tubes and closed chest drains? what is involved in
TRANSCRIPT
NURSINGPRACTICE &SKILL
ICD-934.04
AuthorsArsi L. Karakashian, RN, BSN
Armenian American Medical Society ofCalifornia
Kathleen Walsh, RN, MSN, CCRNCinahl Information Systems, Glendale, CA
ReviewersEliza Schub, RN, BSN
Cinahl Information Systems, Glendale, CA
Teresa-Lynn Spears, RN, MSNCinahl Information Systems, Glendale, CA
Nursing Executive Practice CouncilGlendale Adventist Medical Center,
Glendale, CA
EditorDiane Pravikoff, RN, PhD, FAAN
Cinahl Information Systems, Glendale, CA
August 31, 2018
Published by Cinahl Information Systems, a division of EBSCO Information Services. Copyright©2018, Cinahl Information Systems. All rightsreserved. No part of this may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or byany information storage and retrieval system, without permission in writing from the publisher. Cinahl Information Systems accepts no liability for adviceor information given herein or errors/omissions in the text. It is merely intended as a general informational overview of the subject for the healthcareprofessional. Cinahl Information Systems, 1509 Wilson Terrace, Glendale, CA 91206
Chest Tubes and Closed Chest Drains: Troubleshooting
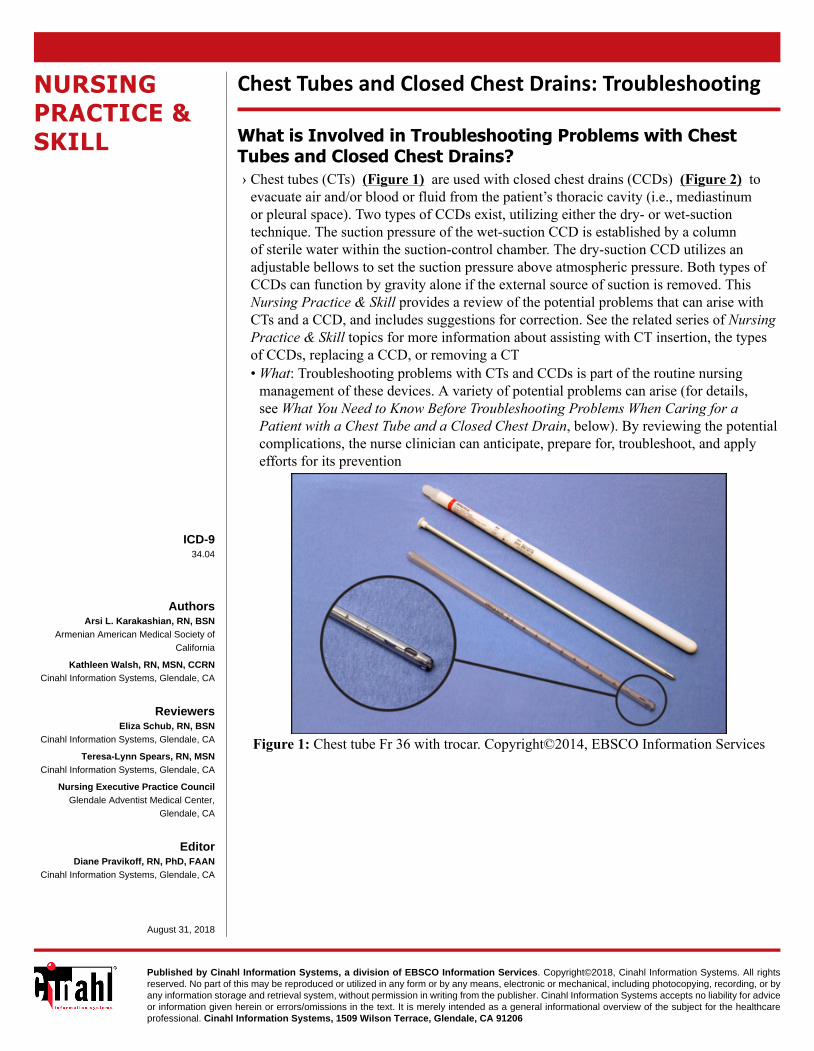
What is Involved in Troubleshooting Problems with ChestTubes and Closed Chest Drains?› Chest tubes (CTs) (Figure 1) are used with closed chest drains (CCDs) (Figure 2) to
evacuate air and/or blood or fluid from the patient’s thoracic cavity (i.e., mediastinumor pleural space). Two types of CCDs exist, utilizing either the dry- or wet-suctiontechnique. The suction pressure of the wet-suction CCD is established by a columnof sterile water within the suction-control chamber. The dry-suction CCD utilizes anadjustable bellows to set the suction pressure above atmospheric pressure. Both types ofCCDs can function by gravity alone if the external source of suction is removed. ThisNursing Practice & Skill provides a review of the potential problems that can arise withCTs and a CCD, and includes suggestions for correction. See the related series of NursingPractice & Skill topics for more information about assisting with CT insertion, the typesof CCDs, replacing a CCD, or removing a CT• What: Troubleshooting problems with CTs and CCDs is part of the routine nursing
management of these devices. A variety of potential problems can arise (for details,see What You Need to Know Before Troubleshooting Problems When Caring for aPatient with a Chest Tube and a Closed Chest Drain, below). By reviewing the potentialcomplications, the nurse clinician can anticipate, prepare for, troubleshoot, and applyefforts for its prevention
Figure 1: Chest tube Fr 36 with trocar. Copyright©2014, EBSCO Information Services
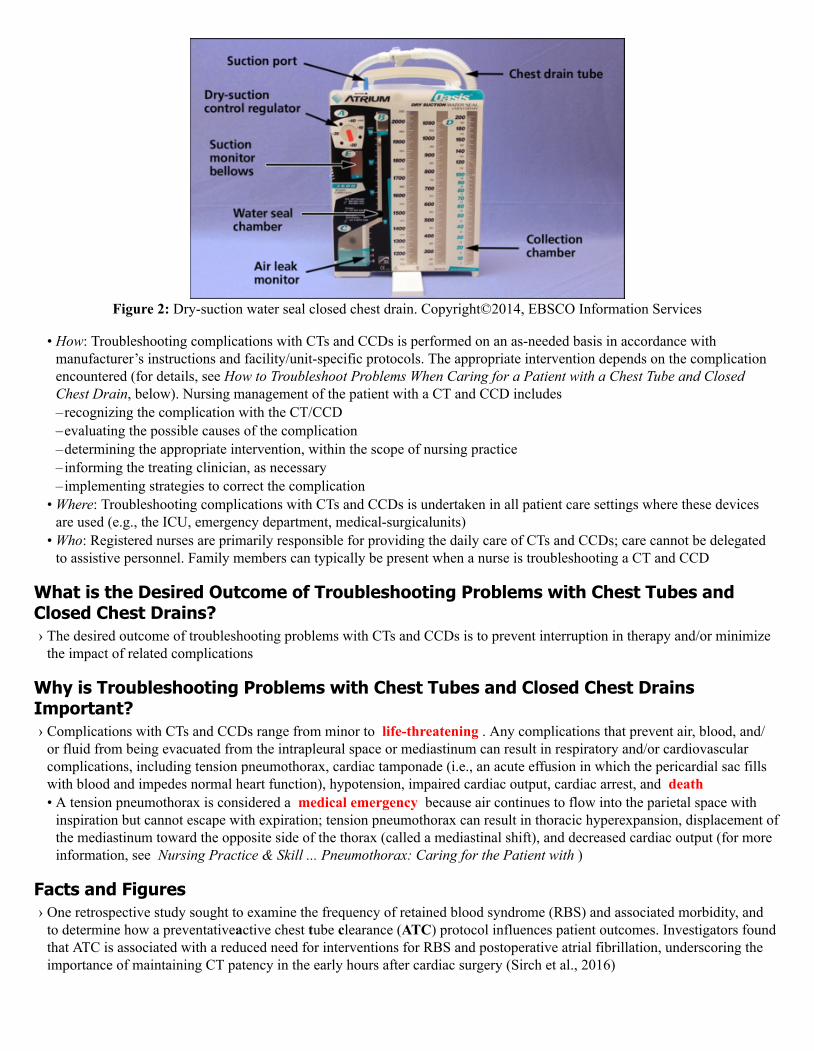
Figure 2: Dry-suction water seal closed chest drain. Copyright©2014, EBSCO Information Services
• How: Troubleshooting complications with CTs and CCDs is performed on an as-needed basis in accordance withmanufacturer’s instructions and facility/unit-specific protocols. The appropriate intervention depends on the complicationencountered (for details, see How to Troubleshoot Problems When Caring for a Patient with a Chest Tube and ClosedChest Drain, below). Nursing management of the patient with a CT and CCD includes–recognizing the complication with the CT/CCD–evaluating the possible causes of the complication–determining the appropriate intervention, within the scope of nursing practice–informing the treating clinician, as necessary–implementing strategies to correct the complication
