units.dm5migu4zj3pb.cloudfront.net/manuscripts/104000/104601/jci62104601.pdf · ionization of...
TRANSCRIPT

Journal of Clinical InvestigationVol. 41, No. 7, 1962
THE SEPARATEEFFECTS OF HYPERPARATHYROIDISM,HYPERCALCEMIAOF MALIGNANCY, RENALFAILURE,
AND ACIDOSIS ON THE STATE OF CALCIUM,PHOSPHATE,ANDOTHERIONS IN PLASMA*
By MACKENZIEWALSER
(From the Department of Pharmacology and Experimental Therapeutics and Department ofMedicine, Johns Hopkins School of Medicine; and the Medical Service,
Johns Hopkins Hospital, Baltimore, Md.)
(Submitted for publication January 22, 1962; accepted March 8, 1962)
The physiological properties of calcium arefunctions of free ionic calcium.1 Total plasmacalcium may fail to reflect the free calcium ionconcentration, particularly in subjects with acido-sis or alkalosis, or with abnormal concentrationsof protein or phosphate. The determination offree ionic calcium is therefore important, not onlyin interpretation of plasma calcium values, but alsoin understanding mechanisms of hypercalcemiaand hypocalcemia, and the relationship of plasmacalcium to plasma phosphate.
The frog heart method of McLean and Hastings(4) for determining ionized calcium has providedmuch useful information but remains a difficultand somewhat unpredictable technique. Further-more, it gives no clue as to the effective phosphateconcentration and, therefore, to the mineralizingpropensity of the blood. Yendt, Connor andHoward (5) showed that the tendency of plasmato calcify rachitic cartilage could be employed asa measure of mineralizing propensity. This indexdid not show a constant relationship to the productof ultrafiltrable calcium by ultrafiltrable phos-phate in patients, especially in renal failure, inwhich calcification failed to occur at products thatwere more than adequate in non-uremic plasma.This observation implied that the ionization ofcalcium or phosphorus, or both, is reduced inrenal failure or, alternatively, that some otherconstituents are inhibiting calcification.
In 1955, Raaflaub (6) introduced a chemicalmethod for determining ionized calcium in pro-
* Supported by U.S. Public Health Service GrantsA-2306 and OG-li. Some of this material has been pre-sented previously in abstract form (1-3).
1 The role of ion-pair complexes, in which calcium isbelieved to be ionized but not free, is reviewed in theDiscussion.
tein-free fluids with murexide. Results obtainedwith this method, referred to below, have gen-erally confirmed the conclusions derived from ex-periments with the frog heart technique, both instudy of normal plasma and in pathological con-ditions. Again, the absence of a method fordetermining effective phosphate concentration haslimited the usefulness of these measurements inproblems concerning mineralization.
Wehave recently reported a method for esti-mating both free Ca2+ and free HPO42- concentra-tions, using a modification of Raaflaub's technique,a new method for free Mg2+ (7), and a set ofequations to derive HPO42- after allowing forcomplexed phosphate. The analysis of normalplasma by this procedure was the subject of aprevious report (8). The purpose of the presentstudy was to determine whether this procedureaffords useful information in hypercalcemic states.in renal failure, and in subjects with both con-ditions.
PATIENTS AND METHODS
Patients. Most of the subj ects were patients in theJohns Hopkins Hospital; a few were patients in theUniversity of Maryland Hospital, the Baltimore CityHospital, or the Union Memorial Hospital. They havebeen classified in four groups and arranged in order ofincreasing serum urea nitrogen concentrations (TablesI and II). Chemical values given in these tables wereperformed in the clinical laboratories, on blood samplesdifferent from those on which the other measurementsreported here were made.
1. Primary hyperparathyroidism. In 13 patients, oneor more parathyroid adenomas were removed and con-firmed histologically; 12 of these patients were treatedsurgically. The other patient (Wel) died before opera-tion could be performed, and the suspected adenoma wasfound at autopsy. In Subject 14 operation has not beenperformed because of advanced age and debility. Thissubject (Ric) is nevertheless included because he presents
1454

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
the full picture of hyperparathyroidism, including poly-uria, nephrolithiasis, bone changes, hypercalcemia, andhypophosphatemia. In the entire group, 7 subjects (50per cent) had nephrolithiasis; 5 (36 per cent) had radio-logic bone changes, 3 showing only generalized demineral-ization. Since these three patients were elderly, it is byno means certain that this change was due to hyper-parathyrtidism rather than to osteoporosis. However,alkaline phosphatase was elevated to 11 units per cent inone of these (Cro). Elevated phosphatase without dem-onstrated bone lesions was seen in two others. Azotemiaof mild degree was seen in four. In three subjects, addi-tional samples were obtained after parathyroidectomy.
2. Vitamin D intoxication. Two patients with hypo-parathyroidism, who developed hypercalcemia and asso-ciated azotemia during therapy with vitamin D, areincluded. In both, samples were obtained before hyper-calcemia developed. One of these patients also had asingle renal stone, apparently related to an episode ofpyelonephritis.
3. Hypercalcemia of malignancy. Twelve patients withhypercalcemia secondary to neoplastic disease were stud-ied. All but two had recognized bone lesions; X-rays andautopsy revealed no bone lesions in these two patients(Mar and Smi). All but four patients were azotemic.Seven were alkalotic (including five with azotemia), asindicated by pH values in excess of 7.5 in venous plasma.Three had phosphatase levels above 8 Bodansky U. Au-topsies were performed in six of these patients; noparathyroid hyperplasia was found except in Subject Mar,who had one slightly enlarged and three other normalglands.
4. Renal disease. Twenty-eight patients with primaryrenal disease were studied. Three without azotemia areincluded for comparison. One showed no chemical ab-normalities, one had hypermagnesemia only, and thethird had hyperphosphatemia only. The other 25 patientshad varying degrees of azotemia and acidosis. Only onehad nephrolithiasis. Bone X-rays were obtained in afew subjects and were negative; almost all had chest
TABLE I
Clinical data, hypercalcemic subjects
Bone Renal Alk.Name Age Sex Diagnoses lesions stones SUN* C02 p'tase
mg% mmoles/ U%tL
I. Primary hyperparathyroidismIck 74 F Parath. adenomat No No 8 29 8.2Cha 35 F Parath. adenomat No No 9 24 6.8Ric 72 M Hyperparath.§ Yes¶ Yes 10 29 5.4Bar 35 F Parath. adenomat No Yes 10 4.7Bak 53 F Parath. adenomat No Yes 10 23 9.0Cro 61 F Parath. adenomat Yes¶ No 11 26 11.0Stu 54 M Parath. adenomat No Yes 11Aba 64 M Parath. adenoma4 No Yes 13 24 6.0Wil 55 F Parath. adenomat No Yes 17 7.5Rit 25 M Parath. adenoma4 Yes Yes 17 18 60.0Wel 72 M Parath. adenomat No No 21 25 6.8Joh 73 F Parath. adenomat Yesv No 30 25 5.3Sla 46 M Parath. adenomat Yes No 31 21 11.1Bot 49 F Parath. adenomat No No 33 22 10.6
II. Vitamin D intoxicationWal 52 F Hypoparath.§, treated with vit. D No Yes 31 27 2.5Har 55 F Hypoparath.§, treated with vit. D No No 33 30 2.1
Il l . Hypercalcemia of malignancyl|Bur 85 M Carc. of lung, metast. Yes No 11 30 2.2Mar 79 M Anapl. neoplasm, ?hepatoma No No 12 26 4.5Gra 32 F Lymphoblastic leukemia Yes No 12 28 20.8Gol 59 F Multiple myeloma Yes No 15 22 8.6Col 53 F Carc. of breast, metast. Yes No 22 29 8.7Oco 34 F Carc. of bladder, metast. Yes Yes 25 30 3.2Wil 69 F Multiple myeloma Yes No 29 35 5.0Smi 57 M Carc. of lung, metast. No No 35 26 3.9Bel 60 M Carc. of lung, metast. Yes No 44 29 2.9Bul 60 M Multiple myeloma Yes No 53 24 2.1Rub 39 M Multiple myeloma Yes No 68 19 3.0Maa 51 F Anapl. neoplasm, ?hepatoma Yes No 93 22 7.0
* Serum urea nitrogen.t Bodansky units.t Pathological diagnosis.§ Clinical diagnosis.II Pathological diagnoses¶T Osteoporosis only.
(except NMar).
1455

