tuberculosis exposure control plan for long term care...
TRANSCRIPT
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 1
Oregon Guidelines
TUBERCULOSIS EXPOSURE CONTROL PLAN For
LONG TERM CARE FACILITIES FOR THE ELDERLY
November 2002 Approved: Evelyn Lancaster, R.N., B.S.N. Mark Loveless, M.D. TB Controller Medical Epidemiologist Oregon Health Services HIV/STD/TB Programs Oregon Health Services Prepared In consultation with:
• Robert Preston, MS, Geriatric Infection Control Consultant • Linda Kirshbaum, BS, NHA, Oregon Health Care Association • Margaret Carley, RN, JD, Oregon Health Care Association • Suzanne Banda, PHN, MPH Oregon TB Nurse Consultant • James Marx, R.N., M.S., C.I.C., Infection Control & Epidemiology
Consultant • Jean Adams, L.V.N., Infection Control Coordinator and Director of Staff
Development for Castle Manor • Virginia Gothard, R.N., Infection Control Coordinator for Friendship
Manor
NOTE: No set of guidelines can cover all individual situations which can and will arise. Thus when questions on individual situations not covered by these guidelines do arise, consult with your local health department Tuberculosis Control program for further information.

Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 2
A. Purpose, Goal, and How to Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-4 B. TB Control Plan 1. TB Risk Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 2. Surveillance / Screening for Infection a. Diagnosis of Infection............................................................................................ 12 (1) Residents ......................................................................................................... 12 (2) Staff and Volunteers......................................................................................... 15 b. Reporting............................................................................................................... 17
3. Containment / Screening for Active TB Disease
a. Resident with a Negative Tuberculin Skin Test ...................................................... 17 b. Resident with a Positive Tuberculin Skin Test ....................................................... 18
c. Staff/Volunteers...................................................................................................... 20 d. Isolation ................................................................................................................. 20
e. Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 f. Investigation of Contacts......................................................................................... 21 4. Assessment ............................................................................................................. 22 5. Education ............................................................................................................... 22 C. Attachments:
A. Guidelines for Interpretation of TB Skin Test Reactions in Oregon . . . . . . . . . . 23 B. Two-Step Tuberculin Skin Tests (Mantoux) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 C. BCG Information Sheet . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 D. Resident Annual Tuberculosis Screening Questionnaire . . . . . . . . . . . . . . . . . . . 27 E. Employee Annual Tuberculosis Screening Questionnaire . . . . . . . . . . . . . . . . . . 29 F. Investigation for Contacts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30 G. Sample post positive TST evaluation forms (3 - staple together as a packet) . . . 33 H. Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36 I. Sample staff TB training preview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 3
PURPOSE This document has been produced to provide standard tuberculosis (TB) screening and surveillance guidelines for facilities licensed as Long Term Care Facilities for the Elderly in Oregon. It is designed to be consistent with OARs 333-019-0041 and is based on local TB epidemiology and follows the Centers for Disease Control and Prevention guidelines:
- Prevention and Control of Tuberculosis in Facilities Providing Long Term Care to the Elderly, 1990, MMWR; Vol 39 No. RR-10, and - Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health-Care Facilities, 1994 MMWR October 28, 1994; Vol.43 No. RR-13); pages 1-132.
Adult foster care homes, board and care homes, other residential and congregate settings, who are not licensed as Long Term Care Facilities for the Elderly, are not required by Oregon rule 333-019-0041 to screen for tuberculosis. In the rare event that an exposure may occur, the facility should follow the case management and contact follow-up recommendations from the local health department. Some facilities may have other rules or regulations regarding TB screening and should contact the agency that requires the screening to obtain direction in complying with those regulations. Facilities who plan to provide care for infectious tuberculosis patients on-site should insert procedures and policies for managing infectious tuberculosis patients into these guidelines.
GOAL It is the goal of all long term care facilities to assure that appropriate tuberculosis prevention and control activities are undertaken to protect residents and staff. The Infection Control Committee is responsible for implementation of the facility’s TB Control Plan. Each facility should assign an appropriate member to oversee implementation of the TB Control activities of risk assessment, surveillance, containment, assessment, and education. There are five elements to the TB Control Plan: 1. Risk Assessment
Annually, each facility should evaluate their TB risk for transmission of M.TB. The results of this assessment will guide the extent to which the other components are followed.
2. Surveillance: Identifying and reporting all cases of TB in the facility, and identify infected residents and staff.
3. Containment: Screening for disease and ensuring that transmission of TB is stopped promptly.
4. Assessment: Monitoring and evaluating surveillance and containment activities of the facility.
5. Education: Providing information and imparting skills to staff, patients, and visitors so that they understand and cooperate with appropriate TB Control Activities.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 4
How to Use this document:
1. Determine your facility’s TB risk - see Section 1. TB Risk Assessment
a. Complete the TB Surveillance / Risk Assessment Record for the last year.
The number of cases in the county and in your facility last year determine your TB risk category (listed below).
b. Select the appropriate “TB Control Plan Summary for the Year ____”
1) Minimal Risk = No TB in county and facility did not have any TB cases in last year.
2) Very Low Risk = TB is reported in the county, but no TB cases occurred in facility last year.
3) Low or Intermediate Risk = TB is reported in the county, and TB cases occurred in facility last year.
(If unsure if there were cases in your county, call your local health department or look online at: www.healthoregon.org/tb )
2. Fill in the date each element/activity was completed or reviewed and by who.
3. Review your TB control plan to make sure your policies are consistent for your type of facility and the guidelines.
a. TB Control Plan reviewed
b. TB Education & Training of Staff is scheduled / performed
c. Screening of Staff (HCWs): policy is current
d. Screening of Residents: policy is current
e. Reporting: have a plan for reporting if needed
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 5
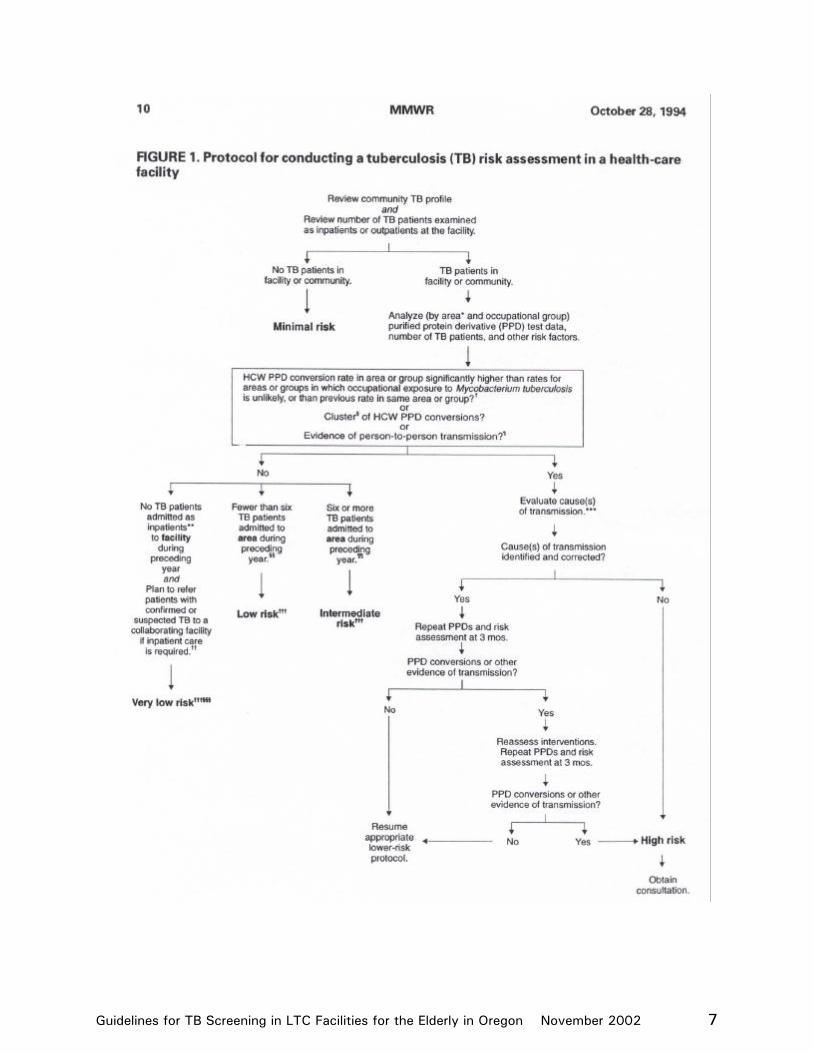
1. TB RISK ASSESSMENT The purpose of the TB risk assessment is to evaluate the actual risk of TB transmission for a particular facility. Facilities should keep a record of the following information for both staff and residents each year: • the number of TST reactors (+ TST who are not currently considered converters), • the number of TST conversions1, and • the number of cases of active TB diagnosed • the number of TB cases in the community (county), and • TB drug resistance patterns for the State. Each year, the designated staff person can check with the Local Health Department or the Oregon Health Services TB Control web page (www.healthoregon.org/tb) for the most current year’s reported active TB and resistance data. Final case counts are reported by county; however, are not available before April of the following year (e.g./ the case count for 2000 will not be available before April of 2001). Facilities can use the TB Surveillance / Risk Assessment Record (see next page) to enter this data and determine the TB risk status for their facility annually. For the TB Surveillance / Risk Assessment Record:
1. Obtain the “community profile” data. 2. Enter Mantoux Test and active TB Disease information from your facility. 3. Determine the TB risk category which matches your facility’s risk category.
1) Minimal Risk =
No TB in county and
facility did not have any TB cases in last year.
2) Very Low Risk =
TB is reported in the county, however
no TB cases occurred in facility last year.
3) Low or Intermediate Risk =
TB is reported in the county, and
TB cases occurred in facility last year.
4) High Risk = Ongoing transmission
Most facilities in Oregon will be Minimal or Very Low Risk categories.
1 Conversion= written documentation of a change in TST result from a negative to a positive within the last 2 years, AND the reaction increased in size by at least 10mm induration.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 6
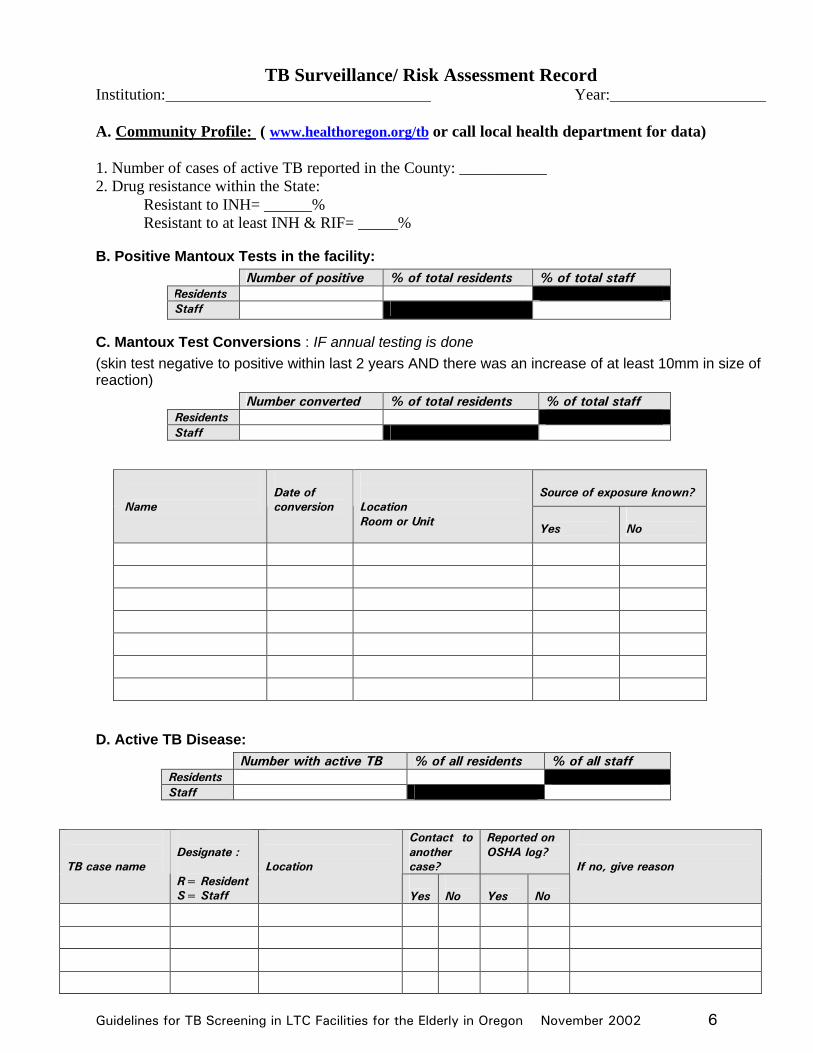
TB Surveillance/ Risk Assessment Record Institution: Year: A. Community Profile: ( www.healthoregon.org/tb or call local health department for data) 1. Number of cases of active TB reported in the County: ___________ 2. Drug resistance within the State:
Resistant to INH= ______% Resistant to at least INH & RIF= _____%
B. Positive Mantoux Tests in the facility: Number of positive % of total residents % of total staff
Residents Staff
C. Mantoux Test Conversions : IF annual testing is done (skin test negative to positive within last 2 years AND there was an increase of at least 10mm in size of reaction)
Number converted % of total residents % of total staff Residents Staff
Source of exposure known?