• Where: Troubleshooting complications with CTs and CCDs is undertaken in all patient care settings where these devicesare used (e.g., the ICU, emergency department, medical-surgicalunits)
• Who: Registered nurses are primarily responsible for providing the daily care of CTs and CCDs; care cannot be delegatedto assistive personnel. Family members can typically be present when a nurse is troubleshooting a CT and CCD
What is the Desired Outcome of Troubleshooting Problems with Chest Tubes andClosed Chest Drains?› The desired outcome of troubleshooting problems with CTs and CCDs is to prevent interruption in therapy and/or minimize
the impact of related complications
Why is Troubleshooting Problems with Chest Tubes and Closed Chest DrainsImportant?› Complications with CTs and CCDs range from minor to life-threatening . Any complications that prevent air, blood, and/
or fluid from being evacuated from the intrapleural space or mediastinum can result in respiratory and/or cardiovascularcomplications, including tension pneumothorax, cardiac tamponade (i.e., an acute effusion in which the pericardial sac fillswith blood and impedes normal heart function), hypotension, impaired cardiac output, cardiac arrest, and death• A tension pneumothorax is considered a medical emergency because air continues to flow into the parietal space with
inspiration but cannot escape with expiration; tension pneumothorax can result in thoracic hyperexpansion, displacement ofthe mediastinum toward the opposite side of the thorax (called a mediastinal shift), and decreased cardiac output (for moreinformation, see Nursing Practice & Skill ... Pneumothorax: Caring for the Patient with )
Facts and Figures› One retrospective study sought to examine the frequency of retained blood syndrome (RBS) and associated morbidity, and
to determine how a preventativeactive chest tube clearance (ATC) protocol influences patient outcomes. Investigators foundthat ATC is associated with a reduced need for interventions for RBS and postoperative atrial fibrillation, underscoring theimportance of maintaining CT patency in the early hours after cardiac surgery (Sirch et al., 2016)
What You Need to Know Before Troubleshooting Problems When Caring for a Patientwith a Chest Tube and a Closed Chest Drain› Before troubleshooting a CT and a CCD, the clinician should be familiar with the following:
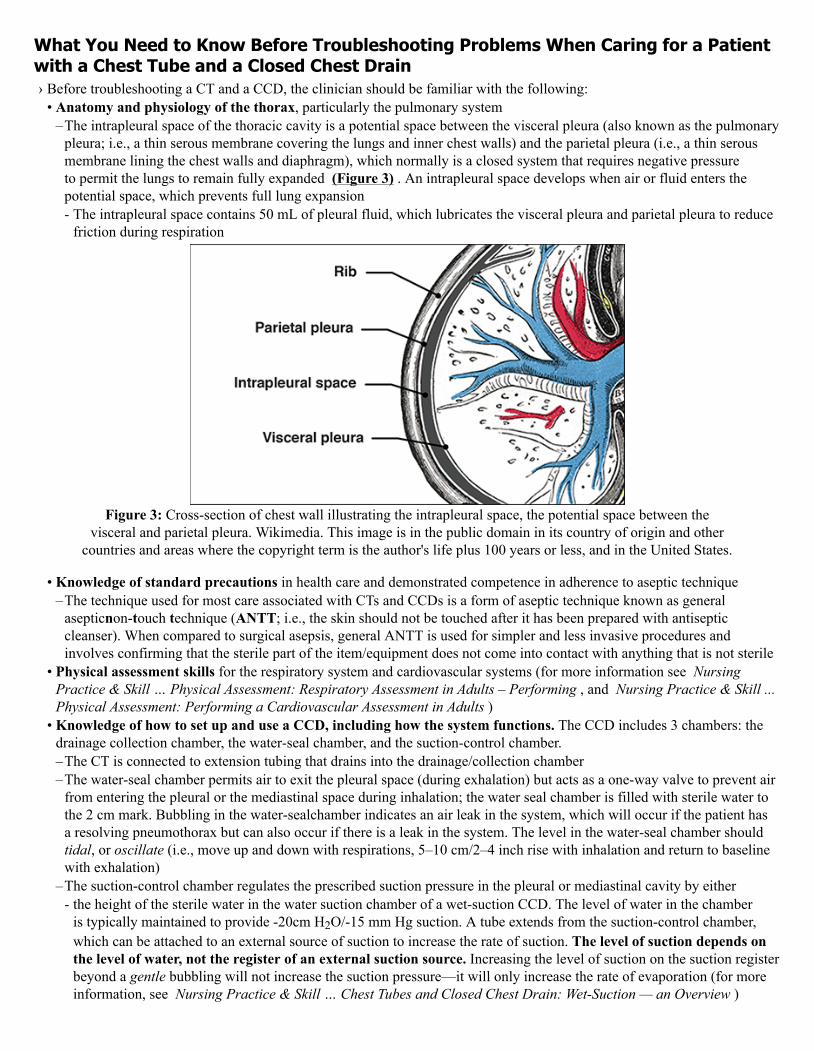
• Anatomy and physiology of the thorax, particularly the pulmonary system–The intrapleural space of the thoracic cavity is a potential space between the visceral pleura (also known as the pulmonary
pleura; i.e., a thin serous membrane covering the lungs and inner chest walls) and the parietal pleura (i.e., a thin serousmembrane lining the chest walls and diaphragm), which normally is a closed system that requires negative pressureto permit the lungs to remain fully expanded (Figure 3) . An intrapleural space develops when air or fluid enters thepotential space, which prevents full lung expansion- The intrapleural space contains 50 mL of pleural fluid, which lubricates the visceral pleura and parietal pleura to reduce
friction during respiration
Figure 3: Cross-section of chest wall illustrating the intrapleural space, the potential space between thevisceral and parietal pleura. Wikimedia. This image is in the public domain in its country of origin and other
countries and areas where the copyright term is the author's life plus 100 years or less, and in the United States.
