uncommon leg ulcers in the lower extremity
TRANSCRIPT

Uncommon leg ulcers in the lower extremityNicos Labropoulos, PhD, DIC, RVT,a,b Danielle Manalo, MD,a Nima P. Patel, MD,b
Jay Tiongson, MD,a Landon Pryor, MD,a and Athanasios D. Giannoukas, MD,c Maywood, Ill; Newark, NJ;and Larissa, Greece
Objective: To determine the prevalence of uncommon ulcers, unrelated to venous or arterial etiology, in patientspresenting to vascular clinics.Methods: This was a multicenter prospective study of consecutive patients presenting with lower extremity ulceration. Thesettings were university hospital outpatient centers and venous clinics. A total of 799 limbs in 710 patients with leg ulcerswere evaluated. Patients with venous ulcer disease and with evidence of arterial disease with an ankle-brachial index lessthan 0.7 were excluded from the study. Out of 710 patients, 17 patients with a total of 21 limbs fit the criteria forinclusion. All limbs included in this study underwent physical examination, ankle-brachial index measurements, duplexultrasonography, and skin biopsies.Results: The mean age of patients with uncommon ulcers was 65.6 years, and the mean duration was 5.5 years. A total of2.1% of all leg ulcers seen were due to uncommon etiology unrelated to venous or arterial pathology. Most of these ulcerswere located in the medial lower calf (n � 19). In six patients with ulcers, the histology did not reveal any specific cause;five had a neoplasia, three had chronic inflammation, two had sickle cell disease, two had vasculitis, one had rheumatoidarthritis, one had pyoderma gangrenosum, and one had ulcer due to hydroxyurea.Conclusions: The prevalence of leg ulcers unrelated to arterial and venous disease that presented with signs and symptomsof chronic venous disease was 2.1%. Their etiology is variable, most often including vasculitis, neoplasia, metabolicdisorders, infection, and other rare causes. Early identification of uncommon ulcers may facilitate timely and appropriate
management. (J Vasc Surg 2007;45:568-73.)Chronic leg ulceration is a common condition withlimited epidemiologic data. Some studies report prevalencerates between 0.18% and 2% of the European population1,2
and up to 5% of the population over 65 years of age.1 Theoverwhelming majority of leg ulcers are of venous origin,cited in the literature from anywhere between 45% and 90%of all leg ulcers.1,2 The second most common cause of legulcers is arterial occlusive disease, followed by neuropathiculcers. Interpretation of these data has been complicated bythe recent shift toward arterial and mixed ulcers, likelybecause of the aging population and improved detection ofarterial disease.1 The high prevalence of risk factors foratherosclerotic occlusion, especially in Western popula-tions, also contributes to the increasing incidence of ulcer-ation.2 Proper identification of the etiology of leg ulcers isimperative for appropriate management, because incorrecttreatment may cause significant harm.2
Venous ulcers are classically located in the gaiter areawith the appearance of an irregular border, fibrinous debris,extensive granulations, and weeping; the surrounding skinmay demonstrate edema, hemosiderin pigmentation, hy-
From the Department of Surgery, Loyola University Medical Center, May-wood,a the Department of Surgery, University of Medicine and Dentistryof New Jersey, Newark,b and the Department of Surgery, University ofThessaly, Larissa.c
Competition of interest: none.Additional material for this article may be found online at www.jvascsurg.org.Reprint requests: Nicos Labropoulos, PhD, Department of Surgery, Vascu-
lar Laboratory, University of Medicine and Dentistry of New Jersey, 150Bergen St, Room D-447, Newark, NJ 07101-1709 (e-mail: [email protected]).
0741-5214/$32.00Copyright © 2007 by The Society for Vascular Surgery.
doi:10.1016/j.jvs.2006.11.012568
perkeratosis, atrophie blanche, or cellulitis.1,2 Some ulcersthat appear to be venous are of other etiologies. Carcino-matous growth can be masked as a deteriorating leg ulcer.3
Case reports have described livedoid vasculitis or calciphy-laxis in patients who were otherwise expected to havevenous ulcers.4,5 However, information on ulcers withuncommon etiologies is lacking. Therefore, this study wasperformed to determine the prevalence of these ulcers inpatients presenting to a vascular clinic.
METHODS
A total of 710 patients and 799 limbs with leg ulcersfrom various centers were evaluated. Patients with legulcers of nonvenous etiology and nonarterial ischemic dis-ease were included in the study. They were selected fromconsecutive patients with leg ulcers (class 6 according to theCEAP classification6) attending a venous clinic. The ulcerswere associated with signs and symptoms of chronic venousdisease. These included pain, swelling, burning sensation,itching, heaviness, restless limb, skin discoloration, andlipodermatosclerosis. They were located on the medialmalleolus, lateral malleolus, or calf. Patients with foot ul-cers were not included in the study. Appreciable arterialdisease that may have contributed to the ulcer formationwas eliminated by including only those patients with anankle-brachial index of greater than 0.7. These patientswere also excluded from the multicenter study and there-fore were not available for this study. Patients with footulcers were unlikely to have venous disease and were ex-cluded as well.
Duplex ultrasonography was used to investigate the veinsin the lower extremity from groin to ankle. The femoropop-
liteal veins; deep calf veins; great saphenous veins, small saphe-
dial; n
JOURNAL OF VASCULAR SURGERYVolume 45, Number 3 Labropoulos et al 569
nous veins, and their tributaries; nonsaphenous veins; andperforating veins were evaluated in all limbs. Reflux was con-sidered to be present when the retrograde flow lasted longerthan 1 second in the femoropopliteal veins and more than0.5 seconds in the superficial and deep calf veins. Evidenceof thrombosis was documented by the noncompressibilityof the vein, visualization of the thrombus, filling defects oncolor mode, intraluminal webs, recanalized intraluminalchannels, and wall thickening. Limbs with reflux or ob-struction were excluded.
The physical examination, the ankle-brachial index,and the ultrasound investigation were performed by spe-cialists in vascular medicine or vascular surgery. The partic-ipating centers had at least 3 years of experience in exam-ining patients with chronic venous disease. All limbs thatwere included in this study underwent skin biopsies. A3-mm punch biopsy or incisional biopsy provides a full-thickness tissue sample with minimal scarring.7 The datawere inserted in a customized Microsoft Access database(Microsoft Corp, Redmond, Wash).
