trust public board of directors - swast.nhs.uk board papers/mayboar… · chair tony fox (tf),...
TRANSCRIPT
Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 3
Trust Public Board of Directors Agenda
Date Friday 25 May 2018 Time 1000-1300
Venue St James A, Great Park Road, Bradley Stoke, Bristol, BS32 4QJ
Chair Tony Fox (TF), Chairman
Members:
Tony Fox (TF), Ken Wenman (KW), Amy Beet (AB), Gail Bragg (GB), Jessica Hodgman (JH), Venessa James (VJ), Minesh Khashu (MK), Jennie Kingston (JK), Paul Love (PL), Rakhee Rankin (RK), Ian Reynolds (IR), Andy Smith (AGS) and Jenny Winslade (JW)
Non Members:
Susan Bradford (SB),Marty McAuley (MM), Martin Roe (MR) and Claire Warner (CW)
Circulation Jo Fowles, Chris Nelson and Council of Governors
Minutes Julie Smalley
Opening Business
No Topic Purpose Format Lead Timing
1 Welcome, Introduction & Apologies Information Verbal TF 1000
2 Declarations of Interest Approval Verbal MM
3 A Patient Experience Information Verbal JW 1005
4 Report from the Chairman Information Verbal TF 1015
5 Report from the Chief Executive Information Verbal KW 1020
6 Questions from the Public Information Verbal TF 1025
7 Minutes of Previous Meeting – 29 March 2018 Approval Paper 1 MM 1030
8 Action Point Register Approval Paper 2 MM
9 Communications Update Information Paper 3 CW 1035

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 3
Quality and Patient Safety
10 Annual Patient Safety and Experience Report Assurance Paper 4 JW 1040
11 Quality Improvement Plan Assurance Paper 5 JW 1050
12 Quality Committee Assurance Report Assurance Paper 6 VJ 1100
13 Mental Health Strategy Approval Paper 7 AGS 1105
People and Culture
14 Annual Health and Safety Report Assurance Paper 8 JW 1115
15 Annual Security, Violence and Aggression Report Assurance Paper 9 JK 1125
16 People and Culture Three Year Strategy (2018-2021) Approval Paper 10 AB 1135
17 People & Culture Committee Terms of Reference Approval Paper 11 RR 1140
Performance and Finance
18 Trust Strategy 2018-2019 Approval Paper 12 KW 1150
19 Integrated Corporate Performance Report Assurance Paper 13 KW 1200
20 Trust Financial Position Assurance Verbal JK 1210
21 Standing Financial Instructions Approval Paper 14 JK 1220
Regulation
22 NHS Improvement Self Certifications Approval Paper 15 JW 1225
23 NHS Improvement Activity Update Assurance Paper 16 JK 1230
24 General Data Protection Regulations (GDPR) Update Assurance Paper 17 MR 1235
Internal Control and Governance
25 Joint Board Assurance and Risk Report Assurance Paper 18 JW 1240
26 KPMG Well Led Governance Review Action Plan Approval Paper 19 MM 1245

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 3
Closing Business
27
Questions Arising from the Meeting Any Other Business Identification of New Risks (incl. Health & Safety)
and New Legislation - Verbal TF
1255
28
Exclusion of the Press and Public To consider whether pursuant to the provisions of
section 1(2) of the Public Bodies (Admission to Meetings) Act 1960, the press and public be excluded from the remainder of the meeting on the grounds that publicity would be prejudicial to the public interest by reason of the confidential nature of the business about to be transacted.
Approval Verbal TF
Date of Next Meeting: Thursday 26 July 2018 Derriford Training College, Morlaix Drive, Plymouth, PL6 5AB
Page 1 of 25
Minutes Trust Public Board of Directors Date: 24 May 2018
Paper Title: Minutes of Trust Public Board of Directors Meeting 29 March 2018
Prepared by: Julie Smalley
Presented by: Tony Fox, Chairman
Action: Approval
Recommendation: The Trust Board of Directors is asked to review and approve the Minutes from the Trust Public Board of Directors Meeting on 29 March 2018.
Confidentiality Status Implications
Trust Public Board of Directors Meeting 29 March 2018 10:00 hours North Bristol Operations Centre, 400 North Bristol Park, Filton, Bristol, BS34 7QH Members: Mr T Fox TF Chairman Mr K Wenman KW Chief Executive Dr I Reynolds IR Non-Executive Director Mrs G Bragg GB Non-Executive Director Mrs R Rankin RR Non-Executive Director Mrs S Bradford SB Associate Non-Executive Director Mrs J Kingston JK Deputy Chief Executive/Executive Director of Finance Dr A Smith AGS Executive Medical Director Mr F Gillen FG Executive Director of IM&T Ms J Hodgman JH Acting Executive Director of Operations Non Members:

Page 2 of 25
Mr M McAuley MM Trust Secretary Mrs A Beet AB Acting Director of HR & OD Mrs C Warner CW Head of Marketing, PR and Communication Guests: Mrs S James SJ Deputy Director of Nursing and Quality Mrs V Williams VW Head of Quality Mr C Holmes CH Public Governor, Gloucestershire Mr R Care RC Public Governor, Bristol and B&NES Ms J Fowles JF Staff Side Representative Ms H Guest HG Patient Experience Speaker No Agenda Item Action 1.0 Welcome, Introduction & Apologies 1.1 1.2 1.3
TF welcomed everyone to the meeting and thanked them for attending. TF welcomed Sarah James, Deputy Director of Nursing and Quality, Vanessa Williams, Head of Quality representing Jenny Winslade, Executive Director of Nursing and Quality, Craig Holmes, Public Governor, Rae Care, Public Governor and Jo Fowles, Staff Side Representative. Apologies were received from Jenny Winslade, Executive Director of Nursing and Quality, Venessa James, Non-Executive Director, Minesh Khashu, Non-Executive Director and Paul Love, Non-Executive Director.
2.0 Declarations of Interest 2.1 There were no declarations of interest.
3.0 A Patient’s Experience 3.1 3.2 3.3
TF welcomed Hannah Kent to the Trust Board of Directors Meeting and thanked her for attending to share her experience of the Trust. Hannah shared her experience with the Trust Board of Directors when her son had fallen from a zip wire injuring his arm. The Paramedic in a Rapid Response Vehicle had initially found it difficult to find the patient from the details provided and Hannah received a call from the

Page 3 of 25
3.4 3.5 3.6
Clinical Hub and, though, she did not know the road name she was able to provide details of how to get to them. On arrival Hannah advised that the Paramedic’s attitude and initial comments had upset her and her son. The Paramedic diagnosed a left wrist fracture and Hannah took her son to hospital where it was discovered that he had fractured both wrists, the left requiring an operation. As a result of the investigation into the incident, the Paramedic was referred to the Learning and Development Team. The Paramedic wrote a letter of apology to the patient. The Chief Executive thanked Hannah for attending the Trust Board of Directors Meeting and for sharing her experience. The Chief Executive apologised to Hannah for the unsatisfactory care provided and he was concerned that a member of staff had not displayed a professional and caring attitude to her son. This was unacceptable. The Chief Executive was pleased to hear that the Paramedic had reflected and learned from the incident. This case would be used as a learning example for training and from a serious incident perspective. TF thanked Hannah for attending the Trust Board of Directors Meeting and for sharing her and her son’s experience.
4.0 Report from the Chairman 4.1 4.2 4.3 4.4
TF reported that the Health Watch Open Day held at Trust HQ on Friday 23 February 2018 had been a success. The Council of Governors Development Day had been a positive and productive day with good feedback and good development. TF had attended the Association of Ambulance Chief Executives Chairs’ Meeting. TF reported that the new Chairs had started to shape how they would be involved and have a voice. TF and the Chief Executive had met with the MP for Swindon recently and this had been a valuable meeting. TF advised that he would be meeting with MPs in the Trust area over the next few months to talk about pressures and challenges on the service. TF would also be meeting with Acute Trust Chairs, Clinical Commissioning Group Chairs and STP Chairs.

Page 4 of 25
4.5 4.6 4.7
TF, the Executive Team and various members of staff from the Trust had attended the Ambulance Leadership Forum. The agenda was good and had covered items on culture and leadership. Simon Stevens, Chief Executive of NHS England had been a Speaker and had provided his insights recognising there would be a longer term funding issue for the NHS and the challenges associated with that. The Deputy Chief Executive/Executive Director of Finance reported that she had met Simon Stevens when he visited Plymouth City Council recently. He had talked about the NHS and the Social Care Agenda. The visit was to understand how the NHS and Council work together on shared budgets. At the visit Simon Stevens had fed back how positively the ambulance services had received the news at the Ambulance Leadership Conference regarding frontline paramedics and the system risk that the service carries particularly in the clinical hubs. TF formally thanked the Executive Director of IM&T for attending his last Trust Board of Directors Meeting and for his contribution to the Trust Board of Directors and the Trust. TF wished him all the very best with his new ventures.
5.0 Report from the Chief Executive 5.1 5.2 5.3 5.4
The Chief Executive provided an update on the Ambulance Response Programme (ARP) and that this presented a funding gap of £12m. The Chief Executive advised that interviews had taken place to appoint a new Executive Director of IM&T. The process had been good with a good set of candidates. There had been an External Specialist and Non-Executive Director on the Interview Panel. The Chief Executive confirmed that the position had been offered to one of the candidates and they had accepted the role subject to the substantive offer and references. The Chief Executive provided an update on the Salisbury Incident. The Hazardous Area Response Team (HART) was still deployed and would be for another six weeks. No mutual aid had been requested at the time of the meeting. The Trust had carried out two debriefs and a meeting had taken place at Salisbury Ambulance Station to say thank you to the staff. The Trust awaits information on whether the two ambulances and two Rapid Response Vehicles used at the Salisbury Incident would be returned to the Trust following decontamination or whether they would need to be destroyed.

Page 5 of 25
5.5 5.6 5.7
Two ambulance stations remained closed at Amesbury and Salisbury. The staff from the Salisbury and Amesbury are working from Salisbury Hospital. The Trust had not yet commenced decontamination of the two ambulance stations involved. GB asked whether other Trust resources than HART were involved with the Salisbury Incident. The Chief Executive advised that there was a Gold Command teleconference every day and the senior level command structure was involved. IR was concerned about the closure of the Ambulance Stations. The Chief Executive advised that there was a source of funds from Government that the Trust could apply for to assist with costs of equipment, resources and buildings incurred during the Salisbury Incident, though the amount the Trust would receive had not been confirmed. The Chief Executive was pleased to advise that the Care Quality Commission (CQC) had invited the Trust to present at a Development Day for CQC Inspectors. The Trust would present on Caring. The Trust had been asked as it had achieved outstanding for the Caring domain as part of its inspection and rating. The Trust Team presented well and positive feedback had been received.
6.0 Questions from the Public 6.1 6.2 6.3
The Trust Board of Directors had received a question from a member of the public, Bren McInerney: “How many times has the Trust cited the NHS Constitution in its strategic work over the last 12 months?” The Trust Secretary advised that the NHS Constitution had been cited in the following documents; New Trust Strategy Trust Corporate Statements Human Resource and Organisational Development Strategy National Standard Contract and Contract with sub-contractors Communications and Engagement Strategy. TF confirmed that following today’s meeting he would be sending a letter answering the question to Bren McInerney as agreed. ACTION: TF to write to Bren McInerney in response to his question to the Trust Board of
TF

Page 6 of 25
Directors.
7.0 Minutes of the Previous Meeting – 25 January 2018 7.1 The Minutes of the Trust Public Board of Directors on 25 January 2018 were
approved as a correct record of proceedings.
8.0 Action Point Register 8.1 The Trust Secretary presented the Action Point Register. Updates and
commentary were noted by the Trust Board of Directors.
9.0 Communications Update 9.1 9.2 9.3 9.4 9.5 9.6
The Head of Communications presented the Communications Update for information. The Head of Communications highlighted a significant proportion of the articles published since the last report had been deemed to be positive, 37.9% and only 1% of press coverage was class as negative, with the remainder of the enquiries being neutral/balanced. The Head of Communications was pleased to announce that the Volunteer of the Year Award had been presented to Mike Kemp, Community First Responder and that three other members of staff and volunteers had been shortlisted for the Unsung Hero Awards. Social Media Activity was discussed and the Head of Communications advised that the team had worked hard over the winter period with partners to co-ordinate messages and audiences. The number of followers had risen. The reach and likes had significantly increased which was extremely positive for the Trust. The Trust Website had highlighted the Time to Care Campaign and the Student Paramedic Conference. GB asked if the Chief Executive’s interactive e-bulletin was received by Volunteers. The Head of Communications advised that the Volunteers had a monthly Responder Review which included corporate messages and as the e-bulletin is staff focused this was not currently shared. Articles that are relevant would be added to the Responder Review.

Page 7 of 25
9.7 9.8 9.9 9.10
The Chief Executive asked whether the e-bulletin was not shared because Volunteers do not have a Trust email account. The Executive Director of IM&T advised that some parts of the e-bulletin would be available externally. The Head of Communications advised that the full bulletin is not shared because there may be Union articles and stories directly related to staff and she would not wish to overwhelm Volunteers with unnecessary information. TF thanked the Head of Communications for the work undertaken with the media. TF asked the Head of Communications how the Trust compared to other services in the South West. ACTION: The Head of Communications is currently undertaking a piece of work involving other Ambulance Trusts for a comparison and would report on this at the next Trust Board Meeting in May 2018. The Trust Board of Directors noted the Communications Update for information.
CW
10.0 Patient Safety and Experience 10.1 10.2 10.3 10.4
The Head of Quality presented the Patient Safety and Experience Report which was a summary of two papers that had been submitted to the recent Quality Committee. The Report covered the period 1 October 2017 to 31 December 2017. The Report was provided for assurance. The Head of Quality reported that the Trust had seen a decrease in Serious Incidents relating to the A&E Service line and a decrease in complaints and Adverse Incidents. There had been an increase in plaudits which was positive for the Trust. There had been nine Serious Incidents raised for A&E Service Line plus an additional two for IM&T. There had been no serious or moderate incidents for the Urgent Care Service. The Head of Quality was pleased to announce that during Quarter three the Trust had met its responsibilities under the statutory Duty of Candour. GB asked for clarification of the campaign ‘Bare below the elbow’. The Chief Executive advised all that uniform wearing ambulance staff must not wear anything below the elbows eg watches, bangles, rings etc. This is part of the Trust ethos, culture and infection control.

Page 8 of 25
10.5 10.6 10.7 10.8 10.9 10.10 10.11
SB asked how non-injury fallers become adverse incidents. The Head of Quality advised that as part of the system with Right Care the staff have to report if there has been an inappropriate attendance at a Care Home for someone who has fallen but not sustained an injury. If this relates to another organisation the Trust would ask for an investigation by that service and then the Trust would provide feedback to staff. The Executive Medical Director confirmed that the Right Care Team would offer training to the external healthcare organisation on how to lift non-injured fallers. ACTION: The Head of Quality to amend the report under section 5, Claims to all A&E Service Line. The Trust Secretary read out comments received from PL in his absence. PL had noted the marked reduction in serious and adverse incidents and complaints. Given the early winter pressures and comments he had received from staff that Quarter 3 had been difficult with demand and resourcing this was a significant achievement. SB asked if there should be an average over the past few years rather than just one year for data. GB agreed with SB that it would be good to receive trend graphs. ACTION: The Chief Executive requested more graphs with less narrative and asked the Head of Quality to consider providing a trend analysis once a quarter with exceptions and explanation of trends and why they have changed. The Head of Quality to work with VJ. TF advised weighting per 1,000 incidents less complaints to the 1,000 incidents. The Executive Medical Director reported that he and the Head of Quality had attended the Joint QGARD and National Ambulance Service Medical Directors Meeting at the recent Ambulance Leadership Forum and there is work being undertaken on a national learning reporting system (PROCLUS).. This product would allow more benchmarking data and shared learning on Serious Incident and Coroners decisions. TF thanked the Head of Quality for providing the report. The Trust Board of Directors took assurance from the Patient Safety and Experience Report.
VW VW
11.0 Trust Quality Improvement Plan
Page 9 of 25
11.1 11.2 11.3 11.4 11.5 11.6
The Head of Quality presented the Trust Quality Improvement Plan (QIP) for assurance. The Head of Quality advised that the QIP is monitored by the Quality Programme Board. The Plan contained a number of actions some of which had been transferred from the previous QIP and some identified as a result of ambulance station visits that had taken place. The Head of Quality reported that there were 63 actions open on the QIP. The team is undertaking a programme of mock inspections at Ambulance Stations. The Quality Buddy Scheme had also been introduced. This scheme provides managers in the Operations Directorate with a buddy from the Quality Team. The buddy provides local support. The Head of Quality reported that this was working well and that positive feedback had been received. The Head of Quality advised that the Trust had received the letter from CQC with the Provider Information Request (PIR). The first set of information had been returned by the deadline of 28 March 2018. The deadline for the final submission is 18 April 2018. The Deputy Chief Executive/Executive Director of Finance noted that some items on the QIP had been reopened. The Head of Quality advised that they had been reopened to test embeddedness. GB commended the Head of Quality and team on having no overdue actions. The Trust Board of Directors took assurance from the Quality Improvement Plan.
12.0 Freedom to Speak Up 12.1 12.2
The Acting Director of HR and OD presented the update on the Freedom to Speak Up arrangements. The new structure had been introduced incorporating the Trust Peer Support Guardians who had taken on an extended role of with the Freedom to Speak up agenda. The Human Resources Business Partners provide advice, guidance and mentorship to the Peer Support Guardians. The Trust Secretary provides independence to the role and is the nominated Freedom to Speak Up Guardian. The Non-Executive Director lead is VJ. GB supported the solution and asked how the Trust would measure that the system is working. The Acting Director of HR and OD advised that the Trust would measure whistle blowing returns quarterly. It was noted that these are

Page 10 of 25
12.3 12.4 12.5 12.6 12.7
also reported nationally. By monitoring that with the new structure the Trust would be able to identify if this increases for the numbers being reported. The Team would also review any concerns raised by staff via Datix, grievances and other avenues for observation, not always under public disclosure. Awareness of Freedom to Speak Up will be raised through the new structure. RR asked that when reporting would the Trust be looking at geography and different types of work groups. The Acting Director of HR and OD confirmed that geography and different types of work groups would be included in the monitoring. The Trust Secretary read out comments received from PL in his absence. PL reported that during recent visits to ambulance stations the notice boards had displayed the Peer Support Network contacts. ACTION: The Chief Executive asked Jo Fowles, Unison Representative in attendance at the meeting to promote Freedom to Speak Up and the new structure with the Peer Support Guardians through Unison. The Acting Director of HR and OD reported that the Peer Support Network had welcomed the recognition and the training provided to them. The Trust Board of Directors approved the new structure for the Freedom to Speak Up Agenda within the Trust and took assurance from the updates provided.
JF
13.0 Affordable Quality 13.1 13.2 13.3
The Deputy Chief Executive/Executive Director of Finance presented the update on Affordable Quality for assurance on the work being undertaken by the Quality Standards Working Group. The Deputy Chief Executive/Executive Director of Finance advised that the Quality Standards Working Group had been developed and members included; Management from both the clinical and non-clinical areas. The 10 Affordable Quality Principles were noted by the Trust Board of Directors. The Deputy Chief Executive/Executive Director of Finance advised that the principles provide a guide for thinking and these are being tested by the Senior Leadership Team and review has been undertaken of the Flexible Working Policy and Special Leave Policy. Following the principles the

Page 11 of 25
13.4 13.5 13.6 13.7
Executive Directors Group had referred one of their agenda items to the Quality Standards Working Group regarding resources in the Safeguarding Team. The Quality Standards Working Group provides assurance to the Quality Committee and the Finance Committee. The Deputy Chief Executive/Executive Director of Finance advised that the group is an informal group for ideas that are fed back into existing structures. It is a tool for staff to use. IR recognised the value of the Group. The Trust Board of Directors noted that comments made by PL that he was content with this approach. The Trust Board of Directors took assurance from the Affordable Quality Update.
14.0 Quality Committee Assurance Report 14.1 14.2 14.3 14.4 14.5 14.6 14.7
IR presented on the Quality Committee Assurance Report on behalf of VJ. IR reported that the Quality Committee had taken assurance from the Affordable Quality Report. The Quality Committee had reviewed the documents relating to the Supporting Hear and Treat Standard Operating Procedure. The Quality Committee had approved the Review of Shifts Overrun Report and for the pilot to commence on 19 February 2018. The pilot is ongoing. IR highlighted two issues that had been formally referred back to the Board of Directors. These related to the Quality Improvement Plan and Affordable Quality Working Group which have now been addressed by the Trust Board of Directors at the meeting today and are noted in the Minutes above. The Chief Executive advised that the Shift Overruns Trial in the North Division had been extended to the end of April 2018 to enable increased data capture for review. The Trust Board of Directors took assurance from the Quality Committee Assurance Report.

Page 12 of 25
15.0 Health & Safety Report 15.1 15.2 15.3 15.4 15.5 15.6 15.7 15.8
The Head of Quality presented the Health and Safety Report providing the Board of Directors with an overview of health and safety compliance during the period 1 April 2017 to 28 February 2018. ACTION: The Head of Quality highlighted there had been an error identified in section 4.6 and advised that the report would be re-circulated with the correct figure. The Head of Quality highlighted the key elements of the report and that it had been a positive to see fire warden training arranged and that risk assessment training was moving forwards. There had been a decrease in injuries to staff and an increase in RIDDOR incidents. Completion of Mandatory Training had been reviewed by the Health and Safety Committee and staff had been encouraged to complete the mandatory training. The Health and Safety Committee was working well with excellent engagement from staff side. The Committee is fully represented from every function across the organisation. The Managing Safety Course, previously provided by an external provider, would be provided by Health and Safety Officers moving forwards. The Trust has arranged for them to be accredited. This would be a cost saving. TF stated that it was a positive to see a reduction in incidents. The Head of Quality advised that data is being reviewed and an update on the graphs within the report would be presented to the next meeting. The Head of Quality Violence and Aggression would be in the Health and Safety Plans for the next year. ACTION: The Head of Quality to ensure this information is provided. The Trust Board of Directors took assurance from the Health and Safety Report.
VW VW
16.0 2017 Staff Survey – Early Review 16.1
The Acting Director of HR and OD presented the results of the 2017 Staff Survey published on 6 March 2018.

Page 13 of 25
16.2 16.3 16.4 16.5 16.6 16.7
The Summary position had decreased year on year. The Trust had held its own within the ambulance sector. Experiences reported by staff need to be in context of what taken staff have been through. The Trust Board of Directors noted that impact of the large scale rota review within the responses received. The Acting Director of HR and OD reported that the Top 5 results remained in line with results from the Staff Survey in 2016. Bullying and harassment had received a lower score and the Trust approach to Health and Wellbeing had been positive. The Acting Director of HR and OD advised that early actions in terms of work on bullying and harassment and WRES indicators had commenced. The team is engaging with Council of Governors and the national lead for WRES would be presenting to the Trust Board Seminar in April 2018. GB was concerned about the dissatisfaction of staff on the quality of care they can give and asked if this related to pressure and performance targets. The Acting Director of HR and OD advised that with increased demand over the last 12 months, the impact of the rota review and perceptions of staff around the demand placed on them would add to their feelings of not being able to provide the level of care that they would want to. The Chief Executive advised that the feedback from staff is in respect to the Trust not having enough resource leading to delays for patients and staff frustration in getting to patients quickly. Once on scene staff have all the tools they require and they are the best trained staff in country. The Chief Executive advised that there is pressure for staff to come off scene because some are far too long, however, the CQC event on caring mentioned earlier showed the dichotomy for the Trust with palliative care patients. Staff want to do the best for their patients. The Chief Executive advised that the cultural survey in the summer should provide feedback on bullying and harassment. He was concerned about claims of bullying and harassment from staff to staff. The growth of that was a concern. RR advised that she had visited ambulance stations and asked if it is actual bullying and harassment or the perception of the way in which overruns are managed or conversations around certain key performance indicators. Do managers need training on engaging with staff. The Acting Director of HR and OD advised that in order to grain better understanding the People and Culture Committee had requested a deep dive on Bullying and Harassment.

Page 14 of 25
16.8 16.9 16.10 16.11 16.12
The Executive Medical Director asked the Staff Side Representative for their thoughts on whether the survey gives a good reflection of what staff are concerned about. The Staff Side Representative suggested that not enough staff complete the survey and that contented staff do not always complete it. First contact by the managers with members of staff sets the tone for the meeting with them. The way this is handled makes the difference. The Acting Director of HR and OD advised that LGBT and disability data would be reviewed. The Trust had planned a BME Workshop on 4 May 2018. The Trust Secretary read out comments received from PL in his absence. PL was concerned by the marginal decline in staff engagement but the overall report was highly positive. Sector comparisons are strong, director of travel mainly in the right way, and those areas where the Trust has worsened could be a result of better reporting amongst informed and encouraged staff. The proposed actions were proportionate. GB asked that with WRES data does the Trust report management structure against staff. The Acting Director of HR and OD advised that the data is available. ACTION: WRES Data to be discussed by the People and Culture Committee. The Acting Director of HR and OD to action. The Trust Board of Directors noted the headline results of the Staff Survey 2017 and took assurance from the actions proposed.
AB
17.0 Integrated Corporate Performance Report 17.1 17.2 17.3 17.4
The Acting Executive Director of Operations presented the Integrated Corporate Performance Report (ICPR) for assurance. The ICPR provided an overview of Trust Performance up to and including the end of February 2018. The Acting Executive Director of Operations reported that the Spring Review of the Ambulance Response Programme would be published in April 2018 and would be ratified towards the end of the April 2018 prior to full implementation. There are a number of Ambulance Services that would not be able to deliver the ARP Standards by September 2018 and they are working on Transition Plans with their Lead Commissioners. The Acting Executive Director of Operations reported that there had been a number of challenges with performance over the previous two months mainly

Page 15 of 25
17.5 17.6 17.7 17.8 17.9 17.10 17.11 17.12 17.13
due to adverse weather. The resourcing levels had been good but there had been an increase in activity. Normal business rules have returned and this is reflected in the more recent Trust performance. There had been a number of documents produced and debrief meetings undertaken by the Trust following the adverse weather. The Easter Plan had been drafted and resourcing levels over Easter are good across the Trust but would be subject to last minute sickness and absenteeism. It was noted that activity in Somerset, East Division had increased. No reason had been identified for the increase. The Head of Clinical Hubs had been working with the Acting Executive Director of Operations to meet every Dispatcher as part of continuing training. There had been attention to profiling of resources during the day in terms of staff and fleet mix. The Head of Resourcing had been working with IT and a new report had been developed identifying resource cover. To deliver performance improvements and where possible reduce the Trust response times to all categories of incident the Trust had undertaken a three phase approach as noted within the ICPR. Phase One included the Trust wide Rota Review to align rotas and fleet ratios to meet the new (increased) demand profiles and tackle inefficiencies. The Trust is now in the phase of reviewing issues raised following the six month review of the rotas in the East and West Divisions. The Programme Lead for the QPIP was on secondment to the role and this had been extended to the end of June 2018. The Acting Executive Director of Operations meets with the Executive Team to review the Performance Improvement Plan and contributions from other directorates to this. 111 Service The Trust Board of Directors noted that the 111 Service performance had now stabilized and noted that there would be changes to some of the rotas in this area. GP Out of Hours Service The Acting Executive Director of Operations reported some improvement to

Page 16 of 25
17.14 17.15 17.16 17.17 17.18
granularity and compliance. There had been improvement in the home visiting targets. Tiverton Urgent Care Centre Tiverton Urgent Care Centre performance had dropped the previous week. This was the first time this had happened since the contract commenced. Craig Holmes, Public Governor, noted the percentage of calls closed by telephone advice. The Trust had previously been ahead of other ambulance services but was now at 5%. He asked if the measure had changed. The Executive Medical Director advised that the measure had changed was significantly different. Craig Holmes, Public Governor noted that in December 2017 extra resources had been put into the Hub and asked whether that had been cost effective. The Executive Medical Director stated that it had been more cost effective. SB asked whether any other learning had been gained than that included in the ICPR with regard to the 7 Minute Category 1 incidents. The Chief Executive reported that the Trust liaises with other services and the most common denominator is resources. The Chief Executive provided assurance that through the ORH modelling work and the call cycle work everything had been done but there would need to be a stepped increase in resource before the Trust would see a major change. Everything in the Performance Improvement Plan should make a difference. The Trust is currently working with East of England Ambulance Service to ensure the Trust is capitilising on everything that it can. Rae Care, Public Governor was concerned about the performance figures for Cornwall. The Chief Executive advised that Cornwall is the most rural area of the Trust and other areas of the Health System in Cornwall had also been challenged. The Trust Board of Directors took assurance from the ICPR.
18.0 Trust Financial Position 18.1
See item below (19.0)
19.0 Finance Committee Assurance Report 19.1 The Deputy Chief Executive/Executive Director of Finance provided a verbal

Page 17 of 25
19.2 19.3 19.4 19.5 19.6 19.7 19.8 19.9 19.10 19.11
update on the Finance Committee and Trust Financial Position which had been included in the ICPR. The end of financial year had been discussed at the Finance Committee. The Finance Committee had noted that the Month 11 position and Month 12 position remained consistent with reporting year to date. The Trust would aim to deliver a breakeven position. The Deputy Chief Executive/Executive Director of Finance reported that the more detailed position for the Capital Programme would be approximately 75%. The Deputy Chief Executive/Executive Director of Finance advised that this did not raise any concerns as this should improve during 2018/19. The Deputy Chief Executive/Executive Director of Finance had been concerned about the increasing level of salary overpayments. The Trust Board of Directors took assurance that the Finance Committee and Audit and Assurance Committee were monitoring them. The Deputy Chief Executive/Executive Director of Finance advised that the Dorset Integrated Urgent Care tender process was progressing in line with the timeline dates. Tiverton Urgent Care Contract was noted to be commercially sensitive and was therefore not appropriate for the public session. The Draft Operating Plan 2018/19 had been submitted in line with the deadline in March 2018. The final Operating Plan 2018/19 would be considered by the Trust Board of Directors on 26 April 2018 prior to submission to NHS Improvement on 30 April 2018. The Finance Committee had received a presentation on National Procurement Activity. GB advised that it was reassuring that the Trust is part of the national project. GB advised that the Finance Committee had also discussed benchmarking and data within the Carter Pack. GB had met and received an update from the Programme Lead for the Quality Performance Improvement Plan (QPIP). The Finance Committee had reviewed the continuity of services asset register

Page 18 of 25
19.12 19.13
and reviewed the Committee work plan for the next year. The Finance Committee had discussed the marketing process for the disposal of the Chippenham site and the options appraisal associated with this. GB thanked the Executive Director of IM&T for the work he had undertaken in supporting the Finance Committee over the past number of years. The Trust Board of Directors took assurance from the Trust Financial Position update and the Finance Committee Assurance update.
20.0 Charitable Funds Committee Assurance Report 20.1 20.2 20.3
IR presented the Charitable Funds Committee Assurance Report. IR highlighted that the Trust is accumulating charitable funds. The Committee would be developing an expenditure plan for the use of the funds. The Committee would give consideration to ensure that any initiative being explored would not conflict with the use of any other charities accessed by the Trust. The Trust Board of Directors took assurance from the Charitable Funds Committee Assurance Report.
21.0 NHS Improvement Activity Report 21.1 21.2 21.3
The Deputy Chief Executive/Executive Director of Finance presented the NHS Improvement Activity Report for information and assurance. The Deputy Chief Executive/Executive Director of Finance highlighted that at the Performance Review Meeting with NHS Improvement on 19 February 2018 NHS Improvement had agreed to the closure of the final action which had addressed specific issues raised over the NHS 111 Service two years previously. The Trust had provided an Executive Position Statement setting out the progress against the remaining action linked to the Trust’s Well Led Review. The Chief Executive provided an update for assurance following the Dorset Coroners Report and the action to stagger shifts. Negotiations had been held with Trust staff and it had been identified that the more staggered the shifts the more imposition would be put on staff.

Page 19 of 25
21.4 The Trust Board of Directors took assurance from the NHS Improvement Activity Report.
22.0 Revised Trust Corporate Statements 22.1 22.2 22.3
22.4
22.5
The Deputy Chief Executive/Executive Director of Finance presented the Revised Trust Corporate Statements and requested that the Trust Board of Directors to consider and approve the Mission Statement and the Vision, The Values and Strategic Goals of the Trust. The Deputy Chief Executive/Executive Director of Finance advised that the Trust had previously agreed to keep the current Mission Statement. However, on reflection of the presentation on the MacMillan Cancer Project at the Trust Board Seminar in February 2018 there had been a view that it would be appropriate to consider the Trust’s role in providing end of life care. The Trust Board of Directors reviewed three Mission Statements provided one of these was the current Trust Mission Statement. The Trust Board of Directors agreed to adopt option b): To respond quickly and safely to patients’ emergency and urgent care needs, at every stage of life, to reduce anxiety, pain and suffering; The Deputy Chief Executive/Executive Director of Finance confirmed that following discussions regarding the Strategic Goals at the Trust Board Seminar in February 2018 compassionate had been added in Every Patient Matters and robust in Every Pound Matters. The Trust Board of Directors approved the Vision Statement: Exceptional patient care delivered by exceptional people.
23.0 Joint Board Assurance and Risk Report 23.1 23.2 23.3
The Head of Quality presented the Joint Board Assurance and Risk Report for information and assurance. The Head of Quality Reported that one risk had increased. The Incident Stacking (A&E) risk had escalated to 25. The Trust Board of Directors noted that this had been discussed by the Quality Risk Assurance Group, Audit and Assurance Committee and at the Senior Leaders Team Meeting. The Head of Quality advised that an additional risk had been added to the Risk

Page 20 of 25
23.4 23.5 23.6 23.7 23.8 23.9
Register. The Sending of EPCR Referral Forms to Incorrect Services. It had been identified that the EPCR was not always sent to the correct GP Surgery. The Clinical Records team identify when the errors take place and forward the EPCRs to the correct surgery. The Trust is moving towards an automated system to improve this. The Head of Quality reported that actions and controls in the Board Assurance Framework (BAF) and the Risk Register had been completely refined following meetings with Directorate leads. The Trust had procured the new Risk Platform. This is called Pentana and the Risk Team is working with the new company to implement the system. The new platform would link risks to the new Strategic Goals. The new platform would be presented to the Trust Board of Directors at the Board Seminar in April 2018. The Head of Quality confirmed that the Trust Board of Directors Meeting in May 2018 would receive a new report based on the new risk system. GB had noted the Incident Stacking (A&E) risk had escalated to 25 and asked what consequence would make this risk a 5 by 5. The Head of Quality advised that safety, media, reputation, and the potential for a serious patient safety incident are considered. The levels of incidents stacking had significantly increased. The Executive Director of IM&T advised that the difference is that where previously the Trust would have had a resource available for the patient for Category 1 incidents, resourcing is now challenged and could cause delay. The Trust Secretary advised with regard to the patient quality pillar that drives this risk and the likelihood. Incidents happen daily and the consequence to the patient experience becomes 5 by 5. IR asked what the Trust would be doing now that the risk had risen to 25. The Chief Executive advised that controls and assurances would require further narrative and the work was being undertaken. The Head of Quality provided assurance that further information would be added to the controls. The Deputy Chief Executive/Executive Director of Finance stated that the Incident Stacking (A&E) risk was volatile, particularly around adverse weather, bank holidays and peak periods. The Trust had been living with the risk and it had steadily increased over a decade. This is the highest area of concern in managing patient safety and this had distinguished it from other risks.

