university of groningen early intervention in infants …ties that require motor coordination is...
TRANSCRIPT
University of Groningen
Early intervention in infants at high risk for developmental motor disordersBlauw-Hospers, Cornill Henriëtte
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2010
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Blauw-Hospers, C. H. (2010). Early intervention in infants at high risk for developmental motor disorders.Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 11-05-2020
Early intervention in infants at high risk
for developmental motor disorders
RIJKSUNIVERSITEIT GRONINGEN
Early intervention in infants at high risk
for developmental motor disorders
Proefschrift
ter verkrijging van het doctoraat in de
Medische Wetenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. F. Zwarts,
in het openbaar te verdedigen op
woensdag 1 december 2010
om 11.00 uur
door
Cornill Henriëtte Blauw-Hospers
geboren op 8 januari 1978
te Groningen

Promotor: Prof. dr. M. Hadders-Algra
Beoordelingscommissie: Prof. dr. J.G. Becher
Prof. dr. O.F. Brouwer
Prof. dr. P.J.M. Helders
Paranimfen: Victorine de Graaf-Peters
Joke de Boer

Contents
CHAPTER 1 Introduction
CHAPTER 2 The ‘Vroegtijdig Interventie Project’ (VIP)
CHAPTER 3 A systematic review of the effects of early intervention
on motor development
CHAPTER 4 Does early intervention in infants at high risk for a devel-
opmental motor disorder improve motor and cognitive
development?
CHAPTER 5 Development of a quantitative tool to assess the content
of physical therapy for infants
CHAPTER 6 Differences between the Family-centered Program
“Coping and Caring for Infants with Special Needs”
and Infant Treatment based on Principles of
NeuroDevelopmental Treatment
CHAPTER 7 A Randomized Controlled Trial on pediatric physical
therapy in infancy: from nightmare to dream?
CHAPTER 8 Additional results on outcome measures of the
VIP project
CHAPTER 9 General discussion
Summary
Samenvatting
Dankwoord
About the author
List of publications
Appendix
page 9
page 25
page 39
page 65
page 87
page 105
page 131
page 154
page 161
page 175
page 179
page 184
page 186
page 187
page 188
© C.H. Blauw-Hospers, 2010
Early intervention in infants at high risk for developmental motor disorders.
ISBN: 978 90 367 4606 9
Ontwerp + vormgeving: Mark van Houten, grafisch ontwerper
Druk: Grafische Industrie De Marne, Leens
All rights reserved. No part of this publication may be reproduces or transmitted in any form or by
any means, electronic or mechanical, including photocopy, recording, or any information storage
or retrieval system, without permission in writing from the author.
Niets uit deze uitgave mag worden verveelvoudigd en/of openbaar gemaakt door middel van druk,
fotokopie, microfilm of op welke andere wijze dan ook, zonder voorafgaande schriftelijke toestem-
ming van de uitgever.
9
C H a P t E r 1
I n t rod u c t Ion
10 11
In approximately 8% of all live births in the Netherlands preterm delivery occurs (CBS 2008). Ad-
vanced technology in neonatal intensive care over the past 20 years has increased the survival of
preterm and high-risk full term infants (Hack and Fanaroff 2000, Stoelhorst et al 2005). Follow-up
studies, however, have shown an increased incidence of motor disability later in life, ranging from
developmental coordination disorder to cerebral palsy (CP) (Hack and Fanaroff 2000, Marlow
2004, Stoelhorst et al 2005, Fawke 2007). To optimize developmental outcome of these infants
extensive early intervention programmes have been developed over the years. In this thesis I will
focus specifically on the effects of paediatric physical therapy programmes that have been applied
to infants up to 18 months corrected age who are at risk for a developmental motor disorder.
The aim of this thesis is to contribute to the body of knowledge about the effects of early
physiotherapeutic intervention for young infants who are considered to be at risk for a develop-
mental motor disorder. Existing programmes are reviewed and a new physiotherapeutic interven-
tion programme called ‘COPCA’ (COPing with and CAring for infants with special needs - a fam-
ily centred programme; Dirks and Hadders-Algra 2003) is evaluated. The goal of this evaluation is
twofold. First, the contents of COPCA are analysed and compared to the existing physiotherapeu-
tic approach. And second, the effects of the COPCA intervention on developmental outcome are
evaluated.
In this introductory chapter brief background information will be provided about the key subjects
in this thesis. In the following paragraphs information about early intervention, developmental
motor disorders of the infants in the studied cohort, and the main influences on paediatric physi-
cal therapy in the Netherlands will be provided. The chapter concludes with an outline of the
individual studies of this thesis.
Early Intervention
Young infants who are discovered to be at risk for developmental motor disorders are often re-
ferred to early intervention services. Early intervention (EI) consists of multidisciplinary services
provided to children from birth to 5 years of age (Shonkoff and Meisels 2000). The aims pursued
with EI are remedial or preventative in nature and comprise the following: 1) promote child
health and well-being, 2) enhance emerging competencies, 3) minimize developmental delays, 4)
remediate existing or emerging disabilities, 5) prevent functional deterioration and, 6) promote
adaptive parenting and overall family functioning (Shonkoff and Meisels 2000). These goals are
accomplished by providing individualized developmental, educational and therapeutic services for
children in conjunction with mutually planned support for their families. EI can be provided in
the hospital, in a rehabilitation centre, in the physical therapy practice, at home or in a combina-
tion of these four. Although EI may start at any moment between birth and 5 years of age it is
advocated to intervene as early as possible. It is recognized that only through early identification
and appropriate programming infants can reach their full potential. In a recent review on brain
development de Graaf-Peters and Hadders-Algra (2006) recommended that, based on develop-
mental processes, the best time window for EI in terms of active stimulation of the infant lies
between 40-44 weeks post menstrual age and 15 months postnatally. In this period, processes of
dendritic outgrowth and synapse formation are highly active which offer the best opportunities
to reconnect and find functional solutions than later periods (Kolb et al 2001, de Graaf-Peters and
Hadders-Algra 2006). Active stimulation consists of activities which induce active responses of
the infant, for example offering toys to stimulate head balancing exercises in prone position. De
Graaf-Peters and Hadders-Algra (2006) suggest also that EI prior to 40-44 weeks post menstrual
age should be restricted to forms which aim at mimicking the intrauterine environment in order
to reduce stress. Other advantages of intervening early are possible beneficial effects on the family.
From the literature it is known that families who encounter problems with their infant’s develop-
ment experience higher levels of stress (Singer et al 1999, King et al 2004, Muller-Nix et al 2004,
Butcher et al 2008). EI can help to minimize the impact of developmental problems on the family.
Summarizing, the research field of EI is very broad. It covers a wide age span and a whole range
of services. Therefore in this thesis the term early intervention is limited to paediatric physical
therapy for infants up to 18 months corrected age who are at risk for a developmental motor disorder.
Developmental motor disorders
Cerebral palsy and developmental coordination disorder are two important forms of developmen-
tal motor disorders. Cerebral Palsy (CP) is defined as “a group of disorders of the development of
movement and posture causing activity limitation, which are attributed to non-progressive distur-
bances that occurred in the developing foetal or infant brain. The motor disorders of cerebral
palsy are often accompanied by disturbances of sensation, perception, cognition, communication,
behaviour, by epilepsy and by secondary musculoskeletal problems” (Bax et al 2005, Rosenbaum
et al 2007). The prevalence of CP in the Netherlands is around 1 or 2 children per 1000 live births
with an incidence which is higher in males than in females (1.33:1) (Wichers et al 2005). CP is the
result of an injury or abnormal development of the brain which may occur during pregnancy,
birth or within the first two to three years of life. In many cases, the exact cause of CP is unknown
(Rosenbaum 2003). Currently, problems occurring during intrauterine development, congenital
disorders, hypoxic-ischemic insults, and preterm birth are considered to account for the major-
ity of the cases with CP (Moster et al 2001, Jones et al 2007). Infants born prematurely have an
increased risk for intraventricular hemorrhage (IVH) or periventricular leukomalacia (PVL) result-
ing in injury to the periventricular white matter of the brain. PVL is a good predictor for CP, with
CP developing in 80% to 85% of the infants (Perlman et al 1996, Jones et al 2007). All children with
CP suffer from some degree of motor impairment which in most cases manifests itself before 18
months of age and persists throughout the lifespan. During early infancy CP cannot be diagnosed,
because in many cases the characteristic features belonging to CP have not manifested them-
selves. The way CP affects each individual will vary widely. Characteristics may include a lack of
coordination, spasticity, involuntary movements, muscle weakness, increased tendon reflexes, dif-
ferent walking patterns (i.e. scissors gait, toe walking, wide-based gait), dysarthria, difficulty with
12 13
gross and fine motor skills, and abnormal perception and sensation.
The clinical picture of CP evolves with time, development, learning, training, therapies, and
other factors (Bower and McLellan 1994, Bax et al 2005). Therapy therefore focuses on helping the
individual to maximize his or her potential (Scrutton 1984). In general it is believed that the earlier
treatment starts the better chance children have of learning new ways to accomplish challenging
daily tasks. While this seems intuitively obvious, strong scientific support is lacking to support
this assumption (Damiano 2006).
Developmental coordination disorder (DCD) denotes children whose performance in daily activi-
ties that require motor coordination is substantially below what can be expected given the child’s
chronological age and intellectual ability, in the absence of other neurological disorders (APA;
DSM-IV; 2000). The disturbance in the performance of daily activities interferes with academic
achievement or activities of daily living. Estimates of the prevalence of DCD range from 5% to
15% in the primary school population (Wilson 2005). Most studies on children with DCD report
a higher prevalence in boys than girls, but the actual sex ratio is variable and depends on the
method used to identify children (Missiuna et al 2006).
Children with DCD not only differ in the motor skills they experience problems with, or the
underlying processes that are causing the deficit, but also in the extent to which they suffer from
co-morbidities such as attention, behavioural or emotional problems (Dewey et al 2002, Gillberg
and Kadesjö 2003). Studies on the underlying processes have shown that children with DCD can
have deficits in many areas of performance, including motor planning, motor programming, pos-
tural control, proprioceptive or kinesthetic deficits, and visual spatial processing (Niemeijer 2007).
About half of children with DCD will not outgrow their motor problems (Losse et al 1991, Cantell
et al 2003).
DCD is difficult to diagnose before school-age. Clumsy motor behaviour becomes more evi-
dent with increasing difficulty of motor tasks. Research has shown that a relation exists between
the presence of neurological dysfunction in infancy and DCD (Jongmans et al 1997, Hadders-Algra
2003). A few studies have shown that early identification (i.e. before school-age), effective interven-
tion and vocational counselling are important for children diagnosed with DCD to diminish the
negative experiences that can affect their later academic and social life (Cantell et al 2003, Mis-
siuna et al 2003).
advances in paediatric physical therapy
In the early 1900s European physical therapists were trained in manipulation by a London in-
ternist and orthopaedic surgeon Dr. James Cyriax. CP at this time was considered to be a disease
which they tried to cure with orthopaedic surgery. Over the years many different intervention
programmes have been developed for young children with CP varying from different types of
physical therapy and occupational therapy to the use of drug such as baclofen or botox, orthotic
devices, etcetera. The variety in approaches might result from the diversity in effect that CP has
on the daily functioning of the child (Mayston 2004). In this introductory chapter a brief overview
of the main influences on paediatric physical therapy for infants with or at risk for CP is provided.
In the Netherlands the main influences come from Neurodevelopmental Treatment (NDT), Vojta,
Sensory Integration Therapy, and more recently from functional therapy. The intervention pro-
grammes differ in their treatment methods, but all aim at ‘leading the children with cerebral palsy
… towards the greatest degree of independence possible, and so to prepare them for as normal as
an adolescent and adult life as can be achieved. This is the aim of all schools of treatment’ (Bobath
and Bobath 1984, p.6).
NeuroDevelopmental Treatment
The NDT approach was developed by Berta and Karl Bobath in the 1940s. The basic assumption of
NDT was that sensorimotor problems in CP arise from central nervous system dysfunction, which
interferes with the establishment of normal motor development. Inhibition of spasticity and
facilitation of normal posture and motor behaviour were the main aims of treatment, which the
Bobaths tried to accomplish by tone influencing patterns with the use of various therapeutic han-
dling techniques (Bobath and Bobath 1984, Mayston 2001). The normal developmental sequence
was advocated as a framework for treatment (Bly 1991, Howle 2002). In the sixties Elizabeth Köng
and Mary Quinton started to adapt and develop the techniques for early treatment of babies based
on the Bobath concept (Köng 1966, Quinton and Nelson 2002).
During the years the NDT approach evolved from a practice-based concept to a more theory-
based and partly evidence-based approach (Bly 1991, Palmer 1997, Mayston 2000, Howle 2002).
This means that based on new theoretical constructs and practical knowledge NDT gradually
evolved and caused a shift in goals, treatment techniques and treatment application (Howle 2002).
The original goal ‘inhibition of spasticity and facilitation of normal posture and motor behaviour’
to give the child the opportunity to move more normally nowadays has shifted to ‘optimize func-
tion’ (Howle 2002). This implies that NDT intervention aims to prepare and guide the children
towards their greatest possible independence in everyday functioning (Bobath and Bobath 1984).
Based on experience and new insights in neurosciences the emphasis on certain treatment
techniques changed. In the early years specific postures were imposed on the child with the aim
of achieving a normalization of muscle tone. The ‘reflex-inhibiting’ postures and tone influenc-
ing patterns indeed did reduce spasticity during treatment, but lacked carry-over effects into
movement and function (Mayston 2001, Howle 2002). Next, the Bobaths promoted the use of ‘key
points of control’, i.e. special combinations of hand placement on the body that allowed the thera-
pist to control the child’s sensorimotor input and motor output. These handling techniques had
the dual aim of inhibiting abnormal movement patterns and facilitation of normal movements
(Bobath and Bobath 1984, Butler and Darrah 2001, Howle 2002). Moreover, therapeutic handling
from key points of control made it possible for the child to - systematically and increasingly - take
over control of his/her own movement.
Over the years therapists gradually became more aware that their treatment had not automat-

14 15
ically carried over into activities of daily life. As a consequence, preparations for functional tasks
currently are carried out in settings where children live, play and learn (Bobath and Bobath 1984,
Butler and Darrah 2001, Howle 2002). The principles for the NDT baby treatment (Bly 1999) aim
at helping the infant in its development by the use of sensorimotor experiences (handling) and in-
structing the caregivers. In this regard caregivers play a specific role in NDT treatment. They have
a role as co-therapist (Finnie 1996). Through guiding and training of caregivers, the therapist tries
to establish carry-over from treatment into activities of daily life (Bobath and Bobath 1984). The
hands of the therapist facilitate, assist or control the infants’ posture and movements until the
infant can take over. The treatment consists of a sequence of developing, kinesiological, sensory
and environmental factors.
Treatment techniques
Tone influencing patterns are the primary intervention strategy of NDT that are achieved through
various therapeutic handling techniques. The use of a tone influencing pattern inhibits abnormal
activity, while at the same time the way is paved for more normal movements (e.g. facilitation)
(Howle 2002). However, in 1965 the Bobaths already acknowledged that: “unless you stimulate or
activate your patient in a way in which new activities are possible, you have done nothing at all. So
the tone influencing patterns as such are only the very first step in treatment, though they are very
important” (Mayston 2005). Thus, during NDT treatment inhibition and facilitation always act as
interactive partners in order to prepare the body for the performance of functional tasks. Further-
more, therapeutic handling techniques allow the therapist to provide sensorimotor experience, to
feel responses to changes in posture and movement, to gain control of muscle tone, to influence
the alignment of the body, to direct the attention of the child and to recognize the moment when
the child can become independent of assistance (Howle 2002). Therapeutic handling consists of
the following interactive components:
1) Key points of control are predefined parts of the body on which the hands of the therapist are
placed to influence directly the area beneath the hands of the therapist and other parts of the
body. The key points of control allow the therapist to inhibit abnormal movement patterns
and to facilitate normal movements simultaneously (Bobath and Bobath 1984). Key points are
located all over the body and are used interchangeably and in combinations. During treatment
there is a shift in the use of key points from proximal (e.g. shoulder, pelvic girdle) to distal (e.g.
extremities) to give the child the opportunity to gradually gain control over his movements.
2) Facilitation is the strategy of therapeutic handling that makes a posture or movement more
likely to occur. It can modify postural control by increasing degrees of freedom, supporting a
body segment, or activating the postural system. Placing the child in an imposed posture creates
a possibility to promote the occurrence of normal movement patterns (Howle 2002) (p.255-256).
3) Inhibition originally referred to reducing tone and abnormal reflex activity resulting from dys-
function in the central nervous system. Currently, inhibition refers to the reduction of specific
underlying impairments that interfere with function (Howle 2002) (p.257). Specific goals are to
gain control of muscle tone, to decrease excessive co-activation patterns and to prevent the oc-
currence of atypical postures.
As NDT is the most widely applied method in the treatment of infants with or at risk for develop-
mental disorders, many studies are undertaken to demonstrate its effectiveness. In three recent
reviews (Butler and Darrah 2001, Blauw-Hospers and Hadders-Algra 2005, Spittle et al 2007)
attention was paid to the effectiveness of NDT. All three concluded that there was no advantage
to NDT over other alternatives to which it was compared. No clear evidence was found that NDT
was beneficial for motor development or functional motor activities. Also other potential benefits
such as the enhancement of cognitive development or improved caregiver-infant interaction could
not be demonstrated. Possible explanations that are provided for the scarceness of evidence are
for instance the ongoing change of the constructs of NDT over time, the skill level of the therapist
and the impossibility to deliver treatment in a standardized manner (Butler and Darrah 2001).
While for research purposes the treatment setting can be standardized, the child with CP and
his family can never be. Moreover, CP is a highly heterogeneous condition which is complicated
by ongoing change in the children due to processes of growth and maturation. The change of the
NDT constructs over time also includes that techniques of NDT were more often used together
with techniques from other approaches that gained influence in the treatment of children with
developmental disorders, like for example the Vojta concept and sensory integration therapy.
Treatment according to Vojta
The Vojta concept, also called reflex locomotion, was developed during the 1950s by Vaclav Vojta
based on empirical observations. It was implemented in the Netherlands in the 1970s and is still
applied, especially in the southern part of the country. The method is primarily considered to be
a facilitatory approach that can be applied to all neuromuscular conditions, not just CP. Goals of
reflex locomotion are: 1) to facilitate the automatic control of the body position, 2) to facilitate the
uprighting mechanism of the body, and 3) to stimulate coordinated muscle activity. These skills
are disturbed in children with brain lesions or developmental motor disorders.
The concept is based on the observation that through specific peripheral stimulation nor-
mal motor reactions throughout the body can be elicited when the patient is placed in a specific
position. Vojta believed that the persistence of newborn reflexes in a child with CP interferes
with normal postural development. It is assumed that the activation of newborn reflexes through
stimulation of the global reflex pattern facilitates the development of reflex locomotion (Vojta
1984, Stanger and Oresic 2003, Mayston 2004).
Treatment techniques
The Vojta concept actually consists of two parts: clinical evaluation and treatment. Before the
physiotherapist can start with the reflex locomotion treatment, he can use the Vojta concept as
16 17
a clinical evaluation to define the goals for the treatment. The clinical evaluation is divided into
three parts. The first part is the study of the automatic postural reactivity. To discover potential
problems in the organization of automatic responses by the CNS, reactions to sudden postural
changes of the body, i.e. disturbances of the equilibrium position, are tested. This helps to identify
the degree of development at time of the examination. The second part consists of the kinesio-
logic analysis of spontaneous motor function. The placement of the extremities at specific angles
is important to maintain the equilibrium of the body. The third part is reflexology. A series of
reflexes completes the examination to refine the immediate evaluation but also to specify the
prognosis (Vojta 1984).
In the practical application reflex locomotion utilises two so-called coordination complexes:
the reflex creeping and rolling. Vojta identified a number of reflex points which can be used
to stimulate the human body to crawl and turn. From several start positions (supine, prone or
side-lying) the flow of motor responses is provoked by giving pressure on specific body parts, the
so-called ‘zones’. During the reflex locomotion it is essential that the placement of the extremities
at specific angels is optimal. The motor responses that arise during the application of the reflex
locomotion are called ‘global patterns’. Global implies that skeletal muscles throughout the body
are activated in a coordinated manner and that the central nervous system (CNS) is addressed at
all it’s regulatory levels (Vojta 1976).
Caregivers play a specific role in treatment according to Vojta. They are thoroughly instructed
to carry out the patterns of reflex locomotion. Optimally, the therapy should be carried out 4
times a day. The child is not actively involved in the treatment.
Vojta states that the best results of reflexlocomotion are achieved in babyhood when the plastic-
ity of the brain is greatest. He claimed that pathological motor patterns are already present but
not yet fixated and that the opportunity to gain access to normal movement patterns is merely
blocked (Vojta 1976, 1984).
The effect of treatment according to Vojta is evaluated in only a few studies. Blauw-Hospers
and Hadders-Algra (2005; see Chapter 3) showed that there was no evidence that treatment ac-
cording to Vojta supports the development of infants at high risk for developmental motor disor-
ders. The Vojta approach has been criticized for the emotional stress it may produce in child and
family (d’Avignon et al 1981).
Sensory Integration Therapy
Sensory integration therapy was developed during the 1960s by Jean Ayres. She was interested
in the way in which sensory processing and motor planning disorders interfere with activities of
daily living and learning. Sensory integration is the process by which people register, modulate,
and discriminate sensations received through the sensory systems to produce purposeful, adap-
tive behaviours in response to the environment (Ayres 2005). Sensory integration therapy is based
on the assumption that learning is dependent on the ability to take in sensory information from
the environment, to process and integrate the sensory inputs within the central nervous system
and to use this information for the planning and production of organized behaviour (Ayres 1972,
Mayston 2004). Sensory integration focuses on the five sensory areas: vestibular, tactile, pro-
prioceptive, visual and auditory information. The goal of intervention is to improve the ability
to process and integrate sensory information and to provide a basis for improved independence
and participation in daily life activities, play, and school tasks (Schaaf and Miller 2005). Although
originally sensory integration therapy was developed to treat children with learning disabilities,
Ayres recognized the utility of the theory for other clinical populations (Schaaf and Miller 2005).
As a significant amount of the children with CP also experience sensory impairments, sensory
integration may assist the child during the intake and processing of sensory information and thus
enhance function.
The theory of Sensory Integration is based on principles from developmental psychology,
education, neuroscience, and occupational therapy. It entails four main principles that are: 1)
sensorimotor development is an important substrate for learning; 2) the interaction of the indi-
vidual with the environment shapes brain development; 3) the nervous system is capable of change
(plasticity); and 4) meaningful sensory–motor activity is a powerful mediator of plasticity (Schaaf
and Miller 2005).
Treatment techniques
The therapy is driven by four main principles: 1) Just right challenge (the child must be able to
meet the challenges through playful activities), 2) Adaptive response (the child adapts behaviour
to meet the challenges presented), 3) Active engagement (the child wants to participate because
the activities are fun), 4) Child-directed (the child’s preferred activities are used in the session).
Therapy provides opportunities for the child to engage in sensory motor activities rich in tactile,
vestibular, and proprioceptive sensations. A key point for therapy success is the inner drive of the
child (Ayres 2005). Based on the tasks the child would like to master, the therapist designs the
environment which has to be appealing to the child and which is adapted to the child’s develop-
mental level. The treatment setting looks like a play-area with equipment designed to provide
the required form of stimulation. During these play activities the child can actively explore its
environment. The therapist assists the child to accomplish the task by manipulating the environ-
ment in such a way that the most adaptive response is elicited. Fun and success are prerequisites
for feelings of competency that are needed to achieve progress in the processing of sensory input.
During the activity the therapist observes the child’s responses and increases or decreases the
sensory and motor demands when necessary.
Over the past 30 years a number of studies have been conducted to investigate whether sensory
integration therapy is effective. The majority of studies have focused on the use of sensory inte-
gration therapy with children with learning disabilities and have aimed at improving motor skills,
academic performance, behavioural performance and/or sensory and perceptual skills. Two re-
18 19
views (Vargas and Camilli 1999, Schaaf and Miller 2005) reported that the evidence for the effects
of sensory integration is inconclusive. Bumin and Kayihan 2001 conducted a study to examine the
effects of sensory integration therapy in children with spastic diplegia. They found that children
who received the sensory integration programme performed better compared to a no treatment
control group. No studies were found which evaluated the effect of sensory integration therapy for
infants.
Functional Therapy
In the past decades the assumptions of the traditional treatment approaches have been questioned
in a considerable number of studies. Evidence for the effectiveness of the approaches is inconclu-
sive. A number of studies have shown that treatment often was not automatically transferred into
meaningful activities of daily life (Bobath and Bobath 1984, Butler and Darrah 2001, Ketelaar et al
2001). This finding initiated a conceptual shift in treatment from focusing on normality to func-
tionality. Nowadays, the concept of functional therapy is increasingly emphasized in literature on
interventions for children with CP.
The theoretical background of the functional approach is formed by the dynamic systems
theory (Thelen and Smith 1994) and family-centred service. Functional therapy consists of an
approach guided by principles of motor learning and function (Ketelaar et al 2001, Ekström-Ahl
et al 2005). Exploration and selection in finding solutions for new task demands in combination
with the adaptation to changes in the environmental context are considered to be critical parts
of motor learning (Ketelaar et al 2001). Main features of a functional approach to therapy are: 1)
Focus on the improvement of functional tasks which are problematic in daily life, 2) The child acts
as an active participant of the therapy, who gets the opportunity to actively explore his possibili-
ties and to find the best strategies and solutions for a functional task, 3) Training should take place
in a context specific environment, 4) Focus on assisting the child and his family to achieve more
satisfactory performance of daily activities (Harris 1990, Law et al 1998, Ketelaar et al 2001), 5)
Caregivers are involved in all stages of the programme (from goal-setting and implementation in
daily life to evaluation).
In the last decades the involvement of caregivers in the care process has become the basis of
the care approach in rehabilitation. This concept of family centered care (FCC) is described as a
holistic approach towards service delivery, in which the unique strengths, resources and set of
needs of each child and its family form the base for a highly individualized and dynamic model
of care (King et al 2004, MacKean et al 2005). Keywords in FCC are partnership, information
exchange and respectful and supportive treatment (King et al 1997, Rosenbaum et al 1998). Care-
givers are considered as equal partners who work together with the rehabilitation team to
optimize their child’s care process. This implies that caregivers are involved in all stages of the
rehabilitation program, from goal-setting and implementation to evaluation. However, (Law et
al 2003) state that true FCC gives caregivers the opportunity to decide their own level of involve-
ment. The intervention programme must be adapted to families’ capabilities, their situation and
daily schedule and not vice versa. This view is supported by Nijhuis and coworkers (2007) who
showed that to provide true FCC a family-specific evaluation of FCC, i.e. making an accurate
inventory of the specific needs and wishes of the individual families, is essential to avoid possible
discrepancies between the views of caregivers and health care professionals.
Research has indicated that the involvement of caregivers in the care process can be associated
with positive effects both on the development of the child (Ketelaar et al 1998, Law et al 1998, King
et al 2004) as well as on the caregivers in terms of an increase in parental skills, improved well-
being and a decreased level of parental stress (King et al 1996, Rosenbaum et al 1998, Jansen et al
2003, King et al 2004, Raina et al 2005). Caregivers can play a major role in assisting their children
to reach their maximum potential by training the transfer of functional skills form one context to
another. Moreover, the involvement of caregivers in their child’s intervention may improve their
understanding of their child’s development (Palmer et al 1988). From the literature it is assumed
that daily home-based physical therapy provided by the parents is more efficient than physical
therapy given by a therapist once a week for a half hour (Ketelaar et al 1998).
Evidence for the efficacy of functional therapy is slowly increasing. One of the first studies that
evaluated a somewhat functional approach was an often cited study by Palmer et al (1988). Forty-
eight infants, aged 12 to 19 months, were randomly assigned to receive an infant stimulation
programme including motor, sensory, language and cognitive activities of increasing complexity
or NDT. The infant stimulation programme turned out to be more beneficial for developmental
outcome than the NDT approach. Another study which showed that functional physical therapy
was beneficial for children with cerebral palsy was written by Ketelaar et al (2001). They showed
in 55 children with CP aged 2 to 7 years that the children who received the functional therapy
programme (n=28) after the intervention period improved more on functional skills in daily situ-
ations than the control group. In 2005 a pilot study was published which evaluated the effects
of a functional therapy programme on motor development and functional outcome measures of
preschool children with CP (Ekström Ahl et al 2005). Fourteen children aged 18 months to 6 years
participated in the five-month intervention. The study showed that after the programme the
children had better gross motor function and performed better on daily activities. Also in relation
to the children’s mobility a decrease was found in the amount of caregiver assistance. A major
drawback of this pilot study however was the lack of a control group. At the moment a large multi-
centred RCT is running on the effects of a functional therapy programme for young children with
CP in Canada (Law et al 2007). The study aims at an inclusion of 220 children with CP aged 12
months to 5 years.
Initially, the functional approach was developed for children with developmental disorders.
Applying this concept to young infants (less than 18 months of age) implies that therapy mainly
focuses on the encouragement of self produced motor behaviour (Resnick et al 1987, Palmer et al
1988, Ketelaar et al 2001, Ekström-Ahl et al 2005). Infants act as active participants of the therapy
(Damiano 2006, Callahan et al 2006) who get the opportunity to actively explore their motor pos-

20 21
sibilities and to find an appropriate solution for any given motor task. The therapist coaches the
caregiver to stimulate the infant to perform tasks that are both challenging and meaningful with
appropriate success and failure rates (Dirks and Hadders-Algra 2003). The focus lies on assisting
the family to achieve more satisfactory performance of daily activities (Harris 1990, Law et al
1998, Ketelaar et al 2001).
Concluding remarks
Paediatric physical therapy for infants at high risk for a developmental motor disorder can be
considered as a field in development. Based on findings that evidence for the effectiveness of the
traditional EI programmes (NDT, treatment according to Vojta, and Sensory Integration Therapy)
is limited, shifts in the application of therapy were initiated. The most important advances are
functionality instead of normality, the infant as an active participant of the therapy and the inclu-
sion of the family.
aims and outline of this thesis
The advances in paediatric physical therapy show that the physiotherapeutic guidance of infants
with or at high risk for a developmental motor disorder is very diverse. The evidence for the effec-
tiveness of the intervention programmes is inconclusive. Most studies have evaluated the effects
of early intervention at the time during infancy or preschool age when the condition is already
expressed in dysfunction. As mentioned before, the term early intervention in this thesis is limited
to paediatric physical therapy for infants up to 18 months corrected age. Therefore, the first aim of
this thesis was to review the effects of early physiotherapeutic intervention on motor and cogni-
tive development of infants with a high risk for developmental motor disorders aged less than 18
months. Two systematic reviews were performed to gain more insight in the currently available
evidence on early intervention. In these reviews specific attention is paid to unravelling elements
in intervention programmes which might contribute to a beneficial effect on motor or cognitive
development. The results of these reviews are presented in Chapter 3 and 4.
The results of both reviews indicated that intervention programmes with an onset after term
age which focus on the stimulation of self-produced motor behaviour can exert a beneficial effect
on motor and cognitive development. This knowledge served as a base for the development of a
new type of physiotherapeutic intervention, COPCA. COPCA is the abbreviation of Coping with
and Caring for infants with special needs – a family centered programme (Dirks and Hadders-Al-
gra 2003). The rationale behind the COPCA programme is presented in Chapters 2 and 6. To evalu-
ate the effects of COPCA on the development of infants at high risk for a developmental disorder
an early intervention project VIP (in Dutch “vroegtijdig interventie project”) was designed. In the
VIP project the effects of the COPCA intervention on neuromotor and cognitive development
were evaluated and compared to the effects of the traditional approach towards traditional infant
therapy (TIP). For a description of the study design, subjects and outcome measures involved in
the early intervention project VIP see Chapter 2.
The second aim of this thesis was to evaluate the effects of COPCA and TIP on developmental
outcome. The results of this evaluation are presented in Chapter 4, 7, and 8. In Chapter 4 some
preliminary results on developmental outcome for the first half of the study group are described.
Chapter 7 has a twofold focus. In the first part of the study the effects of COPCA and TIP on the
developmental outcome at 6 and 18 months are described. In the second part the findings of the
randomized controlled trial were extended with the findings on the contents of the intervention
(described in Chapter 5 and 6). In this way we attempted to identify whether changes in develop-
mental outcome were associated with the contents of the intervention or that they could be ex-
plained by other factors. Chapter 8 discusses the outcomes of the VIP project including some data
which have not been published earlier.
The third aim of this thesis was to evaluate the application of COPCA in daily practice by
means of video analysis. This process evaluation is a prerequisite for the implementation of
COPCA within paediatric physiotherapy. Through detailed analysis of videos of physiotherapeu-
tic intervention sessions we gathered knowledge on the actual contents of both the COPCA and
TIP intervention. This analysis will help to discover the effective and ineffective elements in the
interventions and will consecutively result in knowledge about the implementation of intervention
by different paediatric physical therapists in different settings. Chapter 5 introduces an observation
protocol which we developed for the analysis of actions that physiotherapists use during treat-
ment. Eight main categories of physiotherapeutic actions were defined to explore the contents
of COPCA and TIP. Chapter 6 reports the contents of TIP and COPCA. Here the similarities and
differences between COPCA and TIP are lined out.
The thesis concludes with a general discussion of the reported findings focusing on implica-
tions for further research and practice.

22 23
Jansen LM, Ketelaar M, Vermeer A. Parental experi-ence of participation in physical therapy for children with physical disabilities. Dev Med Child Neurol 2003;45:58-69.
Jones MW, Morgan E, Shelton JE, Thorogood C. Cerebral palsy: introduction and diagnosis (part I). J Pediatr Health Care 2007;21:146-152.
Jongmans M, Mercuri E, de Vries L, Dubowitz L, Henderson SE. Minor neurological signs and percep-tual-motor difficulties in prematurely born children. Arch Dis Childh 1997;76:F9-14.
Ketelaar M, Vermeer A, Helders PJM, ’t Hart H. Paren-tal participation in intervention programs for children with cerebral palsy: a review of research. Top Early Child Spec 1998;18:108-117.
Ketelaar M, Vermeer A, Hart H, van Petegem-van Beek E, Helders PJ. Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys Ther 2001;81:1534-1545.
King SM, Rosenbaum PL, King GA. Parents’ percep-tions of caregiving: development and validation of a measure of processes. Dev Med Child Neurol 1996;38:757-772.
King GA, Rosenbaum PL, King SM. Evaluating family-centred service using a measure of parents’ percep-tions. Child Care Health Dev 1997;23:47-62.
King S, Teplicky R, King G, Rosenbaum P. Family-centered service for children with cerebral palsy and their families: a review of the literature. Semin Pediatr Neurol 2004;11:78-86.
Kolb B, Brown R, Witt-Lajeunesse A, Gibb R. Neural compensations after lesion of the cerebral cortex. Neural Plast 2001;8:1-16.
Köng E. Very Early Treatment of Cerebral Palsy. Dev Med Child Neurol 1966;8:198-202.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Oc-cup Ther Pediatr 1998;18:83-102.
Law M, Hanna S, King G, Hurley P, King S, Kertoy M, Rosenbaum P. Factors affecting family-centred service delivery for children with disabilities. Child Care Health Dev 2003;29:357-366.
Law M, Darrah J, Pollock N, Rosenbaum P, Russell D, Walter SD, Petrenchik T, Wilson B, Wright V. Focus on Function - a randomized controlled trial comparing two rehabilitation interventions for young children with cerebral palsy. BMC Pediatr 2007;27:7-31.
Losse A, Henderson SE, Elliman D, Hall D, Knight E, Jongmans M. Clumsiness in children – do they grow out of it? A 10-year follow-up study. Dev Med Child Neurol 1991;33:55-68.
MacKean GL, Thurston WE, Scott CM. Bridging the divide between families and health professionals’ perspectives on family-centred care. Health Expect 2005;8:74-85.
Marlow N. Neurocognitive outcome after very preterm birth. Arch Dis Child Fetal Neonatal Ed 2004;89:F224-228.
Mayston MJ. Motor learning now needs meaningful goals. Physiotherapy 2000;86:492-493.
Mayston MJ. People with cerebral palsy: effects of and perspectives for therapy. Neural Plast 2001;8:51-69.
Mayston M. Physiotherapy management in cerebral palsy: an update on treatment approaches. Clinics in Developmental Medicine 2004;161:147-160.
Mayston M. Bobath concept: a view from the United Kingdom. NDTA Network 2005;12.
Missiuna C, Rivard L, Bartlett D. Early identification and risk management of children with development coordination disorder. Pediatr Phys Ther 2003;15:32-38.
Missiuna C, Gaines R, Soucie H, McLean J. Parental questions about developmental coordination disorder: A synopsis of current evidence. Paediatr Child Health 2006;11:507-512.
Moster D, Lie RT, Irgens LM, Bjerkedal T, Markestad T. The association of Apgar score with subsequent death and cerebral palsy: A population-based study in term infants. J Pediatr 2001;138:798-803.
Muller-Nix C, Forcada-Guex M, Pierrehumbert B, Jaunin L, Borghini A, Ansermet F. Prematurity, mater-nal stress and mother-child interactions. Early Hum Dev 2004;79:145-158.
Niemeijer AS. Neuromotor Task Training. Physiothera-py for children with developmental coordination disorder. Dissertation University of Groningen; 2007.
references
American Psychiatric Association. Diagnostic and Sta-tistical Manual of Mental Disorders (4th edition). Wash-ington, DC: American Psychiatric Publishing; 2000.
d’Avignon M, Norén L, Ǻrman T. Early physiotherapy ad modum Vojta or Bobath in infants with suspected neu-romotor disturbance. Neuropediatrics 1981;12:232-241.
Ayres AJ. Sensory Integration and Learning Disorders. Los Angeles: Western Psychological Services; 1972.
Ayres AJ. Sensory Integration and the child. Los Angeles: Western Psychological Services; 2005 (original work published in 1976).
Bax M, Goldstein M, Rosenbaum P, Leviton A, Paneth N, Dan B, Jacobsson B, Damiano D; Executive Com-mittee for the Definition of Cerebral Palsy. Proposed definition and classification of cerebral palsy, April 2005. Dev Med Child Neurol 2005;47:571-576.
Blauw-Hospers CH, Hadders-Algra M. Fact or fiction: a systematic review on the effects of early interven-tion on motor development. Dev Med Child Neurol 2005;47:421-432.
Bly L. A historical and current view of the basis of NDT. Pediatr Phys Ther 1991;3:131-135.
Bly L. Baby treatment based on NDT principles. PRO-Ed, Austin Texas;1999.
Bobath K and Bobath B. The neuro-developmental treat-ment. In: D. Scrutton (ed), Management of the motor disorders of children with cerebral palsy. Oxford: Clin-ics in Developmental Medicine 90, Spastics Interna-tional Medical Publications; 1984:6-18.
Bower E, McLellan DL. Evaluating therapy in cerebral palsy. Child Care Health Dev 1994;20:409-19.
Bumin G, Kayihan H. Effectiveness of two differ-ent sensory-integration programmes for children with spastic diplegic cerebral palsy. Disabil Rehabil 2001;23:394-399.
Butler C, Darrah J. Effects of neurodevelopmental treatment (NDT) for cerebral palsy: an AACPDM evi-dence report. Dev Med Child Neurol 2001;43:778-790.
Butcher PR, Wind T, Bouma A. Parenting stress in moth-ers and fathers of a child with a hemiparesis: sources of stress, intervening factors and long-term expressions of stress. Child Care Health Dev 2008;34:530-541. Callahan J, Parlman K, Beninato M, Townsend E. Per-
spective: impact of the IIISTEP conference on clinical practice. J Neurol Phys Ther 2006;30:157-166.
Cantell MH, Smyth MM, Ahonen TP. Two distinct path-ways for developmental coordination disorder: Persist-ence and resolution. Hum Mov Sci 2003;22:413-431.
Centraal Bureau voor de Statistiek. http://statline.cbs.nl/statweb; 2008.
Damiano DL. Activity, activity, activity: rethinking our physical therapy approach to cerebral palsy. Phys Ther 2006;86:1534-1540.
De Graaf-Peters VB, Hadders-Algra M. Ontogeny of the human central nervous system: what is happening when? Early Hum Dev 2006;82:257-266.
Dewey D, Kaplan BJ, Crawford SG, Wilson BN. Devel-opmental coordination disorder: Associated problems in attention, learning, and psychosocial adjustment. Hum Mov Sci 2002;21:905-918.
Dirks T, Hadders-Algra M. COPCA working manual; 2003.
Ekström Ahl L, Johansson E, Granat T, Brogren Carl-berg E. Functional therapy for children with cerebral palsy: an ecological approach. Dev Med Child Neurol 2005;47:613-619.
Fawke J. Neurological outcomes following preterm birth. Semin Fetal Neonatal Med 2007;12:374-382.
Finnie NR. Handling the young child with cerebral palsy at home. Oxford: Butterworth-Heinemann; 1996.
Gillberg C, Kadesjö B. Why bother about clumsiness? The implications of having developmental coordina-tion disorder (DCD). Neural Plast 2003;10:59-68.
Hack M, Fanaroff AA. Outcomes of children of extremely low birthweight and gestational age in the 1990s. Semin Neonatol 2000;5:89-106.
Hadders-Algra M. Developmental Coordination Disor-der: Is clumsy motor behavior caused by a lesion of the brain at early age? Neural Plast 2003;10:39-50.
Harris SR. Efficacy of physical therapy in promoting fam-ily functioning and functional independence for children with cerebral palsy. Ped Phys Ther 1990;2:160-164.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association; 2002.
24 25
Nijhuis BJG, Reinders-Messelink HA, De Blécourt ACE, Hitters MWMCG, Groothoff JW, Nakken H, Postema K. Family-centred care in family-specific teams. Clin Rehab 2007;21:660-671.
Palmer FB, Shapiro BK, Wachtel RC, Allen MC, Hiller JE, Harryman SE, Mosher BS, Meinert CL, Capute AJ. The effects of physical therapy on cerebral palsy. A controlled trial in infants with spastic diplegia. N Eng J Med 1988;318:803-808.
Palmer FB. Evaluation of developmental therapies in cerebral palsy. Ment Retard Dev Disabil Res Rev 1997;3:145-152.
Perlman JM, Risser R, Broyles RS. Bilateral cystic periventricular leukomalacia in the premature infant: associated risk factors. Pediatrics 1996;97:822-827.
Quinton MB, Nelson CA. Concepts&Guidelines for Baby Treatment. Clinician´s view, Albuquerque, New Mexico; 2002.
Raina P, O’Donnell M, Rosenbaum P, Brehaut J, Walter SD, Russell D, Swinton M, Zhu B, Wood E. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005;115:626-636.
Resnick MB, Eyler FD, Nelson RM, Eitzman DV, Bucciarelli RL. Developmental Intervention for low birth weight infants: Improved early developmental outcome. Pediatrics 1987;80:68-74.
Rosenbaum P, King S, Law M, King G, Evans J. Family-centred service: A conceptual framework and research review. Phys Occup Ther Pediatr 1998;18:1-20.
Rosenbaum P. Controversial treatment of spasticity: exploring alternative therapies for motor function in children with cerebral palsy. J Child Neurol 2003;18 Suppl 1:S89-94.
Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, Dan B, Jacobsson B. A report: the defi-nition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl 2007;109:8-14.
Schaaf RC, Miller LJ. Occupational therapy using a sensory integrative approach for children with devel-opmental disabilities. Ment Retard Dev Disabil Res Rev 2005;11:143-148.
Scrutton D. Management of the motor disorders of children with cerebral palsy. Oxford: Clinics in Devel-opmental Medicine 90, Spastics International Medical Publications; 1984.
Shonkoff JP, Meisels SJ, editors. Handbook of early childhood intervention. Cambridge: Cambridge Univer-sity Press; 2000.
Singer L, Salvator A, Guo S, Collin M, Lilien L, Baley J. Maternal psychological distress and parenting stress after the birth of a very low-birth-weight infant. JAMA 1999;28:799-805.
Spittle AJ, Orton J, Doyle LW, Boyd R. Early de-velopmental intervention programs post hospital discharge to prevent motor and cognitive impair-ments in preterm infants. Cochrane Database Syst Rev 2007;18:CD005495.
Stanger M, Oresic S. Rehabilitation approaches for children with cerebral palsy: overview. J Child Neurol 2003;18 Suppl 1:S79-88.
Stoelhorst GMSJ, Rijken M, Martens SE, Brand R, den Ouden AL, Wit JM, Veen S; Leiden Follow-Up Project on Prematurity. Changes in neonatology: Comparison of two cohorts of very preterm infants (gestational age <32 weeks): The project on preterm and small for gestational age infants 1983 and the Leiden follow-up project on prematurity. Pediatrics 2005;115:396-405.
Thelen E, Smith LB. A dynamic systems approach to the development of cognition and action. MIT Press, Cambridge, Mass; 1994.
Vargas S, Camilli G. A meta-analysis of research on sensory integration treatment. Am J Occup Ther 1999;53:189-198.
Vojta V. Die cerebralen Bewegungsstörungen im Säu-glingsalter: Frühdiagnose und Frühtherapie. Stuttgart: Enke; 1976.
Vojta V. The basic elements of treatment according to Vojta. In: D. Scrutton (ed), Management of the motor disorders of children with cerebral palsy. Oxford: Clin-ics in Developmental Medicine 90, Spastics Interna-tional Medical Publications; 1984:75-85.
Wichers MJ, Odding E, Stam HJ, Van Nieuwenhuizen O. Clinical presentation, associated disorders and aetiological moments in Cerebral Palsy: a Dutch popu-lation-based study. Disabil Rehabil 2005;27:583-589.
Wilson PH. Practitioner review: Approaches to assess-ment and treatment of children with DCD: An evalua-tive review. J Child Psychol Psyc 2005;46:806-823.
C H a P t E r 2
t h e
‘ V roe g t I j dIg
I n t e rV e n t I e
P roj e c t ’ ( V I P)

26 27
Dirks and Hadders-Algra (2003) developed a new physiotherapeutic intervention programme,
named COPCA, for infants at high risk for a developmental motor disorder. COPCA stands for
COPing with and CAring for infants with special needs – a family centred programme. The
COPCA intervention is based on new insights in the field of education and family care and in
the normal and abnormal development of the central nervous system. The effects of COPCA on
the development of infants at high risk for a developmental motor disorder were evaluated in the
early intervention project VIP (in Dutch “vroegtijdig interventie project”). The VIP project was
started in 2003 and the results are presented in this thesis (see Chapter 4,5,6,7, and 8). Infants who
had been admitted to the Neonatal Intensive Care Unit (NICU) of the University Medical Center
Groningen between March 2003 and May 2005 and showed definitely abnormal General Move-
ments (GM) were eligible for this study. The presence of definitely abnormal GMs indicates a high
risk for developmental motor disabilities, such as cerebral palsy (CP) (Prechtl 2001, Hadders-Algra
2004). Infants with severe congenital anomalies and infants whose parents had an inappropriate
understanding of the Dutch language were excluded from the study. The VIP project was designed
as a randomized controlled trial. Through block randomization infants were assigned to the ex-
perimental group who received the COPCA intervention or to the control group who got the tradi-
tional form of infant physical therapy (TIP). The second goal of the VIP project was to evaluate
the application of COPCA in daily practice by means of video analysis. This process evaluation is a
prerequisite for the implementation of COPCA within paediatric physiotherapy at a later stage.
In the next section a brief outline of the TIP and COPCA intervention is provided. The
remaining sections of this chapter describe the study design, subjects and outcome measures
involved in the early intervention project VIP. The outcomes of the VIP project are described in
Chapter 4, 5, 6, 7, and 8.
tIP
TIP consists of infant physical therapy as it is nowadays applied in the Netherlands. TIP includes
treatment strategies from a variety of physiotherapy programmes such as NDT, treatment accord-
ing to Vojta and the Functional approach. For a description of these programmes see Chapter 1.
For the most part TIP consists of the implementation of the ‘living concept’ of neurodevelopmen-
tal treatment (NDT; Howle 2002). Influences from the functional approach, such as the encour-
agement of self produced motor behaviour, are more and more incorporated into the treatment.
Due to the different influences which are incorporated in TIP a large heterogeneity in treatment
application can be expected.
COPCa
COPCA is a relationship family focused intervention programme built on two theoretical com-
ponents. The first component is based on the transactional model of development (Sameroff and
Chandler 1975, Fiese and Sameroff 1989) and recent findings in the field of education and family
care (Dale 1996, Law et al 1998, Rosenbaum et al 1998). The second component, a neurodevelop-
mental one, is based on the principles of the Neuronal Group Selection Theory (NGST; Edelman
1993).
An important base of COPCA is formed by the transactional model of development (Sameroff
and Chandler 1975, Fiese and Sameroff 1989) and new insights in the field of education and family
care (Dale 1996, Law et al 1998, Rosenbaum et al 1998). In the transactional model development
is seen as a result of a continuous dynamic interplay among child behaviour, caregiver responses
to the child’s behaviour, and environmental variables that may influence both the child and the
caregiver. Therefore in COPCA optimizing the interaction between caregiver and child is a key
factor of the intervention. The physiotherapist can be seen as an environmental factor that may
influence both the child and the caregiver. The physiotherapist acts as a coach who respects the
autonomy of the family and intends to make him- or herself superfluous. Caregivers are key-
persons in the COPCA programme. The physiotherapist and the family are partners, in which the
family defines the priorities for intervention, while the therapist coaches the family throughout
the intervention period (Law et al 1998). The PT provides information on infant development, the
specific problems of infants with neurological dysfunction, basic principles on infant education.
Specific ways in which development may be promoted and problems may be tackled. By means of a
continuous dialogue with the PT, caregivers develop their own ways to cope with the problems of
the infant.
The second component of COPCA is based on the principles of the NGST. The NGST em-
phasizes that development is the consequence of a complex interaction between genetic infor-
mation and environmental influences. According to the NGST development is characterized by
two phases of variability, i.e. primary and secondary variability. During primary variability the
child explores all variations of motor possibilities that are available in the nervous system. In this
phase the child is not yet able to adjust his behaviour to external conditions. In typically develop-
ing infants this phase is characterized by abundant variation. At function specific ages the infant
reaches the phase of secondary variability. The child gradually learns to select the most efficient
solution for a given task out of his motor repertoire. This selection is based on trial and error
experiences (Hadders-Algra 2000a). This means that during the phase of secondary variability
the child learns to adapt his/her motor behaviour to specific situations. Infants with a pre- or
perinatally acquired brain lesion resulting in a developmental motor disorder such as CP have a re-
duced repertoire of motor strategies available. This is already expressed during the first postnatal
months in a limited repertoire of general movements and continues when goal-directed motility
emerges (Hadders-Algra 2000b). In addition, these infants have problems with the selection of the
most appropriate solution for a certain task out of the repertoire due to deficits in the processing
of sensory information (Hadders-Algra 2000b). Therefore COPCA aims to promote variation in
motor behaviour and trial-and-error experiences by the means of play. The ultimate goal is to
provide an infant with a larger diversity in neuronal networks that will help to find an appropriate
solution for any given motor task.

