understanding the costs and benefits of health information
TRANSCRIPT

U.S. Department of Health and Human Services Assistant Secretary for Planning and Evaluation
Office of Disability, Aging and Long-Term Care Policy
UNDERSTANDING THE COSTS AND BENEFITS OF HEALTH
INFORMATION TECHNOLOGY IN NURSING HOMES AND HOME HEALTH AGENCIES:
CASE STUDY FINDINGS
June 2009

Office of the Assistant Secretary for Planning and Evaluation The Office of the Assistant Secretary for Planning and Evaluation (ASPE) is the principal advisor to the Secretary of the Department of Health and Human Services (HHS) on policy development issues, and is responsible for major activities in the areas of legislative and budget development, strategic planning, policy research and evaluation, and economic analysis. ASPE develops or reviews issues from the viewpoint of the Secretary, providing a perspective that is broader in scope than the specific focus of the various operating agencies. ASPE also works closely with the HHS operating divisions. It assists these agencies in developing policies, and planning policy research, evaluation and data collection within broad HHS and administration initiatives. ASPE often serves a coordinating role for crosscutting policy and administrative activities. ASPE plans and conducts evaluations and research--both in-house and through support of projects by external researchers--of current and proposed programs and topics of particular interest to the Secretary, the Administration and the Congress.
Office of Disability, Aging and Long-Term Care Policy The Office of Disability, Aging and Long-Term Care Policy (DALTCP), within ASPE, is responsible for the development, coordination, analysis, research and evaluation of HHS policies and programs which support the independence, health and long-term care of persons with disabilities--children, working aging adults, and older persons. DALTCP is also responsible for policy coordination and research to promote the economic and social well-being of the elderly. In particular, DALTCP addresses policies concerning: nursing home and community-based services, informal caregiving, the integration of acute and long-term care, Medicare post-acute services and home care, managed care for people with disabilities, long-term rehabilitation services, children’s disability, and linkages between employment and health policies. These activities are carried out through policy planning, policy and program analysis, regulatory reviews, formulation of legislative proposals, policy research, evaluation and data planning. This report was prepared under contract #HHS-100-03-0028 between HHS’s ASPE/DALTCP and the University of Colorado. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: [email protected].
UNDERSTANDING THE COSTS AND BENEFITS OF HEALTH INFORMATION TECHNOLOGY IN
NURSING HOMES AND HOME HEALTH AGENCIES:Case Study Findings
Andrew Kramer, MD Angela A. Richard, MS, RN
Anne Epstein, PhD Dennis Winn, MA, BSN, RN
Karis May
University of Colorado, Denver Division of Health Care Policy and Research
June 2009
Prepared for Office of Disability, Aging and Long-Term Care Policy
Office of the Assistant Secretary for Planning and Evaluation U.S. Department of Health and Human Services
Contract #HHS-100-03-0028 The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS EXECUTIVE SUMMARY ................................................................................................iv I. INTRODUCTION..................................................................................................... 1
A. Background ..................................................................................................... 1 B. Literature on Costs and Benefits of Health Information
Technology for Nursing Homes and Home Health Agencies .......................... 2 C. Study Objectives ............................................................................................. 6
II. METHODS .............................................................................................................. 7
A. Site Selection .................................................................................................. 7 B. Site Visit Preparation and Data Collection .................................................... 11
III. RESULTS ............................................................................................................. 14
A. Perceived Benefits of Health Information Technology in Nursing Homes........................................................................................................... 14
B. Perceived Costs of Health Information Technology for Nursing Homes........................................................................................................... 21
C. Perceived Benefits of Health Information Technology for Home Health Agencies ............................................................................................ 23
D. Perceived Costs of Health Information Technology for Home Health Agencies ............................................................................................ 31
IV. SUMMARY AND DISCUSSION............................................................................ 34
A. Anytime and Anywhere Access to Health Information................................... 34 B. Greater Efficiency in Meeting Administrative and Federal
Requirements................................................................................................ 35 C. Improved Quality Management ..................................................................... 36 D. Health Information Exchange ........................................................................ 37
V. POLICY IMPLICATIONS ...................................................................................... 38 REFERENCES.............................................................................................................. 39 APPENDICES
APPENDIX A. Pre-Visit Questionnaire...................................................................A-1 Nursing Home Component ................................................................................A-2 Home Health Component ................................................................................A-11
APPENDIX B. Site Visit Data Collection Forms ...................................................A-20 HIT Benefits Table...........................................................................................A-21 HIT Costs/Burden Table ..................................................................................A-22 Costs and Benefits Financial Forms ................................................................A-23
i
LIST OF TABLES TABLE 1: Booz Allen Hamilton Reported Benefits and Costs of Health Information Technology Adoption ................................................................. 4 TABLE 2: Sites Participating in Screening Survey........................................................ 7 TABLE 3: Electronic Clinical Applications of Interest .................................................... 7 TABLE 4: Characteristics of Study Sites....................................................................... 9 TABLE 5: Nursing Homes -- Benefits Associated with Administrative Functions.................................................................................................... 43 TABLE 6: Nursing Homes -- Benefits Associated with Electronic Health Records ...................................................................................................... 45 TABLE 7: Nursing Homes -- Benefits Associated with Medication Administration Records .............................................................................. 49 TABLE 8: Nursing Homes -- Benefits Associated with Quality Management and Reporting ....................................................................... 51 TABLE 9: Nursing Homes -- Benefits Associated with Health Information Exchange ................................................................................................... 54 TABLE 10: Nursing Homes -- Costs Associated with Hardware and Software............. 56 TABLE 11: Nursing Homes -- Costs Associated with Labor ......................................... 59 TABLE 12: Nursing Homes -- Miscellaneous Costs Associated with Health Information Technology .............................................................................. 61 TABLE 13: Home Health Agencies -- Benefits Associated with Administrative Functions ............................................................................ 63 TABLE 14: Home Health Agencies -- Benefits Associated with Electronic Health Records........................................................................................... 68 TABLE 15: Home Health Agencies -- Benefits Associated with Medication
Administration Records/e-Prescribing/Computerized Provider Order Entry................................................................................................. 71 TABLE 16: Home Health Agencies -- Benefits Associated with Quality Management and Reporting ....................................................................... 72
ii

TABLE 17: Home Health Agencies -- Benefits Associated with Health Information Exchange................................................................................. 74 TABLE 18: Home Health Agencies -- Benefits Associated with Telehealth Applications ................................................................................................ 76 TABLE 19: Home Health Agencies -- Costs Associated with Hardware and Software ..................................................................................................... 78 TABLE 20: Home Health Agencies -- Costs Associated with Labor ............................. 81 TABLE 21: Home Health Agencies -- Miscellaneous Costs Associated with Health Information Technology................................................................... 83
iii

EXECUTIVE SUMMARY
One of the major cited barriers to adopting health information technology (HIT) in long-term care is a lack of information on the benefits and costs of HIT in nursing homes and home health agencies (HHAs). While rigorous cost and benefit studies of information technology are limited in health care as a whole, establishing a business case for HIT in long-term care has become a priority in order to stimulate adoption of information technology applications that go beyond supporting administrative functions and federal data requirements. Several completed and ongoing multi-site studies in nursing homes and HHAs have demonstrated selective benefits of HIT in long-term care.
Site Selection The eight sites for this study were selected from a larger group of purposefully
selected providers that had a reputation for advanced HIT systems. Site selection was based on their self-reported level of HIT implementation, using a screening survey that utilized a previously-developed taxonomy of HIT functions. The minimum criteria for inclusion were the use of HIT functionality that included administrative functions and some form of electronic health record (EHR), with one or more of the following types of functions: quality reporting and decision-support tools, medication administration and e-prescribing, and/or health information exchange (HIE) and secure messaging capability. The five nursing homes and four HHAs (at one site two nursing homes were visited) included providers that were and were not affiliated with other long-term care settings, hospitals, physician offices, and retirement settings. They varied in terms of system design (e.g., web-based vs. software that was resident on local hardware), development (private vs. vendor designed), and functionality. Site visits involved structured interviews with administrative, financial, and a full range of clinical staff that assessed the specific benefits and costs associated with each functionality included in the taxonomy.
Reported Benefits of HIT Implementation The single most frequently-cited benefit for both the nursing home and home
health staff was anytime and anywhere access to health information afforded by an EHR. This access to electronic records was sharply contrasted to locating and retrieving the single copy of the resident’s paper chart, which may be in use by another individual, requiring not only the time to find and retrieve the record but also delays in waiting for the record to become available. Numerous examples were given of the advantages of being able to immediately access the chart in a nursing home when receiving a call from the family or the physician. In HHAs, the time savings and care coordination benefits were clearly substantial with various clinicians at multiple locations needing to review or make an entry into the record. A major benefit cited was access to
iv

health records from remote locations, which enabled remote providers such as physicians to review charts, make clinical decisions, authorize orders, and perform other tasks in a timely manner without traveling to the facility/agency.
A second benefit that was articulated at most all the sites was greater efficiency in
meeting administrative and federal requirements in long-term care. With complexities related to determining eligibility for coverage, case mix reimbursement, and the numerous federal, state, and insurance carrier requirements in long-term care, administrative systems that were integrated with clinical information in EHRs yielded substantial benefits to providers. Bills were automatically generated from clinical information entered into the EHR leading to shorter billing cycles. Information used for payment was reported to be more accurate with automated edit checks, and ensured that services that were provided were billed and that billed services were provided. Minimum Data Set and Outcome and Assessment Information Set data were reported to be more accurate. Administrative staff could be more efficient and accurate, as they did not need to enter information that could be automatically pulled from the EHR. Claims denials and resubmissions were reduced. Most providers reported reductions in administrative staffing because of accrued time savings.
A third benefit that was universal, while not fully realized in most sites, was
improved quality management through reports, alerts, and decision-support tools. Electronic reports to routinely track status, alerts that identified specific residents/clients with a more immediate concern, dashboards that required an action before logging out, and automated risk tracking were the basis for numerous examples of early intervention to prevent problems like falls, weight decline, skin breakdown, and hospitalization. The availability of quality information required an informed user to review reports on a systematic and regular basis, which often was difficult for nursing homes and HHAs to achieve. Many sites were discovering how to manage all the information that they were able to generate through now-available quality management systems. For the potential of HIT to be realized with regard to improved quality management, personnel must be allocated and trained in generating and using reports and the HIT systems to support these efforts require continued refinement.
Finally, HIE between providers was a large benefit in the few cases where sites
had the capability. Data exchange with physicians for order review and approval minimized duplicate data entry, and data exchange with hospitals facilitated patient admission and transfer processes. To fully benefit from HIT in long-term care, interoperable systems that allow for HIE are an essential step to achieving care coordination and effective transitions across settings.
While these benefits exist in almost any health care setting, in long-term care they
may be particularly pronounced. Long-term care is provided by interdisciplinary teams of clinicians that all have to share the same record in order to coordinate services. In home health care, both the patients and the care team are geographically dispersed, which is also the case for some members of the nursing home care team that work on a contractual basis. Physicians, an integral member of the team, are almost always
v
remote from a nursing home or HHA and often need to review information to make clinical decisions and write orders. In addition, the patients are often frail and less able to advocate for themselves.
The following are enumerated benefits of HIT implementation reported by the
nursing homes and HHAs included in this case study.
Reported Costs of HIT Implementation On the cost side, sites described large financial outlays for servers and back-up
systems, although the costs varied widely depending on the storage size and processing speed. An advantage of using a web-based system was that data were stored and backed up on the vendor’s server, thus it was not necessary for providers to directly purchase and maintain a large server. Hardware and software costs varied considerably depending on the systems purchased, bundling of applications vs. individually purchased applications, organization size, and individual vendor negotiations. Labor costs included needs for information systems staff that varied greatly, and clinician time for system and workflow re-design, as well as time to learn the system and how to manage and use the health information that was made available through the use of HIT. Maintaining duplicate paper systems in whole or in part was a cost at some sites, while other sites were paperless.
Conclusion This study adds to the growing body of literature through case studies reporting
benefits and costs/burdens in eight sites with advanced HIT systems. While all eight of the case study sites noted that they would “never go back” to paper-based systems for administration and clinical service delivery, no site had conducted a rigorous cost-benefit analysis of their HIT systems. Thus, the case studies necessarily focused on the costs and benefits reported by system users and managers. Respondents cited numerous examples of system benefits and rated their magnitude, as well as identified the types of increased costs and burdens resulting from HIT implementation.
The qualitative findings from the site visits may have implications for recent policy
initiatives. The newly enacted American Recovery and Reinvestment Act (ARRA) included many provisions to accelerate adoption of HIT across health care providers, including nursing homes, HHAs, and other long-term care facilities. One provision of ARRA requires the Department of Health and Human Services to study the extent to which payment incentives should be made available to health care providers, such as nursing homes and HHAs, which are receiving minimal or no payment incentives for purposes of implementing certified EHR technology. The study has direct bearing on this provision in that it demonstrates some of the potential benefits of HIT in these settings that would be realized through incentives for EHR adoption.
vi
vii
Empirical studies that quantify benefits and costs have an important place in expanding our knowledge base so that we can emphasize functions that offer the greatest value. However, compelling qualitative evidence from this study and others on benefits of HIT provides ample rationale for why nursing homes and HHAs should move forward with HIT adoption. Failing to support and accelerate widespread HIT adoption in nursing homes and HHAs while awaiting large-scale empirical studies would be a disservice to the many beneficiaries and staff in long-term care settings who would benefit from improvements in quality of care and more efficient service delivery that were reported by the respondents in this case study.
I. INTRODUCTION
A. Background Calls for greater use of health information technology (HIT) to improve quality and
efficiency in the United States health care system have been issued since the early 1990s. In Crossing the Quality Chasm, the Institute of Medicine (IOM) recommended the development of a national technology infrastructure, with the goal of eliminating most handwritten clinical data by the end of the decade (IOM, 2001). In April 2004, President George W. Bush signed Executive Order 13335 -- Incentives for the Use of Health Information Technology and Establishing the Position of the National Health Information Technology Coordinator. In support of this initiative, the Secretary for the Department of Health and Human Services (HHS) advocated for the nationwide adoption of interoperable HIT as a mechanism to improve health care quality and lower costs by: (a) preventing medical errors; (b) providing clinicians with better clinical decision-making tools; (c) facilitating information transfer across clinicians and health care providers; (d) allowing tracking of health outcomes; and (e) coordinating public health activities. In 2009, the American Recovery and Reinvestment Act (ARRA) provided $2 billion for implementing and/or evaluating HIT as part of a platform to improve health care efficiency and patient safety and approximately $17 billion in Medicare and Medicaid payment incentives to eligible professionals and acute care hospitals for their meaningful use of certified electronic health records (EHRs).
The term HIT refers to an array of computer applications ranging from those used
by administrators (e.g., census management, billing), managers (e.g., staffing and scheduling modules), direct care providers (e.g., EHRs) and in some cases, patients (e.g., personal health records [PHRs]) (Division of Health Care Policy and Research, 2007b). EHRs have the potential to improve quality, patient safety (particularly related to medication errors), and patient satisfaction, and to decrease costs and inefficiencies by making current patient information and clinical decision-making tools accessible to clinicians in an easily-readable format (Booz Allen Hamilton [BAH], 2006; Shekelle, Morton, & Keeler, 2006; Bates & Gawande, 2003; Kaushal, Shojania, & Bates, 2003; Bates, 2002).
Despite the known and hypothesized benefits of HIT, long-term care settings such
as nursing homes and home health agencies (HHAs) have been slow to adopt the technology. Estimates of HIT adoption rates vary widely, in part due to problems such as imprecision in definitions of terms. Estimates of EHR adoption in skilled nursing facilities range from approximately 1% to 42% (Kaushal et al., 2005; National Center for Health Statistics, Centers for Disease Control and Prevention, 2008) and from 5% to 58.5% in HHAs (Fazzi, Ashe, & Doak, 2007; Poon et al., 2006). However, adoption of EHRs with broad functionality is believed to be at the low end of these ranges. Slow HIT/EHR adoption rates have been attributed to several factors, including the costs of acquiring, implementing, and maintaining HIT/EHR; uncertainty about the benefits that may be realized as a result of EHR implementation and to whom these benefits will
1

accrue; delay in adoption of national standards for HIT functionality and interoperability; and a history of instability in the vendor market (Ash & Bates, 2005; BAH, 2006; Poon et al., 2006; Middleton, Hammond, Brennan, & Cooper, 2005; Sidorov, 2006).
Efforts to promote HIT adoption for nursing homes and HHAs have been
spearheaded by private and public sector leaders. These leaders have brought together health information experts, providers, vendors, government representatives, and researchers at Long-Term Care Health Information Technology Summits in 2005, 2007, 2008, and 2009. These summits represent an ongoing collaborative effort by long-term care and aging services stakeholders to assess current progress and advance HIT adoption by long-term care providers. The 2008-2010 LTC HIT Road Map includes recommendations to: (a) strengthen the cross-organizational collaboration of long-term care stakeholders; (b) increase the consumer-focused approach to quality initiatives and HIT applications; (c) advocate for tools to support providers in HIT adoption; (d) prioritize electronic prescribing (e-prescribing) of medications and medication management initiatives to improve patient safety; (e) certify EHR and e-prescribing products; (f) demonstrate interoperability of HIT through emerging standards; and (g) encourage further research investigating relationships between HIT, quality, and outcomes across the full spectrum of aging services and care (American Health Information Management Association, 2008a).
In 2003, the IOM recommended that the United States health care system make a
commitment to the development of a national health information infrastructure by the year 2010 (Institute of Medicine of the National Academies, 2003a). The IOM identified the EHR-System (EHR-S) functions and timeframes over which these functions could be introduced for particular health care settings, including nursing homes (IOM Committee on Data Standards for Patient Safety, 2003b). In late 2006, the Certification Commission for Healthcare Information Technology (CCHIT) was petitioned by long-term care stakeholder groups to include nursing homes in the development of accreditation criteria for EHR products. A draft version of EHR-S functions for long-term care/nursing home (the LTC-NH EHR-S Functional Profile) was developed by a workgroup of long-term care industry stakeholders and became a health level seven (HL7) standard in January 2009. CCHIT will use the HL7 standard to inform the identification of long-term care/nursing home EHR certification criteria (American Health Information Management Association, 2007a, 2007b).
B. Literature on Costs and Benefits of Health Information Technology for Nursing Homes and Home Health Agencies Little research has been published that describes HIT use and assesses benefits
and costs of HIT in long-term care. However, studies of HIT in other settings or studies of cross-cutting HIT functions can be generalized to long-term care settings in some cases. For example, Kaushal and colleagues evaluated costs and benefits of a computerized provider order entry (CPOE) implemented at Brigham and Women’s Hospital (BWH), using actual cost and benefit data to report costs and cumulative
2

savings. They concluded that the CPOE system at BWH resulted in substantial savings over a ten year period. The benefits that resulted in greatest savings were renal dosing guidance, nursing time, specific drug guidance, and adverse drug event prevention (Kaushal et al., 2006).
Shekelle et al. conducted a comprehensive literature review on costs and benefits
of HIT within various health care settings, primarily hospitals and ambulatory care providers. In general, they found that EHR-S implementation requires substantial capital investments and organization change. However, benefits including improvement in service and resource utilization, productivity, care efficiency, documentation quality, clinical decision-making, guideline compliance, and decreased costs of care were cited in the literature (Shekelle et al., 2006). A literature review of research on the impact of HIT on quality, efficiency, and costs of medical care was also conducted by Chaudry et al. Benefits cited were increased adherence to guideline-based care, enhanced surveillance and monitoring, and decreased medication areas. A major efficiency benefit cited was decreased utilization of care. They found empirical data on costs to be limited (Chaudhry et al., 2006).
Using predictive models to estimate costs and benefits of implementation in
hospitals and physician practices, RAND researchers hypothesized that net potential savings in excess of $77 billion could be realized in increased efficiencies in areas such as laboratory tests and through the use of EHRs and CPOE (Girosi, Meili, & Scoville, 2008). Amarasingham and colleagues assessed outcomes for 41 urban Texas hospitals for which physicians reported using automated systems for notes and records, order entry, decision-support, and test results. They found that: (a) an increase in automation of clinical notes was associated with a 15% decrease in odds of death; (b) higher scores in order entry were associated with odds of death for myocardial infarction and coronary artery bypass graft procedures; (c) higher automation scores for decision-support were associated with a 16% decrease in the odds of complications; and (d) higher scores on automation for test results, order entry, and decision-support were associated with lower costs (Amarasingham, Plantinga, Diener-West, Gaskin, & Powe, 2009).
In 2006, BAH was funded by the HHS Office of the Assistant Secretary for
Planning and Evaluation to design an evaluation to establish a business case for HIT in long-term care (BAH, 2006). BAH synthesized extant literature on HIT costs and benefits in other health care settings, particularly acute and ambulatory care settings. With technical expert panel feedback, they identified potential HIT benefits and costs in long-term care (Table 1), and specified potential metrics that could be used in a net benefit analysis.
Information specific to acute and ambulatory care settings, however, may not
always be directly applicable to the nursing home and home health settings due to substantial differences in patient, organizational, and payer characteristics. Fortunately, there is a small but growing body of research with a focus on the costs and benefits of HIT in HHAs and nursing homes. Rumberger and Dansky (2006) focused on a
3

business case for telehealth within HHAs in Pennsylvania. Using a breakeven analysis, the authors determined the estimated costs of telehealth adoption using cost reports and total revenue before and after implementation. The analysis demonstrated that telehealth can have a positive financial impact on HHAs (Rumberger & Dansky, 2006). Another study highlighted the implementation of CPOE in a long-term care setting consisting of a chronic care hospital, a nursing home, and residential units in Toronto, Canada and found no initial clinician time savings with CPOE implementation (Rochon et al., 2005).
TABLE 1: Booz Allen Hamilton Reported Benefits and Costs of Health Information
Technology Adoption Benefits Costs
• Patient Safety/Quality of Care (Number of adverse drug events, avoidable hospitalizations, pressure ulcers, falls, urinary tract infections, reduced length of stay, improved communication, duplicative testing)
• Labor (Time for admission, clinical documentation, medication administration, care plan input, overtime hours, staff retention and recruitment,)
• Revenue (Revenue per patient, patient volume increase, payor mix)
• Malpractice Insurance/Litigation (Number and value of claims, reduction in premiums)
• Improved Regulatory Compliance (State audit improvements, Outcome and Assessment Information Set, Minimum Data Set)
• HIT Needs Assessment (Information technology labor, information technology personnel, time/hours for information technology assessment)
• Hardware/Software (Price of hardware, software, network)
• Training (Personnel, hours, productivity loss)
• Licenses (Cost, annual fees, other)
• Upgrades/Maintenance (Hardware, software)
• Information Technology Support (Labor and hours of labor)
• Interface (Connections, labor hours)
• Deployment (Testing, personnel, labor)
In the same setting, implementation of CPOE-embedded decision-support
functionality that generated alerts from medication orders was found to have very little effects on clinician practice. Prescribers who received alerts were slightly more likely to take an appropriate action than those who did not (Judge et al., 2006). Rantz et al. (2006) evaluated the use of bedside electronic medical records (EMRs) to improve quality of care in skilled nursing facilities and attempted to ascertain the extent to which outcomes are affected by the use HIT. Qualitative study findings showed staff perceptions of improvement in documentation accuracy and efficiency; quantitative findings indicated improvements for only some outcomes (i.e., improvement in the activities of daily living (ADLs) of bed mobility, transferring, eating, and toileting), decline in range of motion, and decline in urinary tract infection (Rantz et al., 2006).
Cherry conducted a one-year evaluation of a web-based EMR for long-term care
facility management. The author assessed costs for overall service, nursing and other staff overtime, communication line items, staff turnover, and resulting quality measures in evaluating whether the implementation of an EMR system improved quality of care
4
and staff satisfaction. Results from the findings were mixed. Benefits noted were decreased hospitalization rates, lower staff turnover rates, and staff-perceived satisfaction. However, findings also indicated no significant decrease in the overall costs of providing services, an increase in costs for staff overtime, and a general lack of physician buy-in (Cherry, Owen, & Bachetti, 2007; Cherry & Owen, 2004; Cortes & Chou, 2004). A second study by Cherry and colleagues did not focus on costs and benefits of HIT but instead attempted to identify the factors that were barriers and facilitators to the adoption of HIT in long-term care. For both users and non-users, the top three barriers identified were costs, culture change, and staff training (although there were differing priorities reported between users and non-users) (Cherry et al., 2007; Cherry, Carter, Owen, & Lockhart, 2008).
Several projects to assess costs and benefits of HIT adoption in nursing homes
are currently underway. The New York State Nursing Home Project: Quality of Care Demonstration Project is focusing on several aspects of nursing home and HIT adoption. In collaboration with Cornell University and in a partnership with United Health Care Workers East SEIU/1199 and nursing homes in New York, researchers are evaluating the effects of the introduction of digital medical records on employment and labor relations. The two year study, which began in 2007, will assess how the implementation of digital recordkeeping influences key workplace outcomes such as recruitment and retention, conflict, and resistance to change (American Health Information Management Association, 2008b; Cornell University Survey Research Institute, 2008). A study to identify the business case for HIT in nursing homes is also being conducted by the University of Pennsylvania, Wharton School as part of this state-funded demonstration project. One component of the project will examine the business case for HIT adoption at 15 New York nursing homes that are currently implementing HIT systems. Other researchers from Cornell University and the Wharton School of the University of Pennsylvania are conducting a study to examine the impacts of technology on three key areas in long-term care: clinical outcomes and quality of care, workforce retention and recruitment, and financial and business operations. The final report is scheduled for release in 2009, however, preliminary data analysis indicated that one long-term care facility, the Sands Point Center, showed improvements in several quality indicators including decreased rates of resident cognitive impairment and moderate to severe pain. Preliminary results also identified cost savings in staff overtime, the reduction of paper forms, and decreased pharmacy costs as well as increased Medicare Part A reimbursement (ehealthsolutions-SigmaCare, 2008; Pacicco, 2008).
The University of Pittsburgh is conducting a study entitled, “Availability and Use of
Health Information Technology in Nursing Homes,” (Degenholtz, 2007). Using a national survey of nursing home administrators and professional staff, researchers are examining the extent of HIT implementation and utilization within nursing homes.
5

Study Objectives The three objectives of this study were to:
1. Further our understanding of how HIT, including point-of-care (e.g., electronic data capture of ADL information, vital signs, progress notes, and charting) and health information exchange (HIE) tools are being used in selected nursing homes and HHAs.
2. Identify the types of costs and benefits associated with these HIT applications,
including the entities to whom these costs and benefits accrue.
3. Develop a data collection and analysis plan to assess the magnitude of the costs and benefits.
To address the first goal, we developed a taxonomy of HIT applications in use by
nursing homes and HHAs based on extant literature, a review of existing HIT systems used in long-term care settings, and five focus groups (Division of Health Care Policy and Research, 2007a). This taxonomy was used to select the site visit locations to be included in this study based on the type of HIT these sites reported using. This case study report summarizes the findings from these site visits.
6

