unit three lesson 5 general surgery - rnpdcrnpdc.nshealth.ca/images/pdf/unit 3 lesson 5 general...
TRANSCRIPT

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 1
UNIT Three
Lesson 5 General Surgery
Introduction It is important for perioperative nurses to understand the processes involved with various general surgeries and respective nursing considerations. Although you will be exposed to various types of surgery during the program, the primary focus will be general surgery which will provide a foundation for all surgeries experiences. Learning Outcomes 1. Identify some of the common surgical procedures in general surgery.
2. Outline the different body cavities. 3. Differentiate between parietal peritoneum and visceral peritoneum.
4. List the layers of abdominal wall.
5. Describe some common general surgery nursing considerations.
6. Describe some of the nursing considerations when caring for a patient having
breast surgery.
7. Explain the difference between the different types of breast surgery: breast biopsy, lumpectomy, simple mastectomy, and a modified radical mastectomy.
8. Outline in detail a modified radical mastectomy.
9. Describe some of the nursing considerations when caring for a patient having hernia surgery.
10. Explain the difference between a direct and indirect hernia.
11. Outline in detail an inguinal repair-open procedure.
12. Explain the difference between the different types of bowel surgery: right hemicolectomy, right hemicolectomy, anterior resection, and an abdominal perineal resection.

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 2
13. Describe some of the nursing considerations when caring for a patient having bowel surgery.
14. Outline in detail an anterior resection-open procedure.
15. Describe some of the nursing considerations when caring for a patient having biliary surgery.
16. Describe some of the common nursing consideration when caring for a patient
having abdominopelvic surgery.
Required Readings Rothrock, J. C. (Ed.). (2015). Alexander’s care of the patient in surgery (15th ed.).
Toronto: Mosby.
• Breast Surgery, page 558-579 o Focus on pages 577-579 Modified Radical Mastectomy
• Repair of Hernias, page 383-404
o Focus on pages 392-396 Repair of Inguinal Hernia
• Gastrointestinal surgery, page 295-311 o Refer to page 297, Blood supply of the colon
• Surgery of the Colon, page 335-346
o Focus on pages 340-341 Anterior Resection
• Laparoscopic Cholecystectomy, page 360-363 (Review from Unit 3 Lesson 3D MIS)
Tighe, S.M. (2016). Instrumentation for the Operating Room - a Photographic Manual
(9th ed.). Missouri: Mosby.
• Breast Surgery: Chapter 16/17, page 84-87 • Laparotomy: Chapter 3, page 31-38 • Abdominal Retractors: Chapter 4, page 39-44 • Bowel Resection: Chapter 15, page 69-70
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 3
General Surgery Although you will be exposed to various types of surgery during the program, the primary focus will be on general surgery while touching on some of the other perioperative specialties further on in following lessons. A solid foundation in general surgery will provide you with a basis in concepts related to open procedures and minimally invasive procedures, which can then be expanded into other perioperative specialties. A surgical specialty’s name is usually determined by the anatomical areas of the body involved. For example, cardiac surgery refers to all surgical procedures involving the heart. This is usually the case for most surgeries except general surgery. The primary focus of general surgery is the gastrointestinal system; however, it may also include the breast, some head and neck, endocrine system, and some vascular depending on the surgeon’s education/training and specialty breakdown at each health care facility (Phillips, 2013). For the purposes of this program, we will include the following in our general surgery discussion: abdominal wall, the biliary tract (gallbladder and associated structures), gastrointestinal tract (stomach, colon, rectum), spleen, pancreas, and the breast for general surgery. The following table provides a few examples of some common general surgery procedures and some common indications. There are many more general surgery procedures and indications for those surgeries.
Surgical Procedure
Common Indications
Laparotomy Acute abdomen
Appendectomy Appendicitis
Small bowel resection Crohn’s disease
Large bowel resection Colon cancer or Diverticular disease
Abdominal perineal resection Rectal cancer or Crohn’s disease
Herniorrhaphy Inguinal hernia
Incisional/ventral hernia Previous abdominal surgery
Cholecystectomy Symptomatic gallstones
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 4
Segmental Resection of the Liver Benign or malignant tumor
Breast biopsy Mammographic abnormality (Diagnostic)
Mastectomy Breast cancer
Thyroidectomy Thyroid nodule
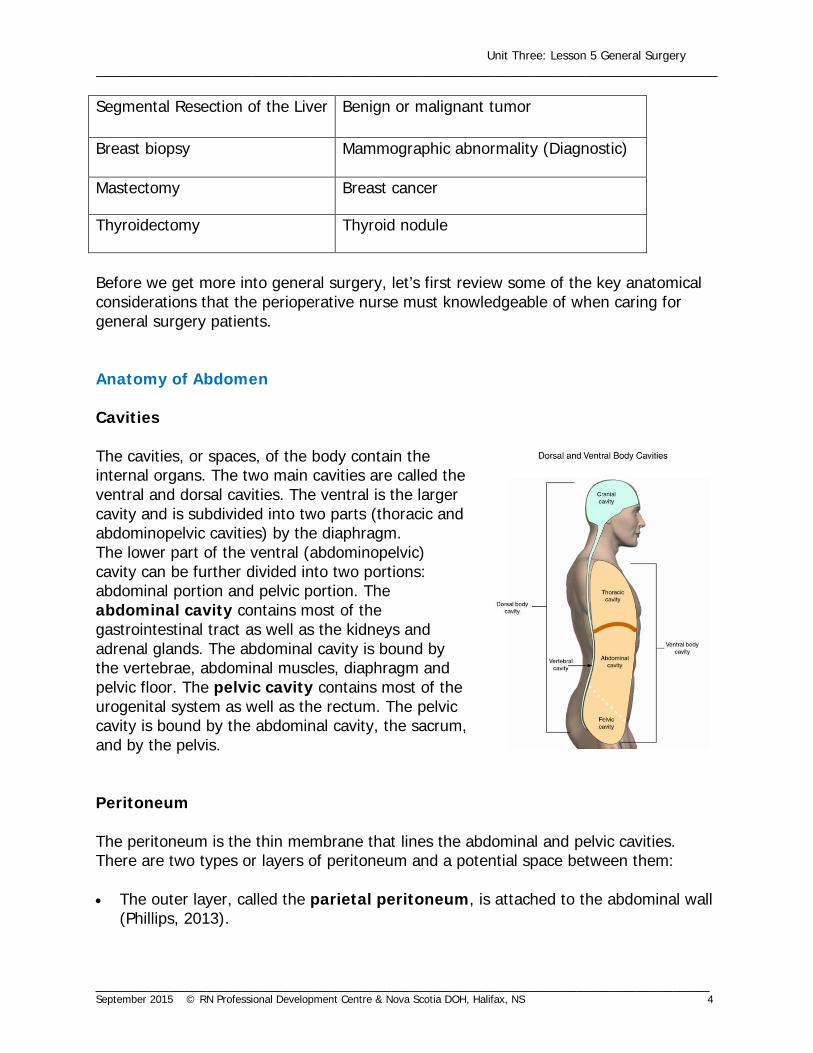
Before we get more into general surgery, let’s first review some of the key anatomical considerations that the perioperative nurse must knowledgeable of when caring for general surgery patients. Anatomy of Abdomen Cavities The cavities, or spaces, of the body contain the internal organs. The two main cavities are called the ventral and dorsal cavities. The ventral is the larger cavity and is subdivided into two parts (thoracic and abdominopelvic cavities) by the diaphragm. The lower part of the ventral (abdominopelvic) cavity can be further divided into two portions: abdominal portion and pelvic portion. The abdominal cavity contains most of the gastrointestinal tract as well as the kidneys and adrenal glands. The abdominal cavity is bound by the vertebrae, abdominal muscles, diaphragm and pelvic floor. The pelvic cavity contains most of the urogenital system as well as the rectum. The pelvic cavity is bound by the abdominal cavity, the sacrum, and by the pelvis. Peritoneum The peritoneum is the thin membrane that lines the abdominal and pelvic cavities. There are two types or layers of peritoneum and a potential space between them: • The outer layer, called the parietal peritoneum, is attached to the abdominal wall
(Phillips, 2013).