Name
Date of conversion
Location Room or Unit
Yes No
D. Active TB Disease: Number with active TB % of all residents % of all staff Residents Staff
Contact to another case?
Reported on OSHA log?
TB case name
Designate : R= Resident S= Staff
Location
Yes
No
Yes
No
If no, give reason
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 7
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 8
2. TB EXPOSURE CONTROL PLANS The results of the risk assessment will determine to what extent the different aspects of the TB Control Plan the facility will follow. Listed below are the criteria facilities should follow to identify their TB risk. Annual summary sheets are available to identify which components the facility should follow if a Minimum Risk, Very Low Risk, or Low / Intermediate Risk Facility. Enter the current data, pencil in dates various elements are planned, and write in ink when the element has been completed for that year. Those facilities in High Risk status should consult with their local health department to evaluate and correct the TB transmission problem.
A. Minimum Risk These facilities have not had active TB patients and are located in counties without active TB (eg/ have not reported active TB during the previous year). Therefore, these facilities have very minimal risk for TB exposure, and only need to have a few essential elements of a TB Control Plan. See Minimal Risk Facility TB Control Plan Summary
B. Very Low Risk
These facilities are located in counties where active TB has been reported, but the facility has not reported any active TB in staff or residents. Therefore, these facilities have very low risk for TB exposure, and only need to have the basic elements of a TB Control Plan. See Very Low Risk Facility TB Control Plan Summary
C. Low Risk or Intermediate Risk
These facilities are located in counties where active TB has been reported and the facility admitted cases of active TB during the preceding year. Therefore, these facilities have some risk for TB exposure, and need to include more components to their TB Control Plan. See Low / Intermediate Risk Facility TB Control Plan Summary
D. High Risk
These facilities have evidence of ongoing TB transmission. Consult with the local health department.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 9
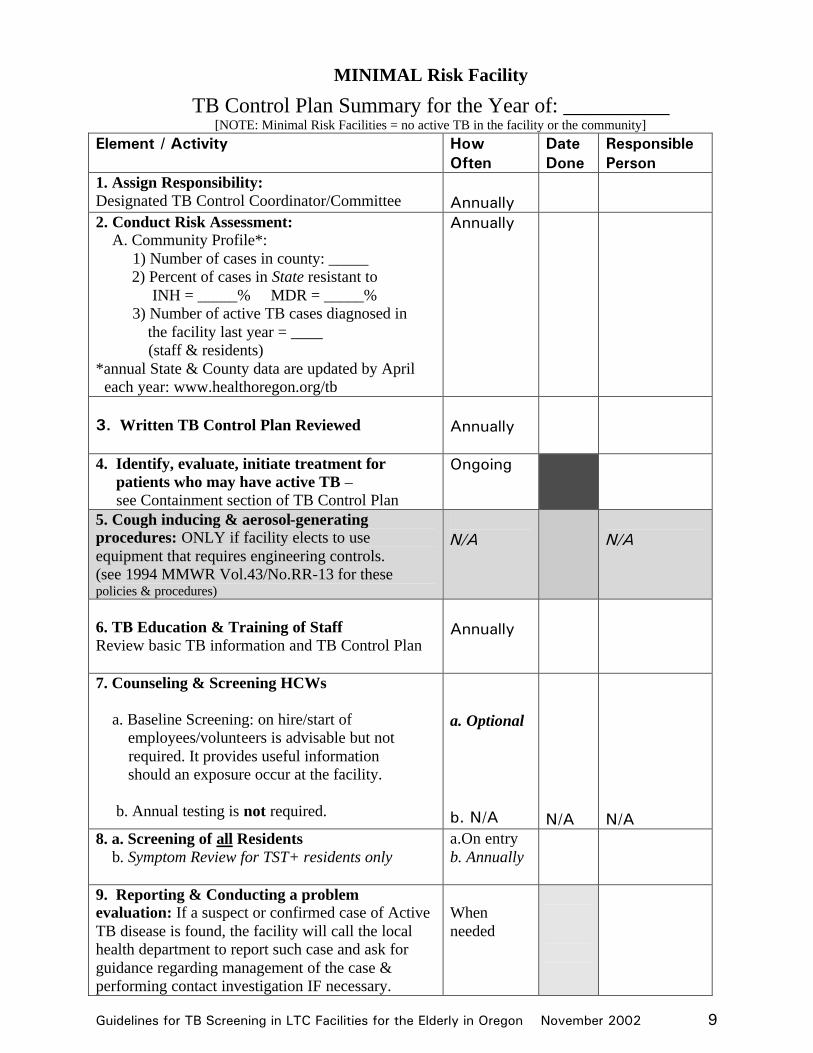
MINIMAL Risk Facility
TB Control Plan Summary for the Year of: __________ [NOTE: Minimal Risk Facilities = no active TB in the facility or the community]
Element / Activity How Often
Date Done
Responsible Person
1. Assign Responsibility: Designated TB Control Coordinator/Committee
Annually
2. Conduct Risk Assessment: A. Community Profile*: 1) Number of cases in county: _____ 2) Percent of cases in State resistant to INH = _____% MDR = _____% 3) Number of active TB cases diagnosed in the facility last year = ____ (staff & residents) *annual State & County data are updated by April each year: www.healthoregon.org/tb
Annually
3. Written TB Control Plan Reviewed
Annually
4. Identify, evaluate, initiate treatment for patients who may have active TB – see Containment section of TB Control Plan
Ongoing
5. Cough inducing & aerosol-generating procedures: ONLY if facility elects to use equipment that requires engineering controls. (see 1994 MMWR Vol.43/No.RR-13 for these policies & procedures)
N/A
N/A
6. TB Education & Training of Staff Review basic TB information and TB Control Plan
Annually
7. Counseling & Screening HCWs a. Baseline Screening: on hire/start of employees/volunteers is advisable but not required. It provides useful information should an exposure occur at the facility. b. Annual testing is not required.
a. Optional b. N/A
N/A
N/A
8. a. Screening of all Residents b. Symptom Review for TST+ residents only
a.On entry b. Annually
9. Reporting & Conducting a problem evaluation: If a suspect or confirmed case of Active TB disease is found, the facility will call the local health department to report such case and ask for guidance regarding management of the case & performing contact investigation IF necessary.
When needed
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 10
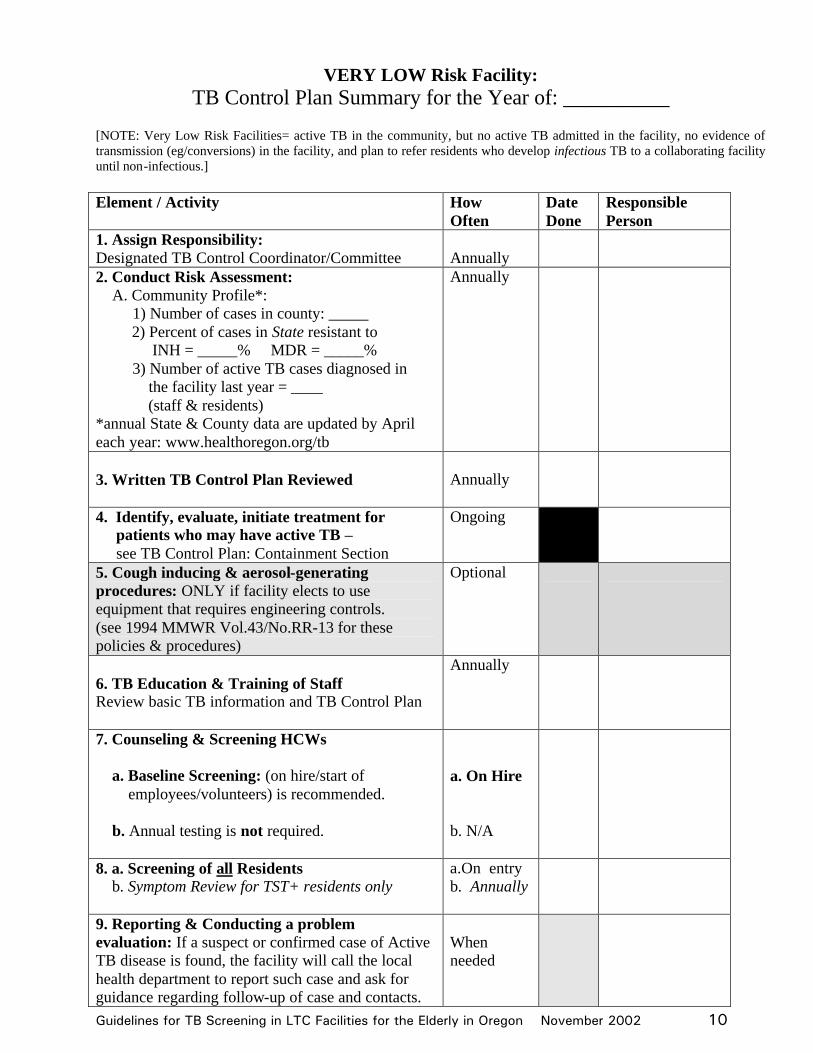
VERY LOW Risk Facility: TB Control Plan Summary for the Year of: __________
[NOTE: Very Low Risk Facilities= active TB in the community, but no active TB admitted in the facility, no evidence of transmission (eg/conversions) in the facility, and plan to refer residents who develop infectious TB to a collaborating facility until non-infectious.] Element / Activity How
Often Date Done
Responsible Person
1. Assign Responsibility: Designated TB Control Coordinator/Committee
Annually
2. Conduct Risk Assessment: A. Community Profile*: 1) Number of cases in county: _____ 2) Percent of cases in State resistant to INH = _____% MDR = _____% 3) Number of active TB cases diagnosed in the facility last year = ____ (staff & residents) *annual State & County data are updated by April each year: www.healthoregon.org/tb
Annually
3. Written TB Control Plan Reviewed
Annually
4. Identify, evaluate, initiate treatment for patients who may have active TB – see TB Control Plan: Containment Section
Ongoing
5. Cough inducing & aerosol-generating procedures: ONLY if facility elects to use equipment that requires engineering controls. (see 1994 MMWR Vol.43/No.RR-13 for these policies & procedures)
Optional
6. TB Education & Training of Staff Review basic TB information and TB Control Plan
Annually
7. Counseling & Screening HCWs a. Baseline Screening: (on hire/start of employees/volunteers) is recommended. b. Annual testing is not required.
a. On Hire b. N/A
8. a. Screening of all Residents b. Symptom Review for TST+ residents only
a.On entry b. Annually
9. Reporting & Conducting a problem evaluation: If a suspect or confirmed case of Active TB disease is found, the facility will call the local health department to report such case and ask for guidance regarding follow-up of case and contacts.
When needed
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 11
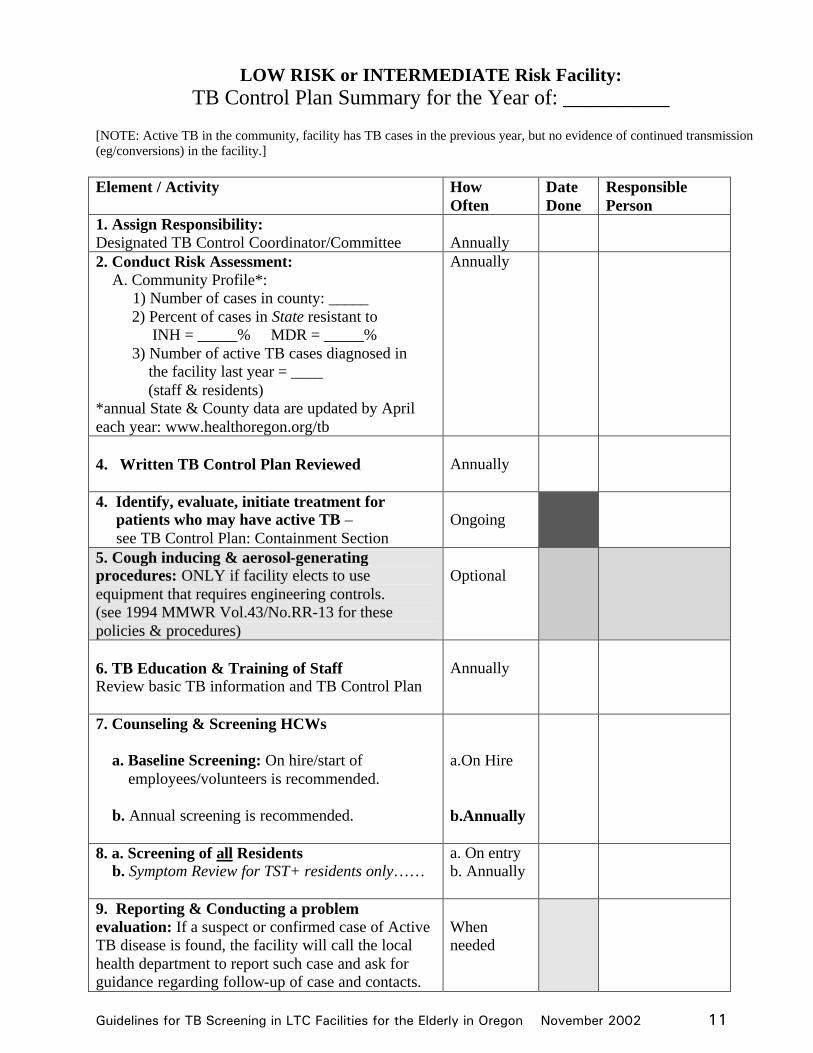
LOW RISK or INTERMEDIATE Risk Facility: TB Control Plan Summary for the Year of: __________
[NOTE: Active TB in the community, facility has TB cases in the previous year, but no evidence of continued transmission (eg/conversions) in the facility.] Element / Activity How
Often Date Done
Responsible Person
1. Assign Responsibility: Designated TB Control Coordinator/Committee
Annually
2. Conduct Risk Assessment: A. Community Profile*: 1) Number of cases in county: _____ 2) Percent of cases in State resistant to INH = _____% MDR = _____% 3) Number of active TB cases diagnosed in the facility last year = ____ (staff & residents) *annual State & County data are updated by April each year: www.healthoregon.org/tb
Annually
4. Written TB Control Plan Reviewed
Annually
4. Identify, evaluate, initiate treatment for patients who may have active TB – see TB Control Plan: Containment Section
Ongoing
5. Cough inducing & aerosol-generating procedures: ONLY if facility elects to use equipment that requires engineering controls. (see 1994 MMWR Vol.43/No.RR-13 for these policies & procedures)
Optional
6. TB Education & Training of Staff Review basic TB information and TB Control Plan
Annually
7. Counseling & Screening HCWs a. Baseline Screening: On hire/start of employees/volunteers is recommended. b. Annual screening is recommended.
a.On Hire b.Annually
8. a. Screening of all Residents b. Symptom Review for TST+ residents only……
a. On entry b. Annually
9. Reporting & Conducting a problem evaluation: If a suspect or confirmed case of Active TB disease is found, the facility will call the local health department to report such case and ask for guidance regarding follow-up of case and contacts.