II. METHODS
A. Site Selection Thirteen nursing homes and HHAs that were purposefully selected because of
their reputation for using advanced HIT solutions were chosen to complete a screening tool or survey based on the taxonomy of HIT applications. See Table 2 for the selected nursing home and HHA sites participating in the screening survey.
TABLE 2: Sites Participating in Screening Survey
Nursing Homes Home Health Agencies • Citizens Memorial • Benedictine Health System • Gurwin Jewish Geriatric Center • Erickson Communities • Mission Health Services • Sava Senior Care • AG Rhodes • The Mildred and Shirley L. Garrison
Geriatric Education and Care Center
• Citizens Memorial Home Care • Professional Home Health Care, Inc. • Neighborhood Health Agencies • At Home Care • Encompass Home Health Care • Visiting Nurse Service of New York
The survey results for eight nursing homes and six HHAs (one site had both a
nursing home and an HHA) were reviewed to prioritize sites for case study visits. To be eligible for a site visit, providers had to be using both automated administrative systems (e.g., automated census and billing), and some form of EHR (some sites used the term EMR), including one or more of the electronic clinical applications of particular interest to the project (see Table 3).
TABLE 3: Electronic Clinical Applications of Interest
Nursing Homes Home Health Agencies • Quality reporting functions • Health information exchange functions
(particularly referrals and the ability to receive electronic documents from other providers such as labs, etc.)
• Secure electronic messaging • Decision-support tools • Medication administration record/
medication administration tools • E-prescribing
• Quality reporting functions • Health information exchange functions
(particularly referrals and the ability to receive electronic documents from other providers such as labs, etc.)
• Secure electronic messaging • CPOE (using medical doctor portals for
direct entry or entry performed at HHA in response to verbal/telephone orders)
• Decision-support tools • Telehealth-telemonitoring (including
assessment of functional status using these tools)
Electronic quality management and reporting applications extract data from the
EHR or other clinical applications (e.g., electronic medication administration record [e-MAR]) to generate reports allowing tracking of quality indicators. These may include incident reporting, tracking of adverse outcomes, tracking of infections, calculation of
7

outcomes from Minimum Data Set (MDS) data, risk audits for quality areas of concern for surveyors, dashboard reports of key quality indicators, occupancy rates and trends, etc.
HIE is electronic health data shared across organizations. This data sharing may
be one-way (i.e., view-only) or bidirectional. In nursing homes and HHAs, this may include on-line access for referrals, laboratory data, radiology data, patient consults, patient history from other settings, physician and/or pharmacist access to EHR, pharmacy data, and/or HIE with patients/caregivers.
Secure electronic messaging permits the facility/agency to send messages
containing protected health information between care team members, which may or may not include messaging with physicians.
CPOE allows the ordering physician (or designee) to directly enter medication or
other orders and transmit them to the facility or agency electronically. In many cases, a less direct system of order entry allows facility/agency staff to enter data into the EHR or e-MAR based on verbal or faxed orders.
Decision-support tools are those that provide the care providers with alerts (e.g.,
allergy information, falls risk profiles), reminders (e.g., labs due), or suggestions (e.g., clinical pathways) designed to cue care providers on effective care delivery strategies.
E-MARs include current medication lists and allow for documentation of medication
administration via barcode readers or direct data entry. E-prescribing functionality permits standards-based electronic transmission
between the ordering provider and the nursing home and/or pharmacies. Both the e-MAR and e-prescribe may include decision-support tools for medication dosing, interactions, duplicate therapy, allergies, etc.
Telehealth applications may include telemonitoring of vital signs, tracking systems,
wireless personal emergency response systems, medication reminders, in-home messaging device, virtual visits, patient education materials, health chat lines, communication with patient/family regarding relevant patient information, teleimage transmission, and cellular phones with photo capabilities.
Based on the reviews of the taxonomy screening tools, eight sites were chosen to
include as many nursing homes and HHAs as possible, and to ensure inclusion of as many examples of the applications of interest as possible, as well as variation in provider affiliations (e.g., freestanding vs. hospital-based) and system development (e.g., privately developed vs. vendor designed). A recruitment letter outlining the nature of the site visits, including a request that the selected site share quantitative and qualitative information on costs and benefits of HIT applications, was sent via e-mail to the selected providers. Seven of the chosen providers agreed to host site visits. One provider declined and was replaced by another provider meeting the criteria discussed
8

above. Table 4 provides a summary of characteristics of the selected providers and additional characteristics are provided in the narrative summary following the table.
TABLE 4: Characteristics of Study Sites
Nursing Homes Facility Visited Location Area
Served Nursing Home Beds
Hospital- Based
A.G. Rhodes Home at Wesley Woods Atlanta, GA Urban 150 Yes
Renaissance Gardens at Riderwood Campus (Erickson Retirement Community)
Silver Spring, MD Urban 132 No
Mission Health Services Alpine Valley Care Center
Pleasant Grove, UT Urban/Rural 52 No
Hillside Rehabilitation Salt Lake City, UT Urban/Rural 121 No
Citizens Memorial Healthcare Facility (CMHCF) Bolivar, MO Rural/Urban 111 Yes
Home Health Agencies Facility Visited Location Area
Served Home Health
Annual Admissions
Home Health Visits
Annually
Hospital- Based
At Home Care, Inc. Oneonta, NY Rural 2,400 31,000 No Professional Home Health Care, Inc. Longmont, CO Urban 629 212,000 No
Citizens Memorial Healthcare (CMH) Bolivar, MO Rural/Urban 957 15,000 Yes
VNS of New York New York, NY Urban 131,600 2,248,000 No
Nursing Homes
A.G. Rhodes Homes, Inc., serves the metropolitan Atlanta, Georgia area and
operates three non-profit nursing home facilities. Each Rhodes Home offers long-term and short-term rehabilitation in sub-acute units, serving Medicaid, Medicare, private pay, and Veterans Affairs (VA) residents. The three homes combined have a total of over 400 beds. The original A.G. Rhodes Home was one of the first three nursing home organizations to be licensed in the State of Georgia. The visited site, A.G. Rhodes Home at Wesley Woods, is affiliated with Emory Hospital and Emory University. The facility used a web-based system that incorporated an EHR and e-MAR, along with decision-support tools. Quality management reporting functionality allowed charge nurses and managers to track medications and clinical activities in real-time.
Erickson Retirement Communities, a continuous care retirement community
based in Baltimore County, Maryland, began operations in 1983. Erickson is a privately held, standalone company developing and managing retirement communities on 23 campuses located in Colorado, Illinois, Kansas, Maryland, Massachusetts, Michigan, Missouri, New Jersey, North Carolina, Ohio, Pennsylvania, Texas, and Virginia. In the Baltimore area, in addition to corporate headquarters, other services include eight long-term nursing care facilities and short-term rehabilitation, Alzheimer’s care, respite care, and 13 HHAs. Comprehensive services at Erickson include a Medical Center staffed by board-certified primary care physicians who specialize in geriatrics and practice only at Erickson campuses. At the time of the site visit, Erickson used two different EHR applications -- one for physicians and another for the nursing home -- which were not interoperable. E-MARs were being pilot-tested in two homes, but were not implemented
9

system-wide. Both EHR-S incorporate decision-support tools and quality management reporting functions.
Mission Health Services, headquartered in Huntsville, Utah, is a community-
based non-profit organization. Facilities include four skilled nursing homes and one center for individuals with developmental disabilities. The site visit included both Alpine Valley Care Center (45 beds) in Pleasant Grove and Hillside Rehabilitation Center (122 beds) in Salt Lake City. At the time of the site visit, Mission Health had fully implemented secure electronic messaging, MARs, EHRs, and CPOE. They were planning to develop functionality to allow HIE for laboratory and radiology results.
Citizens Memorial Healthcare Facility (CMHCF), located in Bolivar, Missouri, is
a non-profit organization and is one of five nursing home facilities operated by Citizens Memorial Healthcare (CMH). CMHCF is a Medicare and Medicaid certified skilled nursing facility with 111 beds. The parent organization, CMH, consists of Citizens Memorial Hospital, a 74-bed acute care hospital, plus 29 primary care and specialty physician clinics, five long-term care facilities, one residential care facility, five independent living communities, home health, hospice, homemaker plus, heath transit services, home medical equipment, and rehabilitation services. In 2003, CMH implemented a universal EHR-S, which can be accessed throughout the Citizens system, including the hospital, nursing homes, and physician offices (for hospital-employed physicians). Thus, the nursing home had access to clinical data from the hospital and affiliated physician offices, including radiology, laboratory, medication, and clinical notes information. The EHR-S included CPOE, an e-MAR with barcode functionality, decision-support tools, and quality management reports.
Home Health Agencies
At Home Care, Inc., is a freestanding, non-profit Medicare-certified HHA, based in
Oneonta, New York. At Home Care, Inc. (which operates one branch office in Herkimer County) is the only HHA serving three rural counties and provides approximately 31,000 visits annually. At Home Care is associated with the community-based AO Fox Memorial Hospital in Oneonta and the regional health care delivery system, Bassett Healthcare in Cooperstown, New York. Affiliation with both groups has increased access to information technology, clinical, and management support. At Home Care first implemented an EHR in 1997, and then purchased a new system from another vendor in 2001, which has secure electronic messaging, decision-support, some quality reporting functionality, and MARs. Orders were entered into the EHR-S manually by the home care staff taking verbal or faxed orders. They contracted with a separate vendor for additional quality reports derived from Outcome and Assessment Information Set (OASIS) data. At Home Care initiated a telehealth program under a two-year New York State Department of Health telemedicine demonstration project. Because they were able to demonstrate a positive return on investment for telehealth, they recently expanded that program.
10
Professional Home Health Care, Inc. (PHHC), consists of two small, for-profit, freestanding HHAs, one with offices serving the urban metropolitan areas of Denver, Colorado Springs, and Pueblo, and the other serving the urban metropolitan areas of Boulder and Longmont, Colorado. PHHC serves primarily a Medicaid and private pay payer population, providing approximately 212,000 annual visits. They do not have a hospital affiliation. PHHC was using an HIT system that incorporated EHR, decision-support, MARs, quality reporting, and limited CPOE. They had recently implemented a telephony system for home health aide scheduling and documentation.
Citizens Memorial Home Health (CMHH), Bolivar, Missouri, is operating under
the non-profit Citizens Memorial organization. As noted earlier, CMH consists of Citizens Memorial Hospital, a 74-bed acute care hospital, plus 29 primary care and specialty physician clinics, five long-term care facilities, one residential care facility, five independent living communities, hospice, homemaker plus, heath transit services, home medical equipment, rehabilitation services, and home health. CMHH provides approximately 15,000 annual visits. CMHH had access to hospital, physician office, lab and other data contained within the system’s universal EHR records. CMHH was using an EHR-S produced by the same vendor who provided the hospital’s and nursing home’s EHR-S, but information exchange between the two systems was limited. The CMHH EHR-S included the ability to enter medical doctor (MD) orders into the record and incorporated decision-support tools and quality reporting functions. A separately-purchased system provided additional quality reporting functionality. CMHH had a telehealth program that allowed monitoring of physiologic data and medication compliance. The vendor was building additional interfaces for more robust system integration between the CMH EHR and the home health EHR.
Visiting Nurse Service of New York (VNSNY) is the largest non-profit HHA in the
United States, established in 1893. In 2007, the VNSNY provided services to more than 131,600 patients and made 2,248,000 professional visits. VNSNY uses a self-developed EHR-S. Data were accessed and entered using pen-based tablet computers, then stored on a mainframe and made available for quality reporting via a data warehouse. VNSNY had recently implemented a new electronic visit scheduling system and maintained a telehealth program. They were able to accept electronic referrals from approximately 22 of their 150 referring hospitals. VNSNY is affiliated with numerous hospitals and ambulatory care clinics through participation in several regional health information organizations (RHIOs). As part of the RHIO activities, VNSNY was developing and testing HIE capabilities with participating hospitals and physician practices, as well as patient access to a limited set of information via a patient portal.
B. Site Visit Preparation and Data Collection A pre-visit questionnaire was developed to obtain initial information on specific
costs and benefits of HIT functions adopted by provider sites (Appendix A). Pre-visit questionnaires were customized for each provider, highlighting the applications that they had identified during the completion of the taxonomy. Instructions accompanying
11

the pre-visit questionnaire noted that if the provider had completed a return on investment or other quantitative cost-benefit analysis, summary information could be provided in lieu of completing survey sections. None of the selected providers were able to provide a detailed quantitative cost-benefit analysis specific to the setting (i.e., unbundled from a corporate cost-benefit analysis). However, the information provided as part of the pre-visit questionnaire was useful in identifying areas for discussion during the site visit interviews.
In addition to the pre-visit questionnaire, the providers were asked to schedule a
series of interviews during the site visits with individuals who could provide either quantitative or qualitative data on costs and benefits of HIT applications. We requested that the provider attempt to schedule interviews with the following types of staff:
• Administrator, or someone who could speak to costs-benefits of HIT from the overall agency/facility perspective;
• Financial officer, or someone who could provide either specific cost-benefit information or qualitative impressions;
• Information systems administrator (or designee); • Nursing manager; • Quality Improvement Manager; • Clinical staff using the HIT applications (e.g., registered nurse [RN], therapist,
certified nurse aides [CNAs], etc.); • Individuals external to the agency who use the HIE applications (e.g.,
pharmacist, physician), and who would be willing to provide qualitative information on costs-benefits from their perspective.
The project team developed data collection forms intended to guide interviews
during the site visit (Appendix B). These data collection forms were developed for each application for which the cost and benefit information would be gathered, including: administrative systems, EHR, e-MAR/e-prescribe, decision-support, quality monitoring systems, secure electronic messaging, HIE systems, and telehealth systems. The form for collecting data on benefits included sections for description of the benefit, identification of to whom the benefit accrued, assessment of the benefit magnitude, and potential methods for quantifying the benefit. The same sections were incorporated on the cost form. In addition, more detailed information on costs were collected using a data collection form with sections for specific costs that could be identified for hardware, software, labor, and other miscellaneous costs during implementation and for system maintenance.
After the first visit, the forms were modified to allow for the collection of qualitative
cost-benefit data that applied either to specific applications or functions, or to groups of applications (the modified form is included in Appendix B). During the on-site portion of the case studies, 2-3 study team members traveled to the sites. Project team members consisted of individuals with expertise in nursing home care, home health care, and health care economics. These staff met individually or in groups with the scheduled interviewees. During the one to two-hour interviews, team members determined which
12

of the HIT functions the interviewees used and probed on perceived benefits and costs of those functions. Users were asked to describe the benefits and costs they experienced or perceived. Information on the extent of use of the applications also was obtained during the interviews. In the interests of confidentiality, sites are coded as A-D rather than using site names in the descriptions and tables.
13

III. RESULTS Rarely could respondents at the site visits provide rigorous data on benefits and
costs of HIT; however, they were able to articulate evidence of both benefits and costs/burdens. When asked, they were sometimes able to quantify these benefits and the cost/burdens, and suggest ways that these could be rigorously measured. The results are presented separately for the two provider types and benefits are presented separately from costs/burdens, resulting in four sections of results: nursing home benefits, nursing home costs/burdens, HHA benefits, and HHA costs/burdens. A narrative summary of findings by function is provided in addition to more detailed tables that tabulate reported benefits and costs/burdens across the sites.
A. Perceived Benefits of Health Information Technology in Nursing Homes Benefits of HIT implementation in nursing homes were categorized and collected
based on the following functions: Administrative, EHRs, MARs (including e-prescribing and CPOE), quality management and reporting, and HIE capabilities. Tables 5-9 summarize, by function and facility, the perceived benefit findings.
1. Administrative Functions (Table 5)
Functionality: Administrative functions are those automated non-clinical functions used by administrative staff to manage facility operations. These include agency census, financial management and billing, payroll, human resources management, employee staffing/scheduling, and automated referral systems.
Applications: The four facilities visited used administrative applications to
manage census and for billing/financial management. Sites C and D noted using separate software systems for administrative functions from their clinical systems, although Site D reported the ability to interface with clinical systems. Site D was part of a larger system and financial management was addressed centrally. Sites A and B used a single system with both administrative and clinical functions, although Site A had a separate system for payroll. All four sites included information technology applications for producing MDS.
Benefits: One benefit cited by all four nursing homes was the more accurate
capture of MDS functional data used for resource utilization groups (RUGs) case mix classification, which resulted in both increased revenues and enhanced regulatory compliance. Site C noted that their case mix-based Medicaid reimbursement had increased by 30%. Sites B and D discussed fewer problems with claims denials due to the improved accuracy of charge capture and billing. Efficiencies noted by individual providers included improved cash flow, reduction in the time needed to close monthly billing, the ability to bill centrally for several facilities, and the enhanced ability to bill to
14

multiple payer sources (i.e., by virtue of electronically managing payer-specific forms and requirements).
Oversight benefits realized by administrative HIT systems, especially when
integrated with clinical systems, were efficiencies in the utilization review process (cited by Sites B and D), reduced office supply costs, allowed faster access and more complete information to respond to payer inquiries on a timely basis, increased the ability to determine patient eligibility for Medicare Part A and Medicare health maintenance organizations (HMOs) (due to more accurate information) and the ability to review pre-authorization requirements centrally. Sites A and B realized decreased staffing needs for billing and/or insurance verification, and Site D perceived that administrative efficiencies allowed existing staff to handle increases in admissions, preventing the need for additional personnel. Site B highlighted the improved ability to manage staffing resources to address patient needs (i.e., appropriate assignment of nurses qualified to deliver intravenous therapy and better management of therapist workload). Site B also noted that the electronic availability of source information needed to complete the MDS resulted in increased efficiencies for the MDS coordinator, allowing her to work off-site.
Benefits noted for census management included increased efficiencies in
determining patient placement and more timely care transitions from hospital to nursing home bed. Site D observed that these benefits were particularly important in a multi-facility organization, where patients can be directed to facilities with open beds.
2. Electronic Health Records (Table 6)
Functionality: The EHR as defined here consists of electronic demographic information, clinical assessments, care plan and updated physician orders, clinical progress notes, and other summary reports including discharge summaries.
Applications: All four nursing homes used an EHR that incorporated
demographic information, clinical assessments (beyond MDS), care plans, clinical notes, summary reports, and physician orders. All sites reported that authorized users were able to access EHR data from remote locations, including home and off-site offices. Site D was the only site that considered themselves to be paperless.
Benefits: All facilities commented favorably on the benefits of EHRs. The
benefits cited most often accrued from anytime and anywhere access to patient information simultaneously by multiple care team members. Benefits of greater access to the clinical record enhanced quality of care team coordination and communication, aided in decision-making, reduced response time to negative events (e.g., out-of-range lab data), reduced duplicative diagnostic labs and X-rays, and potentially reduced emergency room visits and rehospitalizations. This benefit was noted to be particularly useful to physicians or others who could access the record from off-site, which reduced telephone time and in some cases, reduced the need to physically travel to the nursing home to assess the patient. The easy access to the record enhanced the ability of
15
nursing home managers to respond to questions from the insurer or family member. EHRs enabled the use of clinical decision-support tools (e.g., flags for potential medication interactions) that would not have been feasible without electronic clinical records. Integration of EHR and administration systems increased billing staff efficiency and improved accuracy of invoicing. Sites A and D noted that access to EHR data allowed management staff to monitor staff training needs more efficiently and effectively by identification of problematic processes and documentation.
Sites A and D pointed out that the EHR provided more secure documentation
systems, and Sites B, C, and D all noted that more information was maintained in an EHR than a paper chart. These same three facilities discussed the direct role of the EHR in improving the quality of documentation by noting that some charting fields had to be completed before the clinician could continue charting. Improved staff productivity was noted, but none of the facilities reported changes in staffing patterns, only that they were able to spend more time with residents. More prompt and complete documentation was helpful when responding to telephone calls from families or physicians.
The EHR-S for Sites B and C contained workflow management functions for
CNAs. These systems allowed CNAs to better self-manage their time, which resulted in enhanced job satisfaction. The CNAs using these applications reported an increased sense of autonomy and acknowledgement of the value they bring to the care team. In addition, the charge nurses were more efficient in managing the CNA assignments and workflow, and were able to identify CNAs falling behind on assignments or needing assistance. Thus, reports generated from this functionality played a large role in the facilities quality management program.
Other perceived benefits of EHRs included reduction in the administrative
overhead needed to manage medical records departments, with some facilities reporting that they were able to reduce medical records staff. The time needed for managers, RNs, or others to request old charts and wait for medical records clerks to find the records was mostly eliminated in three facilities. Reductions in paper and copying costs were cited by Site B, and Sites C and D noted reduction in storage costs (either reduction in the need for off-site storage facilities or the ability to re-use existing space once needed for storage).
Site A used the EHR in marketing efforts and Site C commented that the system
enhanced their reputation in the community, bringing in additional referrals. Improvement in regulatory compliance was cited by Sites A, B, and C, whereas Site D found greater challenges with regulatory compliance after implementing the EHR. They attributed this to the possibility that more accurate documentation may have led surveyors to identify more problems.
16
3. Medication Administration Records/e-Prescribing/Computerized Provider Order Entry (Table 7)
Functionality: Automated functions related to medications include the use of e-
MARs, and electronic prescribing functions/CPOE. E-prescribe/CPOE functions typically include decision-support tools for medication dosing, interactions, duplicate therapy, allergies, etc.
Applications: All facilities reported use of e-MARs, although Site A had only
begun pilot testing with two facilities. Site D had autofax capability such that medication orders were automatically sent to the pharmacy. The pharmacy then used specially-provided software to barcode labels, which were scanned at point-of-care during medication administration. In Site A, physicians could directly enter orders (CPOE) into the system on-site or at remote locations. Sites B and C required data entry (i.e., no bar code functions) for medication management. Site C had the capacity for CPOE but had not fully implemented the system at the time of the site visit. Site B did not have CPOE capacity, and verbal or faxed orders were entered into the EHR, which then populated the e-MAR. As with Site C, they entered verbal or faxed medication orders into the e-MAR on-site. None of the facilities were using e-prescribing functions that permitted HIE across systems.
Benefits: Sites B, C, and D had fully implemented e-MARs. All three sites noted
that benefits of these applications included improved workflow resulting in time savings for medication administration, although one clinician from Site C disagreed, indicating the MAR was hard to navigate and would prefer to return to paper. Site C reported a decline in the time needed for medication administration from nine hours per 12-hour shift to six hours per 12-hour shift. Sites B, C, and D noted that staff time for the monthly pharmacy medication reconciliation process was significantly reduced, reporting that time associated with the reconciliation process dropped from several days and nights at the close of a month to less than an hour. Site B reported that the ability to update the e-MAR immediately with changed medication orders saved money and enhanced quality by reducing the potential for discontinued medications to be ordered and administered. Sites B, C, and D noted substantial improvements in medication error rates from both the new system of administration and the alerts within the e-MAR system. Integrated decision-support systems (e.g., prompts to take pulse prior to administering digoxin, lab results management) resulted in improvements in staff compliance with medication monitoring, and helped reduce missed labs and other orders. The reduction in error rates manifested as a reduction in survey deficiencies for medication administration (med pass) performance at Site C. Printable medication teaching guides were found to be useful by Site B.
Sites C and D cited benefits of CPOE applications including reductions in
medication errors (fewer transcription errors), fewer calls needed to follow up with questions or to confirm orders (saving time and improving both accuracy and physician satisfaction), and integrated decision-support systems to identify potential adverse events. However, one potential problem with medication decision-support systems, as
17

identified by Site D, was the large number of potential errors flagged, which required time-consuming reviews by physicians. This facility commented that some physician staff were dissatisfied with the long lists of flags and found that most flags did not result in medication changes. Site C suggested that the electronic systems emphasized the large numbers of prescribed medications for many residents, which potentially had the effect of encouraging physicians to reduce medications where possible. Site D’s system required physicians to review the medication list monthly, which helped identify discontinued and unnecessary medications, thereby improving quality of care and regulatory compliance. They noted however, that many physicians renewed the list of medications with little review. For urgent issues needing medication changes, at all sites it was common for the physician to fax an order to the facility where facility staff subsequently entered changes into the system.
4. Quality Management and Reporting (Table 8)
Functionality: Quality management and reporting includes tools within the clinical record used by providers at the patient level, as well as reports used by managers to assess quality at an organizational-level. Organizational-level quality reports may include summary data pulled from charts such as numbers or percentages of patients experiencing adverse events, negative clinical outcomes (e.g., falls, pressure ulcers), numbers or percentages of patients receiving immunizations, meeting clinical goals, or experiencing missed medications. These electronic reports may be defined within a system (e.g., dashboard reports) or may be created by the facility or a contractor. Alert and incident reports consist of identification of specific residents or incidents that require follow up. These alerts may be in the form of drill-down functionalities within quality reports or may be delivered as e-mails or on a dashboard. Alerts often require resolution of some type before the user signs out. Electronic decision-support tools used at point-of-care or during a care episode can include clinical pathways, flags or reminders (e.g., labs due), risk assessment tools (e.g., falls risk), flags for potential medication errors, and trend reports that highlight out-of-range values.
Applications: Electronic quality management reports used by Site D included
adverse events, infection rates, medication errors, risk audits, and occupancy rates and trends. These reports were generated from their system for administration and clinical managers. Site C created various quality management reports, including a special report designed for a state survey visit. Site B used quality monitoring dashboard reports of self-defined indicators. Systems at Sites B and C incorporated detailed reports on CNA task completion and results, allowing managers the ability to run real-time reports on task status, and providing alerts to managers when medications or treatments were late or missed. Site A’s system produced monthly nursing summaries on key resident issues (e.g., falls, psychotropic medication management problems). All sites reported the use of decision-support tools for medications and other clinical functions. The EHR-S for Sites B, C, and D incorporated prompts for labs and immunizations, risk assessment tools, and trending for vital signs and lab results. The EHR-S at Site A provided numerous clinical support functions including timely reporting and analysis of reportable incidents (e.g., falls) and early identification of residents at
18

risk for different clinical conditions (e.g., pressure ulcers) so that necessary care planning could take place. In a pilot of an interface between the nursing home and physician’s electronic systems, the nursing summary proved valuable by providing the physician with current information on key resident issues prior to the monthly on-site visit.
Benefits: Quality tracking reports were perceived to save significant time over
reviews of books of weights, food consumption, and/or chart reviews, which allowed managers to monitor specific clinical indicators on a daily basis. Real-time reports with drill-down functionality allowed managers to quickly identify and prioritize individual patient needs, particularly if trending was offered for decision-support. Other benefits noted were improved accuracy of the reports compared to prior paper systems, which enhanced communication across shifts. In addition to reviewing quality, the reports were used to assist with staffing decisions (e.g., appropriate staff assignments). Sites A, C, and D found these reports helpful in facilitating central quality review and monitoring in multi-facility sites. All facilities reported incident reporting capabilities, allowing constant monitoring and immediate follow up for problems. Tracking reports enhanced timely problem identification with the opportunity to implement corrective actions.
Sites A and B commented that reports using EMR data that identified high-risk
patients (e.g., falls risk) allowed timely care planning to specifically address these issues. One facility using electronic reports noted a decline in adverse events such as falls, fractures, and unresolved pain, and attributed the decline to better identification of at-risk patients. Site C noted that electronic quality reports on immunizations or use of PRN medications facilitated managers’ ability to proactively monitor and respond to patient needs. Sites B and C identified other particularly beneficial electronic reports that improved manager efficiency, including documentation of CNA activities, information for CNA workflow management (e.g., reports of delinquent tasks facilitated identification of the need to modify CNA assignments), and the use of therapist efficiency reports to manage therapy staffing (i.e., ensure appropriate staffing levels).
Additional benefits of the quality management and reporting functions included
enhanced regulatory compliance by virtue of more efficient and more accurate monitoring of problem areas. Site C noted that surveys were much less time-consuming on facility staff because many of the reports that surveyors requested could quickly be generated upon request. Sites A and B reported decreases in liability insurance premiums because they were experiencing fewer adverse patient events and fewer corresponding insurance claims. While both sites speculated that EHR adoption may have played a role in lowering the rate of adverse events, neither could directly attribute these outcomes solely to the HIT system.
One of the difficulties encountered at most of the sites was developing systematic
approaches to reviewing the reports and addressing the potential quality concerns that were identified. Availability of real-time electronic reporting of risks, resident care issues, and adverse events, created a responsibility for someone to review these
19
reports in a timely manner rather than at a monthly or quarterly review of the plan of care. A couple of the visited sites were only beginning to use the information generated by these reports. One feature that helped in these areas was the use of a dashboard to highlight pressing care issues and which required an action to remove or even sign out.
5. Health Information Exchange (Table 9)
Functionality: HIE functions are those that allow the electronic transfer of patient information among and across organizations (e.g., hospital, physician) and with patients/families.
Applications: Site D, part of a large health care system, used a universal EHR
that incorporated hospital and physician office notes (for physicians who were hospital employees). Thus, the EHR was interoperable with the system used in the other parts of their health care system. However, the EHR used in this health care system did not incorporate the use of HIT standards and was not interoperable with providers outside their system. Sites B and C were not transmitting or sharing data with other providers, although Site C had the electronic HIE capacity built into the EHR-S. Site A was pilot testing an interface between their EHR and physician EHR-S.
All sites allowed authorized users, including other health care professionals who
were not nursing home employees but provided services to nursing home residents, to view clinical information from remote locations, and they also could enter information or orders through most access points. However, the physician offices frequently utilized a different EHR that was not interoperable with the nursing home system. All four providers had secure electronic messaging systems. Sites C and D used messaging functionality built into their clinical software system, while Sites A and B used other messaging systems (e.g., Microsoft Outlook).
Benefits: Site C noted perceived benefits of electronically sharing clinical
information with off-site providers included shorter response times to changes in the resident’s conditions; fewer duplicated diagnostic labs and X-rays; and potential reductions in emergency room visits and rehospitalizations, because physicians had more available clinical information from remote sites. Sites B and D reported less time spent on the telephone gathering information necessary to make decisions (for physicians, nurse practitioners, physician assistants, and on-call clinical managers), although Site B pointed out that some physicians, nurse practitioners, and physician assistants were reluctant to use the system. Sites C and D cited benefits of improved quality of transitions to and from the hospital due to standard order lists, discharge/transfer summaries, and other clinical data that was available on the system. Site A reported that access to hospital data increased their ability to initiate necessary services and treatments (e.g., meds, therapies) in a timely manner. Site A used a secure electronic messaging system with physicians to provide information and request review and approval of the care plan and other orders. They found this system improved coordination of care and increased physician efficiency (e.g., fewer phone calls between the physician and the facility provider). Access to hospital clinical data
20

