undifferentiated carcinoma of the pancreas: analysis of intermediate filament profile and ki-ras...
TRANSCRIPT

, . 185: 53–60 (1998)
UNDIFFERENTIATED CARCINOMA OF THEPANCREAS: ANALYSIS OF INTERMEDIATE FILAMENT
PROFILE AND Ki-ras MUTATIONS PROVIDESEVIDENCE OF A DUCTAL ORIGIN
1, 2, . 2 ̈ ̈3*1Department of Pathology, Academic Hospital Jette, Free University of Brussels, Laarbeeklaan 101, B-1090 Brussels, Belgium
2ICRF Oncology Unit, RPMS, Hammersmith Hospital, London W12 0NN, U.K.3Department of Pathology, University of Kiel, Michaelisstrasse 11, D-24105 Kiel, Germany
SUMMARY
Undifferentiated carcinomas and osteoclast-like giant cell tumours of the pancreas commonly contain foci of neoplastic ductal glands.To test the hypothesis that undifferentiated carcinomas and osteoclast-like giant cell tumours have a ductal origin, the immunocyto-chemical cytokeratin pattern and the frequency and type of Ki-ras mutations at colon 12 were studied in a series of 17 undifferentiatedcarcinomas and two osteoclast-like giant cell tumours. The cytokeratin features of undifferentiated carcinomas and osteoclast-like giantcell tumours were compared with those found in 10 ductal adenocarcinomas, 20 acinar cell carcinomas, 25 neuroendocrine tumours, and15 solid-pseudopapillary tumours. All undifferentiated carcinomas and osteoclast-like giant cell tumours stained with at least onecytokeratin antibody, and 13/19 of them with antibodies against cytokeratins 7, 8, 18, and 19. The latter cytokeratins were expressedin all ductal adenocarcinomas, but only in 15/20 acinar cell carcinomas, 2/25 neuroendocrine tumours, and 1/15 solid-pseudopapillarytumours. In addition to cytokeratin, 15/19 undifferentiated carcinomas/osteoclast-like giant cell tumours were positive for vimentin.Ki-ras mutations at codon 12 were found in 10 undifferentiated carcinomas and one osteoclast-like giant cell tumour from which DNAcould be successfully amplified. The Ki-ras mutation patterns were analysed in six tumours and corresponded to those typical of ductaladenocarcinomas. In tumours with ductal and anaplastic components, both components revealed identical mutation patterns. From thesefindings, it is concluded that both undifferentiated carcinomas and osteoclast-like giant cell tumours belong to the pancreatic tumoursthat show a ductal phenotype. Since undifferentiated carcinomas and osteoclast-like giant cell tumours share the same cytokeratin andKi-ras features, they are probably derived from the same cell lineage. ? 1998 John Wiley & Sons, Ltd.
J. Pathol. 185: 53–60, 1998.
KEY WORDS—pancreatic tumours; undifferentiated carcinoma; osteoclast-like giant cell tumour; cytokeratin pattern; vimentin; Ki-rasmutation; ductal phenotype
INTRODUCTION
Undifferentiated carcinoma (UC) and osteoclast-likegiant cell tumour (OLGT) of the pancreas are rarepancreatic neoplasms, with a reported incidence varyingfrom 2·1 to 12·8 per cent.1 While UC has an unfavour-able prognosis, that of OLGT occasionally seems to bemuch better. Because focal glandular elements are acommon component of both tumour types,2–4 it isthought that they are of duct cell origin and represent avariant of ductal adenocarcinoma of the pancreas.1,5,6
Other possibilities that have been discussed are an originfrom acinar cells, especially for OLGT,7 and a primarilymesenchymal nature.3,8–10
Evidence of the ductal phenotype of the morefrequent adenocarcinoma of the pancreas can be foundin the histological and ultrastructural similarities
between the neoplastic glands and the interlobularpancreatic ducts. Further indications are that ductaladenocarcinomas express the same set of cytokeratinsas the normal duct cells of the pancreas, namely cyto-keratins (CKs) 7, 8, 18, and 19.11–14 Finally, ductaladenocarcinomas are characterized by a high frequencyof mutation in the oncogene Ki-ras, a feature which isabsent or only rarely present in pancreatic neoplasmswith acinar or endocrine cell differentiation.15,16
In this study, we analysed a series of 17 UCs and twoOLGTs of the pancreas by means of immunocytochem-istry and molecular biology. In particular, we looked forevidence of their ductal origin and their relationship toductal adenocarcinoma. For this purpose, we comparedtheir intermediate filament expression with that of othertypes of pancreatic tumours. We also investigatedwhether the frequency of Ki-ras gene activation in UC issimilar to that of ductal adenocarcinomas.17–20
MATERIALS AND METHODS
We investigated a series of 17 UCs and two OLGTs ofthe pancreas. The most important clinicopathologicalfindings are summarized in Table I. The age of the
*Correspondence: Professor G. Klöppel, Department of Pathology,University of Kiel, Michaelisstrasse 11, D-24105 Kiel, Germany.