When needed
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 12
2. SURVEILLANCE: Screening for Infection a. Diagnosis of Latent TB Infection The intradermal administration of 0.1 ml of 5TU strength purified protein derivative (PPD) tuberculin (the Mantoux test) is to be used to identify persons infected with TB. Multiple puncture tests are not acceptable. Mantoux tuberculin skin tests (TST) should be administered and read by appropriately trained licensed personnel and the results recorded in millimeters of induration in the individual’s medical record. See Attachment A, Guidelines for Interpretation of TB Skin Test Reactions in Oregon. Note:
• Anergy Testing: The use of anergy testing in conjunction with tuberculin skin testing is no longer recommended.
• New diagnostic tests are being developed, but are not in use at this time. 1) Residents (See Diagram 1) Baseline: A Mantoux TST should be administered to all new residents on entry (within 14 days of their admission), unless they have documentation2 of a previous positive Mantoux test.
A. Those with documentation of a past positive TST and a subsequent past negative chest x-ray for active TB only need a symptom review (see Attachment D).
B. All residents who test positive on entry, should be referred for a chest x-ray and evaluation to rule out active TB and to evaluate for treatment of latent TB infection (LTBI).
C. If a resident has symptoms consistent with active pulmonary TB, follow guidelines in the Containment Section.
Two Step Skin Testing: In order to establish a reliable baseline, a two-step skin test procedure is advisable for the initial testing of residents aged 55 and older, who have not been tested within the last year. (see Attachment B, Two-Step Tuberculin Skin Tests). Transferring between Licensed Health Care Facilities: Patients who are transferred between “licensed health care facilities” do not need to be re-tested upon their return to a facility. Patients who have been discharged to the community should be re-tested upon re-admission.
Annual TB Screening: Residents with a Negative Skin Test: Routine testing of residents who have a negative Mantoux skin test is not necessary. Residents with a Positive Skin Test:
• Residents with a positive Mantoux skin test should be screened annually with a TB symptom questionnaire. (Attachment D, Resident Annual Tuberculosis Screening Questionnaire).
• Routine, periodic chest x-rays are no longer recommended for asymptomatic persons with latent TB infection.
2 Documentation should be written and should include the following: Type of test ( Mantoux vs. multiple puncture); date of test; and millimeters of induration.

Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 13
The questionnaire should be done at the time of the resident’s annual medical evaluation. This is an awareness tool to remind staff about persons at risk for TB and to maintain familiarity with TB symptoms. If a resident becomes symptomatic, early identification and treatment may prevent transmission.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 14
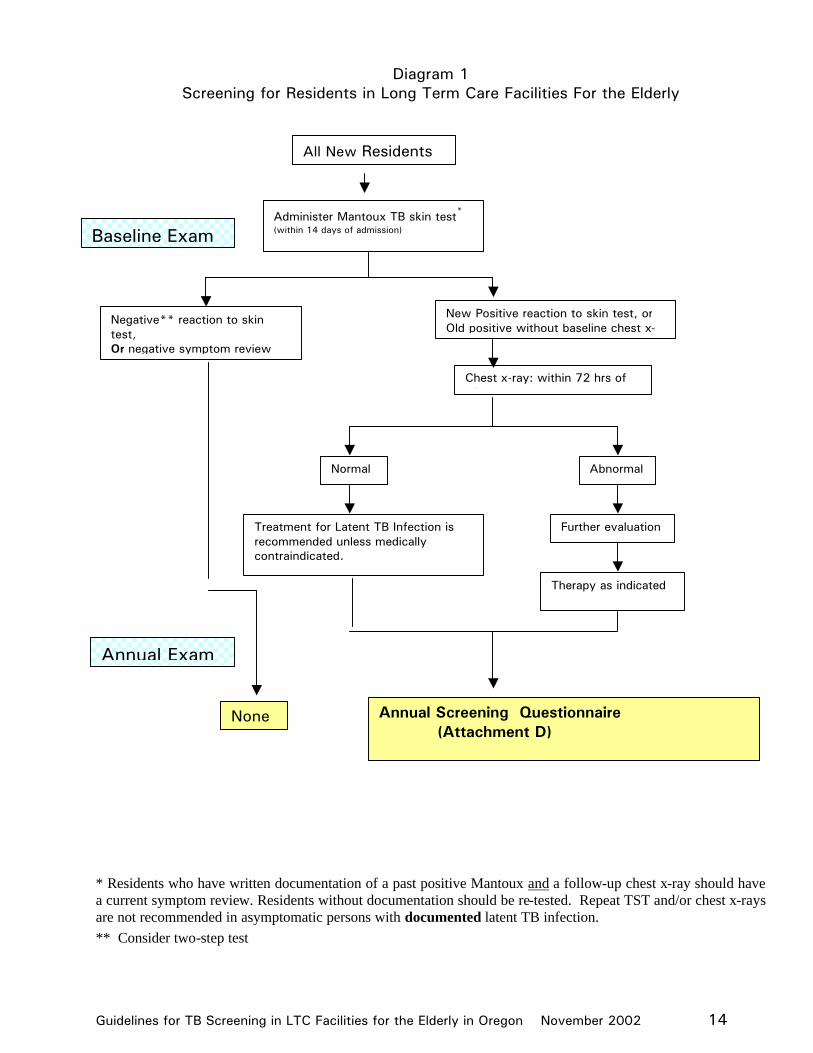
Diagram 1 Screening for Residents in Long Term Care Facilities For the Elderly
* Residents who have written documentation of a past positive Mantoux and a follow-up chest x-ray should have a current symptom review. Residents without documentation should be re-tested. Repeat TST and/or chest x-rays are not recommended in asymptomatic persons with documented latent TB infection. ** Consider two-step test
All New Residents
Administer Mantoux TB skin test*
(within 14 days of admission)
Negative** reaction to skin test, Or negative symptom review
New Positive reaction to skin test, or Old positive without baseline chest x-
Chest x-ray: within 72 hrs of TST
Abnormal Normal
Further evaluation Treatment for Latent TB Infection is recommended unless medically contraindicated.
Therapy as indicated
None Annual Screening Questionnaire (Attachment D)
Annual Exam
Baseline Exam
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 15
2) Staff and Volunteers3
BASELINE: (Note: Optional for Minimal Risk Facilities) A Mantoux TB skin test should be administered to all new staff and volunteers, unless they have documentation2 of a previous positive Mantoux test. This exam should be completed during the pre-employment physical4. If pre-employment physicals are not done, the TB exam should be completed within two weeks (14 days) of employment Those with documentation of a past positive test and negative chest x-ray for active TB only need a symptom review (see Attachment E). Routine periodic chest x-rays of persons with positive skin tests are not indicated Staff/volunteers who test positive should be referred for a chest x-ray and evaluation by their physician to rule out active TB and to evaluate for treatment of LTBI. If the staff/volunteer is symptomatic for active pulmonary TB, follow guidelines in the Containment Section.
Note: Two Step Skin Testing: In order to establish a reliable baseline, a two-step procedure is advisable for the initial testing of staff and volunteers aged 55 and older who have not had a documented negative test in the past year. However, the decision to do two step skin testing for ALL staff (regardless of age) who have not been tested within the last year should be based on the frequency of boosting in the facility4
ANNUAL SCREENING: Minimal Risk Facilities and Very Low Risk Facilities:
Staff & Volunteers with a negative skin test: NO annual TB skin test
Staff & Volunteers with a positive skin test: Those who have a positive Mantoux skin test should be screened annually with a TB symptom questionnaire. (Attachment E, Employee Annual Tuberculosis Screening Questionnaire). This is an awareness tool to remind staff that they are at risk for TB. If they become symptomatic, early identification and treatment may prevent transmission.
Low or Intermediate Risk Facilities: Annual testing is required
Staff & Volunteers with a negative skin test: need annual TB skin test
Staff & Volunteers with a positive skin test: Those who have a positive Mantoux skin test should be screened annually with a TB symptom questionnaire. (Attachment E, Employee Annual Tuberculosis Screening Questionnaire). This is an awareness tool to remind staff that they are at risk for TB. If they become symptomatic, early identification and treatment may prevent transmission.
Note: Routine annual chest x-rays of persons with positive skin tests are not indicated. Chest x-rays should be performed, with a complete work-up, if a known reactor develops symptoms consistent with active TB.
3 Volunteers who have an average of > 10 hours of contact per week with residents should be tested. 4 CDC, Guidelines for the Prevention and Control of Tuberculosis in Health Care Facilities, 1994
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 16
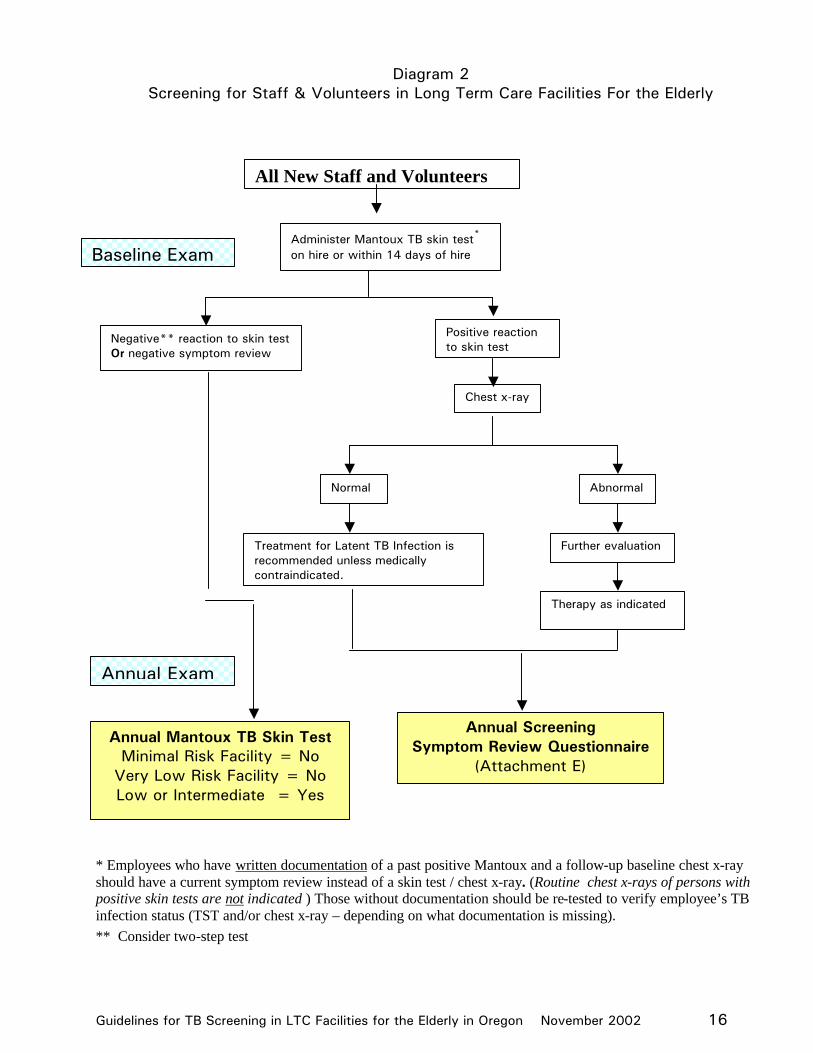
Diagram 2 Screening for Staff & Volunteers in Long Term Care Facilities For the Elderly
* Employees who have written documentation of a past positive Mantoux and a follow-up baseline chest x-ray should have a current symptom review instead of a skin test / chest x-ray. (Routine chest x-rays of persons with positive skin tests are not indicated ) Those without documentation should be re-tested to verify employee’s TB infection status (TST and/or chest x-ray – depending on what documentation is missing). ** Consider two-step test
All New Staff and Volunteers
Administer Mantoux TB skin test*
on hire or within 14 days of hire
Negative** reaction to skin test Or negative symptom review
Positive reaction to skin test
Chest x-ray
Abnormal Normal
Further evaluation Treatment for Latent TB Infection is recommended unless medically contraindicated.
