twin-twin transfusion syndrome - uams.eduuams.edu/angels/perinatal_conference/presentations... ·...
TRANSCRIPT
TWIN-TWIN TRANSFUSION
SYNDROMESYNDROME
Shannon Barringer, MS, CGCAR Reproductive Genetics/ANGELSAR Reproductive Genetics/ANGELS
Department of OB/GYN--UAMS

Twin Pregnanciesg
MZ TWINS DZ TWINS• Identical• 1:250 pregnancies
• Fraternal, Non-Identicalg
• One fertilized ovum splits after
• More common• Two separate ova
conception• Increased risk for
• Some genetic component?
many complications• Rarely familial
• Inc. risks with inc. maternal age.

Monozygotic Twinsyg
Risk for complications dependent on timing of split
• Monochorionic/Monoamniotic• Monchorionic/Diamniotic• Dichorionic/Diamniotic• Conjoined Twinsj
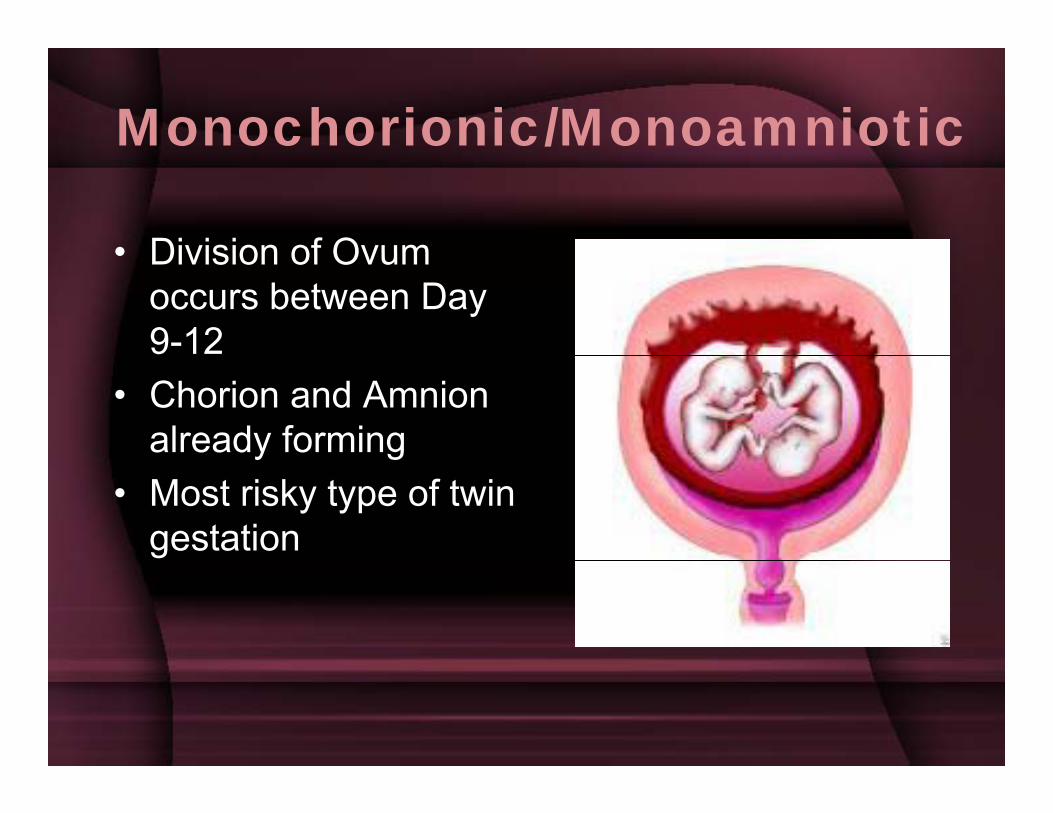
Monochorionic/Monoamniotic
• Division of Ovum• Division of Ovum occurs between Day 9-12
• Chorion and Amnion already formingy g
• Most risky type of twin gestation

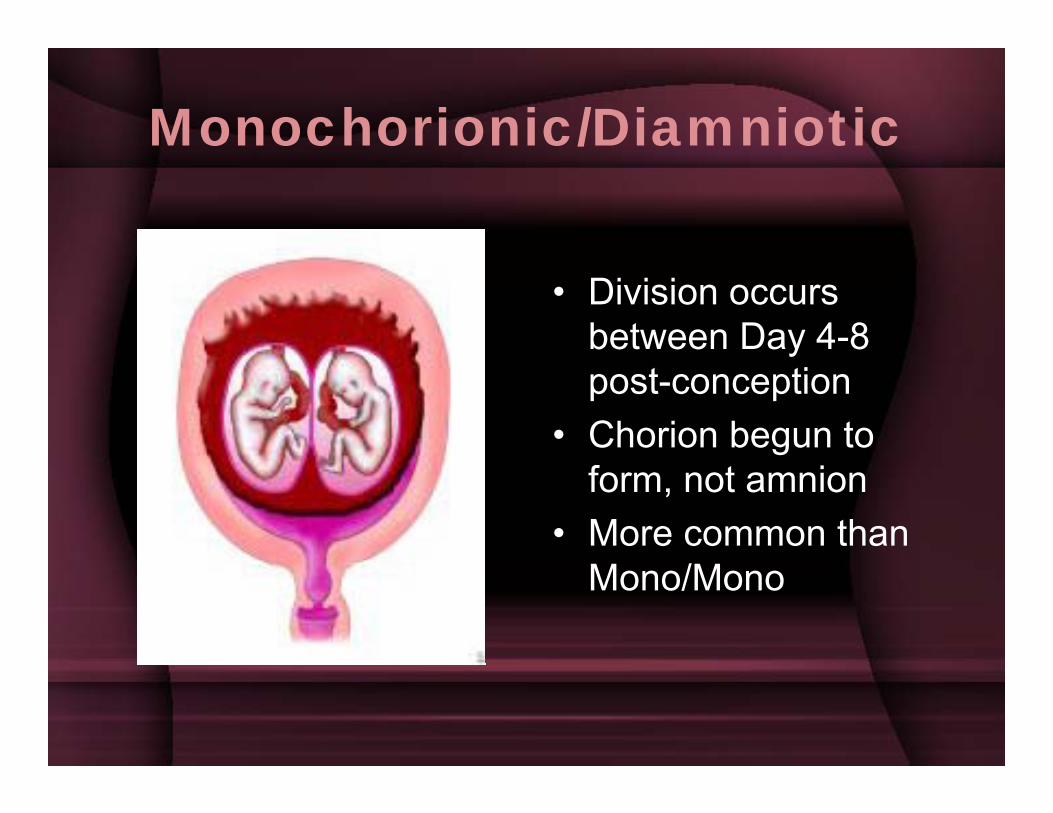
Monochorionic/Diamniotic
• Division occurs between Day 4-8 ypost-conception
• Chorion begun to form, not amnion
• More common than Mono/Mono

Sonography Assessment of Multiple Gestation