• Knowledge of standard precautions in health care and demonstrated competence in adherence to aseptic technique–The technique used for most care associated with CTs and CCDs is a form of aseptic technique known as general
asepticnon-touch technique (ANTT; i.e., the skin should not be touched after it has been prepared with antisepticcleanser). When compared to surgical asepsis, general ANTT is used for simpler and less invasive procedures andinvolves confirming that the sterile part of the item/equipment does not come into contact with anything that is not sterile
• Physical assessment skills for the respiratory system and cardiovascular systems (for more information see NursingPractice & Skill … Physical Assessment: Respiratory Assessment in Adults – Performing , and Nursing Practice & Skill ...Physical Assessment: Performing a Cardiovascular Assessment in Adults )
• Knowledge of how to set up and use a CCD, including how the system functions. The CCD includes 3 chambers: thedrainage collection chamber, the water-seal chamber, and the suction-control chamber.–The CT is connected to extension tubing that drains into the drainage/collection chamber–The water-seal chamber permits air to exit the pleural space (during exhalation) but acts as a one-way valve to prevent air
from entering the pleural or the mediastinal space during inhalation; the water seal chamber is filled with sterile water tothe 2 cm mark. Bubbling in the water-sealchamber indicates an air leak in the system, which will occur if the patient hasa resolving pneumothorax but can also occur if there is a leak in the system. The level in the water-seal chamber shouldtidal, or oscillate (i.e., move up and down with respirations, 5–10 cm/2–4 inch rise with inhalation and return to baselinewith exhalation)
–The suction-control chamber regulates the prescribed suction pressure in the pleural or mediastinal cavity by either- the height of the sterile water in the water suction chamber of a wet-suction CCD. The level of water in the chamber
is typically maintained to provide -20cm H2O/-15 mm Hg suction. A tube extends from the suction-control chamber,which can be attached to an external source of suction to increase the rate of suction. The level of suction depends onthe level of water, not the register of an external suction source. Increasing the level of suction on the suction registerbeyond a gentle bubbling will not increase the suction pressure—it will only increase the rate of evaporation (for moreinformation, see Nursing Practice & Skill … Chest Tubes and Closed Chest Drain: Wet-Suction — an Overview )
- the adjustable bellows of the suction-control chamber of the dry-suction CCD. The level of pressure is controlled bya manual or rotary dial that can be adjusted beyond the typical pressure, -20 cm H2O/-15mm Hg. Dry-suction CCDsrequire higher levels of air-flow from an external suction source for efficient drainage. Complications associated withuse of a CT and a CCD range from minor to serious
• CT complications . The CCD might need to be removed and replaced if the unit is damaged (for more information, see Nursing Practice & Skill ... Chest Tubes: Removing . CCD complications are usually related to patency issues (see belowfor discussion). Other management issues involve–positioning of the CCD and tubing—if the CCD is not kept below the level of the patient’s chest, blood and air can be
siphoned back into the chest cavity. CTs should be positioned so they remain straight or coiled for optimal drainage. Donot permit a fluid-filled dependent CT loop, which can change pleural pressures from -18 cmH2O to +8 cmH2O, a changeof 26 cmH2O within minutes (American Association of Critical-CareNurses, 2016; Halm, 2007)
–improper use of external suction to increase the rate of suction pressure. Suction pressure is controlled by the level offluid in the suction chamber, not by the amount of external suction. Excessive external suction increases the rate of fluidevaporation and has no impact on suction pressure
–clamping the tubing—CTs should be clamped for extremely short periods and only when necessary due to the risk fortension pneumothorax
• Acute and late complications–Acute complications are usually related to placement/securement technique or improper CT positioning, such as
- the CT placed too deeply resulting in pain as it abuts the mediastinum or against the pleura- the CT placed too shallowly, or penetrating the diaphragm, abdominal cavity, or subcutaneously so that the CT is