Therapy as indicated
Annual Mantoux TB Skin Test Minimal Risk Facility = No
Very Low Risk Facility = No Low or Intermediate = Yes
Annual Screening Symptom Review Questionnaire
(Attachment E)
Annual Exam
Baseline Exam
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 17
b. Reporting
Report, within 1 working day (Monday – Friday) of knowledge, any resident, staff, or volunteer who is diagnosed with suspected or confirmed active TB. To report a diagnosed case, call the local County Health Department. Reporting is required under Oregon Administrative Rule 333-018-000 and 333-018-0015. The local health department can provide consultation and or assistance regarding treatment, containment and exposure follow-up for all reported cases. Refer to www.healthoregon.org/tb for list of local health departments.
Skin Test Converters:5 There is no requirement to report persons who convert their skin tests upon repeat testing to the local health department. However, if there is concern about multiple conversions within a facility, the local health department should be consulted. Documented converters are at increased risk for progression to active TB and should have a medical evaluation. If active TB is ruled out, converters are candidates for treatment of their TB infection (unless they have a medical contraindication). When a unique conversion occurs, a history of probable exposure to TB should be obtained to determine the most likely source of infection. If the history suggests the exposure was from outside the facility, no further follow-up is indicated. If the history does not identify a probable source in the facility, the investigation can be terminated. If the history identifies a probable source in the facility (and/or other conversions), further evaluation as described in the October 28, 1994 MMWR, “1. Investigating PPD test conversion and active TB in HCWs” (pages 42-47) should occur.
3. CONTAINMENT / Screening for disease In long term care settings, many residents have chronic pulmonary conditions which can produce symptoms consistent with TB. The following provides guidance in evaluation of persons to identify suspect pulmonary TB cases.
a. Residents with a Negative Tuberculin Skin Test Persons with a negative skin test can have active TB. Therefore, pulmonary TB should be
considered in any person with suggestive symptoms regardless of skin test status. Residents who develop the following need further follow-up:
• Hemoptysis, and/or • Cough for > 2 weeks, • and two or more of:
Ø Fever that lasts more that 1 week; Ø Sputum production for more than 1 week; Ø Feeling of fatigue for more than 2 weeks; Ø Night sweats (heavy perspiring thru pajamas and sheets); Ø Unexplained weight loss (approx. 10% or more of usual body weight)
5 Converters can be defined as those whose skin test reaction has been documented to have converted from a negative to a positive test within the past 2 years, and has increased in size by at least 10mm.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 18
A physician should be consulted and the patient examined. The physician should indicate a diagnosis, document any chest x-ray findings, and a plan for follow-up. If symptoms persist or worsen, the physician should be notified. If TB is part of the differential diagnosis, sputum should be collected on 3 consecutive days and sent to the lab on the day collected. Call the lab if smear6 results are not back within 2 days. If any of the sputums are AFB smear positive, the person should be considered a suspect infectious TB case and be placed in respiratory TB isolation until they are on medicine and have clinical and bacterial evidence that they are no longer infectious (usually 3 consecutive negative AFB smears on sputum). If isolation is not possible, the resident must be transferred to a facility that can provide TB isolation. The resident may return when they have become non-infectious, and are on a Health Department approved TB treatment regimen. (See Section d. ISOLATION).
A resident whose three sputums for AFB are all negative (or is unable to produce sputum), may stay in the facility. The resident may be started on TB treatment, if he/she clinically appears to have TB, until culture results are known. If a resident is diagnosed with TB, call the local health department to report the case and discuss case management and contact follow-up recommendations.
b. Residents with a Positive Tuberculin Skin Test
Staff should be aware of which residents are known to be infected with TB, so that they will remain alert to early symptoms of active TB. The resident’s TB skin test result should be placed prominently on the medical record.
(1) Residents Without Chronic Pulmonary Problems:
Residents who develop the following need further follow-up:
• Hemoptysis, and/or • Cough for > 2 weeks, • and two or more of:
Ø Fever that lasts more that 1 week; Ø Sputum production for more than 1 week; Ø Feeling of fatigue for more than 2 weeks; Ø Night sweats (heavy perspiring thru pajamas and sheets); Ø Unexplained weight loss (approx. 10% or more of usual body weight)
A physician should be consulted, an order obtained for chest X-ray, and 3 sputums for AFB smear and culture (and routine C & S, if indicated). The sputums should be collected on 3 consecutive days and each sent on the day collected. Call the lab if smear7 results are not back within 2 days.
6 Each sputum specimen should be sent for AFB (acid fast bacilli) smear, culture, and drug susceptibility testing (susceptibility on first positive culture). Smears give an indication of infectiousness and should be available in 24 hours, cultures confirm a TB diagnosis and take 3-8 weeks. 7 Each sputum specimen should be sent for AFB (acid fast bacilli) smear, culture, and drug susceptibility testing (susceptibility on first positive culture). Smears give an indication of infectiousness and should be available in 24 hours, cultures confirm a TB diagnosis and take 3-8 weeks.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 19
If at least one sputum was smear positive for AFB: If any of the sputums are AFB smear positive, the person should be considered a suspect infectious TB case and be placed in respiratory TB isolation until the resident is on medicine and have clinical and bacterial evidence that he/she is no longer infectious (usually 3 consecutive negative AFB smears). If isolation is not possible, the resident must be transferred to a facility that can provide TB isolation. The resident may return when he/she has become non-infectious, and is on a Health Department approved TB treatment regimen. (See Section d. ISOLATION).
If all sputums were negative for AFB: A resident whose three sputums for AFB are all negative, may stay in the facility. The resident may be started on TB treatment, if he/she clinically appears to have TB, until culture results are known. If a resident is diagnosed with TB, call the local health department to report the case and discuss case management and contact follow-up recommendations.
(2) Residents With Chronic Pulmonary Problems:
Residents who develop the following symptoms need further follow-up:
• Hemoptysis, and/or • Cough has increased: lasting more than 2 weeks, • and who have 2 or more of the following symptoms:
Ø Fever that lasts more that 1 week; Ø Sputum production has increased and/or changed color (e.g. whitish to green or
yellow); Ø Feeling of fatigue for more than 2 weeks; Ø Night sweats (heavy perspiring thru pajamas and sheets); Ø Unexplained weight loss (approx. 10% or more of their usual body weight)
A physician should be consulted and the patient examined. The physician should indicate a diagnosis, document any chest x-ray findings, and a plan for follow-up. If symptoms persist or worsen, the physician should be notified, and TB should be considered if it has not already been ruled out. Anytime TB is part of the differential diagnosis, 3 sputums for AFB smear and culture should be collected on 3 consecutive days and sent to the lab on the day collected. Call the lab if smear8 results are not back within 2 days.
If at least one sputum was smear positive for AFB: If any of the sputums are smear positive, the resident should be considered a suspect infectious TB case and be placed in respiratory TB isolation until he/she is on medicine and have clinical and bacterial evidence that they are no longer infectious (usually 3 consecutive negative AFB smears). If isolation is not possible, the resident must be transferred to a facility that can provide TB isolation. The resident may return when he/she has become non-infectious, and is on a Health Department approved TB treatment regimen. (See Section d. ISOLATION).
8 Each sputum specimen should be sent for AFB (acid fast bacilli) smear, culture, and drug susceptibility testing (susceptibility on first positive culture). Smears give an indication of infectiousness and should be available in 24 hours, cultures confirm a TB diagnosis and take 3-8 weeks.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 20
If all sputums were negative for AFB: A resident whose three sputums for AFB are all negative, may stay in the facility. The resident may be started on TB treatment, if he/she clinically appears to have TB, until culture results are known. If a resident is diagnosed with TB, call the local health department to report the case and discuss case management and contact follow-up recommendations.
c. Staff / Volunteers Any staff member or volunteer who develop the following need further follow-up: • Hemoptysis or • Cough that lasts more than 2 weeks, • and two or more of the following symptoms:
Ø Fever that lasts more than 1 week, Ø Sputum production for more than 1 week, Ø Feeling of fatigue for more than 2 weeks, Ø Night sweats Ø Unexplained weight loss (approximately 8 lbs. or more)
The staff member / volunteer should remain off work until the diagnosis of TB is excluded, or, if TB is diagnosed, until they become noninfectious. A note from their treating physician will be needed before the person can return to work.
If an employee is diagnosed with TB, call the local health department to report the case and discuss case management and contact follow-up recommendations.
d. ISOLATION
(1) Residents A resident with suspected infectious pulmonary TB (sputum AFB smear positive) must be placed in TB respiratory isolation until he/she becomes non-infectious. If the facility is unable to provide TB respiratory isolation, the resident will be transferred to a facility that can provide TB isolation until non-infectiousness is established. During transport, the patient should be masked (with a surgical mask).
(2) Staff / volunteers A staff member or volunteer who has been identified as a suspect case of infectious TB must be excluded from work until non-infectiousness is established and therapy instituted. A note from their physician stating that the person is not infectious will be needed for the individual to return to work. You may call the local health department for verification of the worker’s non-infectious status.
(3) TB Respiratory Isolation To provide TB respiratory isolation, the facility must have TB isolation room(s) that are:
• single patient room
• special ventilation, which meets current standards for the purpose of TB isolation9
9 For discussion of these standards, refer to Section 5197 Prevention of Occupational Tuberculosis, Title 8, Calif. Code of Regulations, Division 1, Chapter 4, Subchapter 7, Group 16, CONTROL OF HAZARDOUS SUBSTANCES,
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 21
< Insert facility policy which ensures above procedures if facility is able to provide TB Isolation.>
(4) Non-Infectiousness
A resident or staff member / volunteer may return to the facility when non-infectiousness has been established by meeting the following criteria:
• Has consecutively negative sputum smear for AFB on 3 separate days; and • Has completed at least 2 weeks of multidrug anti-tuberculosis therapy to which his/her
organisms are likely to be susceptible;* and • Has shown symptomatic improvement; and • Will have continued close medical supervision.
*If the patient has not had positive sputum AFB smears, placement or return to work can be considered before the completion of 2 weeks of therapy.
e. Treatment Centers for Disease Control/American Thoracic Society recommendations should be followed in treating and managing persons with suspected or confirmed TB. Each dose of medication should be dispensed by a staff person who watches the patient swallow the pills and who is trained to monitor for drug toxicity.
f. Investigation of Contacts (Exposure Follow-up)
Contact Follow-up: As soon as a diagnosis of infectious pulmonary TB is suspected, follow-up of exposed contacts will be initiated. Guidelines established for Long Term Care facilities are outlined in Appendix III of CDC’s Prevention and Control of Tuberculosis in Facilities Providing Long-Term Care to the Elderly, July 1990. (Attachment F, Investigation for Contacts). These guidelines, in conjunction with case-specific recommendations from the local health department, will be followed when performing an exposure follow-up. Identified contacts should be notified of exposure and be given follow-up recommendations in writing.
Treatment for Latent TB Infection: Contacts who have documented Mantoux skin test conversions and no evidence of active TB, should be offered at least 6 months of treatment with INH, unless medically contraindicated. Other currently accepted regimens may be recommended by the person’s private physician. Contacts who have had significant exposure to an infectious case and who are at high risk to progress to disease if infected (e.g., HIV-infected persons), should be offered treatment regardless of their skin test reaction. After 3 months of treatment, those who were skin test negative should have the skin test repeated. Therapy may be discontinued if the skin test is still negative and contact with the infectious case is broken. Persons who are severely
Article 109, Hazardous Substances and Processes; and current Centers for Disease Control and Prevention: Guidelines for Preventing the Transmission of Tuberculosis in Healthcare Facilities, Second Edition.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 22
immunocompromised (eg., HIV- infected, immunosuppressive therapy) may need to complete the 6-9 months of treatment, even if skin test remains negative. When treatment for LTBI is recommended, but the individual refuses or is unable to complete the recommended course, they will be advised to seek prompt medical attention if signs or symptoms of active TB develop. This should be documented in their medical file. Sample records are provided: Attachment G1-3. Routine annual chest x-rays of tuberculin reactors are not useful for detecting disease when the person is asymptomatic.
4. ASSESSMENT
The following information will be reviewed annually with the Infection Control committee:
• Number of cases in the County where the facility is located. • TB drug resistance for INH and INH+RIF± other (MDR-TB) in the State • Number/percent of residents and staff with positive Mantoux tests; • Number/percent of persons who convert their Mantoux test after employment (IF annual
testing is done); • Number/percent of residents and staff diagnosed with active tuberculosis.
(TB Surveillance/Risk Assessment Record, may be used to record this data.)
5. EDUCATION
Training of staff and volunteers will occur on hire and annually. TB inservices will include:
Ø Groups at risk for TB (including impact of HIV infection); Ø Transmission and pathogenesis; Ø Diagnosis and treatment of:
A. Infection: • Positive skin test, no active disease; • Treatment for latent TB infection (LTBI). B. Disease: • Symptoms • Work up: Infectious vs. not infectious • Treatment: Drug susceptible vs. multi-drug resistant.
