unilateral vocal fold paralysis after congenital...
TRANSCRIPT

Unilateral Vocal Fold Paralysis After CongenitalCardiothoracic Surgery: A Meta-analysis
abstractBACKGROUND AND OBJECTIVE: There is variation in the literature inregard to the occurrence of unilateral vocal fold paralysis (UVFP) aftercongenital cardiothoracic surgery. The objective of this study was toidentify and appraise the evidence for the occurrence of UVFP aftercongenital cardiothoracic surgery in a meta-analysis.
METHOD: A comprehensive search strategy in Medline, Embase, andthe Cochrane Library was conducted, limited to English publications.Two independent reviewers screened studies for eligibility criteria. Ofthe 162 identified studies, 32 (20%) met the inclusion criteria. Using theOxford Centre for Evidence-Based Medicine guidelines, 2 reviewersappraised the level of evidence, extracted data, and resolveddiscrepancies by consensus. Weighted pooled proportion and 95%confidence intervals (CIs) are reported.
RESULTS: Thirty-two studies (n = 5625 patients) were included. Levelsof evidence varied from level 3 to 4. Among all studies, the weightedpooled proportion of UVFP was 9.3% (95% CI, 6.6% to 12.5%), andamong 11 studies (n = 584 patients) that postoperatively evaluatedpatients with flexible nasopharyngolaryngoscopy to documentpresence of UVFP, the weighted pooled proportion of UVFP was29.8% (95% CI, 18.5% to 42.5%). Twenty-one studies (n = 2748patients) evaluated patients undergoing patent ductus arteriosusligation surgery, and the weighted pooled proportion of UVFP was8.7% (95% CI, 5.4% to 12.6%). Six of these (n = 274 patients) assessedall patients postoperatively, and the weighted pooled proportion ofUVFP was 39% (95% CI, 18% to 63%). Pooled analyses of risk factorsand comorbidities are reported. Heterogeneity and publication biaswere detected.
CONCLUSIONS: UVFP is a demonstrated risk of congenital cardiotho-racic surgery. Routine postoperative nasopharyngolaryngoscopy forvocal fold assessment by an otolaryngologist is suggested. Pediatrics2014;133:e1708–e1723
AUTHORS: Julie E. Strychowsky, MD,a Gavin Rukholm, MD,FRCSC,a,b Michael K. Gupta, MD, MSc, FRCSC,a and DianeReid, MD, FRCSCa
aDepartment of Surgery, Division of Otolaryngology–Head andNeck Surgery, McMaster University, Hamilton, Ontario, Canada;and bPeterborough Regional Health Centre, Peterborough,Ontario, Canada
KEY WORDSunilateral vocal fold paralysis, cardiothoracic surgery, patentductus arteriosus
ABBREVIATIONSCI—confidence intervalG-tube—gastrostomy tubeOCEBM—Oxford Centre for Evidence-Based MedicinePDA—patent ductus arteriosusUVFP—unilateral vocal fold paralysis
Dr Strychowsky conceptualized and designed the study,designed the data collection instruments, performed theliterature search and data extraction, appraised the levels ofevidence, carried out the initial analyses and interpretation ofdata, and drafted the initial manuscript; Dr Rukholmconceptualized and designed the study, performed the literaturesearch and data extraction, appraised the levels of evidence,interpreted the data, and critically reviewed and revised themanuscript; Dr Gupta conceptualized and designed the study,carried out the statistical analysis, interpreted the data, andcritically reviewed and revised the manuscript; Dr Reidconceptualized and designed the study, interpreted the data,and critically reviewed and revised the manuscript; and allauthors approved the final manuscript as submitted.
This article was presented as a podium presentation at theAnnual Meeting of the American Society of PediatricOtolaryngology in Arlington, Virginia, on April 26, 2013.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-3939
doi:10.1542/peds.2013-3939
Accepted for publication Mar 4, 2014
Address correspondence to Julie E. Strychowsky, MD, Departmentof Surgery, Division of Otolaryngology–Head and Neck Surgery,McMaster University, 1200 Main St West, Hamilton, Ontario,Canada, L8N 3Z5. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
e1708 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

Unilateral vocal fold paralysis (UVFP)secondary to left recurrent laryngealnerve injury during cardiothoracic sur-gery is a known risk.1 The path of thenerve, which loops around the arch ofthe aorta, makes it susceptible to injury.This is especially true in patent ductusarteriosus (PDA) ligation surgery, giventhe nerve’s proximity to the PDA.2 Se-quelae of UVFP may include stridor, ab-sent or weak cry, aspiration, or feedingand swallowing difficulties.3 Therefore,adequate and timely diagnosis can helpguide appropriatemanagement. Althoughsome patients are asymptomatic, thisdoes not preclude proper assessment.Flexible nasopharyngolaryngoscopy isa short and well-tolerated procedureperformed without sedation by otolar-yngologists that allows direct visualiza-tion of the larynx and subsequentdiagnosis of UVFP.
There is variation in the literature inregard to the occurrence of UVFP aftercongenital cardiothoracic surgery. Thismay result from the lack of routinepostoperative vocal fold function as-sessment. To date, there has been nosystematic review of the evidence forthe occurrence of UVFP after cardio-thoracic surgery in infants and chil-dren.
The primary objective of this study wasto identify and appraise the evidence forthe occurrence of UVFP after congenitalcardiothoracic surgery (all types ofsurgeryandPDA ligationsurgeryonly) ininfants and young children. We alsosought to determine the occurrence ofUVFP in patients who underwent post-operative assessment by flexible naso-pharyngolaryngoscopy. Other outcomesinvestigated included UVFP-associatedrisk factors and comorbidities.
METHODS
This review was conducted in accor-dance with the Preferred ReportingItems for Systematic Reviews andMeta-Analyses guideline.4
Literature Search Strategy
The literature was searched using OvidMedline (1946 to October 2012), Embase(1980to2012Week41),andtheCochraneLibrary (Cochrane Database of Sys-tematic Reviews, 2012, Issue 3). Theelectronic database search combinedintervention-specific terms (cardiotho-racic surgery, cardiac surgery, heartsurgery, cardiopulmonary bypass, pat-ent ductus arteriosus, PDA ligation, li-gation, closure) and outcome-specificterms (vocal fold, vocal cord, recurrentlaryngeal nerve, immobility, mobility,paralysis, paresis, injury). To ensure thatall relevant published articles werecaptured, the search was not limited bypublication date or study design. Rele-vant articles and abstracts were se-lected and reviewed. Reference listsfrom these sources and recent reviewarticles were searched for additionalpublications.
Study Selection Criteria
Articles were assessed for eligibilityindependently by2 reviewauthors (J.E.S.and G.R.) and were included if theywere prospective or retrospective fullypublished studies that reported oc-currence of UVFP after congenitalcardiothoracic surgery in infants andyoung children. Secondary outcomesincluded type of surgery (PDA ligationor other), postoperative assessmentof vocal cord function by flexiblenasopharyngolaryngoscopy, patient de-mographics, respiratory and swallow-ing outcomes, and comorbidities. Non-English publications were excluded.
Assessment of Quality
Methodological quality of identifiedstudieswas appraised using the OxfordCentre for Evidence-Based Medicine(OCEBM) 2011 Levels of Evidence5:
� Level 1: Systematic review of ran-domized trials, systematic reviewof nested case–control studies,n-of-1 trials
� Level 2: Individual randomized tri-als or (exceptionally) observa-tional studies with dramatic effect
� Level 3: Nonrandomized controlledcohort/follow-up studies providedthere are sufficient numbers torule out a common harm
� Level 4: Case series, case–control,or historically controlled studies
� Level 5: Mechanism-based reason-ing
Data Analysis
Relevant data were extracted from fullypublished reports by 2 independentreview authors (J.E.S. and G.R.) follow-ing prescribed tables developed a pri-ori. Disagreement was resolved byconsensus.
Descriptive statistics were extractedor calculated for occurrence of UVFP.Cases of bilateral vocal fold paralysiswere excluded. A qualitative synthesisof results was performed when appli-cable. Meta-analysis was performed bycalculating pooled proportion of theweighted occurrence for UVFP usingDerSimonian–Laird weights for therandom effects model. Subgroup anal-yses developed a priori for post-operative assessment for UVFP and PDAligation surgery only were conducted.Inverse variance measuring mean dif-ference for the random effects modelwas used for the analysis of continuousvariables. Heterogeneity between stud-ies was tested using the Q statistic withthe I2 approach. Publication bias was an-alyzed by visual inspection of the funnelplot and Egger’s test. StatsDirect software1.7.8 (StatsDirect Limited, Cheshire, UK)and Review Manager 5.1.7 (The NordicCochrane Centre, The Cochrane Collabo-ration, Oxford, UK) were used.
RESULTS
One hundred sixty-two studies wereidentified through the literaturesearch.Titles and abstracts of these studies
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1709
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