• Is there a membrane separating fetuses?– Membrane = Diamniotic– No membrane ≠ Monoamniotic– Thick membrane = Di/Di, Thin = Mono/Di
• Are there two placentas?T Di h i i O ≠ M h i i– Two = Dichorionic, One ≠ Monochorionic
• Sex of fetuses?• Sex of fetuses?
Twin-Twin Transfusion Syndrome (TTTS)Syndrome (TTTS)
M h i i t i• Monochorionic twins only (? Mono/Di)
• Approximately 10-• Approximately 10-20% of these twins affected
• Mortality rates can approach 80-100% for at least one babyfor at least one baby
• Worst outcome if present < 20 weekspresent 20 weeks
TTTS• Blood is disproportionately passed to
monochorionic babies• Passed through shared placental blood
vessels: one baby gets “too much”, other baby gets “too little”.
• TRAP
Twin-Twin Transfusion Syndrome (TTTS)Syndrome (TTTS)
• Monochorionic/Diamniotic gestations (4 35% of all MC)• Monochorionic/Diamniotic gestations (4-35% of all MC)• Recipient Twin: poly, cardiac enlargement/failure,
hydrops• Donor Twin: oligo, growth restriction• Overall mortality:50-100% depending on
severity/treatment.severity/treatment.• Abnormal vascular connections, but more than simple
transfusion process; hemodynamic changes, renin shunting from donorshunting from donor.