Ø Facility TB Control Plan • Use and limitations of all methods used by the facility to prevent TB exposure; • Employer’s responsibility • Employee’s responsibility • Surveillance
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 23
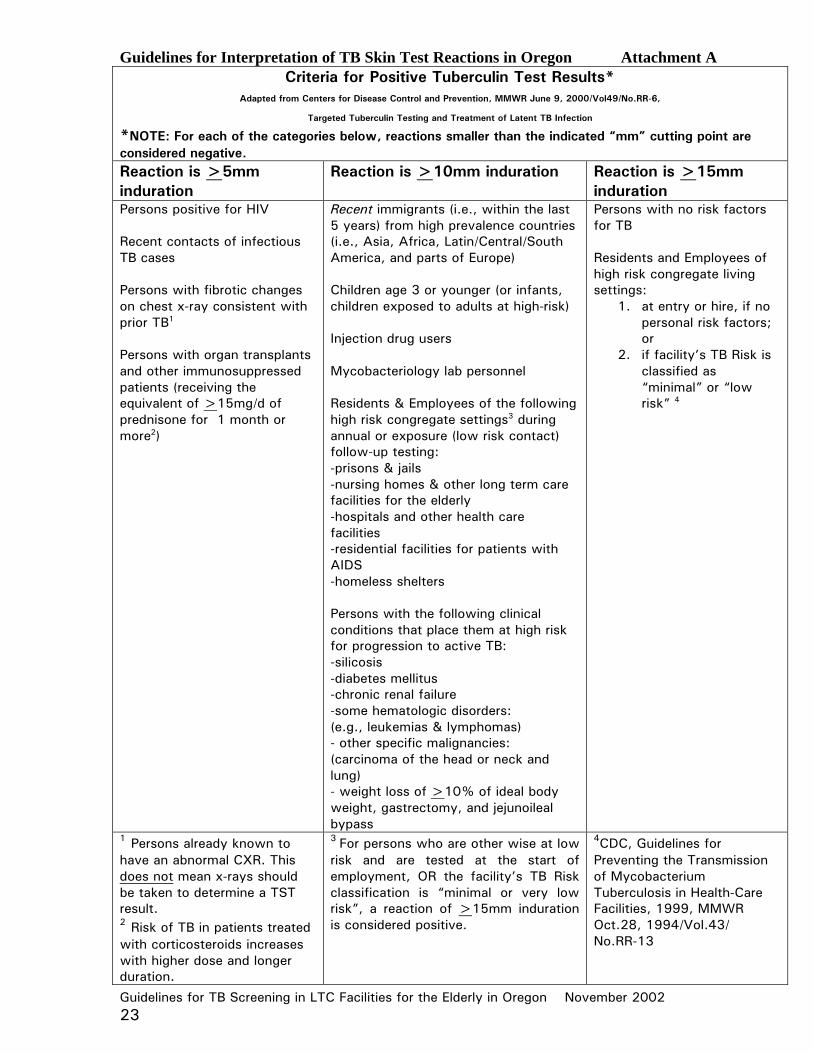
Guidelines for Interpretation of TB Skin Test Reactions in Oregon Attachment A Criteria for Positive Tuberculin Test Results*
Adapted from Centers for Disease Control and Prevention, MMWR June 9, 2000/Vol49/No.RR-6,
Targeted Tuberculin Testing and Treatment of Latent TB Infection
*NOTE: For each of the categories below, reactions smaller than the indicated “mm” cutting point are considered negative. Reaction is >5mm induration
Reaction is >10mm induration Reaction is >15mm induration
Persons positive for HIV Recent contacts of infectious TB cases Persons with fibrotic changes on chest x-ray consistent with prior TB1
Persons with organ transplants and other immunosuppressed patients (receiving the equivalent of >15mg/d of prednisone for 1 month or more2)
Recent immigrants (i.e., within the last 5 years) from high prevalence countries (i.e., Asia, Africa, Latin/Central/South America, and parts of Europe) Children age 3 or younger (or infants, children exposed to adults at high-risk) Injection drug users Mycobacteriology lab personnel Residents & Employees of the following high risk congregate settings3 during annual or exposure (low risk contact) follow-up testing: -prisons & jails -nursing homes & other long term care facilities for the elderly -hospitals and other health care facilities -residential facilities for patients with AIDS -homeless shelters Persons with the following clinical conditions that place them at high risk for progression to active TB: -silicosis -diabetes mellitus -chronic renal failure -some hematologic disorders: (e.g., leukemias & lymphomas) - other specific malignancies: (carcinoma of the head or neck and lung) - weight loss of >10% of ideal body weight, gastrectomy, and jejunoileal bypass
Persons with no risk factors for TB Residents and Employees of high risk congregate living settings:
1. at entry or hire, if no personal risk factors; or
2. if facility’s TB Risk is classified as “minimal” or “low risk” 4
1 Persons already known to have an abnormal CXR. This does not mean x-rays should be taken to determine a TST result. 2 Risk of TB in patients treated with corticosteroids increases with higher dose and longer duration.
3 For persons who are other wise at low risk and are tested at the start of employment, OR the facility’s TB Risk classification is “minimal or very low risk”, a reaction of >15mm induration is considered positive.
4CDC, Guidelines for Preventing the Transmission of Mycobacterium Tuberculosis in Health-Care Facilities, 1999, MMWR Oct.28, 1994/Vol.43/ No.RR-13
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 24
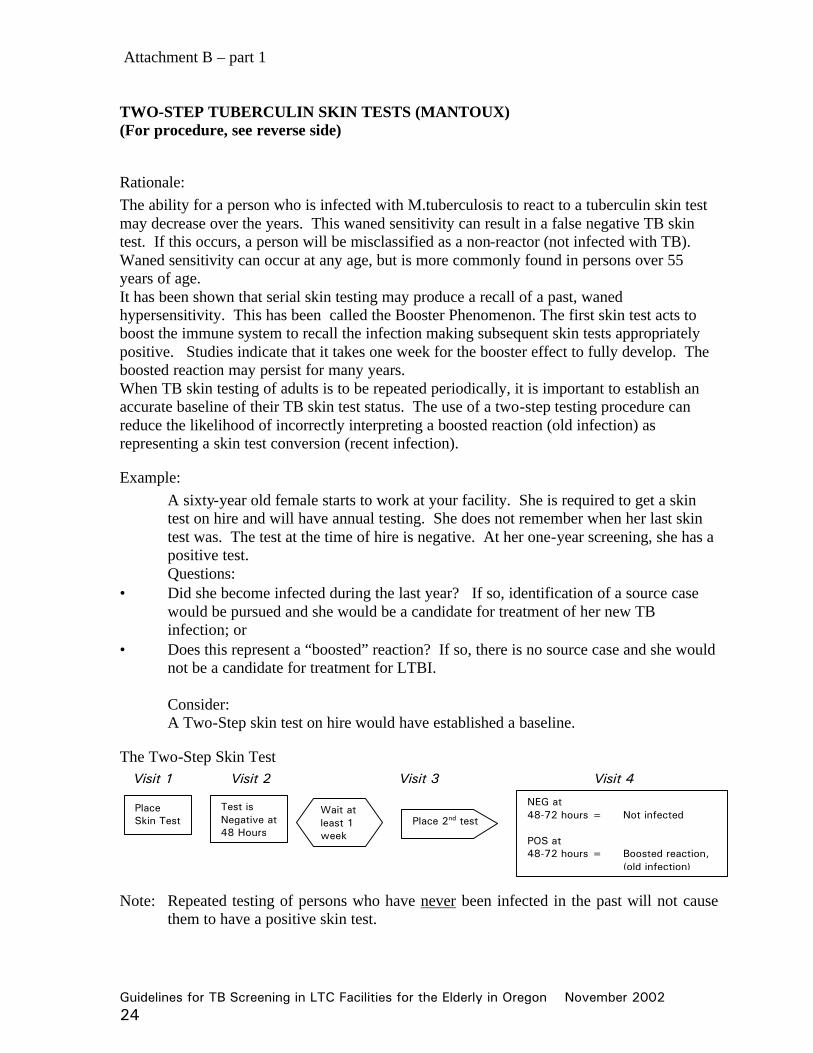
Attachment B – part 1 TWO-STEP TUBERCULIN SKIN TESTS (MANTOUX) (For procedure, see reverse side)
Rationale: The ability for a person who is infected with M.tuberculosis to react to a tuberculin skin test may decrease over the years. This waned sensitivity can result in a false negative TB skin test. If this occurs, a person will be misclassified as a non-reactor (not infected with TB). Waned sensitivity can occur at any age, but is more commonly found in persons over 55 years of age. It has been shown that serial skin testing may produce a recall of a past, waned hypersensitivity. This has been called the Booster Phenomenon. The first skin test acts to boost the immune system to recall the infection making subsequent skin tests appropriately positive. Studies indicate that it takes one week for the booster effect to fully develop. The boosted reaction may persist for many years. When TB skin testing of adults is to be repeated periodically, it is important to establish an accurate baseline of their TB skin test status. The use of a two-step testing procedure can reduce the likelihood of incorrectly interpreting a boosted reaction (old infection) as representing a skin test conversion (recent infection).
Example: A sixty-year old female starts to work at your facility. She is required to get a skin test on hire and will have annual testing. She does not remember when her last skin test was. The test at the time of hire is negative. At her one-year screening, she has a positive test. Questions:
• Did she become infected during the last year? If so, identification of a source case would be pursued and she would be a candidate for treatment of her new TB infection; or
• Does this represent a “boosted” reaction? If so, there is no source case and she would not be a candidate for treatment for LTBI.
Consider: A Two-Step skin test on hire would have established a baseline.
The Two-Step Skin Test Visit 1 Visit 2 Visit 3 Visit 4
Note: Repeated testing of persons who have never been infected in the past will not cause
them to have a positive skin test.
Place Skin Test
Test is Negative at 48 Hours
Wait at least 1 week
Place 2nd test
NEG at 48-72 hours = Not infected POS at 48-72 hours = Boosted reaction,
(old infection)
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 25
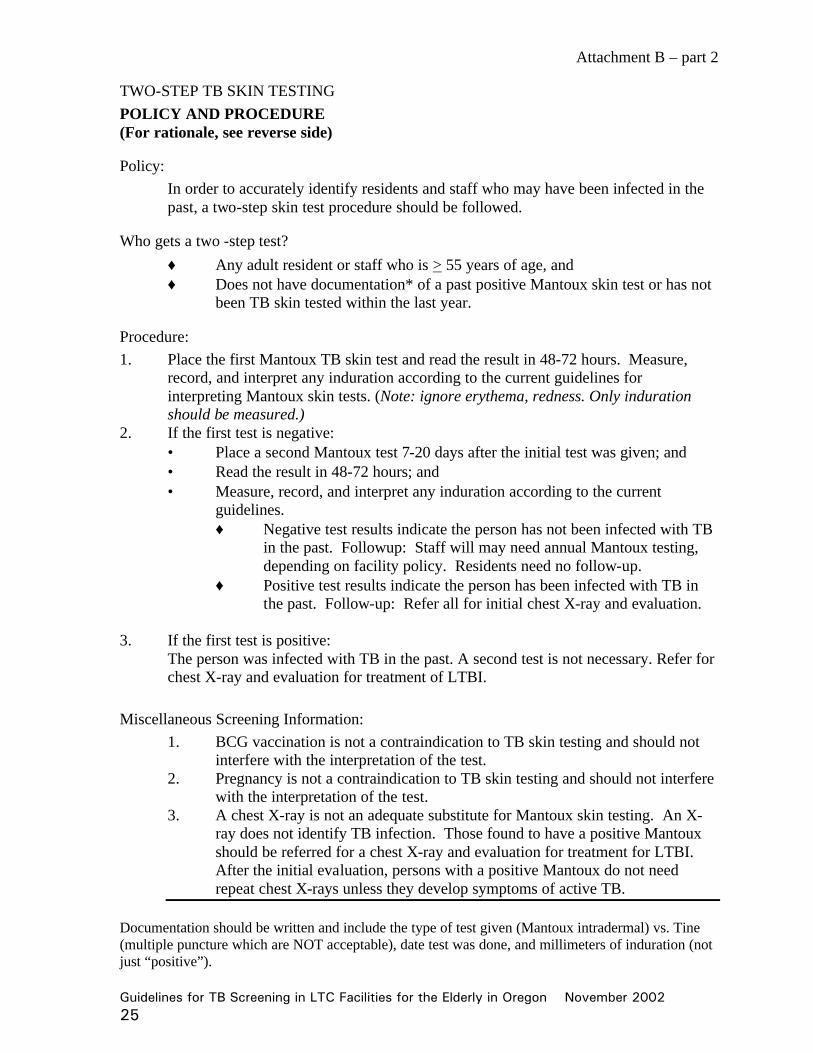
Attachment B – part 2
TWO-STEP TB SKIN TESTING POLICY AND PROCEDURE (For rationale, see reverse side)
Policy: In order to accurately identify residents and staff who may have been infected in the past, a two-step skin test procedure should be followed.
Who gets a two -step test? ♦ Any adult resident or staff who is > 55 years of age, and ♦ Does not have documentation* of a past positive Mantoux skin test or has not
been TB skin tested within the last year.
Procedure: 1. Place the first Mantoux TB skin test and read the result in 48-72 hours. Measure,
record, and interpret any induration according to the current guidelines for interpreting Mantoux skin tests. (Note: ignore erythema, redness. Only induration should be measured.)