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 5
• The inner layer, the visceral peritoneum, is wrapped around the internal organs, e.g., spleen or stomach, which is located inside the intraperitoneal cavity (Phillips, 2013).
• The potential space between these
two layers is the peritoneal cavity; it is filled with a small amount of serous fluid that allows the two layers to slide freely over each other.
• The term mesentery is often used to refer to a double layer of visceral peritoneum. There are often blood vessels, nerves, and other structures between these layers. It should be noted that the space between these two layers is technically outside of the peritoneal sac, and thus not in the peritoneal cavity.
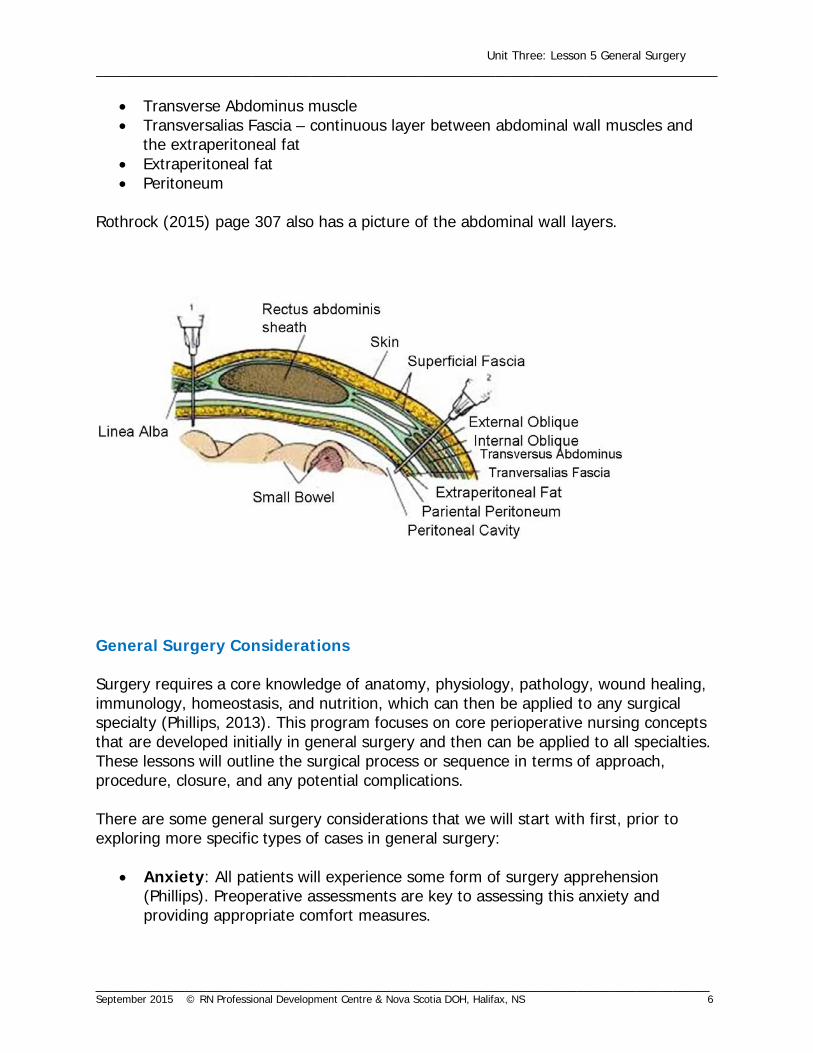
Layers of Abdominal Wall The abdominal wall consists of the following layers:
• Skin • Superficial fascia • External Oblique muscle • Internal Oblique muscle
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 6
• Transverse Abdominus muscle • Transversalias Fascia – continuous layer between abdominal wall muscles and
the extraperitoneal fat • Extraperitoneal fat • Peritoneum
Rothrock (2015) page 307 also has a picture of the abdominal wall layers.
General Surgery Considerations Surgery requires a core knowledge of anatomy, physiology, pathology, wound healing, immunology, homeostasis, and nutrition, which can then be applied to any surgical specialty (Phillips, 2013). This program focuses on core perioperative nursing concepts that are developed initially in general surgery and then can be applied to all specialties. These lessons will outline the surgical process or sequence in terms of approach, procedure, closure, and any potential complications. There are some general surgery considerations that we will start with first, prior to exploring more specific types of cases in general surgery:
• Anxiety: All patients will experience some form of surgery apprehension (Phillips). Preoperative assessments are key to assessing this anxiety and providing appropriate comfort measures.

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 7
• Foley catheter: A foley catheter may be inserted preoperatively to decompress bladder and/or monitor urinary output (Phillips, 2013). Urinary stents may also be placed prior to the start of the surgical procedure to identify the location of urinary structures for complex dissection around abdominal organs (Phillips, 2013).
• NG Tube: A NG tube may be passed by the anesthetist before or during the surgical procedure to decompress the stomach and bowel. Depending on the surgical procedure and the patient’s reaction to interventions, the NG tube may or may not be removed at the end of the procedure (Phillips, 2013).
• Positioning: The bulk of general surgery position entail supine, but lithotomy
and occasional prone positioning may be required.
• Draping: Standard draping for abdominal incisions is usually required, with occasional variances for breast and neck procedures.
• Instrumentation: Most facilities have standardized instrument sets for general surgery procedure, e.g., laparotomy (major/minor) set, breast set, bowel set, etc. With abdominal surgery, some of the surgical procedure may require deeper/longer instrumentation to reach structures deep into the abdominal or pelvic cavity.
Now let’s start with some general surgery procedures. The remainder of the lesson will focus on specific types of general surgery: breast surgery, hernia surgery, biliary, and bowel surgery. Breast Surgery Most non-cosmetic surgical procedures of the breast are performed for the treatment of cancer (Fuller, 2013).When planning for a breast procedure, there are a few considerations that the perioperative nurse must consider to provide quality care for their patient.
• Breast Tissue: Consists of glandular, connective, and fat tissue. Breast tissue is highly vascular (Phillips, 2013). The blood supply comes from the axillary, intercostals and internal mammary arteries (Phillips, 2013; Rothrock, 2015).
• Psychological state: Surgery on the breast(s) may threaten the patient’s body image and cause anxiety and depression. The patient may be emotional and/or upset and it is important for the perioperative nurse to listen, acknowledge, and provide support to her feelings (Fuller, 2013).
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 8
• Patient Markings: The surgeon may or may not mark the patient preoperatively, to distinguish the incision and/or for reconstructive purposes.
• Positioning and Draping: Usually supine, but may require some additional positioning of the affected side (e.g., elevate shoulder). Standardized draping may not provide sufficient exposure and therefore, free draping may be required. Always check with the surgeon prior to draping.
• Radiology: Mammography films or other imaging films may accompany the patient, or may be required to pull up in the diagnostic imaging system in the OR room.
• Anesthesia: The smaller breast procedures may be done with local, local and IV sedation, a LMA, or general anesthetic. It depends on the patient and their assessment with the anesthetist. The more complex breast surgeries (e.g., mastectomies) are usually done under general anesthesia.