RESULTS
Out of 799 patients with leg ulcers, 17 patients with 21ulcerated limbs were included in the study (Table I). Fourpatients had bilateral ulcers. The mean age was 65.6 years(SD, 15.2 years), and the mean duration of the ulcers was5.5 years. The location of the ulcers was predominately onthe medial aspect of the lower calf (n � 19): one waslocated in the anterolateral and one in the posterior aspectof the calf. Three patients demonstrated venous reflux byduplex ultrasonography. Two of them underwent strippingof the great saphenous vein and stab avulsions of thevaricosities. The third patient had injection sclerotherapy of
Table I. Characteristics of the ulcers found on 21 patients
Sex Age (y) Limb Location on calf Duration (y)
M 63 L u-l/med 3R u-l/med 3
F 72 L l/med 5R l/med 5
F 52 L m-l/med 4M 73 R l/med 8M 54 R l/ant-lt 2M 68 L m/post 1M 79 L l/med 16F 76 R l/med 18F 73 R l/med 15F 64 L m-l/med 3
R m-l/med 3M 71 L l/med 4F 82 R m-l/med 7F 73 R l/med 14M 78 L m/med 2
59 L l/med 0.17M 17 R l/med 0.33M L l/med 0.25F 62 R l/med 0.75
ABI, Ankle-brachial index; u, upper calf; m, mid calf; l, lower calf; med, me
a calf tributary. The deep veins were normal in all three
patients, and no other venous abnormality was found.Despite of the successful treatment for the reflux, the ulcersstill persisted. The third patient had also an ankle-brachialindex of 0.7, which decreased to 0.58 after exercise. He hada significant stenosis in the superficial femoral and poplitealarteries. Both lesions were successfully treated with percu-taneous transluminal angioplasty, and the ankle-brachialindex increased to 0.92. The ulcer was reduced in size afterthe arterial and venous treatment but never healed. None ofthe patients had trauma, deep venous thrombosis, superfi-cial venous thrombosis, congestive heart failure, chronicrenal failure, hepatic failure, diabetes mellitus, or depen-dency.
The size of the ulcer varied. The largest diameterranged from 2 to 14 cm. The ulcers had characteristics of achronic wound. Most of them were highly inflamed andhad necrotic tissue and hyperproliferation in the sur-rounding skin. On closer inspection, there were differentcharacteristics in many ulcers, but this information wasnot systemically collected. When the patients were foundnot to have arterial or venous disease, they were sent to adermatologist and had a skin biopsy.
Three patients were being treated with antibiotics forcellulitis with concurrent lymphedema. Two other pa-tients were also being treated with antibiotics. These twopatients were given antibiotics by their referring physi-cians but were not shown to have an infection. Obesitywas not an exclusion factor, and two of our patients withundetermined pathology were obese, with a body massindex of 34 and 39 kg/m2.
Pathology was identified in 15 limbs of 13 patients(Table II). Two patients had no histologic analysis becausethe biopsy specimens were lost in the pathology depart-
Duplex ABI Medication Pathology
nl abx Undeterminednl abx Undeterminednl Vasculitisnl Vasculitisnl abx Chronic inflammationnl abx Chronic inflammationnl abx Chronic inflammationnl Kaposi sarcomanl Carcinoma
ous reflux nl Squamous cell carcinomaous reflux nl Squamous cell carcinoma
nl Undeterminednl Undeterminednl No histologynl abx No histologynl Basal cell carcinomanl Pyoderma gangrenosumnl Hydroxyureanl Sickle cellnl Sickle cell
d reflux 0.7 Rheumatoid arthritis
l, normal; abx, antibiotics; post, posterior; ant-lt, anterior lateral.
nlnlnlnlnlnlnlnl
VenVennlnlnlnlnlnlnlnlnlMil
ment and the patients refused to have another biopsy

JOURNAL OF VASCULAR SURGERYMarch 2007570 Labropoulos et al
performed. Two of the four patients with bilateral ulcershad undetermined pathology despite histologic study. Twopatients with venous reflux had a histologic diagnosis ofsquamous cell carcinoma (SCC). One patient each hadulcer pathology that revealed Kaposi sarcoma, carcinoma,basal cell carcinoma (BCC), pyoderma gangrenosum, andhydroxyurea. The patient with the Kaposi sarcoma wasimmunosuppressed. Histologic diagnoses were obtained intwo patients with bilateral ulcers. One patient had nonspe-cific vasculitis; the other had pathology that confirmedsickle cell anemia.
One patient with a combination of mild reflux and anankle brachial index of 0.7 had an ulcer etiology of rheu-matoid arthritis. Three patients with cellulitis receivingantibiotic therapy had pathology consistent with chronicinflammation.
DISCUSSION
The differential diagnosis for leg ulcers is extensive.Fortunately, most of the conditions are rare and exist inthe literature as small case series or case reports. Themost common etiologies of leg ulcers can be groupedinto venous, arterial, or neuropathic ulcers. In our study,uncommon leg ulcers accounted for 2.1% of all legulcers. Appendix II (online only) includes the results froma literature search for case reports of uncommon leg ulcersin adults. Clearly, our study has underestimated the preva-lence of uncommon leg ulcers because many of thosepatients do not go to vascular clinics. This was also becausein this study, only ulcers that had a venous appearance andlocation were included. Furthermore, the rest of the pa-tients who had venous etiology and arterial disease did nothave a biopsy performed. Therefore, other patients fromthe same pool were missed.