2. If the first test is negative: • Place a second Mantoux test 7-20 days after the initial test was given; and • Read the result in 48-72 hours; and • Measure, record, and interpret any induration according to the current
guidelines. ♦ Negative test results indicate the person has not been infected with TB
in the past. Followup: Staff will may need annual Mantoux testing, depending on facility policy. Residents need no follow-up.
♦ Positive test results indicate the person has been infected with TB in the past. Follow-up: Refer all for initial chest X-ray and evaluation.
3. If the first test is positive:
The person was infected with TB in the past. A second test is not necessary. Refer for chest X-ray and evaluation for treatment of LTBI.
Miscellaneous Screening Information: 1. BCG vaccination is not a contraindication to TB skin testing and should not
interfere with the interpretation of the test. 2. Pregnancy is not a contraindication to TB skin testing and should not interfere
with the interpretation of the test. 3. A chest X-ray is not an adequate substitute for Mantoux skin testing. An X-
ray does not identify TB infection. Those found to have a positive Mantoux should be referred for a chest X-ray and evaluation for treatment for LTBI. After the initial evaluation, persons with a positive Mantoux do not need repeat chest X-rays unless they develop symptoms of active TB.
Documentation should be written and include the type of test given (Mantoux intradermal) vs. Tine (multiple puncture which are NOT acceptable), date test was done, and millimeters of induration (not just “positive”).
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 26
Attachment C
BCG: TB Vaccine What you should know
What is TB? TB is a life-threatening disease that can be spread from person to person. TB usually affects the lungs, but can develop in any part of the body. What is BCG? BCG is a vaccine that is used to protect against TB in many parts of the world. The effectiveness of the vaccine varies widely. Can people who have been vaccinated with BCG develop TB? Yes. BCG does not always protect people from TB. After vaccination, people can still become infected with TB and may develop disease. BCG is somewhat effective in decreasing the chance that infants and very young children will develop serious forms of TB. Can people who have been vaccinated with BCG get a TB skin test? Yes. BCG is not a contraindication for TB skin testing. A positive skin test (usually >10mm), even in a person who has been vaccinated with BCG, usually means they have been infected with TB. What will happen if my TB skin test is positive? You will need a chest x-ray and medical evaluation. If there is no evidence of active TB disease, treatment for TB infection is usually recommended. If you have questions, talk to your doctor or your local health department. 11/2000
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 27
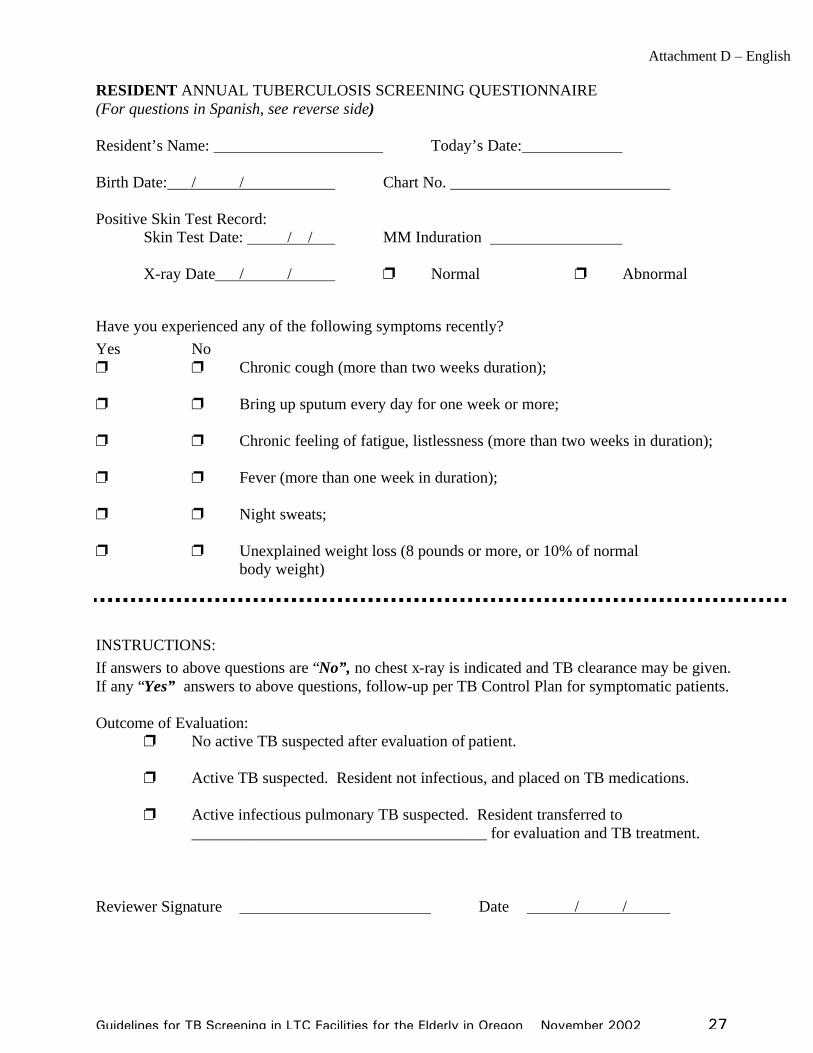
Attachment D – English RESIDENT ANNUAL TUBERCULOSIS SCREENING QUESTIONNAIRE (For questions in Spanish, see reverse side) Resident’s Name: Today’s Date: Birth Date: / / Chart No. Positive Skin Test Record:
Skin Test Date: / / MM Induration
X-ray Date / / p Normal p Abnormal
Have you experienced any of the following symptoms recently? Yes No p p Chronic cough (more than two weeks duration); p p Bring up sputum every day for one week or more; p p Chronic feeling of fatigue, listlessness (more than two weeks in duration);
p p Fever (more than one week in duration);
p p Night sweats; p p Unexplained weight loss (8 pounds or more, or 10% of normal body weight)
INSTRUCTIONS: If answers to above questions are “No”, no chest x-ray is indicated and TB clearance may be given. If any “Yes” answers to above questions, follow-up per TB Control Plan for symptomatic patients. Outcome of Evaluation:
p No active TB suspected after evaluation of patient. p Active TB suspected. Resident not infectious, and placed on TB medications. p Active infectious pulmonary TB suspected. Resident transferred to _____________________________________ for evaluation and TB treatment. Reviewer Signature Date / /
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 28
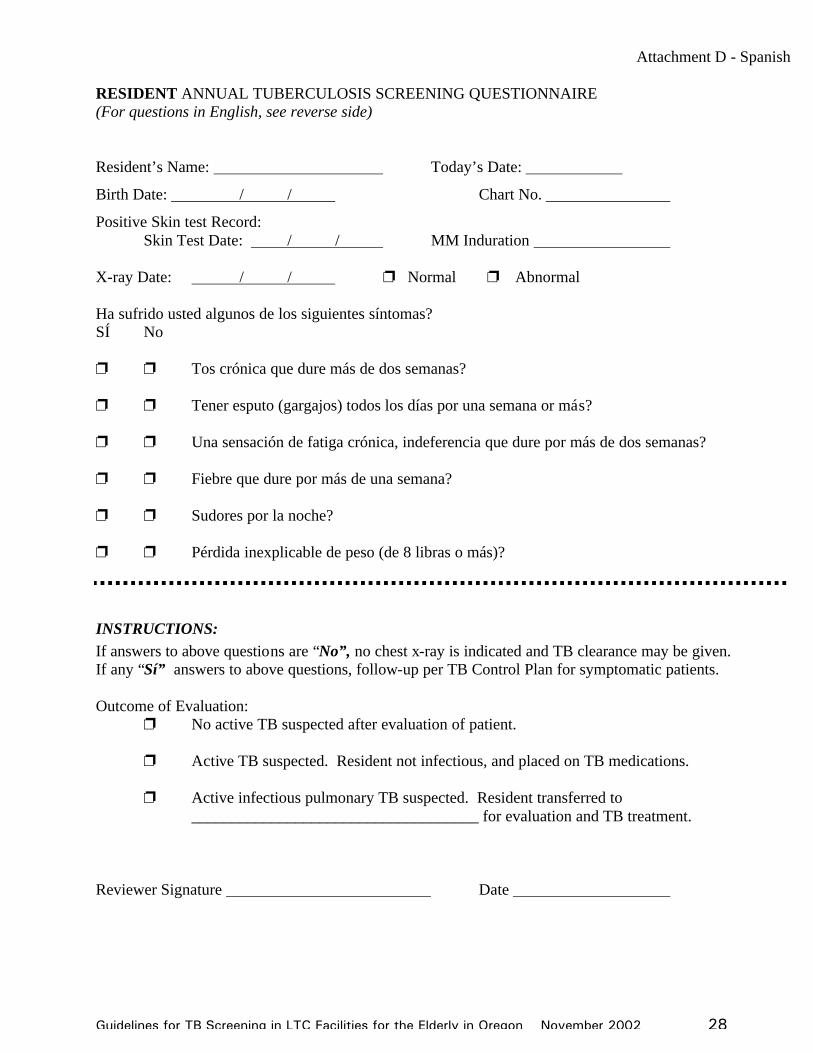
Attachment D - Spanish RESIDENT ANNUAL TUBERCULOSIS SCREENING QUESTIONNAIRE (For questions in English, see reverse side) Resident’s Name: Today’s Date:
Birth Date: / / Chart No.
Positive Skin test Record: Skin Test Date: / / MM Induration X-ray Date: / / p Normal p Abnormal Ha sufrido usted algunos de los siguientes síntomas? SÍ No p p Tos crónica que dure más de dos semanas? p p Tener esputo (gargajos) todos los días por una semana or más? p p Una sensación de fatiga crónica, indeferencia que dure por más de dos semanas? p p Fiebre que dure por más de una semana? p p Sudores por la noche? p p Pérdida inexplicable de peso (de 8 libras o más)?
INSTRUCTIONS: If answers to above questions are “No”, no chest x-ray is indicated and TB clearance may be given. If any “Sí” answers to above questions, follow-up per TB Control Plan for symptomatic patients. Outcome of Evaluation: p No active TB suspected after evaluation of patient. p Active TB suspected. Resident not infectious, and placed on TB medications. p Active infectious pulmonary TB suspected. Resident transferred to ____________________________________ for evaluation and TB treatment. Reviewer Signature Date
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 29
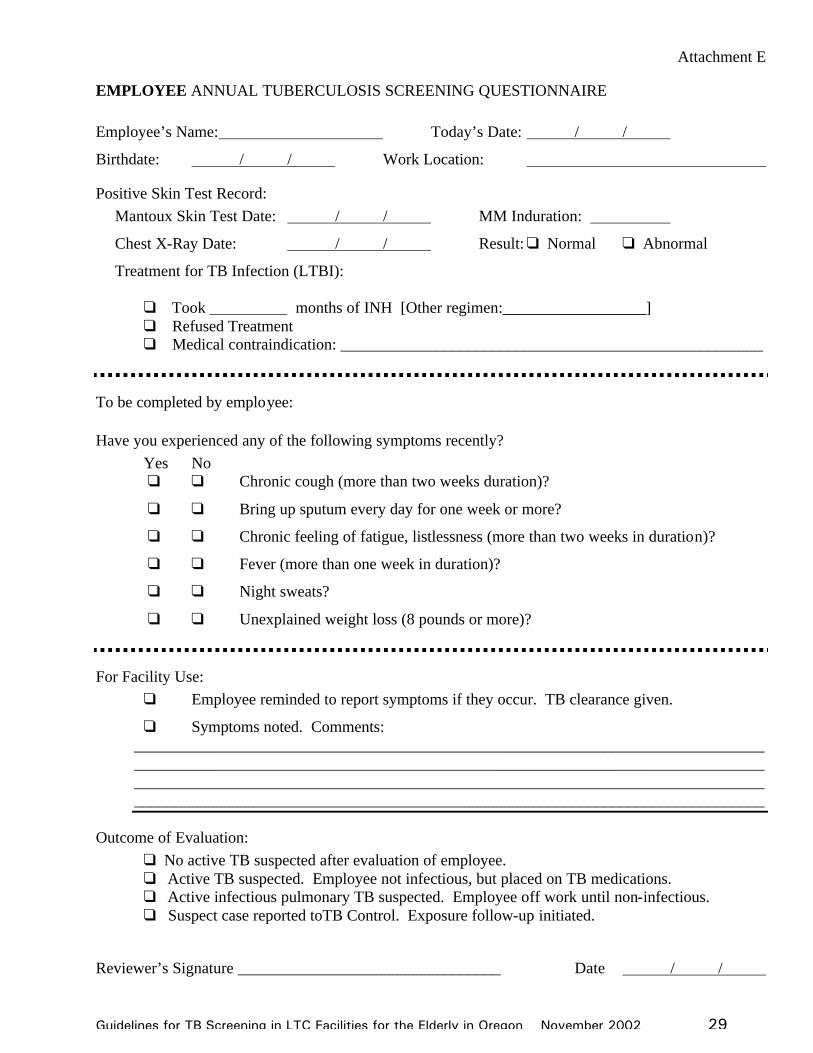
Attachment E
EMPLOYEE ANNUAL TUBERCULOSIS SCREENING QUESTIONNAIRE Employee’s Name: Today’s Date: / /
Birthdate: / / Work Location:
Positive Skin Test Record: Mantoux Skin Test Date: / / MM Induration:
Chest X-Ray Date: / / Result: q Normal q Abnormal
Treatment for TB Infection (LTBI):
q Took months of INH [Other regimen:__________________] q Refused Treatment q Medical contraindication: _____________________________________________________
To be completed by employee:
Have you experienced any of the following symptoms recently? Yes No q q Chronic cough (more than two weeks duration)?
q q Bring up sputum every day for one week or more?
q q Chronic feeling of fatigue, listlessness (more than two weeks in duration)?
q q Fever (more than one week in duration)?
q q Night sweats?
q q Unexplained weight loss (8 pounds or more)?