MACKENZIEWALSER
TABLE II
Clinical data, subjects with renal disease
Parathyroid Renal Alk.Name Age Sex Diagnoses hyperplasia stones SUN C02 p'tase
mg% mmoles/ U%*L
Joh 29 F Chronic pyelonephritist ? No 11Fis 45 M Nephrosclerosist ? No 16 28 5.4New 39 M Acute glomerulonephritist ? No 18 27Sta 15 M Chronic glomerulonephritist ? No 23 29 6.8Jon 40 F Chronic pyeloneph., nephroscler.T No No 33 28Fis 42 F Nephrosclerosis,t diabetest No No 58 20 5.6Edw 77 F Nephrosclerosist ? No 76 13 4.8Hew 40 M Nephrosclerosist No No 83 20 7.8Tho 49 M Nephrosclerosist ? Yes 89 33 9.2Gre 67 M Nephrosclerosist No No 90 17Dis 46 F Subacute glomerulonephritist ? No 104 11Har 59 M Chronic pyeloneph., nephroscler.t No No 113 11 5.8Tyl 68 F Chronic pyelonephritist ? No 121 13Bro 56 F Nephrosclerosist ? No 122 22War 31 F Nephrosclerosist ? No 124 20Aut 35 F Chronic pyeloneph., nephroscler.t ? No 129 17 6.7Wil 59 F Nephrosclerosis, thymomat No No 152Sta 45 M Chronic pyeloneph., hepatitist ? No 158 17 11.9Jac 48 F Nephrosclerosist No No 160 12 5.1Wol 45 F Chronic glomeruloneph.t No No 168 14 4.2Hic 49 M Nephrosclerosist Yes No 172 18Seg 55 M Nephrosclerosist ? No 194Goo 48 M Nephrosclerosist No No 208 13Fri 40 F Nephrosclerosist No No 210 18She 58 M Chronic pyelonephritist ? No 214 8Flo 49 M Nephrosclerosis4 Yes No 218 11 1.9Lip 56 M Chronic pyelonephritist No No 252 13Bie 53 M Nephrosclerosist Yes No 300 17 3.4
* Bodansky units.t Clinical diagnosis.t Pathological diagnosis.
films or kidney films, or both, which showed no bonelesions. Alkaline phosphatase levels were obtained inhalf of the subj ects and were above 8 Bodansky U inonly two. The parathyroid glands were examined atautopsy in 13 patients and at operation in one (Bie).Hyperplasia was found in the operated subj ect and intwo others. The diagnosis "nephrosclerosis" in the tablerefers to arteriosclerosis or arteriolosclerotic nephropathyassociated with hypertension, or both. One patient (Wil)was found at autopsy to have a malignant thymoma.This had extended only locally, and no bone lesions weredetected. Subject Bie underwent hemodialysis and para-thyroidectomy and is discussed further in Results.
Methods. In each subj ect, 35 to 50 ml of venous bloodwas obtained anaerobically with minimal stasis in aheparinized syringe. In almost every instance the sub-j ects were either fasting or in the postabsorptive state.Annino and Relman (9) have shown that an ordinarybreakfast has no effect on any of the constituents meas-ured in this study except phosphate, which falls about 30per cent 45 minutes after eating but has returned to thefasting value within 2 hours. Plasma was separatedpromptly, and pH was determined at room temperature.pH values were corrected for temperature by adding0.01 U per ° C. Plasma was stored under oil in thefrozen state until analyzed. In hypercalcemic plasma,100 per cent CO2 was bubbled through the samples fora few minutes before storage. Prior to ultrafiltration,
the pH was permitted to rise to the original value byexposure to air. At the start of ultrafiltration the pHwas therefore identical with the pH of venous plasma.The ultrafiltration chambers were filled with 5 per centCO2. In samples with low pCO2 values this might tendto lower pH during ultrafiltration. However, only mod-erately reduced pCO2 values were encountered (see be-low). Ultrafiltration was carried out at 350 to 390 C.2
2 One of the reviewers of this paper raised the questionas to whether complexed calcium (particularly CaHCO,+)might be altered by adding Tris buffer to ultrafiltrates.There are two conceivable ways in which this mightoccur. 1) Tris might complex calcium or some of thecalcium ligands in solution. We have shown (7) thatmeasured [Ca2+] in standard solutions is the same in Trisbuffer and diethylbarbiturate buffer, after allowance forcomplexing by the latter. We have also shown thatTris does not complex citrate (J. phys. Chem. 1961, 65,159). It has apparently not been shown that Tris formsany complexes other than with transition metals. 2)Bicarbonate or other anions might complex less calciumthan in native plasma, owing to lowered concentrations.However, the bicarbonate concentration is not reducedsignificantly more than that of other anions, the per-centage decrease being 20 for all. Since allowance forthis dilution factor is made in calculating the results, theunderestimation of complexed calcium cannot exceed 20
1456
IONIZATION OF PLASMACALCIUM AND PHOSPHATE
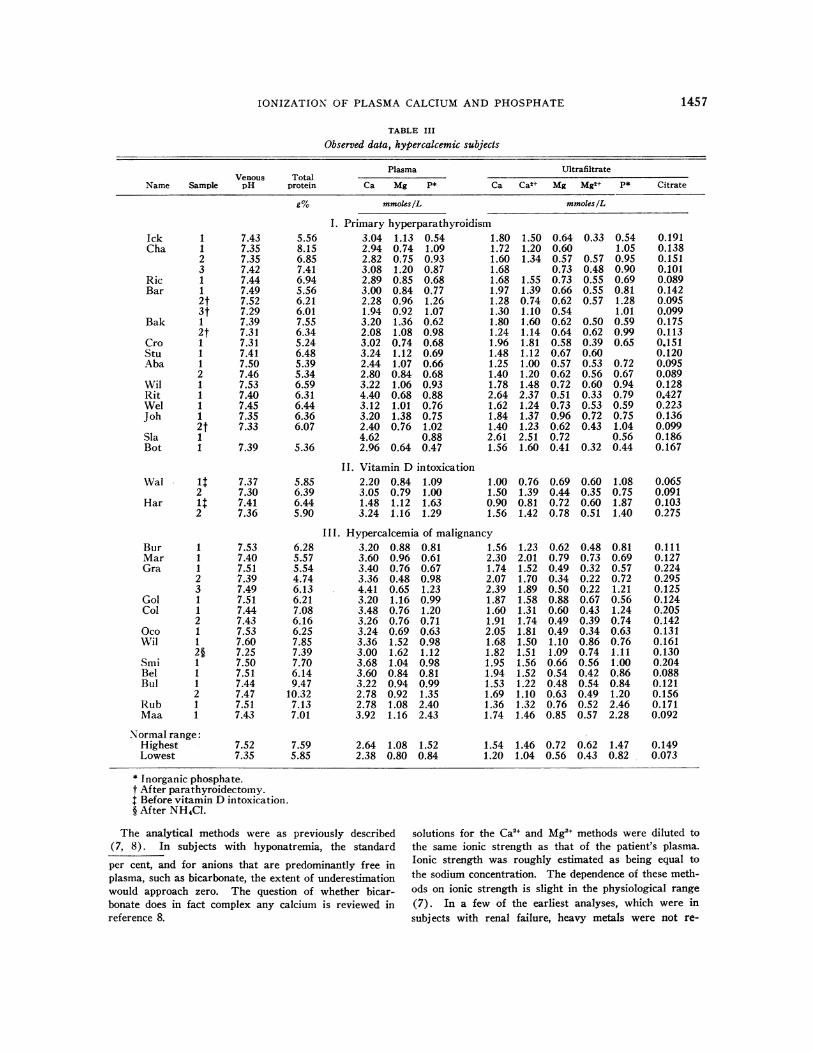
TABLE III
Observed data, hypercalcemic subjects
Plasma UltrafiltrateVenous Total
Name Sample pH protein Ca Mg P* Ca Ca2+ Mg Mg2+ P* Citrate
gO mmoles/L mmoles/L
I. Primary hyperparathyroidismIck 1 7.43Cha 1 7.35
2 7.353 7.42
Ric 1 7.44Bar 1 7.49
2t 7.523t 7.29
Bak 1 7.392t 7.31
Cro 1 7.31Stu 1 7.41Aba 1 7.50
2 7.46Wil 1 7.53Rit 1 7.40Wel 1 7.45Joh 1 7.35
2t 7.33Sla 1Bot 1 7.39
5.568.156.857.416.945.566.216.017.556.345.246.485.395.346.596.316.446.366.07
5.36
3.042.942.823.082.893.002.281.943.202.083.023.242.442.803.224.403.123.202.404.622.96
1.130.740.751.200.850.840.960.921.361.080.741.121.070.841.060.681.011.380.76
0.64
0.541.090.930.870.680.771.261.070.620.980.680.690.660.680.930.880.760.751.020.880.47
1.801.721.601.681.681.971.281.301.801.241.961.481.251.401.782.641.621.841.402.611.56
1.501.201.34
1.551.390.741.101.601.141.811.121.001.201.482.371.241.371.232.511.60
0.640.600.570.730.730.660.620.540.620.640.580.670.570.620.720.510.730.960.620.720.41
0.33
0.570.480.550.550.57
0.500.620.390.600.530.560.600.330.530.720.43
0.32
0.541.050.950.900.690.811.281.010.590.990.65
0.720.670.940.790.590.751.040.560.44
0.1910.1380.1510.1010.0890.1420.0950.0990.1750.1130.1510.1200.0950.0890.1280.4270.2230.1360.0990.1860.167
Wal it 7.37 5.852 7.30 6.39
Har it 7.41 6.442 7.36 5.90
II. Vitamin D intoxication2.20 0.84 1.093.05 0.79 1.001.48 1.12 1.633.24 1.16 1.29
1.00 0.76 0.69 0.60 1.08 0.0651.50 1.39 0.44 0.35 0.75 0.0910.90 0.81 0.72 0.60 1.87 0.1031.56 1.42 0.78 0.51 1.40 0.275
Bur 1 7.53Mar 1 7.40Gra 1 7.51
2 7.393 7.49
Gol 1 7.51Col 1 7.44
2 7.43Oco 1 7.53Wil 1 7.60
2§ 7.25Smi 1 7.50Bel 1 7.51Bul 1 7.44
2 7.47Rub 1 7.51Maa 1 7.43
6.285.575.544.746.136.217.086.166.257.857.397.706.149.47
10.327.137.01
III. Hypercalcemia of malignancy3.20 0.88 0.81 1.563.60 0.96 0.61 2.303.40 0.76 0.67 1.743.36 0.48 0.98 2.074.41 0.65 1.23 2.393.20 1.16 0.99 1.873.48 0.76 1.20 1.603.26 0.76 0.71 1.913.24 0.69 0.63 2.053.36 1.52 0.98 1.683.00 1.62 1.12 1.823.68 1.04 0.98 1.953.60 0.84 0.81 1.943.22 0.94 0.99 1.532.78 0.92 1.35 1.692.78 1.08 2.40 1.363.92 1.16 2.43 1.74
7.52 7.597.35 5.85
2.64 1.08 1.522.38 0.80 0.84
1.54 1.46 0.72 0.62 1.471.20 1.04 0.56 0.43 0.82
* Inorganic phosphate.t After parathyroidectomy.t Before vitamin D intoxication.§ After NH4CL.
The analytical methods were as previously described(7, 8). In subjects with hyponatremia, the standard
per cent, and for anions that are predominantly free inplasma, such as bicarbonate, the extent of underestimationwould approach zero. The question of whether bicar-bonate does in fact complex any calcium is reviewed inreference 8.
solutions for the Ca2" and Mg2` methods were diluted tothe same ionic strength as that of the patient's plasma.Ionic strength was roughly estimated as being equal to
the sodium concentration. The dependence of these meth-ods on ionic strength is slight in the physiological range
(7). In a few of the earliest analyses, which were in
subjects with renal failure, heavy metals were not re-
1.232.011.521.701.891.581.311.741.811.501.511.561.521.221.101.321.46
0.620.790.490.340.500.880.600.490.491.101.090.660.540.480.630.760.85
0.480.730.320.220.220.670.430.390.340.860.740.560.420.540.490.520.57
Normal range:HighestLowest
0.810.690.570.721.210.561.240.740.630.761.111.000.860.841.202.462.28
0.1110.1270.2240.2950.1250.1240.2050.1420.1310.1610.1300.2040.0880.1210.1560.1710.092
0.1490.073
1457