Page 21 of 25
23.10 23.11
The Trust Secretary read out comments received from PL in his absence. With regard to risk scoring PL noted that the Audit and Assurance Committee had requested a presentation on the new reporting framework to the Trust Board Seminar in April 2018. The longevity of items on the risk register should be considered in the Trust’s forward approach as this had been a criticism from CQC. The Trust Board of Directors took assurance from the Joint Board Assurance and Risk Report and noted the increase in score to 25 of the Incident Stacking (A&E) risk.
24.0 Use of the Trust Seal 24.1 24.2 24.3 24.4
The Trust Secretary presented use of the Trust Seal. The Trust Board of Directors was asked to take assurance from the report. In answer to the question as to why the seals were not sequential the Trust Secretary advised that the documents had been entered into the book as they needed to be sealed but this changed and they did not require the seal so it was not used and therefore not reported. IR asked why the Deed of Variation on the Acorn Building, St Leonard’s was included. The Deputy Chief Executive/Executive Director of Finance advised that this related to the flexibility of the notice period of the Dorset Urgent Care Contract. The Trust Board of Directors took assurance from the Use of the Trust Seal 2017-18 Report.
25.0 Audit & Assurance Committee Assurance Report 25.1 25.2 25.3
GB presented the Audit and Assurance Committee Assurance Report. The Trust Board of Directors noted that the Audit and Assurance Committee had been presented with the Internal Audit Progress Report. The delivery of the report had been further advanced than the previous year. The Committee had considered the projected number of days against the plan. Some days exceeded the existing plan for some reviews. Assurance had been obtained from the supplier that the cost of additional days that might be necessary would be absorbed within the existing budget.

Page 22 of 25
25.4 25.5 25.6 25.7
GB reported that there had been good progress on Internal Audit Recommendations. There had been 28 actions completed against 39. The Audit and Assurance Committee had received the draft Head of Internal Audit Opinion. Internal Audit had confirmed its intention to provide the Trust with significant assurance against its system for internal control. Internal Audit had reported that based on the findings of the audits undertaken to date, it did not envisage the position changing between the date of the Committee and the Internal Audit Opinion being presented to the Committee in May 2018. The Audit and Assurance Committee had discussed the challenges it faced in progressing criminal investigations due to the quality of records versus the ability to evidence fraud. It had been agreed that future reports would need to be strengthened to clearly specify the reason for which it had not been possible to progress an investigation. The Trust Board of Directors took assurance from the Audit and Assurance Committee Assurance Report.
26.0 Board of Directors Draft Work Plan 2018-19 26.1 26.2 26.3 26.4
The Trust Secretary presented the Board of Directors Draft Work Plan for 2018-19 for approved. The Trust Secretary advised of an amendment to the Work Plan for an additional Trust Board of Directors Meeting that had been added to the cycle. The Trust Board of Directors noted that there had been a review of business and a review of the items taken to both the Confidential and Public sections of the Trust Board of Directors Meetings. The Trust Board of Directors approved the Board of Directors Draft Work Plan for 2018-19.
27.0 Well Led Governance Review Action Plan 27.1
The Trust Secretary presented the KPMG Well Led Governance Review for approval. There had been 11 actions formulated into an Action Plan following the review. These actions would be monitored by the Trust Board of Directors. The Trust Secretary reported that of the 11 actions 4 were fully complete for

Page 23 of 25
27.2
closure to be agreed by the Trust Board of Directors today. The Trust Board of Directors noted the progress of the delivery of the Well Led Action Plan and agreed that the 4 completed actions could be formally closed.
28.0 Third Party Body Schedule 28.1 28.2 28.3
The Trust Secretary presented the Third Party Body Schedule for assurance. The Trust Secretary advised that it is a Code of Governance requirement that the Trust Board of Directors reviewed the relationship that it had with third party bodies used to drive independent declarations of interest. The Trust Secretary presented the updated compliance with Monitor’s Code of Governance requirement of NHS Foundation Trust Boards. The Trust Board of Directors reviewed and noted the Third Party Body Schedule which provided an overview of the arrangements in place and took assurance from this.
29.0 Annual Declaration
29.1 29.2 29.3
The Trust Secretary thanked the member of the Trust Board of Directors for completing the annual declarations of independence, the Fit and Proper Person declarations and for providing permission for their salary to be disclosed in the Annual Report. The Trust Secretary confirmed that no conflicts of concern had been reported. The Trust Board of Directors took assurance from the Annual Declaration.
30.0 Digital Strategy
30.1 30.2
The Executive Director of IM&T presented the Summary Digital Strategy 2017-2021. The Digital Strategy had been mapped to the Trust Strategic Goals and Visions. The Strategy identified the Trust’s position within the NHS England Maturity Index. The Executive Director of IM&T reported that the Annual Return for the Information Governance Toolkit had been submitted and the Trust had

Page 24 of 25
30.3
achieved 81%. The Trust Board of Directors approved the five year Digital Strategy.
31.0 Environmental Strategy and Sustainability Commitment 31.1 31.2 31.3
The Chief Executive presented the Trust’s Environmental Strategy and Sustainability Commitment for approval. The Trust Board of Directors approved the Environmental Strategy and Sustainability Commitment. ACTION: TF to consider and identify which Committee should monitor the Trust’s Environmental Strategy and Commitment.
TF
32.0 Questions Arising from the Meeting Any Other Business Identification of New Risks (incl. Health & Safety) and New Legislation
32.1 32.2 32.3 32.4
Questions Arising from the Meeting No questions had been raised from the meeting. Any Other Business No further business was discussed. Identification of New Risks (incl. Health & Safety) No new risks had been identified. Identification of New Legislation No new Legislation had been identified.
33.0 Exclusion of the Press and Public To consider whether pursuant to the provisions of section 1(2) of the Public
Bodies (Admission to Meetings) Act 1960, the press and public be excluded from the remainder of the meeting on the grounds that publicity would be prejudicial to the public interest by reason of the confidential nature of the business about to be transacted.
Signed:

Page 25 of 25
(Chair) Dated: Copies of the approved final minutes are available from the meeting administrator on request.
Date of Meeting Minutes Reference
Agenda Item (Topic) Action Allocated To Deadline Progress Date Completed
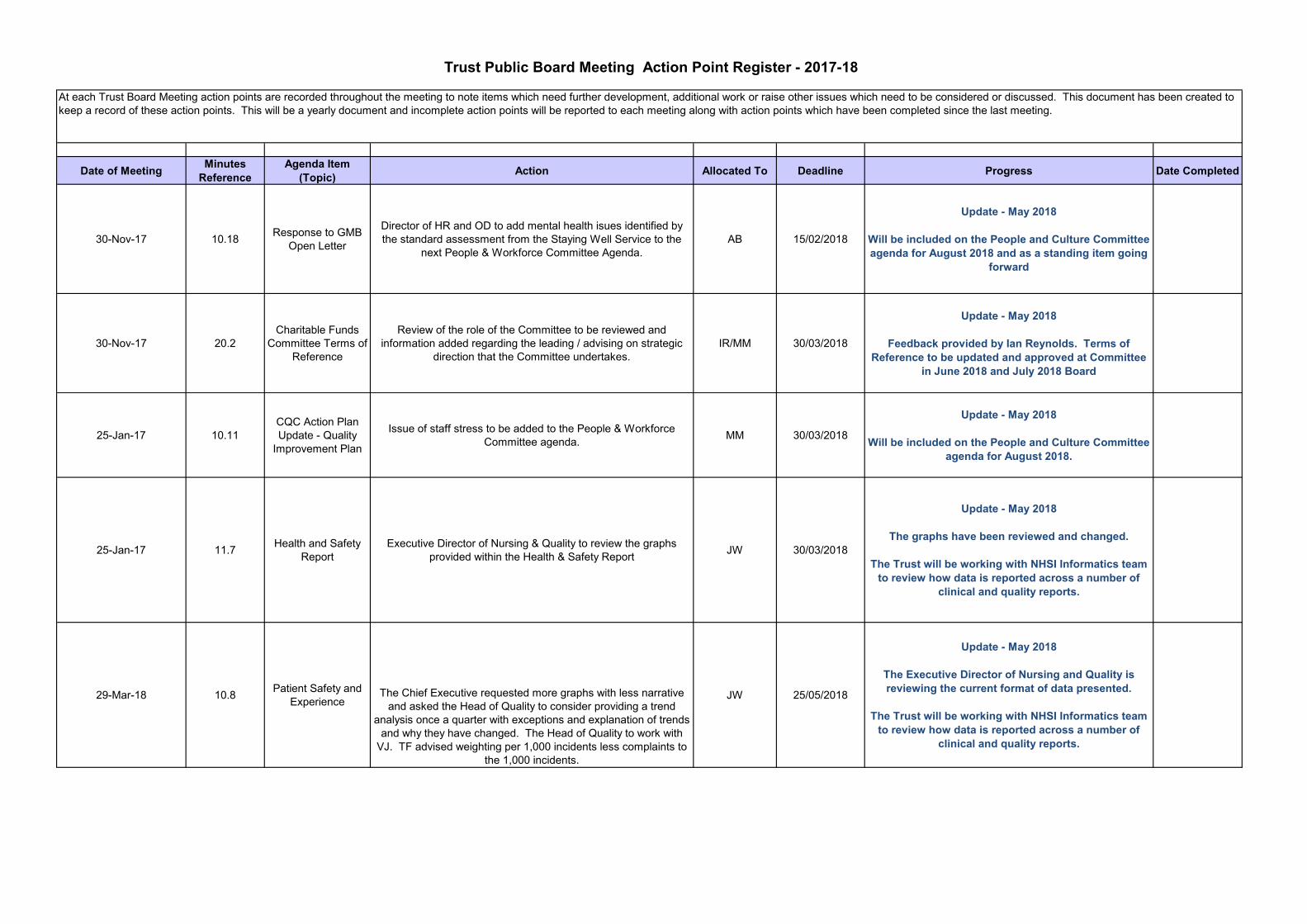
30-Nov-17 10.18 Response to GMB Open Letter
Director of HR and OD to add mental health isues identified by the standard assessment from the Staying Well Service to the
next People & Workforce Committee Agenda.AB 15/02/2018
Update - May 2018
Will be included on the People and Culture Committee agenda for August 2018 and as a standing item going
forward
30-Nov-17 20.2Charitable Funds
Committee Terms of Reference
Review of the role of the Committee to be reviewed and information added regarding the leading / advising on strategic
direction that the Committee undertakes.IR/MM 30/03/2018
Update - May 2018
Feedback provided by Ian Reynolds. Terms of Reference to be updated and approved at Committee
in June 2018 and July 2018 Board
25-Jan-17 10.11CQC Action Plan Update - Quality
Improvement Plan
Issue of staff stress to be added to the People & Workforce Committee agenda. MM 30/03/2018
Update - May 2018
Will be included on the People and Culture Committee agenda for August 2018.
25-Jan-17 11.7 Health and Safety Report
Executive Director of Nursing & Quality to review the graphs provided within the Health & Safety Report JW 30/03/2018
Update - May 2018
The graphs have been reviewed and changed.
The Trust will be working with NHSI Informatics team to review how data is reported across a number of
clinical and quality reports.
29-Mar-18 10.8 Patient Safety and Experience
The Chief Executive requested more graphs with less narrative and asked the Head of Quality to consider providing a trend
analysis once a quarter with exceptions and explanation of trends and why they have changed. The Head of Quality to work with
VJ. TF advised weighting per 1,000 incidents less complaints to the 1,000 incidents.
JW 25/05/2018
Update - May 2018
The Executive Director of Nursing and Quality is reviewing the current format of data presented.
The Trust will be working with NHSI Informatics team to review how data is reported across a number of
clinical and quality reports.
Trust Public Board Meeting Action Point Register - 2017-18
At each Trust Board Meeting action points are recorded throughout the meeting to note items which need further development, additional work or raise other issues which need to be considered or discussed. This document has been created to keep a record of these action points. This will be a yearly document and incomplete action points will be reported to each meeting along with action points which have been completed since the last meeting.

29-Mar-18 15.7 Health and Safety
The Head of Quality advised that data is being reviewed and an update on the graphs within the report would be presented to the next meeting. The Head of Quality advised that data could not be
provided by call but could be done via the Datix System. Violence and Aggression would be in the Health and Safety Plans
for the next year.
JW 25/05/2018
Update - May 2018
The graphs have been reviewed and changed. The HR and Training department have reviewed the ability to upload the mandatory training data to ESR but this
has been put on hold.
25-Jan-17 11.9 Health and Safety Report
Executive Director of Nursing & Quality to bring the Health & Safety Committee Plan for 2018 to the March Board meeting. JW 30/03/2018
Update - May 2018
Work has begun to look at the correlation of the time a call is received to the time the crew arrive on scene to
treat the patient. As only one months worth of data has been collected to date there is nothing to report at this stage. To allow further data, this has been added
to the agenda for the September Board Meeting.
25-Jan-17 11.12 Health and Safety Report
Executive Director of Nursing & Quality to discuss further how to evidence the benefit of training with the Health & Safety
Committee.JW 30/03/2018
Update - May 2018
A discussion was had at the People and Culture Committee which took place on 10 May 2018. It was agreed that the Mandatory Training workbooks were insufficient and the online training was to be kept for 2018/19. A new training platform is being looked at for
2019/20.

29-Mar-18 12.5 Freedom to Speak Up
The Chief Executive asked the Unison Representative in attendance at the meeting to promote Freedom to Speak Up and
the new structure with the Peer Support Guardians through Unison.
JF 25/05/2018
The Trust is planning on doubling the numbers of Peer Support Guardiand and Unison collegaue to help
support this
ACTION COMPLETE
30-Nov-17 10.21 Response to GMB Open Letter
Deep Dive on Bullying and Harassment by the People & Workforce Committee to be undertaken, to include
benchmarking. Director of HR and OD to prepare a paper. Trust Secretary to add to the Agenda.
AB/MM 15/02/2018
Update - May 2018
Included on 18 April 2018 agenda.
ACTION COMPLETE
30-Nov-17 10.22 Response to GMB Open Letter
Director of HR and OD to meet with Unison to plan an engagement meeting with both Unison and Staff. They will agree
principles and data before sharing with the staff.AB 15/02/2018
Update - May 2018
The Health and Wellbeing Group has been established. The Terms of Reference were approved at
the People and Culture Committee which took place on 10 May 2018.
ACTION COMPLETE
30-Nov-17 10.23 Response to GMB Open Letter
Director of HR and OD to provide a greater breakdown of claims of bulying and harassment with BME and gender for the next
People and Workforce Committee.AB 15/02/2018
Update - May 2018
Included on 18 April 2018 agenda.
ACTION COMPLETE
30-Nov-17 16.2People & Workforce Committee Terms of
Reference
Updated Terms of Reference for the People & Workforce Committee to be presented to the next meeting of that Committee
in February 2018.RR 15/02/2018
Update - May 2018
Included on 18 April 2018 People & Culture agenda and Board agenda for 25 May 2018.
ACTION COMPLETE
29-Mar-18 9.9 Communications Update
TF thanked the Head of Communications for the work undertaken with the media.TF asked the Head of Communications how the Trust compared to other services in the South West. ACTION:
The Head of Communications is currently undertaking a piece of work involving other Ambulance Trusts for a comparison and
would report on this at the next Trust Board Meeting in May 2018.
CW 25/05/2018
Update - May 2018
This work has been completed and has been included in the May Board of Directors Report.
ACTION COMPLETE
29-Mar-18 10.6 Patient Safety and Experience
The Head of Quality to amend the report under section 5, Claims to all A&E Service Line. JW 25/05/2018
Update - May 2018
The Patient Safety and Experience Report has been amended.
ACTION COMPLETE
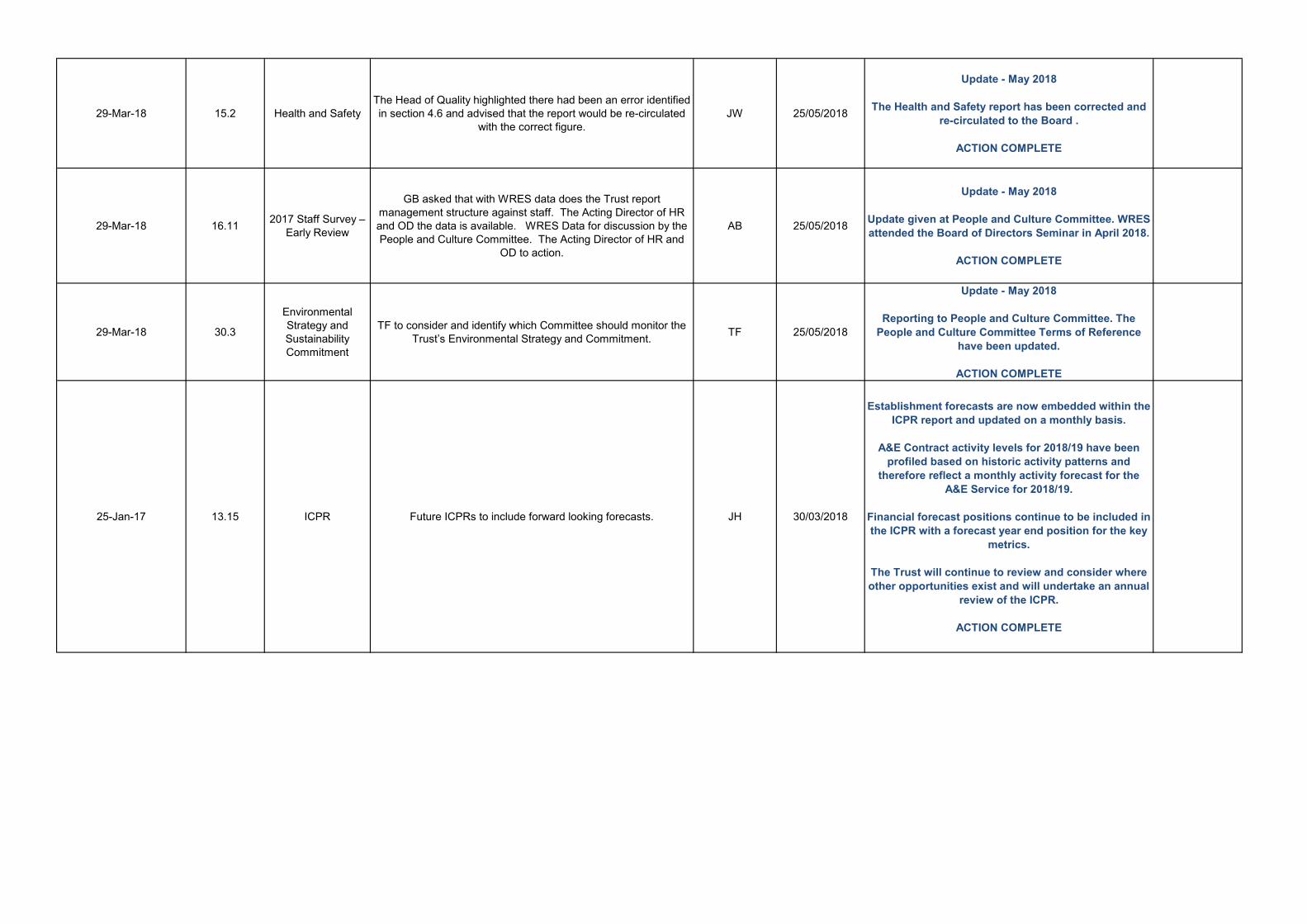
29-Mar-18 15.2 Health and Safety The Head of Quality highlighted there had been an error identified in section 4.6 and advised that the report would be re-circulated
with the correct figure. JW 25/05/2018
Update - May 2018
The Health and Safety report has been corrected and re-circulated to the Board .
ACTION COMPLETE
29-Mar-18 16.11 2017 Staff Survey – Early Review
GB asked that with WRES data does the Trust report management structure against staff. The Acting Director of HR and OD the data is available. WRES Data for discussion by the People and Culture Committee. The Acting Director of HR and
OD to action.
AB 25/05/2018
Update - May 2018
Update given at People and Culture Committee. WRES attended the Board of Directors Seminar in April 2018.
ACTION COMPLETE
29-Mar-18 30.3
Environmental Strategy and Sustainability Commitment
TF to consider and identify which Committee should monitor the Trust’s Environmental Strategy and Commitment. TF 25/05/2018
Update - May 2018
Reporting to People and Culture Committee. The People and Culture Committee Terms of Reference
have been updated.
ACTION COMPLETE
25-Jan-17 13.15 ICPR Future ICPRs to include forward looking forecasts. JH 30/03/2018
Establishment forecasts are now embedded within the ICPR report and updated on a monthly basis.
A&E Contract activity levels for 2018/19 have been profiled based on historic activity patterns and
therefore reflect a monthly activity forecast for the A&E Service for 2018/19.
Financial forecast positions continue to be included in the ICPR with a forecast year end position for the key
metrics.
The Trust will continue to review and consider where other opportunities exist and will undertake an annual
review of the ICPR.
ACTION COMPLETE
Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 5
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Communications Update
Prepared by: Claire Warner, Head of Communications
Presented by: Claire Warner, Head of Communications
Action: Information
Recommendation:
The Trust Board of Directors is asked to note the contents of this report for information.
Executive Summary:
This report looks at media and communications activity since the last Board meeting. Highlights include:
Media activity generated coverage with a total news value of £3.5 million.
Media activity generated coverage has lowest rate of negative scoring (16 articles, 1.5%) for 2018.
Significant coverage generated from a number of media events to reunite patients with ambulance crews and call handlers.
Media activity dominated by severe weather and poisoning incident in Salisbury.
Social media activity has increased 40% year on year.
Trust Public Board of Directors Meeting – 25 May 2018 Page 2 of 5
Communications Update
1. Media monitoring and activity
1.1 Media activity during the period March to April 2018 can be broken down as follows:
Media activity relating to the work of South Western Ambulance Service NHS Foundation Trust (SWASFT) remained at a consistent level when compared to the previous two months, with just over 1,000 articles generated each month.
This media activity generated articles and broadcasts achieving a reach of 49.6 million. This is a drop in reach from 75.9 million people in the last reporting period, although this is likely to be attributed to an unprecedented spike in relation to the winter communications activity.
However, the total news value attributed to media activity in March and April rose to £3.5 million, compared to £2.78 million in the previous period.
Of the articles generated in March and April, just 16 (1.5%) were deemed to be negative by the Kantar media monitoring service employed. This is the lowest rate so far for 2018.
9% of the articles generated were deemed to be positive (a drop from the spike of 37.9% in the last reporting period) with the majority of articles (89.5%) classified as neutral / balanced. This is still an improvement on the 4% average reported in 2017.
1.2 Proactive media coverage included:
Heroic Henry Saves the Day! Excellent coverage in the Mirror and regional broadcast
media of six year old Henry who dialed 999 when his mum was unconscious. Henry and his mum Bethany met up with the crew and call handler for a reunion.
Eight other media events to reunite patients with the call handlers and crews have been held during this period with opportunities taken to raise awareness of health conditions and provide health advice. Excellent regional broadcast and print media coverage of all events, including:
o A gentleman in Bournemouth who had a cardiac arrest whilst driving o A lady who had a heart attack in a pub o A lady and her safely delivered baby boy in Cornwall o A lady who had a severe asthma attack at home in Devon and nearly died o An eight year old girl who wanted to meet the crew and see inside an
ambulance, where she was delivered The Student Paramedic Conference received good coverage in both regional
broadcast and print media. Regional BBC coverage of the Thorncombe Community First Responders’ 20th
anniversary. Joint working with partners, particularly across social media, ensured consistent and
timely messages to try and manage demand ahead of both Easter and the Bank Holiday.
BBC1 Close Calls series continues and new series of Channel 4’s 999 What’s Your Emergency begins. Exploring a new series with Mentorn Media looking at holiday emergencies.

Trust Public Board of Directors Meeting – 25 May 2018 Page 3 of 5
Somerset Live reporter spent a shift with a paramedic on a RRV in Shepton Mallet and gave a positive report of his day.
Several staff have been shortlisted for HSJ and regional healthcare awards. Announcements to follow.
1.3 Reactive media included:
Media activity throughout March and April was dominated by the Salisbury poisoning
incident. Significant levels of activity were managed via the multi-agency media cell. Excellent joint working across all agencies and the NHS in the South West resulted in
a consistent response to the severe weather experienced in early March. BBC Radio 5 Live featured a SWASFT paramedic working a shift in the heavy snowfall. ITV Westcountry interview with the Winter Planning Lead. The Chief Executive issued a message of thanks to staff and the local community for their considerable efforts.
Significant work involved in responding to a number of GMB press releases. Opportunities to generate positive coverage taken to follow up on GMB figures in relation to abuse of ambulance staff, including several interviews with a Consultant Paramedic. Work to correct several stories about possible strike action and hoax calls.
Following national media coverage of a note left on an ambulance by an angry member of the public, we achieved positive coverage of a note left on a Bristol ambulance thanking the crew for all their hard work.
Response provided to a small number of stories regarding delays in responding to patients during the severe weather, including a 93 year old lady who had fallen and a man who’s motorbike had fallen on him and Devon Live contacted him after he posted on Facebook.
Joint statement with NEW Devon CCG in relation to the extension of the Tiverton Urgent Care Centre contract.
Local media coverage following the inquest into the death of a teenager who had taken Ecstasy.
2. Stakeholders
2.1 SWASFT attended the following Health and Scrutiny Committees (HOSC): Bournemouth on 22 March Somerset on 11 April 2018 West Somerset on 12 April 2018 Wiltshire on 24 April 2018
2.2 Gloucestershire HOSC committee members had a very successful visit to the north clinical hub on 20 March 2018.
2.3 The Trust participated in #CoastSafe on 5 April 2018. This was a joint event for partners
including Devon & Cornwall Police, Cornwall Fire & Rescue Service, HM Coastguard, RNLI and Cornwall Air Ambulance to launch a programme of work to reduce harm and fatalities on our coastlines.
Trust Public Board of Directors Meeting – 25 May 2018 Page 4 of 5
2.4 The Trust attended a Health Weston event to contribute to the future planning of health and social care in Weston-super-Mare on 19 April 2018.
3. Social media
3.1 Social media activity has increased by around 40% year on year over the past few years and is one of the most effective communication tools for sharing timely messages with the public, media and SWASFT staff. During this time the presentation of these messages has been developed to include more graphics/ memes to convey corporate messages and encourage behaviour change in relation to staying well and demand management.
3.2 As at April 2018, SWASFT had almost 24,000 social media followers, split equally between
Twitter and Facebook. The Trust sits just below the midpoint of the social media league table across all ambulance trusts, with SECAMB totaling 18,814 social media followers and LAS totaling 151,500 social media followers. Work is underway with ambulance service communications colleagues to learn from others and improve our reach.
3.3 Whilst the number of followers continues to rise, the significant increase in ‘reach’ and
number of engagements (the number of times people engage with our posts through likes and comments etc.) during January and February has returned to just above previous levels during this period. This is likely to be due to the significant impact of winter / demand management messaging during the previous reporting period.
3.4 The most popular tweet in this period was sent on 2 March 20018 and was seen 64,713
times: “Please spread the word – due to the ongoing adverse weather conditions we are currently experiencing severe difficulty in raching some of our patients across the South West. #WeatherSW”
3.5 The most popular Facebook posts during this period were:
1 March 2018 – warning people not to travel as the South West faces a RED weather warning for snow (295,000 people reached).
13 April 2018 – “Always nice to get a #Thanks note left on @swasft ambulance…dear #paramedics #team999 you are amazing… (22,996 people reached).
4. Internal communications
4.1 The new interactive e-bulletin continues to be well-read amongst staff, with an average of
10,200 views each week in March and April.
4.2 The number of staff ‘liking’ and commenting on articles continues to improve.
4.3 As always, the internal communications with SWASFT staff covered a wide range of topics, including: activity following the poisoning incident in Salisbury; the Initial Operational Response ‘Remove, Remove, Remove’; input into the new vision for SWASFT; NHS staff survey results; forthcoming CQC inspection; updates on the trial to reduce shift overruns; mandatory training reminders; NHS70 activities; response to the GMB press releases; the Student Paramedic and Young People conference and the national ambulance LGBT network conference.

Trust Public Board of Directors Meeting – 25 May 2018 Page 5 of 5
5. Trust website
5.1 The team received 142 requests for updates to the Trust website during April. The website has been updated to include: A new clinical guidelines section A new infections, prevention and control section A new Dorset Integrated Urgent Care section A new Governor events section Work continues on the new SWASFT charity pages
5.2 Consistently over this reporting period, the most popular website pages include:
The news section (around 40,000 hits per month) Frequently asked questions (5,600 hits per month) Defibrillator accreditation scheme (around 4,000 hits per month)
5.3 The team has provided training on the website to:
The urgent care team The procurement team
5.4 Work continues on the new SWASFT website, which is expected to ‘go live’ at the end of June 2018.
6. Recommendations
6.1 The Trust Board of Directors is asked to note the contents of this report for information.
Claire Warner Head of Communications

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 6
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Annual Patient Safety and Experience Report
Prepared by: Vanessa Williams, Head of Quality
Presented by: Jenny Winslade, Executive Director of Nursing and Quality
Action: Assurance
Recommendation:
The Trust Board of Directors is asked to take assurance from this Annual Patient Safety and Experience Report which summarises the individual Patient Safety and Compliments, PALS, Comments, Concerns and Complaints Annual Reports presented to the Quality Committee in May 2018.
Executive Summary:
The Trust is committed to the delivery of high quality services designed around the needs of patients, staff, carers, local communities and the public. We continually seek to improve what we do, but must also consider action where services fall short of what patients and service users expect and deserve. This involves investigating and learning from patient safety incidents and patient feedback which includes serious, moderate and adverse incidents, compliments, PALS, comments, concerns and complaints. This paper provides a summary of feedback and learning which took place during the year 2017/18 and contains a summary of key information which was presented in full, with supporting appendices, to the Quality Committee in May 2018. The principle themes arising from the reports relate to:
Delayed responses; Non-conveyance Directory of Services usage; Clinician call backs; Welfare calls.

Trust Public Board of Directors – Friday 25 May 2018 Page 2 of 6
Patient Safety and Experience Report 1. A&E Service Line 1.1 Serious Incidents
51 serious incidents were confirmed for the A&E service line during the year compared with 57 in 2016/17, a decrease of 6. 21 of the confirmed Serious Incidents during 2017/18 related to delays, including those reported due to demand and resourcing, processes within the Hub and address issues. This compares with 36 incidents during the preceding year. 16 incidents related to non-conveyance of patients and 5 related to clinical care.
1.2 Moderate Incidents
Thirteen moderate harm incidents were confirmed for the A&E service line during the year compared with 14 during the same period last year. Ten of those reported this year related to delays, 2 related to accidents when moving patients and one related to a road traffic collision.
1.3 Adverse Incidents (including Healthcare Professional Feedback)
During the year the Trust received 6,951 adverse incidents and Health Care Professional Feedbacks (HCPFs) relating to the A&E service line. This compares with 7,986 adverse incidents and HCPFs during the same period in 2016/17, a decrease of 1,035. The Trust saw a reduction in the number of incidents relating to treatment and intervention, and handovers delays at hospital. The year did see an increase in the number of incidents reported relating to confidentiality which was due to EPCR referrals being sent to the incorrect GP Practice. This issue has been the subject of a risk assessment and an action plan is in place to minimise the likelihood of these errors occurring.
1.4 Key Issues Arising From Patient Safety Incidents The primary theme for A&E patient safety incidents during 2017/18 was demand and resourcing, this follows the main theme identified in 2016/17. Other key issues for the year were non- conveyance and clinical decision making in isolation, long waits following falls, intubation, manual handling and Emergency Department capacity. Actions relating to the following topics were identified following investigations into patient safety incidents during the year. Further detail around each of these areas was presented to the Quality Committee as part of the Annual Patient Safety report:
Paediatrics; Resource management; Call categorisation; Head Injuries; Bias; Calls from other emergency services; Carry chair maintenance; Palliative/end of life care; Hypothermia; Welfare Calls (the new SOP was issued during Quarter 3).

Trust Public Board of Directors – Friday 25 May 2018 Page 3 of 6
1.5 Compliments 2,582 compliments were received for the A&E service line during the year compared to 2,114 during 2016/17, an increase of 468 and more than double the number of complaints.
1.6 Comments, Concerns and Complaints During the year the Trust received 1,224 complaints for the A&E service line, compared to 1,404 during 2016/17. This is a reduction of 180.
1.7 Themes Arising From Comments, Concerns and Complaints
Many complaints are multifaceted, during the year the 1,224 complaints resulted in the identification of 1,500 separate areas of concern. The highest area of feedback received this year was within the category ‘Access and Waiting’ (629) which remained consistent during each quarter of 2017/18. This is not unexpected as the Trust continues to face two acute challenges; demand for services at peak times and challenges in resourcing to meet that demand. The second highest area of concern related to Communication (386).
Themes arising from complaints regarding the Clinical Hub included concerns regarding delayed ambulance attendance which predominantly related to Category 3 and Category 4 incidents; triage errors and the attitude of staff. A number of complaint investigations identified concerns with the welfare call process, a new welfare call procedure was implemented towards the end of the year and is now based on the clinical need of the patient to ensure that those patients who are most in need receive a welfare call. In terms of complaints relating to ambulance attendances, trends included the non-conveyance of patients, communication, health and safety warning markers, safeguarding referrals and driving concerns. Actions relating to the following topics were identified following complaint investigations this year. The majority of these are local Level 2 actions, further information regarding each of these actions and those relating to lower level complaints, was presented to the Quality Committee as part of the Annual Complaints report:
Review of the Trust’s welfare call process; Reinforcement of call handling procedures; Individual feedback following call audits; Written reflections on topics including PCR completion, dehydration, stroke
diagnosis, empathy, Right Care, securing patients in ambulances, pain management and breakdown in communication;
Reinforcement of seatbelt usage; Learning Development Officer shifts.
1.8 Patient Advice and Liaison Service (PALS)
The Trust received 790 PALS enquiries for the service line during the year compared to 751 for 2016/17, in increase of 49. PALS enquiries, in general, relate to lost property enquires, signposting and service users looking for closure following the death of a loved one.

Trust Public Board of Directors – Friday 25 May 2018 Page 4 of 6
2. Urgent Care Service Line 2.1 Serious Incidents
During 2017/18 no serious incidents were reported which related to the Urgent Care Service Line, this compares to 3 being reported during 2016/17.
2.2 Moderate Incidents Two moderate incidents were confirmed for the UCS service line during 2017/18, one in
relation to the 111 service and the other to the GP Out of Hours Service. This compares with one Moderate Harm incident being confirmed during 2016/17.
2.3 Adverse Incidents and Healthcare Professional Feedback The Trust received 528 adverse incidents and Health Care Professional Feedbacks
(HCPFs) during the reporting period which related to the UCS service line. This compares with 1,175 adverse incidents and HCPFs being received in 2016/17, a decrease of 647. This decrease is predominantly due to the changes in the UCS contracts managed by the Trust.
2.4 Key Issues Arising From Patient Safety Incidents Analysis of UCS service line Patient Safety data identified that there continues to be a
reduction in the number of incidents relating to internal clinical and treatment issues. The majority of internal adverse incident reports relating to the111 service concerned process issues whilst those reported by our 111 staff regarding other healthcare organisations related to clinical issues, Directory of Services issues or communication issues
Actions have been identified in relation to:
Recognition of cervical fractures; Palliative/end of life care; Support plans; Directory of Services usage.
2.5 Compliments 55 compliments were received for the UCS service line during the year compared to 69
during 2016/17, a decrease of 14. 2.6 Comments, Concerns and Complaints During 2017/18 the Trust received 102 complaints for the UCS service line compared to
208 for 2016/17. 2.7 Themes Arising From Comments, Concerns and Complaints Of the 102 complaints received there were 134 separate areas of concern. The
complaints predominantly related to concerns regarding the perception of clinical care (70) and communication issues (39).

