stress is felt more intensely by those withpossible dysfunctional responses of the autonomic nervous systemas shown by the correlation between systolic blood pressure andtypology parameter N. Sensitivity to various occupationalcomponents is given also by the personality as follows: N isassociated with all components predominantly multiple tasking, Ais associated with multiple tasking and interpersonal relations,predominantly interpersonal relations, as well as C, except thatprevail multiple tasking; E stands only for multiple tasking and Dfor interpersonal relations and multiple tasking equally.Sensitivity distribution helps in the selection of personnel exposedto chronic stress.
The dominant stressor factor mentioned has been workvolume - multiple tasking (62%).
The evaluation of coping strategies, caffeine (85.71% ingroup 1 versus 60% in group 2) and nicotine (64.28% in group 1as compared to 46.66% in group 2) highlights the abuse of suchsubstances for the subjective depreciation of the perception ofoccupational stress and the fact that the changes in coping withoccupational stress is an important component of stressmanagement program.
The results of the cardiometabolic parameters withstatistically significant differences for all parameters in group 1and group 2 for diastolic blood pressure parameters and themetabolic ones supports the initial research hypothesis. Thisindicates that adaptogens administration with counsellingregarding the harmful lifestyle changes are an effective way ofmanaging cardiometabolic disorders caused by chronic
40
occupational stress, the adaptogen role in the prevention schemebeing additionally and participant to the harmful patterns ofbehavior. The lipid-lowering and cardio-vascular action isattributed to both components of adaptogens, the glico-regulatoryaction belonging only to the OE component.
Study 4- identification of the typology vulnerable toalternating shift work in employees exposed to a sudden change inwork schedule
Results confirm the research hypostesis and confirm the resultsof recent studies from the specialty literature indicating MSA and OPas risk factors for cardiovascular and metabolic diseases: abnormallipid and carbohydrate metabolism due to the lack of regularity of thephysiological systems.
This brings to our attention the implementation of someeffective strategies to manipulate the circadian rhythms as part of thesecondary prevention programs, a better MSA and PO managingscheme, the introduction of screening procedures for employees withlow tolerance to MSA and OP and combating harmful patterns ofbehaviour (consumption of nicotine, caffeine and disorganized diet).An extensive study on a larger population sample under MSA andOP can provide valuable scientific information and remains a goalfor future research.
Study 5- dishomeostatic response of the autonomic nervoussystem and of the HPA axis measured by cardiometabolicdysfunctions and implementation of a preventive pillar 2 scheme inemployees exposed to alternating shift work and extended workinghours
Study 5 comes as a natural consequence of Study 4 andproposes a management model of the dishomeostatic response of theautonomic nervous system and HPA axis in employees exposed toMSA and OP.
41
There were significant differences in all parameters in bothgroups, except that for the work group, these differences are moreimportant than those for the control group; this fact confirms theresults from the specialty literature regarding ES and its adaptogenand regulatory activity and communicates that using adaptogens inthe prevention schemes beside the counselling on the harmfulpatterns of behaviour adds something to the effective managing ofcardiometabolic disorders caused by MSA and OP for the targetpopulation with a low tolerance to MSA and OP.
Study 6- exaggerated response alarm in employees exposed tochronic occupational stress and implementation of a preventivepillar 2 scheme
For the studied cases, there have been determined statisticallysignificant differences in cardiovascular parameters in the studygroup. Thus NPY stimulation using an Adaptonic combination ofadaptogens improved tolerance to a new stressor in subjects exposedto chronic occupational stress. In the control group, statisticallysignificant differences were recorded only for the diastolic bloodpressure parameter. This may be due to the previous experience ofthe NPY systems with the stressor used in the study, even if thisstressor was used after 30 days from the first use, influencing theperipheral vascular tone, the stressor adaptation being incompletewhile the other two cardiovascular parameters showed statisticallyinsignificant differences.