MACKENZIEWALSER
TABLE IV
Observed data, subjects with renal disease
Plasma UltrafiltrateVenous Total
Name Sample pH protein Ca Mg P* Ca Ca2+ Mg Mg2+ P* Citrate
g%
6.616.655.545.937.225.705.965.728.087.396.475.536.245.626.596.935.116.996.226.815.785.68
7.366.445.705.56
6.204.936.904.765.195.336.166.015.05
mmoles/L
2.52 0.70 1.072.30 1.20 1.022.32 1.07 1.612.35 0.92 1.672.31 1.23 1.702.17 1.16 2.052.09 1.60 1.751.73 3.142.26 0.98 1.492.56 1.39 1.412.32 0.81 1.122.14 0.98 3.441.87 0.65 1.971.60 0.80 2.541.90 1.11 1.802.30 1.08 3.022.16 1.62 2.832.42 1.83 1.712.11 1.37 1.412.34 0.89 1.801.91 0.90 3.182.24 1.25 1.81
2.14 1.53 5.321.63 1.20 5.072.27 2.791.56 1.58 7.06
1.62 3.482.32 0.84 3.331.82 1.18 4.032.52 1.00 4.652.48 1.00 2.191.76 0.92 2.881.44 0.96 3.991.48 1.04 4.311.36 1.04
1.421.301.381.26
.1.291.221.191.031.331.381.591.431.300.921.021.381.461.601.141.490.941.511.031.101.371.380.830.881.071.661.051.321.280.840.920.770.74
1.171.181.261.271.211.101.080.631.221.091.231.181.030.710.840.831.041.240.960.961.081.440.800.990.641.220.310.420.741.320.580.781.020.640.630.500.50
mmoles/L
0.53 0.540.68
0.64 0.610.57 0.57
0.750.68 0.561.11 0.780.83 0.500.53 0.411.04 0.650.47 0.340.91 0.760.30 0.240.64 0.270.93 0.810.59 0.341.40 1.201.041.31 0.960.620.73 0.400.77 0.782.18 1.001.14 0.580.76 0.661.09 0.871.171.10 0.520.48 0.180.68 0.510.97 0.660.88 0.530.66 0.450.72 0.510.67 0.530.72 0.500.82 0.54
0.990.981.471.601.591.921.713.051.261.411.033.081.802.671.583.052.891.571.261.643.031.792.205.145.232.576.967.893.363.494.494.952.163.234.354.773.23
0.1160.0950.1120.1450.1470.1580.1900.1020.0760.1830.1230.1270.0940.1080.1830.1340.1070.1730.1000.1970.0800.0910.0960.0760.1340.1060.0960.0900.0710.0420.0710.0630.0670.0840.1160.1380.073
2.64 1.08 1.522.38 0.80 0.84
1.54 1.46 0.72 0.62 1.471.20 1.04 0.56 0.43 0.82
* Inorganic phosphate.t After parathyroidectomy.
moved before determination of Ca2+ and Mg+. Thiscauses a greater error in the Mg2+ than in the Ca`+ method(7) and may account for the fact that free ionic mag-nesium appeared to exceed ultrafiltrable magnesium in a
few samples (Sta and Jac).
RESULTS
Observed data in the patients are given inTables III and IV. The range of values in 24normal subjects, including 20 previously presented(8), is also shown. Statistical comparison was
not made because the data were not normallydistributed. The data have been analyzed interms of the separate effects of 1) azotemia, 2)
acidosis, 3) hyperparathyroidism, and 4) hyper-calcemia of other types, upon several parameters:1) the percentage ionization of plasma calcium;2) the ion product [Ca2+] X [HPO42-]; 3) theability of the plasma proteins to bind calcium,measured as Kcaprot; and 4) the fraction of plasmacalcium present as diffusible complexes.
Percentage ionization of plasma calcium
1. Role of acidosis and of renal failure. It isoften stated that the hypocalcemia of uremia doesnot usually produce tetany because of the asso-
ciated acidosis. The protective effect of acidosis
JohFisNewStaJonFisEdw
HewThoGreDisHarTylBroWarAutWil
StaJac
WolHicSegGooFri
SheFloLipBie
1 7.461 7.531 7.461 7.451 7.501 7.361 7.342 7.361 7.411 7.601 7.281 7.061 7.181 7.161 7.361 7.381 7.361 7.292 7.281 7.461 7.262 7.311 7.421 7.411 7.281 7.141 7.242 7.401 7.161 7.271 7.271 7.302 7.353t 7.354t 7.13St 7.096t 7.30
Normal range:HighestLowest
7.52 7.597.35 5.85
0.1490.073
1458

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
is attributed to one or both of the following mech-anisms: first, an alteration in the percentage ion-ization of calcium due to diminished protein bind-ing; and second, a specific effect of the hydrogenion itself on neuromuscular irritability. As indi-cated in Figure 1, the percentage ionization ofcalcium was no higher in uremic subjects withsevere acidosis (venous pH < 7.30) than in thosewith mild acidosis, normal pH, or mild alkalosis.In fact, it was frequently subnormal (in one-thirdof the acidotic samples). As indicated below, thiswas due to increased amounts of diffusible calciumcomplexes rather than to increased protein-boundcalcium. Only one subject (Jac) showed a highpercentage ionization of plasma calcium; total cal-cium was close to normal in this sample, so thattetany would- not have been anticipated. Despitesubnormal calcium ion concentrations in more
than half of the azotemic subjects, tetany was
not seen; positive Chvostek signs, however, were
elicited in several patients. Tremulousness, con-
vulsions, and coma were not predictably related tocalcium or magnesium ion concentrations. Car-popedal spasm was not seen, even at calcium ionconcentrations one-fourth of normal (Fri) or afterparathyroidectomy (Bie).
In the nonacidotic uremics, the percentage ion-ization of calcium was usually normal. Further-more, in the three groups of hypercalcemic sub-jects, the azotemic samples exhibited neitherhigher nor lower percentage ionization values.Mild to moderate renal failure thus has no effect
0'
C"cmtA
z
co
0
C02+Co
ECMlCMtV
z
cn
e Parathyroid hyperplasia or adenomaNo parathyroid hyperplasia
o Parathyroids not examined
0
0.0E 0- , .° E 0 ES0 a~0 ~C0
z C > a.
FIG. 1. THE RATIO OF FREE IONIC CALCIUM TO TOTAL
PLASMACALCIUM IN SIX GROUPSOF PATIENTS.
on the ionization of plasma calcium. A decreasein ionization may occur in severe uremia.
2. Role of hypercalcemia. The percentage ofplasma calcium bound to protein is not altered bymoderate elevations of plasma calcium (10). Onewould not anticipate, therefore, that the percent-
TABLE V
Effect of parathyroidectomy on four indices of the state of plasma calcium
RatioSubject Sample [Ca] [Ca2+]/[Ca] Kcaptot [Ca2+][HPO42-] Complexed Ca
mmoles/L M MX10-6 %of total
Primary hyperparathyroidismBar Preop. 3.00 0.46 0.0110 0.59 19
Postop. 2.28 0.32 0.0084 0.50 24Postop. 1.94 0.53 0.0109 0.57 10
Bak Preop. 3.20 0.50 0.0100 0.49 6Postop. 2.08 0.55 0.0102 0.58 5
Joh Preop. 3.20 0.43 0.0087 0.52 15Postop. 2.40 0.51 0.0090 0.65 7
Secondary hyperparathyroidismBie Preop. 2.48 0.41 0.0055 1.13 10
Postop. 1.76 0.36 0.0051 1.06 11
1459

