university of groningen computer assisted surgery in orthopaedic ... · · 2016-03-09computer...
TRANSCRIPT

University of Groningen
Computer assisted surgery in orthopaedic oncologyGerbers, Jasper Gerhard
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2015
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Gerbers, J. G. (2015). Computer assisted surgery in orthopaedic oncology: Indications, applications andsurgical workflow [Groningen]: University of Groningen
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 31-05-2018

Computer Assisted Surgery in Orthopaedic OncologyIndications, applications and surgical workflow
Jasper Gerbers2015

Sponsors
Implantcast Benelux BVJ.W. Hanssen-F.C. van der Linden BV
Colophon
The studies in this thesis were conducted within the Research Institute SHARE of the Graduate School of Medical Sciences, University Medical Center Groningen, University of Groningen and under the auspices of the research program Public Health Research.
© Jasper Gerbers, 2015
All rights reserved. No part of this thesis may be reproduced or transmitted, in any form or by any means, without the written permission of author.
ISBN: 978-90-367-8083-4ISBN: 978-90-367-8082-7 (pdf)
Cover design: Wiebren de JongLay-out: Jasper GerbersPrint: Ipskamp Drukkers
Chapter image: Theatrum Orbis Terrarum - Abraham Ortelius (1570)

Computer Assisted Surgery in Orthopaedic Oncology
Indications, applications and surgical workflow
PhD thesis
to obtain the degree of PhD at the University of Groningen on the authority of the
Rector Magnificus Prof. E. Sterken and in accordance with
the decision by the College of Deans.
This thesis will be defended in public on
Wednesday 23 September 2015 at 16.15 hours
by
Jasper Gerhard Gerbers
born on 31 October 1988 in Groningen

Supervisor Prof. S.K. Bulstra
Co-supervisors Dr. P.C. Jutte Dr. M. Stevens
Assessment Committee Prof. R.G.H.H. Nelissen Prof. H.J. Hoekstra Prof. R.P.H. Veth

“I do not fear computers. I fear the lack of them”.- Isaac Asimov

Paranimfen Tim Blikman Wietske Rienstra
Contents
1. General introduction 9
2. Computer-assisted surgery in orthopedic oncology:Technique, indications, and a descriptive study of 130 cases 21
3. Hip sparing approach using computer navigation in peri- acetabular chondrosarcoma: Added safety in difficult resections 37
4. Computer-assisted surgery for curettage of atypical cartilaginoustumors / chondrosarcoma grade 1 in the long bones comparedto fluoroscopic guidance 47
5. Computer-assisted surgery for allograft shaping in hemicorticalresection: A technical note involving 4 cases 63
6. Enhancing precision and accuracy in bone tumour treatment.An experimental comparison of freehand, computer assistance(CAS) and a novel universal CAS saw guide 71
7. General discussion and future perspectives 89
8. Summery / Samenvatting 113
9. Dankwoord 119
Curiculum Vitae 123
Previous SHARE Disserations 127

General introduction

General introduction
11
General introduction
10
Accuracy:The closeness of agreement between a test result and the accepted reference value.
Precision: The closeness of agreement between independent test results obtained under stipulated conditions.BS ISO 5725-1: “Accuracy (trueness and precision) of measurement methods and results - Part 1: Generalprinciplesanddefinitions.”,pp.1(1994)
Figure1:(firstimage,lefttoright)highaccuracy,highprecision,(secondimage)lowaccuracy,highprecision, (third image) high accuracy, low precision, (fourth image) low accuracy, low precision

1
General introduction
11
General introduction
10
Introduction
Orthopaediconcologyisthemedicalfieldthatspecialisesinthesurgicaltreatmentof bone tumours: primary bone sarcoma, intermediate and benign bone tumours, and metastases. Sarcomas are malignant tumours deriving from cells of non-hematopoietic mesenchymal origin (e.g. cartilage, muscle, bone, vessels). While bone makes up around 13-15% of the human adult body weight, cancers of the bone are relatively rare (1). The registry of the IKNL (Netherlands Integral Cancer Centre) shows an incidence rate of 0.97/100,000 (world standardised rate) for primary bone tumours in the Netherlands in 2013, or less than 0.2% of all neoplasms (2). This includes not only sarcomas but also intermediate-grade and benign lesions. The Dutch incidence is comparable to reported rates from other Western countries like the UK and United States (3, 4). Incidence of malignant tumours has two peaks. The firstisinchildrenandadolescents,primarilyosteosarcomaandEwingsarcoma,andthe second around 40-60 years of age, primarily chondrosarcoma. Treatment of these tumours often involves major and challenging procedures.
Thanks to advances in surgical techniques, adjuvant/neoadjuvant chemotherapy and knowledge of tumour biology, there has been a trend in orthopaedic oncology not only towards better survival rates but also towards more minimal and less invalidating procedures. Examples are the increase in limb salvage surgery for osteosarcoma using tumour prostheses, joint salvaging procedures using allografts, and the development of periacetabular resections (5-7). At the heart of this transformationliesadifficultbalance,aseachprocedurerequiresacarefulweighingof two competing interests: margin and function. Adequate margins are required to lower the chances of recurrence or, in case of malignant tumours, improve survival rates. As the margin is presumably healthy tissue, resection impacts function in terms of decreasing mobility or increasing the chances of complications. This is thefinelinethatanorthopaediconcologysurgeonisexpectedtojuggleduringaprocedure – enough margin to prevent recurrence, but not too much so function can be protected. And when the margin of error is small, accuracy is vital.
Surgical orientation systems
Multiple tools are used in the operating theatre to assist the surgeon in surgical orientation,whichistheprocessoffindingthepointsofinterest,resectionplanes,screw entry points, etc. during the procedure. Imaging data is displayed on large screens on the wall. Preoperative plans are drawn, often referencing anatomical landmarks. This is frequently measured using rulers. Currently there are two options for intraoperative orientation support, one widely applied and one new.
General introduction
13
General introduction
12
Fluoroscopy
Fluoroscopy machines are intraoperative X-ray devices that are widely used in orthopaedicandtraumasurgery.JustlikeastandardX-raymachine,afluoroscopicimaging modality works by displaying variances of absorption of X-ray photons, also known as Röntgen radiation, by different human tissues. The name is derived from a formofluminescencecalledfluorescence.Lightorotherelectromagneticradiation,in this case X-ray radiation, strikes a substance that absorbs and then re-emits the energy when electrons fall back to their ground state. Due to energy losses in this process, the electromagnetic radiation produced is of a lower wavelength. When the right material is chosen, it becomes visible light.
The effect was discovered in 1895 by Wilhelm Röntgen, who noticed that a barium platinocyanide screen glowed when exposed to X-radiation (8). Early medical use required darkened rooms, red darkness adaptation goggles and head-mounted screens with funnels due to low image brightness. With the development of image intensifiersinthe1950’s,fluoroscopycouldbeusedinilluminatedrooms.Recordingof fluoro-cine or fluoro-movies (with the accompanyingdecreased image framerate, thus decreased exposure) and image storage became possible with camera integration.Currentfluoroscopymachinesuseadigitalflatpaneldetector,furtherdecreasing the required radiation dose while producing a similar or better image. Even so, intraoperative radiation is not harmless (the linear no-threshold model holds that every exposure has a risk) and thus requires strict protocols (9, 10). Inherent to the technique is that single imaging only provides two-dimensional (2D) images. There is also a need to balance patient dose and image quality. Using an isocentricarmandreconstructionsoftwareafluoroscopecanbeusedtoproduceintraoperative, CT-like, three-dimensional (3D) datasets. This technique is called 3D fluoroscopyorisocentric(iso-c)3Dscanning.
Computer-Assisted Surgery
Computer-Assisted Surgery (CAS) is the term used to describe a relatively new concept of applying computers to enable preoperative planning and provide intraoperative orientation, instrument feedback and/or guidance. This concept enables surgeons to objectify the spatial position of anatomical locations, instruments or implants. This is done by using imaging datasets or computational models. The first rudimental CAS systemswere developed in the early 1970s, only about 40years after the theoretical description of a modern computer by Alan Turing (11). These systems did computations for and gave feedback on instrument positioning in stereotactical neurosurgery (12). The development of computer tomography (CT) provided detailed three-dimensional datasets; this was quickly applied in the firststereo-opticalCASsystems(13). ThefirstapplicationofCASinorthopaedicsurgerywasatotalkneearthroplastyin1997(14).Thefirstorthopaediconcology

1
General introduction
13
General introduction
12
procedures reported were three high-grade pelvic sarcoma resections in 2004 (15).
Most orthopaedic CAS systems are based around a stereoscopic optical device. There are two digital cameras, on a mount, that register and follow instrument and patient trackers. These trackers can be active, emitting infrared light, or passive,reflectinginfraredlightfromlightsourcesinthecameramount.Usingthedifference between the two cameras, timing data between pulses, distance between the reflectors/light-emittingdiodes (LEDs)andorientationof the reflectors/LEDs,the computer can calculate the position of the tracker relative to the camera. This measurement data can then be used for intraoperative measurements, imageless navigation or – with matching of spatial and virtual coordinates in CT and/or MRI datasets – image-based navigation. There are CAS systems that use electromagnetic radiation for instrument localisation. This technique has the advantage that it does not require a direct line of sight between the cameras and the trackers; the signal is vulnerable to interference though.
Software and offered functionalities differ between manufacturers, but the two basic modi operandi are comparable for all systems. There is an imageless mode, based on computational kinematic and/or statistical models, that is used in prosthetic placement. Image-based mode uses three-dimensional imaging datasets. This requires matching of the imaging dataset and the real-world coordinates. Usually this is done by landmark (point-to-point) and surface matching (bone surface detection),butcanalsobeperformedusing imageacquisition (fluoro-matching)or positional referencing (tracking of the intraoperative CT using an isocentric fluoroscope).
Application of orientation systems
Without the use of a CAS system, surgical orientation is mostly subjective. The
Figure 2: Surgical planning relies heavily on an accurate frame of reference. The left image shows a planning in an AP view with the tumour 5 cm above the joint line. The right image shows a lateral view. An interpretation (incorrect, but logical) of the joint line would probably result in an intralesional resection.
3 cm 3 cm
5 cm5 cm

General introduction
15
General introduction
14
localisation of the tumour and resection planes depends on knowledge of anatomy andtheskilltotranslatetwo-dimensionalimaging(radiographs,fluoroscopyor2dviews of 3d datasets) into three-dimensional actions. Both skills depend heavily on an accurate frame of reference [Fig. 2]. The occurrence of inadequate surgical margins is highest in the bones with the most complex three-dimensional anatomy. Recent large studies report the occurrence of intralesional pelvic tumour resection in at least one of the margins of 26 and 30% (16, 17). Experimental studies have demonstrated that this is due not only to the localisation within a complex anatomical region or to the characteristics of pelvic tumours. Simulation of pelvic resections by Cartiaux et al. has shown that even experienced surgeons struggle with this. Four surgeons could achieve a good 10-mm resection margin, with 5-mm tolerance, on sawbones (without soft tissue) in only half of resections (18). The authors called for larger margins to compensate for the inaccuracy. A subsequent follow-up study to check these surprising results, using 10 senior and 13 junior surgeons, found 5 out of 23 intralesional resections in the freehand group (19). Studies like these can explain the high number of intralesional resections and (partially) local recurrences in the surgical treatment of pelvic sarcoma (20-22). Our frame of reference and thus our accuracy may not be as good as we think it is.
While complicated pelvic resections that rely heavily on accurate resection plane placement are currently the most common application of CAS in orthopaedic oncology, other orthopaedic oncology procedures depend on high accuracy too. An example is the creation and reconstruction of intercalary or hemicortical bone defects ormulti-planarresections.Thesetypesofprocedures,whileofferinglargebenefitsto patients over tumour prostheses, require two separate surgical plans and highly accurate resections to get a safe oncological result and functional reconstruction (23, 24). As CAS can be used as a three-dimensional spatial measurement system, its use can hypothetically improve resection and reconstruction accuracy.
As a modality that offers three-dimensional imaging, CAS can also be used as a replacement of fluoroscopy for the curettage of bone tumours. Hypotheticallyimproved, real-time orientation in 3D can reduce the observed occurrence rate of post-procedure (potential) residue (13%) or recurrence (3.5% and 13.3%) (25-27), while reducing ionising radiation exposure to the team and the patient.
Imageless CAS is a technique that has been applied mainly to total knee (TKA) and hip (THA) arthroplasty. While the discussion on its use and usefulness, primarily in terms of actual clinical results, still rages, meta-analyses show that CAS leads to a decrease in outliers in cup placement and knee joint line reconstruction (28-30). This observation shows that objective navigation can still show improvements on an already highly evolved surgical procedure and instruments. As reconstruction length of tumour prostheses is far larger, small errors in deviation angle have a larger overall effect. Hence correct positioning will rely even more on accurate
1
General introduction
15
General introduction
14
placement. This is something that imageless CAS can potentially improve, if it can reliably be applied to tumour prosthesis placement.
Overall, CAS use can potentially decrease the impact of a diagnosis of bone cancer on the lives of patients, in terms of effect on clinical outcome and functioning after the procedure.
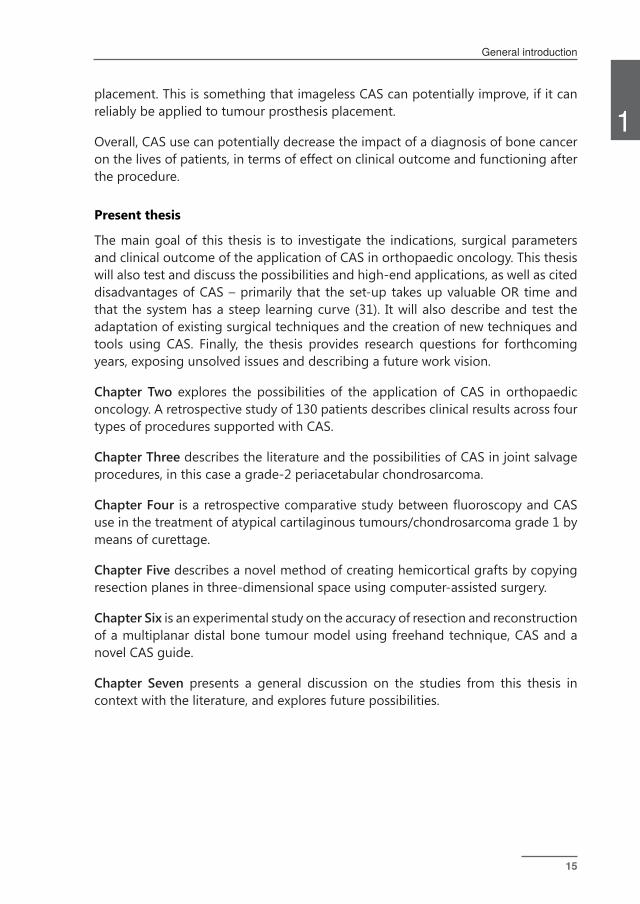
Present thesis
The main goal of this thesis is to investigate the indications, surgical parameters and clinical outcome of the application of CAS in orthopaedic oncology. This thesis will also test and discuss the possibilities and high-end applications, as well as cited disadvantages of CAS – primarily that the set-up takes up valuable OR time and that the system has a steep learning curve (31). It will also describe and test the adaptation of existing surgical techniques and the creation of new techniques and tools using CAS. Finally, the thesis provides research questions for forthcoming years, exposing unsolved issues and describing a future work vision.
Chapter Two explores the possibilities of the application of CAS in orthopaedic oncology. A retrospective study of 130 patients describes clinical results across four types of procedures supported with CAS.
Chapter Three describes the literature and the possibilities of CAS in joint salvage procedures, in this case a grade-2 periacetabular chondrosarcoma.
Chapter Four isaretrospectivecomparativestudybetweenfluoroscopyandCASuse in the treatment of atypical cartilaginous tumours/chondrosarcoma grade 1 by means of curettage.
Chapter Five describes a novel method of creating hemicortical grafts by copying resection planes in three-dimensional space using computer-assisted surgery.
Chapter Six is an experimental study on the accuracy of resection and reconstruction of a multiplanar distal bone tumour model using freehand technique, CAS and a novel CAS guide.
Chapter Seven presents a general discussion on the studies from this thesis in context with the literature, and explores future possibilities.
General introduction
17
General introduction
16
References
(1) Valentin J. Basic anatomical and physiological data for use in radiological protection: reference values: ICRP Publication 89. Ann ICRP 2002;32(3):1-277.
(2) IKNL. Cijfers over kanker. 2013. http://cijfersoverkanker.nl/selecties/dataset_1/img54ff61be61805 (accessed 5-3-2015).
(3) Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013;63(1):11-30.
(4) Whelan J, McTiernan A, Cooper N, Wong YK, Francis M, Vernon S, et al. Incidence and survival of malignant bone sarcomas in England 1979–2007. Int J Cancer 2012;131(4):E508-E517.
(5) Ayerza MA, Farfalli GL, Aponte-Tinao L, Muscolo DL. Does increased rate of limb-sparing surgery affect survival in osteosarcoma? Clin Orthop Relat Res 2010;468(11):2854-2859.
(6) Bird JE. Advances in the Surgical Management of Bone Tumors. Curr Oncol Rep 2014;16(7):1-6.
(7) Aponte-Tinao L, Ayerza MA, Muscolo DL, Farfalli GL. Survival, Recurrence, and Function After Epiphyseal Preservation and Allograft Reconstruction in Osteosarcoma of the Knee. Clin Orthop Relat Res 2014:1-8.
(8) Mould RF. The early history of x-ray diagnosis with emphasis on the contributions of physics 1895-1915. Phys Med Biol 1995;40(11):1741.
(9) Mastrangelo G, Fedeli U, Fadda E, Giovanazzi A, Scoizzato L, Saia B. Increased cancer risk among surgeons in an orthopaedic hospital. Occ Med 2005;55(6):498-500.
(10) Mehlman CT, DiPasquale TG. Radiation exposure to the orthopaedic surgical teamduringfluoroscopy:“howfarawayisfarenough?”.JOrthopTrauma1997;11(6):392-398.
(11) Turing AM. On computable numbers, with an application to the Entscheidungsproblem. J.of Math 1936;58:345-363.
(12) Thompson CJ, Bertrand G. A computer program to aid the neurosurgeon to locate probes used during stereotaxic surgery on deep cerebral structures. Comput Programs Biomed 1972;2(4):265-276.
(13) Adams L, Krybus W, Meyer-Ebrecht D, Rueger R, Gilsbach JM, Moesges R, et al. Computer-assisted surgery. Computer Graphics and Applications, IEEE 1990;10(3):43-51.
(14) Delp SL, Stulberg DS, Davies B, Picard F, Leitner F. Computer assisted knee replacement. Clin Orthop 1998;354:49-56.
(15) Hüfner T, Kfuri Jr M, Galanski M, Bastian L, Loss M, Pohlemann T, et al. New
1
General introduction
17
General introduction
16
indications for computer-assisted surgery: tumor resection in the pelvis. Clin Orthop 2004;426:219-225.
(16) Ozaki T, Flege S, Kevric M, Lindner N, Maas R, Delling G, et al. Osteosarcoma of the pelvis: experience of the Cooperative Osteosarcoma Study Group. J Clin Oncol 2003 Jan 15;21(2):334-341.
(17) Fuchs B, Hoekzema N, Larson DR, Inwards CY, Sim FH. Osteosarcoma of the pelvis: outcome analysis of surgical treatment. Clin Orthop 2009;467(2):510-518.
(18) Cartiaux O, Docquier P, Paul L, Francq BG, Cornu OH, Delloye C, et al. Surgical inaccuracy of tumor resection and reconstruction within the pelvis: an experimental study. Acta orthopaedica 2008;79(5):695-702.
(19) Cartiaux O, Banse X, Paul L, Francq BG, Aubin C, Docquier P. Computer-assisted planning and navigation improves cutting accuracy during simulated bone tumor surgery of the pelvis. Computer Aided Surgery 2013;18(1-2):19-26.
(20) Fuchs B, Hoekzema N, Larson DR, Inwards CY, Sim FH. Osteosarcoma of the pelvis: outcome analysis of surgical treatment. Clin Orthop 2009;467(2):510-518.
(21) Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of local recurrence in patients with a tumour of the pelvis or sacrum? Bone Joint J 2013 Oct;95-B(10):1417-1424.
(22) Donati D, El Ghoneimy A, Bertoni F, Di Bella C, Mercuri M. Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005 Nov;87(11):1527-1530.
(23) Aponte-Tinao LA, Ritacco LE, Albergo JI, Ayerza MA, Muscolo DL, Farfalli GL. The principles and applications of fresh frozen Allografts to bone and joint reconstruction. Orthop Clin North Am 2014;45(2):257-269.
(24) Deijkers RL, Bloem RM, Hogendoorn PC, Verlaan JJ, Kroon HM, Taminiau AH. Hemicortical allograft reconstruction after resection of low-grade malignant bone tumours. J Bone Joint Surg Br 2002 Sep;84(7):1009-1014.
(25) Donati D, Colangeli S, Colangeli M, Claudia Di Bella M, Bertoni F. Surgical treatment of grade I central chondrosarcoma. Clinical Orthopaedics and Related Research® 2010;468(2):581-589.
(26) Campanacci DA, Scoccianti G, Franchi A, Roselli G, Beltrami G, Ippolito M, et al. Surgical treatment of central grade 1 chondrosarcoma of the appendicular skeleton. Journal of Orthopaedics and Traumatology 2013:1-7.
(27) Verdegaal SH, Brouwers HF, van Zwet EW, Hogendoorn PC, Taminiau AH. Low-

General introduction
19
General introduction
18
Grade Chondrosarcoma of Long Bones Treated with Intralesional Curettage Followed by Application of Phenol, Ethanol, and Bone-Grafting. The Journal of Bone & Joint Surgery 2012;94(13):1201-1207.
(28) Hetaimish BM, Khan MM, Simunovic N, Al-Harbi HH, Bhandari M, Zalzal PK. Meta-analysis of navigation vs conventional total knee arthroplasty. J Arthroplasty 2012.
(29) Brin YS, Nikolaou VS, Joseph L, Zukor DJ, Antoniou J. Imageless computer assisted versus conventional total knee replacement. A Bayesian meta-analysis of 23 comparative studies. Int Orthop 2011;35(3):331-339.
(30) Moskal JT, Capps SG. Acetabular component positioning in total hip arthroplasty: an evidence-based analysis. J Arthroplasty 2011;26(8):1432-1437.
(31) Saidi K. Potential use of computer navigation in the treatment of primary benign and malignant tumors in children. Current reviews in musculoskeletal medicine 2012:1-8.

General introduction
19
General introduction
18


Computer-assisted surgery in orthopedic oncology Technique, indications, and a descriptive study of 130 cases
JG Gerbers, M Stevens, JJW Ploegmakers, SK Bulstra, and PC Jutte
Published: Acta Orthopaedica 2014;85(6):663-9

Computer-assisted surgery in orthopedic oncology
23
Computer-assisted surgery in orthopedic oncology
22
AbstractBackground and purpose:
In orthopaedic oncology, computer-assisted surgery (CAS) can be considered an alternativetofluoroscopyanddirectmeasurementfororientation,planning,andmargincontrol.However,onlysmallcaseseriesreportingspecificapplicationshavebeen published. We therefore describe possible applications of CAS and report preliminary results in 130 procedures.
Patients and methods:
We conducted a retrospective cohort study of all oncological CAS procedures in a single institution from November 2006 to March 2013. Mean follow-up time was 32 months. We categorised and analysed 130 procedures for clinical parameters. The categories were image-based intralesional treatment, image-based resection, image-based resection and reconstruction, and imageless resection and reconstruction.
Results:
Application to intralesional treatment showed 1 inadequate curettage and 1 (other) recurrence in 63 cases. Image-based resections in 42 cases showed 40 R0 margins; 16 in 17 pelvic resections. Image-based reconstruction facilitated graft creation with a mean reconstruction accuracy of 0.9 mm in one case. Imageless CAS was helpful in resection planning and length- and joint line reconstruction for tumour prostheses.
Interpretation:
CAS is a promising new development. Preliminary results show a high number of R0 resections and low short-term recurrence rates for curettage.