28 29
Subjects and Procedure
The study groups of the VIP project consisted of infants who had been admitted to the Neonatal
Intensive Care Unit (NICU) of the University Medical Center Groningen between March 2003
and May 2005. At ten weeks corrected age (CA) a video recording was made of the infants’ General
Movements (GM). The assessment of the quality of GM can be considered as a technique to evalu-
ate the quality of the brain function in young infants (Prechtl 1990, 2001, Hadders-Algra 2004).
General Movements
GM are spontaneously generated complex movements involving the head, trunk, arms and legs.
They emerge at seven to eight weeks postmenstrual age and remain the most frequently observed
movement pattern until the age of three to four months after term age when they gradually are
replaced by goal-directed motor behaviour (Hadders-Algra 1996, 2001). Four classes can be distin-
guished in the assessment of GM quality: normal-optimal, normal-suboptimal, mildly abnormal
and definitely abnormal GM. In typical development GM are characterized by a considerable vari-
ation and complexity and to a smaller extent by fluency. When GM are less optimal fluency is the
first aspect that disappears, the movements become more jerky or stiff. Variation and complexity
disappear when the movements become more abnormal. Various studies have shown that the
presence of definitely abnormal GM at the age of two to four months corrected age (CA), the so-
called fidgety GM phase, is associated with a high risk for developmental motor disorders such as
CP (Prechtl et al 1997, Prechtl 2001, Hadders-Algra 2004, Groen et al 2005). Research showed that
the GM method has a good predictive validity for both major and minor developmental disorders
Heineman and Hadders-Algra, 2008). Hadders-Algra (2004) showed that the infants who show
definitely abnormal GM, but do not develop a CP usually show other developmental problems,
such as minor neurological dysfunction (MND) and behavioural problems. Also the construct and
concurrent validity and reliability of the GM method are satisfactory (Heineman and Hadders-
Algra 2008). The early detection of infants at high risk for developmental disorders offers the
opportunity for intervention at young age, during a phase in which the central nervous system is
characterized by high plasticity (Kolb et al 2001, De Graaf-Peters and Hadders-Algra 2006). Plas-
ticity means that the brain can reorganize itself to some extent. Neurons neighbouring a lesioned
part can change function and become incorporated into the affected repertoires, thereby increas-
ing the variation of the movement repertoire of the child (Hadders-Algra 2000b).
During the period of March 2003 till May 2005 in total 257 video recordings of GM were made
for the VIP project. Infants and their families were selected to participate in the project when
the quality of the infants’ GM was classified as definitely abnormal. Sixty-two infants showed
definitely abnormal GM (Figure 2.1). Infants with severe congenital anomalies and infants whose
caregivers had an inappropriate understanding of the Dutch language were excluded from the
study. Forty-six families decided to participate in the VIP project. Through block randomization
(full term infants blocks of n=2; preterm infants blocks of n=12) the infants were assigned to the
experimental group who received the COPCA intervention (n=21) or to the control group who got
the traditional form of paediatric physical therapy (TIP; n=25). The randomized intervention was
provided between 3 to 6 months corrected age (CA). The COPCA intervention was carried out by
4 physiotherapists, who were intensively trained in the application of this method. COPCA was
applied twice a week for one hour in a home based setting. The application of TIP varied. Infants
received therapy with a median value of once a week, the mean duration of sessions was 30 min-
utes. TIP was also mainly applied in the home situation by the paediatric physiotherapist working
in the area. After the intervention period physical therapy was only continued when the paedia-
trician in charge of the care of the infant considered it necessary. In the TIP group were three
infants who did not receive physiotherapeutic guidance during the intervention period since their
paediatrician did not refer them to a physiotherapist.
Figure 2.1. Infants included into the VIP project.
Total number of infant GMs March 2003 – May 2005N = 257
Definitely abnormal GM qualityN = 62
RandomizedN = 46
COPCAN = 21
Assessed at 18 mo CAN = 21
TPPN = 25
Assesses at 18 mo CAN = 232 did not attend
Not randomizedN = 161 non-Dutch speaking parents3 severe congenital anomalies12 parental refusals
30 31
Evaluation and Outcome measures
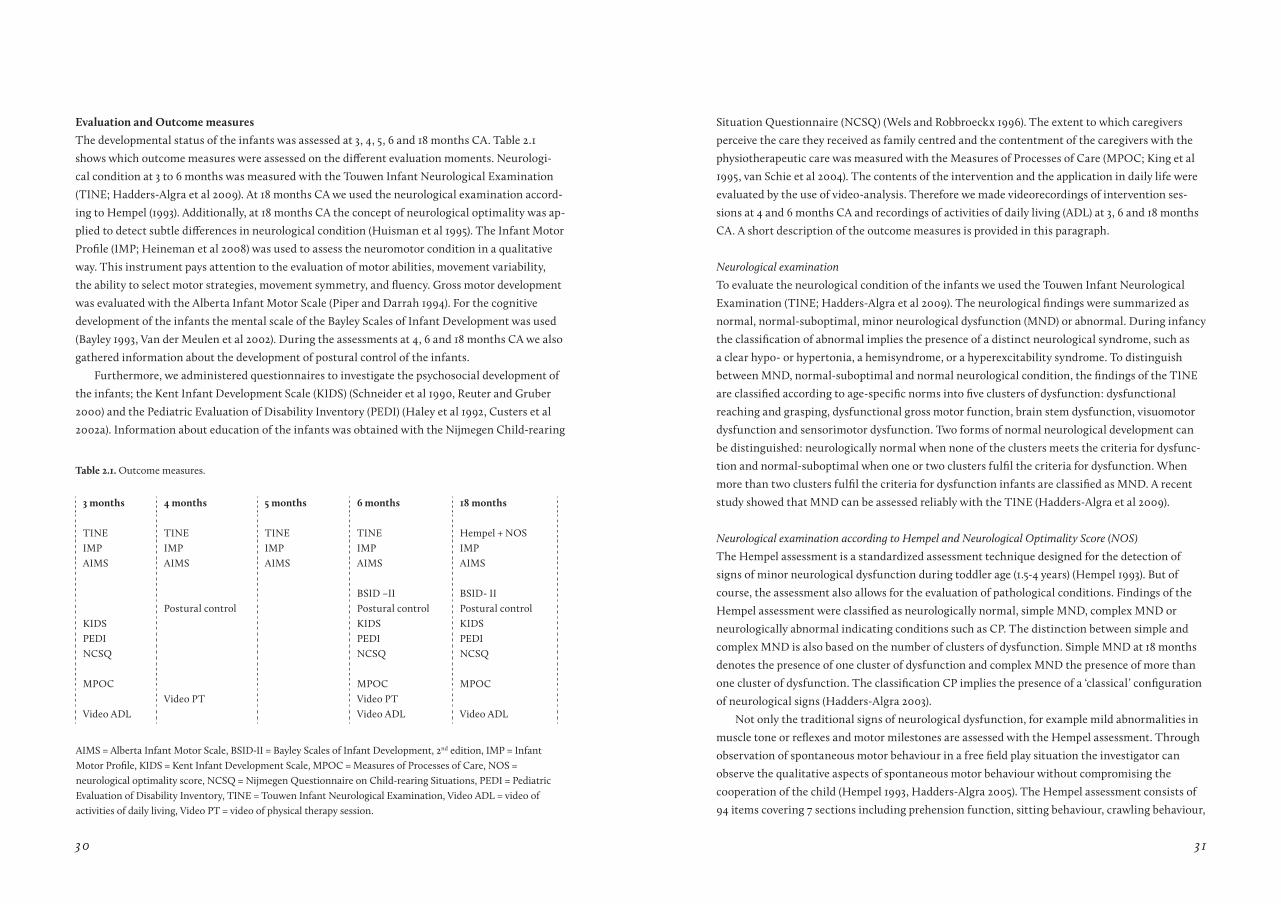
The developmental status of the infants was assessed at 3, 4, 5, 6 and 18 months CA. Table 2.1
shows which outcome measures were assessed on the different evaluation moments. Neurologi-
cal condition at 3 to 6 months was measured with the Touwen Infant Neurological Examination
(TINE; Hadders-Algra et al 2009). At 18 months CA we used the neurological examination accord-
ing to Hempel (1993). Additionally, at 18 months CA the concept of neurological optimality was ap-
plied to detect subtle differences in neurological condition (Huisman et al 1995). The Infant Motor
Profile (IMP; Heineman et al 2008) was used to assess the neuromotor condition in a qualitative
way. This instrument pays attention to the evaluation of motor abilities, movement variability,
the ability to select motor strategies, movement symmetry, and fluency. Gross motor development
was evaluated with the Alberta Infant Motor Scale (Piper and Darrah 1994). For the cognitive
development of the infants the mental scale of the Bayley Scales of Infant Development was used
(Bayley 1993, Van der Meulen et al 2002). During the assessments at 4, 6 and 18 months CA we also
gathered information about the development of postural control of the infants.
Furthermore, we administered questionnaires to investigate the psychosocial development of
the infants; the Kent Infant Development Scale (KIDS) (Schneider et al 1990, Reuter and Gruber
2000) and the Pediatric Evaluation of Disability Inventory (PEDI) (Haley et al 1992, Custers et al
2002a). Information about education of the infants was obtained with the Nijmegen Child-rearing
3 months 4 months 5 months 6 months 18 months
TINE TINE TINE TINE Hempel + NOSIMP IMP IMP IMP IMPAIMS AIMS AIMS AIMS AIMS
BSID –II BSID- IIPostural control Postural control Postural control
KIDS KIDS KIDSPEDI PEDI PEDINCSQ NCSQ NCSQ
MPOC MPOC MPOCVideo PT Video PT
Video ADL Video ADL Video ADL
table 2.1. Outcome measures.
AIMS = Alberta Infant Motor Scale, BSID-II = Bayley Scales of Infant Development, 2nd edition, IMP = Infant Motor Profile, KIDS = Kent Infant Development Scale, MPOC = Measures of Processes of Care, NOS = neurological optimality score, NCSQ = Nijmegen Questionnaire on Child-rearing Situations, PEDI = Pediatric Evaluation of Disability Inventory, TINE = Touwen Infant Neurological Examination, Video ADL = video of activities of daily living, Video PT = video of physical therapy session.
Situation Questionnaire (NCSQ) (Wels and Robbroeckx 1996). The extent to which caregivers
perceive the care they received as family centred and the contentment of the caregivers with the
physiotherapeutic care was measured with the Measures of Processes of Care (MPOC; King et al
1995, van Schie et al 2004). The contents of the intervention and the application in daily life were
evaluated by the use of video-analysis. Therefore we made videorecordings of intervention ses-
sions at 4 and 6 months CA and recordings of activities of daily living (ADL) at 3, 6 and 18 months
CA. A short description of the outcome measures is provided in this paragraph.
Neurological examination
To evaluate the neurological condition of the infants we used the Touwen Infant Neurological
Examination (TINE; Hadders-Algra et al 2009). The neurological findings were summarized as
normal, normal-suboptimal, minor neurological dysfunction (MND) or abnormal. During infancy
the classification of abnormal implies the presence of a distinct neurological syndrome, such as
a clear hypo- or hypertonia, a hemisyndrome, or a hyperexcitability syndrome. To distinguish
between MND, normal-suboptimal and normal neurological condition, the findings of the TINE
are classified according to age-specific norms into five clusters of dysfunction: dysfunctional
reaching and grasping, dysfunctional gross motor function, brain stem dysfunction, visuomotor
dysfunction and sensorimotor dysfunction. Two forms of normal neurological development can
be distinguished: neurologically normal when none of the clusters meets the criteria for dysfunc-
tion and normal-suboptimal when one or two clusters fulfil the criteria for dysfunction. When
more than two clusters fulfil the criteria for dysfunction infants are classified as MND. A recent
study showed that MND can be assessed reliably with the TINE (Hadders-Algra et al 2009).
Neurological examination according to Hempel and Neurological Optimality Score (NOS)
The Hempel assessment is a standardized assessment technique designed for the detection of
signs of minor neurological dysfunction during toddler age (1.5-4 years) (Hempel 1993). But of
course, the assessment also allows for the evaluation of pathological conditions. Findings of the
Hempel assessment were classified as neurologically normal, simple MND, complex MND or
neurologically abnormal indicating conditions such as CP. The distinction between simple and
complex MND is also based on the number of clusters of dysfunction. Simple MND at 18 months
denotes the presence of one cluster of dysfunction and complex MND the presence of more than
one cluster of dysfunction. The classification CP implies the presence of a ‘classical’ configuration
of neurological signs (Hadders-Algra 2003).
Not only the traditional signs of neurological dysfunction, for example mild abnormalities in
muscle tone or reflexes and motor milestones are assessed with the Hempel assessment. Through
observation of spontaneous motor behaviour in a free field play situation the investigator can
observe the qualitative aspects of spontaneous motor behaviour without compromising the
cooperation of the child (Hempel 1993, Hadders-Algra 2005). The Hempel assessment consists of
94 items covering 7 sections including prehension function, sitting behaviour, crawling behaviour,
32 33
standing and walking behaviour, evaluation of cranial nerve functions, and sensorimotor
function by means of manipulation including the assessment of muscle tone and the intensity and
threshold of reflexes. Little information is available about the concurrent and predictive validity of
the Hempel assessment. The interrater reliability is satisfactory (Hempel 1993).
Additionally at 18 months CA we used the Neurological Optimality Score (NOS) (Huisman et
al 1995) to summarize neurological condition. Based on the neurological examination an optimal-
ity score can be calculated to detect small deviations in neurological condition. The NOS is the
sum of 57 items representing the neurological examination that meet predefined criteria for opti-
mality. Note that the definition of optimal is narrower than that of normal or typical, and that a
reduced optimality not always means abnormal (Prechtl 1980). The NOS has been proven to be an
excellent instrument to evaluate subtle differences in neurodevelopmental outcome (Bouwstra et
al 2006).
Infant Motor Profile
The IMP is a video-based assessment of motor behaviour in infancy (Heineman et al 2008). The
IMP consists of 80 items that evaluate motor abilities, movement variability, the ability to select
motor strategies, movement symmetry, and fluency. It is applicable in children from 3 to 18
months. The advantage of the IMP is that it evaluates motor behaviour in a qualitative way. The
IMP has sound psychometric properties. The intra- and interobserver agreement are satisfactory
and the concurrent validity with the AIMS was good. Moreover the IMP was able to differentiate
between infants with normal neurological condition, simple MND, complex MND, and abnormal
neurological condition (Heineman et al 2008). No information is available on the predictive vali-
dity of the IMP.
Alberta Infant Motor Scale
The Alberta Infant Motor Scale (AIMS; Piper and Darrah 1994) is an observational instrument to
measure gross motor development for infants from birth to independent walking. The AIMS con-
sists of 58 items and is organized into four positions: prone, supine, sitting and standing. Through
observation of spontaneous motor behaviour each item can be scored on three aspects of motor
performance, namely weight bearing, posture and antigravity movements. The AIMS can be used
for two purposes. First, to identify infants who are delayed or atypical in their motor performance
and second to evaluate motor development over time (Piper and Darrah 1994). The AIMS has very
good reliability coefficients (Piper and Darrah 1994, Heineman and Hadders-Algra 2008). Also the
validity of the AIMS is well examined and proven to be satisfactory (Piper and Darrah 1994, Dar-
rah et al 1998, Liao and Campbell 2004).
Bayley Scales of Infant Development
The Bayley Scales of Infant Development (BSID-II; Bayley 1993) is a psychometric sound instru-
ment to assess mental and psychomotor development of children aged 1 to 42 months. In the early
intervention project the Dutch version of the BSID-II was used to assess the cognitive develop-
ment at the age of 6 and 18 months CA (Van der Meulen et al 2002). The BSID-II consists of a
mental developmental index (MDI) and a psychomotor developmental index (PDI). A limitation of
the BSID-II psychomotor scale is that the emphasis is placed on cognitive motor performances.
Therefore we decided to administer only the MDI for the VIP project and to assess gross motor
development with the AIMS and the qualitative aspects of motor performance with the IMP. The
MDI was scored based on the items successfully completed. The MDI consists of items concern-
ing problem solving, memory, discrimination, classification, language and social skills. Since the
children were not exactly 6 or 18 months at time of the assessment, the scores were converted
into age-equivalent scores, as derived from the Dutch norms (van der Meulen et al 2002). The
interrater reliability of the MDI is sufficient, the construct and concurrent validity are moderate
(Heineman and Hadders-Algra 2008).
Postural control
The development of postural control was assessed, because infants with high risk for developmen-
tal disorders often have problems with their postural control which interfere with the activities
of daily life (Brogren et al 2001, Van der Heide et al 2004). Postural activity was assessed at 4 and 6
months CA during reaching while lying in supine and while sitting with support, and at 18 months
CA while sitting with support and – when possible – without support. Reaching was elicited by
presenting toys when the infant was in a calm and alert behavioural state. Elecromyografic (EMG)
recordings were measured continuously during the testing session with bipolar surface electrodes
placed on the following muscles: deltoid, pectoralis major, biceps brachii, triceps brachii, neck
flexor (m. sternocleidomastoid), neck extensor, rectus abdominis, thoracal extensor, lumbar ex-
tensor, rectus femoris, and hamstrings on the right side of the body. Simultaneous with the EMG
recordings, movements were recorded kinematically. For a detailed description of the procedure
see de Graaf-Peters et al (2007).
Kent Inventory of Developmental Skills (KIDS)
The Kent Inventory of Developmental Skills is a caregiver-completed developmental assessment
instrument for healthy infants, infants at risk, and for young children with developmental disabil-
ities who are chronologically or developmentally under the age of 15 months (Schneider et al 1990,
Reuter and Gruber 2000). The KIDS was used as comparison to the BSID-II. Both measures aim to
evaluate the developmental level of the infant. At 3 months CA only the KIDS was administered to
minimize the physical effort of the infant. At 6 and 18 months CA both instruments were assessed,
being aware that the KIDS at 18 months might suffer from a ceiling effect. Parents were asked to fill
out the questionnaire at home at 3,6, and 18 months CA and return it to the researchers.
The main idea of the KIDS is that all new behaviours are acquired in a more or less fixed order
which is age dependent. The KIDS comprises of 252 behavioural items which are divided into
five areas: motor behaviour (78 items), cognition (52 items), social behaviour (51 items), ability to
34 35
perform things independently (39 items) and language (38 items). Caregivers fill in whether or not
their child shows the described behaviour. The total score provides an impression whether the
developmental status of the child corresponds with the average chronological age of its peers with
similar behavioural repertoires, and the status of the child as having no delay, at risk or develop-
mentally delayed. Research showed that the interrater agreement, test-retest reliability and vali-
dity were high (Schneider et al 1990, Reuter and Gruber 2000). As the KIDS is a parent reported
questionnaire it can be discussed whether caregivers are capable to objectively judge the develop-
ment of their infant. Research has shown that most caregivers are very well capable of judging
their infants’ developmental level (Harris 1994, Johnson et al 2008). Therefore we assume that this
is also the case in the VIP project.
Pediatric Evaluation of Disability Inventory
The Pediatric Evaluation of Disability Inventory (PEDI; Haley et al 1992) was used to measure the
functional ability of the child. This assessment instrument is developed for young children from
6 months to 7.5 years of age with developmental disabilities and adapted to a Dutch version by
Custers et al (2002a). The PEDI is a discriminative measure which aims to detect whether a child
has a delay in his functional status and if so to determine the extent and content area of the delay.
With the PEDI both the capability of the child (what a child can do) and the performance (what
the child actually does do) of routine daily activities can be evaluated. Capability is measured by
the functional skills scale (197 items), while the caregiver assistance scale and the modifications
scale provide information on the performance (20 items). Each scale consists of three domains
namely self-care, mobility and social function. The PEDI can be considered as a reliable and valid
instrument (Custers et al 2002a, 2002b, Wassenberg-Severijnen et al 2003).
Measures of Processes of Care (MPOC)
The MPOC is designed to determine the extent to which caregivers perceive the health services
they receive as family centred (King et al 1995, 1997). In the VIP project we used the Dutch trans-
lation of the MPOC (Van Schie et al 2004). Additionally, the MPOC was also used to evaluate
whether the attitude of caregivers regarding health services changed over time. The MPOC is a
56-item self-administered questionnaire categorised in five domains: a) enabling and partnership,
b) providing general information, c) providing specific information about the child, d) coordinated
and comprehensive care, e) respectful and supportive care. The items ask to what extent a particu-
lar behaviour occurred during the past year. The responses are given on a 7-point scale ranging from
‘not at all’ to ‘to a very great extent’ with an additional ‘not applicable’ category. Domain scores are
calculated as the mean of the ratings for the items in the scale and is only considered as valid when
at least two third of the items in the scale received a score. The validity criterion for the question-
naire was completion of at least half of the items. The Dutch translation of the MPOC has sound
psychometric properties; the construct validity and reliability measures are good (Van Schie et al
2004).
Nijmegen Child-rearing Situation Questionnaire (NCSQ)
The Nijmegen Child-rearing Situation Questionnaire (NCSQ, Wels & Robbroeckx 1996) was used
to investigate the existing parenting situation. The questionnaire is based on the stress model
of Lazarus and the attribution theory of Weiner (Wels and Robbroeckx 1996). The instrument
consists of 4 scales: A) Subjective Family Stress. This scale consists of 46 items which form eight
categories: a) acceptance of the child, b) coping, c) experience problems, d) need for change, e)
child is a strain, f) managing on one’s own, g) having pleasure, h) relation. B) Assessment of the
childrearing situation. Parents are instructed to indicate which of eight descriptions fits best
their own situation. In the first situation, no problems in child-rearing are present and support
is absolutely unnecessary. In situation eight, child-rearing is highly problematic and parents are
in urgent need of support. C) Attributions on the Child-rearing situation. This scale consists of
34 items which form five categories: a) ability, b) effort of oneself and partner, c) task difficulty, d)
share of partner, e) luck/fate. D) Expectation for help. This last scale has 36 items divided over five
categories: a) satisfaction, b) need for change, c) need for help, d) expectation for help (internal
orientation), and e) expectation for help (external orientation). The answers of the y questions in
scale A, C and D are rated on a 5-point Likert scale, ranging from 1 = ‘‘does not apply to me at all’’
to 5 = ‘‘applies to me’’. Sum scores were calculated for each category and converted into weighted
scores. Higher scores indicate that the caregivers experience a relatively greater burden on the
child’s education. The reliability and the validity are sufficiently assessed (Wels and Robbroeckx
1996). Note however that later research showed that the norms are insufficiently assessed, because
the reference groups were too small (Evers et al 2000). The caregivers are asked to fill in the NCSQ
at 3, 6 and 18 months corrected age.
Video recordings of physical therapy sessions and ADL activities
During the VIP project video recordings were made of physiotherapeutic intervention sessions
and of daily caregiving tasks. Albrecht et al (2005) showed that video recording hardly affects the
behaviour of people that are being filmed, because they tend to forget the camera after a while. In
order to ensure that the recording would resemble a natural situation and to minimize intrusion
we took the following precautions: the camera was positioned as far away from the physiothera-
pist, caregiver and infant as possible and the physiotherapist and caregiver were asked to ignore
the person making the video.
Video recordings of intervention sessions were made at 4 and 6 months CA. They were used to
gain knowledge on the contents of paediatric physiotherapeutic intervention. On the one hand,
this clearly showed whether the contents of COPCA were significantly different from the contents
of TIP. On the other hand, the analysis of the video recordings enabled us to answer the question
whether the COPCA programme could be well implemented in daily physiotherapeutic practice
(see for more detail Chapter 5 and 6).
The video recordings of activities of daily living – i.e. bathing and playing – showed how well
principles of the COPCA programme were implemented in the daily life of the families. These
36 37
activities were recorded at 3, 6 and 18 months CA. In this thesis the analysis and results of the ADL
video recordings will not be further described.
The outcomes of the VIP project are presented in Chapter 4, 5, 6, 7, and 8. In Chapter 4 some pre-
liminary results of the first half of the study group on the neurological examination, NOS, AIMS
and MDI of the BSID-II are described. Chapter 5 and 6 report the results of the video analysis on
the contents of paediatric physiotherapeutic intervention, i.e. COPCA and TIP. In Chapter 7 the
developmental outcome of the infants on the neurological examination, NOS, AIMS, MDI of the
BSID-II and PEDI is described. Subsequently, to examine whether developmental outcome could
be associated with treatment principles used by the PT or caregiver during intervention or with
confounding factors we applied process evaluation to the data. Finally, in Chapter 8 an overview
of the results on outcome measures which were also assessed during the VIP project, but were not
the focus in the previous Chapters is provided. Attention is paid to the results of the following
questionnaires: KIDS, MPOC, and NQCS. Also some preliminary results on the postural control
of the infants are described. Data of the IMP, the ADL video recordings and postural control are
currently being assessed.
references
Albrecht TL, Ruckdeschel JC, Ray FL, Pethe BJ, Riddle DL, Strohm J, Penner LA, Coovert MD, Quinn G, Blanchard CG. Portable, Unobtrusive Device for Vid-eorecording Clinical Interactions. Behav Res Methods 2005;37:165-169.
Bayley N. Manual of the Bayley Scales of Infant Develop-ment (second edition). San Antonio, The psychological Corporation; 1993.
Bouwstra H, Dijck-Brouwer J, Decsi T, Boehm G, Bo-ersma ER, Muskiet FA, Hadders-Algra M. Neurologic condition of healthy term infants at 18 months: posi-tive association with venous umbilical DHA status and negative association with umbilical trans-fatty acids. Pediatr Res 2006:60;334-339.
Brogren E, Forssberg H, Hadders-Algra M. Influence of two different sitting positions on postural adjust-ments in children with spastic diplegia. Dev Med Child Neurol 2001;43:534-546.
Custers JWH, Wassenberg-Severijnen JE, van der Net J, Vermeer A, ’t Hart H, Helders PJM. Dutch adaptation and content validity of the Pediatric Evaluation of Dis-ability Inventory (PEDI). Dis Rehab 2002a;24:250-258.
Custers JWH, van der Net J, Hoijtink H, Wassenberg-Severijnen JE, Vermeer A, Helders PJM. Discrimina-tive validity of the Dutch Pediatric Evaluation of Disability Inventory (PEDI). Arch Phys Med Rehabil 2002b;83:1437-1441.
Dale N. Working with families of children with Special Needs. Routledge London; 1996.
Darrah J, Piper M, Watt MJ. Assessment of gross motor skills of at-risk infants: predictive validity of the Alberta Infant Motor Scale. Dev Med Child Neurol 1998;40:485-491.
De Graaf-Peters VB, Hadders-Algra M. Ontogeny of the human central nervous system: what is happening when? Early Hum Dev 2006;82:257-266.
De Graaf-Peters VB, Blauw-Hospers CH, Dirks T, Bakker J, Bos AF, Hadders-Algra M. Development of postural control in typically developing children and children with cerebral palsy: possibilities for interven-tion? Neurosci Biobehav Rev 2007;31:1191-1200.
Dirks T, Hadders-Algra M. COPCA working manual; 2003.
Edelman GM. Neural Darwinism: Selection and reentrant signalling in higher brain function. Neuron 1993;10:115-125.
Evers A, Van Vliet-Mulder JC, Groot CJ. Documenta-tie van Tests en Testresearch in Nederland. Assen: Van Gorcum; 2000.
Fiese BH, Sameroff AJ. Family context in pediatric psy-chology: a transactional perspective. J Pediatr Psychol 1989;14:293-314.
Groen SE, de Blecourt AC, Postema K, Hadders-Algra M. General movements in early infancy predict neu-romotor development at 9 to 12 years of age. Dev Med Child Neurol 2005;47:731-738.
Hadders-Algra M. The assessment of general move-ments is a valuable technique for the detection of brain dysfunction in young infants. A review. Acta Paediatr Suppl 1996;416:39-43.
Hadders-Algra M. The Neuronal Group Selection Theory: an attractive framework to explain variation in normal motor development. Dev Med Child Neurol 2000a;42:566-572.
Hadders-Algra M. The neuronal group selection theory: promising principles for understanding and treating developmental motor disorders. Dev Med Child Neurol 2000b;42:707-715
Hadders-Algra M. Early brain damage and the development of motor behavior in children: clues for therapeutic intervention? Neural Plast 2001;8:31-49.
Hadders-Algra M. Developmental coordination disor-der: is clumsy motor behaviour caused by a lesion of the brain at early age? Neural Plast 2003;10:39–50.
Hadders-Algra M. General movements: a window for early identification of children at high risk of develop-mental disorders. J Pediatr 2004;145:S12–S18.
Hadders-Algra M. The neuromotor examination of the preschool child and its prognostic significance. Ment Retard Dev Disabil Res Rev 2005;11:180-188.
Hadders-Algra M, Heineman KR, Bos AF, Middel-burg KJ. Minor neurological dysfunction in infancy: strengths and limitations. Dev Med Child Neurol 2010:52;87-92.
Haley SM, Coster WJ, Ludlow LH, Haltiwanger JT, Andrellos PJ. Pediatric Evaluation of Disability Inven-tory: Development, standardization, and administration manual. Boston, MA: New England Medical Centre Inc. and PEDI Research Group; 1992.
Harris SR. Parents’ and caregivers’ perceptions of their children’s development. Dev Med Child Neurol 1994;36:918-923.

38 39
Heineman KR, Bos AF, Hadders-Algra M. The Infant Motor Profile: a standardized and qualitative method to assess motor behaviour in infancy. Dev Med Child Neurol 2008:50;275-282.
Heineman K, Hadders-Algra M. Evaluation of neu-romotor function in infancy - a systematic review of methods available. J Dev Behav Pediatr 2008;29:315-323.
Hempel MS. Neurological development during tod-dling age in normal children and children at risk of de-velopmental disorders. Early Hum Dev 1993:34;47–57.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association; 2002.
Huisman M, Koopman-Esseboom C, Lanting CI, Van der Paauw CG, Tuinstra LGMTh, Fidler V, Weisglas-Kuperus N, Sauer PJJ, Boersma ER, Touwen BCL. Neurological condition in 18-month-old children perinatally exposed to polychlorinated biphenyls and dioxins. Early Hum Dev 1995:43;165-176.
Johnson S, Wolke D, Marlow N; Preterm Infant Parenting Study Group. Developmental assessment of preterm infants at 2 years: validity of parent reports. Dev Med Child Neurol 2008;50:58-62.
King S, Rosenbaum P, King G. The Measures of Proc-esses of Care, MPOC. Hamilton, Ontario, Canada, Neu-rodevelopmental Clinical Research Unit, McMaster University and Chedoke-McMaster Hospitals; 1995.
King GA, Rosenbaum PL, King SM. Evaluating family-centred service using a measure of parents’ percep-tions. Child Care Health Dev 1997;23:47-62.
Kolb B, Brown R, Witt-Lajeunesse A, Gibb R. Neural compensations after lesion of the cerebral cortex. Neural Plast 2001;8:1-16.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Oc-cup Ther Pediatr 1998;18:83-102.
Liao PM, Campbell SK. Examination of the item struc-ture of the Alberta Infant Motor Scale. Pediatr Phys Ther 2004;16:31-38.
Piper MC, Darrah J. Motor assessment of the developing infant. Philadelphia: Saunders; 1994.
Prechtl HFR. The optimality concept. Early Hum Dev 1980;4:201-205.
Prechtl HF. Qualitative changes of spontaneous move-ments in fetus and preterm infant are a marker of neu-rological dysfunction. Early Hum Dev 1990;23:151-158.
Prechtl HF, Einspieler C, Cioni G, Bos AF, Ferrari F, Sontheimer D. An early marker for neurological deficits after perinatal brain lesions. Lancet 1997;349:1361-1363.
Prechtl HFR. General movement assessment as a method of developmental neurology: new para-diGM and their consequences. Dev Med Child Neurol 2001;43:836-842.
Reuter J, Gruber C. KIDS. Kent Inventory of Develop-mental Skills. Manual. Los Angeles: Western Psycho-logical Services; 2000.
Rosenbaum P, King S, Law M, King G, Evans J. Family centered service: a conceptual framework and re-search review. Phys Occup Ther Pediatr 1998;18:1-20.
Sameroff AJ, Chandler MJ. Reproductive risk and the continuum of caretaking casualty. In Horowitz FD, Hetherington M, Scarr-Salapatek S and Siegal G (Eds.). Review of child development research. Chicago: Uni-versity of Chicago Press; 1975:187-244.
Schneider MJ, Loots GMP, Reuter J. Kent Infant Development Scale. Nederlandse bewerking. Handleiding. Lisse: Swets en Zeitlinger; 1990.
Van der Heide JC, Begeer C, Fock A, Otten B, Strem-melaar EF, van Eykern LA, Hadders-Algra M. Postural control during reaching in preterm children with cerebral palsy. Dev Med Child Neurol 2004;46:253-266.
Van der Meulen BF, Ruiter SAJ, Spelberg HCL, Smrko-vsky M. Bayley Scales of Infant Development - II. Dutch version. Lisse, Swets Test Publishers; 2002.
Van Schie PEM, Siebes RC, Ketelaar M, Vermeer A. The Measure of Processes of Care (MPOC): valida-tion of the Dutch translation. Child Care Health Dev 2004;30:529-539.
Wassenberg-Severijnen JE, Custers JWH, Hox JJ, Vermeer A, Helders PJM. Reliability of the Dutch Pediatric Evaluation of Disability Inventory (PEDI). Clin Rehabil 2003;17:457-462.
Wels PMA, Robbroeckx LMH. NVOS: Nijmeegse Vra-genlijst voor de opvoedingssituatie. Handleiding en Test. Lisse, Swets en Zeitlinger; 1996.
C H a P t E r 3
A s ys t e m At Ic r e V I e w
of t h e e f f e c t s of
e A r ly I n t e rV e n t Ion on
mo tor de V e l oPm e n t--------------------------------------------------------------------------------------------
CH BLAUW-HOSPERS, M HADDERS-ALGRA
Developmental Medicine and Child Neurology, 2005, 47; 421-432

40 41
abstract
We present a systematic review on the effect of early intervention starting between birth and the
corrected age of 18 months on motor development in infants at high risk for or with developmen-
tal motor disorders. Thirty-four studies fulfilled the selection-criteria.
Seventeen studies were applied within the NICU environment. Eight had a high methodologi-
cal quality. They evaluated various forms of intervention. The results indicated that NIDCAP
intervention might have a temporary positive effect on motor development. Twelve of the 17 post-
NICU studies had a high methodological quality. They addressed the effect of NDT and specific
or general developmental programmes. The results showed that intervention according to the
principles of NDT does not have a beneficial effect on motor development. They also indicated
that specific or general developmental programmes can have a positive effect on motor outcome.
We concluded that the type of intervention which might be beneficial for infants at preterm
age differs from the type which is effective in infants who have reached at least term age. At pre-
term age infants seem to benefit most from intervention which aims at mimicking the intra-
uterine environment, such as NIDCAP intervention. After term age, intervention by means of
specific or general developmental programmes has a positive effect on motor development.
Keywords
Early intervention, motor development, NDT, NIDCAP, infant stimulation
Introduction
In the last decades the importance of Early Intervention (EI) is generally recognized. But what ex-
actly is early intervention? Typically a single definition is used, which is applied for EI to children
at biological risk for developmental disorders and children with developmental disabilities. “Early
Intervention consists of multidisciplinary services provided to children from birth to 5 years of
age to promote child health and well-being, enhance emerging competencies, minimize devel-
opmental delays, remediate existing or emerging disabilities, prevent functional deterioration
and promote adaptive parenting and overall family functioning. These goals are accomplished
by individualized developmental, educational and therapeutic services for children in conjunc-
tion with mutually planned support for their families” (Shonkoff and Meisels 2000). In general,
EI programmes use techniques derived from the domains of physiotherapy, occupational therapy,
developmental psychology and education. Little attention is paid to the effect of nutrition, even
though it is well known that cognitive outcome of breastfed children is significantly better than
that of formula-fed children (Anderson et al 1999). The earliest studies on EI programmes prima-
rily addressed the improvement in motor skills. Later, the focus shifted towards family-focused
and other functional outcomes (Harris 1997). Thus, it appears that EI serves as an umbrella term
covering the whole field of childhood intervention.
One of the problems associated with the use of the term EI is the interpretation of ‘early’.
‘Early’ can be understood in two ways, namely as ‘early in life’ and as ‘early in the expression of the
condition’. Each of the two types of ‘earliness’ is associated with advantages and disadvantages for
intervention. The major advantage of intervening early in life is that the brain is considered to be
very plastic. The brain is especially plastic in the phase occurring after the completion of neuronal
migration during which the processes of dendritic outgrowth and synapse formation are highly
active (Kolb et al 2001). This means that high plasticity can be expected between 2 to 3 months
before until about 6 to 8 months after term age (Hadders-Algra 2001). However, there are two
potential disadvantages which might be associated with intervention early in life. First, the type of
problems the infant will develop later in life will not yet be clear. This makes effective goal setting
for EI difficult. Second, a part of the at-risk population will not develop a developmental disorder,
thereby making intervention perhaps superfluous for these children.
Intervention in children with a developmental disorder in general starts later in life, i.e. at the
time during infancy or preschool age when the condition is expressed in dysfunction. Two advan-
tages of the latter situation are that intervention is applied to children who are really in need of
EI and that the goals of the intervention can be formulated relatively easily. The most important
disadvantage of intervention which first starts when the disorder has become undeniable is that
it starts relatively late from a point of view of the plasticity of the brain (Hadders-Algra 2001).
Indeed, previous studies indicated that programmes which started before the ninth month post
term provided more improvement in both motor and personal skills than programmes starting
later (Shonkoff and Hauser-Cram 1987, Sharkey et al 1990). Thus, it seems wise to start early in
life.

42 43
Therefore, the aim of the present study is to systematically review studies on intervention starting
early in life in children at high biological risk for developmental disorders. In particular we aim
at unravelling the elements, which might contribute to a beneficial effect on motor development.
Specific attention is paid to the timing of intervention in order to see whether we can find indica-
tions for the existence of a crucial age period in which EI results in the most beneficial outcome.
Method
Selection procedure
A literature search was performed using the following electronic databases: MEDLINE (1966 to
July 2004), CINAHL (1982 to July 2004), AMED (1985 to July 2004), PsycINFO (1967 to July 2004)
and PEDro. Reference lists in original studies and reviews were also examined for appropriate
articles. The keyword ‘early intervention’ initially revealed 13,699 hits. In order to reduce the
number of hits the following additional keywords were used: ‘infant’, ‘motor development’, ‘low
birth weight’, ‘preterm’, ‘high-risk’ and ‘cerebral palsy’. Thereafter the number of hits was limited
to 485.
From these 485 papers only studies were included in the review when they fulfilled the follow-
ing four criteria: a) subjects of study: infants with high biological risk for or with developmental
disabilities, b) aim of the intervention (mostly amongst others): to improve motor development, c)
onset of intervention in at least 50% of the participating children: between birth and the (cor-
rected) age of 18 months, d) journal in which the study was published had an impact factor of > 0.3.
Excluded from the review were studies restricted to medical and orthopaedic interventions and
studies in populations of healthy low-risk preterm infants or in populations of socially disadvan-
taged children without specific biological risk for developmental disorders.
Based on the abstract, 60 papers were selected as potential candidates for the review. Reading
the entire paper left 36 original studies which met all inclusion criteria. There were two studies
within this selection of which the results were published in more than one paper (Resnick et al
1987, 1988, Palmer et al 1988, 1990). In the present review these studies were treated as single
entities. The papers not included in the review mainly were review articles, studies focusing on
improvement of cognitive function and studies in which the intervention was applied after the age
of 18 months.
Evaluation procedure
The evaluation of the studies focused on the type and size of groups included in the study, the
level of evidence (Table 3.1) and the internal and external validity of the study (criteria specified in
Table 3.2). The level of evidence of a study and its internal and external validity were the determi-
nants for the methodological quality of the study. All studies were rated independently by both
reviewers. Interrater agreement was calculated for each of the determinants of methodological
quality. Agreement was high: Cohen’s Kappa varied from K = 0.86 (internal validity), K = 0.94
(level of evidence) to K = 0.95 (external validity). Disagreements were discussed till consensus was
reached. In addition, attention was paid to specifics of the intervention programme, such as the
type of intervention, its period of application and intensity, the location where the intervention
had been carried out and parental involvement (Table 3.2). Finally, the age of the infants at evalu-
ation, the outcome measures and the results were specified to further evaluate the effect of the
intervention.
In order to assess the effect of the age period during which EI took place, we divided the stud-
ies into three age-groups (cf. Shonkoff & Hauser-Cram 1987, Sharkey et al 1990). The first group
consisted of a) studies dealing with intervention programmes applied in the Neonatal Intensive
Care Unit (NICU), b) the second group contained studies where the intervention programme
started between discharge from NICU care and 9 months corrected age, c) the third group in-
cluded studies where intervention started between 9 and 18 months corrected age.
The studies turned out to be so heterogeneous in type of intervention evaluated, outcome
measures used to evaluate the effect of intervention and age at which outcome was studied, that
no meta-analysis to examine effect sizes of interventions could be performed.
table 3.1. Levels of evidence (Sackett 1989, Butler and Darrah 2001).
Level Group research Single individual research
I Randomised controlled trials N=1 randomised controlled trialII Non-randomised controlled trials
Prospective cohort studies with concurrent control groupABABA designAlternating treatments (e.g. ABACA)Multiple baseline across participants
III Case studies with control participantsCohort studies with historical control group
ABA design
IV Case series without control participants AB designV Case reports
Non-empirical methodsCase reportsNon-empirical methods
results
Seventeen of the 34 studies dealt with interventions carried out within a NICU setting, eight
evaluated intervention starting between discharge from the NICU and 9 months and six studies
assessed intervention which started between 9 and 18 months corrected age. In three studies, the
age at onset of intervention exceeded the pre-set period criteria. Therefore, a fourth category of
age at onset of intervention was added, consisting of studies where intervention started at some
age between discharge from the NICU and 18 months corrected age. Within the age periods, stud-
ies were ranked primarily according to level of evidence, next based on internal validity, external
validity and effect (Tables 3.3-3.6).

44 45
Group & design DescriptionSample size
?Total, Experimental group, control or contrast groupNot present
Attrition?
NumberUnspecified
Study group?
High-risk (i.e. preterm/LBW), CP, DownUnspecified
Levels of evidence Levels according to Sackett’s method for grading research (Sackett, 1989) modified by Butler and Darrah (2001); see Table 3.1.
Internal validity: can measured effects be attributed to intervention under study?
+++-
High internal validityFair internal validityLow internal validityInternal validity can be reduced by various study variations such as subject assignment, contamination, co-intervention, and blind assessment
External validity: can results of research be generalized?
+++-
Generalization is plausibleSome possibilities for generalizationNo information about generalization
Methodological quality Based on level of evidence, internal and external validity
Intervention Method of treatmentContents description ++
+-
Detailed descriptionSummary onlyVery limited information
Period of application?
Description Unspecified
Intensity?
DescriptionUnspecified
Location Hospital, Home, CentreCombination
Parental involvement PT?
Enhance parental skillsParent is therapistUnspecified
Evaluation of effectAge at evaluation < term, around term, 1-9 mo post term, 9-18 mo, > 18 mo Outcome measures Neuromotor
DevelopmentalResults E=C, E>C, E<C
table 3.2. Evaluation criteria (modification of Siebes and Vermeer 2002). Populations and methods of intervention
The number of children included in the studies ranged from 10 to 746 individuals (median value:
n= 44.5; Table 3.3). Information about the rate of attrition was provided in 33 studies. It varied
from 0% to 64%, with a median value of 13%. In the majority of studies (24 out of 34) the study
group consisted of so-called high-risk infants, i.e. infants born preterm or infants with a low birth
weight. The remaining studies evaluated the effect of intervention in infants with cerebral palsy,
delayed mental and motor development or Down syndrome.
The intervention programmes applied showed considerable diversity (Table 3.4). In 29 studies,
at least brief information about the intervention method was given of which 10 studies gave a
more detailed description. In order to get some insight into the intervention strategies and pro-
cedures applied, we assessed whether programmes contained the following elements: procedures
to reduce stress, sensory stimulation (specific unimodal, specific multimodal, general multimo-
dal), motor intervention strategies (passive handling techniques, active training of specific motor
abilities, general motor training) and parent infant interaction strategies (Table 3.6). Both authors
assessed the composition of the intervention programmes independently. Interrater agreement
was high: Cohen’s Kappa for the various components varied from 0.79 to 1.00. NICU intervention
programmes mainly consisted of combinations of procedures aiming at the reduction of stress,
the provision of auditory, tactile, visual or vestibular stimuli and passive motor handling proce-
dures. Amongst the programmes which started after discharge from the NICU, Neurodevelop-
mental Treatment (NDT), which consists of a mix of general sensory stimulation and passive and
active motor intervention strategies, was the intervention most frequently used. Other frequently
applied forms of intervention were various forms of developmental programmes, which always in-
cluded general sensory stimulation and general stimulation of motor development, but also could
imply passive handling techniques and the enhancement of parent infant interaction.
Information about the period of application of the intervention was supplied in 30 studies.
Most NICU interventions were applied during variable periods, as most interventions took place
between the age of some postnatal days till discharge. The application period in the post-NICU
studies varied between 2 months and more than 4 years. Also the intensity of intervention showed
considerable heterogeneity. It ranged from once a month to continuous intervention. Programmes
starting after discharge from the NICU were mostly applied within a home based setting. Another
frequently used way to supply intervention was the use of hospital or centre based intervention
combined with home care. In 24 out of the 34 studies parents were incorporated into the interven-
tion. In 19 studies the focus was on enhancing parental skills, in the other five studies the parents
carried out (a part of) the intervention, i.e. the parents functioned as a therapist.
General evaluation of effects (Tables 3.3-3.7)
Most studies evaluated the effect of intervention on motor performance during the intervention,
immediately after the end of intervention and/or some months or 1-2 years after intervention. Var-
ious sorts of outcome measures were used for effect evaluation. We categorized the measures into

46 47
Stud
y N
E
C
Attr
itio
n
(%)
Stud
y gr
oup
Evid
ence
leve
l
Inte
rnal
valid
ity
Exte
rnal
valid
ity
NIC
UA
ls e
t al.
1994
3820
180
HR
I++
++R
esni
ck e
t al.
1987
/198
825
510
711
413
HR
I+
+D
arra
h et
al.
1994
107
5354
51H
RI
++
Ari
agno
et a
l. 19
9735
1414
20H
RI
++
Cha
rpak
et a
l. 20
0174
638
236
416
HR
I+
+N
elso
n et
al.
2001
3721
1630
HR
or
CN
S in
jury
I+
+K
lebe
rg e
t al.
2002
2511
920
HR
I+
+Te
ssie
r et
al.
2003
431
183
153
22H
RI
++
Wes
trup
et a
l. 20
0441
2120
37H
RI
+-
Kor
ner
et a
l. 19
8356
128
64H
RI
--
Feld
man
et a
l. 20
0214
673
739
HR
II-
-H
elde
rs e
t al.
1989
149
6782
34H
RII
--
Als
et a
l. 19
8616
88
0H
RII
I+
-Le
ib e
t al.
1980
2814
140
HR
III
--
Mou
radi
an a
nd A
ls 19
9440
2020
0H
RII
I-
-B
ecke
r et
al.
1999
38?
?61
HR
III
--
Kle
berg
et a
l. 20
0033
1518
?H
RII
I-
-
aft
er N
ICU
– 9
mo
Goo
dman
et a
l. 19
85
8040
4001
HR
I++
++Pi
per
et a
l. 19
8613
466
6814
HR
I++
++Le
kscu
lcha
i and
Col
e 20
0184
4341
14H
RI
+++
Bar
rera
et a
l. 19
8680
3248
26H
RI
+++
Wei
ndlin
g et
al.
1996
105
5154
21H
R o
f CP
I++
+R
othb
erg
et a
l. 19
9149
2821
391
HR
I+
+D
’ Avi
gnon
et a
l. 19
8132
12/1
028
6H
RI
+-
Kan
da e
t al.
2004
105
50
CP
III
--
9 m
o –
18 m
oU
lric
h et
al.
2001
3015
150
DS
I++
++Pa
lmer
et a
l. 19
88/1
990
4825
232
CP
I++
++R
eddi
houg
h et
al.
1998
6632
349
CP
I+
+M
ahon
ey 2
001
5028
220
CP/
DS
II++
+Ei
ckm
ann
et a
l. 20
0315
678
7813
Del
ayed
cog
n/ m
ot d
evII
++
Pipe
r an
d Pl
ess
1980
3721
160
DS
III
+-
aft
er N
ICU
– 1
8 m
oM
ayo
1991
2917
120
Susp
ecte
d C
PI
+++
Sche
rzer
et a
l. 19
7624
148
8C
PI
+++
Har
ris
1981
2010
100
DS
I+
+
tab
le 3
.3. G
roup
s an
d de
sign
.
C =
Con
trol
/con
tras
t gro
up, C
NS
= C
entr
al N
ervo
us S
yste
m, C
P =
cere
bral
pal
sy, D
elay
ed c
ogn
/mot
dev
= D
elay
ed c
ogn
itiv
e/m
otor
dev
elop
men
t,
DS
= D
own
synd
rom
e, E
= E
xper
imen
tal g
roup
, HR
= H
igh
risk
1 In t
he t
ime
betw
een
the
two
stud
ies
31 c
hild
ren
wer
e lo
st to
follo
w-u
p 2 Te
n in
fant
s re
ceiv
ed a
diff
eren
t kin
d of
inte
rven
tion
48 49
neuromotor ones or as tests which provide a more general description of the child’s developmental
level (Table 3.7). The Bayley Scales of Infant Development were most frequently used as outcome
measure for both neuromotor (PDI) and developmental (MDI) outcome. In 26 studies develop-
mental tests were used to evaluate the effect of intervention. In nine of these a beneficial effect of
intervention on the developmental parameters was reported. In 26 studies neuromotor tests were
used. In 13 of these, experimental infants had a better neuromotor outcome than control infants.
Most studies were designed as randomised controlled trials. Twenty-three of the 34 studies
had the highest level of evidence, i.e. level I according to Sackett (see Table 3.1), four studies had a
grade II level of evidence and seven studies were classified as level III. Internal validity was high in
11 studies, fair in 15 and low in eight studies. External validity was in general moderate only: in five
studies generalization was plausible, 17 studies offered some possibilities for generalization and
12 studies had low external validity. Validity of post-NICU studies was usually better than that of
NICU studies.
In the next paragraphs we report the effects of intervention on motor development for the dif-
ferent age periods during which intervention had started, while taking into account the methodo-
logical strength of the studies.
Effect of intervention starting in the NICU
From the 17 NICU studies, eight had a high methodological quality. These studies had an evidence
level I, a fair to high internal validity and they provided at least some possibilities for generaliza-
tion. In two of these eight studies a significantly positive effect of intervention on motor outcome
could be demonstrated. One of the positive studies dealt with the effect of NIDCAP (Als et al
1994). The focus of intervention in this study was stress reduction in combination with general
sensory stimulation. The other intervention aimed at improving the infant’s general developmen-
tal level by means of a developmental programme, including general sensory stimulation, general
stimulation of motor development, passive handling techniques and the enhancement of parent
infant interaction (Resnick et al 1987, 1988). In the other six NICU studies of high methodologi-
cal quality, intervention had no statistically significant effect on motor development (Darrah et
al 1994, Nelson et al 2001, Ariagno et al 1997, Charpak et al 2001, Kleberg et al 2002, Tessier et al
2003). The interventions used in these studies all included procedures to reduce the infant’s level of
stress and multimodal sensory stimulation (either specific or general), which was or was not com-
bined with passive motor intervention techniques or the facilitation of parent infant interaction.
Five of the nine NICU studies with a lower methodological quality pointed to a positive effect of
intervention (Als et al 1986, Mouradian and Als 1994, Feldman et al 2002, Korner et al 1983, Leib et al
1980). Intervention used in these studies consisted of various combinations of procedures to reduce
stress, multimodal sensory stimulation, passive motor intervention strategies or the facilitation of
parent infant interaction. The remaining four studies were unable to demonstrate a beneficial effect
of intervention (Kleberg et al 2000, Westrup et al 2004, Helders et al 1989, Becker et al 1999).
Effect of intervention starting between NICU-discharge and 9 months
Six of the eight studies in which intervention started in the period between discharge from the
NICU and the corrected age of 9 months had a high methodological quality. In four studies,
amongst them the two methodologically strongest studies, the effects of NDT were evaluated
(Goodman et al 1985, Piper et al 1986, Rothberg et al 1991, Weindling et al 1996). None of the
NDT-studies demonstrated a statistically significant effect of intervention on motor develop-
ment. It should be noted however, that in two studies (Goodman et al 1985, Rothberg et al 1991)
outcome was evaluated only by means of global developmental tests. Two other studies (Barrera et
al 1986, Leksculchai and Cole 2001) applied a programme to stimulate infant motor development.
Both programmes consisted of general sensory stimulation and general stimulation of motor
development. In addition, the intervention in the Barrera et al. study included enhancement of
parent infant interaction, that of Leksculchai and Cole passive handling techniques. Both studies
reported a statistically significant positive effect of intervention on motor development. Two stud-
ies addressing the effect of intervention starting in this age period were of limited methodological
quality. One study evaluated in relatively small groups the effect of NDT and that of treatment
according to Vojta (d’Avignon et al 1981). It concluded that outcome in the two treatment groups
did not show a statistically significant difference. The other study reported a dose-response effect
of treatment according to Vojta on motor outcome (Kanda et al 2004).
Effect of intervention starting between 9 and 18 months
Three of the six post-NICU studies, in which intervention started between 9 and 18 months of
age, had a high methodological quality. One study demonstrated a positive effect of specific mo-
tor training on motor development of infants with Down syndrome (Ulrich et al 2001), another
revealed that a general infant stimulation programme facilitated motor development more than
NDT did (Palmer et al 1988, 1990). The third did not find a significant effect of conductive educa-
tion on motor development (Reddihough et al 1998). The other three late post-NICU studies had
a more limited methodological quality. One evaluated the effect of NDT and did not demonstrate
a significant positive effect of intervention (Mahoney 2001). The other two used general pro-
grammes to stimulate motor development. One of them found a beneficial effect of intervention
(Eickmann et al 2003).
Effect of intervention starting between NICU-discharge and 18 months
The three studies in which intervention started between discharge from the NICU and the age
of 18 months were all level I studies with a moderate to high internal validity and a moderate
external validity. Two studies evaluated the effect of NDT. The study which assessed the effect of
a short period of intensive NDT was unable to demonstrate a significant effect of intervention on
motor development (Harris 1981), the other which applied less intensive NDT for half a year did re-
port a positive effect of intervention on motor development (Mayo 1991). The third study evaluated
the effect of a general physical therapy programme and did not find a significant beneficial effect
of the intervention on motor development (Scherzer et al 1976).

50 51
tabl
e 3.
4. T
ype
of in
terv
enti
on.
ATVV = Auditory-Tactile-Visual-Vestibular Stimulation, C = Control group, Ce = Centre, CE = Conduc-tive Education, d = day, Descr. = description, Dev hand = Developmental Handling, Dev Int = Develop-mental Intervention, Dev mile = Developmental milestones, Dev pgm = Developmental programme, Dev S = Developmental Skills, Dev stim = Developmental stimulation, DPI = Developmental Program Intervention, E = Experimental group, h = hour, Hm = home, Hp = Hospital, I = Instruction, IS = Infant
Stud
yM
etho
dD
escr
.Pe
riod
of a
ppli
cati
onIn
ten
sity
Loc
atio
nPa
rent
sO
nse
tE
nd
NIC
U
A
ls e
t al.
1994
NID
CA
P++
3 d
afte
r bi
rth
?C
onti
nuou
sly
Hp
PR
esn
ick
et a
l. 19
87/1
988
Dev
Int
++B
irth
24 m
oH
p: d
aily
H
m: 2
x/m
oH
p/H
mP
Dar
rah
et a
l. 19
94W
b+
2-7
d af
ter
birt
hPl
acem
ent i
n op
en c
ots
Con
tinu
ousl
yH
p?
Ari
agno
et a
l. 19
97N
IDC
AP
+?
?C
onti
nuou
sly
Hp
P
Cha
rpak
et a
l. 20
01K
C+
3-5
d af
ter
birt
hPo
siti
on n
o lo
nger
acc
epte
dC
onti
nuou
sly
Hp
P
Nel
son
et a
l. 20
01AT
VV
++33
wk
PMA
2 m
oH
p: 1
5 m
in, 2
x/d
5x/w
k ,
Hm
: 2x/
d H
p/H
mT
Kle
berg
et a
l. 20
02N
IDC
AP
+1 d
aft
er b
irth
? C
onti
nuou
sly
Hp
PTe
ssie
r et
al.
2003
KC
++co
ndit
ion
stab
le
Dis
char
geC
onti
nuou
sly
Hp
PW
estr
up e
t al.
2004
NID
CA
P+
1 d a
fter
bir
th36
wk
PMA
Con
tinu
ousl
yH
pP
Kor
ner
et a
l. 19
83W
b+
< 4
d af
ter
birt
hT
ill e
valu
atio
nC
onti
nuou
sly
Hp
?
Feld
man
et a
l. 20
02K
C++
31-3
4 w
k PM
AD
isch
arge
, du
rati
on ≥
14d
> 1 h
/dH
pP
Hel
ders
et a
l. 19
89T
sti
m/ R
F-
Bir
thD
isch
arge
?H
p?
Als
et a
l. 19
86N
IDC
AP
++9
d af
ter
birt
hD
isch
arge
Con
tinu
ousl
yH
pP
Lei
b et
al.
1980
Sen
s En
r+
Bir
thD
isch
arge
?H
p?
Mou
radi
an a
nd A
ls
1994
NID
CA
P+
?<
40 w
PM
AC
onti
nuou
sly
Hp
P
Bec
ker
et a
l. 19
99D
ev h
and
+B
irth
36 w
k PM
A?
Hp
?K
lebe
rg e
t al.
2000
NID
CA
P+
3 d
afte
r bi
rth
36 w
k PM
A?
Hp
P
aft
er N
ICU
– 9
mo
Goo
dman
et a
l. 19
85N
DT
-3
mo
12 m
oI:
1x/
mo
> 45
min
P:
dai
ly (h
ome
prog
ram
me)
Hp/
Hm
P
Pipe
r et
al.
1986
ND
T+
Term
age
12 m
oI:
0-3
mo:
1x/
wk
3-
12 m
o: 1
x/2w
kP:
dai
lyH
mP
Lek
scul
chai
and
Col
e 20
01D
ev p
gm++
Term
age
4 m
oI :
1x/
mo
P: d
aily
Hm
T
Bar
rera
et a
l. 19
86D
PI /
PIT
+4
mo
16 m
oI:
4-7
mo:
1-2
h/w
k
7-13
mo:
1x/
2wk
13
-16
mo:
1x/
mo
Hm
P
Wei
ndli
ng e
t al.
1996
ND
T-
Term
age
12 m
o (C
P
con
tinu
e)I:
0-6
mo:
1x/
wk
6-
9 m
o: 1
x/2w
k
9-
12 m
o: 1
x/m
o
Hm
?
Rot
hber
g et
al.
1991
ND
T+
3 m
o12
mo
I: 1
x/m
o >
45 m
in
P: d
aily
(h
ome
prog
ram
me)
Hp/
Hm
P
D’ A
vign
on e
t al.
1981
Vojt
a/N
DT
-4-
7 m
oB
: > 3
mo
V: >
6 m
o ?
??
Kan
da e
t al.
2004
Vojt
a-
1 mo
E: M
ean
52 m
oC
: Mea
n 25
mo
E: ≥
30
min
, 3-
4x/d
ayH
mT
9 m
o –
18 m
oU
lric
h et
al.
2001
TT
+9-
12 m
o In
depe
nden
t w
alki
ng8
min
/d, 5
d/w
k H
mT
Palm
er e
t al.
1988
/199
0N
DT/
IS++
12-1
9 m
o D
urat
ion
12 m
oI:
1 h
1x/2
wk
P: d
aily
(h
ome
prog
ram
me)
Ce/
Hm
P
Red
diho
ugh
et a
l. 19
98C
E++
12-3
6 m
oD
urat
ion
6 m
oE:
2.8
h/w
k C
: 2.9
h/w
kC
e?
Mah
oney
200
1N
DT/
Dev
S+
Mea
n ag
e 14
mo
Dur
atio
n 12
mo
3x/m
o, 4
5 m
inC
e/H
m?
Eick
man
n et
al.
2003
Dev
sti
m+
13 m
o18
mo
I: 1
1 hm
vis
its
30-4
5 m
in,
3 w
orks
hops
Hm
P
Pipe
r an
d Pl
ess
1980
Dev
mile
+M
ean
age
9 m
oD
urat
ion
6 m
oI:
1 h
1x/2
wk
P: h
ome
prog
ram
me
Ce/
Hm
P
aft
er N
ICU
– 18
mo
May
o 19
91N
DT
+4-
18 m
oD
urat
ion
6 m
oE:
1 h/
wk
C: 1
h/m
o H
p/H
mP
Sche
rzer
et a
l 197
6Ph
ys T
+5-
17 m
o24
mo
1h 1
x/2w
kH
mT
Har
ris
1981
ND
T++
2-21
mo
Dur
atio
n 9
wk
E: 3
x/w
k >4
0 m
inH
m?
Stimulation, KC = Kangaroo Care, min = minutes, mo = months (corrected age), NDT = Neurodevelopmental Treatment, NIDCAP = Newborn Individualized Developmental Care and Assessment Program, P = parents, P= enhance parental skills, PIT = Parent-Infant treatment, PMA = post menstrual age, Phys T = Physical Therapy, Sens. Enr. = Sensory Enrichment, T = parents are ‘therapist’, T stim/RF = Tactile Stimulation/ Range Finding, TT = Treadmill Training, Wb = Waterbed, wk = weeks, ? = no information available

52 53
tab
le 3
.5. E
valu
atio
n of
eff
ect o
f int
erve
ntio
n.
age
s of
eva
luat
ion
Out
com
e m
easu
res1
res
ults
2
<ter
mte
rm1-
9 m
o9-
18 m
o>1
8 m
o N
euro
mot
orD
evel
opm
enta
l
NIC
UA
ls e
t al.
1994
--
19
-A
PIB
, Bay
ley
PDI
Bay
ley
MD
IE
> C
Res
nic
k et
al.
1987
/198
8-
--
1224
Bay
ley
PDI
Bay
ley
MD
IE
> C
Dar
rah
et a
l. 19
941x
+4,
812
18M
AI
Peab
ody
E =
CA
riag
no e
t al.
1997
1x-
1,4
1224
Bay
ley
PDI,
NA
PI, A
PIB
Bay
ley
MD
IE
= C
Cha
rpak
et a
l. 20
01-
+3,
69,
12-
-G
riffi
thE
= C
Nel
son
et a
l. 20
01-
-2,
412
-B
ayle
y PD
IB
ayle
y M
DI
E =
CK
lebe
rg e
t al.
2002
--
-12
-B
ayle
y PD
IB
ayle
y M
DI
E =
CTe
ssie
r et
al.
2003
--
-12
--
Gri
ffith
E =
CW
estr
up e
t al.
2004
--
--
66M
ovem
ent A
BC
-E
= C
Kor
ner
et a
l. 19
831x
--
--
LA
PPI
-E
> C
Feld
man
et a
l. 20
021x
-3,
6-
-B
ayle
y PD
IB
ayle
y M
DI
E >
CH
elde
rs e
t al.
1989
pre,
aft
er 2
wk,
wee
kly
till
disc
harg
e-
-PM
Dev
E =
CA
ls e
t al.
1986
4x+
1,3,
69
-A
PIB
, Bay
ley
PDI
Bay
ley
MD
IE
> C
Lei
b et
al.
1980
2x-
6-
-B
ayle
y PD
I, N
BA
SB
ayle
y M
DI
E >
CM
oura
dian
and
Als
1994
--
1-
-A
PIB
-E
> C
Bec
ker
et a
l. 19
993x
--
--
VA-
E =
CK
lebe
rg e
t al.
2000
--
--
36-
Gri
ffith
E =
C
aft
er N
ICU
– 9
mo
Goo
dman
et a
l. 19
85
--
69,
12-
-G
riffi
thE
= C
Pipe
r et
al.
1986
--
612
-W
olan
ski
Mil
ani,
Gri
ffith
E =
C
Leks
culc
hai a
nd C
ole
2001
-+
1,2,
3,4
--
TIM
P-
E >
CB
arre
ra e
t al.
1986
--
416
-B
ayle
y PD
IB
ayle
y M
DI
E >
CW
eind
ling
et a
l. 19
96-
--
1230
MA
IG
riffi
thE
= C
Rot
hber
g et
al.
1991
--
--
72-
Gri
ffith
-II
E =
CD
’Avi
gnon
et a
l. 19
81-
--
-36
-72
CP
clas
s-
E =
CK
anda
et a
l. 20
04-
-1,
2,3,
5ev
ery
3 m
o 59
Neu
rEx
-E
> C
9 m
o –
18 m
oU
lric
h et
al.
2001
--
ever
y 2
wk
Bay
ley
PDI
Bay
ley
MD
IE
> C
Palm
er e
t al.
1988
/199
0-
--
-18
,24
Bay
ley
PDI
Bay
ley
MD
IE
< C
Red
diho
ugh
et a
l. 19
98-
-pr
e-po
stG
MFM
-E
= C
Mah
oney
200
1-
--
-14
,26
-B
ayle
y M
DI,
Peab
ody
E =
C
Eick
man
n et
al.
2003
--
-12
18B
ayle
y PD
IB
ayle
y M
DI
E >
CPi
per
and
Ples
s 19
80-
--
pre-
post
-G
riffi
thE
= C
aft
er N
ICU
– 18
mo
May
o 19
91-
-pr
epo
stW
olan
ski
Bay
ley
MD
I,Ges
ell
E >
C
Sche
rzer
et a
l 197
6-
-pr
e24
MD
CG
esel
lE
= C
Har
ris
1981
--
pre
post
Bay
ley
PDI
Bay
ley
MD
I, Pe
abod
yE
= C
C =
Con
trol
gro
up, E
= E
xper
imen
tal g
roup
, mo
= m
onth
s, M
P =
mot
or p
erfo
rman
ce, p
re =
bef
ore
inte
rven
tion
, pos
t = a
fter
inte
rven
tion
, wk
= w
eeks
1 For
expl
anat
ion
of a
bbre
viat
ion
s se
e T
able
3.7
2 St
atis
tica
lly s
ign
ifica
nt d
iffer
ence
s fo
und
in m
otor
out
com
e at
old
est a
ge o
f eva
luat
ion:
E >
C:
Exp
erim
enta
l gro
up s
ign
ifica
ntly
bet
ter
outc
ome
than
C
ontr
ol G
roup
, E =
C: n
o di
ffer
ence
bet
wee
n gr
oups
, E <
C:
Con
trol
Gro
up b
ette
r ou
tcom
e th
an E
xper
imen
tal G
roup
.