Contract grant sponsor: Belgian National Fund for ScientificResearch (FGWO); Contract grant number: V41B-MW.D4738).
Contract grant sponsors: Deutsche Krebshilfe; Imperial CancerResearch Fund; Medical Research Council; Mike Stone CancerResearch Fund.
CCC 0022–3417/98/050053–08 $17.50? 1998 John Wiley & Sons, Ltd.
Received 2 May 1997Accepted 31 October 1997

patients ranged from 44 to 96 years (mean 63 years).The male to female ratio was 11:8. In 11 patients alaparotomy was performed, which led to a Whippleresection in ten patients and a tail resection inone patient. Autopsy specimens were available fromeight patients. For purposes of comparison, weinvestigated a series of 10 ductal adenocarcinomas,20 acinar cell carcinomas, 25 neuroendocrinetumours (12/25 malignant and 9/25 functioning), and 15solid-pseudopapillary tumours.
The tumour specimens were fixed in 10 per centformaldehyde, except for five samples which werefixed in Bouin’s solution. Four-micrometre-thick serialsections were cut from paraffin-embedded tissue blocks(1–5 per specimen, mean 2). The first two sectionswere stained with haematoxylin and eosin (H&E)and periodic acid–Schiff with diastase pretreatment.
Immunocytochemical analysis was carried out onsubsequent sections by means of the streptavidin–biotin–peroxidase complex method. The sections werestained with the primary antisera listed in Table II.Peroxidase staining was done using 3,3*-diaminobenzidine tetra-hydrochloride (0·05 per centw/v) and hydrogen peroxide (0·01 per cent w/v) inphopshate-buffered saline (PBS) buffer. For antigenretrieval of CKs 7, 8, 18, and 19, deparaffinized sectionswere pretreated with 0·1 per cent trypsin (Sigma) for1–10 min. Sections from normal pancreas (n=5) wereused as positive controls for the antisera againstintermediate filaments and neuroendocrine markers.
All 19 tumours were examined for abnormalities inKi-ras at codon 12. In all tumours with a ductalcomponent, Ki-ras codon 12 was analysed in two differ-ent tumour areas, a region with ductal structures and a
Table I—Clinicopathological findings in 19 patients with pancreatic undifferentiated carcinomas (UCs) orosteoclast-like giant cell tumours (OLGTs)
Case No.
Age (years)/sex/type ofresection
Pleomorphiccarcinoma type
Site(in pancreas)
Size(cm)
Ductalcomponent
1 44/F/W UC Head 7#5#5 +2 44/F/W UC Head 6#4#4 +3 44/M/W UC Head 5#4#4 +4 46/M/W UC Head 3#2#1·5 +5 53/M/A UC Body 5#5#4 "6 55/M/W UC Head 2#1·5#1·5 +7 58/M/W UC Head 3#2·5#2·5 "8 62/M/W UC Head 3#2·5#2·5 +9 63/F/A UC Body–tail 7#6#4 "
10 65/F/T UC Tail 5#5#4 "11 71/M/W UC Head 6#4#2 "12 71/M/A UC Body 8#7#5 "13 73/M/W UC Head–body 9#8#8 "14 78/M/A UC Tail 6#4#4 +15 86/F/A UC Head 4#4#3·5 +16 91/F/A UC Body 5#5#4 +17 96/F/A UC Tail 6#5#5 +18 44/F/W OLGT Head 6#5#5 +19 57/M/A OLGT Head–body 6#6#5 +
F=female patient; M=male patient; A=autopsy; W=whipple resection; T=tail resection; + =present; " =absent.
Table II—Antisera
AntigenAntiserum
codeWorkingdilution Source
Keratins 1, 2, 5, 6, 7, 8, 11, 14, 16, 17, and 18 M (KL1) 1:500 Immunotech, Marseille, FranceKeratins 8, 18, and 19 M (CAM 5.2) 1:10 Becton Dickinson, Mountain View, CA, U.S.A.Keratin 7 M (CK 7) 1:100 Biogenex, San Ramon, CA, U.S.A.Keratin 8 M (CK 8) 1:100 Biogenex, San Ramon, CA, U.S.A.Keratin 18 M (CK 18) 1:10 Biogenesis, Bournemouth, U.K.Keratin 19 M (CK 19) 1:20 Dr Raemaekers, Nijmegen, The NetherlandsVimentin (Vim) M 1:20 Boehringer, Mannheim, GermanyCD45, leucocyte common antigen (LCA) M 1:50 Dako, Glostrup, DenmarkCD68 M (KP1) 1:500 Dako, Glostrup, Denmark
P=polyclonal; M=monoclonal.