2
Computer-assisted surgery in orthopedic oncology
23
Computer-assisted surgery in orthopedic oncology
22
Introduction
Oncological surgical treatment can be considered to be a trade-off between margins and function, with margins being the most important factor to consider. Accuracy isneededtoachieveanefficientbutoncologicallysaferesult.Toassistinthis,mostproceduresinbonetumoursurgeryrequireintraoperativeimagingwithfluoroscopyand/or measurements with rulers for anatomical orientation and margin control. The best examples of this are pelvic resections. Cartiaux et al. (2008) demonstrated that 4 experienced surgeons could achieve a 10-mm resection margin, with 5-mm tolerance, on pelvic sawbones in only half of the resections. The supportive imaging and measuring modalities have, however, remained more or less unchanged for manyyears.Ina2-dimensional(2D)workflowsuchasfluoroscopy,thereisstilltherequirement for an accurate frame of reference based on anatomical landmarks for adequate 3-dimensional (3D) margin control.
In recent years, the use of computer-assisted surgery (CAS) in orthopaedic surgery has become more common as an alternative for intraoperative imaging and measurements, providing the necessary precision in bone tumour surgery. The technique that is mostly used in orthopaedic oncology is image-based navigation. Thepatient’sownanatomy(MRIand/orCT) isenteredintothesystemandusedduring surgery. This provides real-time, continuous, 3D imaging feedback and may lead to more precise margin control, better tissue preservation, and new approaches to reconstruction while remaining oncologically safe. Several publications have supported CAS as being a safe navigation platform for planning and performing resections (1-3). A recent publication describes lessons in the technological approachandofferscommentsonCASworkflow(4).However,todatethelargestcase series have involved only 20 and 31 cases (5-6). The reported use has mostly been limited to complex tumour resections (e.g. pelvic), and due to the novelty of the technique, applications, approaches, and set-up times differ greatly (7). Here we describe possible applications of CAS in bone tumour surgery (also outside of complex resections), consider their usefulness, and report preliminary results from 130 CAS procedures performed at a single institution.
Patients and methodsWe conducted a retrospective cohort study at the University Medical Center Groningen (UMCG) between November 2006 and March 2013. We included all patients with a bone tumour for whom a CAS procedure was planned. The included group was split into a successful CAS procedure group and a CAS set-up failure group. Procedures were regarded as being successful when the CAS set-up was successfully completed and the system was used. If the set-up of the system failed or unsolvable inaccuracies were found during the set-up process, the procedure was
Computer-assisted surgery in orthopedic oncology
25
Computer-assisted surgery in orthopedic oncology
24
regarded as a CAS set-up failure and the surgery was performed by conventional means. The successful CAS procedures were analysed based on the following outcome parameters: recurrence/residue rate and margins achieved. CAS set-up failures were assessed for cause of failure. These failures were not included in the outcome analysis, as the procedures were performed using conventional methods and the purpose was to analyse the CAS application, not indications.
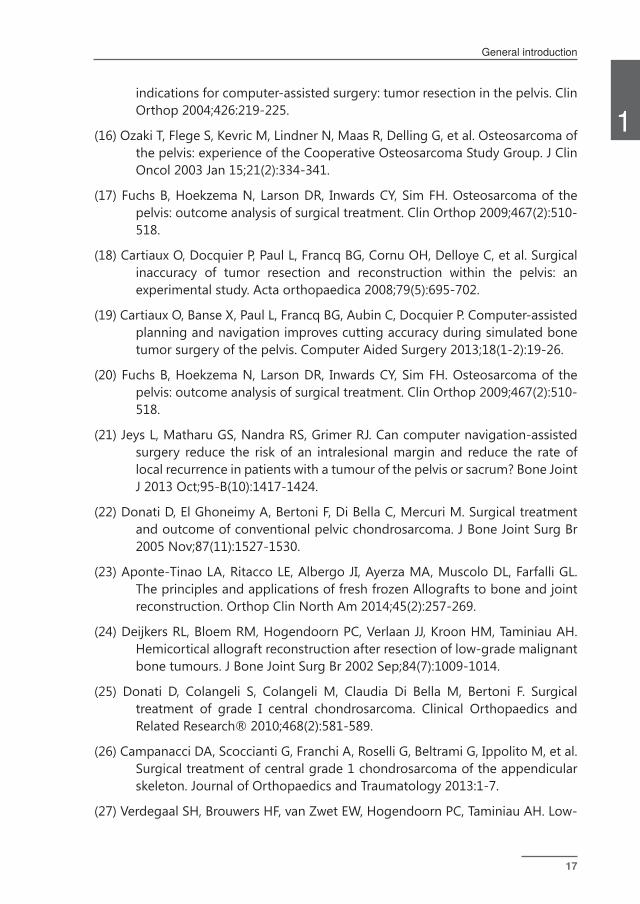
AllCASprocedureswerefirstclassifiedaccording to the techniqueused: image-based or imageless. The image-based group was then subdivided into “intra-lesional procedures” (curettages), “resection procedures”, and “resection with reconstruction procedures” (figure 1). The imageless group comprised tumourprosthesis placement around the knee.
Figure 1: Flow chart showing the decision-making process on CAS use, requirements per technique, and planned procedures per technique. From left to right: intralesional treatment with a navigated curette, image-based resection, image-based resection and reconstruction, and imageless resection and reconstruction.
Image-based workflow
The standardised preoperative workflow consisted of a CT-scan of the affectedbone, following a CAS protocol. Slice thickness was 1.0–1.5 mm for CT. If required, preoperative planning was performed to pre-plan resection planes and/or reconstruction options. This pre-planning was performed in advance on the planning laptop and often included CT/MRI fusion, tumour colouration, and resection planning.
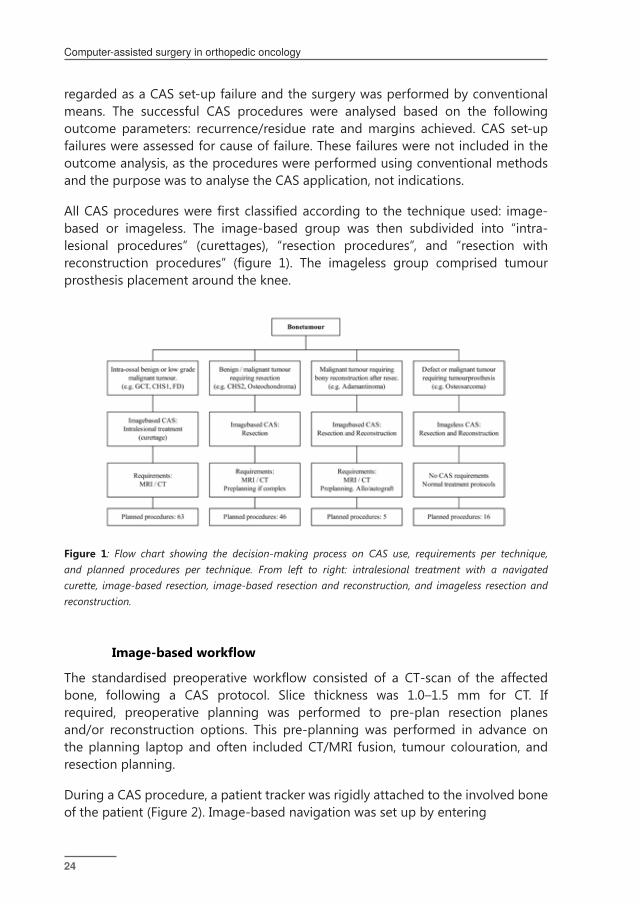
During a CAS procedure, a patient tracker was rigidly attached to the involved bone of the patient (Figure 2). Image-based navigation was set up by entering
2
Computer-assisted surgery in orthopedic oncology
25
Computer-assisted surgery in orthopedic oncology
24
Figure 2: A. Tracker rigidly attached to the tibia using percutaneous pins. Visible is the pointer tool being used for planning the distal resection plane around a Ewing sarcoma. The corresponding CAS view can be seen in the image. B. Surgical plan: a dome-shaped proximal resection very close to the tibial plateau, distal resection, and then reconstruction with a hybrid, allogenic and autogenic massive allograft.
referencepoints,firstinthenavigationsystemandthenonlandmarksonthebone.Theresultwasa fairly roughmatchingwithmoderateaccuracy.Thiswasrefinedusing surface matching, where data points were entered with the pointer tool directly on the navigated bone. The software matched this to the bone surface on the CT. Approximate accuracies under 1.5 mm were accepted and a landmark check was performed routinely. If the landmark check failed after multiple set-up attempts, the procedure was considered to be a CAS set-up failure, the navigation was discontinued, and the surgery was performed by conventional means. Set-up time and accuracy were measured using a digital registration system. Postoperative marginswereclassifiedbytheRclassification(8).Clinicalfollow-upwasroutinelyperformed with radiographs and MRI scans. We used the Stryker Navigation System II with OrthoMap 3D software (Stryker, Mahwah, NJ).
Intralesional treatment
Intentional intralesional treatment (curettage) was used for benign and low-grade malignant bone tumours such as giant cell tumour (GCT), aneurysmal bone cyst, fibrous dysplasia, and grade-1 chondrosarcoma (CHS-1) (now renamed atypicalcartilaginous tumour (ACT)). All CHS-1 lesions were curetted and treated with adjuvant phenol and ethanol. Some lesions were treated with radiofrequency ablation (RFA) beforehand. Most reconstructions were done with PMMA bone cement; some were done with cancellous bone chip: Vitoss (Orthovita, Malvern, PA). Most recent reconstructions were done with Engipore (Finceramica SpA, Faenza, Italy). We did
Computer-assisted surgery in orthopedic oncology
27
Computer-assisted surgery in orthopedic oncology
26
notusefluoroscopic control at the endof surgery. Follow-upwas standardised,with radiographic controls and a baseline MRI scan 3 months postoperatively. As an indicator of the effect of CAS on surgical time, we documented reported surgical time in the operating room management software for all procedures in the largest homogenousgroup,CHS-1intralesionaltreatment,witheitherCASorfluoroscopy,within the inclusion period.
Image-based resections
Resection planes were planned before surgery, incorporating the margin required forthespecificlesion,andcheckedintraoperatively.Preoperativeplanningconsistedof CT/MRI image fusion if available, segmentation (colouring) of the tumour and critical structures, depending on tumour type and location. The pointer tool was used before and after each resection to determine and check the resection plane. Planes for the bone saw were sometimes marked with Kirschner wires, placed with navigation, as a guide for plane orientation and angulation. As proof of complete resection, screen shots of the pointer tool or navigated chisel on the planned resection plane behind the tumour were saved on the CAS machine. Every bone resection had a routine postoperative radiographic control and pathological examination.
Image-based resections and reconstructions
This procedure was performed for hemicortical resections, creating and reconstructing a partial defect and 1 full resection. Preoperative planning consisted of CT/MRI image fusion, digital linking of the host bone CT with the allograft CT, planning of the resection planes (and subsequent reconstruction planes), and entering of special interest points where resection planes intersected other planes or the cortex. Exactly the same resection planes were used for both resection of thetumourandcreationoftheallograftpiece,tocreateanexact-fittinggraft.Thereconstructions of these defects were done with allogenic inlay bone grafts, in 1 case combined with a vascularised autograft. The allografts from the bone bank were selected based on matching of the dimensions to the host bone. The planned resection was then performed on the patient bone and subsequently repeated on the allograft bone.
Imageless workflow and imageless resection and reconstruction
Imagelessworkflowcomprisedanormalimagelesskneeset-up,withtrackersonthefemur and tibia. The imageless system provided accurate measurements of length and rotation. The software used in these cases was Precision Knee Navigation on

2
Computer-assisted surgery in orthopedic oncology
27
Computer-assisted surgery in orthopedic oncology
26
the same navigation system. All imageless cases were performed on or around thekneejoint.TheresectionlengthwasidentifiedbyCASusingthepointertool.Joint line reconstruction, length-checking, and rotation were done with the normal imageless prosthesis-placement checking tools. We used a modular GSMS/MRH tumour prosthesis (Stryker) in all cases.
Results The most performed procedure was grade-1 chondrosarcoma curettage (Table). The “reactive lesions” group contained cases where the surgery was performed by oncological principles but the pathological diagnosis was not a tumour. Most CAS procedures were done for a lesion in the femur (68 of 130). Figure 3 demonstrated the anatomical distribution. Mean follow-up time was 32 (4–80) months.
Intralesional treatment
CASwasusedasanalternativetofluoroscopyin60procedures(Figure4).Themeanfollow-up time was 25 (4–68) months. Most procedures were done for CHS-1. In 1 case of CHS-1 of the humerus, the postoperative radiographic control showed residualtumour.Thiswasconfirmedbybiopsyandwastreatedwithradiofrequencyablation (RFA). There was 1 recurrence of a CHS-1, 15 months after primary treatment. A biopsy showed vital tumour tissue and no dedifferentiation, and the lesion was treated with RFA. 43 CHS-1 patients were treated using CAS. This resulted in a recurrence rate of 1 in 43 for this group, at a mean follow-up time of 24 (7–61) months. There were 4 pathological fractures, all of which were treated and healed withinternalfixation.Mediansurgicaltimewassimilarinthe2groups:itwas1hourand 24 min (0:54–3:10) in 88 non-CAS CHS-1 intralesional treatment procedures and it was 1 hour and 26 min (0:37–2:25) in the 43 CAS procedures (p = 0.7).
Image-based resection
There were 43 CAS procedures with a mean follow-up time of 39 (5–80) months. 40of43procedureswereclassifiedasR0resections;1CHSgrade-2periacetabularresection had R1 margins due to a compromised soft-tissue margin, 1 CHS grade-1B proximal tibia had R1 margins due to a compromised bone margin, and 1 pelvic CHS grade-2A had an R2 resection—also due to compromised bone margins. The patientwithperipheralCHS-1ofthefibulawithinadequatebonemargins(R1)hada re-resection, but it did not show residual tumour, and the patient is disease-free 6 years after surgery.

Computer-assisted surgery in orthopedic oncology
29
Computer-assisted surgery in orthopedic oncology
28
Image-based intralesional treatment
Image-based resection
Image-based resection &
reconstruction
Image-less resection &
reconstruction
Total Procedures
CHS grade 1 43 3 46
Osteochondroma 26 26
Osteosarcoma 1 10 11
Reactive lesions 7 7
Fibrous dysplasia 7 7
CHS grade 2 5 5
Adamantinoma 4 4
Chondroblastoma 4 4
Giant cell tumor 3 3
Metastasis 1 2 3
Other 2 2
ABC 2 2
CHS grade 3 1 1
Ewing sarcoma 1 1
Total successful CAS 60 43 5 14 122
Total CAS failures 3 3 2 8
Total Procedures 63 46 5 16 130
Table 1: CAS patients with distribution of diagnoses for all CAS procedures, and individually for each procedure type. The index of diagnoses has been sorted by the number of patients
6 of 17 pelvic resections were performed for high-grade tumours. 2 of 4 Enneking type-2/3 resections (9), 1 of 1 type-1/2/3 hemipelvectomy, and 1 of 1 type-2 resection had R0 margins. 1 of 2 type-2/3 resections had a soft-tissue R1 resection as described above. All others, except 1 type-3 resection for a large osteochondroma, were partial resections. All had R0 margins.
There were 4 local recurrences: pelvic chondrosarcoma grade-2 (2 resections, R2 and R0), pelvic CHS grade-3 (1 resection, R0) and osteosarcoma of the femur (1 resection, R0). 3 patients—all of whom had local recurrence and dedifferentiation—died of disease, pelvic CHS grade 2 (2 patients), and pelvic CHS grade 3 (1 patient). In these 3 patients, dedifferentiation of the tumour was found in the biopsy of the local recurrence.
Joint-sparingprocedureswereperformedusingCAS,forexampleusingamodifiedEnneking 2/3 acetabulum-sparing resection in a case of grade-2 chondrosarcoma of the pelvis (Figure 5).

2
Computer-assisted surgery in orthopedic oncology
29
Computer-assisted surgery in orthopedic oncology
28
Fig 3 (left): Illustration of the bone localisations of the CAS cases. Based on Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist; “Human skeleton diagrams, lateral and anterior views” via Wikimedia Commons, Creative Commons Attribution 2.5.
Fig 4 (right): A screenshot acquired on the CAS system during curettage. Patient information is digitally edited out. The case is a 31-year-old patient with fibrous dysplasia of the femoral head. The location was such that there was a risk of damaging the cartilage on the femoral head during curettage, potentially invalidating the patient. The cavity was filled with PMMA. Weight bearing was 50% in the first 6 weeks, gradually increasing to full in the subsequent 6 weeks.
Image-based resection and image-based reconstruction
4 adamantinoma cases were treated with hemicortical resections and 1 Ewing sarcoma was treated with a segmental resection and solid allograft bone reconstruction. Mean follow-up time was 20 (10–33) months. The mean length of reconstruction for the hemicortical cases was 8 (6–9) cm, for the segmental reconstruction case it was 19 cm. In 3 of 4 hemicortical cases, half or more of the bone circumference was affected by the tumour. A CT-scan of 1 case showed a mean gap between host and allograft of 0.9 (0–5.4) mm along the 6-cm resection (Figure 6) (10). All margins wereclassifiedasR0.Therewas1localrecurrenceinanadamantinoma,afteranR0 resection with adequate margin, located in the soft-tissue resection plane. There were no complications.
Imageless resection and reconstruction
There were 14 procedures with a mean follow-up of 41 (8–60) months. The CAS group comprised 10 osteosarcomas, 2 metastases, and 2 tumour prosthetic placements in non-union or allograft failure after earlier tumour surgery. All tumour resections were reported as R0 resections. The 10 osteosarcomas could besubdividedusingMSTSclassificationinto:IA(1),IB(1),IIB(6),andIII(2).Therewere 2 local recurrences— R0 resections—both of osteosarcomas of the femur with MSTSclassificationsIIBandIII.1patientwith localrecurrencehadare-resection

Computer-assisted surgery in orthopedic oncology
31
Computer-assisted surgery in orthopedic oncology
30
and is disease-free. The other patient was treated with hip ex-articulation but died of metastatic disease. 1 osteosarcoma patient had proven lung metastasis at the time of surgery and had a local recurrence 1 year later. Figure 7 demonstrates a rotation and joint line check.
CAS failures
There were 8 failures, including 3 set-up failures for intralesional treatment CAS procedures; these were due to matching error, software failure, and loss of match after set-up. 3 failures in image-based resections were due to to software failure, matching error, or loss of match after set-up on the before-first-use accuracycheck. These last 2 failures were both in the ulna and were considered to be due to unstablefixationinthissmallbone,whichwasdetectedduringtheset-upphase.There were 2 failures in imageless CAS mode for tumour prosthesis placement due to tracker issues: 1 due to loss of accuracy on check because of instability caused by a preoperative pathological fracture and 1 where it proved impossible to place the trackersinsidethesoftware-definedworkfield.
System use
There were no direct complications and no morbidity related to use of the CAS system. There were no fractures or infections due to the pin placement. All software-reported accuracies were between 0.3 mm and 1.2 mm. Set-up time was measured in the last 47 cases. Mean set-up time was 6.5 (2.3–14) min.
Discussion Intralesional treatment is currently the standard surgical treatment for CHS-1/ACT lesions and an accepted alternative to resection (11, 12). There is a risk of local recurrence with intralesional treatment. Intraoperative image assistance is normally performedwithfluoroscopy.TheadvantagesofCASoverfluoroscopyaremainlyreal-time 3D feedback and high-resolution images. Both the patient and the surgical team are exposed to ionising radiation during a CAS procedure, and although the exposure is usually low, the effects of long-term multiple low-dosage exposure are unknown (13).
Of60successfulCAScases,therewasonly1withaninadequatecurettageidentifiedon the baseline MRI and another case with recurrence of grade-1 CHS. The follow-up is short, and longer follow-up is needed for a conclusion on CAS curettage. There were 4 fractures in this treatment group, all in the diaphysis of the femur. We then started routine plating and no more fractures occurred. The main indication where CAS offers additional value with better feedback is large lesions, especially situated

2
Computer-assisted surgery in orthopedic oncology
31
Computer-assisted surgery in orthopedic oncology
30
Figure 5: A. (left panel). Surgical planning of the resection planes in the Orthomap oncology module with colouration of the tumour on the fused MRI/CT image. Patient information has been digitally edited out in the bottom-left panel. The bottom-right panel shows a 3D rendering of the pelvic bone and the resection planes. Two-thirds of the acetabulum could be saved. The patient was disease-free at the 5-year follow-up, functions well, and has resumed work. B. (right panel). 3D AP volume rendering of the 3.5-year follow-up CT.
Figure 6 (left): A. An image-based resection and reconstruction procedure; intraoperative screen shot of the navigation system. The pointer tool is being used to align 1 of the 2 resection planes of the proximal “dome”-type resection. An intraoperative view is shown in Figure 2. B. Anteroposterior radiograph of the patient 11 months after surgery. Progressive incorporation of the allograft and vascularised autograft.
Figure 7 (right): Imageless resection and reconstruction. The CAS tibial guide is used to check the cut angulation and placement of the tibial component. Reconstruction was done with a GMRS/MRH prosthesis, with the CAS system being used for rotation control, joint angulation control, and length reconstruction.

Computer-assisted surgery in orthopedic oncology
33
Computer-assisted surgery in orthopedic oncology
32
indifficultanatomicallocationssuchasthefemoralheadandpelvis.However,withdatasets available CAS can be used as a technologically superior alternative without increased surgical time.
Regarding image-based resection, margin control was good with 40 of 43 R0 resections in the CAS cases. 1 was a soft-tissue R1 margin. The R1 and R2 resections in bone occurred in the first 10 cases. Most procedures were osteochondromaresections, where the system was used to support anatomical orientation. There was 1 local recurrence in an osteosarcoma of the tibia after resection with adequate margins. This recurrence may have been caused by multiple core needle biopsy attempts before referral, as 1 attempt punctured the tumour. R0 margin in pelvic resection was reached in 15 of 17 cases. 1 R1 resection was a soft-tissue margin; CAS was not used for this resection plane. The cause of the R2 resection is unknown. Sometimes it was possible, with careful planning and CAS precision support, to spare structures that would otherwise have had to be sacrificed due to lack ofresection plane control using conventional means (14). This— together with the pelvic resections and procedures for malignant lesions—is the main indication for CAS. Osteochondroma resections have little additional value, except better orientation and instrument position feedback.
In image-based resection and image-based reconstruction, the CAS system served as an objective measurement and guidance tool for the allograft-creation process. The ease with which the allograft could be created made the operation less demanding and more precise. A study of hemicortical resections showed complications, early and late fractures, in 6 of 21 patients, and called for better means of reconstruction (15). Use of CAS for reconstruction enables highly accurate bony reconstruction with massive hybrid (allogenic and autogenic) bone grafts. This may reduce the risk of complications and enable earlier mobilization. More complex resection and reconstruction shapes were possible, for minimal bone loss. We feel that the most inaccurate step at present in this type of procedure is the inaccuracy of the oscillating saw blade.
There have been reports of the use of CAS with good functional results in imageless resection and imageless reconstructions with custom tumour prostheses (16). As far as we know, there have been no reports of using imageless CAS in the placement of modular tumour prostheses. CAS can be helpful in accurate planning and measurement of resection length. It can also helpful in joint line reconstruction, as direct feedback on angulation, reconstruction length, and rotation is available in the software.However,nospecificimplantplacementdataareyetavailabletoclinicallysupport this improved feedback.
Margin control was excellent, with R0 resections in all 12 oncological procedures. The local recurrence rate for osteosarcoma was 20% (2 out of 10)—which is higher than
2
Computer-assisted surgery in orthopedic oncology
33
Computer-assisted surgery in orthopedic oncology
32
the recurrence rates of around 10% reported in the literature (17-19). The cause of this is unknown. However, in both cases where local recurrence occurred there was a poor response to chemotherapy, a well-known predictor of local recurrence. Use ofCASmostlikelydoesnotinfluencerecurrencerate,asthisismostlydependenton soft-tissue margins and response to chemotherapy.
Overall margin control using CAS was excellent. The pathologist reported R0 resections in 59 of 62 resections. 1 of the 3 resections that were not R0 was a soft-tissue R1 margin. Of the 18 high-grade tumour resections, there were 16 adequate bone margins.
Most set-up failures occurred early in the learning curve. Set-up time was measured for the last 47 cases and the mean value was 6.55 min. There were no complications related to CAS.
Due to the large heterogeneity and small number of patients per diagnosis and procedure, limited conclusions can be drawn from these data on clinical outcomes and functional results. Furthermore, there was insufficient follow-up and therewereinsufficientpatientnumbersforustobeabletodrawconclusionsabouttherecurrence rate.
In summary, CAS appears to be a promising new development in orthopaedic oncology. With limb salvage and function-saving surgery, there is a need for accurate navigation. It is also our opinion that CAS can be used in less complex procedures such as image-based resections and curettages too, where it is an accurate,technologicallysuperior,andradiation-freealternativetofluoroscopy.
Computer-assisted surgery in orthopedic oncology
35
Computer-assisted surgery in orthopedic oncology
34
References
(1) Wong KC, Kumta S, Chiu K, Antonio G, Unwin P, Leung K. Precision tumour resection and reconstruction using image-guided computer navigation. J Bone Joint Surg (Br) 2007; 89(7): 943-7.
(2) So TY, Lam Y, Mak K. Computer-assisted navigation in bone tumor surgery: Seamlessworkflowmodel and evolution of technique. ClinOrthop 2010;468(11): 2985-91.
(3) Cho HS, Oh JH, Han I, Kim HS. The outcomes of navigation-assisted bone tumour surgery: Minimum three-year follow-up. J Bone Joint Surg (Br) 2012; 94(10): 1414-20.
(4) Wong KC. A Practical Guide to Computer Assisted Tumor Surgery: CATS. : Red Corporation Limited; 2010.
(5) Cheong D, Letson GD. Computer-assisted navigation and musculoskeletal sarcoma surgery. Cancer Control 2011;18(3):171-6.
(6) Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of local recurrence in patients with a tumour of the pelvis or sacrum? Bone Joint J 2013; 95-B(10): 1417-24.
(7) Saidi K. Potential use of computer navigation in the treatment of primary benign and malignant tumors in children. Curr Rev Musculoskelet Med 2012; 5(2): 83-90.
(8) Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010; 17(6): 1471-4.
(9) Enneking WF, Dunham WK. Resection and reconstruction for primary neoplasms involving the innominate bone. Bone Joint Surg (Am) 1978; 60(6): 731-46.
(10) Gerbers JG, Ooijen PMV, Jutte PC. Computer-assisted surgery for allograft shaping in hemicortical resection: A technical note involving 4 cases. Acta Orthop 2013; 84(2): 224-6.
(11) Campanacci DA, Scoccianti G, Franchi A, Roselli G, Beltrami G, Ippolito M, et al. Surgical treatment of central grade 1 chondrosarcoma of the appendicular skeleton. . J Orthop Traumatol 2013; 14(2): 101-7.
(12) Hickey M, Farrokhyar F, Deheshi B, Turcotte R, Ghert M. A systematic review and meta-analysis of intralesional versus wide resection for intramedullary grade I chondrosarcoma of the extremities. Ann Surg Oncol 2011; 18(6): 1705-9.
(13) Giordano BD, Grauer NJ, Miller C P, Morgan T L, Rechtine II G R. Radiation
2
Computer-assisted surgery in orthopedic oncology
35
Computer-assisted surgery in orthopedic oncology
34
exposure issues in orthopaedics. J Bone Joint Surg (Am) 2011; 93(12): e69 1-10
(14) Gerbers J, Jutte PC. Hip-sparing approach using computer navigation in periacetabular chondrosarcoma. Comput Aided Surg 2013; 18.1-2: 27-32.
(15) Deijkers RL, Bloem RM, Hogendoorn PC, Verlaan JJ, Kroon HM, Taminiau AH. Hemicortical allograft reconstruction after resection of low-grade malignant bone tumours. J Bone Joint Surg Br 2002 Sep;84(7):1009-1014.
(16) Wong KC, Kumta SM. Joint-preserving Tumor Resection and Reconstruction Using Image-guided Computer Navigation. Clin Orthop 2013; 471(3): 762-73.
(17) Allison DC, Carney SC, Ahlmann ER, Hendifar A, Chawla S, Fedenko A, et al. A meta-analysis of osteosarcoma outcomes in the modern medical era. Sarcoma 2012; 2012: 704872.
(18) Picci P. Osteosarcoma (osteogenic sarcoma). Orphanet J Rare Dis 2007;2(6).
(19) Grimer RJ, Sommerville S, Warnock D, Carter S, Tillman R, Abudu A, et al. Management and outcome after local recurrence of osteosarcoma. Eur J Cancer 2005;41(4):578-583.

