tuberculosis richard moriarty, md umass medical school
TRANSCRIPT

Tuberculosis
Richard Moriarty, MD
UMass Medical School
“Yet the captain of all these men of death that came against him
to take him away was consumption, for it was that that brought him down to the grave.”
John Bunyan 1680
Tuberculosis
• 1/3 of world’s population is infected
• 2nd most common ID cause of death
• 8 million new cases every year
• 2 million deaths annually
• Sub-Saharan Africa highest rate 290/100,000
• 2004 Liberia incidence 310/100,000

Tuberculosis in Children
• 500,000 children die annually from TB
• Children more likely to develop TB once infected and are more vulnerable to disseminated TB
• Children get infected from adults
• Children with TB / latent TB infection (LTBI) indicate recent TB transmission
• Report 2 groups: 0-4 and 5-14

TB – The Bacterium
• Mycobacterium tuberculosis
• Aerobic, non-motile, non-spore forming
• Persists for long periods of time
• Waxy fatty capsule
• Slow-growing

TB Transmission
• Droplet nuclei 1-5 um
• Aerosolized by talking, singing, sighing, coughing, sneezing, yelling
• Inhaled into alveoli
• Only 1-5 bacilli needed to cause infection

TB – Primary Infection
• Multiply in macrophages
• Lyse macrophages and spread to surrounding cells and regional lymph nodes (Ghon complex)
• Initial CMI and DHS response prevents spread but takes 6 weeks to develop
• Residual bacilli persist
• 5-10% will develop disease later in life



TB - Symptoms
• Many children are asymptomatic• Low grade fevers• Weight loss or poor weight gain• Primary focus usually in the lungs• Chronic cough, wheezing• 25-35% present with lymphadenitis• 13% present with meningitis• Miliary

TB Findings in Non-pulmonary foci
• gibbus, especially of recent onset • non-painful enlarged cervical lymphadenopathy with
with or without fistula formation;• meningitis not responding to antibiotic treatment,
with a subacute onset or raised intracranial pressure• pleural effusion• distended abdomen with ascites• non-painful enlarged joint• signs of tuberculin hypersensitivity (e.g.
phlyctenular conjunctivitis, erythema nodosum)

TB SUSPICION INDICATOR TABLE
FeatureScore
Cough > 4 weeks (not whooping cough) ORPneumonia that does not improve after 3 weeks of treatment
11
Fever lasting 2 weeks or more without explained cause 1
Not recovering from measles after 2 months 2
Child < 3 years old not gaining weight appropriately for 3 months ORChild > 3 years old with a regression of the general condition (not gaining weight appropriately or losing weight)
12
No recovering from malnutrition on treatment ORNo recovering from a severe malnutrition (hospitalised)
12
Co-dweller with sputum (afb+) ORMother (or caregiver) sputum (afb+)
24
BCG done during the last 2 years -1
If you get: 0-2 = TB less likely3-4 = TB more likely5 or more = TB likely

TB - Diagnosis
• Careful history
• Clinical examination with growth assessment
• Tuberculin skin testing
• Bacteriological confirmation whenever possible
• HIV testing (in high HIV prevalence areas)
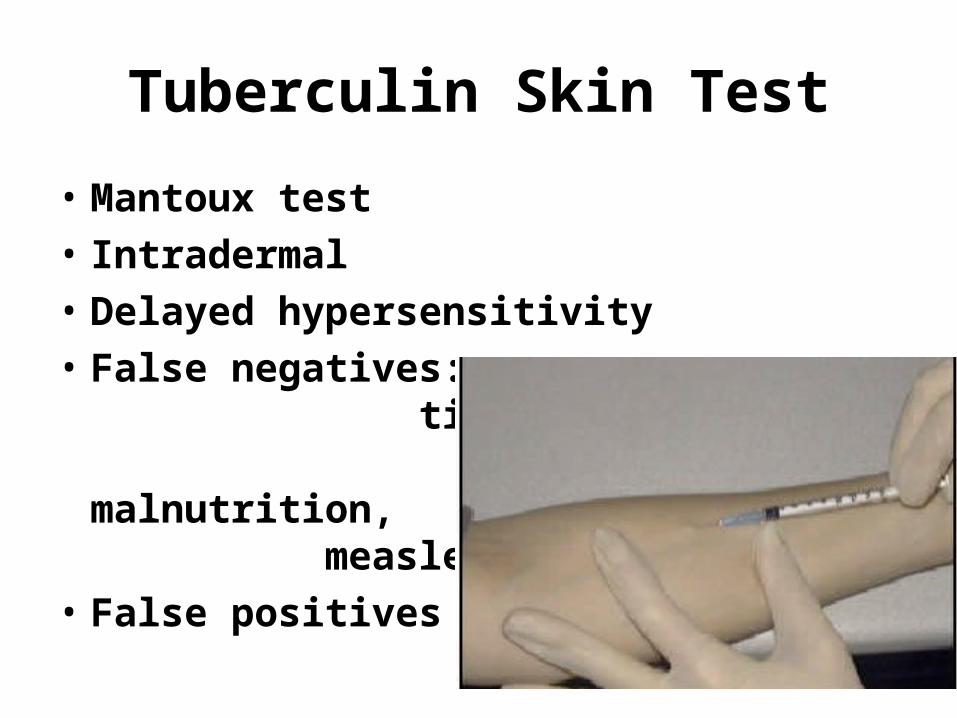
Tuberculin Skin Test
• Mantoux test
• Intradermal
• Delayed hypersensitivity
• False negatives: time, malnutrition, measles,
• False positives


Bacteriologic confirmation whenever possible
• Sputum
• Gastric aspirate

Auramine O fluorescent stain for TB

HIV counselling and testing is indicated for all TB patients as
part of their routinemanagement.