• Neurologic morbidity risks can also be high: related to polycythemia/venous stasis (recipient) and
i /h t i (d )anemia/hypotension (donor).
Recipient Twinp
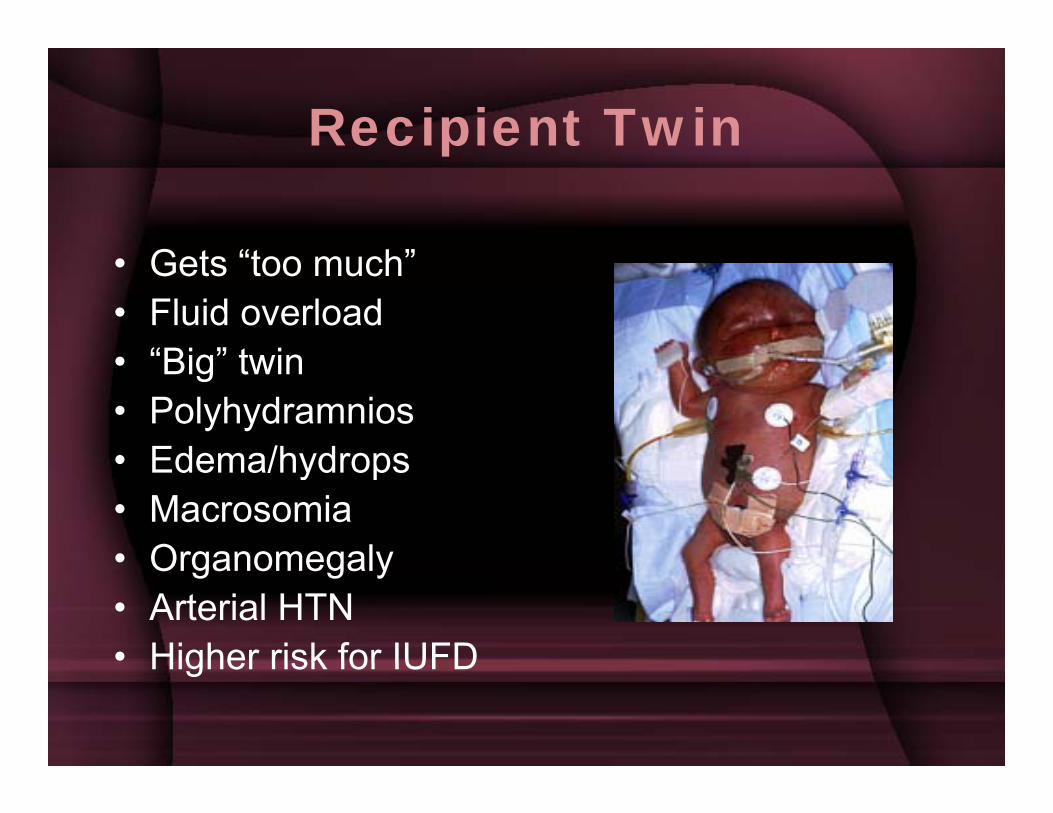
G t “t h”• Gets “too much”• Fluid overload
“Big” twin• “Big” twin• Polyhydramnios• Edema/hydrops• Edema/hydrops• Macrosomia• Organomegaly• Organomegaly• Arterial HTN• Higher risk for IUFDHigher risk for IUFD
Donor Twin
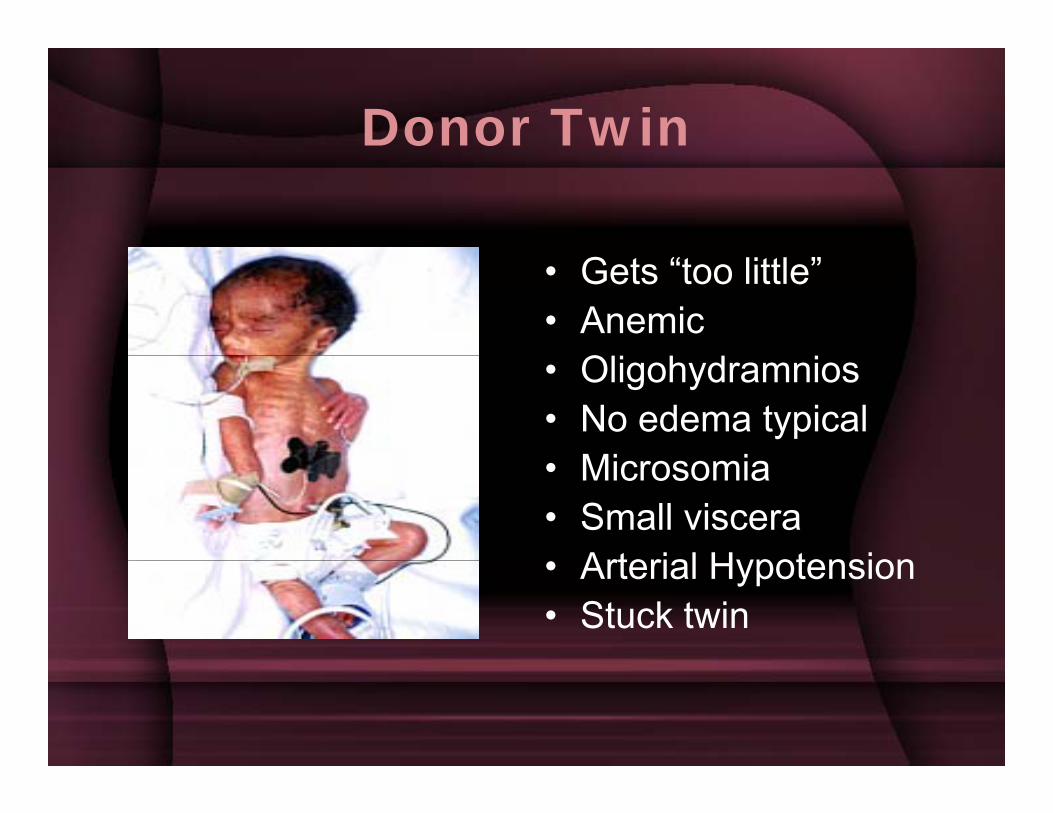
• Gets “too little”• Anemic