Hip sparing approach using computer navigation in periacetabu-lar chondrosarcoma: Added safety in difficult resections
JG Gerbers, PC Jutte
Published: Computer Aided Surgery 2013; 18.1-2: 27-32

Hip sparing approach using computer navigation in periacetabular chondrosarcoma
39
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
38
AbstractChondrosarcomaofthepelvis isdifficulttotreatduetoanatomical locationanddo often recur. Treatment is primarily surgical. Margins, based on MSTS criteria, have shown to be predicative of the disease recurrence and mortality. However too wide margins can decrease post operative function. CAS was used in this case to safely enable a joint salvaging approach in amodified type 2/3 resection ofa chondrosarcoma grade 2 of the os ischium and os pubis. The CAS navigation was vital in achieving the desired safe margins. Current follow-up is 3.5 years. The patient is disease free, no local recurrences or metastases were found. Post operative function is excellent, with good MSTS and SF36 scores. This case is a very good example of the additional value of CAS in certain cases.
3
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
39
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
38
IntroductionBone tumour resections in the pelvic bone are known as difficult due to theanatomical shape and surrounding structures (1). Chondrosarcomas located in the pelvis have a higher recurrence rate than chondrosarcomas located in the long bones (2). Treatment of chondrosarcomas, both in the pelvis and the long bones, is primarily surgical. Intermediate grade and high grade (II and III) chondrosarcoma in the pelvis are treated with wide resection, therapy for grade I chondrosarcoma can differ. Radiotherapy and chemotherapy effectiveness in chondrosarcoma only have a role as an adjuvant in compromised margins or high grade tumours (3, 4).
Depending on the location and grade of the chondrosarcoma the type of resection is chosen. These resections are described by the model proposed by Enneking and Dunham (5). Because of life over limb (or function) considerations, adequate margins are always the primary goal. Margins, based on MSTS criteria, have shown to be predicative of the disease recurrence and mortality (1). However too wide margins can decrease post operative function. A joint sparing approach is usually preferable over prosthesis placement or hip arthrodesis, especially in younger patients.
Ten year survival of chondrosarcoma grade 2 in the pelvis has been reported around 75 percent (1, 6). Recurrence has been reported in 44 percent of cases with a median time to recurrence of 23 months (6).
Computer-assisted surgery (CAS) has proved to be a safe means of navigation in tumour resections and has already been reported as being used in resections of pelvic tumours (7,8). In this case CAS makes a joint sparing approach possible, which is a really good example of the additional value CAS can have. This is the reason to report this case.
Case reportA 46 year old woman presented with pain symptoms in the right hip region. Four years earlier an X-pelvis made in another hospital had shown a small lesion near the right symphysis, in the upper ramus of the os pubis, interpreted as a cyst. There was nofollow-uptothesefindings.Becauseofprogressivestiffnessoftherighthipjointan X-ray and MRI were made 3.5 years later and a suspect lesion was found. The patient was referred to the orthopaedic oncologist. A new MRI localised the lesion to both the rami of the right os pubis and an expansion to the os ischium, close to the acetabulum.
A needle biopsy, analysed by a musculoskeletal pathologist, showed a grade 2 chondrosarcoma.ItcanbeclassifiedasastageIIBlesion(5,9).Thetumourlength
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
41
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
40
was 9.3 cm and volume was calculated using the Göbel et al method as 92.69 ml, with one episodical and one cylindrical arm (10). CT-thorax and bone scan showed no metastases.
Because of the localization near the hip joint and no soft tissue involvement, the two options for the resection were joint sparing local resection, or segmental resection andreconstructionwithasaddleprosthesis.Alocalresection,modifiedtype2/3ontheEnnekingetal.classification,wasdecidedupon,partlyresectingthefrontalpartof the right acetabulum to attain a safe margin (9). A pre-operative CT and MRI were obtained and the navigation was prepared in advance on the CAS system (Stryker Mahwah,US)(figure1,2).
The patient was prepared for surgery. An illo-inguinal incision was made, with subsequent preparation from the symphysis in the lateral direction to the os ilium. Thefemoralneurovascularbundlewasidentifiedandmarked.Twoortho-lockpinswere placed in the right crista iliaca for the patient tracker. CAS setup was performed andanaccuracyof0.5mmreported.Thenervusobturatoriuswas identifiedandreleased. With careful preparation the os ischium was uncovered. Then with the helpof thenavigationsystemthedeep resectionplane identified,checked forasafe margin, and a Kirschner wire was placed to mark the plane. The symphysis joint was considered possibly contaminated and a resection plane on the left os pubis was marked with a Kirschner wire, with the help of CAS. Finally the resection planearound thehip jointwas identifiedwith theCAS systemandmarkedwithdiathermia.
With an osteotome the hip joint was cut along the marked planes. The same was done for the symphysis resection and os ischium resection plane. The tumour was then carefully removed, after cutting the hamstrings, while carefully preserving the n. obturatorius. A Marlex mesh was used to reconstruct the inguinal channel. The subcutis and cutis were closed in layers. One deep drain was left in situ. After an uneventful wound healing period she was mobilised using two elbow crutches. The pathologist reported wide margins with a macroscopic and microscopic R0 resection, with a minimum margin of one centimetre in the acetabulum resection plane. It showedan infiltrativegrowingprocesswith infiltration in the trabecularbone and was reported as a grade two chondrosarcoma as in the biopsy specimen.
Current follow-up is 3.5 years. The patient is disease free, no local recurrences or metastaseswerefound.Thefollow-upwasdonewithMRIs,multidetectorCT(figure3),bonescans,andX-rayofthepelvisandX-rayofthethoraxatspecificintervals.
Function is currently good. The Musculo-Sketelal Tumor Society score (MSTS 1993) and the Short Form health survey (SF36 v2) score 2 years post operative were excellent. The MSTS was 29/30, or 98%, while the SF36 was 42.1 PCS-36 and 36.2 MCS-36.Aftertwoyearsthefunctionoftherighthipwas110/0/5degreesflexion/

3
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
41
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
40
Figure 1 (left): CT/MRI fusion with MRI based tumour colouration using the Orthomap Oncology Module (Stryker Mahwah, US), showing the peri-acetabular part of the grade 2 chondrosarcoma.
Figure 2 (right): Surgical planning of the resection planes in the Orthomap Oncology Module with tumour colouration on the fused MRI/CT image. Patient information is digitally edited out in the bottom left panel. The bottom right panel shows a 3D render of the pelvic bone and the resection planes.
Figure 3 (left): 3D AP volume rendering of the three and a half year follow-up CT.
Figure 4 (right): The femur was removed using iNtuition (TeraRecon) software applying semi-automatic, region growing based, segmentation. Subsequently a small parts removal was performed to remove remaining bone fragments which also removed all surgical clips from the data.

Hip sparing approach using computer navigation in periacetabular chondrosarcoma
43
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
42
extension, 20/0/10 degrees abduction/adduction and 30/0/20 degrees exorotation/endorotation. The patient is limited in end-range exorotation and kneeling can be somewhat painful. However, she can walk unaided, has no pain and has fully resumed her work.
DiscussionPost operative functions were excellent because two third of the acetabulum could be salvaged (figure 4). Rehabilitation time was relatively short. Alternateapproaches as allograft reconstruction, (pseudo)arthrodesis or tumour prostheses reconstruction are reported with lower post operative function then joint salvage (11). The post-operative functions with saddle prostheses are generally better then allograft reconstruction (12). However saddle prostheses can suffer from upward migration or dislocation and are limited in range of motion (12, 13).
Custom endoprostheses can be a good alternative to saddle prosthesis in pelvic tumours, but this case did not warrant the use of such prosthesis. Hip resection was not considered an option in this case due to limited range of motion and leg shortening. Reconstruction of the pelvic girdle is not necessary after resection.
The CAS navigation was vital in achieving the desired safe margins. It provided precise continuous 3d imaging. During the operation the resection planes could becheckedaccuratelyformargin,greatlyincreasingtheconfidenceofachievingawide resection. Preplanning the operation on the CAS machine has the advantage of already prepared resection planes, which can easily be followed intra-operatively. The CAS system was used as a guide for the resection planes. In more recent operations the system was used as well for guiding the instruments by attaching a tracker to e.g. an osteotome.

3
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
43
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
42
ConclusionChondrosarcomaof thepelvis isdifficult totreatduetoanatomical locationanddooftenrecur.Asthemarginsareaveryimportantpredictoroffollow-up,thefirstgoal should always be to achieve adequate margins. CAS has already been reported helpful in the resection of pelvic tumours. CAS was used in this case to safely enable ajointsalvagingapproachinamodifiedtype2/3resectionofachondrosarcomagrade 2 of the os ischium and os pubis. Joint salvaging approach is preferable over allograft reconstruction or saddle prosthesis placement whenever possible. Current follow up is 3.5 years and the patient is in remission. Post operative function is excellent, with good MSTS and SF36 scores. This case is a very good example of the additional value of CAS in certain cases. We think a joint sparing resection like in this case cannot safely be done without it.

Hip sparing approach using computer navigation in periacetabular chondrosarcoma
45
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
44
References
(1) Pring M-E, Weber K-L, Unni K-K, Sim F-H. Chondrosarcoma of the pelvis. A review of sixty-four cases. J Bone Joint Surg Am 2001;83-A:1630-1642.
(2) Bjornsson J, McLeod R-A, Unni K-K, et al. Primary chondrosarcoma of long bones and limb girdles. Cancer 1998;83:2105-2119.
(3) Gelderblom H, Hogendoorn P-C, Dijkstra S-D, et al. The clinical approach towards chondrosarcoma. Oncologist 2008;13:320-329.
(4) Sanerkin N-G, Gallagher P. A review of the behaviour of chondrosarcoma of bone. J Bone Joint Surg Br 1979;61-B:395-400.
(5) Enneking W-F, Dunham W-K. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am 1978;60:731-746.
(6) Sheth D-S, Yasko A-W, Johnson M-E, et al. Chondrosarcoma of the pelvis. Prognostic factors for 67 patients treated with definitive surgery. Cancer1996;78:745-750.
(7) Reijnders K, Coppes M-H, van Hulzen A-L, et al. Image guided surgery: new technology for surgery of soft tissue and bone sarcomas. Eur J Surg Oncol 2007;33:390-398.
(8) Wong K-C, Kumta S-M, Chiu K-H, et al. Precision tumour resection and reconstruction using image-guided computer navigation. J Bone Joint Surg Br 2007;89:943-947.
(9) Enneking W-F, Spanier S-S, Goodman M-A. A system for the surgical staging of musculoskeletal sarcoma. 1980. Clin Orthop Relat Res 2003;(415):4-18.
(10)GobelV,JurgensH,EtspulerG,etal.PrognosticsignificanceoftumorvolumeinlocalizedEwing’ssarcomaofboneinchildrenandadolescents.JCancerResClin Oncol 1987;113:187-191.
(11) Windhager R, Karner J, Kutschera H-P, et al. Limb salvage in periacetabular sarcomas: review of 21 consecutive cases. Clin Orthop Relat Res 1996;(331):265-276.
(12) Cottias P, Jeanrot C, Vinh T-S, et al. Complications and functional evaluation of 17 saddle prostheses for resection of periacetabular tumors. J Surg Oncol 2001;78:90-100.
(13) Aljassir F, Beadel G-P, Turcotte R-E, et al. Outcome after pelvic sarcoma resection reconstructed with saddle prosthesis. Clin Orthop Relat Res 2005;438:36-41.

Hip sparing approach using computer navigation in periacetabular chondrosarcoma
45
Hip sparing approach using computer navigation in periacetabular chondrosarcoma
44

Computer-assisted surgery for curettage of atypical cartilaginous tumors / chondrosarcoma grade 1 in the long bones compared to
fluoroscopic guidance
JG Gerbers, EF Dierselhuis, M Stevens, JJW Ploegmakers, SK Bulstra, PC Jutte
Under review
Computer-assisted surgery for curettage of ACT/CHS1
49
Computer-assisted surgery for curettage of ACT/CHS1
48
Abstract
Background and Objectives: Fluoroscopy is currently the standard imaging modality for curettage of atypical cartilaginous tumours (ACT/CS1). Computer-assisted surgery (CAS) is a possible alternative, offering higher resolution imaging and continuous three-dimensional feedback without ionizing radiation use. CAS hypothetically makes curettage more accurate, thereby improving residue or recurrencerate.ThisstudyaimstocompareCASandfluoroscopy.
Methods: Patients were selected from a prospectively kept local bone tumour database.CASandfluoroscopywereusedinparallel.Includedwerepatientswhohad curettage for ACT in the long bones, with a minimum follow-up of 12 months. Tumour volume was measured on pre-operative MRI scans. Outcome comprised local recurrence and residue rates, complications like fractures and procedure time.
Results: 77patientswere included, 17 in theCAS cohort, 60 in thefluoroscopycohort.TumourvolumewassignificantlylargerintheCAScohort(p=0.04).Residualtumour (2/17 vs. 6/60), fracture rate (3/17 vs. 6/60) and surgical time (1.26h vs. 1.34h)didnotdiffersignificantly.Therewerenorecurrencesineithergroup.
Conclusions: CAS curettage showed good oncologic results. Outcome was comparable tofluoroscopy,whilenotusing ionizing radiation.Residue rates canlikelybedecreasedwithspecificsoftwarefunctionsandsurgicaltools.
4
Computer-assisted surgery for curettage of ACT/CHS1
49
Computer-assisted surgery for curettage of ACT/CHS1
48
Introduction
Atypical cartilaginous tumour (ACT), previously named chondrosarcoma grade one (CS-1), is one of the most frequently treated lesions in orthopaedic oncology (1). The most commonly affected sites are the diametaphysis of the proximal and distal femur, the pelvis, the proximal tibia and humerus. Incidence of chondrosarcoma as a whole was estimated in an analysis of the American Surveillance, Epidemiology and End Results (SEER) database as 1 in 200.000 per year (2). A report of the European ESMO/EUROBONET registration describes the yearly incidence of chondrosarcoma as ~0.1/ 100.000 (3).
Because of ACT/CS-1’s potentiallymalignant nature, the surgical goal is a 100%removal of the tumour to prevent local recurrences and its associated decrease in patientsurvival(4,5).Upuntilaroundthe1980’streatmentofallchondrosarcomaconsisted of resection with wide margin. Better clinical and pathological knowledge and improved diagnostic techniques suggested this was not necessary for the less aggressive, low grade, lesions. The current standard surgical treatment consists of intralesional curettage often supported with fluoroscopy and the use of alocal adjuvant such as phenol/ethanol or liquid nitrogen (6, 7). Reconstruction is frequentlydonewithpolymethylmethacrylate(PMMA),syntheticfillers,allograftsorautografts. Depending on location and tumour characteristics, like X-ray visibility, it canbedifficulttoperformacompletecurettage.Cartilagecontentofthetumourdoesnotalwayscontainsufficientcalcificationtoreliablydepictthewholelesionon fluoroscopy. The percentage of residual tumour after curettage is possiblysignificant,assumingthat(early) localrecurrenceisofteninfact localresidue(8).Three-dimensional intra-operative imaging based on MRI may very well be an improvement in this aspect.
Fluoroscopy, the current standard, offers two-dimensional imaging and fluoro-video using X-band radiation (9). With the advances of computer technology in the operating room, a new potential alternative has been developed. Computer-assisted surgery (CAS) is a relatively new modality, originally developed for neurosurgery in theearly1990’s.ThemainadvantageofCASoverfluoroscopyisthatitgivesreal-time, continuous, high resolution 3D feedback, without the use of ionizing radiation. It uses pre-operative computed tomography (CT) and/or magnetic resonance imaging (MRI) scans as visual datasets. This means the surgeon is continuously aware of the tumour location and location of the instruments, with feedback on movement in three dimensions. In theory better orientation through CAS could make the surgery less demanding and improve clinical outcome in recurrence and residue rates. Cited disadvantages for CAS use are that there is no intra-operative assessment of the actual surgical result (i.e. the system shows a virtual result) and thesystemtakesvaluablesurgicaltimetosetupandconfigure(10,11).Thisstudy

Computer-assisted surgery for curettage of ACT/CHS1
51
Computer-assisted surgery for curettage of ACT/CHS1
50
aimstocomparefluoroscopyandCASintermsofsafetyandefficacyintreatmentof ACT/CS1 in the long bones.
Patients and methods
Design
A single centre retrospective cohort study was performed using the prospectively kept local bone tumour database. All patients with the procedure code for curettages of bone tumours were analysed. In accordance to regulations of the local Medical Ethical Review Board, all patients were informed about the fact that their data could beusedforscientificresearch. Ifpatientshadobjectionstotheuseoftheirdatathese data were not included in the study.
Patients
Inclusion criteria were: a curettage type procedure for histologically proven ACT/CS-1 in the long bones with the use of the adjuvants phenol and ethanol with a minimum follow-up of one year. Exclusion criteria were: the use of other means of treatment for the same lesion (e.g. radiofrequency ablation or cryotherapy), a non-complete follow-up and procedures that treated a recurrence. As this was a retrospective study the techniques were not actively randomised. Both techniques were used in parallel, with CAS use depending on system availability, planning and dataset quality.
Outcome measures
The primary outcome measure was potential residue or local recurrence. Potential residuewasdefinedasasuspect lesion (i.e. showing tumour likecharacteristics)reported on post-operative imaging, with consensus between the radiologist and orthopaedic surgeon. When there was no consensus an independent radiologist or orthopaedic surgeon was consulted. Recurrence was defined as a positivepathological sample for ACT/CS-1 after a (radiologically) tumour-free period. Secondaryoutcomemeasureswere:fractures,definedasafractureatthesurgicalsite regardless of adequate or inadequate trauma, other complications and intra-operative and surgical time.
Tumour volume approximation was done for each case on pre-operative MRI scans. The method used was as described by Verdegaal et al: calculation of the volume of animaginarycylinder(π*rmax2*hmax).Forrmaxthesumofmaximummeasured

4
Computer-assisted surgery for curettage of ACT/CHS1
51
Computer-assisted surgery for curettage of ACT/CHS1
50
radii anterior-posterior and medial-lateral was divided by two to produce the maximumradius.Wedefinedhmaxasthelargestmeasurementofproximal-distalsize (8).
Technique related time requirements were compared using the surgical time andpatient-in-ORtime.Thesurgicaltimewasdefinedasthehoursandminutesbetweenfirstincisionandwoundclosureasregisteredintheoperativeproceduresregistration database. Duration of the patient-in-OR time was defined as theperiod between the registered times of the patient entered the operating room and patient leaving the operating room.
Patient work-up
Pre-operative workup included a high resolution CT scan (for the CAS navigation group), a gadolinium enhanced MRI with or without Short inversion-Time Inversion Recovery (STIR) fat suppression sequences. Core needle biopsies were performed to rule out grade 2 chondrosarcoma; they were done under CT-guidance and classifiedby a specializedmusculoskeletal pathologist. In caseof earlier biopsyandreferral,thematerialwasrevisedbythepathologist.Pathologyclassificationisstandardized in the Netherlands by the Dutch Bone Tumour Committee, following theWHOclassifications(12).Theprocedureswereperformedbytwoorthopaedicsurgeons, assisted over the inclusion period by multiple orthopaedic surgeons in training.
CAS workflow
The curettages were done without pre-operative planning. Image fusion, generally CT with MRI, was done in the operating room while the patient was being prepared for surgery. The time consumption of tracker placement and software matching was measured using a stopwatch.
Afterboneexposure,theproceduredifferentiatesfromastandard(fluoroscopic)procedure. During a navigated procedure a CAS patient tracker was rigidly attached to the affected bone using two 3 mm pins. The pointer tool was then used for position checking, system calibration and remote control of the software. Image-based navigation was set-up by entering reference points both in software and on thepatient.Thepointbasedmatchwasrefinedbysurfacematchingwheredatapoints are entered with the pointer tool directly on the navigated bone. The system then presents an approximation of accuracy based on the difference between the entered points and the bone surface. The aim was an approximation of accuracy of lower than 1.0 mm. A Stryker Navigation System II with OrthoMap 3D software (Stryker Mahwah, NJ) was used in all cases. Surface matching on MRI is not

Computer-assisted surgery for curettage of ACT/CHS1
53
Computer-assisted surgery for curettage of ACT/CHS1
52
supported on the used system. After the setup of the CAS the place for the bone window is determined using the pointer tool and the window is made in a regular fashion. The curettage technique, from a surgical point of view, is not different from a normal procedure; curettes are used to scrape out the lesion.
The CAS system was used as a continuous-on imaging modality during the curettage process.Thecurettewasattachedtoatracker(figure1).Duringtheprocedurethesituation on screen did not update as it was still based on pre-operative imaging data(figure2).Assuchtherewasnodefinitivefeedbackuntilthepost-operativeradiographs.Afinalcheckattheendoftheprocedureisperformedbyusingthenavigated curette; it should access beyond all edges of the tumour. Screenshots weretakentoregistertheextentofthecurettage,comparabletoaworkflowwithfluoroscopy. All CAS procedures were done without intra-operative fluoroscopycontrol.
Fluoroscopy workflow
During a fluoroscopy supported curettage procedure imaging data was loadedonto digital displays in the OR for use during surgery. After dissection the lesion was localised with the fluoroscope to guide the place for the bone window. Awindow was made in a regular fashion in the cortex of the bone with an osteotome and hammer or electrical saw. The cavity was then curetted in a systematic way. Fluoroscopy was used for orientation during the procedure and to check if the curette reaches beyond all the visible edges of the tumour.
In both procedures the second part of the surgery is the same: when the curettage resultwassatisfying,thecavitywasthenfilledwiththefirstadjuvant:phenol.Smallswabs were used to clean the edges of the cavity. The phenol was then washed out with 95% ethanol. The bone window was also cleaned using this protocol. The cavitywasthenfilledwithPMMAorallograftbonechips.Whenindicatedpreventiveosteosynthesis material was applied to prevent a postoperative fracture (large window size, cortical resorption, diaphyseal localization). Plating was performed with a tibial LCP plate in diaphyseal lesions with 2 bicortical screws proximal and distal of the bone window.
Follow-up
After surgery, a standard X-ray was obtained as a routinely post-operative check. Three to four months later a baseline Gadolinium enhanced MRI was performed. After one year this was repeated. Further controls were done with radiographs. When a residue was suspected or if the lesion appeared active a more frequent MRI follow-up pattern was chosen. If the osteosynthesis material caused a too large