Trust Public Board of Directors – Friday 25 May 2018 Page 5 of 6
Themes identified from complaints regarding the OOH Service related to concerns regarding GP assessments, delays in call backs and communication issues.
Themes relating to the 111 service included concerns about the triage process and care
advice provided by Trust staff, delays in clinician call backs and communication matters. Actions relating to the following topics were identified following complaint investigations
this year. The majority of these are local Level 2 actions; further information regarding each of these actions and those related to lower level complaints was presented to the Quality Committee as part of the Annual Complaints report:
Reinforcement of the ‘Bare below the elbows’ campaign; Reminding staff of the ‘Hello my name is’ campaign; Organising name badges for all of the GPs; Displaying Safeguarding posters to help improve communication between patients
and members of staff; Sharing anonymized cases to raise awareness of atypical symptoms; Dissemination of shared learning regarding Mastoiditis; Reminders regarding the use of the Directory of Services (DoS); The introduction of a ‘latest call back time’ process to better manage patient
expectations for overnight call backs; Individual feedback and completion of personal reflections regarding specific cases.
In addition, the Trust referred concerns regarding advice provided within the triage system
to NHS Pathways who subsequently released National workaround guidance for all 111 and 999 providers using NHS Pathways for ventilated patients with a tracheostomy tube.
In order to try and better manage the periods of extremely high demand and reduce call
back times, the NHS 111 service has introduced a weekly resource management meeting where staffing for both call handlers and clinicians for the coming weekend is reviewed.
2.8 Patient Advice & Liaison Service (PALS) The Trust received 24 PALS enquiries for the service line during the year compared to 19
during 2016/17. 3. Duty of Candour 3.1 During the year the Trust met its responsibilities under the statutory Duty of Candour. Of
the 51 Serious Incidents and 16 Moderate Harm incidents identified during 2017/18, contact has been made with the patient or their Next of Kin, or attempted in all the cases where this has been possible and deemed appropriate.
3.2 Contact was been deemed inappropriate or impossible for a number of reasons, including
ongoing police investigations (5), inability to trace a next of kin (3), for reasons of sensitivity (2) or where it is not necessary as the incident was a Near Miss or relates to a business continuity event rather than patient care (4).

Trust Public Board of Directors – Friday 25 May 2018 Page 6 of 6
4. Parliamentary and Health Service Ombudsman (PHSO) independent reviews
4.1 During the year the Trust was asked to submit five complaint files for independent review. 4.2 The Trust received five outcome reports, none of which were upheld by the PHSO. 5. Claims 5.1 The Trust received 20 clinical negligence claims during 2017/18 compared to 18 for
2016/17. Of these, 18 related to the A&E service line. 5.2 The Trust also received 29 potential clinical negligence claims during the year which
required investigation, compared to 41 received in 2016/17. 5.3 Eight personal injury claims were received during 2017/18 compared to 21 received last
year. 5.4 The Claims and Inquests team also deal with small miscellaneous claims, for example
damage to patients property, which require investigation and feedback. During year the Trust received 27 small claims, compared to 13 in 2016/17.
6. Inquests 6.1 Two Regulation 28 reports were received during the year which related to the Trust, details
of these have been provided separately to the Trust Board of Directors. 6.2 The Trust received notification of 134 new inquests during the year where the Trust was
directly involved and investigation was required; this is a decrease on the 144 received last year.
6.3 142 Inquests were closed during the year, compared to 71 last year. 7. Recommendation 7.1 The Board of Directors is asked to take assurance from the Patient Safety and Experience
Report. Vanessa Williams Head of Quality

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 2
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Quality Improvement Plan
Prepared by: Emma Murgatroyd, Quality Support Manager
Presented by: Jennifer Winslade, Executive Director of Nursing and Quality
Action: Assurance
Recommendation: The Trust Board of Directors is asked to take assurance from the content of this paper.
Executive Summary:
The Trust developed a Quality Improvement Plan (QIP) in August 2016 in order to drive forward the Trust’s continuous quality development agenda. To re-energise quality improvement throughout all areas of the Trust, it was agreed that the QIP would be refreshed annually – QIP 2018 was therefore developed and is currently supporting continuous quality improvement across the Trust. Of the original 81 actions identified in QIP 2018, the closure of 51 actions has been confirmed by the Quality Programme Board or the Executive Director of Nursing and Quality. 38 of these are awaiting evidence of closure and are therefore pending full closure. 30 actions are currently open on the plan with no actions currently overdue. A review of all closed QIP 2017 actions is also being completed to provide additional assurance and actions will be reopened as appropriate where further assurance of completion is required or sustainability or embeddedness of the action is of concern. 28 actions have so far been reopened and added to QIP 2018 for review.

Trust Public Board of Directors – Friday 25 May 2018 Page 2 of 2
Quality Improvement Plan (QIP) 1. Introduction 1.1 The Trust developed a Quality Improvement Plan (QIP) in August 2016 order to drive
forward the Trust’s continuous quality improvement agenda. In order to re-energise quality improvement throughout all areas of the Trust, a revised QIP for 2018 is now in place.
1.2 QIP 2018 was developed with its main purpose being to support continuous quality
improvement across the Trust, to review the embeddedness of previous and current actions and to ensure that any new concerns are addressed. The QIP is monitored through the Quality Programme Board (QPB), chaired by the Clinical Director. Quality development and regulatory compliance is the main feature of the Programme Board.
2. QIP 2018 2.1 Of the 121 actions identified in the original QIP, 112 were signed off as being complete by
the Quality Development Group (QDG) or the UCS Service Line. The nine remaining open actions were transferred to the 2018 QIP to continue ongoing work on these areas. In addition to these nine actions, a further 28 actions were reopened following an assurance review of the embeddedness, effectiveness and completion of actions closed under the original QIP.
2.2 At the QDG meeting of 29 September 2017, it was agreed that a review schedule would
be built to test the embeddedness and effectiveness of completed QIP 2017 actions in order to ensure that improvements have been maintained. This review is in progress and will include a review of associated processes, policies and procedures which were introduced in order to complete the action. This has formed a core part of the 2018 QIP. Evidence to provide assurance that QIP actions have been completed is sought prior to closure and all evidence is subject to review.
2.3 Of the 81 original actions included within QIP 2018, 30 are open and within deadline
(shown at Appendix A). No actions are currently overdue. 2.4 51 actions have been closed (confirmed by the Quality Programme Board or the Executive
Director of Nursing and Quality). 38 of these are awaiting evidence of closure and are therefore pending full closure.
3. Recommendation 3.1 The Trust Board of Directors is asked to take assurance from the content of this paper. Emma Murgatroyd Quality Support Manager

Ref No
Prev Ref Priority Core
Service Risk or Requirement Executive LeadObjective Owner/ Management Team
Quality Improvement Actions Date of Last Update
Current Deadline Current Status Summary of Progress
Risks to completion or other issues
Assurance Required Forum to Receive Assurance (and date)
Documents provided as assurance
Review date post completion
Expected Action Completion Impact Effectiveness
Actual Action Completion
Impact
QIP1 QIP
29
1 All Ensure work intensity and fatigue is monitored and actions
put in place to mitigate risks to staff
Quality Summit Comment
• Raise the profile of monitoring of indicators of intensity and
fatigue e.g. reporting meal break management to Quality
Committee and the Board
• Increase the pace of roll out of existing actions already in
place such as: the rota review which should lead to improved
meal break compliance; and the improving position in
relation to sickness absence
Executive Director
of Operations
Executive Director of
Operations with
support from Deputy
Director of HR and
OD
1. Identify a set of indicators of intensity and fatigue (including measures showing
improvement) e.g.:
- missed meal breaks
- SWS (staying well service) referrals related to stress at work
- reduction in sickness absence
for inclusion within the ICPR (integrated corporate performance report)
2. Review after 3/6 months, providing a full assurance report and, if necessary, plan
for further action to Quality Committee
3. Overruns - Number/Volume and Length - currently reported by the ROC to
Divisional Managers. Overruns to be reported and reviewed at;
(a) Divisional Meetings
(b) the Trust RMG.
4. Review of the Meal Break policy to be completed.
In the interim this forms part of the QPIP(2) Plan.
15/05/2018 31/12/2018 In progress
15/05/2018: Intensity and Fatigue position statement, Rest Break provision and End of Shift Protection papers presented to the Executive
Directors Group on 15 May 2018. The Direcotrs Group approved the Rest Break Provision and End of Shift Protection paper. This was also
approved by the Quality Committee on 10 May 2018 subject to the approval of the Directors Group.
14/05/2018: Deputy Director of HR and OD presented the Intensity and Fatigue Quality Programme Board report and Intensity and Fatigue
position statement to the QPB meeting of 14 May 2018.
16/04/2018: Deputy Director of HR and OD advised that paper was not ready for presentation at last committee, but under review with HR and
Operations, with aim for a position statement to be presented at the May QDPB.
02/03/2018: Deputy Director of HR and OD has drafted a paper to set out the measures (although some discussion for agreement is still required).
05/02/2018: Deputy Director of HR and OD will seek to develop a set of metrics to measure intensity and fatigue along with Unison and
Operations colleagues. Through this process we will seek to agree a BAU level (as we know some level of intensity and fatigue will always be
present) and an escalation level which means it will be monitored via the QIP and discussed through the Quality Programme Board. Once there is
an outcome based on the work that will be undertaken further actions will be identified.
30/01/2018:
1. Set of indicators identified by the Executive Director of Operations;
• Overruns - Number/Volume and Length - this is currently reported by the ROC to Divisional Managers. The ICPR is a public facing document and
this would not be routinely reported there. The recommendation is therefore that this is reported and reviewed at the (a) Divisional Meetings (b)
the Trust RMG. In the interim this forms part of the QPIP(2) Plan.
• Meal Break Compliance - the policy is due to be reviewed in Q4 of 2018/19. This is also part of QPIP(2).
• Sickness Absence - focussing on the reported causes of absence
• Referrals to the SWS - focussing on referrals relating to stress at work
2. Deep Dive drafted and due to be presented to the Quality Programme Board.
None Quality Development
Group
Board of Directors
Quality Committee
QIP
2.1
N/A 1
A&
E Ensure that quality is embedded operationally in all areas of
the Trust at a local level, including the alignment of local risk
registers with Directorate and the Corporate and Directors
Risk Registers
Executive Director
of Nursing and
Quality
Executive Director of
Nursing and Quality
Review the effectiveness of the Quality Buddy system six months after
implementation
09/05/2018 31/07/2018 In progress
09/05/2018: The Quality Buddy system has been reviewed and it will continue to be embedded in Operations - this will integrate with Learning
From Experience to create a new Continuous Learning Group.
12/04/2018: Quality Buddy R|eport in place, system to be aligned with learning from experience.
20/02/2018: Quality Buddy system implemented in January 2018 - six month review to be undertaken June/July 2018. Action not yet due.
None
TOR of new Quality
Buddy/Learning from
Experience merged group -
the Continuous Learning
Group
Quality Committee
Quality Development
Group
Continuous
Learning Group TORTBC
Confirmation of the
effectiveness of the
Quality Buddy scheme
and of the new
Continuous Learning
Group
TBC TBC
QIP
2.4
QIP
39
1
A&
E Ensure governance meetings at local levels contain a strong
focus upon quality and safety. This will include performance
reports on training, appraisals, patient outcomes, complaints
and incidents relevant to the local level. Actions from
addressing any shortcomings or changes must be recognised
and completed
Quality Summit Comment
• Seek and utilise local, national, and international expertise,
to support better ways of communicating quality and safety
standards through methods such as: the use of station peer
reviews; establishing a network of safety champions; and
considering the use of communication media i.e. posters and
screen messages
Executive Director
of Nursing and
Quality
Head of Quality Seek and utilise local, national, and international expertise, to develop a suite of tools
for communicating quality and safety standards through methods such as: the use of
station peer reviews; establishing a network of safety champions; and considering
the use of communication media i.e. posters and screen messages and OM level
dashboards on ePCR
14/05/2018 31/03/2019 In progress
14/05/2018:The Quality Directorate attend Divisional meetings and reports are shared on Quality, HR and Patient Safety metrics. Progress will
continue once the new Operational structure is in place - quality will realign to the new operations structure and further developments of
communication mechanisms will be developed. Currently screensavers and bulletins as well as face to face opportunities are utilised.
09/05/2018: A Comms approach is required for Quality. Head of Quality to lead.
09/03/2018: Long term piece of work - deadline 31/03/2019.
TBC Enhanced and effective
communication of quality
and safety standards
TBC TBC
QIP
2.7
QIP
39
1
A&
E Ensure governance meetings at local levels contain a strong
focus upon quality and safety. This will include performance
reports on training, appraisals, patient outcomes, complaints
and incidents relevant to the local level. Actions from
addressing any shortcomings or changes must be recognised
and completed
Executive Director
of Nursing and
Quality
Quality Support
Manager
Introduce a Quality Folder for each Trust premises, including air bases, bespoke to
stations, to be regularly reviewed and updated
16/05/2018 31/09/2018 New
16/05/2018: QSM and QSA to meet with Comms 17/05/2018.
10/05/2018: Chase sent to Comms for access to build Intranet pages to enable work to start.
06/04/2018: Visit to Torquay Ambulance Station took place to review what was already in place - physical folders are already in existence and
concerns were raised regarding the updating and upkeep of folders as well as physical locations on station. Feedback from Operations suggests
that an online folder accessible via the Intranet would be a more effective method. Online station folders are to be created.
23/03/2018: Request for access for Quality team to build pages sent to Comms to enable Risk and Quality pages to be built on the Intranet.
14/03/2018: Due to diary pressures, initial scoping meeting to be booked followed by follow up streamlining meetings with Operations.
09/03/2018: The Quality Support Manager is currently liaising with area administrators in Derriford to set this meeting up.
QIP
2.8
QIP
40
2
A&
E Ensure governance meetings at local levels contain a strong
focus upon quality and safety. This will include performance
reports on training, appraisals, patient outcomes, complaints
and incidents relevant to the local level. Actions from
addressing any shortcomings or changes must be recognised
and completed
Executive Director
of Nursing and
Quality
Quality Support
Manager
Produce a quality proforma to enable regular quality checks to be completed by
Operational Officers and as part of annual station audits
16/05/2018 31/09/2018 New
16/05/2018: This has been completed by the Clinical Director and circulated to all Operational Managers and EPRR with a focus initially on
Infection Control and Health and Safety.
06/04/2018: As per previous update.
09/03/2018: Will be completed as part of the above piece of work.
QIP 3 QIP
61
1 All Ensure mandatory training for all staff, including
safeguarding for vulnerable people, is updated and
maintained in accordance with the Trust’s target
The culture of and attitude towards training should be
considered to ensure that staff feel more responsible for
undertaking their mandatory training and appraisals.
Consideration should be given to making these a part of the
staff contract of employment
Executive Director
of Operations
Director of HR and
OD
Head of Clinical Hubs
Head of Education
and Training
Gain assurance that staff in the EOCs are provided with adequate protected time in
order to complete their mandatory training, increasing establishment where under
established in order to facilitate this.
14/05/2018 30/06/2018 Reopened
14/05/2018: EOC staff now recieve Development Day training. Futther clarity is required regarding what is mandatory for each role within the
Trust. The Deputy Director of HR and OD and Head of Training to produce a proforma for managers.
16/04/2018: Safeguarding figures at 91% for Level 1 and 93% for Lever 2 for the Clinical Hubs. Awaiting confirmation of other mandatory training
completion rates.
28/02/2018: Q3 figures for Safeguarding training figures in the EOCs are currently running at 52%.
26/02/2018: Completion of Mandatory Training is progressing.
25/04/2017: EOC managers have agreed to release staff at a suitable rate in order to attend the annual development day.
12/04/2017: EOC training is underway with a plan for completion. The challenge is not delivering the training but releasing the staff to attend the
training which is being monitored by Head of Clinical Hubs. EOC training establishment is currently being reviewed within the EOC. An agreement
has been made between the Head of Training and the Head of the EOCs for staff to attend mandatory on overtime from early November 2016.
L&D (learning and development) will provide this training on behalf of the EOCs prior to full integration.
Staff not being
released to
undertake their
mandatory training
6 monthly assurance report
Section from 2016/17 Quality
Account
Quality Committee Deep Dive
presented to QDG
31.05.17
SWAST0717 - SME
Training Follow Up -
Final Report
South Hub AMPDS
Transition plan
2017/18
Clinical Hub
Development Day
Content Proposal
2017-2018 RG input
CQC Quarterly
Monitoring reports:
Q4
Training Data in
Quality Account
2016/17
QIP
3.3
QIP
61
1 All Ensure mandatory training for all staff, including
safeguarding for vulnerable people, is updated and
maintained in accordance with the trust’s target
A particular focus is required on Support Services, NHS 111
and agency staff
The culture of and attitude towards training should be
considered to ensure that staff feel more responsible for
undertaking their mandatory training and appraisals.
Consideration should be given to making these a part of the
staff contract of employment
Director of Human
Resources and
Organisational
Development
Head of Clinical Hubs
Head of Education
and Training
Ensure all Heads of Department are held accountable for the completion of
mandatory training for staff in their department (including support services) and test
compliance
14/05/2018 30/06/2018 Reopened
14/05/2018: Assurance is required that all Heads of are held to account for ensuring mandatory training is completed - assurance is being collated
through 1:1 meetings and the appraisal process. The Deputy Director of HR and OD is to request a peice of work from Training which details how
managers can access training completion rates for their staff.
24/04/2018- Clinical Hub managers are invited to attend an initial delivery of development day so that they can promote the benefit to their
teams. This is planned for the 22nd May 2018. They are made responsible for attendance of their staff on DD as of this year.
11/04/2018: Ongoing monitoring by line managers has led to exceeding the training compoance target in EOC as described in row 14. Clinical
Hub Managers continue to promote and monitor mandatory training completion
01/03/2018: The Senior Clinical Hub Management Team continue to monitor completion rates.
31/01/2018: Compliance to be tested and assurance to be gathered.
QIP4 QIP 34 1 All Ensure that staff follow procedures with respect to the safe
and secure management of controlled drugs registers
Executive Director
of Nursing and
Quality
Pharmaceutical
Advisor
Reinforce the importance of full completion of CD (controlled drugs) registers and
monitor compliance with the quality of completion of CD registers through the
quarterly station audit and annual inspections.
16/05/2018 31/02/2020 Reopened16/05/2018: The Trust's Pharmaceutacal Advisor is visiting all stations over the next two years ensuring that all stations are compliance checked.
09/05/2018: JW confirmed that she will arrange to meet with the Trust's Pharmaceutacal Advisor regarding Medicines Management actions going
forward.
20/02/2018: The Trust's Pharmaceutacal Advisor will liaise with the Executive Director of Nursing and Quality to redevelop Medicines
Management related QIP actions to ensure that they are fit for purpose.
None Compliance review during
station audits
Paper to Clinical
Effectiveness Group
confirming Staverton changes
Clinical Effectiveness
Group
South Western Ambulance Service Quality Improvement Plan 2018 - 18.05.2018
Open Actions (30 actions)
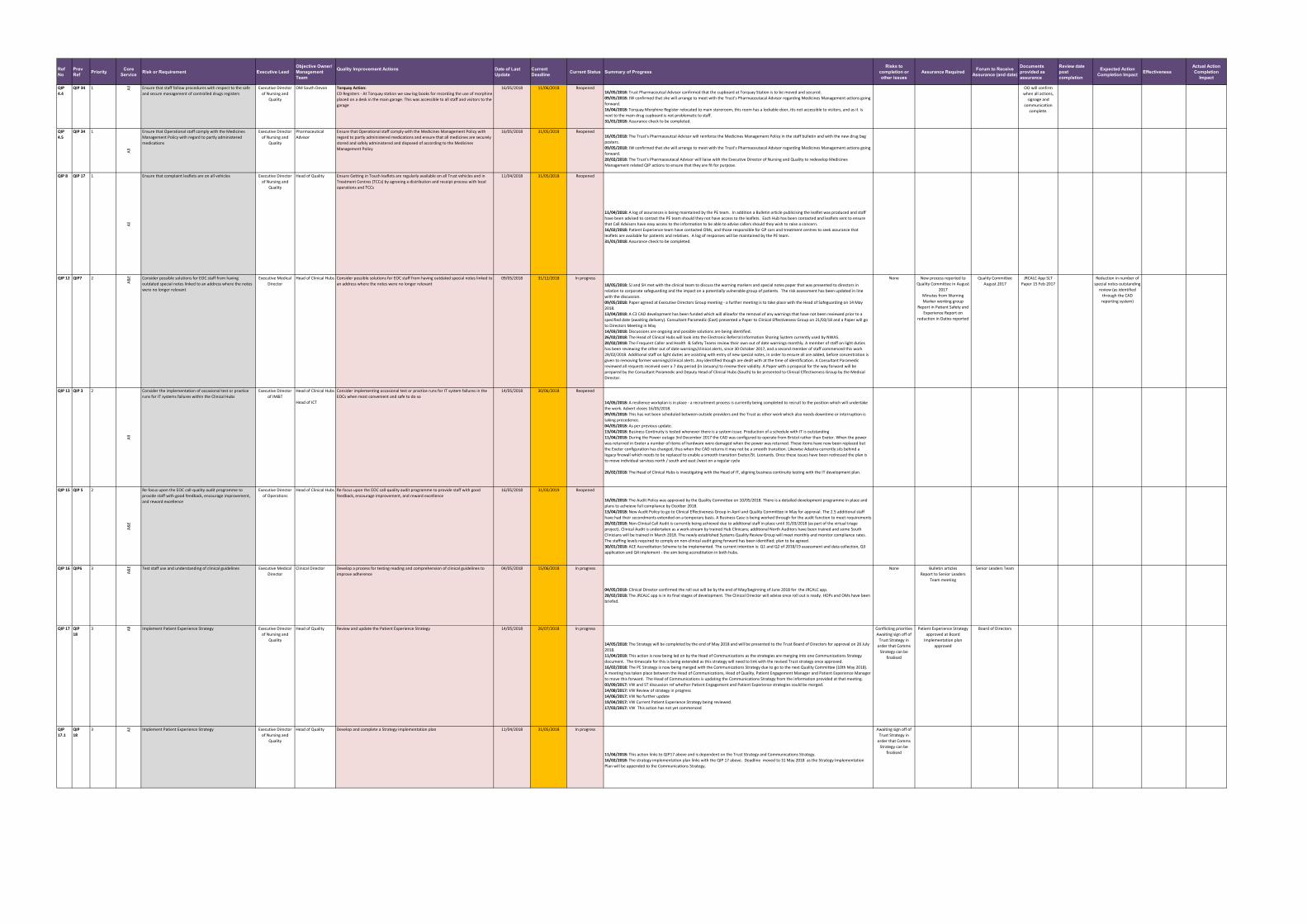
Ref No
Prev Ref Priority Core
Service Risk or Requirement Executive LeadObjective Owner/ Management Team
Quality Improvement Actions Date of Last Update
Current Deadline Current Status Summary of Progress
Risks to completion or other issues
Assurance Required Forum to Receive Assurance (and date)
Documents provided as assurance
Review date post completion
Expected Action Completion Impact Effectiveness
Actual Action Completion
Impact
QIP
4.4
QIP 34 1 All Ensure that staff follow procedures with respect to the safe
and secure management of controlled drugs registers
Executive Director
of Nursing and
Quality
OM South Devon Torquay Action:
CD Registers - At Torquay station we saw log books for recording the use of morphine
placed on a desk in the main garage. This was accessible to all staff and visitors to the
garage
16/05/2018 11/06/2018 Reopened16/05/2018: Trust Pharmaceutcal Advisor confirmed that the cupboard at Torquay Station is to be moved and secured.
09/05/2018: JW confirmed that she will arrange to meet with the Trust's Pharmaceutacal Advisor regarding Medicines Management actions going
forward.
16/04/2018: Torquay Morphine Register relocated to main storeroom, this room has a lockable door, itis not accessible to visitors, and as it is
next to the main drug cupboard is not problematic to staff.
31/01/2018: Assurance check to be completed.
OO will confirm
when all actions,
signage and
communication
complete.
QIP
4.5
QIP 34 1A
llEnsure that Operational staff comply with the Medicines
Management Policy with regard to partly administered
medications
Executive Director
of Nursing and
Quality
Pharmaceutical
Advisor
Ensure that Operational staff comply with the Medicines Management Policy with
regard to partly administered medications and ensure that all medicines are securely
stored and safely administered and disposed of according to the Medicines
Management Policy
16/05/2018 31/05/2018 Reopened16/05/2018: The Trust's Pharmaceutcal Advisor will reinforce the Medicines Management Policy in the staff bulletin and with the new drug bag
posters.
09/05/2018: JW confirmed that she will arrange to meet with the Trust's Pharmaceutacal Advisor regarding Medicines Management actions going
forward.
20/02/2018: The Trust's Pharmaceutacal Advisor will liaise with the Executive Director of Nursing and Quality to redevelop Medicines
Management related QIP actions to ensure that they are fit for purpose.
QIP 8 QIP 17 1
All
Ensure that complaint leaflets are on all vehicles Executive Director
of Nursing and
Quality
Head of Quality Ensure Getting in Touch leaflets are regularly available on all Trust vehicles and in
Treatment Centres (TCCs) by agreeing a distribution and receipt process with local
operations and TCCs
11/04/2018 31/05/2018 Reopened
11/04/2018: A log of assurances is being maintained by the PE team. In addition a Bulletin article publicising the leaflet was produced and staff
have been advised to contact the PE team should they not have access to the leaflets. Each Hub has been contacted and leaflets sent to ensure
that Call Advisors have easy access to the information to be able to advise callers should they wish to raise a concern.
16/02/2018: Patient Experience team have contacted OMs, and those responsible for GP cars and treatment centres to seek assurance that
leaflets are available for patients and relatives. A log of responses will be maintained by the PE team.
31/01/2018: Assurance check to be completed.
QIP 12 QIP7 2
A&
E Consider possible solutions for EOC staff from having
outdated special notes linked to an address where the notes
were no longer relevant
Executive Medical
Director
Head of Clinical Hubs Consider possible solutions for EOC staff from having outdated special notes linked to
an address where the notes were no longer relevant
09/05/2018 31/12/2018 In progress
18/05/2018: SJ and SH met with the clinical team to discuss the warning markers and special notes paper that was presented to directors in
relation to corporate safeguarding and the impact on a potentially vulnerable group of patients. The risk assessment has been updated in line
with the discussion.
09/05/2018: Paper agreed at Executive Directors Group meeting - a further meeting is to take place with the Head of Safeguarding on 14 May
2018.
13/04/2018: A C3 CAD development has been funded which will allowfor the removal of any warnings that have not been reviewed prior to a
specified date (awaiting delivery). Consultant Paramedic (East) presented a Paper to Clinical Effectiveness Group on 21/03/18 and a Paper will go
to Directors Meeting in May
14/03/2018: Discussions are ongoing and possible solutions are being identified.
26/02/2018: The Head of Clinical Hubs will look into the Electronic Referral Information Sharing System currently used by NWAS.
20/02/2018: The Frequent Caller and Health & Safety Teams review their own out of date warnings monthly. A member of staff on light duties
has been reviewing the other out of date warnings/clinical alerts, since 30 October 2017, and a second member of staff commenced this work
28/02/2018. Additional staff on light duties are assisting with entry of new special notes, in order to ensure all are added, before concentration is
given to removing former warnings/clinical alerts. Any identified though are dealt with at the time of identification. A Consultant Paramedic
reviewed all requests received over a 7 day period (in January) to review their validity. A Paper with a proposal for the way forward will be
prepared by the Consultant Paramedic and Deputy Head of Clinical Hubs (South) to be presented to Clinical Effectiveness Group by the Medical
Director.
None New process reported to
Quality Committee in August
2017
Minutes from Warning
Marker working group
Report in Patient Safety and
Experience Report on
reduction in Datixs reported
Quality Committee
August 2017
JRCALC App SLT
Paper 15 Feb 2017
Reduction in number of
special notes outstanding
review (as identified
through the CAD
reporting system)
QIP 13 QIP 3 2
All
Consider the implementation of occasional test or practice
runs for IT systems failures within the Clinical Hubs
Executive Director
of IM&T
Head of Clinical Hubs
Head of ICT
Consider implementing occasional test or practice runs for IT system failures in the
EOCs when most convenient and safe to do so
14/05/2018 30/06/2018 Reopened
14/05/2018: A resilience workplan is in place - a recruitment process is currently being completed to recruit to the position which will undertake
the work. Advert closes 16/05/2018.
09/05/2018: This has not been scheduled between outside providers and the Trust as other work which also needs downtime or interruption is
taking precedence.
04/05/2018: As per previous update.
13/04/2018: Business Continuity is tested whenever there is a system issue. Production of a schedule with IT is outstanding
11/04/2018: During the Power outage 3rd December 2017 the CAD was configured to operate from Bristol rather than Exeter. When the power
was returned in Exeter a number of items of hardware were damaged when the power was returned. These items have now been replaced but
the Exeter configuration has changed, thus when the CAD returns it may not be a smooth transition. Likewise Adastra currently sits behind a
legacy firewall which needs to be replaced to enable a smooth transition Exeter/St. Leonards. Once these issues have been redressed the plan is
to move individual services north / south and east /west on a regular cycle
26/02/2018: The Head of Clinical Hubs is investigating with the Head of IT, aligning business continuity testing with the IT development plan.
QIP 15 QIP 5 2
A&
E
Re-focus upon the EOC call-quality audit programme to
provide staff with good feedback, encourage improvement,
and reward excellence
Executive Director
of Operations
Head of Clinical Hubs Re-focus upon the EOC call-quality audit programme to provide staff with good
feedback, encourage improvement, and reward excellence
16/05/2018 31/03/2019 Reopened
16/05/2018: The Audit Policy was approved by the Quality Committee on 10/05/2018. There is a detailed development programme in place and
plans to acheieve full compliance by Ocotber 2018.
13/04/2018: New Audit Policy to go to Clinical Effectiveness Group in April and Quality Committee in May for approval. The 2.5 additional staff
have had their secondments extended on a temporary basis. A Business Case is being worked through for the audit function to meet requirements
26/02/2018: Non-Clinical Call Audit is currently being achieved due to additional staff in place until 31/03/2018 (as part of the virtual triage
project). Clinical Audit is undertaken as a work-stream by trained Hub Clinicans; additional North Auditors have been trained and some South
Clinicians will be trained in March 2018. The newly established Systems Quality Review Group will meet monthly and monitor compliance rates.
The staffing levels required to comply on non-clinical audit going forward has been identified; plan to be agreed.
30/01/2018: ACE Accreditation Scheme to be implemented. The current intention is: Q1 and Q2 of 2018/19 assessment and data collection, Q3
application and Q4 implement - the aim being accreditation in both hubs.
QIP 16 QIP6 3
A&
E Test staff use and understanding of clinical guidelines Executive Medical
Director
Clinical Director Develop a process for testing reading and comprehension of clinical guidelines to
improve adherence
04/05/2018 15/06/2018 In progress
04/05/2018- Clinical Director confirmed the roll out will be by the end of May/beginning of June 2018 for the JRCALC app.
28/02/2018: The JRCALC app is in its final stages of development. The Clinical Director will advise once roll out is ready. HOPs and OMs have been
briefed.
None Bulletin articles
Report to Senior Leaders
Team meeting
Senior Leaders Team
QIP 17 QIP
18
3 All Implement Patient Experience Strategy Executive Director
of Nursing and
Quality
Head of Quality Review and update the Patient Experience Strategy 14/05/2018 26/07/2018 In progress
14/05/2018: The Strategy will be completed by the end of May 2018 and will be presented to the Trust Board of Directors for approval on 26 July
2018.
11/04/2018: This action is now being led on by the Head of Communications as the strategies are merging into one Communications Strategy
document. The timescale for this is being extended as this strategy will need to link with the revised Trust strategy once approved.
16/02/2018: The PE Strategy is now being merged with the Communications Strategy due to go to the next Quality Committee (10th May 2018).
A meeting has taken place between the Head of Communications, Head of Quality, Patient Engagement Manager and Patient Experience Manager
to move this forward. The Head of Communications is updating the Communications Strategy from the information provided at that meeting.
03/09/2017: VW and ST discussion ref whether Patient Engagement and Patient Experience strategies could be merged.
14/08/2017: VW Review of strategy in progress
14/06/2017: VW No further update
19/04/2017: VW Current Patient Experience Strategy being reviewed.
17/03/2017: VW This action has not yet commenced
Conflicting priorities
Awaiting sign off of
Trust Strategy in
order that Comms
Strategy can be
finalised
Patient Experience Strategy
approved at Board
Implementation plan
approved
Board of Directors
QIP
17.1
QIP
18
3 All Implement Patient Experience Strategy Executive Director
of Nursing and
Quality
Head of Quality Develop and complete a Strategy implementation plan 11/04/2018 31/05/2018 In progress
11/04/2018: This action links to QIP17 above and is dependent on the Trust Strategy and Communications Strategy.
16/02/2018: The strategy implementation plan links with the QIP 17 above. Deadline moved to 31 May 2018 as the Strategy Implementation
Plan will be appended to the Communications Strategy.
Awaiting sign off of
Trust Strategy in
order that Comms
Strategy can be
finalised