ineffective—CTs should be positioned so all drainage eyelets in the proximal end of the CT are within the thoraciccavity
- the CT placed in abdominal cavity resulting in injury to stomach or colon- injury during CT placement (e.g., hemothorax from laceration of intercostal vessel, lung laceration)- inadequate CT securement resulting in dislodgement or inadvertent removal
–Late complications include- occlusion (e.g., clots within the CT, proximal holes of the CT are blocked with lung tissue—can occur if the CT has
been tracked posteriorly, when it can fall posteriorly and end up wedged in the oblique fissure [i.e., division between theupper and lower lobes of the lungs])
- infection- pneumothorax after removal due to poor technique- retained hemothorax (e.g., clotted blood in the pleural space)—the bacterial contamination of the retained hemothorax
can result in an empyema- break in the closed system, increasing risk of contamination and air entry into the pleural space
• Chest tube patency . Avoid aggressive CT manipulation/compression for the purpose of dislodging blood clots, suchas stripping (i.e., compressing the chest tube with the thumb and forefinger and, with the other hand, using a pullingmotion down the remainder of the tube away from the insertion site) or milking to create bursts of suction (e.g., squeezing,kneading, fan-folding, or twisting) (El-Said et al. 2018; Halm, M.A., 2007)–There is no evidence demonstrating benefit of these practices in maintaining chest tube patency and substantial evidence
exists that the extreme negative pressures, as high as -450cmH2O, can damage pleural tissue, clog chest tube eyelets,increase bleeding, and potentially impact left ventricular function due to increased negative intrathoracic pressure
–If visible clots are observed, anecdotal evidence and “contemporary expert opinion” recommends the practice of gentlesqueezing hand-over-hand along the tubing and release the tubing between squeezes to help move the clots toward thedrain
–PleuraFlow Active Clearance Technology is a device attached to the chest tube that permits nurses to periodically cleanthe entire length of chest tubes with a loop on a guide wire without breaking sterile technique. Literature indicates thatfurther studies are required to establish the best-useprotocols, cost to benefit analysis, and how this technology canimprove outcomes following coronary surgery. Note: This information is presented for educational purposes only withoutendorsement(16)
• Insertion site dressing changes–Do not routinely change CT dressing unless it is compromised or a change in the patient’s condition requires wound
assessment. Frequent access to the CT wound site increased the risk for hospital acquired infection (HAI)
–Use dry, sterile gauze secured with wide paper tape to dress CT insertion sites. Avoid bulky dressings that restrict chestmovement and increase moisture retention
–Petroleum gauze should be avoided due to strong evidence it does not prevent air leaks and causes suture knots used tosecure chest tubes to fail at a significantly higher rate than those not exposed to petroleum gauze
–Wide paper tape is preferred instead of occlusive tape, which increases the risk of medical adhesive-related skin injury(MARSI; i.e., tissue damage from the “peel force” and skin irritation due to the chemical components in the adhesive)
–Secure CTs to the abdominal wall using an omental tag of tape to relieve traction on CT insertion site› Preliminary steps to be taken before caring for a patient with a CT and a CCD include the following:
• Review the facility/unit-specific protocol for troubleshooting problems with a CT and a CCD, if available• Review the treating clinician’s orders regarding care of the CT and CCD (e.g., suction; collection of specimens)• Familiarize yourself with the manufacturer’s instructions for the type of CT/CCD in use• Verify completion of facility informed consent documents, if appropriate• Review the patient’s medical record for
–any allergies (e.g., to latex, medications, or other substances); use alternative materials if appropriate–results of recent chest X-ray to assess CT placement–laboratory test results to check for coagulopathies or blood dyscrasias (e.g., CBC, PTT if the patient is receiving heparin,
or PT if the patient is using warfarin)› Gather the supplies necessary for caring and troubleshooting problems with a CT and a CCD, which typically include