54 55
Intervention Sensory Stimulation
Motor Intervention
Enhancing PII
S. r. S. u. S. m. G. m. P. a. s. a. g.Waterbed + - + - + - - -ATVV intervention + - + - - - - -NIDCAP + - - + + - - +KC + - - + + - - +Developmental handling + - - + + - - ?Treadmill training - + - - - + - -Tactile stimulation/Range finding - + - - + - - -Vojta - + - - + - - -Sensory enrichment - - + - - - - -Developmental intervention - - + - + - + +NDT - - - + + - + -Developmental program - - - + + - + -Developmental milestones - - - + - - + +Developmental Stimulation - - - + - - + +Developmental Parent intervention - - - + - - + +Infant Stimulation - - - + - - + +Conductive Education - - - + - - + -Developmental skills - - - + - - + ?Parent Infant treatment - - - - - - - +
+ = procedure used, - = procedure not used,? = insufficient information available,
PII = Parent Infant Interaction; for other abbreviations see legends Table 3.4.
S. R. = Stress Reduction, S. u. = Specific –unimodal, S. m. = Specific – multimodal, G. m. = General – multimo-
dal, P. = Passive, A. s. = Active – specific, A. g. = Active – general
Stress reduction: decreasing stressful events to the body by restricting input from the environment until the
infant is capable of maintaining an adequate organization of its behavioural state; placing the infant in a way as
to provide a sense of containment similar to the intrauterine environment.
Sensory stimulation:
a) specific-unimodal: procedures during which a single sensory modality is stimulated (e.g., specific tactile
stimulation)
b) specific-multimodal: procedures during which multiple specific sensory modalities are stimulated (e.g.,
ATVV which consists of the application of auditory, tactile, visual and vestibular stimuli)
c) general-multimodal: procedures during which multiple forms of not explicitly described sensory stimuli are
applied (e.g., verbal and tactile encouragement as part of general developmental programmes)
table 3.6. Composition of programmes used in EI. Motor intervention strategies:
a) passive procedures: the therapist or the parent carries out specific techniques, which do not require active
motor behaviour of the child, i.e., the child has a passive role (e.g. handling, positioning, and facilitation
procedures)
b) active-specific: the child is encouraged to actively train a specific motor ability (e.g., walking by means of
treadmill training)
c) active-general: the child is encouraged to train a variety of motor abilities; stimulation of activities occurs
in general by means of structured activities which are designed to meet the child’s developmental level.
Practice and play are important elements in the latter type of intervention.
Enhancing parent-infant interaction: parents receive information on infant behaviour. The increased knowl-
edge on infantile behaviour facilitates parent’s sensitivity to the child’s needs and promotes developmentally
supportive behaviour.
Discussion
We are not the first to write a review on the effects of early intervention for children at high risk
for developmental disabilities, others preceded us: Simeonsson et al 1982, Parette and Hourcade
1984, Casto and Mastropieri 1986, Shonkoff and Hauser-Cram 1987, Parry 1992, Turnbull 1993,
Guralnick 1997, Majnemer 1998. The major conclusion from these reviews is that the evidence
favouring EI is inconclusive. The results from this present review indicate that we have moved a
bit forward. In the following paragraphs we will point out the direction of progress. But before we
address the issues of ‘which programme at what age’, we first discuss some methodological issues.
Methodological considerations
The studies included in this review were very heterogenic in nature. Not only a large variation
existed in the number of subjects included in the studies, but also in the intervention methods
which started prior to 18 months. The interventions themselves, the outcome measures used
to evaluate the intervention methods and the ages at which outcome was determined were too
heterogeneous to allow for a formal meta-analysis. The methods of intervention in the NICU
period varied from NIDCAP and Kangaroo Care to different kinds of stimulation programmes.
In post NICU studies NDT was the leading method of intervention, but there were also studies
which used interventions like infant stimulation, conductive education and other developmental
programmes.
It was encouraging to notice that 20 out of 34 studies had a high methodological quality, i.e.,
they had an evidence level I and a fair to high internal and external validity. This reflects that
during recent years the requirement of good quality studies on the effect of early intervention has
been increasingly materialized (Siebes et al 2002). Previous studies indicated that with an increase
in the rigorousness of the studies the support for effectiveness of EI decreases (Parette and Hour-
cade 1984, Siebes et al 2002). For the studies included in the present review this also holds true.
Of the 20 studies with a high methodological quality only six (30%) were able to demonstrate a sig-

56 57
Neu
rom
otor
test
Dev
elop
men
tal t
est
Bay
ley
Scal
es o
f In
fant
Dev
elop
men
t -
Psyc
hom
otor
Dev
elop
men
t Ind
ex
Bay
ley-
PDI
1969
19
93G
riffi
ths
Dev
elop
men
tal S
cale
s G
riffi
th19
5419
70
Wol
ansk
i Gro
ss M
otor
Eva
luat
ion
Wol
ansk
i19
73M
ilan
i-C
ompa
rett
i Mot
or
Dev
elop
men
t Scr
een
ing
test
M
ilan
i19
67
Neo
nat
al B
ehav
iora
l Ass
essm
ent
Scor
e N
BA
S19
73
1984
Bay
ley
Scal
es o
f In
fant
Dev
elop
men
t -
Men
tal D
evel
opm
ent I
ndex
B
ayle
y-M
DI
1969
19
93M
otor
Dev
elop
men
t Che
ckli
st
MD
C
1976
Ges
ell D
evel
opm
enta
l Sch
edul
es
Ges
ell
1974
Mov
emen
t Ass
essm
ent o
f In
fant
s M
AI
1980
Peab
ody
Dev
elop
men
tal M
otor
Sca
les
Peab
ody
1974
Ass
essm
ent o
f Pre
term
Infa
nts’
Beh
avio
r A
PIB
1982
Mue
nche
ner
Fun
ktio
nelle
En
twic
klun
gs D
iagn
osti
kM
FED
1978
Lon
gitu
din
al n
euro
beha
vior
al a
sses
smen
t
proc
edur
e fo
r pr
eter
m in
fant
sL
APP
I19
83Ps
ycho
mot
or D
evel
opm
ent p
rofi
le
(bas
ed o
n G
esel
l)PM
Dev
1981
Supp
lem
enta
l Mot
or T
est f
or P
ostu
ral C
ontr
ol
PoC
o19
87N
euro
beha
vior
al A
sses
smen
t of t
he P
rete
rmIn
fant
NA
PI19
90
Mov
emen
t Ass
essm
ent B
atte
ry fo
r C
hild
ren
Mov
emen
t A
BC
1992
Gro
ss M
otor
Fun
ctio
n M
easu
re
GM
FM19
93Te
st o
f In
fant
Mot
or P
erfo
rman
ce
TIM
P19
95
Vid
eo-a
nal
ysis
(am
ount
and
var
iati
on in
mov
e-m
ents
)VA
1999
Cli
nic
al N
euro
logi
cal e
xam
inat
ion
Cli
n N
eur
Ex
n.f.
s.*
CP
clas
sific
atio
nC
P cl
ass
1981
*not
furt
her
spec
ified
tabl
e 3.
7. C
lass
ifica
tion
of o
utco
me
mea
sure
s in
to n
euro
mot
or te
sts
and
deve
lopm
enta
l tes
ts.
nificant beneficial effect of intervention on motor development. From the 14 studies with a limited
methodological quality, seven (50%) reported a positive effect of intervention.
Studies on the effect of intervention in children with or at risk for developmental disorders -
like the ones included in the present review - are often hampered by specific problems (Majnemer
1998, Siebes et al 2002). First, many studies include small study groups with a large heterogeneity
of degree and type of problems thereby diminishing generalizability and statistical power. Second,
assigning participants to a control group which does not receive treatment usually is considered
unethical. Therefore, the results of most intervention studies represent only the additional value
of the intervention under study. Another significant problem concerns the existing standard-
ized outcome measures. In general they are characterized by a lack of sensitivity to detect small
changes in motor development although these small changes may have an important influence
on the functional abilities of the child. The studies included in this review not only used a large
variation in outcome variables (see Table 3.7), but the measures were also mainly discriminative.
The use of discriminative measures, which focus on the comparison of a child’s score with an
age-equivalent score, may be one of the reasons that so little effect of EI is found. Another problem
associated with the used outcome measures is that they mainly measure quantitative changes in
motor development instead of qualitative ones and measures which focus on changes in func-
tional abilities (Ketelaar et al 1998).
Few studies addressed the effect of intervention on outcome beyond preschool age. This
means that we lack information on the effect of EI on the child’s activities of daily life and the
child’s socialization brought about by the potentially beneficial effect of EI on motor development.
Future studies should address the effect of EI on these outcome parameters, as they have a major
impact on the child’s participation in society.
The results of our review are discussed while taking age at the onset of intervention as a pri-
mary focus. The number of studies with a high methodological quality in the various age periods
after NICU discharge was so low that it precluded conclusions on the effect of age at onset of
intervention after term age. We therefore decided to discuss the results of our review in two sec-
tions, one for NICU studies and one for post-NICU studies.
NICU studies
Eight of the 17 NICU studies had a high methodological quality. Three of those evaluated the
effects of NIDCAP intervention. One demonstrated a significant positive effect on motor develop-
ment as measured by the psychomotor index of the Bayley Scales of Infant Development (Bayley –
PDI; Als et al 1994), but the other two were unable to reveal such an effect on Bayley – PDI (Kleberg
et al 2002, Ariagno et al 1997). The difference in outcome between the three studies might be
attributed to the age at which outcome was assessed.
Outcome in the positive effect study of Als et al (1994) was evaluated at 9 months corrected
age, in the two ‘no effect’ studies at 12 and 24 months. Thus, it could be that NIDCAP has a tem-
porary beneficial effect on motor development of infants at high risk for developmental disorder.
58 59
This notion is in line with results of two recent meta-analyses which concluded that NIDCAP
has a temporary beneficial effect on cognitive and motor development (Jacobs et al 2002, Sym-
ington and Pinelli 2003). But it should be kept in mind that only the study of Westrup et al (2004)
assessed the effect of NIDCAP beyond the age of two years. The latter small study was unable to
demonstrate a significant positive effect of NIDCAP on developmental outcome at the age of 5½
years. Nevertheless, considering reports that NIDCAP intervention in low risk preterm infants
has a significant positive effect on electrophysiological and MRI correlates of brain development
at 42 weeks postmenstrual age (Buehler et al 1995, Als et al 2004), it is conceivable that NIDCAP
might affect complex motor behaviour and cognitive abilities at school age. It might be that this
putatively positive effect will be found in particular in low risk preterm infants and not in high
risk preterms.
Two other high quality studies used Kangaroo Care to improve motor outcome (Charpak et
al 2001, Tessier et al 2003). The application of Kangaroo Care had no effect on developmental
outcome as measured by the Griffiths Developmental Scales at 6 and 12 months corrected age. Two
explanations for this result can be offered. First, it could be that Kangaroo Care does not affect
motor development. It is likely that the effect of the relatively simple Kangaroo Care is weaker
than that of the rather complex NIDCAP programme. Second, it is possible that the effects are too
subtle to be caught by the Griffiths scales.
Two high quality studies applied intervention strategies consisting of procedures to reduce
stress in combination with specific multimodal sensory stimulation with or without passive mo-
tor intervention procedures (Darrah et al 1994, Nelson et al 2001). Both studies were unable to find
a positive effect of intervention on motor development at 12 and 18 months corrected age.
The last high quality NICU study showed that developmental intervention had a significant
positive effect on motor development (Resnick et al 1987, 1988). In this programme intervention
started in the hospital with vestibular and visual stimulation to promote development. After dis-
charge, intervention was continued for two years by means of a developmental programme in the
home situation. The parents played an important role in carrying out the intervention programme
which consisted of 400 different motor, social and cognitive activities complemented by several
parenting activities. The positive outcome of the intervention probably can be attributed more to
the duration of the programme and the continuous involvement of the parents in the development
of their children than by the NICU part of the intervention.
In conclusion, the current review provides little evidence that intervention during the NICU
period in infants at high risk for developmental disorders has a beneficial effect on motor develop-
ment. Yet, a potential advantageous effect of NIDCAP on motor development cannot be excluded.
We recommend that further studies address the effect of NIDCAP on developmental outcome at
school age in low risk and high risk preterm infants.
Post NICU studies
From the 17 studies which started after the NICU period, 12 had a high methodological qual-
ity. Only four of those were able to show a beneficial effect of intervention on motor develop-
ment. Eight of the 12 studies evaluated the effects of NDT or physiotherapy mainly based on the
principles of NDT. It is striking that only one of these studies reported a better motor outcome in
the experimental group than in the control group (Mayo 1991). The positive effect study of Mayo
differed from the other studies, by being the only study which compared intensive NDT treatment
(once a week) to less intensive NDT (once a month). The other eight studies compared NDT to in-
fant stimulation (Palmer et al 1988, 1990) or to a not further defined form of standard care. In six
of the seven studies motor outcome in the NDT group was similar to that of the contrast group.
In the seventh study motor development was worse in children treated according to the principles
of NDT than in children who received an infant stimulation programme (Palmer et al 1988, 1990).
The above studies indicate that NDT during the first years of life does not have a measurable
positive effect on motor development. This is in line with the conclusion of a recent review on the
effects of NDT for people with cerebral palsy, aged 5 months to 22 years, that NDT did not have a
clear beneficial effect on developmental outcome (Butler and Darrah 2001).
The other four high quality studies evaluated the effects of a developmental programme, treadmill
training or conductive education. The two developmental programme studies (Barrera et al 1986,
Leksculchai and Cole 2001) and the treadmill training study (Ulrich et al 2001) reported a positive
effect of intervention on motor development. The fourth study compared the effect of conductive
education with that of traditional neurodevelopmental programmes. Both types of intervention
were associated with similar degrees of developmental progress (Reddihough et al 1998).
Treatment according to Vojta was only evaluated in two studies. D’Avignon and colleagues
(1981) compared in a small randomised trial with a limited methodological quality the effect of
treatment according to Vojta with NDT. They reported that the groups did not differ significantly
in developmental outcome. Kanda et al (2004), who studied the effect of the amount of Vojta
treatment on developmental outcome, reported a better outcome for the group which received suf-
ficient Vojta training compared to the group which had had insufficient Vojta therapy. However, a
major drawback of the study is that the design suffered from self-selection of the groups.
In conclusion, the current review indicates that intervention programmes in the first post-
natal years according to the principles of NDT or Vojta do not have a beneficial effect on motor
development in children at high risk for developmental disorders or children with CP or Down
syndrome. However, substantial evidence has been provided that specific developmental training
and general developmental programmes in which parents learn how to promote infant develop-
ment can exert a positive effect on motor development.

60 61
Concluding remarks
The present review indicates that intervention in children at risk of developmental disabilities
should be adapted to the infant’s age, i.e. the type of intervention which might be beneficial for
infants at preterm age differs from the type which is effective in infants who have reached at least
term age.
At preterm age infants seem to benefit most from intervention which aims at mimicking the
intrauterine environment, such as the NIDCAP intervention. Some evidence has been provided
that NIDCAP might have a temporary beneficial effect on infant motor (and cognitive) devel-
opment. Future studies should address the question whether NIDCAP affects developmental
outcome at school age.
The studies conducted after term indicated that intervention programmes according to the
principles of NDT or Vojta, i.e., programmes in which passive handling techniques play a promi-
nent role, do not have a clear beneficial effect on motor development. But intervention by means of
specific motor training programmes, such as training of locomotor movements on a treadmill and
general developmental programmes, where intervention aims at stimulation of the child’s explora-
tion of active motor behaviour, can exert a positive effect on motor development. Too few of these
training and developmental programme studies were available to answer the question whether
the age at which intervention starts matters, leaving this question for future research.
acknowledgements
We gratefully acknowledge the critical comments of Prof. Dr. B.F. van der Meulen, Drs. V.B.
de Graaf-Peters, Ms. T. Dirks on a previous version of the manuscript. CHB-H was financially
supported by the Johanna KinderFonds, Stichting Fonds de Gavere and the Graduate School for
Behavioural and Cognitive Neurosciences (BCN).
references
Als H, Duffy FH, McAnulty GB, Rivkin MJ, Vajapeyam S, Mulkern RV, Warfield SK, Huppi PS, Butler SC, Conneman N, Fischer C, Eichenwald EC. Early experi-ence alters brain function and structure. Pediatrics 2004;113:846-857.
Als H, Lawhon G, Duffy FH, McAnulty GB, Gibes-Grossman R, Blickman JG. Individualized Develop-mental Care for the very low-birth-weight preterm infant. Medical and neurofunctional effects. JAMA 1994;272:853-858.
Als H, Lawhon G, Brown E, Gibes R, Duffy FH, McAnulty G, Blickman JG. Individualized behavioural and environmental care for the very low birth weight preterm infant at high risk for bronchopulmonary dys-plasia: Neonatal Intensive Care Unit and Developmen-tal Outcome. Pediatrics 1986;78:1123-1132.
Anderson JW, Johnstone BM, Remley DT. Breast-feed-ing and cognitive development: a meta-analysis. Am J Clin Nutr 1999;70:525-535.
Ariagno RL, Thoman EB, Boeddiker MA, Kugener B, Constantinou JC, Mirmiran M, Baldwin RB. Develop-mental care does not alter sleep and development of premature infants. Pediatrics 1997;100:E9.
d’Avignon M, Norén L, Ǻrman T. Early physiotherapy ad modum Vojta or Bobath in infants with suspected neuromotor disturbance. Neuropediatrics 1981;12:232-241.
Barrera ME, Cunningham CE, Rosenbaum PL. Low birth weight and home intervention strategies: pre-term infants. Dev Behav Pediatr 1986;7:361-366.
Becker PT, Grunwald PC, Brazy JE. Motor organiza-tion in very low birth weight infants during caregiv-ing: effects of a developmental intervention. J Dev Behav Pediatr 1999;20:344-354.
Buehler DM, Als H, Duffy FH, McAnulty GB, Lieder-man J. Effectiveness of individualized developmental care for low-risk preterm infants: behavioral and elec-trophysiologic evidence. Pediatrics 1995;96:923-932.
Butler C, Darrah J. Effects of neurodevelopmental treatment (NDT) for cerebral palsy : an AACPDM evi-dence report. Dev Med Child Neurol 2001;43:778-790.
Casto G, Mastropieri MA. The efficacy of early intervention programs: a meta-analysis. Except Child 1986;52:417-424.
Charpak N, Ruiz-Peláez JG, Figueroa de C. Z, Charpak Y. A randomized, controlled trial of Kangaroo Mother Care: Results of follow-up at 1 year of corrected age. Pediatrics 2001;108:1072-1079.
Darrah J, Piper M, Byrne P, Watt MJ. The use of waterbeds for very low-birthweight infants: effects on neuromotor development. Dev Med Child Neurol 1994;36:989-999.
Eickmann SH, Lima ACV, Guerra MQ, Lima MC, Lira PIC, Huttly SRA, Ashworth A. Improved cognitive and motor development in a community-based interven-tion of psychosocial stimulation in northeast Brazil. Dev Med Child Neurol 2003;45:536-541.
Feldman R, Eidelman AI, Sirota L, Weller A. Compari-son of Skin-to-skin (Kangaroo) and Tradional Care: Parenting outcomes and preterm infant development. Pediatrics 2002;110:16-26.
Goodman M, Rothberg AD, Houston-McMillan JE, Cooper PA, Cartwright JD, van der Velde MA. Effect of early neurodevelopmental therapy in normal and at-risk survivors of neonatal intensive care. Lancet 1985;14:1327-1330.
Guralnick MJ (editor). The effectiveness of early interven-tion. Baltimore: Paul H. Brookes Publishing Co; 1997.
Hadders-Algra M. Early brain damage and the development of motor behavior in children: clues for therapeutic intervention. Neural Plast 2001;8:31-49.
Harris SR. Effects of Neurodevelopmental Therapy on motor performance of infants with Down’s Syndrome. Dev Med Child Neurol 1981;23:477-483.
Harris SR. The effectiveness of early intervention for children with Cerebral Palsy and related motor disor-ders. In: Guralnick MJ, editor. The effectiveness of early intervention. Baltimore: Paul H. Brookes Publishing Co. 1997;327-347.
Helders PJM, Cats BP, Debast S. Effects of a tactile stimulation/range-finding programme on the develop-ment of VLBW-neonates during the first year of life. Child Care Health Dev 1989;15:369-379.
Jacobs SE, Sokol J, Ohlsson A. The Newborn Individu-alized Developmental Care and Assessment Program is not supported by meta-analyses of the data. J Pediatr 2002;140:699-706.
Kanda T, Pidcock FS, Hayakawa K, Yamori Y, Shikata Y. Motor outcome differences between two groups of children with spastic diplegia who received different
62 63
intensities of early onset physiotherapy followed for 5 years. Brain Dev 2004;26:118-126.
Ketelaar M, Vermeer A, Helders PJM. Functional motor abilities of children with cerebral palsy: a sys-tematic literature review of assessment measures. Clin Rehabil 1998;12:369-380.
Kleberg A, Westrup B, Stjernqvist K. Developmental outcome, child behaviour and mother-child interaction at 3 years of age following Newborn Individualized De-velopmental Care and Intervention Program (NIDCAP) intervention. Early Hum Dev 2000;60:123-135.
Kleberg A, Westrup B, Stjernqvist K, Lagercrantz H. Indications of improved cognitive development at one year of age among infants born very prematurely who received care based on the Newborn Individual-ized Developmental Care and Assessment Program (NIDCAP). Early Hum Dev 2002;68:83-91.
Kolb B, Brown R, Witt-Lajeunesse A and Gibb R. Neu-ral compensations after lesion of the cerebral cortex. Neural Plast 2001;8:1-16.
Korner AF, Schneider P, Forrest T. Effects of vestibu-lar-proprioceptive stimulation on the neurobehavioral development of preterm infants: a pilot study. Neuro-pediatrics 1983;14:170-175.
Lekskulchai R, Cole J. Effect of a developmental pro-gram on motor performance in infants born preterm. Aust J Physiother 2001;47:169-176.
Leib SA, Benfield DG, Guidubaldi J. Effects of early intervention and stimulation on the preterm infant. Pediatrics 1980;66:83-90.
Mahoney G. The effects of early motor intervention on children with Down Syndrome or Cerebral Palsy: A field-based study. J Dev Behav Pediatr 2001;22:153-162.
Majnemer A. Benefits of early intervention for chil-dren with developmental disabilities. Semin Pediatr Neurol 1998;5:62-69.
Mayo NE. The effect of physical therapy for children with motor delay and cerebral palsy. A randomized clinical trial. Am J Phys Med Rehabil 1991;70:258-267.
Mouradian LE, Als H. The influence of Neonatal Intensive Care Unit caregiving practices on motor functioning of preterm infants. Am J Occup Ther 1994;48:527-533.
Nelson MN, White-Traut RC, Vasan U, Silvestri J, Comiskey E, Meleedy-Rey P, Littau S, Gu G, Patel
M. One-year outcome of auditory-tactile-visual-vestibular intervention in the neonatal intensive care unit: effects of severe prematurity and central nervous system injury. J Child Neurol 2001;16:493-498.
Palmer FB, Shapiro BK, Wachtel RC, Allen MC, Hiller JE, Harryman SE, Mosher BS, Meinert CL, Capute AJ. The effects of physical therapy on cerebral palsy. A controlled trial in infants with spastic diplegia. N Eng J Med 1988;318:803-808.
Palmer FB, Shapiro BK, Allen MC, Mosher BS, Bilker SA, Harryman SE. Infant stimulation curriculum for infants with cerebral palsy: effects on infant tempera-ment, parent-infant interaction, and home environ-ment. Pediatrics 1990;85:411-415.
Parette HP, Hourcade JJ. A review of therapeutic in-tervention research on gross and fine motor progress in young children with cerebral palsy. Am J Occup Ther 1984;38:462-468.
Parry TS. The effectiveness of early intervention: a critical review. J Paediatr Child Health 1992;28:343-346.
Piper MC, Pless IB. Early intervention for infants with Down Syndrome: a controlled trial. Pediatrics 1980;65:463-468.
Piper MC, Kunos VI, Willis DM, Mazer BL, Ramsay M, Silver KM. Early physical therapy effects on the high-risk infant: a randomized controlled trial. Pediatrics 1986;78:216-224.
Reddihough DS, King J, Coleman G, Catanese T. Ef-ficacy of programmes based on Conductive Education for young children with cerebral palsy. Dev Med Child Neurol 1998;40:763-770.
Resnick MB, Eyler FD, Nelson RM, Eitzman DV, Bucciarelli RL. Developmental Intervention for low birth weight infants: Improved early developmental outcome. Pediatrics 1987;80:68-74.
Resnick MB, Armstrong S, Carter RL. Developmental Intervention Program for high-risk premature infants: effects on development and parent-infant interactions. J Dev Behav Pediatr 1988;9:73-78.
Rothberg AD, Goodman M, Jacklin LA, Cooper PA. Six-year follow-up of early physiotherapy intervention in very low birth weight infants. Pediatrics 1991;88:547-552.
Sackett DL. Rules of evidence and clinical recommen-dations on the use of antithrombotic agents. Chest 1989;95:2S-4S (supplement).
Scherzer AL, Mike V, Ilson J. Physical therapy as a determinant of change in the cerebral palsied infant. Pediatrics 1976;58:47-52.
Sharkey MA, Palitz ME, Reece LF, Rutherford BL, Akers JP, Alvin BL, Budenholzer BR. The effect of early referral and intervention on the developmentally disa-bled infant: evaluation at 18 months of age. J Am Board Fam Pract 1990;3:163-170.
Shonkoff JP, Hauser-Cram P. Early Intervention for disabled infants and their families: a quantitative analysis. Pediatrics 1987;80:650-658.
Shonkoff JP, Meisels SJ, editors. Handbook of early childhood intervention. Cambridge: Cambridge Univer-sity Press; 2000.
Siebes RC, Wijnroks L, Vermeer A. Qualitative analysis of therapeutic motor intervention programmes for children with cerebral palsy: an update. Dev Med Child Neurol 2002;44:593-603.
Simeonsson RJ, Cooper DH, Scheiner AP. A review and analysis of the effectiveness of early intervention programs. Pediatrics 1982;69:635-641.
Symington A, Pinelli J. Developmental care for promoting development and preventing morbid-ity in preterm infants. Cochrane Database Syst Rev. 2003;(4):CD001814.
Tessier R, Cristo MB, Velez S, Giron M, Nadeau L, Figueroa de Calume Z, Ruiz-Paláez JG, Charpak N. Kangaroo Mother Care : A method for protect-ing high-risk low-birth-weight and premature infants against developmental delay. Infant Beh Dev 2003;26:384-397.
Turnbull JD. Early intervention for children with or at risk of cerebral palsy. Am J Dis Child 1993;147:54-59.
Ulrich DA, Ulrich BD, Angulo-Kinzler RM, Yun J. Treadmill training of infants with Down syndrome: evidence based developmental outcomes. Pediatrics 2001;108:E84.
Weindling AM, Hallam P, Gregg J, Kenka H, Rosen-bloom L, Hutton JL. A randomized controlled trial of early physiotherapy for high-risk infants. Acta Paediatr 1996;85:1107-1111.
Westrup B, Bohm B, Lagercrantz H, Stjernqvist K. Preschool outcome in children born very prematurely and cared for according to the Newborn Individual-ized Developmental Care and Assessment Program (NIDCAP). Acta Paediatr 2004;93:498-507.

65
C H a P t E r 4
d oe s e A r ly
I n t e rV e n t Ion I n
I n fA n t s At h Ig h r I s k
f or A de V e l oPm e n tA l
mo tor dI s or de r
I m P ro V e mo tor
A n d c o g n I t I V e
de V e l oPm e n t ? ---------------------------------------------------------------------------------------------------
CH Blauw-Hospers, VB de Graaf-Peters, T Dirks, AF Bos, M Hadders-Algra
Neuroscience and Biobehavioral Reviews, 2007, 31(8); 1201-1212
66 67
abstract
Infants at high risk for developmental motor disorders are in general referred to early interven-
tion (EI) services. It is a matter of debate to which extent EI may facilitate outcome in various
developmental domains. We reviewed the effects of EI programmes aiming at promoting motor
and cognitive development. With respect to motor development the data indicated that EI prior to
term age probably is most effective when it aims at mimicking the intrauterine environment; after
term age general developmental programmes probably are most effective. Some evidence was pro-
vided that EI prior to term age has a beneficial effect on cognitive development regardless the type
of intervention which is applied. After term age only general developmental programmes seemed
to have an effect on cognitive development. The review concludes with preliminary data on the
effect a new intervention programme, COPCA, applied between 3 and 6 months corrected age on
developmental outcome till 18 months. The results indicated that COPCA was more beneficial for
the development of sitting behaviour and cognition than traditional paediatric physiotherapy.
Keywords
Early intervention, motor development, cognitive development, developmental disorder, infant,
COPCA
Introduction
Infants who are born with a low birth weight or preterm are at biological risk for developmental
disorders (Aylward et al 1989, Bhutta et al 2002). Therefore these infants often are called high
risk (HR) infants. In general HR infants have poorer cognitive, motor and behavioural outcomes
than infants born at term. The less advantageous outcome is not only present at school-age, but
persists into adolescence and adulthood (Bhutta et al 2002, Marlow 2004, Johnson et al 2005). The
developmental outcome of infants born prematurely is heterogeneous and can be partly associ-
ated with biological risk factors, such as gestational age, birth weight, brain damage acquired in
the pre- or perinatal period or subsequent illnesses. However, these factors account only for a
portion of the variance associated with long term outcomes. In part the outcome is also mediated
by environmental experience (Shonkoff and Meisels 2000, Vohr et al 2000, Aylward 2005, Johnson
et al 2005, Spittle et al 2005). The complex character of influences on development makes it almost
impossible to determine the relation between biological risk, environmental risk and neurodevel-
opmental outcome. Another factor which influences developmental outcome is the so-called plas-
ticity of the brain. Depending on the timing of the insult to the brain and the size and site of the
lesion functional recovery may occur. The brain is plastic in particular during the phase occurring
after the completion of neuronal migration, during which the processes of dendritic outgrowth
and synapse formation are highly active (Kolb et al 2001). The latter means that considerable
plasticity can be expected between 2-3 months before until about 12-15 months after term age (de
Graaf-Peters and Hadders-Algra 2006).
While major disorders such as mental retardation, epilepsy or cerebral palsy – which occur
in 6-25% of HR infants (Aylward 2005) – are often identified during infancy, the effects of minor
neurological dysfunction (MND) become more obvious with increasing age and are for instance
expressed in learning disorders, attention deficit hyperactivity disorder (ADHD), clumsiness or
other behavioural problems. MND occurs in as many as 50-70% of HR infants (Aylward 2005). Two
basic forms of MND have been distinguished, i.e. simple and complex MND (Hadders-Algra 2002).
Simple MND occurs relatively frequently and it is most probably caused by genetic predisposition
and stress during pre- or perinatal life. Simple MND might be considered to represent the less
optimal but still normal brain function. Complex MND is strongly related to perinatal adversities.
It might be considered as a borderline form of CP and shows a clear association with motor, cogni-
tive and behavioural problems (Hadders-Algra 2002, 2003).
The variety in developmental problems that may occur as a result of pre- and perinatal adver-
sities makes it difficult to recognize infants at high risk for both major and minor neurological
dysfunction at early age. The development of imaging techniques has improved the possibilities to
identify these infants at early age (Aylward 2005). However, these techniques are not always able
to visualize abnormalities in the brain (Hadders-Algra 2000b). Another instrument which might
assist the early identification of HR infants is the assessment of the quality of General Movements
(GMs) (Prechtl 2001, Hadders-Algra 2004). GMs are complex movement patterns involving head,
trunk, arms and legs. They are present from early foetal life and disappear around 3-4 months

68 69
post term when goal-directed motor behaviour emerges. The quality of GMs, which is primarily
determined by movement complexity and variation, reflects the integrity of the nervous system.
Various studies indicate that the presence of definitely abnormal GMs around 3 months post-term,
i.e. in the last phase of GM-development, is associated with a high risk for developmental motor
disorders, such as CP (Prechtl et al 1997, Prechtl 2001, Hadders-Algra 2004, Groen et al 2005).
The early detection of infants at high risk for developmental disorders offers the opportunity
for intervention at young age, i.e. during a phase in which the central nervous system is character-
ized by considerable plasticity. It is however still a matter of debate to what extent early interven-
tion (EI) may facilitate outcome in various developmental domains. Therefore the first aim of the
present paper is to review the effects of EI programmes which aim primarily at the improvement
of motor development on a) motor and b) cognitive outcome. The analyses were restricted to in-
terventions starting prior to 18 months corrected age. The third part of the paper summarizes the
first results of an ongoing EI-study in which the effect of a recently developed physiotherapeutic
intervention programme for infants with high risk for developmental disorders is compared to the
effect of EI based on the principles of NeuroDevelopmental Treatment (NDT).
Effects of EI on motor development of Hr infants
Recently we reviewed the literature on the effects of EI on motor development of HR infants
(Blauw-Hospers and Hadders-Algra 2005). We first will summarize the findings of this review.
This will be followed by a discussion and integration of additional studies which have subsequent-
ly been published. We started with a literature search which covered various databases, including
Medline, CINAHL, PsycINFO and PEDro, in the period 1966 – June 2004. Thirty four studies
were identified which fulfilled the following four criteria: a) subjects of study: infants with high
biological risk for or with developmental disabilities, b) aim of the intervention (mostly amongst
others): to improve motor development, c) onset of intervention in at least 50% of the participating
children: between birth and the (corrected) age of 18 months, d) journal in which the study was
published had an impact factor of > 0.3. Excluded were studies restricted to medical and orthopae-
dic interventions and studies in populations of healthy low-risk preterm infants or in populations
of socially disadvantaged children without specific biological risk for developmental disorders.
The data revealed that a large diversity of EI programmes is applied. Before term age New-
born Individualized Developmental Care and Assessment Program (NIDCAP; Als et al 1994) is
mostly used, after term age a whole range of specific and general developmental programmes are
applied, together with more traditional physiotherapeutic interventions such as NeuroDevelop-
mental Treatment (NDT; Bobath 1980, Howle 2002) and treatment according to Vojta (Vojta 1976).
Specific developmental programmes aim at the improvement of one aspect of motor development
for example walking skills, while general developmental programmes aim at improvement in all
developmental domains. Parents usually play an important role in the implementation of the
specific and general developmental programmes.
The methodological quality (MQ) of each study was analysed systematically by taking into ac-
count 1) the level of evidence (Sackett 1989), 2) internal and 3) external validity. It was encouraging
to note that 20 out of 34 studies had a high MQ, i.e. they had an evidence level I and a fair to high
internal and external validity. This indicates a considerable improvement in the quality of studies
evaluating the effect of early intervention (Siebes et al 2002). Previous studies indicated that with
an increase in the rigorousness of the studies the evidence for the effectiveness of EI decreases
(Parette and Hourcade 1984, Siebes et al 2002). For the studies included in the present review this
also held true. Of the 20 studies with a high methodological quality only six (30%) showed a sig-
nificant beneficial effect of intervention on motor development. From the 14 studies with a limited
methodological quality, seven (50%) reported a positive effect of intervention.
The review indicated that intervention which might be beneficial for infants at preterm age is
different from the type which is effective in infants who have reached at least term age. At preterm
age infants seem to benefit most from intervention which aims at mimicking the intrauterine
environment, such as NIDCAP intervention. After term age, intervention by means of specific or
general developmental programmes has a positive effect on motor development. No evidence was
found for a beneficial effect of traditional forms of paediatric physiotherapy like NDT and Vojta.
An additional literature search was performed to cover the period July 2004 – September
2006. The results of this search are shown in Table 4.1. Another five studies were identified which
fulfilled the four aforementioned selection criteria. In two studies the onset of intervention was
during the period of stay at the Neonatal Intensive Care Unit (NICU; Oghi et al 2004, Cameron
et al 2005). Both studies had a fair methodological quality (MQ), consisting of a combination of
level I evidence (Sackett 1989), a fair internal validity, and a limited external validity. The stud-
ies applied different intervention techniques in different groups of children and were unable to
demonstrate a beneficial effect of intervention on motor development. The other three studies
started between discharge from the NICU and the age of 9 months (Koldewijn et al 2005, Badr et
al 2006, Gianni et al 2006). Gianni et al (2006) evaluated the effects of a mother-child intervention.
The study had a fair methodological quality and was unable to demonstrate a beneficial effect of
intervention on motor development. The other studies had a lower MQ. Badr et al (2006) studied
the effects of a cognitive/sensorimotor stimulation programme on motor development, but was not
able to demonstrate an effect of the intervention. The study of Koldewijn et al (2005) reported the
results of a pilot study on the Infant Behavioral Assessment and Intervention Program (IBAIP). They
demonstrated that at both 3 and 6 months motor development improved significantly compared to
the control group. But due to the fact that they had used a historical control group the methodologi-
cal quality of this study was limited (evidence level III, fair internal but low external validity).
We conclude that the five recent studies on the effect of early intervention in infants at high
risk for developmental motor disorders do not alter the conclusions of the original review (Blauw-
Hospers and Hadders-Algra 2005): intervention prior to term age probably is most effective when
it aims at mimicking the intrauterine environment; intervention after term age probably is most
effective when it consists of stimulation of motor development by means of the promotion of self-
produced motor behaviour.

70 71
tabl
e 4.
1. C
hara
cter
isti
cs o
f add
itio
nal
stu
dies
(Jul
y 20
04-S
epte
mbe
r 20
06) o
n th
e eff
ect o
f EI o
n m
otor
dev
elop
men
t.
Stud
y ch
arac
teri
stic
s
Stud
y N
EC
Attr
itio
n(%
)St
udy
grou
p Ev
iden
cele
vel
Inte
rnal
valid
ity
Exte
rnal
valid
ity
NIC
UO
hgi e
t al.
2004
2412
12
4H
R w
ith
CN
S in
jury
I+
-C
amer
on e
t al.
2005
7234
3817
HR
I++
+
aft
er N
ICU
– 9
mo
Kol
dew
ijn e
t al.
2005
4424
2011
HR
III
(his
tori
cal
cont
rol)
+-
Gia
nn
i et a
l. 20
0636
1818
0H
RI
+++
Bad
r et
al.
2006
6232
3031
HR
wit
h C
NS
inju
ryI
+-
Pro
gram
me
char
acte
rist
ics
Stud
yM
etho
dD
escr
.Ap
plic
atio
n pe
riod
Inte
nsit
yLo
cati
onPa
rent
s
NIC
UO
hgi e
t al.
2004
EIP
++pr
ior
to d
isch
arge
-6
mo
prio
r to
dis
char
ge:
3-4x
30
min
.A
fter
: 1x
wk/
2w
k 40
-60
min
Hos
pita
l/C
ente
rP
Cam
eron
et a
l. 20
05N
eon
atal
Dev
pg
m, l
arge
ly
base
d on
ND
T
++bi
rth
- 4 m
o - h
ospi
tal d
aily
- dep
endi
ng o
n ri
sk m
ax
1x 2
wk
Hos
pita
l /
Hom
eP
aft
er N
ICU
– 9
mo
Kol
dew
ijn e
t al.
2005
IBA
IP++
1 wk
afte
r di
scha
rge
- 6 m
o3x
eva
luat
ion,
6-8
hom
e in
terv
enti
ons
Hom
eP
Gia
nn
i et a
l. 20
06M
othe
r-ch
ild
inte
rven
tion
+3
mo
- 12
mo
2x p
er m
onth
, 1.5
hC
ente
rP
Bad
r et
al.
2006
Cog
nit
ive-
sen
sori
mot
or
stim
ulat
ion
prog
ram
+di
scha
rge
- 12
mo
1 mo:
2x
wk,
til
l 4 m
o:
1x w
k,th
erea
fter
1x
2wk
Hom
eP
C =
Con
trol
gro
up, C
NS
= C
entr
al N
ervo
us S
yste
m, E
= E
xper
imen
tal g
roup
, EIP
= E
arly
Inte
rven
tion
Pro
gram
, h =
hou
r, H
R =
Hig
h ri
sk,
IBA
IP =
Infa
nt B
ehav
iora
l Ass
essm
ent a
nd In
terv
enti
on P
rogr
am, m
in =
min
utes
, mo
= m
onth
s (c
orre
cted
age
), n
= nu
mbe
r, N
DT
= N
euro
de-
velo
pmen
tal T
reat
men
t, N
eon
atal
Dev
pgm
= N
eon
atal
Dev
elop
men
tal p
rogr
am, P
= p
aren
ts, P
= en
hanc
e pa
rent
al s
kills
, T =
par
ents
are
‘th
erap
ist’,
wk
= w
eeks
, ? =
no
info
rmat
ion
avai
labl
eO
utco
me
mea
sure
s: A
IMS
= A
lber
ta In
fant
Mot
or S
cale
, Gri
ffith
= G
riffi
ths
Dev
elop
men
tal S
cale
s, IB
A =
,MD
I = B
ayle
y Sc
ales
of I
nfa
nt D
e-ve
lopm
ent –
Men
tal D
evel
opm
ent I
ndex
, NB
AS
= N
eon
atal
Beh
avio
ral A
sses
smen
t Sco
re B
ayle
y, B
ayle
y PD
I = B
ayle
y Sc
ales
of I
nfa
nt D
evel
op-
men
t – P
sych
omot
or D
evel
opm
ent I
ndex
, 1 St
atis
tica
lly s
ign
ifica
nt d
iffer
ence
s fo
und
in m
otor
out
com
e at
old
est a
ge o
f eva
luat
ion:
E >
C:
Exp
erim
enta
l gro
up s
ign
ifica
ntly
bet
ter
out-
com
e th
an C
ontr
ol G
roup
, E =
C: n
o di
ffer
ence
bet
wee
n gr
oups
, E <
C:
Con
trol
Gro
up b
ette
r ou
tcom
e th
an E
xper
imen
tal G
roup
.
The
tab
le s
how
s th
e ch
arac
teri
stic
s of
stu
dies
on
earl
y in
terv
enti
on fo
cusi
ng o
n m
otor
dev
elop
men
t pub
lishe
d be
twee
n Ju
ly
2004
and
Oct
ober
200
6. In
the
tab
le ‘s
tudy
cha
ract
eris
tics
’ the
sam
ple
size
, stu
dy g
roup
and
cri
teri
a fo
r th
e m
etho
dolo
gica
l qu
alit
y ar
e pr
esen
ted.
The
sec
ond
part
‘pro
gram
me
char
acte
rist
ics’
desc
ribe
s th
e m
etho
ds o
f int
erve
ntio
n to
geth
er w
ith
the
dura
tion
and
inte
nsi
ty o
f tre
atm
ent,
the
loca
tion
whe
re t
he t
reat
men
t was
app
lied
and
the
role
of t
he p
aren
ts in
the
inte
rven
-ti
on p
rogr
amm
e. In
the
thi
rd p
art t
he a
ges
at w
hich
dev
elop
men
tal o
utco
me
is e
valu
ated
, the
out
com
e m
easu
res
to d
eter
min
e pr
ogre
ss in
mot
or d
evel
opm
ent a
nd th
e ov
eral
l res
ults
of t
he E
I pro
gram
mes
are
sho
wn
(for d
etai
led
desc
ript
ion
see
Tabl
e 3.
3-3.
5,
Cha
pter
3, p
age
46-5
3.
Eval
uati
on m
omen
ts, o
utco
me
mea
sure
s an
d re
sult
s
Stud
yAg
es o
f eva
luat
ion
Out
com
e m
easu
res
Res
ults
1
<Ter
mTe
rm1-
9 m
o9-
18m
o>1
8 m
o N
euro
mot
orD
evel
opm
enta
l
NIC
UO
hgi e
t al.
2004
1x1,
6N
BA
S, B
ayle
y PD
IB
ayle
y M
DI
E=C
Cam
eron
et a
l. 20
054
AIM
SE
=C
aft
er N
ICU
– 9
mo
Kol
dew
ijn e
t al.
2005
1x3,
6N
BA
S, B
ayle
y PD
I, IB
AB
ayle
y M
DI
E>C
Gia
nn
i et a
l. 20
0612
24,3
6G
riffi
thE
=CB
adr
et a
l. 20
066
12, 1
8B
ayle
y PD
IB
ayle
y M
DI
E=C

72 73
Do EI programmes which focus on motor development affect cognitive outcome?
It is generally acknowledged that HR infants, as a group, have lower cognitive scores than typically
developing infants and that their cognitive abilities may deteriorate over time (Vohr and Garcia
Coll 1985, Aylward 1989, Bhutta et al 2002, Ment et al 2003). Therefore early intervention pro-
grammes often do not only aim at the improvement of motor outcome but also at the facilitation
of cognitive development.
Over the years the effects of various general developmental intervention programmes aiming
at the improvement of cognitive development have been studied extensively for both environmen-
tally and biologically disadvantaged infants. Studies on early intervention by means of general
developmental programmes in children who are environmentally disadvantaged indicate both a
short and long term beneficial effect on cognitive development (Ramey and Campbell 1984, Wasik
et al 1990, Campbell and Ramey 1994). The programmes designed for infants at biological risk
for developmental disorders show less consistent effects of EI by means of general developmental
programmes on cognitive development. For instance, the Vermont Intervention Program found
both short and long term effects on cognitive function (Rauh et al 1988, Achenbach et al 1990,
Achenbach et al 1993). Studies on the Infant Health and Development Program (IHDP) however
indicated that immediately after the intervention at the age of three years a positive effect on
cognitive development was present (Infant Health and Development Program 1990), but that
the effect disappeared in the follow up at 5 and 18 years for the group with the higher biological
risk status, i.e. the infants with a gestational age at birth of less than 37 weeks and a birth weight
of less than 2000 grams (Brooks-Gunn et al 1994, McCormick et al 2006). In the children with
the lower biological risk, i.e. who had a birth weight between 2001 and 2499 grams, the effect
of intervention was still visible at the age of 18 years. The findings of the IHDP programme are
consistent with the results of a more recent study on a general developmental programme, the
Avon Premature Infant Project, which showed that the beneficial effect of the intervention which
was observed at two years (Avon Premature Infant Project 1998) had disappeared when the study
group was re-examined at five years of age (Johnson et al 2005). Thus general developmental pro-
grammes aiming at the improvement of cognitive development are indeed successful.
We wondered whether EI programmes focussing primarily on motor development have a
similar effect on cognitive outcome. The hypothesis underlying this assumption is that improve-
ment of early motor development allows the infant more opportunities to interact with the
environment, which in turn may facilitate cognitive development (Becker 1999). To this end we re-
examined whether the EI programmes which primarily aimed to improve motor development and
were included in the review described in the previous section also evaluated cognitive outcome.
To ensure the completeness of our study we carried out an additional literature search covering
different databases including MEDLINE (1966 to November 2006), CINAHL (1982 to November
2006), AMED (1985 to November 2006), PsycINFO (1967 to November 2006) and PEDro. The
keyword ‘early intervention’ was searched in combination with one of the following keywords:
‘infant’, ‘motor development’, ‘cognitive development’, ‘low birth weight’, ‘preterm’, ‘high-risk’,
‘developmental disabilities’ and ‘cerebral palsy’. We used the same inclusion and exclusion criteria
as in the review on motor development, be it that in the current review both motor and cognitive
outcome measures had to be included. The search did not yield other studies than those already
identified for the previous review. Twenty six studies of the previous 34 studies included in the
review also had a cognitive outcome measure. The results of the effect of EI on cognitive develop-
ment are summarized in Table 4.2.
In 13 of the 26 identified studies intervention had started in the NICU period, in eight studies
intervention was initiated in the period between discharge from the NICU and the corrected age
of 9 months and in three studies intervention started between 9 and 18 months. In two other
studies the preset age criteria were not fulfilled i.e. they started at some age between discharge
from the NICU and 18 months. All studies were reviewed on methodological quality (MQ). A fair
MQ was present in sixteen studies. They all evaluated cognitive outcome with either the men-
tal scale of the Bayley Scales of Infant Development (BSID) or with the Griffiths Developmental
Scales.
Seven studies with a fair MQ evaluated outcome of intervention which had started during the
NICU period. Five out of these seven studies reported a beneficial effect of intervention on cogni-
tive development (Resnick et al 1987, 1988, Als et al 1994, Nelson et al 2001, Kleberg et al 2002,
Tessier et al 2003). Interestingly the five studies evaluated four different types of early interven-
tion programmes: Developmental Program including stimulation, NIDCAP, Auditory-Tactile-
Visual-Vestibular Stimulation, and Kangaroo Care. The other six studies had a lower MQ. Three
suggested a positive effect on cognitive development (Leib et al 1980, Als et al 1986, Feldman et al
2002). Six of the eight studies that started after discharge from the NICU but before the corrected
age of nine months had a fair MQ. Two demonstrated that EI had a beneficial effect on cognitive
outcome (Barrera et al 1986, Gianni et al 2006). Both studies evaluated the effects of a general
developmental programme. The other four studies with fair MQ which did not find a positive
effect of EI on cognitive development all addressed the effects of NeuroDevelopmental Treatment
(Goodman et al 1985, Piper et al 1986, Rothberg et al 1991, Weindling et al 1996).

74 75
StudyEvidence Level1
Internal validity2
External validity3
Results
motor4
Results cognitive4
NICUAls et al. 1994 I ++ ++ E > C E > CResnick et al. 1987/1988 I + + E > C E > CAriagno et al. 1997 I + + E = C E = CCharpak et al. 2001 I + + E = C E = CNelson et al. 2001 I + + E = C E > CKleberg et al. 2002 I + + E = C E > CTessier et al. 2003 I + + E = C E > CWestrup et al. 2004 I + - E = C E = COhgi et al 2004 I + - E = C E = CFeldman et al. 2002 II - - E > C E > CAls et al. 1986 III + - E > C E > CLeib et al. 1980 III - - E > C E > CKleberg et al. 2000 III - - E = C E = C
after NICU – 9 moGoodman et al. 1985 I ++ ++ E = C E = CPiper et al. 1986 I ++ ++ E = C E = CBarrera et al. 1986 I ++ + E > C E > CWeindling et al. 1996 I ++ + E = C E = CRothberg et al. 1991 I + + E = C E = CGianni et al. 2006 I ++ + E = C E > CBadr et al. 2006 I + - E = C E = CKoldewijn et al. 2005 III + - E > C E > C
9 mo – 18 moPalmer et al. 1988/1990 I ++ ++ E < C E = CEickmann et al. 2003 II + + E > C E > CPiper and Pless 1980 III + - E = C E = C
after NICU – 18 moMayo 1991 I ++ + E > C E > CHarris 1981 I + + E = C E = C
table 4.2. Effect of early intervention on cognitive development.
Only one of the three studies in which intervention started between 9 and 18 months had a fair
MQ (Palmer et al 1988, 1990). This study demonstrated a beneficial effect of an infant stimulation
programme on motor development, but the programme did not affect cognitive outcome. Both
studies in which intervention started between discharge from the NICU and 18 months had a fair
MQ. The study of Mayo (1991) on the effect of NDT demonstrated a significant improvement in
cognitive function for the group which received the intensive treatment approach. The study of
Harris (1981) addressed the effect of NDT in children with Down syndrome; it failed to demon-
strate a positive effect on cognitive development.
In conclusion, the review provides some evidence that intervention during the NICU period
in infants at high risk for developmental motor disorders has a beneficial effect on cognitive devel-
opment. Interestingly, the effect seems to be independent of the type of intervention. The studies
in which intervention had started after term age indicated that intervention by means of a general
developmental programme might be beneficial for cognitive development. This finding is consist-
ent with the results of studies on the effect of EI in infants with high biological risk for develop-
mental disorders which primarily aim at improving cognitive outcome. Our review indicated that
NDT applied during infancy does not produce benefits in the cognitive domain – a finding in line
with an earlier review of Butler and Darrah (2001).
the early intervention project in Groningen (VIP project)
The review above indicates that convincing evidence for a beneficial effect of physiotherapy
programmes most frequently used in early intervention (NDT and treatment according to Vojta)
is lacking. This inspired two members of the Groningen team (TD and MHA) to develop a new
physiotherapeutic EI programme: COPCA (Coping with and Caring for infants with neurological
dysfunction – a family centred programme). COPCA is based on the principles of the Neuronal
Group Selection Theory (NGST; Edelman 1993) and on new insights in the field of education and
family care (Dale 1996, Rosenbaum et al 1998). According to NGST typical development is charac-
terized by two phases of variability, i.e. primary and secondary variability. During primary vari-
Table lay-out is based on Blauw-Hospers and Hadders-Algra 2005.1 Evidence level according to Sackett’s method for grading research (Sackett 1989):
I = Randomised controlled trials; II = Non-randomised controlled trials / Prospective cohort studies with concurrent control group; III = Cohort studies with historical control group / Case studies with control participants
2 Internal validity is determined by various study variations such as subject assignment, study design, attri-tion, confounders, validity of outcome measures, blind assessment
3 External validity is determined by possibilities for generalization (group size and internal validity)4 Statistically significant differences found in motor outcome at oldest age of evaluation:
E > C: Experimental group significantly better outcome than control group E = C: No difference between groups E < C: Control group better outcome than experimental group

76 77
ability the nervous system explores all motor possibilities available. In typically developing infants
this phase is characterized by abundant variation. At function specific ages the infant reaches the
phase of secondary variability. The child gradually learns to select the most efficient solution for a
given task out of his motor repertoire. This selection is based on trial and error. This means that
during the phase of secondary variability the child learns to adapt his/her motor behaviour to
specific situations (Hadders-Algra 2000a). Infants with a brain lesion resulting in a developmental
motor disorder have a reduced repertoire of motor strategies available for exploration. In addition,
these infants have problems with the selection of the most appropriate solution for a certain task
out of the repertoire (Hadders-Algra 2000a). Therefore COPCA aims to promote variation in mo-
tor behaviour and trial-and-error experiences, with the ultimate goal that the child will be able to
find an appropriate solution for any motor task.
An equally important base of COPCA are new insights in the field of education and family
care (Dale 1996, Law et al 1998, Rosenbaum et al 1998). Family centred care implies a partnership
between the family and the professional, in which the family defines the priorities for interven-
tion, while the therapist assists the family throughout the intervention period (Law et al 1998). In
COPCA the physiotherapist (PT) acts as a coach who respects the autonomy of the family and in-
tends to make him- or herself superfluous. Caregivers are key-persons in the COPCA programme.
They determine the goals to be achieved. The PT provides information on infant development, the
specific problems of infants with neurological dysfunction, basic principles on infant education,
and specific ways in which development may be promoted and problems may be tackled. By means
of a continuous dialogue with the PT, caregivers thus develop their own ways to cope with their
infant.
In the so-called VIP project (VIP is the abbreviation of the Dutch term for Early Intervention
Project, namely Vroegtijdige Interventie Project) the effect of COPCA on developmental outcome
till the age of 18 months is currently studied. Here we will present preliminary data on the first
20 infants included in the project who have already reached the age of 18 months. The aim of the
study is to assess whether COPCA is more beneficial for developmental outcome at 18 months cor-
rected age than traditional paediatric physiotherapy (TPP), which in the Netherlands in general
consists of the implementation of the ‘living concept’ of NDT. The latter implies that TPP is
practised with significant heterogeneity.
The study groups of the VIP project consisted of infants who had been admitted to the NICU
of the University Medical Center Groningen (UMCG) between March 2003 and May 2005 and
showed at ten weeks corrected age definitely abnormal GMs. As indicated in the introduction the
presence of definitely abnormal GMs indicates a high risk for developmental motor disabilities,
such as cerebral palsy (CP) (Prechtl 2001, Hadders-Algra 2004). Infants with severe congenital
anomalies and infants whose parents had an inappropriate understanding of the Dutch language
were excluded from the study. All parents of the infants gave informed consent and the project
was approved by the Ethics Committee of the University Medical Center Groningen.
The infants were randomly assigned to the COPCA or the control group. The randomised
intervention period lasted from 3 to 6 months corrected age1. Thereafter the intervention followed
the suggestions of the paediatrician in charge of the care of the infant. COPCA intervention was
provided twice a week for one hour in the home environment by one of four specially trained
paediatric physiotherapists. The control group received TPP with a frequency varying from 2 to 20
times (median value: 7) during the intervention period. The duration of the TPP sessions varied
from 15 to 36 minutes (median value: 30); in general they were also applied in the home environ-
ment. During the study the assessors were blind regarding group allocation.
Of the first twenty infants enrolled in the VIP project nine had been assigned to COPCA in-
tervention and 11 to the control group. The latter got physiotherapeutic guidance indicated by the
paediatrician. It turned out that nine infants in the control group had received TPP and two got
no specific guidance. As the results of the two infants who did not receive TPP did not differ from
those who did, we decided to include these two infants without TPP in the control group. The
COPCA and control group were similar in terms of gender distribution, gestational age at birth
and birth weight (Table 4.3). All but two infants had been born preterm.
table 4.3. Clinical characteristics of the two study groups.
COPCa (n = 9) tPP (n = 11)
Gender 4 male
5 female
5 male
6 female
Preterm (GA<37 wk) n = 8 n = 10
Term n = 1 n = 1
Gestational age (wk) 27-37
(median 29)
27-39
(median 31)
Birth weight (g) 585-3640
(median 1160)
825-3460
(median 1340)
1 Throughout the rest of the document ages in months are ages corrected for preterm birth.
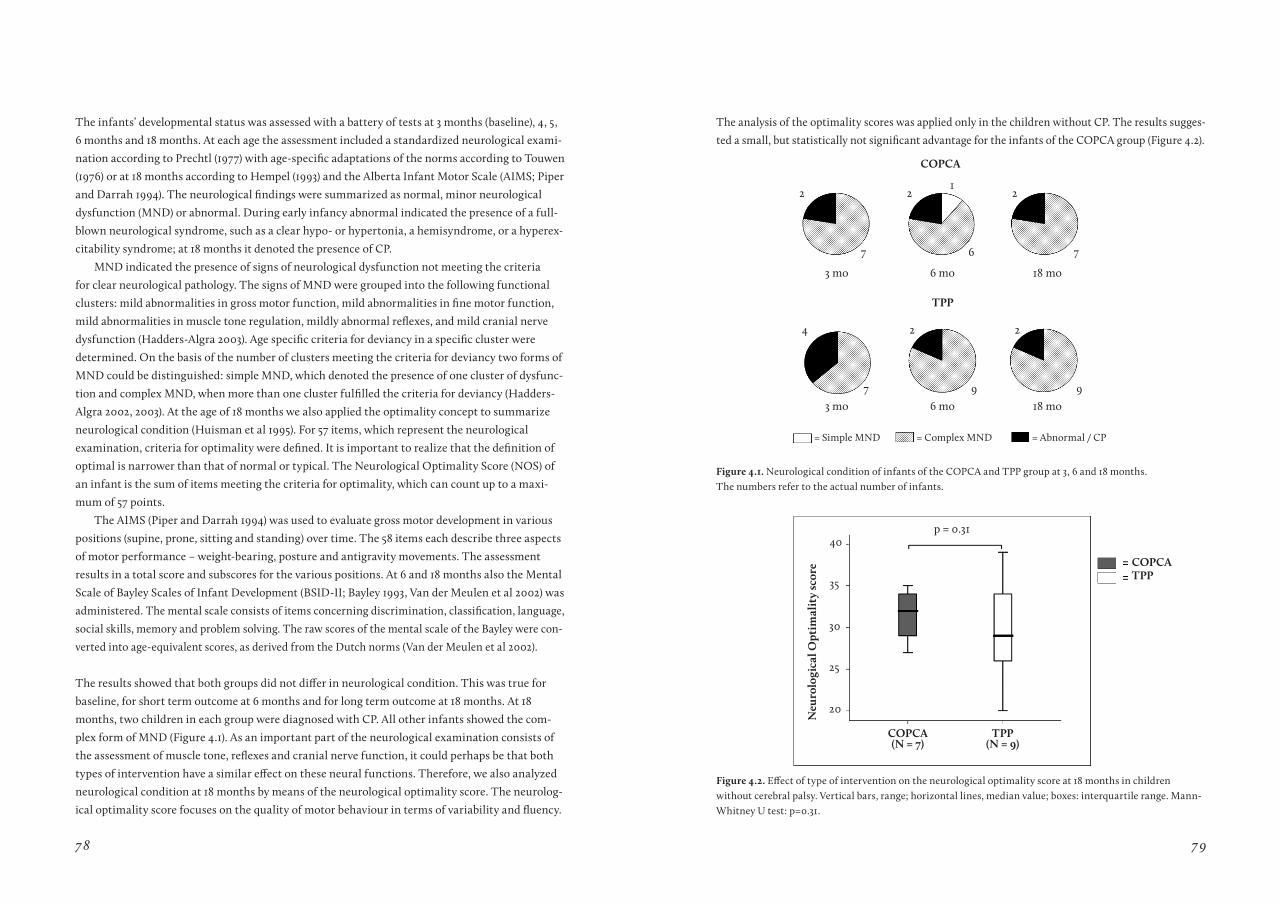
78 79
The infants’ developmental status was assessed with a battery of tests at 3 months (baseline), 4, 5,
6 months and 18 months. At each age the assessment included a standardized neurological exami-
nation according to Prechtl (1977) with age-specific adaptations of the norms according to Touwen
(1976) or at 18 months according to Hempel (1993) and the Alberta Infant Motor Scale (AIMS; Piper
and Darrah 1994). The neurological findings were summarized as normal, minor neurological
dysfunction (MND) or abnormal. During early infancy abnormal indicated the presence of a full-
blown neurological syndrome, such as a clear hypo- or hypertonia, a hemisyndrome, or a hyperex-
citability syndrome; at 18 months it denoted the presence of CP.
MND indicated the presence of signs of neurological dysfunction not meeting the criteria
for clear neurological pathology. The signs of MND were grouped into the following functional
clusters: mild abnormalities in gross motor function, mild abnormalities in fine motor function,
mild abnormalities in muscle tone regulation, mildly abnormal reflexes, and mild cranial nerve
dysfunction (Hadders-Algra 2003). Age specific criteria for deviancy in a specific cluster were
determined. On the basis of the number of clusters meeting the criteria for deviancy two forms of
MND could be distinguished: simple MND, which denoted the presence of one cluster of dysfunc-
tion and complex MND, when more than one cluster fulfilled the criteria for deviancy (Hadders-
Algra 2002, 2003). At the age of 18 months we also applied the optimality concept to summarize
neurological condition (Huisman et al 1995). For 57 items, which represent the neurological
examination, criteria for optimality were defined. It is important to realize that the definition of
optimal is narrower than that of normal or typical. The Neurological Optimality Score (NOS) of
an infant is the sum of items meeting the criteria for optimality, which can count up to a maxi-
mum of 57 points.
The AIMS (Piper and Darrah 1994) was used to evaluate gross motor development in various
positions (supine, prone, sitting and standing) over time. The 58 items each describe three aspects
of motor performance – weight-bearing, posture and antigravity movements. The assessment
results in a total score and subscores for the various positions. At 6 and 18 months also the Mental
Scale of Bayley Scales of Infant Development (BSID-II; Bayley 1993, Van der Meulen et al 2002) was
administered. The mental scale consists of items concerning discrimination, classification, language,
social skills, memory and problem solving. The raw scores of the mental scale of the Bayley were con-
verted into age-equivalent scores, as derived from the Dutch norms (Van der Meulen et al 2002).
The results showed that both groups did not differ in neurological condition. This was true for
baseline, for short term outcome at 6 months and for long term outcome at 18 months. At 18
months, two children in each group were diagnosed with CP. All other infants showed the com-
plex form of MND (Figure 4.1). As an important part of the neurological examination consists of
the assessment of muscle tone, reflexes and cranial nerve function, it could perhaps be that both
types of intervention have a similar effect on these neural functions. Therefore, we also analyzed
neurological condition at 18 months by means of the neurological optimality score. The neurolog-
ical optimality score focuses on the quality of motor behaviour in terms of variability and fluency.
The analysis of the optimality scores was applied only in the children without CP. The results sugges-
ted a small, but statistically not significant advantage for the infants of the COPCA group (Figure 4.2).
Figure 4.1. Neurological condition of infants of the COPCA and TPP group at 3, 6 and 18 months. The numbers refer to the actual number of infants.
2
4
2
2
2
2
1
7
3 mo
COPCa
tPP
3 mo
6 mo
6 mo
18 mo
18 mo7
6
9
7
9
= Simple MND = Complex MND = Abnormal / CP
Neu
rolo
gica
l Opt
imal
ity
scor
e
COPCa(N = 7)
COPCatPP
tPP(N = 9)
p = 0.3140
35
30
25
20
Figure 4.2. Effect of type of intervention on the neurological optimality score at 18 months in children without cerebral palsy. Vertical bars, range; horizontal lines, median value; boxes: interquartile range. Mann-Whitney U test: p=0.31.