• Instrumentation/Surgical Supplies: Some of the specific instrumentation (in
addition to standard instrumentation-scissors, hemostats, kellys, right angle clamps/gallbladders, forceps, etc.) required for breast surgery may be:
o Retractors: Senn/rakes (sharp or dull) Skin hooks Richardsons
o Hemoclips/ties/reels o Drains (e.g., hemovac, penrose)
• Surgical Counts: Usually only a small count of sponges, sharps, and
miscellaneous items is required as a cavity is not entered during breast surgery. Instruments are not usually counted. However, if there is a potential to lose an instrument during the case, an instrument count may be performed.
In general, what is the connection between the type of tissue and the type of instrumentation for breast surgery? Breast tissue consists of fat slippery tissue, therefore, breast procedures require instrumentation that can grasp and not slip. Hence, retractors like senns, skin hooks, and sharp rakes are frequently used. Hemoclips and/or ties are used due to the vascular nature of the tissue. Before we get into each type of breast procedure, please refer to Rothrock (2015) page 569 for a sample plan of care for a breast procedure.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 9
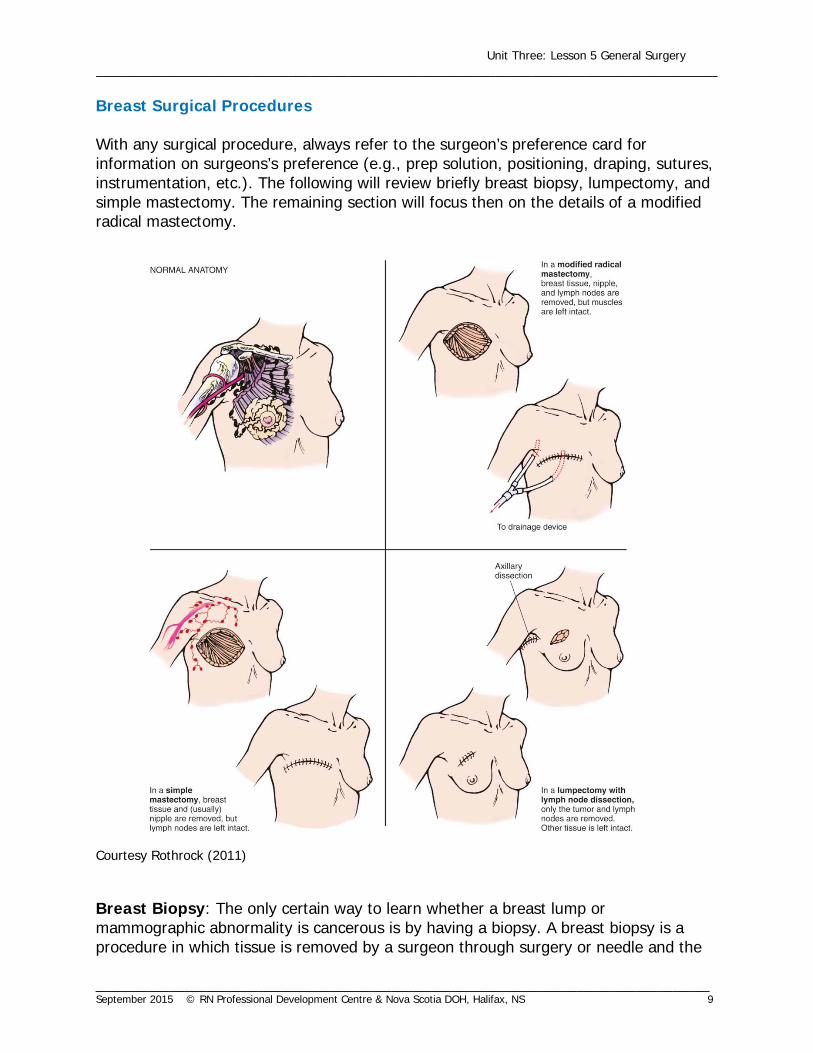
Breast Surgical Procedures With any surgical procedure, always refer to the surgeon’s preference card for information on surgeons’s preference (e.g., prep solution, positioning, draping, sutures, instrumentation, etc.). The following will review briefly breast biopsy, lumpectomy, and simple mastectomy. The remaining section will focus then on the details of a modified radical mastectomy. Courtesy Rothrock (2011) Breast Biopsy: The only certain way to learn whether a breast lump or mammographic abnormality is cancerous is by having a biopsy. A breast biopsy is a procedure in which tissue is removed by a surgeon through surgery or needle and the
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 10
specimen is examined in pathology. The surgeon’s choice of biopsy technique depends on such things as the nature and location of the lump, as well as the patient’s general health. A breast biopsy can either be excisional or incisional. An excisional biopsy removes the entire lump or suspicious area. It is similar to a lumpectomy in that it removes the lump and a margin of surrounding tissue. An excisional biopsy may be performed in the outpatient department of a hospital or a day surgery procedure in the operating room. An incisional biopsy removes only a portion of the tumor (by slicing into it) for the pathologist to examine. Incisional biopsies are generally reserved for tumors that are larger. Lumpectomy (Segmental Mastectomy): A wedge or quadrant of the breast tissue is removed. The wedge includes the tumor mass and the lobe in which it was growing. It may be combined with an axillary node dissection and radiation (Phillips, 2013). Simple Mastectomy: The entire breast is removed without lymph node dissection (negative lymph nodes) for extensive benign disease or if the tumor is believed to be only in the breast tissue. Modified Radical Mastectomy: The term modified encompasses various techniques but all include the removal of the entire breast in addition to the axillary lymph nodes after a confirmed invasive tissue diagnosis. The underlying major pectoral muscle is left in place; however, the minor pectoralis muscle may or may not be removed. Radical Mastectomy: The breast is removed along with the axillary lymph nodes, pectoral muscles, and all adjacent tissues, after a more invasive diagnosis. Other Types of Breast Procedures Needle/Wire Localization: Insertion of a fine wire/hook needle into the breast mass in Mammography or Ultrasound. Once this is completed the patient and mammograpghy films are transported to the OR. The breast mass, including the wire, and original mammography films are removed carefully and sent back to mammography for comparison, and then on to Pathology for examination. Sentinel Lymph Node Biopsy: Radioactive material is injected into the breast mass or nearby, usually in Nuclear Medicine prior to patient coming to OR. The patient is transported to OR, with a Geiger counter and the patient is injected with a blue dye once in the OR. This procedure allows identification of the lymph nodes that take up the blue dye. The nodes are excised and will determine the need for additional or more
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 11
extensive surgery (Phillips, 2013). This procedure is done on patients thought to have a low to moderate risk for involvement of lymph nodes (Rothrock, 2015). Modified Radical Mastectomy Surgical Procedure • Surgical safety checklist is performed.
• Under general anesthetic, the patient is positioned in supine. The involved arm
is abducted no greater than 90 degrees on a padded armboard.
• Approach: An elliptical incision, with lateral extension towards the axilla, is made with a #10 or # 21 blade (depending on surgeon preference) through the skin and subcutaneous tissue. The initial skin incision should only be a centimeter or so deep as the skin flaps will require careful elevation. Skin hooks or senn retractors are used to elevate the skin flaps and bleeding points are controlled as the dissection progresses (Rothrock, 2015). Bleeding may be controlled at this point with electrocautery, hemoclips, or ties.
Refer to Page 578 in your required text Rothrock (2015) for illustrations.