For Facility Use: q Employee reminded to report symptoms if they occur. TB clearance given.
q Symptoms noted. Comments: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Outcome of Evaluation: q No active TB suspected after evaluation of employee. q Active TB suspected. Employee not infectious, but placed on TB medications. q Active infectious pulmonary TB suspected. Employee off work until non-infectious. q Suspect case reported toTB Control. Exposure follow-up initiated.
Reviewer’s Signature _________________________________ Date / /
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 30
Attachment F : page 1 of 3 MMWR July 13, 1990 Prevention & Control of Tuberculosis in Facilities Providing Long-Term Care to the Elderly
Appendix III
Investigation for Contacts Contacts of persons with newly diagnosed tuberculosis are at risk of infection and disease. The risk to contacts is related to various factors pertaining to the person who has the source case (the “source patient”), the contact, and the environment that they share. Many factors interact to influence the transmission of infectious particles (droplet nuclei) from the source patient to the contact. As soon as the diagnosis is reasonably established on laboratory and/or clinical bases, investigation of contacts should begin. Health-care personnel should not wait for positive cultures if history, sputum smears, and chest radiographs are suggestive of tuberculosis. A. Development of Transmission Probability Data
When a source patient has been identified, the appropriate procedure in contact investigation entails the development of a data base and an evaluation of each of the factors noted below. These data are usually gathered by interviewing the source patient and by reviewing related historic and laboratory records. A visit to the source patient’s home or place of employment will usually be necessary to assemble a satisfactory initial data base.
Source-patient characteristics. Any person who is generating aerosolized particles containing tubercle bacilli is a potential transmitter of infection. Factors that indicate the probability of spreading tuberculosis infection are:
• If the source patient is not receiving adequate antituberculosis chemotherapy, the probability of his or her producing infectious particles is enhanced.
• The presence of acid-fast bacilli in the appropriately examined sputum smear is indicative of a greater potential for infection.
• The ability to culture Mycobacterium tuberculosis from secretions of the source patient is less important quantitatively, as an indicator, than is the positive sputum smear.
• The presence of tuberculosis laryngitis increases infectiousness.
• The volume and viscosity of respiratory secretions influence the production of infectious particles; high volume and watery sputum are regarded as risk factors.
• Forceful exhalation (e.g., singing or shouting) may increase the potential for producing infectious particles.
• Prolonged duration of respiratory symptoms may augment the likelihood that infection will be transmitted.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 31
Attachment F: page 2 of 3 Environmental air factors. Air is the vehicle by which the infectious particle or droplet nucleus is transported from the source patient to susceptible persons. The greater the concentration of these droplet nuclei in air shared by the source patient and his or her associates, the greater the risk to these contacts. The following factors alter the concentration of infectious particles in the air:
• The volume of air common to the source patient and contact is critical. If low, the
concentration of infectious particles is increased (e.g., as in sharing a small room).
• Ventilation with outside air dilutes the concentration of potentially infectious droplets.
• Recirculating air may result in the accumulation of high concentrations of infectious particles because droplet nuclei remain suspended in the air (e.g., ships, hospitals, and other structures with closed-circuit heating and air-conditioning systems).
• Filtering air by high-efficiency particulate air (HEPA) filters removes the droplet nuclei from recirculated air.
• Ultraviolet irradiation of the upper air within the shared space (when feasible) may reduce the spread of infection by killing tubercle bacilli suspended in the droplet nuclei.
Contact risk factors.
Persons who have recently shared air with the source patient may be considered potentially infected contacts. The following factors are known to modify the risk of infection for these persons:
• Prior infection with tuberculosis, as indicated by a significant skin-test reaction before exposure to the identified source patient, reduces risk.
• Increased time in association with the source patient influences the probability of infection.
• Physical closeness between the source patient and the contact may influence the likelihood of infection.
B. Structuring a Contact Investigational Program
Establishment of Investigational priorities. The estimated probability of transmission, based on information obtained by following the steps described above, should influence the priority, rapidity, and thoroughness with which a contact investigation is conducted. By using this systematic approach, appropriate and productive public health programs can be implemented.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 32
Attachment F : page 3 of 3 Classification of contacts. For each source patient, the contact investigation should proceed in an orderly manner, starting with persons who are most likely to have been infected. Members of the immediate family or others who have shared accommodations with the source patient in the recent past usually are labeled household contacts. Contacts in working, leisure, or other settings are designated by other terms such as “close”, “intimate”, or “casual”. The most important consideration in a contact investigation is the probability of infection among contacts; therefore, the first step is to allocate contacts into higher and lower-risk contacts.
A higher-risk contact is defined as any person who shared the environment air with a source patient for a relatively longer time and who has other risk factors relatively higher than those of other known contacts. Nursing home/facility residents sharing the same wing or ventilation circuit should usually be considered close contacts. C. Establishing Limits for Contact Investigations
By initially evaluating the higher-risk contacts for evidence of tuberculous infection and/or disease, the actual infectiousness of the source patient can be inferred. The following are guidelines for limiting the extent of a contact investigation:
• Initiate investigation with higher-risk contacts; If there is no evidence of recent transmission of infection in this group, extending the investigation is not appropriate.
• If data indicate recent infection in the higher-risk group, extend the limits of investigation to progressively lower-risk contacts until the levels of infection detected approximate the levels of infection in the local community.
• At each stage of the investigation, establish the number and identity of contacts to be examined. Establishing such a denominator helps to assure that no contact who should be examined is missed.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 33
Attachment G-1
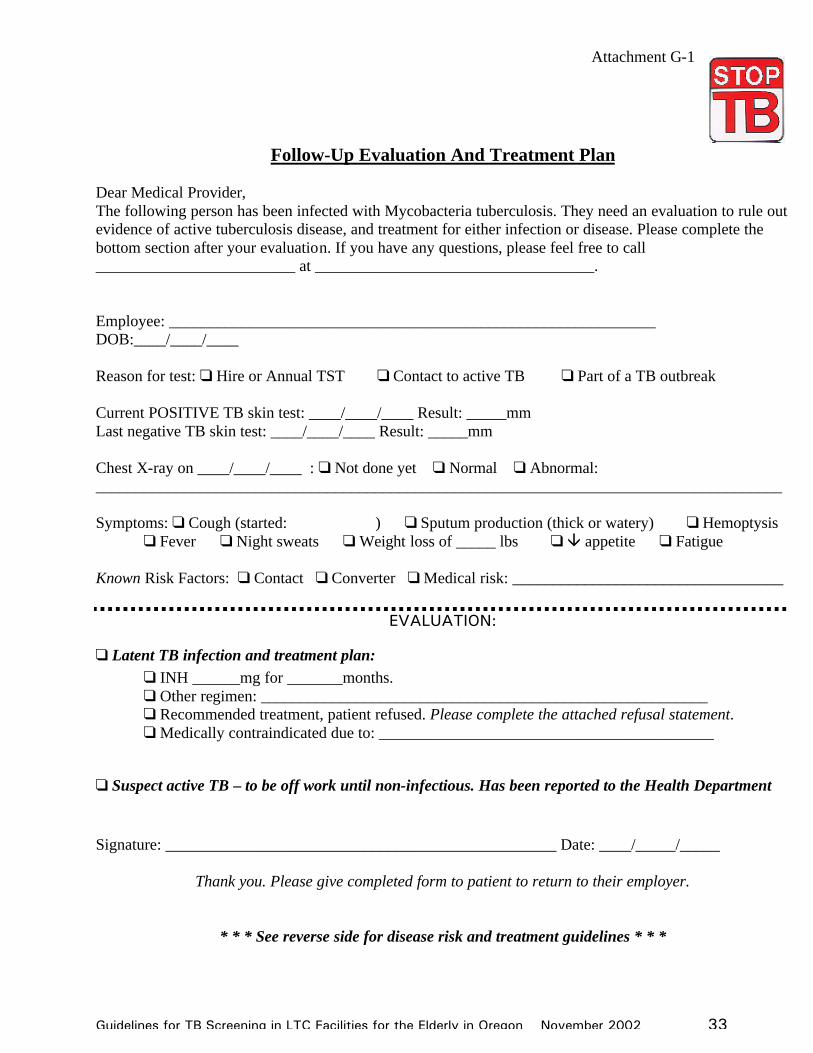
Follow-Up Evaluation And Treatment Plan Dear Medical Provider, The following person has been infected with Mycobacteria tuberculosis. They need an evaluation to rule out evidence of active tuberculosis disease, and treatment for either infection or disease. Please complete the bottom section after your evaluation. If you have any questions, please feel free to call _________________________ at ___________________________________. Employee: _____________________________________________________________ DOB:____/____/____ Reason for test: q Hire or Annual TST q Contact to active TB q Part of a TB outbreak Current POSITIVE TB skin test: ____/____/____ Result: _____mm Last negative TB skin test: ____/____/____ Result: _____mm Chest X-ray on ____/____/____ : q Not done yet q Normal q Abnormal: ______________________________________________________________________________________ Symptoms: q Cough (started: ) q Sputum production (thick or watery) q Hemoptysis
q Fever q Night sweats q Weight loss of _____ lbs q â appetite q Fatigue Known Risk Factors: q Contact q Converter q Medical risk: __________________________________
EVALUATION:
q Latent TB infection and treatment plan: q INH ______mg for _______months. q Other regimen: ________________________________________________________ q Recommended treatment, patient refused. Please complete the attached refusal statement. q Medically contraindicated due to: __________________________________________
q Suspect active TB – to be off work until non-infectious. Has been reported to the Health Department Signature: _________________________________________________ Date: ____/_____/_____
Thank you. Please give completed form to patient to return to their employer.
* * * See reverse side for disease risk and treatment guidelines * * *
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 34
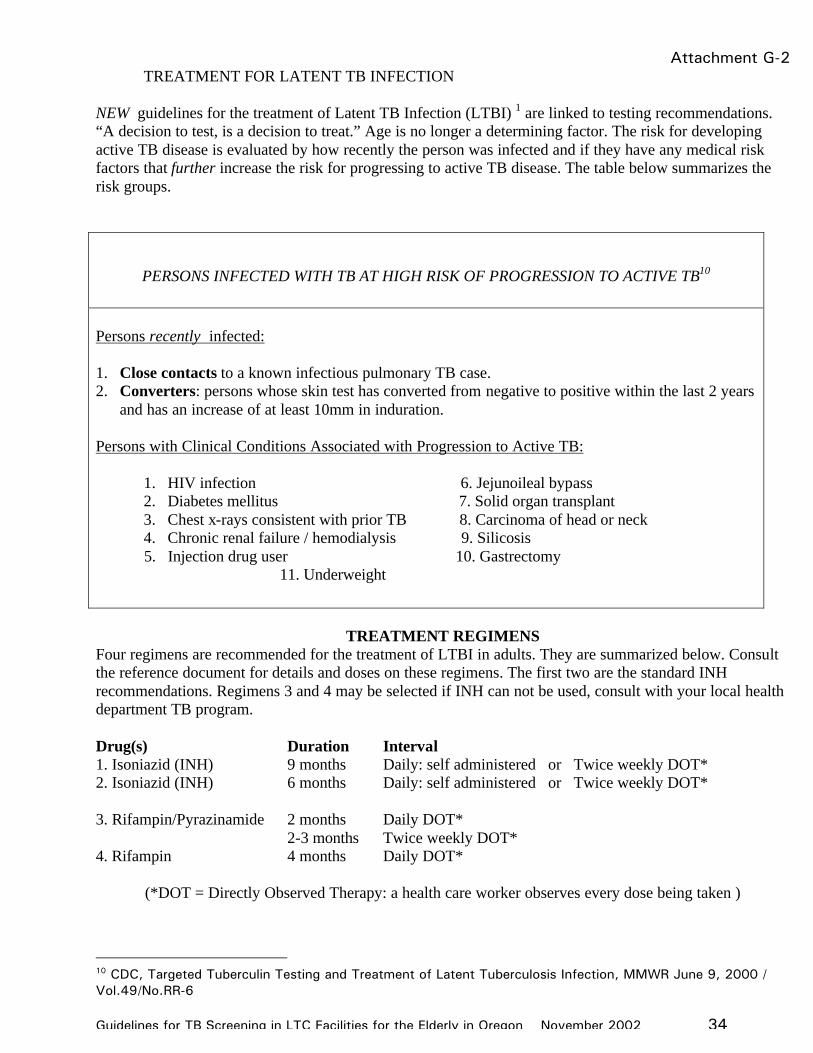
Attachment G-2TREATMENT FOR LATENT TB INFECTION
NEW guidelines for the treatment of Latent TB Infection (LTBI) 1 are linked to testing recommendations. “A decision to test, is a decision to treat.” Age is no longer a determining factor. The risk for developing active TB disease is evaluated by how recently the person was infected and if they have any medical risk factors that further increase the risk for progressing to active TB disease. The table below summarizes the risk groups.