MACKENZIEWALSER
3.02.5
o aox
0ia. 1.0
'' 0.8rl,% 0.6
u 0.5
0.4
0.3
E ENu NA Vz z
CO* 0
a 0
o o
2
Parathyroid hyperplasia or adenomaNo porathyroid hyperplosiaParathyroids not examined
I
mlII
a
II
I
I
d
d
t
p90
90
:Z :s .o, *-
,
E o.z 0. ,O YE Ea rn0~~~
FIG. 2. THE PRODUCTOF FREE CALCIUM ION CONCEN-TRATION BY FREE DIBASIC PHOSPHATEION CONCENTRATIONIN THE SAME SUBJECTS. The scale is logarithmic, inorder to emphasize the low values seen in some subj ects.
age ionization of plasma calcium would changeunless some other specific effects occurred. AsFigure 1 shows, no alteration in percentage ioniza-tion was noted in these 34 hypercalcemic samples.
3. Role of hyperparathyroidism. In neitherprimary nor secondary hyperparathyroidism wasthere a significant change in percentage ionization.Parathyroidectomy in four subjects failed to alterthis value (Table V). The significance of thesefindings in comparison with other studies is con-sidered in the Discussion.
The ion product [Ca2+] [HP042-]
In Figure 2 are shown the calculated values forthis product in the various groups of subjects,designated in the same manner as in Figure 1.It should be emphasized that the value [HP042-]is calculated, rather than measured directly (8).A logarithmic scale has been used in order toemphasize the low values seen in some subjects.
1. Role of acidosis. Since the relative propor-tion of the ions HP042- and H2P04- is dictatedby pH, the percentage of total plasma phosphate
present as HPO42- was smaller in the severelyacidotic subjects. Nevertheless, the product[Ca2+] [HP042-] was somewhat larger, on theaverage. These acidotic subjects usually hadmore severe uremia (see Table II). Since renalfailure tends to raise this product, as indicatedbelow, the higher products found probably reflectan effect of renal failure rather than of acidosis.
2. Role of renal failure. In many of the az-otemic subjects (including those without para-thyroid hyperplasia) this product was consider-ably increased, often many-fold, as a result of arise in [HP042-]. There was some correlationbetween the product and the degree of azotemia,as shown in Figure 3. Similarly, higher productswere seen in those hypercalcemic subj ects whowere also azotemic.
3. Role of hypercalcemnia. In the hypercalcemiaof malignancy, the product [Ca2+] [HPO42-] wasnot elevated in the absence of azotemia except inone subject. No discernible effect of hypercal-cemia per se on this product is seen in thesesamples, despite elevated ionic calcium concentra-tions in most of them. This is because HPO42-concentrations tended to fall in reciprocal fashionuntil renal failure supervened. In the two sub-jects with hypoparathyroidism, the developmentof vitamin D intoxication was associated with onlya slight rise in this product despite the appear-ance of azotemia; in other words, [HPO42-] fell(Table VI).
3.0r
2.5 h
0
x 2.0-
r-n 1.00a.
rM.0 S
S. Normalrange
100 200Serum Urea N, mg%
300
FIG. 3. THE RELATIONSHIP BETWEENTHE ION PRODUCT[CA"+] [HPO4' ] ANDUREARETENTION IN SUBJECTS WITHPRIMARY RENAL DISEASE. The scale is linear.
1460
l l
.
*
00
0

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
TABLE VI
The effect of vitamin D intoxication on four measures of the state
RatioSubject Sample [CaJ [Ca2+]/[CaJ Kcaprot [Ca2+][HPO42-] Complexed Ca
mmoles/L M MX10-6 %of totalWal On low dosage 2.20 0.35 0.0050 0.43 11
Toxic 3.05 0.46 0.0060 0.53 4
Har Untreated 1.48 0.44 0.0113 0.79 6Toxic 3.24 0.44 0.0051 1.02 4
4. Role of hyperparathyroidism. In patientswith parathyroid tumors the product [Ca2+][HP042-] tended to be reduced and was belownormal in 36 per cent. This finding is in contrastto the other hypercalcemic subjects and indicatesthat, in hyperparathyroidism, [HP042-] may fallmore than [Ca2+] rises. In secondary hyper-plasia, however, the opposite occurred. Thehighest values for the product were seen in thesethree cases, as is shown in Figure 2.
This finding was further investigated by re-peated samples in Subject Bie. This individualshowed progressive renal failure of 2 months'duration, apparently owing to hypertension andhyperphosphatemia without hypocalcemia (seeTables II and IV). In the hope of improvingrenal function, a parathyroidectomy was per-formed. Three extremely large hyperplasticglands and part of a fourth were removed. Beforesurgery and again 1 week afterward, hemodialvsiswas performed. The results of repeated measure-
Dialysis DialysisMX 10'- arfthyroidectom 4l
To
a-
'(II-
mM/L
a*2 ~~~~~HP042ac
October 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
T T Date T
FIG. 4. SERIAL OBSERVATIONS IN A PATIENT WITH
ARTERIOLAR NEPHROSCLEROSIS AND SECONDARY HYPER-
PARATHYROIDISMWHOWAS SUBJECTED TO HEMODIALYSIS
AND SUBTOTAL PARATHYROIDECTOMY.
ments of [Ca2+], [HPO42-], and their product areshown in Figure 4. Despite normocalcemia, somedepression of [Ca2+] was evident in the firstsample, owing to increased complexed calcium.[HP042-] was markedly elevated, and thereforethe product was also elevated. Hemodialysisraised [Ca2+j to normal, in association with a fallin complexed calcium, but lowered [HP04 2-] con-siderably more, so that the product fell almostto normal. After parathyroidectomy, plasma cal-cium, which had been stable for several weeks,fell progressively. The ion product, however, re-mained constant because of a reciprocal rise in[HPO42-]. Total phosphate rose much morerapidly in this interval than in the precedingweeks. A second hemodialysis again lowered theion product. Parathyroidectomy in three patientswith parathyroid adenomas had no effect on thisproduct, as shown in Table V.
These results suggest that parathyroid hormonehas little or no effect on this product except byway of its phosphaturic action, which tends todecrease it. In the absence of this mechanism,the product is held at a relatively constant value,i.e., [HP042-] varies reciprocally with [Ca2+] inany given subject. The product about which thesereciprocal adjustments occur may be greatly in-creased by uremia. In secondary hyperparathy-roidism the degree and duration of nitrogen reten-tion may be marked, so that the product may beunusually high. All three of the patients withparathyroid hyperplasia had severe uremia. Pre-sumably, if hyperplasia developed in a patient withmild uremia, little or no elevation of the productmight be seen. This is borne out by the findingsin the mildly azotemic subjects with parathyroidtumors, in whom the products were normal ordecreased (Figure 2).
1461

MACKENZIEWALSER
TABLE VII
Apparent dissociation constant of calcium proteinate,Kcaprot, in various conditions
No. of Standardsamples Mean deviation
M MNormal 24 0.0086 + 0.0016
Renal diseaseVenous pH < 7.30 15 0.0101 i 0.0040Venous pH > 7.30 15 0.0096 d 0.0017
Hypercalcemia of malignancy 17 0.0086 i 0.0029Primary hyperparathyroidism 16 0.0084 i 0.0021
Secondary hyperparathyroidism 3 0.0089
Calcium-binding ability of plasma protein
In order to obtain a measure of the affinity ofthe plasma proteins for calcium, one procedure isto isolate the individual proteins and performequilibrium dialysis with calcium solutions (11).A simpler technique estimates the effective dis-sociation constant of calcium proteinate in plasma,using ultrafiltration data and considering all of theplasma proteins together (12). In such calcula-tions the role of complexed calcium is uncertain.Although chelating anions such as citrate formcomplexes with calcium which are apparently notbound to protein (13, 14), simple multivalentanions like phosphate and sulfate form ion-paircomplexes with calcium which are bound to pro-
tein as much as are free calcium ions (14). Aconsiderable proportion of the complexed calciumof plasma is unidentified (8), particularly in ure-
mia, so that it is uncertain how much of the cal-cium bound to protein is also bound to anions.In calculating the dissociation constant, Kaaprot,it is therefore not clear whether one should employthe free calcium ion concentration or all of theultrafiltrable calcium. On the unproven assump-
tion that most of the anions that complex calciumdo not alter its protein binding, we have employedthe ultrafiltrable calcium. The conclusions are
not altered by employing the calcium ion con-
centration.KcaProt is calculated as follows:
KCnProt [Ca]uF X ([Prot] - [CaProt])[CaProt]
[CaProt] = [Ca]p- [Ca]uFwhere [Ca]p and [Ca]uF, represent plasma andultrafiltrate concentrations in moles per liter, and
[Prot] represents protein equivalents in moles perliter calculated as 1.22 times total protein con-centration in grams per 100 ml (15).
The results are summarized in Table VII.In the 24 normal subjects, Kaaprot calculated in
this manner is 0.0086 M + 0.0016 M (SD).1. Role of acidosis. In 15 samples from uremic
subjects with venous pH < 7.30, Ka.Prot was0.0101 M + 0.0040 M. Although this mean issomewhat higher than the normal mean, the dif-ference is not statistically significant. However,the magnitude of the difference correspondsclosely to that found in rabbit serum by Peterson,Feigen and Crismon (15). In Subject Wil, withhypercalcemia of malignancy, administration ofNH4Cl sufficient to lower plasma pH from 7.60to 7.25 was associated with a rise in Kcaprot from0.0079 M to 0.0121 M.
2. Role of renal failure. In nonacidotic sub-jects with renal disease, Kcaprot was 0.0096 'M+ 0.0017 M, which is not significantly differentfrom the normal subjects. There was a sugges-tive correlation between Kcaprot and the serumurea nitrogen, the highest values of KCaprot beingseen in the most severe uremics. Of five subjectswith serum urea nitrogen values above 100 mgper100 ml, three had Kcaprot values (0.0130 M,0.0113 M, and 0.0115 M) above the normal range.Hence renal failure itself may diminish the abilityof plasma proteins to bind calcium, either by alter-ing the relative proportions of individual proteinsor by a qualitative change in the proteins them-selves.
3. Role of hypercalcemia. In the 17 samplesfrom patients with hypercalcemia of malignancy,KCaprot was 0.0086 M + 0.0029 M, or almost thesame as in normal subjects. Keaprot in the twosubjects with vitamin D intoxication was low,0.0051 Mand 0.0060 M, respectively. An earliersample in one of these two subjects with hypo-parathyroidism, obtained before any therapy,yielded a value of 0.0113 M.
4. Role of hyperparathyroidism. Kcaprot inplasma from patients with primary hyperpara-thyroidism was 0.0084 M + 0.0021 M, which isagain almost the same as in normal subjects. Inthe three patients with secondary hyperparathy-roidism, Kcaprot averaged 0.0089 M. Parathy-roidectomy had no effect on the product in threepatients with tumors; in Bie, the preoperative and
1462