• Procedure: The surgeon proceeds to release the skin from the underlying
breast tissue starting superiorly to the clavicle, moving inferiorly to the rectus fascia, medially to the sternum, and laterally to the latissimus dorsi muscle, using a #10 blade or cautery. Clips may be used to control bleeding of any large vessels.
• Now the breast and pectoralis fascia are resected, using cautery or blade,
starting near the clavicle and extending downward over the mid-portion of the sternum taking care not include any muscle in the specimen. Branches of the internal mammary artery must be clamped and ligated with ties.
• The axillary flap is retracted upward using a right-angle retractor in beginning
the dissection of the axilla. Forceps, metzenbaum scissors and/or a #15 blade are used with vessel clips to avoid damage to the axillary vein and the medial and lateral nerves of the pectoralis major muscle. Hence, care is taken to avoid injury to the nerve supply to various muscles.
As a scrub nurse, be aware that if the surgeon is using a #15 blade, it may be changed frequently to ensure precise dissection in the axilla. This is surgeon preference to use a blade, cautery, or scissor for dissection.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 12
• Fascia is dissected from the lateral edge of pectoralis minor and several veins are ligated as they come off the axillary vein. A lot of hemoclips are used in the axillary dissection. As a scrub nurse, always have your clip appliers loaded.
• Fascia over the serratus anterior muscle is dissected free and the axillary fat and
lymph nodes are mobilized off the chest wall, taking care to avoid the long thoracic nerve and thoracodorsal nerves.
Refer to the illustration on page 576 of Rothrock (2015) for axillary dissection.
• The specimen is freed from the latissimus dorsi muscle and finally the suspensory
ligaments in the axilla. The specimen can be handed off the field.
As a circulating nurse, always check with the surgeon regarding the description and care of the specimen.
• The site is inspected for any bleeders, which are ligated and the two major
nerves, long thoracic and thoracodorsal, are checked to be certain they are free. The wound may be irrigated with normal saline, however, some surgeons may prefer sterile water as it lessens the survival of cancerous cells (Phillips, 2013; Goldman, 2009). Always check with the surgeon regarding this preference for irrigation solution.
• Closure: Drains (e.g., Hemovac, JP drain, etc.) may be inserted for drainage
through stab wounds. The ends are generally placed in the lower flap posteriorly and secured with a 2-0 or 3-0 non-absorbable suture.
• The dermal layer may be approximated with an absorbable taper suture. There
is controversy on whether the skin should be closed using an absorbable running suture, a non-absorbable interrupted suture, or staples. The dressing can be a thin Mepore type or a bulky gauze dressing, and also a dressing for the drain.
Repair of Hernias A hernia is the protrusion of an organ or part of an organ through a defect in the supporting structure that normally contains it (Phillips, 2013). Hernias can be classified as inguinal, femoral, umbilical, incisional, or epigastric (Rothrock, 2015). Hernias in any of these can be reducible or irreducible. A reducible hernia is when the hernia contents can be returned to the normal cavity by manipulation (Phillips, 2013). An irreducible or incarcerated hernia cannot be returned to its normal cavity. For example, bowel may be incarcerated but also may lack blood
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 13
supply or may become obstructed, which is then known as strangulated hernia (Phillips, 2013).
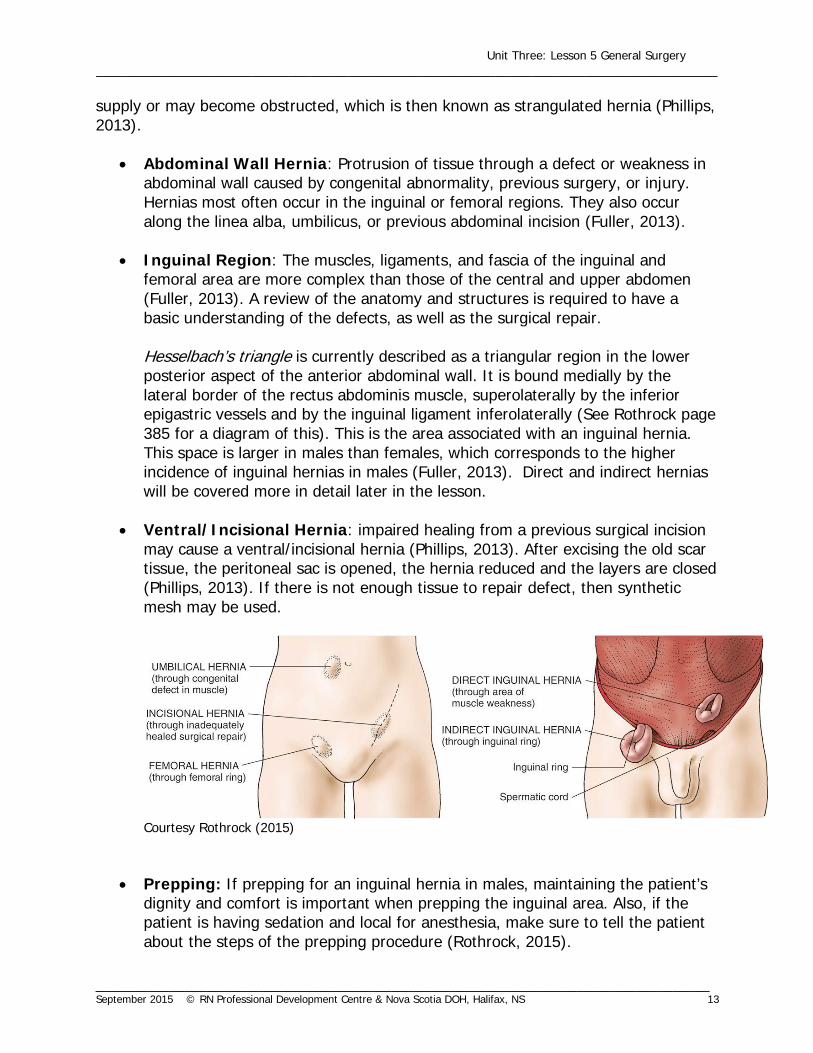
• Abdominal Wall Hernia: Protrusion of tissue through a defect or weakness in
abdominal wall caused by congenital abnormality, previous surgery, or injury. Hernias most often occur in the inguinal or femoral regions. They also occur along the linea alba, umbilicus, or previous abdominal incision (Fuller, 2013).
• Inguinal Region: The muscles, ligaments, and fascia of the inguinal and femoral area are more complex than those of the central and upper abdomen (Fuller, 2013). A review of the anatomy and structures is required to have a basic understanding of the defects, as well as the surgical repair. Hesselbach’s triangle is currently described as a triangular region in the lower posterior aspect of the anterior abdominal wall. It is bound medially by the lateral border of the rectus abdominis muscle, superolaterally by the inferior epigastric vessels and by the inguinal ligament inferolaterally (See Rothrock page 385 for a diagram of this). This is the area associated with an inguinal hernia. This space is larger in males than females, which corresponds to the higher incidence of inguinal hernias in males (Fuller, 2013). Direct and indirect hernias will be covered more in detail later in the lesson.
• Ventral/Incisional Hernia: impaired healing from a previous surgical incision
may cause a ventral/incisional hernia (Phillips, 2013). After excising the old scar tissue, the peritoneal sac is opened, the hernia reduced and the layers are closed (Phillips, 2013). If there is not enough tissue to repair defect, then synthetic mesh may be used.
Courtesy Rothrock (2015)
• Prepping: If prepping for an inguinal hernia in males, maintaining the patient’s
dignity and comfort is important when prepping the inguinal area. Also, if the patient is having sedation and local for anesthesia, make sure to tell the patient about the steps of the prepping procedure (Rothrock, 2015).