54 A. HOORENS ET AL.
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)

region with a pleomorphic, undifferentiated phenotype.For detection of Ki-ras mutations, genomic DNA wasextracted from sections cut from paraffin-embeddedtissue blocks as described by Levi et al.21 Briefly, 10 ìmsections were made from each block. The area of interestwas microdisected with sterile scalpels and 18-gaugeneedles, placed in a sterile Eppendorf tube, dewaxed intwo changes of warm xylene, and washed twice inalcohol before drying. The tissue was then resuspendedin digestion buffer (50 m Tris–HCl, 1 m EDTA, 0·5per cent Tween 20, pH 8·0) containing 0·1 mg/ml pro-teinase K (Sigma Chemical Co., St Louis, MO, U.S.A.)and incubation at 37)C overnight. Nucleic acid waspurified by organic extraction with phenol/chloroformand then chloroform. The nucleic acid was then ethanol-precipitated, washed, and dried before dissolving in200 ìl of Tris–EDTA buffer. Ten microlitres of sampleDNA solution was used for each polymerase chainreaction (PCR) amplification. Genomic DNA wasamplified in a volume of 100 ml containing 75 m KCl,10 m Tris–HCl (pH 8·8), 1·5 m MgCl2, 0·4 m ofeach of four dNTPs (Pharmacia, Piscataway, NJ,U.S.A.), 0·4 ìg of a pair of primers (K12F:5*-CATGTTCTAATATAGTCACA-3*, K12A1:5*-CGTCAAGGCACTCTTGCC-3*), and 1 unit of TaqDNA polymerase (Perkin Elmer Cetus Corp., Norwalk,CT, U.S.A.). The conditions for the PCR using athermal cycler (Perkin Elmer Cetus) were as follows:95)C for 5 min for initial denaturation, 35 cycles of 94)Cfor 30 s, annealing for 45 s at 42)C, and extension at72)C for 30 s. The efficiency of amplification waschecked by electrophoresis of an aliquot of each reactionin agarose gel before single-strand conformation poly-morphism (SSCP) analysis was performed. 0·5 ìl of thisproduct mix was taken as template for a further tencycles of amplification in 20 ìl of reaction mix preparedin the same proportions as the initial amplificationexcept for the addition of 1 ìCi of 32P-á-dATP. Twomicrolitres of the radioactively labelled product wasloaded on a 6 per cent non-denaturing acrylamide gelwith 10 per cent glycerol and run at 4 W overnight at
room temperature. In addition, mutations at codon 12of the Ki-ras oncogene were detected by the method ofLevi et al.,21 in which mismatched primers (Fig. 1) areused in the PCR to create restriction fragment lengthpolymorphisms (RFLPs). Samples were screened for thepresence or absence of the wild-type sequence by BstNIdigestion of DNA produced by amplification with prim-ers K12S and K12ABstNI. Twenty microlitres of the100 ìl PCR was digested with the restriction enzymeBstNI (Promega Ltd, Southampton, U.K.). The reactionconditions adhered to the supplier’s recommendations.The DNA was then electrophoresed through 2·5 per centNusieve/1 per cent agarose gel and the ethidiumbromide-stained gel was photographed using an ultra-violet light transilluminator and a gel documentationsystem (UltraViolet Products, Cambridge, U.K.). Thosesamples in which a mutant sequence was suspected werefurther investigated by cloning the cold PCR products inpBluescript. A single-stranded template was obtainedby phage rescue. It was sequenced in an automaticsequencing machine (Applied Biosystems ABI 373,Norwalk, CT, U.S.A.).
RESULTS
Histological findings
All UCs exhibited pleomorphic cells growing inpoorly cohesive sarcomatoid formations, supported by ascanty fibrous stroma. Mononuclear tumour cells wereadmixed with bizarre, mononucleated or multinucleargiant cells. All cells had hyperchromatic nuclei andusually eosinophilic cytoplasm. In seven tumours themultinucleated neoplastic giant cells were very abundantand prominent (Fig. 2). Four tumours contained areaswith small and more spindle-shaped tumour cells (Fig.3). In 12 tumours, either single (five cases) or multiplefoci of neoplastic duct-like structures were found.Scattered areas of necrosis were present in about halfof the cases. Mitoses were always very abundant. Thetwo OLGTs displayed numerous benign-appearing
Fig. 1—DNA from the microdissected tissue samples was amplified with the primers K12S and K12ABstNI, and thendigested with BstNI and run in 2·5 per cent Nusieve/1 per cent agarose gel. Undigested PCR product is a fragment of157 bp, while BstNI digestion produces a fragment of 143 bp in Ki-ras 12 mutant DNA and a fragment of 114 bp inKi-ras 12 wild-type DNA. Samples 1a, 14, and 15 have homozygous mutant Ki-ras and samples 19, 8a/b, 16a/b, and2a/b have heterozygous mutant Ki-ras patterns
55UNDIFFERENTIATED CARCINOMA OF THE PANCREAS
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)

osteoclast-like giant cells, which were scatteredamong pleomorphic mononuclear tumour cells andspindle-shaped fibroblast-like cells.
Immunocytochemical findings
Normal pancreatic duct cells contained CKs 7, 8, 18,and 19, while normal acinar cells and pancreaticendocrine cells were only positive for CKs 8 and 18.
