tshwane district wbot presentation - unicef · pdf filetshwane district wbot presentation...
TRANSCRIPT

TSHWANE DISTRICT WBOT PRESENTATION
Presenter: Mrs Lekwetji Komane
Date: 9 November 2016
Burgerspark Hotel
1
ECD KBS 2016 ©Lekwetji Komane

Introduction
Ward Based Outreach Team is one of the 4 streams of PHC Reengineering strategy that provides services to communities, families and individuals at community-based institutions and at a household level within a ward
WBOT serve as the cornerstone of community based PHC services and spearhead primary health activities, while providing links to referral networks, thereby helping to ensure the provision of services, care and support at local or municipal level.
2

AIMS
3
Strengthen the district health system (DHS) and do the basics better
Team approach including community health
workers (CHWs)
Improvement of health outcomes
Strengthening school health services
Ensures that outreach services are provided to communities door to door
Ward based PHC outreach team for each electoral ward

Benefits of WBOT
• Health promotion and preventive activities• Early diagnosis and referral of patients identified• Follow up of patients discharged from the Hospitals
different levels• Outreach into communities and homes of families
with family census• Early identification of individuals within families at
risk• Community involvement • Greater interaction with communities to get their
support
WBOT Structure
• WBOT Operational Manager per sub district
• Team Leader can be Professional Nurse or Enrolled Nurse
• Community Health Workers (CHW’s)

WBOT Team
Team Leader
CHW270
CHW270
CHW 270
CHW270
CHW 270
CHW270
WBOT Operational Manager

WBOT Structure
• WBOT DD
WBOT AD
WBOT OPS MANAGERS
WBOT OPS MANAGERS
WBOT OPS MANAGERS
WBOT OPS MANAGERS/CLUSTER
WBOT OPS MANAGER
TEAM LEADER TEAM LEADER TEAM LEADER TEAM LEADER TEAM LEADER
CHW CHW CHW CHW CHW
FACILITY MANAGERS
AREA MANAGERS AREA MANAGERS

Activities
8
Team Leader allocate 250 to 270 households to CHW
CHW’s visits households as per allocated number
DOTS for TB patients
Monitor treatment compliance
Data collected from all family members using standardised tool
Data collected is analysed and intervention strategies put in place by the team
Activities
9
Data is shared with the PHC facility
Delivery of medications
HBC
Follow up of PCR Pos Babies
Individuals are referred to different departments such as Social Department, Home Affairs
Awareness campaigns are conducted to address poor performance

Implementation of WBOT
• Community mobilization was conducted• Involvement of Ward councillors• Identification of Gov funded NGO’s• Appointment of Team Leaders• NGO management and CHW’s orientation• Mapping in the identified sites• Conducting institutional analysis• Allocation of 270 households to CHW• Training of CHW’s and Team Leaders data collection• 10 days training for CHW’s was conducted from April
2012 in partnership with FPD• CHW’s are in serviced on different topic in each site

Implementation of WBOT
• Tshwane District and City of Tshwane outreach programme are integrated
• Mapping was conducted and wards were shared by CoT and Tshwane
• An integration and Mapping document was compiled awaiting to be signed
• Institutional Analysis was conducted by Team Leaders
• Combined WBOT reporting since January 2015

Referral Route
12
Community Based Health Services
Health related activities organized by community leaders community health workers and other community based workers
Community Health Centre / Clinic
Organization by qualified personnel of Community Health Activities and supervision of Health Clinics and Health Post
District Hospital

WBOT Expansion
Year Team Leaders Teams Wards
2011 7 7 9
2012 8 9 14
2013 18 24 33
2014 46 43 47
2015 ( August) 103 118 68
2016 (August) 243 243 72
13

140
50
100
150
200
250
2011 2012 2013 2014 2015 ( August) 2016 (August)
7 8
18
46
103
243
7 9
24
43
118
243
914
33
47
6872
Team Leaders
Teams
Wards
WBOT Expansion from 2011 – 2016 (August)

Teams per Sub District
Sub District
Teams
1 86
2 31
3 28
4 14
5 10
6 57
7 17
Totals 243
15

160
50
100
150
200
250
1 2 3 4 5 6 7 Totals
86
31 28
1410
57
17
243
Teams per Sub District
Teams

Ward Coverage
Sub District Total Wards Wards Covered
1 28 23
2 12 10
3 23 13
4 11 2
5 3 3
6 23 16
7 5 5
17

Ward Coverage
180
20
40
60
80
100
120
1 2 3 4 5 6 7 Total
28
12
23
11
3
23
5
105
23
1013
2 3
16
5
72
Total Wards
Wards Covered