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 14
• Surgical Mesh: Synthetic material made of similar material to suture material (e.g., Prolene, Dacron, Mersilene). Mesh provides a bridge of strong material over the abdominal wall weakness. During healing, scar tissue forms in the space of the mesh. Mesh is available in sheets or patches in a variety of shapes and sizes. Mesh is a surgical implant, and therefore, requires special handling and documentation (see Lesson on Specimen & Implants)
• Anesthesia: Choice of anesthesia depends on the patient’s condition, planned surgical procedure, and an assessment by anesthesia. Some surgeons may prefer for a scheduled open inguinal hernia to be repaired under sedation and local. The choices for hernia surgery may be general, inguinal nerve block, spinal/epidural, regional with sedation, or a local with sedation (Rothrock, 2015).
• Instrumentation/Surgical Supplies: Some of the specific instrumentation (in
addition to regular open or MIS instruments) required for hernia surgery may be: o Self retainer/weitlaner retractor o Moistened penrose drain/umbilical tape o Sponges (peanuts, 4x4, etc.) o Laparoscopic: tacking stapler, balloon dissector
• Surgical Counts: As there is a chance of entering the peritoneal cavity during a
hernia repair, a full count, including an instrument count is done at the beginning of the procedure. If the cavity was not entered during the case, then only a small count (sponges, sharps, misc.) is required. Always check facility P&P.
Before we get into the inguinal hernia, please refer to Rothrock (2015) page 388 for a sample plan of care for a patient having surgery for repair of a hernia. Inguinal Hernias An inguinal hernia is a protrusion of tissue or a loop of bowel through an opening in the wall of the abdominal cavity where the lining of the abdominal cavity becomes the hernia sac. A hernia can be classified as direct or indirect. A direct hernia is usually related to heavy lifting, chronic coughing, or straining. The hernia sac exits through the transversalis fascia (abdominal wall) protruding into the inguinal canal but not into the spermatic cord. This area is associated with Hesselbach’s triangle (Phillips, 2013). The direct hernia almost always occurs in the middle-aged and elderly men because their abdominal walls weaken as they age. An indirect hernia is generally a congenital defect where the hernia (peritoneal) sac exits at the internal inguinal ring and may pass with the spermatic cord down the inguinal canal, outside of Hesselbach’s triangle (Phillips, 2013). An indirect hernia is the
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 15
most common type of groin hernia. An indirect inguinal hernia may occur at any age but becomes more common as people age, from a congenital defect in the floor of the inguinal canal (Phillips, 2013). Refer to page 384 Rothrock (2015) Fig. 13-1 for the different types of abdominal hernias. There are different types of repairs; however, a common type done today is the Mesh-Plug repair using the Perfix Plug. A plug repair requires less overall dissection, produces a tension-free repair, and has a lower recurrence rate. Using the Mesh Plug, repair of the hernia sac--direct or indirect, is rarely opened except for incarcerated or sliding hernias. Refer to page 395 in Rothrock (2015). Inguinal Hernia Surgical Procedure-Open
The inguinal hernia repair can be done easily with a local anesthetic but some are still done under general with local infiltration for post-op pain control. The patient is positioned in supine with both arms out on arm boards and a pillow under the knees to reduce the tension in the inguinal area. The area is prepped with betadine or CHG according to the surgeon’s preference for antimicrobial solutions and any patient allergies.
A full count is required at the beginning of the repair as there is always the possibility of entering the peritoneum. • Surgical safety checklist is performed.
• Approach: The initial transverse inguinal incision is made using a #10 blade and
is located 1-2 cm above and parallel to the inguinal ligament which follows the crease where the abdomen meets the thigh.
• Procedure: The superficial and deep fascias are incised using cautery to the
level of the external oblique aponeurosis which is then opened along its fibers to the external inguinal ring. Care must be taken to avoid the ilioinguinal nerve. Hemostasis may achieved using cautery or fine (2-0 absorbable) ties.
Anatomy note: Refer to Rothrock (2015) page 386 Fig 13-5.
• Surgical exposure is obtained by using a Weitlaner self-retaining retractor or
Richardson right angle retractors.

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 16
• The cremaster muscles are continuous with the internal oblique muscles and form an envelope around the spermatic cord. The cord is exposed using sharp dissection with Metzenbaum scissors and toothed forceps.
• The spermatic cord is freed using gentle dissection with a peanut or fingers. A
moistened penrose or umbilical tape (if patient has latex allergy) is used to gently retract the cord which contains vessels and the vas deferens. If the hernia is indirect, then the hernia sac is dissected out from the cord structures (may use metzenbaum scissors) and carefully dissected up to the internal ring.
• If the sac is to be opened, it is carefully opened with a metzenbaum scissor as a
portion of bowel could be in the sac. Hemostats are used to grasp the sac edges and hold it open. The contents of the indirect sac are reduced back into the abdominal cavity. Direct sacs do not usually need to be opened as they will usually reduce back into the abdominal cavity.
• The internal ring is the area where the plug is to be placed for an indirect hernia
and the floor of the defect is the area where the plug is placed for a direct hernia. Generally, a large or extra large mesh plug is used and sometimes two plugs are required to fill the defect. The cone shape of the plug and the mesh petals allow it to fit the contour of the defect. A heavy non-absorbable suture, usually 0 or 1 Prolene/Surgipro (may differ between surgeons), is used to fix the plug in place using interrupted sutures. Usually several sutures are required. Care must be taken to avoid the epigastric vessels.
• A second piece of flat mesh (patch) may be used for reinforcement. The
technique used with this patch will vary between surgeons. It may be cut with straight scissors to match the shape of the inguinal canal and is placed on the anterior surface of the posterior inguinal canal wall. The proximal end is split to allow an opening for the spermatic cord and the mesh tails are brought together with the same heavy non-absorbable suture.
Refer to page 396 in Rothrock (2015) for a diagram of mesh placement.
• Closure: The spermatic cord structures are placed on top of the flat mesh and the external oblique fascia is re-approximated over the structures with a running, absorbable suture (e.g., 2-0 Vicryl/Polysorb)
• A subcuticular absorbable running stitch is used to close skin (e.g., 3-0 or 4-0).