were screened for the inclusion andexclusion criteria. The search strategydid not include a limit for study design;therefore, many of the studies excludedwere comments, editorials, or reviews.A resultant 50 full-text articles werefurther screened. Thirty-two studiesthatsatisfiedthe inclusioncriteriawereincluded in the analysis (Fig 1).6–37
OCEBM levels of evidence varied fromlevel 3 (9 studies)9–11,14–16,20,23,26 to level4 (23 studies)6–8,12,13,17–19,21,22,24,25,27–37
(Table 1). Occurrence of UVFP, type ofsurgery, patient demographics, andvocal fold assessment are reported inTable 1.
Analysis by Type of Surgery
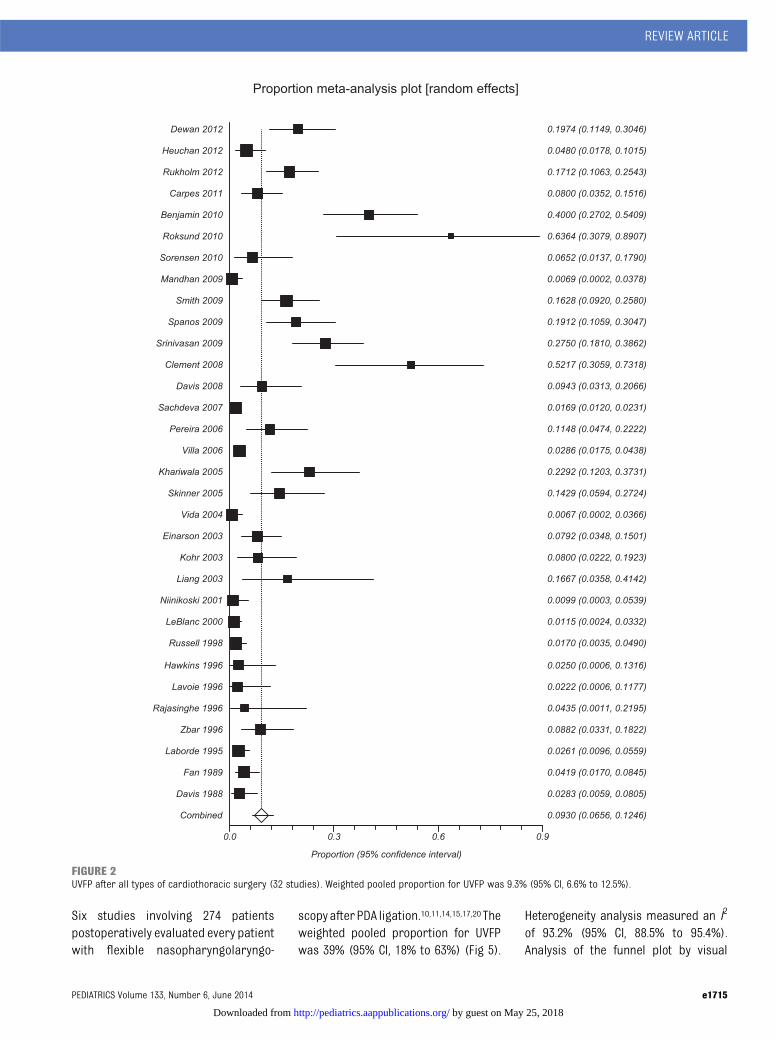
Thirty-two studies involving 5625 pa-tients reported the occurrence ofUVFP after any type of cardiothoracic
surgery.6–37 The weighted pooled pro-portion for UVFP was 9.3% (95% CI,6.6% to 12.5%) (Fig 2). Heterogeneityanalysis measured an I2 (incon-sistency) of 91.4% (95% CI, 89.3% to92.9%). This is the percentage of vari-ation across studies that is due toheterogeneity rather than chance.Funnel plot analysis revealed a possi-ble publication bias; Egger’s testshowed the presence of bias (bias =2.5; 95% CI, 1.8 to 3.2; P , .0001).
Twenty-onestudies involving2748patientsreported the occurrence of UVFP afterPDA ligation only.7,8,10–15,17,20,21,24,27–31,34–37
The weighted pooled proportion was8.7% (95% CI, 5.4% to 12.6%) (Fig 3).Heterogeneity analysis measured anI2 of 81.6% (95% CI, 65.0% to 88.4%).Funnel plot analysis and Egger’s testshowed the presence of publication
bias (bias = 3.3; 95% CI, 2.2 to 4.4; P,.0001).
Analysis for PostoperativeAssessment of Vocal Fold Function
Only 10% of patients underwentpostoperative vocal fold functionassessment. Among patients un-dergoing any type of cardiothoracicsurgery procedure, 11 studies in-volving 584 patients postoperativelyevaluated every patient with flexiblenasopharyngolaryngoscopy.6,9–11,14–17,20,22,23
The weighted pooled proportion forUVFP was 29.8% (95% CI, 18.5% to42.5%) (Fig 4). Heterogeneity analysismeasured an I2 of 90.4% (95% CI, 85.2%to 93.1%). Both funnel plot and Egger’stest analyses showed publication biasamong the studies (bias = 7.0; 95% CI,2.3 to 11.7; P = .0079).
FIGURE 1Flow diagram of study selection.
e1710 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