Chapter V
FINAL CONCLUSIONS OF THE RESEARCH
● Occupational stress in the military field has a significant impact onemployees, these quantifying their subjective perception of stress atwork place above the average (6.04 ± 1.67)● The application of questionnaires specific to the military activity(eg ESO survey) allows to assess the degree of stress faced by the
42
employee providing important information about the most stressfuloccupational characteristics (multiple tasking, extended workinghours, interpersonal relations) and stress coping strategies(consumption of caffeine, nicotine, food supplements)● About the same level of subjective perception on the occupationalstress, the difference is due to the typology of reaction to stress,cardiac stressors showing significant changes in average arterialpressure and resting heart rate.● The evaluation of the personality type can give us information onreactivity to stress factors, N typology (neuroticism/ emotionalstability) feeling more intensely stress, being able to develop earlyautonomic nervous system dysfunction as shown by the correlationsin Study 3 and the results of assessing the level of stress at the cardiacstressors group of Study 2.● Acceptance of the prevention solutions depends on the type ofresponsibilities: those who support the perspective of promotionaccept more easily drugs or non-traditional relaxation techniques● Among the relaxation techniques, the military employee preferscultural activities (cinema, theatre) and accepts less yoga techniques,fact suggesting that relaxation techniques must be adapted to thecultural specific.● Cardiovascular risk caused by exposure to chronic barracks stress,measured by the significant percentage of cardiac stressors from therandomized population can be augmented by adjacent metabolicdysfunctions (see Studies 3 and 5) and harmful stress copingstrategies with cumulative or contributory role. Regular consumptionof caffeine in the study group is statistically significant as comparedto that of the control group, which is statistically insignificant; thenicotine consumption between groups suggests the favourable role ofcaffeine and the cumulative role of nicotine.● The increase of the individual resistance to stress by usingstandardized adaptogens as part of the programs of prevention inworkplace stress is supported by the results from Studies 3 and 5, inwhich there were statistically significant differences in terms of

43
cardiometabolic parameters between group receiving adaptogens andthe control group.● The unsheduled changes in the work scheme with the need for rapidadaptation (Study 4) or exposure to new stressors, similar to the needof adaptation in theatres of operations may result cardiometabolicdisorders in the vulnerable employee. Our findings contribute to theindividualized application of the preventive measures of pillar 1:knowing the personality type of the individual, he or she may besupported by changes of an improper lifestyle also through substanceswhich increase the stress resistance phase, such as adaptogensubstances or substances of pillar 2, installed dysfunction beingadjusted by the same adaptogen substances.● Counselling on the changes of the maladaptive strategies to stresscan be considered pillar 1 measure when it is applied to an individualwith a dysfunctional predisposition to chronic stress or pillar 2 stressas part of the prevention program when dysfunctions are alreadyobserved.
ORIGINALITY OF THE THESIS
The thesis contains original elements, such as the method andthe work instruments, as follows:- Chronic barracks stress evaluation using a questionnaire validatedfor assessing occupational solicitation adapted to the military fieldand to the dishomeostatic potential as stage prior to exposure to acutestressors in theatres of operations, concept of prevention of pillar 2for the exaggerated alarm response- Identification of the types vulnerable to stress and predictiveelements as a step in pillar 2 prevention programs- The correlation of the structure of personality with thedishomeostatic response to occupational stressors, as stage in thepillar 1 and 2 prevention programs- Use of substances with adaptogen role in pillar 2 occupationalchronic stress management programs in order to increase resistanceto stress and the mediation of a new homeostatic status

44
- Considering as substances with adaptogen role the embryonic planttissues with properties absent in adult tissues
FUTURE PROSPECTS
In order for the results of the current study to be improved, itis necessary to increase the lot of employees in the military field.With view to disseminating preventive methods also in the civil area,it is necessary the diversification of occupations and the applicationof the proof-of-concept prevention program on large populationgroups. In the military practice, the chronic occupational stressmanagement proof-of-concept program may constitute a best practiceguide to be used in other Military Hospitals, for research and/ ordaily practice.
The exaggerated alarm response can become temporaryunfitness for large operations, involvement in theatres of operations.
The use of adaptogens can expand also in the commonpathology for the current practice, where causation involves anelement of stress. Involvement of adaptogens in the modification ofneuropeptide Y can be a starting point for a new class of drugsagainst obesity and its comorbidities, including the metabolicsyndrome and cardiovascular diseases.
Dosage of neuropeptide Y as hormonal parameter specific tothe dishomeostatic response can bring important information toprepare and involve military men in the theatre of operations.
The evaluation of the occupational solicitation must become aprimary goal of the daily practice in occupational medicine. The useof substances with adaptogen role can be an important instrument formodifying stress occupational components and counselling regardingthe unhealthy behaviours as important parts in occupational stressmanagement programs, whether military or civilian.