One patient in our study had pyoderma gangrenosumlocated on the medial aspect of the mid calf. It is anuncommon but impressive ulcer of unknown etiology. Fifty
Table II. Pathology results
Pathology Limbs No. Patients
Undetermined 5 3No histology available* 1 1Chronic inflammation 3 3SCC 2 2Kaposi sarcoma 1 1Carcinoma 1 1BCC 1 1Sickle cell anemia 2 1Vasculitis 2 1Pyoderma gangrenosum 1 1Hydroxyurea 1 1RA 1 1Total 21 16% of uncommon ulcers out of
total leg ulcers 1.3% 2.1%
SCC, Squamous cell carcinoma; BCC, basal cell carcinoma.*The histology specimen was lost, and the biopsy was not repeated.
percent of cases are associated with chronic disease, and the
other 50% are considered idiopathic.8 Lesions are mostcommonly found on the lower legs, but they may occuranywhere on the skin.9 Usually they begin as painful pus-tules, with rapid development of necrosis and ulceration.Fully established lesions show single or multiple ulcers withwell-defined, raised, purple, serpiginous, and underminedborders.7 There are also several variants, and this can makethe diagnosis difficult. Investigations including skin biopsyshould be undertaken to rule out other etiologies.7 Theinitial goals of treatment are to address any underlyingdisorders and provide adequate wound care. Systemic treat-ment with corticosteroids followed by cyclosporine orother immunomodulatory agents has been successful intreating pyoderma gangrenosum.2
Leg ulcers are a common complication in patients withhomozygous sickle cell disease and those with associated�-thalassemia, with prevalence rates from 8% to 10% ofpatients aged 10 to 50 years.10 Contributing factors toulcer formation include vessel obstruction by sickled cells,increased venous and capillary pressure, secondary bacterialinfection, and decreased oxygen-carrying capacity of theblood.9 The medial malleoli are the most common site ofleg ulceration in sickle cell disease and in other chronichemolytic anemias, suggesting perhaps that stasis may playa role in leg ulceration associated with chronic hemolyticanemia. These ulcers are often bilateral, persistent, andrecurrent. This was illustrated in the patient in our studywith bilateral ulcers on the medial aspect of the lowercalves. Depending on the extent of the lesions, treatmentmodalities may include bed rest, debridement, wet-to-drysaline dressings, blood transfusions, and topical antibiot-ics.11 Skin grafts and myocutaneous flaps may be requiredfor extensive ulcers.
Rheumatoid arthritis and Felty syndrome are com-monly associated with leg ulcers. Studies report that 9% to10% of patients with rheumatoid arthritis12,13 and approx-imately 25% of patients with Felty syndrome have legulcers. The etiologies of these ulcers are frequently multi-factorial. Concurrent venous or arterial disease is oftencontributory, as seen in our study with one patient who hadrheumatoid arthritis with concurrent mild venous refluxand an ankle-brachial index of 0.7. Other causes includevasculitis, diabetes, deformities, trauma, or pressure fromill-fitting shoes.2 Occasionally the cause is uncertain. Oienet al12 reviewed 20 cases of leg ulcers in patients withrheumatoid arthritis and reported 1 patient with a leg ulcerof undetermined etiology. No further discussion was maderegarding this finding. This nonvenous, nonarterial ulcerlikely represents a less common ulcer similar to those seenin our study. Two patients had undetermined pathologydespite histologic study.
Leg ulcers have been documented as a rare complica-tion of long-term hydroxyurea treatment in patients under-going therapy for myeloproliferative disorders.14 Thesepainful, persistent ulcers may not manifest until after aduration of 2 to 15 years of treatment.2 Usually located onthe malleoli, the ulcer appears fibrous, with atrophic peri-
ulcerous skin. Twenty-four case reports were found in the
JOURNAL OF VASCULAR SURGERYVolume 45, Number 3 Labropoulos et al 571
literature between 1996 and June 2004. One multicenterretrospective study of 41 cases of leg ulceration duringhydroxyurea therapy noted that 80% of the ulcers com-pletely recovered after discontinuation of the drug; the resthad improvement and reduction in ulcer size.15 One pa-tient in our study had a hydroxyurea ulcer on the medialaspect of the lower calf for 2 months. The duration ofhydroxyurea therapy was 3 years. After the discontinuationof the drug, the ulcer was healed.
Calciphylaxis is a rare condition that can develop as acomplication of secondary hyperparathyroidism, whichmost commonly occurs in patients with end-stage renaldisease. Up to 4% of patients receiving renal dialysis mayshow signs of calciphylaxis.16 It is characterized by exces-sive calcium deposition in the skin, soft tissues, and arteries.Patients may present with a range of skin manifestations,from painful subcutaneous nodules to nonhealing extrem-ity ulcers and gangrene.17 The exact pathogenesis remainsuncertain. Ischemic necrosis preferentially affects cutane-ous vessels of the trunk and limb girdle. There is often rapidonset, with large, painful plaques that evolve into full-thickness necrosis and gangrene, similar to that seen withwarfarin-associated necrosis.7 Treatment includes localwound care, correction of the calcium/phosphorus ratio,and surgical evaluation for possible arterial revasculariza-tion and parathyroidectomy.16
Five patients had ulcers of neoplastic origin. Two pa-tients with venous reflux presented with ulcer etiologies ofSCC. As mentioned previously, stasis ulcers are likely todegenerate into malignancy.3 The ulcers may often bepainless, appear hypertrophic or hemorrhagic with irregularborders, and exhibit a slow progressive growth. The dura-tion of each ulcer with SCC in our study was 18 and 15years. One epidemiologic study noted an increase in theincidence of SCC in venous ulcers.18 It is the second mostcommon form of skin cancer and often arises on sun-exposed areas of middle-aged and elderly individuals of faircomplexion. It can also occur on non–sun-exposed areassuch as the genitals and mucous membranes. It is interest-ing to note that SCC is the most common type of skincancer in African Americans, often involving skin that is notchronically sun-exposed.17 The ulcers with SCC in ourstudy were in the gaiter area, a location consistent withvenous ulcers.
BCC is the most common type of skin cancer, typicallyarising on areas of chronic sun exposure, especially the headand neck. However, 8% of BCC arises on the lower extrem-ity.19 It may appear as a chronic ulcer refractory to treat-ment or may even appear as a benign ulcer with adequategranulation tissue, without the classic rolled pearly borderor surface telangiectasia. One patient in our study had ahistologic diagnosis of BCC. He had an ulcer that waslocated in the lower calf/malleolus. Most lesions of bothSCC and BCC can be treated with various surgical modal-ities, including cryosurgery, electrodesiccation and curet-tage, excision, and Mohs surgery.20
A variety of other atypical causes, as well as idiopathic or
unknown causes of leg ulcerations, have been reported.21For instance, vasculitis is a known condition that causesulcerations.22 Scott et al23 diagnosed leg ulcers in 38% ofpatients with systemic rheumatoid vasculitis. Both limbs inone patient in our series were diagnosed with vasculitisby ulcer biopsy, and this was the likely cause for persis-tence. The diagnosis of vasculitis as the causative agentfor an ulcer is difficult, given the low yield associatedwith ulcer edge biopsies.24 Furthermore, microbial col-onization of the ulcer per se can cause a histologicpicture of bacterial necrotizing vasculitis. Ulcers in fourlimbs in our patient population were not attributable toany of the known causes. The patients had a normalduplex scan and biopsy of the ulcer.