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 17
Inguinal Hernia Surgical Procedure-Laparoscopic Laparoscopic hernia repair are done using two techniques:
1. Transabdominal preperitoneal (TAPP) repair 2. Total extraperiotoneal (TEP) repair
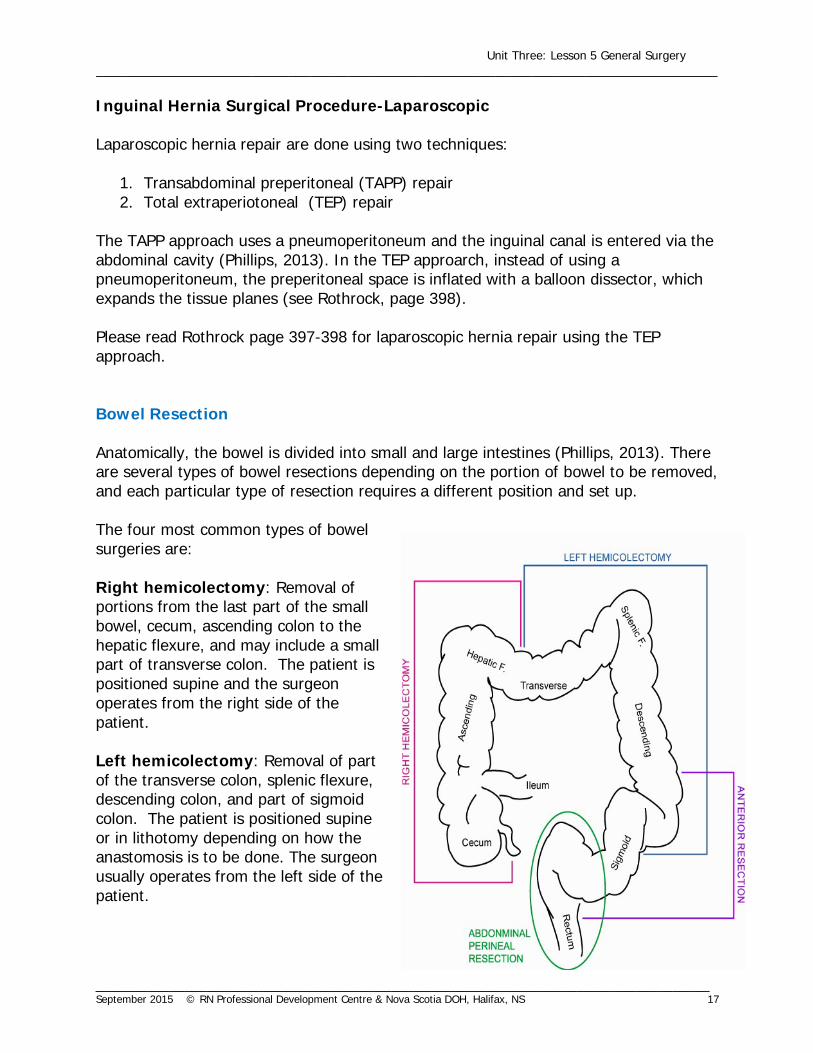
The TAPP approach uses a pneumoperitoneum and the inguinal canal is entered via the abdominal cavity (Phillips, 2013). In the TEP approarch, instead of using a pneumoperitoneum, the preperitoneal space is inflated with a balloon dissector, which expands the tissue planes (see Rothrock, page 398). Please read Rothrock page 397-398 for laparoscopic hernia repair using the TEP approach. Bowel Resection Anatomically, the bowel is divided into small and large intestines (Phillips, 2013). There are several types of bowel resections depending on the portion of bowel to be removed, and each particular type of resection requires a different position and set up. The four most common types of bowel surgeries are: Right hemicolectomy: Removal of portions from the last part of the small bowel, cecum, ascending colon to the hepatic flexure, and may include a small part of transverse colon. The patient is positioned supine and the surgeon operates from the right side of the patient. Left hemicolectomy: Removal of part of the transverse colon, splenic flexure, descending colon, and part of sigmoid colon. The patient is positioned supine or in lithotomy depending on how the anastomosis is to be done. The surgeon usually operates from the left side of the patient.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 18
Anterior resection: Removal of lesions in the lower descending colon, sigmoid, and rectosigmoid. The patient is positioned in lithotomy and the surgeon operates from the left side of the patient. A separate smaller sterile table is usually set up with a sigmoidoscope, a hemostat, and the lower part of the end-to-end anastomosis (EEA) stapler, in addition to the larger sterile back table. Note: The anus is considered dirty even after prepping with 10% betadine. Once the surgeon goes down to the bottom and uses the bottom table he/she must re-gown and glove prior to returning to the upper sterile abdominal field. Any surgical instruments or items (e.g., sponge, hemostat) that were used on the bottom cannot be used for the upper sterile abdominal field (Rothrock, 2015).
Abdominal perineal resection: Removal of lesions in the low rectosigmoid, rectum, and anus. Part of sigmoid colon and the entire rectum is removed. The patient is positioned in lithotomy and the surgeon operates from the left side of the patient. A separate sterile table of instruments and a scrub nurse is required for the instruments to be used on the anal end of the surgery. The anal end of the surgery can be done simultaneously if an assistant/extra scrub nurse is available. If the extra surgical team members are not available, the team can move to the lower table after the upper sigmoid resection is complete. It is expected that one person remains sterile to assist from above. Once the anal end is complete and the surgical team moves back up the upper sterile abdominal field, new gowns and gloves must be donned. Note: A separate count is required for the lower table for an open abdominal perineal resection along with a separate kick bucket for discarding sponges. Therefore, the procedure will require two separate counts and two separate kick buckets. Always check your facility P&P. Bowel Considerations
• Bowel Prep: Patients who are coming to the operating room for bowel surgery may be required to have a certain bowel preparation prior to surgery. It is important for the circulating perioperative nurse to assess any bowel prep (e.g., bowel cleansing methods and/or diet restrictionsclear liquids) prior before taking the patient into the operating theatre. Bowel cleaning can cause depletion of electrolytes and is performed only as necessary as per the surgeon’s preoperative orders based on the surgical procedure and the patient’s condition (Phillips, 2013).
• NG Tube and Urinary Catheter: These may be placed for bowel surgery depending on the surgical procedure, surgeon preference, and patient condition.

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 19
• Blood Supply: The mesentry, a peritoneal fold, attaches the small and large bowels to the posterior abdominal wall and contains arteries, veins, and lymph nodes that supply the intestines (Phillips, 2013). See Rothrock page 297 for a diagram of the blood supply of the bowel.
• Patient Condition: It is important to check the complete blood count (CBC) on patients undergoing bowel surgery as certain tumors can be bleeding and blood products should be administered prior to surgery. These clients may also be malnourished and receive total parental nutrition (TPN) to improve their nutritional status prior to surgery. Steroid and antibiotic therapy are also common medical interventions and should be maintained intraoperatively.
• Mobilizing Bowel: a technique of clamping the tissue, cutting it, and tying it, is
used to mobilize sections of bowel (Fuller, 2013). The GI tract is a continuous “tube” attached to abdominal and pelvic wall. The attachments limit mobility of sections in abdominal cavity and help prevent obstruction (Phillips, 2013). To transform a section of bowel, the surgeon must free up portions of these attachments (mesentry and omentum) (Fuller, 2013). This clamp/clamp/cut/tie technique is used to do this.
• Bowel Technique: It is important to remember that, if the bowel is perforated
with any instrument during any type of bowel resection, then that instrument should be isolated or handed off the sterile field. If the stapler is inserted into the bowel for an anastomosis, it should be isolated or passed off. Please refer to Rothrock (2015) page 304 for review of “contamination” during bowel cases. If there is gross spillage, the wound classification changes from clean-contaminated to contaminated or dirty and the wound should be irrigated and areas of contamination should be covered.
• Instrumentation/Surgical Supplies: Some of the specific instrumentation (in
addition to regular open or MIS instruments) required for bowel surgery may be: o Retractor
Bookwalter, balfour, etc. o Non-traumatic and non-performating instruments for bowel
Babcocks, allis, bowel clamps Debakey forceps
o Poole suction for irrigation o Surgical Staplers (please review Unit 2 Lesson 3B Wound Healing and
Closure)- open and MIS procedures o Possible harmonic scalpel or ligasure
Before we get into the open anterior resection, please refer to Rothrock (2015) page 301 for a sample plan of care for a patient having surgery for bowel surgery.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 20
Anterior Resection: Triple Stapling Technique- Open • Surgical safety checklist is performed.
• Under general anesthetic with an endotracheal tube in place and a urinary
catheter indwelling, the patient is placed in lithotomy using a boot-type stirrup (e.g., yellow fins). When performing both abdominal and perineal skin prep, the perineal area is prepped first. Preps are performed sequentially and not simultaneously, with a new prep kit for each area (Phillips, 2013).