4
Computer-assisted surgery for curettage of ACT/CHS1
53
Computer-assisted surgery for curettage of ACT/CHS1
52
interference for radiological analysis, CT scans were used to assess follow-up.
Statistical analyses
Descriptive statistics were used to describe the main characteristics of the patient groups. General patient data as age and sex were compared, depending on data type, using independent sample t-tests or Pearson chi-square tests. Specificcategorical or dichotome variables, as recurrence and fracture rates, were compared with Fishers Exact test due to small sample sizes. Distribution of the different categoriesof reconstructionmethodsand theASAclassificationwerecomparedwiththeFreeman-HaltonextensionofFisher’sexacttest,usingtheexactmethod.
Numerical surgical characteristics data were tested for normality using the Shapiro-WilktestandweretestedwithaStudent’s t-test.Non-continuousvariableswerecompared with a Mann–Whitney U test. To assess potential causes for fractures binary logistic regression tests were performed with the dichotomous fractures variable as a dependant and calculated lesion size variable as continuous predictor and for the fracture variable as dependant and cement use as dichotomous predictor.All testsweredone two-sidedwhenapplicable.A significance levelof0.05 was chosen. Analysis of the data was performed with IBM Statistical Package for the Social Sciences (SPSS) version 22.
Figure 1 (left): Instrument tracker attached to a large curette. Note the maximized three-dimensional spacing of the infrared LED lights. The backside and battery compartment of another instrument tracker is visible in the background.
Figure 2 (right): Photograph during a typical CAS supported curettage procedure. Image-based visualization mode is set to standard view. The system shows the relevant MRI slices, fused to the CT dataset, based on position of the tool. The ACT lesion is coloured yellow by manual segmentation. The curette is visible as the blue line and the blue dotted line shows its vector in each direction. The lower right screen shows a volume render of the dataset, with the curette as the blue tool.
Computer-assisted surgery for curettage of ACT/CHS1
55
Computer-assisted surgery for curettage of ACT/CHS1
54
Results
Patient characteristics
77 patients were included who were treated between October 2006 and September 2013; 17 patients in the CAS cohort and 60 patients in the fluoroscopy cohort.Mean age at surgery was 53 years (range 24-82 years). Females were slightly more affected than males with a ratio of 1.1:1. Median follow-up was 43 months. Of the 79 patients included for analysis, 76 patients are currently alive; three patients have died of unrelated disease. Further demographic information is displayed in table 1 andfigure3.
Figure 3: General distribution of location of the ACT lesions.
Surgical characteristics
Analysis of the pre-operative data showed a significant difference between thelesion width (medial-lateral), with larger dimensions in the CAS cohort (p = 0.01). Median tumour volume was 18 cm3.Tumourvolumewassignificantlylarger(p=0.04) in the CAS cohort; 23 cm3
(9 cm3 -100 cm3) versus 16 cm3 (1 cm3 – 61 cm3) (see table 2).
Patient time in the operating room (patient-in-OR time) (2.15h versus 2.27h) and surgical time (1.26h versus 1.34h) was lower in the CAS cohort than in the fluoroscopy cohort, however both differences were not significant. CAS setup,measured in ten procedures, took on average 4 minutes and 25 seconds (range 2:03 min to 5:40 min).
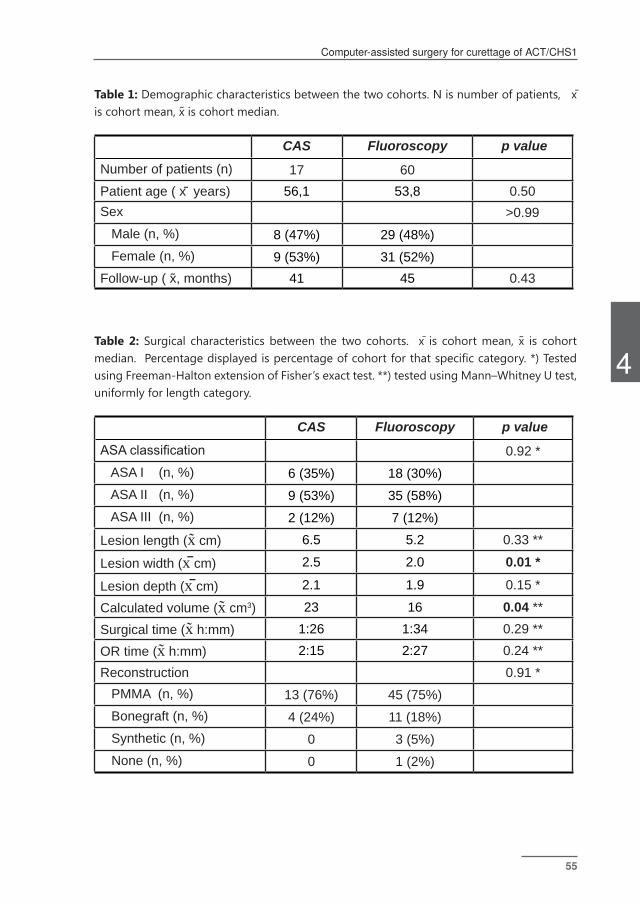
4
Computer-assisted surgery for curettage of ACT/CHS1
55
Computer-assisted surgery for curettage of ACT/CHS1
54
Table 1: Demographic characteristics between the two cohorts. N is number of patients, x̄ is cohort mean, x̃ is cohort median.
CAS Fluoroscopy p valueNumber of patients (n) 17 60Patient age ( x̄ years) 56,1 53,8 0.50Sex >0.99 Male (n, %) 8 (47%) 29 (48%) Female (n, %) 9 (53%) 31 (52%)Follow-up ( x,̃ months) 41 45 0.43
Table 2: Surgical characteristics between the two cohorts. x̄ is cohort mean, x̃ is cohort median.Percentagedisplayedispercentageofcohortforthatspecificcategory.*)TestedusingFreeman-HaltonextensionofFisher’sexacttest.**)testedusingMann–WhitneyUtest,uniformly for length category.
CAS Fluoroscopy p valueASA classification 0.92 * ASA I (n, %) 6 (35%) 18 (30%) ASA II (n, %) 9 (53%) 35 (58%) ASA III (n, %) 2 (12%) 7 (12%)
Lesion length (x̃ cm) 6.5 5.2 0.33 **
Lesion width (x̄ cm) 2.5 2.0 0.01 *
Lesion depth (x̄ cm) 2.1 1.9 0.15 *
Calculated volume (x̃ cm3) 23 16 0.04 **
Surgical time (x̃ h:mm) 1:26 1:34 0.29 **
OR time (x̃ h:mm) 2:15 2:27 0.24 **Reconstruction 0.91 * PMMA (n, %) 13 (76%) 45 (75%) Bonegraft (n, %) 4 (24%) 11 (18%) Synthetic (n, %) 0 3 (5%) None (n, %) 0 1 (2%)
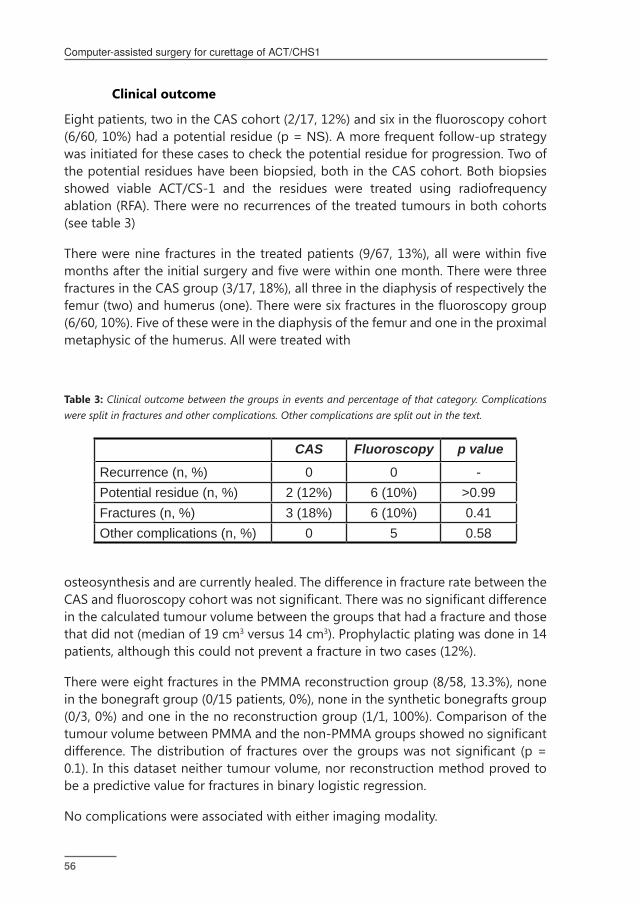
Computer-assisted surgery for curettage of ACT/CHS1
57
Computer-assisted surgery for curettage of ACT/CHS1
56
Clinical outcome
Eightpatients,twointheCAScohort(2/17,12%)andsixinthefluoroscopycohort(6/60, 10%) had a potential residue (p = NS). A more frequent follow-up strategy was initiated for these cases to check the potential residue for progression. Two of the potential residues have been biopsied, both in the CAS cohort. Both biopsies showed viable ACT/CS-1 and the residues were treated using radiofrequency ablation (RFA). There were no recurrences of the treated tumours in both cohorts (see table 3)
Therewereninefractures inthetreatedpatients (9/67,13%),allwerewithinfivemonthsaftertheinitialsurgeryandfivewerewithinonemonth.Therewerethreefractures in the CAS group (3/17, 18%), all three in the diaphysis of respectively the femur(two)andhumerus(one).Thereweresixfracturesinthefluoroscopygroup(6/60, 10%). Five of these were in the diaphysis of the femur and one in the proximal metaphysic of the humerus. All were treated with
Table 3: Clinical outcome between the groups in events and percentage of that category. Complications were split in fractures and other complications. Other complications are split out in the text.
CAS Fluoroscopy p valueRecurrence (n, %) 0 0 -Potential residue (n, %) 2 (12%) 6 (10%) >0.99Fractures (n, %) 3 (18%) 6 (10%) 0.41Other complications (n, %) 0 5 0.58
osteosynthesis and are currently healed. The difference in fracture rate between the CASandfluoroscopycohortwasnotsignificant.Therewasnosignificantdifferencein the calculated tumour volume between the groups that had a fracture and those that did not (median of 19 cm3 versus 14 cm3). Prophylactic plating was done in 14 patients, although this could not prevent a fracture in two cases (12%).
There were eight fractures in the PMMA reconstruction group (8/58, 13.3%), none in the bonegraft group (0/15 patients, 0%), none in the synthetic bonegrafts group (0/3, 0%) and one in the no reconstruction group (1/1, 100%). Comparison of the tumourvolumebetweenPMMAandthenon-PMMAgroupsshowednosignificantdifference.Thedistributionof fracturesover thegroupswasnotsignificant (p=0.1). In this dataset neither tumour volume, nor reconstruction method proved to be a predictive value for fractures in binary logistic regression.
No complications were associated with either imaging modality.

4
Computer-assisted surgery for curettage of ACT/CHS1
57
Computer-assisted surgery for curettage of ACT/CHS1
56
Figure 4: Series of images of a female patient after a CAS procedure for CHS1 in the right distal femur. A: the post-operative radiograph (Follow-up: 0 days). The defect is reconstructed with a bonechips (bonegraft). No residue visible. B: shows the baseline MRI scan of the same patient (follow-up 3 months). The depicted TIRM sequence shows a reactive response to the graft, with local oedema. However below the reconstruction is another lobular, fluid rich structure: retrospectively a potential residue but the radiologist describes it as most likely a postoperative reaction of the bone. Further radiographic follow-up shows no recurrence. C: TIRM sequence of the same patient (follow-up: 25 months) shows a nearly died down reaction to the graft but a more clear, reactive, lobular structure on the distal part of the lesion. Biopsy before RFA treatment confirmed CHS-1 tissue.
DiscussionComputer-assistedsurgeryhasbecomeanacceptedtreatmentmodalityfordifficulttumour resections (11, 13). While it offers potentially superior imaging feedback there have been no reports on use of CAS for the curettage of bone tumours, other than a few reported cases for bone tumours located in the spine (14). The higher resolution imaging, three-dimensional feedback and no limitations in feedback timemakeCASalogicalandtechnologicallysuperioralternativetofluoroscopy.
Clinical results of the CAS and fluoroscopy cohorts were comparable, with asignificantly larger tumour volume in the CAS cohort. There were no tumourrecurrences according to the definition; however eight residues were identified(12%).Althoughtheseoutcomefiguresseemsatisfying,theyaredifficulttocompareto literature, were recurrence rates are reported between 3.5% and 13.3%, in studies with similar adjuvants (15, 16). Important is that this depends on the interval and type of follow-up imaging.
As Verdegaal et al. have demonstrated, some local recurrences might actually be residues (8). ACT/CS-1 is a low grade tumour and generally grows slowly. Thus, suspect lesions on the 3 month baseline scans should be considered tumour residue.

Computer-assisted surgery for curettage of ACT/CHS1
59
Computer-assisted surgery for curettage of ACT/CHS1
58
In fact all lesions detected within one year should probably be considered residues. Furthermore studies reporting recurrence rates using radiographs will likely miss smaller tumour residues. An example of a potentially missed residue can be seen in animagecollageinfigure4.Whilethepost-operativeradiographsofthekneeshowno apparent tumour residue the baseline MRI shows a suspect lesion. Taking this into account, recurrence will likely be over-reported and residue under-reported in studies using radiographs during follow-up. As residue is primarily a problem of intra-operative orientation, this is something the three-dimensional and high-resolution feedback aspect of CAS can possibly improve.
Potential residues were found in two out of 17 CAS patients and in six out of 60 fluoroscopy patients. Both potential residue cases in the CAS cohorts showedtumour tissue at biopsy. Actual residue rate for the fluoroscopy cohortmay belower than six as GD-MRI has positive prediction rate of 45% for actual residue on suspect follow-up scans (8). Analysis of the CAS residue cases did not show a clear cause. Our hypothesis is that the feedback mode is currently not yet good enough forCAStobebetterthanfluoroscopy,especially the lackofprogresstracking. Italsoshowsthatit’snotaninfallibleguide.Whilenonavigationalinaccuracieswereexperienced, regular accuracy checks, on a known landmark, are advised.
Fracture rates in this study (12%) are high compared to literature. Recent studies, with the same adjuvants, show a fracture rate ranging from 5.0 to 6.6 percent. A possible cause for this can be difference in preventive osteosynthesis strategies (7, 16-20). 58 of the 77 patients treated in this study had a reconstruction with PMMA. While it is suspected that the exothermic PMMA hardening process can have a beneficialeffectasanadditionaladjuvant,itmayhaveadetrimentaleffectonthehost bone. Literature shows no significant difference in recurrence and fracturerates between using PMMA or other reconstruction methods (16, 21). As there were no recurrences, we cannot draw conclusions on PMMA and recurrence rate. Fracture rate in PMMA seems higher with 8 fractures out of 58 patient treated (14%) compared with a 6% fracture rate in the other reconstruction methods, although thisdidnotreachsignificance.Asthefractureratewasconsideredtoohigh,amoreaggressive plating strategy was adopted for procedures in the diaphysis of the femur. There was also a possible bias in fracture risk as a concurrent radiofrequency ablation (RFA) trial meant the exclusion of patients with mainly smaller ACT/CS-1 lesions in the femoral metaphysis (22).
The often cited downside of CAS use, the long set-up time, was not experienced (10). Set-up time, measured in the later cases, was on average just 4 minutes and 25 seconds. The median surgical time, even with the learning curve for CAS, was less thanforfluoroscopy.Whilenotsignificantlybetter,itshowsthattheset-uptimeisrecouped during the procedure.

4
Computer-assisted surgery for curettage of ACT/CHS1
59
Computer-assisted surgery for curettage of ACT/CHS1
58
Use of CAS has been described by both surgeons as useful, due to the continuous three-dimensional feedback, compared with the intermitted two-dimensional feedbackinfluoroscopy.ApplicationofCASinthehumeruswasconsideredmoredifficultduetoissueswithtrackerplacementintheworkingfield.Smallertrackerscould solve this issue. There were no direct complications nor any morbidity related to use of the CAS system. Possible complications as pin tract fractures or pin tract infections did not occur.
This study has some limitations. It was set-up as a retrospective cohort study, the study population was not equally divided and the techniques were not actively randomized. Both the techniques were however used in parallel, with CAS use only depending on system availability, planning and dataset quality. As far as we know, this is thefirststudyontheusageofCASforcurettageofACT/CS-1 inthe longbones. It is encouraging that CAS as new technique achieves good results.
Some improvements to workflow and instruments will probably have a positiveeffectonoutcomemeasurements.Currentlyit’snotpossibletoseetheextentofthealreadytreatedarea.A‘paintbrush’mode,wherethepositionofthetipispaintedinto the three-dimensional view would provide feedback on surgical progress. This together with the addition of a planning mode to the software could provide an intra-operative residue check. Furthermore it is likely that a more accurate curettage with less healthy bone removed can decrease fracture rates. Also there should be support for non-straight tools like bended, hockey stick, shaped curettes and pointers, for easier access to tumour tissue in corners of the lesion.
ConclusionsCAS curettage with phenol/ethanol adjuvants has showed excellent oncological results,atleastcomparabletothefluoroscopycohortandliterature.CAScurettageis safe and effective. There were no recurrences, and no difference in the occurrence ofresiduesbetweenthecohorts,thisdespitesignificantlylargerlesionsintheCAScohort. Fracture rates in both groups were higher than expected. In this study this was not linked to technique, PMMA use or size of the lesions. This study also supports the use of MRI follow-up for residue and recurrence detection. Studies with only radiographic follow-up likely underreport on residue- and over-report on recurrence-rate. Especially a suspected high residue rate after curettage supports the development of better intra-operative orientation. Clinical outcome of the present study supports CAS use as an alternative to fluoroscopy. With CAS noionizing radiation was used during these surgeries and there was no increase in surgicaltime.Residueratescanlikelybeimprovedwithspecific,curettagetargeted,software modules and tools.

Computer-assisted surgery for curettage of ACT/CHS1
61
Computer-assisted surgery for curettage of ACT/CHS1
60
References:(1) Damron TA, Ward WG, Stewart A. Osteosarcoma, chondrosarcoma, and Ewing’s
sarcoma: national cancer data base report. Clin Orthop 2007;459:40-47.
(2) Giuffrida AY, Burgueno JE, Koniaris LG, Gutierrez JC, Duncan R, Scully SP. Chon-drosarcoma in the United States (1973 to 2003): an analysis of 2890 cases from the SEER database. J Bone Joint Surg Am 2009;91(5):1063-1072.
(3) Hogendoorn P, Athanasou N, Bielack S, De Alava E, Dei Tos A, Ferrari S, et al. Bone sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2010;21(suppl 5):v204-v213.
(4) Gelderblom H, Hogendoorn PCW, Dijkstra S, van Rijswijk C, Krol A, Taminiau AHM, et al. The clinical approach towards chondrosarcoma. Oncologist 2008;13(3):320-329.
(5) Andreou D, Ruppin S, Fehlberg S, Pink D, Werner M, Tunn P. Survival and prog-nostic factors in chondrosarcoma: Results in 115 patients with long-term follow-up. Acta Orthop 2011;82(6):749-755.
(6) Hickey M. A systematic review and meta-analysis of intralesional versus wide resection for intramedullary grade I chondrosarcoma of the extremities. Ann Surg Oncol 2011;18(6):1705-1709.
(7) Van Der Geest I, De Valk M, De Rooy J, Pruszczynski M, Veth R, Schreuder H. Oncological and functional results of cryosurgical therapy of enchondromas and chondrosarcomas grade 1. J Surg Oncol 2008;98(6):421-426.
(8) Verdegaal SH, Brouwers HF, van Zwet EW, Hogendoorn PC, Taminiau AH. Low-grade chondrosarcoma of long bones treated with intralesional curettage followed by application of phenol, ethanol, and bone-grafting. J Bone Joint Surg Am 2012;94(13):1201-1207.
(9) Kahler D. Image guidance: fluoroscopic navigation. Clin Orthop 2004(421):70-76.
(10) Saidi K. Potential use of computer navigation in the treatment of primary benign and malignant tumors in children. Curr Rev Musculoskelet Med 2012:1-8.
(11) Wong KC, Kumta SM. Computer-assisted Tumor Surgery in Malignant Bone Tumors. Clin Orthop Relat Res 2012:1-12.
(12) Rosenberg AE. WHO Classification of Soft Tissue and Bone, fourth edition: summary and commentary. Curr Opin Oncol 2013;25(5):571-3.
(13) Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of
4
Computer-assisted surgery for curettage of ACT/CHS1
61
Computer-assisted surgery for curettage of ACT/CHS1
60
local recurrence in patients with a tumour of the pelvis or sacrum? Bone Joint J 2013;95-B(10):1417-24.
(14) Rajasekaran S, Kamath V, Shetty AP. Intraoperative Iso-C three-dimensional navigation in excision of spinal osteoid osteomas. Spine 2008;33(1):E25-9.
(15) Donati D, Colangeli S, Colangeli M, Claudia Di Bella M, Bertoni F. Surgi-cal treatment of grade I central chondrosarcoma. Clin Orthop Relat Res 2010;468(2):581-9.
(16) Campanacci DA, Scoccianti G, Franchi A, Roselli G, Beltrami G, Ippolito M, et al. Surgical treatment of central grade 1 chondrosarcoma of the appendic-ular skeleton. J Orthop Traumatol 2013: 14(2), 101-7
(17) Aarons C, Potter BK, Adams SC, Pitcher Jr JD. Extended intralesional treat-ment versus resection of low-grade chondrosarcomas. Clin Orthop Relat Res 2009;467(8):2105-2111.
(18) Souna BS, Belot N, Duval H, Langlais F, Thomazeau H. No recurrences in select-ed patients after curettage with cryotherapy for grade I chondrosarcomas. Clin Orthop Relat Res 2010;468(7):1956-1962.
(19) The International Agency for Research on Cancer (IARC). Who Classification of Tumours of Soft Tissue and Bone. World Health Organization; 2013.
(20) Verdegaal SH, Brouwers HF, van Zwet EW, Hogendoorn PC, Taminiau AH. Low-Grade Chondrosarcoma of Long Bones Treated with Intralesional Curettage Followed by Application of Phenol, Ethanol, and Bone-Grafting. The J Bone Joint Surg Am 2012;94(13):1201-1207.
(21) Streitbürger A, Ahrens H, Balke M, Buerger H, Winkelmann W, Gosheger G, et al. Grade I chondrosarcoma of bone: the Münster experience. J Cancer Res Clin Oncol 2009;135(4):543-550.
(22) Dierselhuis EF, van den Eerden PJ, Hoekstra HJ, Bulstra SK, Suurmeijer AJ, Jutte PC. Radiofrequency ablation in the treatment of cartilaginous le-sions in the long bones: results of a pilot study. Bone Joint J 2014 Nov;96-B(11):1540-1545.


Computer-assisted surgery for allograft shaping in hemicortical resection: A technical note involving 4 cases
JG Gerbers, PMA Van Ooijen , PC Jutte
Published: Acta Orthopaedica 2013; 84(2): 224-6

Computer-assisted surgery for allograft shaping in hemicortical resection
65
Computer-assisted surgery for allograft shaping in hemicortical resection
64
IntroductionHemicorticalresectionwasfirstdescribedbyCampanaccietal(1982)(1).Severalstudies support the technique as a safe alternative to larger segmental resections for low-grade chondrosarcoma (Deijkers et al. 2002), pareostal osteosarcoma (Lewis et al. 2000, Pezzillo et al. 2008) and adamantinoma (Agarwal et al. 2007) (2-5). However there have been several complications reported with this resection and reconstruction, the most important being fractures of the host bone, inadequate margins, and infection.
The resections and reconstructions are usually done without objective 3-D measurements. Computer-assisted surgery (CAS) offers objective measurements in 3D with high accuracy. It can be used to produce an exact copy of the resected part of the host bone by using the same resection planes in both tumour and allograft resection. In this technical note we describe the technique, report results and identify shortcomings and possibilities.
Surgical techniqueWe used a fresh frozen donor tibia with similar dimensions as the host tibia. A preoperative CT-scan was performed of both the patient and the donor bone. These scans were imported in the CAS system (Stryker, Mahwah, NY. Orthomap software) andmanually matched to find the optimum overlay. Special care was given tomatch the cortices of the host and donor bone. The resection was planned with both resection planes and annotation points. The planned resection planes (Figure 1) from the CAS setup of the host bone are now also usable in the allograft dataset because the two datasets are linked and matched in the CAS system.
Normal CAS setup was performed using a patient tracker placed on the tibia. A system calculated deviation, between the CT and spatial data, of less than 1.0 mm was accepted as in our normal image-based set-up. The pointer tool was then used to identify and mark the edges and entry points of the planned trapezoid or wedge-like shape. The excision planes were marked with a pen and checked with the pointer tool for accuracy. The corners of the resection shape were marked with annotation points (as special interest points) as extra feedback. We used an oscillating bone saw to perform the pre-planned trapezoid or wedge shaped resection. Angulation of the saw was checked at intervals using the pointer tool. Resection planes were checked again for margin after resection. The exact same procedure was followed in theallograftbone(Figure2).2screwswereusedforfixationofthegrafts.
Patients4 patients were selected for hemicortical resection using CAS. All had a diagnosis of adamantinoma, reported by a specialized musculoskeletal pathologist. Mean
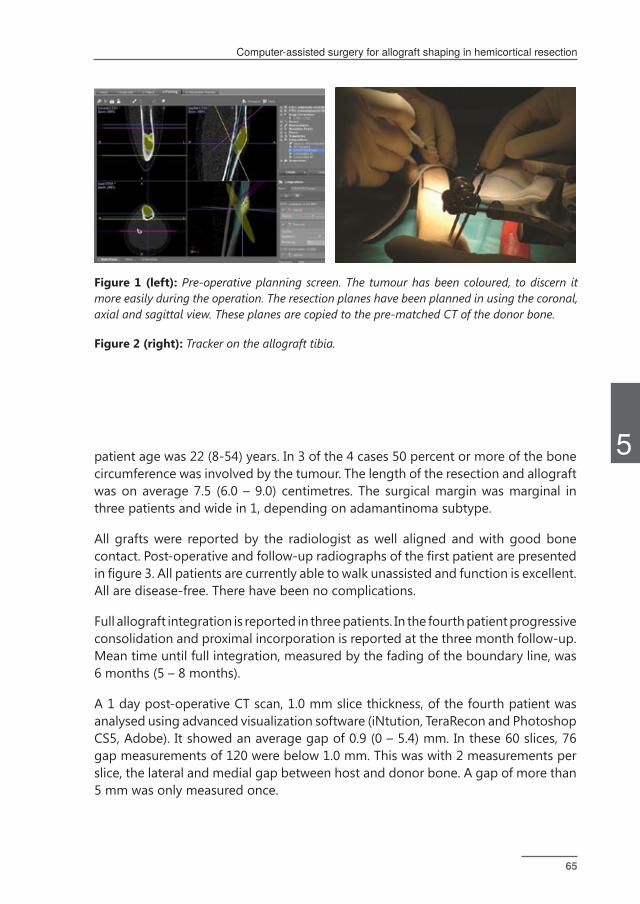
5
Computer-assisted surgery for allograft shaping in hemicortical resection
65
Computer-assisted surgery for allograft shaping in hemicortical resection
64
patient age was 22 (8-54) years. In 3 of the 4 cases 50 percent or more of the bone circumference was involved by the tumour. The length of the resection and allograft was on average 7.5 (6.0 – 9.0) centimetres. The surgical margin was marginal in three patients and wide in 1, depending on adamantinoma subtype.
All grafts were reported by the radiologist as well aligned and with good bone contact.Post-operativeandfollow-upradiographsofthefirstpatientarepresentedinfigure3.Allpatientsarecurrentlyabletowalkunassistedandfunctionisexcellent.All are disease-free. There have been no complications.
Full allograft integration is reported in three patients. In the fourth patient progressive consolidation and proximal incorporation is reported at the three month follow-up. Mean time until full integration, measured by the fading of the boundary line, was 6 months (5 – 8 months).
A 1 day post-operative CT scan, 1.0 mm slice thickness, of the fourth patient was analysed using advanced visualization software (iNtution, TeraRecon and Photoshop CS5, Adobe). It showed an average gap of 0.9 (0 – 5.4) mm. In these 60 slices, 76 gap measurements of 120 were below 1.0 mm. This was with 2 measurements per slice, the lateral and medial gap between host and donor bone. A gap of more than 5 mm was only measured once.
Figure 1 (left): Pre-operative planning screen. The tumour has been coloured, to discern it more easily during the operation. The resection planes have been planned in using the coronal, axial and sagittal view. These planes are copied to the pre-matched CT of the donor bone.
Figure 2 (right): Tracker on the allograft tibia.
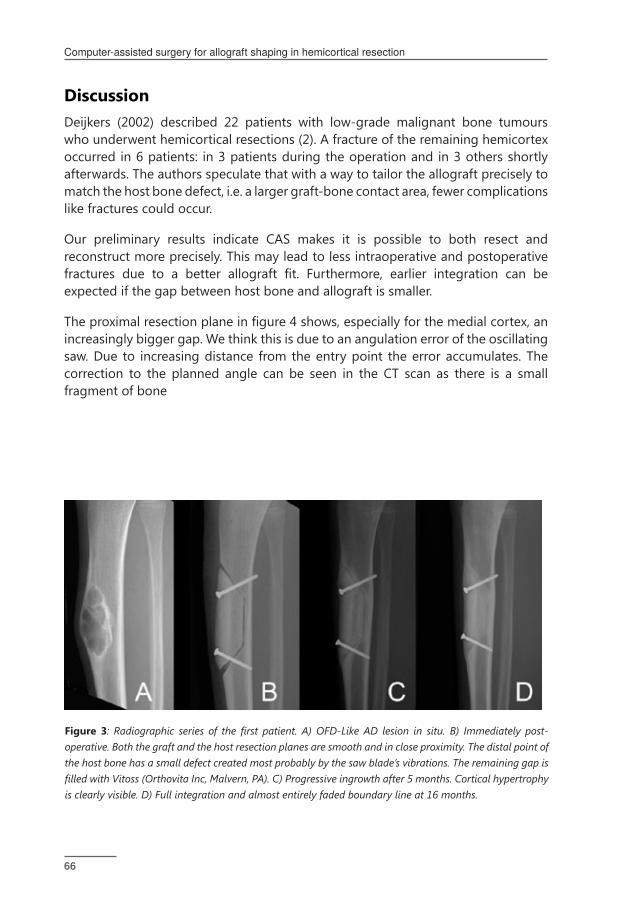
Computer-assisted surgery for allograft shaping in hemicortical resection
67
Computer-assisted surgery for allograft shaping in hemicortical resection
66
DiscussionDeijkers (2002) described 22 patients with low-grade malignant bone tumours who underwent hemicortical resections (2). A fracture of the remaining hemicortex occurred in 6 patients: in 3 patients during the operation and in 3 others shortly afterwards. The authors speculate that with a way to tailor the allograft precisely to match the host bone defect, i.e. a larger graft-bone contact area, fewer complications like fractures could occur.
Our preliminary results indicate CAS makes it is possible to both resect and reconstruct more precisely. This may lead to less intraoperative and postoperative fractures due to a better allograft fit. Furthermore, earlier integration can beexpected if the gap between host bone and allograft is smaller.
Theproximalresectionplaneinfigure4shows,especiallyforthemedialcortex,anincreasingly bigger gap. We think this is due to an angulation error of the oscillating saw. Due to increasing distance from the entry point the error accumulates. The correction to the planned angle can be seen in the CT scan as there is a small fragment of bone
Figure 3: Radiographic series of the first patient. A) OFD-Like AD lesion in situ. B) Immediately post-operative. Both the graft and the host resection planes are smooth and in close proximity. The distal point of the host bone has a small defect created most probably by the saw blade’s vibrations. The remaining gap is filled with Vitoss (Orthovita Inc, Malvern, PA). C) Progressive ingrowth after 5 months. Cortical hypertrophy is clearly visible. D) Full integration and almost entirely faded boundary line at 16 months.