TABLE1
Outcom
es
Author,YearR
ef(Country),YearsofStudy
Type
ofSurgery
Patient
Demographics
Occurrence
ofUVFP
(Cases/Total)
(%)
Assessmentfor
VocalCordFunction
Levelof
Evidence
Dewan
etal,20126
(USA),May
2007–May
2008
Allcardiothoracicsurgery
+VCP:
15/76(19.7%
)FlexibleNPLafterextubation,sw
allowing
evaluation
4SA
8.86
65.99
dSW
2.99
60.54
kg2VCP:
SA10.366
6.73
dSW
3.11
60.50
kgHeuchanetal,20127
(UK),2001–2007
PDAligation
GA26
wk(25–27)
6/125(4.8%)
NR4
BW840g(730–1035)
SA31
d(25–41)
Rukholmetal,20128
(Canada),Jul2003–Jul
2010
PDAligation
+VCP:
19/111
(17.1%
)27.9%NPLpostoperative
4GA
25.4wk(24.8–26.0)
0.9%
NPLpreoperative
BW743.8g(665.4–822.1)
SA28.9wk(28.0–30.0)
SW845.8g(766.5–925.2)
2VCP:
GA26.7wk(26.0–27.5)
BW990.0g(858.4–1121.5)
SA34.0wk(29.5–38.5)
SW1404
g(966.3–1843.3)
Carpes
etal,20119
(Canada),Nov
2008–Aug
2009
Allcardiothoracicsurgery
+VCP:
8/100(8%)
FlexibleNPLimmediatelypreoperatively
andwithin72
hofextubation
3SA
0.7m(0.1–14.2)
SW3.7kg
(3.2–9.2)
2VCP:
SA7.8m(4.1–36.7)
SW7.5kg
(4.9–15.7)
Benjam
in,20101
0(USA),Jan2004–Dec2006
PDAligation
Extrem
elylowBW
22/55(40%
)FlexibleNPLifsuspectedVCP
3+VCP:
22/25(88%
)scoped
GA24.56
1.1wk
BW7226
122g
SA17
68.7d
SW7226
140g
2VCP:
GA24.86
1.3wk
BW7286
132g
SA22
614.5d
SW7986
219g
Roksund,2010
11(Norway),1982–1985
(surgery),
2008–2009
(study)
PDAligation
GA,28
wkor
BW,1000
g7/11
(64%
)FlexibleNPLandcontinuous
laryngoscopy
during
maximal
treadm
illexercise
3SA
12d(4–29)
+VCP:
GA27.16
1.5wk
BW8746
138g
2VCP:
GA27.06
2.9wk
BW9286
283g
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1711
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

TABLE1
Continued
Author,YearR
ef(Country),YearsofStudy
Type
ofSurgery
Patient
Demographics
Occurrence
ofUVFP
(Cases/Total)
(%)
Assessmentfor
VocalCordFunction
Levelof
Evidence
Sørensen,20101
2(Denmark),1998–2007
PDAligation
GA,37
wk
3/46
(7%)
NR4
GA26
66.5wk(236
3to34)
BW943.5g(535–1793)
SA29
64.7wk(256
6to40
64)
SW1104
g(525–2520)
Mandhan,20091
3(New
Zealand),Jan
1987–Dec
2005
PDAligation
GA25.56
2.3wk
1/145(0.7%)
NR4
BW837.76
277.2g
SA14.16
1.8d
SW881.36
338.1g
Smith,20091
4(USA),Apr2004–Oct2007
PDAligation
Prem
atureinfants:
14/86(16%
)PostextubationflexibleNPL
3GA
26.66
2.5wk
BW1000
6394g
SA17
612
dSpanos,20091
5(USA),1995–2005
PDAligation(sutureligatureor
clip)
SW,1kg
13/68(19%
)FlexibleNPLafterextubation
3Suture
ligature:
GA25
62.0wk
BW7406
288g
SW1054
6626g
Clip:
GA24.76
1.3wk
BW6516
169g
SW7626
210g
Srinivasan,20091
6(USA)
Norw
oodprocedure
Group1:
4/40
(10%
)FlexibleNPLallpatientsinGroup2
3SA
10d(3–218)
18/40(45%
)(allscoped)
Group1,2001–2004
SW3.2kg
(2.0–5.7)
Group2,2005–2007
(standardized
managem
ent)
Group2:
SA6d(2–64)
SW3.3kg
(2.3–4.3)
Clem
ent,2008
17(Canada),Oct2003–May
2004
PDAligation
+VCP:
12/23(52%
)FlexibleNPL,20
pts
4GA
24.8wk(24–26)
Videofluoroscopicsw
allowstudy
BW725g(580–887)
SA14.5d(6–31)
2VCP:
GA27.0wk(25–31)
BW1040
g(700–1540)
SA13.8d(4–53)
Davis,2008
18(USA)
Hypoplastic
leftheartsyndrom
e;TGA
BW3.19
60.69
kg5/27
(18.5%
)NR
4
SA6.16
3.8d
0/26
(0%)
BW3.35
60.65
kgSA
9.26
10.0d
e1712 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