All 17 UCs and two OLGTs were positive for at leastone of the antisera directed against various cytokeratins.KL1, which is a broad spectrum keratin marker, stained18/19 tumours. The one tumour that was KL1-negativewas positive for CK 7. All but two tumours stained forCAM 5·2 (which detects CKs 8, 18, and 19), while CK 7was found in 18 tumours (Table III and Fig. 4). In 15tumours (including one of the two OLGTs), the neoplas-tic cells were also positive for vimentin (Fig. 5). Amongthe tumour cells, there were usually macrophages whichwere labelled by the markers LCA and CD68, inaddition to vimentin. In the two OLGTs, the non-neoplastic osteoclast-like cells stained for vimentin,LCA and CD68. The LCA staining was in a finesubmembranous pattern.
All but one ductal adenocarcinoma were positive forCKs 7, 8, 18, and 19. The 20 acinar cell carcinomasstained positively for CKs 8 and 18, but 18 cases were
additionally positive for CKs 7 and/or 19. None of theductal adenocarcinomas or acinar cell carcinomasshowed positively for vimentin.
In the series of 25 neuroendocrine neoplasms, 23/25tumours were positive for CK 8 and 25/25 for CK 18.Only two cases were faintly positive for CK 7, and 10/25tumours expressed CK 19. One of the 25 tumours waspositive for vimentin. We found no correlation betweenpositivity for CK 7 or 19 and malignancy or functionalstate.
All but three solid-pseudopapillary tumours werepositive for vimentin, while cytokeratin expression wasfound in only six tumours (Table III). None of thetumours stained for CD45 (LCA) or CD68.
Molecular analysis
PCR failed repeatedly on samples from eight patients(cases 3, 5, 6, 9, 11, 12, 13, and 19), but was successful in11 cases (cases 1, 2, 4, 7, 8, 10, 14, 15, 16, 17, and 18), sixof which also contained a ductal component (cases 1, 2,4, 8, 16, and 18). SSCP analysis was able to identify onlyone case with a possible abnormality (case 4). By meansof RFLP, however, it was possible to demonstratemutations of codon 12 in all 11 cases in which DNA wassuccessfully amplified (Fig. 1). Automatic sequencing ofPCR fragments of exon 1 was successful in six of these
Fig. 2—Undifferentiated carcinoma of the pancreas showing abundantpleomorphic neoplastic giant cells (H&E, #120)
Fig. 3—Undifferentiated carcinoma of the pancreas. Pleomorphictumour cells next to an area with spindle-shaped cells (H&E, #120)
56 A. HOORENS ET AL.
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)

11 cases (cases 1, 2, 4, 14, 15, and 18). In two cases each,the mutations were G to C transversion at position 1, Gto T transversion at position 1, and G to A transversionat position 2. In all cases with a ductal component inwhich a mutation was found, it was identical in both theundifferentiated component and the ductal component.
DISCUSSION
Undifferentiated or anaplastic carcinoma (UC) of thepancreas is an uncommon tumour with a poor progno-sis.1,5,22 Because of its sarcomatoid appearance, electronmicroscopy and/or immunocytochemistry are required
to demonstrate the tumour’s epithelial nature. A further,though inconsistent, indication of its epithelial origin isthat neoplastic glandular elements and duct-like struc-tures may be observed in some of the tumours. Thetumour is therefore considered to be a variant of ductaladenocarcinoma.1,5,23 A similar histogenetic originhas been discussed for the osteoclast-like giant celltumour (OLGT) of the pancreas, since it also maycontain a ductal component.2–4,24 However, it has alsobeen reported that the neoplastic cells in OLGT donot stain for cytokeratin and also do not show anyevidence of epithelial differentiation by electronmicroscopy.3,9 Against the background of theseconflicting results, we conducted a study to analyse thecell lineage pattern in UC and OLGT and to test themfor Ki-ras codon 12 activation, a well-known feature ofductal adenocarcinoma.25
Our results provide strong evidence of a ductal originof UC and OLGT. Firstly, we found that more thantwo-thirds of the UCs and OLGTs stained for anti-bodies directed against CKs 7, 8, 18, and 19 of Mollet al.’s catalogue.26 This CK pattern characterizes thepancreatic duct cell system and also ductaladenocarcinoma.11–13,27,28 Secondly, in all tumours ofour series in which we were able to perform a molecularanalysis (ten of 17 UCs and one of two OLGTs), aKi-ras point mutation at codon 12 was demonstrated,confirming recently published data.29,30
In the normal pancreas, ductal cells contain CKs 7, 8,18, and 19, while acinar cells and endocrine cells expressonly CKs 8 and 18.11–13,28 In addition to CKs 7, 8, 18,and 19, some duct cells may also stain for CKs 4, 5, 14,and 17.12,1428 Pancreatic tumours with a ductal pheno-type express the same set of CKs as the normalduct cells, i.e., predominantly CKs 7, 8, 18, and19.11–13,27,28,31 Expression of additional CKs, such asCK 14, may be observed in pancreatic carcinomas witha squamous component,12 and CK 20, a relatively newmember of this class of intermediate filaments,32 seemsto be only exceptionally expressed in ductal adenocarci-nomas of the pancreas.32 Since, with five exceptions, the17 UCs of our series reacted with antibodies against thefour ‘ductal’ CKs, i.e., CKs 7, 8, 18, and 19, we concludethat the majority of UCs adhere to the phenotype ofductal adenocarcinoma. This also holds true for the twoOLGTs examined, since they both displayed a ductalCK pattern.