5
Computer-assisted surgery for allograft shaping in hemicortical resection
67
Computer-assisted surgery for allograft shaping in hemicortical resection
66
Distance between host bone cortex and allograft cortex (mm)
0
1
2
3
4
5
6
7
8
9
10
1 6 11 16 21 26 31 36 41 46 51 56 61
Dist
ance
in M
M
Medial Cortex Gap
Lateral Cortex Gap
Figure 4 (left): Graph of the post-operative CT scan of the fourth patient. Average gap was 0.9 mm (range 0 mm – 5.4 mm). The sharp increase of the medial gap is due to an angulation error during resection.
Figure 5 (right): 3D rendered images of the fourth patient. Made with iNtution (TeraRecon). The allograft is auto-segmented and coloured green. Medial view shows the defect caused by an angulation misalignment in the last stage of the proximal resection plane. A) Medial view. Two distinct resection cuts are visible B) Anterior-posterior view. C) Lateral view.

Computer-assisted surgery for allograft shaping in hemicortical resection
69
Computer-assisted surgery for allograft shaping in hemicortical resection
68
between the too wide resection plane and the correct one (Figure 5B). We think that thisfindingsupportstheneedofanavigatedmeansofresection,asthesystemcancheck the angulation of the saw at any point of the resection.
Wetriedtoattachatrackertoabonesawanduseitwithnavigationinthefirstprocedure, to excise the tumour and cut the graft, but it proved inaccurate. The tracker was attached to the saw and calibrated in a universal calibration tool but thebladewastooflexibletocalibratereliably.
Alternatives can be pre-planned saw blocks for both the patient and allograft bone. CAS has the advantage that the resection planes can be adjusted during surgery and there is no placement inaccuracy. Another alternative is the pre-fabrication by3dprintingofafillermaterial.Accurateresectionhastobeperformedforthefillertofit,andwefeelnavigationisagainrequired.Furthermoreanon-biologicalsolution is more likely to fail in the long run.
The CAS system makes the creation of the allograft easier. The technique can be applied to any bone tumour eligible for hemicortical resection but also other defects requiring bony reconstructions.

5
Computer-assisted surgery for allograft shaping in hemicortical resection
69
Computer-assisted surgery for allograft shaping in hemicortical resection
68
References(1) Campanacci M, Capanna R, Stilli S. Posterior hemiresection of the distalfemur in
parosteal osteosarcoma. Ital J Orthop Traumatol 1982; 8 (1): 23-8.
(2) Deijkers R L, Bloem R M, Hogendoorn P C, Verlaan J J, Kroon H M, Taminiau A H. Hemicortical allograft reconstruction after resection of low-grade malig-nant bone tumours. J Bone Joint Surg Br 2002; 84 (7): 1009-14.
(3) Lewis V O, Gebhardt M C, Springfield D S. Parosteal osteosarcoma of the poste-rior aspect of the distal part of the femur. Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000; 82-A (8): 1083-8.
(4) Pezzillo F, Maccauro G, Nizegorodcew T, Rossi B, Gosheger G. Resection of parosteal osteosarcoma of the distal part of the femur: An original recon-struction technique with cement and plate. Sarcoma 2008; 2008: 763056.
(5) Agarwal M, Puri A, Anchan C, Shah M, Jambhekar N. Hemicortical excision for low-grade selected surface sarcomas of bone. Clin Orthop Relat Res 2007; 459: 161-6.


Enhancing precision and accuracy in bone tumour treatment. An experimental comparison of freehand, computer assistance
(CAS) and a novel universal CAS saw guide
JG Gerbers, PK Tomaszewski, M Stevens, N Verdonschot, SK Bulstra, PC Jutte
Under review

Enhancing precision and accuracy in bone tumour treatment
73
Enhancing precision and accuracy in bone tumour treatment
72
AbstractHemicortical (multiplanar) bone tumour resections and reconstructions are demanding procedures. The technique depends on high surgical accuracy to achieve an oncologically safe resection and it is associated with complications suchas fractures.Usual care isfluoroscopyguided freehand resection.CAScanimprove intra-operative orientation but is not directly used in the resection, thereby potentially decreasing total accuracy. Investigated was if computer-assisted surgery (CAS) can improve the resection and reconstruction accuracy and precision, either with CAS guided freehand resection or using a novel CAS guide.
An experimental study was performed on six cadavers (12 femurs), providing two procedures per technique. A virtual tumour was resected and the defect reconstructed with a graft from a matching femur. Pre-operative and post-operative imaging, together with surgical planning software, provided both a surgical objective and offered high-resolution measurements.
Three procedures had intra-lesional resections, the two freehand procedures and one of the CAS procedures Point-measured resection accuracy (measured in mm deviation) was lowest in the freehand procedures (6.1 and 4.0 mm), good in CAS (3.9 and 3.2 mm) and highest in the two CAS guide procedures (3.0 and 1.2 mm). Plane smoothness (precision) was lowest in the freehand procedures and highest in the CAS-guide procedures. Achieved accuracy for CAS was comparable to literature. CAS-guides did slightly better.
CAS and especially the CAS-guide procedures have demonstrated higher accuracy resections and reconstructions than freehand. The CAS guide is a tool that can be used to enhance the actually achieved accuracy closer to the real accuracy of the CAS system. This enhanced accuracy and precision potentially increases functional outcome, oncological outcome and complication rates.
6
Enhancing precision and accuracy in bone tumour treatment
73
Enhancing precision and accuracy in bone tumour treatment
72
IntroductionBetter knowledge of tumour biology, multimodal treatment and advances in imaging and surgical technology have enabled a trend in orthopaedic oncology to save more healthy tissue while safely removing the tumour. This enabled that some low-malignant lesions can be treated without resecting the full diameter of the bone. These hemicortical or hemicylindrical multiplane resections were firstdescribed for the resection of low grade cortical tumours by Campannaci et al. in 1982 (1). It’s considered a oncologically safe alternative to larger segmentalresections for low-grade chondrosarcoma (2), parosteal osteosarcoma (3, 4), and adamantinoma (5). The same technique, a multi-planar resection, has also been applied to reconstruction after large curettages and joint salvage procedures (6, 7). Due to the complex shape of resection and the need for high accuracy, it is described as a very demanding procedure. Lack of accuracy can easily lead to intralesional resections and complications like fractures and/or pseudo-arthroses due to a lack ofsufficientbonecontactat thehost/graft interface(2).Several techniqueshaverecently been developed that can assist in the resection and reconstruction of these defects.
Computer-assisted surgery (CAS) can offer objective measurements in three dimensions with high accuracy. It has become an accepted treatment modality for difficult tumour resections (8-10). Furthermore CAS can be used to simplifythe creation of highly accurate allografts by exactly duplicating the used tumour resection paths (6, 11-13). However CAS only provides intra-operative feedback as it just helps in orientation, the resection is still performed free-handed. The achieved accuracy, while good, is lower than the maximal accuracy and precision that the CAS system can offer (14). A combination of both orientation and execution objectification can potentially further increase surgical accuracy and decreasesassociated complications in this type of procedure. Simply put, we can accurately find the ‘directions’ of our surgical planning, but we cannot reproduce this asaccurately because the actual sawing is free-hand.
The present study introduces a new versatile universal tool, designed to offer objective navigation and resection guidance during surgery. This tool can be used asanon-patientspecific,adjustable,CASnavigatedresectionguide (CASguide).Accuracy and precision of the resection and reconstruction procedure was compared between three surgical techniques, freehand, CAS and CAS guide, in a distal femoral cadaver bone-tumour model.
Materials and methodsAn experimental study was performed. A distal femoral cadaver bone-tumour model

Enhancing precision and accuracy in bone tumour treatment
75
Enhancing precision and accuracy in bone tumour treatment
74
was chosen to accurately simulate a real procedure. Six Thiel-embalmed cadavers were used (15). The surgical plan was to resect a virtual tumour in the one femur and to reconstruct the defect with a graft resected from a matching femur.
High resolution, high sharpness (0.4 mm slices, 0.4 mm pixel size and B70 reconstruction) computer tomography (CT) scans were made before the experiment of all femora; scans were performed from mid-diaphysairy to the condyles. These scans were then compared using pre-operative planning software (OrthoMap 3D, Stryker Mahwah, NJ). Each distal femur was paired with its closest anatomical match on the same side in another cadaver. These pairs were randomised over the three treatment techniques, providing two procedures per technique. Three cadavers would undergo a simulated tumour resection on both sides and three cadavers would undergo the graft resection on both sides.
Using the preoperative planning software on a laptop computer a high grade sarcoma was simulated in each of the distal femoral sites in the three tumour resectionspecimens.Thetumourwas ‘created’ontheanteriorsideofthefemur.Each resection was planned as 80 mm long and to a maximum depth of 70% of the diameter of the bone. Figure 1 demonstrates the surgical plan. The end of the patellar groove was taken as the entry point of the distal resection. The resection planes (green) were then planned. The proximal resection plane was angled at 75 degrees and the distal plane at 55 degrees. As the aim was to resect this tumour with a margin of 10 mm, the tumour was placed 10 mm inside the planned resection planes. The simulation and planning was done the same way for each of the six resection sites.
For the creation of the grafts the planning software was used to correlate the resection site with the donor site. This was done by manually matching the two CT datasets and linking them, optimizing for coverage over the graft sites. As the datasets were linked all planes planned for the resection sites also become available on the allograft sites, resulting in an exact duplication of the resection surgical plan.
All procedures were performed by one experienced orthopaedic oncologic surgeon (PCJ).
Freehand procedure
ThefreehandprocedurewassupportedbyasimulationofafluoroscopeontheCASmachine(NavigationSystemII,StrykerMahwah,NJ)astherewasnofluoroscopeavailable in the lab setting. A composition of the CT volume and this tumour was made; both elements were adjusted to look like a radiograph. During the procedure the surgeon only saw the full screen anterior posterior or lateral view of the 3D composition(figure2).

6
Enhancing precision and accuracy in bone tumour treatment
75
Enhancing precision and accuracy in bone tumour treatment
74
Figure one (left): Overview of the surgical planning. The zone coloured red is the planned tumour. The green lines are the resection planes for the tumour resection, the blue lines are the planes for the graft resection.
Figure two (right): Compilation of two screenshots made in the fluoroscopy simulation view, corresponding to an AP view (A) and a lateral view (B). During surgery the pointer tool would be visible on screen in the view, similar to using radio-opaque tools during fluoroscopy to find anatomical structures.
Figure three: Identification of the intersection between the distal angulated plane and the longitudinal base plane. Both the host and allograft CT slices are visible on the three 2D views.
Enhancing precision and accuracy in bone tumour treatment
77
Enhancing precision and accuracy in bone tumour treatment
76
An extended medial knee-arthrotomy approach was performed and the patella was flippedlaterallytoexposethedistalfemur.AstandardCASset-upwasperformed,using landmark and surface matching, to provide simulated fluoroscopy. Theresection planes were marked on the bone, using a detailed surgical planning, arulerandsimulatedfluoroscopyshots. TheresectionwasdoneusingaCADIIoscillating saw (Compact Air Drive, Synthes, Welwyn Garden City, UK), using 0.6 mm thick blades. The surgeon then used the same method to create the reconstruction allograft, also using the en-bloc resected tumour as model for the allograft creation.
This allograft was then used to reconstruct the defect caused by the tumour resection. As in a real surgical situation minor changes to the shape and tumour resection site were made as required. The en-bloc tumour was placed in the defect causedbytheallograftresection,withoutmodificationsofeither,tobeexaminedlaterforsurgicalaccuracyonthepost-operativeCT.Bothwerefixatedusinga50mm titanium small fragment screw. The wound was then closed.
CAS procedure
As the navigated resection planes are in principle 2D planes they demarcate the exact edge of the required margin (i.e. 10 mm from the tumour). However the oscillating saw removes more than the thin line displayed, for the 0.6 mm blade this was minimally 0.8 mm due to the teeth size. As the surgeon aligns the saw exactly to the plane this has to be compensated so the resection does not compromise the margin. Thus the resection planes were moved 0.4 mm away from the tumour (the thickness of the saw blade at its teeth divided by 2). These planes were duplicated to provide the allograft resection planes and moved another 0.8 mm away for the graft tocompensateforthesawlossofthefirstresection.Thisisvisualisedinfigure1.
The same surgical approach was performed. CAS was set-up using landmark and surface matching on the resection CT volume. The tumour site resection planes were then located on the bone surface using the pointer tool and drawn on the bonesurfaceusingBonney’sblueink.Thecornersoftheresectionweremarkedandtheangulationoftheplaneschecked(figure3).Theresectionwasthenperformedfree-handed along these planes.
The planning was then switched to the allograft site and the CAS was set-up for the allograft providing bone. The resection planes, corrected for the saw thickness and the saw defect of the resection, were located on the bone surface, marked, and the graft was resected free-handed along these CAS determined planes. Angulation was checked intermittently using the pointer tool. For a more detailed description we refer to our previous paper (11).
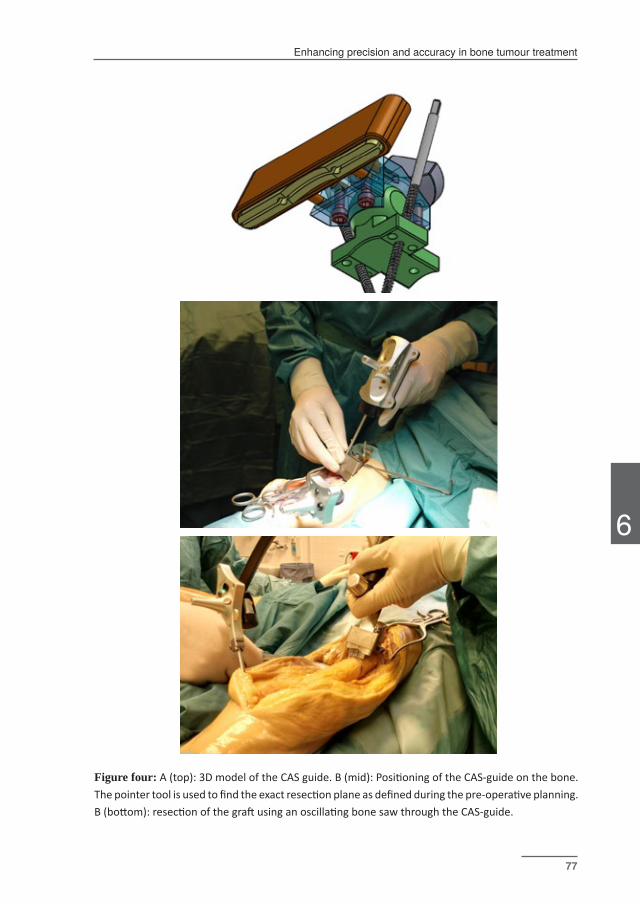
6
Enhancing precision and accuracy in bone tumour treatment
77
Enhancing precision and accuracy in bone tumour treatment
76
Figure four: A (top): 3D model of the CAS guide. B (mid): Positioning of the CAS-guide on the bone. The pointer tool is used to find the exact resection plane as defined during the pre-operative planning. B (bottom): resection of the graft using an oscillating bone saw through the CAS-guide.
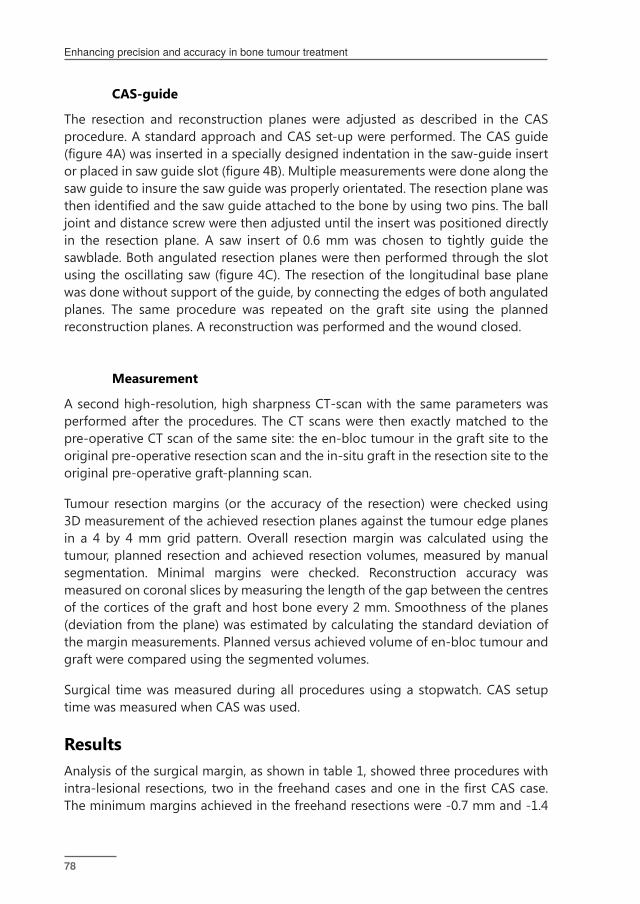
Enhancing precision and accuracy in bone tumour treatment
79
Enhancing precision and accuracy in bone tumour treatment
78
CAS-guide
The resection and reconstruction planes were adjusted as described in the CAS procedure. A standard approach and CAS set-up were performed. The CAS guide (figure4A)wasinsertedinaspeciallydesignedindentationinthesaw-guideinsertorplacedinsawguideslot(figure4B).Multiplemeasurementsweredonealongthesaw guide to insure the saw guide was properly orientated. The resection plane was thenidentifiedandthesawguideattachedtothebonebyusingtwopins.Theballjoint and distance screw were then adjusted until the insert was positioned directly in the resection plane. A saw insert of 0.6 mm was chosen to tightly guide the sawblade. Both angulated resection planes were then performed through the slot usingtheoscillatingsaw(figure4C).Theresectionofthelongitudinalbaseplanewas done without support of the guide, by connecting the edges of both angulated planes. The same procedure was repeated on the graft site using the planned reconstruction planes. A reconstruction was performed and the wound closed.
Measurement
A second high-resolution, high sharpness CT-scan with the same parameters was performed after the procedures. The CT scans were then exactly matched to the pre-operative CT scan of the same site: the en-bloc tumour in the graft site to the original pre-operative resection scan and the in-situ graft in the resection site to the original pre-operative graft-planning scan.
Tumour resection margins (or the accuracy of the resection) were checked using 3D measurement of the achieved resection planes against the tumour edge planes in a 4 by 4 mm grid pattern. Overall resection margin was calculated using the tumour, planned resection and achieved resection volumes, measured by manual segmentation. Minimal margins were checked. Reconstruction accuracy was measured on coronal slices by measuring the length of the gap between the centres of the cortices of the graft and host bone every 2 mm. Smoothness of the planes (deviation from the plane) was estimated by calculating the standard deviation of the margin measurements. Planned versus achieved volume of en-bloc tumour and graft were compared using the segmented volumes.
Surgical time was measured during all procedures using a stopwatch. CAS setup time was measured when CAS was used.
ResultsAnalysis of the surgical margin, as shown in table 1, showed three procedures with intra-lesionalresections,twointhefreehandcasesandoneinthefirstCAScase.The minimum margins achieved in the freehand resections were -0.7 mm and -1.4

6
Enhancing precision and accuracy in bone tumour treatment
79
Enhancing precision and accuracy in bone tumour treatment
78
mm, and -1.2 in the CAS case. Negative margins were found in the base plane (3), proximal (1) and distal plane (1)
Resection accuracy was measured as the deviation from the planned plane and overall largest in the freehand procedures (6.1 and 4.0 mm) and smallest in the two CASguideprocedures(3.0and1.2mm).Thelargedeviationof7.3mminthefirstCASprocedure was unexpected. Another approach of calculation of accuracy by volume, as shown in table 2, showed an overall margin (optimally 10 mm) ranging from 4.0 mm (freehand) to 9.0 mm (CAS guide). Volume measurement also demonstrated that all removed en-bloc tumours were undersized. Some were severely undersized; themost extremewas first freehand procedurewith an en-bloc tumour of only65% of expected volume. Smoothness of the planes also differed with the standard deviation ranging from 2.4 and 2.6 mm in the freehand procedures to 0.9 and 0.8 in the CAS guided procedures.
The accuracy of the planes, in rotation and angulation was low in the freehand procedure groups. In one procedure an angulation error of 28.6 degrees was found compared to the planned planed. Achieved rotation and angulation was very accurate in the second CAS procedure and the two guided procedures, with some planes having below 1 degree errors.
The reconstruction gap was small in all procedures, with the lowest in the CAS and CASguideprocedures. The smoothness of the fit, asmeasuredby the standarddeviation, was high in all the procedures. Achieved graft volume compared to the planned graft volume, as seen in table 2, was lowest in the freehand group (45% and 68%) and highest in the CAS-guide procedures (76% and 99%).
Surgical time was much faster in the freehand procedures, with the CAS guide procedures 30 minutes longer than the freehand procedures. CAS setup time was on average 4 minutes and 24 seconds (range 2:49 – 7:50), as measured over ten set-ups. There were no observed CAS inaccuracies during the procedures. There were no intra-operative complications like host bone fractures.
DiscussionThe result of this experiment underlines the observation that these types of multi-planar resections are very demanding. None of the six resections, even with imaging support, achieved the exact required margin. All resections resulted in cuts that were too conservative, i.e. cuts with less than 10 mm margin surrounding the tumour. Three procedures even had a local error of over 10 mm, resulting in intra-lesional resections. While the optimum result was not achieved, a clear trend in resection and reconstruction accuracy is visible in the results.