TABLE1
Continued
Author,YearR
ef(Country),YearsofStudy
Type
ofSurgery
Patient
Demographics
Occurrence
ofUVFP
(Cases/Total)
(%)
Assessmentfor
VocalCordFunction
Levelof
Evidence
Sachdeva,20071
9(USA),Jan2000–Jan2006
Allcardiothoracicsurgery
SA13.5d(1–1604)
38/2255(1.7%)
NRifallscoped
4SW
3.45
kg(0.9–14.5)
Pereira,2006
20(USA),Mar
2001–Feb2004
PDAligation
GA25
wk
7/61
(11.5%
)FlexibleNPLpostextubation
3BW
740g
SA23
dSW
914g
Villa,20062
1(France),Sep
1991–Feb2004
PDAligation
LowBW
infants,24
pts
LowBW
infants:
NR4
LowBW
infants:2.16
0.4kg
2/24
(8.3%)transient
1/24
(4.2%)persistent
Children:
15/676
(2.2%)transient
2/676(0.3%)persistent
Khariwala,2005
22(USA),4-yperiod
Allcardiothoracicsurgery
Pediatric
11/48(23%
)UVFP
3/48
(6%)BilateralVCP
Inpatient
ORLconsultation
4
Skinner,2005
23(USA),Apr2003–Dec2004
Norw
oodprocedure
SA6d(2–19)
3/33
(9%)
FlexibleNPL(m
edian10
dpostoperative)
3Aorticarch
reconstruction
SW3.1kg
(1.9–4.2)
4/16
(25%
)Modified
barium
swallow
SA9d(4–33)
SW3.1(2.0–3.7)
Vida,20042
4(Italy),Jun
1994–Dec2002
PDAligation
SA45
m(3–161)
1/150(0.7%)
NR4
SW18
kg(4.2–73)
Einarson,20032
5(Canada),Jan
1998–Dec1999
Allcardiothoracicsurgery
Neonates
,28
d:8/101(8%)
ORLassessmentnotspecified
4SA
7.86
5.6d(1–25)
SW3.22
60.62
kg(1.5–4.8)
Kohr,20032
6(USA),Mar
1999–Sep1999
Allcardiothoracicsurgery
SA4.86
5.2y(1
d–16.7y)
4/50
(8%)
ORLifrecommendedby
speech–language
pathologist
3SW
19.66
17.8kg
(3.1–72.6)
Prem
atureinfantsexcluded
Liang,2003
27(Taiwan),Mar
1998–May
2001
PDAligation
Subgroup
,1y
3/18
(16.7%
)Bronchoscopy
ifhoarseness,
inspiratorystridor,or
weakcry
4+VCP:
SW9.0kg
(8.9–9.1)
2VCP:
SW10.3kg
(6.2–11.5)
Niinikoski,20012
8(Finland),1988–1998
PDAligation
Very
lowBW
infants,1500
g:1/101(1%)
NR4
GA27.2wk
BW9636
239g
SA12
68d
SW9696
231g
LeBlanc,2000
29(Canada),Jan
1985–Dec1998
PDAligation
Nonprematureinfants
3/261(1.1%)
NR4
Russell,1998
30(Canada),Jan
1985–Dec1997
PDAligation
Prem
atureinfants:
3/176(1.7%)
NR4
GA26
wk(23–36)
BW847.5g(400–2300)
SA21
d(4–60)
SW982.5(475–2740)
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1713
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

TABLE1
Continued
Author,YearR
ef(Country),YearsofStudy
Type
ofSurgery
Patient
Demographics
Occurrence
ofUVFP
(Cases/Total)
(%)
Assessmentfor
VocalCordFunction
Levelof
Evidence
Hawkins,19963
1(USA),Jul1994–Mar
1996
PDAligation(coilocclusion
orsurgicalclosure)
Coilocclusion:
0/20
(0%)
NR4
SA4.16
4.9y(6
m–15
y)1/20
(5%)
SW18
616
kgSurgicalclosure:
SA36
3.9y(4
m–10
y)SW
126
7kg
Lavoie,19963
2(USA),DatesNR
VATS
forvariousprocedures
SA2.65
y(1
d–14.1y)
1/45
(2.2%)
NR4
SW11.78kg
(580
g–45.9kg)
Rajasinghe,19963
3(USA),Jul1992–Jan1995
Aorticcoarctation
andtubularhypoplasiarepair
SA13
d(3–34)and
69d(61–78)
1/23
(4.3%)
NR4
SW2.9kg
(1.3–5)
Zbar,19963
4(USA),Jan1991–Jan1994
PDAligation
,12
m6/68
(8.8%)
ORLassessmentonlyifsymptom
atic
4+VCP:
22.7%forextrem
elylowBW
(,1kg)
GA26.3wk
BW0.9kg
SA31.9d
SW1.1kg
2VCP:
GA33.8wk
BW2.3kg
SA88.4d
SW3.4kg
Laborde,1995
35(USA),Sep1991–Mar
1995
PDAligation
,6m,70pts(30%
)6/230(2.6%)
Postoperativelaryngoscopy
46–48
m,123
pts(54%
)5transient
.48
m,37pts(16%
)1persistent
SW12.6kg
(1.2–65)
Fan,1989
36(USA),DatesNR
PDAligation
,1500
g7/167(4.2%)
Fiberopticlaryngoscopy
4Davis,1988
37(USA),Jun1980–Jul1987
PDAligation
Prem
atureinfants
3/106(2.8%)
NR4
BW,birthweight;GA,gestationalage;NPL,nasopharyngolaryngoscopy;NR
,notreported;ORL,otorhinolaryngology;pts,patients;SA,age
atsurgery;SW
,weightatsurgery;TGA,transpositionofthegreatarteries;VATS,video-assistedthoracoscopicsurgery;
VCP,vocalcordparalysis.
e1714 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from
Six studies involving 274 patientspostoperatively evaluated every patientwith flexible nasopharyngolaryngo-
scopyafterPDA ligation.10,11,14,15,17,20 Theweighted pooled proportion for UVFPwas 39% (95% CI, 18% to 63%) (Fig 5).
Heterogeneity analysis measured an I2
of 93.2% (95% CI, 88.5% to 95.4%).Analysis of the funnel plot by visual
FIGURE 2UVFP after all types of cardiothoracic surgery (32 studies). Weighted pooled proportion for UVFP was 9.3% (95% CI, 6.6% to 12.5%).
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1715
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

inspection did not suggest publicationbias; Egger’s test confirmed its absence(bias = 7.6; 95% CI,23.4 to 18.5; P = .13).
Analysis for Demographics
Five studies involving 354 patients re-ported birthweights for patientswith andwithout UVFP after surgery.8,10,11,14,17,34 Forpatients with and without UVFP, birthweights ranged from 725 to 900 g and 728to 2300 g, respectively. The weightedpooled mean difference between patientswith and without UVFP was2201 g (95%CI, 2372 g to 230 g) (P = .02) (Fig 6);patients with UVFP were 201 g smaller
than those without. Heterogeneity analy-sis measured an I2 of 79%.
Weight at the time of surgery wasreported among 6 studies (373patients) as a comparison for patientswith and without UVFP.6,8,9,27,34 Surgicalweight ranged from 846 g to 9000 gamong patients with UVFP and 1404 gto 10 300 g for those without. Theweighted pooled mean difference was2820 g (95% CI,21564 g to276 g) (P =.03), showing patients with UVFP tohave significantly smaller weights atthe time of surgery (Fig 7). Heteroge-neity analysis measured an I2 of 71%.
Gestational age of patients with andwithout UVFP was reported among 6studiesinvolving399patients.8,10,11,14,17,34
Among patients with and without UVFP,gestational ages ranged from 24.5 to27.1 weeks and 24.8 to 33.8 weeks, re-spectively. The weighted pooled meandifferencewas21.1weeks (95%CI,21.7to 20.46 weeks, P = .0007), statisticallysignificantly correlating younger gesta-tional ages with a higher incidence ofUVFP (Fig 8). There was low heteroge-neity among the studies (I2 = 28%).
Five studies involving 378 patientsreported age at the time of surgery for
FIGURE 3UVFP after PDA ligation only (21 studies). Weighted pooled proportion of UVFP was 8.7% (95% CI, 5.4% to 12.6%).
e1716 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