improved Site D’s ability to accurately capture functional status from the look-back period, thus maximizing RUG data accuracy, which resulted in enhanced revenue capture.
Site A reported the use of a PHR. This site also provided flash drives loaded with
a small amount of clinical data from their EMR for residents to take to clinic appointments. Some providers were able to enter data and transfer it back to the flash drive, which went back to the nursing home for entry into the clinical record. Personal health data also were available to the family for review and allowed them to verify medications, allergies, etc., via a resident health portal.
Sites C and D reported HIE capabilities with radiologists. Radiographs, however,
were not integrated into the EHR in Site C. They perceived benefits of faster response times and some efficiencies due to decreased transportation costs, although the X-ray technician still had to come to the nursing home or the resident had to go to the radiologist to take the films.
B. Perceived Costs of Health Information Technology for Nursing Homes Costs of HIT implementation in nursing homes were categorized as hardware and
software purchases, labor costs, and other. A variety of actual costs for hardware and software purchases were available in some of the facilities, others simply noted areas that required financial outlays. Table 10, Table 11 and Table 12 summarize qualitative findings on costs.
1. Hardware and Software Purchases (Table 10)
Costs of data storage included purchase, maintenance, and periodic replacement
of servers and back-up systems. These costs varied depending on the type of EHR-S, storage size, and speed needed. For example, Site B reported using a web-based system where data were stored and backed up on the vendor’s server, thus it was not necessary for them to directly purchase and maintain a large server. Other hardware costs included data entry hardware, including desktop and laptop computers, personal digital assistants (PDAs), and rolling medication carts to support computers. Other cited hardware costs included printers, scanners, and space for housing servers and information systems staff. The combined costs of all hardware and data storage were typically cited as large.
Network and connectivity costs were cited as major expenditures. These included
costs for installing and maintaining local area networks (LAN), wide area/metro networks, wireless networks/bridges, internet connectivity, and remote access.
Software costs varied depending on the combination of applications purchased
and whether the applications were bundled (e.g., decision-support tools embedded
21

within EMRs) or purchased separately. It was noted that most software purchases include a fee for a certain number of licenses and a percentage of that fee is paid annually for ongoing maintenance. Site C reported “sunk” costs for an EMR system they had purchased but never implemented because they decided to develop a proprietary system to better meet their needs.
2. Labor Costs (Table 11)
Reported labor costs included the need to hire information systems personnel;
however the number of information systems staff needed was facility-specific. Sites A, C, and D reported the need to allocate staff time for existing staff given responsibility for analyzing and re-designing workflow processes, to facilitate effective use of the HIT systems, and for system and report design. Identified clinical labor costs included staff turnover related to the implementation of new systems (although this was noted to be minimal), initial and ongoing training costs, and an increase in the time spent on clinical documentation, due to the more complete and descriptive documentation required within the EMR.
Labor costs for planning new system implementation were reported to include
travel and site visits for investigating and negotiating new system purchases. While these costs were not tracked in any detail, planning and oversight of the transition reportedly absorbed substantial time from multiple administrators and managers. Training costs were described in terms of staff hours for in-house staff designated as “super-users” or trainers, followed by hours spent training all staff. Short-term loss of productivity was noted by Sites C and D. Site C specified that some of these costs were paid as overtime to existing staff members taking on additional new responsibilities.
3. Miscellaneous Other Costs (Table 12)
While several facilities commented that improved regulatory compliance was a
benefit of their HIT system, Site D noted surveyor reluctance to review electronic versions of records. This site had to print out paper versions of selected records for surveyor review, which was both costly and frustrating. Site D also commented that the EMR allowed them to better identify and track problems (e.g., falls), but that this allowed surveyors to identify deficiency areas that previously may have been missed, resulting in increased deficiency citations. Site C noted that they had created special reports to respond to surveyor data requests. While costs were involved with report specifications, they felt that benefits in terms of improved response times to surveyors were worthwhile.
The need to re-design workflow to utilize the systems led to minor inefficiencies in
Site B, where one person had to complete data entry before anyone else could access the chart. Sites A and B reported that the use of multiple systems that are not compatible resulted in the need for duplicate data entry. For example, Site A noted that charting completed in the EHR did not populate their MDS.
22

Other miscellaneous costs reported were inefficiencies during system down-times.
Because these down-times (typically less than an hour) interrupted workflow, they occasionally affected the ability of staff to complete work in a timely manner. Slower data access times that occurred with larger databases can have the same effect. Site C noted costs/inefficiencies created by physician unwillingness to use the CPOE functions directly. This resulted in creation of a paper version of the order that was subsequently data entered by a staff member. The increase in the availability of data increased the time spent by managers in monitoring and following up on report findings. For example, Site A commented that medication review flags for potential medication problems required additional physician time to review. Site C reported costs of maintaining both paper and electronic copies of the records, as there was concern that records may be lost.
C. Perceived Benefits of Health Information Technology for Home Health Agencies
1. Administrative Functions (Table 13) Functionality: Administrative functions are those automated non-clinical functions
used by administrative staff to manage agency operations. These include agency census, financial management and billing, payroll, employee staffing/scheduling, and automated referral systems.
Applications: All HHAs used software for financial management, including
general ledger (A/R and A/P) and automated billing systems. Site A was part of a larger health delivery system and their financial management systems were handled centrally. All four HHAs used automated staffing and scheduling systems to facilitate scheduling across multiple field clinicians. Site C reported using administrative systems for personnel management, allowing tracking of personnel licenses and satisfaction of training requirements. Site D used an e-learning system for staff education, which provided them with the ability to monitor individual staff progress in completing agency education requirements. Sites C and D used telephony systems for home health aides. Aides used telephony to document arrival and departure times, as well as to electronically document the tasks accomplished during the patient visit. These systems interfaced with billing systems so that bills could be automatically generated. Site A received patient referral information electronically from their affiliated hospital by virtue of having access to the hospital medical record. Site D used three unique automated referral systems (e-Referral, e-Cin, and Provider Link) with 22 referring hospitals and the perceived benefits of these systems are noted in the section on benefits below.
Benefits: Sites B, C, and D discussed benefits of automated systems for billing
and support for ICD-9-CM coding. These systems assisted with optimizing cash flow due to shorter billing cycles and more accurate coding. Declines in claims denials also were cited by Sites B, C, and D. Site A cited additional benefits of administrative
23

functions, including the ability to quickly review patient eligibility for Medicare Part A and requirements for pre-authorization, which reduced provision of non-reimbursable services and minimized time lags in starting care. Site B noted that benefits included the enhanced ability to monitor admission and home health resource group (HHRG) patterns and the elimination of month-end financial document “closings.” Many of Site B’s patients changed insurer during the episode of care and they perceived that their systems allowed them to more efficiently manage these situations. They used administrative systems to more effectively justify referrals for special services (e.g., wound care nursing). They also minimized the occurrence of providing more home health visits than were approved by the insurer, for which payment can be denied, by providing the clinician access to current insurance approval data.
Sites A and B found that the drill-down capabilities of their systems (i.e., the ability
to view specific types of charges) were useful in helping them to identify wasteful supply purchases. Site A noted that the transition to automated systems allowed a single administrator to oversee more than one department, thus eliminating 2.5 administrative full-time employees (FTEs) by attrition. The instant access to current revenue and expenditure patterns allowed administrators to track and correct potential problems before they became widespread. Also, this access to information about patient case mix and profit gave administrators information to guide marketing efforts (e.g., profitable diagnoses).
Sites A, B, and D discussed staffing and scheduling benefits of administrative
systems, both for administrative and clinical staff. Site B noted that the HIT system facilitated their ability to manage centrally a large geographic area. These administrative efficiencies in combination with clinical efficiencies described in Section 2 below enabled Site B to close two branch offices and recognize the resultant elimination of staff and facility costs. The increased system efficiencies for payroll and billing departments resulted in elimination of administrative staff in Sites A, B, and D. Sites B and D noted that they were better able to predict staffing needs and mileage, allowing them to more accurately budget for increases in patient census.
Staffing/scheduling modules provided data to ensure appropriate clinical staff were
assigned to each patient based on care needs (e.g., prompts to ensure that an IV therapy-certified nurse was assigned to patients with these needs), or to address patient requests and preferences. Site C noted that their scheduling system assisted in minimizing overlapping visits that could not be reimbursed (e.g., a nurse and an aide in the home at the same time). Sites C and D noted that their systems allowed improved efficiencies for clinical managers by facilitating rapid re-assignment of patient visits in response to staff illnesses and absences. Clinical staff were able to access schedules from home, thus decreasing the need to travel to the office. This benefit reduced costs, improved staff satisfaction, and facilitated the agency’s ability to address clinical staff shortage issues by allowing them to hire staff living further distances from the office. Site D’s scheduling system incorporated the ability to map the patient’s address, which enhanced the manager’s ability to assign staff more efficiently and provided clinical staff with a tool to assist them in planning visits (e.g., arranging visits for patients living in
24

close proximity). Other cited benefits of scheduling systems included fewer missed visits to patients, better monitoring of the number of visits approved on the plan of care and the visits delivered, and the ability to schedule multiple disciplines on the same day (e.g., aide and nurse). These benefits increased regulatory compliance and quality of care. Site C noted that their human resources management system was beneficial in facilitating tracking personnel requirements (e.g., up-to-date licenses) and facilitating regulatory compliance. Site D reported that use of an e-learning system for the monitoring and delivery of staff training saved travel costs and produced efficiencies for managers.
Sites C and D discussed the use of telephony for home health aide scheduling and
documentation. These systems required the aides to place a phone call when they entered the home and electronically document visit activities via the telephone at the close of the visit. Benefits of telephony systems included a decline in administrative time needed to track aide documentation and bill for aide services. Site C noted that the immediate submission of aide visit documentation allowed them to move to a weekly payroll for aides, which improved aide satisfaction and served as a tool to facilitate aide recruitment and retention. Another benefit of the telephony system was the improved ability to monitor aide visits, including the amount of time spent in the home and travel time, as well as visits that began later than the scheduled appointment time. Calls to patients were made to follow up when the scheduled aide had not called at the appointed visit time, which was noted to improve coordination with the patient and patient satisfaction. Because the aides were able to access their schedule and the patient name, location, directions, and care plan from home, there was less need for the aide to visit the office physically. In addition, the system tracked discrepancies between activities performed and approved care plan activities, which minimized the possibility of the aide performing tasks that were non-reimbursable. Both Sites C and D noted that the telephony systems saved paper and eliminated the possibility of lost patient documentation.
Electronic referral systems were used by Site D. This system had both
administrative and clinical benefits, including more accurate and complete patient information, faster decisions about patient eligibility, and shorter turnaround times from receipt of the referral to the initiation of services. Other cited benefits were increased referrals from participating hospitals due to the convenience of the electronic referral systems for the discharge planners.
2. Electronic Health Records (Table 14)
Functionality: The EHR consists of electronic demographic information, clinical assessments, care plan and updated physician orders, clinical progress notes, and other summary reports including discharge summaries and referral documents. The use of an EHR enabled remote access to the clinical record by multiple users simultaneously.
25

Applications: All visited HHAs used EHRs for maintaining patient clinical records, incorporating all the applications described above. HHA clinical staff were able to view and enter clinical data in the EHR from both office and remote locations, including their homes. Sites A, B, and D encouraged clinicians to enter clinical data at point-of-care, while Site C required care providers to enter data at home or at the office at the end of the shift.
Benefits: All providers consistently reported that the greatest benefit of the EHR
was anytime and anywhere access to the clinical record by multiple providers. This access minimized the need for clinical staff to travel to the agency office to acquire information and retrieve or submit paper documentation, forms, or other data. This workflow benefit was considered large, and resulted in efficiency benefits, cost savings, improved coordination of care and patient hand-offs (e.g., to cover for a sick call), and increased staff satisfaction. Other perceived benefits of remote access to clinical and other data included more historical patient data available to clinical staff, immediate access to lab results, quality of care efficiencies in allowing multiple users access to data simultaneously, and increased information available to clinical managers to respond to calls from physicians, patients/families, and other care providers. These perceived benefits resulted in decreased time needed to track down information by telephone or other methods. Sites A, C, and D discussed the benefits of enhanced access to clinical data for facilitating care coordination across multiple providers.
A perceived benefit of EHR documentation cited by all four HHAs was improved charting. By virtue of a structured format, patient information was collected in a consistent manner and the necessary fields had to be completed prior to closing a record. Sites A and D noted that submission of visit documentation was more complete and timely, and that point-of-care documentation likely improved clinical data accuracy. Improved access to clinical documentation was identified as an increased efficiency for field staff, eliminating the need to request and pull old charts for repeat patients (Sites A and B) and eliminating travel to the office for documentation. As described above, Site B reported that by increasing clinical data access to all staff and implementing administrative information technology applications, they were able to close two branch offices, eliminating management staff and associated office space. Other perceived quality benefits of greater access to clinical data included: (a) reductions in duplicate labs and X-rays; (b) the ability to access decision-support tools within the EMR, such as medication checking systems; and (c) enhanced communication with consulting clinicians (e.g., access to wound and ostomy care nurse [WOCN] notes). Site B estimated that their EHR increased clinical productivity (i.e., the number of visits/clinician) by one visit per day.
Because EHR-S typically interfaced with administrative systems (e.g., referral data
populated the EHR), there was less chance of transcription error. In addition, the systems automatically guided clinicians through OASIS patient assessment documentation (i.e., item skip patterns), which improved the accuracy of OASIS data and increased the efficiency of documentation by minimizing redundant data entry. Site B noted that their plan of care was automatically populated from assessment and care
26

planning data, saving time and improving the continuity between the plan of care and other clinical documentation.
Other perceived benefits of an EHR reported by all sites included cost savings
realized by minimizing the need for support staff to track visit notes, make phone calls, and “chase paper.” The system allowed greater efficiency for specialty clinicians (e.g., WOCN, dietitian) and allowed them to consult on more patients. In Site D, managers were able to run reports from the system, providing them with data to assist with staff workload assessments and appropriate assignments that improved staff efficiency. Sites A and C cited potential cost savings in the reduction of paper and copy costs; however, others that were maintaining dual paper and electronic storage systems did not realize these savings. Site B noted a benefit in terms of patient education, as they were able to print educational materials from the EHR to provide to patients. Site D noted that the EHR made it easier to have multiple clinicians providing care to one patient. This was perceived as a quality benefit (e.g., enhanced care coordination) and a staffing benefit.
3. Medication Administration Records/e-Prescribing/Computerized Provider
Order Entry (Table 15)
Functionality: Automated functions related to medications include the use of e-MARs, electronic prescribing functions, and CPOE. E-prescribe/CPOE functions typically include decision-support tools for medication dosing, interactions, duplicate therapy, allergies, etc. In home health care, unless the patient is receiving IV therapy, most home care patients self-administer medications and e-MARs are not applicable. However, Medicare-certified HHAs are required to conduct a drug regimen review for all patients, which consists of checks for potential adverse reactions, drug and food interactions, duplicate medications, etc., and many use software systems to perform the checks.
Applications: All HHAs incorporated medication lists into EHRs and used
medication databases for their drug regimen reviews. Sites B and D also were able to print patient medication teaching guides (e.g., instructions on how to administer medications, monitor for side effects). Sites C and D noted use of an e-MAR for IV therapy. All four sites took verbal or faxed orders from physicians, then transcribed them into the EHR. For medication ordering, physicians involved in caring for patients at Site A used an EHR that was separate from and not fully compatible with the EHR at the HHA. As a result, staff at the HHA at Site A had to re-enter medication orders in the HHA EHR. Site D reported that they were pilot testing a similar program allowing a select group of physicians to review, update, and electronically sign orders. Although functioning without full CPOE, agencies had some level of order automation. In Site C’s system, non-medication orders (e.g., lab draws) were entered into the EHR which automatically placed the orders on the patient schedule.
Benefits: Sites B, C, and D noted perceived benefits of medication checking
functionality including improved efficiency over manual medication checking (particularly
27

with long lists of medications), ease in identifying the highlighted potential drug interactions, and better regulatory compliance. Because the list of medications was maintained electronically, medications needed to be entered only once, which was considered both an efficiency and a quality benefit. Sites B and D reported that the ability to print medication teaching guides standardized medication instruction. Clinical managers were better equipped to respond to phone calls from the physician about current medications, which improved response times to these requests and increased physician satisfaction (Sites B and C).
HHAs were able to run reports tracking the status of the order approval (e.g.,
orders sent to physician for signature, signed order received). In Agencies A and D, the electronic review and approval system for medications increased physician efficiency and allowed them to review the orders from home at a convenient time. Additionally, this system allowed more effective tracking of the status of orders and reduced the need to contact physicians for follow up.
4. Quality Management and Reporting (Table 16)
Functionality: Electronic quality management and reporting includes tools within
the clinical record used by providers at the patient level, as well as reports used by managers to assess quality at an organizational-level.
Applications: Organizational-level electronic quality reports reported to be used
by the HHAs hosting site visits included summary data pulled from EHRs such as numbers or percentages of patients experiencing adverse events; negative clinical outcomes (e.g., emergency department use); and numbers or percentages of patients receiving immunizations, meeting clinical goals, or experiencing missed medications. These reports were sometimes defined within the HIT system (e.g., pre-defined dashboard reports), and at other times were created by the agency or a consultant. Electronic alert and incident reports consisted of identification of specific patients or incidents that required follow up. These alerts were sometimes drill-down applications within quality reports, and at other times were delivered as e-mails or on a dashboard. These alerts oftentimes required resolution of some type before the user could sign out. Electronic decision-support tools used by the HHAs at point-of-care or during a care episode included clinical pathways, flags or reminders (e.g., labs due), risk assessment tools (e.g., falls risk), flags for potential medication errors, and trend reports that highlight out-of-range values (e.g., labs, vital signs, etc.).
Sites A, B, and C contracted with external vendors to provide reports on outcome
and case mix-based on OASIS and other clinical data; Site D provided these in-house, along with reports on other quality indicators. All four sites used dashboard reports of key quality indicators (e.g., hospitalizations) to guide quality improvement and management programs. Site C had real-time alerts from the telephony system for late or missed CNA visits, allowing them to contact the patient and reschedule or re-assign visits if needed. All four agencies reported the use of decision-support tools within their EHRs, including alert flags for labs due to be drawn and use of clinical pathways to
28

manage specific clinical conditions (e.g., diabetes). Additionally, all four sites used risk assessment tools (e.g., falls risk, pressure ulcer risk, rehospitalization risk) within their EHR assessments.
Benefits: Three sites (A, C, and D) reported using electronic quality reports based
on OASIS and other data (e.g., lab results) to identify areas for quality/performance improvement initiatives. Agency C noted that drill-down capabilities for these reports allowed identification of specific patient data to include in these initiatives (e.g., specific patients who were rehospitalized). Benefits of other reports included availability of data to improve aide assignments and care planning, and the enhanced ability of managers to monitor the care being delivered in homes (i.e., identification of patients with out-of-range lab values) and respond quickly to problems. Sites B and C reported the ability to run reports on average HHRG by clinician, enabling them to identify individuals needing retraining on admission documentation to improve OASIS accuracy. Site D used EHR data to calculate quality scores, which were used to evaluate and reward clinical teams for excellent or improved care performance. This agency also noted that they were able to use quality reports to evaluate the success of new programs in the pilot phase, which gave them information on whether to implement the new programs agency wide.
Decision-support tools were perceived to improve care coordination and
consistency across care providers. Site D noted that they were able to reduce hospitalizations for wounds after implementing a specialized wound care program that used electronic images of wounds and enabled review/consultation by a wound specialist. All four sites noted that automated flags for ordered procedures, such as lab draws, improved coordination across care providers and increased the likelihood that treatments were carried out as ordered. Sites B, C, and D reported that electronic clinical pathways improved the quality of care provided to patients. Risk assessment tools integrated into their EHR to enhance care planning for patients at risk for falls, pressure ulcer development, or hospitalization were reported to improve clinician ability to identify and plan care for high-risk patients. Site D noted that electronic trending of vital signs and other parameters, and reports of potential drug interactions provided important information to facilitate clinical decisions.
5. Health Information Exchange (Table 17)
Functionality: HIE functions are those that allow the electronic transfer of patient data among organizations (e.g., hospital, physician) and with patients/families.
Applications: All sites had secure messaging systems allowing care providers
the ability to share patient-level information with other care team members. Site A had access to electronic hospital data and by virtue of an interface, were able to import some data into their home care EHR (i.e., patient demographics, etc.). Site A also was able to communicate electronically with physicians in the health care system for messaging and to obtain orders. Physicians had access to telemonitoring and other home care clinical data. Site B had a portal allowing physician access to the home care data in one affiliated hospital, but reported very low usage of the portal. Site D had
29
developed electronic data sharing applications with selected health care organizations and laboratories and in several instances, was able to view other organization data (e.g., lab results) and/or send data within RHIOs. This site used three different systems for obtaining referral information from several referring hospitals.
Benefits: Site A, which had adopted an EHR that was partially integrated with the
hospital EHR (i.e., some information was shared across the EHRs), noted benefits including fewer transcription errors, less need to ask patients multiple times for the same information (i.e., demographics), and more complete documentation. While only Site D was using electronic referral systems with several hospitals and they perceived large benefits related to improved patient safety through more accurate information and minimal need for transcription of paper orders. The electronic referral system was efficient in that it allowed the hospital to transfer information that was then integrated into the patient’s HHA EHR. (See Administrative Functions, for more discussion on electronic referral benefits.) Site D developed a system with a small group of hospitals in which a patient was flagged as a prior home care referral upon registration in the emergency department. The emergency department contacted the agency, which in turn contacted a home care nurse assigned to that hospital. The home care nurse visited the patient during the emergency department visit or shortly thereafter, potentially allowing the patient to return home in lieu of being hospitalized, or shortening the hospital length of stay (due to facilitating transfers to the home). Other benefits to this system were reduced emergency department wait times and reductions in duplicative tests.
All four agencies reported the use of secure messaging systems allowing clinicians
to correspond about specific patient concerns or questions. Site A used the system for communications with physicians and Site D had pilot-tested a similar physician communication system. Benefits of the system included increased efficiency and quality of communications with physicians. For agencies that only used secure messaging systems with internal staff, perceived benefits included facilitation of information hand-offs (e.g., patient reports), efficiencies in using broadcast functions for agency announcements, improvements in the ability of the clinician to respond to questions about a patient while respecting patient confidentiality (e.g., responding privately to messages while in another patient’s home), increased confidence that the intended recipient will get the message, improved documentation that the message was sent, improved communication across branch offices, and decreased need for clinical staff to travel to the office. Site C noted that the secure messaging system had positively affected nurse employee retention.
6. Telehealth (Table 18)
Functionality: Telehealth functions include telemonitoring of vital signs and other
clinical parameters, tracking systems, personal emergency response systems, teleimage transmission, digital cameras or cellular phones with photo capabilities, and medication administration devices.
30
Applications: Sites A, B, and D reported using telehealth applications including telemonitoring of vital signs and medication reminders for specific groups of patients, such as those with heart failure or chronic obstructive pulmonary disease (COPD). Sites B and D provided nurses with cameras to document wound images and Site B forwarded images to consulting wound care experts or physicians. Sites B and D allowed therapists (e.g., physical therapist, speech-language pathologists) to make virtual visits. The degree to which the telehealth data were integrated into the EHR varied with the application and across HHAs.
Benefits: Perceived benefits of home telemonitoring units included fewer visits,
with Site A reporting an average decrease of 2.2 visits per episode. Site B noted that telemonitoring enabled them to handle an increased census with fewer staff. Other perceived benefits were improved medication compliance and an increase in the home care clinician’s confidence that a patient could be safely maintained at home, as well as the patient’s confidence in their ability to self-manage in the home (although some patients declined telehealth because they perceived it to be too intrusive). Increased communication with patients, including more opportunities for positive reinforcement of self-care was noted. The telemonitoring systems provided information allowing faster identification of problems and response to clinical changes. Site B commented that access to services was increased because clinicians in short supply (i.e., therapists, wound care specialists, etc.) could be involved in patient care without visiting the patient’s home. Wound care images enhanced wound care specialist and physician ability to track patient progress and identify the need for changes in the plan of care. Sites B and D reported decreased emergency department visits and rehospitalizations, while Site A did not see reduced acute care utilization. Site B perceived that telemonitoring could potentially keep patients at home rather than being admitted to a nursing home. In addition, Site B perceived that they benefited from increased referrals due to their telehealth program.
D. Perceived Costs of Health Information Technology for Home Health Agencies
1. Hardware and Software Purchases (Table 19) Large financial outlays were identified for servers and back-up systems, although
the costs varied widely depending on the storage size and processing speed. Different servers were sometimes dedicated to different applications (e.g., one for secure messaging, another for EMR storage). Each HHA reported using between two and 20 servers. Servers had to be maintained and periodically replaced. Site C noted that servers were replaced every four years. Data entry hardware included laptops or pen-based tablets for clinical staff and personal computers for office staff. Some clinical staff used personal home computers to enter data via secure web portals. HHAs using telemonitoring systems reported expenditures for hardware purchase or lease, and Site B noted that they had to create a “clean room” to sterilize units between uses. Other
31
identified hardware costs included printers, scanners, and cameras and/or telephones with high-resolution photograph capability for wound care documentation.
Network and connectivity expenditures included costs for installing and maintaining
LAN, wide area/metro networks, wireless networks/bridges, internet connectivity, and remote access. Site C purchased several toll-free telephone lines for incoming telephony data from multiple branch offices.
Software costs varied considerably depending on the systems purchased, bundling
of applications vs. individually purchased applications, agency size and number of licenses needed, and individual vendor negotiations. Additional costs were reported for development of interfaces between separately purchased software applications. Only one HHA (Site B) was able to provide quantitative data on costs for several individual applications.
2. Labor Costs (Table 20)
Costs incurred for information systems/technology personnel varied greatly, from
one HHA contracting for information systems/technology expertise and support, to another very large agency with a staff of 172 in the information systems/technology department. Costs for workflow re-design also varied. Site B used a vendor that provided workflow design consultation prior to and during system implementation, others assigned these responsibilities to existing staff. Only two sites (B and C) reported costs associated with staff turnover as a result of the implementation of a new system. Training costs for new employees were cited by all four HHAs. Site C perceived that there were some labor costs due to repetitive charting when patients are seen more than once per day (e.g., IV therapy cases are often visited more than once/day and certain data must be re-entered at every visit). This site did not document the visit at point-of-care, and one clinician commented that taking notes during the visit and then charting at another time was inefficient. Sites A and B noted that they had hired new staff for their telemonitoring programs. These included nurses and in Site B, an equipment delivery/installation person.
Labor costs for planning a new system implementation included travel and site visit
expenditures for investigating and negotiating new system purchases. As with nursing homes, these costs were unlikely to be tracked in any detail, although planning and oversight of the transition can absorb substantial time from multiple administrators and managers. Some HHA staff received additional training as “super-users” so that they could function as first-line responders for staff questions. Initial and ongoing staff training costs were noted. Additional training may be needed for system upgrades and new features. Short-term loss of productivity was noted by three facilities, one noted that this productivity “dip” lasted approximately four weeks. Site D reported some loss of productivity for systems that were not fully implemented or used, such that a combination of manual and electronic systems was maintained.
32