O• Oligohydramnios• No edema typical
Mi i• Microsomia• Small viscera
Arterial Hypotension• Arterial Hypotension• Stuck twin
Staging Criteria for TTTS
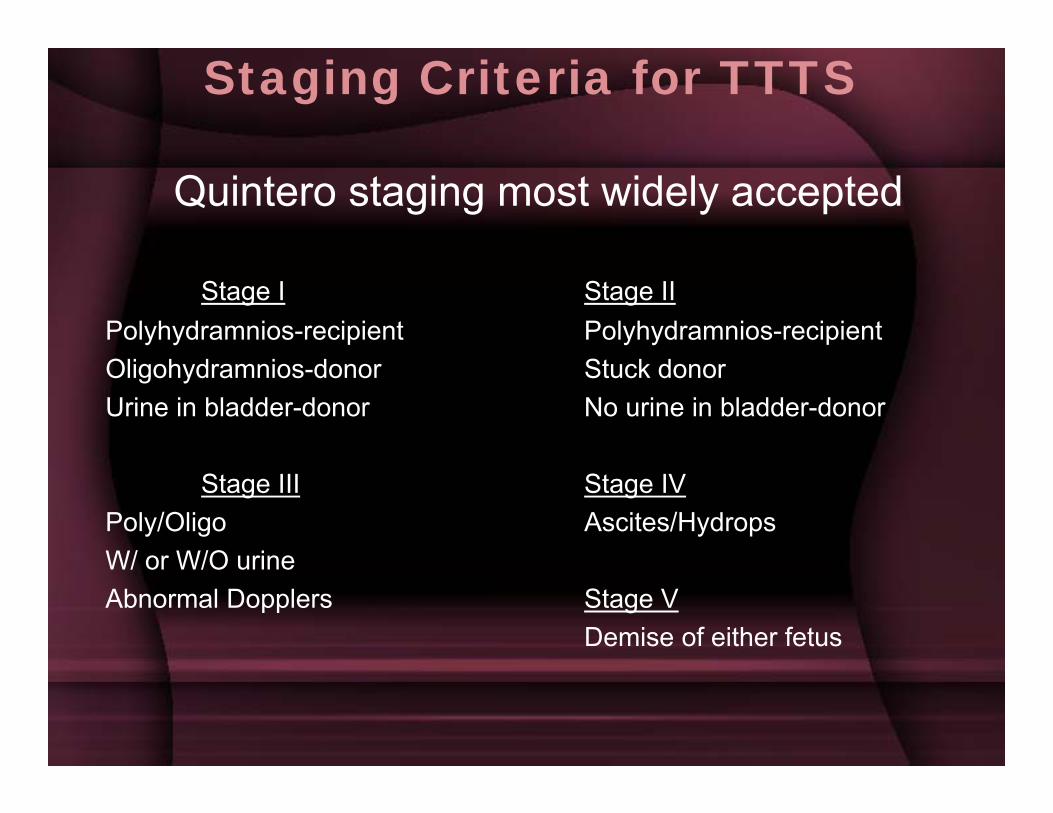
Quintero staging most widely accepted
Stage I Stage IIPolyhydramnios-recipient Polyhydramnios-recipientOligohydramnios-donor Stuck donorUrine in bladder-donor No urine in bladder-donor
Stage III Stage IVPoly/Oligo Ascites/Hydrops W/ or W/O urineW/ or W/O urineAbnormal Dopplers Stage V
Demise of either fetus