Ref No
Prev Ref Priority Core
Service Risk or Requirement Executive LeadObjective Owner/ Management Team
Quality Improvement Actions Date of Last Update
Current Deadline Current Status Summary of Progress
Risks to completion or other issues
Assurance Required Forum to Receive Assurance (and date)
Documents provided as assurance
Review date post completion
Expected Action Completion Impact Effectiveness
Actual Action Completion
Impact
QIP 18 QIP
47
3
Sup
po
rt S
ervi
ces Driving licence check records requested by inspectors. This is
already acknowledged as a Trust risk.
Executive Director
of Operations
Director of Human
Resources and
Organisational
Development
Head of Driver
Training
Review and improve compliance with completion of driving licence checks within
support services
(Operational RMG (resource management group) reports have driving licence
compliance levels reported weekly within the set of operational reports. All OM
areas are reported both on current levels of compliance and outstanding numbers to
be checked. It also includes the number of licences that have never been checked)
18/05/2018 30/06/2018 In progress
18/05/2018: Each directorate will complete their own checks, aided by a described process and proforma which the Deputy Director of HR and the
HR team are developing. This task can then be assigned and completed accordingly within each Directorate but with a degree of consistency.
14/05/2018: Driving licence check completion rates are reported to the Trust Resource Management Group (RMG) weekly for all frontline staff.
Check completion can be seen on GRS - support services reporting and ownership is to be confirmed - the Executive Director of Nursing and
Quality will request that Directors take responsibility for their teams' completion of driving licence checks via the Executive Directors Group. QPB
to take assurance that frontline checks are completed and will request the stats from the Head of Resource Management.
02/03/2018: The Head of Driver Training has sent the Deputy Director of HR and OD some information relating to driver licence checks and will be
pulled together to make a recommendation. Further discussions are required to agree who will take ownership of driving licence checks.
19/02/2018: Paper completed by Head of Driver Training and sent to Deputy Director of HR. Awaiting decision.
02/02/2018: HR lead on this at recruitment stage and once in employment, the responsibility for licence checks sits with OOs and OCs (and a much
greater level of responsibility due to the volume of annual checks required). In support of this, HR are currently revising the appraisal guidance
which will include a reminder to managers to check this annually. In addition, Robin Gwinnett (Head of Driver Training) is currently writing a
paper.
to be added Report on driving licence
completion to Quality
Committee
Quality Committee Happy App:
* Poster
* User Guide
* Administrator
Guide
FAQ
QIP 20 QIP
56
3 All Ensure that all third party arrangements are supported by
appropriate governance and do not compromise patient
safety
Deputy Finance
Director
Head of
Procurement
Ensure that all third party arrangements are supported by appropriate governance
and do not compromise patient safety
18/05/2018 30/06/2018 In progress
18/05/2018: Robust specification document created to support the tender process for private ambulance providers. As part of the process, each
provider had to provide assurance against a wide range of criteria, designed to explore whether their systems and processes met the Trusts
governance requirements. Each provider then presented to the Trust and had to complete clarifying questions. Providers who met the
specification requirements and passed this process have been awarded a place on the framework. A site audit will be conducted with each
provider to further check compliance against the specification, before they are able to attend patients on behalf of the Trust. Quarterly monitoring
meetings will then occur, together with an annual re-inspection. Any DATIXs and AI received will be fed into this monitoring process.
04/05/2018- Head of EPRR confirmed that thet he air ambulance SLAs have been approved and signed off by the Chief Executive and the charity
CEOs.
12/04/2018: Head of Procurement confirmed that the framework has been awareded subject to clinical audit inspections which are yet to take
place.
22/02/2018: The Head of Procurement confirmed that the ITT for Private Ambulance Providers is pending award.
Tender process
delays
Tender award confirmation Audit & Assurance
Committee
QIP 22 N/A 3
All
Welfare of staff subjected or who have the potential to be
subjected to verbal abuse, including Operational staff, call
handlers, the Patient Experience team and receptionists.
Director of Human
Resources and
Organisational
Development
Deputy Director of
HR and OD
Consider the welfare of staff subjected or who have the potential to be subjected to
verbal abuse, including Operational staff, call handlers, the Patient Experience team
and receptionists.
16/05/2018 30/06/2018 In progress
16/05/2018: Narrative requested from the Health, Safety and Securituy Lead - the Quality Programme Board of 14/05/2018 noted that there is
more work to be done with the Clinical Hubs and that mental health issues tends to be the issue of most concern. During 2018/19 there will be
further joint working between Communications and Health and Safety with the Unions to support staff.
18/04/2018: Comms are working on a joint campaign with Devon and Cornwall Police that aims to tackle all assaults on emergency service staff,
including verbal abuse- named #unacceptable.
Topic to be discussed via the Wellbeing Engagement Group for verbal abuse that’s experienced by call handlers, receptionists and the Patient
Experience team. First meeting of this group is 26 April 2018.
02/03/2018: Sam Fraser (Senior HR Business Partner) is working with the Head of Communications on this and hope to present an overview to
QDPB on 14.03.2018.
20/02/2018: Deputy Director of HR confirmed that she will provide narrative as action has been completed and is ready for closure.
QIP 23 N/A 3
All
Ensure that information (e.g. training data) is recorded
correctly against ESR designations
Director of Human
Resources and
Organisational
Development
Head of Education Data cleansing to be completed by Heads of Departments - to be coordinated and led
by the Head of Education
11/04/2018 31/12/2018 New
11/04/2018: Training compliance reports are derived from ESR staff lists. In order for accurate reports to be developed it is essenatial that Heads
of department ensure ESR is reflective of the staff they have in post. L+D and HR have been working with department leads by reporting non
compliant staff to open dialogire about their structure within ESR. This work continues and is significantly improving reproting data. It is
imperative that managers keep on top of change of circumstance and termination forms. This work will conclude on Friday 13th April.
21/02/2018: Action is being picked up by the Head of Education.
QIP 26 N/A 3
Fin
ance
Contracts: The governance and controls in place for all
service contracts within the Trust. This includes whether a
standard MOU/formal contract/signed letter of agreement is
in place for any service provided by the Trust.
Deputy Chief
Executive/Executive
Director of Finance
Planning Manager Quality Support Manager to meet with Planning Manager to discuss actions to be
taken to address contract governance and controls
09/03/2018 31/12/2018 New
09/03/2018: Priority is to ensure the Trusts core service contracts have been agreed and the appropriate contract paperwork is in place for
2018/19. Expected by the end of April 18.
By the end of Q1 18/19 the planning and performance team will have prepared a register of all known ad hoc service contracts that link to the
Trust's core services. This will be used to instigate and manage a programme of work from Q2 onwards to review each ad hoc contract, develope
standard in house template documents to ensure contracts are aligned and standardised where appropriate and a central register of all contracts
with expiry dates, copies of signed contracts etc is maintained going forward.
Transition in the
Planning and
Performance Team
and current sickness
absenceAppropriate governance
and controls in place for
all ad hoc core service
contracts
QIP
26.1
N/A 3
Fin
ance
Ensuring ‘other contracts’ have the correct documentation
and income is secured
Deputy Chief
Executive/Executive
Director of Finance
Planning Manager Quality Support Manager to meet with Planning Manager to discuss actions to be
taken to address contract governance and controls
09/03/2018 31/12/2018 New
09/03/2018: Priority is to ensure the Trusts core service contracts have been agreed and the appropriate contract paperwork is in place for
2018/19. Expected by the end of April 18.
By the end of Q1 18/19 the planning and performance team will have prepared a register of all known ad hoc service contracts that link to the
Trust's core services. This will be used to instigate and manage a programme of work from Q2 onwards to review each ad hoc contract, develope
standard in house template documents to ensure contracts are aligned and standardised where appropriate and a central register of all contracts
with expiry dates, copies of signed contracts etc is maintained going forward.
Transition in the
Planning and
Performance Team
and current sickness
absence
Appropriate governance
and controls in place for
all ad hoc core service
contracts
QUP
26.2
N/A 3
Fin
ance
Managing the smaller contracts/additional services to
contracts. Particularly historical ones, which have rolled on
with a lack of detail
Deputy Chief
Executive/Executive
Director of Finance
Planning Manager Quality Support Manager to meet with Planning Manager to discuss actions to be
taken to address contract governance and controls
16/05/2018 31/12/2018 New
09/03/2018: Priority is to ensure the Trusts core service contracts have been agreed and the appropriate contract paperwork is in place for
2018/19. Expected by the end of April 18.
By the end of Q1 18/19 the planning and performance team will have prepared a register of all known ad hoc service contracts that link to the
Trust's core services. This will be used to instigate and manage a programme of work from Q2 onwards to review each ad hoc contract, develope
standard in house template documents to ensure contracts are aligned and standardised where appropriate and a central register of all contracts
with expiry dates, copies of signed contracts etc is maintained going forward.
Transition in the
Planning and
Performance Team
and current sickness
absence Appropriate governance
and controls in place for
all ad hoc core service
contracts
QIP 29 N/A 3
A&
E
Local GP shortages & challenges. This has a knock on effect
that several GP practises are recruiting our highest skilled
clinicians and depleting our workforce of suitably qualified
SPs
Executive Director
of Operations
Operational
Managers
Medical Directorate
The Trust is to discuss SP/Paramedic recruitment plans with the STP leads and with
A&E Commissioners with a view to understanding;
(a) what their STP plans are assuming in terms of Paramedic numbers
(b) what the timescales are that they are working to
16/05/2018 31/12/2018 New
16/05/2018: A review of the Specialist Paramedic Strategy will be led by the Trust's Executive Medical Director.
11/05/2018: Ken Wenman, Dr Andy Smith, Amy Beet, Neil Lentern and Jess Hodgman met with two SPLDOs yesterday to discuss internal plans.
The action arising from this meeting in the first instance is with AGS to arrange a follow up call/meeting to agree a short placement for the SPLDOs
to assist in writing a strategy for Specialist Paramedics and to work with HR to finalise a Portfolio Contract template.
30/01/2018: The Trust's position is that there needs to be a joint plan which forecasts forwards 2/3 years with a clear strategy. The contract
meeting on 01/02/2018 will be the first opportunity to discuss this across the SW. In the interim from an operational resourcing point of view,
managers are backfilling vacancies created in the SP workforce with overtime, new Paramedics.
QIP 33 3
A&
E
Align the culture between Exeter and Bristol 999 Hubs Executive Director
of Operations
Head of Clinical Hubs The theme and focus for 2018/19 is consolidation and performance in the clinical
hubs. The actions underpinning this are as follows:
1. New Management Structure / Head of Clinical Hubs and new Deputy in South
2. Work Plan includes a focus on aligning practices and behaviour across the 2 hubs
in order for the hubs to act more consistently
3. New single triage system, telephony, standardised CAD means that the hubs
operate on the same platforms and can therefore work virtually in the true sense of
the word
4. Hub participation in the cultural surveys
5. Re establishment of regular communication events run by the senior team in order
to present a consistent and coherent work plan to staff and to provide a forum for
staff engagement and contribution
17/05/2018 31/03/2019 New17/05/2018: The Head of Clinical Hubs has confirmed that the deputy post in the South Hub secondment has been extended for six months due to
the successful completion of objectives. An objective has been developed to build on success of last six months. Consolidation task and finish
groups have been set up with nominated leads for each function of call taking, dispatch and clinical. Metrics for success will include completion of
action logs, score survey results, subsequent staff survey and CQC review. A single triage system is in place and the Hubs have paticipated in a
SCORE cultural survey. Dispatcher engagement days have been held and were a huge success, clinical education days scheduled for June,
Facebook live also created with view to broadcast before June 2018.
13/04/2018: Continuation of programme to align structures, processes and practice
26/02/2018: The new management structure is to be embedded. A piece of work is in process to identify disparate practices and to bring about
alignment of process and practice (following completion of implementation of virtual systems). There is regular engagement with unions and a
series of staff communications events are being arranged.
15/02/2018: New Head of Clinical Hubs and new Deputy Head of Clinical Hubs South started. A programme of work will be ongoing to enable
consistent virtual hub working.
QIP 36 N/A 3
All
Ensure that staff are engaged in obtaining the views of
patients
Executive Director
of Nursing and
Quality
Patient Engagement
Manager
Implement Engagement Plan, including events, station Open Days and complaints
leaflets
12/04/2018 31/12/2018 New
09/05/2018: Current Engagement Plan is in place and includes a number of engagement events.
12/04/2018: 4 set station Open Days have been confirmed.
20/02/2018: Patient Engagement Manager is currently working on an engagement plan for 2018/19, station open days and freew shows have
been booked and focus groups will be run once the quality priorities have been set and agreed.
QIP 37 N/A 3
All
Consider how the flow of feedback from the public can be
improved
Executive Director
of Nursing and
Quality
Patient Engagement
Manager
Produce and implement revised joint Communications/Engagement/Experience
Strategy
16/05/2018 31/12/2018 New16/05/2018: Patient Engagement Plan for 2017/18 agrred. A joint Communications, Experience and Engagement Strategy will be produced by the
end of May 2018.
19/02/2018: A joint communications and engagement strategy will be drafted to support the new Trust Strategy.

Ref No
Prev Ref Priority Core
Service Risk or Requirement Executive LeadObjective Owner/ Management Team
Quality Improvement Actions Date of Last Update
Current Deadline Current Status Summary of Progress
Risks to completion or other issues
Assurance Required Forum to Receive Assurance (and date)
Documents provided as assurance
Review date post completion
Expected Action Completion Impact Effectiveness
Actual Action Completion
Impact
QIP 40 QIP 65 2
All
Quality Summit Comment
●Consider how the Trust can ensure visible and available
leadership across the organisation which is accessible to staff,
eg:
o Director chatrooms
o Investigate the national ‘Listening in Action’ programme
o Resurrect daily performance briefings
●Ensure we care for our staff in the same way we care for
our patients, ie “If you look after your staff, they will look
after your customers,” Richard Branson
Directors Group Trust Secretary
Head of
Communications
Review what the Trust already does well in terms of making its leadership more
visible (eg chatrooms and paid staff meetings) and develop a targeted programme of
leadership engagement
09/03/2018 30/06/2018 Reopened
09/03/2018: Review of last year's Board visits to Trust sites completed, forward planning to be completed.
QIP 41 RCAP
6.1
2
All
Complete the review of reporting to Trust groups and
committees to produce a clear table of the information
presented to each forum and review effectiveness of
reporting arrangements
Executive Director
of Nursing and
Quality
Trust Secretary Complete the review of reporting to Trust groups and committees to produce a clear
table of the information presented to each forum and review effectiveness of
reporting arrangements
14/05/2018 30/06/2018 Reopened
14/05/2018: A review of reporting paper will be presented to the Executive Directors Group on 15/05/2018.
09/03/2018: Action started, to be completed.

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 6
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Quality Committee Assurance Report
Prepared by: Helen White, EA to the Executive Director of Nursing and Quality
Presented by: Venessa James, Non-Executive Director
Action: Assurance
Recommendation: The Trust Board of Directors is asked to take assurance from the report of the meeting of the Quality Committee held on 10 May 2018.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 6
Quality Committee Assurance Report 1. Overview of the Meeting 1.1 Venessa James (Non-Executive Director) chaired the meeting, it was noted that the 111
Care Quality Committee (CQC) Inspection went very well and the chair commended the Trust on the improvement of the service and thanked all those involved. This was clearly recognised by the CQC Inspectors is a positive indicator for the up and coming unannounced Trust core service CQC inspection.
1.2 The Chair noted that the Non-Executive Director’s (NEDS) completed mandatory training
on Safeguarding which was led by Simon Hester, Head of Safeguarding. The training left a lasting impression on the NEDS and Executive Directors which led to two policies being considered for review - The Lone working Policy and Chaperone Policy.
1.3 The Chair commented that she had met with the seven New Zealand paramedics at St
Leonard’s last week and was impressed how keen and enthusiastic they were which will hopefully cascade throughout the Trust.
1.4 The format of the agenda has changed with the three Director level reports - Executive
Director of Nursing & Quality, Executive Medical Director and Clinical Director which now include some of the reports previously listed separately. The Committee agreed although the reports are far bigger it does streamline the agenda.
1.5 The Executive Director of Nursing & Quality presented her report to the meeting and noted
that the 111 CQC Inspection report is expected at the end of May 2018, which should be in time for the main unannounced inspection, this is anticipated to be in the first two weeks of June 2018.
1.6 The updated and reviewed Never Events Framework and Policy was published by NHS
Improvement in January 2018. Originally, this included a new never event relating to undetected esophageal intubation. Following a number of queries from ambulance services, including SWASFT, in relation to its practical application, the never event is currently suspended pending further review.
1.7 In late 2017, SWASFT was nominated by NHS Improvement to participate in a programme called ‘Moving to Good’, facilitated by the Korn Ferry a part of the Hay Group. A team of 12 members of staff participated in the programme on behalf of the Trust, and have attended a half day workshop (at HQ) with the facilitators, in addition the team attended a two-day residential event in Reading, with the three other provider organisations participating from the South Region. The half day workshop focused on the approach for the programme and an introduction to some of the tools and techniques the group will employ during the process. The two-day residential expanded on how to use these tools, and the group focused on developing a series of actions that it would begin to take forward within the engagement work.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 6
1.8 The Nursing & Quality Directorate in partnership with the Medical and Learning & Development Teams have been engaged within a ‘Quality Buddy’ arrangement with Operational Managers, this has been well received within operations. The Quality Buddy group meets on a monthly basis to discuss the informal and formal issues raised and to agree actions. Due to the similarity of the issues the Learning from Experience Group will be merged with the Quality Buddy Group into a new Continuous Learning Group, this will meet for the first time in May. This includes the development of a proactive engagement process with staff regarding how the quality of care can be improved. The Board receives assurance on the risk to Patient Safety through the Quality Committee and the Board Assurance Framework.
1.9 The ARP Position Statement was shared with the Quality Committee, this had been
requested by NHS Improvement to describe the residual risk to patient’s whilst there remains a gap in the delivery of ARP standards.
1.10 The National SI Policy - NHS Improvement is currently in the process of reviewing the
Serious Incident framework and have been seeking the views of a wide range of people which has included experts in investigations to members of the public. This engagement period remains open until the 12 June 2018. Once the engagement period has closed NHS Improvement plan to analyse the results and use the information to inform a new version of the National Serious Incident framework. The revised framework is to be drafted over the summer and it is hoped that the new document will be published by the end of 2018.
2. Assurance
Document Further assurance requested by Committee Executive Director of Nursing & Quality
Assurance was taken by the Executive Director of Nursing & Quality Report which included the Draft Quality Report and Account 2017/18. The priorities within the Quality Account are classified into one of three categories – Clinical Effectiveness, Patient Experience and Patient Safety. The Council of Governors selected the“Management of the Older Patient” priority for external audit and review. Assurance was taken by the Quality Committee from the reports on Risk Management and the Quality Improvement Plan (QIP). A separate report will be provided to the Trust Board and Directors. Risk Register Platform - The next steps have been agreed with Paul Love (NED) for the content of the Board reports for risk moving forwards. The structure of directorate risk registers are to be refined and incorporated within the Pentana system. Training will be disseminated to directorate leads when the risks are fully incorporated and the system has been tested.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 4 of 6
Executive Medical Director Report
Assurance was taken by the Quality Committee from the Executive Medical Directors Report which included the primary aims of the Clinical Strategy which are to deliver safe and effective clinical care to achieve the best possible patient outcomes. Improving Triage in the Clinical Hub - Clinical Severity/Risk Stratification and the Ambulance Response Programme (ARP) - clinical Quality Indicators (CQI) were discussed and assurance taken. The Quality Committee requested further assurance on the Ambulance Quality Indicators at future meetings.
Clinical Director Report
Assurance was taken by the Quality Committee from the Clinical Directors Report which includes and update from the Clinical Effectiveness Group, Clinical Research, Audit and Quality Improvement and CQUINS.
Infection Prevention and Control and Annual Hand Decontamination Report
Assurance was taken by the Quality Committee from the Infection and Prevention and Control and Annual Hand Decontamination Report. A request was made to receive absolute numbers of staff compliant with Bare Below the Elbow and Hand decontamination as well as percentages
Patient Safety
Assurance was taken by the Quality Committee from the Patient Safety Report. The annual report will be provided to the Trust Board and Directors.
Clinical Hub Report 999
Assurance was taken by the Quality Committee from the Clinical Hub Report 999. The key themes for Clinical and Non-Clinical Audit were provided, along with a summary of the new Governance Structure and position statements on the plans to work towards achieving full Audit Compliance by October. The Trust has submitted an application to become an Accredited Centre of Excellence (MPDS).

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 5 of 6
Clinical Hub Report Integrated Urgent Care Service
Assurance was taken by the Quality Committee from the Clinical Hub Report - Integrated Urgent Care Service. The IUC service line can demonstrate full audit compliance with the NHS Pathways licence requirement. This continues the compliant position seen in Q3. Three thematic reviews took place on non-clinical call audits in Quarter 3. Key projects are detailed in section 4 of the report. Remote/home clinical working has been launched, clinical floorwalking is being planned and the Trust are submitting the tender response for the Dorset IUC contract.
Safeguarding Report
Assurance was taken by the Quality Committee from the Safeguarding Report.
Patient and Public Engagement
Assurance was taken by the Quality Committee from the Patient and Public Engagement Report.
Patient Experience
Assurance was taken by the Quality Committee from the Patient Experience Report. The annual report will be provided to the Trust Board and Directors. The high quality of complaint response to the public was noted, it was noted that timeliness of response had also improved but that this required further improvement activity.
EPRR
Assurance was taken by the Quality Committee from the EPRR report and approved the actions to meet the recommendations made within the National Ambulance Resilience Unit (NARU) Capabilities Review and independent West Midlands Ambulance Service HR review of HART.
3. Documents for Review 3.1 The Quality Committee was asked to approve the new 999 Quality Assurance Audit Policy.
The purpose of the policy is to outline the process for quality assurance and feedback to ensure a fair and appropriate approach to the auditing of calls, and to ensure that EMDs, Clinicians and Auditors are supported during their duties. The policy will outline the process for accreditation for MPDS and LowCode. The Trust is dedicated to providing high standards of care; in order to do this the Clinical Hubs will strive to achieve and maintain Accredited Centre of Excellence ACE standards of compliancy and deliver excellent customer service to all service users.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 6 of 6
3.2 Due to statutory requirements and the important nature of the work of the Medicines
Governance Group, the group will report directly to the Quality Committee. The terms of reference have been altered to reflect this and the Quality Committee approved the change in reporting and the terms of reference
3.3 The Quality Committee was asked to approve the amended Responder Governance
Policy. This policy aims to provide a robust framework for the recruitment, management and deployment of Responders across the organisation. The objectives of the policy are to ensure patient safety, Responder welfare and compliance with all relevant legislative and regulatory requirements. The Committee requested as there is not a specific Governance reporting root at present that The Responder service reports to the Quality Committee six monthly.
3.4 The Quality Committee received a short presentation on Welfare Calls to provide a clinical
assessment if a resource is not available. David Fletcher, Head of Clinical Hubs was tasked to complete an audit on the Emergency Medical Dispatcher (EMD) and Clinician Primary Review process which is set out in SOP VH07 - Procedure for Welfare Call Management. It was concluded that the policy and process require improvement but the action plan moving forward is that Welfare Call Management is on the divisional risk register, clinical hub clinician establishment and measurement, establishment is improving with trajectory but to be fully established by the end of June and information management request. The Quality Committee took assurance from the update.
4. Issues Referred to the Board of Directors 4.1 The Quality Committee requested that the Board note that due to timing and the
importance of the Mental Health Strategy this will go straight to Board rather than through the Quality Committee first. This is due to the increasing importance of the recognition of the needs of Mental Health Service Users and the legislative framework
5. Issues Referred to the Executive Directors Group 5.1 The Quality Committee received a proposal for Rest Break Provision and End of Shift
Protection which has yet to go to Directors but the Quality Committee was happy with the proposal subject to approval at Directors. The Committee asked for a further update in six months.
6. Recommendation 6.1 The Trust Board of Directors is asked to take assurance from the report of the meeting of
the Quality Committee held on 10 May 2018. Helen White EA to the Executive Director of Nursing

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 2
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Mental Health Strategy
Prepared by:
Dave Partlow, Consultant Paramedic Marty McAuley, Trust Secretary Jenny Winslade, Executive Director of Nursing and Quality Dr Andy Smith, Executive Medical Director
Presented by: Dr Andy Smith, Executive Medical Director
Action: Approval
Recommendation: The Trust Board of Directors is asked to approve the Mental Health Strategy.
Executive Summary:
The provision of care to patients suffering mental health crisis is as important as the provision of care to those suffering a physical crisis. However, there are clearly major challenges for all those engaged in developing services to meet the needs of those patients suffering mental health issues. As a Trust, we are committed to working with and supporting health and social care partners in developing services to better meet the needs of patients who make contact with us following a mental health crisis. We are further committed to ensuring that those who make contact with the ambulance service are managed with a Parity of Esteem, that is to say as equal partners with those whose need follows a medical crisis. This strategy outlines how the Trust will aim to balance the physical needs and the mental needs of patient health. It explains the vision we have to support patients with mental health needs who use the South Western Ambulance Service. Through the successful delivery of this strategy the following objectives will be delivered:
Support delivery of strategic goal three – Every Patient Matters Compliance with the requirement to provide a 30minute response to patients detained under section 136 of the Mental Health Act;

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 2
Contribution to performance with % of patients treated vs conveyed
to hospital; Delivery of the quality strategy through good patient experience; Support the delivery of aims and objectives of the Crisis Care
Concordat in relation to the delivery of urgent and emergency care;
Ensure the principle of Parity of Esteem is delivered for those accessing urgent and emergency care through the Trust Services
Support the development of system wide service reconfiguration; Work to improve staff education and awareness of mental ill health
presentations; Continue to ensure that the needs of patients suffering from
mental ill health are considered in wider strategic developments and in particular in the further development of national programmes including the Ambulance Response Programme.
To enable the strategy to be delivered there will be six themes of work to be undertaken. A number of these have significant external reliance.
Theme 1 - Development of mental health pathways. Theme 2 - Mental health triage. Theme 3- MH support within the SWASFT Clinical Hub. Theme 4 - Access to medical notes and associated Care Plans for
patients known to mental health services. Theme 5 - Independent review of the Mental Health Act and
potential for expansion of lawful powers. Theme 6 - Consideration of Specialist Paramedics in Mental
Health. The Executive Medical Director is accountable for the successful delivery of the Strategy and quarterly monitoring will take place through the Quality Committee. This Strategy will be subject to annual review by the Quality Committee and authority to approve the strategy and any amendments is to rest with the Board.

Mental Health Strategy
Page 1 of 14
Mental Health Strategy
Version: DRAFT
Approved by: Trust Board of Directors
Date approved: 25 May 2018
Name of originator/author: Dave Partlow, Consultant Paramedic (East) Marty McAuley, Trust Secretary Jenny Winslade, Executive Director of Nursing and Quality Dr Andy Smith, Executive Medical Director
Name of responsible task group:
Date issued:
Review date:

Mental Health Strategy
Page 2 of 14
Contents
1. Introduction .................................................................................................................. 4
2. Aims and Principles of Delivery ................................................................................... 4
3. Scope and Context ...................................................................................................... 5
4. Service and Function Analysis .................................................................................. 10
5. Key Performance Indicators ...................................................................................... 11
6. SWOT Analysis ......................................................................................................... 11
7. Planned Developments ............................................................................................. 11
8. Environmental Management ...................................................................................... 13
9. Business Continuity and Resilience .......................................................................... 14
10. Risk ........................................................................................................................... 14
11. Monitoring, Review and Governance ........................................................................ 14
12. Associated Documentation ........................................................................................ 14

Mental Health Strategy
Page 3 of 14
Trust Strategy Foreword SWASFT has a number of specific corporate responsibilities relating to patient and staff safety and wellbeing which should be included within all Trust policy and strategy, as a foreword inside the front cover: Code of Conduct and Conflict of Interest Policy - The Trust Code of Conduct for Staff and its Conflict of Interest and Anti-Bribery policies set out the expectations of the Trust in respect of staff behaviour. SWASFT employees are expected to observe the principles of the Code of Conduct and these policies by declaring any gifts received or potential conflicts of interest in a timely manner, and upholding the Trust zero-tolerance to bribery. Compassion in Practice – SWASFT will promote the values and behaviours within the Compassion in Practice model which provide an easily understood way to explain our role as professionals and care staff and to hold ourselves to account for the care and services that we provide. These values and behaviours reflect the Trust’s commitment to developing an outstanding service through the conduct and actions of all staff. SWASFT will encourage staff to demonstrate how they apply the core competencies of Care, Compassion, Competence, Communication, Courage, and Commitment to ensure our patients experience compassionate care. Duty of Candour - SWASFT will, as far as is reasonably practicable, apply the statutory Duty of Candour to all reported incidents where the Trust believes it has caused moderate or severe harm or death to a patient. This entails providing the affected patient or next of kin (within strict timescales) with: all information known to date; an apology; an explanation about any investigation; written follow-up; reasonable support; and the outcome fed back in person (unless they do not want it). The only exception is where making contact could have a negative impact upon the next of kin. SWASFT employees are expected to support this process by highlighting (early) any incident where they believe harm may have been caused. Equality Act 2010 and the Public Sector Equality Duty - SWASFT will act in accordance with the Equality Act 2010, which bans unfair treatment and helps achieve equal opportunities in the workplace. The Equality Duty has three aims, requiring public bodies to have due regard to: eliminating unlawful discrimination, harassment, victimization and any other conduct prohibited by the Act; advancing equality of opportunity between people who share a protected characteristic and people who do not share it; and fostering good relations between people who share a protected characteristic and people who do not share it. SWASFT employees are expected to observe Trust policy and the maintenance of a fair and equitable workplace. Fit and Proper Persons - SWASFT has a statutory duty not to appoint a person or allow a person to continue to be an executive director or equivalent or a non-executive director under given circumstances. They must be: of good character; have the necessary qualifications, skills and experience; able to perform the work they are employed for (with reasonable adjustments); able to provide information required under Schedule 3 (Health and Social Care Act 2008 (Regulated Activities) Regulations 2014). The definition of good character is not the test of having no criminal convictions but instead rests upon judgement as to whether the person’s character is such that they can be relied upon to do the right thing under all circumstances. This implies discretion for boards in reaching a decision and allows that people can change over time. Health and Safety - SWASFT will, so far as is reasonably practicable, act in accordance with the Health and Safety at Work etc. Act 1974, the Management of Health and Safety at Work Regulations 1999 and associated legislation and approved codes of practice. It will provide and maintain, so far as is reasonable, a working environment for employees which is safe, without risks to health, with adequate facilities and arrangements for health at work. SWASFT employees are expected to observe Trust policy and support the maintenance of a safe and healthy workplace. Information Governance - SWASFT recognises that its records and information must managed, handled and protected in accordance with the requirements of the Data Protection Act 1998 and other legislation, not only to serve its business needs, but also to support the provision of highest quality patient care and ensure individual’s rights in respect of their personal data are observed. SWASFT employees are expected to respect their contact with personal or sensitive information and protect it in line with Trust policy. NHS Constitution - SWASFT will adhere to the principles within the NHS Constitution including: the rights to which patients, public and staff are entitled; the pledges which the NHS is committed to uphold; and the duties which public, patients and staff owe to one another to ensure the NHS operates fairly and effectively. SWASFT employees are expected to uphold the duties set out in the Constitution. Risk Management - SWASFT will maintain good risk management arrangements by all managers and staff by encouraging the active identification of risks, and eliminating those risks or reducing them to the lowest level that is reasonably practicable through appropriate control mechanisms. This is to ensure harm, damage and potential losses are avoided or minimized, and the continuing provision of high quality services to patients, stakeholders, employees and the public. SWASFT employees are expected to support the identification of risk by reporting adverse incidents or near misses through the Trust web-based incident reporting system.

Mental Health Strategy
Page 4 of 14
1. Introduction 1.1 The Trust is committed to delivering high quality affordable care to those in need,
irrespective of the nature of the illness or injury. SWASFT fully support the national requirement to ensure that health and social care providers look to achieve a Parity of Esteem between physical and mental ill health.
1.2 The provision of care to patients suffering mental health crisis is as important as the
provision of care to those suffering a physical crisis. However, there are clearly major challenges for all those engaged in developing services to meet the needs of those patients suffering mental health issues.
1.3 As a Trust, we are committed to working with and supporting health and social care
partners in developing services to better meet the needs of patients who make contact with us following a mental health crisis. We are further committed to ensuring that those who make contact with the Ambulance Service are managed with a Parity of Esteem, that is to say as equal partners with those whose need follows a medical crisis.
2. Aims and Principles of Delivery
2.1 This Strategy outlines how the Trust will aim to balance the physical needs and the
mental needs of patient health. It explains the vision we have to support patients with mental health needs who use the South Western Ambulance Service.
2.2 Through the successful delivery of this strategy the following objectives will be
delivered:
Support delivery of strategic goal three – Every Patient Matters Compliance with the requirement to provide a 30minute response to patients detained under section 136 of the Mental Health Act;
Contribution to performance with % of patients treated vs conveyed to hospital Delivery of the quality strategy through good patient experience; Support the delivery of aims and objectives of the Crisis Care Concordat in
relation to the delivery of urgent and emergency care; Ensure the principle of Parity of Esteem is delivered for those accessing urgent
and emergency care through the Trust Services; Support the development of system wide service reconfiguration; Work to improve staff education and awareness of mental ill health
presentations; Continue to ensure that the needs of patients suffering from mental ill health are
considered in wider strategic developments and in particular in the further development of national programmes including the Ambulance Response Programme.

Mental Health Strategy
Page 5 of 14
2.3 To enable the strategy to be delivered there will be six themes of work to be
undertaken. A number of these have significant external reliance. Theme 1 - Development of mental health pathways. Theme 2 - Mental health triage. Theme 3- MH support within the SWASFT Clinical Hub. Theme 4 - Access to medical notes and associated Care Plans for patients
known to mental health services. Theme 5 - Independent review of the Mental Health Act and potential for
expansion of lawful powers. Theme 6 - Consideration of Specialist Paramedics in Mental Health.
2.4 In delivering the proposals set out in the previous sections, this Strategy will need
to consider the following areas: Area Detail
Communications
This Strategy proposes a number of significant changes. Implementation of these may require formal engagement activities with key stakeholders as a minimum, with the potential for statutory consultation. Through the Trust Communications Strategy the Trust will ensure it has the appropriate tools and resources in place to manage these requirements.
Partnership Working Significant support from external partners, in regards to the commissioning and provision of alternatives to ED conveyance and to the support for ambulance access
Availability of staff Significant shortages of mental health professionals is being experienced nationally, improvements in recruitment and retention of staff will need to be considered for any development that involves specialist clinical staff
Digital development Any extension of access to appropriate care plans will require commitment from all parties to work together to deliver significant digital improvements
3. Scope and Context 3.1 Due to the nature of the presentation and potential for there to be a physical
component to their illness, in many cases, patients with mental health problems who make contact with the Trust will require conveyance to an Emergency Department.
3.2 However, in some cases the patients' condition may not warrant conveyance to an
acute hospital and in such circumstances a general lack of available alternatives to acute conveyance create particular difficulties in delivering the most appropriate care. This is especially problematic when there are no lawful mechanisms by which detention may be enforced by ambulance clinicians and conveyance undertaken under the auspices of the Mental Health Act 1983.
3.3 Places of Safety (136 suites) will not accept patients who are not detained as they
are then unable to hold individuals for the purpose of assessment.