3. Miscellaneous Costs (Table 21) Site A identified that they continued to print out paper versions of forms for state
surveys but they noted that surveyor comfort with their EHR had improved. Changes in workflow patterns created both temporary and permanent inefficiencies. Site C cited the need for additional administrative time to monitor and use additional data created with a new electronic scheduling system. Other comments on added costs of HIT applications included time needed to review data that were previously unavailable, such as e-mail and quality reports. Lack of compatibility across systems was cited as a source of inefficiency by Sites A and C. Site C further noted inefficiencies because they were unable to access electronic data from the hospitals via their point-of-care system, which made it necessary for clinical staff to review patient information from two separate systems (electronic and paper). Other miscellaneous costs included inefficiencies when it was necessary to recover data due to system downtimes and interruptions (e.g., “crashes”), and interruptions due to system upgrades. Increased printing and paper costs were identified for Site C, due to the need to print out the EHR notes that were larger than old narrative charting forms due to including additional data (Site C maintained dual paper and electronic storage systems). Site B noted that a few patients were dissatisfied with point-of-care data collection, noting that the nurses paid too much attention to the computer. Site B also noted challenges in discharging patients on telemonitoring programs, as patients were not confident in their ability to manage their condition without constant monitoring.
33
IV. SUMMARY AND DISCUSSION While all eight of the case study sites noted that they would “never go back” to
paper-based systems for administration and clinical service delivery, no site had conducted a rigorous cost-benefit analysis of their HIT systems. Thus, the case studies necessarily focused on perceived costs and benefits from the perspective of system users and managers. Respondents were, however, able to cite numerous examples of system benefits and identify the types of increased costs and burdens resulting from HIT implementation, providing valuable insights for long-term care providers or policymakers considering investments in HIT.
The single most highlighted benefit for both the nursing home and HHA sites was
anytime and anywhere access to health information afforded by an EHR. A second benefit articulated at most all the sites was a greater efficiency in meeting administrative and federal requirements in long-term care. A third benefit that was universal, while not fully realized in most sites, was improved quality management through reports, alerts, and decision-support tools. Finally, in the few cases where sites had the capability, HIE between providers was reported to be a large benefit. These four major benefits are discussed further below.
A. Anytime and Anywhere Access to Health Information A major benefit that was reiterated at every site by clinicians and administrators
was access to the patient’s health record from any location, at any time, and by multiple users. This access to electronic records was sharply contrasted to locating and retrieving the single copy of the resident’s paper chart that may be in use by another individual, requiring not only the time to find and retrieve the record but also delays in waiting for the record to become available. Numerous examples were given of the advantages of being able to immediately access the chart in a nursing home when receiving a call from the family or the physician. In HHAs, the time savings and care coordination benefits were clearly substantial with various clinicians at multiple locations needing to review or make an entry into the record.
Access to health records from remote locations enabled remote providers, such as
physicians, to review charts, make clinical decisions, authorize orders, and complete other tasks in a timely manner without traveling to the facility. In HHAs, this feature was a major benefit to all care providers who typically work remotely from the office. Some system designs required LAN access to a local server, whereas other systems managed the electronic record system in a web-based application that could be accessed from any hardware or PDA wirelessly. Taking advantage of wireless technology made system access particularly efficient.
While this benefit is apparent in almost any health care setting, in long-term care it
is particularly pronounced. Long-term care is provided by teams of clinicians that all
34

have to share the same record in order to coordinate services. In home health care, both the patients and the entire care team are geographically dispersed, which is also the case for some members of the nursing home care team that work on a contractual basis. Physicians, an integral member of the team, are almost always remote from a nursing home or HHA, and often need to review information to make clinical decisions and write orders. Family members of nursing home residents are also often remote and when they call, the ability of the provider to rapidly retrieve resident information is a major benefit.
Added burdens and costs were associated with the anytime and anywhere access
to the record, although they were not reported to outweigh the substantial benefits. One potential burden related to inputting clinical information, and the training associated with learning to do this. The value of retrieving electronic resident information is of course limited by the completeness and accuracy of the information in the system. Most of the visited sites were nearly paperless (and one nursing home and one HHA were fully paperless), which completely obviated the need for locating any paper record information. However, training clinical staff to use the systems to input information was often a burden. While physicians often reviewed the EHR, they frequently relied on nursing home staff or office staff to input their orders. With turnover and employment of part-time staff, many CNA and other nursing staff acknowledged added time to learn and even to chart using the electronic systems. Two system issues affected these burdens: (1) the utility of the user interface for clinical staff to enter information at point-of-care; and (2) whether the physician’s office system was integrated and interoperable with the nursing home or home health EHR-S. Optimizing these areas could reduce the burden of providing access to the necessary information.
B. Greater Efficiency in Meeting Administrative and Federal Requirements With complexities related to determining eligibility for coverage, case mix
reimbursement, and the numerous federal, state, and insurance carrier requirements in long-term care, administrative systems that are integrated with clinical information were reported to yield substantial benefits to providers. Administrative staff could be more efficient and accurate, as they did not need to enter information that could be automatically pulled from the EHR. Bills could be automatically generated from clinical information entered into the EHR leading to shorter billing cycles. Information used for payment was more accurate with automated edit checks both to ensure that services that are provided are billed and to ensure that billed services are being provided.
Additionally, both nursing homes and HHAs reported substantial declines in the
number of claims denials and resubmissions, which can affect the provider’s and/or patient’s finances. With the proliferation in Medicare Advantage plans, each of which has different billing requirements, integrated billing allowed for expedited pre-authorizations that minimized time lags in initiating patient services. Other clinical/administrative functions benefited from these systems such as improved
35

accuracy of MDS and OASIS data. In HHAs, scheduling systems (particularly when linked with patient health information) ensured that patient visits were provided as specified within the physician-ordered plan of care. Time savings accrued to most providers that resulted in reductions in administrative staffing.
Providers cited mixed results in terms of their experiences with state surveys since
implementing HIT. While some noted that they had experienced declines in deficiency citations, one noted that they received more deficiencies. This was attributed in part to the difficulty that surveyors encountered in finding the documentation that they relied on to assess care in an EHR with which they were not familiar, and to more accurate documentation that may have led surveyors to identify more problems than would have been possible in a paper system. In some cases, state surveyors were not comfortable reviewing EHRs and selected records had to be printed out for surveys. One provider met with the survey agency and developed reports for the surveyors with information that had to be compiled during surveys. When the surveyors appeared, they were able to provide the requested information very quickly, minimizing disruption to facility staff, and facilitating surveyor efficiency.
C. Improved Quality Management Sites highlighted the benefits of their HIT system for quality management through
three types of applications: (1) automated generation of standardized reports on all residents; (2) alert, incident, and event reporting; and (3) decision-support tools. Standardized reports were based on information obtained as part of MDS and OASIS assessments (quality indicators and HHRGs), ongoing CNA resident assessment (e.g., bowel and bladder, skin, weight, food consumption), medication administration (e.g., missed doses, PRN use), and laboratory values (e.g., out-of-range). Alert and incident reporting consisted of identification of specific residents on a dashboard or in an e-mail oftentimes requiring resolution of some type before the user could sign out. Such alerts that were generated based on inputs from a CNA might also be directed to the unit charge nurse or supervising RN. Decision-support tools often included risk assessment and reporting tools (e.g., risk for falls, pressure ulcer, or hospitalization), and specialized treatment protocols and monitoring (e.g., wound care) or trending of data (e.g., vital signs, weight).
For nursing and management staff, one of the major benefits of such reporting was
substantial time savings in reviewing resident/client information to identify problems requiring attention. Reviewing weight books, bowel and bladder books, med sheets, lab reports, and other paper-based resident/client documentation was clearly more time-consuming and less complete. The benefit for the residents/clients was higher quality care. The combination of electronic reports to routinely track status, alerts that identified specific residents/clients with a more immediate concern, dashboards that required an action before logging out, and risk tracking led to numerous examples of early intervention to prevent development of problems like falls, weight decline, skin breakdown, and hospitalization. For the provider, this resulted in better quality
36

indicators and fewer survey deficiencies in cases where problems were avoided and all documentation was present.
These benefits were associated with some added costs/burdens. The availability
of information required an informed user to review it on a systematic and regular basis, which often was difficult for nursing homes and HHAs to achieve. This was an added task for clinical management staff, who were already busy with pressing demands, often requiring the addition of a person or portion of one designated to review and follow up on the reports. Many sites were discovering how to manage all the information that they were generating through quality reporting systems. The number of residents and clients identified on these reports can be large depending on the quality of the information, the criteria used to identify residents/patients, and the frequency with which the reports were reviewed, sometimes leading to an overwhelming situation. Alert systems highlighting the most critical issues were less problematic in this regard. For the potential of HIT to be realized with regard to improved quality management, systems for reviewing and acting on the information required developments and refinements in workflow in addition to HIT implementation.
D. Health Information Exchange While only a few providers had HIE capabilities among different providers, the
benefits of data exchange were noted to be substantial in terms of efficiencies, data accuracy, and enhancements to care coordination and transitions. Data exchange with physicians for order review and approval minimized duplicate data entry, saved time spent tracking orders, decreased telephone calls for order clarification, and improved physician satisfaction overall. Data exchange with hospitals facilitated patient admission and transfer processes, reduced telephone and data entry time, and minimized potential transcription errors. Access to data from other providers (including lab and X-ray data) minimized duplicate labs and other procedures. Electronic referral information exchange resulted in more complete and accurate clinical information during care transitions resulting in more efficient and coordinated care across settings.
37

V. POLICY IMPLICATIONS With passage of the ARRA, the President and Congress have identified
implementation of HIT as a critical component to bring about necessary health care reforms including improving quality and coordination of care, reducing medical errors, and lowing health care costs. The ARRA provided:
(i) $2 billion to assist in implementing the “HITECH” (Health IT for Economic
and Clinical Health) provisions to support the implementation of HIT for all persons in the U.S. by 2014; and
(ii) approximately $17 billion for incentive payments generally directed to Medicare and Medicaid physicians and hospitals who are determined to be "meaningful users" of certified EHR technologies.
The ARRA requires HHS to conduct a study to determine the extent to which
payment incentives should be made available to health care providers who are receiving minimal or no payment incentives or other funding for purposes of implementing and using certified EHR technology (ARRA, Title IV, §4104(a)). While the types of health care providers that will be included in this study have not yet been defined by the Department, the definition of “health care provider” in HITECH includes skilled nursing facilities, nursing facilities, and home health entities.
The findings from this study on the “Costs and Benefits of Health Information
Technology in Nursing Facilities and Home Health Agencies” address some of the issues the §4104(a) study is required to examine. The ARRA §4104(a) requires study of whether and how payment incentives should be made available to other providers, and requires the examination of several issues, including:
(i) the clinical utility of such technology by such health care providers; and (ii) whether the services furnished by such health care providers are
appropriate for or would benefit from the use of such technology. The findings from these qualitative case studies have highlighted the clinical and
administrative benefits and costs of using EHRs, including technologies for HIE activities needed and used by nursing facilities and HHAs. We strongly recommend that approaches be considered for supporting and accelerating HIT adoption in nursing homes and HHAs to realize the quality improvements and efficiency gains suggested by these case studies.
38

REFERENCES
Amarasingham, R., Plantinga, L., Diener-West, M., Gaskin, D.J., & Powe, N.R. (2009). Clinical information technologies and inpatient outcomes: A multiple hospital study [see comment]. Archives of Internal Medicine, 169(2):108-14.
American Health Information Management Association. (2007a). 2007 Long Term Care
(LTC) Health Information Technology (HIT) Summit Working Document. Unpublished Work.
American Health Information Management Association. (2007b). HL7 LTC-Nursing
Home EHR-S Functional Profile and Letter of Invitation. Unpublished Work. American Health Information Management Association (2008a). A Road Map for Health
IT in Long Term Care 2008-2010. http://www.ahima.org/meetings/ltc/documents/LTCSummitRoadmap_Final_2008-03-17_000.pdf [On-line].
American Health Information Management Association (2008b). The New York State
Nursing Home Demonstration Project (power point presentation). http://www.ahima.org/meetings/ltc/documents/DelvingintotheDetailsTheNYStateResearchStudy_000.pdf [On-line].
Ash, J.S., & Bates, D.W. (2005). Factors and forces affecting EHR system adoption:
Report of a 2004 ACMI discussion. Journal of the American Medical Informatics Association, 12:8-12.
Bates, D.W. (2002). The quality case for information technology in healthcare. BMC
Medical Informatics & Decision Making, 2:7. Bates, D.W., & Gawande, A.A. (2003). Improving safety with information technology.
New England Journal of Medicine, 348(25):2526-34. Booz Allen Hamilton. (2006). Evaluation Design of the Business Case of Health
Information Technology in Long-Term Care: Final Report. Washington, DC: Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, HHS. http://aspe.hhs.gov/daltcp/reports/2006/BCfinal.htm [On-line].
Chaudhry, B., Wang, J., Wu, S., Maglione, M., Mojica, W., Roth, E. et al. (2006).
Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Annals of Internal Medicine, 0000605-200605160.
39

Cherry, B., Carter, M., Owen, D., & Lockhart C. (2008). Factors affecting electronic health record adoption in long-term care facilities. Journal for Healthcare Quality, 30:37-47.
Cherry, B., & Owen, D. (2004). Evaluation of a Web-based Electronic Medical Record
and Communication System for Long-Term Care Facility Management: Final Report. Lubbock, TX: Texas Tech University Health Sciences Center. Unpublished Work.
Cherry, B., Owen, D., & Bachetti, B. (2007). Determining Factors of Organizational
Readiness for Technology Adoption in Long-Term Care Facilities, Phase 2 Report: Focus Group Survey Results. Lubbock, TX: Texas Tech University Health Sciences Center, Garrison Institute on Aging. Unpublished Work.
Cornell University Survey Research Institute. (2008). New York Nursing Home Project:
Quality Care Technology Demonstration Project. http://www.sri.cornell.edu/sri/projects.project.cfm?projid=123420 [On-line].
Cortes, L.L., & Chou, J.Y. (2004). Using Electronic Medical Records in the Nursing
Home: 2004 Centers of Excellence Report. Texas: Texas Department of Aging and Disability Services.
Degenholtz, H.B. (2007). Availability and Use of Health Information Technology in
Nursing Homes. University of Pittsburgh, Department of Health Policy and Management.
Division of Health Care Policy and Research. (2007a). Report Categorizing Point-of-
Care and Health Information Exchange Tools: Report A: Review by Representatives from Standards Development Organizations. Aurora, CO: University of Colorado Denver.
Division of Health Care Policy and Research. (2007b). Report Categorizing Point-of-
Care and Health Information Exchange Tools: Report C: Review by Representatives from Home Health Agencies. Aurora, CO: University of Colorado Denver.
ehealthsolutions-SigmaCare. (2008). Mitigating Risk in Long-Term Care Workflow
Automation Through Operational Transformation: The Sands Point Center Case Study. http://www.ahima.org/meetings/ltc/documents/SigmaCareCaseStudy.pdf [On-line]. Available: http://www.ehealthsolutions.com/pdf/SigmaCare_Sands_Point_Case_Study.pdf.
Fazzi, R., Ashe, T., & Doak, L. (2007). Philips National Study on the Future of
Technology and Telehealth in Home Care: An Executive Level Briefing. http://www.medical.philips.com/main/products/telemonitoring/assets/docs/Philips_National_Study_%20Dr.%20Fazzi_Oct_25_07.pdf [On-line].
40

Girosi, F., Meili, R., & Scoville, R. (2008). Extrapolating Evidence of Health Information Technology Savings and Costs. http://www.rand.org/pubs/monographs/2005/RAND_MG410.pdf [On-line].
Institute of Medicine. (2001). Crossing the Quality Chasm: A New Health System for the
21st Century. Washington, DC: National Academy Press. Institute of Medicine of the National Academies. (2003a). Priority Areas for National
Action: Transforming Health Care Quality. Washington, DC: The National Academies Press.
Institute of Medicine, Committee on Data Standards for Patient Safety. (2003b). Key
Capabilities of an Electronic Health Record System, Letter Report. Washington, DC: The National Academies Press.
Judge, J., Field, T.S., DeFlorio, M., Laprino, J., Auger, J., Rochon, P. et al. (2006).
Prescribers' responses to alerts during medication ordering in the long term care setting. Journal of the American Medical Informatics Association, 13:385-390.
Kaushal, R., Blumenthal, D., Poon, E.G., Jha, A.K., Franz, C., Middleton, B. et al.
(2005). The costs of a national health information network. Annals of Internal Medicine, 143:15-173.
Kaushal, R., Jha, A.K., Franz, C., Glaser, J., Shetty, K.D., Jaggi, T. et al. (2006). Return
on investment for a computerized physician order entry system. Journal of the American Medical Informatics Association, 13:261-266.
Kaushal, R., Shojania, K.G., & Bates, D.W. (2003). Effects of computerized physician
order entry and clinical decision support systems on medication safety: A systematic review. Archives of Internal Medicine, 163:1409-1416.
Middleton, B., Hammond, W.E., Brennan, P.F., & Cooper, G.F. (2005). Accelerating
U.S. EHR adoption: How to get there from here. Recommendations based on the 2004 ACMI retreat. Journal of the American Medical Informatics Association.12(1):13-9, Feb.
National Center for Health Statistics, Centers for Disease Control and Prevention.
(2008). National Nursing Home Survey 2004 Facility Tables. http://www.cdc.gov/nchs/data/nnhsd/nursinghomefacilities2006.pdf#01 [On-line]. Available: http://www.cdc.gov/nchs/about/major/nnhsd/Facilitytables.htm.
Pacicco, S. (2008). The Current State of EMRs in LTC Settings (Nursings/Long Term
Care Management). SigmaCare [On-line]. Available: http://www.ehealthsolutions.com/content.asp?content_id=140&content=newsdir/articles.
41

42
Poon, E.G., Jha, A.K., Christino, M., Honour, M.M., Fernandopulle, R., Middleton, B. et al. (2006). Assessing the level of healthcare information technology adoption in the United States: A snapshot. BMC Medical Informatics & Decision Making, 6:1.
Rantz, M., Scott-Cawiezell, J., Alexander, G., Conn, V., Madsen, R., Petroski, G. et al.
(2006). Evaluation of the Use of Bedside Technology to Improve Quality of Care in Nursing Facilities. http://www.cms.hhs.gov/reports/downloads/Rantz.pdf [On-line].
Rochon, P.A., Field, T.S., Bates, D.W., Lee, M., Gavendo, L., Erramuspe-Mainard, J. et
al. (2005). Computerized physician order entry with clinical decision support in the long-term care setting: Insights from the Baycreast Centre for Geriatric Care. Journal of the American Geriatrics Society, 53:1780-1789.
Rumberger, J.S. & Dansky, K. (2006). Is there a Business Case for Telehealth in Home
Health Agencies? http://www.liebertonline.com/doi/pdfplus/10.1089/tmj.2006.12.122 [On-line].
Shekelle, P., Morton, S., & Keeler, E. (2006). Costs and Benefits of Health Information
Technology (Rep. No. Evidence Report/Technology Assessment No. 132, Prepared by the Southern California Evidence-based Practice). Rockville, MD: Agency for Healthcare Research and Quality.
Sidorov, J. (2006). It ain't necessarily so: The electronic health record and the unlikely
prospect of reducing health care costs. Health Affairs, 25:1079-1081.

TABLE 5: Nursing Homes -- Benefits Associated with Administrative Functions Administrative functions include census management, general ledger/accounts payable, verification of insurance and eligibility of services, accounts receivable/billing, track Medicare/non-Medicare claim denials, contracts management, payroll, MDS data entry/management/submission.
Benefits Site A Site B Site C Site D BILLING/REVENUE More accurate ADL measurement to derive case mix, increase revenues, and reduce MDS errors
X X X Medicaid payments were case mix-based, the revenue per patient day increased by $37 per day (30%)
X
Optimized cash flow because of increased efficiency getting bills out
X
Decrease in claim denials, flags problems before billing occurs
X X
Reduces time to close accounts each month
X Customized reports can catch errors and exceptions without looking at each bill individually
Allows for centralized billing with multiple homes, increasing efficiency and limiting staff
X
Allows nursing home to serve a larger number of payers since payer-specific requirements can be computerized
X One nursing home has 30 different payers, which nursing home says they could not accept without electronic billing
OVERSIGHT Reduced office supply and other costs from an ability to drill-down into individual purchase orders and reduce wasteful ordering
X
Makes utilization review more efficient (saves time) and more quickly identifies needed services
X X
Allows all staff to respond to insurer queries even on nights and weekends
X
Can review patient eligibility for Medicare Part A; review requirements for pre-authorization for Medicare HMOs centrally
X
STAFFING Reduced administrative staff for billing/insurance verification, etc., or allowed existing staff to handle growth in admissions or in complexity of billing
X For nursing home systems, centralization reduces needed staff
X
43

TABLE 5 (continued) Benefits Site A Site B Site C Site D
Improved staff resource management; better able to link to qualified staff (e.g., IV nurse) with patient needs; clinicians able to see more patients
X
Automated reports can reduce audit time for administrative staff by allowing MDS coordinator to see all data, even working from home when necessary
X
Fewer FTEs needed for admissions and case management
X In one facility, two positions were consolidated into one
Improved management and allocation of therapist’s time (by reviewing workload reports) and better management of therapists’ billing
X
CENSUS Census reporting functionality may include a census report by unit allowing A/D/T coordinator to see open beds by unit and more efficiently assist with placement
X X
More efficient checks of admission bed availability fosters more timely discharge from hospital and supports beneficiary/family search for services
X X May be enhanced for nursing homes that are part of a hospital system; one such found reduced hospital length of stay
Improved ability to review and manage census information centrally for multiple homes and direct patients to homes with open beds
X
44

TABLE 6: Nursing Homes -- Benefits Associated with Electronic Health Records
The EHR as defined here consists of electronic demographic information, clinical assessments, care plan and other physician orders, clinical progress notes, and summary reports including discharge summaries.
Benefits Site A Site B Site C Site D MULTIPLE/ANYTHING/ANYWHERE ACCESS Staff can access and patient/family get information immediately
X X X X
Enabled staff, including physicians, access to complete record and history (including labs, X-rays, etc.) from clinic or from home for long-term care patients NOTE: Quicker intervention by the provider who ordered the labs, may improve patient safety with timelier physician involvement
X A small sample showed 20% of labs were signed off on within 24 hours pre-system and 90% post-system
X X X
Physician/nurse practitioner access can reduce calls between MDs and nurses
X MDs, nurse practitioners and physician assistants are sometimes reluctant to use the systems
X
Real-time access to health information by clinicians reduced duplicative labs and x-rays, total labs, and ER visits
X Found approximately 50% reduction in ordered labs in a short sample period
X
Shared common electronic record available to staff used for discharges, including standard list of orders and information needed for a safe discharge
X X
Time savings for creating summary and real-time history for transfers; leads to safer transfers out and faster delivery of needed services upon arrival of the patients
X X Benefit primarily accrues to emergency room, hospital, and MDs
X When hospital records are shared, therapy can start earlier in skilled nursing facility
Health record and patient data are available when and where needed for all authorized staff
X X X X
45

TABLE 6 (continued) Benefits Site A Site B Site C Site D
Clinical staff are able to access patient information more quickly (e.g., specialists able to share recommendations more quickly, case managers able to access patient information more quickly and share with others, such as insurers, reduces response time to critical lab results or events)
X X X X
Real-time access to health information by clinicians reduces duplicated labs and X-rays, total labs, and emergency room visits
X X Reported some physician resistance to EMR use
X Reported some physician resistance to EMR use
Improved on-call response time for nurses, MDs/nurse practitioners and reductions in travel time and costs with a remotely-accessible EMR. May prevent hospitalization/emergency room use
X X Noted that large benefits accrue to outside providers such as physicians who are able to avoid travel to facility
X
Improved access to clinical decision-support tools (e.g., teaching plans) and education guidelines/handouts (e.g., teaching plans/education) for staff and patients
X Physicians can make better care plans
X
Import features to billing save time and increase billing accuracy NOTE: Also listed as benefit under administrative functions
X X X
Allows oversight by training coordinator and enabling them to focus training where most needed
X Facility reached goal of at least 95% compliance with ADL documentation
X
Can’t lose your work NOTE: This benefit is not apparent to some staff, particularly those who are not technologically experienced, who are more afraid with EMR that their work will be lost. An effort should be made to clearly explain the back-up system to staff so that they understand the redundancy of information in the system.
X X
46

TABLE 6 (continued) Benefits Site A Site B Site C Site D
More information is in chart in electronic vs. paper record
X Especially valuable if resident is new to a CNA’s care
X X
REDUCED DUPLICATION OF INFORMATION Fewer quality problems and improved patient safety (e.g., reduced data entry errors, reminds staff to perform certain functions)
X X X
Increased staff productivity (e.g., data entry duplication reduced, assessment charting faster) NOTE: Most facilities reported no decreases in clinical staff; they hope that potential time savings in documentation or elsewhere are applied to increased face-to-face patient care
X X
Patients don’t have to answer the same questions asked at hospital or during previous admissions if they are anywhere in the system
X Another area that reduces the possibility of error
More prompt and complete documentation
X Information is not missing when physician or nurse practitioner calls; less delay reporting to family
X X Less delay reporting to family
Can write one note for everyone in a recreational therapy group
X Reduction of 30 minutes to 10 minutes with group charting results in extra activities for residents
STAFFING CNAs are better able to manage own time and are more in control of work processes. They feel more empowered, more valued, able to see that the work they do and document is very important, leading to increased job satisfaction
X X
Oversight of CNAs/physical therapists can increase efficiency
X X Oversight can happen centrally
47