• Approach: A long, midline skin incision is required which is made with a #10
blade and runs from just above the symphysis to the left side and slightly above the umbilicus. After the initial skin incision, cautery is generally used to incise the subcutaneous, fascia, and the rectus abdominus muscle. Right angle retractors are used to provide surgical exposure. The linea alba is identified, freed of fat, and incised in the midline. Bleeding vessels are clamped with forceps or hemostats and then tied or cauterized.
• Procedure: The peritoneum is identified and lifted with two hemostats to tent it
away from the abdominal contents. It is incised with a #10 blade and extended with metzenbaum scissors or cautery. The sides of the peritoneum are retracted using kocher clamps while the incision is extended. Once the peritoneum is opened, the surgeon takes the time to explore the liver and upper abdomen for metastasis and the bowel for respectability of the lesion. An area of the sigmoid colon is generally elevated and the small bowel is packed off with wet sponges/tapes and a self-retaining retractor, such as a Balfour, is put in place.
• The patient may be positioned slightly in Trendelenberg if greater surgical exposure is required. The scrub nurse may require a stepping stool to keep within the sterile field and the mayo stand may need to be adjusted as the legs of the patient raise.
• Peritoneal attachments are divided from around the sigmoid colon with
metzenbaum scissors and non toothed forceps and/or blunt finger dissection. Branches of the inferior mesenteric artery and vein are ligated with 2-0 absorbable ties using a clamp, clamp (hemostats), cut (metzenbaum scissors) and tie technique. The technique used is a clamp, clamp, cut, tie approach. The general rule is if you clamp with Hemostats, you tie with 2-0 ties and, if you clamp with Kellys, you tie with 0 ties. The ureters must be identified before any vessels are divided to avoid damage.
• The mesentery of the left colon is marked with electrocautery at the point of
division and the blood supply is ligated and divided. Care must be taken to avoid

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 21
tension on the splenic flexure as bleeding can occur and, if the spleen is torn, an incidental splenectomy may need to be performed.
• The wall of the bowel needs to be cleaned of fat. It cannot be too thick as the
entire circumference of the bowel may not fit into the end-to-end anastomosis stapler (EEA). A 3-5 cm margin above the tumor is clamped with Kelly’s or Bowel Clamps.
• The surgeon will chose an appropriate sized linear stapler and the circulating
nurse will open to the sterile field. The linear stapler is then applied to the sigmoid portion, above the Kelly or Bowel Clamp. The linear stapler is fired and a blade is used to cut along the edge of the stapler. This creates a double row of staples across the rectosigmoid portion while leaving the sigmoid end open with the Kelly clamp across it.
• The upper end of the sigmoid bowel should be brought down to the rectal end to
verify the adequacy of free bowel and to ensure a tension-free suture or staple line.
• The rectosigmoid section is then resected. The bowel must have a clear margin
of 5 centimeters below the tumor in the presacral area. Surgical exposure may be obtained with a hand held retractor which is held by an assistant positioned between the patient’s legs. The bottom of the laparotomy sheet covers the anal area.
• If the tumor is high enough, the rectum can be clamped with Kelly’s or bowel
clamps. The rectal section is then divided with the linear stapler (could also use a linear cutter-surgeon preference) and a #10 blade on a long handle is used to divide the rectal section and the surgical specimen is handed off. This leaves a double row of staples across the rectal portion of the rectosigmoid.
• Babcock clamps are used to grasp the bowel edges on the surgeon returns to the
sigmoid portion and blunt sizers may be used to determine the size of EEA stapling device to be used.
See Rothrock (2015), page 339 for a diagram of the EEA. • If the surgeon chooses to use a purse-string option, then a non-absorbable 2-0
suture (e.g., Prolene) may be used to secure with the anvil from the EEA stapler inside the sigmoid portion. See Figure 11-28 (a) page 339 and Figure 7-6 page 194 in Rothrock (2015) for images of a purse-string.
• If the surgeon chooses to use another firing (re-load) of the
linear stapler, then the anvil from the EEA (with sharp trocar
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 22
attached) is positioned inside the sigmoid portion and the stapler fired. This leaves a double row of staplers with the anvil inside the sigmoid section. The sharp point of the anvil is then pushed through the stapler line, leaving the shaft of the anvil poking through the sigmoid section.
• The assistant then goes to the bottom, dirty area and
gently dilates the anus and inserts the end of the straight or curved stapling device using some lubrication. The surgeon assists from above and guides the anvil in place connecting to the end of the stapler, assuring orientation and placement. The mucosal layer is checked for completeness to ensure there are no gaps. The stapling device perforates through the linear staple line on the rectum.
• The stapler is tightened to the desired thickness and the instrument is fired,
putting in place a circumferential staple line, which creates an anastomosis of the bowel wall. The instrument is carefully released and removed so as not to disrupt the staple line. Some surgeons may prefer to reinforce the staple line with interrupted 3-0 absorbable (taper) sutures.
• The stapler is opened on a separate table for the dirty area and the two
‘doughnuts’ are removed with a hemostat and inspected for a complete circle. Warm saline is placed in the abdomen by the clean surgical team and a sterile sigmoidoscope is passed up the rectum by the dirty assistant who injects air. The sterile team observes for any air bubbles indicating a leak in the anastomosis, which must be closed with absorbable interrupted sutures (Rothrock, 2015).
If the surgeon has any doubt about the security of the anastomosis, a temporary colostomy may be considered. The wound is irrigated with warm saline.
• Closure: Fascia and muscle layers are closed with a heavier absorbable suture
(e.g., 1 PDS) in a mattress fashion. • The skin is approximated with adson or bony forceps and skin clips are applied
with a stapler. The area is cleaned and dried and a dressing is applied. Laparoscopic Bowel Surgery While this lesson has discussed general surgery in terms of “open” abdominal cases, keep in mind that minimally invasive surgeries are becoming more popular and the above mentioned bowel resections may also be performed laparoscopically. Please refer to Rothrock (2015) page 338-340 for laparoscopic bowel and Tighe page 68.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 23
As mentioned in the Minimally Invasive Surgery lesson, there is always a chance the the MIS case may convert to an open procedure. Therefore, the circulating and scrub nurses must always be prepared for an open procedure. Biliary Surgery The biliary system includes the gallbladder, hepatic ducts, common bile ducts, and cystic ducts. The function of this biliary system is to produce, store, and release bile which stimulates peristalsis in the small bowel during digestion. Bile is formed in the liver and stored in the gallbladder (Fuller, 2013). A laparoscopic cholecystectomy is the most common surgical intervention for cholelithiasis (presence of gallstones) and cholecystitis (inflammation of the gallbladder).
• Preoperatively, the patient must be informed of the possibility of conversion to an open cholecystectomy and this should also be reflected in the surgical consent.
• The most common complication of a laparoscopic cholecystectomy is nausea and vomiting. It is also important for the patient to have support for 24 hours post operatively upon discharge from the hospital.
• The positioning of the equipment required for laparoscopic work will define the
work area for the surgical team (see Tighe page 62). For patient safety, the monitor screen and insufflator must be within the surgeon’s view. Each facility has different equipment and therefore, the setup may vary slightly.
• Intraoperative cholangiograms may be done during the procedure. This
comprises imaging studies in which a contrast medium is injected into the biliary ducts to detect gallstones or a stricture (Fuller, 2013).
Please review the laparoscopic cholecystectomy procedure outlined in Unit 3 Lesson 3D Minimally Invasive Surgery.