Three patients with cellulitis and lymphedema hadchronic inflammation on the biopsy sample. Probably thesepatients do not need to have a biopsy, but it is difficult tomake such a recommendation because the sample is sosmall. These patients had no other vascular disease.Usually patients with lymphedema and ulceration havearterial or venous disease or cancer.25,26 The prevalenceof lymphedema alone in a large prospective study was2.5% (17/689).27
An ulcer that fails to heal after 3 to 4 months of woundcare should be biopsied. The biopsy should be performedof the ulcer edge for a diagnosis and to rule out malignancy.If a biopsy is intended to determine an uncommon cause ofulceration, including vasculitis, both the edge of the ulcerand the ulcer bed should be sampled.28 Punch biopsies(3-4 mm) or a wedge or a rectangular biopsy using a scalpelwill harvest sufficient tissue for histologic analysis. If malig-nancy is suspected, several biopsies should be obtainedfrom the wound bed by using either a shave or punchmethod. If an atypical wound infection is considered, abiopsy for tissue culture should be performed.29 A total oftwo patients with four limbs in our study had pathologyreports showing undetermined pathology. If an unusual legulcer is present and the biopsy is not helpful, more specifictests should be part of the workup. For example, cryo-globulins may be associated with hepatitis C and leg ulcer-ation. Therefore, hepatitis C serologies and serum levelsof cryoglobulins may be helpful in making the diagno-sis.30 It is important to keep in mind that there arenumerous staining techniques available to detect vascu-lar pathology, micro-organisms, malignancies, dermato-logic disorders, or storage diseases. The pathologistshould receive detailed information about the clinicalproblem and the potential differential diagnoses.2 In ourcase, an extensive battery of tests was performed, but allresults were nondiagnostic.
In general, though, we recommend arterial and venoustesting before any other test because the prevalence ofvascular disease has been shown to be very high in manyclinical and epidemiologic studies. Also, many ulcers havemixed etiology, and arterial and venous testing can demon-strate the vascular pathology that may contribute to the
ulcer formation.
JOURNAL OF VASCULAR SURGERYMarch 2007572 Labropoulos et al
CONCLUSION
Extremely rare ulcers of numerous etiologies exist onlyas case reports scattered throughout the literature. Wefound uncommon leg ulcers in 17 patients out of 710patients evaluated for leg ulcers. Vasculitic, bacterial, viral,metabolic, and neoplastic ulcers have been described insingle case reports or small case series. Such ulcers and thoserefractory to initial treatment necessitate referral for furtherevaluation. As mentioned previously, biopsies are not al-ways confirmatory. However, identification of these pa-tients in the setting of a vascular clinic may provide moreaccurate data on the prevalence and etiology of uncommonleg ulcers. More importantly, it may facilitate the earlieridentification neoplastic ulcers.31-88
AUTHOR CONTRIBUTIONS
Conception and design: NLAnalysis and interpretation: NL, JT, LP, ADGWriting the article: NL, DM, NPP, JT, LP, ADGCritical revision of the article: NL, DM, NPP, JT, LP, ADGFinal approval of the article: NL, DM, NPP, JT, LP, ADGStatistical analysis: NLOverall responsibility: NL
REFERENCES
1. Lautenschlager S, Eichmann A. Differential diagnosis of leg ulcers. CurrProbl Dermatol 1999;27:259-70.
2. Mekkes JR, Loots MAM, Van der Wal AC, Box JD. Causes, investiga-tion and treatment of leg ulceration. Br J Dermatol 2003;148:388-401.
3. Baldursson BT, Hedblad MA, Beitner H, Lindelof B. Squamous cellcarcinoma complicating chronic venous leg ulceration: a study of thehistopathology, course, and survival in 25 patients. Br J Dermatol1999;140:1148-52.
4. Acland KM, Darvay A, Wakelin SH, Russel-Jones R. Livedoid vasculitis:a manifestation of the antiphospholipid syndrome? Br J Dermatol1999;140:131-5.
5. Srikuroja W, Takahashi PY. 73-year-old woman with painful lowerextremity ulcers. Mayo Clin Proc 2001;76:745-8.
6. Porter JM, Moneta GL. International Consensus Committee onChronic Venous Disease. Reporting standards in venous disease: anupdate. J Vasc Surg 1995;21:635-45.
7. Reynolds PL, Strayer SM. Treatment of skin malignancies. J Fam Pract2003;52:456-64.
8. Choucair MM, Fivenson DP. Leg ulcer diagnosis and management.Dermatol Clin 2001;19:659-78.
9. Habif TP. Clinical dermatology. 4th ed. Philadelphia: Mosby; 2004.10. Koshy M, Entsuah R, Koranda A, Kraus AP, Johnson R, Bellvue R, et al.
Leg ulcers in patients with sickle cell disease. Blood 1990;74:1403-8.11. Weinzweig N, Schuler J, Vitello J. Simultaneous reconstruction of
extensive soft-tissue defects of both lower limbs with free hemiflapsharvested from the omentum. Plast Reconstr Surg 1997;99:757-62.
12. Oien RF, Hakansson A, Hansen BU. Leg ulcers in patients withrheumatoid arthritis—a prospective study of aetiology, wound heal-ing and pain reduction after pinch grafting. Rheumatology 2001;40:816-20.
13. Hafner J, Schneider E, Burg G, Cassina P. Management of leg ulcers inpatients with rheumatoid arthritis or systemic sclerosis: the importanceof concomitant arterial and venous disease. J Vasc Surg 2000;32:322-9.
14. Best PJ, Daoud MS, Pittelkow MR, Petitt RM. Hydroxyurea-inducedleg ulceration in 14 patients. Ann Intern Med 1998;128:29-32.
15. Sirieix ME, Debure C, Baudot N, Dubertret L, Roux ME, Morel P,et al. Leg ulcers and hydroxyurea: forty-one cases. Arch Dermatol
1999;135:818-20.16. Angeles M, Wong LL, Myers SA, Womg LM. Calciphylaxis in patientson hemodialysis: a prevalence study. Surgery 1997;122:1083-90.