45
REFFERENCES1. Chrousos GP. Stress and disorders of the stress system. Nat RevEndocrinol 2009; 5, 374–381.2. Chrousos GP, Loriaux DL, Gold P. Mechanisms of Physical andEmotional Stress, New York, Plenum Press,1988.3. Theoharides TC, Spanos C, Pang X, Alferes L, Ligris K et al.Stress-induced intracranial mast cell degranulation. A corticotropin-releasing hormone-mediated effect. Endocrinology 1995; 136,5745–5750.4. Warren J. Presocratics: Natural Philosophers before Socrates(University of California,Berkeley, 2007).5. Chrousos GP. The stress response and immune function: clinicalimplications. Ann NY Acad Sci 2000; 917, 38–67.6. Papanicolaou DA, Wilder RL, Manolagas SC, Chrousos GP.The pathophysiologic roles of interleukin-6 inhumans. Ann InternMed 1998;128, 127–137.7. Morgan M, LeDoux JE. Differential contribution of dorsal andventral medial prefrontal cortex to the acquisition and extinction ofconditioned fear. Behav Neurosci 1995;109, 681–688.8. Chrousos GP. Hans Selye memorial lecture: stressors, stress andneuroendocrine integration of the adaptive response. Ann NYAcadSci 1997; 851, 311–335.9. Banks J, Marmot M, Oldfield Z, Smith JP.Disease anddisadvantage in the United States and in England. JAMA 2006; 295,2037–2045.10. Adhikari Raju. Effects of yoga practices on occupational stressamong indian army personnel- National Yoga Week, Desai NationalInstitute of Yoga New Delhi, 2008.11. Sudom K , Dursun S, Flemming. PERSTEMPO in theCanadian Forces: The role of copin and cohesion in the relationshipbetween job stress and morale. In Human Dimensions in Militaryoperations. Military leaders strategies for adressing stress andpsychological support 2007; 1:9-22.12. Brekhman II, Dardymov IV. New substances of plant originwhich increase nonspecific resistance. Ann Rev Pharmacol 1969; 9,410–426.
46
13. Lazarev NV. General and specific in action of pharmacologicalagents. Farmacol Toxicol 1958; 21, 81–86.14. Hiai S, Yokoyama H, Oura H, Yano S. Stimulation ofpituitary-adrenocortical system by ginseng saponin. Endocrinol Jpn1979; 26, 661–665.15. Hiai S, Yokoyama H, Oura H. Features of ginseng saponin-induced corticosterone secretion.Endocrinol Jpn 1979; 26, 737–740.16. Wang LC, Lee TF. Effect of ginseng saponins on cold tolerancein young and elderly rats.Planta Med 2000; 66, 144–147.17. Panossian A, Wikman G, Wagner H. Plant adaptogens III:Earlier and more recent aspects and concepts on their modes ofaction. Phytomedicine 1999; 6, 287–300.18. Samuelsson G, Bohlin L. Drugs of Natural Origin: A Treatise ofPharmacognosy, 6th Edn Stockholm: Swedish Academy ofPhramaceutical Sciences, 2009.19. Selye H. The physiology and pathology of exposure to stress. Atreatise based on the concepts of the General Adaptation Syndromeand the Disease of Adaptation. Acta Inc Medical Publishers,Montreal,1950.20. Panossian A, Wikman G. Effects of adaptogens on the CentralNervous System and the molecular mechanisms associated with theirstress protective activity. Pharmaceuticals 2010,3:188-224.21.Panossian A, Wikman G. Evidence-based efficacy ofadaptogens in fatigue, and molecular mechanisms related to theirstress-protective activity. Current ClinPharmacol 2009; 4, 198–219.22. Panossian A, Wikman G, Kaur P, Asea A. Adaptogensstimulate neuropeptide Y and Hsp72 expression and release inneuroglia cells. Front Neurosci 2012; 6: 6.23. Karasek R, Baker D, Marxer F, Ahlbom A, Theorell T . Jobdecision latitude, job demands, and cardiovascular disease: Aprospective study of Swedish men. Am J PublicHealth.1981;71(7):694-705.24. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excessdeaths associated with underweight, overweight, and obesity. JAMA2005; 298,1861–1867.

47
25. McCrae RR, John OP. An introduction to the five factor modeland its applications. Journal of Personality 1992; 60(2), 175-215.
48
PUBLISHED WORKS1. Ciumaşu- Rîmbu M, Vulpoi C. Occupational stress managementin the military domain. Bulletin de la National Defense University „Carol I” 2011; 2, 155-165.2. Ciumaşu- Rîmbu M, Vulpoi C. Long hours, shift work andoccupational stress alternating from a military perspective. ActaMedica Transilvanica 2011; 3, 33-34.3. Ciumaşu- Rîmbu M, Popa L, Vulpoi C. Neuropeptide Ystimulation as primary target for preventive measures ofmaladaptative cardiovascular reactions in occupational chronic stressexposure. Revista Medico-Chirurgicală 2012; 3, 818-821.