80 81
tota
l aIM
S sc
ore
COPCatPP
21
18
15
12
6
61
91
9
3 4 6
Figure 4.3. Effect of type of intervention on the total AIMS score at 3, 4 and 6 months. Vertical bars, range; horizontal lines, median value; boxes: interquartile range.
The effect of intervention on the development of gross motor skills was analyzed with the AIMS.
The data revealed that at the age of 18 months the AIMS suffers from a ceiling effect (Darrah et al
1998, Liao and Campbell 2004). We therefore restricted our analyses to the data of 3 to 6 months.
The analyses were carried out twice, once for all infants and once without the children who devel-
oped CP. The rationale behind the second series of analyses was that it is conceivable that children
with mild to moderate dysfunction profit more from intervention than children with severe dys-
function. The analyses showed no differences in total AIMS scores between the COPCA and the
control group at baseline, during and immediately after the intervention period (Figure 4.3). Nei-
ther did the groups differ in scores on the subscales which assess motor behaviour in supine, prone
and standing position. On the sitting subscale however a significant positive effect of the COPCA
intervention was observed whether or not the infants who developed CP were included into the
analysis (p=0.03 with CP included and p=0.02 with CP excluded; Figure 4.4a, 4.4b). Furthermore,
the effect of COPCA intervention tended to increase with increasing age when children with CP
were left out of the analysis (p=0.08) (Figure 4.4b). The results suggest that the infants who re-
ceived COPCA intervention have a better postural control at 6 months than the infants of the TPP
group. These findings match with the results of de Graaf-Peters et al (2006), who demonstrated by
means of EMG recordings that the infants who received COPCA intervention showed at 6 months
a more typical pattern of postural control during sitting than the infants of the TPP group.
Figure 4.4 Effect of type of intervention on the sitting subscale of the AIMS at 3, 4, and 6 mo: a) with infants with CP included, b) with infants with CP excluded. Vertical bars, range; horizontal lines, median value; boxes: interquartile range. MANOVA: main effect of intervention * p=0.03, ** p=0.02. Intervention and age tended to interact (p=0.08).
Finally, the results showed that COPCA intervention might also have an effect on cognitive
development. At 6 months the MDI of both groups was identical. In the TPP group we found a
significant decrease in the median MDI score over time from 109 at 6 months to 99 at 18 months
(p=0.03). In general it is known that cognitive abilities of preterm infants deteriorate with increas-
ing age (Vohr and Garcia Coll 1985, Aylward 1989, Bhutta et al 2002, Ment et al 2003). In contrast
to the TPP group, the MDI score of the infants who had received COPCA intervention remained
stable over time (median values at 6 months 110, at 18 months 111; Figure 4.5). This indicates that
COPCA intervention might be able to counteract a cognitive deterioration.
Sitt
ing
subs
cale
Sitt
ing
subs
cale
COPCattP
a. B.
1
3
55 21
17
21
98 98
49 49
34 46 6
1
2 2
3 3
4 4
5 5

82 83
Concluding remarks
Prior to term age intervention which aims at mimicking the intrauterine environment is probably
most effect for motor development; for cognitive development any type of intervention seems to
be beneficial. After term age EI probably is most effective for motor and cognitive development
when a general developmental programme is applied. No evidence is available supporting the
notion that intervention according to the principles of NDT has a positive effect on motor or
cognitive development. The limited amount of evidence favouring EI encouraged two members
of the Groningen team (TD and MHA) to develop a new physiotherapeutic intervention, COPCA.
Preliminary results indicate that COPCA has a significant effect on the development of sitting
abilities and that COPCA might be able to counteract a cognitive deterioration. However, further
research is needed to explore clinical effectiveness of the COPCA programme.
acknowledgements
We kindly acknowledge the contribution of our collaborators Kune Blaauw PT, Lily van Doormaal
MD, Ellen Janssen PT, Peter Logtenberg PT and Wilma Renkema PT MSc. CHB-H was financially
supported by the Johanna KinderFonds, Stichting Fonds de Gavere, the Cornelia Stichting and the
Graduate School for Behavioural and Cognitive Neurosciences (BCN).
Figure 4.5 Bayley Scales of Infant Development: MDI scores at 6 and 18 months in COPCA and TPP group. Vertical bars, range; horizontal lines, median value; boxes: interquartile range. Wilcoxon: * p=0.03.
BSI
D-I
I MD
I
COPCatPP
60
80
100
120
140
6 mo 6 mo18 mo 18 mo
*
COPCa tPP
references
Achenbach TM, Phares V, Howell CT, Rauh VA, Nurcombe B. Seven-year outcome of the Vermont In-tervention Program for Low-Birthweight Infants. Child Dev 1990;61:1672-1681.
Achenbach TM, Howell CT, Aoki MF, Rauh VA. Nine-year outcome of the Vermont intervention program for low birth weight infants. Pediatrics 1993;91:45-55.
Als H, Lawhon G, Brown E, Gibes R, Duffy FH, McAnulty G, Blickman JG. Individualized behavioural and environmental care for the very low birth weight preterm infant at high risk for bronchopulmonary dysplasia: Neonatal Intensive Care Unit and Develop-mental Outcome. Pediatrics 1986;78:1123-1132.
Als H, Lawhon G, Duffy FH, McAnulty GB, Gibes-Grossman R, Blickman JG. Individualized Develop-mental Care for the very low-birth-weight preterm infant. Medical and neurofunctional effects. JAMA 1994;272:853-858.
Ariagno RL, Thoman EB, Boeddiker MA, Kugener B, Constantinou JC, Mirmiran M, Baldwin RB. Develop-mental care does not alter sleep and development of premature infants. Pediatrics 1997;100:E9.
Avon Premature Infant Project. Randomised trial of parental support for families with very preterm children. Avon Premature Infant Project. Arch Dis Child Fetal Neonatal Ed 1998;79:F4-11.
Aylward GP, Pfeiffer SI, Wright A, Verhulst SJ. Outcome studies of low birth weight infants published in the last decade: a meta-analysis. J Pediatr 1989;115:515-520.
Aylward GP. Neurodevelopmental outcomes of infants born prematurely. J Dev Behav Pediatr 2005;26:427-440.
Badr LK, Garg M, Kamath M. Intervention for infants with brain injury: results of a randomized controlled study. Infant Behav Dev 2006;29:80-90.
Barrera ME, Cunningham CE, Rosenbaum PL. Low birth weight and home intervention strategies: pre-term infants. Dev Behav Pediatr 1986;7:361-366.
Bayley N. Manual of the Bayley Scales of Infant Develop-ment (second edition). San Antonio, The psychological Corporation; 1993.
Becker PT, Grunwald PC, Brazy JE. Motor organiza-tion in very low birth weight infants during caregiving: effects of a developmental intervention. J Dev Behav Pediatr 1999;20:344-354.
Bhutta AT, Cleves MA, Casey PH. Cognitive and behav-ioral outcomes of school-aged children who were born preterm. JAMA 2002;288:728-737.
Blauw-Hospers CH, Hadders-Algra M. Fact or fiction: a systematic review on the effects of early interven-tion on motor development. Dev Med Child Neurol 2005;47:421-432.
Bobath K. A neurophysiological basis for the treatment of Cerebral Palsy. Clinics in Developmental Medicine no 75. London, The Lavenham Press LTD; 1980.
Brooks-Gunn J, McCarton CM, Casey PH, McCor-mick MC, Bauer CR, Bernbaum JC, Tyson J, Swanson M, Bennett FC, Scott DT, et al. Early intervention in low-birth-weight premature infants. Results through age 5 years from the Infant Health and Development Program. JAMA 1994;272:1257-1262.
Butler C, Darrah J. Effects of neurodevelopmental treatment (NDT) for cerebral palsy: an AACPDM evi-dence report. Dev Med Child Neurol 2001;43:778-790.
Cameron EC, Maehle V, Reid J. The effects of an early physical therapy intervention for very preterm, very low birth weight infants: a randomized controlled clinical trial. Pediatr Phys Ther 2005;17:107-119.
Campbell FA, Ramey CT. Effects of early intervention on intellectual and academic achievement: a follow-up study of children from low-income families. Child Dev 1994;65:684-698.
Charpak N, Ruiz-Peláez JG, Figueroa de Calume Z, Charpak Y. A randomized, controlled trial of Kangaroo Mother Care: Results of follow-up at 1 year of cor-rected age. Pediatrics 2001;108:1072-1079.
Dale N. Working with families of children with Special Needs. Routledge London; 1996.
Darrah J, Piper M, Watt MJ. Assessment of gross motor skills of at-risk infants: predictive validity of the Alberta Infant Motor Scale. Dev Med Child Neurol 1998;40:485-491.
De Graaf-Peters VB, Blauw-Hospers CH, Dirks T, Bakker J, Bos AF, Hadders-Algra M. Effect of early in-tervention on early postural development in infants at high risk for a motor developmental disorder. Neurosci Biobehav Rev, 2006 (accepted for publication).
De Graaf-Peters VB, Hadders-Algra M. Ontogeny of the human central nervous system: what is happening when? Early Hum Dev 2006;82:257-266.
84 85
Edelman GM. Neural Darwinism: Selection and reentrant signalling in higher brain function. Neuron 1993;10:115-125.
Eickmann SH, Lima ACV, Guerra MQ, Lima MC, Lira PIC, Huttly SRA, Ashworth A. Improved cognitive and motor development in a community-based interven-tion of psychosocial stimulation in northeast Brazil. Dev Med Child Neurol 2003;45:536-541.
Feldman R, Eidelman AI, Sirota L, Weller A. Compari-son of Skin-to-skin (Kangaroo) and Tradional Care: Parenting outcomes and preterm infant development. Pediatrics 2002;110:16-26.
Gianni ML, Picciolini O, Ravasi M, Gardon L, Vegni C, Fumagalli M, Mosca F. The effects of an early developmental mother-child intervention program on neurodevelopment outcome in very low birth weight infants: A pilot study. Early Hum Dev 2006;82:691-695.
Goodman M, Rothberg AD, Houston-McMillan JE, Cooper PA, Cartwright JD, van der Velde MA. Effect of early neurodevelopmental therapy in normal and at-risk survivors of neonatal intensive care. Lancet 1985;14:1327-1330.
Groen SE, de Blecourt AC, Postema K, Hadders-Algra M. General movements in early infancy predict neu-romotor development at 9 to 12 years of age. Dev Med Child Neurol 2005;47:731-738.
Hadders-Algra M. The Neuronal Group Selection Theory: an attractive framework to explain variation in normal motor development. Dev Med Child Neurol 2000a;42:566-572.
Hadders-Algra M. The neuronal group selection theory: promising principles for understanding and treating developmental motor disorders. Dev Med Child Neurol 2000b;42:707-715.
Hadders-Algra M. Two distinct forms of neurological dysfunction: perspectives emerging from a review of data of the Groningen Perinatal Project. Dev Med Child Neurol 2002;44:561–571.
Hadders-Algra M. Developmental coordination disor-der: is clumsy motor behaviour caused by a lesion of the brain at early age? Neural Plast 2003;10:39–50.
Hadders-Algra M. General movements: a window for early identification of children at high risk of develop-mental disorders. J Pediatr 2004;145:S12–S18.
Harris SR. Effects of Neurodevelopmental Therapy on motor performance of infants with Down’s Syndrome. Dev Med Child Neurol 1981;23:477-483.
Hempel MS. Neurological development during tod-dling age in normal children and children at risk of developmental disorders. Early Hum Dev 1993;34:47–57.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Prac-tice. Laguna Beach, CA 92651, Neuro-Developmental Treatment Association; 2002.
Huisman M, Koopman-Esseboom C, Lanting CI, Van der Paauw CG, Tuinstra LGMTh, Fidler V, Weisglas-Kuperus N, Sauer PJJ, Boersma ER, Touwen BCL. Neurological condition in 18-month-old children perinatally exposed to polychlorinated biphenyls and dioxins. Early Hum Dev 1995;43:165-176.
Infant Health and Development Program. Enhancing the outcomes of low-birth-weight, premature infants. A multisite, randomized trial. The Infant Health and Development Program. JAMA 1990;263:3035-3042.
Johnson S, Ring W, Anderson P, Marlow N. Ran-domised trial of parental support for families with very preterm children: outcome at 5 years. Arch Dis Child 2005;90:909-915.
Kleberg A, Westrup B, Stjernqvist K. Developmental outcome, child behaviour and mother-child interac-tion at 3 years of age following Newborn Individualized Developmental Care and Intervention Program (NID-CAP) intervention. Early Hum Dev 2000;60:123-135.
Kleberg A, Westrup B, Stjernqvist K, Lagercrantz H. Indications of improved cognitive development at one year of age among infants born very prematurely who received care based on the Newborn Individualized De-velopmental Care and Assessment Program (NIDCAP). Early Hum Dev 2002;68:83-91.
Kolb B, Brown R, Witt-Lajeunesse A, Gibb R. Neural compensations after lesion of the cerebral cortex. Neural Plast 2001;8:1-16.
Koldewijn K, Wolf MJ, van Wassenaer A, Beelen A, de Groot IJ, Hedlund R. The Infant Behavioral Assessment and Intervention Program to support preterm infants after hospital discharge: a pilot study. Dev Med Child Neurol 2005;47:105-112.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Occup Ther Pediatr 1998;18:83-102.
Leib SA, Benfield DG, Guidubaldi J. Effects of early intervention and stimulation on the preterm infant. Pediatrics 1980;66:83-90.
Liao PM, Campbell SK. Examination of the item struc-ture of the Alberta Infant Motor Scale. Pediatr Phys Ther 2004;16:31-38.
Marlow N. Neurocognitive outcome after very preterm birth. Arch Dis Child Fetal Neonatal Ed 2004;89:F224-228.
Mayo NE. The effect of physical therapy for children with motor delay and cerebral palsy. A randomized clinical trial. Am J Phys Med Rehabil 1991;70:258-267.
McCormick MC, Brooks-Gunn J, Buka SL, Goldman J, Yu J, Salganik M, Scott DT, Bennett FC, Kay LL, Bernbaum JC, Bauer CR, Martin C, Woods ER, Martin A, Casey PH. Early intervention in low birth weight premature infants: results at 18 years of age for the Infant Health and Development Program. Pediatrics 2006;117:771-780.
Ment LR, Vohr B, Allan W, Katz KH, Schneider KC, Westerveld M, Duncan CC, Makuch RW. Change in cognitive function over time in very low-birth-weight infants. JAMA 2003;289:705-711.
Nelson MN, White-Traut RC, Vasan U, Silvestri J, Comiskey E, Meleedy-Rey P, Littau S, Gu G, Patel M. One-year outcome of auditory-tactile-visual-vestibular intervention in the neonatal intensive care unit: effects of severe prematurity and central nervous system injury. J Child Neurol 2001;16:493-498.
Ohgi S, Fukuda M, Akiyama T, Gima H. Effect of an early intervention programme on low birthweight infants with cerebral injuries. J Paediatr Child Health 2004;40:689-695.
Palmer FB, Shapiro BK, Wachtel RC, Allen MC, Hiller JE, Harryman SE, Mosher BS, Meinert CL, Capute AJ. The effects of physical therapy on cerebral palsy. A controlled trial in infants with spastic diplegia. N Eng J Med 1988;318:803-808.
Palmer FB, Shapiro BK, Allen MC, Mosher BS, Bilker SA, Harryman SE. Infant stimulation curriculum for infants with cerebral palsy: effects on infant temperament, parent-infant interaction, and home environment. Pediatrics 1990;85:411-415.
Parette HP, Hourcade JJ. A review of therapeutic intervention research on gross and fine motor progress in young children with cerebral palsy. Am J Occup Ther 1984;38:462-468. Piper MC, Darrah J. Motor assessment of the developing infant. Philadelphia: Saunders; 1994.
Piper MC, Pless IB. Early intervention for infants with Down Syndrome: a controlled trial. Pediatrics 1980;65:463-468.
Piper MC, Kunos VI, Willis DM, Mazer BL, Ramsay M, Silver KM. Early physical therapy effects on the high-risk infant: a randomized controlled trial. Pediatrics 1986;78:216-224.
Prechtl HFR. The neurological examination of the full term newborn infant: a manual for clinical use from the Department of Developmental Neurology, University of Groningen. London: Heinemann Medical Publications; 1977.
Prechtl HF, Einspieler C, Cioni G, Bos AF, Ferrari F, Sontheimer D. An early marker for neurological deficits after perinatal brain lesions. Lancet 1997;349:1361-1363.
Prechtl HFR. General movement assessment as a method of developmental neurology: new para-digms and their consequences. Dev Med Child Neurol 2001;43:836-842.
Ramey CT, Campbell FA. Preventive education for high-risk children: cognitive consequences of the Carolina Abecedarian Project. Am J Ment Defic 1984;88:515-523.
Rauh VA, Achenbach TM, Nurcombe B, Howell CT, Teti DM. Minimizing adverse effects of low birth-weight: four-year results of an early intervention program. Child Dev 1988;59:544-553.
Resnick MB, Eyler FD, Nelson RM, Eitzman DV, Bucciarelli RL. Developmental Intervention for low birth weight infants: Improved early developmental outcome. Pediatrics 1987;80:68-74.
Resnick MB, Armstrong S, Carter RL. Developmental Intervention Program for high-risk premature infants: effects on development and parent-infant interactions. J Dev Behav Pediatr 1988;9:73-78.

86 87
Rosenbaum P, King S, Law M, King G, Evans J. Family centered service: a conceptual framework and research review. Phys Occup Ther Pediatr 1998;18:1-20.
Rothberg AD, Goodman M, Jacklin LA, Cooper PA. Six-year follow-up of early physiotherapy intervention in very low birth weight infants. Pediatrics 1991;88:547-552.
Sackett DL. Rules of evidence and clinical recommen-dations on the use of antithrombotic agents. Chest 1989;95:2S-4S (supplement).Shonkoff JP, Meisels SJ. Handbook of early childhood intervention. Cambridge: Cambridge University Press; 2000.
Siebes RC, Wijnroks L, Vermeer A. Qualitative analysis of therapeutic motor intervention programmes for children with cerebral palsy: an update. Dev Med Child Neurol 2002;44:593-603.
Spittle AJ, Orton J, Boyd R. Early developmental inter-vention programs post hospital discharge to prevent motor and cognitive impairments in preterm infants (protocol). Cochrane Database Syst Rev 2004; Issue 4. Art. No.: CD005495. DOI: 10.1002/14651858.CD005495.
Tessier R, Cristo MB, Velez S, Giron M, Nadeau L, Figueroa de Calume Z, Ruiz-Paláez JG, Charpak N. Kangaroo Mother Care : A method for protecting high-risk low-birth-weight and premature infants against developmental delay. Infant Beh Dev 2003;26:384-397.
Touwen BCL. Neurological development in infancy. Clinics in Developmental Medicine No. 58. London, Heinemann Medical Publications; 1976.
Van der Meulen BF, Ruiter SAJ, Spelberg HCL, Smrko-vsky M. Bayley Scales of Infant Development - II. Dutch version. Lisse, Swets Test Publishers; 2002.
Vohr BR, Garcia Coll CT. Neurodevelopmental and school performance of very low-birth-weight infants: a seven-year longitudinal study. Pediatrics 1985;76,345-350.
Vohr BR, Wright LL, Dusick AM, Mele L, Verter J, Steichen JJ, Simon NP, Wilson DC, Broyles S, Bauer CR, Delaney-Black V, Yolton KA, Fleisher BE, Papile LA, Kaplan MD. Neurodevelopmental and functional outcomes of extremely low birth weight infants in the National Institute of Child Health and Human Development Neonatal Research Network, 1993-1994. Pediatrics 2000;105:1216-1226.
Vojta V. Die cerebralen Bewegungsstörungen im Säugling-salter: Frühdiagnose und Frühtherapie. Stuttgart: Enke; 1976.
Wasik BH, Ramey CT, Bryant DM, Sparling JJ. A longitudinal study of two early intervention strategies: Project CARE. Child Dev 1990;61:1682-1696.
Weindling AM, Hallam P, Gregg J, Kenka H, Rosen-bloom L, Hutton JL. A randomized controlled trial of early physiotherapy for high-risk infants. Acta Paediatr 1996;85:1107-1111.
Westrup B, Bohm B, Lagercrantz H, Stjernqvist K. Preschool outcome in children born very prematurely and cared for according to the Newborn Individual-ized Developmental Care and Assessment Program (NIDCAP). Acta Paediatr 2004;93:498-507.
C H a P t E r 5
de V e l oPm e n t of A
q uA n t I tAt I V e to ol
to A s s e s s t h e c on t e n t
of P h ys Ic A l t h e r A P y
f or I n fA n t s
------------------------------------------------------------------------------------------------------------
CH Blauw-Hospers, T Dirks, LJ Hulshof, M Hadders-Algra
Pediatric Physical Therapy, 2010; 22: 189-198

88 89
abstract
Purpose. The study aim was to describe and quantify physical therapy interventions for infants at
high risk for developmental disorders.
Methods. An observation protocol was developed based on knowledge about infant physical thera-
py and analysis of directly observable physiotherapeutic (PT) actions. The protocol’s psychometric
quality was assessed. Videos of 42 infant physical therapy sessions at 4 or 6 months corrected age
were analyzed.
results. The observation protocol classified PT actions into 8 mutually exclusive categories.
Virtually all PT actions during treatment could be classified. Interrater and intrarater agreement
were satisfactory (intraclass correlations, 0.68-1.00). Approximately 40% of treatment time was
spent on challenging the infants to produce motor behavior by themselves whereas approximately
30% of time facilitation techniques were applied. Tradition-based sessions could be differentiated
from function-oriented ones.
Conclusions. It is possible to document PT actions during physical therapy treatment of infants at
high risk for cerebral palsy in a systematic, standardized and reliable way.
Key Words
Physical Therapy, Infants, Cerebral Palsy, Program evaluation, Video observation, Quantitative
tool, Reliability
Introduction and purpose
In pediatric physical therapy, multiple intervention programs are used for the treatment of infants
with or at risk for developmental disorders, such as cerebral palsy (CP). Programs frequently used
during a stay in the neonatal intensive care unit are the Newborn Individualized Developmental
Care and Assessment Program, Kangaroo Care and sensory stimulation programs. Programs
used after term age are quite different in approach and vary from treatment according to Vojta, to
NeuroDevelopmental Treatment (NDT), to multiple forms of specific and general developmental
programs (Blauw-Hospers and Hadders-Algra 2005). Four recent reviews (Butler and Darrah 2001,
Blauw-Hospers and Hadders-Algra 2005, Blauw-Hospers et al 2007, Spittle et al 2007) did not find
conclusive evidence that early physical therapy intervention improves motor outcome in children
with or at risk for CP. Literature also does not provide evidence that early physical therapy pro-
duces other benefits, such as the enhancement of social-emotional or cognitive function (Butler
and Darrah 2001, Blauw-Hospers et al 2007).
A “theory driven evaluation” (Chen 1990) might help to understand why evidence for the ef-
fectiveness of early intervention (EI) programs is lacking. Theory driven evaluations pay attention
to the mechanisms underlying outcome. This means that they do not only evaluate the effect of
intervention on outcome (eg, “does application of EI result in a higher score on the Bayley Scales of
Infant Development?”), but also the pathway along which the outcome is achieved (eg, “is applica-
tion of a specific physiotherapeutic (PT) action related to outcome?”).
Theory driven evaluation offers a framework to understand the relation between program
inputs, the contents of the program - the ‘black box’ -, and the outcomes (Brazil et al 2005). Know-
ledge about the effect of specific elements of an intervention is crucial for improvement of physi-
cal therapeutic guidance. Guidance should focus on elements which have a beneficial effect on
outcome and elements which do not affect outcome or have an adverse effect should be discarded.
Uncovering the actual contents of practiced physical therapy will shed light on potentially effec-
tive and ineffective elements of the intervention.
The aim of the present study is to develop an instrument to objectify what physical therapists
actually do during treatment, that is, to open the black box of physical therapy sessions in daily
practice, applied to infants at high risk for a developmental disorder such as CP. It should be noted
that CP develops in only a portion of infants at high risk for developmental disorders. Yet, motor
problems and difficulties in learning develop in a substantial proportion of these infants at school
age (Aylward 2005).
To this end, we developed an observation protocol based on the theoretical constructs of the
most commonly used physical therapy approaches for high risk infants in the Netherlands, that
is, NDT and functional therapy (Ketelaar et al 2001, Ekström et al 2005). The term functional in
the latter approach may give the impression that NDT does not aim at improving the infant’s
function. This is a false impression; all approaches in infant physical therapy aim at improving
the child’s function. Nevertheless, some differences exist between NDT and functional therapy.
For instance, NDT is characterized by a broad repertoire of therapist-infant contact strategies,
90 91
whereas the functional approach relies entirely on infant self-produced motor behavior. Primary
questions addressed in this study deal with the psychometric properties of the protocol. 1) Is the
observation protocol complete, that is, is it possible to classify the majority (> 90%) of the contents
of physical therapy sessions? 2) Are the observation items mutually exclusive? 3) Can the items
be assessed reliably in terms of inter- and intraassessor agreement? Secondary questions address
the actual content of the physical therapy sessions during early infancy: 4) Which observable
therapeutic strategies can be distinguished? 5) What proportion of time is spent on the different
strategies?
Methods
Development of the observation protocol
Protocol development started with a systematic analysis of the literature on the application of
physical therapy in infants with or at risk for developmental motor disorders such as CP. This
analysis gave us clues to the most important strategies that are used by pediatric physical thera-
pists. These strategies are based on the theoretical constructs of the most commonly used physical
therapy programs for high-risk infants, that is, NDT and functional therapy. The NDT approach
was developed in the 1940s by Karl and Berta Bobath. Inhibition of spasticity and facilitation of
normal posture and motor behavior were the main aims of treatment, which the Bobaths tried to
accomplish by tone-influencing patterns with the use of various therapeutic handling techniques
(Bobath and Bobath 1984, Mayston 2001). Over the years, NDT gradually evolved based on new
theoretical constructs and practical knowledge. Although the basic philosophy and the approach
to treatment remained the same, goals, treatment techniques and treatment application obtained
a more functional orientation (Mayston 2001, Howle 2002). Currently the main goals of NDT are
to increase or improve the skill repertoire, to maintain the functional level of performance, and
the general management and minimization of contractures and deformities (Mayston 2001).
The way in which NDT is applied depends on the child’s age and the severity of the disability.
Already in the 1960s Elizabeth Köng and Mary Quinton started to adapt and develop techniques
for early treatment of babies based on the Bobath concept (Bly 1999, Quinton and Nelson 2002).
The principles of NDT baby treatment (Bly 1999) aim at helping the infant’s motor development
by giving the infant sensorimotor experiences of typical motor patterns. This is achieved by using
several forms of facilitation techniques, such as handling or pressure techniques, by using sup-
port devices or by giving sensory experience to the infant. Therapy should not be restricted to the
therapy sessions; the therapist aims by means of training the caregivers to achieve a carry-over
from treatment into activities of daily life (Bobath and Bobath 1984, Finnie 1996, Mayston 2001).
The focus of functional therapy lies on improvement of functional tasks (Ketelaar et al 2001,
Ekström et al 2005). Application of the concept of functional therapy to young infants implies that
the cornerstone of guidance consists of encouragement of self produced motor behavior during
functional tasks, such as feeding, dressing, bathing and playing (Resnick et al 1987, Palmer et al
1988, Ketelaar et al 2001, Ekström et al 2005). From the literature, it is known that infants at high
risk for a developmental motor disorder have a reduced repertoire of motor strategies available for
exploration. This is already expressed during the first postnatal months in a limited repertoire of
general movements (GMs) and continues when goal-directed motility emerges. The infants also
have difficulties in selecting the most appropriate solution for a certain task out of their motor
repertoire (Hadders-Algra 2000b). Functional therapy therefore aims through play to promote
variation in motor behavior and opportunities to explore the motor possibilities to find appropri-
ate solutions for motor tasks (Hadders-Algra 2000b, Ketelaar et al 2001, Damiano 2006). Part and
parcel of the more functional approach is the coaching role of the therapist, that is, the caregivers
determine how developmental strategies highlighted by the therapist may be integrated into the
child and family’s daily life.
In the next stage of protocol development we analyzed 20 pilot video recordings of infant
treatment sessions in terms of directly observable PT actions. All actions that physical therapists
performed were documented. These PT actions were classified and defined into categories. The
categories varied from classic NDT actions such as handling techniques to categories describing
functional activities (self produced motor behavior) and family involvement and education. The
observation protocol is the final result of a cyclical process that incorporated knowledge about
physical therapy for infants and the observation of overt and directly observable therapeutic
actions during treatment from video recordings. During the development of the observation pro-
tocol, we paid attention to required psychometric requirements: completeness, mutual exclusive-
ness, reliability, and construct validity (Reynders 1992).
Subjects
The contents of physical therapy sessions were analyzed for a study group of 22 infants, who had
been admitted to the neonatal intensive care unit of the University Medical Center Groningen. All
infants had an indication for early physiotherapeutic intervention on the basis of the presence of
definitely abnormal GMs at the age of ten weeks corrected age. The GM method is a standardized
technique to assess neurological integrity on the basis of the quality of spontaneous motor behav-
ior (Einspieler et al 2004, Hadders-Algra 2004). GMs are spontaneously generated complex move-
ments involving the head, trunk, arms, and legs. Four classes of GM quality can be distinguished:
normal-optimal, normal-suboptimal, mildly abnormal and definitely abnormal. Various studies
showed that the presence of definitely abnormal GMs at 2 to 4 months post-term indicates a high
risk for developmental disabilities, such as CP (Prechtl et al 1997, Prechtl 2001, Hadders-Algra
2004). The GM assessment has a good predictive validity for both major and minor developmental
disorders. Also construct and concurrent validity and reliability of the GM method are satisfac-
tory (Heineman and Hadders-Algra 2008). Infants with severe congenital anomalies and infants
whose caregivers had an inappropriate understanding of the Dutch language were excluded from
the study. All caregivers of the infants signed an informed consent and the research project was
approved by the Ethics Committee of the University Medical Center Groningen.
Twenty of the infants were born preterm with a gestational age at birth that varied from

92 93
28 to 32 weeks (median, 31) and a birth weight between 630 and 2090 g (median, 1205 g). Two
infants were born at term with a median birth weight of 3560 g. Neurological condition was as-
sessed at 6 months corrected age (CA) with the Touwen Infant Neurological Examination (TINE)
(Hadders-Algra et al 2009). Three infants showed clear neurological dysfunction. Fourteen
infants showed a high number of signs of minor neurological dysfunction (MND). The remaining
five infants had a normal-suboptimal neurological condition at 6 months (Table 5.1).
table 5.1. Birth characteristics and neurological outcome (n=22).
total (n = 22)
Gender 10 boys
12 girls
Gestational age (wk)
Median
Range
Preterm (n=20)
31
28-32
Term (n = 2)
38
37-39
Birth weight (g)
Median
Range
Preterm (n=20)
1205
630-2090 g
Term (n =2)
3560
3460-3660 g
Neurological examination at 6 mo* 4 Normal-suboptimal
15 MND
3 Abnormal
* corrected for prematurity
g = gram, MND = Minor Neurological Dysfunction, mo = months, wk = weeks
Recording of intervention sessions
All 22 infants received physical therapy between the ages of 3 to 6 months corrected age. Therapy
was delivered by 17 physical therapists who were registered in the Netherlands as pediatric physi-
cal therapists. Fifteen therapists treated the infants in their home environment and 2 applied the
intervention in a clinical setting. Treatment duration varied from 12 to 50 minutes per session
(mean, 30 minutes per session; SD 9 minutes per session).
At 4 and 6 months corrected age, a video recording of a treatment session of each infant was
made. To minimize intrusion, the camera was positioned as far away from the physical therapist
and infant as possible. In addition, therapist and caregiver were asked to ignore the person ma-
king the video so that the recording would resemble a natural situation. Research has shown that
video recording hardly affects the behavior of people that are being filmed because they tend to
forget the presence of the camera after awhile (Albrecht et al 2005). Care was taken that physical
therapist, caregiver, and infant were continuously in view of the camera.
The video recordings were analyzed with the standardized observation protocol with help of
the Noldus software program The Observer (Version 5.0; Noldus, Wageningen, the Netherlands),
a program specially designed for behavioral observation. The program allows the quantification
of the duration, frequency and serial order of defined therapeutic actions. For example, imagine
the following sequence of actions: A) a physical therapist offers an infant a toy in the midline;
B) after 6 seconds the therapist facilitates rolling behavior with the pelvis or legs as keypoint, C)
meanwhile the therapist gives the caregiver instructions on handling during rolling movements.
In the Observer action A is scored as category H (see Appendix 1, p. 188; the infant is challenged
to produce motor behavior by himself or herself; activity flows over into therapeutic handling).
As the toy is offered in the midline only, the action is performed with little variation (H1). Action
B is scored as category C1 (facilitation techniques - handling), but at the same time the physical
therapist interferes with the infant’s behavior and interrupts his or her activity (category A.4.1).
Action C is scored as category A.4.3 (caregiver training). Start and stop of an action are indicated
by pressing a key on the computer keyboard. It is important to note that The Observer program al-
lows scoring of multiple actions occurring simultaneously (eg, action B). To compare the results of
different treatment sessions, the duration of the PT actions was converted into a relative duration,
which represented a percentage of the total treatment time. Relative duration (%) = (Time spent on
PT action / Total time of treatment session) * 100.
Psychometric quality of the observation protocol
Completeness of the protocol was tested by checking whether all possible PT actions observed
by the researchers were covered by the categories of the observation protocol. Completeness was
considered satisfactory if major part of the PT actions (> 90% of the observation time) could be
classified into protocol categories. Mutual exclusiveness was determined by means of the in-
ter- and intrarater agreement. Substantial agreement indicates that a single PT action is clearly
related to a specific category of the observation protocol. Reliability of the observation protocol

94 95
was measured through inter- and intrarater agreement. Three time intervals, each lasting five
minutes, were selected from within each of 5 randomly selected treatment sessions (n=15). The
intervals 100-400 seconds, 500-800 seconds and 1000-1300 seconds were analyzed. The start of
the treatment session, that is, the first 100 seconds, was excluded from the analyses because dur-
ing this period mainly preparatory actions were performed. Interrater agreement was assessed
by comparing observational scores of the third author with those of the first author. Intrarater
agreement was assessed by comparing the observational scores of the first author who reanalyzed
the video sequences with an interval of at least three weeks.
Data Analysis
The data were analyzed using the computer package SPSS (version 14.0; SPSS Inc, Chicago, Illinois).
Inter- and intrarater agreements were calculated by intraclass correlations (ICCs) of frequency and
relative duration of PT actions. ICC values between 0.50 to 0.75 were considered to indicate satis-
factory reliability, ICC values exceeding 0.75 indicate good reliability (Portney and Watkins 2000).
For the comparison of the relative duration of the main categories and subcategories of PT ac-
tions and the amount of postural support at 4 months with the data at 6 months, Wilcoxon signed
rank tests were used.
To get an impression of the current state of the daily practice in pediatric physical therapy
in The Netherlands we analyzed whether sessions were dominated by PT actions that are in line
with the concept of NDT in baby treatment13 or by PT actions belonging to the functional ap-
proach. A treatment session was classified as NDT-like when the time spent on the category facili-
tation techniques exceeded the 75th percentile of current group data. Similarly, sessions in which
time spent on the category ‘challenging the infant to produce motor behavior by himself or herself
- action continued by the infant’ exceeded the 75th percentile were classified as functional sessions.
Correlations and differences with a p-value < 0.05 were considered as statistically significant.
results
Observation protocol
The observation protocol contains three levels of observation. The first level consists of eight
mutually exclusive main categories of PT actions (see Appendix 1). The second level consists of
the subcategories of the main techniques. For example, the main category facilitation techniques
has the following subcategories: handling, pressure techniques, transitions and support devices.
The third level of the protocol entails concrete PT-actions. For example, in the supine or sitting
position: shoulders function as a key point, handling hands guide the shoulders of the infant in
protraction to control the infants movements and to facilitate hand-hand contact and symmetry.
The degree of postural support provided by the physical therapist or caregiver when the infant
was in prone, side or sitting position was scored as an additional variable. Postural support was
classified into four categories: no postural support, minimal postural support, clear postural sup-
port and full postural support
Psychometric properties
The contents of 42 physical therapy sessions were analyzed. For two infants, only one video
recording was available for observation. In one case, the therapist had already discontinued treat-
ment before 6 months. In the other case, the family was on holiday when the video recording was
scheduled.
Major part of the observed PT actions could be classified into the categories of the observa-
tion protocol. Only 3% of the duration of physical therapy sessions could not be classified into the
categories of the observation protocol, that is, they were classified in the category ‘not specified’.
This indicates that the observation protocol meets the criterion for completeness.
Inter- and intrarater agreement on the frequency of PT actions was moderate to good with
ICCs varying from 0.68 to 1.00 (interrater) and 0.70 to 0.98 (intrarater). The same was true for the
inter- and intrarater agreement on the relative duration of actions; ICCs ranged from 0.76 to 1.00
(interrater) and 0.69 to 0.99 (intrarater; Table 5.2). The confidence intervals of the PT actions are
presented in Table 5.2. The data indicate that the PT actions of the observation protocol can be
assessed in a reliable way. Moreover the moderate to good inter- and intrarater agreement points
to a sufficient degree of mutually exclusiveness.
Relative duration of therapeutic actions
The data on frequency and relative duration of PT actions were highly correlated (Spearman
rank correlation at 4 months: 0.89, at 6 months: 0.88). This suggests that both parameters carry
virtually identical information. We therefore decided to restrict our report on the contents of the
sessions to one parameter. We chose relative duration as it had slightly better inter- and intrarater
agreement values than frequency.
The relative duration of the majority of the PT actions applied at 4 months did not differ sig-
nificantly from those at 6 months (Table 5.3). The only exceptions were challenging the infant to
produce motor behavior by himself which flows over into handling, which occurred slightly more
at 6 months than at 4 months (p=0.03) and in the provision of postural support. Less postural sup-
port was provided during PT actions in infants aged 6 months than in those aged 4 months (Table
5.3).
In the following report on the contents of the NDT sessions, we pooled the 4- and 6-month
data for those actions in which the relative duration of PT actions at 4 and 6 months were identi-
cal. Table 5.3 shows that the application of physical therapy in infancy is characterized by a large
heterogeneity. Most of treatment time was spent with PT actions in the categories of motor
behavior produced by the infant, that is, motor behavior that was initiated by the infant and
behavior that was challenged by caregiver or physical therapist who a) let the infant try on her or
his own or b) took over control of the infant’s movements by means of handling (together ~40%),
and facilitation techniques (29%; Figure 5.1). We noted that during both challenging the infant to
produce motor behavior by himself/herself, which flows over into handling (5.6%) and challenging
the infant to produce motor behavior by himself/herself which is continued by the infant (13.2%),

96 97
tab
le 5
.2. I
nter
rate
r an
d in
trar
ater
agr
eem
ent (
ICC
) on
mai
n an
d su
bcat
egor
ies
of p
hysi
othe
rape
utic
ac
tion
s (f
requ
ency
and
rel
ativ
e du
rati
on o
f PT
act
ion
s; n
=15
vide
o fr
agm
ents
of 5
min
utes
).
Inte
rven
tion
In
terr
ater
agr
eem
ent
Intr
arat
er a
gree
men
tFr
eque
ncy
(n=1
5)D
urat
ion
(n=1
5)Fr
eque
ncy
(n=1
5)D
urat
ion
(n=1
5)
ICC
(95%
CI)
ICC
(95%
CI)
ICC
(95%
CI)
ICC
(95%
CI)
Fam
ily
invo
lvem
ent a
nd E
duca
tion
al c
ompo
nent
E
duca
tion
al a
ctio
ns
0.78
(0.4
8-0.
92)
0.78
(0.4
8-0.
92) b
0.80
(0.4
9-0.
93) b
0.88
(0.6
6-0.
96) b
- Car
egiv
er in
terf
eres
wit
h in
fant
’s ac
tivi
ties
n.o
.an
.o.a
n.o
.an
.o.a
- PT
inte
rfer
es w
ith
infa
nt’s
acti
viti
es
0.76
(0.4
3-0.
91)
0.76
(0.4
3-0.
91) b
0.89
(0.7
0-0
.96)
b0.
80 (0
.51-
0.93
) b
- PT
gui
des
the
infa
nt1.
00 (1
.00
-1.0
0)0.
99 (0
.98-
1.00
) b0.
74 (0
.38-
0.90
) b0.
75 (0
.40
-0.9
0) b
- PT
giv
es c
areg
iver
tra
inin
gn
.o.a
n.o
a0.
95 (0
.86-
0.98
) b0.
78 (0
.46-
0.92
) b
- PT
coa
ches
the
car
egiv
ern
.o.a
n.o
.an
.o.a
n.o
.a
Com
mun
icat
ion
0.87
(0.6
6-0.
95)
0.98
(0.9
4-0.
99) b
0.89
(0.6
9-0.
96) b
0.96
(0.8
0-0
.98)
b
- In
form
atio
n ex
chan
ge0.
87 (0
.68-
0.95
)0.
98 (0
.93-
0.99
) bn
.o.a
n.o
.a
- C
onte
nts
of in
form
atio
n0.
81 (0
.54-
0.93
)0.
83 (0
.59-
0.94
) b0.
86 (0
.63-
0.95
) b0.
81 (0
.52-
0.93
) b
- In
stru
ct0.
86 (0
.64-
0.95
)0.
81 (0
.54-
0.93
) b0.
85 (0
.61-
0.95
) b0.
83 (0
.57-
0.94
) b
- P
rovi
de fe
edba
ck0.
78 (0
.48-
0.92
)0.
96 (0
.89-
0.99
) b0.
82 (0
.54-
0.94
) b0.
87 (0
.65-
0.95
) b
- Im
part
kno
wle
dge
0.87
(0.6
8-0.
95)
0.91
(0.7
6-0.
97) b
0.75
(0.4
7-0.
92) b
0.74
(0.3
9-0.
91) b
Neu
rom
otor
com
pone
ntFa
cilit
atio
n te
chn
ique
s
0.95
(0.8
6-0.
98)
0.97
(0.9
0-0
.99)
b0.
97 (0
.91-
0.99
) b0.
99 (0
.99-
1.00
) b
- Han
dlin
g 0.
72 (0
.37-
0.89
)0.
80 (0
.52-
0.93
) b0.
95 (0
.86-
0.98
) b0.
91 (0
.76-
0.97
) b
- Pre
ssur
e te
chn
ique
s0.
97 (0
.91-
0.99
)0.
88 (0
.69-
0.96
) b0.
93 (0
.80
-0.9
8) b
0.97
(0.9
2-0.
99) b
- Sup
port
dev
ice
n.o
.an
.o.a
n.o
.an
.o.a
- Tra
nsi
tion
0.86
(0.6
4-0.
95)
0.91
(0.7
5-0.
98) b
0.89
(0.6
9-0.
96) b
0.87
(0.6
5-0.
95) b
Sen
sory
exp
erie
nce
0.85
(0.6
3-0.
95)
0.88
(0.7
0-0
.96)
b0.
76 (0
.42-
0.91
) b0.
78 (0
.46-
0.92
) b
Pass
ive
mot
or e
xper
ienc
e0.
71 (0
.35-
0.89
)0.
91 (0
.77-
0.97
) b0.
70 (0
.70
-0.8
9) b
0.92
(0.7
9-0.
97) b
Self
-pro
duce
d m
otor
beh
avio
r –
no in
terf
eren
ce0.
95 (0
.85-
0.98
)0.
97 (0
.93-
0.99
) b0.
82 (0
.53-
0.93
) b0.
94 (0
.83-
0.98
) b
Cha
lleng
ed to
sel
f-pr
oduc
ed m
otor
beh
avio
r –
acti
on c
onti
nued
by
infa
nt0.
86 (0
.64-
0.95
)0.
80 (0
.51-
0.92
) b0.
86 (0
.63-
0.95
) b0.
86 (0
.62-
0.95
) b
- Lit
tle
vari
atio
n0.
90 (0
.74-
0.96
)0.
87 (0
.67-
0.95
) b0.
85 (0
.60
-0.9
5) b
0.83
(0.5
7-0.
94) b
- Lar
ge v
aria
tion
0.75
(0.4
1-0.
90)
0.82
(0.5
5-0.
93) b
0.84
(0.5
9-0.
94) b
0.89
(0.7
1-0.
96) b
Cha
lleng
ed to
sel
f-pr
oduc
ed m
otor
beh
avio
r –
wit
h ov
erflo
w in
to h
andl
ing
0.80
(0.5
2-0.
93)
0.88
(0.7
0-0
.96)
b0.
84 (0
.59-
0.94
) b0.
72 (0
.34-
0.90
) b
- Lit
tle
vari
atio
n0.
85 (0
.62-
0.95
)0.
84 (0
.59-
0.94
) b0.
86 (0
.64-
0.95
) b0.
72 (0
.35-
0.90
) b
- Lar
ge v
aria
tion
0.72
(0.3
6-0.
89)
0.90
(0.7
4-0.
96) b
n.o
.an
.o.a
Not
spe
cifi
ed a
ctio
ns
0.68
(0.3
0-0
.88)
0.84
(0.6
1-0.
94) b
0.81
(0.5
2-0.
93) b
0.79
(0.4
9-0.
93) b
No
post
ural
sup
port
0.93
(0.8
1-0.
98)
0.99
(0.9
7-1.
00)
0.97
(0.9
1-0.
99)
0.98
(0.9
5-0.
99)
Min
imal
pos
tura
l sup
port
0.78
(0.4
8-0.
92)
0.89
(0.7
2-0.
96)
0.77
(0.4
4-0.
92)
0.69
(0.2
9-0.
88)
Cle
ar p
ostu
ral s
uppo
rt0.
69 (0
.31-
0.88
)0.
89 (0
.70
-0.9
6)0.
89 (0
.71-
0.96
)0.
89 (0
.70
-0.9
6)Fu
ll po
stur
al s
uppo
rt0.
69 (0
.31-
0.88
)1.
00 (0
.99-
1.00
)0.
98 (0
.94-
0.99
)0.
91 (0
.74-
0.97
)
95%
CI =
95%
con
fiden
ce in
terv
al, I
CC
= in
trac
lass
cor
rela
tion
coe
ffici
ent
a Not
obs
erve
d b p
<.05
; for
defi
nit
ion
of t
he v
ario
us c
ateg
orie
s se
e A
ppen
dix
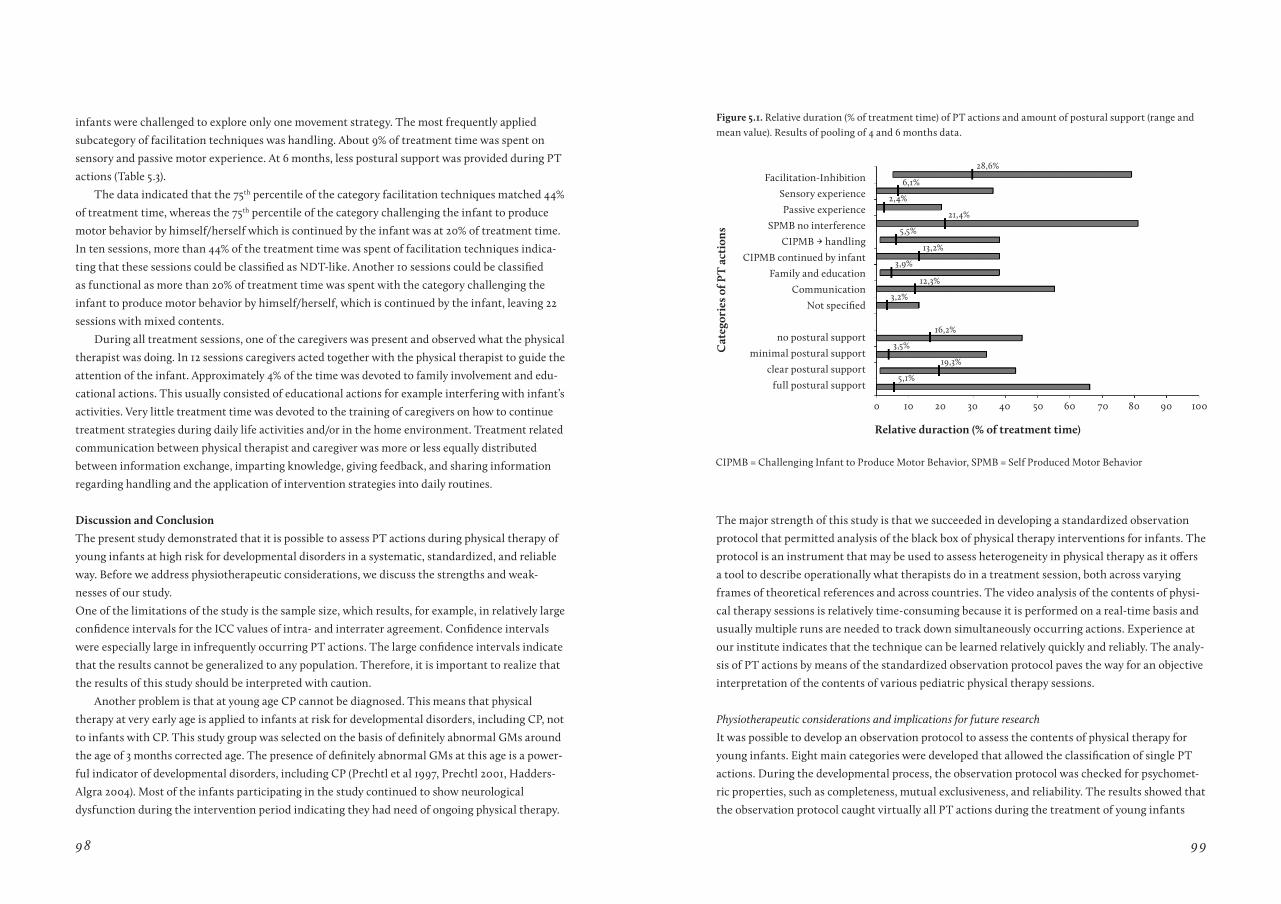
98 99
infants were challenged to explore only one movement strategy. The most frequently applied
subcategory of facilitation techniques was handling. About 9% of treatment time was spent on
sensory and passive motor experience. At 6 months, less postural support was provided during PT
actions (Table 5.3).
The data indicated that the 75th percentile of the category facilitation techniques matched 44%
of treatment time, whereas the 75th percentile of the category challenging the infant to produce
motor behavior by himself/herself which is continued by the infant was at 20% of treatment time.
In ten sessions, more than 44% of the treatment time was spent of facilitation techniques indica-
ting that these sessions could be classified as NDT-like. Another 10 sessions could be classified
as functional as more than 20% of treatment time was spent with the category challenging the
infant to produce motor behavior by himself/herself, which is continued by the infant, leaving 22
sessions with mixed contents.
During all treatment sessions, one of the caregivers was present and observed what the physical
therapist was doing. In 12 sessions caregivers acted together with the physical therapist to guide the
attention of the infant. Approximately 4% of the time was devoted to family involvement and edu-
cational actions. This usually consisted of educational actions for example interfering with infant’s
activities. Very little treatment time was devoted to the training of caregivers on how to continue
treatment strategies during daily life activities and/or in the home environment. Treatment related
communication between physical therapist and caregiver was more or less equally distributed
between information exchange, imparting knowledge, giving feedback, and sharing information
regarding handling and the application of intervention strategies into daily routines.
Discussion and Conclusion
The present study demonstrated that it is possible to assess PT actions during physical therapy of
young infants at high risk for developmental disorders in a systematic, standardized, and reliable
way. Before we address physiotherapeutic considerations, we discuss the strengths and weak-
nesses of our study.
One of the limitations of the study is the sample size, which results, for example, in relatively large
confidence intervals for the ICC values of intra- and interrater agreement. Confidence intervals
were especially large in infrequently occurring PT actions. The large confidence intervals indicate
that the results cannot be generalized to any population. Therefore, it is important to realize that
the results of this study should be interpreted with caution.
Another problem is that at young age CP cannot be diagnosed. This means that physical
therapy at very early age is applied to infants at risk for developmental disorders, including CP, not
to infants with CP. This study group was selected on the basis of definitely abnormal GMs around
the age of 3 months corrected age. The presence of definitely abnormal GMs at this age is a power-
ful indicator of developmental disorders, including CP (Prechtl et al 1997, Prechtl 2001, Hadders-
Algra 2004). Most of the infants participating in the study continued to show neurological
dysfunction during the intervention period indicating they had need of ongoing physical therapy.
Cat
egor
ies
of P
t a
ctio
ns
relative duraction (% of treatment time)
0 10
28,6%
6,1%
2,4%
21,4%
5,5%
13,2%
3,9%
12,3%
3,2%
16,2%
3,5%
19,3%
5,1%
20 30 40 50 60 70 80 90 100
Facilitation-Inhibition
Sensory experience
Passive experience
SPMB no interference
CIPMB --> handling
CIPMB continued by infant
Family and education
Communication
Not specified
no postural support
minimal postural support
clear postural support
full postural support
The major strength of this study is that we succeeded in developing a standardized observation
protocol that permitted analysis of the black box of physical therapy interventions for infants. The
protocol is an instrument that may be used to assess heterogeneity in physical therapy as it offers
a tool to describe operationally what therapists do in a treatment session, both across varying
frames of theoretical references and across countries. The video analysis of the contents of physi-
cal therapy sessions is relatively time-consuming because it is performed on a real-time basis and
usually multiple runs are needed to track down simultaneously occurring actions. Experience at
our institute indicates that the technique can be learned relatively quickly and reliably. The analy-
sis of PT actions by means of the standardized observation protocol paves the way for an objective
interpretation of the contents of various pediatric physical therapy sessions.
Physiotherapeutic considerations and implications for future research
It was possible to develop an observation protocol to assess the contents of physical therapy for
young infants. Eight main categories were developed that allowed the classification of single PT
actions. During the developmental process, the observation protocol was checked for psychomet-
ric properties, such as completeness, mutual exclusiveness, and reliability. The results showed that
the observation protocol caught virtually all PT actions during the treatment of young infants
CIPMB = Challenging Infant to Produce Motor Behavior, SPMB = Self Produced Motor Behavior
Figure 5.1. Relative duration (% of treatment time) of PT actions and amount of postural support (range and mean value). Results of pooling of 4 and 6 months data.
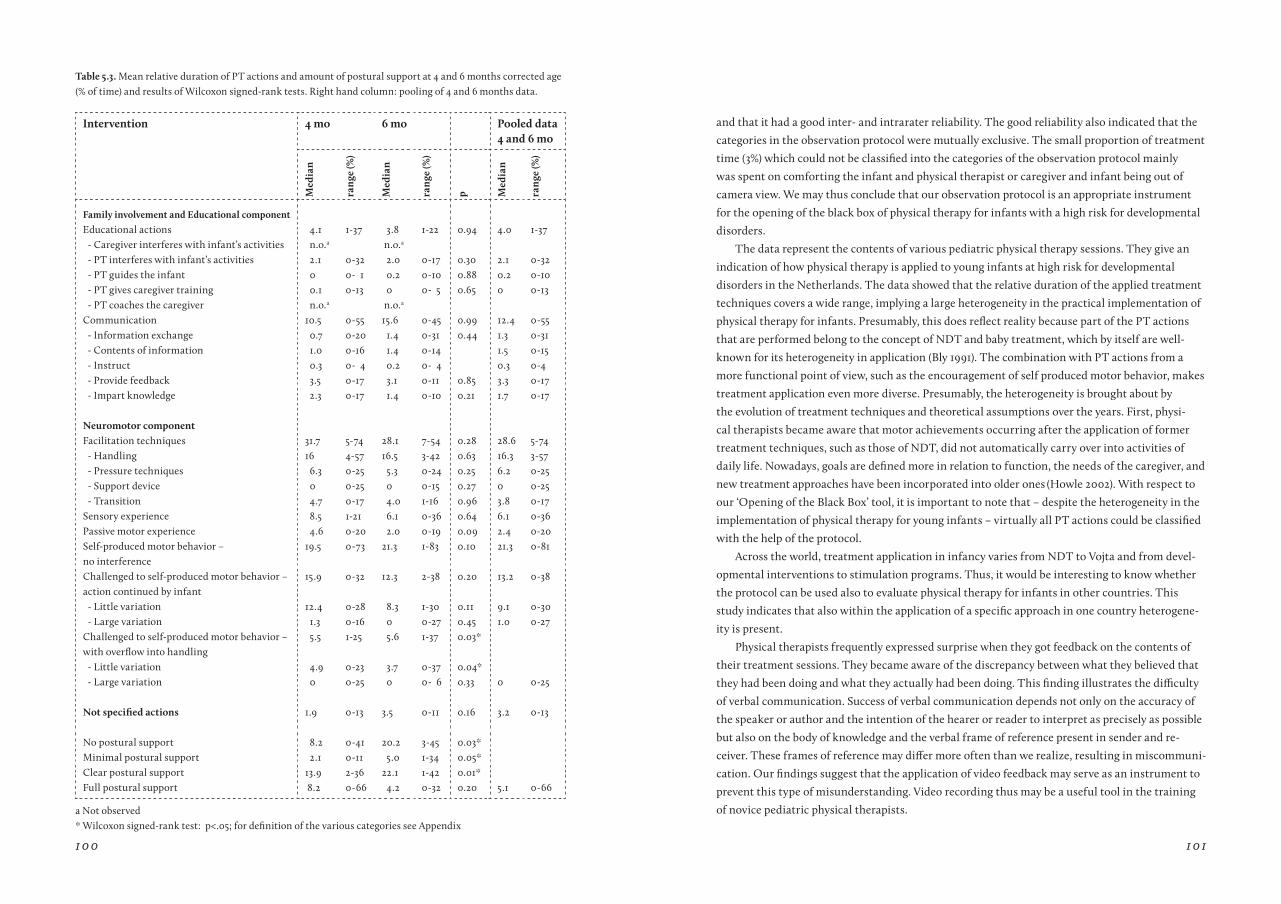
100 101
Intervention 4 mo 6 mo Pooled data 4 and 6 mo
Med
ian
ran
ge (%
)
Med
ian
ran
ge (%
)
p Med
ian
ran
ge (%
)
Family involvement and Educational component
Educational actions 4.1 1-37 3.8 1-22 0.94 4.0 1-37- Caregiver interferes with infant’s activities n.o.a n.o.a
- PT interferes with infant’s activities 2.1 0-32 2.0 0-17 0.30 2.1 0-32- PT guides the infant 0 0- 1 0.2 0-10 0.88 0.2 0-10- PT gives caregiver training 0.1 0-13 0 0- 5 0.65 0 0-13- PT coaches the caregiver n.o.a n.o.a
Communication 10.5 0-55 15.6 0-45 0.99 12.4 0-55 - Information exchange 0.7 0-20 1.4 0-31 0.44 1.3 0-31 - Contents of information 1.0 0-16 1.4 0-14 1.5 0-15 - Instruct 0.3 0- 4 0.2 0- 4 0.3 0-4 - Provide feedback 3.5 0-17 3.1 0-11 0.85 3.3 0-17 - Impart knowledge 2.3 0-17 1.4 0-10 0.21 1.7 0-17
Neuromotor componentFacilitation techniques 31.7 5-74 28.1 7-54 0.28 28.6 5-74
- Handling 16 4-57 16.5 3-42 0.63 16.3 3-57- Pressure techniques 6.3 0-25 5.3 0-24 0.25 6.2 0-25- Support device 0 0-25 0 0-15 0.27 0 0-25- Transition 4.7 0-17 4.0 1-16 0.96 3.8 0-17
Sensory experience 8.5 1-21 6.1 0-36 0.64 6.1 0-36Passive motor experience 4.6 0-20 2.0 0-19 0.09 2.4 0-20Self-produced motor behavior – no interference
19.5 0-73 21.3 1-83 0.10 21.3 0-81
Challenged to self-produced motor behavior – action continued by infant
15.9 0-32 12.3 2-38 0.20 13.2 0-38
- Little variation 12.4 0-28 8.3 1-30 0.11 9.1 0-30- Large variation 1.3 0-16 0 0-27 0.45 1.0 0-27
Challenged to self-produced motor behavior – with overflow into handling
5.5 1-25 5.6 1-37 0.03*
- Little variation 4.9 0-23 3.7 0-37 0.04*- Large variation 0 0-25 0 0- 6 0.33 0 0-25
Not specified actions 1.9 0-13 3.5 0-11 0.16 3.2 0-13
No postural support 8.2 0-41 20.2 3-45 0.03*Minimal postural support 2.1 0-11 5.0 1-34 0.05*Clear postural support 13.9 2-36 22.1 1-42 0.01*Full postural support 8.2 0-66 4.2 0-32 0.20 5.1 0-66
table 5.3. Mean relative duration of PT actions and amount of postural support at 4 and 6 months corrected age (% of time) and results of Wilcoxon signed-rank tests. Right hand column: pooling of 4 and 6 months data.
a Not observed * Wilcoxon signed-rank test: p<.05; for definition of the various categories see Appendix
and that it had a good inter- and intrarater reliability. The good reliability also indicated that the
categories in the observation protocol were mutually exclusive. The small proportion of treatment
time (3%) which could not be classified into the categories of the observation protocol mainly
was spent on comforting the infant and physical therapist or caregiver and infant being out of
camera view. We may thus conclude that our observation protocol is an appropriate instrument
for the opening of the black box of physical therapy for infants with a high risk for developmental
disorders.
The data represent the contents of various pediatric physical therapy sessions. They give an
indication of how physical therapy is applied to young infants at high risk for developmental
disorders in the Netherlands. The data showed that the relative duration of the applied treatment
techniques covers a wide range, implying a large heterogeneity in the practical implementation of
physical therapy for infants. Presumably, this does reflect reality because part of the PT actions
that are performed belong to the concept of NDT and baby treatment, which by itself are well-
known for its heterogeneity in application (Bly 1991). The combination with PT actions from a
more functional point of view, such as the encouragement of self produced motor behavior, makes
treatment application even more diverse. Presumably, the heterogeneity is brought about by
the evolution of treatment techniques and theoretical assumptions over the years. First, physi-
cal therapists became aware that motor achievements occurring after the application of former
treatment techniques, such as those of NDT, did not automatically carry over into activities of
daily life. Nowadays, goals are defined more in relation to function, the needs of the caregiver, and
new treatment approaches have been incorporated into older ones (Howle 2002). With respect to
our ‘Opening of the Black Box’ tool, it is important to note that – despite the heterogeneity in the
implementation of physical therapy for young infants – virtually all PT actions could be classified
with the help of the protocol.
Across the world, treatment application in infancy varies from NDT to Vojta and from devel-
opmental interventions to stimulation programs. Thus, it would be interesting to know whether
the protocol can be used also to evaluate physical therapy for infants in other countries. This
study indicates that also within the application of a specific approach in one country heterogene-
ity is present.
Physical therapists frequently expressed surprise when they got feedback on the contents of
their treatment sessions. They became aware of the discrepancy between what they believed that
they had been doing and what they actually had been doing. This finding illustrates the difficulty
of verbal communication. Success of verbal communication depends not only on the accuracy of
the speaker or author and the intention of the hearer or reader to interpret as precisely as possible
but also on the body of knowledge and the verbal frame of reference present in sender and re-
ceiver. These frames of reference may differ more often than we realize, resulting in miscommuni-
cation. Our findings suggest that the application of video feedback may serve as an instrument to
prevent this type of misunderstanding. Video recording thus may be a useful tool in the training
of novice pediatric physical therapists.