Training progress 2013 -2015
19
481
977
2541
0 0
571
0
500
1000
1500
2000
2500
3000
3500
4000
2013 2014 2015
CHWs phase 1 CHWs phase 2 Target

CHW Competency Rate
20
321
214
79
18
970
752
156
62
0
200
400
600
800
1000
1200
CHWs Assessed Competent Re-Assessment Incompetent
76% passed ; 20,7% Re-exam ;04% Failed
2014 2015

WBOT Perfomance 2015 -2016
• Household Registration – 360,651
• Follow Up – 299,248
• Supervised Visit – 20,899
• Pregnant Mothers referred – 21,939
• Postnatal seen – 21,263
• Ref to Clinic – 95,464
• Ref Social Services – 155,176
• Vit A given – 53,773
• HCT – 41,620
21
Narratives
• Total coverage 72/105 = 68.6 %
• Sub District 3 & 4 are the elite areas and thus not yet covered by teams
• Coverage of Disadvantaged areas is 89 %
• Wards covered are not entirely covered
22

NUTRITION Target 201516 201617 (1ST Q)
Vitamin A dose 12-59
months coverage
(annualised) 50 % 36.5% 50.2 %
Antenatal 1st visit
before 20 weeks rate 70 % 46.7 % 57.2 %
23
Improved performance
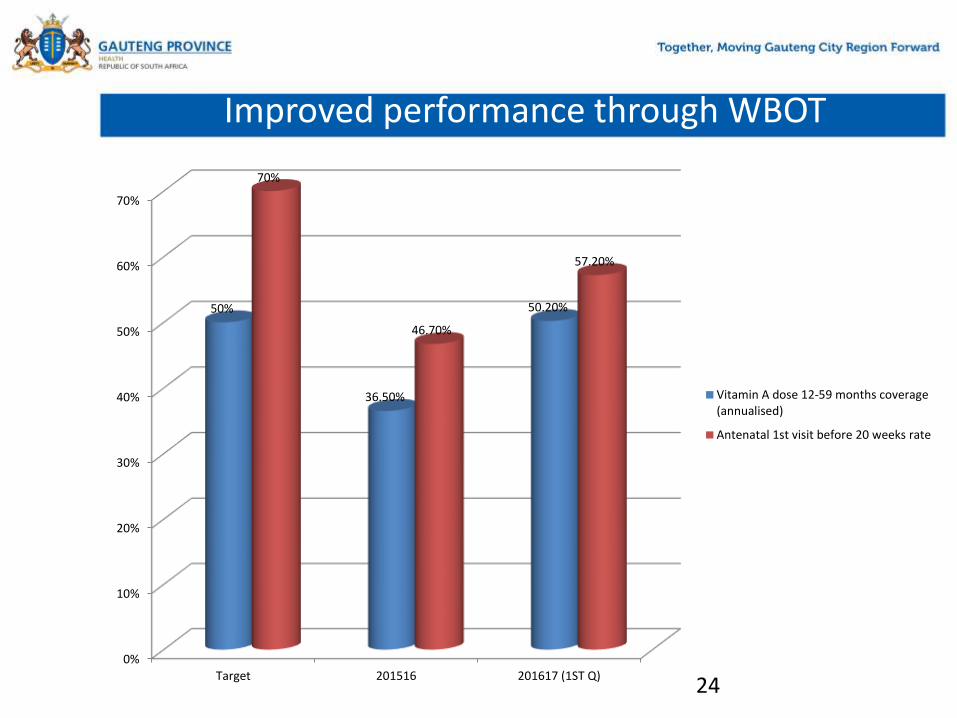
Improved performance through WBOT
240%
10%
20%
30%
40%
50%
60%
70%
Target 201516 201617 (1ST Q)
50%
36.50%
50.20%
70%
46.70%
57.20%
Vitamin A dose 12-59 months coverage(annualised)
Antenatal 1st visit before 20 weeks rate

Improved Performance
25
• Vit A :
Training of CHW’s on Vit A , RTH Booklet and Administration of Vit A
Collection of Vit A from the PHC Facility
Provision of Vit A at household level
Submission of data to facility managers
Community awareness and campaigns

Improvement Performance
• Early ANC Booking:
History taking at household level
Identification of Pregnant mothers
Referral for ANC booking
Follow up of referred pregnant mothers per facilities
Comparison of referred vs those referred who booked at PHC facilities
26

WBOT Intervention
• Identified challenges are addressed differently eg Referral to different department such as Home affairs, Social workers etc
• Health challenges can be addressed through awareness campaigns
27