The neoplastic counterparts of pancreatic acinar orendocrine cells, acinar cell carcinomas and neuroendo-crine tumours, only partly matched the CK pattern of
Table III—Cytokeratin and vimentin expression in pancreatic tumours
Tumourtype KL1
CAM5.2 CK 7 CK 8 CK 18 CK 19 Vim
Undifferentiated carcinoma 18/19 17/19 18/19 13/19 15/19 17/19 15/19Ductal carcinoma 10/10 10/10 10/10 9/10 10/10 10/10 0/10Acinar cell carcinoma 20/20 20/20 15/20 20/20 20/20 15/20 0/20Neuroendocrine tumours 25/25 25/25 2/25 23/25 25/25 10/25 1/25Solid-pseudopapillary tumours 6/15 1/15 1/15 2/15 1/15 2/15 12/15
Fig. 4—Undifferentiated carcinoma of the pancreas. Both neoplasticductal structures and anaplastic tumour cells stain positively for CK 19(#120)
57UNDIFFERENTIATED CARCINOMA OF THE PANCREAS
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)
the respective normal cells. They almost all stained forCKs 8 and 18, but some were additionally positive forCKs 7 and/or 19. In acinar cell carcinomas, CK 7 and/orCK 19 reactivity was seen in two-thirds of the tumours,while in endocrine tumours, CK 7 was only expressed intwo cases and CK 19 in ten tumours. This deviationfrom the normal CK pattern, which may be attributed tothe loss of cellular differentiation in these neoplasms,shows that pancreatic tumours with either a ductal,acinar, or endocrine phenotype cannot be distinguishedfrom each other on the basis of their reactivity with CK7, 8, 18, or 19 with certainty in all cases. Additional testsare necessary to make this distinction. We therefore alsotested the UCs and OLGTs of our series for the neuro-endocrine marker synaptophysin and the pancreaticenzymes trypsin and lipase15,33,34 and obtained negativeresults (data not shown). These data further support theductal origin of UC and OLGT of the pancreas.
Vimentin expression is absent in pancreatic acinarcell carcinomas. It is a very rare finding in pancreaticductal adenocarcinomas13 or neuroendocrine tumours(one tumour in our series), but is common in solid-pseudopapillary tumours,35,36 in which CK expressionappears to be rather the exception. Positivity for vimen-tin is also a frequent finding in our series of UCs andOLGTs, being observed in 75 per cent of cases. Thisfinding has been interpreted as an indication of a
mesenchymal origin of the tumour cells.3,8,10 Expressionof vimentin in carcinomas is, however, a well-knownphenomenon in other anaplastic carcinomas, such asanaplastic thyroid or hepatocellular carcinomas.10,28,37
The expression of vimentin in UC and OLGT of thepancreas cannot therefore be considered as evidence of aprimarily mesenchymal nature of the tumour. The dis-crepancy between our findings and reports in whichOLGTs were found to be positive only for vimentin andto lack any CK staining may be attributed to the failureof the antiserum or the technique used to detect CK,rather than to the lack of CK expression. In our study,we found that proper immunocytochemical recognitionof some CKs required digestive treatment of the sectionsprior to staining.