(Figure 4) :• Nonsterile gloves. Other personal protective equipment (PPE; e.g., eye protection, gown, and mask) can be necessary
depending on the patient’s condition or if exposure to body fluids is anticipated• The supplies needed for a specific intervention depend on the cause of the problem to be resolved; however, typical
supplies used when caring for a patient with CTs and CCDs can include:–Adhesive tape (2.5 cm/1 inch in width) to secure connections–Two 20 cm/8-inch curved Pean clamps (i.e., hemostatic clamp with serrations along the entire curved length of the jaw
—padded or with rubber tips). Note: Two clamps or hemostats placed at opposite angles are used when it is necessary tobriefly occlude a CT
–Absorbent pad, optional. Many clinicians use the inner wrap from the CCD as a protective linen cover when changing outthe used CCD for the new unit
–Sterile water–Sterile 4 x 4 split gauze pads–Sterile 4 x 4 gauze pads–Wide paper tape–Facility-approved antiseptic solution–Sterile CCD, if replacing the CCD–Funnel/catheter (for refilling suction-control chamber of CCD) or 60 mL catheter-tipped syringe–Suction set-up (e.g., regulator, canister, tubing, and suction source), if changing out suction equipment
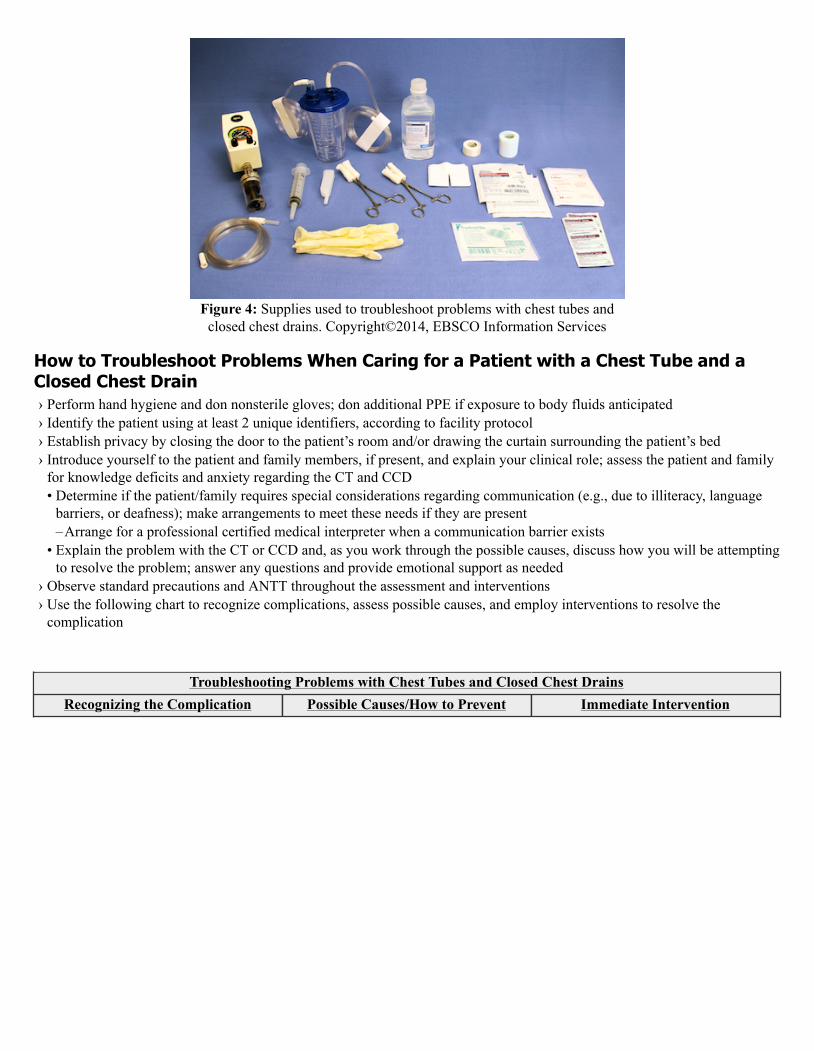
Figure 4: Supplies used to troubleshoot problems with chest tubes andclosed chest drains. Copyright©2014, EBSCO Information Services
How to Troubleshoot Problems When Caring for a Patient with a Chest Tube and aClosed Chest Drain› Perform hand hygiene and don nonsterile gloves; don additional PPE if exposure to body fluids anticipated› Identify the patient using at least 2 unique identifiers, according to facility protocol› Establish privacy by closing the door to the patient’s room and/or drawing the curtain surrounding the patient’s bed› Introduce yourself to the patient and family members, if present, and explain your clinical role; assess the patient and family
for knowledge deficits and anxiety regarding the CT and CCD• Determine if the patient/family requires special considerations regarding communication (e.g., due to illiteracy, language
barriers, or deafness); make arrangements to meet these needs if they are present–Arrange for a professional certified medical interpreter when a communication barrier exists
• Explain the problem with the CT or CCD and, as you work through the possible causes, discuss how you will be attemptingto resolve the problem; answer any questions and provide emotional support as needed
› Observe standard precautions and ANTT throughout the assessment and interventions› Use the following chart to recognize complications, assess possible causes, and employ interventions to resolve the
complication
.Troubleshooting Problems with Chest Tubes and Closed Chest Drains
Recognizing the Complication Possible Causes/How to Prevent Immediate Intervention
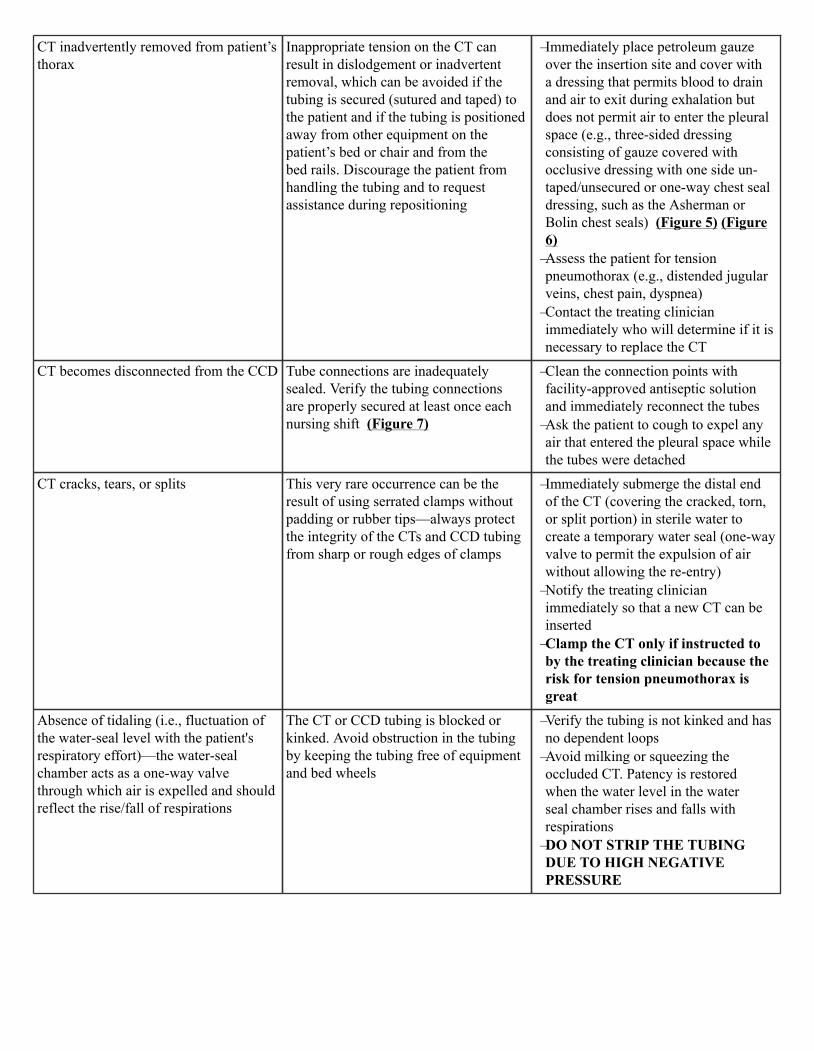
CT inadvertently removed from patient’sthorax
Inappropriate tension on the CT canresult in dislodgement or inadvertentremoval, which can be avoided if thetubing is secured (sutured and taped) tothe patient and if the tubing is positionedaway from other equipment on thepatient’s bed or chair and from thebed rails. Discourage the patient fromhandling the tubing and to requestassistance during repositioning_
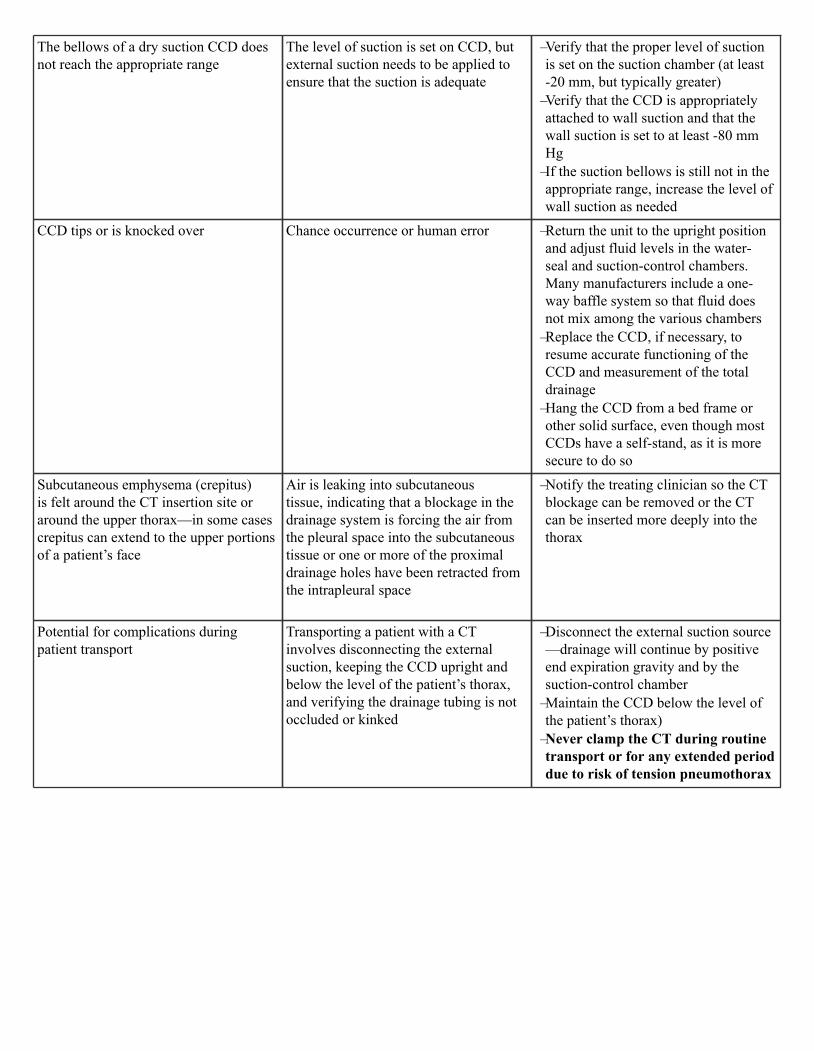
–Immediately place petroleum gauzeover the insertion site and cover witha dressing that permits blood to drainand air to exit during exhalation butdoes not permit air to enter the pleuralspace (e.g., three-sided dressingconsisting of gauze covered withocclusive dressing with one side un-taped/unsecured or one-way chest sealdressing, such as the Asherman orBolin chest seals) (Figure 5) (Figure6)
–Assess the patient for tensionpneumothorax (e.g., distended jugularveins, chest pain, dyspnea)
–Contact the treating clinicianimmediately who will determine if it isnecessary to replace the CT
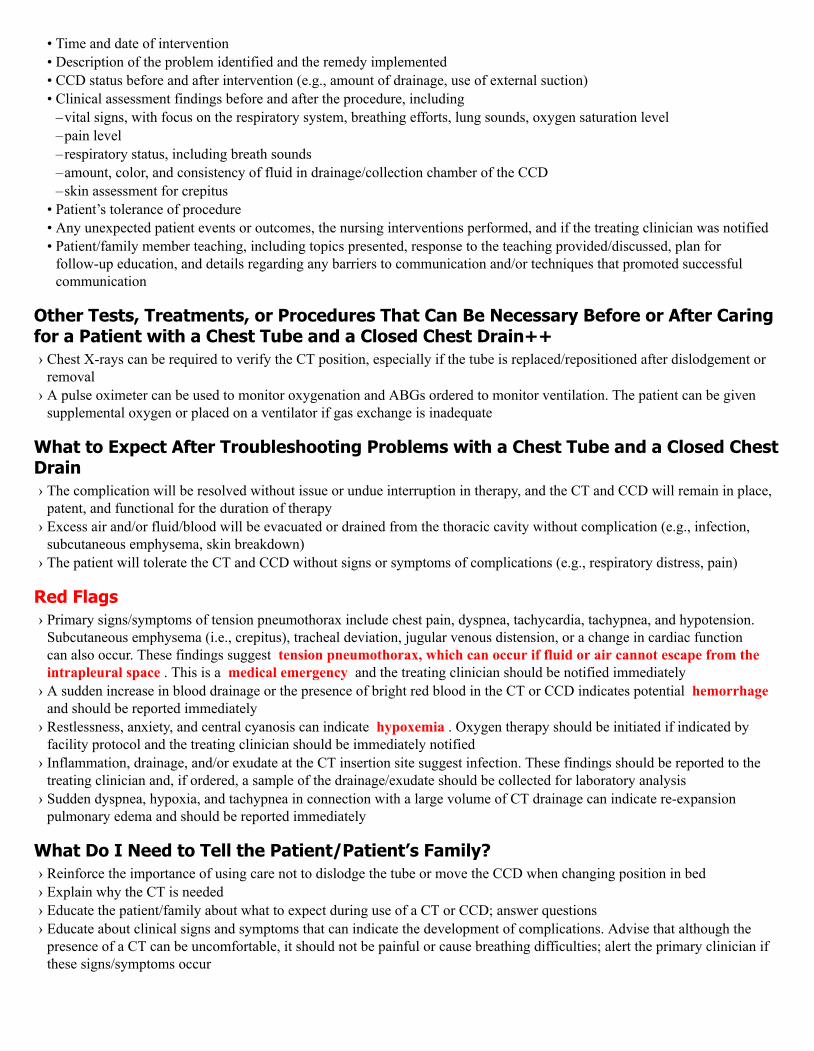
CT becomes disconnected from the CCD Tube connections are inadequatelysealed. Verify the tubing connectionsare properly secured at least once eachnursing shift (Figure 7)_
–Clean the connection points withfacility-approved antiseptic solutionand immediately reconnect the tubes
–Ask the patient to cough to expel anyair that entered the pleural space whilethe tubes were detached
CT cracks, tears, or splits This very rare occurrence can be theresult of using serrated clamps withoutpadding or rubber tips—always protectthe integrity of the CTs and CCD tubingfrom sharp or rough edges of clamps_