Mental Health Strategy
Page 6 of 14
3.4 Services for those patients with mental health problems are locally defined and vary greatly both in their availability and in the application of access criteria. However the Trust is committed to engaging with partners to ensure that patients receive the most appropriate care, that meets their needs in a timely fashion and that ensures a continued commitment to the Parity of Esteem.
3.5 In February 2014 the Government published its Mental Health Crisis Care
Concordat: Improving outcomes for people experiencing mental health crisis. 3.6 The Concordat challenges local areas to make sure:
That health-based places of safety and beds are available 24/7 in case someone experiences a mental health crisis.
That Police custody should not be used because mental health services are not available and police vehicles should also not be used to transfer patients.
That timescales are put in place so police responding to mental health crisis know how long they have to wait for a response from health and social care workers. This will make sure patients get suitable care as soon as possible.
That people in crisis should expect that services will share essential ‘need to know’ information about them so they can receive the best care possible. This may include any history of physical violence, self-harm or drink or drug history.
Figures suggest some black and minority ethnic groups are detained more frequently under the Mental Health Act. Where this is the case, it must be addressed by local services working with local communities so that the standards set out in the Concordat are met.
A 24-hour helpline should be available for people with mental health problems and the crisis resolution team should be accessible 24 hours a day, 7 days a week.
3.7 Clearly there are major challenges for all those engaged in developing the
provision of care to meet the needs of those in crisis, not least of which will be the provision of adequate services to accept appropriate referral and reduce the inappropriate use of police cells for patients who have committed no crime.
3.8 As an Ambulance Service, we will be called upon to ensure that all patients who
require transport following a mental health crisis are managed with a Parity of Esteem, that is to say as equal partners with those patients whose need for transport follows a medical crisis. The Trust is committed to better understanding how parity can be applied and how mental health presentations can be matched across to equivalent physical health presentations and thereby how this can be further applied to the Ambulance Response Programme and the determination of resource allocation priorities.
3.9 The Trust has formalised its commitment to the Crisis Care Concordat, both
nationally through an AACE declaration and also locally by signing a Concordat declaration within each locality.

Mental Health Strategy
Page 7 of 14
3.10 In addition to the Crisis Care Concordat a number of key changes have been made to the Mental Health Act 1983 following the implementation of the Policing and Crime Act 2017.
3.11 These changes, which came into effect on 11 November 2017 impact on the Trust
and particularly when engaged in supporting the care of patients who require detention under section of the Mental Health Act.
3.12 The most relevant changes are detailed below:
Section 136 powers may be exercised anywhere other than in a private dwelling, this includes the private garden and any associated outbuildings.
It is unlawful to use a Police Station (not just Police Cells) as a place of safety for anyone under the age of 18 in any circumstances.
A Police Station can only be used as a place of safety for adults in specific circumstances, which are set out in regulations.
The previous maximum detention period of up to 72 hours will be reduced to 24 hours (unless a doctor certifies that an extension of up to 12 hours is necessary).
Before exercising a section 136 power Police Officers must, where practicable, consult a health professional (definition of health professional includes “Paramedic”).
Where a section 135 warrant has been executed, a person may be kept at their home for the purposes of an assessment rather than being removed to another place of safety (in line with what is already possible under section 136).
A new search power will allow Police Officers to search persons subject to section 135 or 136 powers for protective purposes.
3.13 The Five Year Forward View reminds us that mental health is a key deliverable
when reviewing the provision of effective health care. The often quoted statistic is that one in four of us, around 13 million people, will suffer from a diagnosable mental disorder in any given year. Below the age of 16, one in ten children suffers from a diagnosable condition, the equivalent of three pupils in every classroom. With around 70% of adult mental ill health being traceable to events prior to the 14th birthday, child and adolescent mental health is a primary objective.
3.14 As reported in the National Health Executive Bulletin
(http://www.nationalhealthexecutive.com/Health-Care-News/calls-for-ringfenced-mh-budget-as-ambulance-call-outs-soar-by-25 ) Mental Health activity has increased by 23% against the levels from 2014/15.
3.15 Trust C3 data from the 2016/17 financial year identified around 45,000 patients that
appeared to have made contact with SWASFT after experiencing mental ill health. The actual figure is likely to be nearer to 60,000, as the identification of a mental health cause is often hidden in the initial triage, with calls being categorised as laceration or trauma, when for example, the underlying cause is significant self-harm. To put this in context, calls following identification of stroke symptoms for the same period would equate to around 15,000.

Mental Health Strategy
Page 8 of 14
3.16 Calls are predominantly received from the patient and/or a family member, although a proportion of calls come from 111 or Police colleagues. This profile is dissimilar to physical health, where a significant proportion come from health care professionals.
3.17 In addition, it is acknowledged that current triage systems including MPDS and
NHS Pathways are inadequate and do not effectively triage mental health presentations. This is particularly true when the chief complaint relates to an acute psychosis or other behavioural disturbance. This increases the likelihood of a dispatch disposition being reached and the requirement to respond for face to face intervention.
3.18 This strategy has been developed in the context of the following key publications
and the overall strategic direction of the Trust: Context Description Implications
Political Crisis Care Concordat 2014, Five Year Forward View for Mental Health 2016 ACQI
Significant commitment from central government to improve care provided to patients experiencing mental health illness Inclusion of a Mental Health Ambulance Clinical Quality Indicator in national metrics being developed in 2018 In addition CQUIN for Acute Trusts in part focus on admission reduction in relation to mental health and seek to deliver: For 2018/19: 1. Sustain the reduction in year 1 of
attendances to A&E for those within the selected cohort of frequent attenders who would benefit from mental health and psychosocial interventions.
2. Reduce total number of attendances
to A&E by 10% for all people with primary mental health needs.
Economic Significant factor in increasing demand and increasing call cycle times associated with face to face and remote management of mental health presentations
Significant potential to better manage activity and increase ability of the trust to manage a portion of demand without recourse to resource allocation to scene. Increasing challenge from health care partners and commission organisations regarding compliance with contractual obligations.
Social Heads Together Campaign and other high profile social awareness campaigns, increasing prevalence of mental health illness and decreasing stigma associated with mental ill health
This has the potential to further increase the demand by empowering those affected to seek help

Mental Health Strategy
Page 9 of 14
Context Description Implications
Technological Developing systems integration and digital programmes
Potential to provide access to patient clinical records to aid decision making and care plan compliance
Environmental N/A N/A
Legal Mental Health Act 1983, Mental Capacity Act 2005, Policing and Crime Act 2017
Policing and Crime Act and Mental Health Act Code of Practice in particular reinforce the requirement for ambulance services to assess and convey patients in crisis. It is unacceptable for patients to be conveyed by police resources unless in extremis.
Trust Strategic Goals The Trust commits to placing the patient at the heart of everything it does and this strategy is intended to strengthen and support patient services particularly in relation to:
SG1: Every Patient Matters Delivering compassionate, clinically-effective care across all Trust services that is safe, responsive and provides confidence and reassurance to patients and their families. SG2: Every Team Member Matters Delivering strong, inclusive and caring leadership to a team made up of the right people, with the right skills, values and behaviours. SG3: Every Pound Matters Delivering robust financial discipline, including reduced variation and increased productivity and efficiency, to ensure “healthy” finances.
Delivery of the Parity of Esteem is a fundamental cornerstone of SG1, “every patient”, must not just mean each patient matters to the trust, it also must mean that every patient is of importance in equal measure irrespective of the nature of the clinical presentation. Our staff require the right skills, need the right values and need to demonstrate the right behaviours when managing complex and often challenging scenarios that come with some mental health incidents. Opportunities exist to better manage patients in crisis, to utilise and enhance the ability of the Clinical Hubs to provide appropriate care without the requirement for face to face intervention. Significant improvements in community based services with direct access protocols better meet the needs of the patients, the Trust and the wider health and social care arena.
Strategic Objectives
ACQI for Mental Health and Crisis Care Concordat
ACQI for mental Health is likely to mirror the current requirement under the Crisis Care Concordat to ensure that patients detained under the Mental Health Act section 136 are provided with a 30minue Response

Mental Health Strategy
Page 10 of 14
4. Service and Function Analysis 4.1 The Trusts faces significant demand from patients experiencing mental health
illness. Frequency carries through each 24 period and by day of week, as illustrated by Figure 1 which shows the time of call and Figure 2 by the day of the week.
Figure 1 - Incident Frequency by Time of Call
4.2 Activity peaks later in the evening as mental health services close and increases
during the weekend period. Reduced access to mental health services and a complex legal framework requires ambulance crews to utilise the Emergency Department as the single option for conveyance, often irrespective of the appropriateness of such a pathway of care.
Figure 2 - Incident Frequency by Day of Week

Mental Health Strategy
Page 11 of 14
5. Key Performance Indicators 5.1 The provision of clinical indicators for mental health are complex, however this
strategy sets out a commitment to evaluate the provision of key indicators. Reviewing what measurements of quality can be achieved and how these can be measured over time.
5.2 Key metrics will include:
Compliance with the requirement to provide a 30minute response to patients detained under section 136 of the Mental Health Act.
Percentage of patients managed as hear and treat Percentage of patients conveyed to an Emergency Department Percentage managed at scene without requirement for conveyance On-scene and call cycle times Patient experience and feedback
6. SWOT Analysis 6.1 The Table 1 outlines the SWOT analysis with regards to the management of
mental health activity within the Trust. Strengths and weaknesses have been outlined as those internal to the Trust, with external threats and opportunities then being considered. Each has been prioritised in terms of its positive or negative implications for the function, with those presenting the most significant impact rated first.
Table 1 - SWOT Analysis
Strengths Weaknesses
1. Strong commitment to meet the requirement of the Parity of Esteem
2. Mental Health lead engaged at national level
1. Triage of mental ill health presentations utilising current triage systems.
2. Lack of a multi-professional mental health workforce
Opportunities Threats
1. Significant engagement with health and social care partners
2. Political will to improve response to mental ill health 3. Engagement with MPDS and NHS England to
support clinical triage review 4. Potential for Ambulance Response Programme
mental health developments
1. Increase in activity matched against resource 2. National lack of Mental Health professionals 3. Lack of progression of national digital
programmes
7. Planned Developments
7.1 Plans for improvement are based on the continued emphasis on delivering efficiencies whilst maintaining high quality care. Where costings are not yet known, assumptions are made that reductions in resource allocation and call cycle times would be sufficient to meet the associated costs of any increase in clinical expertise.

Mental Health Strategy
Page 12 of 14
7.2 It is further assumed that developments within the clinical structure of the Clinical Hub, could be utilised alongside this Strategy to enhance the availability of mental health expertise to both support increases in hear and treat and to provide remote clinical support to maximise the delivery of the Right Care and avoidable admissions.
Developments Theme Strategic driver Proposed developments Theme 1: Development of Mental Health Pathways
Significant numbers of patients are conveyed to Emergency Departments, particularly when ambulance staff have engaged with a patient who is suffering from mental health illness, but either has a physical component requiring medical intervention, or is not under detention and therefore is unable to access a section 136 Place of Safety.
Engagement with partners in health and social care to push the case for alternatives to ED, these may include Crisis Cafes and third sector Peer Led support.
Alternatives to ED conveyance will reduce call cycle times, positively impact on handover delays and improve patient outcomes.
Theme 2: Mental Health Triage
Limitations of current triage processes via NHS Pathways (111) and MPDS (999) to effectively triage and assign clinical prioritisation. This is particularly seen with presentations including acute psychosis and behavioural disturbances. The inability to assign an appropriate clinical priority means that delivering the Parity of Esteem is complex and a significant challenge.
Work with MPDS and NHS Pathways to review current and proposed models of triage. Improved triage will enhance the Trusts ability to deliver parity and to meet the needs of patients in crisis.
Theme 3: MH support within the SWASFT within Clinical Hub
Clinical expertise available within the Clinical Hub is very limited with regards to mental health. This coupled with the triage challenges detailed in Theme 2 can lead to a high level ambulance disposition. Opportunities for the management of patients within the Clinical Hub is limited and this leads to increased dispatch and subsequent conveyance.
In addition the availability of clinical support for operational crews and difficulties gaining access to mental health teams in the community increases the likelihood of conveyance with the
Pilot to be undertaken within the 2nd quarter of 2018/19, this will investigate whether the provision of mental health professionals within the clinical hub would have a positive impact on mental health activity and patient outcomes.
Theme 4: Access to medical notes and associated Care Plans for patients known to mental health services
Operational staff may make decisions regarding patient care that may be at odds with developed escalation plans or developed care plans.
Access to care plans will provide opportunity for compliance and for appropriate care to be delivered.
Work within current digital strategy to engage with partners and with NHS Digital to enable access to health and social care records.

Mental Health Strategy
Page 13 of 14
Theme 5: National independent review of the Mental Health Act and potential for expansion of lawful powers.
Currently Paramedics have no power within the Mental Health Act and cannot therefore utilise this legislative framework to support the delivery of care to those in crisis. Increasing ambulance powers could enable earlier intervention and remove involvement of Police forces if threat to patient or others is not a consideration.
Mental Health Lead to engage with national partners to promote that the role of the ambulance service is fully considered.
Theme 6: Consideration of Specialist Paramedics in Mental Health
Currently ambulance resources are often unable to provide the clinical intervention required. It has been demonstrated in many areas that the provision of early specialist intervention significantly improves the patient experience and the appropriateness of any care pathway provided. It also enables ambulance clinician decision making to be supported and enhances the confidence of ambulance clinicians to make appropriate and sometimes difficult decisions.
Provide a comprehensive educational pathway to develop Specialist Paramedics in Mental Health to be generated.
7.3 The Strategy has been developed with the Trust’s affordable Care model in mind. The principles of affordable care are: affordable care
1. To empower managers to have the courage to make difficult decisions,
ensuring the interests of the Trust are prioritized without compromising patient safety.
2. To reduce internal regulation and promote more autonomous decision making.
3. To consider a range of perspectives when making decisions, including: the Trust’s perspective, health systems and communities.
4. To achieve a clear understanding of legislative, contractual and regulatory obligations and the impact on decision making, thereby absolving ambiguity.
5. To consider any unintended consequences before a decision is ratified. 6. To give the patient the care they need. 7. To ensure decision making is evidence based and founded on accurate data
analysis. 8. To ensure the outcome of the decision is ‘fit for purpose’. 9. The decision will generate a return on investment. 10. Work towards eliminating Trust-wide variations in practice.
8. Environmental Management
8.1 The Trust acknowledges that its activities and operations have an effect on the local, regional and global environment. To minimise the impact of this effect the Trust is committed to making continual improvements in environmental performance and preventing pollution. In making this commitment the Trust will aim to meet the requirements of current environmental regulations, laws and codes of practice as a minimum standard

Mental Health Strategy
Page 14 of 14
9. Business Continuity and Resilience
All development planned in the strategy will increase the ability of the Trust to 9.1.support the delivery of high quality care. Where enhanced services are made available all aspects of business continuity will be evaluated and associated action plans will be maintained. Where services are provided through partnership arrangements detailed continuity plans will be included within any Agreements.
10. Risk 10.1 This strategy has no detrimental effect on patients. The strategy’s risk assessment
and QEIA, its key risks, controls and actions to reduce the level of risk will be reviewed annually at Quality Risk Assurance Group (QRAG) and the Quality Committee.
11. Monitoring, Review and Governance 11.1 The Executive Medical Director is accountable for the successful delivery of the
Strategy. Quarterly monitoring will take place through the Quality Committee. 11.2 The Quality Committee will receive a quarterly update from the Executive Medical
Director through their Quality Committee reporting and will share progress and escalate issues.
11.3 This Strategy will be subject to an annual review by the Quality Committee and it is
the responsibility of the Board to approve the strategy and any amendments to it. 12. Associated Documentation 12.1 The following internal and external documentation is listed below:
Mental Health Act 1983 https://www.legislation.gov.uk/ukpga/1983/20/contents Mental Capacity Act https://www.legislation.gov.uk/ukpga/2005/9/contents Policing and Crime Act http://www.legislation.gov.uk/ukpga/2017/3/contents/enacted Crisis Care Concordat https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/281242/36353_Mental_Health_Crisis_accessible.pdf Five Year Forward View for Mental Health https://www.england.nhs.uk/wp-content/uploads/2016/02/Mental-Health-Taskforce-FYFV-final.pdf SWASFT Mental Health and Mental Capacity Clinical Guideline http://intranet.swast.nhs.uk/SWASFT%20instructions/SWASFT%20clinical%20guidelines/CG28_MentalHealthandMentalCapacity.pdf

Trust Public Board of Directors Meeting – 25 May 2018 Page 1 of 9
Trust Public Board of Directors Date: 25 May 2018
Paper Title: Annual Health & Safety Report
Prepared by: Anne Payne, Health, Safety and Security Manager
Presented by: Jenny Winslade, Executive Director for Nursing and Quality
Action: Assurance
Recommendation:
The Trust Board of Directors is asked to take assurance from the information and actions included in this report.
Executive Summary:
The Health and Safety at Work etc. Act 1974 provides a legislative framework to promote, stimulate and encourage high standards of health and safety at work. The legislation is enforced by the Health and Safety Executive (HSE). This report is to provide the Trust Board of Directors with an over view of health and safety compliance as reported during 1 April 2017 to 31 March 2018. This report looks at the year 2017/18 of positive progress for the Trust with regards to management of Health & Safety. It captures achievements and performance during this period of time and how reporting of incidents has been used to help make SWAST a safer place for its staff and patients. The approach of identifying gaps and risks associated with any of the Health & Safety regulations benefits the Trust in gaining a wider picture of Health & Safety compliance. This is reflected in the diversity of our activities, which include: actively reviewing incidents that affect staff whilst at work providing training to staff to ensure they have an understanding of
their responsibilities within health and safety including manual handling, Fire, DSE etc.
carrying out Workplace Inspections, Fire Risk Assessments and Security Checks with Estates and Unison to ensure the Trust’s premises are fit for use and secure and monitor the completion of actions identified.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 9
working closely with Health & Safety representatives across the Trust. monitoring HSE enforcement actions and notices ensuring that they
are shared with the relevant departments across the Trust for learning working closely with local managers to complete Site Specific Risk
Assessment and monitor the completion of actions

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 9
Annual Health and Safety Report 1. Overview of Health and Safety Performance 1.1 This report focuses on exceptional performance. The three reporting categories assigned to
individual performance metrics contained within this report are as follows:
Performance is in Line with Plan Early Warning Escalated Performance Issue
Table 1 – Performance Exception Overview in the Reporting period
Fire Warden Training – Five training days have been identified and been completed for the
year 2017/18 – 63 staff trained COSHH training – Has reached and exceeded the target for the year 2017/18 Risk Assessment (F2F) Training – Training takes places monthly Injuries to staff during 2017/18 – has decreased compared with the same period from 1 April
to 31March 2017 from 641 incidents to 631 incidents reported. Injuries to patients - has decreased compared with the same period from 1 April to 31March
2017 from 135 incidents to 105 incidents reported. Fire Risk Assessments –Fire Risk Assessments have been completed on all 162 premises
used by SWAST due 2017/18 Workplace Inspections Assessments - Workplace Inspection Assessments have been
completed on all 162 premises used by SWAST due 2017/18 Security Checklists - Security Checklists have been completed on all 162 premises used by
SWAST due 2017/18 Reporting of patient injury incidents to the HSE under RIDDOR has risen from 1 incident
during 2016/17 to 8 during 2017/18. The HSE notify the CQC directly of these incidents Reporting of incidents to the HSE under RIDDOR within the timescale is currently at 97% Risk Management training - Completion percentage for the rolling year is 65% 1256 DSE Assessments completed for the last 24 months however there are still a number
outstanding – email reminder was circulated to staff using DSE in December and a bulleting article circulated in March 2018
Mandatory Fire training – Completion percentage for 2017/18 is 86% - as this training is mandatory all staff should have completed it in order to achieve 100%. Bulletin article was issued during January 2018 and again in March 2018 to remind staff to complete training.
Handle with Care training - Completion percentage for 2017/18 is 70% - as this training is mandatory all staff should have completed it in order to achieve 100%. Bulletin article was issued during January 2018 and again in March 2018 to remind staff to complete training.
Patient Handling training - Completion percentage for 2017/18 is 77%. Bulletin article was issued during January 2018 and again in March 2018 to remind staff to complete training.
Slips, Trips and Falls incidents – have increase compared with 2016/17 from 132 incidents to 147 incidents reported – this was due to the severe weather conditions
.No areas to report

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 4 of 9
2. Objective 1 - Increase staff involvement in health and safety by providing them with guidance, training and development to enable them to understand their responsibilities, participate in risk assessments, reporting and investigating accidents and incidents; encouraging a strong sense of responsibility and ownership and the development of a health and safety culture.
2.1 Within the Trust there are a number of training packages provided by the Health, Safety and
Security Department. There is availability for ad hoc health and safety training on request and guidance and advice where required.
2.2 The on-line Fire Training (Table 2 in the appendix) is classed as mandatory and therefore all
staff must complete it annually. Regular bulletins are circulated to staff and Area Coordinators are responsible to ensuring staff complete this training. Fire Safety is also included within the Mandatory Workbook.
2.3 There are four further training packages available to staff within the Fire e-learning portal
which includes Handle with Care, Patient Handling, Risk Management and Asbestos Awareness. (Tables 3, 4, 5 and 6 in the appendix).
2.4 Manual Handling training is provided in various forms to staff including the Mandatory
Workbook, online training and face to face training. Learning Development Officers (LDO) carry out annual observations of front line staff whilst utilizing manual handling equipment during patient care, they can then provide real time interventions where concerns are identified. The manual handling assessment carried out by the LDO includes: Kinematics Avoidance of task Correct use of equipment Risk assessment
2.5 There are several other types of training available for staff to access including COSHH
(Table 7) and Risk Assessment Training (Table 8). The Health and Safety Department are advised of any concerns relating to access and completion of the training provided on the ATF Portal.
2.6 Currently the Trust has 138 trained Fire Wardens based at Trust Headquarters, St Leonard’s, St James A and other key sites such as Vehicle Maintenance Units. During the period 1 April 2017 to 31 March 2018 63 staff received Fire Warden training.
2.7 10 licenses for the IOSH Managing Safely course have been procured and assigned to
Operations Manager, Operations Officer and other key Managers during February 2018. Currently 1 member of staff has completed the IOSH Managing Safely successfully whilst the other 9 staff are making progress through the course.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 5 of 9
3. Objectives 2 and 3 3.1 Reduce work related ill-health by developing and maintaining standards around safety
resulting in the identification and implementation of prevention methods. 3.2 To provide a safe working environment without risks to health by complying with all
appropriate health and safety standards. 3.3 Display Screen Equipment (DSE)
3.3.1 Due to the nature of the work carried out by the Trust there is a high proportion of staff that
use DSE during their working day. When a member of staff uses DSE for a significant part of their working day they must complete a DSE assessment. This assessment allows the Trust to identify any issues which relate to the DSE or workstation assessments including chairs. Those staff who use DSE must complete a DSE assessment every two years or when there are significant changes to their workstation (Table 9). The DSE Assessment is available for all staff to access via the intranet. Posters have been displayed at St James A and THQ advising staff how to set up their workstations correctly. This information is also available on the intranet for staff at stations.
3.3.2 All of the Hot Desks available at St James A have been assessed by a Health Safety and
Security Officer and this process will be rolled out at Trust Headquarters and St Leonard’s. 3.3.3 Regular bulletin articles are issued together with posters to assist staff to complete their
DSE assessments. The Trust has 25 DSE Assessors based at key locations 3.4 Fire Risk Assessments 3.4.1 During period 1 April 2017 to 31 March 2018, all 162 stations/premises have been assessed
and the Fire Risk Assessments have been reviewed and updated (Table 10). Fire Evacuation Plans are being developed and issued to larger stations where there are staff on site for the majority of their working day such as Derriford, Taunton, and Bristol etc.
3.4.2 An Approved Fire Engineer has been appointed and he was impressed with the level of fire
safety within the Trust and noted that the Fire Safety and Prevention Policy produced by the Health, Safety and Security Team was the best he had seen.
3.5 Workplace Inspections 3.5.1 Action WP1 on the Health and Safety Improvement Plan related to the joint workplace
inspection program involving representatives from Estates, Infection Control, Unison, Health and Safety as well as the Operations Officer for the station. During period 1 April 2017 to 31 March 2018, all 162 stations/premises have received a Workplace Inspection (Table 11).

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 6 of 9
3.5.2 An audit of the actions identified following the completion of the workplace inspections has identified the following:
87.6% of the actions identified have been reported to Estates to complete. 11.99 % of the actions identified have been passed to the Local Operations Officer to
complete. 0.5% of the actions identified related to the Health, Safety and Security Department
to complete.
3.5.3 All outstanding actions are now being reviewed and updated after 3 months following the inspection to ensure they are completed. Where the actions have not been completed additional support and guidance is being provided by the Health, Safety and Security Team to assist in the completion of the action.
3.5.4 Following a Workplace Inspection each station/premise receives a compliance score. For the Workplaces Inspections completed: 22% of stations/premises receive a gold compliance score 52% of stations/premises receive a silver compliance score 25.5% of stations/premises receive a bronze compliance score 0.5% of stations/premises receive a red compliance score. Additional advice and
guidance has been provided to assist low scoring stations and premises to improve. 4. Objectives 4 and 5 4.1 Develop a proportionate health and safety system to allow for the simplification of the
management of risks encouraging a greater ownership of health and safety, enabling the formation of a positive health and safety culture across the organization.
4.2 To develop coherent policies and procedures - make sure internal policies, procedures,
guidance and advice are simplifies and understood and are easily accessible to all staff, and where appropriate, patients, visitors and contractors.
4.3 During 1 April 2017 to 31 March 2018 the Health, Safety and Security Department processed 1906 Datix reports. This compares to 1829 Datix reports for the same period during 2016/17 – an increase of 77 Datix reports. Table 12 shows the number of injuries sustained by staff during the period 1 April 2017 to 31 March 2018.
Incident by Type 1 April 2016 to
31 March 2017 1 April 2017 to 31 March 2018
Patient Injuries/Incidents 135 105 Staff Accidents 641 631 Security Incidents 101 121 Abuse of staff 952 1049 Total 1829 1906

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 7 of 9
4.4 The following table shows a breakdown of staff accidents by type.
Injury incident by Detail 1 April 2016 to
31 March 2017 1 April 2017 to 31 March 2018
Accidents in the course of moving patients 205 214 Slips, trips, falls and collisions 132 147 Accident caused by some other means 141 95 Needle stick injury or other incident connected with Sharps 76 74
Injury caused by physical or mental strain 26 41 Lifting accidents 38 19 Exposure to electricity, hazardous substance, infection etc. 23 41
Total 641 631 4.5 The highest injury to staff category was ’Accident in the course of moving patients’ with 214
Datix reports in the period compared with 205 Datix reports for the same period during 2016/17 – an increase of 9 Datix reports. Table 13 show the number of injuries sustained by staff from Patient Handling incidents during the period 1 April 2017 to 31 March 2018.
4.6 A review of the injuries sustained by staff from manual and patient handling has taken place
for the period 1 April 2017 to 31 March 2018. Out of 214 Datix reports received only 12 staff have reported two or more incidents. This information has been referred relevant Investigator in order for these staff to receive additional manual handling training.
4.7 The second highest injury to staff category was ‘Slips, trips, falls and collisions’ with 147
Datix reports in the period compared with 132 Datix reports for the same period during 2016/17 – an increase of 15 Datix reports. There was an increase in injuries during February and March 2018 due to the severe weather conditions. Table 14 show the number of injuries sustained by staff from Patient Handling incidents reported during 2017/18 compared with the same period in 2016/17.
4.8 The third highest category was ‘Accident caused by other means’ with 95 Datix reports
received in the period compared with 141 Datix reports for the same period during 2016/17 – a decrease of 46 Datix reports.
4.9 RIDDOR 4.9.1 Of the 1906 Datix reports received, 123 injuries were reported to the HSE under
RIDDOR. This compares to 95 injury incidents for the same period during 2016/17– an increase of 28 RIDDOR reports.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 8 of 9
Injury incident by Detail 1 April 2016 to 31 March 2017
1 April 2017 to 31 March 2018
Staff Patients Staff Patients Slips, trips, falls and collisions 18 0 44 2 Lifting accidents 9 0 6 0 Accidents in the course of moving patients 39 1 42 5 Abuse of staff by patients 5 0 1 0 Accident caused by some other means 14 0 13 1 Needle stick injury 1 0 1 0 Injury caused by physical or mental strain 6 0 8 0 Exposure to electricity, hazardous substances, infection etc. 2 0 0 0
Total 94 1 115 8 4.9.2 Under RIDDOR, 123 incidents (97%) were reported to the HSE within the 15 day timescale
(Table 16). 3 incidents were not reported within the timescale, this was due to late reporting of an injury incident by a member of staff and information was not received regarding an injury to a patient until after the 15 day period.
4.9.3 The Trust is also required to report Dangerous Occurrences and Occupational Diseases to
the HSE under RIDDOR. During period 1 April 2017 to 31 March 2018 the Trust were not required to report any incidents of Dangerous Occurrences and Occupational Diseases to the HSE under RIDDOR.
4.9.4 Of the 123 injuries reported to the HSE under RIDDOR, 8 related to injuries to patients whist
in our care. RIDDOR 2013 states “Accidents to members of the public or others i.e. patients who are not at work must be reported if they result in an injury and the person is taken directly from the scene of the accident to hospital for treatment to that injury. Examinations and diagnostic tests do not constitute ‘treatment’ in such circumstances. There is no need to report incidents where people are taken to hospital purely as a precaution when no injury is apparent”.
4.9.5 It is noted that there is a memorandum of Understanding between the HSE, Local Authorities and the CQC and therefore once a report has been submitted to the HSE under RIDDOR this is automatically forwarded on the CQC for their information.
4.9.6 On reviewing the Datix reports submitted during 1 April 2017 to 31 March 2018, Table 17 shows the number of Datix reports which resulted in an injury to staff where the member of staff took sick leave in comparison to the number of Datix reports received where no sick leave was taken.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 9 of 9
5. HSE Inspection and Visit 5.1 Following the HSE Inspection in March 2016, an Improvement Plan was developed from the
actions identified during the visit. This Improvement Plan was completed in December 2017.
5.2 In January 2018 Alan Craddock Head of Public Services, HSE visited the Trust and met
with the Trust Board of Directors to discuss how the Trust manages musculoskeletal injuries which is a key priority with the HSE for 2018/19.
5.3 The Trust was able to demonstrate that it is proactive and that it is keen to benchmark
incidents with other Ambulance Trusts and also to carry out peer reviews on the health and safety management system.
5.4 Overall it was felt that the meeting was a success and now awaiting feedback at the
National Ambulance Risk and Safety Forum in May 2018 which the HSE attend. 6. Recommendation 6.1 The Trust Board of Directors is asked to take assurance from the information and actions
included in this report. Anne Payne Health, Safety and Security Manager

Appendix A Table 2 The aim of this training is to ensure staff are aware what to do in the event of a fire. There is a requirement under the Regulatory Reform Order 2005 to provide all staff with fire safety training and not doing so could lead to prosecution. This training should be completed on induction to the Trust and annually. All staff must complete the training; fire safety is also included within the Mandatory Workbook. Table 2 below shows the number of staff who have completed the training for the period 1 April 2017 to 31 March 2018.
Table 3 and 4 Tables 3 and 4 shows the number of staff who have completed the Handle with Care and Patient Handling training for the period 1 April 2017 to 31 March 2018.
754 278 262 271 261 205 258 240 287 209 166 237
754 1,032 1,294 1,565 1,826 2,031 2,289 2,529 2,816 3,025 3,191 3,428
0
1,000
2,000
3,000
4,000
5,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 2 Total Number of Staff Completing Fire Training between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18 Total number of staff
580 272 199 185 156 179 199 150 198 268 150 233 580 852 1,051 1,236 1,392 1,571 1,770 1,920 2,118 2,386 2,536 2,769
0
1,000
2,000
3,000
4,000
5,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 3 - Total Number of Staff Completing Manual Handling Training between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18 Total number of staff

Only Front Line staff are expected to complete this training i.e. those staff who may have to assist, lift or transfer patients. Tables 5 and 6 Tables 5 and 6 show the number of staff who have completed training in the areas listed below for the period of time 1 April 2017 to 31 March 2018. Only certain staff are encouraged to complete this training such as Operation Managers, Operation Officers, Key Managers, Estates, IT and Fleet.
426 190 141 145 132 111 134 135 145 125 96 136
426 616 757 902 1,034 1,145 1,279 1,414 1,559 1,684 1,780 1,916
0
500
1,000
1,500
2,000
2,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 4 - Total Number of Front Line Staff Completing Patient Handling Training between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18 No of Front Line staff
75 27 9 20 21 18 22 33 31 8 6
46 75 102 111 131 152 170 192 225 256 264 270 316
0
100
200
300
400
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 5 - Total Number of Key Staff Completing Risk Management Training between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18

Only 800 licences are available for the Asbestos and Risk Management Training and therefore only key staff to have access to this training - it is not open to all staff. The key staff include: Operation Managers, Operation Officers, Key Managers, Estates, IT Fleet Health, Safety and Security Table 7 Table 7 - Control of Substances Hazardous to Health (COSHH) – this training is aimed at those staff who regularly works with chemicals such as the Make Ready Team and Fleet. This training is expected to be completed on an annual basis. However this training is available to all staff who wish to complete it as it is ready available on the intranet under Health, Safety and Security.
104 36 13 36
173
25 42 25 43 9 8 15 104 140 153 189 362 387 429 454 497 506 514 529
0
100
200
300
400
500
600
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 6 - Total Number of Key Staff Completing Asbestos Awareness Training between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18
16 29 12 17 13 7 10 12 21 12 12 18 16
45 57 74 87 94 104 116
137 149 161 179
0
50
100
150
200
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 7 - Total Number of Staff Completing the COSHH Training between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18

Table 8 Table 8 - The Health Safety and Security Department offer risk assessment courses to those staff who are expected to carry out risk assessments within their role. This was initially started to assist the Fleet Department to carry out risk assessments however other departments have requested this training for their teams including Make Ready, Estates, Unison Representations, Emergency Care Assistants and Operations Officers.
Table 9 Table 9 show the number of staff who have completed and submitted their DSE assessment to the Health and Safety Department for the period 1 April 2017 to 31 March 2018. Staff need to complete their DSE Assessment every two years or if there are significant changes to their workstation.
0 0 14 15 10 15 12 15 15 12 14 13
0 0 14
29 39 54
66 81
96 108
122 135
0
50
100
150
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 8 - Total Number of Risk Assessment Training (F2F) completed between 1 April 2017 and 31 March 2018
In Month 2017/18 YTD 2017/18
31 34 169
99 66 60 59 64 63 56 90 59 45 15 26 18 34 32 42 46 39 60 49 30 31
65
234 33
3 399 45
9 518 58
2 645 70
1 791 85
0 895
910
936
954
988
1020
1062
1108
1147
1207
1256
1286
0
200
400
600
800
1000
1200
1400
Table 9 - DSE Assessments completed in last 24 months
In Month YTD 2017/18

To identify Staff who use display screen equipment and should complete this assessment every two years should satisfy the following criteria from the HSE Regulation: normally use DSE for continuous or near-continuous spells of an hour or more at a
time; and use DSE in this way more or less daily; and have to transfer information quickly to or from the DSE; and also need to apply high levels of attention and concentration; or are highly dependent on DSE or have little choice about using it; or need special training or skills to use the DSE. The regulations don’t apply to workers who use DSE infrequently or only use it for a short time. Staff who should complete a DSE Assessment include: All Clinical and 111 Hub Staff All office based staff Those staff in a management position And those staff who fulfil the criteria of the regulations Table 10 and 11
15 30
46 62
76 90
105 120 132 141 153 162
0
50
100
150
200
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 10 - Number of Fire Risk Assessments completed for Trust Premises during 1 April 2017 and 31 March 2018 - 162 Premises in Total
Year to Date Year End Target