102 103
This study indicates that the categories challenging the infant to produce motor behavior by
himself and facilitation techniques were applied most. Three types of motor behavior produced
by the infant were distinguished: behavior which was initiated by the infant and behavior which
was challenged by caregiver or therapist, who a) let the infant try on her/his own or b) took over
control of the infant’s movements by means of handling. We observed that self initiated activity of
the infant usually occurred when the therapist started to communicate with the parents, leaving
the infant in a situation in which his or her capacities were not challenged. Another observation
was that during motor skill practice the physical therapist usually challenged the infant to explore
only one movement strategy. This means that during the physical therapy sessions of this study,
little variation in motor behavior was practiced. This is surprising because current concepts of in-
fant motor dysfunction suggest that varied practice is beneficial for motor development (Hadders-
Algra 2000b).
The protocol pays specific attention to family involvement and educational actions. In the
latter, we distinguished between educational actions regarding the child and educational actions
regarding the caregiver, that is, caregiver training and caregiver coaching. It was remarkable that
during treatment, little time was spent training the caregiver on how to apply treatment strate-
gies during daily life activities and/or in the home environment. According to the traditional
treatment approach, merely based on NDT, guiding and training of caregivers are the primary
technique to achieve carryover from treatment to everyday life (Bobath and Bobath 1984, Finnie
1996, Howle 2002). In the functional approaches caregivers are the key persons in the child’s
development and education (Law et al 1998, Rosenbaum et al 1998, Ketelaar et al 2001, Ekström et
al 2005). Thus, it seems that actual practice of the therapists involved in this study differed from
current notions because caregivers mainly acted as a passive observer of treatment instead of be-
ing actively involved and instructed.
Future research should aim firstly at a replication of this study in infants at various ages, with
various degrees of neurological dysfunction, and in various countries. A next step will be to relate
the contents of infant physical therapy sessions to developmental outcome. This knowledge might
shed light on the potentially effective and ineffective elements in infant physical therapy.
In conclusion, this study demonstrated that it is possible to assess PT actions during physical
therapy of young infants at high risk for CP in a systematic, standardized, and reliable way despite
the heterogeneity in the implementation of infant physical therapy. The study indicated that
opening the black box of infant physical therapy has shown that in the Netherlands the applica-
tion is very heterogeneous and varies between more traditional (NDT-like) to more functionally
oriented treatment. Our study may be seen as a first step in the development of a tool to describe
therapists’ actions during physical therapy interventions. Objective knowledge on the contents of
physical therapy sessions is an essential step towards evidence-based practice. The next steps to be
taken are replication studies on reliability assessment, studies in different populations (eg, older
children with CP or developmental coordination disorder) and in different countries, and studies
connecting the contents of physical therapy sessions with developmental outcome.
references
Albrecht TL, Ruckdeschel JC, Ray FL 3rd, Pethe BJ, Riddle DL, Strohm J, Penner LA, Coovert MD, Quinn G, Blanchard CG. Portable, Unobtrusive Device for Videorecording Clinical Interactions. Behav Res Meth-ods 2005;37:165-169.
Aylward GP. Neurodevelopmental outcomes of infants born prematurely. J Dev Behav Pediatr 2005;26:427-440.
Blauw-Hospers CH, de Graaf-Peters VB, Dirks T, Bos AF, Hadders-Algra M. Indications that early interven-tion in infants at high risk for a developmental motor disorder may improve motor and cognitive develop-ment. Neurosci Biobehav Rev 2007;31:1201-1212.
Blauw-Hospers CH, Hadders-Algra M. Fact or fiction: a systematic review on the effects of early interven-tion on motor development. Dev Med Child Neurol 2005;47:421-432.
Bly L. A historical and current view of the basis of NDT. Pediatr Phys Ther 1991;3(3):131-135.
Bly L. Baby treatment based on NDT principles. PRO-Ed, Austin Texas;1999.
Bobath K and Bobath B. The neuro-developmental treat-ment. In: D. Scrutton (ed), Management of the motor disorders of children with cerebral palsy. Oxford: Clin-ics in Developmental Medicine 90, Spastics Interna-tional Medical Publications; 1984:6-18.
Brazil K, Ozer E, Cloutier MM, Levine R, Stryer D. From theory to practice: improving the impact of health services research. BMC Health Serv Res 2005;5:1.
Butler C, Darrah J. Effects of neurodevelopmental treatment (NDT) for cerebral palsy: an AACPDM evi-dence report. Dev Med Child Neurol 2001;43:778-790.
Chen H-T. Theory-driven evaluations. Newbury Park, CA: SAGE Publications; 1990.
Damiano DL. Activity, activity, activity: Rethinking our physical therapy approach to cerebral palsy. Phys Ther 2006;11:1534-1540.
Einspieler C, Prechtl HFR, Bos AF, et al. Prechtl’s method on the qualitative assessment of General Move-ments in preterm, term and young infants. Clinics in Developmental Medicine No. 167. London: Mac Keith Press; 2004.
Ekström Ahl L, Johansson E, Granat T, Brogren Carl-berg E. Functional therapy for children with cerebral palsy: an ecological approach. Dev Med Child Neurol 2005;47:613-619.
Finnie NR. Handling the young child with cerebral palsy at home. Oxford: Butterworth-Heinemann; 1996.
Hadders-Algra M, Heineman KR, Bos AF, Middel-burg KJ. Minor neurological dysfunction in infancy: strengths and limitations. Dev Med Child Neurol 2009 Jun 22 (Epub ahead of print).
Hadders-Algra M. General movements: a window for early identification of children at high risk of develop-mental disorders. J Pediatr 2004;145:S12–S18.
Hadders-Algra M. The neuronal group selection theory: promising principles for understanding and treating developmental motor disorders. Dev Med Child Neurol 2000b;42:707-715.
Heineman K, Hadders-Algra M. Evaluation of neu-romotor function in infancy - a systematic review of methods available. J Dev Behav Pediatr 2008;29:315-323.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association; 2002.
Ketelaar M, Vermeer A, Hart H, van Petegem-van Beek E, Helders PJ.Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys Ther 2001;81:1534-1545.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Oc-cup Ther Pediatr 1998;18:83-102.
Mayston MJ. People with cerebral palsy: effects of and perspectives for therapy. Neural Plast 2001;8:51-69.
Palmer FB, Shapiro BK, Wachtel RC, Allen MC, Hiller JE, Harryman SE, Mosher BS, Meinert CL, Capute AJ. The effects of physical therapy on cerebral palsy. A controlled trial in infants with spastic diplegia. N Eng J Med 1988;318:803-808.
Portney LG, Watkins MP. Part IV Data analysis: Correlation. 2000. Foundations of clinical research. Ap-plications to practice. 2nd ed. Upper Saddle River, NJ: Prentice Hall Health; 2000.

104 105
Prechtl HF, Einspieler C, Cioni G, Bos AF, Ferrari F, Sontheimer D. An early marker for neurological defi-cits after perinatal brain lesions. Lancet 1997;349:1361-1363.
Prechtl HFR. General movement assessment as a method of developmental neurology: new para-digms and their consequences. Dev Med Child Neurol 2001;43:836-842.
Quinton MB, Nelson CA. Concepts & Guidelines for Baby Treatment. Clinician´s view, Albuquerque, New Mexico; 2002.
Resnick MB, Eyler FD, Nelson RM, Eitzman DV, Bucciarelli RL. Developmental Intervention for low birth weight infants: Improved early developmental outcome. Pediatrics 1987;80:68-74.
Reynders K. [Kinderrevalidatie in pedagogisch per-spectief] Educational perspective on child rehabilitation. Groningen, The Netherlands, Stichting Kinderstudies; 1992 (PhD-thesis).
Rosenbaum P, King S, Law M, King G, Evans J. Family-centred service: A conceptual framework and research review. Phys Occup Ther Pediatr 1998;18:1-20.
Spittle AJ, Orton J, Doyle LW, Boyd R. Early de-velopmental intervention programs post hospital discharge to prevent motor and cognitive impair-ments in preterm infants. Cochrane Database Syst Rev 2007;18:CD005495.
C H a P t E r 6
dI f f e r e nc e s be t w e e n
t h e fA m I ly-c e n t e r e d
P ro g r A m “c oP I ng A n d
c A r I ng f or I n fA n t s
w I t h s P e c I A l n e e d s”
A n d I n fA n t t r e At m e n t
b A s e d on P r I nc I P l e s
of u rode V e l oPm e n tA l
t r e At m e n t --------------------------------------------------------------------------------------------------------------
Tineke Dirks, Cornill H. Blauw-Hospers, Lily J. Hulshof, and Mijna Hadders-Algra
Submitted for publication
106 107
abstract
Background. Evidence for effectiveness of pediatric physical therapy in infants at high risk for
developmental motor disorders is limited. Therefore, we have developed the early intervention
program COPCA: COPing with and CAring for infants with special needs – a family-centered
program. COPCA is based on two components: 1) family involvement and educational parenting,
2) the neuromotor principles of the Neuronal Group Selection Theory. The COPCA coach uses
principles of coaching to encourage the family’s own capacities for solving problems of daily care
and incorporate variation, along with trial and error in daily activities.
Objective. To evaluate whether the content of COPCA sessions differs from that of traditional
infant physical (TIP) therapy sessions.
Design. Quantitative video analysis of therapy sessions with infants participating in a randomized
controlled trial.
Subjects and methods. Forty-six high-risk infants were randomly assigned to receive COPCA
(n=21) or TIP (n=25) between 3 and 6 months corrected age (CA). TIP in the Netherlands is gene-
rally based on NeuroDevelopmental Treatment (NDT) principles. Intervention sessions were
videotaped at 4 and 6 months CA, and analyzed with a standardized observation protocol for the
classification of physiotherapeutic (PT) actions. Outcome parameters were relative amounts of
time spent on specific PT actions.
results. The content of COPCA and TIP differed substantially. For instance, in TIP sessions 20
more time was spent on facilitation techniques, including handling (29% vs. 3%, p<0.001) than in
COPCA sessions. During COPCA more time was spent on family coaching and education (16% vs.
4%, p<0.001) than during TIP.
Conclusion. COPCA differs broadly from TIP in terms of its NDT basis, justifying the label “novel
program.” Studies on the effectiveness of this family-centered program are required.
Introduction
Worldwide, therapists are trained in specialized infant treatment based on the principles of the
NeuroDevelopmental treatment (NDT) approach. The original philosophy – the basic assump-
tions and clinical concepts of NDT in infancy – can be attributed to Karl and Bertha Bobath
(Bobath 1967) and Elsbeth Köng (Köng 1966), whereas Mary Quintin was responsible for a major
part of the practical implementation of the Bobath principles in infant treatment (Bly 1999).
However, daily practice of the approach in different countries and healthcare settings reveals that,
since then, numerous modifications and changes in the implementation of infant treatment have
occurred.
Notwithstanding the occurrence of substantial changes in NDT treatment in infancy, three
recent systematic reviews on the effect of early intervention in infants at high risk for develop-
mental disorders indicated that application of NDT does not result in improved developmental
outcome (Blauw-Hospers and Hadders-Algra 2005, Blauw-Hospers et al 2007, Spittle et al 2007).
The reviews also indicated that best results are achieved by application of specific motor-training
programs and general developmental programs.
These findings and novel insights into the biological and psychological principles governing
motor development after a lesion of the brain at early age (Hadders-Algra 2000b, Hadders-Algra
2008b, Diamond 2009), along with an evolving shift in the manner in which family-centered
services (FCS) are delivered, have inspired us to develop the COPCA program (Dirks and Hadders-
Algra 2003). During the last few decades it has become clear that “family-centered” is a crucial
aspect of interventions applied in infants and young children (Als 1992, Rosenbaum et al 1992,
Dunst and Trivette 1996, McBride and Petersen 1997, Law et al 1998, King et al 2004, Rosenbaum
2004, Sanders et al 2004, Nijhuis et al 2007).
COPCA, that is, COPing with and CAring for infants with special needs, a family-centered
program, is an intervention program for families of infants at high risk for developmental motor
disorders after term age. The theoretical contents of COPCA differ broadly from Traditional
Infant Physical Therapy (TIP) based on NDT (see Table 6.1 for an overview). Before we move on to
the actual study, we should first summarize the principles of the COPCA program and TIP based
on NDT.
COPCa
COPCA is rooted in the framework of the International Classification of Functioning, Disabil-
ity and Health for Children and Youth (World Health Organisation 2007). It aims to promote
activities and participation of the family, including the infant with special needs, while taking
into account the limitations imposed by the infant’s bodily impairments. COPCA consists of two
components:
1. A family involvement and educational parenting component in which the key elements are: a)
family autonomy in decision-making processes and family responsibility for the quality of life
(Law et al 1998) and b) family-specific education, that is, the family-specific styles of parents for

108 109
educating the child to independency and personal responsibility. This means that COPCA not
only respects the autonomy of the family in the process of parenting, but also values the role of
the individual characteristics of both caregiver and child within the process (Scarr 2001, Sanders
et al 2004).
2. A neurodevelopmental component based on the principles of the Neuronal Group Selection
Theory (Edelman 1989).
The major aims of COPCA, which are listed below, are closely related to these two components.
1. The family involvement and educational component
A fundamental idea of COPCA is the transactional perspective on patterns of reciprocal contin-
gent interactions between caregiver, siblings, and infant, along with the notion that changing pat-
terns of behavior are a characteristic of early development (Fiese 1997, De Weerth and Van Geert
2002). This means that the family is regarded as a dynamic system of bidirectional dyads. The
family itself is nested in a larger system including societal influences, socioeconomic factors, and
current living conditions (Bronfenbrenner 1967). COPCA aims to encourage family responsive-
ness, in other words, it aims to promote the capacity of those involved in the family relationships
in order to respond appropriately to each other’s signals, communication, and changing states.
In the case of infants with special needs, responsiveness includes the caregiver’s recognition of
the signals of the infant and the caregiver’s responses to the actual needs of the infant, and not
to preconceived ideas of what the baby might need (Mahoney 1998). To achieve these goals, the
principles of coaching are used. The term “coaching” has various connotations. For instance, Als
(1992) uses verbal and non-verbal coaching strategies to instruct parents in the neonatal intensive
care unit on how to observe and analyze the infant’s neurobehavior and to hold, handle, feed, and
bathe the infant. In NDT, treatment coaching is used to teach parents special therapeutic skills
such as handling. NDT provides parents with references about what the therapist is doing and
furnishes parental assignments while the therapist treats the infant (Howle 2002). The therapist
uses parent training to teach parents what they have to do or could do in daily care activities.
In COPCA, coaching implies the promotion of creative exploration of the competencies of the
family members, including the infant with special needs, in order to stimulate self-made decisions
and improve the quality of life (Hamlin et al 2009). In other words, COPCA encourages families to
follow their own ideas. This is a strategy that fits the following parental expression. “Don’t tell me
what I can do, have to do, or must do; help me to discover it by myself.” This also implies that the
coach does not have an instructional role but instead supports family members on the basis of an
ongoing equal partnership in order to reveal their competencies, goals, desires, and hopes. To this
end, the coach uses focused bidirectional, nuanced, and detailed conversations. An important as-
pect of the process of coaching is the unconditional acceptance of the responsibility of the family.
COPCA coaches the family by creating a process in which the family’s needs and wants are
translated into solutions for how to cope with the problems related to the infant’s development,
while respecting the roles, culture, traditions, and routines of the family (Fiese 1997), along with
the family’s own educational perspective. The coach listens, informs, and observes while the
caregiver is involved in daily routines with the child, including play, thereby creating a situation
in which the caregivers feel free to explore and discuss alternative strategies. Specific attention is
paid to the role of siblings in care and play, along with sibling well-being. The above implies that
COPCA is not a program in which professionals, parents, or others are engaged in “treating” the
infant. COPCA is a family-centered program for professionals involved in the care of infants with
special needs such as physical therapists. The aim of the program is to encourage the family’s
own capacities for solving the problems of daily care in naturally occurring parenting situations.
Therefore, the program is delivered preferably in the home environment. Our primary target as
far as professionals are concerned is pediatric physical therapists, since infants at high risk for
motor disorders are generally referred to these professionals. However, other professionals, such
as nurses, special educators, social workers, or occupational therapists could also become COPCA
coaches. To underline the importance of coaching, we would rather call the professional applying
the COPCA program a “coach” rather than a “therapist.”
The problems of parenting are often complex and may vary from concerns about the infant’s
future locomotor development, feeding difficulties, and choice of toys, to concerns about under-
standing infant behavior and educational problems such as to what extent should a parent inter-
fere with the infant’s actions or whether siblings should be allowed to play with the infant. Other
factors which may contribute to family distress are social issues such as time management (how
to distribute time between child, siblings, partner, family, friends, work, etc.) and concerns about
service delivery.
COPCA acknowledges that raising a child is a life-long challenge. Raising an infant with
special needs due to an early lesion of the brain and/or neurological dysfunction adds to this
challenge (Brehaut et al 2004, Raina et al 2005). Some examples of additional challenges which
caregivers of infants with special needs may encounter and the way COPCA coaches deal with
them are:
• The uncertain developmental of an infant with neurological dysfunction and/or an early lesion
of the brain may induce parental stress (Rentinck et al 2007). Coaching addresses these uncer-
tainties about the child’s health, prognosis, and need for special services. The family members
are encouraged to improve their personal coping skills.
• Stress may be associated with processes of bereavement – the mourning associated with the
loss of the prospect of a typically developing child – when the chances of persisting disability
are high (Kearney and Griffin 2001). Typically the process of mourning is a step-by-step process,
involving cycles of feelings of disappointment, sadness, grief, anger, and guilt, which occur each
time that caregivers realize that the future prospects have to be adjusted once again. COPCA
focuses on discussing these processes with family members and encouraging the family to accept
and express feelings of bereavement. COPCA coaches highlight the family’s own strengths and
capacities, and discuss the possibility of external sources of support such as relatives, neighbor-
hood, friends, or the religious community, or the option of professional help.

110 111
• The infant’s neurological dysfunction may induce atypical infant behavior which may inter-
fere with intuitive parenting capacities (Papousek and Papousek 1984). COPCA focuses on the
promotion and restoration of the intuitive parenting capacities by explaining to caregivers the
mechanisms of caregiver-infant interaction and the effect of neurological dysfunction on this
interaction (Sameroff and McKenzie 2003). It also stresses that parenting is a developmental
process involving trial and error, in addition to life-long learning on the part of both caregiver
and child (Cowan 1998). Specific attention is paid to educational actions, including play in child-
preferred activities whereby the motor principles of NGST are taken into account.
• The infant’s neurological dysfunction and/or an early lesion of the brain may result in atypical
motor development. This may introduce the need for additional equipment such as a special
chair or a supporting device for walking. COPCA coaches inform and discuss with caregivers the
possible strategies and options for handling these additional needs, and it is here that the motor
principles of NGST are taken into account.
• The prospect of having a child with a persisting disability introduces many practical and emo-
tional problems into the family, problems which may vary from practical care issues for the child
with special needs to dealing with service providers and organizing technical adaptations to the
living environment (Raina et al 2005). COPCA focuses on coaching the family members in such
a way that they are fully able to participate in the community, including the practical problems
related to the presence of an infant with special needs.
In general, pediatric physical therapists are trained in addressing issues of motor development
and motor dysfunction, while at the same time providing their work within the framework of
family-centered philosophy (Bly 1999, Chiarello and Effgen 2006). Nevertheless, translation of the
principles of family-centered services into the actual behavior of service providers in an appropri-
ate family-centered approach may be difficult (O’Neill and Palisano 2000, Nijhuis et al 2007). This
is illustrated by the findings of O’Neil and coworkers (2000) which suggest that therapists who be-
lieve in family-centered care consider the aspects of functional activities and child characteristics
– reflective of a child-focused perspective – as being of paramount importance in clinical decision
making. COPCA’s perspective on family-centered care is to empower the family to use their own
competences and problem-solving skills in the process of coping with the daily task of caring for
and rearing a child with special needs. This implies a shift from family-centered care with a child
focused perspective to a family-relationship-focused perspective in which the motor principles of
NGST are only one of the elements taken into account
COPCA recognizes that professionals may perceive limitations in the coaching approach, since
family autonomy implies limitations in terms of the extent to which educational action problems
and difficulties in the community may be resolved. In those cases where the infant has complex
morbidity, for instance, motor dysfunction associated with serious feeding, speech, and language
problems, low vision, or in those cases where a need for additional equipment arises, the COPCA
coach functions as one of the members of the interdisciplinary team involved in guiding the family.
2. The Neurodevelopmental component: NGST
According to NGST, typical motor development is characterized by two phases of variability: the
phases of primary and secondary variability. The borders of variability are determined by genetic
instructions (Edelman 1989, Hadders-Algra 2000a, 2008a). During the phase of primary vari-
ability, motor behavior is characterized by abundant variation. The motor variations represent a
fundamental developmental phenomenon; they are brought about by explorative activity of the
nervous system. The exploration generates a wealth of self-produced afferent information which,
in turn, is used for further shaping of the nervous system. At that stage, the afferent information
is not used for adaptation of motor behavior to environmental constraints. In other words, the
phase of primary variability is characterized by variable but non-adaptive motor behavior.
At a certain point in time, the nervous system is able to use the afferent information produced
by behavior and experience in order to select the motor behavior which fits the specific situation
best; the phase of secondary or adaptive variability then starts. This selection process is based on
active self-produced sensorimotor trial and error experiences. The transition from primary to
secondary variability occurs at function-specific ages. For instance, in the development of sucking
behavior the phase of secondary variability starts prior to term age, and in the development of foot-
placing during walking it starts between 12 and 18 months (Hadders-Algra 2000a). Around the age
of 18 months all basic motor functions have reached the first stages of secondary variability.
Due to the ingenious interaction between self-produced motor activities with trial and error
learning and the long lasting developmental processes in the brain, it takes until the age of 18
to 20 years before the secondary neural repertoire has obtained its mature, adult configuration
(Hadders-Algra 2008a).
In terms of NGST an early lesion of the brain has two major consequences (Hadders-Algra
2000b, 2008b). First, the repertoire of motor strategies is reduced. This results in less variable
and more stereotyped motor behavior. In addition, infants with a prenatally, perinatally, or early
postnatally acquired lesion or malformation of the brain have problems with the selection of the
most appropriately adapted strategy out of the repertoire. The selection problems have a dual
origin: they are related to the deficits in the processing of sensory information and to the fact that
the best solution may not be available due to repertoire reduction.
The practical consequences of the above-mentioned problems are twofold. First, the limited
motor repertoire may result in the absence of a specific motor strategy which would be available
as the best solution in a specific situation for a typically developing infant. Due to absence of the
“best” solution, the infant with an early lesion of the brain may have to choose a motor solution
which differs from that of the typically developing infant. This implies that the different motor
behavior of an infant with an early lesion of the brain should not a priori be regarded as deviant,
that is, as something which deserves to be “treated away,” as it may be the infant’s best and most
adaptive solution for the situation (Latash and Anson 1996). Second, due to the deficits in the
processing of sensory information which hamper the process of selection of the best strategy,
infants with an early lesion of the brain need ten- to a hundredfold more active motor experience
112 113
than typically developing children (Valvano and Newell 1998).
Translating NGST principles into daily practice of the COPCA program means that the
COPCA coach will inform and coach family members while taking into account the family’s
educational perspective. Family members receive suggestions for incorporating variation and trial
and error in daily activities, since this might enhance the infant’s motor repertoire and promote
the ability to select the best strategy for different conditions. This also implies that COPCA is
characterized by being “hands-off.” Some examples of variation in activities are those variations in
which the infant is challenged to produce self-initiated motor behavior in natural daily situations
such as playing, bathing, or sitting. In addition, suggestions are provided about various ways the
infant may be encouraged to explore the limits of its growing capacities. Interestingly, typical play
with siblings usually is an excellent means of promoting sensorimotor challenge, variation, and
exploration. At the same time, family members are informed about the basic principles of atypi-
cal development. The guidelines are: a) the notion that the appearance of motor behavior of the
child with special needs may differ from that of a typically developing child, but that this does not
matter as it is functional performance that counts; and b) the idea that development implies trial
and error during self-produced activity, in other words, that “error” production does not mean
failure but the presence of an active learning process, where learning may be enhanced by verbal
encouragement or non-verbal expressions of affection (e.g., hugging, touching, or tickling) by the
caregiver. The notions of NGST are not taught but discussed by means of bi-directional, equiva-
lent, and deliberate conversation, in line with the family involvement and educational component
of COPCA.
tIP based on NDt
TIP based on NDT is a multidisciplinary approach which primarily focuses on limitations
imposed by bodily impairments and functional activities of the infant with special needs. The as-
sumptions of the approach can be summarized with the help of these two major components:
1. Neurodevelopmental principles which consist of a mix of neuromaturational assumptions,
sensorimotor problem-solving strategies resembling those based on NGST, and the principles
of dynamic systems. The therapist plays a key role in the application of these principles due to
her/his instructional qualities of specific handling techniques and experiences. The therapist
teaches the infant to engage in developmental activities by providing sensorimotor experiences
accompanied by manual guidance, toys, a bolster, or a ball (Bly 1999, Howle 2002).
2. The family. The role of the family in the planning of the treatment program has been eloquent-
ly expressed by Bly (1999): “The family members are obviously the most important people on
the baby’s team” and “The more involved the family becomes, the more consistent therapeutic
management becomes for the baby” (p. 8).
The major aims of TIP based on NDT, which are listed below, are closely related to these two
components.
1. The neurodevelopmental component
In NDT the understanding of how typical developmental changes across a lifespan provides a
critical framework for the problem-solving approach and the planning of treatment. Development
is understood as an interplay between endogenous maturational processes and the infant’s own
environment. NDT uses problem solving to identify missing or atypical elements of functional
movements and posture in infants with a prenatally, perinatally, or early postnatally acquired le-
sion or malformation of the brain (Howle 2002).
The process of the guidance of an infant starts with the examination of functional limita-
tions. Next, on the basis of proposed relationships between limitations, intervention strategies are
systematically planned and applied. NDT emphasizes the individual as a whole with his/her own
competencies and limitations. The current enablement model of NDT addresses these competen-
cies and limitations – in line with the ICF-CY – in body, motor, individual, and social dimensions.
In infant treatment NDT emphasizes impairment as the starting point of therapeutic guidance
and improvement of impairment as a means to facilitate activity and participation (Bly 1999).
According to Mayston (2001) the basic philosophy underlying the sensorimotor deficits of the
infant with a brain lesion are pathophysiological insights into the mechanisms underlying the
problems in the coordination of posture and movement combined with atypical qualities of mus-
cle tone. The problems contribute directly to functional limitations. The impairments of function
can be classified into primary impairments, that is, those impairments that result directly from
the neuropathology along with secondary impairments. Two forms of primary impairments can
be distinguished: positive impairments such as spasticity and deficits in postural control, and
negative impairments such as muscle weakness and changes in muscle length. Those impairments
that are associated with atypical interactions within and between neural and body systems and
other environmental influences, such as contractures and atrophy, are classified as secondary im-
pairments (Howle 2002). For the implementation of NDT in daily practice this means that a broad
repertoire of tone-influencing facilitation techniques such as handling are used to reduce atypical
functional activities and to prepare the infant for optimally independent function.
Bly (1999) emphasized the importance of tactile, proprioceptive, kinesthetic, and vestibular
sensory input and the integration with the motor system in infant treatment based on NDT. The
sensory input enables the infant to perform movements and postural adjustments, and to learn
and use motor skills. Therefore, assessment of the infant must include attention to the sensory
system and treatment must include techniques that integrate sensory input with motor control.
The forms of NDT able to achieve this most precisely are the facilitation techniques of handling,
intermittent pressure, and tactile and vestibular stimulation. The hands of the therapist are used
to control sensory input, motor output, and muscle tone in such a way that the infant with neuro-
logical dysfunction gains an experience of typical movements and movement sequences with the
aim of enhancing the infant’s development of learning skills (Bly 1999).
At the same time the approach recognizes that typical development of postural control and
movements relies on the concept of dynamic systems (Thelen et al 1993). According to dynamic sys-
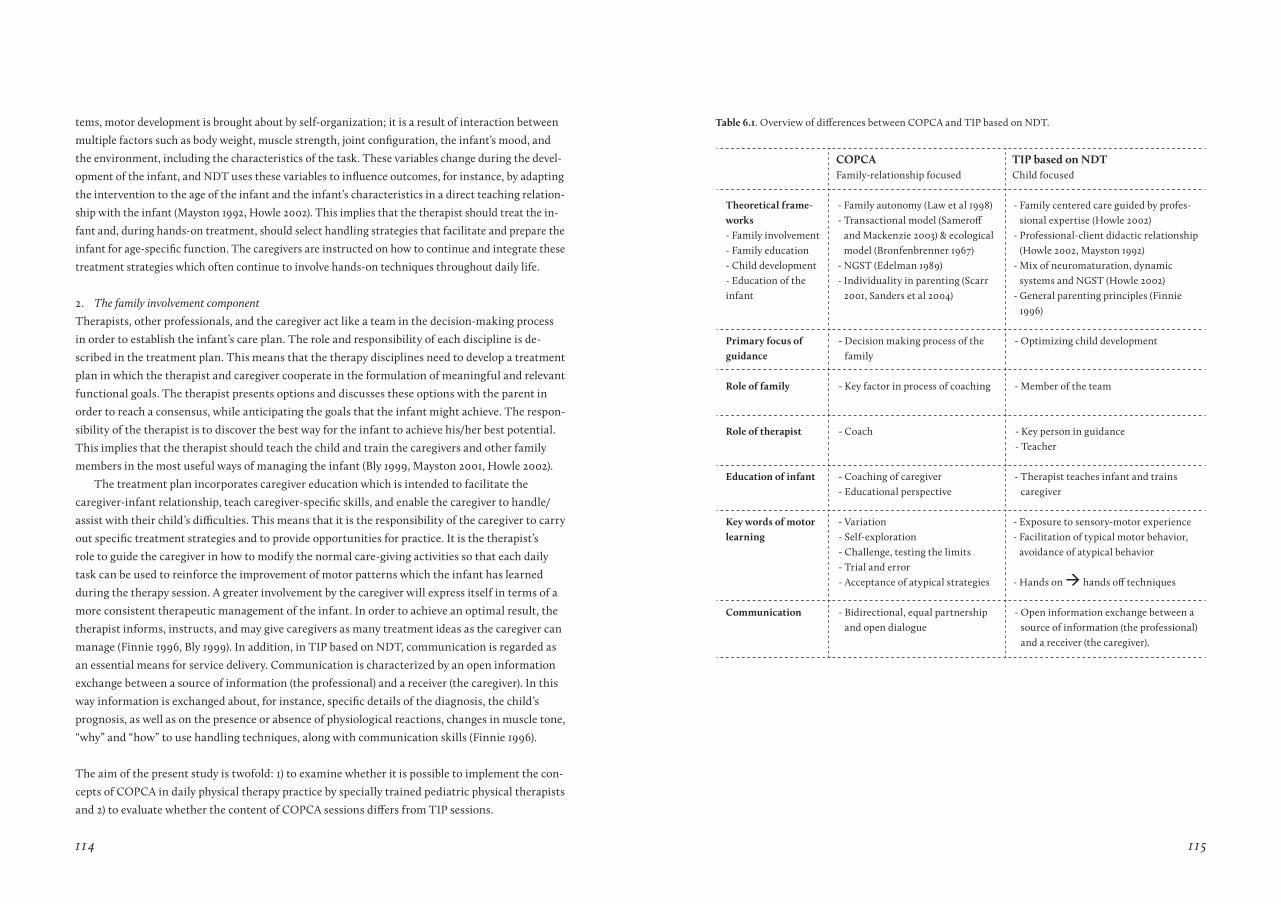
114 115
tems, motor development is brought about by self-organization; it is a result of interaction between
multiple factors such as body weight, muscle strength, joint configuration, the infant’s mood, and
the environment, including the characteristics of the task. These variables change during the devel-
opment of the infant, and NDT uses these variables to influence outcomes, for instance, by adapting
the intervention to the age of the infant and the infant’s characteristics in a direct teaching relation-
ship with the infant (Mayston 1992, Howle 2002). This implies that the therapist should treat the in-
fant and, during hands-on treatment, should select handling strategies that facilitate and prepare the
infant for age-specific function. The caregivers are instructed on how to continue and integrate these
treatment strategies which often continue to involve hands-on techniques throughout daily life.
2. The family involvement component
Therapists, other professionals, and the caregiver act like a team in the decision-making process
in order to establish the infant’s care plan. The role and responsibility of each discipline is de-
scribed in the treatment plan. This means that the therapy disciplines need to develop a treatment
plan in which the therapist and caregiver cooperate in the formulation of meaningful and relevant
functional goals. The therapist presents options and discusses these options with the parent in
order to reach a consensus, while anticipating the goals that the infant might achieve. The respon-
sibility of the therapist is to discover the best way for the infant to achieve his/her best potential.
This implies that the therapist should teach the child and train the caregivers and other family
members in the most useful ways of managing the infant (Bly 1999, Mayston 2001, Howle 2002).
The treatment plan incorporates caregiver education which is intended to facilitate the
caregiver-infant relationship, teach caregiver-specific skills, and enable the caregiver to handle/
assist with their child’s difficulties. This means that it is the responsibility of the caregiver to carry
out specific treatment strategies and to provide opportunities for practice. It is the therapist’s
role to guide the caregiver in how to modify the normal care-giving activities so that each daily
task can be used to reinforce the improvement of motor patterns which the infant has learned
during the therapy session. A greater involvement by the caregiver will express itself in terms of a
more consistent therapeutic management of the infant. In order to achieve an optimal result, the
therapist informs, instructs, and may give caregivers as many treatment ideas as the caregiver can
manage (Finnie 1996, Bly 1999). In addition, in TIP based on NDT, communication is regarded as
an essential means for service delivery. Communication is characterized by an open information
exchange between a source of information (the professional) and a receiver (the caregiver). In this
way information is exchanged about, for instance, specific details of the diagnosis, the child’s
prognosis, as well as on the presence or absence of physiological reactions, changes in muscle tone,
“why” and “how” to use handling techniques, along with communication skills (Finnie 1996).
The aim of the present study is twofold: 1) to examine whether it is possible to implement the con-
cepts of COPCA in daily physical therapy practice by specially trained pediatric physical therapists
and 2) to evaluate whether the content of COPCA sessions differs from TIP sessions.
table 6.1. Overview of differences between COPCA and TIP based on NDT.
COPCaFamily-relationship focused
tIP based on NDtChild focused
theoretical frame-works- Family involvement- Family education- Child development- Education of the infant
- Family autonomy (Law et al 1998)- Transactional model (Sameroff
and Mackenzie 2003) & ecological model (Bronfenbrenner 1967)
- NGST (Edelman 1989)- Individuality in parenting (Scarr
2001, Sanders et al 2004)
- Family centered care guided by profes-sional expertise (Howle 2002)
- Professional-client didactic relationship (Howle 2002, Mayston 1992)
- Mix of neuromaturation, dynamic systems and NGST (Howle 2002)
- General parenting principles (Finnie 1996)
Primary focus of guidance
- Decision making process of the family
- Optimizing child development
role of family - Key factor in process of coaching - Member of the team
role of therapist - Coach - Key person in guidance- Teacher
Education of infant - Coaching of caregiver - Educational perspective
- Therapist teaches infant and trains caregiver
Key words of motor learning
- Variation- Self-exploration- Challenge, testing the limits- Trial and error- Acceptance of atypical strategies
- Exposure to sensory-motor experience- Facilitation of typical motor behavior,
avoidance of atypical behavior
- Hands on hands off techniques
Communication - Bidirectional, equal partnership and open dialogue
- Open information exchange between a source of information (the professional) and a receiver (the caregiver).

116 117
Method
Subjects
Forty-six infants, who had been admitted to the Neonatal Intensive Care Unit (NICU) of the Uni-
versity Medical Center Groningen between March 2003 and May 2005 and who presented at the
age of ten weeks corrected age with definitely abnormal general movements (GMs), were included
in the study. GM assessment was carried out by MH-A and neonatologist AFB, who agreed on the
infant’s GM quality. The presence of definitely abnormal GMs indicates a high risk for develop-
mental disorder, including CP (Hadders-Algra 2004). Infants with severe congenital anomalies
and infants whose caregivers had insufficient understanding of the Dutch language were excluded
from the study. All caregivers of the infants signed an informed consent and the research project
was approved by the Ethics Committee of the University Medical Center Groningen. The trial was
registered under ISRCTN85728836.
Block randomization (full-term infants blocks of n=2; preterm infants blocks of n=12) alloca-
ted 21 infants to the experimental COPCA group and 25 infants to the control group. The infants
who were randomized into the control group received traditional infant physiotherapy (TIP) on
indication of the pediatrician. As a result, 22 infants were referred to TIP and three infants did not
receive physical therapy. Each group contained two full-term infants; the other infants had been
born preterm at gestational ages which varied from 25 to 36 weeks. Details of perinatal and social
characteristics of both groups are provided in Table 6.2.
The randomized intervention was provided at between 3 and 6 months corrected age (CA).
The COPCA sessions were performed twice a week for one hour in the home environment by
one of four COPCA coaches. The COPCA coaches were certified and registered pediatric physical
therapists who had received specific education in the COPCA program. The educational curricu-
lum of a COPCA course starts off with two days of training in the basic COPCA principles. These
two days include discussions of videos of recent intervention sessions carried out by participants.
Discussion of the videos allows for clarification of key characteristics of COPCA and the differ-
ences between COPCA and TIP. After the introductory two days, training is continued with four
one-day sessions with an interval of six weeks. During the interval, coaches-in-training videotape
their own intervention activities. Again, the videos are the starting point for discussion of how
the principles of COPCA may be applied in daily practice. The COPCA curriculum also involves
obligatory reading. During the study, COPCA coaches continued to receive supervision from the
first author. In earlier phases of their careers, three of the four COPCA coaches had completed the
NDT basic and infant course based on Neurodevelopmental Treatment (NDT) principles. Seven-
teen pediatric physical therapists were involved in the TIP treatment sessions. Sixteen of them
had completed the NDT basic and infant treatment course based on NDT. The frequency of TIP
sessions varied from two to 28 times (median 9), and their duration from 12 to 50 minutes (median
29). The great majority of TIP sessions were also carried out in the home environment (n=20; 91%)
Therapists for both groups had at least five years experience in treating infants and children with
special needs. None of the infants received additional forms of therapeutic guidance.
COPCa (n=21) tIP (n=25)Gender
Male
Female
n (%)n (%)
9 (43)12 (57)
11 (44)14 (56)
Gestational age at birth (wk) median (range) 29 (27-40)
30 (25-39)
Birth weight (g) median (range) 1210 (585-4750)
1143 (635-3460)
Maternal age mean ± SD 30.5 ± 6.2 31.8 ± 4.3
Firstborn child n (%) 12 (57) 13 (52)
Twin pairs n (%) 9 (43) 7 (28)
Abnormal cerebral ultrasound IVH gr. 3-4
PVL gr. 3-4
n (%)n (%)
1 (5) 2 (10)
1 (4) 1 (4)
Cerebral Palsy at 18 months n (%) 5 (24)
5 ( 20)
Maternal education * Low
Middle
High
n (%)n (%)n (%)
3 (14)16 (76) 2 (10)
3 (12)11 (44)11 (44)
* high vs middle + low education: Chi square: p<0.05 SD = standard deviation; wk = weeks; g = gram; gr = grade; IVH, grading according to Volpe (2000) = intraven-tricular haemorrage; PVL, grading according to de Vries et al. (1992) = Periventricular leukomalacia; Levels of education: low = primary education/ junior vocational training, middle = secondary education / senior vocational training, high = university education / vocational colleges.
Video recording and video analysis
At 4 and 6 months CA, a video recording of a physical therapy session was made. To minimize intru-
sion, the camera was positioned as far away from the therapist and infant as possible. Albrecht and
coworkers (2005) demonstrated that video recording scarcely affects the behavior of the people be-
ing filmed. In the COPCA group, one recording was missing at four months and three at six months
due to logistical difficulties. In the TIP group, one recording was missing at four months (logistics)
and one at six months (treatment had already stopped). This resulted in 41 video recordings at four
table 6.2. Perinatal and social characteristics of both study groups.

118 119
months (COPCA n=20, TIP n=21) and 39 recordings at six months (COPCA n=18, TIP n=21).
Two persons, CBH and LH, analyzed the contents of the sessions with a standardized observa-
tion protocol for the classification of PT actions (Blauw-Hospers et al 2010). Both assessors were
blind to group allocation. The analysis was performed with the Noldus software program “The
Observer” (Version 5.0; Noldus, Wageningen, the Netherlands), a program specifically designed for
behavioral observation. The program allows for the quantification of the duration, frequency, and
serial order of defined actions. The therapeutic actions defined in the protocol reflect the specific
components of COPCA and TIP (see Appendix 1, p. 188). The observation protocol classifies PT
actions into eight main categories: A) Family involvement and educational actions; B) Communi-
cation, C) Handling techniques; D) Sensory experience; E) Passive motor experience; F) Self-pro-
duced motor behavior, no interference; G) Challenge to self-produce motor behavior where infant
is allowed to continue activity; and H) Challenge to self-produce motor behavior that flows over
into therapeutic handling. In addition, the position of the infant and the amount of postural sup-
port the infant received during the PT actions was scored. The majority of outcome parameters
resulted in relative amounts of time spent on PT actions. Items from Sections 1 to 3 of Category A
(Family involvement and educational actions, A1 to A3) were categorical data. Categories A and B
describe aspects of family involvement and educational interaction in the intervention programs.
In Categories C to H, the position and postural support parameters deal with the neuromotor
components of treatment.
Previously we demonstrated that inter- and intra-assessor agreement on assessment with the
protocol were satisfactory. The ICCs on the relative duration of actions ranged from 0.76 to 1.00
for inter-assessor agreement and 0.69 to 0.99 for intra-assessor agreement (Blauw-Hospers et al
2010).
Data analysis
Statistical analyses were performed using the computer package SPSS (version 14.0). Non para-
metric statistics were used since none of the variables were normally distributed. The effect of
age was assessed with the Wilcoxon signed rank test. Differences between COPCA and TIP were
evaluated with the Mann-Whitney U test, the Chi-square test or Fisher Exact test. Differences
with a p-value <0.05 were considered statistically significant.
results
Family involvement and educational components of intervention
The caregivers were involved in both types of intervention, albeit in different ways. During TIP
sessions, caregivers were engaged especially in handling, and during COPCA, in playing (Table
6.3). The difference in approach between COPCA and TIP was also reflected in the way the child
was dressed: during TIP, infants were more often undressed than during COPCA, a difference
which reached statistical significance at four months (Table 6.3). In both types of intervention,
mothers were usually present during treatment sessions.
Intervention 4 months 6 monthsCOPCan= 20
tIPn= 21
COPCan= 18
tIPn= 21
Family involvementa.1 Family members involved in intervention session
Mother present only- 13 13 15 11Father present only- 1 1 2 0Both caregivers present, no other family members- 4 3 1 3In addition to parent(s) other family members - present 1
2 4 0 7
a.2 Role of parent, caregiver2
Physical therapist performs treatment by means of - handling
1 15 0 15
Physical therapist performs treatment (handling) - and parent guides attention of infant
0 5 0 5
Parent performs treatment by means of handling. - Physical therapist instructs how to handle
0 1 0 1
Parent and physical therapist act together (hands - off); parent is playing with the infant; physical the-rapist observes parent –infant relationship; parent gives ample opportunities for exploration
13 0 14 0
Parent is playing with infant (hands-off), ample op-- portunities for exploration
6 0 4 0
a.3 Infant dressing3
Dressed- 15 5 9 6Partially dressed- 4 5 6 5Undressed (wearing underwear only)- 1 11 3 10
1 In the current study other persons present were always grandparents. 2. Role of parent, caregiver: small (first three categories) vs large (last two categories). Chi Square p<0.001.3. Infant dressing: Chi Square for trend p<0.001.
table 6.3. Family involvement during COPCA and TIP sessions.

120 121
Inte
rven
tion
t
IPC
OPC
a
4 m
o6
mo
Pool
ed
4 an
d 6
mo
4 m
o6
mo
Pool
ed
4 an
d 6
mo
med
ra
nge
(%)
med
ra
nge
(%)
med
ra
nge
(%)
med
ra
n-ge
(%
)
med
ra
n-ge
(%
)
med
ra
nge
(%)
a. F
amil
y in
volv
emen
t and
Edu
cati
onal
co
mpo
nent
a.4
Edu
cati
onal
act
ion
s4.
1 1-
373.
8 1-
224.
0 1-
3717
.00
-44
12.7
0-3
616
.0**
0-4
4
- C
areg
iver
inte
rfer
es w
ith
in
fant
’s ac
tivi
ties
0.0
0-1
0.0
0-2
0.0
0-2
0.3
0-3
0.9
0-5
0.6*
*0
-5
-
PT
inte
rfer
es w
ith
infa
nt’s
acti
viti
es
2.1
0-3
22.
00
-17
2.1
0-3
20.
40
-80.
20
-70.
2**
0-8
-
PT
gui
des
the
infa
nt0.
00
-10
0.2
0-1
00.
2 0
-10
0.0
0-7
0.0
0-0
0.0*
*0
-7
- P
T g
ives
car
egiv
er t
rain
ing
0.1
0-1
30.
00
-50.
00
-13
0.0
0-3
0.0
0-1
0.0
0-3
-
PT
coa
ches
the
car
egiv
er0.
00
-10.
00
-10.
0 0
-112
.40
-43
11.3
0-3
511
.9**
0-4
3B
. Com
mun
icat
ion
10.5
0-5
515
.60
-45
12.4
0-5
517
.60
-50
14.7
2-52
15.7
0-5
2
- In
form
atio
n ex
chan
ge1.
60
-16
1.3
0-1
41.
40
-16
1.8
0-9
0.9
0-9
1.3
0-9
-
Con
tent
s of
info
rmat
ion
-
Dev
elop
men
tal e
duca
tion
0.7
0-2
01.
40
-31
1.3
0-3
11.
00
-20
2.1
0-3
11.
30
-31
-
Han
dlin
g0.
40
-10
0.3
0-1
40.
4 0
-14
0.0
0-1
0.0
0-0
0.0*
*0
-0
- Va
riat
ion
0.0
0-1
0.3
0-1
40.
0 0
-11.
60
-90.
50
-81.
3**
0-9
0
- A
DL
hand
ling
0.0
0-1
00.
00
-50.
0 0
-10
0.0
0-0
0.0
0-0
0.0*
*0
-0
- A
DL
vari
atio
n0.
00
-00.
00
-00.
0 0
-00.
0
0
-20.
00
-70.
0**
0-7
-
Inst
ruct
-
Ass
ign
0.2
0-3
0.2
0-3
0.2
0-3
0.9
0-1
21.
00
-61.
0**
0-1
2
- G
ive
hint
s0.
00
-40.
00
-10.
0 0
-42.
50
-11
2.1
0-5
2.3*
*0
-11
-
Pro
vide
feed
back
3.5
0-1
73.
10
-11
3.3
0-1
7 3
.70
-14
5.1
0-1
34.
50
-14
-
Impa
rt k
now
ledg
e2.
30
-17
1.4
0-1
01.7
0-1
72.
80
-14
1.7
0-9
1.70
-14
Neu
rom
otor
com
pone
ntC
. Fac
ilit
atio
n te
chn
ique
s 31
.75-
7428
.17-
5428
.6
5-74
2.6
0-4
33.
30
-11
2.9*
*0
-43
- Han
dlin
g 16
.04-
5716
.53-
4216
.3
3-57
0.4
0-3
20.
30
-40.
4**
0-3
2- P
ress
ure
tech
niq
ues
6.3
0-2
55.
30
-24
6.2
0-2
50.
00
-50.
00
-80.
0**
0-8
- Sup
port
dev
ice
0.0
0-2
50.
00
-15
0.0
0-2
50.
00
-51.
80
-50.
0**
0-5
- Tra
nsi
tion
3.6
0-1
74.
01-
163.
8 0
-17
1.8
0-5
0.0
0-1
1.8*
*0
-5D
. Sen
sory
exp
erie
nce
8.5
1-21
6.1
0-3
66.
1 0
-36
1.9
0-1
11.7
0-7
1.8*
*0
-11
E. P
assi
ve m
otor
exp
erie
nce
4.6
0-2
02.
00
-19
2.4
0-2
00.
00
-40.
00
-10.
0**
0-4
4F.
Sel
f-pr
oduc
ed m
otor
beh
avio
r –
no
inte
rfer
ence
21
.30
-43
21.3
1-83
21.3
0-8
141
.02-
7152
.57-
6944
.3**
2-71
G. C
halle
nge
to s
elf-
prod
uced
mot
or b
e-ha
vior
– a
ctio
n co
ntin
ued
by in
fant
15.9
0-3
212
.32-
3813
.2
0-3
835
.23-
8130
.817
-70
31.0
**3-
81
- Lit
tle
vari
atio
n12
.40
-28
8.3
1-30
9.1
0-3
010
.70
-34
2.4
0-4
16.
50
-41
- Lar
ge v
aria
tion
1.3
0-1
60.
00
-27
1.0
0-2
726
.52-
5925
.57-
3725
.8**
2-59
H. C
halle
nge
to s
elf-
prod
uced
mot
or b
e-ha
vior
– w
ith
over
flow
into
han
dlin
g5.
51-
255.
61-
375.
6 0
-37
0.0
0-6
0.0
0-5
0.0*
*0
-6
- Lit
tle
vari
atio
n4.
90
-23
3.7
0-3
74.
9 0
-37
0.0
0-6
0.0
0-1
0.0*
*0
-6- L
arge
var
iati
on0.
00
-25
0.0
0-6
0.0
0-2
50.
00
-10.
00
-40.
00
-4
I. U
nsp
ecifi
ed a
ctio
ns
1.9
0-1
33.
50
-11
3.2
0-1
32.
91-
93.
11-
93.
11-
9
Bol
d in
dica
tes
a si
gnifi
cant
age
-eff
ect,
Man
n W
hitn
ey, p
< 0
.05.
Diff
eren
ces
betw
een
TIP
and
CO
PCA
**
p <
0.01
A
DL
= ac
tivi
ties
of d
aily
life
, Med
= M
edia
n, M
o =
mon
ths
(cor
rect
ed a
ge),
PT
= p
hysi
cal t
hera
pist
.
tabl
e 6.
4. C
onte
nts
of T
IP a
nd C
OPC
A in
terv
enti
on a
t 4 a
nd 6
mon
ths
corr
ecte
d ag
e: p
ropo
rtio
n of
tim
e sp
ent o
n va
riou
s ac
tion
s.
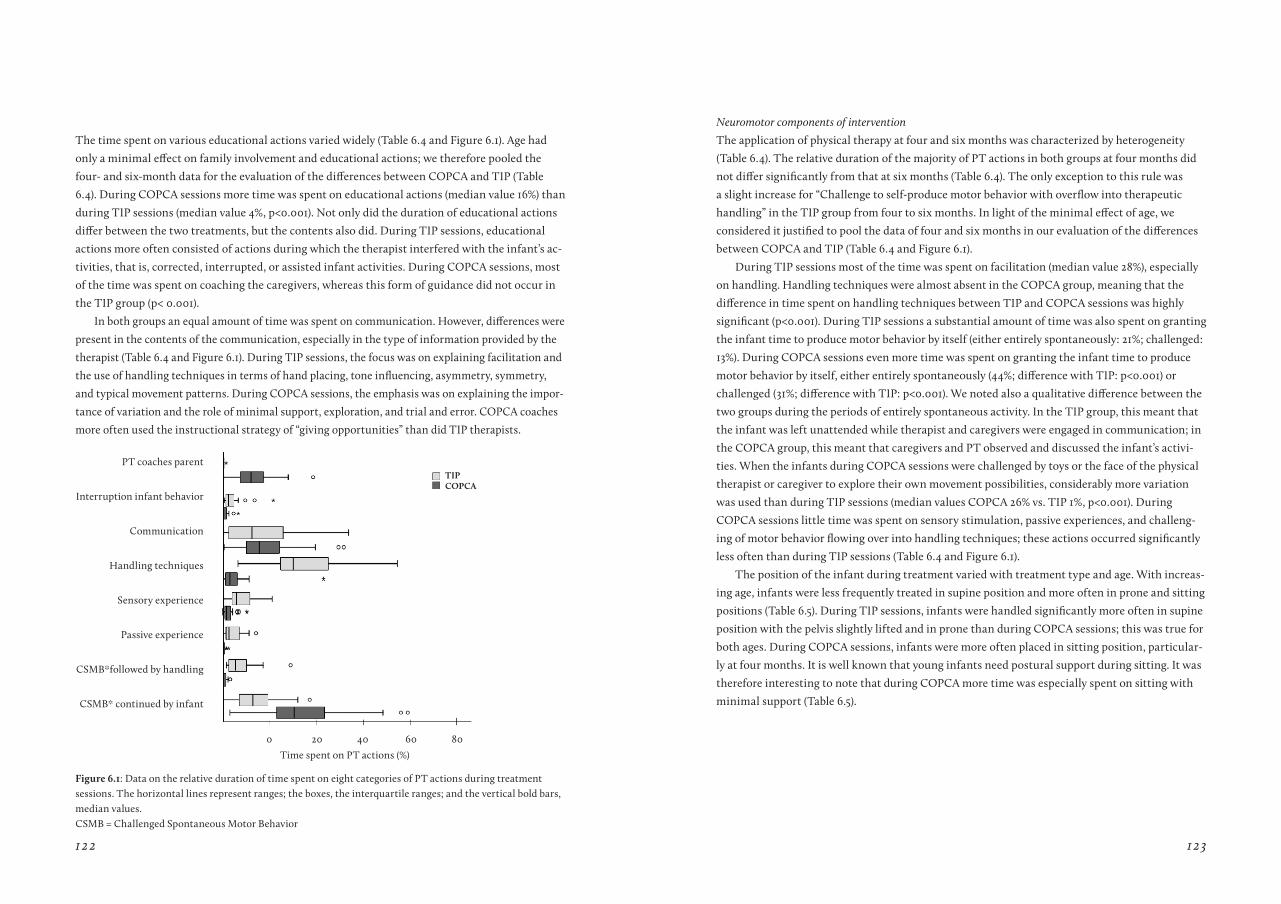
122 123
The time spent on various educational actions varied widely (Table 6.4 and Figure 6.1). Age had
only a minimal effect on family involvement and educational actions; we therefore pooled the
four- and six-month data for the evaluation of the differences between COPCA and TIP (Table
6.4). During COPCA sessions more time was spent on educational actions (median value 16%) than
during TIP sessions (median value 4%, p<0.001). Not only did the duration of educational actions
differ between the two treatments, but the contents also did. During TIP sessions, educational
actions more often consisted of actions during which the therapist interfered with the infant’s ac-
tivities, that is, corrected, interrupted, or assisted infant activities. During COPCA sessions, most
of the time was spent on coaching the caregivers, whereas this form of guidance did not occur in
the TIP group (p< 0.001).
In both groups an equal amount of time was spent on communication. However, differences were
present in the contents of the communication, especially in the type of information provided by the
therapist (Table 6.4 and Figure 6.1). During TIP sessions, the focus was on explaining facilitation and
the use of handling techniques in terms of hand placing, tone influencing, asymmetry, symmetry,
and typical movement patterns. During COPCA sessions, the emphasis was on explaining the impor-
tance of variation and the role of minimal support, exploration, and trial and error. COPCA coaches
more often used the instructional strategy of “giving opportunities” than did TIP therapists.
0 20 40 60 80
PT coaches parent
Interruption infant behavior
Communication
Handling techniques
Sensory experience
Passive experience
CSMB*followed by handling
CSMB* continued by infant
Time spent on PT actions (%)
tIPCOPCa
Figure 6.1: Data on the relative duration of time spent on eight categories of PT actions during treatment sessions. The horizontal lines represent ranges; the boxes, the interquartile ranges; and the vertical bold bars, median values. CSMB = Challenged Spontaneous Motor Behavior
Neuromotor components of intervention
The application of physical therapy at four and six months was characterized by heterogeneity
(Table 6.4). The relative duration of the majority of PT actions in both groups at four months did
not differ significantly from that at six months (Table 6.4). The only exception to this rule was
a slight increase for “Challenge to self-produce motor behavior with overflow into therapeutic
handling” in the TIP group from four to six months. In light of the minimal effect of age, we
considered it justified to pool the data of four and six months in our evaluation of the differences
between COPCA and TIP (Table 6.4 and Figure 6.1).
During TIP sessions most of the time was spent on facilitation (median value 28%), especially
on handling. Handling techniques were almost absent in the COPCA group, meaning that the
difference in time spent on handling techniques between TIP and COPCA sessions was highly
significant (p<0.001). During TIP sessions a substantial amount of time was also spent on granting
the infant time to produce motor behavior by itself (either entirely spontaneously: 21%; challenged:
13%). During COPCA sessions even more time was spent on granting the infant time to produce
motor behavior by itself, either entirely spontaneously (44%; difference with TIP: p<0.001) or
challenged (31%; difference with TIP: p<0.001). We noted also a qualitative difference between the
two groups during the periods of entirely spontaneous activity. In the TIP group, this meant that
the infant was left unattended while therapist and caregivers were engaged in communication; in
the COPCA group, this meant that caregivers and PT observed and discussed the infant’s activi-
ties. When the infants during COPCA sessions were challenged by toys or the face of the physical
therapist or caregiver to explore their own movement possibilities, considerably more variation
was used than during TIP sessions (median values COPCA 26% vs. TIP 1%, p<0.001). During
COPCA sessions little time was spent on sensory stimulation, passive experiences, and challeng-
ing of motor behavior flowing over into handling techniques; these actions occurred significantly
less often than during TIP sessions (Table 6.4 and Figure 6.1).
The position of the infant during treatment varied with treatment type and age. With increas-
ing age, infants were less frequently treated in supine position and more often in prone and sitting
positions (Table 6.5). During TIP sessions, infants were handled significantly more often in supine
position with the pelvis slightly lifted and in prone than during COPCA sessions; this was true for
both ages. During COPCA sessions, infants were more often placed in sitting position, particular-
ly at four months. It is well known that young infants need postural support during sitting. It was
therefore interesting to note that during COPCA more time was especially spent on sitting with
minimal support (Table 6.5).
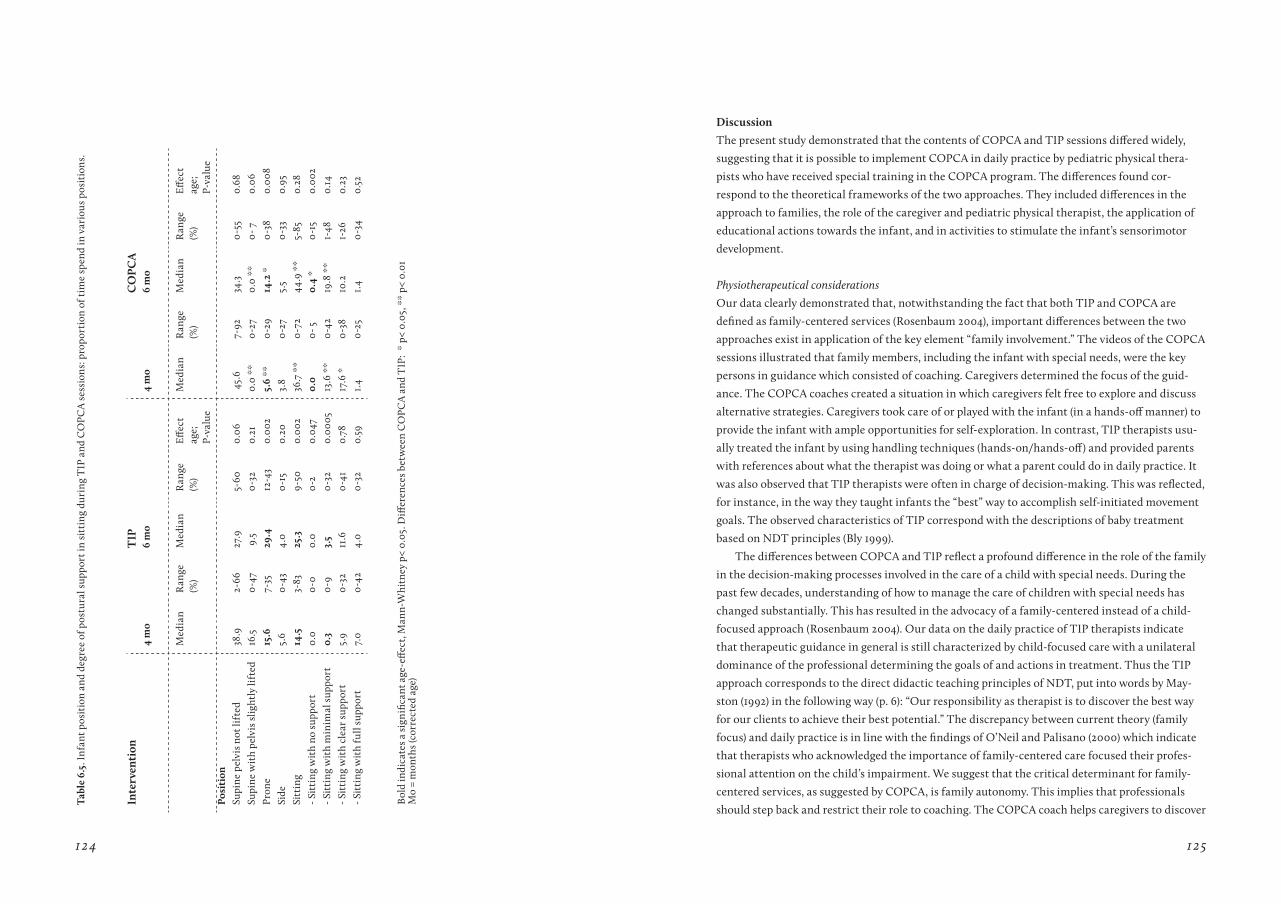
124 125
Inte
rven
tion
tIP
CO
PCa
4 m
o6
mo
4 m
o6
mo
Med
ian
R
ange
(%)
Med
ian
R
ange
(%)
Eff
ect
age;
P-va
lue
Med
ian
R
ange
(%
) M
edia
n
Ran
ge
(%)
Eff
ect
age;
P-va
lue
Posi
tion
Su
pine
pel
vis
not l
ifte
d 38
.92-
6627
.95-
600.
06 4
5.6
7-92
34.3
0-5
50.
68Su
pine
wit
h pe
lvis
slig
htly
lift
ed16
.50
-47
9.5
0-3
20.
210.
0 **
0-2
70.
0 **
0- 7
0.06
Pron
e15
.67-
3529
.412
-43
0.00
25.
6 **
0-2
914
.2 *
0-3
80.
008
Side
5.6
0-4
34.
00
-15
0.20
3.8
0-2
75.
50
-33
0.95
Sitt
ing
14.5
3-83
25.3
9-50
0.00
236
.7 *
*0
-72
44.9
**
5-85
0.28
- Sit
ting
wit
h no
sup
port
0.0
0-0
0.0
0-2
0.04
70.
00
- 50.
4 *
0-1
50.
002
- Sit
ting
wit
h m
inim
al s
uppo
rt0.
30
-93.
50
-32
0.00
0513
.6 *
*0
-42
19.8
**
1-48
0.14
- Sit
ting
wit
h cl
ear
supp
ort
5.9
0-3
211
.60
-41
0.78
17.6
*0
-38
10.2
1-26
0.23
- Sit
ting
wit
h fu
ll su
ppor
t7.
00
-42
4.0
0-3
20.
591.
40
-25
1.4
0-3
4
0.52
Bol
d in
dica
tes
a si
gnifi
cant
age
-eff
ect,
Man
n-W
hitn
ey p
< 0.
05. D
iffer
ence
s be
twee
n C
OPC
A a
nd T
IP:
* p<
0.0
5, *
* p<
0.0
1M
o =
mon
ths
(cor
rect
ed a
ge)
tab
le 6
.5. I
nfa
nt p
osit
ion
and
degr
ee o
f pos
tura
l sup
port
in s
itti
ng d
urin
g T
IP a
nd C
OPC
A s
essi
ons:
pro
port
ion
of t
ime
spen
d in
var
ious
pos
itio
ns.
Discussion
The present study demonstrated that the contents of COPCA and TIP sessions differed widely,
suggesting that it is possible to implement COPCA in daily practice by pediatric physical thera-
pists who have received special training in the COPCA program. The differences found cor-
respond to the theoretical frameworks of the two approaches. They included differences in the
approach to families, the role of the caregiver and pediatric physical therapist, the application of
educational actions towards the infant, and in activities to stimulate the infant’s sensorimotor
development.
Physiotherapeutical considerations
Our data clearly demonstrated that, notwithstanding the fact that both TIP and COPCA are
defined as family-centered services (Rosenbaum 2004), important differences between the two
approaches exist in application of the key element “family involvement.” The videos of the COPCA
sessions illustrated that family members, including the infant with special needs, were the key
persons in guidance which consisted of coaching. Caregivers determined the focus of the guid-
ance. The COPCA coaches created a situation in which caregivers felt free to explore and discuss
alternative strategies. Caregivers took care of or played with the infant (in a hands-off manner) to
provide the infant with ample opportunities for self-exploration. In contrast, TIP therapists usu-
ally treated the infant by using handling techniques (hands-on/hands-off) and provided parents
with references about what the therapist was doing or what a parent could do in daily practice. It
was also observed that TIP therapists were often in charge of decision-making. This was reflected,
for instance, in the way they taught infants the “best” way to accomplish self-initiated movement
goals. The observed characteristics of TIP correspond with the descriptions of baby treatment
based on NDT principles (Bly 1999).
The differences between COPCA and TIP reflect a profound difference in the role of the family
in the decision-making processes involved in the care of a child with special needs. During the
past few decades, understanding of how to manage the care of children with special needs has
changed substantially. This has resulted in the advocacy of a family-centered instead of a child-
focused approach (Rosenbaum 2004). Our data on the daily practice of TIP therapists indicate
that therapeutic guidance in general is still characterized by child-focused care with a unilateral
dominance of the professional determining the goals of and actions in treatment. Thus the TIP
approach corresponds to the direct didactic teaching principles of NDT, put into words by May-
ston (1992) in the following way (p. 6): “Our responsibility as therapist is to discover the best way
for our clients to achieve their best potential.” The discrepancy between current theory (family
focus) and daily practice is in line with the findings of O’Neil and Palisano (2000) which indicate
that therapists who acknowledged the importance of family-centered care focused their profes-
sional attention on the child’s impairment. We suggest that the critical determinant for family-
centered services, as suggested by COPCA, is family autonomy. This implies that professionals
should step back and restrict their role to coaching. The COPCA coach helps caregivers to discover