–Immediately submerge the distal endof the CT (covering the cracked, torn,or split portion) in sterile water tocreate a temporary water seal (one-wayvalve to permit the expulsion of airwithout allowing the re-entry)
–Notify the treating clinicianimmediately so that a new CT can beinserted
–Clamp the CT only if instructed toby the treating clinician because therisk for tension pneumothorax isgreat
Absence of tidaling (i.e., fluctuation ofthe water-seal level with the patient'srespiratory effort)—the water-sealchamber acts as a one-way valvethrough which air is expelled and shouldreflect the rise/fall of respirations
The CT or CCD tubing is blocked orkinked. Avoid obstruction in the tubingby keeping the tubing free of equipmentand bed wheels_
–Verify the tubing is not kinked and hasno dependent loops
–Avoid milking or squeezing theoccluded CT. Patency is restoredwhen the water level in the waterseal chamber rises and falls withrespirations
–DO NOT STRIP THE TUBINGDUE TO HIGH NEGATIVEPRESSURE
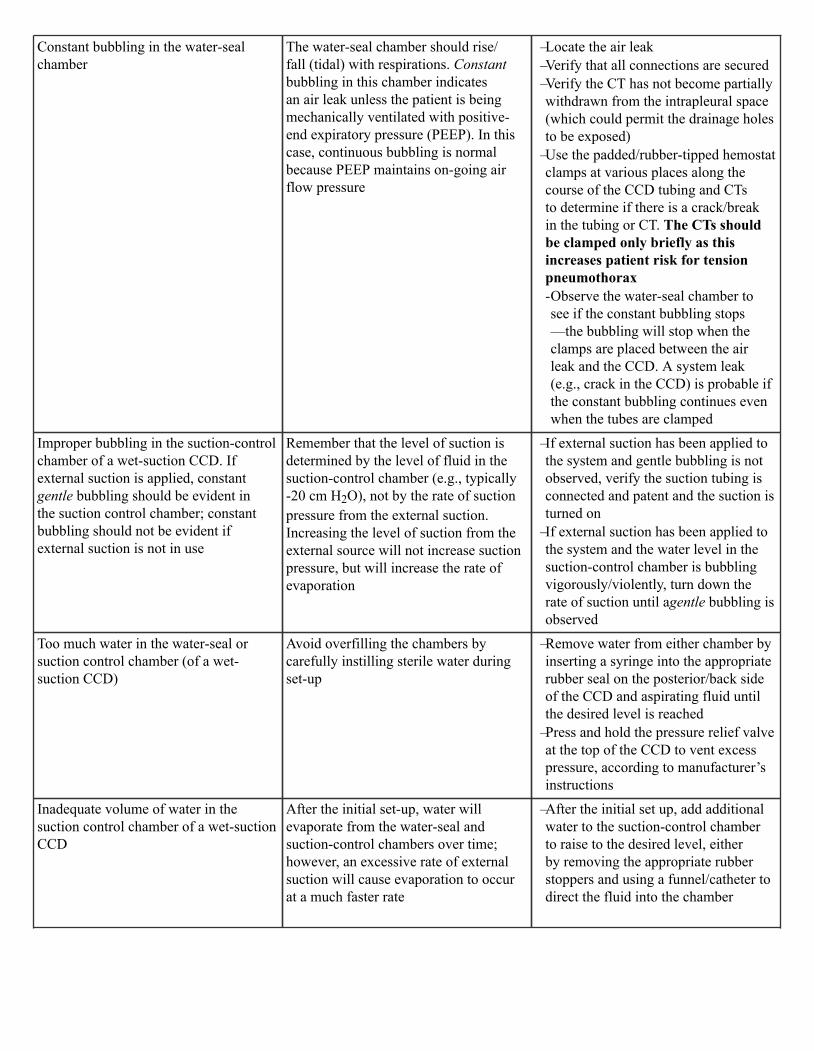
Constant bubbling in the water-sealchamber
The water-seal chamber should rise/fall (tidal) with respirations. Constantbubbling in this chamber indicatesan air leak unless the patient is beingmechanically ventilated with positive-end expiratory pressure (PEEP). In thiscase, continuous bubbling is normalbecause PEEP maintains on-going airflow pressure_
–Locate the air leak–Verify that all connections are secured–Verify the CT has not become partiallywithdrawn from the intrapleural space(which could permit the drainage holesto be exposed)
–Use the padded/rubber-tipped hemostatclamps at various places along thecourse of the CCD tubing and CTsto determine if there is a crack/breakin the tubing or CT. The CTs shouldbe clamped only briefly as thisincreases patient risk for tensionpneumothorax-Observe the water-seal chamber tosee if the constant bubbling stops—the bubbling will stop when theclamps are placed between the airleak and the CCD. A system leak(e.g., crack in the CCD) is probable ifthe constant bubbling continues evenwhen the tubes are clamped
Improper bubbling in the suction-controlchamber of a wet-suction CCD. Ifexternal suction is applied, constantgentle bubbling should be evident inthe suction control chamber; constantbubbling should not be evident ifexternal suction is not in use
Remember that the level of suction isdetermined by the level of fluid in thesuction-control chamber (e.g., typically-20 cm H2O), not by the rate of suctionpressure from the external suction.Increasing the level of suction from theexternal source will not increase suctionpressure, but will increase the rate ofevaporation_
–If external suction has been applied tothe system and gentle bubbling is notobserved, verify the suction tubing isconnected and patent and the suction isturned on
–If external suction has been applied tothe system and the water level in thesuction-control chamber is bubblingvigorously/violently, turn down therate of suction until agentle bubbling isobserved
Too much water in the water-seal orsuction control chamber (of a wet-suction CCD)
Avoid overfilling the chambers bycarefully instilling sterile water duringset-up_
–Remove water from either chamber byinserting a syringe into the appropriaterubber seal on the posterior/back sideof the CCD and aspirating fluid untilthe desired level is reached
–Press and hold the pressure relief valveat the top of the CCD to vent excesspressure, according to manufacturer’sinstructions
Inadequate volume of water in thesuction control chamber of a wet-suctionCCD
After the initial set-up, water willevaporate from the water-seal andsuction-control chambers over time;however, an excessive rate of externalsuction will cause evaporation to occurat a much faster rate_
–After the initial set up, add additionalwater to the suction-control chamberto raise to the desired level, eitherby removing the appropriate rubberstoppers and using a funnel/catheter todirect the fluid into the chamber
The bellows of a dry suction CCD doesnot reach the appropriate range
The level of suction is set on CCD, butexternal suction needs to be applied toensure that the suction is adequate_
–Verify that the proper level of suctionis set on the suction chamber (at least-20 mm, but typically greater)
–Verify that the CCD is appropriatelyattached to wall suction and that thewall suction is set to at least -80 mmHg