Table 12 Table 12 show the number of injuries Datix reports submitted reported by staff during the period 1 April 2017 to 31 March 2018 in comparison with the same period during 2016/17. Please note this does include injuries from Physical Assaults.
Table 13 Table 13 show the number of injuries sustained by staff from Lifting and Moving and Handling incidents during the period 1 April 2017 to 31 March 2018 in comparison with the same period during 2016/17. It has been noted that of the 233 Datix reports received,
233 incidents involved A&E staff,
15 30
46 62
76 90
105 120
132 141 153 162
0
50
100
150
200
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 11 - Number of Workplace Assessments completed for Trust Premises during 1 April 2017 and 31 March 2018 - 162 Premises in Total
Year to Date Year End Target
41 49 45 50 51 56 54 59 56 55 57 58 41
90 135
185 236
292 346
405 461
516 573
631
69 112
170 240
304 366
410 471
520 562
602 641
0
100
200
300
400
500
600
700
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 12 - Staff - Number of Injuries During Course of Work
In Month 2017/18 YTD 2017/18 YTD 2016/17

And 209 of the incidents occurred at either patient’s homes or at other public premises/places. 16 incidents occurred in the rear of the ambulance whilst in transit. 8 incidents occurred on Trust premises.
Table 14 The second highest category was ‘Slip Trips and Falls’ with 147 Datix reports received in the period compared with 132 Datix reports for the same period during 2016/17 – an increase of 15 Datix reports. Table 14 show the number of injuries sustained by staff from Slips, Trips and Falls incidents during the period 1 April 2017 to 31 March 2018 in comparison with the same period during 2016/17.
19 19 21 18 15 15 20 16 19 21 27 23 19
38 59
77 92
107 127
143 162
183
210 223
20 40
65 90
113 135
149 169
189 205
224 243
0
50
100
150
200
250
300
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 13 - Injuries to Staff during Manual and Patient Handling Activities
In Month 2017/18 YTD 2017/18 YTD 2016/17
7 7 10 10 14 13 16 16 17 14 12 11 7 14
24 34
48 61
77 93
110 124
136 147
12 20
35 52
62 72
84 100
108 116
124 132
0
20
40
60
80
100
120
140
160
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 14 - Staff - Slips, Trips and Fall Injuries Whilst at Work
In Month 2017/18 YTD 2017/18 YTD 2016/17

It has been noted that of the 147 Datix reports received;
135 incidents involved A&E staff, 7 incidents involved Control (999) staff 2 incidents involved Support staff 3 incident involved UCS (111) Staff
and 92 of the incidents occurred at either patient’s homes or at other public
premises/places. 23 incidents occurred during transit 32 incidents occurred on Trust premises.
On reviewing the Datix reports submitted in detail;
45 Incidents occurred whilst colliding with an object 16 incidents occurred due to some other reason 15 incidents occurred due to a fall from height 24 incidents occurred due to fall on level ground 16 incidents occurred when tripping over an object 16 incidents occurred due to slipping on a wet surface 8 incidents occurred due to slipping on a vehicle ramp 7 incidents occurred due to ice and snow
Table 15 Where the injury reported does not fit into any other category it is coded under ‘Accident caused by other means’ and includes injuries such as: Road Traffic Collisions Dog Bites Flea Bites Scolding Finger/hand traps
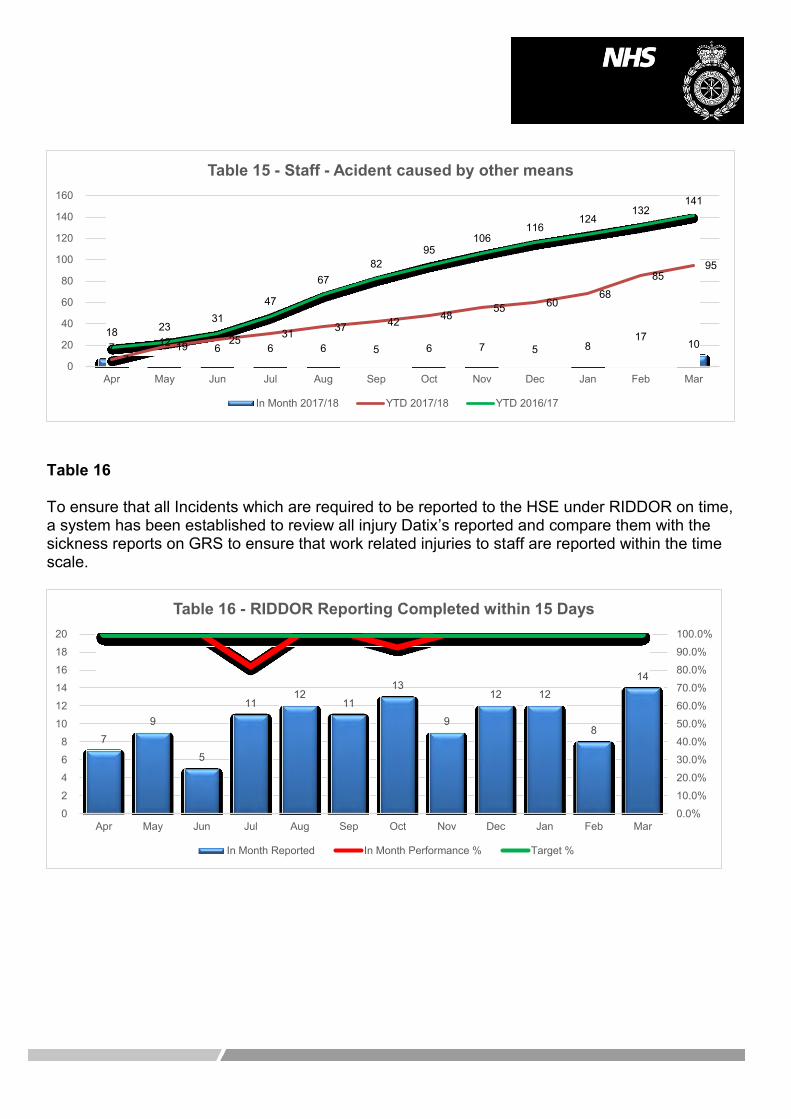
Table 16 To ensure that all Incidents which are required to be reported to the HSE under RIDDOR on time, a system has been established to review all injury Datix’s reported and compare them with the sickness reports on GRS to ensure that work related injuries to staff are reported within the time scale.
7 12 6 6 6 5 6 7 5 8 17
10 7
19 25 31 37 42 48 55 60
68
85 95
18 23 31
47
67 82
95 106
116 124
132 141
0
20
40
60
80
100
120
140
160
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 15 - Staff - Acident caused by other means
In Month 2017/18 YTD 2017/18 YTD 2016/17
7
9
5
11 12
11
13
9
12 12
8
14
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
0
2
4
6
8
10
12
14
16
18
20
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 16 - RIDDOR Reporting Completed within 15 Days
In Month Reported In Month Performance % Target %

Table 17 Of the 115 staff who were involved in incidents and sustained injuries which were reported to the HSE under RIDDOR, the sickness equates to 4596 days lost, 2,369 working days lost to the Trust.
429
840 986
1,608 1,889
2,309 2,531
2,800
3,428
3,894 4,248
4,596
215 450 527 835 962 1,162 1,279 1,416
1,748 1,989 2,191 2,369
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
5,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 17 - Days Lost to RIDDOR Reportable Accidents/Injuries
YTD Days Lost 2017/18 YTD Working Days Lost 2017/18

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 9
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Annual Security, Violence and Aggression Report
Prepared by: Anne Payne, Health, Safety and Security Manager / LSMS
Presented by: Jennie Kingston, Deputy Chief Executive and Executive Director of Finance
Action: Assurance
Recommendation: The Trust Board of Directors is asked to take assurance from this report.
Executive Summary:
The Health and Safety at Work etc. Act 1974 provides a legislative framework to promote, stimulate and encourage high standards of health and safety at work. The legislation is enforced by the Health and Safety Executive (HSE) and NHS Directions 2004 This report is to provide the Trust Board of Directors with an update of all security issues affecting staff and the Trust during 2017/18. This includes violence and aggression, theft and criminal damage. Over the last 12 months staff have reported 1049 datix reports relating to violence and aggression – an increase of 97 reports for the same period in 2016/17. Datix reports received relating to physical assaults on staff has increase by 8% from 2016/17 however only 9 staff were required to take sickness and only one incident where a member of staff went sick was reported to the HSE under RIDDOR. Datix reports received relating to verbal abuse incident by patients has also increased by 20% however incidents of verbal abuse by members of the public and relatives of the patient have reduced by 24%. Of the 52 incidents reported to the police following a physical assault, 1 perpetrator received a 16 week prison sentence. There has been a 63% increase of information report to the Trust by staff regarding violent patients. This information has been passed to the Trust by other agencies.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 9
Annual Security, Violence and Aggression Report 1. Introduction 1.1 All employers have a duty ‘so far as reasonably practical’ to protect the health, safety and
welfare of staff under the Health and Safety at Work etc. Act 1974.
1.2 The manifestation of violence and aggression depends on a combination of factors, such as the consumption of alcohol and drugs, personality characteristics, medical/mental health conditions, attitudes and behaviours and not just from patients. The physical setting and any restrictions that limit the patient’s freedom can also have an adverse effect on the patient causing the impact of violence and aggression to be significant and diverse.
1.3 Absolute avoidance of violence is impossible and unachievable due to the nature of the
work carried out by the Trust and therefore training and guidance is needed to prevent minor violence from escalating into severe violence.
2. Violence and Aggression 2.1 During the period 1 April 2017 to 31 March 2018 the Health, Safety and Security
Department processed 1049 Datix reports which related to abuse of staff. This compares to 952 Datix reports for the same period during 2016/17 – an increase of 97 Datix reports.
Incident by Adverse Event
1 April 2016 - 31 March 2017
1 April 2017 - 31 March 2018
Challenging Aggressive Behaviour 219 185 Verbal Abuse – Patient Verbal Abuse – Member of public, relative, other
318 91
382 69
Physical Assaults 152 165 Information received about abusive patients – not witnessed by staff 127 207
Attempted Assaults – No Injury 45 41 Total 952 1049
2.2 Of the 1049 reports received during the period 1 April 2017 to 31 March 2018 where staff
were subjected to violence and aggression (not including ‘Information received about abusive patients’), 840 were affected. Ethnicity of the staff affected is not readily available on ERS without either a NHS or Staff ID Number however this is partly recorded on Datix:
01 White – British = 381 03 White – other White = 34 17 Not Stated = 425

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 9
2.3 Of the 840 staff affected by the violence and aggression during the period 1 April 2017 to 31 March 2018 524 were males and 316 were females. Table 1 in the Appendix show a breakdown in front line staff attendance including the 111 and 999 hubs.
2.4 ‘Information received about abusive patients – not witnessed by staff’ relates to information
provided to the crews from hospitals, GPs, Police and other agencies. This is reported to the Trust in order for a warning marker to be assigned to the address following a checking process with those agencies to ensure the information is up-to-date and correct.
3. Physical Assaults 3.1 Of the 1049 abuse reports received during the period 1 April 2017 to 31 March 2018, 165
reports related to 185 staff who were subjected to a physical assault by a patient. This compares to 152 Datix reports relating to 175 staff who were subjected to a physical assault for the same period during 2016/17 - an increase of 13 Datix reports (Table 2).
3.2 Of the 185 staff who sustained an injury, 9 staff were required to take sick leave (32 days
lost – 17 working days lost to the Trust). 1 incident was reported to the HSE under RIDDOR. Of the other 176 staff who received an injury it would appear that these injuries were of a minor nature however this does not demean the impact these types of events have on staff.
3.3 Of the 165 reports, 110 incidents were reported to the police service. Of the 110 incidents reported, in 58 of the incidents the member of staff involved did not want to take any further action against the perpetrator. Of the other 55 incidents reported, these were only reported to the Trust for information purposes only.
3.4 Actions taken in the 52 incidents reported to the police service:
1 perpetrator receive a 16 week imprisonment sentence 13 perpetrators received a police caution 8 perpetrators were asked to participate in the Restorative Justice Scheme/Impact
meeting with Assailant. 11 perpetrators were detained under Section 136 Mental Health Act 8 incidents are still being investigated by the police service or due to go to court in the
next couple of months. 3 perpetrator was charged with Section 5 Public Order Act 1 perpetrator was found guilty at court and received a Conditional Discharge -
Compensation of £100 to the victims 1 perpetrator was found guilty at court for assault by beating and ordered to attend
Alcohol and Substances abuse program and pay the victim £50 compensation 1 perpetrator was found guilty at court, fined £440, £44 victim surcharge and £160
costs. 1 perpetrator pleaded guilty at court for assault by beating. Fined £120. Compensation
of £50. Surcharge of £30. 1 perpetrator received a 12-month community order, with Rehabilitation Activity
Requirement and ordered to pay £150 compensation
Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 4 of 9
1 perpetrator was found guilty at court, fined £400, £64 victim surcharge and £160 costs.
1 perpetrator pleaded guilty at court for assault by beating. Fined £120. Compensation of £50.
1 perpetrator was sent to prison for 16 weeks
3.5 Of the 165 reports received it has been identified that 101 perpetrators were male and 64 perpetrators were female. A review of the detail of each incident has identified that:
70 incidents were alcohol related. 44 incidents related to a mental health condition 22 incidents were drug related. 21 Incidents related to a medical condition 6 incidents were alcohol/drugs related. 2 Incidents involved patients with dementia
4. Verbal Abuse 4.1 Of the 1049 abuse reports received during the period 1 April 2017 to 31 March 2018, 451
related to verbal abuse towards staff – 382 involved patients and 69 involved members of the public, relatives etc. This compares to 409 Datix reports for the same period during 2016/17 - an increase of 42 Datix reports (Table 3).
4.2 On reviewing the Datix reports submitted to the Trust during 1 April 2017 to 31 March 2018
it was noted that the police services were not notified in the majority of the verbal abuse incidents to staff. On questioning staff as to why incidents are not reported to the police, their responses have been that:
It is part of the job The Police are not interested in minor crime The Police take too long to attend It is quicker to report to the Trust and get a warning marker assigned to the address and
for a letter to be sent out to the person. Some patients don’t realise they are swearing at staff.
Table 4 show a breakdown in report of verbal abuse incidents by OM area. . 5. Warning Markers 5.1 During the period 1 April 2017 to 31 March 2018, 801 warning markers have been assigned
to patient’s home addresses following violence and aggression incidents. NHS England for Devon, Cornwall and Bristol has provided information on 52 patients who have been violent and aggressive towards NHS Staff.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 5 of 9
5.2 Currently the Trust has 1084 warning markers assigned to addresses and these consist of:
1033 Cautionary Approach Advised warning markers 45 Police Attendance Advised warning markers 6 Police Attendance Mandatory warning markers
5.3 Currently only NHS England for Devon, Cornwall and Bristol provide information on patients
who have been violent and aggressive towards NHS Staff. The Health, Safety and Security manager has attended meeting with NHS England for Dorset to arrange a sharing protocol for information. Currently Acute Hospitals also have warning markers on patients however this is not shared with other agencies.
5.4 Tables 5 and 5a show that there is an increase in the number of warning markers assigned to addresses since April 2016.
6. Security 6.1 During the period 1 April 2017 to 31 March 2018 the Health, Safety and Security
Department processed 121 Datix reports which related to security. This compares to 101 Datix reports for the same period during 2016/17 – an increase of 20 Datix reports.
Incident by Adverse Event
1 April 2016 - 31 March 2017
1 April 2017 - 31 March 2018
Other breach of security or public order 7 15 Intruders, Break-ins, Trespassers, Intruder alarms 8 13 Other incident related to Security 32 52 Loss/damage of staff personal property 2 8 Proven, alleged or suspected theft 38 16 Damage caused by vandalism (other than ARSON) 13 7 Accidental or malicious use of an Alarm System 1 1 Fire - Accidental 0 1 Breach of confidentiality of staff records or information 0 6 Breach of patient confidentiality 0 1 Damage to patient's property 0 1 Total 101 121
6.2 It has been identified that uniform and equipment belonging to the Trust has been found for
sale on social media sites such as eBay, Facebook and shpock. Attempts are made to stop the sales, the uniform and equipment is returned to the Trust. In the last 12 months £7,500 worth of uniform and equipment has been returned to the Trust.
6.3 A bulletin article has been issued to remind staff to return uniform and equipment when no
longer required. Staff have also been informed that it is classed as theft and the Trust will take action against them.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 6 of 9
7. Recommendations 7.1 The Trust Board of Directors is asked to take assurance from the information included in
this report. Anne Payne Health, Safety and Security Manager / LSMS

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 7 of 9
Appendix Table 1
Table 2
Table 3
4 34 137
340
183 117
25 0
100200300400
111 999 All female crew All male crew Mixed crew Single maleresponse
Single femaleresponse
Table 1 - Front Line Staff Affected by Violence and Aggression
Staff Group
14 22 33 42 54 64 77 91 104 117 130 138 7 19 34 47
58 72
85 92 107
123 135
152
19 27 46
70 86
101 117
129 141 147
157 164
020406080
100120140160180
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 2 - DATIX - Physical Assaults on Staff
YTD 2015/16 YTD 2016/17 YTD 2017/18
20 42 69 98 122 144 172 209 237 276 297 349 31 57 81 121 145
180 223
266 304
343 370
408
42 79
126 170
218 264
296 338
370 399
426 451
050
100150200250300350400450500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 3 - DATIX - Verbal Abuse towards Staff
YTD 2015/16 YTD 2016/17 YTD 2017/18
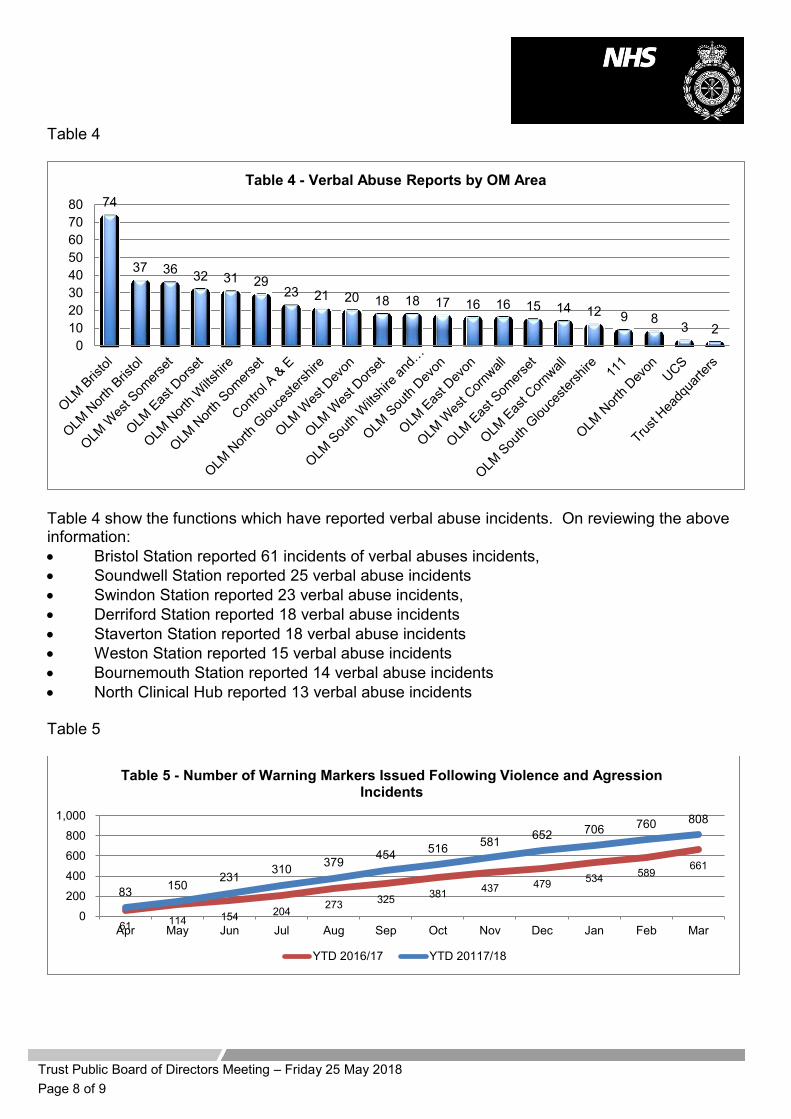
Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 8 of 9
Table 4
Table 4 show the functions which have reported verbal abuse incidents. On reviewing the above information: Bristol Station reported 61 incidents of verbal abuses incidents, Soundwell Station reported 25 verbal abuse incidents Swindon Station reported 23 verbal abuse incidents, Derriford Station reported 18 verbal abuse incidents Staverton Station reported 18 verbal abuse incidents Weston Station reported 15 verbal abuse incidents Bournemouth Station reported 14 verbal abuse incidents North Clinical Hub reported 13 verbal abuse incidents
Table 5
74
37 36 32 31 29 23 21 20 18 18 17 16 16 15 14 12 9 8
3 2 0
1020304050607080
Table 4 - Verbal Abuse Reports by OM Area
61 114 154 204 273 325 381 437 479 534 589 661
83 150 231 310 379 454 516 581 652 706 760 808
0
200
400
600
800
1,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Table 5 - Number of Warning Markers Issued Following Violence and Agression Incidents
YTD 2016/17 YTD 20117/18

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 9 of 9
Table 5a
971 966 928 891
749 736 737 698 740 751 761 819 835 885 916 960 971 984 1009 1024 1050 1048
1116 1033
54 53 52 51 50 49 51 44 44 38 35 35 35 35 34 39 39 48 50 51 49 51 50 45
4 4 4 4 4 4 4 4 4 6 6 6 6 6 6 5 5 5 5 6 6 7 7 6 0
200
400
600
800
1,000
1,200
Table 5a - No of Warning Markers in place since April 2016
Cautionary Approach Advised Police Attendance Advised Police Attendance Mandatory

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 1
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: People and Culture Three Year Strategy (2018-2021)
Prepared by: Amy Beet, Executive Director of People and Culture
Presented by: Amy Beet, Executive Director of People and Culture
Action: Approval
Recommendation: The Trust Board of Directors is asked to approve the People and Culture 3 year Enabling Strategy
Executive Summary:
The People and Culture Strategy three year strategy was completed in draft and first presented in 2017. In the intervening period it has been widely shared and consulted upon allowing revisions and amendments to be incorporated including those arising from the recently ratified Corporate strategy, ensuring this enabling strategy fully aligns and supports delivery of the Trusts strategy. It is now presented to the Board for final ratification.

People and Culture Three-Year Strategy (2018-2021)
Contents
Flowchart Page 2 Executive Summary Page 3 Introduction Page 4 Objectives of the People and Culture Strategy Page 4 Strategic Intentions Page 5 Scope and Context Page 6 Delivering our Objectives Page 7 Right People Page 8-10 Right Values Page 11-12 Right Skills Page 13-14 Delivering the Strategy through the HR and OD Directorate Page 15 Governance Framework Review and Monitoring Page 16
1

Flowchart
Right Values
• Employer of Choice and Establishing our Employer Brand • Health and Wellbeing • Engagement • Equality, Diversity and Inclusion • Values-Based Selection • Employee Relations • Celebrating Success
Right People
• Attraction Strategies • Recruitment and Selection • Sustainable Resourcing • Retention • Talent Management • Diversity • Career Development • Workforce Planning/Redesign and Business Transformation
Right Skills
• Leadership Development • Clinical Workforce Development • Apprentices • Changing Profile of Workforce • Learning and Development • Career and Personal Development • Succession Planning
Professionalism Integrity Compassion
Strategic Goals
Every Patient Matters
Every £ Matters
Every Team Member Matters
2

1. Executive Summary
The People and Culture Strategy 2018–2021, sets out the strategic principles and objectives relating to the
development of both our people and our employment practices.
The Urgent and Emergency Care review identifies the Ambulance sector as holding an important position at the gateway of the health and social care system, a system facing unprecedented demands and a challenging agenda delivering integrated care against a backdrop of financial constraint. This strategy aims to deliver sustainable people focussed solutions and the transformational change required to respond to the economic and social demands our services will face in the coming years.
This overarching strategy now incorporates the previously separate Talent and Clinical Development Strategy 2014–2017 and Equality and Diversity Strategy, ensuring a comprehensive and inclusive strategy.
This strategy is intended to devise a three-year programme which progresses sustainable workforce planning, including; attraction and retention, career development, succession planning, engagement, employee involvement and health and wellbeing. This is concerned with ensuring the presence of a workforce with the capability to improve service delivery and patient outcomes.
3

2. Introduction
The People and Culture strategy is built around the three pillars of Right People, Right Skills and Right Values
with each pillar featuring structured objectives and a three year work programme which ultimately supports
the Trusts vision of ‘Exceptional Care, delivered by Exceptional People’ and enables delivery of the Trusts
three strategic goals:
1. Every Team Member Matters
2. Every Patient Matters
3. Every £ Matters
The strategy is underpinned by the Trust’s behaviours: professionalism, integrity and compassion. Each of the resulting objectives incorporates these behaviours to ensure they are reinforced in the work that we deliver and the initiatives we introduce.
3. Objectives of the People and Culture Strategy
This strategy responds to the organisations strategic intentions and local and national context through the
following objectives:
To provide sustainable workforce plans which respond to labour market challenges, strategic objectives, system-wide
reviews, service redesign and changes in both the education system and professional bodies and colleges which influence
and impact upon the supply and capabilities of our workforce.
To recruit and retain talented people who share the values and behaviours we commit to as an organisation.
To develop our people and support their development to ensure that they are best placed to continue to provide quality services to our patients.
To eliminate discrimination and positively engage with under-represented groups and deliver initiatives to ensure inclusive teams and support the development of a more diverse workforce.
To ensure Trust investment in workforce development is aligned to strategic goals, business priorities and succession planning.
To support the health and wellbeing of our people, responding to the challenges of working longer and the external factors that can impact the health of our teams.
To increase workforce flexibility, resilience and capacity.
To engage meaningfully with our people, celebrate success and encourage a culture of compassion, supported by reflection and feedback to aid continual learning and improvement at an individual, team and organisational level.
Develop an apprenticeship programme which provides meaningful employment and education options, supports our workforce planning and maximises financial return against the apprenticeship levy.
4

4. Strategic Intentions
To ensure the Trust has the ‘Right People’
It is imperative that the Trust forecasts workforce requirements across all of its roles and services, and that service changes are accounted for in workforce planning. Challenging labour markets and a national skills shortage place greater emphasis on the importance of recruitment and attraction strategies, and ensuring return on investment and stability by equally focussing on retention. Developing our internal talent and providing long-term careers will improve our resilience, our leadership capabilities and our ability to meet organisational objectives, whilst providing development opportunities and rewarding careers for our people.
Ensuring our people have the ‘Right Skills’
This strategy features clear objectives to deliver a team with the prerequisite skills/experience to ensure responsive and effective patient care and optimise service outcomes. Our approach ensures staff have clear pathways to progress their careers, enabling SWASFT to nurture, develop and retain talented staff, meeting our business needs now and in the future. Leadership development is a key feature of the strategy in recognition of the influence effective, supportive and compassionate leadership has on the employment experiences of our people and how good leadership can critically impact the culture through the engagement, involvement and wellbeing of our people.
Ensuring our staff have the ‘Right Values’
This strategy is concerned with establishing the Trust as an Employer of Choice, to not only assist our attraction strategies, but to also ensure the existing workforce benefit from working in an environment where excellence is recognised and celebrated. Values and behaviours should support an environment of respect and care for one another with the health, wellbeing and engagement of our workforce a continued priority.
Embedding Equality and Diversity, Dignity and Respect in all we do
Equality and Diversity should no longer be seen as a separate agenda, additional and separate to the priorities detailed above. Therefore, for the first time, this strategy incorporates within it, the aims and objectives from the previously separate Equality and Diversity strategy. In doing so, it ensures our strategic objectives are concerned with demonstrating dignity and respect for the things that make us different and wonderfully unique and that resulting initiatives ensure we can increase and celebrate equal opportunities, and maximise opportunities for diversity, inclusion and engagement.
5

5. Scope and Context
This strategy supports the need for SWASFT to provide a team that can deliver an effective and wide range of clinical skills and support services in order to deliver its objectives, with patient care at the heart of everything we do.
Recent national-level strategic reviews, including the Urgent and Emergency Care Review led by Sir Bruce Keogh (NHS England 2013), position the ambulance service as one of the most important gateways into the health and social care system, and as an integral part of urgent and emergency care provision.
There is an explicit recognition that the ambulance service workforce has a vital role to play in addressing the challenges within urgent and emergency care, and that significant developments in the ambulance workforce will be required to maximise potential and to ensure every patient receives the most appropriate care in the most appropriate setting, enabling more patients to be treated in their own homes or local communities and reducing the amount of patients unnecessarily taken to hospital.
This is brought to life in the Trusts Mission ‘To respond quickly and safely to patients’ emergency and urgent care needs, at every stage of life, to reduce anxiety, pain and suffering and the Trusts vision to provide ‘ Exceptional Care delivered by Exceptional People’. The Trust has a legal obligation to comply with the Equality Act 2010, Human Rights Act 1998 and European Convention on Human Rights 1953 along with Employment Rights Act, Health and Safety legislation and the NHS Constitution. In doing so the Trust is required to demonstrate compliance with the Equality Delivery System 2, Workforce Race Equality Standards, Workforce Disability Equality System and Public Sector Equality Duty and Gender Pay Reporting.
This strategy will help the Trust develop stronger partnerships with local patient stakeholder groups which can be used to understand the health needs of the different communities we serve which in turn can assist in the development and education of our people. This in turn will strengthen the Trusts capability to adapt and develop understanding of the different communities we serve whilst also incorporating equality and diversity into our interactions and development opportunities for our teams.
National guidance suggests that the current system of urgent and emergency care is unaffordable and unsustainable. The number of emergency admissions to hospitals continues to rise at a time when NHS budgets are under significant pressure. There is a clear need to adopt a whole system approach and SWASFT continues to work with its commissioners to achieve this. The first stage of the Urgent and Emergency Care Review (NHS England 2013) sets out key proposals to assist reform:
Helping people with urgent care needs to get the right advice, in the right place, first time
Providing highly responsive urgent care services outside of hospital so people no longer queue at the Emergency Department
Ensuring that those people with more serious or life-threatening emergency care needs receive treatment in centres, with the right facilities and expertise in order to maximise chances of survival and a good recovery
Connecting all urgent and emergency care services so the overall system becomes more than just the sum of its parts.
Additionally the Carter Review (2016) highlights the significant and unwarranted variation in costs and practice across the NHS which, if addressed, could save the NHS £5bn. Of these savings up to £2bn comes from the workforce budget, through cultural reform, the adoption of good people management practices and improving productivity and resource utilisation.
6

The National agreement which underpins the re-banding of Paramedics across England supports the principle aims of the Urgent and Emergency Care Review by maximising the skills and experience of paramedics to support more patients to be treated in their own homes and to avoid unnecessary admissions at hospital. The Berwick Report into Patient Safety (2013) recommended that the NHS Trusts should become learning organisation and that: ‘Its leaders should create and support the capability for learning, and therefore change within the NHS’. The Cavendish Report (2013) on healthcare support workers in the NHS followed the Francis Report (2013) on values and behaviours. Cavendish recommended that better training and education should be provided for NHS staff in pay bands 1 to 4, and that leadership, supervision and support should also be enhanced for these staff.
6. Delivering our objectives – A three year work plan
The following pages feature detailed work plans which describe specific objectives under the three pillars of
this strategy of Right People, Right Values, Right Skills.
Importantly, the objectives seek to recognise the current status of each of these areas, recognising the work already
delivered whilst describing detailed objectives which progress each of these to the planned future state.
A timeframe is contained within each table, demonstrating the timescale associated with delivering the objective in its
entirety and achieving the planned future state. This should not be taken to mean that the objective itself is not being
progressed as a priority; only that as many are delivered incrementally, delivery and completion of the objective may be
achieved over a three year, rather than one year period.
7
6

Right People
Subject
Current Situation
Objectives
Future State
1st
Ye
ar P
rio
rity
Attraction Strategies
A reduction in experienced Paramedic applications.
Improvements on graduate application and conversion in 2017.
Annual Student Conference introduced in February 2015.
Greater engagement with universities both within and outside of LETB area.
Improved creativity in attraction strategies and development of Employer Brand.
Two overseas recruitment programmes delivered.
Develop targeted recruitment and attraction campaigns for hard to recruit roles.
Continue to embed a customer service ethos across recruitment activities and support candidate onboarding.
Positive Action – production of Annual Demographic Report to help inform attraction strategies and positive action/engagement.
Embed Employer Brand and roll out across all attraction activities.
Deliver further Student Conferences and further embed the Trust with universities and HE colleges, both within and outside of Trust area.
Achievement of projected recruitment plans and delivery of model for Paramedic recruitment.
SWASFT positioned as an Employer of Choice within the labour market.
Recognised as a proactive employer, actively engaging with the diverse communities we serve and striving to ensure our recruitment activity reflects our local population.
Diversify supply route to hard to fill roles, using local, national and international routes and initiatives.
Assessment and Selection
Paramedic assessment process reviewed and amended in April 2016.
111/999 advisors being selected using new assessment methods and online selection tools to assess better ‘fit to role’.
Full review and audit of employment processes, change in governance and achievement of good compliance and robust escalation.
Introduce output, input, activity and role profiling methodology for job descriptions.
Review ECA assessment process to ensure it is fit for purpose and relevant to role.
Develop recruitment and assessment training for line managers, focussing on promoting equality and inclusion and eliminating unconcious bias.
Early Employment Review and support process established in areas of high turnover in early employment.
Selection processes positively reflect Employer Brand and value proposition.
Ensuring better fit to role, evidenced through performance and retention data.
Reduced turnover in early employment.
Sustainable Resource Planning
The operational establishment report and forecasting which factors in all known intelligence about the movement of our resource.
Assess resourcing implications of investment/disinvestment and changes in contracted service delivery.
Assessing impact of external factors impacting supply or cost, i.e. Terms and Conditions (T&Cs), BSc, Living Wage, Apprenticeship Levy, Prescribing etc.
Workforce forecasts produced annually in line with A&E Operating Plan and five year workforce return submitted annual to NHS England.
Delivered the National Band 6 banding changes and the implementation of the new NQP role and asscociated infrastructure.
Ensure safe employment levels and aid deployment of core resources.
Development of sustainable contracting and T&Cs, to include bank and flexible worker supply.
Develop organisational and innovative approach to working longer – enabling long-term sustainable careers for the ageing workforce.
Engaging with HEE and individual educational providers to establish new pipelines of supply to meet the forecast need.
Establish internal development programmes to meet workforce plan projections.
Work with the Clinical Hub to determine a sustainable workforce supply plan, focussing both on attraction and career pathways for call advisors and sustainable supply of clinicians.
A sustainable workforce plan which maximises skills to support patient care, diversifies from traditional supply routes and which responds to the changing workforce profiles of the STPs and changes in education.
A resourcing plan which responds to changing expectations from new entrants to the workplace whilst also catering for a changing workforce demographic through creative and innovative role design.
Succession is provided through effective talent management.
Resource plans for all business changes and informed by labour market analysis and innovations in health care delivery and technology advances.
8