TB – Goals of Treatment
• Kill actively growing and semi-dormant bacilli
• Eliminate residual bacilli
• Insure cure without relapse
• Prevent death
• Stop transmission
• Prevent emergence of drug resistance

TB – Treatment of Children
• Children tolerate meds well
• Directly observed therapy (DOT) is the gold standard
• Extended treatment necessary for slow-growing organism
• Irregular or incomplete treatment leads to multi-drug-resistant TB
• Contact tracing is key

TB - Treatment
• Isoniazid
• Rifampin
• Pyrazinamide
• Ethambutol

Advanced Search
First-Line Treatment of Tuberculosis (TB) for Drug-sensitive TB
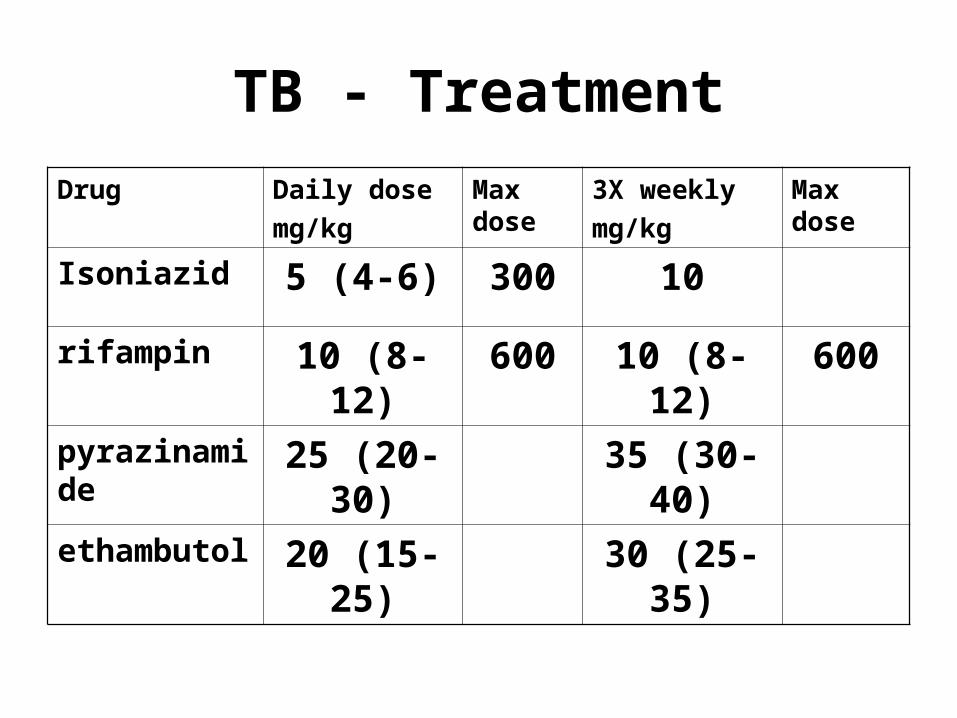
TB - Treatment
Drug Daily dose
mg/kg
Max dose
3X weekly
mg/kg
Max dose
Isoniazid 5 (4-6) 300 10
rifampin 10 (8-12) 600 10 (8-12) 600
pyrazinamide
25 (20-30) 35 (30-40)
ethambutol 20 (15-25) 30 (25-35)

TB – Duration of Therapy
Type of infection
Intensive phase
Continuation phase
New – smear negative
2 HRZ 4 HR or 4 HE
New – smear positive
2 HRZE 4 HR or 6 HE
TB meningitis 2 HRZS 4 HR
Relapse or rx after interruption
2 HRZES / 1 HRZE
5 HRE
BCG Vaccine
• M. bovis – 13 years of serial passage• Different strains around the globe• 50% efficacy; better against miliary and
meningeal TB• No protective effect after 10 years• Complications: adenitis, drainage,
disseminated disease• No additional protection from revaccination• May cause positive skin test
TB-HIV Coinfection
• PPD skin test may be negative
• Be sure of diagnosis – rule out other causes of pneumonia: bacterial, viral, PCP, LIP
• Begin TB treatment first
• Start ART therapy 2-8 weeks after TB rx
• INH preventive therapy if exposed to TB


References
• WHO 2006 Guidance for national tuberculosis programmes on the management of tuberculosis in children
• www.tuberculosistextbook.com