–If the suction bellows is still not in theappropriate range, increase the level ofwall suction as needed
CCD tips or is knocked over Chance occurrence or human error_
–Return the unit to the upright positionand adjust fluid levels in the water-seal and suction-control chambers.Many manufacturers include a one-way baffle system so that fluid doesnot mix among the various chambers
–Replace the CCD, if necessary, toresume accurate functioning of theCCD and measurement of the totaldrainage
–Hang the CCD from a bed frame orother solid surface, even though mostCCDs have a self-stand, as it is moresecure to do so
Subcutaneous emphysema (crepitus)is felt around the CT insertion site oraround the upper thorax—in some casescrepitus can extend to the upper portionsof a patient’s face
Air is leaking into subcutaneoustissue, indicating that a blockage in thedrainage system is forcing the air fromthe pleural space into the subcutaneoustissue or one or more of the proximaldrainage holes have been retracted fromthe intrapleural space_
–Notify the treating clinician so the CTblockage can be removed or the CTcan be inserted more deeply into thethorax
Potential for complications duringpatient transport
Transporting a patient with a CTinvolves disconnecting the externalsuction, keeping the CCD upright andbelow the level of the patient’s thorax,and verifying the drainage tubing is notoccluded or kinked_
–Disconnect the external suction source—drainage will continue by positiveend expiration gravity and by thesuction-control chamber
–Maintain the CCD below the level ofthe patient’s thorax)
–Never clamp the CT during routinetransport or for any extended perioddue to risk of tension pneumothorax
.
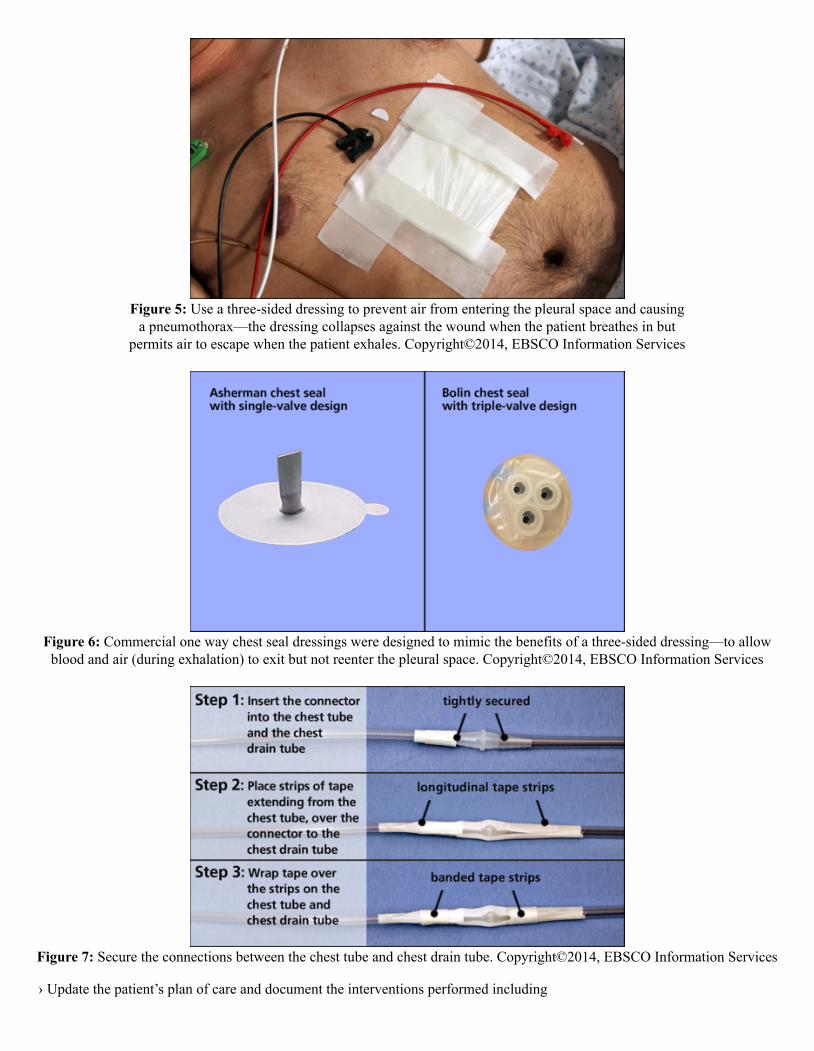
Figure 5: Use a three-sided dressing to prevent air from entering the pleural space and causinga pneumothorax—the dressing collapses against the wound when the patient breathes in but
permits air to escape when the patient exhales. Copyright©2014, EBSCO Information Services
Figure 6: Commercial one way chest seal dressings were designed to mimic the benefits of a three-sided dressing—to allowblood and air (during exhalation) to exit but not reenter the pleural space. Copyright©2014, EBSCO Information Services
Figure 7: Secure the connections between the chest tube and chest drain tube. Copyright©2014, EBSCO Information Services
› Update the patient’s plan of care and document the interventions performed including
• Time and date of intervention• Description of the problem identified and the remedy implemented• CCD status before and after intervention (e.g., amount of drainage, use of external suction)• Clinical assessment findings before and after the procedure, including
–vital signs, with focus on the respiratory system, breathing efforts, lung sounds, oxygen saturation level–pain level–respiratory status, including breath sounds–amount, color, and consistency of fluid in drainage/collection chamber of the CCD–skin assessment for crepitus
• Patient’s tolerance of procedure• Any unexpected patient events or outcomes, the nursing interventions performed, and if the treating clinician was notified• Patient/family member teaching, including topics presented, response to the teaching provided/discussed, plan for
follow-up education, and details regarding any barriers to communication and/or techniques that promoted successfulcommunication
Other Tests, Treatments, or Procedures That Can Be Necessary Before or After Caringfor a Patient with a Chest Tube and a Closed Chest Drain++› Chest X-rays can be required to verify the CT position, especially if the tube is replaced/repositioned after dislodgement or
removal› A pulse oximeter can be used to monitor oxygenation and ABGs ordered to monitor ventilation. The patient can be given
supplemental oxygen or placed on a ventilator if gas exchange is inadequate
What to Expect After Troubleshooting Problems with a Chest Tube and a Closed ChestDrain› The complication will be resolved without issue or undue interruption in therapy, and the CT and CCD will remain in place,
patent, and functional for the duration of therapy› Excess air and/or fluid/blood will be evacuated or drained from the thoracic cavity without complication (e.g., infection,
subcutaneous emphysema, skin breakdown)› The patient will tolerate the CT and CCD without signs or symptoms of complications (e.g., respiratory distress, pain)
Red Flags› Primary signs/symptoms of tension pneumothorax include chest pain, dyspnea, tachycardia, tachypnea, and hypotension.