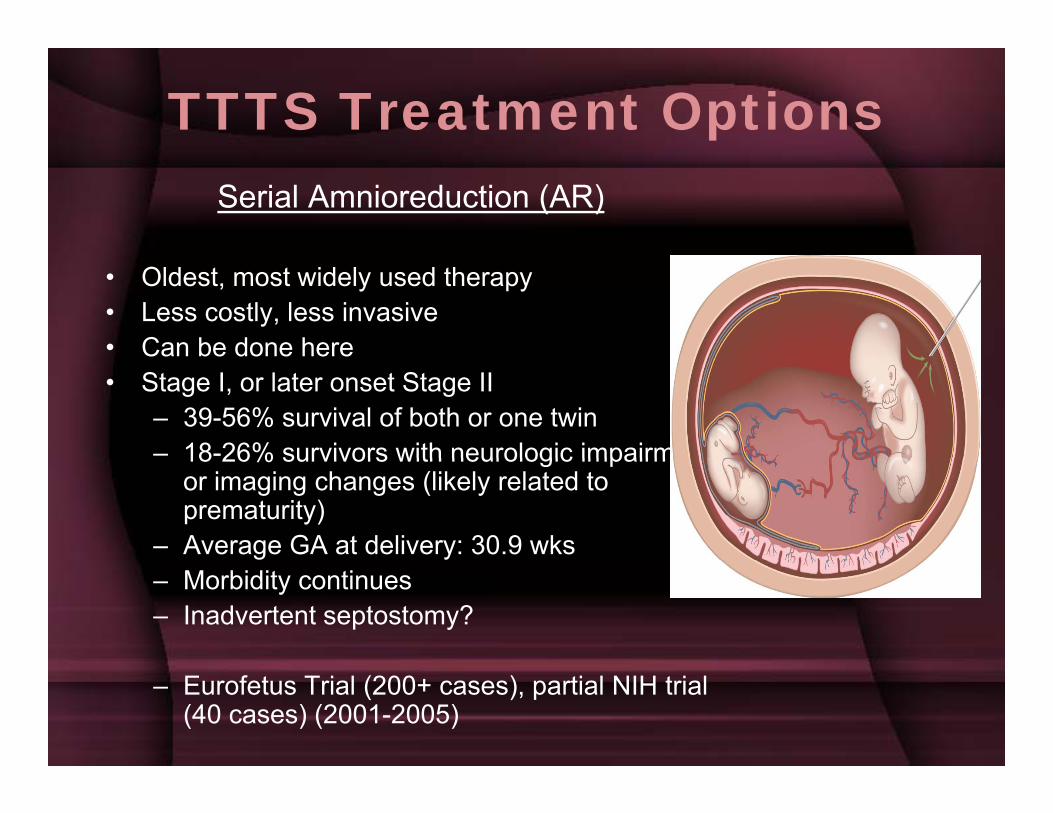
TTTS Treatment OptionsSerial Amnioreduction (AR)
• Oldest, most widely used therapy• Less costly, less invasive• Can be done hereCan be done here• Stage I, or later onset Stage II
– 39-56% survival of both or one twin– 18-26% survivors with neurologic impairment18 26% survivors with neurologic impairment
or imaging changes (likely related to prematurity)
– Average GA at delivery: 30.9 wks– Morbidity continues– Inadvertent septostomy?