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
postoperative samples yielded essentially the sameKeaprot (Table V). These observations indicatethat parathyroid hormone does not appreciablyalter the ability of plasma proteins to bind calcium.
Complexed calcium
The difference between ultrafiltrable calciumand free ionic calcium represents diffusible cal-cium complexes. Calcium citrate and secondarycalcium phosphate account for some of this frac-tion (8), but the remainder is unidentified. Themeasurement of this fraction entails a rather largeerror, since it is obtained as the difference betweentwo values which are usually quite close together.
The results are summarized in Table VIII. Inthe 24 normal subjects, the calculated amount ofcomplexed calcium varied from -0.01 to 0.43mmole per L (average, 0.18), or 7 per cent ofthe total plasma calcium. Only one value wasgreater than 0.33 mmole per L, or 13 per centof the total.
1. Role of acidosis. At low pH values, hydro-gen ions displace metal ions from ligand anions,and the extent of complexing of calcium mighttherefore decrease in acidosis. Fanconi and Rose(16) have presented evidence that hyperventila-tion alkalosis increases complexed calcium; theseauthors pointed out that, under these circum-stances, accumulation of organic anions in plasmamay account for the effects observed. In acidoticsubjects with renal failure, complexed calcium wasoften increased, but not out of proportion to theeffect of uremia itself, discussed below.
2. Role of renal failure. Morison, McLean andJackson (17), using the frog heart method, re-ported high values for complexed calcium in twosubjects with the nephrotic syndrome. The pres-ence or absence of azotemia in these two subjectswas not stated. They concluded that nephroticplasma may contain a factor toxic to the frogheart, invalidating these results. Fanconi andRose (16), using Raaflaub's method (6), foundan increase in complexed calcium in eight of tenpatients with renal failure, including three withprimary hyperparathyroidism, but not in thenephrotic syndrome uncomplicated by uremia.The upper limit of complexed calcium in theirnormal subjects was 0.15 mmole per L. Thehighest value seen in renal failure was 0.48 mmoleper L in a subject with a parathyroid adenoma.
TABLE VIII
Complexed calcium in various conditions, in millimoles perliter and as percentage of total plasma calcium
No. ofsamples Mean and range
mmoles/L %of totalNormal 24 0.18 7
-0.01-0.43 -1-18Renal disease
Venous pH < 7.30 15 0.32 170.00-0.73 0-45
Venous pH > 7.30 15 0.23 100.00-0.55 0-24
Hypercalcemia of malignancy 16 0.28 90.17-0.59 1-20
Primary hyperparathyroidism 15 0.27 9-0.04-0.58 -1-24
Secondary hyperparathyroidism 3 0.33 140.11-0.54 5-21
In the present series, complexed calcium ex-pressed as a fraction of total plasma calcium wasabove 13 per cent in more than half of patientswith serum urea nitrogen values over 100 mg per100 ml, the highest fraction being 45 per cent(Fri). This latter value was confirmed by asecond sample in the same subject, which con-tained only slightly less complexed calcium. Inthe other subjects with renal disease, complexedcalcium was within normal limits. Higher valueswere seen in those hypercalcemic subjects whowere also azotemic. Hemodialysis resulted in areduction of complexed calcium from 21 per centof the total calcium to 10 per cent in Bie.
3. Role of hypercalcemia. The subjects withhypercalcemia of malignancy, considered as agroup, show significantly more complexed calciumthan do normal subjects. However, most of themwere mildly to moderately azotemic, so that thisobservation is probably attributable to renal fail-ure rather than to any specific effect of malignantdisease or hypercalcemia per se. Only two ofthem exhibited complexed calcium values abovethe normal range when expressed as per cent oftotal plasma calcium. In the hypoparathyroidsubjects the rise of plasma calcium from a hypo-parathyroid level to a toxic level, occasioned byvitamin D, was not associated with an increase incomplexed calcium despite the appearance of mildazotemia (Table VI).
4. Role of hyperparathyroidism. Plasma citrateis commonly increased in hyperparathyroidism(18-21), and therefore an increase in complexedcalcium might be expected. In the subjects with
1463

MACKENZIEWALSER
primary hyperparathyroidism, citrate levels abovethe upper limit of the normal subjects (0.15mmole per L) were seen in half. Nevertheless,complexed calcium was not increased, either inconcentration or as a fraction of the total, exceptin Subject Bar. The contribution of the calciumcitrate complex to the complexed calcium in thesesubjects is considered below. Two of the threepatients with secondary hyperparathyroidismshowed high complexed calcium (without hyper-citremia) but not more than would be consistentwith their severe uremia. Parathyroidectomyproduced significant decreases in the percentageof plasma calcium complexed in two of four sub-jects (Table V). In Subject Bar, a transient riseoccurred in a sample obtained a few days post-operatively; a sample several weeks later con-tained less than the preoperative specimen of com-plexed calcium.
Vitamin D intoxication did not increase the per-centage of plasma calcium complexed (Table VI).In a large series of cases, Anning, Dawson, Dolbyand Ingram (22) found an increase in complexedcalcium in most.
Other observationsThe data in Tables III and IV are also relevant
to the effect of these various conditions on thestate of phosphate, citrate, and magnesium inplasma.
1. Phosphate. The distribution of phosphatebetween H2PO4- and HPO42- ions is dictated bypH. Protein binding of phosphate, expressed aspercentage of total plasma phosphate, was notaltered by renal disease, as demonstrated in a pre-vious paper (23). Hypercalcemia has been foundby other workers to decrease the ultrafiltrabilityof plasma phosphate (24, 25). In 5 of 17 samplesfrom patients with hypercalcemia of malignancy,and in 2 of 15 samples from patients with para-thyroid tumors, the percentage of plasma phos-phate found to be nonultrafiltrable was above theupper limit of normal (25 per cent). No increasewas seen in the two subj ects with vitamin D in-toxication. The amount of the complex CaHPO4parallels the product [Ca2+] [HPO42-] discussedabove, since the quotient of these two quantitiesis a constant. The amount of the complexNaHPO4, parallels the total phosphate concentra-tion. The complex MgHPO- exhibited large
variations, particularly in the uremic subj ects, inwhom it was often much increased.
2. Citrate. The incidence of hypercitremia inthe hyperparathyroid samples has been mentioned.In the two patients with hypoparathyroidism (Ta-ble III), citrate rose with the development ofvitamin D intoxication. In the patients withhypercalcemia of malignancy, half of the samplescontained elevated amounts of citrate, in accordwith previous evidence (26). In each of thesethree groups of patients, increased values for freecitrate ion concentration were frequently seen;however, total citrate was above normal withouta rise in the calculated value for free citrate in afew instances. The calculated amount of the com-plex CaCit- was always considerably smaller thanwas the total amount of complexed calcium. Thus,hypercitremia appears to be a nonspecific responseto hypercalcemia, and is usually not explicablesimply as an increase in the concentration of thecalcium citrate complex.
In renal disease (Table IV), one-sixth of thesamples exhibited modest elevations of citrate con-centration, and one-sixth contained less citratethan normal. Hypercitremia was not seen inthe three patients with secondary hyperpara-thyroidism.
3. Magnesium. Total and free ionic magne-sium concentrations were variable in renal failure.Elevated total magnesium was more frequent (50per cent) than was elevated ionic magnesium (34per cent). Although low total magnesium wasseen in only 12 per cent, low ionic magnesium wasseen in 20 per cent (Table IV). As these resultssuggest, complexed magnesium was frequently in-creased (55 per cent). Neither MgHPO, norMgCit- accounted for this increase in most cases.Percentage protein binding of magnesium wasusually normal, but was reduced in 23 per cent.No separate effect of acidosis could be discerned.
In the hypercalcemia of malignancy (Table III),total magnesium was usually reduced unless renalfailure supervened. Protein binding of magne-sium was normal in all. Complexed magnesiumwas increased in four patients, of whom threewere azotemic. Vitamin D intoxication had noclear effect on magnesium.
In primary hyperparathyroidism (Table III),total and ionic magnesium were variable, beingincreased in some and decreased in others. Com-
1464