TABLE 6 (continued) Benefits Site A Site B Site C Site D
Reduced medical records time, ward secretary time NOTE: Medical records clerk is one of the only areas where staffing (FTE) was reduced
X X
Reduced RN/CNA time charting and finding chart
X X X
OTHER MDS assessments are completed more efficiently, with increased accuracy, and care plans are more accurate
X One facility was able to get more patients into higher rehabilitation levels
Reductions in paper and copying costs NOTE: Many facilities specifically reported no real reduction in paper costs.
X Reported that paper reduction occurred in the admissions process, where having electronic versions of discharge and referrals saved a lot of faxed paper
Reduction in costs to store information, either off-site costs or an ability to re-use the space formerly used for storage NOTE: Facilities choose to either start their EMR from a fixed point and store old paper charts, or they may scan in old charts, eliminating paper storage
X X
Use EMR as a marketing tool (i.e., advertising and recruiting potential residents)
X One facility said that they found many residents who used community physicians made an annual appointment with a facility physician to get their most current information into the EMR
Enhanced reputation and increased referrals
X
Improved regulatory compliance X X X One facility dropped from 13 to 2 citations after EMR was installed
48
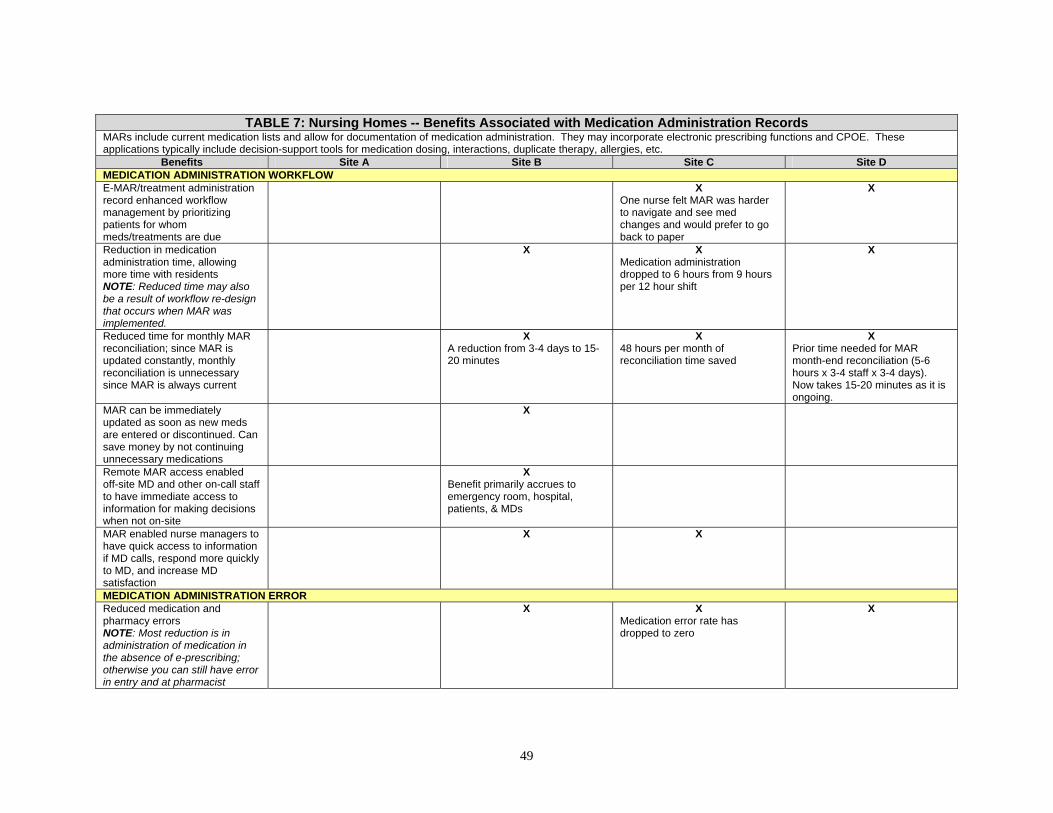
TABLE 7: Nursing Homes -- Benefits Associated with Medication Administration Records
MARs include current medication lists and allow for documentation of medication administration. They may incorporate electronic prescribing functions and CPOE. These applications typically include decision-support tools for medication dosing, interactions, duplicate therapy, allergies, etc.
Benefits Site A Site B Site C Site D MEDICATION ADMINISTRATION WORKFLOW E-MAR/treatment administration record enhanced workflow management by prioritizing patients for whom meds/treatments are due
X One nurse felt MAR was harder to navigate and see med changes and would prefer to go back to paper
X
Reduction in medication administration time, allowing more time with residents NOTE: Reduced time may also be a result of workflow re-design that occurs when MAR was implemented.
X X Medication administration dropped to 6 hours from 9 hours per 12 hour shift
X
Reduced time for monthly MAR reconciliation; since MAR is updated constantly, monthly reconciliation is unnecessary since MAR is always current
X A reduction from 3-4 days to 15-20 minutes
X 48 hours per month of reconciliation time saved
X Prior time needed for MAR month-end reconciliation (5-6 hours x 3-4 staff x 3-4 days). Now takes 15-20 minutes as it is ongoing.
MAR can be immediately updated as soon as new meds are entered or discontinued. Can save money by not continuing unnecessary medications
X
Remote MAR access enabled off-site MD and other on-call staff to have immediate access to information for making decisions when not on-site
X Benefit primarily accrues to emergency room, hospital, patients, & MDs
MAR enabled nurse managers to have quick access to information if MD calls, respond more quickly to MD, and increase MD satisfaction
X X
MEDICATION ADMINISTRATION ERROR Reduced medication and pharmacy errors NOTE: Most reduction is in administration of medication in the absence of e-prescribing; otherwise you can still have error in entry and at pharmacist
X X Medication error rate has dropped to zero
X
49

TABLE 7 (continued) Benefits Site A Site B Site C Site D
Integrated decision-support (e.g., prompts to take pulse prior to digoxin administration) that cannot be bypassed decreased medication errors
X
Reductions in missed treatments (e.g., test for BSLs, BP) NOTE: Much of the benefit occurs downstream, to the resident.
X X X
Improvements in medication pass performance on survey
X
Can print off medication teaching guides
X
CPOE Reduced chance of medication error since pharmacist does not need to read writing
X Some facilities have but MDs don’t use; nurses indicated if MDs would use the function it would increase accuracy
X
Less chance of transcription errors
X Still use fax for urgent issues
Fewer calls from nursing home, floor, or pharmacist to MD to confirm medication order
X
Flagging program can identify potential adverse medication interactions or doses NOTE: This feature also can lead to annoyance in physician staff due to the generally large number of medications a nursing home patient is on and the amount of overrides the physician must do. Facility did record that in one-quarter MDs changed med 105 times in response to an alert so it does have potential to reduce ADEs
X
Emphasis on the number of medications a patient is on could lead to MDs making greater effort to reduce meds
X Anecdotal evidence of this; requires that MDs actually use the software
Monthly medication renewal helps discontinue/reduce meds reducing unnecessary meds; could reduce F-tags
X Variation among MDs. Some simply renew all, others spend time in review
50

TABLE 8: Nursing Homes -- Benefits Associated with Quality Management and Reporting Quality management and reporting applications extract data from the EHR or other clinical applications (e.g., e-MAR) to generate reports allowing tracking of quality indicators. These may include incident reporting, tracking of adverse outcomes, tracking of infections, calculation of outcomes from MDS data, risk audits for quality areas of concern for surveyors, dashboard reports of key quality indicators, occupancy rates and trends, etc.
Benefits Site A Site B Site C Site D REPORTS Electronically generated reports are automatically produced, saving staff time sifting through paper or electronic files NOTE: In-house report writers may enhance report value. For all nursing homes, the value of reports may depend more on the design of the reports than their existence. EMRs and billing now have almost too much information. Facilities need to create the right reports for their staff.
X X X X
Electronically generated reports are produced more quickly, allowing faster response times
X X X X
Ability to run real-time reports can facilitate more efficient patient care, fast prioritization of patient needs, identification of patients needing spot checking NOTE: Benefit is enhanced with trending capability
X X X
Electronically generated reports have more complete/ accurate content, improving coordination of care across shifts
X X Many reports save manager time
X
Ability to run reports repeatedly can help with staffing decisions NOTE: Benefit is enhanced with trending capability
X
Can centralize review if multiple nursing home in a system NOTE: Benefit is enhanced with trending capability
X X X Avoids travel time
51

TABLE 8 (continued) Benefits Site A Site B Site C Site D
SPECIALIZED REPORTS Incident reporting capabilities allows faster response times and reduces time and costs of responding to incidents
X X Reduction of time to close out incident from 2 weeks to 2 days
X X
Real-time incident reporting and follow up facilitates a more immediate responses to family inquiries
X X X X
Tracking reports can foster administrator’s and clinician’s ability to discover problems quickly and move to correct them
X X X X
Summary reports may be generated for transfers to hospital/emergency room, physician review NOTE: Need reporting feature within EMR
X Biggest benefit may accrue to the hospital or MD who is downstream of the nursing home, but it saves nurse time at the facility pulling information
A/D/T coordinator may be prompted to obtain needed information
X
Reports indentifying high-risk patients (fall indicators, Coumadin administration) improved care, increased compliance NOTE: One facility has seen a decline in quality indicators/ measures reported by CMS in falls, fractures, pain
X X
Immunization and PRN medication prompts improve follow up and compliance
X
STAFFING CNAs can quickly see what activities are needed for each patient
X
Therapist efficiency can be charted and supervisors can better reach targeted percentage time with residents
X
Administrative staff are more quickly able to access and review records, able to spend more time with residents and staff
X
52

TABLE 8 (continued) Benefits Site A Site B Site C Site D
Automatically generated reports can reduce audit time for administrative staff
X Daily reports on staff work reduced monitoring time from 2 hours/day to 15 minutes/day
X One facility reported audit time dropped from 15 hours to 5-6 hours
OTHER Improved quality indicator, survey
X X Noted that improved reporting led to possibly finding more falls
X Large increase (from 40 to 80%) in the percentage of their quality indicator above the national average
Surveys are smoother, less interference in daily functioning of staff NOTE: Some facilities have had difficulties with surveyors refusing to use EMR. Facilities that were pro-active with their state agencies setting up the structure of surveys had better results
X
Decrease in liability claims and premiums
X Facility had to prove the reduction in claims over 2 years before the insurer lowered the premiums
X
53

TABLE 9: Nursing Homes -- Benefits Associated with Health Information Exchange
HIE is electronic health data shared across organizations. In nursing homes and HHAs, this may include on-line access for referrals, laboratory data, radiology data, patient consults, patient history from other settings, physician and/or pharmacist access to EMR, pharmacy data, HIE with patients/caregivers.
Benefits Site A Site B Site C Site D EXCHANGE WITH OTHER SETTINGS Local hospital access: emergency room gets electronic provider summary and nursing home can get electronic discharge summary or other information ensuring it is timely in the record NOTE: Enhanced to the degree sharing information occurs
X Smoother transitions; therapy and meds are started sooner in the nursing home
X Increased skilled nursing facility reimbursement for condition capture and RUGs maximization
Secure electronic messaging can flag and send message to primary care physician for transfer to emergency room, saves phone calls
X
PERSONAL HEALTH RECORD Health record can be stored on flash drive
X Some residents wear their flash drives around their neck; external providers can enter information that goes back to the nursing home
Personal record availability allows resident/family to review record for allergies, medications, etc.
X
RADIOLOGY Faster response to health issues as facility gets a report or actual image back in hours
X
By having images available, the resident may not have to be sent to clinic/emergency room/hospital for the diagnosis workup; saving transportation costs, staff time, Medicare costs, bed holds
X
54

TABLE 9: Nursing Homes -- Benefits Associated with Health Information Exchange Benefits Site A Site B Site C Site D
E-HIE with radiology achieves time savings by providing: (i) a report back to the facility within hours; and (ii) in some cases an image back to the facility. By having the images available, the resident may not have to be sent to a clinic/emergency room/ hospital for the diagnostic workup, which enhances quality of life for the resident and saves transportation costs, staff time from having to accompany resident, and Medicare costs by preventing emergency room use/hospitalization NOTE: Need direct information exchange with a radiology group
X
55

TABLE 10: Nursing Homes -- Costs Associated with Hardware and Software
Hardware and software costs include purchase, maintenance, and periodic replacement of servers and back-up systems. Other hardware costs included data entry hardware, including desktop and laptop computers, PDAs, and rolling medication carts to support computers.
Costs Site A Site B Site C Site D STORAGE Servers NOTE: Owning and maintaining servers is not necessary under all EMR system types, for example, some web-based systems store all of the data centrally at the software company site. EMR requires the most storage. Also, server costs vary widely depending upon the storage size and speed needed.
X Nursing home EMR uses 3 web servers, 1 database server; had to update to an expensive server since it slowed to a halt on a less expensive server
X Only use server for document storage
X EMR is off-site, web-based; use server for e-mail and administrator duties
X EMR is the source of most of the server requirements (use 20 servers for entire large health care system)
Personal computers, laptops NOTE: Need to expect to replace as necessary
X Now use one laptop per employee
X 12 workstations per facility
X Currently replacing personal computers with a workstation as they break
PDAs/Tablets NOTE: Two of four nursing homes visited had replaced PDA systems with laptops due to problems including breakage.
X Used but kept dropping signal so replaced with laptops, selling the old ones to try and recoup some of the cost
X Used PDAs, had breakage issues, new e-MAR system uses tablets
Back-up system NOTE: Nursing homes can choose to use on-site back-up servers/drives or to subcontract back-up services to outside firms.
X Has a back-up server personal computer in every building
X Web-based, back-up help by software provider
X EMR backed up by web service; e-mail; then backed up copies are held off-site
Cart for e-MAR X Combined with carts currently used for EMR
X Approximately $3,500
X
NETWORK AND CONNECTIVITY COSTS Local Area Networks (LAN) NOTE: In some instances, LAN and wireless networks are substitutes; within a nursing home, you could use either one as the basis for your inter-nursing home network.
X X Use T1, needed network wiring, testing, and a network switch
X
Wide Area/Metro Area Network X Clinical needs T1 lines
X Used to connect multiple long-term care facilities
56
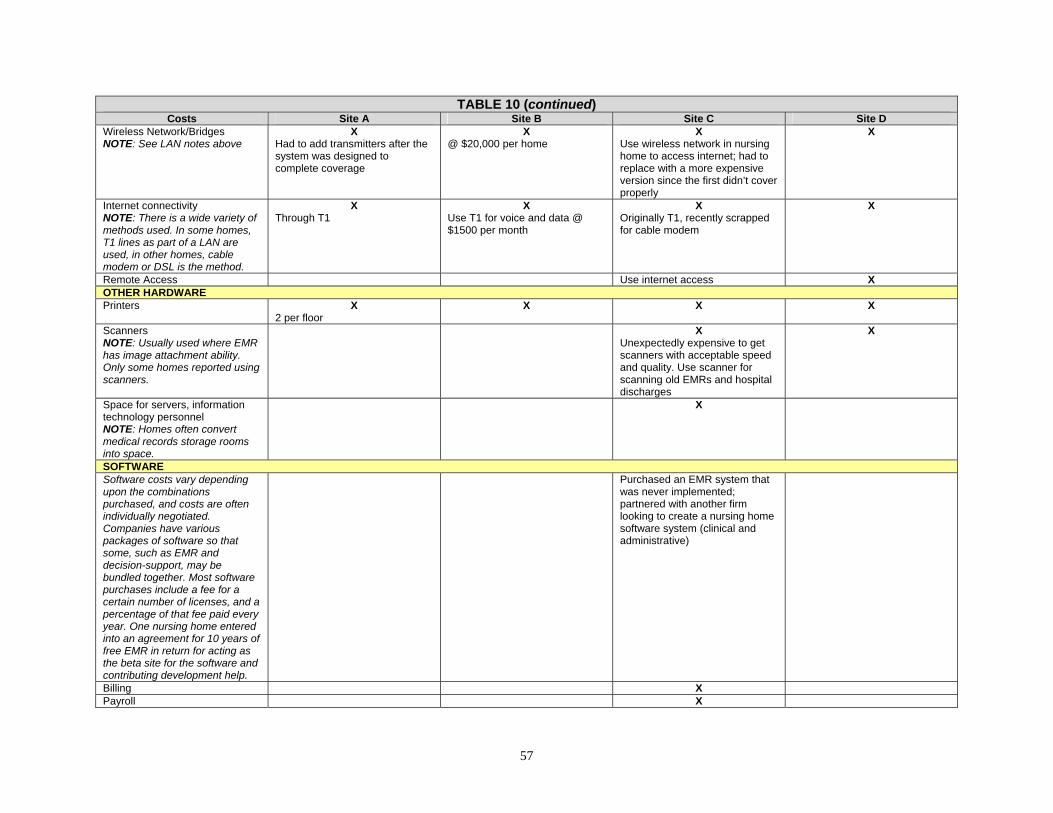
TABLE 10 (continued) Costs Site A Site B Site C Site D
Wireless Network/Bridges NOTE: See LAN notes above
X Had to add transmitters after the system was designed to complete coverage
X @ $20,000 per home
X Use wireless network in nursing home to access internet; had to replace with a more expensive version since the first didn’t cover properly
X
Internet connectivity NOTE: There is a wide variety of methods used. In some homes, T1 lines as part of a LAN are used, in other homes, cable modem or DSL is the method.
X Through T1
X Use T1 for voice and data @ $1500 per month
X Originally T1, recently scrapped for cable modem
X
Remote Access Use internet access X OTHER HARDWARE Printers X
2 per floor X X X
Scanners NOTE: Usually used where EMR has image attachment ability. Only some homes reported using scanners.
X Unexpectedly expensive to get scanners with acceptable speed and quality. Use scanner for scanning old EMRs and hospital discharges
X
Space for servers, information technology personnel NOTE: Homes often convert medical records storage rooms into space.
X
SOFTWARE Software costs vary depending upon the combinations purchased, and costs are often individually negotiated. Companies have various packages of software so that some, such as EMR and decision-support, may be bundled together. Most software purchases include a fee for a certain number of licenses, and a percentage of that fee paid every year. One nursing home entered into an agreement for 10 years of free EMR in return for acting as the beta site for the software and contributing development help.
Purchased an EMR system that was never implemented; partnered with another firm looking to create a nursing home software system (clinical and administrative)
Billing X Payroll X
57
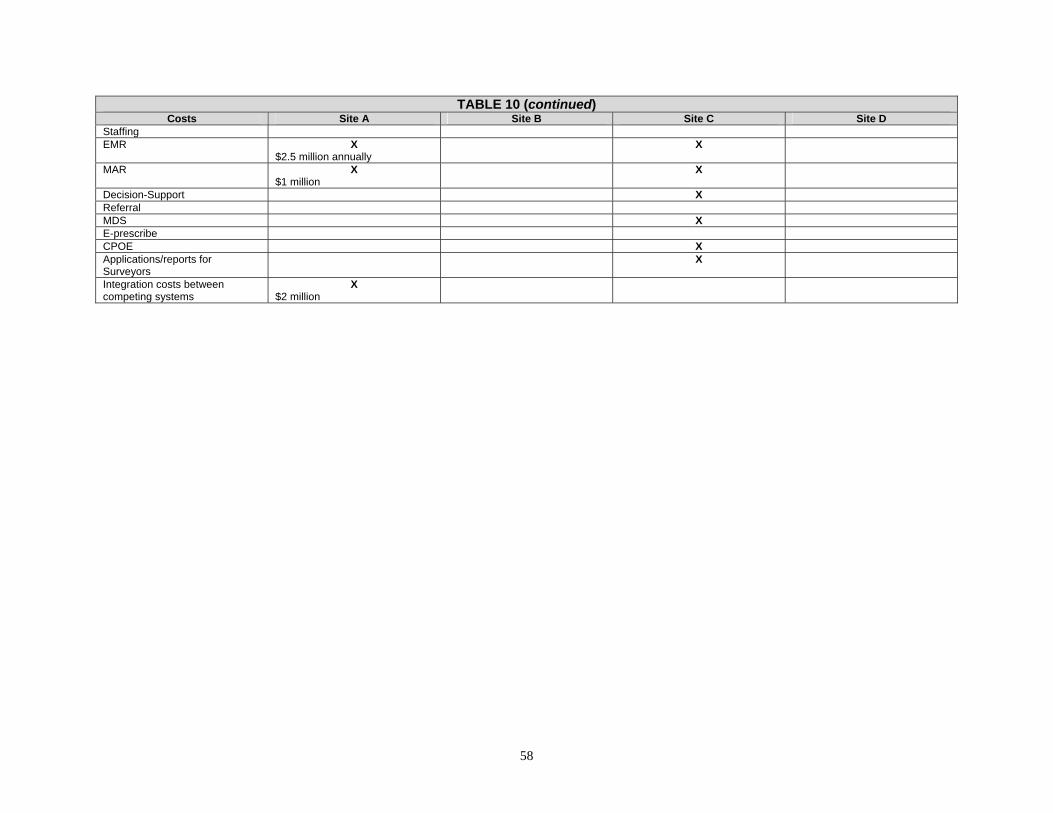
TABLE 10 (continued) Costs Site A Site B Site C Site D
Staffing EMR X
$2.5 million annually X
MAR X $1 million
X
Decision-Support X Referral MDS X E-prescribe CPOE X Applications/reports for Surveyors
X
Integration costs between competing systems
X $2 million
58

TABLE 11: Nursing Homes -- Costs Associated with Labor
Labor costs included the hiring of information systems personnel; clinical labor costs included staff turnover, initial and ongoing training costs, and an increase in the time spent on clinical documentation and resultant short-term loss of productivity.
Costs Site A Site B Site C Site D DIRECT LABOR COSTS Information technology personnel X
Grew from 40 to 125 FTE in past 5 years (313%), most of the increase came from adding clinical software
X One FTE per nursing home
X Added one information technology server specialist, added 1 FTE for report review and development
Workflow management consultants/in-house workflow/report design NOTE: Software firms may provide some level of workflow management assistance as part of their software packages. Others offer it as an additional service or training. Many homes find that having in-house staff that include this as part of their duties results in more useful customized workflow design. Workflow is indicated to be as important as the HIT itself to maximize the benefits of new technology.
X Use in-house clinicians whose time is largely allocated to system and report design
X In-house information technology administrator uses some of her time for this process
X MDS coordinators and nursing staff met to develop assessment and care planning functions
Staff turnover NOTE: All nursing home reported little turnover in response to adding HIT and many noted that it was not necessarily the staff they expected (i.e., older staff) that was most resistant.
Didn’t find any difference in turnover rate
X Less than expected; older nurses responded well to system
Training costs for new staff X Increase from 3.5 to 5 days for new staff; training included teaching basic computer skills
Increased charting time X X More descriptive charting required under new system
PLANNING AND IMPLEMENTATION COSTS Travel for planning and site visits X
To participate in industry events
59

TABLE 11 (continued) Costs Site A Site B Site C Site D
HIT planning NOTE: Unlikely to be tracked rigorously, but planning and oversight of the transition can absorb much of the time of various administrators.
X Indicated that these costs were large
X Likely used significant administrator time but not tracked
X Indicated that these costs were large
Training on new systems NOTE: The level of formal training varied widely. Many nursing homes utilized “super-users,” staff that agree to become more adept in the technology and who act as a first responder to questions from other staff.
X Used overtime, was expensive
X Used overtime during rollout, much smoother when changed EMR system as compared to the first one. For e-MAR, estimated six hour-long sessions per staff
X Had some overtime in lead-up to the roll-over
X
Lost productivity during transition NOTE: Nursing home had various ways to deal with the transition, some experienced added overtime, others utilized nurses from outside agencies to supplement staff.
Didn’t experience X Had some overtime during transition
X
Training for added features X 1 hour in-service for each new feature fielded
60

TABLE 12: Nursing Homes -- Miscellaneous Costs Associated with HIT
Miscellaneous costs include other non-hardware/software and non-labor costs associated with HIT adoption. Costs Site A Site B Site C Site D
STATE SURVEY Surveyor reluctance or frustration X
Had to print out EMR in some locations or for some surveyors; frustration may lead to more deficiencies
Better documentation and access to information can give the appearance of increased negative occurences (falls, etc.)
X Increased deficiencies in some areas
Surveyors not consistent in use of EMR
X
Creating special reports or systems
X
NEW WORKFLOW Admissions director must enter her part of the EMR before anyone else can enter information
X
Incompatible systems NOTE: Many complaints revolve around fields not populating automatically, for example, charting not populating the MDS, which would not occur under a paper system either.
X Need duplicate entry for some things
X May need to exit one system and get into another as opposed to old paper chart with everything in it
OTHER System Downtime X
Maintain paper meds/orders as back-up
X Infrequent and usually less than 1 hour, but med changes and other items cannot be charted and must be passed verbally across shifts
Lack of paper records NOTE: Many staff noted areas where full computerization was not present and they indicated concern with data getting incorrectly entered or lost in these areas
X Specifically, MDs not using the CPOE functions to enter orders or meds
More time in administrative/other monitoring NOTE: This is a result of having more information and reports to use to monitor activities
X New med review system adds to MD time each month
X
61
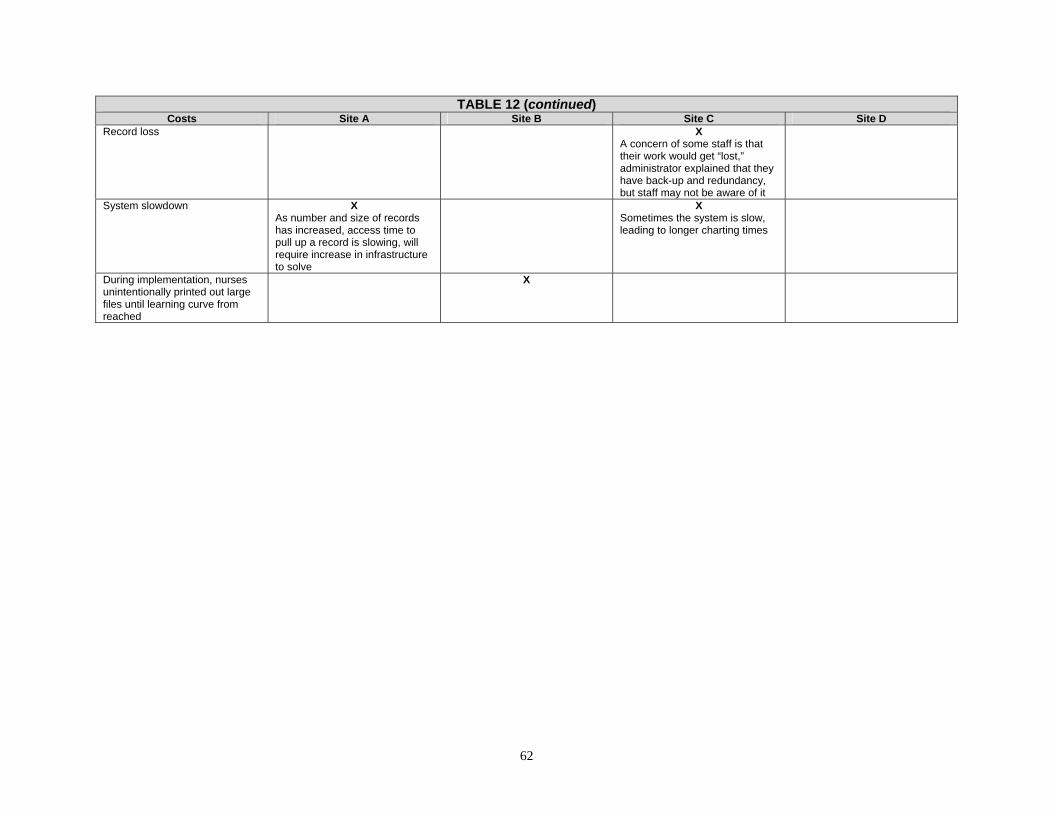
TABLE 12 (continued) Costs Site A Site B Site C Site D
Record loss X A concern of some staff is that their work would get “lost,” administrator explained that they have back-up and redundancy, but staff may not be aware of it
System slowdown X As number and size of records has increased, access time to pull up a record is slowing, will require increase in infrastructure to solve
X Sometimes the system is slow, leading to longer charting times
During implementation, nurses unintentionally printed out large files until learning curve from reached
X
62

TABLE 13: Home Health Agencies -- Benefits Associated with Administrative Functions
Administrative functions include census management, general ledger/accounts payable, verification of insurance and eligibility of services, accounts receivable/billing, track Medicare/non-Medicare claim denials, contracts management, payroll, OASIS data entry/management submission.
Benefits Site A Site B Site C Site D BILLING/REVENUE Optimized cash flow because of increased efficiency getting bills out, faster resident assessment protocols
X Average 5 days from discharge to bill a final
X
Better coding led to decreases in claim denials, flags problems before billing occurs, such as date of service not matching first visit date
X Claim denials decreased dramatically
X X
More accurate coding may increase case mix
X
Can review patient eligibility for Medicare Part A; review requirements for pre-authorization for Medicare HMOs centrally
X
Makes tracking down physician signatures and other pre-authorization requirements easier
X
Can track monthly admissions and HHRGS, etc.
X
No longer need to close each month
X
Can pull notes to check for completeness to bill properly
X
Have been able to handle the increased number of payers and the increased variance in pre-approval requirements, especially patients that switch payers during the course of the home health stay
X
Easier to justify referrals such as wound care with link to EMR
X
System can show clinician what visits have been approved, nurses can get an order for increased visits to be covered if they need it
X
63