FIGURE 4UVFP after all cardiothoracic surgery in patients who underwent postoperative vocal fold assessment (11 studies). Weighted pooled proportion for UVFP was29.8% (95% CI, 18.5% to 42.5%).
FIGURE 5UVFP after PDA ligation only and postoperative vocal fold assessment (6 studies). Weighted pooled proportion for UVFP was 39% (95% CI, 18% to 63%).
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1717
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

patients with and without UVFP.6,8,9,17,34
Surgical ages ranged from 8.9 to 31.9days and 10.4 to 237 days, respectively.The weighted pooled mean differencebetween patients with and withoutUVFP was217.8 days (95% CI,241.8 to6.3 days, P = .15) and not statisticallysignificant (Fig 9). Heterogeneity anal-ysis measured an I2 of 62%.
Analysis for Duration of Ventilation
Five studies, comprising 226 patients,reported a comparison of duration ofventilation forpatientswithandwithoutUVFP.6,10,11,17,20 The weighted pooledmean difference was not statistically
significant (6.88 days; 95% CI, 22.1 to15.9 days; P = .13) (Fig 10). I2 was 51%.
Analysis for Gastrostomy Tube Use
A comparison of gastrostomy tube(G-tube) use in patientswithandwithoutUVFP was reported among 283 patientsin 5 studies.8,10,17,20,23 The pooled oddsratio was 7.3 (95% CI, 1.6 to 32.8, P =.010), suggesting a correlation of G-tubeuse among patients without UVFP(Fig 11). I2 was 49%.
Other Analyses
Additional pooling of data were notpossible because of the nonuniform
reporting of data among studies in-cluded or too few studies that reportedthe same outcome. Length of stay inhospital was reported in 2 studies.6,17
Mean length of stay was statisticallysignificantly longer among patientswith UVFP in both studies. Dewan et al6
reported on patients who underwentmedian sternotomy for cardiac sur-gery (34.9 6 29.5 days vs 22.9 6 14.6days, P = .02), and Clement et al17 in-vestigated extremely low birth weightinfants undergoing PDA ligation (148.2vs 96.8 days, P , .001).
Two studies did not report any recoveryof vocal fold function at follow-up points
FIGURE 6Birth weight (6 studies). Weighted pooled mean difference between patients with and without UVFP was 2201 g (95% CI, 2372 g to 230 g) (P = .02).
FIGURE 7Weight at time of surgery (5 studies). Weighted pooled mean difference was 2820 g (95% CI, 21564 g to 276g) (P = .03).
FIGURE 8Gestational age (6 studies). Weighted pooled mean difference was 21.1 weeks (95% CI, 21.7 to 20.46 weeks) (P = .0007).
e1718 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

of 6 and 5 to 19 months, respectively.34,36
Khariwala et al22 reported a recovery 9 of11 patients (82%). Carpes et al9 reportedrecovery of vocal fold movement in 3 of 7patients at 3 months’ follow-up. Fur-thermore, Spanos et al15 reported long-term follow-up (range 1–18 months) for6 patientswith UVFP. Only 2 patientswerefound to have full recovery. Sachdevaet al19 reported follow-up in 9 patientswith UVFP and found full recovery offunction in 3 patients, partial recovery in4 patients, and no signs of recovery in 2patients; however, no time frame forfollow-up was reported.
DISCUSSION
To our knowledge, this is the first sys-tematic review and meta-analysis to re-port the pooled occurrence of UVFP aftercardiothoracic surgery in infants andchildren. Among 32 studies, involving5625 patients, the weighted pooledproportion of UVFPwas 9.3%. For thoseundergoing only PDA ligation, the pooledproportion was 8.7%. However, it is im-portant to consider the occurrence ofUVFP in the population of patients whounderwent routine postoperative vocalcord function assessment by flexible
nasopharyngolaryngoscopy. Only 10% ofpatients after any type of cardiothoracicsurgeryorPDAligationsurgeryunderwentpostoperative vocal fold function assess-ment. The weighted pooled proportion ofpatients with UVFP in this population was30% for patients undergoing all types ofcardiothoracic surgeryand39% for thoseundergoing PDA ligation.
These data suggest that the occurrence ofUVFP among patients who were post-operatively assessed for vocal fold func-tion is significant. Ninety percent ofpatients included in our analysis of 32
FIGURE 9Age at time of surgery (5 studies). Weighted pooled mean difference between patients with and without UVFP was 217.8 days (95% CI, 241.8 to 6.3 days)(P = .15).
FIGURE 10Duration of ventilation (5 studies). Weighted pooled mean difference was 6.88 days (95% CI, 22.1 to 15.9 days), P = .13.
FIGURE 11G-tube use (5 studies). Pooled odds ratio was 7.3 (95% CI, 1.6 to 32.8) (P = .010).
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1719
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