126 127
and develop their own problem-solving strategies for coping with and caring for the infant with
special needs. The important distinctions between COPCA and TIP are that 1) in COPCA the role
of the family is not restricted to parental involvement in the decision-making in terms of func-
tional treatment goals, and 2) COPCA refrains from teaching caregiver intervention techniques
(Bromwich 1976, Affleck 1982, Mahoney 1998).
The differences observed in activities to stimulate the infants’ sensorimotor development
between the two groups correspond to the theoretical frameworks of the two approaches. The
videos demonstrated that the COPCA approach creates a rich and varied world of opportunities
allowing the infant to explore variable motor behavior (hands-off). A case in point is the challenge
of postural behavior by the provision of as little support as possible. By creating a challenging en-
vironment, the infant may, through active trial and error, experience which motor behavior is the
best he or she can manage. This corresponds to the ideas of NGST. Preliminary results of a study
on the effect of COPCA and TIP on postural development in early infancy suggest that COPCA
may enhance the selection of a functional postural strategy (De Graaf-Peters et al 2007). The TIP
approach also aims at facilitating motor behavior produced by the infant her/himself; however,
our study indicated that TIP therapists frequently incorporated techniques of handling and care-
fully graded stimulation (hands-on). Therapists in the TIP group also applied the basic concept of
NDT to prepare the infant’s motor capacities for a specific function (Mayston 1992). This was, for
instance, reflected in the use of treatment in supine position with the pelvis slightly lifted during
TIP sessions, whereas this type of positioning was virtually absent during COPCA sessions. This
specific handling technique aims to facilitate functional activities such as rolling or reaching and
grasping in the midline, while the therapist controls muscle tone. It should be noted, however,
that the question of how increased muscle tone is related to activity limitations and postural
control is a matter of debate (Damiano 2006, Brogren-Carlberg and Bower 2008). Analogous to
the findings in the family-care domain, our findings in the neuromotor domain match those of
O’Neil and Palissano (2000): Despite the presence of a shift to more functional therapy, therapists
generally pay more attention to movement quality than to functionality so as to achieve a better
long-term outcome. This suggests that the “living concept” approach of NDT – as recognized by
senior NDT tutors – may benefit from a paradigm shift from “quality” (how) to “functionality”
(what) (Mayston 1992).
Methodological considerations
The major strength of the study is the standardized, video-based analysis of the contents of the
two forms of infant physical therapy that allows for an objective quantification of differences
between the two approaches. Other strengths of the study lie in the identical age of the infants at
inclusion in the study, the identical ages at video-assessment, and identical limitations at study
entry, that is, the presence of definitely abnormal GMs. The presence of definitely abnormal GMs
at three months post-term is associated with a high risk of developmental motor disorders such as
cerebral palsy (Prechtl 2001, Hadders-Algra 2004).
It may be considered a weakness that the therapists who applied COPCA had received a specific
COPCA training shortly before the study started, whereas training of the therapists who applied
TIP had taken place at longer and more variable periods prior to study onset. Nevertheless, the
great majority of TIP therapists received certified NDT training including an infant treatment
course. It is well known that therapists practicing NDT, develop a personal, eclectic approach as
their experience increases (Mayston 2008). This was reflected in the variation in percentage of
time spent on specific actions during the treatment sessions – a variation which partly blurred
the contrast between TIP and COPCA. Yet, by using a control group of therapists applying regular
TIP, we were able to demonstrate that the contents of COPCA sessions differed from currently
practiced infant physiotherapy in the Netherlands.
The difference in treatment frequency may be regarded as another limitation, as frequency of
treatment has been associated with outcome (Tsorlakis et al 2004).
At the time of the study, the current design had the highest level of feasibility. In our analysis
of the effect of intervention, we took frequency of treatment into account (Blauw-Hospers et al,
submitted for publication).
Infant physical therapy differs across countries and varies with the cultural context of fami-
lies. This means that the findings of the present Dutch study cannot immediately be generalized
to other countries.
The randomized design of the study was associated with a high degree of similarity for both
groups of infants (Table 6.2). Despite randomization, the level of maternal education differed be-
tween the two groups. This difference may be considered a weakness of the study, since contents
of a treatment session may be affected by the level of maternal education.
Concluding remarks
Bertha and Karl Bobath were well aware of the possibility of future progress in ideas on family
care and motor development. They encouraged therapists to incorporate new ideas into daily ap-
plication of therapy. In a way, one could say that the authors of the COPCA program followed the
advice of the Bobaths. They developed a new program, COPCA. The current study indicates that
COPCA and TIP based on NDT differ widely, justifying the label “novel program.”
Our study underscores the notion that the application of standardized, computer-based video
analysis of treatment sessions is an invaluable tool in the understanding of the daily practice of
pediatric physical therapy. Evaluation of the videos taught us that physical therapists often do
other things than they intended to do (Blauw-Hospers et al 2010). This means that only the evalu-
ation of real action and communication can provide insight into the reality of practice.

128 129
references
Affleck G, McGrade BJ, McQeeney M, Allen D. Promise of relationship-focused early intervention in develop-mental disabilities. J Spec Educ 1982;16:413-430.
Albrecht TL, Ruckdeschel JC, Ray FL 3rd, Pethe BJ, Riddle DL, Strohm J, Penner LA, Coovert MD, Quinn G, Blanchard CG. Portable, Unobtrusive Device for Videorecording Clinical Interactions. Behav Res Meth-ods 2005;37:165-169.
Als A. Individualized, Family-Focused Developmental Care for the Very Low-Birthweight Preterm Infant in the NICU. In Friedman SL and Sigman Sd, eds. The psychological Development of Low Birthweight children. Advances in Applied Developmental Psychology, Vol.6. Norwood: Ablex Publishing, 1992:341-388.
Blauw-Hospers CH, Hadders-Algra M. A systematic review on the effects of early intervention on motor development. Dev Med Child Neurol 2005;47:421-432.
Blauw-Hospers CH, De Graaf-Peters VB, Dirks T, Bos AF, Hadders-Algra M. Does early intervention in in-fants at high risk for a developmental motor disorder improve motor and cognitive development? Neurosci Biohav Rev 2007;31:1201-1212.
Blauw-Hospers CH, Dirks T, Hulshof LJ, Hadders-Algra M. Opening the Black Box of physical therapy in high-infants; development of a quantitative to assess the contents of physical therapy. Pediatr Phys Ther 2010;22:189-198.
Blauw-Hospers CH, Dirks T, Hulshof LJ, Bos AF, Hadders-Algra M. A Randomized Controlled Trial on pediatric physical therapy in infancy: from nightmare to dream. Phys Ther, submitted for publication.
Bly LMA. Baby Treatment based on NDT principles. Austin, TX: Pro-Ed Inc; 1999.
Bobath B. The Very early treatment of Cerebral Palsy. Dev Med Child Neurol 1967;9:373-390.
Brehaut JC, Kohen E, Rainap, Russel DJ, Swinton M, O’donnel M, Rosenbaum P. The health of primary caregivers of children with Cerebral Palsy: How does it compare with that of other Canadian caregivers. Pediatrics 2004; 114;182-191.
Brogren-Carlberg E, Bower E. Management and treat-ment of postural dysfunction in children with cerebral palsy. In: Hadders-Algra M, Bogren Carlberg E, eds. Postural Control; A key issue in developmental disorders. Clin Dev Med No. 179. London: Mac Keith Press; 2008:270-298.
Bromwich R. Focus on maternal behavior in infant intervention. Amer J Orthopsychat 1976; 46; 3: 439-446.
Bronfenbrenner U. The ecology of Human Develop-ment. Cambridge: Harvard University Press 1967.
Chiarello L, Effgen SK. Updated competencies for physical therapists working in early intervention. Pediatr Phys Ther 2006;18:148-158.
Cowan S. Family Life and Self-Esteem. In: Geralis E. ed. Children with Cerebral Palsy: A Parent’s Guide. Bethesda: Woodbine House, Inc.; 1998:147-191.
Damiano DL. Activity, Activity, Activity; Rethinking Our Physical Therapy Approach to Cerebal Palsy. Phys Ther 2006;86:11:1534-1540.
De Graaf-Peters VB, Blauw-Hospers CH, Dirks T, Bakker J, Bos AF, Hadders-Algra M. Development of postural control in typically developing children and children with cerebral palsy: Possibilities for interven-tion? Neurosci Biobehav Rev 2007;31:1191-1200.
De Vries LS, Eken P, Dubowitz LM. The spectrum of leucomalacia using cranial ultrasound. Beh Brain Res 1992;49:1-6.
De Weerth C, Van Geert P. Changing patterns of infant behavior and mother-infant interaction: Intra-and interindividual variability. Infant Beh Dev 2002;24:347-371.
Diamond A. The Interplay of Biology and the environ-ment Broadly Defined. Dev Psychology 2009;45:1-8.
Dirks T, Hadders-Algra M. COPCA working manual. Groningen; 2003.
Dunst CJ, Trivette CM. Empowerment, Effective Help-ing Practices and Family-Centered Care. Ped Nursing 1996; 22-4:334-337.
Edelman GM. Neural Darwinism. The theory of neural group selection. Oxford University Press;1989.
Fiese BH. Family context in pediatric psychology from a transactional perspective; family rituals and stories as examples. Pediatr Psychol 1997;22:183-196.
Finnie NR. Handling the Young Child with Cerebral Palsy at Home. Oxford: Butterworth-Heineman 1996.
Hadders-Algra M. The Neuronal Group Selection Theory; an attractive framework to explain variation in normal motor development. Dev Med Child Neurol 2000a;42:566-572.
Hadders-Algra M. The Neural Group Selection Theory: promising principles for understanding and treating developmental motor disorders. Dev Med Child Neurol 2000b;42:707-715.
Hadders-Algra M. General Movements : a window for early identification of children at high risk for devel-opmental disorders. J Pediatr 2004;145:S12-S18.
Hadders-Algra M. Development of postural control. In: Hadders-Algra M, Brogren Carlberg E, eds. Postural Control; A key issue in developmental disorders. Clin Dev Med No. 179. London: Mac Keith Press; 2008a:22-73.
Hadders-Algra M. The Neuronal Group Selection Theory: a framework to understand typical and atypi-cal motor development. In: LA Ramenghi. P Evrard, E Mercuri, eds. Perinatal brain damage; from pathogen-esis to neuroprotection. Milan: John Libbey Eurotext; 2008b:34-37.
Hamlin RG, Ellinger AD, Beattie RS. Toward a pro-fession of coaching? A definitional examination of ‘Coaching’, Organization Development’, and ‘Human Resource Development’. Int J Ev Based Coach and Mentoring 2009;7:13-38.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association; 2002.
Kearney PM, Griffin T. Between joy and sorrow: being a parent of a child with developmental disability. J Adv Nurse 2001;4:582-592.
King S, Teplicky R, King G, Rosenbaum P. Family-Centered Service for children with cerebral palsy and their families: A review of the literature. Sem in Ped Neur 2004;1:78-86.
Köng E. Very early treatment of cerebral palsy. Dev Med Child Neurol 1966;8:198-202.
Latash Ml, Anson JG. What are “normal movements “in atypical populations? Behav Brain Sci 1996;19:55-68.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Oc-cup Ther Pediatr 1998;18:83-102.
Mahoney G. The relationship of parent-child interac-tion to the effectiveness of early intervention services for at-risk children and childen with disabilities. Top Early Child Spec 1998;18:5-17.
Mayston MJ. The Bobath concept; Evaluation and ap-plication. In Forsberg H, Hirschfeld H. eds. Movement disorder in children. Basel, Medicine and Sport Science/Karger 1992;36:1-6.
Mayston MJ. People with cerebral palsy: effects of and perspectives for therapy. Neur Plast 2001;8:51-69.
Mayston M. Bobath Concept: Bobath@50: mid-life crises – What of the future? Phys Research Inter 2008;13:3;131-136.
McBride SL, Petersen C. Home-Based Early Interven-tion with Families of Children withDisabilities: Who is doing what? Topics in Early Childhood Spec Educ 1997;17;209-232.
130 131
Nijhuis BJG, Reinders-Messelink HA, de Blécourt ACE, Hitters MWMCG, Groothoff JW, Nakken H, Postema K. Family-centered care in Family-specific teams. Clin Reh 2007;21:660-671.
O’Neil E, Palisano RJ. Attitudes toward family-centered care and clinical decision making in early intervention among physical therapists. Ped Phys Ther 2000;12:173-182.
Papousek H, Papousek M. Qualitative transitions in integrative processes during the first trimester of hu-man postpartum life. In: Prechtl HFR, ed. Continuity of neural functions from prenatal to postnatal life. Clin Dev Med No 94; Oxford: Blackwell Scientific Publ.; 1984:220-244.
Prechtl HFR. General movement assessment as a method of developmental neurology: new para-digms and their consequences. Dev Med Child Neurol 2001;43:836-842.
Raina P, O’Donell M, Rosenbaum P, Brehaut J, Walter SD, Swinton M, Zhu B, Wood E. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005;115:626-640.
Rentinck IC, Ketelaar M, Jongmans MC, Gorter JW. Caregiver of children with cerebral palsy, a review of factors related to the processes of adaptation. Child Care Health Dev 2007;33:161-169.
Rosenbaum P, King S, Law M, King G, Evans J. Family-Centered Service: A Conceptual Framework and Research Review. Phys & Occup Ther in Pediatr 1992;18-1:1-20.
Rosenbaum P. Families and service providers: forcing effective connections, and why it matters. In: Scrutton D, Damiano D, Mayston M, eds. Management of the Motor Disorders of Children with Cerebral Palsy. Cam-bridge: Cambridge University Press; 2004:22-31.
Sameroff AJ, Mackenzie MJ. Research strategies for cap-turing transactional models of development; the limits of the possible. Dev Psychopathol 2003;15:613-640.
Sanders MR, Mazzucchelli TG, Studman LJ. Stepping Stones Triple P: the theoretical basis and development of an evidence-based positive parenting program for families with a child who has a disability.Journal of Intell & Dev Disability 2004;29-3:265-283.
Scarr S. Individuality in Parenting Behavior and Chil-dren’s development. In: Gerrits JRM. ed. Dynamics of parenting. Leuven: Gallant; 2001:87-99.
Spittle AJ, Orton J, Doyle LW, Boyd R. Early de-velopmental intervention programs post hospital discharge to prevent motor and cognitive impair-ments in preterm infants. Cochrane Database Syst Rev 2007;18:CD005495.
Thelen E, Corbetta D, Kamm K, Spencer JP, Sch-neider K, Zernicke RF. The transition to reaching: mapping intention and intrinsic dynamics. Child Dev 1993;64:1058-1098.
Tsorlakis N, Evaggelinou C, Grouios G, Tsorbatzoudis C. Effect of intensive Neurodevelopmental treatment in gross motor function of children with cerebral palsy. DevMed Child Neurol 2004;46:740-745.
Valvano J, Newell KM. Practise of a precision isometric grip-force task by children with spastic cerebral palsy. Dev Med Child Neurol 1998;40:464-473.
Volpe JJ. Intracranial hemorrhage. In: Volpe JJ, ed. Neurology of the newborn. Philadelphia: WB Saunders Company; 2000:428-493.
World Health Organisation. International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY). Geneva WHO; 2007.
C H a P t E r 7
P e dI At r Ic P h ys Ic A l
t h e r A P y I n I n fA nc y:
f rom n Ig h t m A r e to
dr e A m ?
A r A n d om I z e d
c on t rol l e d t r I A l ---------------------------------------------------------------------------------------------
Cornill H. Blauw-Hospers MSc, Tineke Dirks PT, Lily J. Hulshof MD,
Arend F. Bos MD, PhD and Mijna Hadders-Algra MD, PhD
Submitted for publication

132 133
abstract
Purpose. To study the effects of a new pediatric physiotherapeutic intervention program on the
development of infants at high risk for developmental disorders. We used a combined approach in
a randomized controlled trial (RCT) and process evaluation.
Subjects and Methods. Forty-six high-risk infants were randomly assigned to receive COPCA
(n=21) or traditional infant physical therapy (TIP; n=25) between three to six months corrected
age (CA). Developmental outcome was assessed at six and 18 months CA with a neurological
examination, AIMS, PEDI, and the mental developmental index (MDI) of the BSID. Contents of
the intervention were analyzed by a quantitative video analysis of therapy sessions. Multivariate
statistics were applied to evaluate associations between intervention and developmental outcome
components.
results. The RCT revealed that developmental outcome in both groups was largely identical, ex-
cept for cognitive outcome. The COPCA group decreased less in MDI score from six to 18 months
CA (106.5 to 100; p=0.07) than the TIP group (115.5 to 98; p=0.001). Process evaluation showed that
typical COPCA actions – 1) family involvement and educational actions, 2) application of a wide
variation in challenging the infant to produce motor behavior by him/herself and allowing the
infant to continue this activity, and 3) stimulation of motor behavior at the limit of the infant’s
capabilities – were associated with a better developmental outcome at 18 months CA. The use of
handling techniques was associated with a lower score on the PEDI.
Conclusion. Extending the RCT by using process evaluation was needed to obtain insight into
associations between the components of intervention and developmental outcome. Specific
components of COPCA were associated with improved outcome, while handling techniques were
associated with worsened functioning.
Introduction
Research has shown that evidence for the effectiveness of pediatric physical therapy on motor and
cognitive development of infants with or at high risk for developmental disorders is inconclusive
(Blauw-Hospers and Hadders-Algra 2005, Blauw-Hospers et al 2007, Spittle et al 2007). However,
early pediatric physical therapy is widely advocated and desired in the management of high-risk
infants. This inconclusiveness may be related to the specific difficulties inherent in studies on
early pediatric physical therapeutic intervention. One important difficulty for these studies is the
heterogeneity of the study group. Early detection of infants at risk for a developmental disorder
implies that the clinical picture of the problems that an infant will eventually develop has not yet
manifested itself. Second, there are many variations in the conditions of families such as social-
economic status and family routines. Another, equally important factor that might explain the
inconclusiveness of results is related to the intervention itself. Treatment application is often ec-
lectic (Howle 2005, Mayston 2005). This would indicate that a broad heterogeneity in implement-
ing a treatment exists, even within treatments that adhere to the same principles (Blauw-Hospers
et al 2010). Pediatric physical therapists tend to include in their treatment those techniques which
they perceive as helpful, while leaving other techniques out. Presumably this heterogeneity in
treatment practice has been brought about by an evolution in treatment techniques and theoreti-
cal assumptions. Finally, the outcome measurements that are chosen to evaluate the effect of an
intervention might not be the appropriate ones. Usually instruments are chosen out of habit, as
well as for practical reasons, and not on the basis of information regarding test accuracy, utility,
and theoretical basis (Ketelaar et al 1998, Heineman and Hadders-Algra 2008).
The best method for controlling the impact of the above-mentioned factors is to evaluate the
effect of intervention in a randomized controlled trial (RCT). RCTs are offered as the most objec-
tive and unbiased design for evaluating intervention programs (Lachin et al 1988). Random alloca-
tion of intervention among the participants ensures that differences in group characteristics that
may affect outcome are minimized. The aim is to have the groups compared as similarly as pos-
sible except for the precisely defined interventions being examined. As in other research designs,
RCTs in pediatric physical therapy also have limitations. RCTs are usually designed to determine
the effect of intervention by measuring the change in developmental outcome previous to and
after the intervention period. Although this is the most straightforward method for measuring ef-
fectiveness, it does not explain the underlying mechanisms that might influence outcome (Watson
et al 2004). Rarely are the contents of pediatric physical therapy programs analyzed despite the
fact that this might serve as an eye-opener in interpreting the results of effectiveness studies. Un-
raveling the components of intervention shows whether the applied intervention is eclectic or not.
Lettinga et al. (2002) stressed the importance of an in-depth understanding of the characteristics
of interventions. They stated that every trial which compares the effects of different types of in-
tervention should start with a detailed analysis of the similarities and differences in the content of
the interventions under study. This analysis will serve as an addition to discovering the effective
and ineffective elements in the interventions, and will consequently result in knowledge about the
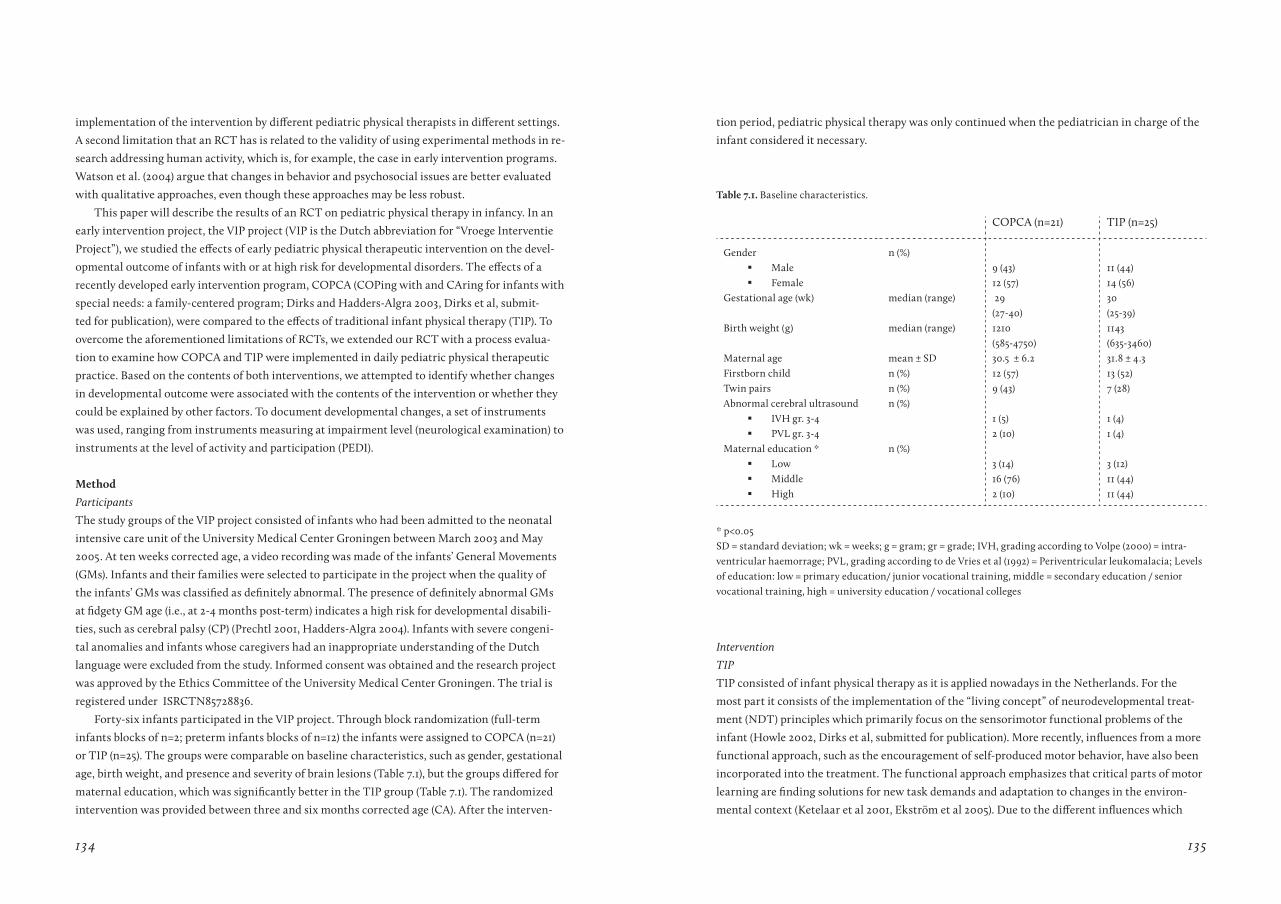
134 135
implementation of the intervention by different pediatric physical therapists in different settings.
A second limitation that an RCT has is related to the validity of using experimental methods in re-
search addressing human activity, which is, for example, the case in early intervention programs.
Watson et al. (2004) argue that changes in behavior and psychosocial issues are better evaluated
with qualitative approaches, even though these approaches may be less robust.
This paper will describe the results of an RCT on pediatric physical therapy in infancy. In an
early intervention project, the VIP project (VIP is the Dutch abbreviation for “Vroege Interventie
Project”), we studied the effects of early pediatric physical therapeutic intervention on the devel-
opmental outcome of infants with or at high risk for developmental disorders. The effects of a
recently developed early intervention program, COPCA (COPing with and CAring for infants with
special needs: a family-centered program; Dirks and Hadders-Algra 2003, Dirks et al, submit-
ted for publication), were compared to the effects of traditional infant physical therapy (TIP). To
overcome the aforementioned limitations of RCTs, we extended our RCT with a process evalua-
tion to examine how COPCA and TIP were implemented in daily pediatric physical therapeutic
practice. Based on the contents of both interventions, we attempted to identify whether changes
in developmental outcome were associated with the contents of the intervention or whether they
could be explained by other factors. To document developmental changes, a set of instruments
was used, ranging from instruments measuring at impairment level (neurological examination) to
instruments at the level of activity and participation (PEDI).
Method
Participants
The study groups of the VIP project consisted of infants who had been admitted to the neonatal
intensive care unit of the University Medical Center Groningen between March 2003 and May
2005. At ten weeks corrected age, a video recording was made of the infants’ General Movements
(GMs). Infants and their families were selected to participate in the project when the quality of
the infants’ GMs was classified as definitely abnormal. The presence of definitely abnormal GMs
at fidgety GM age (i.e., at 2-4 months post-term) indicates a high risk for developmental disabili-
ties, such as cerebral palsy (CP) (Prechtl 2001, Hadders-Algra 2004). Infants with severe congeni-
tal anomalies and infants whose caregivers had an inappropriate understanding of the Dutch
language were excluded from the study. Informed consent was obtained and the research project
was approved by the Ethics Committee of the University Medical Center Groningen. The trial is
registered under ISRCTN85728836.
Forty-six infants participated in the VIP project. Through block randomization (full-term
infants blocks of n=2; preterm infants blocks of n=12) the infants were assigned to COPCA (n=21)
or TIP (n=25). The groups were comparable on baseline characteristics, such as gender, gestational
age, birth weight, and presence and severity of brain lesions (Table 7.1), but the groups differed for
maternal education, which was significantly better in the TIP group (Table 7.1). The randomized
intervention was provided between three and six months corrected age (CA). After the interven-
tion period, pediatric physical therapy was only continued when the pediatrician in charge of the
infant considered it necessary.
* p<0.05SD = standard deviation; wk = weeks; g = gram; gr = grade; IVH, grading according to Volpe (2000) = intra-ventricular haemorrage; PVL, grading according to de Vries et al (1992) = Periventricular leukomalacia; Levels of education: low = primary education/ junior vocational training, middle = secondary education / senior vocational training, high = university education / vocational colleges
COPCA (n=21) TIP (n=25)
Gender Male
Female
n (%)9 (43)12 (57)
11 (44)14 (56)
Gestational age (wk) median (range) 29 (27-40)
30 (25-39)
Birth weight (g) median (range) 1210 (585-4750)
1143 (635-3460)
Maternal age mean ± SD 30.5 ± 6.2 31.8 ± 4.3Firstborn child n (%) 12 (57) 13 (52)Twin pairs n (%) 9 (43) 7 (28)Abnormal cerebral ultrasound
IVH gr. 3-4
PVL gr. 3-4
n (%)1 (5)2 (10)
1 (4)1 (4)
Maternal education * Low
Middle
High
n (%)3 (14)16 (76)2 (10)
3 (12)11 (44)11 (44)
Intervention
TIP
TIP consisted of infant physical therapy as it is applied nowadays in the Netherlands. For the
most part it consists of the implementation of the “living concept” of neurodevelopmental treat-
ment (NDT) principles which primarily focus on the sensorimotor functional problems of the
infant (Howle 2002, Dirks et al, submitted for publication). More recently, influences from a more
functional approach, such as the encouragement of self-produced motor behavior, have also been
incorporated into the treatment. The functional approach emphasizes that critical parts of motor
learning are finding solutions for new task demands and adaptation to changes in the environ-
mental context (Ketelaar et al 2001, Ekström et al 2005). Due to the different influences which
table 7.1. Baseline characteristics.

136 137
have been incorporated into TIP, a broad heterogeneity in treatment applications was expected. In
the TIP group, intervention was applied with a median value of once a week, mainly in the home
environment by the pediatric physical therapist working in the area.
COPCA
COPCA (COPing with and CAring for infants with special needs: a family-centered program)
(Dirks and Hadders-Algra 2003, Dirks et al, submitted for publication) was developed from the
notion that evidence for the effectiveness of the current pediatric physical therapeutic interven-
tion programs was inconsistent. COPCA differs from existing approaches, both in theoretical
background and in implementation (Dirks et al, submitted for publication). It is a family-rela-
tionship-oriented program consisting of two theoretical components. The first is formed by a
family-involvement and educational-parenting component. A fundamental idea of COPCA is the
transactional perspective on family function, in other words, on patterns of reciprocal contingent
interactions between caregiver and infant, with the notion that changing patterns of behavior
are a characteristic of early development (Fiese 1997, De Weerth and Van Geert 2002). This means
that development is seen as a result of a continuous dynamic interplay between child behavior and
caregiver responses to the child’s behavior, along with environmental variables that may influence
both child and caregiver. Caregivers are coached to recognize the infant’s signals and to respond
appropriately to the actual needs of the infant (Dirks et al, submitted for publication). Coaching
implies that the pediatric physical therapist – in the COPCA program, the coach – supports all
family members, including the infant with special needs, in order to reveal their competencies,
goals, desires, and hopes. On the basis of an ongoing equal partnership in which the family defines
the priorities for intervention (Law et al 1998), the coach supports the family in developing their
own ways of caring for the infant and in improving personal coping skills. Specific attention is
paid to educational actions such as spending brief amounts of time playing in child-preferred
activities whereby the motor principles of NGST are taken into account, as well as educational ac-
tions promoting appropriate behavior (Dirks et al, submitted for publication).
The second, equally important, theoretical component of COPCA is a neurodevelopmental
component based on the principles of Neuronal Group Selection Theory (NGST; Edelman 1993).
NGST emphasizes that development is the consequence of a complex interaction between genetic
information and environmental influences. According to NGST, development is characterized by
two phases of variability, that is, primary and secondary variability. During primary variability the
child explores all the variations of motor possibilities that are available in the nervous system. In
this phase the child is not yet able to adjust his behavior to external conditions. In typically devel-
oping infants, this phase is characterized by abundant variation. At function-specific ages the in-
fant reaches the phase of secondary variability, that is, the child gradually learns to select the most
efficient solution for a given task out of his motor repertoire. This selection is based on self-pro-
duced trial and error experiences (Hadders-Algra 2000a). Infants with a prenatally, perinatally, or
early postnatally acquired lesion or malformation of the brain have a reduced repertoire of motor
strategies available for exploration. This is already expressed during the initial postnatal months
by a limited repertoire of general movements and continues when goal-directed motility emerges
(Hadders-Algra 2000b, 2008a). In addition, these infants have problems with the selection of the
most appropriate solution for a certain task out of the repertoire due to deficits in the processing
of sensory information (Hadders-Algra 2000b, 2008a). The aim of COPCA is therefore to promote
self-produced motor behavior (hands-off), variation, and trial-and-error experiences by means of
play, all with the ultimate goal of providing an infant with a wider diversity in terms of neuronal
networks that will help the infant to find an appropriate solution for any given motor task.
COPCA was applied twice a week for one hour at home by one of four specially trained
pediatric physical therapists.
Developmental outcome
The developmental status of the infants was assessed at baseline three months CA and thereafter
at six and 18 months CA. At three and six months, the neurological condition was measured with
the Touwen Infant Neurological Examination (TINE; Hadders-Algra et al 2010). The neurologi-
cal condition was summarized as normal, normal-suboptimal, minor neurological dysfunction
(MND), or as abnormal. The classification of abnormal during early infancy implies the presence
of a distinct neurological syndrome such as a clear hypo- or hypertonia, a hemi syndrome, or a
hyperexcitability syndrome. To distinguish between MND, normal-suboptimal, and normal neu-
rological conditions, the findings of the TINE were classified according to age-specific norms into
five clusters of dysfunction: dysfunctional reaching and grasping, dysfunctional gross motor func-
tion, brain stem dysfunction, visuomotor dysfunction, and sensorimotor dysfunction. Two forms
of normal neurological development could be distinguished: neurologically normal when none of
the clusters met the criteria for dysfunction and normal-suboptimal when one or two clusters ful-
filled the criteria for dysfunction. When more than two clusters fulfilled the criteria for dysfunc-
tion, infants were classified as MND. A recent study has shown that MND can be assessed reliably
with the TINE (Hadders-Algra et al 2010).
At 18 months CA, a neurological assessment was carried out according to Hempel (1993).
The findings of the Hempel assessment were classified as neurologically normal, simple MND,
complex MND, or CP. The distinction between simple and complex MND was also based on the
number of clusters of dysfunction. Note that the clusters of dysfunction of the Hempel assess-
ment are similar to that of TINE but not identical. The criteria for classification also differed for
both assessments. Simple MND at 18 months denotes the presence of one cluster of dysfunction
and complex MND the presence of more than one cluster of dysfunction. The classification CP
implies the presence of a “classical” configuration of neurological signs (Hadders-Algra 2003). Lit-
tle information was available about the concurrent and predictive validity of the Hempel assess-
ment, but the interrater reliability was satisfactory (Hadders-Algra et al 2010).
Additionally, we used the Neurological Optimality Score (NOS; Huisman et al 1995) to sum-
marize neurological condition at 18 months CA. The NOS is the sum of 57 items representing the
138 139
neurological examination that meets predefined criteria for optimality. It is important to realize
that the definition of optimal is narrower than that of normal or typical, and that a reduced
optimality does not always mean abnormal (Prechtl 1980). The NOS has been proven to be an
excellent instrument for evaluating subtle differences in neurodevelopmental outcome (Bouwstra
et al 2006).
Gross motor development was assessed with the Alberta Infant Motor Scale (AIMS; Piper and
Darrah 1994). The AIMS consists of 58 items that evaluate gross motor function in supine, prone,
sitting, and standing positions. Through observation of spontaneous motor behavior, each item
can be scored on three aspects of motor performance: weight bearing, posture, and antigravity
movements. The AIMS has very good reliability coefficients (Piper and Darrah 1994, Heineman
and Hadders-Algra 2008). In addition, the validity of the AIMS has been thoroughly examined and
proven to be satisfactory (Piper and Darrah 1994, Darrah et al 1998, Liao and Campbell 2004).
The cognitive outcome of the infants was assessed at six and 18 months CA using the men-
tal scale of the Dutch version of the Bayley Scales of Infant Development (BSID-II; Bayley 1993,
Van der Meulen et al 2002). The mental developmental index (MDI) consists of items concerning
problem solving, memory, discrimination, classification, language, and social skills. Raw scores
were converted into age-equivalent scores, as derived from the Dutch norms (Van der Meulen et
al 2002). The interrater reliability of the MDI was sufficient; the construct and concurrent validity
were moderate (Heineman and Hadders-Algra 2008).
The Pediatric Evaluation of Disability Inventory (PEDI; Haley et al 1992) was used to measure
the functional ability of the child. The PEDI was developed for young children from six months to
7.5 years of age and adapted to a Dutch version by Custers et al. (2000a) The PEDI is a discrimina-
tive measurement which aims to detect whether a child has limitations in his functional status
and, if so, to determine the extent and content area of the limitations. With the PEDI, both the
capability of the child (what a child can do) and the performance (what the child actually does)
of routine daily childhood activities can be evaluated. Capability is measured by the functional
skills scale, while the caregiver assistance scale and the modifications scale provide information
on the performance. Each scale consists of three domains, namely, self-care, mobility, and social
function. The PEDI can be considered a reliable and valid instrument (Custers et al 2002a, 2002b,
Wassenberg-Severijnen et al 2003).
Analysis of the contents of COPCA and TIP
At four and six months CA, we made video recordings of an intervention session. For 43 infants,
video recordings of infant physical therapy sessions were available. The remaining three infants
(all TIP) had too few intervention sessions to make a video recording. The contents of the sessions
were analyzed with a standardized observation protocol that we recently developed for analysis of
physiotherapeutic intervention sessions in young infants (Blauw-Hospers et al 2010). The protocol
is based on knowledge about infant physical therapy and analysis of directly observable physio-
therapeutic (PT) and caregiver actions. Inter- and intrarater agreement proved to be satisfactory
(Blauw-Hospers et al 2010). The observation protocol classifies PT actions into eight main catego-
ries: 1) Family involvement and educational actions; 2) Communication; 3) Facilitation; 4) Sensory
experience; 5) Passive motor experience; 6) Self-produced motor behavior with no interference; 7)
Challenge to self-produce motor behavior where the infant is allowed and challenged to continue
activity; 8) Challenge to self-produce motor behavior, flowing over into therapeutic handling. We
added a variable which was the amount of postural support provided during PT actions.
The analysis was carried out with the help of the computer program “The Observer” (Noldus).
The Observer software is a tool for collecting and analyzing observational data in a descriptive
and quantitative way. The outcome parameters of the analysis were the relative amounts of time
spent on PT actions. The category self-produced motor behavior without interference of the
physical therapist or the caregiver that is present in the original protocol was left out of the cur-
rent analyses because of a qualitative difference between the two groups during the periods of
entirely spontaneous activity (Dirks et al, submitted for publication). Previously, we reported that
PT actions at four months were largely comparable to those at six months (Dirks et al, submitted
for publication). Assuming that the two measurements at four and six months represented the ac-
tions during the intervention period better than a single measurement, we used the average of the
four-month and six-month values for PT actions in the correlations with developmental outcome.
Data-analysis
Statistical analyses were performed using the computer package SPSS (version 14.0). To evaluate
the effect of type of intervention (COPCA or TIP; group classification on the basis of the video
contents of the physical therapy session) on developmental outcome at 6 and 18 months CA, the
non-parametric Mann-Whitney test was used since the data were not normally distributed. Dif-
ferences having a p-value <0.05 were considered statistically significant.
To examine associations between the contents of intervention and developmental outcome,
univariate analyses were applied first. To minimize the possibility that associations could be
explained by the influence of potential confounders, such as the infant’s baseline condition (neu-
rological outcome and AIMS score at three months, the presence of a severe brain lesion), social
factors (maternal education, being the first child or not), and factors related to the intensity of
physical therapy treatment (number and duration of sessions), we applied multivariate statistics.
Linear regression techniques were used, since the data were skewed to a minimal extent only. In
this way the contribution of the relative duration of PT actions to outcomes on the NOS, AIMS,
BSID-II, and PEDI was assessed. For the associations between the contents of the intervention
and the AIMS score at 18 months CA, logistic regression analysis was carried out, given that at 18
months the AIMS suffered from a ceiling effect. Therefore, we dichotomized the AIMS score into
58 and <58. Correlations with a p-value ≤ 0.01 were considered statistically significant.
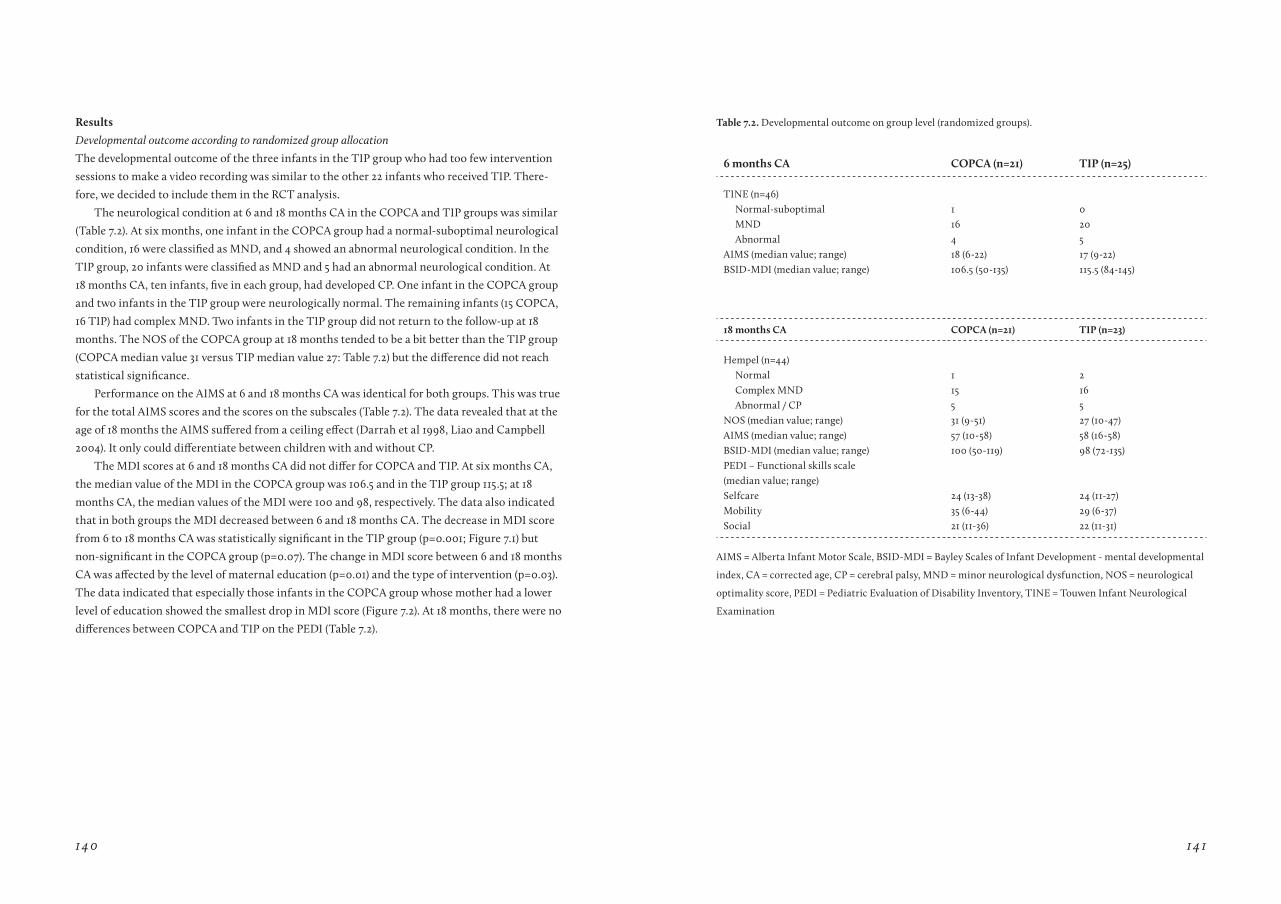
140 141
results
Developmental outcome according to randomized group allocation
The developmental outcome of the three infants in the TIP group who had too few intervention
sessions to make a video recording was similar to the other 22 infants who received TIP. There-
fore, we decided to include them in the RCT analysis.
The neurological condition at 6 and 18 months CA in the COPCA and TIP groups was similar
(Table 7.2). At six months, one infant in the COPCA group had a normal-suboptimal neurological
condition, 16 were classified as MND, and 4 showed an abnormal neurological condition. In the
TIP group, 20 infants were classified as MND and 5 had an abnormal neurological condition. At
18 months CA, ten infants, five in each group, had developed CP. One infant in the COPCA group
and two infants in the TIP group were neurologically normal. The remaining infants (15 COPCA,
16 TIP) had complex MND. Two infants in the TIP group did not return to the follow-up at 18
months. The NOS of the COPCA group at 18 months tended to be a bit better than the TIP group
(COPCA median value 31 versus TIP median value 27: Table 7.2) but the difference did not reach
statistical significance.
Performance on the AIMS at 6 and 18 months CA was identical for both groups. This was true
for the total AIMS scores and the scores on the subscales (Table 7.2). The data revealed that at the
age of 18 months the AIMS suffered from a ceiling effect (Darrah et al 1998, Liao and Campbell
2004). It only could differentiate between children with and without CP.
The MDI scores at 6 and 18 months CA did not differ for COPCA and TIP. At six months CA,
the median value of the MDI in the COPCA group was 106.5 and in the TIP group 115.5; at 18
months CA, the median values of the MDI were 100 and 98, respectively. The data also indicated
that in both groups the MDI decreased between 6 and 18 months CA. The decrease in MDI score
from 6 to 18 months CA was statistically significant in the TIP group (p=0.001; Figure 7.1) but
non-significant in the COPCA group (p=0.07). The change in MDI score between 6 and 18 months
CA was affected by the level of maternal education (p=0.01) and the type of intervention (p=0.03).
The data indicated that especially those infants in the COPCA group whose mother had a lower
level of education showed the smallest drop in MDI score (Figure 7.2). At 18 months, there were no
differences between COPCA and TIP on the PEDI (Table 7.2).
6 months Ca COPCa (n=21) tIP (n=25)
TINE (n=46) Normal-suboptimal MND Abnormal
1164
0205
AIMS (median value; range) 18 (6-22) 17 (9-22)BSID-MDI (median value; range) 106.5 (50-135) 115.5 (84-145)
18 months Ca COPCa (n=21) tIP (n=23)
Hempel (n=44) Normal Complex MND Abnormal / CP
1155
2165
NOS (median value; range) 31 (9-51) 27 (10-47)AIMS (median value; range) 57 (10-58) 58 (16-58)BSID-MDI (median value; range) 100 (50-119) 98 (72-135)PEDI – Functional skills scale(median value; range)Selfcare MobilitySocial
24 (13-38)35 (6-44)21 (11-36)
24 (11-27)29 (6-37)22 (11-31)
AIMS = Alberta Infant Motor Scale, BSID-MDI = Bayley Scales of Infant Development - mental developmental
index, CA = corrected age, CP = cerebral palsy, MND = minor neurological dysfunction, NOS = neurological
optimality score, PEDI = Pediatric Evaluation of Disability Inventory, TINE = Touwen Infant Neurological
Examination
table 7.2. Developmental outcome on group level (randomized groups).