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
plexed magnesium was usually normal, as waspercentage protein binding. Parathyroidectomyhad no definite effect on these measures. No con-sistent effect of parathyroid activity on magnesiummetabolism has been revealed by other studies(27-32).
DISCUSSION
These observations are pertinent to the state ofplasma calcium in patients who exhibit disturb-ances in protein, phosphate, or hydrogen ion con-centration or diminished renal function. Theyalso lead to certain inferences concerning the dis-turbances of calcium metabolism seen in theseconditions.
Calcium ion concentration1. In hyperparathyroidism. When percentage
protein binding of calcium is normal, calcium ionconcentration must be directly proportional toplasma calcium, unless complexed calcium is ab-normally high. In primary hyperparathyroidism,percentage protein binding is normal, and com-plexed calcium is also normal. Consequently, per-centage ionization of plasma calcium is normal;however, it does not follow that the absolute valueof calcium ion concentration is always above nor-mal limits.
Lloyd and Rose (33) reported that elevatedcalcium ion concentration is almost invariable inprimary hyperparathyroidism even when totalplasma calcium is normal. In our series, totalcalcium is above normal in 16 of 17 samples but[Ca2+] is above normal in only 7. This discrep-ancy is more apparent than real. The controlseries of Lloyd and Rose is small and uniform,the percentage ionization of plasma calcium in 7subjects varying from 65 to 69 per cent. In their16 subjects with hyperparathyroidism, percentageionization is 73 ± 5 per cent (SD), four subjectshaving values of 70 per cent or less. Total plasmacalcium in the normal subjects was 9.2 to 10.0 mgper 100 ml, but exceeded 10.0 mg in all of thepatients with hyperparathyroidism. Thus, totalplasma calcium distinguishes hyperparathyroidfrom normal subjects better than does [Ca2+] intheir study, as well as in ours. In ours, the var-iability of [Ca2+] is greater than that of totalcalcium; in theirs, variability of the control seriesis low. Apart from these differences in variabil-
ity, the two studies, as well as three other recentreports (34-36), are substantially in agreementin showing little or no difference in percentageionization of plasma calcium in primary hyper-parathyroidism as compared with normal.
2. In other forms of hypercalcemia. Patientswith hypercalcemia secondary to malignancy andthose with vitamin D intoxication also exhibiteda normal percentage ionization of plasma calcium(Figure 1), in confirmation of earlier studies (22,35). [Ca2+] was above normal in only 12 of these19 samples, although total calcium was elevated inall. Again, this is a reflection of the greatervariability in [Ca2+] than is total calcium in thenormal series. All of these subjects had symp-toms of hypercalcemia, in contrast to the patientswith hyperparathyroidism, many of whomdid not.
3. In renal failure. The usual relationship be-tween [Ca2+] and total calcium can evidentlychange in renal failure in two ways: first, a dimin-ished ability of the plasma proteins to bind calciummay occur, independent of any minor effect ofacidosis; second, complexed calcium may rise con-siderably in severe uremia. The net effect ofthese two opposing alterations on the percentageionization of plasma calcium is unpredictable, andabnormally high as well as abnormally low valuesare seen (Figure 1). The determination of[Ca2+] may be of some value, therefore, in themanagement of severe renal failure, in which thetotal plasma calcium ceases to be a good index ofthe effective calcium concentration.
[Ca] [P] ion products
Neuman and Neuman (37) assert that theproduct [Ca2+] [HPO42j varies with parathyroidactivity, being increased in hyperparathyroidism.3Rasmussen (38) has suggested that it is un-altered. The results of the present experimentsshow that the product [Ca2+] [HPO42-] is de-creased or unchanged in primary hyperparathy-roidism. A single value in untreated hypopara-
3 These authors have also emphasized the importanceof employing ion activities rather than ion concentrations.Although this is an important distinction when ionicstrength is a variable, nothing is gained by applying thiscorrection to plasma, in which ionic strength is nearlyconstant. Furthermore, the use of activities, which aredimensionless quantities, can lead to misleading conclu-sions when they are compared with concentrations.
1465

MACKENZIEWALSER
100
80:3
60- 60
5c 40U1
20
7.4 7.5 7.6 7.7pH
7.1 7.2 7.3
FIG. 5. THE RESULTS OF FOUR PUBLISHED REPORTS OF
THE EFFECT OF PLASMA PH ON PROTEIN BINDING OF
CALCIUM, PLOTTED ON THE SAME GRAPH. Line 1, fromHopkins, Howard and Eisenberg (56), was obtained on
normal human serum at 2500 C by anaerobic ultrafiltra-tion. Line 2, from Toribara, Terepka and Dewey (61),represents human serum subjected to aerobic ultrafiltra-tion at 370 C. Line 3, from Peterson, Feigen and Cris-mon (15), represents normal rabbit serum subjected toanaerobic ultrafiltration at 200 to 250 C. Line 4, fromLoken and co-workers (54), was obtained by ultracentrif-ugation of normal human serum at 370 C.
thyroidism was also normal. Although thisproduct varies twofold between different normalindividuals, it appears to be more constant in a
single subject, as indicated by the values beforeand after parathyroidectomy and by repeated de-terminations in some subjects.
The possibility cannot be entirely excluded thatparathyroid hormone acting on bone, in the ab-sence of a phosphaturic response, can increase theproduct. The two subjects with osteitis fibrosa(Rit and Sla) had the highest [Ca2+] values andalso the highest (although normal) products.
There is clearly a relationship between [Ca2+][HPO42-] and impairment of renal function. Themost reasonable hypothesis from the data is thatinhibitors of calcification accumulate in the plasmaduring the development of uremia and lead to thestabilization of this product at a higher value.This is consistent with the studies of Yendt andco-workers (5), mentioned above. Since hemo-dialysis lowered the product, one may infer thatthe inhibitors of calcification are dialyzable, as
other work has shown (39). Until the determi-nation of the ion product can be correlated witha measure of the mineralizing propensity of plasma,
this interpretation remains conjectural. Never-theless, the dependence of this product on renalfunction and its independence of parathyroid ac-tivity produces some support for the early sug-gestion (40) that plasma calcium falls in renalfailure because phosphate rises. If phosphate ac-cumulates more rapidly than inhibitors of calcifi-cation, then a fall in [Ca2+] owing to mineral depo-sition might occur.
Is the product of total plasma calcium timestotal plasma phosphate a reliable index of [Ca2+][HPO42-] ? In molar units, the latter product is0.2 to 0.3 times the former product in normal sub-jects: In the patients, this relationship was usuallymaintained, but a few samples in each groupshowed even lower values for [Ca2+] [HPPO2-1relative to the other product. In general, however,the correlation between these two products washigh.
The product [Ca2+] 3 [P043-]2 was also calcu-lated in these samples. The variability in the re-sults was very large. This increase in variabilityis not due to the estimation of [P043-], which issimply a function of [HP042-] and pH. Thevariability in the product of [Ca2+] [P043-] istherefore no greater than that of [Ca2+] [HP042-].However, the product [Ca2+]3 [PO43j2 is muchmore variable. These observations do not sup-port the view (41) that this latter product is abetter index of mineralizing propensity than is theproduct [Ca2+] [HP042-]. However, the actualeffective product remains unknown.
Protein binding of calcium
1. Role of plasma pH. Although great emphasishas been laid on the effect of plasma pH on pro-tein binding of calcium, it is doubtful whether themagnitude of this effect warrants such emphasis.In Figure 5 are summarized the results of fourstudies of this effect, recalculated and plotted soas to afford comparison. A change in pH of 0.3unit, which would represent severe acidosis or al-kalosis, is associated with a change in ultrafiltrablecalcium which amounts to approximately 6 percent of the total plasma calcium.
From the technical point of view, control of pHto within 0.1 unit or less during ultrafiltration istherefore unnecessary. Exposure of plasma to airwill of course introduce much larger changes in
4
1466

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
pH and should be avoided. However, the use of a
gas mixture having the same composition as thesubject's alveolar air, as recommended by Rose(42), seems unnecessary. The calculated venous
pCO, in our severely acidotic subjects (venouspH < 7.30) averages 30 mmHg, and the lowestvalue is 22 mmHg. Although precise pCO2 val-ues are not available because the CO2 content andpH were not determined on the same sample, theseresults establish that marked reductions of pCO2did not occur, at least in the venous blood. Eleva-tion of plasma pCO2 from 30 to 40 mmHg, (i.e.,equilibration with 5 per cent CO2 at 370 C) can
be calculated to lower plasma pH approximately0.1 unit, which does not affect protein binding sig-nificantly, as the figure shows. Furthermore, itis doubtful whether the plasma in the cellophanesac reaches gaseous equilibrium with the atmos-phere in the ultrafiltration apparatus we employed.And finally, any effect of metabolic acidosis on
protein binding would be increased rather thandecreased by using a higher pCO,. The use ofvenous rather than arterial plasma for determina-tion of protein binding of calcium is justified bythe same considerations. Since stasis was avoided,there is no reason to suppose that unusually largearteriovenous differences of pH or pCO2 occurred.
The physiological significance of alterations inprotein binding of calcium induced by pH is alsoquestionable. Fanconi and Rose (16) found thathyperventilation to extremely low pCO2 values(8 to 20 mmHg) was associated with reductionsin plasma [Ca2+] averaging 20 per cent, some ofwhich were due to rises in complexed calcium.
Much smaller reductions in pCO2 suffice to cause
tetany (43), but larger reductions in plasma cal-cium without pH change are required to producetetany as, for example, in hypoparathyroidism.In acidosis, as the results reported here indicate,plasma pH is not a major determinant of percent-age protein binding or percentage ionization ofplasma calcium. It has been shown that the hy-drogen (or hydroxyl) ion is directly concernedwith neuromuscular irritability (44), even thoughit does not affect the inotropic response of theheart to calcium ions (4). Thus, the role of plasmapH in producing tetany or protecting againsttetany is evidently a direct one, and only a minorrole can be attributed to any effect mediated byaltered protein binding of calcium.
2. Role of parathyroid hormone. McLean,Barnes and Hastings (45) showed that neitherparathyroid extract administration nor parathy-roidectomy had an effect on KCaprot in cats. InTable IX, the results of studies of protein bindingof calcium in patients with primary hyperpara-thyroidism are summarized, including studiesemploying ultrafiltration and ultracentrifugation.In only one report (33) has a significant differ-ence between normal and primary hyperparathy-roid subjects been shown. In this report the nor-
mal series included only seven subjects, and thevariability in the normal series was small. Nev-ertheless, there was some overlap between patientsand controls. As a result of the mass-law rela-tionship, a slight decrease in percentage proteinbinding of calcium results from hypercalcemiaitself. The slight difference in the mean values for
TABLE IX
Percentage protein binding of calcium in patients with primary hyperparathyroidism, according to various authors *
Hyperparathyroid Controls
Reference No. Range Mean No. Range Mean
Snell 1930 (46) 1 52 ? 40-55 ?Herbert 1933 (47) 2 43, 45 44 NoneMorison et al. 1938 (17) 2 41, 60 50 12 38-57 48Hellstrom 1953 (48) 3 33-38 34 NoneHopkins et al. 1953 (25) 9 24-39 32 10 25-35 32Thomas et al. 1958 (49) 2 30, 31 30 10 25-35 32Lloyd and Rose 1958 (33) 16 16-30 24 7 28-32 30Breen and Freeman 1961 (50) 3 38-45 40 14 44-50 46Fowler et al. 1961 (35) 5 29-40 35 20 ? 39Walser 1962 (this report) 14 34-54 44 24 36-56 47
* Percentage protein binding calculated as 100 X [1 - (UFca/Pca)], without corrections for water content or Don-nan factor.
1467