Enhancing precision and accuracy in bone tumour treatment
81
Enhancing precision and accuracy in bone tumour treatment
80
The clinical results and the accuracy of the freehand procedures were unacceptable. Two out of two procedures had an intralesional resection. Deviation was on average 5.1 mm and the planes had large deviations both in rotation as in angulation. Both freehand procedures also had an undersized en-bloc tumour of almost a third comparedto theplannedsize.Thereconstructionwasa reasonablefithoweverthis was achieved by adjusting the graft, resulting in an undersized reconstruction with 55% and 32% of the planned volume missing. This would have impacted graft strength and very likely the crucial graft/host contact area. Based on these results the freehand technique is not accurate enough for this type of multiplanar resections.
CAS had an unexpected intra-lesional resection in the first procedure, with anacceptable result in the second procedure. Analysis of the images showed that the most likely cause of this inaccuracy was a shift in the matching to proximal of almost 6 mm. During every set-up there was an accuracy check on the bone surfacethatshowedagoodmatch.It’spossiblethatnotenoughpointswereusedinathree-dimensionalconfiguration,resultinginagoodmatchofthecylindricalshape of the bone but not a good match in the absolute position. Interestingly is the result of the associated graft procedure (with its own setup), this was highly accurate,withanachievedvolumeof90%.Thefirstguideprocedurealsoshoweda possible shift, albeit a much smaller one (1-2 mm). This was also not noticed during the experiment. Comparing CAS to freehand the deviation, smoothness and accuracy of plane placement were better. There was less loss of bone for both the en-bloc tumour and graft. Reconstruction accuracy was high with good achieved graft volumes.
The best results, both in the absolute deviation as in the reconstruction, were achieved in the CAS-guide procedures. Especially the second procedure demonstratedanearoptimalresult(figure5).Theminimallyachievedmargininboth the guide procedures and the CAS procedure was the result of a point like defect in the saw cut. After studying the video this was probably the result of either saw blade vibration (a window wiper like defect) or a defect caused by the motion osteotome as the tumour was en-bloc removed from the host bone. Both these defects should be preventable. Achieved volume, overall margin and achieved graft volume were excellent. The reconstruction gap was small. The CAS-guide results, both clinical and measured, were better than the results achieved in the CAS and freehand procedure.
Comparing the results to descriptions of CAS use in literature, our results show a slightly higher deviation (3.6 mm, standard deviation of 2.3 mm). CAS-guided procedures were overall slightly better (2.1 mm, standard deviation of 1.5 mm). Ritacco et al describe resection accuracy using CAS in 61 osteotomy planes of 2.52 mm with a standard deviation of 2.32 mm (14). This report also shows
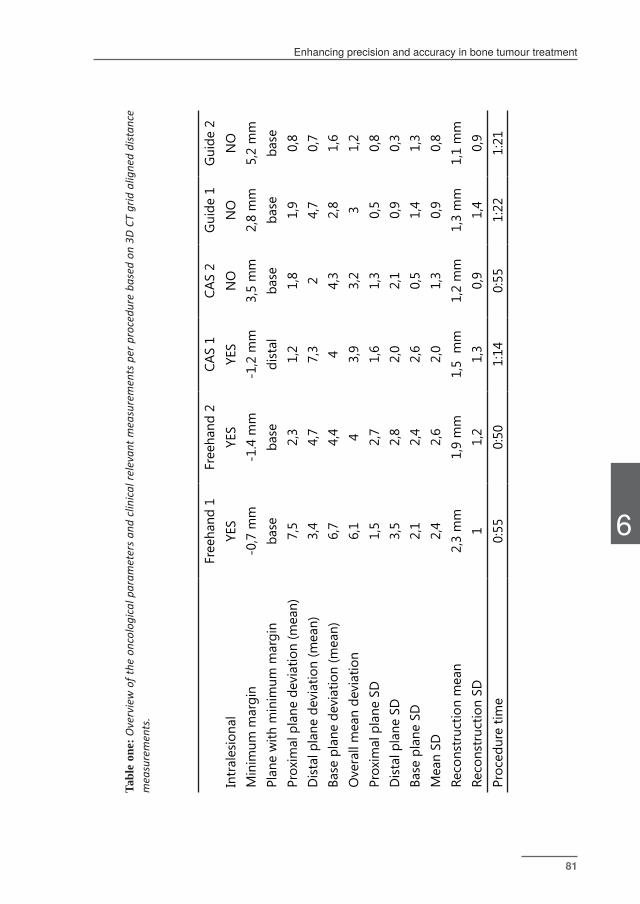
6
Enhancing precision and accuracy in bone tumour treatment
81
Enhancing precision and accuracy in bone tumour treatment
80
Fr
eeha
nd 1
Free
hand
2CA
S 1
CAS
2G
uide
1G
uide
2In
tral
esio
nal
YES
YES
YES
NO
NO
NO
Min
imum
mar
gin
-0,7
mm
-1.4
mm
-1,2
mm
3,5
mm
2,8
mm
5,2
mm
Plan
e w
ith m
inim
um m
argi
nba
seba
sedi
stal
ba
seba
seba
sePr
oxim
al p
lane
dev
iatio
n (m
ean)
7,5
2,3
1,2
1,8
1,9
0,8
Dis
tal p
lane
dev
iatio
n (m
ean)
3,4
4,7
7,3
24,
70,
7Ba
se p
lane
dev
iatio
n (m
ean)
6,7
4,4
44,
32,
81,
6O
vera
ll m
ean
devi
atio
n6,
14
3,9
3,2
31,
2Pr
oxim
al p
lane
SD
1,5
2,7
1,6
1,3
0,5
0,8
Dis
tal p
lane
SD
3,5
2,8
2,0
2,1
0,9
0,3
Base
pla
ne S
D2,
12,
42,
60,
51,
41,
3M
ean
SD2,
42,
62,
01,
30,
90,
8Re
cons
truc
tion
mea
n2,
3 m
m1,
9 m
m1,
5 m
m1,
2 m
m1,
3 m
m1,
1 m
mRe
cons
truc
tion
SD1
1,2
1,3
0,9
1,4
0,9
Proc
edur
e tim
e0:
550:
501:
140:
551:
221:
21
Tabl
e on
e: O
verv
iew
of t
he o
ncol
ogic
al p
aram
eter
s an
d cl
inic
al re
leva
nt m
easu
rem
ents
per
pro
cedu
re b
ased
on
3D C
T gr
id a
ligne
d di
stan
ce
mea
sure
men
ts.
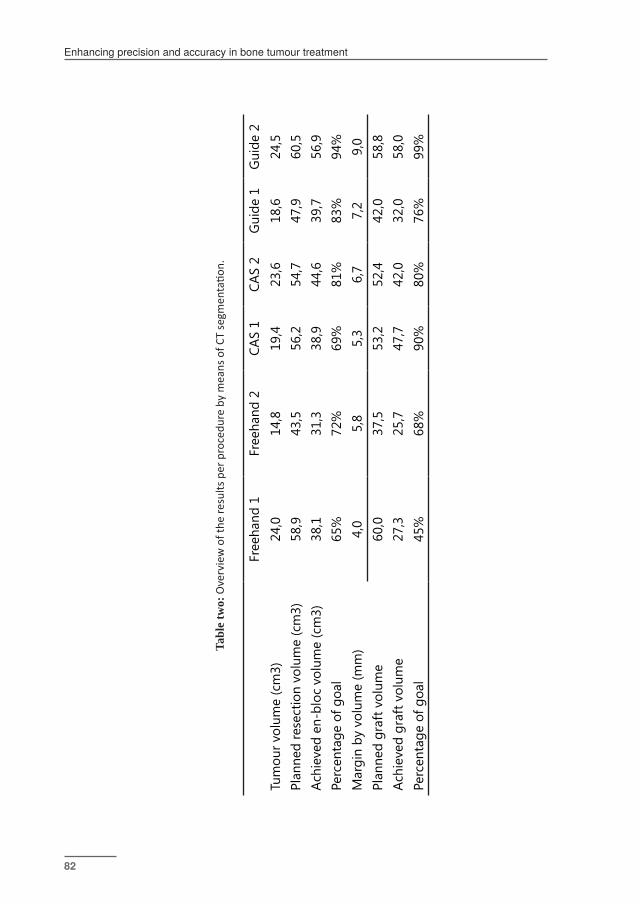
Enhancing precision and accuracy in bone tumour treatment
83
Enhancing precision and accuracy in bone tumour treatment
82
Tabl
e tw
o: O
verv
iew
of t
he re
sults
per
pro
cedu
re b
y m
eans
of C
T se
gmen
tatio
n.
Fr
eeha
nd 1
Free
hand
2CA
S 1
CAS
2G
uide
1G
uide
2Tu
mou
r vol
ume
(cm
3)24
,014
,819
,423
,618
,624
,5Pl
anne
d re
sect
ion
volu
me
(cm
3)58
,943
,556
,254
,747
,960
,5Ac
hiev
ed e
n-bl
oc v
olum
e (c
m3)
38,1
31,3
38,9
44,6
39,7
56,9
Perc
enta
ge o
f goa
l65
%72
%69
%81
%83
%94
%M
argi
n by
vol
ume
(mm
)4,
05,
85,
36,
77,
29,
0Pl
anne
d gr
aft v
olum
e60
,037
,553
,252
,442
,058
,8Ac
hiev
ed g
raft
vol
ume
27,3
25,7
47,7
42,0
32,0
58,0
Perc
enta
ge o
f goa
l45
%68
%90
%80
%76
%99
%
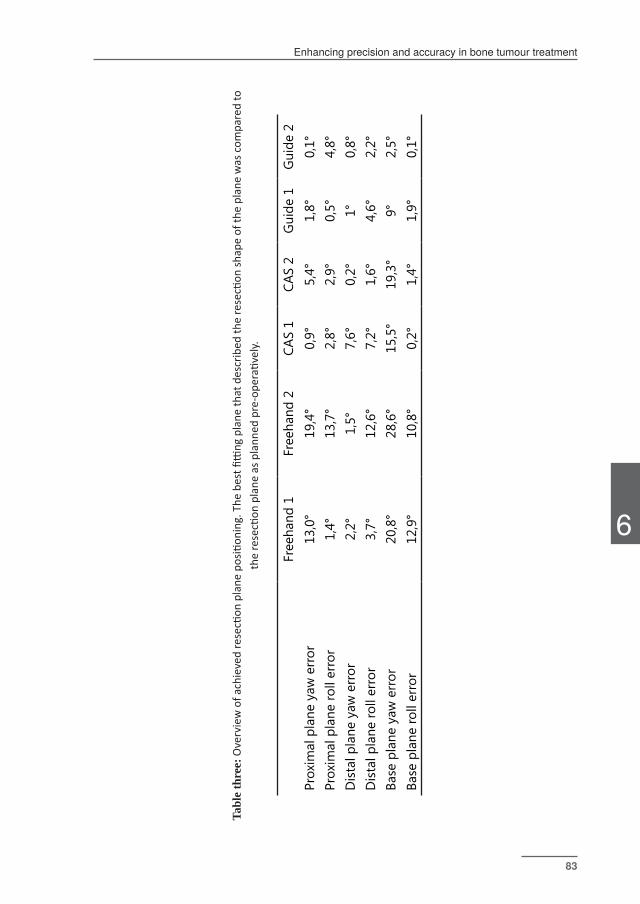
6
Enhancing precision and accuracy in bone tumour treatment
83
Enhancing precision and accuracy in bone tumour treatment
82
Tabl
e th
ree:
Ove
rvie
w o
f ach
ieve
d re
secti
on p
lane
pos
ition
ing.
The
bes
t fitti
ng p
lane
that
des
crib
ed th
e re
secti
on sh
ape
of th
e pl
ane
was
com
pare
d to
th
e re
secti
on p
lane
as p
lann
ed p
re-o
pera
tivel
y.
Fr
eeha
nd 1
Free
hand
2CA
S 1
CAS
2G
uide
1G
uide
2Pr
oxim
al p
lane
yaw
err
or13
,0°
19,4
°0,
9°5,
4°1,
8°0,
1°Pr
oxim
al p
lane
roll
erro
r1,
4°13
,7°
2,8°
2,9°
0,5°
4,8°
Dis
tal p
lane
yaw
err
or2,
2°1,
5°7,
6°0,
2°1°
0,8°
Dis
tal p
lane
roll
erro
r3,
7°12
,6°
7,2°
1,6°
4,6°
2,2°
Base
pla
ne y
aw e
rror
20,8
°28
,6°
15,5
°19
,3°
9°2,
5°Ba
se p
lane
roll
erro
r12
,9°
10,8
°0,
2°1,
4°1,
9°0,
1°

Enhancing precision and accuracy in bone tumour treatment
85
Enhancing precision and accuracy in bone tumour treatment
84
some resections with very large deviations. In an experimental setting on pelvic sawbones Cartiaux et al. demonstrated deviations of “1 and 1.2 mm in the anterior and posterior ilium, 2 mm in the pubis and 3.7 mm in the ischium” using patient specificinstrumentationand6.5mminCASassistedresections(16,17).Sternheim et al demonstrated significantly more accurate cuts in CAS than freehand in sawbones and deviation of entry and exit point of planes in cadavers of 1.5 ± 0.9 mm and 2.1 ± 1.5 mm. Fehlberg et al described a 3.3 mm median deviation (18) Gouin et al showedanaccuracyof2.5mminastudyofpelvicresectionsusingpatientspecificinstrumentation (16).
An interesting observation is that all of the procedures had undersized results. This is a problem that we also observed in the operating theatre. It seems that out of a possible fear of a fracture the margin is compromised, against rational reasoning. The main culprit in volume reduction in this study was the shift and rotation along the axis of the bottom planes. Seen on a transverse view the plane also often resembles a tent shape, with more accurate margins near the edge and a top in the margin. Often the real resection plane is much closer to a 90 degree angle than the planned plane, possibly as this is an easier angle of entry for the oscillating saw. Awareness of this can possibly prevent these errors.
Use of the guide was easy but required extra surgical time, around 20 minutes for thefourguideset-ups.Asthiswasthefirsttimetheguidewasused,theproceduretime will likely decrease in further procedures. During the procedure there were a few moments were the guide needed a second check and sometimes re-orientation because of rotation due to the power oscillating saw. The size of the guide can be further optimised as one cut required enlarging the exposure on the bone for the guidetofit.Anavigationalsystemthatsupportstrackinga3Dfigure,forexamplethe edge of an osteotome, instead of a 2D line / point based approach would greatly reduce the set-up time. The experience of this experiment will be incorporated in an improveddesign(figure6).
Techniques that assist in resection, objective action instead of objective orientation, exist.Patientspecificguides(PSG)offerobjectiveresectionsupportandasdescribedabove have been shown to deliver accurate results. However they rely on non-uniform bone topography, have their own inaccuracies and do not provide direct orientation feedback or accuracy checks. Currently they still carry a high extra cost per procedures and their creation is still time consuming. Robotics is most likely the future modality to turn to for both objective orientation and action. However as demonstrated in this study, the current CAS technique accuracy and precision can beimprovedfurtherwithCASspecifictools,forexampletheuniversalsawguidelikethe one developed for this study.
CAS and especially the CAS-guide procedures have demonstrated highly accurate

6
Enhancing precision and accuracy in bone tumour treatment
85
Enhancing precision and accuracy in bone tumour treatment
84
resections and reconstructions. Compared to freehand there was improvement in clinical results, measured margin, plane placement, gap and volume of en-bloc tumour and graft. CAS guide is a tool that can be used to enhance the actually achieved accuracy closer to the real (orientational) accuracy of the CAS system. The freehand technique demonstrated a large deviation of the planned planes and unacceptable clinical results with two out of two procedures having an intra-lesional cut. Possible CAS matching errors resulted in one other intralesional resection. Better and more careful checks are needed to prevent this type of error. The CAS guide can be applied to more types of procedures. With a modular design it can assist in pelvic resections, wedge osteotomies or any other type of resection. It can be a potentialsuperioralternativetopatientspecificguidesforassistanceinresections.TheadditionoftheCASguidemadeitpossibletofindtheexactplaneaswellasactually achieve the exact planned cuts.
The saw guide will be released under an open-source license.
Figure five: 3D rendered image made from the post-reconstruction scan of the second CAS-guide procedure. Made with iNtution (TeraRecon).

Enhancing precision and accuracy in bone tumour treatment
87
Enhancing precision and accuracy in bone tumour treatment
86
References(1) Campanacci M, Capanna R, Stilli S. Posterior hemiresection of the distal femur
in parosteal osteosarcoma. Ital J Orthop Traumatol 1982 Mar;8(1):23-28.
(2) Deijkers RL, Bloem RM, Hogendoorn PC, Verlaan JJ, Kroon HM, Taminiau AH. Hemicortical allograft reconstruction after resection of low-grade malig-nant bone tumours. J Bone Joint Surg Br 2002 Sep;84(7):1009-1014.
(3) Pezzillo F, Maccauro G, Nizegorodcew T, Rossi B, Gosheger G. Resection of parosteal osteosarcoma of the distal part of the femur: an original recon-struction technique with cement and plate. Sarcoma 2008;2008:763056.
(4) Lewis VO, Gebhardt MC, Springfield DS. Parosteal osteosarcoma of the pos-terior aspect of the distal part of the femur. Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000 Aug;82-A(8):1083-1088.
(5) Agarwal M, Puri A, Anchan C, Shah M, Jambhekar N. Hemicortical excision for low-grade selected surface sarcomas of bone. Clin Orthop Relat Res 2007 Jun;459:161-166.
(6) Aponte-Tinao LA, Ritacco LE, Ayerza MA, Muscolo DL, Farfalli GL. Multiplanar osteotomies guided by navigation in chondrosarcoma of the knee. Ortho-pedics 2013 Mar;36(3):e325-30.
(7) Aponte-Tinao LA, Ritacco LE, Albergo JI, Ayerza MA, Muscolo DL, Farfalli GL. The principles and applications of fresh frozen Allografts to bone and joint reconstruction. Orthop Clin North Am 2014;45(2):257-269.
(8) Cho HS, Oh JH, Han I, Kim HS. The outcomes of navigation-assisted bone tu-mour surgery: minimum three-year follow-up. J Bone Joint Surg Br 2012 Oct;94(10):1414-1420.
(9) Wong K, Kumta S. Use of computer navigation in orthopedic oncology. Current surgery reports 2014;2(4):1-8.
(10) Gerbers JG, Stevens M, Ploegmakers JJ, Bulstra SK, Jutte PC. Computer-assist-ed surgery in orthopedic oncology: Technique, indications, and a descrip-tive study of 130 cases. Acta orthopaedica 2014;85(6):1-7.
(11) Gerbers JG, Ooijen PMV, Jutte PC. Computer-assisted surgery for allograft shaping in hemicortical resection: A technical note involving 4 cases. Acta orthopaedica 2013;84(2):1-3.
(12) Aponte-Tinao LA, Ritacco LE, Albergo JI, Ayerza MA, Muscolo DL, Farfalli GL. The principles and applications of fresh frozen Allografts to bone and joint reconstruction. Orthop Clin North Am 2014;45(2):257-269.

6
Enhancing precision and accuracy in bone tumour treatment
87
Enhancing precision and accuracy in bone tumour treatment
86
(13) Docquier PL, Paul L, Cartiaux O, Delloye C, Banse X. Computer-assisted resection and reconstruction of pelvic tumor sarcoma. Sarcoma 2010;2010:125162.
(14) Ritacco LE, Milano FE, Farfalli GL, Ayerza MA, Muscolo DL, Aponte-Tinao LA. Accuracy of 3-D planning and navigation in bone tumor resection. Orthope-dics 2013 Jul;36(7):e942-50.
(15) Thiel W. The preservation of the whole corpse with natural color. Ann Anat 1992 Jun;174(3):185-195.
(16) Cartiaux O, Banse X, Paul L, Francq BG, Aubin C, Docquier P. Computer-assisted planning and navigation improves cutting accuracy during simulated bone tumor surgery of the pelvis. Computer Aided Surgery 2013;18(1-2):19-26.
(17) Cartiaux O, Paul L, Francq BG, Banse X, Docquier P. Improved accuracy with 3D planning and patient-specific instruments during simulated pelvic bone tumor surgery. Ann Biomed Eng 2014;42(1):205-213.
(18) Fehlberg S, Eulenstein S, Lange T, Andreou D, Tunn P. Computer-assisted pelvic tumor resection: fields of application, limits, and perspectives. Treatment of Bone and Soft Tissue Sarcomas: Springer; 2009. p. 169-182.
(19) Gouin F, Paul L, Odri GA, Cartiaux O. Computer-Assisted Planning and Pa-tient-Specific Instruments for Bone Tumor Resection within the Pelvis: A Series of 11 Patients. Sarcoma 2014;2014.

General discussion and future perspectives

General discussion and future perspectives
91
General discussion and future perspectives
90

7
General discussion and future perspectives
91
General discussion and future perspectives
90
General discussion and future perspectives
The aim of this thesis was to investigate the value of the use of CAS in orthopaedic oncology, either directly measured in accuracy or in clinical results. The question is also proposed as to whether CAS-based objective orientation could result in improved or new surgical procedures. As the use of CAS has consisted of a wide rangeofdiagnosesandprocedures,thefirstpartofthediscussiondealswithdirectclinical use, indications and reports in the literature, and will be broken down into the four basic techniques as described in Chapter Two. The core of the discussion will deal with the technique, offering observations on current system accuracy, system use, evaluation of the current tools and the trend of CAS use in orthopaedic surgery and orthopaedic oncology. The last part of the discussion will analyse current CAS use,describecurrentissueswithCASworkflow,listitsbenefitsandprovidefutureperspectives.
Clinical use
Intralesional treatment
The largest number of clinical procedures reported in this thesis dealt with the intralesional treatment of benign, low-grade and intermediate-grade bone tumours. AsChapterFourhasdiscussedspecifically foratypicalchondroidtumours (ACT)/chondrosarcoma grade 1 (CHS1) and Chapter Two generally for multiple diagnoses, CASisatechnologicallysuperioralternativetostandardfluoroscopy.Intralesionaltreatment, sometimes supported with adjuvants, is also the standard treatment for someofthemostcommonorthopaediconcologylesions.Surprisingly,thescientificliterature reports little about CAS use in intralesional treatments.
Leeetal.described in2012 thatcomputer-guidedcurettage isbeneficial for thetreatmentof‘deeplyseatedormulti-cystic’lesionsorbenignbonetumourscloseto the cartilage (1). They used image fusion as a tool to observe the effect of the procedures and declared the technique safe if the ‘thickness of subchondral bone’wasgreaterthan3mm.Theauthorsalsodescribedthelackofamethodtodelineate progression, possibly resulting in over-curettage. Wong et al. described the use of CAS to assist in the endoscopic removal of six benign bone tumours, offering a minimally invasive approach (NEAT) (2). Somewhat related are the multiple descriptions of the use of CAS, in combination with high-speed burrs, to treat osteoid osteomas in the spine and the long bones (3). An Italian group even described the successful use of a combination of CAS and video-assisted surgery
General discussion and future perspectives
93
General discussion and future perspectives
92
(VATS) for the treatment of an osteoid osteoma in the spine (4). All these publications were case reports or small series.
While the newWorldHealthOrganisation (WHO) classification has downgradedthe low-grade malignant diagnosis CHS-1 to the intermediate ACT, underpinning the need for more watchful waiting, treatment for active or larger lesions is still required.AsLeeetal.havestated,there isalsobenefit inapplyingCAStootherlesions, either for locally aggressive lesions (giant cell tumours) or in anatomically difficult locationsasthefemoralneckandhead.Moreover, itcanbearadiation-free,technologicallysuperioralternativeto2Dfluoroscopyforstandardcurettageprocedures.
Chapter Five is the only comparative study in the literature using CAS for the curettage of bone tumours. The study is also one of the larger published series on the treatment of ACT/CHS-1. It underlines not only the need for accuracy in the procedurebutalsointhemeasurementanddefinitionofthepostoperativeresult.Even before specific procedure-focused applications, CAS curettagewas at leastclinicallyequivalenttofluoroscopyuseinACTtreatmentwithoutrelyingonionisingradiation. CAS curettage takes equally as long and may potentially be even faster thanfluoroscopy-basedcurettage.ArguablyCAScurettage,asdiscussedinChapterTwo,isbetterindifficultanatomicalpositions,forexamplefibrousdysplasiaofthefemoral head or pelvis.
Other benefits are likely to be identified in the future for accurate intralesionaltreatment resulting in an exactly known size of the defect. Finite-element analysis, for example, can be used to select the best place to create a bone window, optimal reconstruction material, and positioning and type of prophylactic plating (5). As described in this study, the use of CAS could decrease the associated fracture risk. Neither the software nor the hardware are yet specialised for the task of highly accurate curettage though. As the surgeon receives no feedback on progression, there still is a potential for over-curettage with an increased risk of fracture, or under-curettage and thus recurrence.
The need to attach trackers to standard curettes introduces a source of inaccuracy astheattachmentmaybecomeinstable,reducingthepotentialbenefitoftheCASsystem. Furthermore, as current systems display instruments as 2D lines, the actual spatialorientationofthetoolisnotvisible.Thisalsomakesitdifficulttoworkwithasymmetrical tools that can enable full curettage through smaller bone windows. With smart tools, aware of their own orientation, percutaneous treatment such as a NEAT-type procedure without the endoscope and with progress tracking becomes an attractive possibility.
An alternative for CT-based CAS procedures as presented in Chapters Two and Four isvirtualfluoroscopy (C-arm-basedcomputer-assistedsurgery) (6).This isa
7
General discussion and future perspectives
93
General discussion and future perspectives
92
hybrid technology that uses CAS and an isometric c-arm-type scanner to track the lesions and the instruments, with automated image acquisition and matching. CT-based CAS systems are often capable of doing both modes, also allowing image fusion (CT/MRI, etc.) on the acquired image. The main advantage is the ability to check the progress of the procedure. The image quality of this type of imaging systems however is not as high as that of standalone CT-scanners (7). Furthermore, as preoperative scans are often already required during the diagnostic process, the radiation dose to the patient is higher. These two techniques on spatial accuracy for curettages have not yet been compared.
Another new alternative technology for the percutaneous treatment of small lesions is radiofrequency ablation (RFA). This technique depends on accurate positioning of the RFA needles and heating of the tissue around the tip of the needle. CT guidance is often used for the placement, yet the technique can be combined with a navigation system to improve positioning accuracy (8). This increase in positioning accuracy togetherwithmodelsofheat-flowcouldleadtoaccuratemulti-pointtreatmentoflarger lesions.
There are not enough data available for a definitive conclusion on CAS as analternative to fluoroscopy. The use of CAS however is ionising radiation-free,accurate in three dimensions and oncologically safe, and has promising future applications, possibly in conjunction with other innovative techniques. Better scientificreportingisneededtodiscernbetweenresidueandrecurrencecases,andto enable comparison of surgical techniques.
Image-based resections
Chapters Two and Three discuss the application of image-based CAS on osteotomies.
Pelvis & sacrum
Pelvic and sacral osteotomies are by far the most studied procedures within the CASfield.This iswithreason,asthetreatmentofdeep-seated,oftenhigh-gradelesions in an anatomically complex region is regarded as extremely demanding. There is ongoing development in chemotherapy for Ewing sarcoma, high-grade chondrosarcoma and osteosarcoma, yet radical surgical treatment of a solitary sarcoma remains critical (9-11). Reports in the literature show a relatively high rate of inadequate (intralesional or smaller than required) margins (12-14). Inadequate pelvicandsacralmarginsinhigh-gradesarcomawereassociatedwithsignificantlyworse clinical outcome and local recurrence (15, 16). Primary pelvic bone tumours overallwereevenassociatedwithsignificantlyworseclinicalresultsthanthoseinthelimbs (17). Experimental research has shown the potential inaccuracy of freehand resection in the pelvis (18). As overviews of CAS use have argued, there is a possible