Subject
Current Situation
Objectives
Future State
1st
Ye
ar P
rio
rity
Retention A retention clause was implemented in 2015 through the use of training contracts.
A new exit process was launched in July 2017, in order to improve our organisational intelligence around the reasons that staff leave the Trust.
Delivery of a change programme to support common deployment model across the Trust area and address legacy variances (ie. Ambulance Technicians/Ambulance Practitioners).
Introduce a staff resignation form that will be submitted directly into HR allowing timely notification, enabling interaction with leaver and reducing overpayments.
Promote the importance of managers engaging with leavers.
Learn from all leavers and encourage open engagement and feedback.
Growth of our bank as a continued option for leavers to remain engaged with the Trust, but with improved governance around their use.
Explore opportunities for rotational roles and dual contracts with other partner organisations to aid retention, whilst giving our workforce exposure to other healthcare/educational settings.
Greater organisational knowledge regarding reasons for leaving which can be overlaid with other data from the staff survey and friends and family test to address reasons for leaving.
Improved workforce planning and faster fill times for vacancies.
Improved engagement scores and reduced turnover.
2n
d Y
ear
Pri
ori
ty
Talent Management
Whole system approach to talent management launched April 2015, with Aspire Career Portal launched to promote this fully in April 2016.
Embed talent management process to identify future leaders, ensuring they achieve their potential through promotion, lateral development or mentorship.
Regular reviews of talent pools undertaken to determine areas of under-representation and skills gaps requiring specific action.
Improved succession plans for future leaders and high performing staff.
More responsive leadership training needs analysis (TNA) which targets identified shortfalls in talent by skill, location or under-representation.
3rd
Ye
ar P
rio
rity
Diversity and Inclusion
Compliance with EDS2, including engagement with local groups.
Areas identified for initial intervention as under representation of women and BME groups.
Engagement with National Ambulance Diversity Forum and Employers Network for Equality and Inclusion.
In conjunction with UWE, development and delivery of a Paramedic pre-entry programme targeted specifically at under-represented groups.
Become a Disability Confident Employer/Leader (replacement of two ticks scheme).
Introduce a programme to help develop future female senior leaders.
Improve accessibility of information in line with NHS England Accessibility Standard.
Incorporate positive action into Apprenticeship Strategy, actively promoting these opportunities to under-represented groups.
Establish an Equality Steering Group to lead, consult with and promote initiatives and help inform future programmes of work.
Improve engagment with underresepented colleagues to learn about their experiences within the workplace to inform positive action. These forums will report in turn to the steering group.
Monitor workforce demographics and utilise data, combined with feedback to inform positive action initiatives.
Successful delivery and evaluation of identified initial programmes.
Continue to promote equality through application of all OD and HR work and act as the advocate for minority groups.
Established engagement forums for staff informing and leading intiatives and objectives
A more representative organisation which is responsive to and strengthened by its diverse workforce.
Established and recognised as a Disability Confident Employer/Leader.
Improvement in the experiences of staff as reported through the staff survey and monitored through data.
9

Subject
Current Situation
Objectives
Future State
3rd
Ye
ar P
rio
rity
Supporting an Aspirant Workforce
Aspire Career Portal for all staff launched in April 2016.
Clear career pathways articulated and available for staff at all operational levels.
New Career Conversation launched supporting open dialogue on aspirations and assisting career and development planning.
Increase in visibility of CPD via www.learnwithswasft.co.uk and opportunities to qualify as Paramedic.
Development Programme and Mentoring Programme in place for all leaders at Band 8a and above.
Development of rotational contracts supporting clinicians to work across the emergency, urgent and primary care arena and developing their skills and experience whilst providing continuity of employment and role security.
Develop Aspire and continue its promotion, establishing this as the ‘go to’ place for all staff wanting to develop.
Establish and widely promote all development opportunities and ensure an effective and responsive programme of CPD and Master Classes is delivered.
Further programmes to support non-clinical career development.
A culture of performance and aspiration.
A clear succession plan for the future and development areas understood and responded to.
A programme of CPD and leadership development which responds effectively to identified and known needs.
Sophisticated rotational contracts developed enabling enhanced employment offering for career development.
Workforce Redesign and Business Transformation
New pathways to development
Overseas recruitment and associated training to support transition.
Delivery of large scale organisational change programmes, including service investment and disinvestments
Delivered efficiencies in support services through Corporate Services Review 17/18
Initial Ambulance Nurse Programme to be effectively implemented and evaluated to include return on investment.
Delivery of service redesign, investment and disinvestment.
Review system and process across functions to improve cross departmental working and deliver efficiencies.
New pathways established for future supply.
Innovative workforce solutions explored in response to labour shortages, changes in the wider healthcare workforce as a result of changing healthcare systems and technological advances and innovation.
An affordable and sustainable workforce aligned with business needs.
10

Right Values
Subject
Current Situation
Objectives
Future State
1st
Ye
ar P
rio
rity
Career Conversation New career conversation launched in 2015 and further supported by Aspire.
Improve reporting and data held, and proactively chase for compliance.
Ensure quality of Career Conversations and engage with staff to ensure process is valued.
Improved compliance on the number of career converstations and the quality of these (as reported in the staff survey).
Employee Relations
Effective case management.
Coaching Managers to deliver routine management (sickness) without HR support.
Good partnership working in place.
Streamlined policy informed by learning arising from the management of cases.
Streamline and modernise processes and practices whilst maintaining quality and safe outcomes.
Coaching and training for managers to equip them to handle difficult employee relations issues, conduct high quality investigations and to effectively run formal processes with compassion, care and with due dillgence.
Monitor and share case outcomes with wider organisation, dispelling myths and sharing learning across the organisation.
Learning to be cascaded from every appeal to inform learning for all involved.
Managers equipped and competent to manage locally and achieve fair, equitable and sensible outcomes for their staff.
Responsive and efficient processes which support a more timely outcome.
Improved outcomes at formal hearings, evidenced through findings at appeal.
Embedding a compassionate leadership culture
People focussed policies and practices.
Management skills development
Ledaership Development and Assessment Centres to inform leadership TNA and PDPs for senior leaders
Better than average staff survey results for Ambulance Sector
Undertake cultural suvery to further understanding prevailing culture and interactions between colleagues
Full leadership development review resulting in leadership framework which promotes and celebrates compassionate, people centric leadership
Raise awareness of zero tolerance to bullying campaign and ensure local and corporate actions support this aim
Improved staff survey result.
A leadership culture that nurtures its people and is person centric in its outcomes
Engaged, motivated and aspirational leaders at every level
Improved performance, staff satisfaction and engagement and improved indicators in relation to bullying at work.
A culture which embraces openness and transparency and welcomes and is responsive to feedback from its people
11

Subject
Current Situation
Objectives
Future State
2n
d Y
ear
Pri
ori
ty
Engagement Staff Roadshows delivered annually.
Local action planning for staff survey and inviting contributions and participation.
Engagement sessions designed to help inform future Aspire developments and encourage feedback on OD initatives.
Develop local and corporate action plans to improve employee engagement.
Run a series of staff roadshows across stations and EDs.
Respond to staff feedback directly through mechanisms such as Aspire, roadshows and Staff Survey.
Introduction of online engagement tools.
Introduction of engagement groups for Health and Wellbeing and forums for all staffside reps to engage on behalf of their membership with Executive Directors of Operations and HR.
Further improved engagement scores in the annual staff survey.
An open culture where staff are encouraged to respond, engage and take the opportunity to do so.
Greater engagement and involvement from under-represented and minority groups to ensure initiatives are informed by rounded feedback from the widest possible audience.
Values Based Selection
Values based assessment practices used across all large scale recruitment (paramedics, call advisors, ECAs).
111/999 Call Advisors being selected using scenario/value-based questioning.
Introduce value-based interviews for every role.
Introduce a new online assessment tool for ECA recruitment, enabling a better fit to to role and values to be assessed throughs scenario/values based questioning.
All employees selected on values and behaviours.
Selection processes positively reflect Employer Brand and value proposition.
Employer of Choice and established Employer Brand
‘Working Wonders’ people brand launched March 2015.
Continue to embed the people brand.
Develop onboarding process for new starters.
SWASFT positioned as an Employer of Choice within the labour market.
Employer Brand fully embedded and reflected in candidate experiences.
Health and Wellbeing
‘Staying Well’ service (SWS) launched December 2015.
Peer Support Network launched April 2016.
Occupational Health and EAP providers sourced in addition to specialist services for PTSD support.
Continue to establish the working practices of the new SWS.
Extend the offering of the SWS to include proactive interventions to better respond to stress, mental health in the workplace and suicide preventation.
Undertake Evaluation and ROI on initiatives.
Establish a programme of health promotion with particular focus on supporting mental wellbeing of our people.
To have a workforce who are supported with their health and wellbeing, have access to a wide range of supportive interventions and are educated in healthy living.
Establish a culture which is open about mental health and responsive to those in need of support.
Act as consultant provider of H&W services to other emergency services.
12

Right Skills
Subject
Current Situation
Objectives
Future State
1st
Ye
ar P
rio
rity
Leadership Development
Introduced development centres for Band 8+ staff in April 2016.
Dedicated leadership programme developed to respond to TNA undertaken from development centre results.
Develop leadership TNA and provide leadership development programme that responds to these needs.
Expansion of OO development programme across each division with specific programmes targeting under-represented groups.
Deliver a programme of master classes and bitesize sessions.
Undertake a further review of Leadership Development requirements following the Operational Structure Review in early 2018, resulting in a targeted programme which is concerned with responding to identified gaps and which supports new entrants to leadership roles.
Improved leadership capability and succession planning.
Improved engagement.
Improved organisational performance.
Responsive TNA to address known leadership gaps.
A leadership programme which prepares and equips new managers to the role of leadership.
Apprentices
Ad hoc apprenticeship offering, departmentally led.
In light of the apprenticeship levy, introduce a wider range of apprenticeships within the Trust, establishing links with Further Education.
Introduce career pathways for apprentices.
Deliver an Organisational Apprenticeship Strategy.
Provider of apprenticeships/qualifications.
Improvements in diversity of workforce profile.
Improved career path and succession planning.
2n
d Y
ear
Pri
ori
ty
Clinical Workforce Development – Paramedics
Development programmes in 2015/2016/2017:
Specialist Paramedic Programme.
ECA to Paramedic Conversion Fast Track.
Distance Learning Programme.
Advanced Paramedic Practice.
CPD Modules.
All supply programmes to be effectively implemented and evaluated to include ROI.
Preparing the workforce through Aspire for future opportunities and pre-entry requirements.
Joint contracting to improve retention and skills development.
Ensure effective promotion of CPD opportunities and encourage engagement with these opportunities
New pathways established for future supply.
Educational and CPPD delivery to support integration and innovation.
13

Subject
Current Situation
Objectives
Future State
3rd
Ye
ar P
rio
rity
Learning and Development
Simbulance launched.
New education centre (North Division Education Centre – NDEC) launched within the grounds of a university (UWE) campus, with shared university facilities now available to SWASFT staff on site.
New Remote Clinical Decision-Making Module launched in collaboration with UWE.
Higher education and teaching modules now availalable to staff.
Advanced Practice project underway.
Incentives for mentors and practice placement educators defined.
Provide a range of pathways within which staff develop, including both short CPD offers and long award programmes which support career development, retention and quality patient care, ensuring these enable our workforce plan.
Improve accessibility of SME utilising e-learning and technology solutions to aid compliance.
For all training activities to come under the remit of education, ensuring SME compliance is appropriately monitored across all subject areas.
Create a vision for advanced clinical practice development.
Introduce clinical supervision sessions as a standard feature of operational clinical development.
Compliance with all SME requirements.
SWASFT will become a learning organisation with a strong research and education culture.
SWASFT will utilise the opportunities provided by apprenticeships to maximum cost benefit, while enhancing opportunities for staff.
Simulation and technology will enhance learning and will be an integral part of our training strategy.
There should be a clear and robust quality loop which allows us to constantly improve our learning and development offer.
Maximising technology to create efficiencies
Paper-based pay slip process.
Limited use of e-forms for staff changes, e-mail driven not automated.
Dual inputting.
Inconsistencies of training records.
Maximise ESR self-service functionality provided through web based portal.
Develop training and comms plan to support staff and manager self-service.
Implement e-Learning and Learning Management within ESR.
Staff and manager ability to view and update information from any location at any time, including pay slip, personal details and address.
Improved data accuracy through one point of entry and no duplication.
14

People, Strategy Programmes and Initiatives Held Monthly.
Meeting with operational heads of department to review, progress and update on objectives.
People and Workforce Committee HR Report presented to every bi-monthly People and Workforce
Committee Meeting. Scrutinises delivery of the Workforce Strategy and holds the Executive
Directors’ Group to account. Provides assurance to Board.
Senior Leadership Team Meeting Held Every Four Weeks.
Trust Board of Directors
Executive Directors’ Group Held Weekly.
Monthly reports relating to Establishment and Sickness presented for assurance. Presents reports on hot topics and proposals arising from the Strategy for
approval.
PRAG & JNCC (Joint Negotiations and Consultative Committee)
Held Quarterly PRAG – Policy Development Group
JNCC - Union engagement, negotiation and policy ratification. Responsible for dealing with issues
arising from themes within the Strategy.
HR AND OD THREE YEAR STRATEGY
HR and OD Management Meetings Chaired by Deputy Director of HR and OD.
Held Monthly.
Informed by: HRBP Meetings
Recruitment Meetings HR Services Meetings
E&D Steering Group Meetings
HR Senior Leadership Team Meeting
Held Monthly.
Chaired by Executive Director of HR and OD
L&D Management Meeting Chaired by Head of Education.
Held Monthly.
Informed by: Commercial and Driver Training Meetings
Divisional L&D Meetings Regional Education Forum (including
representatives from partnership universities)
L&D Management Meeting Chaired by Head of Education.
Held Monthly.
Informed by: Commercial and Driver Training Meetings
Divisional L&D Meetings Regional Education Forum (including
representatives from partnership universities)
National HRD Committee (sub-committee of AACE)
National Education Network for Ambulance Services
Heads of Education Group
National Ambulance Social Partnership Forum
Executive Directors’ Group Held Weekly.
Monthly reports relating to Establishment and Sickness presented for assurance. Presents reports on hot topics and proposals arising from the Strategy for
approval.
People and Culture Committee HR Report presented to every bi-monthly People and Culture Committee
Meeting. Scrutinises delivery of the Workforce Strategy and holds the Executive
Directors’ Group to account. Provides assurance to Board.
Senior Leadership Team Meeting Held Every Four Weeks.
PRAG & JNCC (Policy Review Alignment Group and Joint Negotiations and Consultative Committee)
Held Quarterly. PRAG – Policy Development Group
JNCC - Union engagement, negotiation and policy ratification. Responsible for dealing with issues
arising from themes within the Strategy.
Health and Wellbeing Engagement Forum and Equality and Diversity Steering Group
Both Held Quarterly
Subject specific Employee Engagement forums.
PEOPLE AND CULTURE THREE YEAR STRATEGY
HR and OD Management Meetings Chaired by Deputy Director of HR and OD.
Held Monthly.
Informed by: HRBP Meetings
Recruitment Meetings HR Services Meetings
E&D Steering Group Meetings OD and Project Meetings
HR Senior Leadership Team Meeting
Held Monthly.
Chaired by Executive Director of People and Culture
L&D Management Meeting Chaired by Head of Education.
Held Monthly.
Informed by: Commercial and Driver Training Meetings
Divisional L&D Meetings Regional Education Forum (including
representatives from partnership universities)
National Ambulance Social Partnership Forum
National HRD Committee (sub-committee of AACE)
Heads of Education Group
National Education Network for Ambulance Services
7. Delivering the Strategy through the HR and OD Directorate Governance Framework
This strategy has been shared for consultation with key stakeholders prior to ratification and will be formally launched in January 2018.
The objectives detailed within will be delivered through dedicated work programmes set throughout the HR and OD directorate. Lead individuals will take responsibility for delivering associated programmes of work, ensuring appropriate governance to assess risk, obtain authorisation and ensure widespread engagement and involvement in the design and delivery of the initiatives which will help to shape and progress our workforce in line with the stated intentions within this strategy.
The strategy will be delivered through the following framework, ensuring appropriate governance, overview and assurance is in place to support the directorate in achieving its strategic aims.
Trust Board of Directors
15

8. Review and Monitoring
The delivery of the strategy will be reviewed annually and reported to the Trust Board and the People and Culture Committee as applicable. The objectives within the strategy will be cascaded throughout the HR and OD directorate through the departmental work programmes and the setting of personal and team objectives, with delivery being monitored through the team meetings structure, 121’s and career conversations and through regular reporting to Director and Board Committees.
The HR and OD directorate will undertake regular evaluations and reviews to assess the success of initiatives and programme completion, taking forward learning that arises to ensure a continual cycle of improvement is reflected throughout the delivery of this strategy.
16

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 1
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: People and Culture Committee Terms of Reference
Prepared by: Marty McAuley, Trust Secretary
Presented by: Rakhee Rankin, Chairman of the People and Culture Committee
Action: Approval
Recommendation:
The People and Culture Committee recommend that the Trust Board of Directors approve the Terms of Reference of the People and Culture Committee.
Executive Summary:
At its meeting on 18 April 2018 the People and Culture Committee reviewed its terms of reference to ensure that they remained fit for purpose. During consideration of the terms of reference some minor amendments were made which included: Renaming of the Committee to People and Culture Clarifying that the metrics to be used for monitoring progress against the HR and OD strategy would not be limited to only workforce metrics Incorporating environmental and sustainability issues within the remit of the Committee. The People and Culture Committee agreed the changes and recommend their approval by the Board.

Page 1 of 7
People and Culture Committee
Terms of Reference
Version 3.0
Author Amy Beet, Director of HR and OD Rakhee Rankin, Chair of Committee Marty McAuley, Trust Secretary
Approved By Trust Board of Directors
Approved Date 25 May 2018 – subject to Board approval
Issue Date
Review Date March 2019

Page 2 of 7
1. Purpose 1.1 The Committee will develop and implement effective systems and processes to
secure appropriate assurance, and provide advice to the Board on all strategic matters relating to the workforce and organisational development.
1.2 It will have due regard for the Trust’s strategic aims and overall business needs, relating to the provision of care and services in support of getting the best clinical outcomes and experience for patients, staff (past, present and potential) and the Volunteers of the Trust.
2. Constitution and Authority 2.1 The People and Culture Committee is established in accordance with the Trust
constitution, standing orders and scheme of delegation. 2.2 These Terms of Reference set out the membership; remit; responsibilities and
reporting arrangements of the Committee (and shall have effect as if incorporated into the Trust constitution and standing orders).
2.3 The Committee is established and approved by the Board of Directors as one of its
committees. 2.4 The Committee is authorised by the Board to investigate any activity within its terms
of reference. 2.5 The Committee is accountable to the Board of Directors and any changes to these
terms of reference must be approved by the Board of Directors. 2.6 It is authorised to seek any information it requires from any employee and all
employees are directed to co-operate with any request made by the Committee. 2.7 The Committee is authorised by the Board to obtain outside legal or other
independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
3. Role
3.1 To provide strategic direction and Board assurance in relation to all People and
Culture matters. 3.2 Make recommendations, as appropriate, on People and Culture matters to the Board
of Directors.

Page 3 of 7
3.3 Oversee the implementation and the embedding of the HR and OD Strategy across the Trust.
3.4 Receive assurance reports and deep dive reports to demonstrate the successful
delivery of the objectives and intentions of the HR and OD Strategy.the Health and Safety Strategy.
3.5 Assessing and identifying risk within the Workforce and Culture Development portfolio and escalating this as appropriate.
3.6 Robustly and routinely monitor a set of metrics at the committee to demonstrate
progress made against the HR and OD Strategy. This will include monitoring of numbers and type of employee relations cases and themes arising from these to inform further organisational learning.
3.7 Challenge existing practice to ensure that the People and Culture are supported whilst
delivering the strategic goals of the organisation. 3.8 Consider impact of proposals or innovations on the People and Culture; service
delivery or resource requirements. 3.9 Commission reviews into any area of its scope of activity in order to gain further
assurance or to inform service change. 4. Membership 4.1 The Committee has a core membership supported by regular attendees and
managers presenting papers. The Executive Director of HR and OD is the Executive Lead for the Committee
4.2 The Membership will be as follows: Executive Director of HR and OD Chief Executive Executive Director of Operations Five NEDs (Rakhee, Minesh, Tony, Venessa and Gail)
4.3 The Committee has a number of regular attendees:
Trust Secretary Executive Director of Nursing and Quality Director of Operational Services Deputy Director of HR Deputy Director of Finance Head of Communications Head of Education Unison representative

Page 4 of 7
4.4 Governor involvement may also be invited. 4.5 The Committee is empowered to request attendance by any other individual acting in
an advisory capacity to support the discussions of the Committee. 5. Reporting and Accountability 5.1 The Committee is accountable to the Board of Directors. 5.2 After each People and Culture Committee a report will be produced and presented to
the next available Trust Public Board of Directors meeting for assurance. 5.3 Once approved by the People and Culture Committee a copy of the minutes will also
be presented to the next available Trust Public Board of Directors meeting for assurance.
5.4 The People and Culture Committee may escalate items to the Board for approval or
discussion as well as refer items to the Directors group or a Committee for further consideration. The People and Culture Committee may also receive requests from other forums to consider matters.
5.5 The Committee shall receive the minutes of all working groups reporting to it following
each meeting of each group. These are for information only:
Health and Safety Steering Group and Committee Equality and Diversity Steering Group Joint Negotiating Consultative Committee (JNCC) Staff wellbeing Engagement Group Environmental Management Group
6. Chairperson 6.1 The People and Workforce Committee will be chaired by a Non-Executive Director.
The Committee should appoint a Deputy Chair, who should also be a Non-Executive Director.
7. Administration Support 7.1 The Trust Secretary will provide the administration support to ensure that the
committee cycles; meetings; papers and action point registers are appropriately managed.
7.2 Minute taking will be provided by the EA to the Executive Director HR and OD.

Page 5 of 7
7.3 Papers to be issued one week in advance of the meeting via SharePoint. Paper copies will not be produced.
8. Frequency of Meetings 8.1 There will be a minimum of four meetings a year.
9. Quorum 9.1 The Committee shall be quorate when three Members are present. There must be at
least one Executive and one Non-Executive member present. 10. Self-Assessment 10.1 An annual self-assessment will be completed each year by the Committee. 10.2 An annual report monitoring the effectiveness of the Committee will then be prepared
by the Committee Chair and Executive Lead for discussion each year. The agreed report will then be submitted to the Board for assurance.
10.3 The annual report will include: consideration of all the main duties of the Committee;
accountability, including reporting arrangements; input from sub groups; confirmation of completion of the work of the Committee as set out in its annual business cycle; membership and attendance; quoracy and frequency of meetings.
10.4 These terms of reference will be reviewed on an annual basis as a minimum, however
as a new Committee an interim six month review will be added.

Page 6 of 7
Annex A: Duties – General duties of the Committee:
• Challenge existing practice to ensure that the People and Workforce are supported whilst delivering the strategic goals of the organisation
• Refer and receive items for consideration by Directors, Board or Committee • Provide regular assurance reports to the Board of Directors and other Committee as
appropriate • Approval of a strategic workforce plan that is aligned to the long term financial plan
and Integrated Business Plan Receive national updates and consider the impact on SWASFT including:
• National initiatives • Agenda for change initiatives and changes • NHS constitution – staff pledges and rights • Freedom to speak up Guardians and whistleblowing
Take assurance through robust monitoring of health and safety compliance:
• Monitoring of activity plan focused in priority order on Riddor, then lost time and traffic collisions
• Assurance the trust understands causal affects and mitigating plans for both our employees and patients
• Receive minutes from Health and Safety Committee Provide oversight and scrutiny to Recruitment and Retention levels:
• Oversight of (1) Attrition (2) Retention (3) Vacancies (4) leavers and (5) recruitment plans to assure that the Trust has a workforce plan that is fit for purpose and ensures right resource in the right place at the right time(clinical and non-clinical).
• Review the use of agency staff and skills mix • Consider the Salary Profile of staff • Input into and recommend to the Board of Directors, the approval of pay and reward
strategies for staff Consider initiatives to support Staff Wellbeing and monitor outcomes:
• Compliance to working time directive • Consider the support to staff during retirement planning to transition into retirement • Staff engagement mechanisms • Engagement and culture - what's the top key positive and negative feedbacks • Receive the Staff Survey results and organisational plans to address improvement • Approval of action plans, policies and strategies with regard to health and well-being • Receive report from Staying well service

Page 7 of 7
Monitor Staff Development opportunities and access • Development and training activity and effectiveness include compliance to mandatory
training • Monitor Career conversation compliance • Review talent mapping and plans to ensure we have the best leaders in the
organisation at every level • Agree on the commissioning intentions for training and education through Health
Education England; the Academic Health Science Network; the Local Education Training Board Higher Education Institutions; Deanery and other stakeholders
Oversight of Sickness and Absence Management • Monitoring of sickness absence rates • Compliance and application of sickness policy • Commission root cause of any areas of concern
Promote Equality and Diversity
• Consider the findings of a Gender Pay Audit • Oversight of diversity and gender plans and activity to ensure the trust is positively
and actively engaged in having a diverse workforce that represents the community's • Approval of action plans, policies and strategies with regard to Equality and Diversity
Risk
• Receive People and Workforce related risks and take assurance from the actions being developed
• Consider impact of proposals or innovations on the People and Workforce; service delivery or resource requirements
Environment and Sustainability
Oversee the Trust responsibilities with regard to the environment and sustainability Receive regular updates on progress against our objectives

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 1
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Trust Strategy 2018-19 to 2020-21
Prepared by: Marty McAuley, Trust Secretary
Presented by: Jennie Kingston, Deputy Chief Executive / Executive Director of Finance
Action: Approval
Recommendation: The Trust Board of Directors is asked to formally approve the Trust Strategy 2018-19 to 2020-21
Executive Summary:
The Trust Strategy has been developed over a number of months and been considered by the Board of Directors at its March and April confidential meetings. The final Strategy is now presented in the public domain for final approval. Following approval the Strategy will be published as per the agreed communications and engagement plan. In addition a public facing version will be developed supported by a short video that will summarise the key aims of the Strategy

strategy2018/19 to 2020/21
Trust

The next three years represent an exciting time for the Trust with the opportunities for real transformation being significant. Refocusing the Strategy on our core business
– what we do best, will allow the organisation to make positive change and continue to provide exceptional care to those in need. As a Board we are immensely proud of our teams who go above and beyond day-in-day-out with relentless growing demand and challenge. They demonstrate a remarkable degree of professionalism and commitment treating patients as individuals and giving support and empathy in often the most difficult circumstances. This has been recognised by the Care Quality Commission who rated our services as outstanding for caring with our teams being passionate about patient care and wellbeing. We want to continue to empower our people to deliver services of excellence providing them with the support and tools they need. This Strategy sets out a number of initiatives to deliver on this intention. However, as an organisation there are always lessons to be learnt and delivery of this Strategy will not be without its challenges. Long term sustainable improvements in performance can only
FO
RE
WO
RD
KEY ANNUAL FACTS
Tony FoxChairman
Ken WenmanChief Executive
be delivered in partnership with our Commissioners and wider health systems and a substantial shift in the way we deliver our current 999 service. This carries a cost and can create additional pressure and uncertainty for our teams who continually endeavour to provide the best care for patients every time. Couple this with an environment where the financial pressures on the NHS show no sign of easing the Trust will need to work harder than ever to ensure patient care is not compromised in any way. The aims of this Strategy have been directly influenced by our commitment to ‘deliver exceptional patient care by exceptional people’. We are confident that through delivery of this Strategy we will not only meet this vision but also position the Trust to deliver NHS services that everyone can be proud of.
02
999 calls taken
999 incidents managed out of
an ED setting
NHS111 calls answered in
Dorset
Incidents responded to
by Community Responders
1,000,000+ c54% 224,000+22,000+

The South Western Ambulance Service NHS Foundation Trust is the largest and the most rural ambulance service in the country, covering the entire south west region – roughly 20% of the English mainland. The Trust provides services across the counties of Cornwall and the Isles of Scilly, Devon, Dorset, Somerset, Wiltshire, Gloucestershire and the former Avon area (Bristol, Bath, North and North East Somerset and South Gloucestershire). The operational area is predominantly rural but also includes the City of Bristol and a number of other urban centres including Gloucester, Plymouth, Bath, Bournemouth, Swindon and Poole. Commissioned by 12 Clinical Commissioning Groups the business of the Trust is centered largely around a range of core services, the primary one being emergency ambulance services. These services require clinical hubs including a maximum of call handling facilities, initial triage (clinical assessment), advice, filtering, signposting and call allocation or dispatch capabilities:• Emergency Ambulance Services (999 A&E)
that provide an emergency response to 999 and healthcare professional calls that are likely to require treatment and / or immediate transport to a hospital or other facility. In addition the Trust has two Hazardous Area Response Teams providing the ambulance response to major incidents
• Integrated Urgent Care Services which for the Trust involves four main types of service:
◆ Out of Hours General Practice (OOH GP) services that provide non-emergency responses to people who require, or perceive the need for, urgent (but not emergency) advice, care, diagnosis or treatment
◆ NHS 111 services that include call handling and triage services for individuals with urgent medial concerns
◆ Tiverton Urgent Care Centre that is supported by a team of highly qualified GPs and nurse practitioners and provides treatment for a host of minor injuries and ailments
◆ Single Point of Access that operates 24/7, 365 days a year and is used by health care professionals that need access to community services
Across these services the Trust provides emergency and urgent care services to over 3,400 patients every day. To deliver these services the Trust employs in excess of 3,900 people (WTE), and has access to a range of other individuals from student paramedics, bank, GPs and community responders. As an NHS Foundation Trust, the Trust has a Council of Governors and a membership base drawn from the general public and our teams. Governors are either elected by public and team members or appointed by partnership organisations. The Trust is committed to working with its local partners to address local challenges and improve services for patients and, as a regional provider, spans 18 acute trusts, six partnership trusts, numerous community hospitals and urgent care services and seven sustainability and transformation partnerships. In addition the Trust works in partnership with numerous other organisations including local police and fire and rescue services.
AB
OU
T U
SThe English ambulance sector constitutes 2% of total annual NHS spend at £2.3bn per annum. This is significant in public spending terms and decisions ambulance trusts make have a significant impact on the health sector.
strategy2018/19 to 2020/21
Trust
Out of Hours Patient
Contacts
Population of the south west
Tourists each year
Miles travelled
100,000+5.5+
million23+
million23+
million

CO
NT
EX
T The Trust currently has in place a five year Strategy ‘The Integrated Business Plan’ covering the period 2014/15 to 2018/19. Since its publication there has been a material shift in both the strategic direction of the organisation and national policy that directly impacts upon the ambulance sector. From a former strategy of diversification and expansion, the Trust is now moving to a position of refocusing on its existing core services to embed the significant level of change on the horizon.
2017 marked the 80th anniversary of the introduction of the 999 emergency telephone number. During this time ambulance services have changed beyond recognition from little more than vehicles transporting patients to hospitals, often staffed by volunteers, to the “mobile hospital” model that is seen today. Now a large number of responses focus on the frail elderly rather than traditional medical emergencies. Half of all calls are resolved by paramedics without the need to take patients to hospital, and for specialist care the focus of the ambulance service is increasingly on getting patients to the right hospital rather than simply the nearest.
Nationally 999 emergency ambulance services have been at the forefront of recent NHS reform with a specific focus on each ambulance service in terms of quality, performance, delivery and efficiency. NHS England have in recent years been leading a national change programme
- the Ambulance Response Programme (ARP), that shifts the focus in the ambulance sector from the traditional time based targets to an emphasis on patients’ clinical needs. This change is an important step in enabling the ambulance service to provide patients with the best care possible, within an appropriate timeframe, while also making the most effective use of its resources in the face of rising demand.
A revised set of national standards were rolled out to all ambulance trusts during 2017 however further change is expected during 2018/19. Alongside this the establishment of the national Ambulance Improvement
Programme and Operational Productivity Review (Lord Carter Review), focused on sustainability and efficiency, will have a material impact on the structure and form of ambulance service provision going forward.
Looking at the delivery of urgent care, NHS England’s Next Steps on the Five Year Forward View highlighted the importance of delivering a functionally integrated urgent care service to address the fragmented nature of out of hospital services. The new national service specification for an integrated 24/7 urgent care access, clinical advice and treatment service is set to revolutionise the way in which urgent care services are provided and accessed. This will have a significant impact on both the services the Trust currently delivers within Dorset (NHS 111 and Out of Hours) and the wider urgent care network across the south west region.
For these reasons and more the Trust has taken the decision to refresh its Strategy a year early and produce this document – a three year Strategy to set the foundations for an organisation and a service that will
“transition” in the medium term in response to emerging local and national policy.
In setting this Strategy the Board has focused on retaining the ‘sovereignty’ of the Trust as an organisation whilst acknowledging that the Trust will need to adapt and remain flexible to respond in a way that best serves the interests of patients, the Trust and the local health community.
04

ST
RA
TE
GIC
OV
ER
VIE
WThroughout the delivery of this Strategy the Trust will ensure that quality of clinical care and patient safety is upheld during what will be a period of significant service change. The Trust is likely to be subject to greater scrutiny, performance management and accountability and has therefore considered a number of principles that have influenced the strategic priorities for the Trust.
• The primary focus of the Trust is the delivery of 999 emergency ambulance services to ensure sure that they are as safe a service as is possible to achieve
• The Trust will work hard to retain the urgent care contracts it currently holds
• The Trust will continue to apply its ‘no compromise’ principles in considering new opportunities or material service changes. This means that each opportunity / change must; deliver a high quality service for patients; stand alone in isolation and `wash its face’ financially; deliver against the minimum regulatory, contractual and statutory standards and align to the core business of the Trust
• The financial plan will continue to focus on maintaining the financial sustainability of the organisation, underpinned by an ethos of ‘only spending what we have’
• Participation in pilots will be considered against a number of parameters including the ability to support economies of scale and whether they have the full support of Commissioners
• The Trust will act and form relationships to ensure it is an integrated part of local health systems across the region
• Without a significant change in the current health system environment the Trust will not look to diversify its core business further over the life of this Strategy
If the Trust is to succeed in both transitioning its 999 emergency ambulance services to meet the new national requirements and in delivering a new and integrated urgent care service within Dorset it needs to focus its resources appropriately. The aims and objectives of this Strategy therefore focus the organisation on its existing core business with a view to becoming a leading NHS service that everyone is proud of.
strategy2018/19 to 2020/21
Trust

06
Exceptional patient care delivered by exceptional people
Trust mission statement
Trust vision statement
To respond quickly and safely to patients’ emergency and urgent care needs, at every stage of life, to reduce anxiety, pain and suffering
Trust values
The Trusts values are aligned to those of the NHS Constitution:
Working together for patients: We put patients first in everything we do, by reaching out to staff, patients, carers, families, communities, and professionals inside and outside the NHS;
Respect and dignity: We value each person as an individual, respect their aspirations and commitments in life, and seek to understand their priorities, needs, abilities and limits;
Commitment to quality of care: We earn the trust placed in us by insisting on quality and striving to get the basics of quality of care – safety, effectiveness and patient experience – right every time;
Compassion: We ensure that compassion is central to the care we provide and we respond with humanity and kindness to each person’s pain, distress, anxiety or need;
Improving lives: We strive to improve health and well-being and people’s experiences of the NHS;
Everyone counts: We maximise our resources for the benefit of the whole community, and make sure nobody is excluded, discriminated against or left behind.
Our aims and objectives

strategy2018/19 to 2020/21
Trust
SG3: Every Pound Matters Delivering robust financial discipline, including reduced variation and increased productivity and efficiency, to ensure
“healthy” finances.
SG1: Every Patient Matters Delivering compassionate, clinically effective care across all Trust services that is safe, responsive and provides confidence and reassurance to patients and their families.
SG2: Every Team Member Matters Delivering strong, inclusive and caring leadership to a team made up of the right people, with the right skills, values and behaviours.
Strategic Goals The Trust has three strategic goals for delivery over the life of this Strategy each underpinned by a number of initiatives
Our aims and objectives
• Deliver the new clinical quality indicators
• Further develop the ‘hear and treat’ pathway
• Rollout Community First Responder lifting scheme
• Develop Always Events• Deliver achievable
performance• Refine clinical triage
effectiveness• Deploy remote triage• Collaboration
• Improve and develop our culture
• Ensure a sustainable supply of people
• Develop our future leaders• Improve the wellbeing of our
people• Embed Time to Care
• Embed Lord Carter recommendations
• Embed the Transition Plan• Manage service change impact• Only ‘spend what we have’• Deliver affordable quality

Cornwall Proposals
Clinical Assessment
Service
ST
RA
TE
GIC
DR
IVE
RS The following diagram illustrates
the breadth of existing and emerging national, local and internal strategic drivers that are impacting upon the Trust over the life of this Strategy. Ambulance service sustainability and transformation is a key area of focus and will drive a significant amount of change.
08
Regulation
Sustainability and Transformation Plans
Integrated Care Systems
(ICS)
Integrated Urgent Care
Control Totals,
Transformation Funding
CQC
Joint Assessments Regulatory
National Specification
Dorset ICS
Bristol, North Somerset & South
Gloucestershire
Bath & North East Somerset
NationalPolicy
Cornwall & Isles of ScillyGloucestershire
Somerset
Devon
Internal Drivers
Quality Performance Improvement
Time to Care
Ambulance Response
Programme
NHS Mandates
UEC Delivery
Plan
NHS111 online
Ambulance PillarNHS111
calls
Affordable Quality
Transition Plan
Workforce
Talent Development & Progression
Paramedic & NQP roles
Vacancies & Retention
Productivity
Financial Framework 2018/2021
Ambition for ‘Good’ Rating
STRATEGIC DRIVERS
Local health system plans could result in material service changes for the Trust through changes in activity, the location of a service of facility or the ‘loss’ of ambulance resources through ‘out of area’ activity in each health system.

strategy2018/19 to 2020/21
Trust
Ambulance Improvement Programme
(NHS Improvement)
Commissioning Development
Financial Sustainability
Workforce Development
Organisational Development Configuration
Core Operating
Model Principles
Mandatory Collabratives
Shared Management
Chains
People Development Programmes
Health & Well Being Framework
Band 6 Paramedics
Workforce Supply &
Demand Plans
Five Year Financial Model
National Core 999
Specification
National Ambulance
Commissioning Framework
Carter Review (NHS Improvement)
Data, Metrics and
Benchmarking Model Ambulance
Portal
Procurement
Clinical Workforce
Productivity
Consult and complete
Integration
Improved / extended Access
to GPs
Ambulance Service Sustainability and Transformation
NHS Improvement, a regulator of NHS trusts and independent providers of NHS-funded care, are leading the delivery of a number of ambulance improvement initiatives. These are designed to address the challenges in securing sustainable provision in future years.
The scope of the Carter review includes identifying unwarranted variation; optimising transparency and consistency; identifying efficiency improvements; and specifying the benchmarking criteria for an “optimal model” ambulance trust.
In line with the new national specification increasingly local Clinical Commissioning Groups are moving towards commissioning a service that provides a single entry point into urgent care.