studies did not undergo routine post-operative assessment. Among thesepatients, stridor, absent or weak cry, as-piration, or feeding or swallowing diffi-culties most often prompt additionalinvestigation of vocal fold function. Chil-dren who are asymptomatic initially maynot be diagnosed until early childhood,when they presentwith an inability to singor a weak voice. Smith et al14 reporteda rate of delayed diagnosis of 14%. Timelydiagnosis would ensure that appropriatetreatment options such as use of thick-ened foods, voice therapy, or surgical in-tervention be made available to them.38
Methods of Vocal Fold Assessment
Methods of vocal fold assessment gen-erally included assessment with flexiblenasopharyngolaryngoscopy, a well-tolerated bedside examination thatdoes not require sedation. Ten studiesperformed the assessment after extu-bation.6,9–11,14–17,20,23 One study did notspecify whether patients underwentflexible nasopharyngolaryngoscopy;however, an otorhinolaryngologist as-sessed all the patients, and thereforewe assumed that those needing addi-tional assessment would have un-dergone the diagnostic laryngoscopy.22
Carpes et al9 also performed the as-sessment immediately preoperatively.Roksund et al11 assessed patients ap-proximately 25 years after PDA ligationby performing flexible nasopharyn-golaryngoscopy and continuous laryn-goscopy during maximal treadmillexercise. Three studies also includedswallowing assessments.6,7,23
Preoperative assessment of vocal foldfunction merits discussion. The inherentbenefit is the avoidance of attributing theoccurrence of UVFP to iatrogenic injury ifit is noted preoperatively. However,patients may have associated heart fail-ure, pulmonary failure, and poor re-spiratory reserve secondary to theircardiac anomaly, which may precludeadequate preoperative evaluation. Pre-
operative assessment of vocal fold func-tion was reported only in the study fromBC Children’s Hospital.9 The authors per-formed flexible laryngoscopy immedi-ately before surgery in the operatingroom and within 72 hours after extuba-tion. Twenty-four (15%) patients could notundergo preoperative assessment be-cause of endotracheal intubation, and 4(2.5%) were found to have UVFP pre-operatively andwere excluded from theirstudy. Additional techniques for vocal foldfunction assessment may include extu-bation followed by direct laryngoscopyand rigid bronchoscopy, laryngeal elec-tromyography, or laryngeal ultrasound.Maturo et al39 prospectively showed thatlaryngeal electromyography could pre-dict recurrent laryngeal nerve functionreturnwhen comparedwith diagnosis byflexible fiberoptic laryngeal examination.The authors reported this technique tobe a safe, operator-friendly method fordetermining the likelihood of functionreturn in a variety of patients, includingthose who had undergone PDA ligation.The mean patient age was 21.4 months.Wang et al40 reported the usefulness oflaryngeal ultrasound for vocal fold as-sessment. They showedmaximum glotticangle and vocal fold–arytenoid angle tobe quantitative ultrasonographic indica-tors of vocal fold immobility among 45children of median age 4 years and 6months (range 9 months–13 years).However, the efficacy of laryngeal elec-tromyography or ultrasound has notbeen described in neonates or infants,nor has it been used in the intubatedpatient.
Risk Factors
UVFP was shown to be statistically sig-nificantly associated with younger ges-tational age, lower birth weight, andlower surgical weight among the limitednumber of studies that reported theseoutcomes. Age at time of surgerywas notasignificantrisk factor forUVFP.Lengthofmechanical ventilation was not signifi-
cantly different between groups. G-tubeuse was statistically significantly higheramong patients without UVFP. Theseanalyses are based on limited patientnumbers because of the small numberofstudies that reported these outcomes bypresence or absence of UVFP.
Patients who need congenital cardiacsurgeryoftenhavemultiplecomorbidities.Two studies8,11 reported associations be-tween bronchopulmonary dysplasia andUVFP after PDA ligation. Roksund et al11
reported outcomes for 11 patients;bronchopulmonary dysplasia was pres-ent in 86% of patients with UVFP and50% of those without UVFP (P , .001).Among 111 patients, Rukholm et al8
reported 74% of patients with UVFP tohave bronchopulmonary dysplasia, com-pared with 47% of those without UVFP(P = .043); however, given the Bonferronimethod of statistical analysis for multiplecomparisons, only P , .006 was consid-ered significant. This retrospective studyfrom our center at McMaster Universityshowed only gastroesophageal refluxdisease to be statistically significantlyassociated with UVFP after PDA ligation,and not G-tube feeding, sepsis, pneumo-nia, retinopathy of prematurity, or ane-mia of prematurity.8 Benjamin et al10
comparedneurodevelopmental outcomesbetween patients with and without UVFPafter PDA ligation and found no signif-icant difference between groups.
Surgical technique for PDA ligation andits correlation with occurrence of UVFPhas also been investigated. Spanoset al15 compared rates of paralysisbetween vascular clip and suture liga-tion procedures in a prospective studyand found similar incidence of UVFP inboth groups (19% vs 20%). All cases ofUVFP were in infants who weighed ,1kg at birth. Zbar et al34 showed iatro-genic UVFP to be associated only withthe use of surgical clips and not suture;however, the authors determined thatit was not possible to establish a plau-sible correlation because clips were
e1720 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

used in 91% of premature infants whoneeded PDA ligation. Carpes et al9
reported the use of cautery in 8 (100%)patients with UVFP, compared with 60(65%) patients without UVFP. Additionalinquiry in regard to surgical techniqueand perhaps operator learning curvemay be warranted.
Study Weaknesses
The inherentweaknessofourstudy isdueto the heterogeneity that is introducedwhen data are pooled from studies withnonuniform patient populations andmethods. Variability in the typeof surgery(PDA ligation versusothercardiothoracicsurgery), vocal fold assessment, andpatient demographics contributes to thisweakness. The random effects model forstatistical analysis and a priori subgroupanalyseswere undertaken to account forsome of these limitations.
Caseserieswerethemostcommontypeofstudy. This study type satisfied the criteriafor level 4 evidence according to theOCEBM; future studies should be aimedtoward higher levels of evidence. Signifi-cant publication bias was detected for allanalyses (type of surgery and post-operative vocal fold assessment) exceptfor thesubgroupof6studies that includedpatients who underwent PDA ligation onlyand routine postoperative assessment.
Recovery of Vocal Fold Function
Recovery of vocal fold function warrantsdiscussion. From the studies included inthis analysis, 2 studies reported no re-covery at follow-up points of 6 and 5 to 19months, respectively.34,36 The populationof patients with vocal fold paralysis inthese studies was 6 and 7 patients, re-spectively.34,36 Zbar et al34 hypothesizedthat their high rate of nonrecoveryresulted from the surgical clippingtechnique. Conversely, Khariwala et al22
reported a recovery rate of 82% (9 of 11patients) among their single-center ret-rospective review of patients undergoingsurgical repair of congenital cardiac
defects, attributing the rate of recoveryto stretching of the recurrent laryngealnerve and subsequent return of fullfunction. The time frame for this re-covery ranged from 8 weeks to 10months.22 Carpes et al9 also reportedrecovery of vocal fold movement in 3 of 7patients at 3 months’ follow-up. Spanoset al15 reported long-term follow-up of 6patients with UVFP. Follow-up rangedfrom 1 to 18 months, and of the 6patients, only 2 were found to have fullrecovery. Sachdeva et al19 reportedfollow-up in 9 patients with UVFP andfound recovery of function in 3 patients,partial recovery in 4 patients, and nosigns of recovery in 2 patients. Althoughexcluded from our current analysis be-cause their study population includedonly patients with UVFP, Truong et al41
reported a retrospective case series todetermine the rate of recovery of pedi-atric vocal fold paralysis after cardiacsurgery. They reported that 28 (35%)patients recovered function, with a me-dian time from diagnosis to recovery of6.6 months, and that 52 (65%) of patientshad persistent paralysis, with a medianfollow-up time of 16.4 months. Further-more, the authors reported that pre-mature patients were significantly lesslikely to recover vocal fold function. Giventhe wide variation of results, additionalinvestigation is needed to adequatelydetermine recovery of vocal fold functionafter cardiac surgery. However, it shouldbe noted that recovery of UVFP has beenreported as late as 11 years after theinitial surgery; therefore, the resultsshowing poor recovery may simply re-flect follow-up time that is too short.17
Surgical Management of UVFP
Early identification of UVFP would allowsubsequent surgical interventions suchas medialization laryngoplasty (injectionor surgical) or laryngeal reinnervation ifappropriate. Injection medialization lar-yngoplasty was reviewed in 13 patients(27 injections) with a variety of injectablematerials (Gelfoam, Radiesse Voice, or
Radiesse Voice Gel). Cohen et al42 dem-onstrated the procedure to be a safe andeffective treatment for carefully selectedpatients. Subjective or objective symptomimprovement was experienced in 24 of 27injections (89%). Zur43 reported her re-cent success with recurrent laryngealnerve reinnervation using the ansa cer-vicalis for unilateral vocal fold immobilityin children. Among10 children (9 ofwhomhad previous PDA ligation), 7 demon-strated physiologic frequency range im-provement at 6months’ follow-up.Mediantime from injury to repair was 64.5months. Paniello et al44 reported theresults of a multicenter randomized con-trolled trial comparing medialization lar-yngoplasty with laryngeal reinnervationand showed older patients to be bettersuited for laryngoplasty, whereas rein-nervation was better suited for youngerpatients. Given these possible surgicalinterventions, adequate postoperativeassessment of vocal fold function is war-ranted to identify patients who may ben-efit from these procedures. However,conservative management includingvoice therapy should always be con-sidered before surgical intervention.
Future Studies
Future studies should focus on pro-spectivelyenrollingandfollowingpatientsundergoing congenital cardiothoracicsurgery, assessing vocal fold functionroutinelypostoperatively,anddeterminingrisk factors, comorbidities, and long-termrespiratory function, swallowing, voiceoutcomes, and recovery rates.
CONCLUSIONS
UVFP is a demonstrated risk of cardio-thoracic surgery among infants andchildren. Pooled analysis suggests that itmay be associated with a younger ges-tational age and lower birth weight andweight at time of surgery. Routine post-operativenasopharyngolaryngoscopyforvocal cord assessment by an otolaryn-gologist is suggested.
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1721
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