MACKENZIEWALSER
percentage protein binding in the present series(44 per cent in hyperparathyroidism versus 47 percent in controls) disappears (actually is reversed)when Kaaprot is calculated (0.0084 M in hyper-parathyroidism versus 0.0086 Min controls). Inone subject with untreated hypoparathyroidism,Kcaprot was in the high normal range (0.0113 M),indicating a low normal affinity of plasma pro-tein for calcium in the subject. Terepka, Toribaraand Dewey (10) found normal percentage proteinbinding of calcium in hypoparathyroidism. If allavailable data are considered, it appears that para-thyroid hormone has no effect on the ability ofplasma protein to bind calcium. This is also theconclusion most recently stated by Breen andFreeman (51), although they apparently feelthat their earlier report (50), cited in Table IX,confirmed the conclusions of Lloyd and Rose (33).Furthermore, three recent reports, which do notappear in Table IX because complete data for thiscomparison are not given, agree in indicating nor-mal percentage protein binding or ionization ofplasma calcium, or both, in patients with hyper-parathyroidism (34, 36, 52).
Although a specific abnormality of the electro-phoretic distribution of protein in hyperparathy-roidism was indicated by Gordan (52), no charac-teristic change was found by McGeown (53).
Colloidal calcium phosphate
Approximately 15 per cent of plasma phosphateis not ultrafiltrable in normal subjects (23).Since addition of excess EDTA to plasma beforeultrafiltration does not alter these results (23),neither calcium nor magnesium plays a role inrestricting the passage of phosphate through thecellophane membrane. It is reasonable to concludethat the nonultrafiltrable phosphate is protein-bound (subject to some uncertainty in choice ofthe correct Donnan factor). Similar conclusionshave been reached by Loken, Havel, Gordan andWhittington (54) from ultracentrifugal analysisof plasma.
When plasma phosphate is elevated, the per-centage not ultrafiltrable is unaltered (10, 23),unless very high values are produced experi-mentally (14, 55, 56), at which point the ultra-filtrability of calcium also falls. Presumably, theprecipitation of secondary calcium phosphate is
responsible. Several studies of hypercalcemicplasma have indicated that the ultrafiltrability ofphosphate may also fall sharply under these con-ditions (24, 25, 49, 56).
In one-fifth of the hypercalcemic samples exam-ined in this study, the ultrafiltrability of phosphatewas less than normal. When five of these sam-ples were subjected to ultrafiltration after the ad-dition of 4 mmoles per L of the trisodium salt ofEDTA, the ultrafiltrability of phosphate becamenormal. This observation supports the view thatprecipitation of calcium phosphate is involved. Itremains to be determined, however, whether pre-cipitation occurs in vivo or is produced by thewithdrawal and cooling of blood.
Although the methods employed in this studycan provide useful information, they are distinctlylimited as diagnostic tools in these conditions.They fail to distinguish hyperparathyroidism fromvitamin D intoxication or from the hypercalcemiaof malignancy, except in those instances of hyper-parathyroidism in which [Ca2+] [HPO42-] is be-low normal. They also fail to distinguish primaryhyperparathyroidism with renal failure from sec-ondary hyperplasia. They show no correlationwith the presence or absence of bone disease ornephrolithiasis.
It has been established that the physiologicallyeffective fraction of plasma calcium is the freeionic calcium. Calcium in the form of chelate com-plexes, such as with citrate or EDTA, is knownto be ineffective in promoting the clotting of blood,the contraction of frog cardiac muscle (57), orthe deposition of bone salt. Furthermore, cal-cium which is electrostatically associated withmultivalent ions to form ion-pair complexes is alsoineffective (58-60, 62).
Yendt and co-workers (5) found that calcifica-tion of rachitic cartilage failed to occur in someplasma samples at ultrafiltrable calcium timesphosphate products which were adequate to pro-duce calcification in artificial solutions. This ob-servation may be cited as additional evidence thatinhibitors of calcification are present in normalplasma (39). If this be so, bioassay methods in-volving mineralization of collagen or cartilagecannot yield values for "biologically active" cal-cium. Instead, they give an empirical index ofmineralizing propensity, which is the net result ofthree (or more) factors: 1) the effective calcium
1468

IONIZATION OF PLASMACALCIUM AND PHOSPHATE
concentration, 2) the effective phosphate concen-tration, and 3) the amount of inhibitors present.If 1) and 2) are known, these methods providean estimate of 3).
The only direct method for determining thephysiologically effective calcium concentration isthe frog heart technique. When applied to nor-mal plasma ultrafiltrate, this method indicates thatapproximately 90 per cent of the ultrafiltrable cal-cium is physiologically effective (17, 22). Thefree ionic calcium concentration, as measured bythe murexide method, is also about 90 per cent ofthe ultrafiltrable calcium in normal plasma (8, 16,34, 35, 42). It is reasonable to conclude that theeffective calcium concentration is identical with thefree ionic calcium.
SUMMARY
Plasma from patients with primary and sec-ondary hyperparathyroidism, hypercalcemia ofmalignancy, vitamin D intoxication, and primaryrenal failure, with and without acidosis, has beenanalyzed for total, free, and complexed calcium,magnesium, phosphate, and citrate. An attempthas been made to determine the separate effects ofparathyroid hormone, hypercalcemia itself, renalfailure, and acidosis on four indices of the state ofplasma calcium.
1. The ability of plasma protein to bind calcium,measured as KCaprot. was unaltered in primary orsecondary hyperparathyroidism or in the hyper-calcemia of malignancy. Acidosis had only a minoreffect. Renal failure itself had no effect except insome severe uremics, in whom calcium bindingwas decreased. Increased protein binding of phos-phate, seen in one-fifth of the hypercalcemic sam-ples, was eliminated by adding excess EDTA.
2. Complexed calcium was increased only in se-vere uremia. Neither phosphate nor citrate ac-counted for the increase.
3. The ion product [Ca2+] [HPO42-] was nor-mal or low in primary hyperparathyroidism andwas unaffected by parathyroidectomy in primaryor secondary hyperparathyroidism. It was in-creased in severe renal failure but was unaffectedby hypercalcemia itself. These results support thetraditional concept of reciprocal adjustments inCa and P concentrations to keep this product con-stant. with the modification that inhibitors of cal-
cification accumulating in uremia may greatlyincrease the level about which these adjustmentsoccur.
4. In accordance with these findings, the per-centage ionization of plasma calcium was normalin both primary and secondary hyperparathyroid-ism and also in other types of hypercalcemia.Some decrease was seen in severe uremia due toincreased complexed calcium. Acidosis had onlya minor effect, and the absence of tetany in acidoticuremics with hypocalcemia cannot be attributed toan increase in ionization of plasma calcium.
ACKNOWLEDGMENTS
I am greatly indebted to Dr. Robert A. Johnston, Jr.,Dr. Thomas B. Connor and Mr. Edward B. Marsh, Jr.,for assistance in obtaining some of these samples, and toDr. John Eager Howard for making it possible to studyseveral patients. Sylvia Butler, Mary Jane Ford andRoberta Kromm provided valuable technical assistance.
REFERENCES
1. Walser, M. The ionic composition of uremic plasma(abstract) . J. clin. Invest. 1959, 38, 1052.
2. Marsh, E. B., Jr., and Walser, M. Filtrable cal-cium complexes in the hypercalcemia of malignancy.Clin. Res. 1961, 9, 205.
3. Walser, M. Plasma [Ca2+] and [Ca2+] [HPO42-] inhyperparathyroidism and in renal failure. Clin.Res. 1961, 9, 338.
4. McLean, F. C., and Hastings, A. B. A biologicalmethod for the estimation of calcium ion con-centration. J. biol. Chem. 1934, 107, 337.
5. Yendt, E. R., Connor, T. B., and Howard, J. E. Invitro calcification of rachitic rat cartilage in nor-mal and pathological human sera with some ob-servations on the pathogenesis of renal rickets.Bull. Johns Hopk. Hosp. 1955, 96, 1.
6. Raaflaub, J. tVber ein photometrisches Verfahrenzur Bestimmung des ionisierten Calciums. Hoppe-Seylers Z. physiol. Chem. 1951, 288, 228.
7. Walser, M. Determination of free magnesium ionsin body fluids. Improved methods for free calciumions, total calcium, and total magnesium. Analyt.Chem. 1960, 32, 711.
8. Walser, M. Ion Association. VI. Interactions be-tween calcium, magnesium, inorganic phosphate,citrate and protein in normal human plasma. J.clin. Invest. 1961, 40, 723.
9. Annino, J. S., and Relman, A. S. The effect of eat-ing on some of the clinically important chemicalconstituents of the blood. Amer. J. clin. Pathol.1959, 31, 155.
10. Terepka, A. R., Toribara, T. Y., and Dewey, P. A.The ultrafiltrable calcium of human serum. II.
1469