TABLE 13 (continued) Benefits Site A Site B Site C Site D
OVERSIGHT Reduced office supply and other costs from an ability to drill-down into individual purchase orders and reduce wasteful ordering
X Allowed identification of wasteful supply practices (e.g., $4 file folders)
X
Facilitated faster and more complete oversight
X Allowed one administrator to manage 14 departments, eliminating 2.5 FTE
X X
Can see current revenue and cost variations rather than have the data buried in quarterly reports NOTE: Allows problems to be addressed more rapidly and appropriately, as well as identifying profitable diagnoses to encourage referrals.
X X
Allowed case managers to respond to insurer queries
X
Timely recertifications related to reports on recerts due
X
STAFFING SCHEDULING Reduced administrative staff for billing/insurance verification, etc.; or allows existing staff to handle growth in admissions or in complexity of billing
X X Able to close 2 branch offices, eliminating 2 FTEs and overhead costs
X
Reduced administrative staff, home health financial administrator added departments, leading to reduction in administrator FTEs
X This was unanticipated
Improved back office efficiency X Reduced FTEs in many areas including business manager and payroll
X Able to manage a large increase in patients (50% since 2002) with no additional back office staff
X Reduced billing staff when billing/EMR was integrated, patient volume nearly doubled without increase in admin staff
X
Easier to predict staffing needs, mileage. There is module that allows us to predict staffing needs if we are increasing the patient census.
X X
64

TABLE 13 (continued) Benefits Site A Site B Site C Site D
Note field allowed agency to make sure they are sending qualified personnel (e.g., patient on IV meds needs a nurse with IV certification)
X
Easier to respond to patient requests for specific nurses/aides/ therapists
X
Information technology scheduling allows agency to avoid overlapped visits (e.g., a nurse and an aide in a home at the same time) that would not be reimbursed
X
Can hire people who live further away from offices since they do not need to come into the office
X
Scheduling module allowed rapid rescheduling when assigned nurses/aides are sick
X X
Google map feature that overlays the visits on a map improved scheduler efficiencies by enabling them to assign patients by geographic area. NOTE: Nurses also can use the feature to manage visit workflow/ better plan out their own day.
X
Fewer missed visits X X Missed visit rate is now under 2%
X Haven’t quantified this yet but believe that the number of missed visits has dropped
Improved regulatory compliance: number of visits match the plan of care
X X
Can schedule a new aide/nurse visit on the same day
X X
PERSONNEL MANAGEMENT Can track personnel licensing requirements, etc., and be more compliant
X
65

TABLE 13 (continued) Benefits Site A Site B Site C Site D
E-learning module can allow clinicians to take on-line required education and will track completion, reduces travel time for staff to come in for in-services and improves manager ability to track
X
NURSE AIDE CHARTING THROUGH TELEPHONE (TELEPHONY) Managers can monitor the time aide spent in home, only pay for actual time, and aides are more accountable. Increased efficiency of payroll and billing due to no lag time for aide documentation. NOTE: one agency did lose some aides who refused to use the new system, but they feel that those were most likely to be aides whose time charting was inaccurate previously.
X Process for payroll and billing dropped from 2-3 days a week to 2-3 hours a week
X
All aide visits charted at the end of the visits, speeding the billing process
X Additionally this allows the aides to be paid weekly, increasing aide satisfaction
X
Can check whether aide is on schedule from a central location and reschedule immediately when a visit is missed
X Site agency is not the agency providing the aides, so monitoring benefits accrue to other agency
Saved costs for travel reimbursement for aides coming into office and copy costs
X
Allowed tracking of Medicaid reimbursement for tasks so that work that Medicaid doesn’t cover isn’t performed
X
If aide is late, can call patient, making the patient feel that their aide is being monitored NOTE: some patients don’t like aide using their phones or feel calls take away from time spent with them.
X
Fewer forms and paper X X No lost charting for billing X X
66

TABLE 13 (continued) Benefits Site A Site B Site C Site D
E-REFERRALS/INTAKE Decreased phone calls and time managing paper
X
Referral information is more accurate and complete using structured electronic format
X
Quicker turnaround from referral to first visit
X
Increased referrals to agency since it is easier for the hospital
X
OTHER Less paper, fewer forms, less referral data
X X X
Reduced office overhead rate X From 50% to 30%
67

TABLE 14: Home Health Agencies -- Benefits Associated with Electronic Health Records
The EHR as defined here consists of electronic demographic information, clinical assessments, care plan and other physician orders, clinical progress notes, and summary reports including discharge summaries.
Benefits Site A Site B Site C Site D MULTIPLE/ANYTIME/ANYWHERE ACCESS Nurses don’t have to come to the office to pick up paper versions of referral information
X This is considered a large benefit
X X X
If home health nurses have access to hospital information, they have a better understanding of patient history, disease progression and trends
X Most likely in an integrated hospital, home health setting
Immediate access to labs and other clinical data
X X
Multiple users can access at once from multiple sites
X X
Nurse manager on call has access to information instead of spending additional time on phone for patient information
X X X
Import features to billing saved time and increased billing accuracy
X X
Enabled rapid response to patient/family questions
X X
Easier handoff of patients with multiple care providers
X X X
Don’t need to pull old records for repeat patients
X X
Don’t need to come to office to pick up charts NOTE: Only a benefit with remote access
X X Closed two out of three branch offices; larger benefit when agency covers a large rural area or area with difficult driving weather
X X
Nurses can document from home X X Access to information reduces duplicate labs, X-rays, etc.
X X
Easier to recognize drug interactions--symptoms that may be tied to drug reactions
X
Can see more patients per day No change in patients per day X Clinical team sees one more patient per day
WOCN can share clinical recommendations more quickly
X
68

TABLE 14 (continued) Benefits Site A Site B Site C Site D
IMPROVED CHARTING Improved charting X
In an integrated hospital and HHA, there may be more information available
X X Forces clinicians to enter certain data
X Structured data entry
Possibly more complete charting since done in the home or shortly thereafter
X X Agency is able to get notes within 24 hours, saving tracking costs
Possibly more accurate charting since done in the home or shortly thereafter
X
REDUCED DUPLICATION OF INFORMATION Fewer quality problems and improved patient safety (e.g., reduced data entry errors, reminds staff to perform certain functions)
X X Data at intake flows to EMR
OASIS charting improved because of automatic skip patterns
X X
Increased staff productivity (e.g., data entry duplication reduced, assessment charting faster)
X
With fewer people handling the 485, it is more accurate; some care plan fields automatically filled in
X
STAFFING Fewer support staff needed to chase paper, make phone calls, fewer visits to agency building to pick up supplies and paperwork, fewer trips to medical records
X
Allowed WOCN to handle more patients
X
Manager can get organized and structured views of tasks and workload status
X
OTHER Reduced paper and copying costs NOTE: Two facilities specifically reported no real reduction in paper costs.
X Decreased paper for referrals
X
Accurate charting led to higher quality outcome data
X X
More information available in electronic chart vs. paper record
X X
Can print off educational material for patients as indicated in system
X
69

TABLE 14 (continued) Benefits Site A Site B Site C Site D
Improved care coordination: easier to have different clinicians providing care to one patient
X
Increased OASIS accuracy and compliance with regulations
X
70
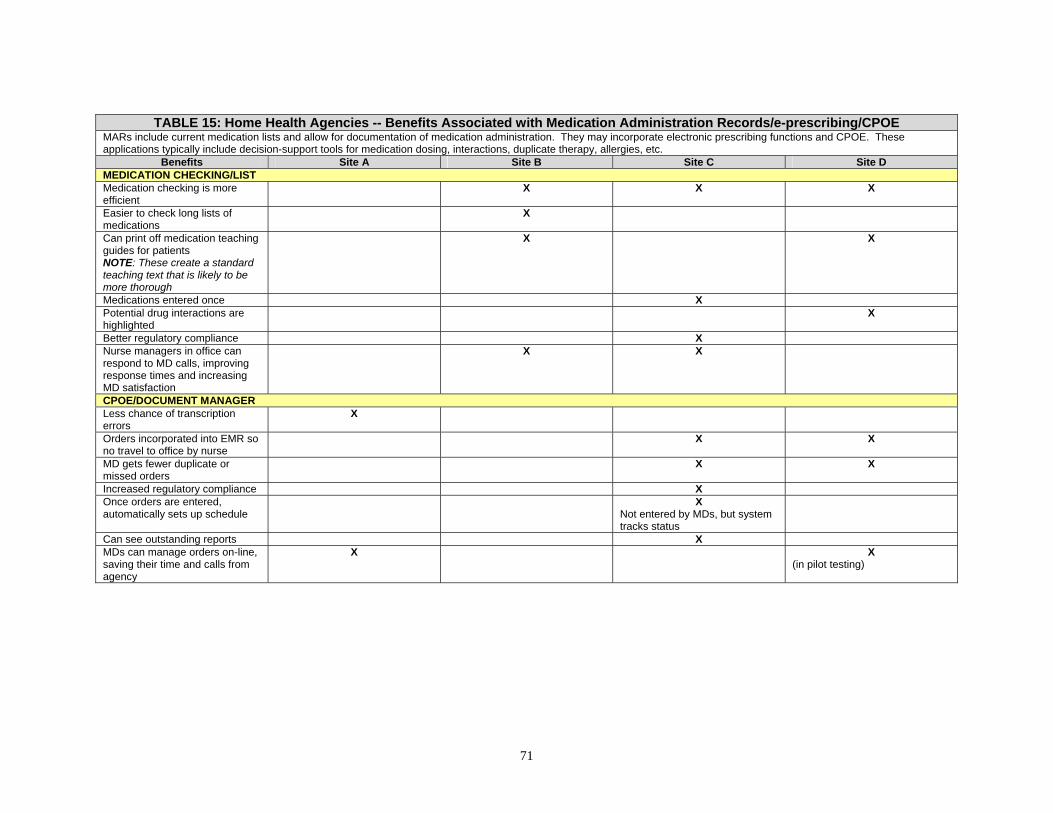
TABLE 15: Home Health Agencies -- Benefits Associated with Medication Administration Records/e-prescribing/CPOE
MARs include current medication lists and allow for documentation of medication administration. They may incorporate electronic prescribing functions and CPOE. These applications typically include decision-support tools for medication dosing, interactions, duplicate therapy, allergies, etc.
Benefits Site A Site B Site C Site D MEDICATION CHECKING/LIST Medication checking is more efficient
X X X
Easier to check long lists of medications
X
Can print off medication teaching guides for patients NOTE: These create a standard teaching text that is likely to be more thorough
X X
Medications entered once X Potential drug interactions are highlighted
X
Better regulatory compliance X Nurse managers in office can respond to MD calls, improving response times and increasing MD satisfaction
X X
CPOE/DOCUMENT MANAGER Less chance of transcription errors
X
Orders incorporated into EMR so no travel to office by nurse
X X
MD gets fewer duplicate or missed orders
X X
Increased regulatory compliance X Once orders are entered, automatically sets up schedule
X Not entered by MDs, but system tracks status
Can see outstanding reports X MDs can manage orders on-line, saving their time and calls from agency
X X (in pilot testing)
71

TABLE 16: Home Health Agencies -- Benefits Associated with Quality Management and Reporting
Quality management and reporting applications extract data from the EHR or other clinical applications (e.g., e-MAR) to generate reports allowing tracking of quality indicators. These may include incident reporting, tracking of adverse outcomes, tracking of infections, calculation of outcomes from MDS data, risk audits for quality areas of concern for surveyors, dashboard reports of key quality indicators, occupancy rates and trends, etc.
Benefits Site A Site B Site C Site D REPORTS Identifies patients for quality indicator studies without quality indicator coordinator manually reviewing records
X X X
Can drill-down to branch or patient or clinician at any time
X
Can assess and standardize health aide hours based on patient’s condition
X X
Reports on labs flagged out-of-range results and identified missing labs
X
SPECIALIZED REPORTS Vendor provides daily e-mail alerts to agency administrator for negative OASIS outcomes
X Allows early identification of problems
X
Flagged problems can be immediately checked for data entry errors
X X
Report on average case mix/RN allowed identification for need to retrain RNs on correct diagnosis coding
X X
Can identify a quality reporting score care and reward clinicians and managers based on outcomes
X
Able to access clinical data to develop predictive models and try new models of care delivery before deciding whether to adopt
X Tried using advanced practice nurse to facilitate care transitions but did not find improved outcomes so didn’t implement fully
DECISION-SUPPORT Clinical pathways increased consistency and continuity of care NOTE: can include a work list that acts as workflow management and increase efficiency
X X Less variation in care and better coordination of care team
X Wound hospitalizations were above national average, now with specialized wound care program, below average
72

TABLE 16 (continued) Benefits Site A Site B Site C Site D
Flags for reminders, such as 28 week antepartum patient with a glucose screen or running reports for labs due, ensured labs are drawn regardless of staffing changes
X X X X
By using canned or self-designed clinical pathways, patients received better care
X X X
Built in falls risk assessment tools allowed better identification of at-risk patients
X
Risk assessments for hospitalizations identified high-risk patients and allows for tailored interventions
X
Trend reporting provided a better basis for clinical decisions
X
Reports for drug interactions that are sent to physician can reduce medication problems
X
OTHER Better regulatory compliance X
Recently had a survey with no deficiencies
73

TABLE 17: Home Health Agencies -- Benefits Associated with Health Information Exchange
HIE is electronic health data shared across organizations. In nursing homes and HHAs, this may include on-line access for referrals, laboratory data, radiology data, patient consults, patient history from other settings, physician and/or pharmacist access to EMR, pharmacy data, HIE with patients/caregivers.
Benefits Site A Site B Site C Site D REDUCED DUPLICATION OF INFORMATION Fewer quality problems and improved patient safety (e.g., reduced data entry errors, reminds staff to perform certain functions)
X X X
Decreased transcription errors X Patients don’t have to answer the same questions asked at hospital or during previous admissions if they are anywhere in the system
X
More timely and complete documentation
X
E-referral allowed hospital EMR information to transfer directly
X
HIE with select hospital emergency departments: During emergency department registration, home care patients are flagged and agency home care coordinator can get involved while patient still in emergency department or shortly after
X Allows home care to coordinate with emergency department, which can reduce wait times, eliminate duplicative testing by providing home care clinical data, potentially eliminate need for hospitalization or reduce hospital lengths of stay by facilitating re-entry into community
SECURE MESSAGING Messaging with MDs increased efficiency for home care clinician and MD and improves quality of care
X X
Saves time, fewer phone calls X X Saves time across workflow-from scheduling to correcting billing errors or omissions to more updated, accurate medical records
Facilitated information hand-offs X X Ability to broadcast messages to specific groups saved time over contacting individuals
X Particularly helpful in a rural area with spotty cell phone reception
X
Can respond to patient issue while in another patient’s home without breaching confidentiality
X
74
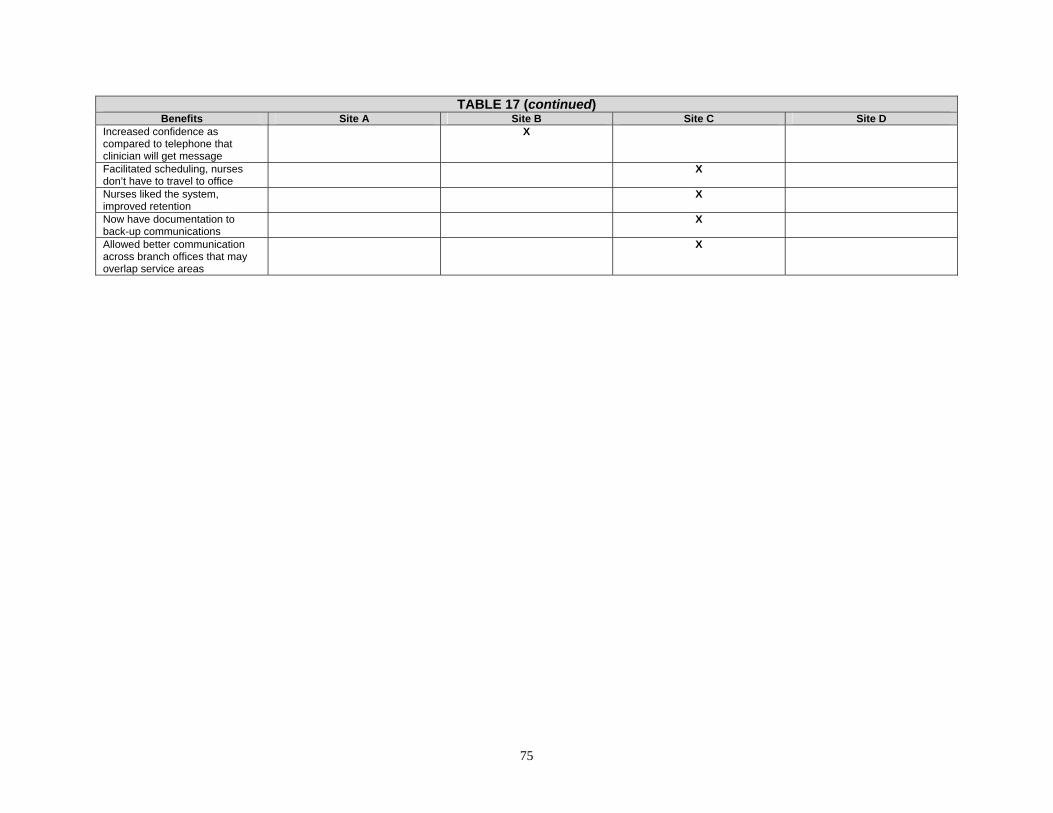
TABLE 17 (continued) Benefits Site A Site B Site C Site D
Increased confidence as compared to telephone that clinician will get message
X
Facilitated scheduling, nurses don’t have to travel to office
X
Nurses liked the system, improved retention
X
Now have documentation to back-up communications
X
Allowed better communication across branch offices that may overlap service areas
X
75
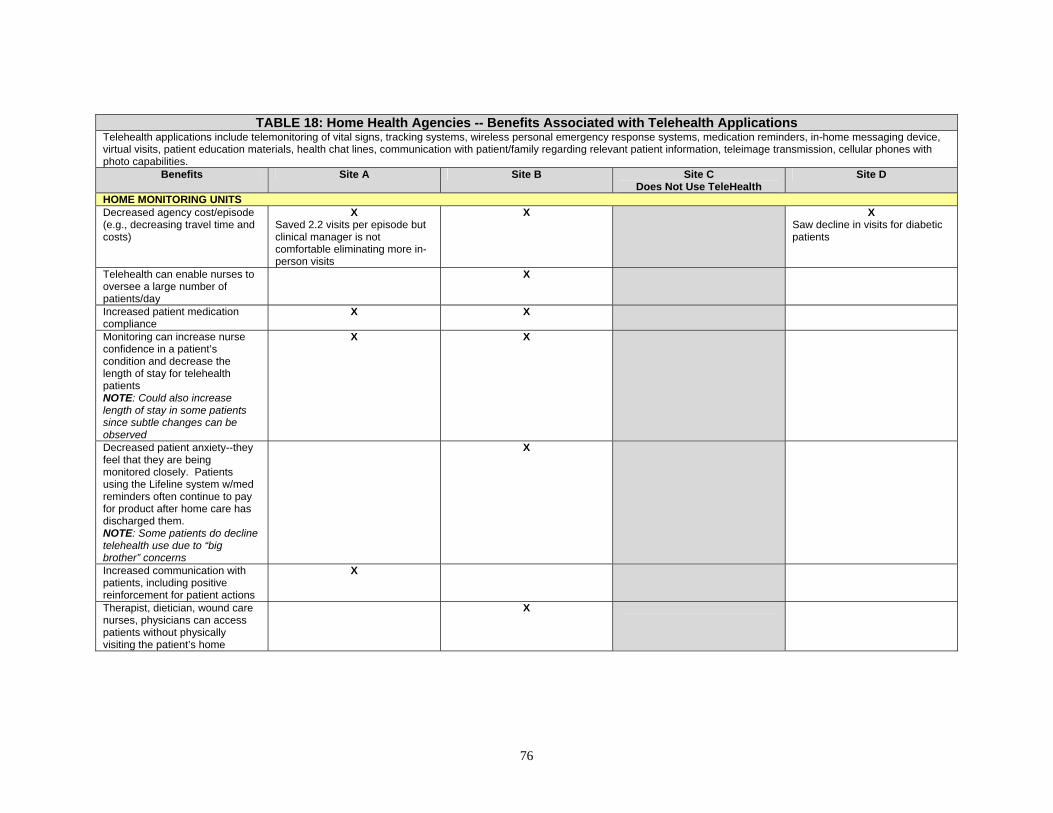
TABLE 18: Home Health Agencies -- Benefits Associated with Telehealth Applications
Telehealth applications include telemonitoring of vital signs, tracking systems, wireless personal emergency response systems, medication reminders, in-home messaging device, virtual visits, patient education materials, health chat lines, communication with patient/family regarding relevant patient information, teleimage transmission, cellular phones with photo capabilities.
Benefits Site A Site B Site C Does Not Use TeleHealth
Site D
HOME MONITORING UNITS Decreased agency cost/episode (e.g., decreasing travel time and costs)
X Saved 2.2 visits per episode but clinical manager is not comfortable eliminating more in-person visits
X X Saw decline in visits for diabetic patients
Telehealth can enable nurses to oversee a large number of patients/day
X
Increased patient medication compliance
X X
Monitoring can increase nurse confidence in a patient’s condition and decrease the length of stay for telehealth patients NOTE: Could also increase length of stay in some patients since subtle changes can be observed
X X
Decreased patient anxiety--they feel that they are being monitored closely. Patients using the Lifeline system w/med reminders often continue to pay for product after home care has discharged them. NOTE: Some patients do decline telehealth use due to “big brother” concerns
X
Increased communication with patients, including positive reinforcement for patient actions
X
Therapist, dietician, wound care nurses, physicians can access patients without physically visiting the patient’s home
X
76

TABLE 18 (continued) Benefits Site A Site B Site C
Does Not Use TeleHealth Site D
Improved staff access to data through a secure web interface (e.g., photos can be reviewed remotely by wound care nurse and physician), saving time, improving quality, increasing staff efficiencies, and reducing costs
X
Better response to changes and faster identification of problems
X X Two COPD patients received pacemakers after the monitoring showed instability
Wound care programs allow a specialized wound care nurse to consult remotely without visiting patients, instead using photos
X X
May decrease emergency room use and re-hospitalization rates
Did not find X Emergency room rate from 13.4/100 to 7.4/100. Hospitalization from 179 /100 to 39.5/100
X Saw decreased hospitalizations in 2 groups: congestive heart failure and hypertension
Can increase the length of time a patient can stay at home vs. being institutionalized
X
Increased referrals due to telehealth presence
X
77

TABLE 19: Home Health Agencies -- Costs Associated with Hardware and Software
Hardware and software costs include purchase, maintenance, and periodic replacement of servers and back-up systems. Other hardware costs included data entry hardware, including desktop and laptop computers, PDAs, and rolling medication carts to support computers.
Costs Site A Site B Site C Site D STORAGE Servers NOTE: Owning and maintaining servers is not necessary under all EMR system types, for example, some web-based systems store all of the data centrally at the software company site. EMR requires the most storage. Also, server costs vary widely depending upon the storage size and speed needed
X EMR is the source of most of the server requirements (use 20 servers)
X 2 servers, $30,000
X 1 web server; 1 Insight server (quality control for providers); 1 e-mail server; 2 application servers; 2 database servers; 1 test environment server; 1 telephony server (really a telephone server).
Database servers are replaced every 4 years and old servers are
then used for other things
X Mainframe, DB2 database, data warehouse, RISC system.
Personal computers, laptops NOTE: Need to expect to replace as necessary
X X 30 laptops at $2000 each
X 54 workstations and laptops
X Workstations and pen-based tablets. Tablets replaced approximately every 3 years
Back-up system NOTE: Nursing homes can choose to use on-site back-up servers/drives or to subcontract back-up services to outside firms
X Use the second server, subcontracted information technology runs system
X Use one drive on a database server and use an off-site back-up system, Off-site is $900/month
X Contract with vendor for disaster recovery services
Telehealth units X Lease; have had problems with 4-5 units not functioning at any given time
X Lease 30 units non-video -- $2800/month; purchase video units -- $8500 per unit
X
Need “clean room” to clean telehealth units
X
OTHER HARDWARE Printers X X X
Printer network has caused the most ongoing difficulty
Scanners NOTE: Usually used where EMR has Image attachment ability. Only some homes reported using scanners.
X
78
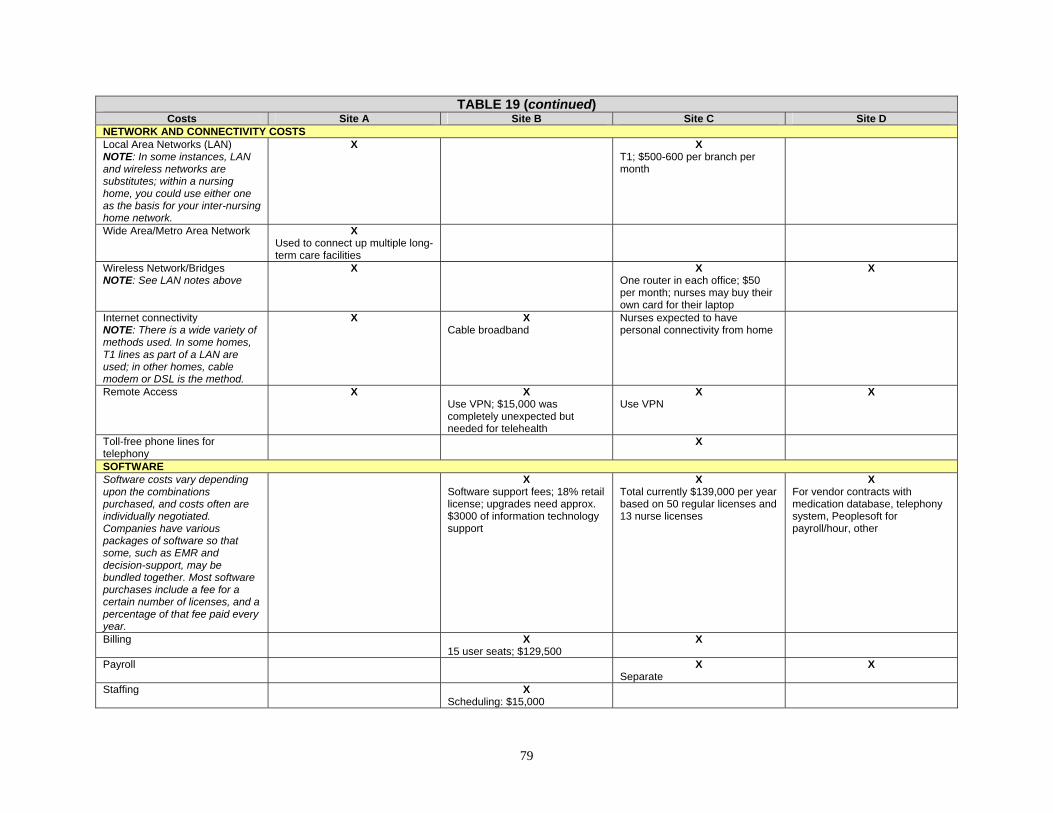
TABLE 19 (continued) Costs Site A Site B Site C Site D
NETWORK AND CONNECTIVITY COSTS Local Area Networks (LAN) NOTE: In some instances, LAN and wireless networks are substitutes; within a nursing home, you could use either one as the basis for your inter-nursing home network.
X X T1; $500-600 per branch per month
Wide Area/Metro Area Network X Used to connect up multiple long-term care facilities
Wireless Network/Bridges NOTE: See LAN notes above
X X One router in each office; $50 per month; nurses may buy their own card for their laptop
X
Internet connectivity NOTE: There is a wide variety of methods used. In some homes, T1 lines as part of a LAN are used; in other homes, cable modem or DSL is the method.
X X Cable broadband
Nurses expected to have personal connectivity from home
Remote Access X X Use VPN; $15,000 was completely unexpected but needed for telehealth
X Use VPN
X
Toll-free phone lines for telephony
X
SOFTWARE Software costs vary depending upon the combinations purchased, and costs often are individually negotiated. Companies have various packages of software so that some, such as EMR and decision-support, may be bundled together. Most software purchases include a fee for a certain number of licenses, and a percentage of that fee paid every year.
X Software support fees; 18% retail license; upgrades need approx. $3000 of information technology support
X Total currently $139,000 per year based on 50 regular licenses and 13 nurse licenses
X For vendor contracts with medication database, telephony system, Peoplesoft for payroll/hour, other
Billing X 15 user seats; $129,500
X
Payroll X Separate
X
Staffing X Scheduling: $15,000
79
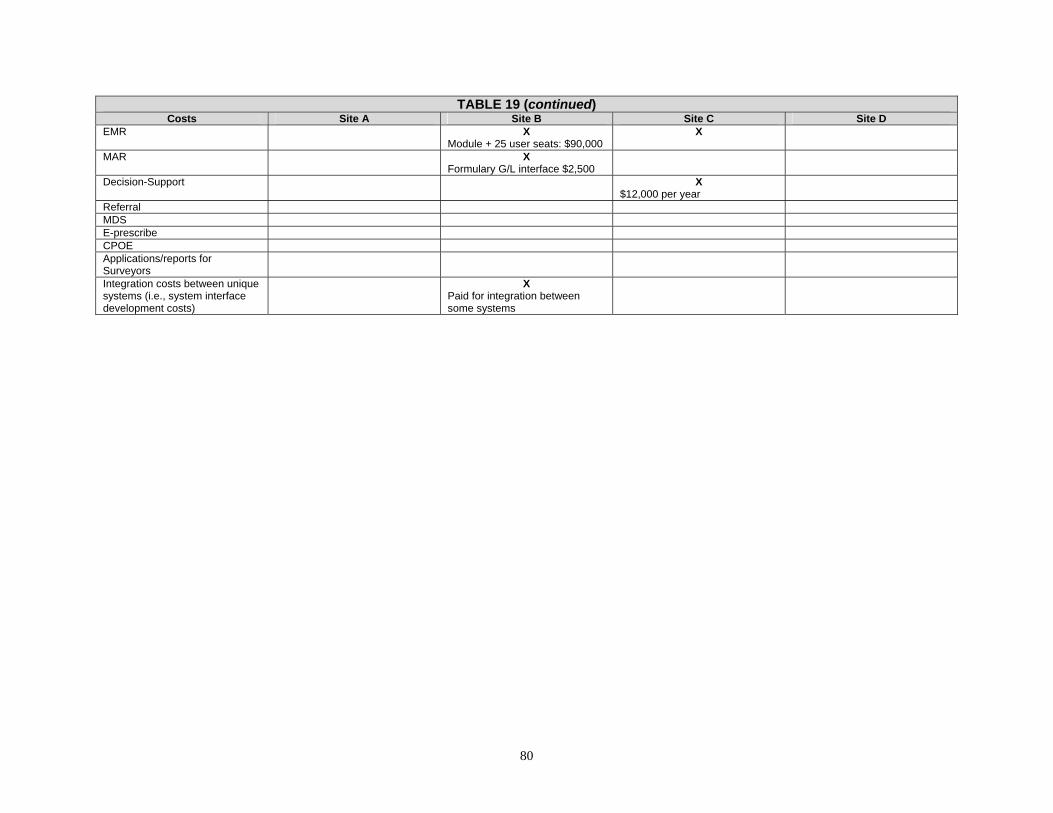
TABLE 19 (continued) Costs Site A Site B Site C Site D
EMR X Module + 25 user seats: $90,000
X
MAR X Formulary G/L interface $2,500
Decision-Support X $12,000 per year
Referral MDS E-prescribe CPOE Applications/reports for Surveyors
Integration costs between unique systems (i.e., system interface development costs)
X Paid for integration between some systems
80