Ki-ras mutation at codon 12 is a feature of ductaladenocarcinomas of the pancreas, occurring in 80–100per cent of the cases.16,25 In other pancreatic tumourswith a ductal phenotype, such as intraductal papillarymucinous tumour, Ki-ras mutations are found in avarying frequency.38 In contrast, pancreatic tumourswith an acinar or endocrine phenotype almost alwayslack Ki-ras mutations.15,39 Our results in UC and OLGTconfirm the data of two recently published studies,29,30
in that they reveal the same high rate of Ki-ras muta-tions as in ductal adenocarcinoma.16,25 In addition, wefound that in the four cases in which we were able to test
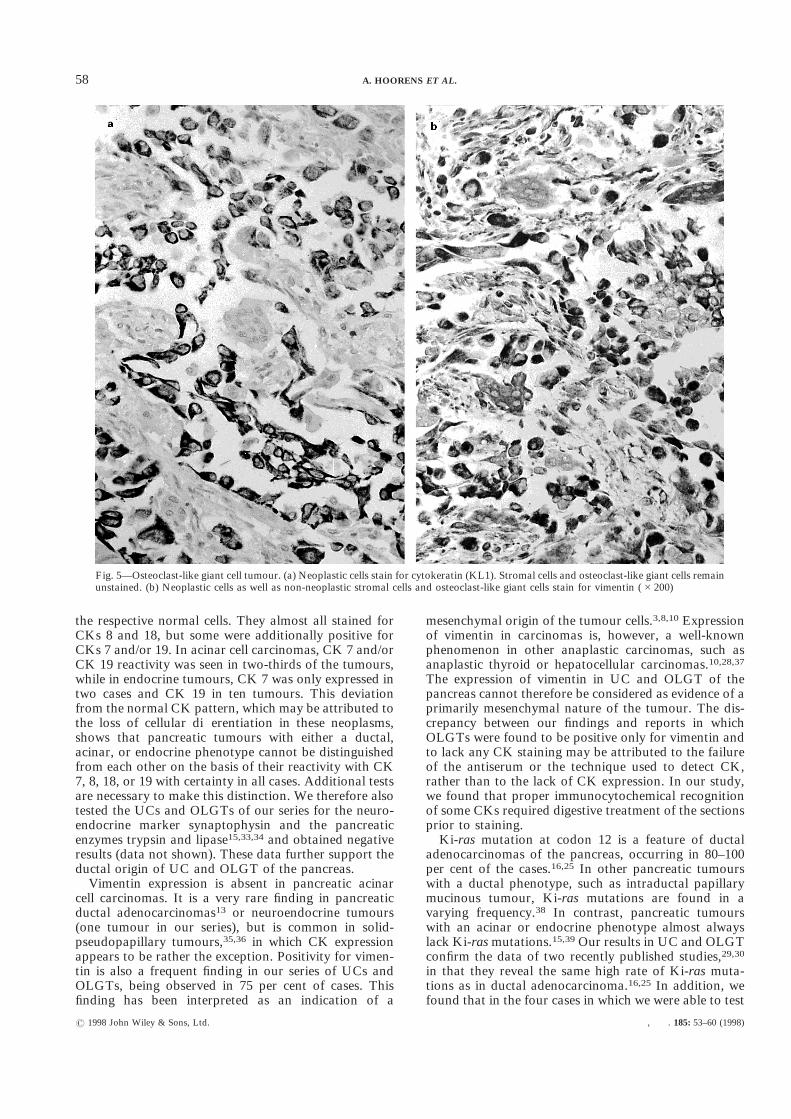
Fig. 5—Osteoclast-like giant cell tumour. (a) Neoplastic cells stain for cytokeratin (KL1). Stromal cells and osteoclast-like giant cells remainunstained. (b) Neoplastic cells as well as non-neoplastic stromal cells and osteoclast-like giant cells stain for vimentin (#200)
58 A. HOORENS ET AL.
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)

a microdissected focus with ductal differentiation forKi-ras mutations and compare its Ki-ras pattern withthat of the adjacent undifferentiated part of the tumour,the same mutation pattern was present in both compo-nents. Finally, the spectrum of mutations detected, i.e.,GGT to TGT, GGT to CGT, and GGT to GAT,corresponds to that most frequently found in ductaladenocarcinoma series.16 On the basis of these findingsand the CK features already discussed, we thereforeconclude that pancreatic UCs and OLGTs are derivedfrom ductal adenocarcinomas. Further support for thisconclusion is provided by the finding that UCs may stainfor pancreatic and gut-type antigens, which are alsofound in ductal adenocarcinomas.40
It is still controversial whether UC and OLGT are twoseparate entities or belong to one group of tumours. Inthe new WHO classification, they are viewed as twocategories.23 Apart from the assumed mesenchymalnature of OLGT, the notion exists that UC and OLGTmight differ in biology because OLGT has a potentiallybetter prognosis. Our findings, however, lead us tobelieve that UC and OLGT are derived from the samecell lineage and therefore have a common origin. OLGTmay be regarded as a variant of UC distinguished by aspecial response of non-neoplastic giant cells to poorlydifferentiated epithelial tumour cells. The non-neoplasticnature of the giant cells has been established in severalprevious reports.3,4,41 The identification as cells of themesenchyme system with features of osteoclast cells isbased on the positive labelling with vimentin and mono-nuclear phagocytic markers such as CD68 and CD45(common leukocyte antigen). Why some of the OLGTsseem to have a much better prognosis than UCs is notknown,42 but it may be related to the response of theinfiltrating non-neoplastic giant cells to tumour cells.
ACKNOWLEDGEMENTS
Anne Hoorens and Günter Klöppel were supportedby a grant from the Belgian National Fund for ScientificResearch (FGWO; V4/B—MW.D4738); Klaus Prenzelby a grant from Deutsche Krebshilfe; and NicholasLemoine by grants from the Imperial Cancer ResearchFund, Medical Research Council, and the Mike StoneCancer Research Fund. We thank Mrs N. Buelens fortechnical assistance and Mrs K. Dege for secretarialwork and helpful English corrections. We are alsograteful to the many colleagues who provided materialand clinical data for this study.