PERSONS INFECTED WITH TB AT HIGH RISK OF PROGRESSION TO ACTIVE TB10 Persons recently infected: 1. Close contacts to a known infectious pulmonary TB case. 2. Converters: persons whose skin test has converted from negative to positive within the last 2 years
and has an increase of at least 10mm in induration. Persons with Clinical Conditions Associated with Progression to Active TB:
1. HIV infection 6. Jejunoileal bypass 2. Diabetes mellitus 7. Solid organ transplant 3. Chest x-rays consistent with prior TB 8. Carcinoma of head or neck 4. Chronic renal failure / hemodialysis 9. Silicosis
5. Injection drug user 10. Gastrectomy 11. Underweight
TREATMENT REGIMENS
Four regimens are recommended for the treatment of LTBI in adults. They are summarized below. Consult the reference document for details and doses on these regimens. The first two are the standard INH recommendations. Regimens 3 and 4 may be selected if INH can not be used, consult with your local health department TB program. Drug(s) Duration Interval 1. Isoniazid (INH) 9 months Daily: self administered or Twice weekly DOT* 2. Isoniazid (INH) 6 months Daily: self administered or Twice weekly DOT* 3. Rifampin/Pyrazinamide 2 months Daily DOT* 2-3 months Twice weekly DOT* 4. Rifampin 4 months Daily DOT*
(*DOT = Directly Observed Therapy: a health care worker observes every dose being taken )
10 CDC, Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection, MMWR June 9, 2000 / Vol.49/No.RR-6
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 35
REFUSAL TO ACCEPT TREATMENT for TUBERCULOSIS INFECTION Print Patient/Employee Name: __________________________________ Date of birth: ____/____/____ I have been advised, and understand the following:
⌦ I am infected with tuberculosis, which is currently not active. - my skin test for tuberculosis is ______mm, which is considered positive for tuberculosis - my chest x-ray does not indicate active tuberculosis in my lung at this time - I have no symptoms of active tuberculosis
q I am at HIGH risk to develop active tuberculosis because I have been recently infected (within the last two years). (check box if patient has medical risk factors) q I have a medical condition that increases the risk that I will develop active tuberculosis. (check
box if patient has medical risk factors) ⌦ If I do not treat my tuberculosis infection, it may become active in the future and make me sick. ⌦ I understand the most common type of active tuberculosis occurs in the lung; however, it can become active in any part of my body. Other sites of active tuberculosis can be in the brain (TB meningitis), bone, lymph nodes, kidneys, stomach or intestines, eye, basically any organ. ⌦ If I develop active tuberculosis I may spread it to other people.
The signs of infectious tuberculosis of the lung are:
1. Cough – lasting 3 or more weeks 2. Sputum production – able to cough up material from the lungs 3. Hemoptysis – coughing up blood 4. Fever – lasting longer than 5 days 5. Night sweats: sweating that dampens bed linens and/or pajamas 6. Fatigue or tiredness 7. Weight loss (unexplained 8 pounds or more)
⌦ Any time I develop the symptoms above (at least #1 and two of the other symptoms), my employer may refuse to let me work until I have been evaluated by my physician and receive written clearance that I do not have infectious tuberculosis.
⌦ I was advised to take m INH m Other: ______________________- to treat my tuberculosis ⌦ I was advised the risk of progressing to disease was greater than the risk of side effects to the medicine.
Signature of Patient/employee : ____________________________________ Date: ____/____/_____
Medical provider signature: ______________________________________ Date: ____/____/______ Please return this signed refusal to the employer who referred the patient in for evaluation and care.
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 36
Attachment H
RESOURCES
TB Guidelines: 1. Prevention and Control of Tuberculosis in Facilities Providing Long Term Care to the Elderly, 1990, MMWR; Vol 39 No. RR-10 2. Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health-Care Facilities, 1994 MMWR October 28, 1994; Vol.43 No. RR-13); pages 1-132. 3. www.cdc.gov/nchstp/tb TB Training Materials: 1. www.cdc.gov/nchstp/tb 2. www.nationaltbcenter.edu 3. www.umdnj.edu/ntbc 4. www.harlemtbcenter.org 5. Attached sample TB training for Long Term Care (to review and download powerpoint from www.healthoregon.org/tb )
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 37
Slide 1-2
TB Control for Long Term Care Facilities in Oregon
Tuberculosis Bacteria: Mycobacteria tuberculosis
• TB Worldwide– 1/3 of population is infected– 8+ million new cases– 3 million deaths
• TB in U.S.– Increased late 1980’s-1992
– Rate decreasing since 1992
Slide 3-4 TB Transmission
• Airborn• Not spread by:
- fomites (things), food, or vectors
• Usually need prolonged, repeated exposure
Usual Groups at Riskfor Exposure to Tuberculosis
• Close contacts to infectious cases of TB• Foreign born from countries where TB is
common• Residents and employees in congregate
settings at high risk for TB
Slide 5-6 Pathogenesis
• Most exposed do NOT become infected
• Breathe germs into base of lungs• If infected, germs spread
throughout the body• The immune system controls the
infection
TB Pathogenesis
• Most infected do NOT progress to disease• Progression risk varies by:
- age- immune status- when infected
50% of risk occurs in 1st 2 years
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 38
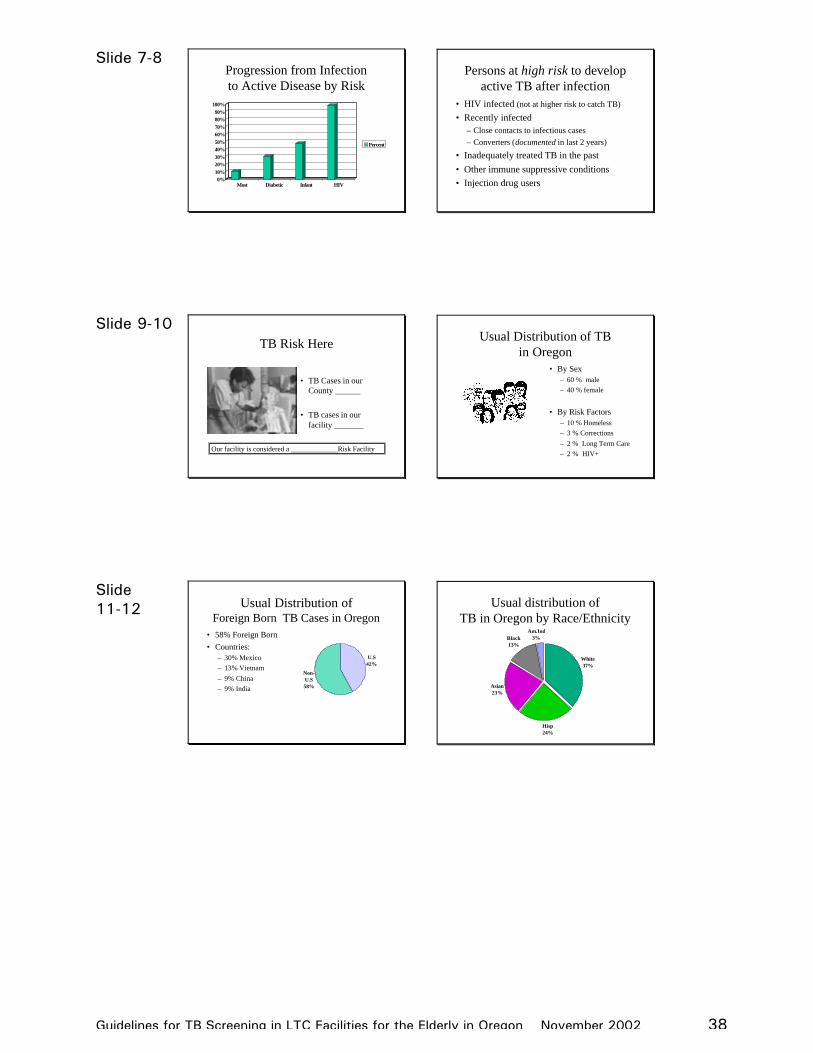
Slide 7-8 Progression from Infection to Active Disease by Risk
0%10%20%30%40%50%60%70%80%90%
100%
Most Diabetic Infant HIV
Percent
Persons at high risk to develop active TB after infection
• HIV infected (not at higher risk to catch TB)
• Recently infected– Close contacts to infectious cases– Converters (documented in last 2 years)
• Inadequately treated TB in the past• Other immune suppressive conditions• Injection drug users
Slide 9-10 TB Risk Here
• TB Cases in our County ______
• TB cases in our facility _______
Our facility is considered a _____________Risk Facility
Usual Distribution of TB in Oregon
• By Sex– 60 % male– 40 % female
• By Risk Factors– 10 % Homeless– 3 % Corrections– 2 % Long Term Care– 2 % HIV+
Slide 11-12 Usual Distribution of
Foreign Born TB Cases in Oregon• 58% Foreign Born• Countries:
– 30% Mexico– 13% Vietnam– 9% China– 9% India
U.S42%
Non-U.S58%
Usual distribution of TB in Oregon by Race/Ethnicity
White37%
Hisp24%
Asian23%
Black13%
Am.Ind3%
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 39
Slide 13-14 Usual Drug Resistance Patterns
in Oregon
• 10-12 % resistant to INH– if >4% start 4 drugs
• 1 % MDR* =– needs specialist– > 2 years of treatment*Multiple drug resistant
Diagnosis & Treatment of
• TB Infection: latent– Not active– NOT infectious– Not sick– (+)TST, CXR normal– Potential for disease in
future– Tx with 1-2 drugs
• TB Active Disease– May be infectious– Sick– (+)TST, CXR
abnormal if pulmonary– Tx with 4 drugs
Slide 15-16 Diagnosis: Latent TB Infection
• Tests:- Mantoux (+) - CXR negative- if asymptomatic, microbiology tests are not needed
• History & Physicalno symptoms
LTBI
Treatment of Infectionwho?
• all high risk for disease– Close contact to infectious case– Converter– HIV infected– other medical risk factors
• No more age cut off
Slide 17-18 Treatment of TB Infection
• Treat with INH (Isoniazid)a. 6-9 months INHb. 9 months if HIV+ , “old TB”, or child
• New regimens:are possible, but should be used by a specialist who will provide proper medical management
Monitor Monthly for:
• Side effects:– physical evaluation
- verbal symptom review- liver function tests if
indicated
• compliance
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 40
Slide 19-20 Diagnosis:
Active TB Disease• History & Physical• Symptoms of long duration
- Generalized:fever, night sweats, wt. loss, fatigue
- Site specific:Pulmonary - cough, sputum, hemoptysisExtra-pulmonary - varies by site
Diagnosis Active TBTests:
• Mantoux(if not already positive)
• Chest x-ray
• Microbiology: – Sputum for AFB x3
smear ,culture, susceptibility
– Biopsy if not pulmonary
Slide 21-22 Treatment of
Active TB Disease• Standard 6 month regimen * :
2 mo: INH + RIF + PZA + EMB4 mo: INH + RIF
• DOT recommended for all
* IF susceptible, compliant, & good response
Alternative Tx Regimens
• for INH resistance: 6 months is ok start: INH + RIF + PZA + EMBcont*: RIF + PZA + EMB
• 9 months: (if can’t use PZA)start: INH + RIF + EMBcont*: INH + RIF
*susceptibility known
Slide 23-24 Alternative Tx Regimens
• TB & HIV on Protease Inhibitors: – 6 months
• start: INH + RBN + PZA + EMB• cont: INH + RBN
• Drug Resistant TB:– Start: INH + RIF + PZA + EMB– Cont: extend treatment & change Rx based on
susceptibilities
Treatment for MDR-TB
MDR-TB• Resistant to at least
INH and RIF
• mortality VERY high
• seek EXPERT consultation
MDR-TB Treatment:• seek EXPERT
consultation• treat with at least 2 oral 1
injectable
• treat minimum of 18-24 months AFTER culture converts to negative
Guidelines for TB Screening in LTC Facilities for the Elderly in Oregon November 2002 41
Slide 25-26 Monitor Monthly for:
• Response to treatment • Side effects:
– verbal symptom review – LFTs - baseline & PRN– visual acuity: EMB
• compliance: ALL on Directly Observed Therapy (DOT)
Employer’s Responsibility
• TB Control Plan• Screen employees &
residents per plan• Educate employees• Evaluate effectiveness of
TB Control Plan• Report active TB &
coordinate with local Health Dept. as needed
Slide 27-28 Reporting TB
• Active TB: at time of diagnosis
• Infection:– not reportable
• Outbreaks of Infection
County Health Dept.
Employee’s Responsibility
• Participate in screening– NOT contraindications:
• BCG, HIV, • History past positive w/o doc
• Attend annual TB education• Stay alert for symptoms of
active TB in at risk residents• Follow TB Control Plan
Slide 29-30 Use & Limits of TB Plan
• Will not prevent all exposures• Can reduce risk if ALL
employees stay alert for signs of active TB
• Infected persons who complete treatment have significantly reduced risk for active TB and spreading TB to others
Review Facility TB Risk Status
• What is facility’s TB Control Plan?
• Screening employees• Screening residents
• Reporting suspect TB