142 143
low middle high
6 mo 6 mo18 mo 18 mo
ns **
140
120
100
80
60
40,00
20,00
0,00
-20,00
-40,00
Maternal Education
dete
rior
atio
n im
prov
emen
t
COPCA(n=21)
TIP(n=23)
tIP
COPCa
BSI
D -
MD
IB
SID
- M
DI
Figure 1: Bayley Scales of Infant Develop-ment: MDI scores at 6 and 18 months in the COPCA and TIP group. Vertical bars, range; horizontal lines, median values; boxes, interquartile range; ns, not significant. ** p=0.001 (Wilcoxon signed ranks test).
Figure 2: Relative deterioration in MDI score between 6 and 18 months and maternal education. The graphs illustrate that MDI is affected by maternal education (p=0.01) and type of intervention (p=0.03) (MANOVA).
Associations between treatment principles and developmental outcome
The results of the RCT showed only minimal differences between COPCA and TIP. We did,
however, observe changes in developmental outcome. To examine whether these changes could be
associated with treatment principles used by the physical therapist or caregiver during interven-
tion or with confounding factors, we applied process evaluation to the data. First, we analyzed
the contents of the intervention sessions. The details of the analysis are described in Dirks et al.
(submitted for publication). Typical COPCA components were: 1) physical therapist coaches the
parent (coaching model); 2) to stimulate self-produced motor behavior at the limit of an infant’s
capabilities; and 3) infant is challenged to produce motor behavior by him/herself and is allowed
to continue activity. Typical TIP components were: 1) physical therapist teaches the infant and
trains the parent (teacher-learner model); 2) in handling techniques; 3) in sensory stimulation; and
4) to challenge for self-produced motor behavior that is followed by a handling technique.
Preliminary analyses showed that the associations between PT actions and developmental
outcome measurements differed for infants with and without CP. An overview of the associations
between treatment principles and developmental outcome is presented in Table 7.3.
In infants who developed CP (n=10) no statistically significant associations were found be-
tween specific PT actions and developmental outcome at six months CA. Some PT actions were
correlated with outcome at 18 months in the infants with CP. The multivariate analyses showed
that more time spent on family involvement and educational actions, more time spent with
postural support at the limit of the infant’s capabilities, and more time during which the infant
was challenged in a widely varying way to produce motor behavior and was allowed to continue
this activity were associated with a higher score on the functional mobility scale of the PEDI at 18
months CA (all p<0.01; Table 7.3). More time spent with passive experience was associated with a
lower NOS at 18 months CA (p<0.01).
In the children without CP (n=33), the amount of time spent on sensory and passive experience
showed a positive correlation with the MDI at six months (both p<0.01), but these associations did
not persist through to the age of 18 months. In children without CP, more time spent on handling
techniques was associated with a lower score on the functional mobility scale of the PEDI at 18
months (p<0.01).
Allocation of intervention based on video analysis
Since the treatment application was very heterogeneous, we decided to regroup the infants on the
basis of the contents of the video into intervention subgroups. The infants who received COPCA
were allocated based on the contents of the intervention to COPCA++ or COPCA+. The interven-
tion sessions of infants who got TIP were classified as TIP++ or TIP+. The ++ notation indicates
that the intervention was performed fully according to the principles of COPCA or TIP. In the
case of TIP, this meant that the principles of the original concept of the Bobaths were used. The
+ notation indicated that the contents of the intervention was more diverse. For COPCA this
implied that COPCA principles were applied incompletely, while for TIP, that treatment consisted

144 145
a) Infants who developed CP (n=10) Outcome measure Model Beta CI p
Family involvement and educational actionsU PEDI - functional mobi-
lity scale 18 moFameduc 0.54 7.59-70.24 0.02
M PEDI - functional mobi-lity scale 18 mo
FameducAIMS 3
0.520.51
11.91-63.660.60-3.40
<0.01<0.01
Postural support - at the verge of infant’s capabilitiesU PEDI - functional mobi-
lity scale 18 moSupport verge 0.60 12.85-69.59 <0.01
M PEDI - functional mobi-lity scale 18 mo
Support vergeAIMS 3
0.560.48
15.09-62.240.56-3.24
<0.01<0.01
Infant challenged to produce motor behavior and allowed to continue activity (large variation offered)U PEDI - functional mobi-
lity scale 18 moCPMB - allowed large var 0.52 4.37-47.72 0.02
M PEDI - functional mobi-lity scale 18 mo
CPMB - allowed large var AIMS 3
0.550.56
10.41-44.570.83-3.53
<0.01<0.01
Passive motor experienceU NOS 18 mo Passive -0.61 -112.69- -22.91 <0.01M NOS 18 mo Passive
Frequency prior to 3 mo-0.790.46
-92.00- -54.720.05- -0.12
<0.01<0.01
b) Infants without CP (n=33)Outcome measure Model Beta CI p
Sensory experienceU MDI 6 Sensory 0.34 19.88-155.07 0.01M MDI 6 Sensory
AIMS 30.360.32
28.36-157.091.00-7.79
<0.010.01
Passive motor experienceU MDI 6 Passive 0.29 11.69-218.80 0.03M MDI 6 Passive
Neur exam 3 mo0.35-0.34
38.77-237.60-26.47- -3.91
<0.01<0.01
Facilitation techniquesU PEDI - functional mobi-
lity scale 18 moFacilitation -0.41 -23.86- -6.00 <0.01
M PEDI - functional mobi-lity scale 18 mo
FacilitationAIMS 3 mo
-0.360.25
-22.03- -4.290.02-2.69
<0.010.05
AIMS = Alberta Infant Motor Scale, CPMB - allowed large var = Infant challenged to produce motor behavior and allowed to continue activity (large variation offered), Fameduc = Family involvement and educational actions, Frequency = number of treatment sessions, MDI = Mental Developmental Index, M = multivariate, Neur exam = neurological examination, NOS = neurological optimality score, PEDI = Pediatric Evaluation of Disability Inventory, U = univariate
table 7.3. Overview of associations between PT-actions and developmental outcome at 6 and 18 months. Results of univariate and multivariate analysis.
of a mix of actions according to the original Bobath concepts along with current NDT principles
involving a more functional approach.
The classification COPCA++ versus COPCA+ was based upon the amount of time that
was spent on the typical COPCA actions where the physical therapist coaches the caregiver to
stimulate motor behavior at the limit of an infant’s capabilities and where the infant is chal-
lenged to self-produce motor behavior that is then continued by the infant. The distinction TIP+
versus TIP++ was made based on the time spent on training the caregiver, handling and pressure
techniques, sensory experience, a challenge to self-produce motor behavior followed by a handling
technique, and the amount of time that actions were performed while the pelvis of the infant in
supine position was lifted slightly by the hands of the physical therapist. Each infant was given a
score on the basis of the average time-values of PT actions observed during the two intervention
sessions on the basis of the percentile values of the present study. When the time spent on a PT ac-
tion was below the 33rd percentile, 1 point was given; a time score between the 33rd and 67th percen-
tile resulted in 2 points; and a time score over the 67th percentile was given 3 points. In this way a
total COPCA score (maximum: 3 actions * 3 points = 9) and a total TIP score (maximum: 5 actions
* 3 points = 15) were calculated. The cut-off for the distinction between the ++ and + classification
was the 67th percentile of the total score. This resulted in a new group allocation that is presented
in Table 7.4. The allocation of the groups based on the time spent on PT actions matched the clas-
sification of the second author (TD) on the basis of Gestalt perception of the video recording.
table 7.4. Reallocation into intervention groups.
Classification total group (n=43)
Infants with CP (n=10) Infants without CP (n=32)*
TIP ++ 14 3 11TIP + 8 2 5COPCA + 7 1 6COPCA ++ 14 4 10
*1 infant did not return to the follow up.TIP++ = classic NDT approachTIP+ = mix of classic NDT and a more functional approachCOPCA+ = COPCA principles applied incompletelyCOPCA++ = COPCA principles fully applied

146 147
Based on the new group allocation, we reanalyzed the outcome measurements. The groups did
not differ in neurological classification, and AIMS and MDI scores at 6 and 18 months. For the do-
main of mobility of the functional skills scale of the PEDI at 18 months, the infants who received
COPCA or TIP+ performed significantly better than the infants in the TIP++ group (Mann-Whit-
ney p < 0.01; Figure 7.3a). They also needed less caregiver assistance in the mobility domain at 18
months (p=0.03; Figure 7.3b). The differences in performance for both PEDI outcomes between
children who received COPCA or TIP+ and those who received TIP++ remained statistically sig-
nificant in the multivariate analyses (details not provided).
Figure 7.3a: Scores on the domain mobility of the functional skills scale of the PEDI at 18 months CA in the COPCA+, COPCA++, TIP+ and TIP++ groups. Vertical bars, range; horizontal lines, median values; boxes, interquartile range.* difference between TIP++ vs other three groups: p <0.01, a significance which persisted in the multivariate analysis.
Figure 7.3b: Scores on the caregiver assistance scale in the domain mobility of the PEDI at 18 months in the COPCA+, COPCA++, TIP+ and TIP++ groups. Vertical bars, range; horizontal lines, median values; boxes, interquartile range.**difference between TIP++ vs other three groups: p=0.03
COPCA++
*
* o
COPCA++COPCA+ COPCA+TIP+ TIP+TIP++ TIP++
50,00
40,00
30,00
20,00
10,00
0,00
* *30,00
25,00
20,00
15,00
10,00
5,00
0,00
3aPEDI - functional mobility scale
group allocation group allocation
3bPEDI - caregiver assistance scale (domain mobility)
21
21 3
Discussion
The RCT revealed that COPCA and TIP were associated with similar effects for developmental
outcome. But the process evaluation indicated that the virtual absence of difference in group
effect may partially have been caused by the extensive heterogeneity in intervention strategies
within the groups, especially within the TIP group. The process analysis indicated that there
was some evidence that important components of the COPCA intervention were associated with
an improved developmental outcome. The therapeutic components of intervention during early
infancy, which were associated with a better developmental outcome at 18 months, were family
involvement and educational actions, application of broad variations in challenging the infant to
produce motor behavior by him/herself and allowing the infant to continue this activity, and the
provision of postural support at the limit of an infant’s capabilities.
Methodological considerations
The major strength of this study was its double approach. The combination of the RCT with a
process evaluation made it possible to determine the influence of the intervention on developmen-
tal outcome. Another strength of this study was that the infants all received intervention during
the same age period, that is, from three to six months post-term. This made the COPCA and TIP
groups more comparable. There was hardly any attrition during the study. Only two infants did
not return to the follow-up at 18 months CA. The final strength was that we used a set of instru-
ments to document outcome, ranging from instruments measuring at impairment level (neuro-
logical examination) to instruments measuring the level of activity and participation (PEDI).
One of the limitations of this study was that we studied a relatively small group of 46 infants.
Although the infants were selected because they all showed definitely abnormal GMs at ten weeks
CA, they had a heterogeneous developmental outcome. Various studies indicated that the pres-
ence of definitely abnormal GM is associated with a high risk for developmental motor disorders
such as cerebral palsy (Prechtl 2001, Hadders-Algra 2004). In this study only a minority of the in-
fants was diagnosed with CP at 18 months. This limitation is inherent to developmental changes
in the central nervous system. Developmental outcome at 18 months CA was relatively good, since
the median values of the MDI were 98-100. It should be noted that the majority of infants showed
complex MND at 18 months, which puts the infant at risk for learning and behavioral disorders at
school age (Hadders-Algra 2005). Another limitation is that we used 18 months CA in this study
to evaluate the long-term outcome of the intervention. As mentioned above, some developmen-
tal problems do not emerge before school age. Therefore, we recommend that future research
should re-examine these children at school age. Finally, the major limitation of this study was the
heterogeneity of the composition of treatment in the TIP group. We anticipated this problem by
including a process analysis, thereby turning a major limitation into a major strength.
148 149
Physiotherapeutic considerations
The RCT revealed only minor differences between the COPCA and the TIP group. One possible
explanation for the small size of the effect is that intervention can affect developmental outcome
in children with brain dysfunction to a limited extent only (Ade-Hall and Moore 2000, Wasiak
et al 2004, Hoare et al 2007, Anttila et al 2008). Animal and human studies indicate that inter-
vention after a lesion of the brain at early age affects motor development considerably less than
cognitive development (Spittle et al 2007, Kolb and Gibb 2007). Another explanation for the lack
of effect could be the heterogeneity of the TIP treatment. For research purposes, it is quite night-
marish that treatment application, although based on the same theoretical background, can be so
diverse. In our opinion this heterogeneity is a major problem in the application of the RCT design
in pediatric physical therapy.
The RCT had two interesting results. First, there was an interaction effect between the type of
intervention and the level of maternal education in the relative drop in MDI score between 6 and
18 months CA. Infants whose mothers had a lower level of education showed less decline in MDI
score over time than infants whose mothers had completed higher education. This effect was es-
pecially present in the COPCA group. This suggests that mothers with lower education especially
benefit more from coaching by a therapist who uses COPCA principles, while mothers with higher
education are less affected by coaching as well as training performed by a therapist. Second, the
finding of a similar neurological outcome in the COPCA and TIP groups is intriguing considering
the diametrically opposed view of TIP and COPCA on the importance of the neurological para-
meters of muscle tone and atypical movements. In the TIP treatment, especially when applied to
the original concepts of Bobath and/or NDT, influencing tone by means of handling techniques
plays an important role in the activities of the therapist during intervention sessions. In COPCA
no attention is paid to these impairments. In other words, handling techniques aimed at influenc-
ing muscle tone and facilitating movement sequences to improve function do not seem to affect
neurological outcome.
Process evaluation indicated that specific components of the interventions in the study were
associated with an improvement in developmental outcome. We would like to stress that observed
associations are not causations. Associations between PT actions and outcome are unavoidably
contaminated by the child’s initial degree of impairment. An infant with a more serious impair-
ment elicits differences in the contents of PT actions than an infant with milder impairments
where the degree of initial impairment to a substantial extent determines later outcome. Our data
indeed revealed clear interactions between the infant’s condition and therapist actions. We there-
fore studied associations separately for infants with and without CP. In addition, we used multi-
variate analysis in order to be able to take into account the infant’s initial degree of impairment.
Nevertheless, it is also conceivable that other infant-specific factors which we did not include in the
analyses did affect the choice of PT actions and the child’s developmental outcome. Yet, the results
of the multivariate analysis may guide our thinking about the effectiveness of specific PT actions.
Several components of COPCA were associated with a higher score in the domain of mobility on
the functional skills scale of the PEDI. An example of this is the category of family involvement
and educational actions which in COPCA implies coaching of family members to develop their
own ways to care for the infant and to cope with the problems of the infant with special needs.
During the intervention, the coach listens, informs, and observes (hands-off), while the caregiver
is involved in daily routines with the child, including play, thereby creating a situation in which
caregivers feel free to explore and discuss alternative strategies. Second, wide variation in self-
produced motor activities (hands-off), trial-and-error experiences, and, if necessary, the provision
of minimal postural support creates a challenging environment in which the infant may explore
and practice his/her motor possibilities (Dirks et al, submitted for publication).
Some typical TIP actions were also associated with developmental outcome. The use of facili-
tation techniques such as handling, which are applied to reduce atypical functional activities and
to prepare the infant for optimally independent function (Dirks et al, submitted for publication),
were associated with a worse performance on the functional skills scale of the PEDI. On the other
hand, sensory and passive experiences were associated with a higher MDI immediately after the
intervention period. Perhaps sensory and passive experiences reflect situations of increased infant
attention which may promote cognitive development (Bahrick et al 2004). Our data indicated that
this beneficial effect disappeared over time.
Since the treatment application was very heterogeneous, we decided to regroup the infants on
the basis of the contents of the video into intervention subgroups. Although this approach lacks
the advantages of an RCT, it was interesting to see that infants in the COPCA and functional TIP
group scored better for domain of mobility on the functional skills scale and needed less car-
egiver assistance for domain of mobility on the PEDI than infants who received a TIP treatment
according to the original Bobath approach. This would indicate that the functionally oriented
interventions succeeded in influencing the performance of functional skills in a beneficial way.
It was interesting to observe that the effects of intervention were clearer at 18 months CA than
immediately after the intervention at 6 months CA. Perhaps this finding is related to the COPCA
approach which aims at supporting family members on the basis of an ongoing equal partnership
in order to uncover their own specific problem-solving strategies for caring and coping with the
infant with special needs.
Concluding remarks
The study showed that our nightmare had a good outcome. Extending the RCT with process
evaluation was necessary in order to answer the question of what components of intervention are
associated with developmental outcome. Our study showed that specific components of COPCA,
especially family involvement and educational actions, challenging the infant with a wide vari-
ation to produce motor behavior by him/herself and then to allow the infant to continue this
activity, and stimulating motor behavior at the limit of an infant’s capabilities according to the
principles of the NGST, were associated with improved developmental outcome.
150 151
references
Ade-Hall RA, Moore AP. Botulinum toxin type A in the treatment of lower limb spasticity in cerebral palsy. Cochrane Database Syst Rev 2000, Issue 1. Art. No.: CD001408. DOI: 10.1002/14651858.CD001408.
Anttila H, Autti-Rämö I, Suoranta J, Mäkelä M, Malmivaara A. Effectiveness of physical therapy inter-ventions for children with cerebral palsy: a systematic review. BMC Pediatr 2008;24;8-14.
Bahrick LE, Lickliter R, Flom R. Intersensory redun-dancy guides the development of Selective Attention, Perception, and Cognition in Infancy. Curr Dir Psychol Sci 2004;13:99-102.
Bayley N. Manual of the Bayley Scales of Infant Develop-ment (second edition). San Antonio, The psychological Corporation; 1993.
Blauw-Hospers CH, de Graaf-Peters VB, Dirks T, Bos AF, Hadders-Algra M. Indications that early interven-tion in infants at high risk for a developmental motor disorder may improve motor and cognitive develop-ment. Neurosci Biobehav Rev 2007;31:1201-1212.
Blauw-Hospers CH, Dirks JF, Hulshof LJ, Hadders-Algra M. Opening the Black-Box: development of a quantitative tool to assess physical therapy contents in infancy. Pediatr Phys Ther 2010;22:189-198.
Blauw-Hospers CH, Hadders-Algra M. Fact or fiction: a systematic review on the effects of early interven-tion on motor development. Dev Med Child Neurol 2005;47:421-432.
Bouwstra H, Dijck-Brouwer J, Decsi T, Boehm G, Bo-ersma ER, Muskiet FA, Hadders-Algra M. Neurologic condition of healthy term infants at 18 months: posi-tive association with venous umbilical DHA status and negative association with umbilical trans-fatty acids. Pediatr Res 2006:60;334-339.
Custers JWH, Wassenberg-Severijnen JE, van der Net J, Vermeer A, ’t Hart H, Helders PJM. Dutch adaptation and content validity of the Pediatric Evaluation of Dis-ability Inventory (PEDI). Disabil Rehabil 2002a;24:250-258.
Custers JWH, van der Net J, Hoijtink H, Wassenberg-Severijnen JE, Vermeer A, Helders PJM. Discrimina-tive validity of the Dutch Pediatric Evaluation of Disability Inventory (PEDI). Arch Phys Med Rehabil 2002b;83:1437-1441.
Darrah J, Piper M, Watt MJ. Assessment of gross motor skills of at-risk infants: predictive validity of the Alberta Infant Motor Scale. Dev Med Child Neurol 1998;40:485-491.
De Vries LS, Eken P, Dubowitz LM. The spectrum of leukomalacia using cranial ultrasound. Behav Brain Res 1992;49:1-6.
De Weerth C, Van Geert P. Changing patterns of infant behavior and mother-infant interaction: Intra-and interindividual variability. Infant Behav Dev 2002;24:347-371.
Dirks T, Blauw-Hospers CH, Hulshof LJ, Hadders-Algra M. Differences between a Family Centered Program “Coping and Caring for Infants with Special Needs” and Infant Treatment based on Principles of NeuroDevelopmental Treatment. Submitted for publication.
Dirks T, Hadders-Algra M. COPCA working manual. 2003.
Edelman GM. Neural Darwinism: Selection and reentrant signalling in higher brain function. Neuron 1993;10:115-125.
Ekström Ahl L, Johansson E, Granat T, Brogren Carl-berg E. Functional therapy for children with cerebral palsy: an ecological approach. Dev Med Child Neurol 2005;47:613-619.
Fiese BH. Family context in pediatric psychology from a transactional perspective; family rituals and stories as examples. Pediatr Psychol 1997;22:183-196.
Hadders-Algra M. The Neuronal Group Selection Theory: an attractive framework to explain variation in normal motor development. Dev Med Child Neurol 2000a;42:566-572.
Hadders-Algra M. The neuronal group selection theory: promising principles for understanding and treating developmental motor disorders. Dev Med Child Neurol 2000b;42:707-715.
Hadders-Algra M. Developmental Coordination Dis-order: Is clumsy motor behaviour caused by a lesion of the brain at early age? Neural Plast 2003;10:39-50.
Hadders-Algra M. General movements: a window for early identification of children at high risk of develop-mental disorders. J Pediatr 2004;145:S12–S18.
Hadders-Algra M. The neuromotor examination of the preschool child and its prognostic significance. Ment Retard Dev Disabil Res Rev. 2005;11:180-188.
Hadders-Algra M. The Neuronal Group Selection Theory: a framework to understand typical and atypi-cal motor development. In: LA Ramenghi. P Evrard, E Mercuri, eds. Perinatal brain damage; from pathogen-esis to neuroprotection. Milan: John Libbey Eurotext; 2008a;34-37.
Hadders-Algra M, Heineman KR, Bos AF, Middel-burg KJ. Minor neurological dysfunction in infancy: strengths and limitations. Dev Med Child Neurol 2010:52;87-92.
Haley SM, Coster WJ, Ludlow LH, Haltiwanger JT,Andrellos PJ. Pediatric Evaluation of Disability Inven-tory: Development, standardization, and administration manual. Boston, MA: New England Medical Centre Inc. and PEDI Research Group; 1992.
Heineman K, Hadders-Algra M. Evaluation of neu-romotor function in infancy - a systematic review of methods available. J Dev Behav Pediatr 2008;29:315-323.
Hempel MS. Neurological development during tod-dling age in normal children and children at risk of de-velopmental disorders. Early Hum Dev 1993:34;47–57.
Hoare BJ, Wasiak J, Imms C, Carey L. Constraint-induced movement therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy. Cochrane Database Syst Rev 2007, Issue 2. Art. No.: CD004149. DOI: 10.1002/14651858.CD004149.pub2.
Howle J. NDT in the United States. NDTA Network 2005;12.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association; 2002.
Huisman M, Koopman-Esseboom C, Lanting CI, Van der Paauw CG, Tuinstra LGMTh, Fidler V, Weisglas-Kuperus N, Sauer PJJ, Boersma ER, Touwen BCL. Neurological condition in 18-month-old children perinatally exposed to polychlorinated biphenyls and dioxins. Early Hum Dev 1995:43;165-176.
Ketelaar M, Vermeer A, Hart H, van Petegem-van Beek E, Helders PJ.Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys Ther 2001;81:1534-1545.
Ketelaar M, Vermeer A, Helders PJ. Functional motor abilities of children with cerebral palsy: a systematic literature review of assessment measures. Clin Rehabil 1998;12:369-380.
Kolb B, Gibb R. Brain plasticity and recovery from early cortical injury. Dev Psychobiol 2007;49:107-118.
Lachin JM, Matts JP, Wei LJ. Randomization in Clini-cal Trials: Conclusions and Recommendations. Control Clin Trials 1988;9:365-74.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Oc-cup Ther Pediatr 1998;18:83-102.
Lettinga AT, Reynders K, Mulder TH, Mol A. Pitfalls in effectiveness research: a comparative analysis of treatment goals and outcome measures in stroke rehabilitation. Clin Rehabil 2002;16:174-81.
Liao PM, Campbell SK. Examination of the item struc-ture of the Alberta Infant Motor Scale. Pediatr Phys Ther 2004;16:31-38.
Mayston M Bobath concept: a view from the United Kingdom. NDTA Network 2005;12.

152 153
Piper MC, Darrah J. Motor assessment of the developing infant. Philadelphia: Saunders; 1994.
Prechtl HFR. General movement assessment as a method of developmental neurology: new para-digms and their consequences. Dev Med Child Neurol 2001;43:836-842.
Prechtl HFR. The optimality concept. Early Hum Dev 1980;4:201-205.
Spittle AJ, Orton J, Doyle LW, Boyd R. Early de-velopmental intervention programs post hospital discharge to prevent motor and cognitive impair-ments in preterm infants. Cochrane Database Syst Rev 2007;18:CD005495.
Van der Meulen BF, Ruiter SAJ, Spelberg HCL, Smrko-vsky M. Bayley Scales of Infant Development - II. Dutch version. Lisse, Swets Test Publishers; 2002.
Volpe JJ. Intracranial hemorrhage. In: Volpe JJ, ed. Neurology of the newborn. Philadelphia: WB Saunders Company; 2000:428-493.
Wasiak J, Hoare B, Wallen M. Botulinum toxin A as an adjunct to treatment in the management of the upper limb in children with spastic cerebral palsy. Cochrane Database of Syst Rev 2004, Issue 3. Art. No.: CD003469. DOI: 10.1002/14651858.CD003469.pub3.
Wassenberg-Severijnen JE, Custers JWH, Hox JJ, Vermeer A, Helders PJM. Reliability of the Dutch Pediatric Evaluation of Disability Inventory (PEDI) Clin Rehabil 2003;17:457-462.
Watson B, Proctor S, Cochrane W. Using randomised controlled trials (RCTs) to test service interventions: issues of standardisation, selection and generalisabil-ity. Nurse Res 2004;11:28-42.
C H a P t E r 8
A ddI t Ion A l r e s u lt s
on o u tc om e m e A s u r e s
of t h e V I P P roj e c t

154 155
In this Chapter some of the results of questionnaires which were also assessed during the VIP
project, but were not the focus in the previous sections, are presented. Successively, attention is
paid to the Kent Infant Development Scales (KIDS), the Measures of Processes of Care (MPOC)
and the Nijmegen Questionnaire on Child-rearing Situations (NCSQ). Furthermore some prelimi-
nary results on postural control will be described. The results of the IMP, video recordings of ADL
activities and postural control will be published separately.
Kent Infant Development Scales
In total, 113 questionnaires (51 COPCA; 62 TIP) were returned (response rate of 82%). Especially at
3 months CA attrition was high (28%). At 6 and 18 months CA attrition was lower, but still ranged
from 8 to 19%. One possible explanation for the attrition rate was that despite the instructions
some caregivers did not complete the questionnaire before the next test session. Reasons they
mentioned were that they did not exactly know the corrected age of the infant, they didn’t see the
necessity to fill out the questionnaire at the right time, or they simply forgot. Caregivers with a
lower educational level or with known psychopathological problems tended to return the ques-
tionnaires less often.
The results showed that KIDS scores of infants in the COPCA group did not differ from those in
the TIP group. Both the total score and the scores on the five subscales were comparable at 3, 6, and
18 months CA (see Table 8.1). The possibility that under- or overestimation of the development of the
infant influenced the KIDS scores is present but almost negligible. The caregivers were only asked
to report whether they had noticed a specific behaviour, not to judge the development of the infant
(Stancin et al 1984).Some outliers were present in the data but they hardly influenced the results.
table 8.1. Median scores and ranges of the KIDS at 3, 6 and 18 months CA.
COPCa tIP3
(n=15)
6
(n=17)
18
(n=18)
3
(n=18)
6
(n=23)
18
(n=21)
Total 68.0
(62-122)
139
(106-189)
243.5
(214-252)
64.0
(31-118)
128.0
(77-221)
246.0
(177-252)
Cognition 16.0
(5-25)
33.5
(24-43)
50.5
(44-52)
15.5
(7-28)
31.0
(14-45)
50.0
(42-52)
Motor 16.0
(4-28)
37.5
(24-65)
77.0
(48-78)
15.0
(4-38)
33.0
(21-72)
75.0
(34-78)
Language 11.0
(5-18)
20.0
(9-24)
37.0
(30-38)
10.0
(3-17)
19.0
(11-34)
37.0
(29-38)
Self-help 8.0
(3-20)
23.5
(15-33)
38.0
(29-39)
6.5
(3-11)
21.0
(11-36)
38.0
(29-39)
Social 16.0
(8-27)
29.0
(22-37)
50.0
(44-51)
15.5
(8-25)
26.0
(13-44)
50.0
(38-51)
Measures of processes of Care (MPOC)
In total, 115 questionnaires (53 COPCA; 62 TIP) were returned (response rate of 83%). Caregivers
with a lower educational level or with known psychopathological problems tended to return the
questionnaires less often. From the 115 questionnaires only 81 (37 COPCA; 46 TIP) were valid
and could be used for the final analysis. The non-valid questionnaires contained a consider-
able amount of missing data, i.e. more than 29 items, resulting in too few answers to calculate a
domain score (Van Schie et al 2004). The large amount of non-valid questionnaires was mainly
caused by the frequent use of the category ‘not applicable’. At both 3 and 6 months CA eleven ques-
tionnaires were non-valid. At 18 months CA twelve questionnaires were non-valid. The caregivers
of the latter twelve infants reported that they had no experience with a rehabilitation setting or
hospital visit during the period between 6 and 18 months CA and judged the MPOC as not suitable
for their situation. They did however return the questionnaire, but answered most questions with
‘not applicable’.
Figure 8.1. Median values of COPCA and TIP on the five domains of the MPOC.
COPCA COPCA COPCATIP TIP TIP
7,00
6,00
5,00
4,00
3,00
2,00
1,00
0,00
7,00
6,00
5,00
4,00
3,00
2,00
1,00
0,00
7,00
6,00
5,00
4,00
3,00
2,00
1,00
0,00
3 3 36 6 618 18 18
7,00
6,00
5,00
4,00
3,00
2,00
1,00
0,00
7,00
6,00
5,00
4,00
3,00
2,00
1,00
0,00
Enabling and Partnership
General information
Coordinated and Comprehensive Care
Specific information
respectfulans Supportive Care
COPCA COPCATIP TIP
3 36 618 18
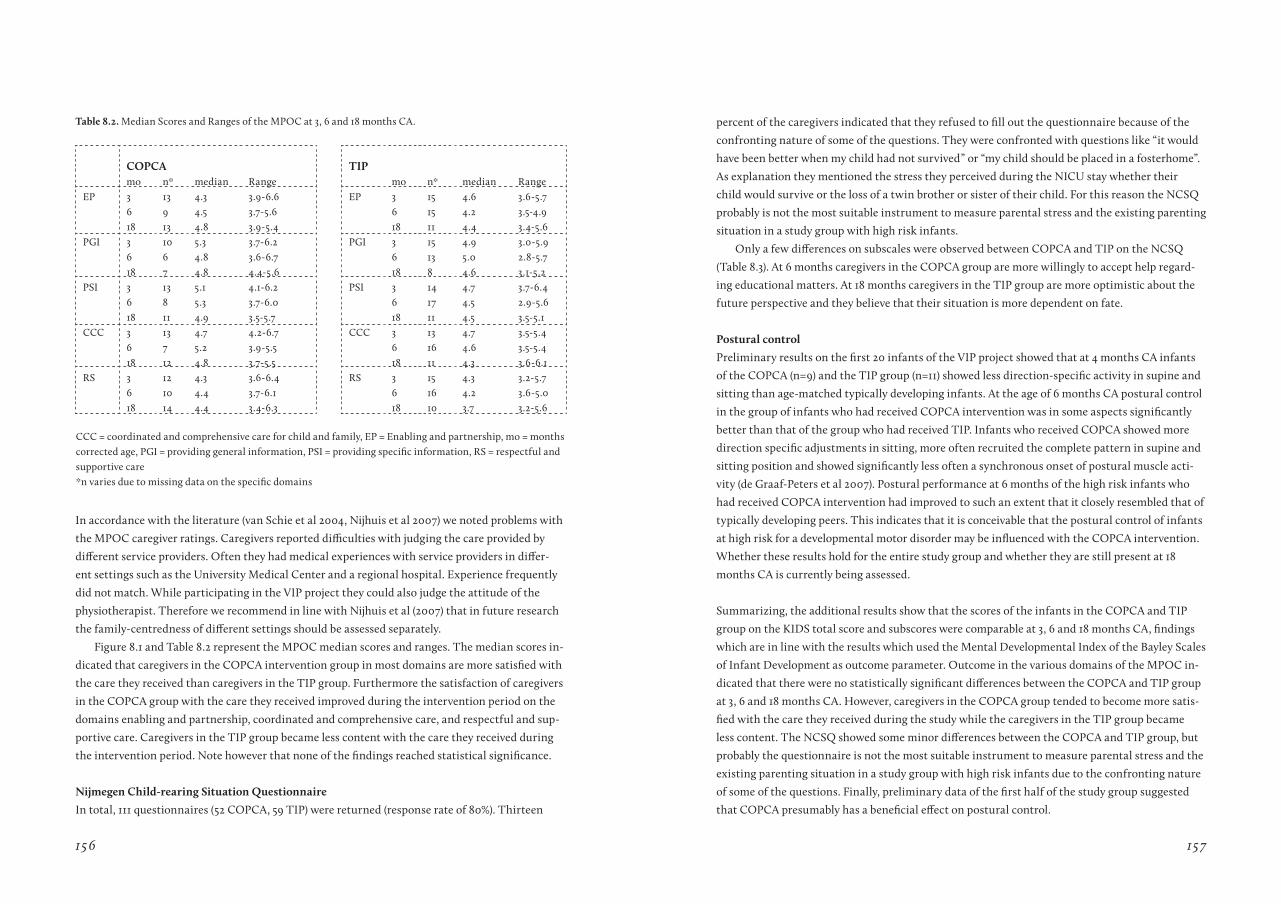
156 157
table 8.2. Median Scores and Ranges of the MPOC at 3, 6 and 18 months CA.
COPCa tIPmo n* median Range mo n* median Range
EP 3 13 4.3 3.9-6.6 EP 3 15 4.6 3.6-5.76 9 4.5 3.7-5.6 6 15 4.2 3.5-4.918 13 4.8 3.9-5.4 18 11 4.4 3.4-5.6
PGI 3 6
10 6
5.3 4.8
3.7-6.2 3.6-6.7
PGI 3 6
15 13
4.9 5.0
3.0-5.9 2.8-5.7
18 7 4.8 4.4-5.6 18 8 4.6 3.1-5.2PSI 3 13 5.1 4.1-6.2 PSI 3 14 4.7 3.7-6.4
6 8 5.3 3.7-6.0 6 17 4.5 2.9-5.618 11 4.9 3.5-5.7 18 11 4.5 3.5-5.1
CCC 3 6 18
13 7 12
4.7 5.2 4.8
4.2-6.7 3.9-5.5 3.7-5.5
CCC 3 6 18
13 16 11
4.7 4.6 4.3
3.5-5.4 3.5-5.4 3.6-6.1
RS 3 12 4.3 3.6-6.4 RS 3 15 4.3 3.2-5.76 10 4.4 3.7-6.1 6 16 4.2 3.6-5.018 14 4.4 3.4-6.3 18 10 3.7 3.2-5.6
CCC = coordinated and comprehensive care for child and family, EP = Enabling and partnership, mo = months corrected age, PGI = providing general information, PSI = providing specific information, RS = respectful and supportive care*n varies due to missing data on the specific domains
In accordance with the literature (van Schie et al 2004, Nijhuis et al 2007) we noted problems with
the MPOC caregiver ratings. Caregivers reported difficulties with judging the care provided by
different service providers. Often they had medical experiences with service providers in differ-
ent settings such as the University Medical Center and a regional hospital. Experience frequently
did not match. While participating in the VIP project they could also judge the attitude of the
physiotherapist. Therefore we recommend in line with Nijhuis et al (2007) that in future research
the family-centredness of different settings should be assessed separately.
Figure 8.1 and Table 8.2 represent the MPOC median scores and ranges. The median scores in-
dicated that caregivers in the COPCA intervention group in most domains are more satisfied with
the care they received than caregivers in the TIP group. Furthermore the satisfaction of caregivers
in the COPCA group with the care they received improved during the intervention period on the
domains enabling and partnership, coordinated and comprehensive care, and respectful and sup-
portive care. Caregivers in the TIP group became less content with the care they received during
the intervention period. Note however that none of the findings reached statistical significance.
Nijmegen Child-rearing Situation Questionnaire
In total, 111 questionnaires (52 COPCA, 59 TIP) were returned (response rate of 80%). Thirteen
percent of the caregivers indicated that they refused to fill out the questionnaire because of the
confronting nature of some of the questions. They were confronted with questions like “it would
have been better when my child had not survived” or “my child should be placed in a fosterhome”.
As explanation they mentioned the stress they perceived during the NICU stay whether their
child would survive or the loss of a twin brother or sister of their child. For this reason the NCSQ
probably is not the most suitable instrument to measure parental stress and the existing parenting
situation in a study group with high risk infants.
Only a few differences on subscales were observed between COPCA and TIP on the NCSQ
(Table 8.3). At 6 months caregivers in the COPCA group are more willingly to accept help regard-
ing educational matters. At 18 months caregivers in the TIP group are more optimistic about the
future perspective and they believe that their situation is more dependent on fate.
Postural control
Preliminary results on the first 20 infants of the VIP project showed that at 4 months CA infants
of the COPCA (n=9) and the TIP group (n=11) showed less direction-specific activity in supine and
sitting than age-matched typically developing infants. At the age of 6 months CA postural control
in the group of infants who had received COPCA intervention was in some aspects significantly
better than that of the group who had received TIP. Infants who received COPCA showed more
direction specific adjustments in sitting, more often recruited the complete pattern in supine and
sitting position and showed significantly less often a synchronous onset of postural muscle acti-
vity (de Graaf-Peters et al 2007). Postural performance at 6 months of the high risk infants who
had received COPCA intervention had improved to such an extent that it closely resembled that of
typically developing peers. This indicates that it is conceivable that the postural control of infants
at high risk for a developmental motor disorder may be influenced with the COPCA intervention.
Whether these results hold for the entire study group and whether they are still present at 18
months CA is currently being assessed.
Summarizing, the additional results show that the scores of the infants in the COPCA and TIP
group on the KIDS total score and subscores were comparable at 3, 6 and 18 months CA, findings
which are in line with the results which used the Mental Developmental Index of the Bayley Scales
of Infant Development as outcome parameter. Outcome in the various domains of the MPOC in-
dicated that there were no statistically significant differences between the COPCA and TIP group
at 3, 6 and 18 months CA. However, caregivers in the COPCA group tended to become more satis-
fied with the care they received during the study while the caregivers in the TIP group became
less content. The NCSQ showed some minor differences between the COPCA and TIP group, but
probably the questionnaire is not the most suitable instrument to measure parental stress and the
existing parenting situation in a study group with high risk infants due to the confronting nature
of some of the questions. Finally, preliminary data of the first half of the study group suggested
that COPCA presumably has a beneficial effect on postural control.
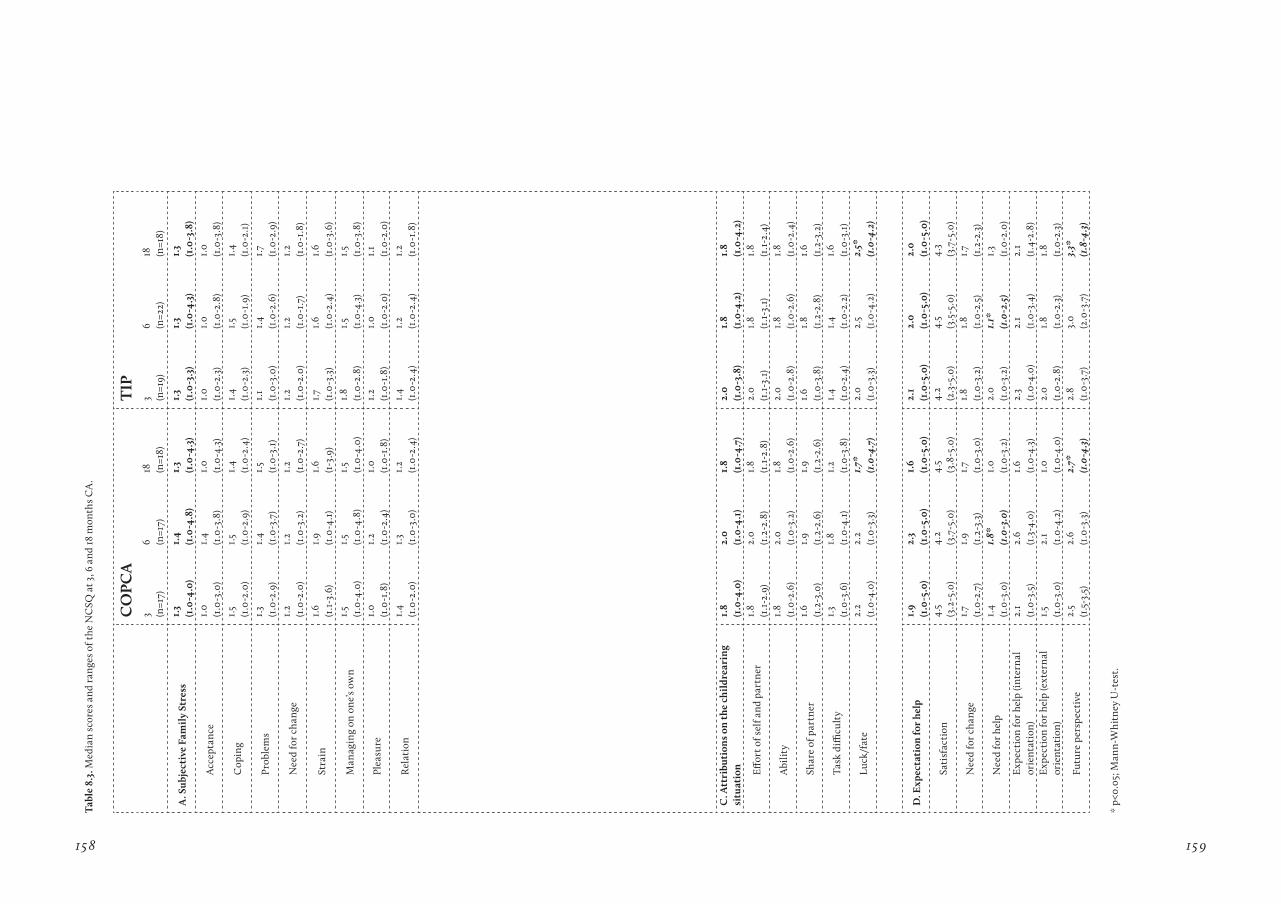
158 159
tabl
e 8.
3. M
edia
n sc
ores
and
ran
ges
of t
he N
CSQ
at 3
, 6 a
nd 18
mon
ths
CA
.
CO
PCa
tIP
3 (n=1
7)6 (n
=17)
18 (n=1
8)3 (n
=19)
6 (n=2
2)18 (n
=18)
a. S
ubje
ctiv
e Fa
mil
y St
ress
1.
3(1
.0-4
.0)
1.4
(1.0
-4.8
)1.
3(1
.0-4
.3)
1.3
(1.0
-3.3
)1.
3(1
.0-4
.3)
1.3
(1.0
-3.8
)
Acc
epta
nce
1.0
(1.0
-3.0
)1.
4(1
.0-3
.8)
1.0
(1.0
-4.3
)1.
0(1
.0-2
.3)
1.0
(1.0
-2.8
)1.
0(1
.0-3
.8)
Cop
ing
1.5
(1.0
-2.0
)1.
5(1
.0-2
.9)
1.4
(1.0
-2.4
)1.
4(1
.0-2
.3)
1.5
(1.0
-1.9
)1.
4(1
.0-2
.1)
Prob
lem
s1.
3(1
.0-2
.9)
1.4
(1.0
-3.7
)1.
5(1
.0-3
.1)
1.1
(1.0
-3.0
)1.
4(1
.0-2
.6)
1.7 (1.0
-2.9
)
Nee
d fo
r ch
ange
1.2
(1.0
-2.0
)1.
2(1
.0-3
.2)
1.2
(1.0
-2.7
)1.
2(1
.0-2
.0)
1.2
(1.0
-1.7
)1.
2(1
.0-1
.8)
Stra
in1.
6(1
.1-3
.6)
1.9
(1.0
-4.1
)1.
6(1
-3.9
)1.7 (1
.0-3
.3)
1.6
(1.0
-2.4
)1.
6(1
.0-3
.6)
Man
agin
g on
one
’s ow
n1.
5(1
.0-4
.0)
1.5
(1.0
-4.8
)1.
5(1
.0-4
.0)
1.8
(1.0
-2.8
)1.
5(1
.0-4
.3)
1.5
(1.0
-3.8
)
Plea
sure
1.0
(1.0
-1.8
)1.
2(1
.0-2
.4)
1.0
(1.0
-1.8
)1.
2(1
.0-1
.8)
1.0
(1.0
-2.0
)1.
1(1
.0-2
.0)
Rel
atio
n1.
4(1
.0-2
.0)
1.3
(1.0
-3.0
)1.
2(1
.0-2
.4)
1.4
(1.0
-2.4
)1.
2(1
.0-2
.4)
1.2
(1.0
-1.8
)
C. a
ttri
buti
ons
on t
he c
hild
rear
ing
situ
atio
n1.
8(1
.0-4
.0)
2.0
(1.0
-4.1
)1.
8(1
.0-4
.7)
2.0
(1.0
-3.8
)1.
8(1
.0-4
.2)
1.8
(1.0
-4.2
)
Eff
ort o
f sel
f and
par
tner
1.8
(1.1
-2.9
)2.
0(1
.2-2
.8)
1.8
(1.1
-2.8
)2.
0(1
.1-3
.1)
1.8
(1.1
-3.1
)1.
8(1
.1-2
.4)
Abi
lity
1.8
(1.0
-2.6
)2.
0(1
.0-3
.2)
1.8
(1.0
-2.6
)2.
0(1
.0-2
.8)
1.8
(1.0
-2.6
)1.
8(1
.0-2
.4)
Shar
e of
par
tner
1.6
(1.2
-3.0
)1.
9(1
.2-2
.6)
1.9
(1.2
-2.6
)1.
6(1
.0-3
.8)
1.8
(1.2
-2.8
)1.
6(1
.2-3
.2)
Tas
k di
fficu
lty
1.3
(1.0
-3.6
)1.
8(1
.0-4
.1)
1.2
(1.0
-3.8
)1.
4(1
.0-2
.4)
1.4
(1.0
-2.2
)1.
6(1
.0-3
.1)
Luck
/fat
e2.
2(1
.0-4
.0)
2.2
(1.0
-3.3
)1.7
*(1
.0-4
.7)
2.0
(1.0
-3.3
)2.
5(1
.0-4
.2)
2.5*
(1.0
-4.2
)
D. E
xpec
tati
on fo
r he
lp1.
9(1
.0-5
.0)
2.3
(1.0
-5.0
)1.
6(1
.0-5
.0)
2.1
(1.0
-5.0
)2.
0(1
.0-5
.0)
2.0
(1.0
-5.0
)
Sati
sfac
tion
4.5
(3.2
-5.0
)4.
2(3
.7-5
.0)
4.5
(3.8
-5.0
)4.
2(2
.3-5
.0)
4.5
(3.5
-5.0
)4.
3(3
.7-5
.0)
Nee
d fo
r ch
ange
1.7 (1.0
-2.7
)1.
9(1
.2-3
.3)
1.7 (1.0
-3.0
)1.
8(1
.0-3
.2)
1.8
(1.0
-2.5
)1.7 (1
.2-2
.3)
Nee
d fo
r he
lp1.
4(1
.0-3
.0)
1.8*
(1.0
-3.0
)1.
0(1
.0-3
.2)
2.0
(1.0
-3.2
)1.
1*(1
.0-2
.5)
1.3
(1.0
-2.0
)E
xpec
tion
for
help
(int
ern
al
orie
ntat
ion)
2.1
(1.0
-3.5
)2.
6(1
.3-4
.0)
1.6
(1.0
-4.3
)2.
3(1
.0-4
.0)
2.1
(1.0
-3.4
)2.
1(1
.4-2
.8)
Exp
ecti
on fo
r he
lp (e
xter
nal
or
ient
atio
n)1.
5(1
.0-3
.0)
2.1
(1.0
-4.2
)1.
0(1
.0-4
.0)
2.0
(1.0
-2.8
)1.
8(1
.0-2
.3)
1.8
(1.0
-2.3
)
Futu
re p
ersp
ecti
ve2.
5(1
.5-3
.5)
2.6
(1.0
-3.3
)2.
7*(1
.0-4
.3)
2.8
(1.0
-3.7
)3.
0(2
.0-3
.7)
3.3*
(1.8
-4.3
)
* p<
0.05
; Man
n-W
hitn
ey U
-tes
t.
160 161
references
De Graaf-Peters VB, Blauw-Hospers CH, Dirks T, Bakker J, Bos AF, Hadders-Algra M. Development of postural control in typically developing children and children with cerebral palsy: possibilities for interven-tion? Neurosci Biobehav Rev 2007;31:1191-1200.
Nijhuis BJG, Reinders-Messelink HA, de Blecourt ACE, Hitters MWMCG, Groothoff JW, Nakken H, Postema K. Family-centred care in family-specific teams. Clin Rehabil 2007;21:660-671.
Stancin T, Reuter J, Dunn V. Validity of caregiver information on the developmental status of severely brain-damaged young children. Am J Ment Defic 1984;8:388-395.
Van Schie PEM, Siebes RC, Ketelaar M, Vermeer A. The Measure of Processes of Care (MPOC): valida-tion of the Dutch translation. Child Care Health Dev 2004;30:529-539.
C H a P t E r 9
g e n e r A l dI s c u s s Ion
162 163
The main aim of this thesis was to contribute to the body of knowledge about the effects of early
physiotherapeutic intervention for young infants who are considered to be at risk for a develop-
mental motor disorder. Therefore existing programmes on the effects of early physiotherapeutic
intervention on motor and cognitive development were reviewed and a new physiotherapeutic
intervention programme COPCA was evaluated. The evaluation of the COPCA programme not
only focused on the effects on developmental outcome but also included a process evaluation of
the contents of the COPCA programme. Section 9.1 discusses the implications of the main find-
ings of the studies in this thesis. Reflections about the VIP project are offered in section 9.2. This
discussion ends with some implications for physiotherapeutic practice and recommendations for
further research (section 9.3).
9.1 Implications of the main findings
9.1.1 The effect of early intervention on developmental outcome
The systematic reviews on the effects of existing early physiotherapeutic intervention program-
mes on motor (Chapter 3 and 4) and cognitive development (Chapter 4) of infants with a high risk
for developmental motor disorders aged less than 18 months corrected age (CA) resulted in three
important findings. First, the effect of early intervention programmes which focus primarily on
the improvement of motor development is inconclusive. It remains a matter of debate to what
extent early intervention may facilitate outcome in various developmental domains. General
developmental programmes seem most promising to influence motor and cognitive development.
Second, we recommend that the choice of an early intervention programme should be adapted to
the infant’s age. It turned out that the type of intervention which might be beneficial for infants
at preterm age differs from the type which is effective in infants who have reached at least term
age. At preterm age infants seem to benefit most from intervention which aims at mimicking the
intrauterine environment, such as NIDCAP intervention. After term age, general developmental
programmes in which parents learn how to promote infant development can exert a positive effect
on motor and cognitive development. This finding is consistent with the results of studies on the
effect of early intervention which primarily aim at improving cognitive outcome. Third, interven-
tion programmes according to the principles of NDT or Vojta do not show a beneficial effect on
motor or cognitive development in infants at high risk for developmental disorders in the first
postnatal years. A limitation of the systematic reviews was that the contents of the programmes
and the methodological quality differed too much to allow for a meta-analysis of the data. The
findings of our reviews are in line with similar reviews performed by others investigating the ef-
fect of early intervention (Simeonsson et al 1982, Parette and Hourcade 1984, Casto and Mastrop-
ieri 1986, Shonkoff and Hauser-Cram 1987, Parry 1992, Turnbull 1993, Guralnick 1997, Majnemer
1998, Butler and Darrah 2001, Spittle et al 2007).
One of the aims of the VIP project was to evaluate the effect of two early intervention pro-
grammes on developmental outcome. COPCA can be considered as an example of a general devel-
opmental programme while TIP, the traditional approach towards infant physical therapy in the
Netherlands, is based for an important part on the principles of NDT treatment. Overall we found
only minor differences in developmental outcome till the age of 18 months between the COPCA
and TIP group. A possible explanation for this small size of the effect is that intervention can af-
fect developmental outcome in children with brain dysfunction to a limited extent only (Ade-Hall
and Moore 2000, Wasiak et al 2004, Hoare et al 2007, Anttila et al 2008).
Developmental outcome of the infants in the VIP project was relatively good as the median
values of the MDI were 98-100 and only a minor part of the groups were diagnosed with CP at
the age of 18 months CA. It should be noted however that the majority of infants showed complex
MND at 18 months, which puts the infant at risk for learning and behavioural disorders at school
age (Hadders-Algra 2005). Important findings of the VIP project were: 1) Neurological outcome at
6 and 18 months in the COPCA and TIP group was similar. This was interesting considering the
position that muscle tone and abnormal movement patterns, which are two important aspects
of neurological condition, have in both interventions. In TIP normalization of muscle tone and
movement patterns plays an important role (Howle 2002), while in COPCA no attention is paid to
these impairments. In other words, therapeutic techniques aiming to influence muscle tone and
movement patterns, do not seem to affect neurological outcome. 2) Motor performance as mea-
sured with the AIMS was similar at 6 and 18 months CA. Where the preliminary analyses for the
first half of the study group showed that infants who received COPCA tended to perform better
on de sitting subscale of the AIMS (Chapter 4), this result could not be replicated when we ana-
lyzed the data of the entire study group (Chapter 7). 3) Although the overall cognitive outcome was
comparable between the COPCA and TIP group at 6 and 18 months CA, we observed a decrease
in the MDI score over time which was statistically significant in the TIP group. This decrease in
cognitive outcome over time is in line with findings in other studies (Vohr and Garcia Coll 1985,
Aylward 1989, Bhutta et al 2002, Ment et al 2003). The change in MDI score between 6 and 18
months CA was affected by the level of maternal education and the type of intervention. Infants
whose mother had a lower level of education showed less decline in MDI score over time than
infants whose mother had finished a higher education. This effect was in particular present in
the COPCA group. This suggests that in particular mothers with a lower education benefit more
from the suggestions made by a physical therapist that uses COPCA concepts, while mothers
with a higher education seem less affected by suggestions of a physical therapist. 4) At 18 months
CA there were no differences between COPCA and TIP on the PEDI. However, it turned out that
the score on the functional mobility scale of the PEDI was associated with several elements of the
intervention (see 9.1.2). 5) Results from the questionnaires (Chapter 8) indicated that caregivers in
the COPCA group tended to become more satisfied with the care they received during the study
while the caregivers in the TIP group became less content (MPOC). Moreover the caregivers in
the COPCA group were more willingly to accept help regarding educational matters (NCSQ). 6)
Data from the first half of the study group suggested that COPCA presumably has a beneficial
effect on postural control. Infants who received COPCA showed more direction specific adjust-
ments in sitting, more often recruited the complete pattern in supine and sitting position and

164 165
showed significantly less often a synchronous onset of postural muscle activity (de Graaf-Peters
et al 2007).
9.1.2. Evaluation of the application of COPCA in daily practice.
The application of COPCA in daily practice was evaluated by means of video analysis. This pro-
cess evaluation is a prerequisite for the implementation of COPCA within paediatric physiotherapy.
It is acknowledged that designing intervention programmes requires more fundamental knowl-
edge about the relations between function, activities and participation than is offered by RCT
research (May et al 2007, Hullegie 2009). Complex therapeutic interventions comprise a number
of separate elements which seem essential to the proper functioning of the interventions, which
may act both independently and interdependently. The components usually include behaviours,
parameters of behaviours (e.g. frequency, timing), and methods of organizing and delivering those
behaviours (e.g. type(s) of practitioner, setting and location) (Medical Research Council 2000).
Randomised controlled trials (RCTs) are considered to be the most rigorous way to evaluate
the effectiveness of interventions, regardless of their complexity. Because of their multifaceted
nature and dependence on social context, complex interventions pose methodological challenges,
and require adaptations to the standard design of such trials (Oakley et al 2006). Process evalua-
tion is needed to describe what really happens in an intervention and to explore hypotheses about
why and how interventions are effective or ineffective (Lettinga et al 2002, Flottorp et al 2003,
Oakley et al 2006). Process evaluation is especially necessary in trials, where the ‘same’ inter-
vention principles may be implemented, but applied and received in different ways. This thesis
contributes to these issues in two ways. First, by developing a standardized observation protocol
which allowed for an objective quantification of the contents of physical add therapy in infancy.
Second, by combining the RCT with the process evaluation it was actually possible to explore
whether specific aspects in the contents of intervention could be associated with developmental
outcome. The study described in Chapter 7 in which we extended the results of the RCT with
process evaluation is a good example of integrating the knowledge about the contents of interven-
tion with the scientific approach of a RCT. The process evaluation has helped deepen our under-
standing of what actually happens during the intervention and which PT-actions contribute to an
improved developmental outcome.
Our inventory has resulted in a standardized observation protocol detailing essential elements
and core features of physiotherapeutic intervention, which permitted analysis of the contents
of physical therapy interventions for infants (see Chapter 5). The protocol was proven to meet
important psychometric requirements and captured nearly all physiotherapeutic actions which
were performed during intervention sessions of infants at high risk. It is an instrument which may
be used to assess heterogeneity in physical therapy as it offers a tool to describe operationally what
therapists do within treatment sessions across varying frames of theoretical references. Four con-
clusions can be drawn from the three studies (Chapter 5-7) which applied the observation protocol.
First, traditional infant physical therapy is characterized by a large heterogeneity in implementa-
tion. Presumably this heterogeneity is brought about by the application of techniques belonging to
different treatment approaches. Not only actions belonging to the concept of Neurodevelopmental
Treatment (NDT) including baby treatment - approaches well known for their heterogeneity in
application (Bly 1991) - are incorporated into treatment but also actions from a more functional
point of view. Research demonstrated that eclectic approaches tend to have smaller effects due to
the fact that there are more confounding factors which might influence the effect size (Mandich et
al 2001).
Second, the analysis of the contents of physical therapy sessions indicated a discrepancy
between actual clinical practice and the physiotherapist’s interpretation of his or her own actions.
The evaluation of the video’s taught us that physical therapists often do other things than they
intend to do. This indicates that it is very important to have a uniform language within physi-
otherapeutic practice. Currently, different treatment approaches use the same word to describe
different things. For instance, let us focus on the word “active”. NDT treatment aims to give the
child sensorimotor experience through the child’s active responses to specialized handling (Brice,
Bobath Centre, instruction video 1990). This implies that the active behaviour of the child is in
part a reaction to the handling technique of the PT. In functional therapy and COPCA “active”
refers to self-produced activities of the child. These frames of reference may differ more often
than we realize, resulting in miscommunication. Video feedback might serve as a tool to capture
this type of misunderstanding and subsequently add to the uniformity in the language used by
therapists. This means that only the evaluation of real action and communication through stand-
ardized, computer-based video-analysis of treatment sessions will provide insight in the reality of
practice.
Third, analysis of the newly developed programme COPCA showed many differences in the
contents of COPCA and TIP (Chapter 6). The differences found between COPCA and TIP corres-
ponds to the theoretical frameworks of both approaches (see Table 6.1). They included differences
in the role of caregivers and the approach of families, the application of educational actions
towards the infant and in activities to stimulate the infant’s sensorimotor development. These
findings indicate that COPCA and TIP based on NDT differ largely justifying the label ‘novel
intervention’ for the COPCA programme.
Fourth, the process evaluation indicated that several aspects of the COPCA intervention were
associated with an improved developmental outcome. Infants seem to benefit the most from
activities that add to a challenging environment in which large variation, trial-and-error experi-
ences and minimal postural support is offered. The physical therapist can coach the caregivers to
incorporate these aspects into all daily activities. Some typical TIP actions were also associated
with developmental outcome. The use of facilitation techniques like handling, which are ap-
plied to reduce atypical functional activities and to prepare the infant for optimally independent
function (Dirks et al, submitted for publication), was associated with a worse performance on the
functional skills scale of the PEDI. The use of sensory and passive experience showed a positive
166 167
short term effect on the cognitive development of the infants. Although the results of the VIP
project seem promising, it is important to realize that the results of the study should be interpret-
ed with caution. After all, associations do not directly mean that there is a causal relation between
a PT-action and developmental outcome. Furthermore the associations between PT-actions and
outcome are unavoidably contaminated with the child’s initial degree of impairment. Multivariate
statistics can be applied to account for this problem but still more research is needed to examine
the influence of the contents of intervention on developmental outcome.
To summarize, although the differences between the COPCA and TIP group on several aspects of
developmental outcome on RCT level are small, the results suggest that COPCA is more promis-
ing than TIP to influence aspects of developmental outcome. This is reflected in the findings that
infants who received COPCA decline less in cognitive function over time and that COPCA pos-
sibly has a beneficial influence on postural control. The most important argument that points to
a promising effect of COPCA is that key-elements of COPCA, i.e. coaching, variation, challenging,
and exploration, are associated with an improved developmental outcome on the functional mo-
bility scale of the PEDI. Hence combining the RCT with a process evaluation turned out to be the
ultimate combination to examine the research questions. The possible promising effect of COPCA
is in line with the results from the systematic reviews which indicated that general developmental
programmes are the most promising to influence developmental outcome in infants with or at
high risk for developmental motor disorders.
9.2 the VIP project; strengths and limitations
The early detection of infants at high risk for developmental motor disorders, such as cerebral
palsy (CP) offers the opportunity for intervention at young age. Research showed that the best
time window for early intervention in terms of active stimulation of the infant lies between 40-44
weeks post menstrual age and 15 months postnatally (De Graaf-Peters and Hadders-Algra 2006).
In the VIP project the infants received intervention from three to six months which lies entirely
within this recommended time window.
Selection procedure and study group
The infants were selected to participate in the VIP project when they showed definitely abnormal
general movements at the age of ten weeks corrected age. Various studies indicated that the pre-
sence of definitely abnormal GM is associated with a high risk for developmental motor disorders
(Prechtl 2001, Hadders-Algra 2004). It turned out that approximately 25% of the infants who had
been admitted to the NICU showed definitely abnormal General Movements (GMs). The response
to participate in the VIP project was 75% which resulted in a final study group of 46 infants. Chief
among the reasons for families to refuse participation were the distance to the UMCG and the
load and duration of the study.
One of the limitations of the VIP project was that we studied a relatively small group of 46
infants. Although power analysis before the start of the project showed that a sample size of 40
infants would be appropriate to detect differences in treatment, it is still a very small group to
detect real, and clinically worthwhile, differences in treatment. This is even more complicated by
the fact that is considered unethical to assign participants to a non-treatment control group (Maj-
nemer 1998, Siebes et al 2002). Also in the VIP project we encountered this challenge. Therefore it
was only possible to compare the effects of COPCA and TIP. The differences which we observed in
the RCT represent only the additional value of COPCA compared to TIP. It would be interesting
to know what the effects of both COPCA and TIP would be when they are compared to a group
that received no intervention. These two aspects indicate that we have to be very careful with the
interpretation and generalization of the results of the VIP project.
Another issue, which poses a challenge to the possibility to detect differences in develop-
mental outcome between two groups of high risk infants, is that development in early childhood
is very variable. In young infants brain dysfunction is expressed as generalized and unspecific.
Infants with a left-sided intraventricular hemorrhage may respond with signs of hypotonia,
hypertonia, hypokinesia or with a hyperexcitability syndrome (Hadders-Algra 2004). To make it
even more complicated, brain dysfunction present at birth is not always permanent. Due to neu-
rodevelopmental changes in the brain part of the infants with neonatal neurological symptoms
may recover (Hadders-Algra 2002, 2004). Note that also the opposite is possible (Hadders-Algra
2002, 2004). This makes the developmental course of infants with a high risk for developmental
motor disorders a fairly unpredictable process (Hadders-Algra 2002, Lebeer and Rijke 2003).
Evaluation and outcome measures
One of the strengths of the VIP project was that we studied the effect of intervention on short
term (immediately after the intervention at 6 months CA) and on long term (one year after the
intervention at 18 months CA). The outcome measures used in the VIP project to evaluate the
developmental outcome were age specific and belong to the international standard. It is however
acknowledged that standardized outcome measures which are often applied to measure changes
in developmental outcome are in general characterized by a lack of sensitivity to detect small
changes in motor or cognitive development although these small changes may have an important
influence on the functional abilities of the child. The use of discriminative measures, which focus
on the comparison of a child’s score with an age-equivalent score, may be one of the reasons that
so little effect of early intervention is found (Ketelaar et al 1998).
Neuromotor outcome was evaluated with two age specific instruments; the TINE (Touwen
Infant Neurological Examination; Hadders-Algra et al 2010) from three to six months and the
Hempel assessment at 18 months CA (Hempel 1993). Additionally the Neurological Optimality
Score (NOS; Huisman et al 1995) was used which is known to be an excellent instrument to evalu-
ate subtle differences in neurodevelopmental outcome (Bouwstra et al 2006). A striking finding
was that the neurological outcome in the COPCA and TIP group were similar at 6 and 18 months.
Considering the opposite view of COPCA and TIP on two important aspects of neurological

168 169
condition, i.e. muscle tone and abnormal movement patterns this was an interesting finding. In
COPCA no attention is paid to these impairments while in TIP treatment, especially in the classic
NDT variant, they play a fundamental role. It seems that therapeutic techniques aiming to influ-
ence muscle tone and movement patterns applied during early infancy do not affect neurological
outcome at 18 months.
While only a minority of the infants at high risk for developmental motor disorders develops
cerebral palsy (Marlow 2004), more than 50 percent shows minor neurological dysfunctions
(Stahlmann et al 2007). Although neurological outcome did not differ between both groups,
also the majority of the infants who participated in the VIP project (n=31) had complex minor
neurological dysfunction (MND) at 18 months CA. During the intervention period most infants
continued to show signs of neurological dysfunction, indicating that they were still in need of
physiotherapeutic guidance. The presence of complex MND during early infancy is a risk-factor
for the development of MND, DCD, attention and behavioural problems at school age (Jongmans
et al 1997, Hadders-Algra 2003, 2004, Groen et al 2005).
Motor development in the VIP project was evaluated with the AIMS. One problem was that at
18 months the AIMS suffered from a ceiling effect as the majority of the infants already reached
the stage of independent walking. Therefore it was not possible to differentiate between the
motor outcome of the COPCA and TIP group at the follow-up. Another problem associated with
the AIMS is that it mainly focuses on the observation of milestones and specific aspects of motor
behaviour. What we need is a reliable, valid and sensitive instrument which in addition to mo-
tor milestones pays attention to qualitative aspects of motor development. Possibly the recently
developed Infant Motor Profile (IMP; Heineman et al 2008) can solve this problem. The IMP is a
video-based assessment of motor behaviour in infancy that does not only address the infant’s mo-
tor abilities but also addresses variation in motor behaviour, the ability to select movement strate-
gies, symmetry, and fluency of motor behaviour. Currently the data of the IMP for the infants who
participated in the VIP project are being processed.
Cognitive outcome was assessed with the mental scale of the Bayley Scales of Infant Develop-
ment (BSID). The BSID mental scale, like most developmental instruments which measure cogni-
tive development in young children, heavily relies on fine motor skills. This will result in lower
scores for motor-impaired infants. Recently an adapted Low Motor version has been developed
especially for children with motor impairments in which the mental scale is less dependent of the
motor capacities of the child. Ruiter (2007) showed that the children with motor impairments
scored significantly higher on the Low motor version compared to the standard version of the
BSID mental scale. Probably this version gives a more adequate representation of the cognitive
abilities of infants with developmental motor disorders and can be used in future research.
One should keep in mind that the questionnaires we used, i.e. the KIDS, MPOC, NCSQ,
carry the risk that caregivers reflect on desired rather than actual behaviour. It is furthermore
important to realize what the effect might be of certain questions on the caregivers. For instance
the NCSQ contains many confronting questions for parents who had experienced stressful
times when the infant was at the neonatal intensive care unit. By completing the MPOC many
caregivers reported difficulties with judging the care provided by different service providers. Often
they had not matching medical experiences with service providers in different settings such as
the University Medical Center and a regional hospital. While participating in the VIP project they
could also judge the attitude of the physiotherapist. Therefore we recommend in line with Nijhuis
et al (2007) that in future research the family-centredness of different settings should be assessed
separately.
Intervention
Research into the evaluation of the effectiveness of early intervention is very complex for a host of
reasons. Chief among them is that physical therapy is not a specific treatment that is delivered in a
standardized manner. In other words, there is no discrete dosage administered under specific, in-
variable procedures in conditions that are held constant. The frequency or duration could be held
constant, but the procedures depend upon the therapists’ skill level and specific aims and vary
accordingly. While the treatment setting could be standardized, the child’s family or the child’s
responses to the treatment could never be (Butler and Darrah 2001).
Some infants already got physical therapy before they entered the VIP project and since they
- as already mentioned - continued to show signs of neurological dysfunction during the interven-
tion period most infants also received some physical therapy sessions after the age of 6 months.
After the intervention period the suggestions of the paediatrician regarding physical therapy were
followed. Twenty-five of the infants (7 COPCA, 16 TIP) received more than 10 sessions after the
age of 6 months, including the ten infants who developed CP. To cope with this additional hetero-
geneity in therapy the frequency of additional intervention sessions was taken into account in the
multivariate analyses of outcome.
It turned out that TIP was characterized by a large heterogeneity in treatment application
which was inherent to the evolvement of treatment techniques and theoretical assumptions
over the years and to the incorporation of new treatment approaches into older ones (Bly 1991,
Howle 2002, Blauw-Hospers et al 2009). This heterogeneity makes it very difficult to interpret the
results because the contents of the individual treatments differ so much that the aspects which
are responsible for the observed changes cannot be distinguished. The process evaluation gave
us a reliable quantification of TIP in the Netherlands. It enabled us to tackle the problem of the
heterogeneity and answer the question which aspects of the TIP treatment are associated with
developmental outcome (Chapter 7).
The fact that most associations between PT-actions, in particular the typical COPCA ac-
tions, during the intervention period were associated with developmental outcome measures at
18 months CA is an interesting finding. Improvement of outcome can likely be expected when
a behavioural change has occurred. In the field of early intervention this means that interven-
tion strategies should be incorporated into daily caregiving tasks, which is one of the goals of the
COPCA programme (Dirks and Hadders-Algra 2003, Dirks et al submitted).