– Eurofetus Trial (200+ cases), partial NIH trial (40 cases) (2001-2005)
Laser Photocoagulationg
• Purpose is to “shut off” the anastomosesp• Need better randomized-controlled trials• Only in true diagnoses• Only in true diagnoses• Deep versus superficial• Arteries are followed (fetoscopy) to make
sure vein drains back to same twin– If not, laser coagulation– Average of 3-4 deep anastomoses per twins
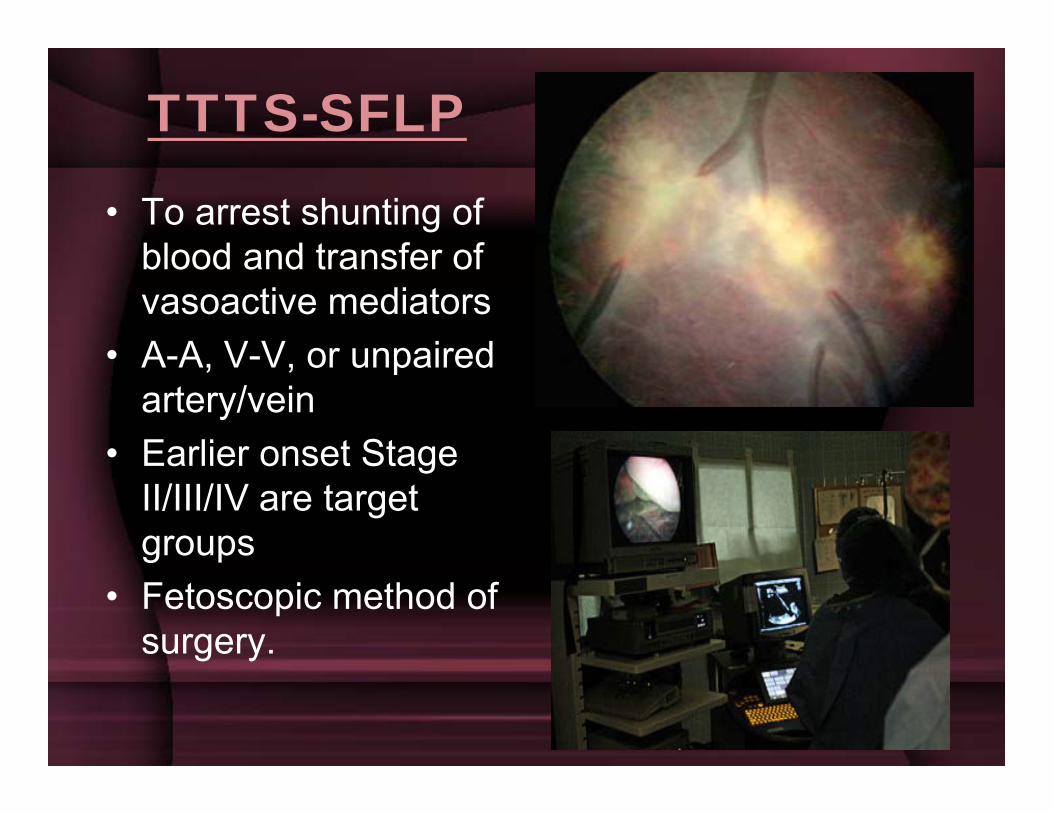
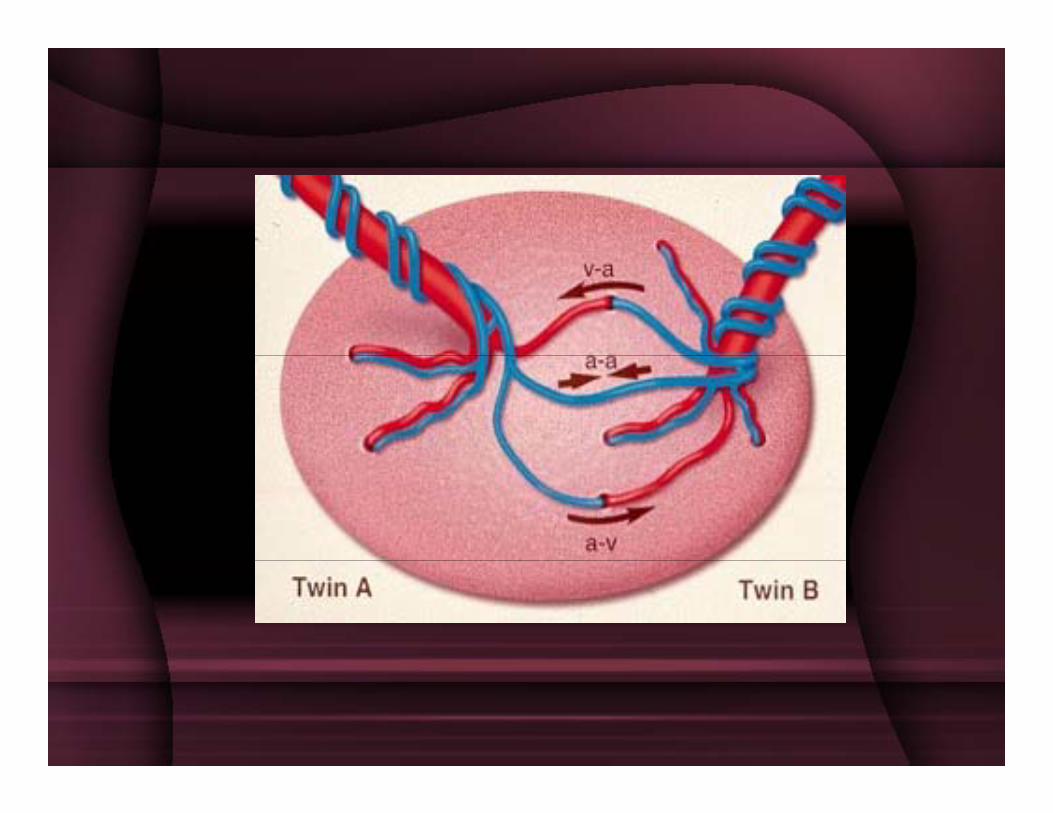
TTTS-SFLP
• To arrest shunting of blood and transfer ofblood and transfer of vasoactive mediators
• A A V V or unpaired• A-A, V-V, or unpaired artery/vein
• Earlier onset StageEarlier onset Stage II/III/IV are target groupsg p
• Fetoscopic method of surgery.
TTTS-SFLP
• Few centers in US (Texas Children’s and Cincinnati Children’s closest to AR)SFLP AR)
• ? Insurance coverage
Eurofetus Trial• Overall survival both twins—36-50%• Survival of one Twin—77-90% (to
birth)• Decreased risk of neurologic/CNS
comps versus AR at 6months of life.• Average GA at birth: 32.1 weeksNIH trial• No sig difference between AR and• No sig. difference between AR and
SFLP overall survival of both twins.• Study halted; Recipient Twin
mortality seemed disprop high inmortality seemed disprop. high in SFLP, as did # of AR failures causing cardiac changes in RTs.
TTTS—Other treatments
• Microseptostomy---jury out, but some promise p y j y , pfrom Eurofetus if stage II/III >24 weeks gestation. Prelim. Data: 65-71% survival of one twin in these groupstwin in these groups.
• Nonselective FLP---higher death rate for donor twin but easier proceduretwin, but easier procedure.
• Cord Coagulation---In twin with hydrops (usually recipient), usually reserved for imminent demise.
• Identification of CV risk indicators: might be helpful in identifying twins who would most likely benefit from SFLPbenefit from SFLP.

Morbidity in TTTSy• Loss of one twin increases risk of neurologic
handicap in surviving twinhandicap in surviving twin• Mesenteric ischemia• Bowel necrosis• Skin necrosis• ? Limb abnormalities
P l th i• Polycythemia• Hydrocephaly• CP• CP• Preterm birth