TABLE 20: Home Health Agencies -- Costs Associated with Labor
Labor costs can encompass hiring of information systems personnel; clinical labor costs included staff turnover, initial and ongoing training costs, and an increase in the time spent on clinical documentation and resultant short-term loss of productivity.
Costs Site A Site B Site C Site D DIRECT LABOR COSTS IT personnel X
0.5 FTE for home care, super-users get $1000 per year
X Outsource their information technology department, need someone who can handle hardware and software issues; retainer based on hardware and software setup, $45,000
X Have information technology supervisor who trains staff; acts as a call center for problems; with new software the information technology supervisor can access nurse/staff computers remotely and one support staff; added clerk for telephony
X 172 staff in the information systems department
Workflow management consultants/ in-house workflow/report design NOTE: Software firms may provide some level of workflow management assistance as part of their software packages. Others offer it as an additional service or training. Many agencies find that having in-house staff that include this as part of their duties results in more useful customized workflow design. Workflow is indicated to be as important as the HIT itself to maximize the benefits of new technology.
X Need more workflow changes to use system more efficiently
X Perform a workflow analysis every year to identify additional ways to streamline and added places for automation
X Do in-house now; spent money to send people to a software company session that proved to be not helpful for their own workflow design
Staff turnover NOTE: All HHAs reported little turnover in response to adding HIT and many noted that it was not necessarily the staff they expected (i.e., older staff) that was most resistant.
X 15%
X
Training costs for new staff X 14 hours for each new nurse
X May take slightly longer for orientation
X Less than before
X 25-person department dedicated to training and implementation. Use e-learning system to facilitate training
Increased charting time X Some repetitive charting to complete full visit note for patient with more than one visit/day (IV therapy cases)
81

TABLE 20 (continued) Costs Site A Site B Site C Site D
Adding specialized telehealth nurses, etc.
X 1.25 FTE licensed practical nurse; 1 driver, installer; per patient fee for pharmacy consultant and for MD; 20% of clinical manager time for oversight
X One RN 75-85% FTE, one licensed practical nurse 75% time spent installing units and teaching, returning units
PLANNING AND IMPLEMENTATION COSTS Travel for planning and site visits X
Indicated that these costs were large
X Had site visits to 2 other agencies
HIT planning NOTE: Unlikely to be tracked rigorously, but planning and oversight of the transition can absorb much of the time of various administrators.
X X
Training on new systems NOTE: The level of formal training varied widely. Many HHAs utilized “‘super-users” which are staff that agree to become more adept in the technology and who act as a first responders to questions from other staff.
X X Services from software company: $42,000
X Administrators and information technology staff spent time in each branch during training and roll out
Lost productivity during implementation transition NOTE: HHAs had various ways to deal with the transition, some experienced added overtime, others utilized nurses from outside agencies to supplement staff.
X Quality indicator coordinator is initially less effective, patient loads dropped for a month or two
X Had about 4 weeks of lower productivity
X Learning curve while aides learned to chart with telephony; transition time varied across branches
Lost productivity due to using systems not fully implemented
X Some hospital personnel don’t use the electronic referral system, thus home care coordinators have to manually gather information to complete the referral
Training for added features X 1-2 hours every couple of months
X X Some of this accomplished through development of e-learning modules
82

TABLE 21: Home Health Agencies -- Miscellaneous Costs Associated with HIT Miscellaneous costs include other non-hardware/software and non-labor costs associated with HIT adoption.
Costs Site A Site B Site C Site D STATE SURVEY Surveyor reluctance or frustration X
Surveyors didn’t want to review electronically. This was better with the last survey
NEW WORKFLOW Scheduling module allows more complex scheduling and schedule revision
X More admin time for scheduling offset by time saved by nurses
Incompatible systems NOTE: Many complaints revolve around fields not populating automatically (example: charting not populating the MDS, which would not occur under a paper system either).
X Double entry for some items
X Can’t access some information such as history and physical from hospital that would appear in a paper chart
Review e-mail daily for messages -- nurses, etc.
X
Time reviewing information X 2 separate admin staff noted that most of their time was now used monitoring information and reports from the new information technology
OTHER System Downtime X X X
Issues with system slowdowns during high-use times have been alleviated with new wireless access system. System must be rebooted monthly for medication updates
System crash X e-mail system sometimes crashes and can be difficult to recover
System upgrades X System required periodic updates for new EMR assessment, problem, and intervention fields
Increased paper/printing cost X Now print one page per visit per aide rather than one per week
83
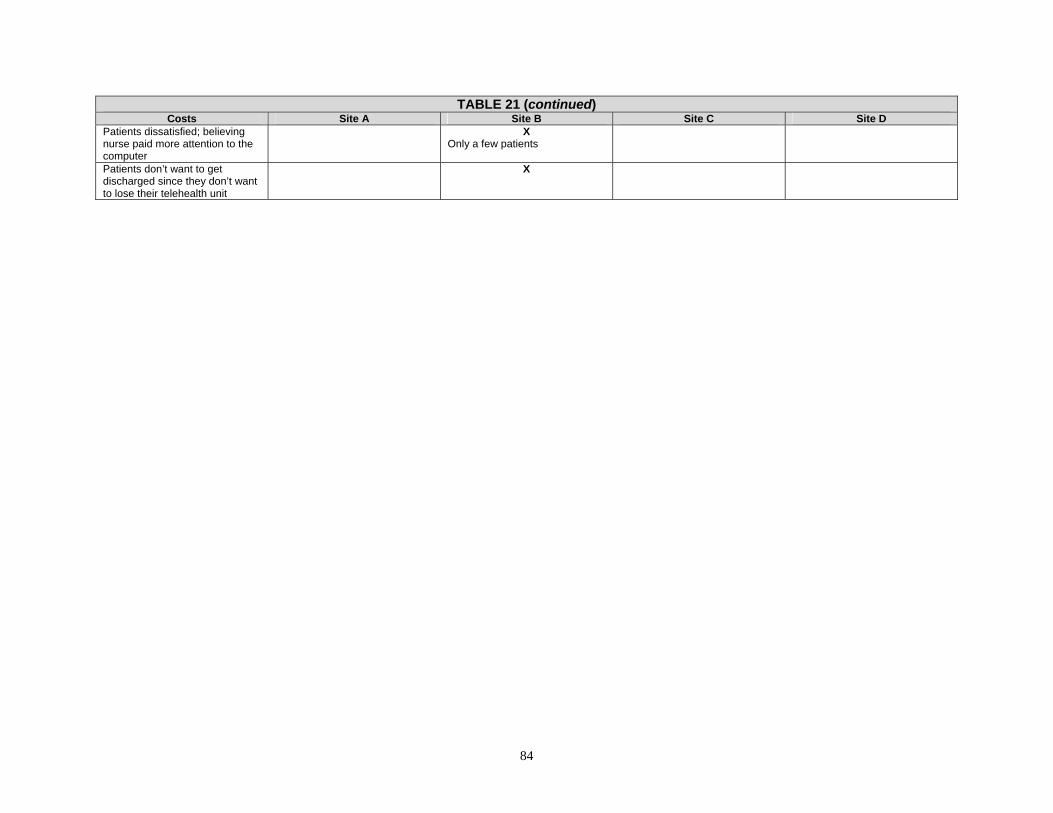
84
TABLE 21 (continued) Costs Site A Site B Site C Site D
Patients dissatisfied; believing nurse paid more attention to the computer
X Only a few patients
Patients don’t want to get discharged since they don’t want to lose their telehealth unit
X

APPENDIX A. PRE-VISIT QUESTIONNAIRE Appendix A contains the following forms used to collect information prior to the
scheduled site visits:
− Nursing Home Component − Home Health Component
A-1
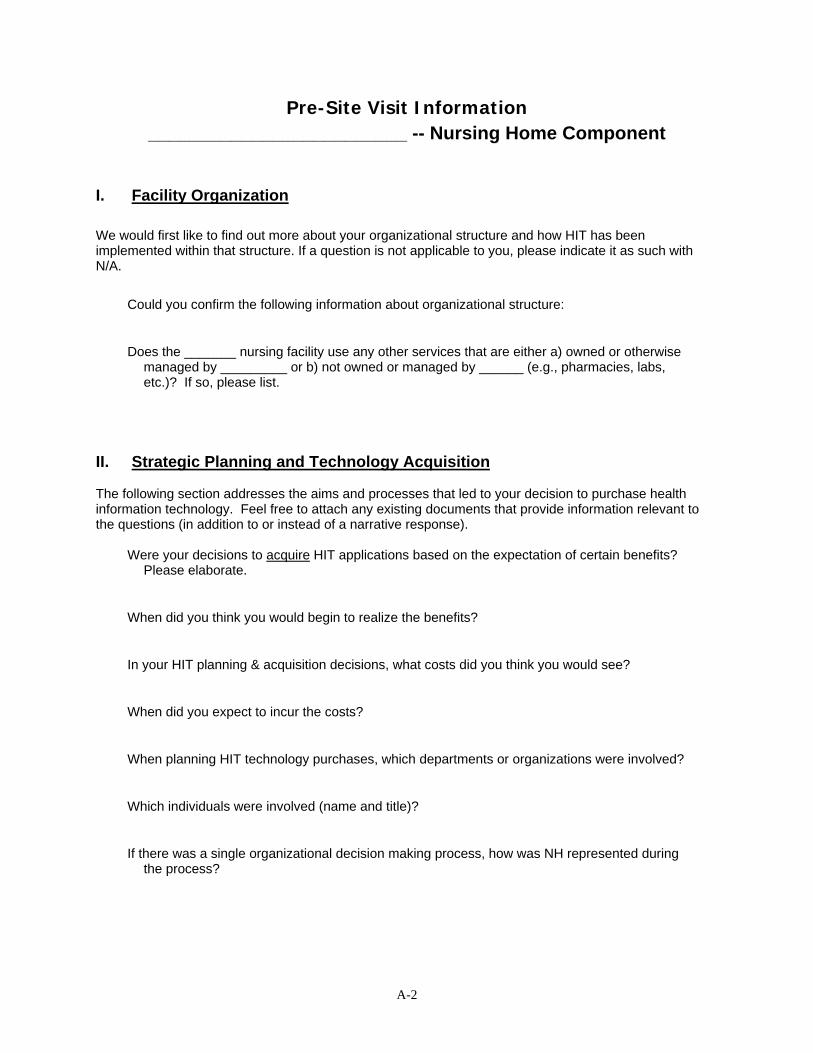
Pre-Site Visit Information _________________________ -- Nursing Home Component
I. Facility Organization We would first like to find out more about your organizational structure and how HIT has been implemented within that structure. If a question is not applicable to you, please indicate it as such with N/A.
Could you confirm the following information about organizational structure:
Does the _______ nursing facility use any other services that are either a) owned or otherwise managed by _________ or b) not owned or managed by ______ (e.g., pharmacies, labs, etc.)? If so, please list.
II. Strategic Planning and Technology Acquisition
The following section addresses the aims and processes that led to your decision to purchase health information technology. Feel free to attach any existing documents that provide information relevant to the questions (in addition to or instead of a narrative response).
Were your decisions to acquire HIT applications based on the expectation of certain benefits?
Please elaborate.
When did you think you would begin to realize the benefits?
In your HIT planning & acquisition decisions, what costs did you think you would see?
When did you expect to incur the costs?
When planning HIT technology purchases, which departments or organizations were involved?
Which individuals were involved (name and title)?
If there was a single organizational decision making process, how was NH represented during the process?
A-2

If there was not a single decision making process, how were HIT investment decisions made for the NH?
Were technology purchases or acquisitions planned and acquired in a sequential manner (e.g., administrative/back office products first, then EMRs, etc.) or was a large purchase made that included many/most of the functionalities you are now using?
If technology purchases were planned sequentially, how and why were the decisions to prioritize applications made?
How did the fact that you are part of a system of care facilities with a continuum of care influence the selection of HIT applications?
Was HIT adoption in the nursing home concurrent with adoption in the other levels of care (e.g., home health)? If so were they the same vendor products? Who determined functional requirements? Please elaborate.
Were you able to take advantage of the size of your health system? For example, did you have negotiating power through purchasing a broader set of applications or through purchasing a larger number of units/modules offered by the vendor?
Was interoperability (i.e., the ability to exchange and reuse data) within the organization an important consideration in your strategic HIT planning and acquisition process? Please explain.
Was interoperability (i.e., the ability to exchange and reuse data) with unaffiliated providers a factor in your strategic HIT planning & acquisition process (i.e., those providers not owned or managed by you)? Please explain.
A-3

TABLE 1. HIT Applications and Purchasing Decisions: Could you indicate whether the following were factors in your decisions not to acquire the HIT applications listed below
(check all that apply)?
HIT Functionality Availability of funding
Lack of inter-
operability
Concern about staff adoption
Unclear financial benefit
Products of interest were unavailable
Other -- Please describe or
note n/a 1) Administrative functions
(e.g., MDS data entry/ management/submission, claims submission, census, Accounts Receivable -- A/R [e.g., claims submission], Accounts Payable -- A/P, general ledger, etc.)
2) Quality Reporting Functions
3) Electronic health information exchange functions
4) Secure electronic messaging
5) Decision Support Tools 6) Medication Administration
Records
7) E-prescribe for medications
8) Computerized Provider Order Entry (CPOE) for other (non-medication) orders
9) Automated Medication Dispensers
10) Telehealth applications
III. HIT Implementation Timeline
Did your facility/agency implement applications in a sequential manner? Please see the list of applications below in Table 2. If so, what were the reasons for phasing in HIT functionality and how did you determine the priority order for implementing HIT applications? When you completed the survey (e.g., the taxonomy of HIT applications), you indicated that your organization has implemented each of the selected HIT applications listed below.
A-4

TABLE 2. Implementation Timeframes:
Please list approximate implementation timeframes (month/year). Also, if applicable, indicate if and when these applications have been upgraded or replaced.
HIT Application Month, Year
(approximate)
Replaced or upgraded
(Y/N)
If replaced or upgraded,
when Priority to Implement
Example: Electronic Billing January, 2000 Y May, 2005 #1 General Ledger/Accounts Payable Verification of Insurance and Eligibility for Services Accounts Receivable/Billing (e.g., claims submission) Tracks Medicare/non-Medicare Claims Denials Resident Trust Fund Management Payroll Registration Acuity Assignment Staffing/scheduling Staff time/attendance tracking Personnel Management Workflow management User-defined financial management reports Dietary Management MDS Data Management Quality Management and Reporting: − Incident Reporting − Tracking of adverse occurrences (e.g., med errors, falls) − Tracking of Infections − Calculation of outcomes from MDS data (e.g.,
ospitalization)
− Risk audits for quality areas of concern for surveyors (e.g. wounds)
− “Dashboard Reports” of key quality indicators (e.g., hospitalizations, infections, and falls)
− Occupancy rates and trends Reporting and Population Health Management Electronic Access to Clinical Guidance Electronic Health Record (EHR)/Electronic Medical Records (EMR) − Maintain patient record, Health Information capture,
management and review
− Comprehensive initial and follow-up assessments and patient originated data
− Summary Reports − Clinical Notes (Physician, RN/LPN, PT, OT, SLT, SW,
Dietician, Aide, Therapy Aide
Receive external clinical documents (laboratory) Problem List Care Planning/Goal Setting: Single Interdisciplinary Plan of Care, Acute Problem Plan of Care Single Plan of Care, Discipline-Specific Plan of Care
Decision Support: − Electronic Clinical Pathways/Standardized Care Plans − Disease Management Programs − Risk assessment tools (e.g., dehydration risk,
contracture risk, falls risk, pressure ulcer risk, etc.)
− Results Management Care Plan Monitoring Trending Secure Electronic Messaging − Intra-facility − Extra-facility (e.g., MD, pharmacy, laboratory) − Health Information Exchange with patients and
caregivers
Patient Education Security/Privacy
A-5
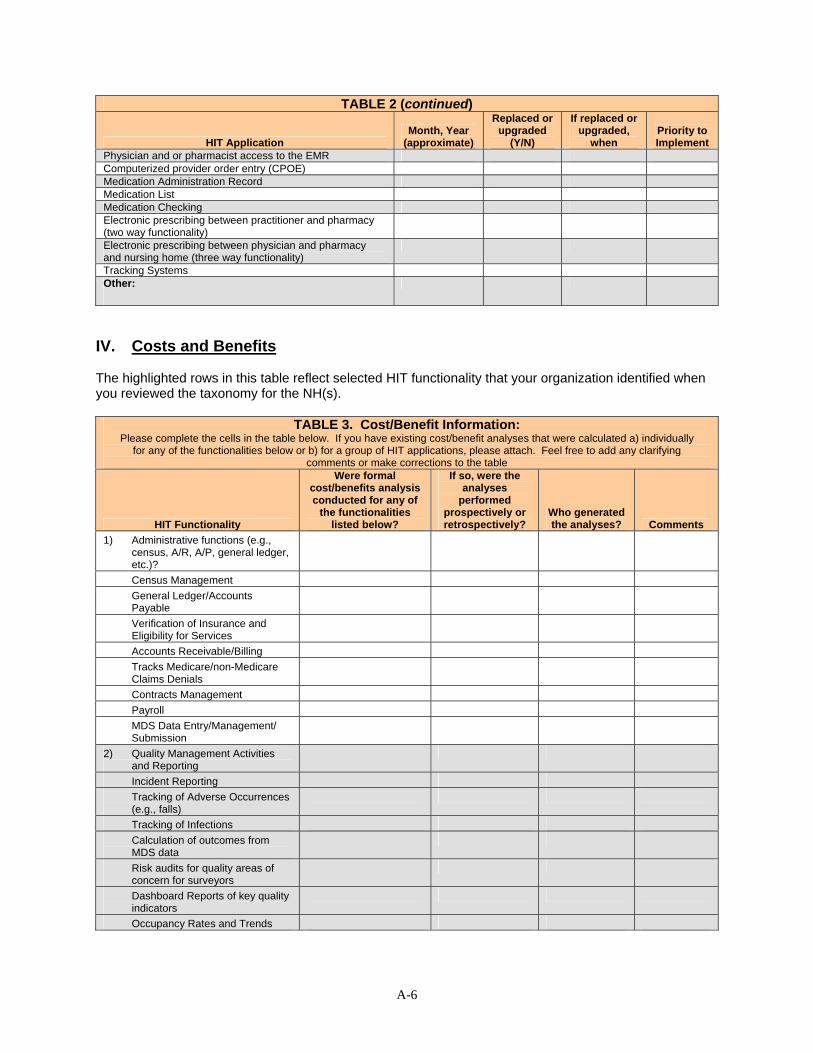
TABLE 2 (continued)
HIT Application Month, Year
(approximate)
Replaced or upgraded
(Y/N)
If replaced or upgraded,
when Priority to Implement
Physician and or pharmacist access to the EMR Computerized provider order entry (CPOE) Medication Administration Record Medication List Medication Checking Electronic prescribing between practitioner and pharmacy (two way functionality)
Electronic prescribing between physician and pharmacy and nursing home (three way functionality)
Tracking Systems Other:
IV. Costs and Benefits
The highlighted rows in this table reflect selected HIT functionality that your organization identified when you reviewed the taxonomy for the NH(s).
TABLE 3. Cost/Benefit Information:
Please complete the cells in the table below. If you have existing cost/benefit analyses that were calculated a) individually for any of the functionalities below or b) for a group of HIT applications, please attach. Feel free to add any clarifying
comments or make corrections to the table
HIT Functionality
Were formal cost/benefits analysis conducted for any of
the functionalities listed below?
If so, were the analyses
performed prospectively or retrospectively?
Who generated the analyses? Comments
1) Administrative functions (e.g., census, A/R, A/P, general ledger, etc.)?
Census Management General Ledger/Accounts Payable
Verification of Insurance and Eligibility for Services
Accounts Receivable/Billing Tracks Medicare/non-Medicare Claims Denials
Contracts Management Payroll MDS Data Entry/Management/ Submission
2) Quality Management Activities and Reporting
Incident Reporting Tracking of Adverse Occurrences (e.g., falls)
Tracking of Infections Calculation of outcomes from MDS data
Risk audits for quality areas of concern for surveyors
Dashboard Reports of key quality indicators
Occupancy Rates and Trends
A-6

TABLE 3 (continued)
HIT Functionality
Were formal cost/benefits analysis conducted for any of
the functionalities listed below?
If so, were the analyses
performed prospectively or retrospectively?
Who generated the analyses? Comments
Other Quality Reports (please describe)
3) Electronic health information exchange functions
On-line Access for Referrals Laboratory data Radiology data Patient Consults Patient History/EHR from other settings
Physician and/or pharmacist access to EHR
Pharmacy data Health information exchange with patients/caregivers
4) Secure electronic messaging Intra-agency Extra-agency (with MD, pharmacy, etc.)
5) Decision Support Tools Electronic Clinical Pathways/ Standardized Care Plans
Disease Management Programs Automated alerts for lab draws Automated prompts for unusual events (e.g., med errors) (bedside med verification)
Automated prompts for preventive practices (e.g., immunizations)
Decision support for e-prescribe for medications prescribing (not for e-prescribe but have other med decision report as part of MAR)
Risk assessment tools Results management Alerts for F-tag (survey) compliance (use Meditech/Crystal Reports to manage compliance with antipsychotics and anti-anxiety drugs)
6) Medication Administration Records (with barcode functionality)
Medication list 7) E-prescribing for medications 8) Computerized Provider Order
Entry (CPOE) for non-medication orders
9) Automated Medication Dispensers
10) Telehealth applications Telemonitoring of vital signs
A-7
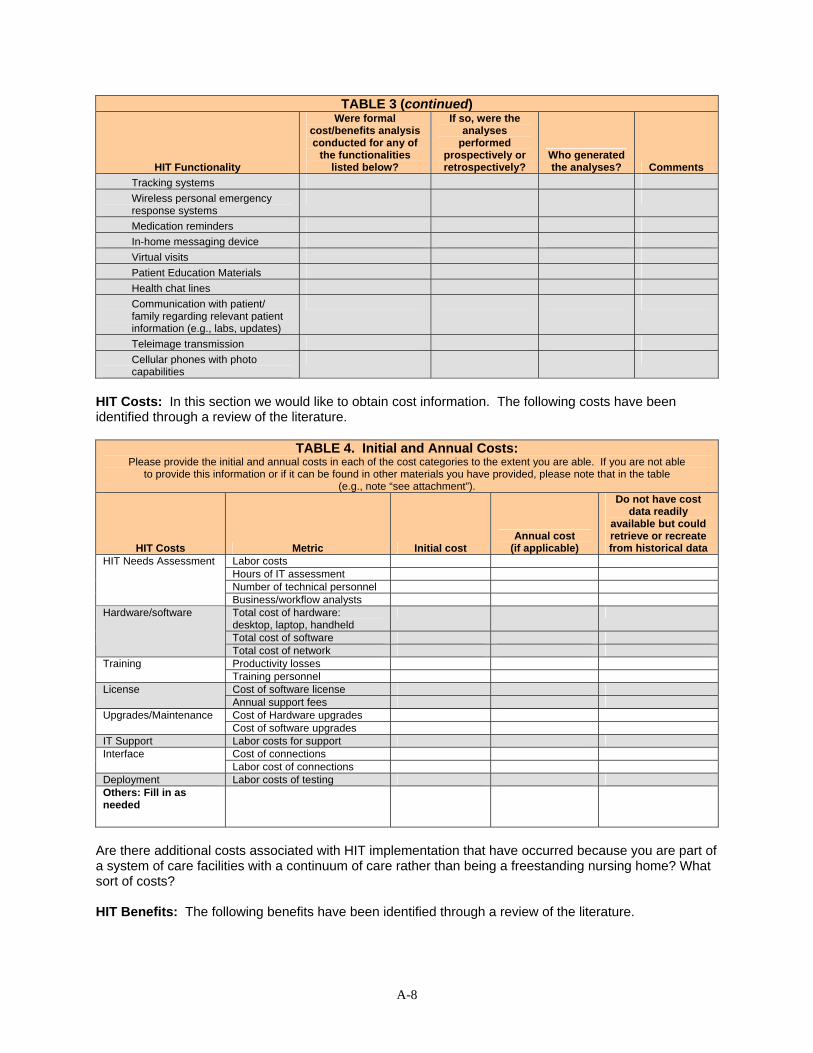
TABLE 3 (continued)
HIT Functionality
Were formal cost/benefits analysis conducted for any of
the functionalities listed below?
If so, were the analyses
performed prospectively or retrospectively?
Who generated the analyses? Comments
Tracking systems Wireless personal emergency response systems
Medication reminders In-home messaging device Virtual visits Patient Education Materials Health chat lines Communication with patient/ family regarding relevant patient information (e.g., labs, updates)
Teleimage transmission Cellular phones with photo capabilities
HIT Costs: In this section we would like to obtain cost information. The following costs have been identified through a review of the literature.
TABLE 4. Initial and Annual Costs:
Please provide the initial and annual costs in each of the cost categories to the extent you are able. If you are not able to provide this information or if it can be found in other materials you have provided, please note that in the table
(e.g., note “see attachment”).
HIT Costs Metric Initial cost Annual cost
(if applicable)
Do not have cost data readily
available but could retrieve or recreate from historical data
Labor costs Hours of IT assessment Number of technical personnel
HIT Needs Assessment
Business/workflow analysts Total cost of hardware: desktop, laptop, handheld
Total cost of software
Hardware/software
Total cost of network Productivity losses Training Training personnel Cost of software license License Annual support fees Cost of Hardware upgrades Upgrades/Maintenance Cost of software upgrades
IT Support Labor costs for support Cost of connections Interface Labor cost of connections
Deployment Labor costs of testing Others: Fill in as needed
Are there additional costs associated with HIT implementation that have occurred because you are part of a system of care facilities with a continuum of care rather than being a freestanding nursing home? What sort of costs?
HIT Benefits: The following benefits have been identified through a review of the literature.
A-8