REFERENCES
1. Klöppel G. Pancreatic, non-endocrine tumours. In: Klöppel G, Heitz PU,eds. Pancreatic Pathology. Edinburgh: Churchill Livingstone, 1984; 79–113.
2. Trepeta RW, Mathur B, Lagin S, LiVolsi VA. Giant cell tumor (‘osteoclas-toma’) of the pancreas: a tumor of epithelial origin. Cancer 1981; 48:2022–2028.
3. Fischer HP, Altmannsberger M, Kracht J. Osteoclast-type giant cell tumourof the pancreas. Virchows Arch A [Pathol Anat] 1988; 412: 247–253.
4. Nojima T, Nakamura F, Ishikura M, Inoue K, Nagashima K, Kato H.Pleomorphic carcinoma of the pancreas with osteoclast-like giant cells. Int JPancreatol 1993; 14: 275–281.
5. Cubilla AL, Fitzgerald PJ. Tumors of the Exocrine Pancreas. Washington,DC: Armed Forces Institute of Pathology, 1984.
6. Morohoshi T, Held G, Klöppel G. Exocrine pancreatic tumours and theirhistological classification. A study based on 167 autopsy and 97 surgicalcases. Histopathology 1983; 7: 645–661.
7. Rosai J. Carcinoma of pancreas simulating giant cell tumor of bone.Electron-microscopic evidence of its acinar cell origin. Cancer 1968; 22:333–344.
8. Suster S, Phillips M, Robinson MJ. Malignant fibrous histocytoma (giantcell type) of the pancreas. A distinctive variant of osteoclast-type giant celltumor of the pancreas. Cancer 1989; 64: 2302–2308.
9. Goldberg RD, Michelassi F, Montag AG. Osteoclast-like giant cell tumorof the pancreas: immunophenotypic similarity to giant cell tumor of bone.Hum Pathol 1991; 22: 618–622.
10. Lewandrowski KB, Weston L, Dickersin GR, Rattner DW, Compton CC.Giant cell tumor of the pancreas of mixed osteoclastic and pleomorphic celltype: evidence for a histogenetic relationship and mesenchymal differentia-tion. Hum Pathol 1990; 21: 1184–1187.
11. Osborne M, van Essen G, Weber K, Klöppel G, Altmannsberger M.Differential diagnosis of gastrointestinal carcinomas by using monoclonalantibodies specific for individual keratin polypeptides. Lab Invest 1986; 55:497–594.
12. Schüssler MH, Skoudy A, Ramaekers F, Real FX. Intermediate filaments asdifferentiation markers of normal pancreas and pancreas cancer. Am JPathol 1992; 140: 559–568.
13. Santini D, Ceccarelli C, Martinelli GN, et al. Expression of intermediatefilaments in normal and neoplastic exocrine pancreas. Zentralbl Pathol1994; 140: 247–258.
14. Real FX, Vilá MR, Skoudy A, Ramaekers FCS, Corominas JM. Intermedi-ate filaments as differentiation markers of exocrine pancreas. II. Expressionof cytokeratins of complex and stratified epithelia in normal pancreas and inpancreas cancer. Int J Cancer 1993; 54: 720–727.
15. Hoorens A, Lemoine NR, McLellan E, et al. Pancreatic acinar cellcarcinoma. An analysis of cell lineage markers, p53 expression, and Ki-rasmutation. Am J Pathol 1993; 143: 685–698.
16. Hruban RH, van Mansfield ADM, Offerhaus GJA, et al. K-ras oncogeneactivation in adenocarcinoma of the human pancreas. A study of 82carcinomas using a combination of mutant-enriched polymerase chainreaction analysis and allele-specific oligonucleotide hybridization. Am JPathol 1993; 143: 545–554.
17. Almoguera C, Shibata D, Forrester K, Martin J, Arnheim N, Perucho M.Most human carcinomas of the exocrine pancreas contain mutant c-K-rasgenes. Cell 1988; 53: 549–554.
18. Smit VTBH, Boot AJM, Smits AMM, Focuren GJ, Cornelasse CJ, Bos JL.K-ras codon 12 mutations occur very frequently in pancreatic adenocarci-noma. Nucleic Acids Res 1988; 16: 7773–7782.
19. Grünewald K, Lyons J, Fröhlich A, et al. High frequency of Ki-ras codon12 mutations in pancreatic adenocarcinomas. Int J Cancer 1989; 43:1037–1041.
20. Lemoine NR, Jain S, Hughes CM, et al. Ki-ras oncogene activation inpreinvasive pancreatic cancer. Gastroenterology 1992; 102: 230–236.
21. Levi S, Urbano-Ispizua A, Gill R, et al. Multiple k-ras codon 12 mutationsin cholangiocarcinomas demonstrated with a sensitive polymerase chainreaction technique. Cancer Res 1991; 51: 3497–3592.
22. Tschang TP, Garza-Garza R, Kissane JM. Pleomorphic carcinoma of thepancreas: an analysis of 15 cases. Cancer 1977; 39: 2114–2126.