MACKENZIEWALSER
Variations in disease states and under experimentalconditions. J. clin. Invest. 1958, 37, 87.
11. Martin, N. H., and Perkins, D. J. The calcium bind-ing of human serum albumin in health and dis-ease. Biochem. J. 1953, 54, 642.
12. McLean, F. C., and Hastings, A. B. The state ofcalcium in the fluids of the body. I. The conditionsaffecting the ionization of calcium. J. biol. Chem.1935, 108, 285.
13. Shelling, D. H., and Maslow, H. L. The effect ofsodium citrate, acetate, and lactate on the ultra-filtrability of serum calcium. J. biol. Chem. 1928,78, 661.
14. Walser, M. Ion Association. I. The effect of mul-tivalent anions on the protein-bound and com-plexed calcium in serum. J. cell. comp. Physiol.1960, 55, 245.
15. Peterson, N. A., Feigen, G. A., and Crismon, J. M.Effect of pH on interaction of calcium ions withserum proteins. Amer. J. Physiol. 1961, 201, 386.
16. Fanconi, A., and Rose, G. A. The ionized, com-plexed, and protein-bound fractions of calcium inplasma. Quart. J. Med. 1958, 27, 463.
17. Morison, R. S., McLean, R., and Jackson, E. B. Ob-servations on the relation between ionized andtotal calcium in normal and abnormal sera andtheir ultrafiltrates. J. biol. Chem. 1937-8, 122, 439.
18. Alwall, N. Studien uber die Regulation vom Citro-nensauregehalt des Blutserums IV: tber die Ein-wirkung von Parathormon auf den Citronensdure-gehalt des Blutserums, ein Beitrag zur Frage desZusammenhangs zwischen Calcium und Citronen-saure. Acta med. scand. 1944, 116, 337.
19. Sj6strom, P. Der Citratgehalt im Blutserum alsDiagnosticum bei Krankheiten der Leber und derGallenwege: Eine methodologische, tierexperi-mentelle und klinische Studie. Acta chir. scand.1937, 79, suppl. 49.
20. L'Heureux, M. V., and Roth, G. J. Influence ofparathyroid extract on citric acid of the serum.Proc. Soc. exp. Biol. (N. Y.) 1953, 84, 7.
21. Watson, L. Citrate metabolism in hyperparathyroid-ism. Proc. roy. Soc. Med. 1959, 52, 349.
22. Anning, S. T., Dawson, J., Dolby, D. E., and In-gram, J. T. The toxic effects of calciferol. Quart.J. Med. 1948, 17, 203.
23. Walser, M. Protein-binding of inorganic phosphatein plasma of normal subj ects and patients withrenal disease. J. clin. Invest. 1960, 39, 501.
24. Grollman, A. The condition of the inorganic phos-phorus of the blood with special reference to thecalcium concentration. J. biol. Chem. 1927, 72,565.
25. Hopkins, T. R., Connor, T. B., and Howard, J. E.Ultrafiltration studies on calcium and phosphorusin pathological human serum. Bull. Johns Hopk.Hosp. 1953, 93, 249.
26. Lemon, H. M., Mueller, J. H., Looney, J. M., Chasen,W. H., and Kelman, M. Hypercitricemia in hu-
man cancer; factors concerned in pathogenesis andtreatment. Brit. J. Cancer 1960, 14, 376.
27. Greenberg, D. M., and Mackey, M. A. The effect ofparathyroid extract on blood magnesium. J. biol.Chem. 1932, 98, 765.
28. Bulger, H. A., and Gausmann, F. Magnesium metab-olism in hyperparathyroidism. J. clin. Invest. 1933,12, 1135.
29. Agna, J. W., and Goldsmith, R. E. Primary hyper-parathyroidism associated with hypomagnesemia.A report of three cases (abstract). J. clin. Endocr.1956, 16, 973.
30. Barnes, B. A., Krane, S. M., and Cope, 0. Mag-nesium studies in relation to hyperparathyroidism.J. clin. Endocr. 1957, 17, 1407.
31. Durlach, J., Stoliaroff, M., Gauduchon, J., Leluc, R.,and Cong-Trieu, T. Studies on the relations be-tween parathyroid glands and magnesium metab-olism. Ann. Endocr. (Paris) 1960, 21, 242.
32. Scholtz, H. G. Notiz uber die Wirkung des Para-thyreoidea-Hormons auf den Magnesiumgehalt desBlutes. Naunyn-Schmiedeberg's Arch. exp. Path.Pharmak. 1931, 159, 233.
33. Lloyd, H. M., and Rose, G. A. Ionised, protein-bound, and complexed calcium in plasma in primaryhyperparathyroidism. Lancet 1958, 2, 1258.
34. Hyde, R. D., Jones, R. V., McSwiney, R. R., andPrunty, F. T. G. Investigation of hyperparathy-roidism in the absence of bone disease. Lancet1960, 1, 250.
35. Fowler, D., Fone, D. J., and Cooke, W. T. Thecalcium fractions of plasma in hypercalcaemic con-ditions and in adult coeliac disease. Lancet 1961,2, 284.
36. McSwiney, R. R., and Prunty, F. T. G. The diag-nosis of minimal hyperparathyroidism. Determina-tion of theoretical renal phosphorus threshold.Proc. roy. Soc. Med. 1961, 54, 639.
37. Neuman, W. F., and Neuman, M. W. The ChemicalDynamics of Bone Mineral. Chicago, Univ. ofChicago Press, 1958.
38. Rasmussen, H. Parathyroid hormone. Nature andmechanism of action. Amer. J. Med. 1961, 30(1),112.
39. Fleish, H., and Neuman, W. F. Mechanisms ofcalcification: Role of collagen, polyphosphates, andphosphatase. Amer. J. Physiol. 1961, 200, 1296.
40. Albright, F., and Reifenstein, E. C., Jr. The Para-thyroid Glands and Metabolic Bone Disease. Bal-timore, Williams & Wilkins, 1948.
41. MacGregor, J., and Nordin, B. E. C. Equilibrationstudies with human bone powder. J. biol. Chem.1960, 235, 1215.
42. Rose, G. A. Determination of the ionised and ultra-filterable calcium of normal human plasma. Clin.chim. Acta 1957, 2, 227.
43. Grant, S. B., and Goldman, A. A study of forcedrespiration: Experimental production of tetany.Amer. J. Physiol. 1920, 52, 209.
1470
IONIZATION OF PLASMACALCIUM AND PHOSPHATE
44. Kugelberg, E. Accommodation in human nerves, andits significance for the symptoms in circulatory dis-turbances and tetany. Acta physiol. scand., 1944,8, suppl. 24.
45. McLean, F. C., Barnes, B. O., and Hastings, A. B.The relation of the parathyroid hormone to thestate of calcium in the blood. Amer. J. Physiol.1935, 113, 141.
46. Snell, A. M. The diffusibility of the calcium in theblood serum under normal and pathologic condi-tions. Proc. Mayo Clin. 1930, 5, 17.
47. Herbert, F. K. The total and diffusible calcium ofserum and the calcium of cerebrospinal fluid inhuman cases of hypocalcaemia and hypercalcaemia.Biochem. J. 1933, 27, 1978.
48. Hellstrom, J. Observations regarding the prognosisand diagnosis of hyperparathyroidism. ClevelandClin. Quart. 1953, 20, 253.
49. Thomas, W. C., Jr., Wiswell, J. G., Connor, T. B.,and Howard, J. E. Hypercalcemic crisis due tohyperparathyroidism. Amer. J. Med. 1958, 24, 229.
50. Breen, M., and Freeman, S. The use of high centrif-ugal force in separating plasma calcium into itsprotein-bound and protein-free fractions. Clin.chim. Acta 1961, 6, 181.
51. Breen, M., and Freeman, S. Plasma calcium dis-tribution in relation to parathyroid function. Amer.J. Physiol. 1961, 200, 341.
52. Gordan, G. S. Current status of laboratory tests forhyperparathyroidism. Acta Endocr. (Kbh.) 1960,suppl. 51, 463.
53. McGeown, M. G. The value of the calcium infusiontest, tests of renal tubular function and changes in
the serum proteins in the diagnosis of hyperpara-thyroidism. Proc. roy. Soc. Med. 1961, 54, 642.
54. Loken, H. F., Havel, R. J., Gordan, G. S., and Whit-tington, S. L. Ultracentrifugal analysis of protein-bound and free calcium in human serum. J. biol.Chem. 1960, 235, 3654.
55. McLean, F. C., and Hinrichs, M. A. The formationand behavior of colloidal calcium phosphate in theblood. Amer. J. Physiol. 1938, 121, 580.
56. Hopkins, T., Howard, J. E., and Eisenberg, H. Ul-trafiltration studies on calcium and phosphorus inhuman serum. Bull. Johns Hopk. Hosp. 1952,91, 1.
57. Hastings, A. B., McLean, F. C., Eichelberger, L.,Hall, J. L., and Da Costa, E. The ionization ofcalcium, magnesium, and strontium citrates. J.biol. Chem. 1934, 107, 351.
58. Giebisch, G., Kraupp, O., Pillat, B., and Stormann, H.Die Wirkung der Sulfationen auf das Membran-potential der isoliert durchstr6mten Saugetier-muskulatur. Experientia (Basel) 1957, 13, 445.
59. Lovelock, J. E., and Porterfield, B. M. Blood clot-ting: The function of electrolytes and of calcium.Biochem. J. 1952, 50, 415.
60. Falk, G., and Landa, J. F. Prolonged response ofskeletal muscle in the absence of penetrating anions.Amer. J. Physiol. 1960, 198, 289.
61. Toribara, T. Y., Terepka, A. R., and Dewey, P. A.The ultrafiltrable calcium of human serum. I. Ul-trafiltration methods and normal values. J. clin.Invest. 1957, 36, 738.
62. Payne, J. W., and Walser, M. Ion Association. II.The effect of multivalent ions on the concentrationof free calcium ions as measured by the frog heartmethod. Bull. Johns Hopk. Hosp. 1959, 105, 298.
1471