17. Milas M, Bush RL, Lin P, Brown K, Mackay G, Lumsden A, et al.Calciphylaxis and nonhealing wounds: the role of the vascular surgeonin a multidisciplinary treatment. J Vasc Surg 2003;37:501-7.
18. Baldursson BT, Hedblad MA, Beitner H, Lindelof B. Squamous cellcarcinoma complicating chronic venous leg ulceration: a study of thehistopathology, course, and survival in 25 patients. Br J Dermatol1999;140:1148-52.
19. Giles GG, Marks R, Foley P. Incidence of non-melanocytic skin cancertreated in Australia. Br Med J (Clin Res Ed) 1988;296:13-7.
20. Thissen MR, Neumann MH, Schouten LJ. A systematic review oftreatment modalities for primary basal cell carcinomas. Arch Dermatol1999;135:1177-83.
21. Hafner J. Differential ulcus cruris diagnosis. Ther Umsch 1998;55:632-42.
22. Nelzén O, Bergqvist D, Lindhagen A. Leg ulcer etiology—a crosssectional population study. J Vasc Surg 1991;14:557-64.
23. Scott DGI, Bacon PA, Tribe CR. Systemic rheumatoid vasculitis: aclinical and laboratory study of 50 cases. Medicine (Baltimore) 1981;60:288-97.
24. Cawley MID. Vasculitis and ulceration in rheumatic diseases of the foot.Baillieres Clin Rheumatol 1987;1:315-33.
25. Franks PJ, Moffatt CJ, Doherty DC, Williams AF, Jeffs E, Mortimer PS.Assessment of health-related quality of life in patients with lymphedemaof the lower limb. Wound Repair Regen 2006;14:110-8.
26. Moffatt CJ, Franks PJ, Doherty DC, Martin R, Blewett R, Ross F.Prevalence of leg ulceration in a London population. QJM 2004;97:431-7.
27. Adam DJ, Naik J, Hartshorne T, Bello M, London NJ. The diagnosisand management of 689 chronic leg ulcers in a single-visit assessmentclinic. Eur J Vasc Endovasc Surg 2003;25:462-8.
28. Khachemoune A, Kauffman CL. Diagnosis of leg ulcers. Internet JDermatol 2002;1(2).
29. Trent J, Federman D, Kirsner R. Skin and wound biopsy: when, whyand how. Adv Skin Wound Care 2003;16:372-5.
30. Mahabir RC, Taylor CD, Benny WB, Dutz JP, Snelling CF. Necrotiz-ing cutaneous cryoglobulinemic vasculopathy. Plast Reconstr Surg2001;107:1221-4.
31. Kelly J. Pyoderma gangraenosum: exploring the treatment options.J Wound Care 2001;10:125-8.
32. Matsumura T, Sato-Matsumura KC, Ota M, Yokota T, Arita K, Ko-dama K, et al. Two cases of pyoderma gangrenosum complicated withnasal septal perforation. Br J Dermatol 1999;141:1133-5.
33. Samuel J, Williams C. Pyoderma gangrenosum: an inflammatory ulcer.J Wound Care 1996;5:314-8.
34. Pieters RC, Rojer RA, Saleh AW, Saleh AE, Duits AJ. Molgramostim totreat SS-sickle cell leg ulcers. Lancet 1995;345:528.
35. Sher GD, Olivieri NF. Rapid healing of chronic leg ulcers duringarginine butyrate therapy in patients with sickle cell disease and thalas-semia. Blood 1994;84:2378-80.
36. Nishikawa JA. Are leg ulcers in rheumatoid arthritis due to vasculitis?Eur J Rheumatol Inflamm 1983;6:288-90.
37. O’Quinn SE, Kennedy CB, Baker DT. Peripheral vascular lesions inrheumatoid arthritis. Arch Dermatol 1965;92:489-94.
38. Paquette D, Falanga V. Leg ulcers. Clin Geriatr Med 2002;18:77-88.39. Sastre JL, Bravo A, Tembras S, Gomez R, Ulibarrena C. Leg ulcers
associated with hydroxyurea therapy. Haematologica 2003;88:EIM01.40. Demircay Z, Comert A, Adiguzel C. Leg ulcers and hydroxyurea: report
of three cases with essential thrombocythemia. Int J Dermatol 2002;41:872-4.
41. Kersgard C, Osswald MB. Hydroxyurea and sickle cell leg ulcers. Am JHematol 2001;68:215-6.
42. Bader U, Banyai M, Boni R, Burg G, Hafner J. Leg ulcers in patientswith myeloproliferative disorders: disease- or treatment-related? Der-matology 2000;200:45-8.
43. Weinlich G, Schuler G, Greil R, Kofler H, Fritsch P. Leg ulcersassociated with long-term hydroxyurea therapy. J Am Acad Dermatol
1998;39(2 Pt 2):372-4.
JOURNAL OF VASCULAR SURGERYVolume 45, Number 3 Labropoulos et al 573
44. Disla E, D’Eamour L, Cioriou M. Hydroxyurea-associated leg ulcer-ation. Ann Intern Med 1998;129:252-3.
45. Banky JP, Dowling JP, Miles C. Idiopathic calciphylaxis. Aust J Der-matol 2002;43:190-3.
46. Howe SC, Murray JD, Reeves RT, Hemp JR, Carlisle JH. Calciphylaxis,a poorly understood clinical syndrome: three case reports and a reviewof the literature. Ann Vasc Surg 2001;15:470-3.
47. Fine A, Fleming S, Leslie W. Calciphylaxis presenting with calf pain andplaques in four continuous ambulatory peritoneal dialysis patients andin one predialysis patient. Am J Kidney Dis 1995;25:498-502.
48. Ivker RA, Woosley J, Briggaman RA. Calciphylaxis in three patientswith end-stage renal disease. Arch Dermatol 1995;131:63-8.
49. Graziano TA, Giampapa V. Muscle transposition in the management ofchronic osteomyelitis and ulceration of the heel. J Foot Surg 1989;28:68-71.
50. Pascher F, Shalita A. Leg ulcer associated with osteomyelitis and stasisdermatitis. Arch Dermatol 1968;98:674-5.
51. Levine N. Deep leg ulceration. Look to underlying systemic disease forthe cause of this dermatologic condition. Geriatrics 2002;57:15.