23. Klöppel G, Solcia E, Longnecker DS, Capella C, Sobin LH. HistologicalTyping of Tumours of the Exocrine Pancreas. 2nd edn. WHO InternationalHistological Classification of Tumours. Berlin: Springer-Verlag, 1996.
24. Hinze R, Knolle J, Holzhausen HJ, Wessel H, Bahn H, Moll R. Pankreas-tumoren mit Riesenzellen vom Osteoklastentyp—immunhistochemische,enzymhistochemische und ultrastrukturelle Untersuchungen. Verh DtschGes Pathol 1996; 80: 668.
25. Klöppel G. Gene changes and pancreatic carcinoma: the significance ofK-ras. Dig Surg 1994; 11: 164–169.
26. Moll R, Franke WW, Schiller DL, Geiger B, Krepler R. The catalog ofhuman cytokeratins: patterns of expression in normal epithelia, tumors andcultured cells. Cell 1982; 31: 11–24.
27. Herzig KH, Altmannsberger M, Fölsch UR. Intermediate filaments in ratpancreatic acinar tumors, human ductal carcinomas, and other gastrointes-tinal malignancies. Gastroenterology 1994; 106: 1326–1332.
28. Vilá MR, Balagué C, Real FX. Cytokeratins and mucins as molecularmarkers of cell differentiation and neoplastic transformation in the exocrinepancreas. Zentralbl Pathol 1994; 140: 225–235.
29. Janatpour KD, Teplitz R, Min B, Heffes C, Gumerlock P, Ruebner BH.Pancreatic tumors with osteoclastic and pleomorphic giant cells. ModPathol 1995; 8: 129 (Abstract 754)..
30. Gocke CD, Dabbs DJ, Benko FA, Silverman JF. KRAS oncogene muta-tions suggest a common histogenetic origin for pleomorphic giant cell tumorof the pancreas, osteoclastoma of the pancreas, and pancreatic ductadenocarcinoma. Hum Pathol 1997; 28: 80–83.
31. Egawa N, Maillet B, Schröder S, Foulis A, Mukai K, Klöppel G. Serousoligocystic and ill-demarcated adenoma of the pancreas: a variant of serouscystic adenoma. Virchows Arch 1994; 424: 13–17.
32. Moll R, Löwe A, Laufer J, Franke WW. Cytokeratin 20 in humancarcinomas. A new histodiagnostic marker detected by monoclonal anti-bodies. Am J Pathol 1992; 140: 427–447.
59UNDIFFERENTIATED CARCINOMA OF THE PANCREAS
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)

33. Morohoshi T, Kanda M, Horie A, et al. Immunocytochemical markers ofuncommon pancreatic tumors. Acinar cell carcinoma, pancreatoblastoma,and solid cystic (papillary-cystic) tumor. Cancer 1987; 59: 739–747.
34. Klimstra DS, Heffess CS, Oertel JE, Rosai J. Acinar cell carcinoma of thepancreas: a clinicopathologic study of 28 cases. Am J Surg Pathol 1992; 16:815–837.
35. Pettinato G, Manivel JC, Ravetto C, et al. Papillary cystic tumor of thepancreas. A clinicopathologic study of 20 cases with cytologic, immuno-histochemical, ultrastructural, and flow cytometric observations, and areview of the literature. Am J Clin Pathol 1992; 98: 478–488.
36. Klöppel G, Maurer R, Hofmann E, et al. Solid-cystic (papillary-cystic)tumours within and outside the pancreas in men: report of two patients.Virchows Arch A [Pathol Anat] 1991; 418: 179–183.
37. Haratake J, Horie A. An immunohistochemical study of sarcomatoid livercarcinomas. Cancer 1991; 68: 93–97.
38. Sessa F, Solcia E, Capella C, et al. Intraductal papillary-mucinous tumoursrepresent a distinct group of pancreatic neoplasms: an investigation oftumour cell differentiation and K-ras, p53, and c-erbB-2 abnormalities in 26patients. Virchows Arch 1994; 425: 357–367.
39. Pellegata NS, Sessa F, Renault B, et al. K-ras and p53 gene mutations inpancreatic cancer: ductal and nonductal tumors progress through differentgenetic lesions. Cancer Res 1994; 54: 1556–1560.
40. Sessa F, Bonato M, Frigerio B, et al. Ductal cancers of the pancreasfrequently express markers of gastrointestinal epithelial cells. Gastroenter-ology 1990; 98: 1655–1665.
41. Newbould MJ, Benbow EW, Sene A, Young M, Taylor TV. Adenocarci-noma of the pancreas with osteoclast-like giant cells: a case report withimmunocytochemistry. Pancreas 1992; 7: 611–615.
42. Dworak O, Wittekind C, Koerfgen HP, Gall FP. Osteoclastic giant celltumor of the pancreas. An immunohistological study and review of theliterature. Pathol Res Pract 1993; 189: 228–231.
60 A. HOORENS ET AL.
? 1998 John Wiley & Sons, Ltd. , . 185: 53–60 (1998)