REFERENCES
1. Clyman RI, Chorne N. Patent ductus arte-riosus: evidence for and against treatment.J Pediatr. 2007;150(3):216–219
2. Matsui H, McCarthy KP, Ho SY. Morphologyof the patent arterial duct: features rele-vant to treatment. Images Paediatr Cardiol.2008;10(1):27–38
3. Dedo DD, Dedo HH. Neurogenic diseases ofthe larynx. In: Bluestone CD, Stool SE, AlperCM, et al, eds. Pediatric Otolaryngology. 4thed. Philadelphia, PA: Saunders; 2003:1505–1510
4. Liberati A, Altman DG, Tetzlaff J, et al. ThePRISMA statement for reporting systematicreviews and meta-analyses of studies thatevaluate health care interventions: expla-nation and elaboration. J Clin Epidemiol.2009;62(10):e1–e34
5. OCEBM Levels of Evidence Working Group.The Oxford levels of evidence 2. OxfordCentre for Evidence-Based Medicine. Avail-able at: www.cebm.net/index.aspx?o=5653
6. Dewan K, Cephus C, Owczarzak V, OcampoE. Incidence and implication of vocal foldparesis following neonatal cardiac surgery.Laryngoscope. 2012;122(12):2781–2785
7. Heuchan AM, Hunter L, Young D. Outcomesfollowing the surgical ligation of the patentductus arteriosus in premature infants inScotland. Arch Dis Child Fetal Neonatal Ed.2012;97(1):F39–F44
8. Rukholm G, Farrokhyar F, Reid D. Vocalcord paralysis post patent ductus arterio-sus ligation surgery: risks and co-morbidities.Int J Pediatr Otorhinolaryngol. 2012;76(11):1637–1641
9. Carpes LF, Kozak FK, Leblanc JG, et al. As-sessment of vocal fold mobility before andafter cardiothoracic surgery in children.Arch Otolaryngol Head Neck Surg. 2011;137(6):571–575
10. Benjamin JR, Smith PB, Cotten CM, Jaggers J,Goldstein RF, Malcolm WF. Long-term morbid-ities associated with vocal cord paralysis af-ter surgical closure of a patent ductusarteriosus in extremely low birth weightinfants. J Perinatol. 2010;30(6):408–413
11. Roksund OD, Clemm H, Heimdal JH, et al.Left vocal fold paralysis after extremepreterm birth, a new clinical scenario inadults. Pediatrics. 2010;126(6). Available at:www.pediatrics.org/cgi/content/full/126/6/e1569
12. Sørensen CM, Steensberg JN, Greisen G.Surgical ligation of patent ductus arterio-sus in premature infants. Dan Med Bull.2010;57(6):A4160
13. Mandhan P, Brown S, Kukkady A, SamarakkodyU. Surgical closure of patent ductus arteriosus
in preterm low birth weight infants. CongenitHeart Dis. 2009;4(1):34–37
14. Smith ME, King JD, Elsherif A, Muntz HR,Park AH, Kouretas PC. Should all newbornswho undergo patent ductus arteriosus li-gation be examined for vocal fold mobility?Laryngoscope. 2009;119(8):1606–1609
15. Spanos WC, Brookes JT, Smith MC, BurkhartHM, Bell EF, Smith RJ. Unilateral vocal foldparalysis in premature infants after ligationof patent ductus arteriosus: vascular clipversus suture ligature. Ann Otol RhinolLaryngol. 2009;118(10):750–753
16. Srinivasan C, Sachdeva R, Morrow WR,et al. Standardized management improvesoutcomes after the Norwood procedure.Congenit Heart Dis. 2009;4(5):329–337
17. Clement WA, El-Hakim H, Phillipos EZ, Coté JJ.Unilateral vocal cord paralysis followingpatent ductus arteriosus ligation in ex-tremely low-birth-weight infants. Arch Oto-laryngol Head Neck Surg. 2008;134(1):28–33
18. Davis D, Davis S, Cotman K, et al. Feedingdifficulties and growth delay in childrenwith hypoplastic left heart syndrome ver-sus d-transposition of the great arteries.Pediatr Cardiol. 2008;29(2):328–333
19. Sachdeva R, Hussain E, Moss MM, et alVocal cord dysfunction and feeding diffi-culties after pediatric cardiovascular sur-gery. J Pediatr. 2007;151(3):312–315, 315.e1–2
20. Pereira KD, Webb BD, Blakely ML, Cox CS Jr,Lally KP. Sequelae of recurrent laryngealnerve injury after patent ductus arteriosusligation. Int J Pediatr Otorhinolaryngol.2006;70(9):1609–1612
21. Villa E, Folliguet T, Magnano D, VandenEynden F, Le Bret E, Laborde F. Video-assisted thoracoscopic clipping of patentductus arteriosus: close to the gold stan-dard and minimally invasive competitor ofpercutaneous techniques. J CardiovascMed (Hagerstown). 2006;7(3):210–215
22. Khariwala SS, Lee WT, Koltai PJ. Laryngo-tracheal consequences of pediatric cardiacsurgery. Arch Otolaryngol Head Neck Surg.2005;131(4):336–339
23. Skinner ML, Halstead LA, Rubinstein CS, AtzAM, Andrews D, Bradley SM. Laryngophar-yngeal dysfunction after the Norwood pro-cedure. J Thorac Cardiovasc Surg. 2005;130(5):1293–1301
24. Vida VL, Rubino M, Bottio T, et al. Thoraco-scopic closure of the patent arterial duct.Cardiol Young. 2004;14(2):164–167
25. Einarson KD, Arthur HM. Predictors of oralfeeding difficulty in cardiac surgicalinfants. Pediatr Nurs. 2003;29(4):315–319
26. Kohr LM, Dargan M, Hague A, et al. The in-cidence of dysphagia in pediatric patientsafter open heart procedures with trans-esophageal echocardiography. Ann ThoracSurg. 2003;76(5):1450–1456
27. Liang CD, Ko SF, Huang SC, Huang CF, Niu CK.Vocal cord paralysis after transcathetercoil embolization of patent ductus arterio-sus. Am Heart J. 2003;146(2):367–371
28. Niinikoski H, Alanen M, Parvinen T, AantaaR, Ekblad H, Kero P. Surgical closure ofpatent ductus arteriosus in very-low-birth-weight infants. Pediatr Surg Int. 2001;17(5–6):338–341
29. LeBlanc JG, Russell JL, Sett SS, Potts JE, Hu-man DG, Culham JA. The evolution of ductusarteriosus treatment. Int Surg. 2000;85(1):1–5
30. Russell JL, Leblanc JG, Potts JE, Sett SS. Issurgical closure of patent ductus arterio-sus a safe procedure in premature infants?Int Surg. 1998;83(4):358–360
31. Hawkins JA, Minich LL, Tani LY, Sturtevant JE,Orsmond GS, McGough EC. Cost and efficacyof surgical ligation versus transcatheter coilocclusion of patent ductus arteriosus. JThorac Cardiovasc Surg. 1996;112(6):1634–1638, discussion 1638–1639
32. Lavoie J, Burrows FA, Hansen DD. Video-assisted thoracoscopic surgery for thetreatment of congenital cardiac defects inthe pediatric population. Anesth Analg.1996;82(3):563–567
33. Rajasinghe HA, Reddy VM, van Son JA, et al.Coarctation repair using end-to-side anasto-mosis of descending aorta to proximal aorticarch. Ann Thorac Surg. 1996;61(3):840–844
34. Zbar RI, Chen AH, Behrendt DM, Bell EF,Smith RJ. Incidence of vocal fold paralysisin infants undergoing ligation of patentductus arteriosus. Ann Thorac Surg. 1996;61(3):814–816
35. Laborde F, Folliguet T, Batisse A, Dibie A,da-Cruz E, Carbognani D. Video-assistedthoracoscopic surgical interruption: thetechnique of choice for patent ductusarteriosus. Routine experience in 230 pe-diatric cases. J Thorac Cardiovasc Surg.1995;110(6):1681–1684, discussion 1684–1685
36. Fan LL, Campbell DN, Clarke DR, WashingtonRL, Fix EJ, White CW. Paralyzed left vocalcord associated with ligation of patentductus arteriosus. J Thorac CardiovascSurg. 1989;98(4):611–613
37. Davis JT, Baciewicz FA, Suriyapa S, Vauthy P,Polamreddy R, Barnett B. Vocal cord pa-ralysis in premature infants undergoingductal closure. Ann Thorac Surg. 1988;46(2):214–215
e1722 STRYCHOWSKY et al
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