General discussion and future perspectives
95
General discussion and future perspectives
94
benefittotheadditionalaccuracyofCASuse(19,20).
Thefirstnavigatedpelvicandsacralresectionsweredescribedin2004byHüfneret al. for two cases and by Krettek et al. for one periacetabular sarcoma (21,22). All three were successful. Reijnders et al. reported the radical resection of two high-gradesarcomas(23).Soetal.describedsurgicalworkflowwithCASandreportedtwo successful pelvic procedures with an average deviation of planes of 6 mm over three planes, as part of a larger case series (24). Wong et al. described the use of CT/MRIfusiontoimproveplanningandidentificationofmargins(25).Thesamegrouphas published papers on the successful use of integration of computer-aided design (CAD) planning and custom prosthesis use for reconstruction (20, 26). Docquier et al. reported using CAS for both a successful resection and allograft reconstruction (27).
In recent years larger case series with longer-term follow-up have been published. Cho et al. published about seven pelvic and sacral resections, part of a larger study of 18 patients. Clear margins were achieved in all resections; there were two local recurrences in the pelvis at a minimum follow-up of three years (25). Wong et al. achievedwideresectionmarginsin16casesandmarginalresectionsinfive,inastudythat included 12 pelvic and sacral resections on a total of 21 cases. Local recurrences were found at a mean follow-up of 39 months in four cases that had had marginal resection; three of these were in the sacral region (20). Young et al. described eight CAS-assisted pelvic sarcoma resections, all with clear margins, and eight planned planes within 5 mm of the planning and one with a 5-mm deviation due to surgeon planning errors. All patients were alive and recurrence-free at a mean follow-up of 25 months (28). Jeys et al. has published the largest case series on pelvic resections, a study of 31 patients (17). A clear resection margin was achieved in the bone in all cases; overall intralesional resection rate was 8.7%. At a follow-up of 13.1 months, four patients had a local recurrence. Chapter Two presents similar results. Out of 17 pelvic resections, 15 had clear margins (R0 resection) with one intralesional R2 resection in bone and one R1 soft-tissue margin. There were three recurrences.
The indication of CAS for pelvic and sacral resections, while not tested in a direct randomised controlled trial, seems clear. Out of a total of 91 reported procedures in the literature there was only one intralesional resection in bone reported (1%) and fiveintotal(5%)ifsofttissuemarginswerecounted,inawidecasemixincludinglesions of all grades. The only occurrence of an intralesional resection in bone was inourcaseseries.Asdiscussedinthatpaper,adirectcausewasnotidentified.Whilethere is a possible bias, given that only early adopters with positive CAS experience are likely to publish case reports, these results are very good. Large overview papers on pelvic resections have reported intralesional resection rates, unknown if in bone or soft tissue, of at least 26% (Ozaki et al.) and 29% (Jeys et al.) (15, 29). Fuchs et al. reported inadequate margins in 13 of 40 cases, or 33% (30). No papers reporting
7
General discussion and future perspectives
95
General discussion and future perspectives
94
cohorts have yet drawn conclusions on oncological parameters because of the lengthof follow-up.Wongetal.madeafirst careful conclusion ina review thatresults at early intervals may be better than comparative studies (20). It is however likely, considering the higher number of radical resections and the risk of recurrence in non-radical resections, that future reports will show clinical improvements.
Long bones
Another well-studied CAS application is in multiplanar, often joint-salvage procedures around the joints of the long bones. Great precision and accuracy is required as there tends to be little room for error in the tight planning. The great advantages of joint salvage, with either reconstruction with custom tumour prostheses or grafts, are better proprioception and joint function (31). The multiplanar resection technique – saving part of the longitudinal continuity of the bone – is seen as a safe alternative tosegmentalresectionandmodularprostheticreconstruction,butisalsodifficultto perform, as argued in Chapters Two, Five and Six.
Cho et al. describe seven patients eligible for joint-salvage surgery (criteria at least 1 cm of epiphysis outside the margin) with lesions in the metaphysis. These were all reconstructed with an allograft and were disease-free at a minimum of three years follow-up (25). According to the authors, the use of MRI datasets was vital to delineate the tumour and achieve accurate results. Kim et al. very thoroughly describe one successful case using MRI guidance, resorbable pin-based matching, a novel matching instrument and an osteoarticular graft (32).
Wong et al. describe eight joint-salvage resections in the long bones. All resections had free margins and deviation was less than 2 mm between planned and achieved planes as measured on the CAS system (31). Most defects were reconstructed using custom-made prostheses in their series. The 3D models were then imported back intotheCASsystemasDICOMfilesandusedtoplanthescrewfixation.Aponte-Tinaoetal.usedCASforfivepatientswithchondrosarcomaaroundtheknee(33).All margins were clear and accuracy between planned and achieved planes was 2.43 mm. Young et al. describe eight successful resections in the long bones with clear margins (28). So et al. report 11 successful procedures, most with prosthetic reconstructions. Planned versus achieved deviation was 6.8 mm in point-based/surfacematchingmode(somedifficulties)and2mminCT-fluoromatchingmode(24).
Li et al. reported in 2014 on joint-salvage procedures in nine paediatric patients with juxta-articular bone sarcomas, mainly in the femur (34). They describe that CAS with CT/MRI image fusion resulted in ‘… an ideal margin as well as preserving the entireorpartofthearticularsurface’,furthermore‘intra-articularandperiarticularstructures … were spared’. The conclusion calls for ‘computer-assisted allografttrimmingtechniques’forpreciseshapingoftheallograft.Finally,Aponte-Tinaoet

General discussion and future perspectives
97
General discussion and future perspectives
96
al. subsequently reported a massive case series on 66 procedures (likely including thefirstfivecases)(35).All66caseshadclearmargins.
Again, there are a high number of radical resections reported, 98 out of 98 cases in the literature. Chapter Two reports 26 resections, mainly of low-grade or benign lesions, and five high-grade lesions for resection and reconstruction. There wasone R1 resection, in a chondrosarcoma grade 1B, out of these 31 procedures. We described the only non-radical resection reported in the literature, with no direct causefound.Overall,thesurgicalresultsforthesedifficultresectionsareimpressive,highlighting the accuracy that CAS adds to this type of demanding surgery.
CAS osteotomies for non-high grade lesions
Chapter Two reported on the use of CAS for the resection of non-malignant tumours such as osteochondroma. There are no reports of this in literature. It is possible to argue that the potential benefits do not outweigh the pre-planningand set-up time costs. However, as argued in Chapter Two, these cases provide excellent possibilities to improve understanding and experience with the system aswellasgainexperienceinworkflow.Identificationoftheplaneswasquickandeasy, especially when the osteochondroma was located in an anatomically complex region like the posterior side of the distal femur, the pelvis, or between the tibia and fibula.Withenoughpractice,planningcouldgenerallybedonebetweenpatientswitches during anaesthesiological prepping. Set-up time had dropped on average to 6:30 minutes – time that was likely recouped in the procedure as shown for the curettages (Chapter Four).
Given this pelvis and long bone surgical outcome data, the conclusion that there is an absolute added value for CAS in highly complex cases is an obvious one. The experience from our centre, however, is that one should also learn to work with the system,adapttoitsworkflow,andlearntotrustthefeedback.IfoneonlyreservesCASforthesehighlycomplexcases,fullbenefitsfromtheaddedvaluewillnotbereapedandaCASsetupwill takeup toomuch time.Besides, it isn’tpossible tooperate CAS reliably and reproducibly if it is only used on an occasional basis.
Additional effect of increased accuracy
As seen in Chapter Three, the application of navigation hasmore benefits thanonly a lower intralesional resection rate. Navigation allowed for more a complex, salvagingsurgicalplan,fittinginwiththetrendoflimbsalvagesurgery.Jeysetal.described that ‘in several cases navigation allowed more complex surgical resections andreconstructions[...]than[...]possibleusingtraditionalmethods’(17).Thishasresulted in the sparing of critical structures such as nerve roots and the avoidance of amputations, the ability to operate otherwise inoperable tumours, and more functional reconstructions. Other authors described similar views (20, 32, 35).

7
General discussion and future perspectives
97
General discussion and future perspectives
96
This thesis offers additional support for that conclusion, as CAS can be used for complex salvaging procedures that are otherwise impossible, adding to the list of critical structures that otherwise could not be spared. Pathologic analysis showed excellent results with a very high number of non-intralesional resections. More follow-up is needed to assess long-term oncological follow-up, but the initial results are promising.
Image-based resections and reconstructions
Grafts are an option for reconstruction after joint salvage procedures, pelvic resections or other large bone defects. The benefits and indications of thehemicortical technique were discussed in Chapters Five and Six. Overall graft performance, techniques and indications have been reviewed by Aponte-Tinao et al., underlining both the complexity and the sparing potential of its use (36). As there is some overlap with the multiplanar resections and reconstructions examined in the image-based long-bone resections, this discussion will focus on the use of CAS for the reconstruction of defects using bone grafts.
Docquieretal.reportedin2010thefirstuseofCASforthereconstructionofalargepelvic sarcoma (27). The paper described a practice session on a printed model of the pelvis and the subsequent surgery. Target plane coordinates were transferred by means of graft-to-patient registration. As the practice demonstrated a gap due to saw loss, the planning for the graft was moved back to compensate for this. The resection is performed with a guided oscillating saw.
Aponte-Tinao et al. and Chapter Five of this thesis report on an independently developed similar, easy-to-follow technique for exact allograft creation in the long bones (37). The resection planes were copied onto the bone and resected using freehandtools.Therewascorrectionforsawloss,tocreateanexactfitofthedonorbone. Aponte-Tinao et al. used imported 3D models of the resection planes during surgery, compared to our technique of planning the planes directly. In a subsequent paper the same group reported a non-union rate of 6% and a complication rate (that includes four non-unions) of 14% in 66 cases (36). The authors state that the non-union rates in their series is lower than in the literature (>10%) but that thecomplicationratedidnotdiffer.Fractureratesspecificallywerenotdiscussedthough. Results in both papers are promising; both mentioned that the technique reduced complexity of multiplanar resection, reconstruction of defects, and increased accuracy and precision.
Young et al. (2015) used CAS as support for the reconstruction of intercalary defects with grafts. They did not direct shape the allograft, but used the navigation to ‘… aidconstructionwithregardtolimblength,rotationandoverallalignment…’,byplanninganadditional axialplane (and likelymarkingson thebone, tofind this

General discussion and future perspectives
99
General discussion and future perspectives
98
plane during reconstruction) (28). This was a technique similar to what we used for intercalary graft orientation after the computer-assisted allograft shaping, as demonstrated in Chapter Two. This technique is very useful, as bone continuity is lost during resection and reconstructing exact joint/leg orientation with the naked eyeisdifficult.
An experiment on sawbones by Lall et al. looked at the surface area across the allograft-host junction site. Computer navigation showed a contact area of 43.7% of the optimal surface over 30.5% contact area in freehand resection, measured using pressure paper (38). The authors speculated that the low contact area may be acauseforthesignificantnon-unionrateintheliterature,andthat‘anincreaseincontactareausing[CAS]mayimproveratesofbonehealing’.
A further increase of accuracy and precision in resection and allograft creation was examined in Chapter Six. It was shown that, in the context of this small study, the already-accurate results of CAS resection and reconstruction could be improved upon. Docquier et al. explored possible sawblock usage to increase accuracy, and dismissed this option based on one paper that described faster and more accurate navigated freehand cuts in arthroplasty compared to saw guides (27). In our experiment, CAS and CAS-guided procedures took somewhat longer, yet the results were good, with CAS comparable to the literature and the CAS-guide slightly better. Accuracy (deviation), precision (positioning and smoothness) and gap all improved over freehand resection. The experiment proved that CAS use can improve accuracy andprecisioninorientation(findingtheplannedresection),butthattheCASguideactually helps to execute the planned bone cuts more accurately and precisely.
Another important step to achieve an optimal reconstructive result with a maximum of bone contact is the selection of allografts on three-dimensional shape. In the Netherlands and in many other countries, this is done by matching patient and donor sex, basic measurements and/or 2D radiographs. Paul et al. demonstrated that for pelvic allografts this process was prone to inaccuracies and suffers from interobserver variability (39). Several studies have published more accurate methods for volumetric allograft selection (40, 41). These methods are currently applied in practice in some clinics and bone banks.
Both in experimental and clinical studies, results with the use of navigation for allograft shaping have been excellent. The complexity of the procedure was reduced. Non-union rates were lower than comparative studies in the literature. Fracture rates have not been investigated yet. Better tools can potentially further increase graft creation accuracy and decrease complications associated with lack of smoothness and host-allograft gaps.

7
General discussion and future perspectives
99
General discussion and future perspectives
98
(Imageless) prosthesis placement
One of the major changes in orthopaedic oncology in recent decades has been the increasing trend of limb salvage surgery, driven by chemotherapy, improved imaging quality and the availability of modular prostheses. Length of reconstruction increases the need for accuracy as small errors in stem position aremagnified.Further, bone stock is limited after large resection so placement has to be accurate thefirsttime.
Image-based placement of custom and pelvic prostheses is the most commonly reported form of CAS-supported prosthesis placement in the literature. Wong et al. have described their extensive experience, mainly with the placement of custom tumour prostheses, both in the long bones and in the pelvis. As stated before, they used navigation not only to achieve the exact resection planes the custom prosthesisismadefor,butalsotoachievetheexactfixatingscrewpositions.Inapaper on eight patients an average MSTS score of 29.1 (range 28-30) was found and their scores were, according to the authors, higher than the scores achieved in comparable studies (31). An interesting observation in this paper is that for close joint salvageproceduresCAS canbenefit survival of the remainingbone ‘as theepiphysis and its capsular and ligamentous attachment no longer have to be fully exposed for reference’, resulting inpreservationofbloodflow.Youngetal.usedimage-based CAS for conic pelvic implant reconstruction to accurately ‘identify the entry point, direction, and depth of reaming for the coned stem’ (28). This is atechnique we have applied as well, in the placement of a stemmed cup (LUMiC), and canconfirmitsusefulness.
There is, as far as we know, only one other reference to imageless (modular) prosthetic placement in the literature. Cheong et al. discussed in 2011 the application of imageless CAS in tumour prosthesis placement in an unknown number of procedures. The authors were able to ‘minimize leg length discrepancies, improve restorationofthejointline,andaddressrotationalconcernsofimplantalignment’.Post-procedure limb length discrepancies were no greater than 1.5 cm (42). Further data on implant positioning or oncological parameters was not given.
Chapter Two described similar conclusions in an overview of 14 imageless cases. The technique was in our experience very helpful for length, joint line and rotation reconstruction. We also reported that the use of the imageless measurement mode is useful in exactly marking the resection plane for both safe resection and adherence to resection and reconstruction planning.
Our comparative study on the benefits of imageless CAS in tumour prosthesisplacementisstillinthefollow-upphase,astheonlywaytodiscernbenefit,withouta direct RCT with CT measurement or a recall of patients, is implant survival.

General discussion and future perspectives
101
General discussion and future perspectives
100
In conclusion, there are not enough data available, either in direct measurements or in implant survival and patient satisfaction data, to draw conclusions on (imageless CAS) prosthetic placement. Expert opinions and small-case series have described thistypeofCASapplicationasbeneficialintheplacementofconicalandcustomprostheses (image-based) and modular tumour prostheses (imageless). More research is needed.
Technical evaluation
CAS accuracy and the need for improved data gathering
For every surgical action there is an uncertainty in the spatial positioning of the tool or implant. This has impact not only on the result actually achieved but also on the planning, as this uncertainty has to be factored in. A support system that is precise but not accurate only improves adequate resection rates (tumour plus minimallyrequiredmargin)ifasufficientlylargemarginischosen.Whilefavourableoncological results are the primary goal of tumour surgery, large margins can compromisepostoperativefunctionaloutcome.ThebenefitsthatCAScanprovideare thus linked not only to the accuracy of the tool placement but also to the precision with which the supported action is performed.
Current CAS research is mainly focused on the clinical effects of application of CAS tosurgicalproceduresinaspecificanatomicalarea.Thestructureofthisthesisisanexample of that. Authors often describe the margins and report on what could be saved that otherwise had to be resected. Yet to better understand the actual accuracy and precision of the CAS systems and its toolset we need clinical measurements. The system error (sometimes reported as matching error), while often reported, is not a real representation of actual system accuracy (43). A further factor that underlines thisneedisthatthereisnosingle,unifiedCASworkflow.System,software,imagequality, registration techniques and tool use differ between clinics. Studies have already found large accuracy differences between surgical systems in imageless (arthroplasty)andimage-based(mandibularresections)workflow(44,45).Ritaccoetal. and Abrahams et al. have argued the need for clinical measurement by measuring planned planes versus achieved cutting planes on postoperative imaging (46,47). Cartiaux et al. have evaluated the use of ISO standards for the measurement of osteotomy accuracy for this exact purpose (48).
Improveddatagatheringthroughimagefusioncanfurthermorebenefittheentirefieldoforthopaediconcology.OurcurrentstandardofreportingformarginsiseitherbasedontheEnnekingcriteria(wide,marginal,intralesional)ortheRclassification(R0 radical, R1 microscopic involvement, R2 macroscopic involvement) (49, 50). The
7
General discussion and future perspectives
101
General discussion and future perspectives
100
minimalmarginoverthewholeresectionisdecisivefortheclassification.Wongetal. argue that ‘a judgement of clear surgical margins is based on sampling … and may underestimate the actual incidence of involvedmargins’ (20).What’smore,resectionswiththesameclassificationcanhavelargedifferencesinaveragemargin.Another argument is that including postoperative margin measurements in our workflowislikelytonotonlybenefitscientificresearchbutalsosupportpathologicalexamination(51).Thisenablesfastidentificationoftumourspillsitesorareasatriskdue to small margins. It would therefore be good to have the resected specimen CT-scanned before histological examination. In postop examination of procedures where normal pathological examination for margins is not possible, like curettages, it is already standard care to perform a baseline MRI as a postoperative check.
Measurement data achieved with different modalities and surgical toolsets, resulting in values for precision and accuracy, can likely be used to enhance our surgical planning and support radical decisions in difficult edge cases. Combining thisuniform data with clinical follow-up can drive the discussion on required margins. Finally, as we are very likely past the stage of an ethically acceptable randomised controlled trial on CAS for high-grade sarcoma, this data can be critical in the scientificevaluationofsurgicaltechniques.
CAS system use
There are different strategies to CAS use, both for matching and instrumentation, in the literature. Most reports and procedures in this thesis used point-based matching and surface matching. Some different strategies described were direct matching on MRIimagesusingresorbablepinsasfiducialmarkersbyChoetal.andKimetal.(32,52). Cho et al. also used K-wires for CT-based matching. These techniques may reduce the chances of large mismatches. The downsides are that a small procedure is needed to implant the markers and that new CT and MRI images have to be made afterthosenecessaryfordiagnosis.AsChapterTwodescribes,diagnosticworkflowfor our cases was designed to have CAS-ready CT-scans made, if necessary during the diagnostic process. This was designed to reduce the need for duplicate scans and to lower patient radiation exposure. 3D MRI-only navigation (in contrast to the more common 2D multi-slice MRI fused to a matched CT) is a potential radiation-free alternative with the advances in MRI sensitivity and resolution. Other techniques with fiducialmarkers like fluoro-CTwere also described. If surfacematching onMRIisavailable,fiduciariesarenolongerrequiredfor(3D)MRI-onlynavigation.Avery interesting, possibly non-invasive future possibility is ultrasound registration through multi-modal matching (53).
There were problems with the navigation systems during procedures, both in the literature and in this thesis. So et al. had two failures on surface registration; the authorsbelievedpoorCTandbonequalitytobethecause.Theyswitchedtofluoro-

General discussion and future perspectives
103
General discussion and future perspectives
102
CT matching (24). Aponte-Tinao et al. reported three failures, one in software and two in hardware (35). Young et al. had problems achieving an accurate match because of high BMIs and limited exposure in one case and inaccuracies experienced due to a match on a mobile bone segment in another case (28). Chapter Two reported oneightissueswithCASnavigation,almostallinthefirstyearofCASuse.Inourexperience most are related to the learning curve.
Thereweren’talotofspecificmentionsofhighinaccuracyduringtheprocedures(i.e. inaccuracies after a successful match). Young et al. is the only example: they discovered the inaccuracies (due to the match on a mobile segment) only when the hip joint was violated. In Chapter Six we saw some possible inaccuracies that were only detected in post-procedure analysis. Chapter Two describes two non-radical resections in procedures where there was a successful and accurate system setup. A computer navigation system that is mismatched can be highly precise but not accurate, according to the ISO definitions. The only safeguard againstthese potentially very dangerous hidden inaccuracies is the surgeon. This requires understandingofthesystems,methodofmatchingandCASworkflow(continuouschecking). It is likely a large part of the clinical learning curve.
As far as we know, there is no mechanism in place that checks match accuracy during the procedure, for example by intermittently checking a known point as a mark on the bone. Redundancy of important systems is standard operating procedure in critical industrial applications of technology, for example in the aviation industry. Currently the only link between spatial and digital anatomical coordinates is the patient tracker. If the tracker is moved relative to the matched bone by mistake, the system accuracy will drop without the surgeon knowing. The same is true for the tools, if a connector moves: the system will still display the point where it is expected to be, not where it actually is. Contact trackers (detect bone contact by means of tools, reconstruct and check surface) or secondary matching mechanisms (3D laser scanning, optical recognition of the bone surface, multi-modal fusion based on ultrasound, etc.) could enable cross-checks to guard against this problem. This will very likely decrease the cognitive load of constantly comparing CAS against surgical intuition. It will also make accepting the objective orientation offered by the system easier, a problem we have especially seen with less CAS-experienced surgeons.
AfinalargumentagainsttheuseofCASorothersystemsforobjectiveintraoperativenavigation was its cost, in terms of (surgical) time and money (43). As Chapter Two demonstrated, surgical set-up time after the initial learning curve can be short. Planning can be done for the most part during patient switches (in anaesthesiology time) or is already required to be done in advance in complex procedures. Chapter Fivedemonstrated that theCASworkflowdoesnot increase intraoperative time,compensating for the set-up time or even saving time compared to a standard procedure. A CAS system is expensive. However, as Jeys et al. speculated, such

7
General discussion and future perspectives
103
General discussion and future perspectives
102
systems can be cost-effective if they reduce complications and local recurrence rates (17). According to a review of Picard et al., it can be cost-effective in standard arthroplasty (54). In addition, use of a CAS system is not limited to orthopaedic oncology.
Current tools
Theworkflowandtechniqueofnavigationandinstrumentationhaschangedlittlesince it was first described in 2004 by Hüfner et al., whomentioned navigatedchisels, and Krettek et al., who used navigated placement of K-wires (21, 22). Optical trackers are still attached to instruments with a binding apparatus, introducing a potential source of inaccuracy. Different instruments have been tracked; some papers describe the use of marking the osteotomy plane with navigated diathermy, drill or bone burr, and perform the resections without navigation support. Others have marked the resection planes on the bone with diathermy, drill holes or K-wires and performed the resection with navigated osteotomes and/or navigated power saws (17).
The need for improved tools can be seen not only in Chapter Six, with the improvements the CAS guide offers over standard CAS – it is also clear in daily practice, with the problems of attaching trackers to instruments and calibrating them, for example in curettage surgery. A major problem addressed in this thesis was that the software and system we use (Orthomap 3D) only offer matching using a calibrator on a 2D point (all instruments are a 2D line). Without direct feedback of orientation of the tool, the surgeon has to interpret this, again relying on an accurate frame of reference. For the placement of the CAS guide we had to rely on two 2D lines to orientate the saw block in a 3d plane, which is not optimal.
In our experience, the use of navigated oscillating saws had a potential drift in accuracy and low precision, whereas other groups have reported successful use of this tool. There are currently no studies available on the accuracy and precision achieved with different instruments or with different CAS systems. In our opinion this information is needed for a better discussion on the application of CAS and for surgical planning.
Analysis of current use and future perspectives
CAS acceptance
AnimportantaspectofCASapplicationisthesurgicalcommunity’sacceptanceofthesystem.Inarthroplasty,CASwasfirstseenasamajorrevolutionbyearlyadopters.However, as Picard et al. state in an article on CAS acceptance in orthopaedic
General discussion and future perspectives
105
General discussion and future perspectives
104
surgery, acceptance has been slow (54). The use of CAS in orthopaedics may even be decreasing. An important aspect in the acceptance of CAS is likely its image: it is still associated with being a demanding technology, requiring an in-depth technicalview,longset-uptimesandhighcosts.Still,theinterfaceandworkflowofthesystemsarestillaimedattechnicalusers.SignificantimprovementshavebeenmadetotheuserinterfaceandworkflowintheCASarthroplastyfield,butbasedonourexperiencethecurrentoncologysystemsandworkflowarenotintuitiveenoughfor CAS novices. Investments in the ecosystem and toolsets requires users, and vice versa.
Current CAS issues
The current low rate of acceptance can hamper the development of the technique and its ecosystem. Some promising applications of CAS need hardware and software support. In addition to the image-related issues mentioned above, there is only a single registration connection, with no backup system in place to prevent drifts in patient or tool accuracy. The current toolset of an orthopaedic surgeon is not adapted for CAS use, requiring adaptors and often limiting the potential for increased usefulness. Finally, CAS research is still in the phase of case series. We couldallbenefitfrommeasurementstandardsforsurgicalprocedures.Thiswouldenable comparisons between studies on outcome as well as on modalities and toolsets.
Current CAS benefits
CAScanbeatechnologicallysuperiorreplacementforfluoroscopyinthecurettageof low-grade malignant, intermediate and benign lesions. With adapted tools and software, increases in clinical parameters are very likely. Application of CAS, both in experimental and clinical studies, has shown a very high percentage of radical resections inwhatareoftenextremelydifficultprocedures inthepelvisand longbones. This increase reaches such a degree that a randomised control for high-grade pelvic sarcoma resections may arguably be unethical. The increase in accuracy andprecisionenablesnewproceduresthatwouldn’thavebeenpossibleotherwise;this often results in the salvage of critical anatomical structures, thereby drastically improving outcome for our patients. CAS can be used to reconstruct large defects with a high degree of accuracy using grafts and/or (custom) prostheses, enabling more joint salvage surgery and/or increase in patient function. In this thesis CAS set-up time is shown not to be an issue in real-world clinical use. Initiatives for increased accuracy in data reporting have been published in CAS-specific orthopaediconcologyscientificliteratureandarepickingupsteam.
7
General discussion and future perspectives
105
General discussion and future perspectives
104
Public health benefits
CAS has a role in the current trend in treatment aimed at more limb and joint salvage surgery. In that sense, CAS can improve function, quality of life and the participation in society of patients who were diagnosed with bone cancer. Previously impossible joint salvage procedures are the prime example in this thesis of the effect CAS can have on post-surgical function. However, at this point in time follow-up is not long enoughandcohort sizenotbigenough tobeable todrawfirmconclusionsonquality of life and participation. More research is needed on this aspect.
Future perspectives
While CAS in orthopaedic oncology is now more than 10 years old, acceptance has been slow. Technological development will nonetheless continue and will likely accelerate. Complete integration of spatial awareness, advanced imaging possibilities and per-patient reconstructions will completely change the surgical oncologyworkflow.
In the near future we will see a further integration of our current toolset into the CAS ecosystem, or the development of a separate toolset (e.g. smart burrs or absorption of CAS into robotics). This will increase both the accuracy in the orientation of the tool (no more adapters and 3D depiction of the tools) and the precision of the surgical action. This increased accuracy will mean that we can use more advanced planning software, availing ourselves of virtual surgery simulation tools and physics-based evaluation tools, which will provide a detailed surgical plan. High precision willallowsurgeonstoadaptprocedurestoamoreefficientbalancingofmarginsversusfunction.Largedefectswillbereconstructedusingamorepatient-specificapproach, using 3d printed prostheses or carefully shaped bone grafts. However, even with these smart tools we will be looking at a 2D screen for the next decade.
In the farther future the interface for CAS devices will likely move to an augmented reality approach with an even larger focus on medical imaging. Pre-planning can be done using virtual surgery to evaluate options. It will be possible to make more accurate predictions on the exact level of functioning the patient will have after the surgery based on kinematic models, enabling a data-driven decision process on procedure type and reconstruction, e.g. allograft or custom prosthesis. The patient’s anatomy during surgery is augmented with markers on the points ofinterest or overlain by the preoperative scans. Low-grade malignant, intermediate and benign lesions will be treated percutaneously. The CAS system will keep track of the position of the bone and instruments in multiple ways, such as multi-modal fusion with ultrasound or 3D (laser) surface detection, ensuring a highly accurate result even when trackers or the robotic connection moves. As high-resolution 3D imaging and overlay headsets are now commonplace, the surgeon can call in
General discussion and future perspectives
107
General discussion and future perspectives
106
support from other orthopaedic surgeons worldwide. Surgical tools will be semi-autonomous, as passive-smart tools, or fully autonomous after the surgeon holds them to the planning site. The high degree of radical resections with optimal margin will increase the need for early diagnosis even more. Accurate reconstructions will allow postoperative function to be closer to preoperative function, lowering the long-term impact of treatment on orthopaedic oncology patients.
General discussion and future perspectives
107
General discussion and future perspectives
106