52. Fishman JR, Parker MG. Malignancy and chronic wounds: Marjolin’sulcer. J Burn Care Rehabil 1991;12:218-23.
53. Ackroyd JS, Young AE. Leg ulcers that do not heal. Br Med J (Clin ResEd) 1983;286:207-8.
54. Oluwasanmi JO, Ofodile FA, Aboyle AA. Neoplastic change in chronicleg ulcer. Int Surg 1982;67:407-8.
55. Tabibzadeh F. Basal cell carcinoma of the leg. Am Fam Phys 1995;52:1684-1689.
56. Neal MS. Treatment of a malignant leg ulcer. J Wound Care 1995;4:300-1.
57. Gosain A, Sanger JR, Yousif NJ, Matloub HS. Basal cell carcinoma ofthe lower leg occurring in association with chronic venous stasis. AnnPlast Surg 1991;26:279-83.
58. Markey AC, Tidman MJ, Rowe PH, Missen GA, Macdonald DM. Aggres-sive ulcerative necrobiosis lipoidica associated with venous insufficiency,giant-cell phlebitis and arteritis. Clin Exp Dermatol 1988;13:183-6.
59. Youshock E, Beninson J. Necrobiosis lipoidica: treatment with porcinedressings, split-thickness skin grafts and pressure garments. A casereport and review of treatment modalities. Angiology 1985;36:821-6.
60. Gilsanz F, Escalante F, Auray C, Olbes AG. Treatment of leg ulcers inbeta-thalassaemia intermedia: use of platelet-derived wound healingfactors from the patient’s own platelets. Br J Haematol 2001;115:710.
61. Josifova D, Gatt G, Aquilina A, Serafimov V, Vella A, Felice A.Treatment of leg ulcers with platelet-derived wound healing factor(PDWHFS) in a patient with beta thalassaemia intermedia. Br JHaematol 2001;112:527-9.
62. Grossman JA, Barrall DT, Dennison A, Lally EV. Successful combinedmedical and surgical treatment of a lower extremity sclerodermal ulcer.Ann Plast Surg 1988;20:582-5.
63. Thomas JR III, Winkelmann RK. Vascular ulcers in scleroderma. ArchDermatol 1983;119:803-7.
64. Kokturk A, Kaya TI, Ikizoglu G, Koca A. Prolidase deficiency. Int JDermatol 2002;41:45-8.
65. Milligan A, Graham-Brown RA, Burns DA, Anderson I. Prolidase defi-ciency: a case report and literature review. Br J Dermatol 1989;121:405-9.
66. Trent JT, Kirsner RS. Leg ulcers secondary to prolidase deficiency. AdvSkin Wound Care 2004;17:468-72.
67. Shih HA, Kao DM, Elenitsas R, Leyden JJ. Livedo reticularis, ulcers,and peripheral gangrene: cutaneous manifestations of primary hyperox-aluria. Arch Dermatol 2000;136:1272-4.
68. Green KM, Lynfield YL, Davis DE. Livedo reticularis with ulcers andcirculating immune complexes. Cutis 1983;31:312-5.
69. Klein AD, Kerdel FA. Purpura and recurrent ulcers on the lower extremi-ties. Essential cryofibrinogenemia. Arch Dermatol 1991;127:115-118.
70. Kleeman D, Kempf W, Burg G, Hafner J. Cutaneous polyarteritisnodosa. Vasa 1998;27:54-7.
71. Mimouni D, Rencic A, Nikolskaia OV, Bernstein BD, Nousari HC.Cutaneous polyarteritis nodosa in patients presenting with atrophy
blanche. Br J Dermatol 2003;148:789-94.72. Andersen JG. Malignant degeneration in chronic ulceration of the legand foot in leprosy patients: two case reports. Lepr Rev 1982;53:265-9.
73. Noe JM, Barber J. Chronic leg ulceration in a patient with leprosy. WestJ Med 1974;121:430-2.
74. Wakelin SH, James MP. Sarcoidosis: nail dystrophy without underlyingbone changes. Cutis 1995;55:344-6.
75. Saxe N, Benatar SR, Bok L, Gordon W. Sarcoidosis with leg ulcers andannular facial lesions. Arch Dermatol 1984;120:93-6.
76. Winkelmann RK, Schroeter AL, Kierland RR, Ryan TS. Clinical studiesof livedoid vasculitis (segmental hyalinizing vasculitis). Mayo Clin Proc1974;49:746-50.
77. Artik S, Miller A, Bretschneider P, Schurer N, Ruzicka T. Leg ulcersassociated with sideroblastic anemia. Dermatology 1998;197:397-8.
78. Kajisawa C, Matsui C, Morohashi M. A specific cutaneous lesionrevealing myelodysplastic syndrome. Eur J Dermatol 1998;8:517-8.
79. Siregusa M, Alberti A, Schepis C. Skin ulcers in a young woman onlow-dose estrogen-combination pill. Int J Dermatol 1997;36:317-8.
80. Aractingi S, Bachmeyer C, Miclea JM, Verola O, Rousselot P, Duber-tret L, et al. Unusual specific cutaneous lesions in myelodysplasticsyndromes. J Am Acad Dermatol 1995;33(2 Pt 1):187-91.
81. Lebel M, Lassonde M. Erythema induratum of Bazin. J Am AcadDermatol 1986;14:738-42.
82. Carbia SG, Chain M, Acuna K, Dei-Cas I, Glorio R, Malah V, et al.Disseminated cryptococcosis with cutaneous lesions complicating ste-roid therapy for Behcet’s disease. Int J Dermatol 2003;42:821-3.
83. Rustin MH, Gilkes JJ, Robinson TW. Pyoderma gangrenosum associ-ated with Behcet’s disease: treatment with thalidomide. J Am AcadDermatol 1990;23(5 Pt 1):941-4.
84. Lombardo GA, Annessi G, Baliva G, Monopoli A, Girolomoni G.Keratosis lichenoides chronica. Report of a case associated with B-celllymphoma and leg panniculitis. Dermatology 2000;201:261-4.
85. Conejo-Mir J, Pulpillo A, Corbi MR, Linares M, Garcia Lopez A,Conde F, et al. Panniculitis and ulcers in a young man. Arch Dermatol1998;134:501-504.
86. Tanzer FR, Lynfield YL. Erythema elevatum diutinum. Arch Dermatol1978;114:802-23.
87. Roenigk HH Jr. Necrotizing vasculitis (erythema elevatum diutinum).Arch Dermatol 1971;104:103-5.
88. Monsuez JJ, Mathieu D, Arnoult F, Passeron J. Cutaneous diphtheriain a homeless man. Lancet 1995;346:649-50.
Submitted Aug 11, 2006; accepted Nov 1, 2006.