Subcutaneous emphysema (i.e., crepitus), tracheal deviation, jugular venous distension, or a change in cardiac functioncan also occur. These findings suggest tension pneumothorax, which can occur if fluid or air cannot escape from theintrapleural space . This is a medical emergency and the treating clinician should be notified immediately
› A sudden increase in blood drainage or the presence of bright red blood in the CT or CCD indicates potential hemorrhage and should be reported immediately
› Restlessness, anxiety, and central cyanosis can indicate hypoxemia . Oxygen therapy should be initiated if indicated byfacility protocol and the treating clinician should be immediately notified
› Inflammation, drainage, and/or exudate at the CT insertion site suggest infection. These findings should be reported to thetreating clinician and, if ordered, a sample of the drainage/exudate should be collected for laboratory analysis
› Sudden dyspnea, hypoxia, and tachypnea in connection with a large volume of CT drainage can indicate re-expansionpulmonary edema and should be reported immediately
What Do I Need to Tell the Patient/Patient’s Family?› Reinforce the importance of using care not to dislodge the tube or move the CCD when changing position in bed› Explain why the CT is needed› Educate the patient/family about what to expect during use of a CT or CCD; answer questions› Educate about clinical signs and symptoms that can indicate the development of complications. Advise that although the
presence of a CT can be uncomfortable, it should not be painful or cause breathing difficulties; alert the primary clinician ifthese signs/symptoms occur

References1. American Association of Critical Care Nurses (AACN). (2016). Evidence-based care of patients with chest tubes. 2016 AACN National Teaching Institute ExpoEd. Retrieved
August 17, 2018, from http://www.atriummed.com/EN/chest_drainage/Documents/NTI%202016.pdf (RV)
2. British Thoracic Society Pleural Disease Guideline Group: BTS pleural disease guideline 2010. (2010). Thorax, 65(Suppl II), ii1-ii76. doi:10.1136/thx.2010.13702 (RV)
3. Chotai, P., & Feliz, A. (2018, April 26). Tube thoracostomy management. Medscape. Retrieved June 5, 2018, fromhttps://emedicine.medscape.com/article/1503275-overview#a01 (GI)
4. Cone, K. J. (2014). Closed chest drainage sytems. In A. G. Perry, P. A. Potter, & W. R. Ostendorf (Eds.), Clinical nursing skills and techniques (8th ed., pp. 655-668). St. Louis,MO: Elsevier Mosby. (PP)
5. El-Said, A., & El-sol, H. (2018). Nursing practices: Troubleshooting thoracostomy tube management. International Journal of Academic Research and Development, 3(2),252-257. (RV)
6. Halm, M. A. (2007). To strip or not to strip? Physiological effects of chest tube manipulation. American Journal of Critical Care, 16(6), 609-612. (RV)
7. Hitchcock, J., & Savine, L. (2017). Medical adhesive-related skin injuries associated with vascular access. British Journal of Nursing, 26(8), S4-S12. doi:10.12968/bjon.2017.26.8.S4 (RV)
8. Jeffries, M., Gryglik, C., Davies, D., & Knoll, S. (2013). Chest tube dressings: outcomes of taking petroleum-based dressings out of the equation on air leak and infection rates.American Journal of Critical Care, 22(3), e28. doi:10.4037/ajcc2013279 (R)
9. Makic, M. B., Rauen, C., Jones, K., & Fisk, A. C. (2015). Continuing to challenge practice to be evidence based. Critical Care Nurse, 35(2), 39-50. doi:10.4037/ccn2015693 (R)
10. Mao, M., Hughes, R., Papadimos, T. J., & Stawicki, S. P. (2015). Complications of chest tubes: a focused clinical synopsis. Current Opinion in Pulmonary Medicine, 21(4),346-386. doi:10.1097/MCP.0000000000000169 (RV)
11. Pickett, J. D. (2017). Closed chest drainage system. In D. L. Wiegand (Ed.), AACN procedure manual for high acuity, progressive, and critical care (7th ed., pp. 195-205). StLouis, MO: Elsevier. (GI)
12. Sirch, J., Ledwon, M., Püski, T., Boyle, E. M., Pfeiffer, S., & Fischlein, T. (2016). Active clearance of chest drainage catheters reduces retained blood. The Journal of Thoracicand Cardiovascular Surgery, 151(3). doi:10.1016/j.jtcvs.2015.10.015 (R)
13. Teleflex Incorporated. (n.d.). Chest drainage as a therapeutic intervention: Chest drainage systems. Retrieved June 1, 2018, from http://www.teleflex.com/en/usa/ucd/chest_drainage_systems.php (GI)
14. Teleflex Incorporated. (n.d.). Chest drainage as a therapeutic intervention: Nursing considerations and troubleshooting. Retrieved June 1, 2018, from http://www.teleflex.com/en/usa/ucd/nursing_considerations_troubleshooting.php (GI)
15. Upton, D. A. (2009). Chest-drainage devices: Atrium. In J. A. Proehl (Ed.), Emergency nursing procedures (4th ed., pp. 214-218). St. Louis, MO: Elsevier Saunders. (GI)
16. Vistarini, N., Gabrysz-Forget, B. S., Beauliueu, Y., & Perrault, L. P. (2016). Tamponade relief by active clearance of chest tubes. Annals of Thoracic Surgery, 101(3),1159-1163. doi:10.1016/j.athoracsur.2015.10.098 (R)
17. Windemuth, B. (2014). Respiratory function and therapy. In S.M. Nettina (Ed.), Lippincott manual of nursing practice (10th ed., pp. 268-275). Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins. (GI)
18. Wynne, R. (2004). Effect of three wound dressings on infection, healing comfort, and cost in patients with sternotomy wounds: A randomized trial. Chest, 125(1), 43-49. (RCT)