170 171
9.3 Implications for physiotherapeutic practice and directions for future research
Paediatric physical therapy for infants at high risk for a developmental motor disorder can be
considered as a field in development. No evidence is available that traditional therapy approaches,
such as NeuroDevelopmental Treatment and treatment according to Vojta have a positive effect
on the development of infants at high risk for developmental motor disorders (Blauw-Hospers
and Hadders-Algra 2005, Blauw-Hospers et al 2007, Spittle et al 2007). This is the reason that
Damiano wrote ‘Based on the existing evidence the traditional approaches demand serious recon-
sideration by those who still advocate them’ (Damiano 2006). The findings that evidence for the
effectiveness of the traditional EI programmes is limited initiated important shifts in the applica-
tion of therapy. The most important advances are emphasis on functionality instead of normal-
ity, the infant is an active participant of the therapy, and focus on family dynamics. Currently,
evidence is accumulating that intervention from a more functional approach focusing on general
development is most promising to influence developmental outcome in a beneficial way (Chapter
3 and 4). Research has indicated that the involvement of caregivers can be associated with positive
effects both on the development of the child (Ketelaar et al 1998, Law et al 1998, King et al 2004)
as well as on the caregivers in terms of an increase in parental skills, improved well-being and a
decreased level of parental stress (King et al 1996, Rosenbaum et al 1998, Jansen et al 2003, King et
al 2004, Raina et al 2005). Another factor which may add to the possibility that intervention will
sort a long term effect is the implementation of intervention strategies into daily activities. In the
COPCA intervention focus is on family function, family autonomy and activities and participation
in daily life activities. The results of the VIP project suggest that this strategy may be effective.
In this thesis the first results on the implementation of the COPCA programme are described.
Although the effects on RCT level were small, the results from the process evaluation showed
that key aspects of COPCA, i.e. family involvement and educational actions, application of large
variation in challenging the infant to produce motor behavior by him/herself and allow the infant
to continue this activity, and stimulation of motor behavior at the verge of the infant’s capabili-
ties, were associated with improvements in developmental outcome at 18 months (Chapter 7).
To establish real insight in the effects and working mechanisms of COPCA on developmental
outcome more research has to be performed. It is likely that the effect of intervention is a combi-
nation of several factors which are related to the condition of the infant, the family, the therapist,
the contents of the intervention, and environmental factors. As some problems related to early
neurological dysfunction become more visible at school age future studies should include a longer
follow-up.
We described a first step in objectifying physiotherapeutic practice. By uncovering the
contents of infant physical therapy in the Netherlands we obtained insight into which actions
constitute practice and we were able to study relations with developmental outcome. A next step
in objectifying physiotherapeutic practice might be a study on the similarities and differences in
the application of infant physical therapy in other countries. Additionally more research must be
performed to optimize the psychometric requirements of the observation protocol.
Future research should not only focus on the development of new intervention strategies. Ade-
quate assessment techniques are also indispensable for the evaluation of the effectiveness of
intervention. There is a need for more scientific sound qualitative instruments which are able to
assess and evaluate the developmental outcome of infants at high risk for developmental motor
disorders more accurately. Current advances show that the psychometric properties of several
qualitative instruments are being examined (for instance the Infant Motor Profile (Heineman et
al 2008), the Touwen Infant Neurological Examination (Hadders-Algra et al 2010), and the Low
Motor Version of the Bayley Scales of Infant Development (Ruiter 2007)) suggesting that these
methods can be applied in future studies.
The implementation and evaluation of a new outcome measure or intervention programme into
clinical practice takes several years (Ketelaar et al 2008). Here a possible threat comes up. As
physiotherapists tend to include only techniques they perceive as helpful into their treatment, the
risk exists that a new intervention is not implemented in the way it was intended. Good education
is essential to diminish this threat. Although the results are still premature and more research
has to be performed, COPCA - a family friendly approach to intervention - has the potential to
influence developmental outcome of infants with high risk for developmental motor disorders in
a beneficial way. Currently another trial on the effectiveness of COPCA is carried out: Learn to
Move 0-2 years (L2M0-2). L2M0-2 is part of a multicenter trial on the effectiveness of intervention
in children and adolescents with CP. In L2M0-2 many of the limitations encountered in the VIP
project are accounted for. In the near future this will result in more knowledge about the effect of
early intervention on the developmental outcome of infants at high risk for developmental motor
disorders.
172 173
references
Ade-Hall RA, Moore AP. Botulinum toxin type A in the treatment of lower limb spasticity in cerebral palsy. Cochrane Database Syst Rev 2000, Issue 1. Art. No.: CD001408. DOI: 10.1002/14651858.CD001408.
Anttila H, Autti-Rämö I, Suoranta J, Mäkelä M, Malmivaara A. Effectiveness of physical therapy inter-ventions for children with cerebral palsy: a systematic review. BMC Pediatr 2008;24;8-14.
Aylward GP, Pfeiffer SI, Wright A, Verhulst SJ. Out-come studies of low birth weight infants published in the last decade: a meta-analysis. J Pediatr 1989;115:515-520.
Bhutta AT, Cleves MA, Casey PH. Cognitive and be-havioral outcomes of school-aged children who were born preterm. JAMA 2002;288:728-737.
Blauw-Hospers CH, Hadders-Algra M. Fact or fiction: a systematic review on the effects of early interven-tion on motor development. Dev Med Child Neurol 2005;47:421-432.
Blauw-Hospers CH, de Graaf-Peters VB, Dirks T, Bos AF, Hadders-Algra M. Indications that early interven-tion in infants at high risk for a developmental motor disorder may improve motor and cognitive develop-ment. Neurosci Biobehav Rev 2007;31:1201-1212.
Blauw-Hospers CH, Dirks T, Hulshof LJ, Hadders-Algra M. Opening the Black-Box: development of a quantitative tool to assess physical therapy contents in infancy. Pediatr Phys Ther 2010;22:189-198.
Bly L. A historical and current view of the basis of NDT. Pediatr Phys Ther 1991;3:131-135.
Bouwstra H, Dijck-Brouwer J, Decsi T, Boehm G, Bo-ersma ER, Muskiet FA, Hadders-Algra M. Neurologic condition of healthy term infants at 18 months: posi-tive association with venous umbilical DHA status and negative association with umbilical trans-fatty acids. Pediatr Res 2006:60;334-339.
Butler C, Darrah J. Effects of neurodevelopmental treatment (NDT) for cerebral palsy: an AACPDM evi-dence report. Dev Med Child Neurol 2001;43:778-790.
Casto G, Mastropieri MA. The efficacy of early intervention programs: a meta-analysis. Except Child 1986;52:417-424.
Damiano DL. Activity, activity, activity: rethinking our physical therapy approach to cerebral palsy. Phys Ther 2006;86:1534-1540.
De Graaf-Peters VB, Blauw-Hospers CH, Dirks T, Bakker J, Bos AF, Hadders-Algra M. Development of postural control in typically developing children and children with cerebral palsy: possibilities for interven-tion? Neurosci Biobehav Rev 2007;31:1191-1200.
Dirks T, Hadders-Algra M. COPCA working manual; 2003.
Dirks T, Blauw-Hospers CH, Hulshof LJ, Hadders-Algra M. Differences between a Family Centered Program “Coping and Caring for Infants with Special Needs” and Infant Treatment based on Principles of NeuroDevelopmental Treatment. Submitted for publication.
Flottorp S, Havelsrud K, Oxman A: Process evaluation of a cluster randomized trial of tailored interventions to implement guidelines in primary care – why is it so hard to change practice? Fam Pract 2003;20:333-339.
Guralnick MJ (editor). The effectiveness of early interven-tion. Baltimore: Paul H. Brookes Publishing Co; 1997.
Hadders-Algra M. Two distinct forms of minor neu-rological dysfunction: perspectives emerging from a review of data of the Groningen Perinatal Project. Dev Med Child Neurol 2002;44: 561-571.
Hadders-Algra M. Developmental Coordination Dis-order: Is clumsy motor behavior caused by a lesion of the brain at early age? Neural Plast 2003;10:39-50.
Hadders-Algra M. General movements: a window for early identification of children at high risk of develop-mental disorders. J Pediatr 2004;145:S12–S18.
Hadders-Algra M. The neuromotor examination of the preschool child and its prognostic significance. Ment Retard Dev Disabil Res Rev 2005;11:180-188.
Hadders-Algra M, Heineman KR, Bos AF, Middel-burg KJ. Minor neurological dysfunction in infancy: strengths and limitations. Dev Med Child Neurol 2010:52;87-92.
Heineman KR, Bos AF, Hadders-Algra M. The Infant Motor Profile: a standardized and qualitative method to assess motor behaviour in infancy. Dev Med Child Neurol 2008;50:275-282.
Hempel MS. Neurological development during tod-dling age in normal children and children at risk of de-velopmental disorders. Early Hum Dev 1993:34;47–57.
Hoare BJ, Wasiak J, Imms C, Carey L. Constraint-induced movement therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy. Cochrane Database Syst Rev 2007, Issue 2. Art. No.: CD004149. DOI: 10.1002/14651858.CD004149.pub2.
Howle JM. Neuro-Developmental Treatment Approach: Theoretical Foundations and Principles of Clinical Practice. Laguna Beach, CA: Neuro-Developmental Treatment Association; 2002.
Huisman M, Koopman-Esseboom C, Lanting CI, Van der Paauw CG, Tuinstra LGMTh, Fidler V, Weisglas-Kuperus N, Sauer PJJ, Boersma ER, Touwen BCL. Neurological condition in 18-month-old children perinatally exposed to polychlorinated biphenyls and dioxins. Early Hum Dev 1995:43;165-176.
Hullegie WAMM. Practice based evidence: contra-intuïtieve inzichten bij oefentherapie. Ned Tijdschr Fysiother 2009;119:112-113.
Jansen LM, Ketelaar M, Vermeer A. Parental experi-ence of participation in physical therapy for children with physical disabilities. Dev Med Child Neurol 2003;45:58-69.
Jongmans M, Mercuri E, de Vries L, Dubowitz L, Henderson SE. Minor neurological signs and percep-tual-motor difficulties in prematurely born children. Arch Dis Childh 1997;76:F9-14.
Ketelaar M, Vermeer A, Helders PJ. Functional motor abilities of children with cerebral palsy: a systematic literature review of assessment measures. Clin Rehabil 1998;12:369-380.
Ketelaar M, Russell DJ, Gorter JW. The challenge of moving evidence-based measures into clinical prac-tice: lessons in knowledge translation. Phys Occup Ther Pediatr 2008;28:191-206.
King SM, Rosenbaum PL, King GA. Parents’ percep-tions of caregiving: development and validation of a measure of processes. Dev Med Child Neurol 1996;38:757-772.
King S, Teplicky R, King G, Rosenbaum P. Family-centered service for children with cerebral palsy and their families: a review of the literature. Semin Pediatr Neurol 2004;11:78-86.
Law M, Darrah J, Pollock N, King G, Rosenbaum P, Russell D, Palisano R, Harris S, Armstrong R, Watt J. Family-centred functional therapy for children with cerebral palsy: an emerging practice model. Phys Oc-cup Ther Pediatr 1998;18:83-102.
Lebeer J, Rijke R. Ecology of development in chil-dren with brain impairment. Child Care Health Dev 2003;29:131-140.
Lettinga AT, Reynders K, Mulder TH, Mol A. Pitfalls in effectiveness research: a comparative analysis of treatment goals and outcome measures in stroke rehabilitation. Clin Rehabil 2002;16:174-81.
Majnemer A. Benefits of early intervention for chil-dren with developmental disabilities. Semin Pediatr Neurol 1998;5:62-69.
Mandich AD, Polatajko HJ, Macnab JJ, Miller LT. Treatment of children with Developmental Coordina-tion Disorder: what is the evidence? Phys Occup Ther Ped 2001;20:51-68.
Marlow N. Neurocognitive outcome after very preterm birth. Arch Dis Child Fetal Neonatal Ed 2004;89:F224-F228.
May CR, Mair FS, Dowrick CF, Finch TL. Process evaluation for complex intervention in primary care: understanding trials using the normalization process model. BMC Fam Pract 2007;24:8:42.

174 175
Medical Research Council: A framework for develop-ment and evaluation of complex interventions to improve health. London: Medical Research Council; 2000.
Ment LR, Vohr B, Allan W, Katz KH, Schneider KC, Westerveld M, Duncan CC, Makuch RW. Change in cognitive function over time in very low-birth-weight infants. JAMA 2003;289:705-711.
Nijhuis BJG, Reinders-Messelink HA, de Blecourt ACE, Hitters MWMCG, Groothoff JW, Nakken H, Postema K. Family-centred care in family-specific teams. Clin Rehabil 2007;21:660-671.
Oakley A, Strange V, Bonell C, Allen E, Stephenson J: Health services research – Process evaluation in randomised controlled trials of complex interventions. Brit Med J 2006;332:413-416.
Parry TS. The effectiveness of early intervention: a critical review. J Paediatr Child Health 1992;28:343-346.
Parette HP, Hourcade JJ. A review of therapeutic in-tervention research on gross and fine motor progress in young children with cerebral palsy. Am J Occup Ther 1984;38:462-468.
Prechtl HFR. General movement assessment as a method of developmental neurology: new para-diGM and their consequences. Dev Med Child Neurol 2001;43:836-842. Raina P, O’Donnell M, Rosenbaum P, Brehaut J, Walter SD, Russell D, Swinton M, Zhu B, Wood E. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005;115:626-636.
Rosenbaum P, King S, Law M, King G, Evans J. Family-centred service: A conceptual framework and research review. Phys Occup Ther Pediatr 1998;18:1-20.
Ruiter SAJ. The BSID-II-NL for assessing children with specific impairments. Groningen, The Netherlands; 2007 (PhD-thesis).
Shonkoff JP, Hauser-Cram P. Early Intervention for disabled infants and their families: a quantitative analysis. Pediatrics 1987;80:650-658.
Siebes RC, Wijnroks L, Vermeer A. Qualitative analysis of therapeutic motor intervention programmes for children with cerebral palsy: an update. Dev Med Child Neurol 2002; 44:593-603.
Simeonsson RJ, Cooper DH, Scheiner AP. A review and analysis of the effectiveness of early intervention programs. Pediatrics 1982;69:635-641.
Spittle AJ, Orton J, Doyle LW, Boyd R. Early de-velopmental intervention programs post hospital discharge to prevent motor and cognitive impair-ments in preterm infants. Cochrane Database Syst Rev 2007;18:CD005495.
Stahlmann N, Hartel C, Knopp A, Gehring B, Kiecksee H, Thyen U. Predictive value of neurodevelopmental assessment versus evaluation of general movements for motor outcome in preterm infants with birth weight < 1500g. Neuropediatrics, 2007;38:91-99.
Turnbull JD. Early intervention for children with or at risk of cerebral palsy. Am J Dis Child 1993;147:54-59.
Vohr BR, Garcia Coll CT. Neurodevelopmental and school performance of very low-birth-weight infants: a seven-year longitudinal study. Pediatrics 1985;76,345-350.
Wasiak J, Hoare B, Wallen M. Botulinum toxin A as an adjunct to treatment in the management of the upper limb in children with spastic cerebral palsy. Cochrane Database Syst Rev 2004, Issue 3. Art. No.: CD003469. DOI: 10.1002/14651858. CD003469.pub3.
S U M M a ry
Young infants, who are at risk for developmental motor disorders, such as cerebral palsy (CP) or
developmental coordination disorder, are often referred to early intervention services. The field of
early intervention consists of multidisciplinary developmental, educational and therapeutic
services provided to children from birth to 5 years of age. In this thesis early intervention is
restricted to paediatric physical therapy for infants up to 18 months corrected age (CA). The intro-
duction (Chapter 1) starts with an overview of the main influences on paediatric physical therapy
in the Netherlands. Paediatric physical therapy for infants at high risk for a developmental motor
disorder can be considered as a field in development. Based on findings that evidence for the
effectiveness of the traditional early intervention programmes (NeuroDevelopmental Treatment,
treatment according to Vojta, and Sensory Integration Therapy) is limited, shifts in the applica-
tion of therapy were initiated. The most important advances are a focus on functionality instead
of normality, the infant as an active participant of the therapy and the inclusion of the family.
The first aim of this thesis was to review the effects of early physiotherapeutic intervention on
motor and cognitive development of infants with a high risk for developmental motor disorders
aged less than 18 months (Chapter 3 and 4). The reviews showed that the effect of early intervention
programmes which focus primarily on the improvement of motor development is inconclusive.
It turned out that the type of intervention which might be beneficial for infants at preterm age
differs from the type which is effective for infants who have reached at least term age. At preterm
age infants seem to benefit most from intervention which aims at mimicking the intrauterine
environment. After term age, general developmental programmes in which parents learn how to
promote infant development can exert a positive effect on motor and cognitive development.
Traditional therapy approaches, such as NeuroDevelopmental Treatment and treatment according
to Vojta, do not influence the developmental outcome of infants at high risk for developmental
motor disorders.
The results of both reviews indicated that intervention programmes with an onset after term
age which focus on the stimulation of self-produced motor behaviour may exert a beneficial effect
on motor and cognitive development. This knowledge served as one of bases for the development
of a new type of physiotherapeutic intervention, COPCA. COPCA is the abbreviation of Coping
with and Caring for infants with special needs – a family centred programme. It is a family
relationship oriented programme consisting of two theoretical constructs. The first component
is formed by a family involvement and educational parenting component. The second theoretical
component, a neurodevelopmental one, is based on the principles of the Neuronal Group Selec-
tion Theory.
The second aim of this thesis was to evaluate the effects of the COPCA intervention on develop-
mental outcome. In the early intervention project VIP (in Dutch “vroegtijdig interventie project”;
176 177
Chapter 2) 46 high-risk infants were randomly assigned to receive COPCA (n=21) or traditional
infant physical therapy (TIP; n=25) between 3 to 6 months CA. Developmental status of the infants
was assessed at 3, 4, 5, 6 and 18 months CA with instruments measuring at impairment level (neu-
rological examination) to instruments on the level of activity and participation (PEDI).
The randomized controlled trial (RCT) revealed that developmental outcome in both groups
was largely identical (Chapter 7), except for cognitive outcome. Ten infants were diagnosed with
CP at the age of 18 months CA. The majority of infants (15 COPCA, 16 TIP) showed complex minor
neurological dysfunction, which puts the infant at risk for learning and behavioural disorders at
school age. The RCT had two interesting results. First, there was an interaction effect between
the type of intervention and the level of maternal education in the relative drop in MDI score
between 6 and 18 months CA. Infants whose mother had a lower level of education declined less
in MDI score over time compared to infants whose mother had finished a higher education. This
effect was in particular present in the COPCA group. This suggests that in particular mothers
with a lower education benefit more from coaching by a therapist who uses COPCA principles,
while mothers with a higher education are less affected by coaching as well as training performed
by a therapist. Second, the finding of a similar neurological outcome in the COPCA and TIP group
is intriguing considering the opposed view of TIP and COPCA on the importance of the neuro-
logical parameters muscle tone and atypical movements. In the TIP treatment, especially when
applied to the original concepts of Bobath and/or NDT, tone influencing by means of handling
techniques plays an important role in the activities of the therapist during intervention sessions.
In COPCA no attention is paid to these impairments. In other words, handling techniques aiming
to influence muscle tone and facilitating movement sequences to improve function, do not seem
to affect neurological outcome.
Some supplementary findings of the VIP project are discussed in Chapter 8. Other data of the
VIP project are currently analysed (motor development in terms of the Infant Motor Profile and
postural control, and video-recordings of daily life activities).
The third aim of this thesis was to evaluate the application of COPCA in daily practice by means
of video analysis. This process evaluation is a prerequisite for the implementation of COPCA
within paediatric physiotherapy. The first step to achieve this was the development of a standard-
ized, theory based, observation protocol detailing essential elements and core features of paedi-
atric physiotherapeutic intervention, which permitted analysis of the content of physical therapy
interventions for infants (Chapter 5). The observation protocol classifies PT actions into eight
mutually exclusive categories: A) Family involvement and educational actions, B) Communication
, C) Facilitation techniques, D) Sensory experience, E) Passive motor experience, F) Self-produced
motor behaviour, no interference with PT /caregiver, G) Challenge to self-produce motor behav-
iour by him/herself; infant is allowed to continue activity, H) Challenge to self-produce motor
behaviour by him/herself; activity flows over into therapeutic handling. The protocol was proven
to meet important psychometric requirements and captured nearly all physiotherapeutic actions
which were performed during intervention sessions of infants at high risk for a developmental
motor disorder. The observation protocol may be used to assess heterogeneity in physical therapy
as it offers a tool to describe operationally what therapists do within treatment sessions across
varying frames of theoretical references. Four conclusions can be drawn from the three studies
(Chapter 5-7) which applied the observation protocol:
1) Traditional infant physical therapy is characterized by a large heterogeneity in implementation
which probably is caused by the application of techniques belonging to different treatment ap-
proaches.
2) A discrepancy exists between actual clinical practice and the physiotherapist’s interpretation of
his or her own actions.
3) The contents of COPCA and TIP sessions differed largely, suggesting that it is possible to
implement COPCA in daily practice by physical therapists who received special training in the
COPCA programme (Chapter 6). The differences found between COPCA and TIP corresponds
to the theoretical frameworks of both approaches. They included differences in the role of care-
givers and the approach of families, in the application of educational actions towards the infant
and in activities to stimulate the infant’s sensorimotor development.
4) Several aspects of the COPCA intervention, i.e. family involvement and educational actions, ap-
plication of large variation in challenging the infant to produce motor behaviour by him/herself
and allow the infant to continue this activity, and stimulation of motor behaviour at the verge
of the infant’s capabilities, were associated with an improved developmental outcome. The use
of facilitation techniques like handling was associated with a worse performance on the func-
tional skills scale of the PEDI. The use of sensory and passive experience was associated with a
short term positive effect on cognitive development.
It is important to realize that the results of this study should be interpreted with caution as the
observed associations do not automatically mean that a causal relation between contents and out-
come exists. Associations between PT actions and outcome are unavoidably contaminated with
the child’s initial degree of impairment. Multivariate statistics were applied to account for this
problem but still more research is needed to examine the influence of the contents of intervention
on developmental outcome.
In Chapter 9 the main findings of this thesis are summarised and discussed and placed into
perspective. Although the differences between the COPCA and TIP group on several aspects of
developmental outcome on RCT level are small, the results suggest that COPCA - a family friendly
approach to intervention - has the potential to influence developmental outcome of infants with
high risk for developmental motor disorders in a beneficial way. The most important argument
that points to a promising effect of COPCA is that key elements of COPCA, i.e. coaching, vari-
ation, challenging, and exploration, are associated with an improved developmental outcome.
Hence combining the RCT with a process evaluation turned out to be the ultimate combination
to examine the research questions. The possible promising effect of COPCA is in line with the

178 179
results from the systematic reviews which indicated that general developmental programmes are
the most promising to influence developmental outcome in infants with or at high risk for devel-
opmental motor disorders.
In the next years the multicenter trial Learn to Move 0-2 years will provide more knowledge about
the effect of early intervention on the developmental outcome of infants at high risk for cerebral
palsy in general and the COPCA programme in particular.
S a M E N Vat t I N G
Jonge kinderen met een verhoogd risico op het krijgen van een motorische ontwikkelingsstoornis,
zoals cerebrale parese (CP) of developmental coordination disorder, komen in aanmerking voor
vroegtijdige interventie. De term vroegtijdige interventie omvat een scala aan multidisciplinaire
therapeutische mogelijkheden die zich richten op de ontwikkeling en opvoeding van kinderen
tussen nul en vijf jaar. In Nederland worden kinderen met een verhoogd risico op het krijgen van
een motorische ontwikkelingsstoornis vaak verwezen naar de kinderfysiotherapeut. In dit proef-
schrift is vroegtijdige interventie afgebakend tot kinderfysiotherapie voor kinderen jonger dan
de gecorrigeerde leeftijd van 18 maanden. De introductie (Hoofdstuk 1) geeft een overzicht van de
belangrijkste ontwikkelingen binnen de kinderfysiotherapie in Nederland. Kinderfysiotherapie is
een discipline die zich de afgelopen decennia sterk heeft ontwikkeld. Er zijn een aantal belangrijke
verschuivingen opgetreden. De nadruk ligt tegenwoordig op functionaliteit in plaats van normale
bewegingspatronen. Ook wordt het gezin actief betrokken bij het therapeutisch proces en neemt
het kind actief deel aan zijn of haar eigen therapie.
Het eerste doel van dit proefschrift was het in kaart brengen van de bestaande effecten van
vroegtijdige fysiotherapeutische interventie op de motorische en cognitieve ontwikkeling van
kinderen die jonger zijn dan 18 maanden en een verhoogd risico hebben op het krijgen van een
motorische ontwikkelingsstoornis (Hoofdstuk 3 en 4). Uit de beide systematische literatuurstudies
blijkt dat het effect van interventies die zich primair richten op het verbeteren van de motorische
ontwikkeling onduidelijk is. Het type interventie dat mogelijk effect heeft, verschilt voor kinderen
op de preterme leeftijd en kinderen die tenminste de à terme leeftijd bereikt hebben. Voor de à
terme leeftijd lijken kinderen het meest baat te hebben bij interventies waarin de situatie van de
baarmoeder wordt nagebootst. Na de à terme leeftijd hebben programma’s die zich richten op de
algemene ontwikkeling van het kind en waarin ouders leren hoe ze de ontwikkeling van hun kind
kunnen stimuleren de meeste potentie. De traditionele benaderingen, zoals NeuroDevelopmental
Treatment en behandeling volgens de methode Vojta, hebben geen effect op de ontwikkeling van
kinderen met een verhoogd risico op het krijgen van een motorische ontwikkelingsstoornis.
De resultaten van beide literatuurstudies laten zien dat interventie programma’s, die starten
na de à terme leeftijd en zich richten op het stimuleren van zelf geproduceerd motorisch gedrag,
de motorische en cognitieve ontwikkeling positief kunnen beïnvloeden. Deze kennis heeft
bijgedragen aan de ontwikkeling van een nieuwe vorm van kinderfysiotherapeutische interven-
tie genaamd COPCA (Coping with and Caring for infants with special needs - a family-centered
programme). COPCA is gericht op de relaties en interacties binnen het gezin. Het programma
is gebaseerd op nieuwe inzichten op het gebied van pedagogiek en gezinsgerichte zorg en op de
principes van de Neuronale Groep Selectie Theorie.

180 181
Het tweede doel van dit proefschrift was het evalueren van het effect van COPCA op de ontwikke-
ling van kinderen met een verhoogd risico op het krijgen van een motorische ontwikkelingsstoor-
nis. Aan het Vroegtijdig Interventie Project (VIP; Hoofdstuk 2) hebben 46 kinderen deelgenomen.
De kinderen zijn via blokrandomisatie verdeeld over de experimentele COPCA groep (21 kinderen)
en de controlegroep (25 kinderen) die de traditionele vorm van kinderfysiotherapeutische begelei-
ding (TIP) op indicatie van de kinderarts kreeg. De interventieperiode duurde van 3 tot 6 maan-
den. De ontwikkeling van de kinderen is gemeten op de gecorrigeerde leeftijd van 3, 4, 5, 6 en 18
maanden aan de hand van meetinstrumenten die zich richten op de neuromotore ontwikkeling,
het psychosociaal functioneren en de neurofysiologische parameters van de houdingsregulatie.
Uit de analyses kwam naar voren dat er op groepsniveau (RCT) weinig verschillen waren
tussen de COPCA en de TIP groep (Hoofdstuk 7), behalve in de cognitieve ontwikkeling. Tien kin-
deren hadden een CP ontwikkeld op de gecorrigeerde leeftijd van 18 maanden. Het merendeel van
de kinderen (15 COPCA, 16 TIP) liet de complexe vorm van minor neurological dysfunction zien,
waardoor ze op de schoolleeftijd meer risico lopen op leer- en gedragsproblemen. Twee interes-
sante resultaten kwamen uit het RCT naar boven. Ten eerste bestond er een interactie tussen het
opleidingsniveau van de moeder en het type interventie met de verandering in de cognitieve uit-
komst tussen 6 en 18 maanden. Dit betekende dat kinderen van moeders met een lagere opleiding
uit de COPCA groep minder achteruitgingen in hun MDI score dan andere kinderen. Dit sugge-
reert dat moeders met een lager opleidingsniveau meer profiteren van het coachen door een the-
rapeut die de COPCA methode gebruikt. Ten tweede viel op dat de neurologische uitkomst in de
COPCA en de TIP groep vergelijkbaar was. Dit is interessant gezien de tegenovergestelde kijk van
TIP en COPCA op neurologische parameters zoals spierspanning en afwijkende bewegingen. In
TIP vormen tonus beïnvloedende strategieën een belangrijke rol in de fysiotherapeutische acties,
terwijl COPCA hier geen aandacht aan besteed. Oftewel, fysiotherapeutische technieken gericht
op het beïnvloeden van de spierspanning en het faciliteren van ‘normale’ bewegingspatronen lij-
ken geen effect te hebben op de neurologische ontwikkeling. In Hoofdstuk 8 staan een aantal aan-
vullende resultaten van meetinstrumenten uit het VIP project beschreven die niet gepubliceerd
zijn. Andere uitkomsten worden momenteel geanalyseerd, zoals de motorische ontwikkeling in
termen van de Infant Motor Profile, parameters van de houdingsregulatie en video opnames van
activiteiten in het dagelijks leven (baden en spelen).
Het derde doel van dit proefschrift was de evaluatie van de toepasbaarheid van COPCA in de da-
gelijkse praktijk. Daarvoor zijn video opnames gemaakt van fysiotherapeutische behandelingen op
4 en 6 maanden. Om de inhoud van de fysiotherapeutische behandeling te kunnen analyseren, is
eerst een gestandaardiseerd observatie protocol ontwikkeld (Hoofdstuk 5). Dit protocol is opge-
bouwd uit de belangrijkste elementen en kern items van kinderfysiotherapeutische interventie.
Fysiotherapeutische handelingen worden ingedeeld in 8 categorieën: A) Mate van betrokkenheid
van het gezin en opvoedingselementen gericht op het kind/gezin, B) Communicatie, C) Facilitatie
technieken, D) Sensorische stimulatie, E) Passief bewegen, F) Zelf geproduceerd motorisch gedrag
zonder tussenkomst van de fysiotherapeut of ouder G) Uitgelokt zelf geproduceerd motorisch
gedrag dat wordt voortgezet door het kind, H) Uitgelokt zelf geproduceerd motorisch gedrag dat
overgaat in handling. Analyses lieten zien dat het protocol voldoet aan belangrijke psychome-
trische eisen zoals een voldoende inter- en intrabeoordelaarsbetrouwbaarheid en dat bijna alle
fysiotherapeutische handelingen gescoord kunnen worden in de categorieën van het protocol. Het
observatieprotocol kan gebruikt worden als instrument om de heterogeniteit in de fysiotherapie
te meten. Het geeft een gedetailleerd overzicht van de handelingen die een kinderfysiotherapeut
toepast binnen zijn of haar behandeling en houdt tegelijkertijd rekening met verschillende theore-
tische referentiekaders. Uit de studies waarin het observatieprotocol toegepast is (Hoofdstuk 5-7),
kunnen vier conclusies worden getrokken:
1) Traditionele kinderfysiotherapeutische begeleiding wordt gekenmerkt door een zeer heterogene
toepassing. Dit wordt mogelijk veroorzaakt door het integreren van technieken uit verschillende
stromingen binnen één behandeling.
2) Er bestaat een discrepantie tussen de werkelijke fysiotherapeutische handelingen en de inter-
pretatie van de kinderfysiotherapeut over de handelingen die hij/zij toepast.
3) De inhoud van COPCA en TIP is zeer verschillend (Hoofdstuk 6). Dit suggereert dat het mogelijk
is om COPCA te implementeren in de dagelijkse praktijk, mits het gegeven wordt door fysiothe-
rapeuten die een formele training in de COPCA methode gevolgd hebben. De verschillen tussen
COPCA en TIP corresponderen met de theoretische kaders van beide interventieprogramma’s.
Er bestaan verschillen in de rol van de ouders en de benadering van de familie, in de opvoe-
dingselementen gericht op het kind en in activiteiten die zich richten op het stimuleren van de
sensomotorische ontwikkeling van het kind.
4) De inhoud van de behandeling speelt wel degelijk een rol bij de ontwikkeling van kinderen met
een hoog risico op een motorische ontwikkelingsstoornis. Een aantal aspecten van de COPCA
interventie , namelijk de mate van betrokkenheid van de familie en opvoedingselementen
gericht op het kind/gezin (met name coaching), het uitlokken van zelf geproduceerd motorisch
gedrag dat wordt voortgezet door het kind met veel variatie en het stimuleren van motorisch ge-
drag op de grens van de mogelijkheden die een kind heeft, zijn geassocieerd met een betere ont-
wikkelingsuitkomst. Het gebruik van facilitatie technieken, zoals handling, was geassocieerd
met een slechtere uitkomst op de functionele vaardigheden schaal van de PEDI. Sensorische
stimulatie en passief bewegen waren op de korte termijn geassocieerd met een betere cognitieve
ontwikkeling, maar dit verband was niet meer aanwezig op 18 maanden. Het is belangrijk om te
beseffen dat de resultaten van deze studie voorzichtig geïnterpreteerd dienen te worden aange-
zien het bestaan van een associatie niet automatisch betekent dat er een causale relatie bestaat
tussen de inhoud en de uitkomstmaat. Associaties tussen fysiotherapeutische handelingen en
ontwikkeling zijn onvermijdelijk gecontamineerd met de uitgangssituatie van het kind. Om dit
probleem te ondervangen hebben we gebruik gemaakt van multivariate statistiek, maar er is
meer onderzoek nodig om de invloed van de inhoud van fysiotherapeutische interventie op de
ontwikkeling vast te kunnen stellen.
182
In Hoofdstuk 9 wordt een overzicht gegeven van de belangrijkste bevindingen uit dit proefschrift.
Alhoewel de verschillen tussen de COPCA en de TIP groep op groepsniveau klein zijn, lijkt het
erop dat COPCA mogelijk de ontwikkeling van kinderen die een verhoogd risico hebben op het
ontwikkelen van een motorische ontwikkelings-stoornis positief kan beïnvloeden. Deze gedachte
wordt m.n. ondersteund door de bevinding dat een aantal kernitems van COPCA, namelijk
coachen, variëren, uitdagen en exploreren, geassocieerd zijn met een betere ontwikkeling. We
concludeerden dan ook dat het uitbreiden van de RCT met een procesevaluatie de mogelijkheid
schepte om de onderzoeksvragen goed te kunnen beantwoorden. Het mogelijke positieve effect
van COPCA komt overeen met de resultaten van de systematische literatuurstudies waaruit
blijkt dat vroegtijdige interventie programma’s, die zich richten op de algehele ontwikkeling
van het kind en waarin ouders leren hoe ze de ontwikkeling van hun kind kunnen stimuleren,
de ontwikkeling van kinderen met een verhoogd risico op het krijgen van een motorische
ontwikkelingsstoornis positief kunnen beïnvloeden.
In de komende jaren zal het onderzoek Learn to Move 0-2 jaar meer inzicht verschaffen in het ef-
fect van vroegtijdige interventie op de ontwikkeling van kinderen met een hoog risico op cerebrale
parese in het algemeen en in het COPCA programma in het bijzonder.

184 185
Da N K WO O r DEindelijk ligt het er dan, mijn proefschrift. Natuurlijk heb ik dit niet alleen gedaan en hebben veel
mensen een bijdrage geleverd aan het tot stand komen van dit proefschrift, direct dan wel indirect.
Ik zou graag op deze plek graag iedereen persoonlijk willen bedanken, maar het is onmogelijk om
iedereen bij naam te noemen. Daarom wil ik graag, voor ik enkele mensen persoonlijk ga bedanken,
alle teamgenoten, toeschouwers en ontspanners, ontzettend bedanken! Zonder jullie steun en aan-
moediging was het nooit gelukt!
Allereerst wil ik de 46 kinderen en hun ouders die hebben deelgenomen aan het VIP project ontzet-
tend bedanken voor hun bereidwilligheid, hun inzet en hun vertrouwen om ons een kijkje te geven
in hun gezin.
Prof. dr. M. Hadders-Algra, beste Mijna, de draaiende motor van het instituut voor Ontwikkelings-
neurologie en mijn eerste en enige promotor. Dankzij jouw enorme betrokkenheid en enthousiasme
is dit proefschrift mede tot stand gekomen. Ik heb in de afgelopen jaren enorm veel van je geleerd
en wil je bedanken voor je vertrouwen dat het met mijn proefschrift wel een keer goed zou komen
(al heb je daar misschien tussendoor wel eens – net als ikzelf – aan getwijfeld). Ik heb me vaak afge-
vraagd uit hoeveel uur jouw dag eigenlijk bestond. Of ik nu ’s avonds of in het weekend een e-mail
stuurde, altijd was daar een bijzonder snelle reactie op mijn vragen en had je de stukken van com-
mentaar en correcties voorzien.
Tineke Dirks, ook al ben je niet officieel promotor, toch voelt het wel een beetje zo. Wat heb ik veel
van jou geleerd over de inhoud van de kinderfysiotherapie. NDT, Vojta, en als klap op de vuurpijl
COPCA. Uren heb je met het popje voor me gezeten om me alle handelingen die een kinderfysiothe-
rapeut met een baby kan uitvoeren, uit te leggen. En dat zijn er nogal wat! Onze oneindige discus-
sies over de inhoud van het observatieprotocol hebben toch al mooi tot drie artikelen geleid.
Prof. Dr. J.G. Becher, Prof. Dr. O.F. Brouwer en Prof. Dr. P.J.M. Helders wil ik bedanken voor het
beoordelen van mijn proefschrift.
Prof.Dr. A.F. Bos en drs. L. van Doormaal wil ik hartelijk bedanken voor hun bijdrage aan het VIP
project. Arie, daarnaast wil ik je bedanken voor je hulp bij het samenstellen van de onderzoeksgroep,
onze gezamenlijke artikelen en het interpreteren van de schedelecho’s.
Kune Blaauw-Schierbeek, Ellen Janssen, Peter Logtenberg en drs. Wilma Renkema, COPCA coaches
van het eerste uur. Jullie hebben een zeer belangrijke rol in het onderzoek gespeeld en geweldig
werk geleverd. Het volledig ombouwen van je dagelijkse routine tot het compleet beheersen van een
nieuwe methode hebben jullie goed onder de knie gekregen. Mijn complimenten!
Beste collega’s van de ontwikkelingsneurologie: Lieke van Baalen, Hylco Bouwstra, Leo van Eykern,
Saskia van Goor, Jolanda van der Heide, Kirsten Heineman, Corina de Jong, Marjolein Jongbloed-
Pereboom, Karin Middelburg, Lieke Peters, Michiel Schrier en Loes de Weerd. Jullie wil ik bedanken
voor al jullie steun, collegialiteit, hulp bij het onderzoek, het filmen, de EMG-metingen en jullie be-
reidheid een luisterend oor te bieden als het weer eens niet liep met het onderzoek of het schrijven.
De studenten die ik mocht begeleiden bij hun doctoraalscriptie of wetenschappelijke stage hebben
mij erg geholpen met het verzamelen en verwerken van de resultaten. Renske van Abbema, Eveline
Nieuwenhuis en Lily Hulshof, jullie hebben een grote bres geslagen in de enorme hoop onderzoeks-
gegevens en van jullie frisse blik op het onderzoek heb ik veel geleerd.
Victorine de Graaf-Peters, mijn raamloze kamergenoot en nu nog steeds vriendin. Je bent met ruime af-
stand de meest praatgrage collega, maar het was altijd weer gezellig om even het weekend of resultaten
door te nemen. Toen je weg was, vond ik het opeens maar stil. Zelfs de sneeuw heb ik gemist. Gelukkig
kun je nu af en toe wat sneeuw vanuit Amersfoort sturen! Geweldig dat je mijn paranimf wilt zijn.
Joke de Boer, wat begon als bovenbuurvrouw en volleybalmaatje is inmiddels uitgegroeid tot veel ge-
zellige muziek-, eet-, en filmavondjes met zijn vieren. Misschien moeten we de frequentie maar weer
eens verhogen… Ik ben enorm blij dat je mijn paranimf wilt zijn. Mark, jou wil ik bedanken voor al je
hulp bij het vormgeven, lay-outen en alle drukadviezen. Ik ben enorm trots op het resultaat en zal je
bij iedereen die een grafisch ontwerper nodig heeft van harte aanbevelen.
Met mijn verhuizing naar het KNGF kreeg ik er een aantal andere geïnteresseerde collega’s voor terug.
Katja Aberson, Marion Bosga, Jeroen Broekhoff, Karin Heyl, en Charlotte Hilbers, het Heerenveen dream-
team! Nou dames en heer, het zit er eindelijk op. Bedankt voor al jullie interesse en veel plezier met lezen…
Lieve pap en mam, altijd staan jullie voor mij klaar. Ik wil jullie dan ook bijzonder graag bedanken
voor de enorme steun en het onvoorwaardelijke vertrouwen dat jullie mij altijd gegeven hebben.
Dan nu speciaal iets voor mijn grote knul Yonah. Lieve, lieve eigenwijze kerel. Je begreep nog niet
altijd goed waar mamma nou al die tijd druk mee was. “Mamma, gaat jij nu weer werken op de kap-
joeter…?’. Maar Yonah, nu is het af en kan ik ook mee fietsen en koeien zoeken in het park op zon-
dagmiddag. En over een paar maanden gaan we met z’n vieren en ben jij de grote broer!
Lieve Levy, als ik moet opsommen waarvoor ik jou wil bedanken, ben ik wel even bezig. Wat een
luxe om jou als partner te hebben. Je hebt me enorm geholpen om structuur te krijgen in de enorme
data-berg. Van jouw fantastische Excel-formules heb ik zeven jaar plezier gehad! Gelukkig kan ik van
jou nog veel langer genieten. Laten we er iets moois van maken, niet alleen met z’n viertjes, maar
ook met elkaar.
186 187
a B O U t t H E aU t H O r
Cornill Blauw-Hospers werd geboren op 8 januari 1978 te Groningen. Na het behalen van haar
VWO diploma aan het Ubbo Emmius Lyceum te Stadskanaal in 1996 startte zij met de opleiding
Bewegingswetenschappen aan de Rijksuniversiteit Groningen. In 2000 studeerde zij af met als
specialisatie Sport en Lichamelijke opvoeding. Haar afstudeerproject betrof de evaluatie van het
effect van fysiotherapie voor kinderen met motorische problemen. Na haar afstuderen werkte
zij enige tijd als onderzoeker bij het Centrum voor Revalidatie Beatrixoord van het Universitair
Medisch Centrum Groningen. Na een verhuizing naar Sneek zette zij haar onderzoeksloopbaan
voort in Groningen waar zij op 1 maart 2003 werd aangesteld als AIO bij het Instituut voor Ontwik-
kelingsneurologie van het UMCG. Zij deed daar onderzoek naar de effecten van vroegtijdige fysio-
therapeutische interventie voor jonge kinderen met een hoog risico op een motorische ontwik-
kelingsstoornis. De resultaten van haar studie staan beschreven in deze dissertatie. Vanaf september
2008 is zij werkzaam bij het Koninklijk Nederlands Genootschap Fysiotherapie te Heerenveen.
Hospers CH, De Graaf-Peters VB, Hadders-Algra M. Het vroegtijdige interventie project in Groningen. Ned Tijdschr Kinderfysiother 2004; 16, nr 40:14-16.
Hadders-Algra M, Dirks T, Blauw-Hospers C, de Graaf-Peters V. The Kozijavkin method: giving parents false hope? Lancet 2005;365:842. Blauw-Hospers CH, Hadders-Algra M. Fact or fiction: a systematic review on the effects of early intervention on motor development. Dev Med Child Neurol 2005;47:421-432.
De Graaf-Peters VB, Blauw-Hospers CH, Dirks T, Bakker J, Bos AF, Hadders-Algra M. Development of postural control in typically developing children and children with cerebral palsy: possibilities for intervention? Neurosci Biobehav Rev 2007;31:1191-1200.
Blauw-Hospers CH, de Graaf-Peters VB, Dirks T, Bos AF, Hadders-Algra M. Does early intervention in infants at high risk for a developmental motor disorder improve motor and cognitive development? Neurosci Biobehav Rev 2007;31:1201-1212.
Blauw-Hospers CH, Dirks JF, Hulshof LJ, Hadders-Algra M. Opening the Black-Box: development of a quantitative tool to assess physical therapy contents in infancy. Pediatr Phys Ther 2010;22:189-198.
Blauw-Hospers CH, Dirks T, Hulshof LJ, Bos AF, Hadders-Algra M. A Randomized Controlled Trial on pediatric physical therapy in infancy: from nightmare to dream. Submitted for publication.
Dirks T, Blauw-Hospers CH, Hulshof LJ, Hadders-Algra M. Differences between a Family Centered Program “Coping and Caring for Infants with Special Needs” and Infant Treatment based on Principles of NeuroDevelopmental Treatment. Submitted for publication.
Hielkema T, Blauw-Hospers CH, Dirks T, Drijver-Messelink M, Bos AF, Hadders-Algra M. Does physiotherapeutical intervention affect motor outcome in high risk infants? A combined approach of RCT and process evaluation. Submitted for publication.
L I S t O F P U B L I C at I ON S
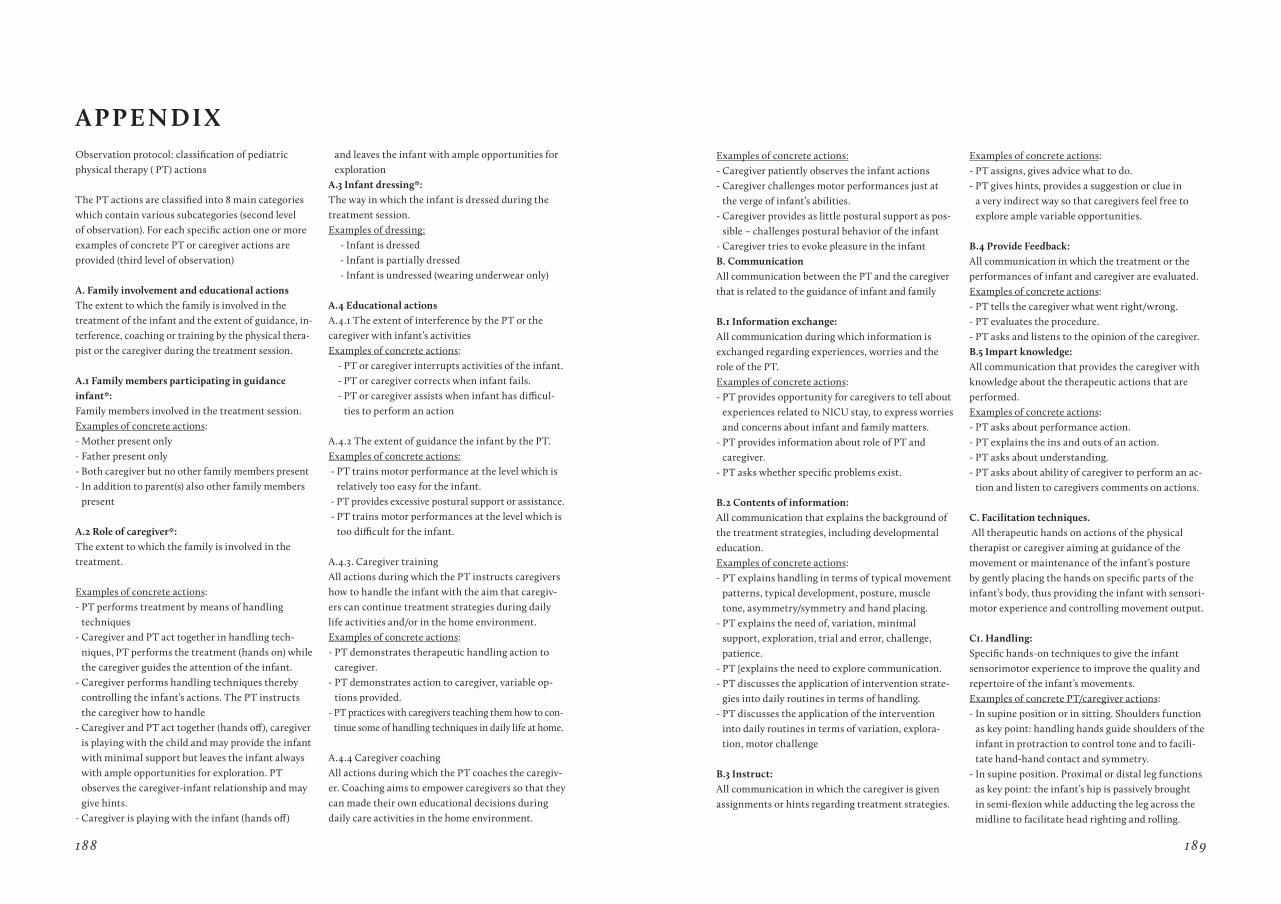
188 189
Observation protocol: classification of pediatric physical therapy ( PT) actions
The PT actions are classified into 8 main categories which contain various subcategories (second level of observation). For each specific action one or more examples of concrete PT or caregiver actions are provided (third level of observation)
a. Family involvement and educational actionsThe extent to which the family is involved in the treatment of the infant and the extent of guidance, in-terference, coaching or training by the physical thera-pist or the caregiver during the treatment session.
a.1 Family members participating in guidance infant*: Family members involved in the treatment session.Examples of concrete actions:- Mother present only - Father present only - Both caregiver but no other family members present - In addition to parent(s) also other family members
present
a.2 role of caregiver*: The extent to which the family is involved in the treatment.
Examples of concrete actions:- PT performs treatment by means of handling
techniques- Caregiver and PT act together in handling tech-
niques, PT performs the treatment (hands on) while the caregiver guides the attention of the infant.
- Caregiver performs handling techniques thereby controlling the infant’s actions. The PT instructs the caregiver how to handle
- Caregiver and PT act together (hands off), caregiver is playing with the child and may provide the infant with minimal support but leaves the infant always with ample opportunities for exploration. PT observes the caregiver-infant relationship and may give hints.
- Caregiver is playing with the infant (hands off)
and leaves the infant with ample opportunities for exploration
a.3 Infant dressing*: The way in which the infant is dressed during the treatment session.Examples of dressing: - Infant is dressed - Infant is partially dressed - Infant is undressed (wearing underwear only)
a.4 Educational actions A.4.1 The extent of interference by the PT or the caregiver with infant’s activities Examples of concrete actions: - PT or caregiver interrupts activities of the infant. - PT or caregiver corrects when infant fails. - PT or caregiver assists when infant has difficul-
ties to perform an action A.4.2 The extent of guidance the infant by the PT.Examples of concrete actions: - PT trains motor performance at the level which is
relatively too easy for the infant. - PT provides excessive postural support or assistance. - PT trains motor performances at the level which is
too difficult for the infant.
A.4.3. Caregiver training All actions during which the PT instructs caregivers how to handle the infant with the aim that caregiv-ers can continue treatment strategies during daily life activities and/or in the home environment.Examples of concrete actions: - PT demonstrates therapeutic handling action to
caregiver. - PT demonstrates action to caregiver, variable op-
tions provided.- PT practices with caregivers teaching them how to con-
tinue some of handling techniques in daily life at home.
A.4.4 Caregiver coachingAll actions during which the PT coaches the caregiv-er. Coaching aims to empower caregivers so that they can made their own educational decisions during daily care activities in the home environment.
a P P E N DI x Examples of concrete actions:- Caregiver patiently observes the infant actions- Caregiver challenges motor performances just at
the verge of infant’s abilities.- Caregiver provides as little postural support as pos-
sible – challenges postural behavior of the infant- Caregiver tries to evoke pleasure in the infantB. Communication All communication between the PT and the caregiver that is related to the guidance of infant and family
B.1 Information exchange: All communication during which information is exchanged regarding experiences, worries and the role of the PT.Examples of concrete actions:- PT provides opportunity for caregivers to tell about
experiences related to NICU stay, to express worries and concerns about infant and family matters.
- PT provides information about role of PT and caregiver.
- PT asks whether specific problems exist.
B.2 Contents of information: All communication that explains the background of the treatment strategies, including developmental education.Examples of concrete actions: - PT explains handling in terms of typical movement
patterns, typical development, posture, muscle tone, asymmetry/symmetry and hand placing.
- PT explains the need of, variation, minimal support, exploration, trial and error, challenge, patience.
- PT [explains the need to explore communication.- PT discusses the application of intervention strate-
gies into daily routines in terms of handling.- PT discusses the application of the intervention
into daily routines in terms of variation, explora-tion, motor challenge
B.3 Instruct: All communication in which the caregiver is given assignments or hints regarding treatment strategies.
Examples of concrete actions:- PT assigns, gives advice what to do. - PT gives hints, provides a suggestion or clue in
a very indirect way so that caregivers feel free to explore ample variable opportunities.
B.4 Provide Feedback: All communication in which the treatment or the performances of infant and caregiver are evaluated.Examples of concrete actions:- PT tells the caregiver what went right/wrong. - PT evaluates the procedure. - PT asks and listens to the opinion of the caregiver.B.5 Impart knowledge: All communication that provides the caregiver with knowledge about the therapeutic actions that are performed.Examples of concrete actions:- PT asks about performance action. - PT explains the ins and outs of an action. - PT asks about understanding. - PT asks about ability of caregiver to perform an ac-
tion and listen to caregivers comments on actions.
C. Facilitation techniques. All therapeutic hands on actions of the physical therapist or caregiver aiming at guidance of the movement or maintenance of the infant’s posture by gently placing the hands on specific parts of the infant’s body, thus providing the infant with sensori-motor experience and controlling movement output.
C1. Handling:Specific hands-on techniques to give the infant sensorimotor experience to improve the quality and repertoire of the infant’s movements.Examples of concrete PT/caregiver actions:- In supine position or in sitting. Shoulders function
as key point: handling hands guide shoulders of the infant in protraction to control tone and to facili-tate hand-hand contact and symmetry.
- In supine position. Proximal or distal leg functions as key point: the infant’s hip is passively brought in semi-flexion while adducting the leg across the midline to facilitate head righting and rolling.

190 191
- In supine position. Pelvis functions as key point: the infant’s pelvis is slightly lifted to elongate the extensor muscles of the trunk and to control tone; in this way hand-foot contact and symmetry are facilitated
- In prone position. Shoulder functions as key point, the arms are placed in puppy position to facilitate head righting, midline orientation and body-alignment.
- In sitting. Shoulder functions as key point: the shoulders are moved alternately forwards and backwards to dissociate and facilitate independent arm movements.
C.2 Pressure techniques: All handling techniques that produce intermittent pressure to stimulate and gain control over muscle tone, posture and movement. Examples of concrete PT /caregiver actions: - In sitting: intermittent downward pressure on
shoulders in the direction of the pelvis to facilitate extension of the trunk
- In sitting: slight intermittent pressure movements on abdominal region in direction of the sacrum to facilitate contraction of the ventral muscles.
C.3 transition: All handling techniques that result in the change of position of the infant.Examples of concrete PT /caregiver actions: - From supine to side, from supine to prone, from
supine to sit, from side to sit, from prone to supine, from sit to supine, etc.
C.4 Support devices: All handling techniques which use additional devices to support the infant.Examples of concrete / additional devices: - Bolster or ball- Supporting sling.
D. Sensory experience All tactile and vestibular stimulation given to the infant during treatment - without the aim of facilita-tion, tapping or passive motor experience - offered to
the infant to provide him/her with the perception of body awareness.Examples of concrete PT /caregiver actions: - Touching skin with toy.- Tickling. - Tapping on muscles
E. Passive motor experienceAll handling techniques induced by the PT or the caregiver in which no activity of the infant is re-quired in the performance of the actions.Examples of concrete PT /caregiver actions:- Passive movements of arms. - Repetitive movements of the upper arm towards
(frontal) support surface.- Passive rocking, small sideways movements.
F. Self-produced motor behavior, no interference with Pt /caregiver All actions during which the infant is given ample opportunities to explore toys or other aspects of the environment or his body without interference of PT or caregiver.Examples of concrete PT /caregiver actions:- Placing an infant activity play center over the infant
and let the infant explore the effect of movements or arms, hands, legs and feet.
- Infant is given opportunity for spontaneous explo-ration with or without toy.
- Postural challenges, infant spontaneously explores postural capacities.
G. Infant is challenged to produce motor behavior by him/herself; infant is allowed to continue activ-ity by her/himselfAll actions in which the infant is challenged by toys or face of PT or caregiver to experience a variety of motor activity, that is continued by the infant her/himself.
G.1 Little variation: All actions in which the infant is challenged by toys or face of PT or caregiver to explore one strategy to reach and grasp, to control posture, to roll, etc.
G.2 Large variation: All actions in which the infant is challenged by toys or face of PT or caregiver the infant is challenged to explore multiple strategies to reach and grasp, to control posture, to roll, etc.
H. Infant is challenged to produce motor behavior by him/herself; activity flows over into therapeutic handling All actions in which the infant is challenged by toys or face of PT or caregiver to experience a variety of motor activity, that is followed by a handling technique.
H.1 Little variation: All actions in which the infant is challenged by toys or face of physical therapist or caregiver to explore one strategy to reach and grasp, to control posture, to roll, etc.
H.2 Large variation: All actions in which the infant is challenged by toys or face of physical therapist or caregiver the infant is challenged to explore multiple strategies to reach and grasp, to control posture, to roll, etc.
I. Not specified All time during the treatment session that can not be classified into the eight defined categories.Examples: - Comforting the infant. - Change the treatment situation.
Postural support in prone, side and sitting position: No postural support: PT or caregiver leaves it to the infant to adjust pos-ture independently. “Hands off” Minimal postural support: PT or caregiver provides as little support as possible in order to challenge postural behavior of the infantExample of concrete action:PT or caregiver challenges motor performance just at the verge of the infant’s abilities, i.e. the infant has to ‘work’ to maintain balance
Clear postural support: PT or caregiver provides support on multiple parts of body or the trunk. Minimal active involvement of the infant to adjust posture is required.Example of concrete action:- PT or caregiver provides support at the neck/shoul-
der girdle and/or upper part of the trunk Full postural support: PT or caregiver supports all parts of the body of the infant that play a role in postural adjustments. No active involvement of the infant is required.
* Independent variable: the value of this variable is supposed not to change during the course of an observation. It gives the observer the opportunity to summarize briefly important characteristics of the observation