Additional material for this article may be found onlineat www.jvascsurg.org.
APPENDIX I: PARTICIPATING CENTERSNicos Labropoulos, Danielle Manalo, Jay Tiongson,
Landon Pryor, Luis Leon, and Apostolos K. Tassiopoulos,Loyola University Medical Center, Maywood, Ill; NimaPatel and Peter J. Pappas, University of Medicine andDentistry of New Jersey, Newark, NJ; Berndt Arfvidsson,Bo Eklof, and Robert Kistner, Straub Foundation, Hono-lulu, Hawaii; Kostas Delis and Andrew N. Nicolaides, StMary’s Hospital, Imperial College, London, UK; DimitrisTsantillas, Praxis für Gef. Chirurgie and Phlebologie, Augs-burg, Germany; Paolo Zamboni, University of Ferrara,Ferrara, Italy; Athanasios D. Giannoukas, University ofThessaly, Larissa, Greece; Carmen L. Porto, State Univer-sity of Rio de Janeiro, Rio de Janeiro, Brazil; Fanilda S.Barros, Angiolab, Vitoria, Brasil; and Carlos A. Engelhornand Ana L. Engelhorn, Pontificia Universidade Catolica do
Parana, Curitiba, Brasil.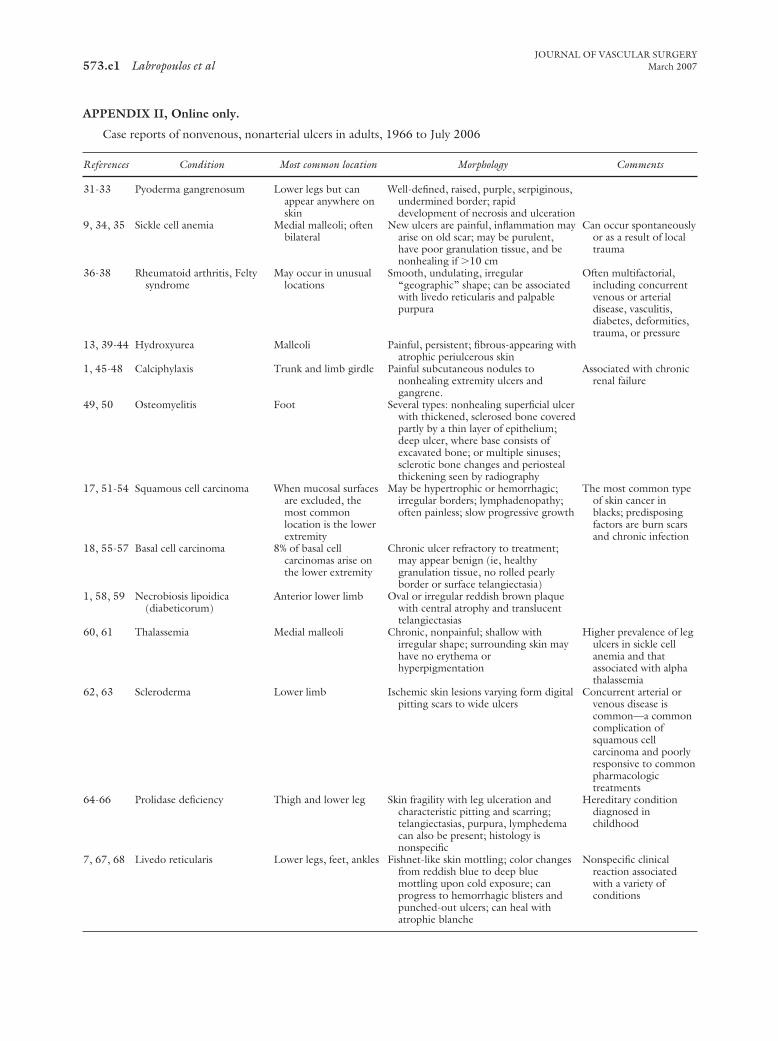
JOURNAL OF VASCULAR SURGERYMarch 2007573.e1 Labropoulos et al
APPENDIX II, Online only.
Case reports of nonvenous, nonarterial ulcers in adults, 1966 to July 2006
References Condition Most common location Morphology Comments
31-33 Pyoderma gangrenosum Lower legs but canappear anywhere onskin
Well-defined, raised, purple, serpiginous,undermined border; rapiddevelopment of necrosis and ulceration
9, 34, 35 Sickle cell anemia Medial malleoli; oftenbilateral
New ulcers are painful, inflammation mayarise on old scar; may be purulent,have poor granulation tissue, and benonhealing if �10 cm
Can occur spontaneouslyor as a result of localtrauma
36-38 Rheumatoid arthritis, Feltysyndrome
May occur in unusuallocations
Smooth, undulating, irregular“geographic” shape; can be associatedwith livedo reticularis and palpablepurpura
Often multifactorial,including concurrentvenous or arterialdisease, vasculitis,diabetes, deformities,trauma, or pressure
13, 39-44 Hydroxyurea Malleoli Painful, persistent; fibrous-appearing withatrophic periulcerous skin
1, 45-48 Calciphylaxis Trunk and limb girdle Painful subcutaneous nodules tononhealing extremity ulcers andgangrene.