TABLE 5. HIT Benefits: Please indicate those for which you have collected data, either prospectively, retrospectively, or believe you have the data
to analyze now. If you are not able to provide this information or if it can be found in other materials you have provided, please note that in the table (e.g., note “see attachment”).
HIT Benefits
Financial Data Available from
pre- and post-HIT implementation
Financial Data Available from
pre-HIT implementation
only
Financial Data Available from
post-HIT implementation
only
Do not have financial data
readily available but could retrieve or recreate from historical data
Number of Adverse Drug Events (ADEs)
Number of avoidable hospitalizations/ re-hospitalization
Number of pressure ulcers and related acute care referrals
Number of falls Number of missed therapies Number of infections (e.g., UTI that could be tracked through antibiotic use)
ADL comparisons pre and post (e.g., improvements in functional status)
Avoidance of duplicate testing costs Length of stay/Days of NH care Number of emergency room visits Revenue per patient Patient volume Days billings outstanding (e.g., A/R days >120)
Payor mix Labor Benefits:
Time to admit patient Time to enter clinical documentation per patient
Time to administer medications Others: Fill in as needed
Are there benefits associated with HIT implementation that have occurred because you are part of system of care facilities with a continuum of care rather than being a freestanding nursing home? What sort of benefits?
Were there strategic benefits to HIT implementation that you experienced that are not readily quantifiable, such as a desire to be a leader in the HIT field or the need to compete with other nursing homes in your area?
A-9
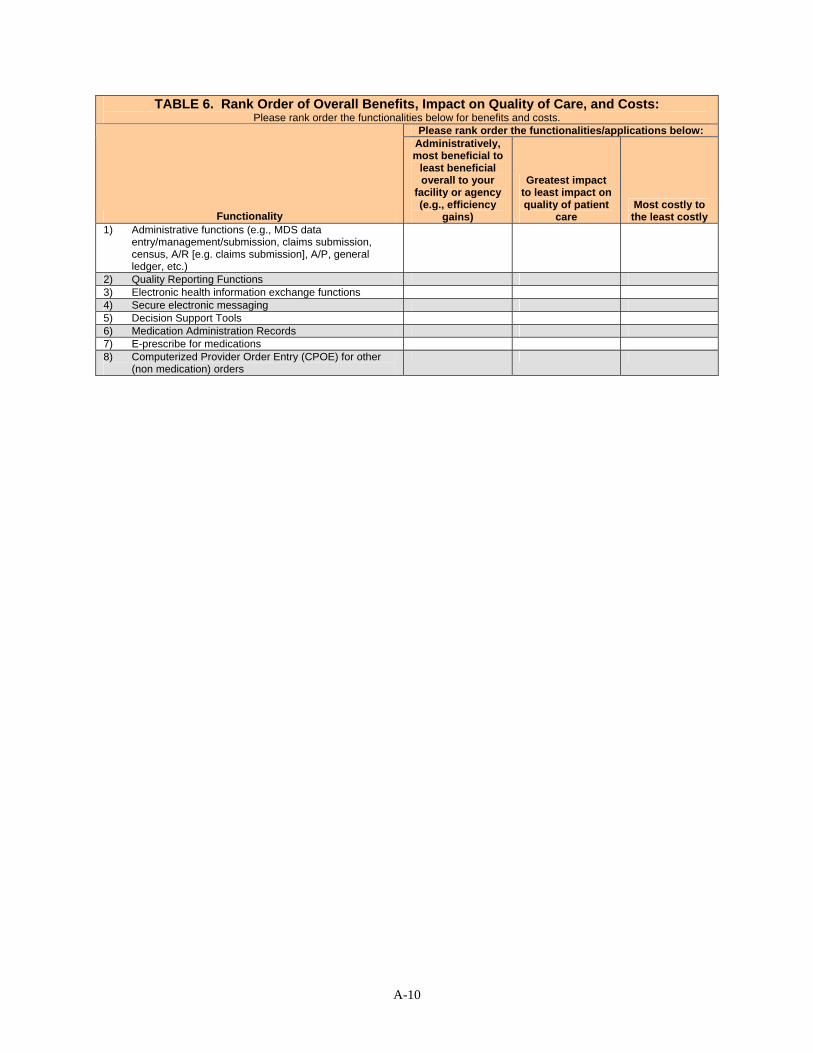
TABLE 6. Rank Order of Overall Benefits, Impact on Quality of Care, and Costs: Please rank order the functionalities below for benefits and costs.
Please rank order the functionalities/applications below:
Functionality
Administratively, most beneficial to
least beneficial overall to your
facility or agency (e.g., efficiency
gains)
Greatest impact to least impact on quality of patient
care Most costly to the least costly
1) Administrative functions (e.g., MDS data entry/management/submission, claims submission, census, A/R [e.g. claims submission], A/P, general ledger, etc.)
2) Quality Reporting Functions 3) Electronic health information exchange functions 4) Secure electronic messaging 5) Decision Support Tools 6) Medication Administration Records 7) E-prescribe for medications 8) Computerized Provider Order Entry (CPOE) for other
(non medication) orders
A-10
Pre-Site Visit Information _________________________ -- Home Health Component
I. Facility Organization We would first like to find out more about your organizational structure and how health information technology (HIT) has been acquired and implemented within that structure. If a question is not applicable to you, please indicate N/A.
Please provide us with additional information about ________________’s organizational structure:
Is _______________ a for-profit or non-profit organization.
Is _______________ a freestanding HHA or part of a larger healthcare system? If part of a larger healthcare system, please describe.
Please provide your annual number of unduplicated admissions.
Please provide your annual number of visits.
Does _______________ use any other services that are either a) owned or otherwise managed by ________; or b) not owned or managed by ____________ (e.g., pharmacies, labs, etc.)? If so, please list.
II. Strategic Planning and Technology Acquisition
The following section addresses the aims and processes that led to your decision to purchase HIT. Feel free to attach any existing documents that provide information relevant to the questions (in addition to or instead of a narrative response).
Were your decisions to acquire HIT applications based on the expectation of certain benefits? Please elaborate.
When did you think you would begin to realize the benefits?
In your HIT planning & acquisition decisions, what costs did you think you would see?
A-11

When did you expect to incur the costs?
When planning HIT technology purchases, which departments or organizations were involved?
Which individuals were involved (name and title)?
Were technology purchases or acquisitions planned and acquired in a sequential manner (e.g., administrative/back office products first, then EMRs, etc.) or was a large purchase made that included many/most of the functionalities you are now using?
If technology purchases were planned sequentially, how and why were the decisions to prioritize applications made?
Was interoperability (i.e., the ability to exchange and reuse data) with affiliated or unaffiliated providers a factor in your strategic HIT planning & acquisition process (i.e., those providers not owned or managed by you)? Please explain.
Hospital-based HHAs or HHAs that are part of a larger health care system please provide information about the system decision processes for acquiring HIT (#1-8 below). If you are a stand-alone HHA, please note N/A and skip to Table 1:
1. If there was a single organizational decision making process, how was the HHA represented during the process?
2. If there was not a single decision making process, how were HIT investment decisions made for the HHA
3. How did the fact that you are part of a larger health care system influence the selection of HIT applications?
4. Was HIT adoption in the HHA concurrent with adoption in other parts of the larger health care system? If so, were they the same vendor products? Who determined functional requirements? Please elaborate.
5. Was HIT adoption in the HHA concurrent with adoption in the hospital? If so, were they the same vendor products? Who determined functional requirements? Please elaborate.
6. Were you able to take advantage of the size of your health system? For example, did you have negotiating power through purchasing a broader set of applications or through purchasing a larger number of units/modules offered by the vendor?
A-12

7. Was interoperability (i.e., the ability to exchange and reuse data) within the organization an important consideration in your strategic HIT planning and acquisition process? Please explain.
8. Was interoperability (i.e., the ability to exchange and reuse data) with unaffiliated providers a factor in your strategic HIT planning & acquisition process (i.e., those providers not owned or managed by you)? Please explain.
TABLE 1. HIT Applications and Purchasing Decisions:
Could you indicate whether the following were factors in your decisions not to acquire any of the HIT applications listed below (check all that apply)?
HIT Functionality Availability of funding
Lack of inter-
operability
Concern about staff adoption
Unclear financial benefit
Products of interest were unavailable
Other -- Please describe or
note n/a 1) Administrative functions
(e.g., OASIS data entry/ management/submission, claims submission, census, Accounts Receivable -- A/R [e.g., claims submission], Accounts Payable -- A/P, general ledger, etc.)
2) Quality Reporting Functions
3) Electronic health information exchange functions (e.g., referral information transfers, labs, radiology data, patient consults, etc)
4) Secure electronic messaging
5) Decision Support Tools 6) Medication Administration
Records
7) E-prescribe for medications
8) Computerized Provider Order Entry (CPOE) for other (non-medication) orders
9) Automated Medication Dispensers
10) Telehealth applications
III. HIT Implementation Timeline
Did your agency implement applications in a sequential manner? Please see the list of applications below in Table 2.
If so, what were the reasons for phasing in HIT functionality and how did you determine the priority order for implementing HIT applications?
When you completed the survey (e.g., the taxonomy of HIT applications, which accompanies this pre-survey tool), you indicated that your organization has implemented each of the selected HIT applications listed below.
A-13

TABLE 2. Implementation Timeframes: Please list approximate implementation timeframes (month/year). Also, if applicable, indicate if and when these
applications have been upgraded or replaced.
HIT Application Month, Year
(approximate)
Replaced or upgraded
(Y/N)
If replaced or upgraded,
when Priority to Implement
Example: Electronic Billing January, 2000 Y May, 2005 #1 Census Management General Ledger/Accounts Payable Verification of Insurance & Eligibility for Services Accounts Receivable/Billing (e.g., claims submission) Tracks Medicare/non-Medicare Claims Denials Contracts management Payroll OASIS data entry/management/submission Quality Reporting: Tracking of infections Quality Reporting: Summary reports of clinical pathways variances
Quality Reporting: Calculation of outcomes from OASIS data (e.g., hospitalization)
Quality Reporting: "Dashboard Reports" of key quality Indicators (e.g., hospitalizations, infections and falls)
Health Information Exchange: Patient Consults Health Information Exchange: Physician and/or pharmacist access to EHR
Secure Electronic Messaging: Intra-agency Decision Support: Electronic Clinical Pathways/Standardized Care Plans
Decision Support: Disease Management Programs Decision Support: Automated prompts for preventive practices (e.g., immunizations).
Decision Support: Decision support for medications.) Decision Support: Risk assessment tools (e.g., dehydration risk, contracture risk, falls risk, pressure ulcer risk, etc.)
Decision Support: Results management Decision Support: OASIS/485 inconsistency alerts. Medication List Computerized provider order entry (CPOE) other non-meds Telemonitoring of vital signs, weights, EKG findings Telehealth: Wireless personal emergency response systems
Telehealth: Medication reminders Telehealth: Patient Education Materials Telehealth: In-home messaging device Teleimage transmission Other:
A-14
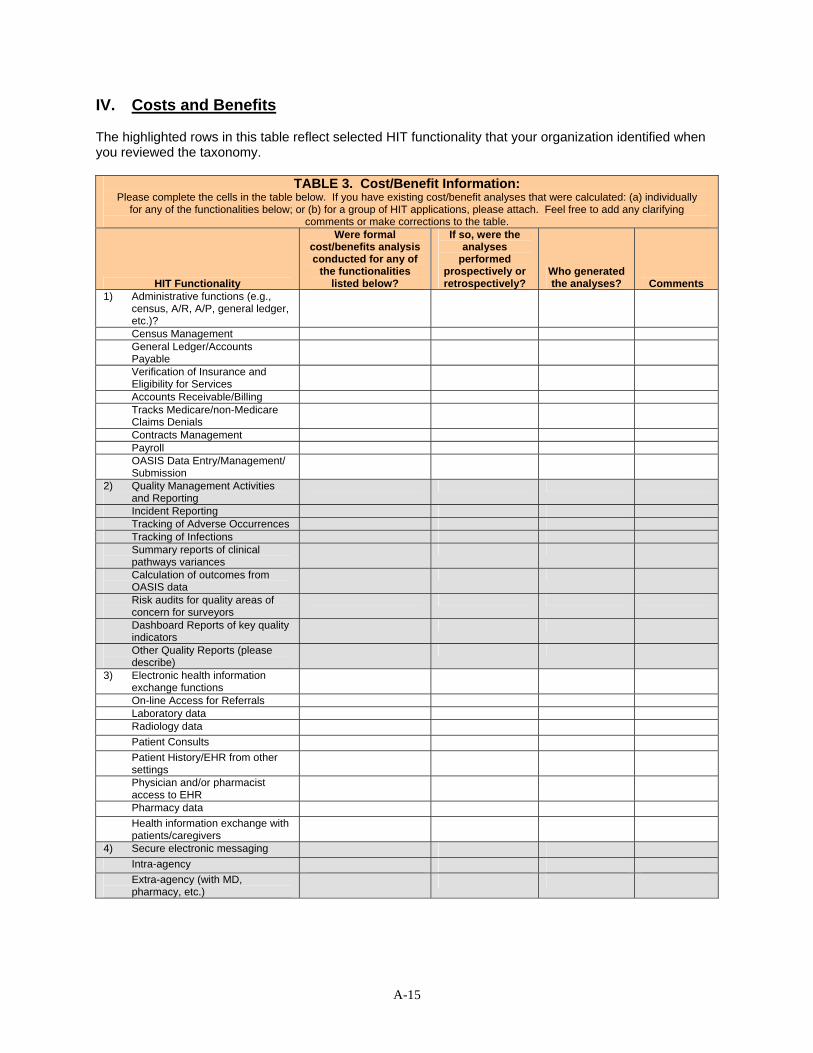
IV. Costs and Benefits
The highlighted rows in this table reflect selected HIT functionality that your organization identified when you reviewed the taxonomy.
TABLE 3. Cost/Benefit Information:
Please complete the cells in the table below. If you have existing cost/benefit analyses that were calculated: (a) individually for any of the functionalities below; or (b) for a group of HIT applications, please attach. Feel free to add any clarifying
comments or make corrections to the table.
HIT Functionality
Were formal cost/benefits analysis conducted for any of
the functionalities listed below?
If so, were the analyses
performed prospectively or retrospectively?
Who generated the analyses? Comments
1) Administrative functions (e.g., census, A/R, A/P, general ledger, etc.)?
Census Management General Ledger/Accounts Payable
Verification of Insurance and Eligibility for Services
Accounts Receivable/Billing Tracks Medicare/non-Medicare Claims Denials
Contracts Management Payroll OASIS Data Entry/Management/ Submission
2) Quality Management Activities and Reporting
Incident Reporting Tracking of Adverse Occurrences Tracking of Infections Summary reports of clinical pathways variances
Calculation of outcomes from OASIS data
Risk audits for quality areas of concern for surveyors
Dashboard Reports of key quality indicators
Other Quality Reports (please describe)
3) Electronic health information exchange functions
On-line Access for Referrals Laboratory data Radiology data Patient Consults Patient History/EHR from other settings
Physician and/or pharmacist access to EHR
Pharmacy data Health information exchange with patients/caregivers
4) Secure electronic messaging Intra-agency Extra-agency (with MD, pharmacy, etc.)
A-15

TABLE 3 (continued)
HIT Functionality
Were formal cost/benefits analysis conducted for any of
the functionalities listed below?
If so, were the analyses
performed prospectively or retrospectively?
Who generated the analyses? Comments
5) Decision Support Tools Electronic Clinical Pathways/ Standardized Care Plans
Disease Management Programs Automated alerts for lab draws Automated prompts for unusual events
Automated prompts for preventive practices (e.g., immunizations)
Decision support for e-prescribe for medications
Risk assessment tools Results management Alerts for g-tag (survey) compliance
OASIS/485 consistency alerts 6) Medication Administration
Records
Medication list 7) E-prescribing for medications 8) Computerized Provider Order
Entry (CPOE) for non-medication orders
9) Automated Medication Dispensers
10) Telehealth applications Telemonitoring of vital signs Tracking systems Wireless personal emergency response systems
Medication reminders In-home messaging device Virtual visits Patient Education Materials Health chat lines Communication with patient/ family regarding relevant patient information (e.g., labs, updates)
Teleimage transmission Cellular phones with photo capabilities
A-16

HIT Costs: In this section we would like to obtain cost information. The following costs have been identified through a review of the literature.
TABLE 4. Initial and Annual Costs:
Please provide the initial and annual costs in each of the cost categories to the extent you are able. If you are not able to provide this information or if it can be found in other materials you have provided, please note that in the table
(e.g., note “see attachment”).
HIT Costs Metric Initial cost Annual cost
(if applicable)
Do not have cost data readily
available but could retrieve or recreate from historical data
Labor costs Hours of IT assessment Number of technical personnel
HIT Needs Assessment
Business/workflow analysts Total cost of hardware: desktop, laptop, handheld
Total cost of software
Hardware/software
Total cost of network Productivity losses Training
Training personnel Cost of software license License
Annual support fees Cost of Hardware upgrades Upgrades/ Maintenance
Cost of software upgrades IT Support Labor costs for support
Cost of connections Interface Labor cost of connections Deployment Labor costs of testing Others: Fill in as needed
If you are part of a health care system, are there additional costs associated with HIT implementation that have occurred because you are part of a healthcare system (hospital, physician clinics, nursing home, and home health agency) rather than being a freestanding home health agency? What sort of costs? (Mark n/a if not part of a health care system.)
If you are part of a health care system, how have HIT/EHR applications that you have implemented in nursing homes and home health agency affected your affiliated assisted living facilities? (Mark n/a is not part of a health care system.)
A-17

HIT Benefits: The following benefits have been identified through a review of the literature.
TABLE 5. HIT Benefits:
Please indicate those for which you have collected data, either prospectively, retrospectively, or believe you have the data to analyze now. If you are not able to provide this information or if it can be found in other materials you have provided,
please note that in the table (e.g., note “see attachment”).
HIT Benefits
Financial Data Available from
pre- and post-HIT implementation
Financial Data Available from
pre-HIT implementation
only
Financial Data Available from
post-HIT implementation
only
Do not have financial data
readily available but could retrieve or recreate from historical data
Number of Adverse Drug Events (ADEs)
Number of avoidable hospitalizations/ re-hospitalization
Number of pressure ulcers and related acute care referrals
Number of falls Number of missed therapies Number of infections (e.g., UTI that could be tracked through antibiotic use)
ADL comparisons pre and post (e.g., improvements in functional status)
Avoidance of duplicate testing costs Length of stay Number of emergency room visits Revenue per patient Patient volume Days billings outstanding (e.g., A/R days > 120)
Payor mix Labor Benefits:
Time to admit patient Time to enter clinical documentation per patient
Time to administer medications Others: Fill in as needed
If your HHA is part of a healthcare system, are there benefits associated with HIT implementation that have occurred because you are part of a healthcare system (hospital, physician clinics, nursing home, and home health agency) rather than being a freestanding home health agency? What sort of benefits? (Mark n/a if not part of a healthcare system.)
Were there strategic benefits to HIT implementation that you experienced that are not readily quantifiable, such as a desire to be a leader in the HIT field or the need to compete with other HHAs in your area?
A-18

TABLE 6. Rank Order of Overall Benefits, Impact on Quality of Care, and Costs: Please rank order the functionalities below for: (a) administrative benefits; (b) quality of care benefits; and (c) costs.
Please rank order the functionalities/applications below:
Functionality
Administratively most beneficial to
least beneficial overall to your
facility or agency (e.g., efficiency
gains)
Greatest impact to least impact on quality of patient
care Most costly to the least costly
1) Administrative functions (e.g., census, A/R, A/P, general ledger, etc.)
2) Quality Reporting Functions 3) Electronic health information exchange functions 4) Secure electronic messaging 5) Decision Support Tools 6) Computerized Provider Order Entry (CPOE) 7) Automated Medication Dispensers 8) Telehealth applications
A-19
A-20
APPENDIX B. SITE VISIT DATA COLLECTION FORMS
Appendix B contains the following forms used for data collection during the
scheduled site visits:
− HIT Benefits Form − HIT Costs/Burden Form − Costs and Benefits Financial Forms

HIT Benefits Application:
Functionality:
Interviewee:
Time/Efficiency Cost Savings/Revenue Increase Quality/Patient Satisfaction 1. What are benefits of
this functionality?
2. To whom do the benefits accrue?
3. Quantify this benefit (large, moderate, minimal) and describe.
4. How would you quantify this benefit (pre and post-HIT)?
Other comments
A-21

HIT Costs/Burden Application:
Functionality:
Interviewee:
Initial Start Up Costs Time/Decreased Efficiency Other 1. What are costs/
burdens of this functionality?
2. To whom do the costs/burdens accrue?
3. Quantify these costs (large, moderate, or minimal) and describe.
4. How would you quantify this cost/ burden (pre and post-HIT)?
Other comments
A-22

Costs/Benefits Financial Forms Name:
Facility:
Position Title/Discipline: 1. COST AND BENEFITS: PLANNING AND IMPLEMENTATION 1.A. Did you complete a Return on Investment (ROI) calculation prior to purchasing any of your HIT applications?
If yes, did you subsequently fill in the actual costs and benefits during and after roll-out? If yes to either, can we see your calculations?
1.B. How did your organization deal with the additional labor required during the implementation process? Did you reduce patient volume? Did you increase/use nurse overtime? Did you have administrative personnel overtime? Did you bring in additional nursing or CNA personnel from temp agencies? Do you have details on the quantity of any of these?
1.C. Did you find benefits from additional administrative oversight, such as refined purchasing or higher occupancy? Please elaborate.
1.D. Did you track the hours devoted to HIT planning/implementation by your clinical and non-clinical staff? If yes, can we see those details?
A-23

2. POTENTIAL FOR FUTURE COST CALCULATIONS
A. Hardware and Software Costs
Cost details How close were your actual
costs to your budgeted costs? What functionalities
contributed most to the cost?
Did you track these costs? How much effort would be needed to
provide these costs? Example: server
Needed one additional server that was not planned for (about 5% over budgeted cost)
EMR 50%
CPOE 25%
Closely tracked hardware, but not network costs. Could be tracked down.
Hardware Costs 1) Servers
2) Client workstations
3) Printers
4) Scanners
5) Backup System
6) Network Backbone
7) Local Area Network (LAN)
8) Metro Area Network
A-24
Did you track these costs? How How close were your actual What functionalities much effort would be needed to
Cost details costs to your budgeted costs? contributed most to the cost? provide these costs? 9) Wide Area Network
10) Wireless Bridges
11) Wireless
12) Internet Connectivity
13) Remote Access Capability
14) Document Management
15) PACs
16) Telehealth Units
Software Costs EMR
CPOE
Administration Applications
Upgrade costs
Staffing Software
A-25

Did you track these costs? How How close were your actual What functionalities much effort would be needed to
Cost details costs to your budgeted costs? contributed most to the cost? provide these costs? Unisource
Coding and Reimbursement
E-Prescribe
Pharmacy Formulary
Other Infrastructure
Space for Servers, IT personnel
Other: Fill in as needed
B. Labor Costs
Cost details How close were your actual
costs to your budgeted costs? What functionalities
contributed most to the cost?
Did you track these costs? How much effort would be needed to
provide these costs? Example: Travel
Needed one additional trip to see EMR at another site (additional $2000)
EMR 50%
CPOE 25%
No we didn’t track specifically
New Personnel Costs Added IS Specialists
A-26

Did you track these costs? How How close were your actual What functionalities much effort would be needed to
Cost details costs to your budgeted costs? contributed most to the cost? provide these costs? Hired workflow management consultants
Staff Turnover due to IT implementation
Planning for HIT costs Travel to view HIT in other LTC/ to meetings
Staff Meetings for HIT planning
Implementation costs Staff meetings during implementation period
Training costs for nurses
Training costs for administrative staff
Training costs for MDs
Lost productivity during implementation
Other Labor Costs: Fill in as needed
A-27

3. POTENTIAL FOR FUTURE BENEFIT CALCULATION
HIT Benefits
HIT that is source of
benefit
How would data exist for Pre-HIT
period?
How would data exist in Post-HIT
period? Effort to calculate Example: Number of Adverse Drug Events
(ADEs)
CPOE In paper charts Tracked in the EMR as a specific tag
Moderate pre-HIT: Need chart review sample. Minimal post-HIT: Data specialist could pull from EMR
Quality of Care Number of Adverse Drug Events (ADEs)
Number of avoidable hospitalizations/ re-hospitalization
Number of pressure ulcers and related acute care referrals
Number of falls
Number of missed therapies
Number of infections (e.g., UTI that could be tracked through antibiotic use)
ADL comparisons pre and post (e.g., improvements in functional status)
Cost of Care Reduction Avoidance of duplicate testing costs
Length of stay/ Days of NH care
A-28

HIT that is How would data How would data
HIT Benefits source of
benefit exist for Pre-HIT exist in Post-HIT
period? period? Effort to calculate Number of emergency room visits
Better purchasing decisions
Reduced administrative positions
Better revenues Revenue per patient
Patient volume
Days billings outstanding (e.g., A/R days > 120)
Payor mix
Labor Benefits Time to admit patient
Time to enter clinical documentation per patient
Time to administer medications
Others: Fill in as needed
A-29

To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human Services Office of Disability, Aging and Long-Term Care Policy Room 424E, H.H. Humphrey Building 200 Independence Avenue, S.W. Washington, D.C. 20201 FAX: 202-401-7733 Email: [email protected]
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]
Assistant Secretary for Planning and Evaluation (ASPE) Home
[http://aspe.hhs.gov]
U.S. Department of Health and Human Services Home [http://www.hhs.gov]