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 24
Nursing Considerations of the Patient Having Abdominopelvic Surgery No procedure is routine and unexpected outcomes can occur even when planning has been done under the most optimal conditions (Rothrock, 2015). 1. Wound Sepsis: The abdominal wall is particularly susceptible to infection.
Many abdominal surgery cases involve opening into the intestinal tract, which is full of pathogenic organisms. Therefore, every effort must be taken to protect the abdominal incision (Phillips, 2013).
These include: • Adequate skin preparation • Proper use of skin towels • Proper draping • Preoperative prepping of the bowel, if required (e.g., bowel prep, emptying) • Proper surgical aseptic technique
2. Exposure: The loops of the small and large intestine create problems related to
optimal surgical exposure. There are many deep abdominal folds which make it difficult to obtain adequate exposure and lighting. Measures that can improve abdominal exposure include: • Proper packing of intestinal loops with laparotomy sponges or tapes. • Correct use of self-retaining and other retractors. • Use of additional spot lights or head lights. • Bed positioning to use gravity to move internal organs.
3. Wound Closure: The abdominal incision is subjected postoperatively to many
stresses during breathing, coughing, and straining. Wound dehiscence is more frequent in abdominal pelvic surgery than in any other surgical region. Measures used to decrease wound dehiscence include:
• Attention to nutritional deficiencies preoperatively. • Meticulous wound closure. • Wound splinting during deep breathing or coughing. • Post-operative appliances (e.g., abdominal binder) to assist with maintaining
wound stability.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 25
4. Postoperative Complications: Some postoperative complications may include:
• Postoperative ileus which is an impairment of gastrointestinal motility and function. It is characterized by abdominal distension and pain, nausea and vomiting, reduced desire to eat, and an inability to pass flatus or stool.
• Postoperative atelectasis which is an abnormal condition characterized by the collapse of lung tissue, preventing the respiratory exchange of carbon dioxide and oxygen.
• Urinary retention • Wound infection • Postoperative bleeding
5. Impact on Respiratory Function: The greatest impact of the surgical
procedure on respiratory function is seen with procedures involving the upper abdomen. Reduced respiratory function is usually greatest 24-48 hours postoperatively. Reasons for alterations in respiratory functioning include splinting, surgical trauma to expiratory muscles, distention of the bowel, and residual pneumoperitoneum from the surgical procedure.
6. Monitoring: Monitoring the physiological functioning of the patient during
surgery is a collaborative effort performed by the whole surgical team. The following areas must be assessed: airway patency, gas exchange, tissue perfusion, hemodynamic status, fluid status, body temperature, effects of anesthesia and patient positioning.
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 26
Learning Check 1. Case Study #1 Hernia B.C., a 46-year-old construction worker, has been admitted for repair of a Right Inguinal Hernia-open. B.C. stated that this condition has affected his performance at work. He is unable to lift over 30 lbs without his “hernia popping”. He has not exhibited any signs of bowel strangulation. Two years ago, he was diagnosed with a hiatus hernia and is taking Zantac BID with relief. Admission Assessment: General Appearance: Medium build, male, height 5’ 10” and weight 180 lbs.,
slightly anxious. Fluid: B/P 130/82, P-72, Rhythm regular. Normal heart sounds.
Palpable radial, femoral, popliteal and pedal pulses. Mucous membranes dry. No edema.
Respiratory: Good inspiratory and expiratory breath sounds throughout
lung fields. Nutrition: Allergic to Penicillin and describes that his lips swelled up
at his daughter’s birthday party when he blew up the balloons. Occasional G.I. upset, relieved with Zantac. Nauseated at present and not tolerating fluids or food x last 24 hrs.
Communication: Slightly anxious (pacing room). Family is aware of surgery
and will visit this p.m. His girlfriend is in the waiting room. Activity: Runs 5 km twice a week. Dizzy and light headed at
present (postural hypotension). Cognitive/Perception: Alert and oriented. Blood Work CBC Normal
Hgb 140 Male (140 – 180) Hct 0.55 Male (0.42 – 0.52)

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 27
WBC 6.0 (5-9/mm³) Plt 130 (130-400 x 10 g/L)
Electrolytes Normal
Na 145 (137 – 147 mEq/L) K 5.0 (3.5 – 5.0 mEq/L) CI 102 (95 – 107 mEq/L) HCO3 22 (22 –26 mEq/L) Gluc 140 (<145 mg/dl) BUN 19 (6 –20 mg/dl)
Urinalysis
Specific Gravity 1.032 Normal (1.010 – 1.025 osmolarity) Case Study #1 Hernia Analysis
1. List the significant assessment data for B.C.
2. What are the potential concerns arising from the assessment data that the perioperative nurse should consider when developing a surgical plan of care for B.C.’s care in the operating room?
3. What nursing interventions would be appropriate for these concerns?
4. What could possibly happen to B.C. during induction given his past medical history?

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 28
2. Case Study #2 Laparoscopic Cholecystectomy C.S. is a 32-year-old male coming for a laparoscopic cholecystectomy. He is in excellent health. He is 180 cm (6 feet) tall, weighs 141 kg (310 pounds), and plays for a professional football team. His hands and upper chest are raw and seeping with a small amount of blood from the rough game he played last weekend. He is allergic to iodine. Case Study Analysis 1. C.S. is allergic to iodine; therefore, what would be an appropriate prepping solution
for his laparoscopic cholecystectomy? a. glutaraldehyde b. chlorhexidine gluconate c. hydrogen peroxide d. betadine
2. Indicate whether the following statement is true or false.
The surgeon has all of his trocars in place and is ready to start the surgical procedure. As a scrub nurse, you anticipate that he will ask for the patient to be put in reverse trendelenberg and tilted to the left.
True ______ False ______

Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 29
Learning Check Answers 1. Case Study #1
1. Significant assessment data for B.C.:
• slightly anxious • dizzy, lightheaded • not tolerating fluids • lips swell when blowing up balloons-questionable latex sensitivty • hernia – hiatus; taking Zantac; reflux • allergy – PCN
2. Issues related to assessment data that the perioperative nurse should consider
when planning B.C.’s perioperative care: 1. anxiety 2. fluid volume deficit (dehydration) 3. potential latex allergy 4. risk for aspiration
3. Appropriate interventions:
1. Verify with B.C. his anxiousness and potential cause. 2. Notify anesthesia for fluid replacement. 3. Alert the OR staff of a potential latex allergy. 4. Ensure all materials to be used in the surgery are latex free (e.g.,
penrose drain) 5. Be ready to assist with cricoid pressure.
4. Gastroesophageal reflux, aspiration
2. Case Study #2
1. Chlorhexidine Gluconate 2. true
Unit Three: Lesson 5 General Surgery ____________________________________________________________________________________
___________________________________________________________________________________ September 2015 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 30
References AORN. (2013). Perioperative Standards and Recommended Practices. Denver, CO.
Author. Fuller, J. (2013). Surgical technology. (6th ed.). Toronto: Mosby. Goldman, M. (2009). Pocket guide to the operating room. Philadelphia: F.A. Davis
Company. Goodman, T. & Spry, C. (2014). Essentials of Perioperative Nursing (5th ed.) Toronto:
Jones and Bartlett Publishing. Phillips, N. (2013). Berry & Kohn’s Operating Room Technique. (12th ed.). Toronto:
Mosby. Rothrock, J. C. (Ed.). (2015). Alexander’s care of the patient in surgery (15th ed.).
Toronto: Mosby. Tighe, S.M. (2016). Instrumentation for the Operating Room (9th ed.). St. Louis: Mosby.