Associated with chronicrenal failure
49, 50 Osteomyelitis Foot Several types: nonhealing superficial ulcerwith thickened, sclerosed bone coveredpartly by a thin layer of epithelium;deep ulcer, where base consists ofexcavated bone; or multiple sinuses;sclerotic bone changes and periostealthickening seen by radiography
17, 51-54 Squamous cell carcinoma When mucosal surfacesare excluded, themost commonlocation is the lowerextremity
May be hypertrophic or hemorrhagic;irregular borders; lymphadenopathy;often painless; slow progressive growth
The most common typeof skin cancer inblacks; predisposingfactors are burn scarsand chronic infection
18, 55-57 Basal cell carcinoma 8% of basal cellcarcinomas arise onthe lower extremity
Chronic ulcer refractory to treatment;may appear benign (ie, healthygranulation tissue, no rolled pearlyborder or surface telangiectasia)
1, 58, 59 Necrobiosis lipoidica(diabeticorum)
Anterior lower limb Oval or irregular reddish brown plaquewith central atrophy and translucenttelangiectasias
60, 61 Thalassemia Medial malleoli Chronic, nonpainful; shallow withirregular shape; surrounding skin mayhave no erythema orhyperpigmentation
Higher prevalence of legulcers in sickle cellanemia and thatassociated with alphathalassemia
62, 63 Scleroderma Lower limb Ischemic skin lesions varying form digitalpitting scars to wide ulcers
Concurrent arterial orvenous disease iscommon—a commoncomplication ofsquamous cellcarcinoma and poorlyresponsive to commonpharmacologictreatments
64-66 Prolidase deficiency Thigh and lower leg Skin fragility with leg ulceration andcharacteristic pitting and scarring;telangiectasias, purpura, lymphedemacan also be present; histology isnonspecific
Hereditary conditiondiagnosed inchildhood
7, 67, 68 Livedo reticularis Lower legs, feet, ankles Fishnet-like skin mottling; color changesfrom reddish blue to deep bluemottling upon cold exposure; canprogress to hemorrhagic blisters andpunched-out ulcers; can heal withatrophie blanche
Nonspecific clinicalreaction associatedwith a variety ofconditions
JOURNAL OF VASCULAR SURGERYVolume 45, Number 3 Labropoulos et al 573.e2
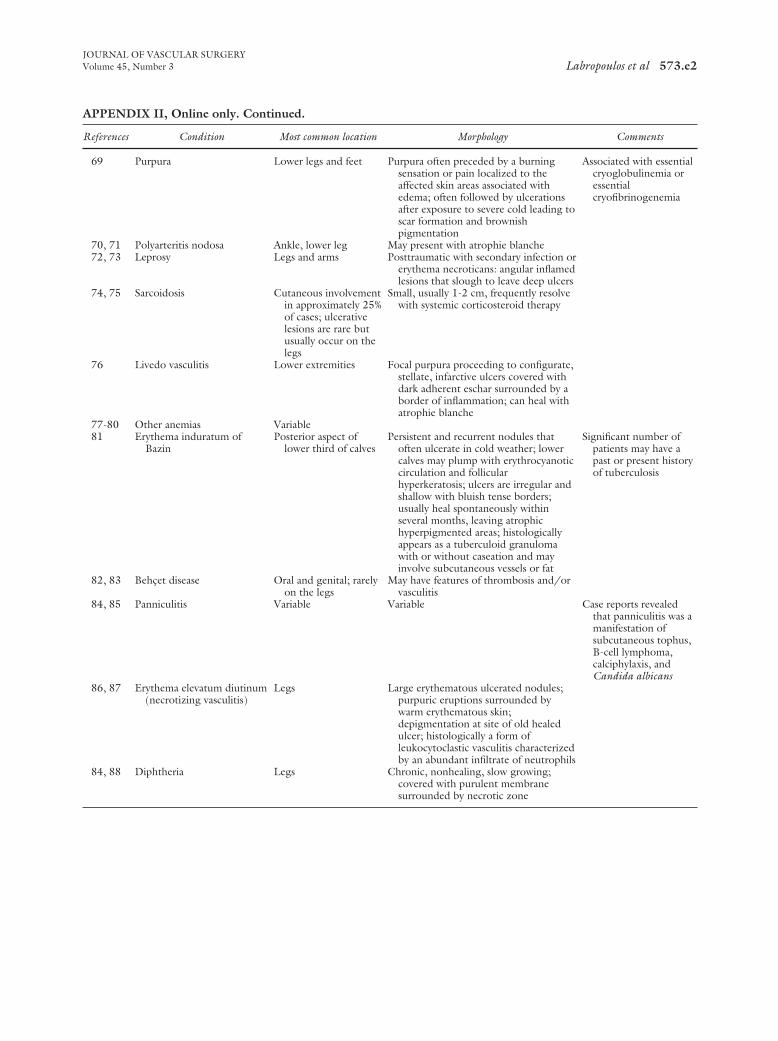
APPENDIX II, Online only. Continued.
References Condition Most common location Morphology Comments
69 Purpura Lower legs and feet Purpura often preceded by a burningsensation or pain localized to theaffected skin areas associated withedema; often followed by ulcerationsafter exposure to severe cold leading toscar formation and brownishpigmentation
Associated with essentialcryoglobulinemia oressentialcryofibrinogenemia
70, 71 Polyarteritis nodosa Ankle, lower leg May present with atrophie blanche72, 73 Leprosy Legs and arms Posttraumatic with secondary infection or
erythema necroticans: angular inflamedlesions that slough to leave deep ulcers
74, 75 Sarcoidosis Cutaneous involvementin approximately 25%of cases; ulcerativelesions are rare butusually occur on thelegs
Small, usually 1-2 cm, frequently resolvewith systemic corticosteroid therapy
76 Livedo vasculitis Lower extremities Focal purpura proceeding to configurate,stellate, infarctive ulcers covered withdark adherent eschar surrounded by aborder of inflammation; can heal withatrophie blanche
77-80 Other anemias Variable81 Erythema induratum of
BazinPosterior aspect of
lower third of calvesPersistent and recurrent nodules that
often ulcerate in cold weather; lowercalves may plump with erythrocyanoticcirculation and follicularhyperkeratosis; ulcers are irregular andshallow with bluish tense borders;usually heal spontaneously withinseveral months, leaving atrophichyperpigmented areas; histologicallyappears as a tuberculoid granulomawith or without caseation and mayinvolve subcutaneous vessels or fat
Significant number ofpatients may have apast or present historyof tuberculosis
82, 83 Behçet disease Oral and genital; rarelyon the legs
May have features of thrombosis and/orvasculitis
84, 85 Panniculitis Variable Variable Case reports revealedthat panniculitis was amanifestation ofsubcutaneous tophus,B-cell lymphoma,calciphylaxis, andCandida albicans
86, 87 Erythema elevatum diutinum(necrotizing vasculitis)
Legs Large erythematous ulcerated nodules;purpuric eruptions surrounded bywarm erythematous skin;depigmentation at site of old healedulcer; histologically a form ofleukocytoclastic vasculitis characterizedby an abundant infiltrate of neutrophils
84, 88 Diphtheria Legs Chronic, nonhealing, slow growing;covered with purulent membranesurrounded by necrotic zone