References(1) Lee H, Shim JS, Jin HJ, Seo SW. Accuracy and limitations of computer-guided
curettage of benign bone tumors. Comput Aided Surg 2012;17(2):56-68.
(2) Wong K, Kumta S, Tse L, Ng E, Lee K. Navigation Endoscopic Assisted Tumor (NEAT) surgery for benign bone tumors of the extremities. Comput Aided Surg 2010;15(1-3):32-39.
(3) Kang HG, Cho CN, Kim KG. Percutaneous navigation surgery of osteoid osteoma of the femur neck. Minim Invasive Ther Allied Technol 2014;23(1):58-62.
(4) Campos WK, Gasbarrini A, Boriani S. Case report: Curetting osteoid osteoma of the spine using combined video-assisted thoracoscopic surgery and navigation. Clin Orthop Relat Res 2013;471(2):680-685.
(5) Li J, Wodajo F, Theiss M, Kew M, Jarmas A. Computer Simulation Techniques in Giant Cell Tumor Curettage and Defect Reconstruction. Comput Sci Eng 2013;15(2):21-26.
(6)KahlerD.Imageguidance:fluoroscopicnavigation.ClinOrthop2004(421):70-76.
(7) Wieners G, Pech M, Beck A, Konig B, Erdmenger U, Stockle U, et al. Comparison of radiation dose and image quality of Siremobil-IsoC(3D) with a 16-slice spiral CT for diagnosis and intervention in the human pelvic bone. Rofo 2005 Feb;177(2):258-264.
(8) Widmann G, Schullian P, Fasser M, Niederwanger C, Bale R. CT-guided stereotactic targeting accuracy of osteoid osteoma. Int J Med Robot Comp 2013;9(3):274-279.
(9) Gelderblom H, Hogendoorn PC, Dijkstra SD, van Rijswijk CS, Krol AD, Taminiau AH, et al. The clinical approach towards chondrosarcoma. Oncologist 2008;13(3):320-329.
(10) Donati D, Giacomini S, Gozzi E, Ferrari S, Sangiorgi L, Tienghi A, et al. Osteosarcoma of the pelvis. Eur J Surg Oncol 2004;30(3):332-340.
(11)BhagatS, SharmaH,PillaiD, JaneM.PelvicEwing’s sarcoma:a review fromScottish Bone Tumour Registry. J Orthop Surg 2008;16(3).
(12) Han I, Lee YM, Cho HS, Oh JH, Lee SH, Kim H. Outcome after surgical treatment of pelvic sarcomas. Clin Orthop Surg 2010;2(3):160-166.
(13) Kawai A, Huvos AG, Meyers PA, Healey JH. Osteosarcoma of the pelvis: oncologic results of 40 patients. Clin Orthop 1998;348:196-207.
(14) Grimer R, Carter S, Tillman R, Spooner D, Mangham D, Kabukcuoglu Y. Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81(5):796-802.
General discussion and future perspectives
108

7
(15) Ozaki T, Flege S, Kevric M, Lindner N, Maas R, Delling G, et al. Osteosarcoma of the pelvis: experience of the Cooperative Osteosarcoma Study Group. J Clin Oncol 2003;21(2):334-341.
(16) Wirbel R, Schulte M, Mutschler W. Surgical treatment of pelvic sarcomas: oncologic and functional outcome. Clin Orthop 2001;390:190-205.
(17) Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of local recurrence in patients with a tumour of the pelvis or sacrum? Bone Joint J 2013;95-B(10):1417-1424.
(18) Cartiaux O, Banse X, Paul L, Francq BG, Aubin C, Docquier P. Computer-assisted planning and navigation improves cutting accuracy during simulated bone tumor surgery of the pelvis. Comput Aided Surg 2013;18(1-2):19-26.
(19) Young P, Bell S, Mahendra A. The evolving role of computer assisted navigation in musculoskeletal oncology. Bone Joint J Orthop Proc 2013;95(SUPP 1):111-111.
(20) Wong K, Kumta S. Use of computer navigation in orthopedic oncology. Curr Surg Rep 2014;2(4):1-8.
(21) Hüfner T, Kfuri Jr M, Galanski M, Bastian L, Loss M, Pohlemann T, et al. New indications for computer-assisted surgery: tumor resection in the pelvis. Clin Orthop 2004;426:219-225.
(22) Krettek C, Geerling J, Bastian L, Citak M, Rücker F, Kendoff D, et al. Computer aided tumor resection in the pelvis. Injury 2004;35(1):79-83.
(23) Reijnders K, Coppes MH, van Hulzen AL, Gravendeel JP, van Ginkel RJ, Hoekstra HJ. Image guided surgery: new technology for surgery of soft tissue and bone sarcomas. Eur J Surg Oncol 2007;33(3):390-398.
(24) So TY, Lam Y, Mak K. Computer-assisted navigation in bone tumor surgery: seamlessworkflowmodelandevolutionoftechnique.Clin Orthop Relat Res 2010;468(11):2985-2991.
(25) Cho HS, Oh JH, Han I, Kim HS. The outcomes of navigation-assisted bone tumour surgery: minimum three-year follow-up. J Bone Joint Surg Br 2012;94(10):1414-1420.
(26) Wong KC, Kumta SM, Chiu KH, Antonio GE, Unwin P, Leung KS. Precision tumour resection and reconstruction using image-guided computer navigation. J Bone Joint Surg Br 2007;89(7):943-947.
(27) Docquier PL, Paul L, Cartiaux O, Delloye C, Banse X. Computer-assisted resection and reconstruction of pelvic tumor sarcoma. Sarcoma 2010;2010:125162.
(28) Young PS, Bell SW, Mahendra A. The evolving role of computer-assisted
General discussion and future perspectives
109
navigation in musculoskeletal oncology. Bone Joint J 2015;97-B(2):258-264.
(29) Jeys L, Grimer R, Carter S, Tillman R, Abudu S. OUTCOMES OF PRIMARY BONE TUMOURS OF THE PELVIS–THE ROH EXPERIENCE. J Bone Joint Surg Br 2012;94(SUPP XIV):39-39.
(30) Fuchs B, Hoekzema N, Larson DR, Inwards CY, Sim FH. Osteosarcoma of the pelvis: outcome analysis of surgical treatment. Clin Orthop 2009;467(2):510-518.
(31) Wong KC, Kumta SM. Joint-preserving Tumor Resection and Reconstruction Using Image-guided Computer Navigation. Clin Orthop Relat Res 2012:1-12.
(32) Kim JH, Kang HG, Kim H. MRI-guided navigation surgery with temporary implantable bone markers in limb salvage for sarcoma. Clin Orthop Relat Res 2010;468(8):2211-2217.
(33) Aponte-Tinao LA, Ritacco LE, Ayerza MA, Muscolo DL, Farfalli GL. Multiplanar osteotomies guided by navigation in chondrosarcoma of the knee. Orthopedics 2013;36(3):e325-30.
(34) Li J, Wang Z, Guo Z, Chen GJ, Yang M, Pei GX. Precise resection and biological reconstruction under navigation guidance for young patients with juxta-articular bone sarcoma in lower extremity: preliminary report. J Pediatr Orthop 2014;34(1):101-108.
(35) Aponte-Tinao L, Ritacco LE, Ayerza MA, Muscolo DL, Albergo JI, Farfall GL. Does Intraoperative Navigation Assistance Improve Bone Tumor Resection and Allograft Reconstruction Results? Clin Orthop Relat Res 2014:1-9.
(36) Aponte-Tinao LA, Ritacco LE, Albergo JI, Ayerza MA, Muscolo DL, Farfalli GL. The principles and applications of fresh frozen Allografts to bone and joint reconstruction. Orthop Clin North Am 2014;45(2):257-269.
(37) Aponte-Tinao LA, Ritacco LE, Ayerza MA, Muscolo DL, Farfalli GL. Multiplanar osteotomies guided by navigation in chondrosarcoma of the knee. Orthopedics 2013;36(3):e325-30.
(38) Lall A, Hohn E, Kim MY, Gorlick RG, Abraham JA, Geller DS. Comparison of Surface Area across the Allograft-Host Junction Site Using Conventional and Navigated Osteotomy Technique. Sarcoma 2012;2012:197540.
(39) Paul L, Docquier P, Cartiaux O, Cornu O, Delloye C, Banse X. Inaccuracy in selection of massive bone allograft using template comparison method. Cell Tissue Bank 2008;9(2):83-90.
(40) Ritacco LE, Farfalli GL, Milano FE, Ayerza MA, Muscolo DL, Aponte-Tinao L. Three-dimensionalvirtualbonebanksystemworkflowforstructuralboneallograft selection: a technical report. Sarcoma 2013;2013.
General discussion and future perspectives
110

7
(41) Paul L, Docquier P, Cartiaux O, Cornu O, Delloye C, Banse X. Selection of massive bone allografts using shape-matching 3-dimensional registration. Acta Orthop 2010;81(2):250-255.
(42) Cheong D, Letson GD. Computer-assisted navigation and musculoskeletal sarcoma surgery. Cancer Control 2011;18(3):171-176.
(43) Saidi K. Potential use of computer navigation in the treatment of primary benign and malignant tumors in children. Curr Rev Musculoskelet Med 2012:1-8.
(44) Casap N, Wexler A, Eliashar R. Computerized navigation for surgery of the lower jaw: comparison of 2 navigation systems. J Oral Maxillofac Surg 2008;66(7):1467-1475.
(45) Carli A, Aoude A, Reuven A, Matache B, Antoniou J, Zukor DJ. Inconsistencies between navigation data and radiographs in total knee arthroplasty are system-dependent and affect coronal alignment. Can J Surg 2014;57(5):305-313.
(46) Ritacco LE, Milano FE, Farfalli GL, Ayerza MA, Muscolo DL, Aponte-Tinao LA. Accuracy of 3-D planning and navigation in bone tumor resection. Orthopedics 2013;36(7):e942-50.
(47) Abraham JA. Recent advances in navigation-assisted musculoskeletal tumor resection. Curr Orthop Pract 2011;22(4):297-302.
(48) Cartiaux O, Paul L, Docquier P, Francq BG, Raucent B, Dombre E, et al. Accuracy in planar cutting of bones: an ISO-based evaluation. Int J Med Robot Comp 2009;5(1):77-84.
(49) Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. 1980. Clin Orthop Relat Res 2003;415:4-18.
(50) Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010;17(6):1471-1474.
(51) Bellanova L, Schubert T, Cartiaux O, Lecouvet F, Galant C, Banse X, et al. MRI-based assessment of safe margins in tumor surgery. Sarcoma 2014;2014.
(52) Cho HS, Park I, Jeon I, Kim Y, Han I, Kim H. Direct application of MR images to computer-assisted bone tumor surgery. J Orthop Sci 2011;16(2):190-195.
(53) James AP, Dasarathy BV. Medical image fusion: A survey of the state of the art. Inform Fusion 2014;19:4-19.
(54) Picard F, Clarke J, Deep K, Gregori A. Computer Assisted Knee Replacement Surgery: Is the Movement Mainstream? Orthopedic & Muscular System: Current Research 2014;3(2):-.
General discussion and future perspectives
111


Summery / Samenvatting

Orthopaediconcologyisthemedicalfieldthatspecializesinthesurgicaltreatmentof bone tumours. With advances in surgical technique, (neo-) adjuvant chemo therapy and knowledge of tumour biology, there has been a trend in orthopaedic oncology not only towards better survival rates but also to more minimal- and less invalidatingprocedures.Attheheartofthistransformationliesadifficultbalance.Each procedure requires a careful weighing of two competing interests: margin and function. Accuracy and precision are needed to balance these to interests and thus to achieve an efficient but oncologically safe result. To assist in this,mostproceduresinbonetumoursurgeryrequireintraoperativeimagingwithfluoroscopyand/or measurements with rulers for anatomical orientation and margin control. Computer-assisted surgery (CAS) in orthopedic surgery is a recently developed alternative for intraoperative imaging and measurements, potentially providing an improvement in the necessary precision and accuracy in bone tumour surgery. The main goal of this thesis was to investigate the indications, surgical parameters and clinical outcome of the application of CAS in orthopaedic oncology. Furthermore it describes the adaptation of existing surgical techniques and creation of new techniques and tools using CAS. Application to four types of surgical procedures has been tested.
CASwasatleastclinicallyequivalenttofluoroscopyuseincurettagetypetreatmentwhile not relying on ionizing radiation use. Arguably CAS curettage is better in difficultanatomicalpositions,forexampleinfibrousdysplasiaofthefemoralheador pelvis. Technically it’s a superior alternativewith real time, three-dimensionalfeedback. While there is additional intra-operative set-up time, CAS curettage takesequallyas longandmaypotentiallybeevenfasterthanfluoroscopybasedcurettage.
For imagebased resection CAS can be used for both simple and complex procedures that include some that are impossible otherwise, sparing critical structures that otherwise could not be spared. Pathologic analysis showed excellent results with a very high number of non-intralesional resections, higher than in comparative non-CAS studies. More follow-up is needed to assess long term oncologic follow-up. Custom resections require custom reconstructions. Both in experimental and clinical studies, the accuracy with the use of navigation for allograft shaping has been excellent. The complexity of the procedure was reduced. Better tools can potentially further increase graft creation accuracy and decrease complications associated with lack of smoothness and host-allograft gaps as has been demonstrated in the experimental study. Imageless resection and tumor prosthesis placement was helpful in length, joint line and rotation reconstruction. Data on these types of procedures is however limited.
Summery / Samenvatting
114

8
Computer-assisted surgery systems are a relatively new development in orthopaedic oncology. The increase in accuracy and precision provided enables new procedures that otherwise would not have been safely possible, often resulting in saving critical anatomical structures and thereby improving outcome for our patients. It can be used to reconstruct large defects with a high degree of accuracy using grafts and/or (custom) prosthesis, enabling more joint salvage surgery and/or increase in patient function. While current low rate of acceptance can hamper the development of the technique and its ecosystem, complete integration of spatial (tool) awareness, advanced imaging possibilities and per-patient reconstructions can potentially completelychangetheoncologicalsurgicalworkflow.
Summery / Samenvatting
115

Orthopedische oncologie is het chirurgische veld dat zich bezighoudt met de behandeling van bottumoren. Door de vooruitgang van chirurgische techniek, (neo-) adjuvante chemotherapie en kennis van tumorbiologie, is er een trend in de orthopedische oncologie in de richting van niet alleen betere overlevingskansen maar ook naar meer minimaal invasieve en sparendere behandelingen. Cruciaal hierbij is het evenwicht tussen marge (veiligheid) en functie. Precisie en nauwkeurigheidzijnnoodzakelijkomditevenwichttevindeneneenefficiëntenoncologisch veilig resultaat te bereiken. Verschillende methodes worden hiervoor gebruikt:intra-operatievebeeldvormingmiddelsfluoroscopieen/ofmetingenvanafherkenningspunten voor anatomische oriëntatie en margecontrole. Computer-assisted surgery (CAS) in orthopedische chirurgie, een soort operatief GPS-systeem, is een recent ontwikkeld alternatief voor deze intraoperatieve beeldvorming en metingen.
Het hoofddoel van dit proefschrift was het onderzoeken van indicaties, chirurgische en klinische uitkomstparameters met betrekking tot de toepassing van CAS in orthopedische chirurgie. Verder beschrijft het de aanpassing van bestaande operatieve technieken en instrumenten voor de toepassing van CAS. Vier verschillende type procedures zijn onderzocht.
CASisklinischgelijkwaardigaanfluoroscopiezonderhetgebruikvanioniserenderöntgenstraling in de behandeling van atypische cartilagineuse tumoren. Het is te beargumenteren dat CAS curettage gunstiger is als het gaat om lastige anatomische locaties, bijvoorbeeld in de femurkoppen of het bekken. Technisch gezien is het een beter alternatief met real-time, driedimensionale feedback. Het systeem vereistopstarttijdvoormatchingvandigitalebeeldenmetdepatiënt,echterCAScurettage blijkt niet meer operatietijd te kosten en kan potentieel zelfs sneller zijn dancurettagemiddelsopfluoroscopie.
CAS kan in het kader van image-based resectie worden toegepast voor zowel eenvoudige als complexe procedures. In anatomisch complexe situaties kan CAS procedures mogelijk maken die normaliter niet veilig uitgevoerd kunnen worden. Het sparen van kritische structuren is hiermee vaak mogelijk. Pathologische analyse liet uitstekende resultaten zien met een hoog aantal radicale resecties. Dit is een hoger aantal dan in vergelijkbare studies zonder CAS. Vervolgonderzoek is nodig om het oncologische verloop op de lange termijn te kunnen beoordelen.
Aangepaste resecties vereisen aangepaste reconstructies. In zowel experimentele als klinische studies is de nauwkeurigheid van het gebruik van CAS voor het maken van reconstructies middels grafts uitstekend. De complexiteit van de procedure wordt ermee gereduceerd. Betere instrumentatie kan potentieel verdere stappen in nauwkeurigheid van graftcreatie mogelijk maken. Dit kan het fractuurrisico verlagen
Summery / Samenvatting
116

8
door het bereiken van een kleinere gaten tussen host en graft en een beter contact. Ook maakt CAS hiermee gewrichtssparende operaties makkelijker.
Imageless resectie en plaatsing van tumorprotheses was nuttig voor het reconstrueren vanledemaatslengte,rotatieenoriëntatievanhetgewrichtsoppervlak.Erisechternog weinig data beschikbaar van dit soort type procedures.
Computer assisted surgery is een relatief nieuwe ontwikkeling binnen de orthopedische oncologie. De toename in nauwkeurigheid en precisie maakt nieuwe procedures mogelijk die anders niet veilig uitgevoerd kunnen worden. Dit met het resultaat dat belangrijke anatomische structuren gespaard kunnen worden, zoals in gewrichtssparende operaties, potentieel met goed effect op het klinische resultaat. Hoewel de huidige lage acceptatiegraad een probleem kan zijn voor de verdere ontwikkelingvandetechniek,lijktdatmetnauwkeurigeidentificatievantumoreninstrumenten,geavanceerdebeeldverwerkingenpatient-specifiekereconstructies,CAS een grotere rol kan gaan spelen binnen de orthopedische oncologie.
Summery / Samenvatting
117

Dankwoord
Het schrijven van een thesis is niet het werk van slechts één PhD student. Gedurende en zelfs vóór de start van mijn MD/PhD project heb ik hulp gekregen van velen. Het schrijven van een boek kan op sommige momenten lijken op een eindeloos en eenzaam traject. Steun kan dan enorm van pas komen. Hier ben ik dan ook zeer dankbaar en erkentelijk voor. Ten eerste wil ik graag mijn supervisoren van de afdeling Orthopedie van het UMCG bedanken:
Beste Sjoerd (Prof. Dr. Bulstra). Jij bent degene die mij op het pad van het MD/PhD traject heeft gezet nadat ik als derde jaars student bij Paul was gestart met onderzoek. Bedankt voor het vertrouwen, voor de ondersteuning en de adviezen die je hebt gegeven. Het traject bleek een prima keus. De mogelijkheden, adaptie van vele nieuwe technologieen, en vooral open atmosfeer die onderzoekers binnen de afdeling Orthopedie worden geboden is fantastisch. Jou enthousiasme was hier een grote factor in.
Beste Paul (Dr. Jutte). Als dagelijks supervisor kon ik geen betere begeleider wensen. Zelf in de drukste weken kon je tijd vrij maken om concepten te beoordelen of feedback te geven op ontwikkelingen. Ook het stimuleren van projecten naast de onderzoekslijnen apprecieer ik zeer. Van medical image analysis tot onderzoeksregistratieenRFAplanning,erwarengenoegideeënenlijnenomuitte werken. De vrijheid van werken hierin was fantastisch. De grote mind-map op de whiteboard liet jaren geleden al plannen zien om toepassingen van lopende losse onderzoekslijnen te combineren. Er is nog zoveel interessants uit te zoeken. Dank voor de inspiratie.
Beste Martin (Dr. Stevens). Bedankt voor alle de ondersteuning tijdens het doorlopen van de PhD. Schrijven is een kunst en kost in het begin vele iteraties om een goed stuk te krijgen. Vele concepten zijn heen en weer gegaan. Bedankt voor de altijd constructieve commentaren. Ook voor de stimulatie als iets af moest zijn en, zeker niet te vergeten, voor de adviezen als het even tegen zat.
Graag zou ik ook de leden van de leescommissie willen bedanken: prof. dr. Nelissen, prof. dr. Hoekstra en prof. dr. Veth. Geachte hooggeleerde heren ik dank u hartelijk voor het beoordelen van dit proefschrift op wetenschappelijke kwaliteit en waarde.
Mijn co-autheurs voor hun enthousiaste ondersteuning: Prof. dr. ir. Verdonschot, dr. van Ooijen, dr. Tomaszewski, dr. Dierselhuis en dr. Ploegmakers.
Verder gaat mijn dank uit naar: Els en Yvonne voor de ondersteuning in alles en nog wat en de humor op het secretariaat. Mijn collega onderzoekers op de orthopedie, Tim, Wietske, Marrigje, voor de gezellige tijd op de onderzoekskamer. Mijn clubgenoten van Invictus, voor begrip als ik avonden bezig was. Mijn mede MD/PhD genoten Jan, Marjolein en Esther voor de vele interessante en leuke discussies nawerktijd.Mijnvrienden-collega’svanTFommijachtermijnpcvandaanteslepen
Dankwoord
120

9
op warme dagen om buiten van muziek of sport te genieten.
Tenslotte wil graag mijn ouders Karel en Trudy, zusje Nynke en vriendin Chantal bedanken voor hun ondersteuning over de jaren. Jullie hebben waarschijnlijk het meeste gezien van het pad tot PhD.
Dankwoord
121


Curiculum Vitae

Curiculum vitae
124
Jasper Gerbers was born on the 31st of October 1988 in Groningen, the Netherlands. He is the son of Karel Gerbers and Trudy Hollander and has a sister called Nynke. After his childhood in Haren, he went to the Praedinius Gymnasium in Groningen. Afterfinishinghighschoolachoicebetweenatechnologicalstudyandmedicinehad to be made. After a successful application Jasper started his medical education at University of Groningen (RUG) in 2006.
Duringhisthirdyear,whilefixingabrokencomputerforanorthopaedicsurgeonin Haren, the author got introduced to computer-assisted surgery and started with extra-curricular research soon after this. This research led to an application for a combinedMD/PhDprogramin2011,withastartinJanuary2012.Thefinalmedicalinternship was done at the Orthopaedics Department of the Leeuwarden medical centre (MCL) with a specialisation period at the emergency medicine department of theUniversityMedicalCenterGroningen.JasperfinishedmedicalschoolinJanuary2014.
During his PhD years the author was active in the SHARE and GUIDE PhD councils, working on improving the information availability for PhD students. A passion for sports was translated in becoming a part of a sport related start-up as a programmer and writer. At the 13th International Society for Computer Assisted Orthopaedic Surgery conference in Orlando, in 2013, the author won the best clinical paper award.
Currently Jasper works as a junior doctor (ANIOS) at the department of Surgery in the University Medical Center Groningen. In 2016 he will start with his 6 year training to become an Orthopedic Surgeon.
Curiculum vitae
125

Previous SHARE Disserations

Previous SHARE Disserations
129
Previous SHARE Disserations
128
Research Institute SHARE
This thesis is published within the Research Institute SHARE (Science in Healthy Ageing and healthcaRE) of the University Medical Center Groningen / University of Groningen.
Further information regarding the institute and its research can be obtained from our internetsite: http://www.share.umcg.nl/.More recent theses can be found in the list below. ((co-) supervisors are between brackets)
2015
Geurts, MME
Integrated pharmaceutical care; cooperation between pharmacist, general practitioner, and patient and the development of a pharmaceutical care plan
(prof JJ de Gier, prof JRBJ Brouwers, prof PA de Graeff)
Sun J
Developing comprehensive and integrated health system reform policies to improve use of medicines in China
(prof HV Hogerziel, prof SA Reijneveld)
Wyk, L van
Management of term growth restriction; neonatal and long term outcomes
(prof SA Scherjon, prof JMM van Lith, dr KE Boers, dr S le Cessie)
Vos FI
Ultrasonography of the fetal nose, maxilla, mandible and forehead as markers for aneuploidy
(prof CM Bilardo, prof KO Kagan, dr EAP de Jong-Pleij)
Twillert S van
Linkingscientificandclinicalknowledgepractices;innovationforprosthetic rehabilitation
(prof K Postema, prof JHB Geertzen, dr A Lettinga)

Previous SHARE Disserations
129
Previous SHARE Disserations
128
Loo HM van
Data-driven subtypes of major depressive disorder
(prof RA Schoevers, prof P de Jonge, prof JW Romeijn)
Raat AN
Peerinfluenceinclinicalworokplacelearning;astudyofmedicalstudents’useofsocialcomparisoninclinicalpractice
(prof J Cohen-Schotanus, prof JBM Kuks)
Standaert BACGM
Exploring new ways of measuring the economic value of vaccination with an application to the prevention of rotavirus disease
(prof MJ Postma, dr O Ethgen)
Kotsopoulos N
Novel economic perspectives on prevention and treatment: case studies for paediatric, adolescent and adult infectious diseases
(prof MJ Postma, dr M Connolly)
Feijen-de Jong, EI
On the use and determinants of prenatal healthcare services
(prof SA Reijneveld, prof F Schellevis, dr DEMC Jansen, dr F Baarveld)
Hielkema M
The value of a family-centered approach in preventive child healthcare
(prof SA Reijneveld, dr A de Winter)
Dul EC
Chromosomal abnormalities in infertile men and preimplantation embryos
(prof JA Land, prof CMA van Ravenswaaij-Arts)