38. Simpson CB. Treatment of vocal fold pa-ralysis. In: Bailey BJ, Johnson JT, NewlandsSD, eds. Otolaryngology Head & Neck Sur-gery. 4th ed. Philadelphia, PA: LippincottWilliams & Wilkins; 2006:848–866
39. Maturo SC, Braun N, Brown DJ, Chong PS,Kerschner JE, Hartnick CJ. Intraoperativelaryngeal electromyography in children withvocal fold immobility: results of a multicen-ter longitudinal study. Arch OtolaryngolHead Neck Surg. 2011;137(12):1251–1257
40. Wang LM, Zhu Q, Ma T, et al. Value of ul-trasonography in diagnosis of pediatricvocal fold paralysis. Int J Pediatr Oto-rhinolaryngol. 2011;75(9):1186–1190
41. Truong MT, Messner AH, Kerschner JE, et al.Pediatric vocal fold paralysis after cardiacsurgery: rate of recovery and sequelae.Otolaryngol Head Neck Surg. 2007;137(5):780–784
42. Cohen MS, Mehta DK, Maguire RC, SimonsJP. Injection medialization laryngoplasty in
children. Arch Otolaryngol Head Neck Surg.2011;137(3):264–268
43. Zur K. Recurrent laryngeal nerve reinner-vation for unilateral vocal fold immobilityin children. Laryngoscope. 2012;122(suppl 4):S82–S83
44. Paniello RC, Edgar JD, Kallogjeri D, PiccirilloJF. Medialization versus reinnervation forunilateral vocal fold paralysis: a multicen-ter randomized clinical trial. Laryngoscope.2011;121(10):2172–2179
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 e1723
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2013-3939 originally published online May 19, 2014; 2014;133;e1708Pediatrics
Julie E. Strychowsky, Gavin Rukholm, Michael K. Gupta and Diane ReidMeta-analysis
Unilateral Vocal Fold Paralysis After Congenital Cardiothoracic Surgery: A
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/133/6/e1708including high resolution figures, can be found at:
References
-1http://pediatrics.aappublications.org/content/133/6/e1708.full#ref-listThis article cites 40 articles, 1 of which you can access for free at:
Subspecialty Collections
rgery_subhttp://classic.pediatrics.aappublications.org/cgi/collection/cardiac_suCardiac Surgery_subhttp://classic.pediatrics.aappublications.org/cgi/collection/cardiologyCardiologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2013-3939 originally published online May 19, 2014; 2014;133;e1708Pediatrics
Julie E. Strychowsky, Gavin Rukholm, Michael K. Gupta and Diane ReidMeta-analysis
Unilateral Vocal Fold Paralysis After Congenital Cardiothoracic Surgery: A
http://pediatrics.aappublications.org/content/133/6/e1708located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 25, 2018http://pediatrics.aappublications.org/Downloaded from