Frailty and Falls Number of frailty cases in patients over 80 set to double in next 20 years. One third of over 65’s fall at least once each year.
Mental HealthTrust estimates around 60,000 999 calls each year are due to mental health issues. Ambulance conveyance to Emergency Departments (ED) is high (c50% of all mental health presentations arriving via ambulance)
NHS111Average number of 999 calls originating from NHS111 providers in the south west varies between 12% and 18% Population
and AgeSouth West population is expected to increase by 16% over the next 20 years. Those aged over 65 use between one and two thirds of all ambulance resources.
Public ExpectationsA survey found that only 31% of callers considered calling another service, suggesting that there is an inherent over-reliance on ‘999’ emergency services and the public can be reluctant to use alternatives
The number of people aged over 65 and
responded to by the Trust following fall is rising.
The proportion of 999 incidents originating from NHS111 continues to rise
from around 18-19% in the early period of the service to around 20-22% now.
There is also a high level of variation across the range of
NHS111 providers.
Consistently positive patient experiences of ambulance
services, and confusion surrounding other areas of
healthcare, are factors that may have contributed to an increased
use of ambulance services by patients with non-urgent
healthcare needs
The number of users of adult mental health services could be a significant contributor to ambulance demand. A significant proportion of the Trust’s patients are currently managed without conveyance to ED. Of those conveyed, the majority are conveyed to an ED.
The size of the population, combined with an annual influx of 23 million tourists to the south west region, correlates highly with ambulance demand. Population needs to be considered alongside the context of an ‘ageing society’ where research shows use of both emergency and non-urgent ambulance services increases as people grow older, and accelerates after the age of 65.
10
KE
Y F
AC
TO
RS
DR
IVIN
G D
EM
AN
D
Over a period of 10 years demand changes within the ambulance sector have been significant. On average, nationally, the number of patient contacts per day has risen by 35% from 15,700 to 21,200 with the total number of calls having risen to around 11 million per year. These trends are expected to continue with the number of patient contacts rising by a further c38% over the next ten years.
Ambulance incidents (calls where the ambulance service responds either by dispatching a vehicle or by providing telephone advice and referral) have increased by 65%
and ambulance journeys (where a patient is taken to hospital) by 40%. The more modest increase in journeys reflects the substantial changes that have taken place during this period which have seen the ambulance service develop from a transport service to a significant provider of emergency and urgent care in its own right; partly as a result of services needing to manage year on year increases in demand. As a consequence, a far greater proportion of 999 calls are now managed either at the time of the call (hear and treat) or by skilled ambulance clinicians at an incident scene or in patients homes (see and treat).
Demand for emergency and urgent care increases year on year creating a source of considerable pressure. The reasons for increases in demand are a complex mix of changing demographic, health and social factors but historically the way urgent and emergency care is delivered has remained broadly the same.
D E M A N D D R I V E R S
I N T H E S O U T H
W E S T

strategy2018/19 to 2020/21
Trust
In developing this Strategy the Trust undertook a SWOT analysis. This was to identify the main factors influencing the successful delivery of the Trust’s strategic aims and, in the short to medium term, organisational sustainability.
• A caring organisation that demonstrates a high level of compassion, kindness and respect towards people
• An innovative organisation that is often a sector leader in testing or delivering change programmes
• A uniquely positioned organisation with established 24/7 services, diverse experience and regional coverage
• A well-led and well-governed Trust with a skilled and stable leadership, a strong and able management team and a highly capable workforce that aspires to deliver the best
• A financially stable organisation that has maintained financial balance and strong financial systems
• An organisation that delivers clinical excellence and is at the forefront of clinical research
STRENG
THS
• Ambulance sector changes arising from national policy and review (e.g. the Ambulance Improvement Programme)
• Access to an extensive range of clinical data and business intelligence that can be used to inform service developments and partnership working
• Ability of the Trust to integrate services across both its own and other services within the region
• Increasing clinical capabilities of the paramedic workforce that will enhance the services provided to patients
• Embed and jointly lead the development of new service models across local health systems
• Specialist knowledge and expertise in areas such as emergency preparedness and resilience
OPPO
RTUN
ITIES
• Little financial headroom and a reduced ability to invest in future innovation
• A fragmented approach to the commissioning of urgent care services driving, in some areas, inefficiencies and market instability
• Ability of the Trust to engage and retain the future workforce with increasing competition
• Ensuring positive engagement and relationships with all stakeholders, and managing system ‘politics’, given the Trust’s geographic coverage
• ‘Performance’ pressures whilst transitioning the service to operate under the new national ambulance standards
• Cost base of the Trust versus other providers and the ability of the Trust to be competitive
WEA
KN
ESSES
• Scale and impact of wider health system changes yet to be fully determined
• Demographic factors in the wider population continuing to drive demand and the need for more flexible services
• Team resilience and morale in the face of increasing pressures
• Increasing competition for the paramedic workforce from primary, secondary and emergency care within the NHS and private sector
• Reducing NHS budgets going forward and the ability of the Trust to remain financially stable with an ever increasing funding gap
• Ability of the Trust to continue delivering ‘affordable quality’ and reconcile quality, performance and money
THREA
TS
SW
OT

12
TH
E F
UT
UR
E O
F E
ME
RG
EN
CY
AN
D U
RG
EN
T C
AR
E S
YS
TE
M
Hear & Treat
Call closed following
triage
Category 1
Life threatening illnesses / injuries
7 minute mean
15 minutes
90th centile
Category 2
Emergency Calls
18 minute mean
40 minutes
90th centile
Category 3
Urgent Calls
120 minutes
90th centile
Category 4
Less Urgent Calls
180 minutes
90th centile for 999 calls
See & Treat
Patient treated at scene
See & Convey
EDPatient
conveyed to an Emergency Department
See & ConveyOtherPatient
conveyed to an alternative
treatment centre
Resource Dispatched
DispatchCertain calls
dispatched to at this point
Triage & Assessment
Call Connect
Nature of Call QuestionsBreathing?Conscious?Bleeding?
In recent years a number of national reviews and programmes have been undertaken that have focused on transforming the delivery of ambulance services with the aim of specifically improving outcomes for patients. This includes the Next Steps on the NHS Five Year Forward View and the subsequent development of the Urgent and Emergency Care Delivery Plan. As a result a number of urgent care systems are beginning coming together to develop integrated models of care that support the delivery of care closer to home. It is widely recognised that these emerging commissioning landscapes require continued integration and collaboration and that ambulance services and commissioners are integral to this system-wide approach.
999 Emergency Ambulance ServicesThe common aim across these national reviews is to improve the clinical outcomes and operational performance of the ambulance service and to provide a more equitable and clinically focussed response that meets patient needs in an appropriate time frame. The Ambulance Response Programme (ARP) has been one of the most material reviews to date implementing changes to both clinical and operational standards for all English ambulance services. Time based standards have been used as a key performance measure for ambulance services both nationally and internationally, despite a lack of evidence that they actually lead to good clinical care. They have been effective in driving improvements and maintaining response times to the most critically ill and injured patients. However, efforts to meet these standards in the face of rising demand have led to a range of operational behaviours that may be inefficient, with the potential to distort the system away from a central focus on patient care and outcome. New national response standards were formally rolled out to every ambulance service in England during 2017. The changes focus on making sure the best, high quality, most appropriate response is provided for each patient first time. Implementation of the new standards is both iterative and dynamic with further changes expected nationally during 2018/19. These will need to be considered in year by the Trust and involve Commissioners in terms of further impact on the 999 service and the target operating model.
DISPOSITIONS
OUTCOMES
999

strategy2018/19 to 2020/21
Trust
Urgent Care Services to Integrated Urgent CareIn line with the new national specification for Integrated Urgent Care increasingly local Clinical Commissioning Groups are moving towards commissioning a service that provides a single entry point into urgent care. In other words moving from separate NHS111, Out of Hours and other services to a fully Integrated Urgent Care system that delivers high quality services, provides clinical assessment when necessary, provides advice and treatment and has clear accountability and leadership. The opportunities to improve the patient’s experience of,
and clinical outcomes from, urgent care as a result are significant. Patients will find it easier to access urgent care clinical advice, on the phone and online through a Clinical Advice Service (CAS) with the CAS becoming the key coordinating function for urgent care needs. GP out of hours and NHS111 services will increasingly be combined. By 2019, NHS111 will be able to book people into urgent face to face appointments where this is needed. As part of this transformation, NHS111 is being enhanced so that patients access urgent care services that have been fully integrated.
VIDEO CONSULTATION
SELF CARE
HEALTHCARE PROFESSIONALS
IN THE COMMUNITY
999
EMERGENCY DEPARTMENTS
DIRECT APPOINTMENT
BOOKING
FACE-TO-FACE
DENTIST
MENTAL HEALTH CRISIS
TEAM
COMMUNITY PHARMACISTSOUT-OF-
HOURS GPs
SPECIALISTS
CLINICAL ADVICE SERVICE (CAS)
Clinical NavigatorsAllied Health ProfessionalsGeneral Practitioners (GPs)
Advanced Nurse PractitionersMidwives / Paediatric Nurses / Dental Nurses
Community Psychiatric NursesSpecialists Advanced Paramedics
Palliative Care NursesPharmacistsED Clinicians
ADVICE / REFERRAL
VIRT
UAL LIN
K TO
SPEC
IALIS
T ADVI
CE
HEALTH ADVISOR
NHS 111

KE
Y S
ER
VIC
E I
NIT
IAT
IVE
S Over the life of this Strategy the Trust is planning to deliver a number of strategic initiatives. Delivery of these will support improvements in patient care, the wellbeing of our people and for the operation of the Trust. Presented here under six key themes, these initiatives represent the strategic activities that will influence how we use our resources to best effect to meet patient need. The materiality of each initiative is indicated by the size of each segment.
14
O U R P E O P L E
P E R F O R M A N C E
PA
TIE
NT
SA
FE
TY
, C
AR
E &
O
UT
CO
ME
ST
EC
HN
OL
OG
Y
E X I ST I N
G
S E R V I CE S
E F F I CI E
N C Y
A N D
B E S T PR A C T I C
E
Time
To Care
Transition Plan
Trust Cultural Review
Five Year Workforce ModelLeadership
Training Needs
Analysis Wellbeing
Initiatives
Performance
Improvem
ent
Plan
Exp
lori
ng
Clin
ical
In
form
atio
n
Am
bulance
Quality
Indicators
Ro
le of
Clin
ical H
ub
sA
lways
Events
Resp
on
der
Lifting
Schem
e
Dorset I
ntegra
ted
Urgen
t Car
e
Service Change
Impact
Vir
tual
Tri
age
Lord
Car
ter
Revie
w
TRUST
STRATEGIC
INITIATIVES

strategy2018/19 to 2020/21
Trust
Our People
Trust Cultural Review: The Trust is working in partnership with Unison, our recognised union, to engage with a leading academic to undertake a Trust wide cultural review. This review will seek to better understand the culture of our organisation and the views of our people. The findings of this review will be used to inform initiatives which will support the development of our values and behaviours and build on the ongoing work of our people to support one another and embed compassion, professionalism and integrity in everything we do. Intention: To better understand the culture of our people and take informed steps to improve and develop our culture in support of the Trust’s values. Five Year Workforce Model: This model is a key piece of work that underpins the development of future recruitment and training plans for A&E 999 operations. The model will map recruitment need and supply routes ensuring the Trust has the right numbers of people in these key roles. In addition the Workforce Model considers future changes that may impact on recruitment plans and supply routes over this time period in order that the Trust can respond quickly and effectively to any changes in the plans. This can include internal changes or external factors such as changes to the wider health and care system. Intention: To ensure the Trust is able to provide a sustainable pipeline of people over the next five years taking into account the changing system in which the Trust operates. Leadership Training Needs Analysis in support of Reshaping Operations: Reshaping operations seeks to achieve a resilient and sustainable structure for 999 A&E operations. The development of this structure is supported by a significant organisational change programme. This includes the creation of new roles and an assessment process to ensure we have the right people who are able to respond effectively to the challenges and opportunities facing the Trust over the coming years. The information gathered through the assessment process will inform a Training Needs Analysis from which leadership development and training events will be based to ensure our leaders are supported to provide effective and compassionate leadership for the Trust and our people.
Intention: To ensure we have a comprehensive understanding of our operational leaders’ strengths and development areas on which future leadership training will be based. Development of Proactive Wellbeing Initiatives: Improving the wellbeing of our people is a key strategic intention. Throughout 2018/19 and beyond more focus will be given to proactive support of wellbeing to ensure our people stay well and are supported by the Trust to do so. This will involve the development of a training plan to assist all our people to identify and support individual wellbeing, as well as expansion of the Staying Well Service and our Peer Support Guardians to allow them to be better equipped in the improvement of wellbeing across the Trust. We will also commence the first Wellbeing Engagement Group to seek feedback on current initiatives and involve our people in the development of new ideas and initiatives throughout the year. Intention: To ensure we work to support and improve the wellbeing of our people through a range of proactive initiatives.
Patient Safety, Care and Outcomes
Ambulance Quality Indicators (AQIs): All ambulance services in England are measured by, and report against, a range of system and clinical quality indicators. These focus on patient safety and outcomes linked to call handling, response, patient transport and clinical assessment and treatment. The AQIs were updated in 2017/18 to include new clinical measures and indicators linked to the new national ambulance response standards. Further changes are expected during 2018/19 as a result of the ARP Spring Review by the Secretary of State. These are likely to include the introduction of new clinical indicators linked to the identification and treatment of sepsis and the response to patients that have fallen and are still on the floor. In addition changes are likely to the existing suite of clinical indicators including ST-elevation myocardial infarction (STEMI – a type of heart attack), Return of Spontaneous Circulation (ROSC) which monitors the number of patients who suffer a cardiac arrest and who are subsequently resuscitated and the heart restarts prior to their arrival at hospital.

Intention: Once published, work to deliver the new clinical quality indicators in line with national guidance Role of Clinical Hubs: The Trust believes that the Clinical Hubs have a key role to play in enabling the safe and effective care of patients – especially in the context of increasing demand. Within the Clinical Hub teams, the input from senior clinicians (Clinical Supervisors) is extremely important. Their higher clinical skills and experience enables enhanced prioritisation of patient needs, and better clinical risk management. There are a number of different roles that they can perform. This includes identifying patients who can safely be dealt with by telephone advice or signposting onto more appropriate providers of care (hear and treat). Over the life of this Strategy the Trust will consider how the skills and knowledge of Hub clinicians, and those clinicians performing remote triage, can add further value in the triage and treatment of patients. This will also form part of the overall considerations into the target operating model for the Trust. Intention: To further understand in detail which patients can be safely and more appropriately managed through the ‘hear and treat’ pathway.
Community First Responders lifting scheme: The Trust continues to face challenges in providing a timely response to patients who have fallen and not injured themselves. The concept of using Community First Responders (CFRs), who are members of the community who operate in a voluntary capacity, to improve the response to this patient group was developed and tested through a lifting scheme feasibility study during 2016/17. The distinction between normal practice and the lifting scheme is that trained CFRs are authorised to lift patients with the use of a lifting device using a falls decision support tool. Following positive results, a Trust wide pilot was initiated during 2017/18 and was subject to a robust clinical and operational evaluation. This concluded that the lifting scheme contributes positively towards improved patient care, the delivery of national ambulance clinical quality indicators and response standards. Intention: To rollout the CFR lifting scheme, over the life of this Strategy, from the current 17 cells to an increased number of CFR groups across the operational area.
16

Always Events: Always Events are defined as those aspects of the care experience that should always occur when patients, their family members or other care partners, and service users interact with health care professionals and the health care delivery system. The Always Events approach is to accelerate improvement efforts to enhance experiences of care for patients, their family members or other care partners, and service users – the goal is for patients and service users to have an “Always Experience.” The creation of Always Events is a methodology for achieving this goal. A key aspect of Always Events is that patients, their care partners, and service users have identified the event as fundamental to improving the experience of care. A fundamental principle in co-designing Always Events is to move from “doing for patients” to “doing with patients” (co-designing). This priority therefore focuses on proactive engagement and will be developed, tested, implemented and expanded over a two year period from 2018/19. Intention: To develop Always Events for a specific patient group to enhance the delivery of care.
Efficiency and Best Practice
Lord Carter Review: The identification of efficiency or productivity savings and models of best practice is the primary focus for one national programme being led by NHS Improvement (NHSI), an NHS regulator. Delivered under the banner of the Ambulance Sector Operational Productivity Review (Lord Carter Review) the programme aims to identify what good looks like in delivering 999 ambulance services, available sector metrics for benchmarking and ‘early wins’ in terms of reducing variation and increasing productivity. Specifically the programme is reviewing; workforce and the optimum model for delivery, Trust operating models, digital and technology use and operational and clinical productivity. The Trust has been fully engaged in this work programme since its inception in 2017/18. This process has provided the Trust with a number of key themes to consider in terms of its cost efficiency programmes and remains a key work stream for 2018/19 onwards. The Trust expects the Review to have a material impact on the structure and form of ambulance service provision going forward
with formal outputs being published from 2018/19. The outputs will directly influence the target operating model for the Trust. Intention: To formulate Trust actions plans in response to the formal publication of outcomes from the Lord Carter Review, and embed recommendations as required. Time to Care: In February 2018 the Trust launched a new initiative called ‘Time to Care’ focused on working together to improve the wellbeing of our people and job satisfaction. The demands faced by our teams on a daily basis are significant and growing. It is vital we improve the working environment in a way that sustains the delivery of safe and high quality services that provide benefits for our people, patients and the Trust. Using team feedback a number of key themes have been identified most which are within the control of the Trust and achievable, although some will prove more challenging to deliver than others and may require an ‘invest to save’ approach. Those issues that have a high impact on the wellbeing of our people and job satisfaction will also impact on operational service delivery. Over the life of this Strategy it is vital that ‘Time to Care’ continues to develop momentum, with managers taking responsibility and ownership of actions. The approach must focus on developing and building relationships between teams and departments through positive engagement. Intention: For Time to Care to become embedded within the Trust as a sustained approach to staff engagement of our people and continuous improvement.
Performance
National Planning Guidance 2018/19 states that the new ambulance response time standards must be met by all trusts by September 2018. The Trust’s aim is always to deliver national standards. However, notwithstanding the efforts being made by the Trust in focusing on productivity gains and cost reductions, there is a very significant resource gap in meeting the requirements
strategy2018/19 to 2020/21
Trust

of the national standards. To deliver performance improvements, and where possible reduce the Trust response times to all categories of incident, the Trust has undertaken a three phase approach. Phases one and two were completed during 2016/17 and 2017/18 and comprised at a high level of a Trust wide rota review to align rotas and fleet ratios to meet the new (increased) demand profiles and the delivery of Quality Performance Improvement Plans to improve patient safety and performance by maximising resource availability. Phase three, launched in February 2018 and continuing to be developed in 2018/19, is referred to as ANITA; Achieving National standards through Investment and Transformation Actions. ANITA is divided between internal activity made up of the Performance Improvement Plan (PIP) and a trajectory, and a co-owned Transition Plan with commissioners. Internal actions will deliver performance in line independent modelling with the Transition Plan moving the Trust to delivering national standards. Performance Improvement Plan (PIP): The main areas of focus for the PIP include:• Reducing extended response times• Improving Call Answering performance• Delivering appropriate improvements in the
proportion of incidents resolved through the Hear and Treat outcome (i.e. telephone advice/referral)
• Recruiting Hub Clinicians to fill current vacancies• Reducing the impact of inappropriate activity
transferred from NHS111 to the ambulance service• Improving the consistency of frontline resourcing
levels in line with operational plans• Delivering improvements in operational call cycles
where appropriate• Supporting changes to the Trust operating model that
will be embedded during delivery of the Transition Plan
Intention: During 2018/19, through the PIP and a performance improvement trajectory, deliver performance levels as determined achievable by independent modelling. Transition Plan: Whilst the ambulance sector is intensely focused on improving efficiency, and the Model Ambulance programme as part of the Lord Carter Review is welcomed, the paradigm shift of the new ambulance response standards comes with a significant investment requirement that cannot be met through internal
efficiencies alone. In recognition of this a ‘Transition Plan’ will be jointly developed and owned, between the Trust and its Commissioners, that will set out the steps to be taken in closing the funding gap and move the Trust from a position of delivering independently modelled performance levels to achieving national response standards. The Transition Plan will have a life of two years covering the period 2018/19 and 2019/20. The Trust is at a very early stage in the development of the Transition Plan and although Commissioners recognise a funding gap they have not reached agreement on additional investment. As part of delivery the Transition Plan there will be a strong focus on the target operating model for the Trust including the optimal fleet mix, type of vehicle, resource modelling and estate. Intention: Subject to sufficient investment and Trust ability to embed transformation the transition plan will enable the delivery of all national performance standards by April 2020
Technology
Exploring Clinical Information: With a finite number of ambulance resources available to send to incidents, it is vitally important that the response priority determined by the MPDS triage system, reflects the actual severity of condition found when an ambulance response is sent. The Trust has developed a data tool that links how emergency 999 calls are initially triaged in the Clinical Hub, with the clinical data collected from every patient who is assessed by an ambulance clinician through the electronic care system (ECS). Using data from over 250,000 incidents, the tool examines a wide range of factors to calculate a score for each patient that represents how severely ill or injured they are. This allows the average severity of patients within each MPDS category to be calculated. The tool has already helped make evidence based decision for enhanced hear and treat and an end of shift allocation trial, and will feed into the national review of ARP categorisations.
Key initiatives will include; utilising the data to further define triage codes that can be managed more effectively within the healthcare system; utilising the data to better understand whether particular triage codes could be signposted to clinicians or specific resources such as Specialist Paramedics; and evaluating the impact of both developments and evidence benefit/harm.
18

Intention: To use the tool to further refine the effectiveness of clinical triage within the Clinical Hubs, in order to improve the appropriateness of the response that patient’s receive. Remote Triage:To enable the Trust to effectively and dynamically meet the demand it faces whilst improving resilience, there is a growing requirement for alternative and flexible models for the management of 999 calls. Currently all triage of 999 calls takes place within dedicated clinical hubs that co-locate call taking, clinical oversight and dispatch functions. However this can create challenge in time of extremis, major incident or extraordinary events where geographical, logistical or technological issues can impact on business continuity. Remote triage enhances system accessibility to a wider clinical resource and facilitates flexible working arrangements for our people. In addition it improves our ability to engage with a wider cohort of health and social care professionals by providing clinical assessment and resource management functionality away from current hub locations. Remote triage was enabled at six of the larger stations during 2017/18 and allows clinicians on station premises to access the call queues and support clinical advice requests, thereby functioning as if they were in the clinical hub. The initial step for this project provides a limited web interface so that Paramedics can update the notes on calls. However phase two allows clinicians to undertake all hub tasks and bring a call to conclusion including the upgrading / downgrading or closing calls as appropriate. The final phase will provide remote triage functionality via a laptop and a smart phone, so that Paramedics can work from any remote location as if they were in the clinical hub.” Intention: To deploy remote triage to all large and medium sized ambulance stations across the south west by 2019/20 and provide key personnel with direct access from other locations via laptops as by 2020/21.
Existing Services
Dorset Integrated Urgent Care: The Trust has significant experience and strengths in delivering integrated urgent care though both its emergency ambulance and urgent care services. The Trust’s existing urgent care contracts are considered to be strong and effective with the benefit of close working
and alignment to the Trust’s 999 emergency services. An the incumbent provider of these services there is an opportunity for the Trust, in partnership with other local NHS providers, to develop and embed a truly integrated system to better meet the current and future health needs of local people. The Dorset NHS111 and Out of Hours Contracts were extended to the 31 March 2019 with NHS Dorset Clinical Commissioning Group commissioning a replacement service known as the Integrated Urgent Care Service. During 2017/18 the NHS Trusts in Dorset (Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust, Poole Hospitals NHS Foundation Trust, Dorset County Hospitals NHS Foundation Trust, Dorset Healthcare Universities NHS Foundation Trust and the Trust) formed an alliance to respond to the tender. The outcome of the bid will not be known until quarter two of 2018/19. Intention: To retain the existing Urgent Care Contracts in Dorset as part of a partnership bid Service Change Impact: Through the development of ‘place based plans’ the combined impact of both sustainability and transformation partnerships and integrated care systems could be material for the Trust over the life of this Strategy. Service changes that are being proposed could create changes in activity, the location of a service or facility or the loss of ambulance resources in a given area. These changes can materially alter the way in which the Trust delivers its services across the region. The potential for impact has been recognised by Commissioners who have introduced a formal mechanism to review proposed service changes. This framework will be strengthened through 2018/19 and will be the primary route through which the Trust addresses service change considerations and implications across the region.
Intention: That the Trust escalates those proposed services changes, that have a material impact on core services, to Commissioners for consideration in line with the contract.
strategy2018/19 to 2020/21
Trust

EN
AB
LIN
G S
TR
AT
EG
Y O
BJE
CT
IVE
S To support delivery of the Trust’s strategic aims and objectives, including the key service initiatives, the Trust has in place a number of ‘enabling strategies’. These set out how the corporate and support services in the Trust will work with clinical and operational teams to deliver and improve patient care. A high level summary of the strategic intentions each enabling strategy is focused on delivering over the next three years is set out here.
Finance
The primary aim of the Finance Strategy is to balance the delivery of performance and improvements in quality alongside sustaining financial health. Strategic intentions of this Strategy are to: • Continue to set sustainable breakeven plans,
recognising that increasingly the Trust will be required to place reliance on non-recurrent measures to support delivery
• Review annually the Trust’s position in terms of NHS Improvement’s Control Total to determine feasibility
• Continue to only ‘spend what we have’• Continued to invest in the replacement and renewal
of Trust infrastructure to ensure continuity of the operating model
• Continue to take a prudent view on capital utilising depreciation and land sales as the source of funds
• Alongside the Quality Strategy, work to a set of ‘affordable quality principles’ to
reconcile issues of performance, quality and money across the Trust. The overriding principle being to ‘do no harm’
• Implement the new patient level costing system (PLICS) for ambulance services to support the national identification and benchmarking of actual costs
• Create a programme of work to reduce variation, increase efficiency and better understand the Trust’s performance, compared to its peers, across a range of metrics related to productivity and quality of care. This will be developed following the publication of the model ambulance portal in April 2019 and the National Operational Productivity Review (Lord Carter Review)
20

People and Culture
The People and Culture Strategy aims to devise a three-year programme that progresses our key strategic intentions to ensure the Trust has the ‘Right People’; ensuring our people have the ‘Right Skills’; ensuring our people have the ‘Right Values’. Strategic intentions of this Strategy are to:• Provide sustainable workforce plans, including a five
year workforce model, aligned to business priorities and succession planning
• Recruit and retain talented people who share the Trust values and behaviours and continued development of our people to ensure that they are best placed to continue to provide quality services to our patients
• Deliver a team with the prerequisite skills and experience to ensure responsiveness and effective patient care through clear career pathways, ensuring we can nurture, develop and retain talented individuals
• Eliminate discrimination, positively engaging with under-represented groups and delivering initiatives to ensure inclusive teams and a more diverse workforce
• Support the health and wellbeing of our people, responding to the challenges of working longer and the external factors that can impact the health of our teams
• Increase workforce flexibility, resilience and capacity and engaging meaningfully with our people, celebrating success and encouraging a culture of compassion
Quality
The primary aim of the Quality Strategy is to develop a culture for quality that is based upon a patient centred approach where compassion and care are a given. Strategic intentions of this Strategy are to:• Achieve at least a ‘good’ in the next CQC inspection,
supported by a desire to be demonstrating elements of outstanding, and to be outstanding within the next five years
• Review and update patient safety policy and management focused on the serious incident process, rebranding it to become a ‘learning review’ with greater engagement of our people and visibility of the actions arising from serious incidents
• Improve the timeliness of response to complainants• Implement annual quality priorities as outlined in
the Quality Improvement Plan, supported by the establishment of a continuous improvement group, and test the impact of actions taken
• Work to a set of ‘affordable quality principles’, alongside the Finance Strategy, to reconcile issues of performance, quality and money across the Trust. The overriding principle being to ‘do no harm’ and to drive high quality and efficient care
• Improve the experience of patients with mental health and end of life care needs including understanding their experience of 999 service and evaluating the impact of actions to drive further quality improvements
• Develop automated solutions within the safeguarding referral management system, develop relationships with Safeguarding Boards and ensure compliance with statutory duties
• Embed quality from frontline to the Board expanding the learning from experience and quality buddy processes to ensure quality and risk are embedded within operational practice
• Identify further areas of outstanding practice in relation to health and safety requirements building on the work of the Health and Safety Improvement plan.
Clinical
The primary aim of the Clinical Strategy is to deliver safe and effective clinical care to achieve the best possible patient outcomes. Strategic intentions of this Strategy are to: • Deliver improvements in Cardiac Arrest Management,
with an aim over the longer term to improve survival to discharge from hospital, including:
◆ Improved identification of this group of patients in the Clinical Hub
◆ Better targeting of appropriate resources to dispatch to the scene
◆ Better on scene management of the cardiac arrest patients
◆ Better post resuscitation care• Maximise the value of senior clinician input into the
work of the Clinical Hub including: ◆ Better understanding the possible roles that can
be performed by clinicians in the hub ◆ Identifying the key training needs of these
individuals and the best way to monitor clinician performance
• Work to refine and improve the accuracy of telephone triage in the Clinical Hub using outcome data taken from the electronic patient record
strategy2018/19 to 2020/21
Trust

• Work to improve the experience of patients with mental health needs including:
◆ Reviewing and improving the triage of patients contacting our services with a mental health crisis
◆ Reviewing the provision of mental health nurses within the Clinical Hub to provide access to a diverse range of clinicians
◆ Reviewing the ability of front line responding clinicians to access specialist mental health advice, including working to enable access to developing clinical advice services and specialist clinicians
• Work to improve the experience of frail patients including:
◆ Working towards identifying frailty during every contact with a healthcare professional, making every contact count, and promoting the onward referral for patients identified as frail or who have fallen to prevent deterioration and support rehabilitation
• Work to improve the experience of patient with end of life care needs including:
◆ Evaluating the Cancer Care Development Project, run with McMillan Cancer Support Teams, to explore sustainable end of life and advanced care planning options moving forward
• Work to improve Trust access to relevant patient information from other healthcare sources including:
◆ Developing, through various partnerships, access to shared patient records including supporting developments associated with the Summary Care Record with Additional Information
Digital
The primary aim of the Digital Strategy is to further develop the Trusts digital capabilities, enhancing and addressing any weaknesses through the smart use of technology. Strategic intentions of this Strategy are to:• Replace the core ambulance radio communications
systems with Emergency Services Multi Communication Protocol (ESMCP) as part of a national programme
• Replace the current ambulance electronic patient record and vital signs services contract following expiry in December 2019
• Implement business intelligence enhancements to ensure the optimum use of resources, attainment of national standards and improve forecasting and clinical capabilities
• Enable care record integration with wider stakeholder groups to ensure the Trust is clinically informed about its patients and to support the onward transfer or notification of care episode
• Align with national control room priorities to deliver savings through economies of scale and deliver more effective solutions using collective resource
• Ensure our systems and our data is protected from the ever increasing cyber threat
• Replace the paper based systems and processes for medicines management to optimise and ensure the safe use of medicines within the organisation
Estates
The primary aim of the Estates Strategy is to create cost effective and fit for purpose estate function with an infrastructure capable of supporting current and future models of service delivery. Strategic intentions of this Strategy are to:• Provide premises that are adequate, functionally
suitable and fit for purpose with appropriate and effective maintenance arrangements and space utilisation
• Identify and appraise station configurations across the Trust, and the associated resource deployments, with the aim of improving the cost effectiveness of cover and the efficiency with which the estate is used
• Consider, and act upon as appropriate, the implications of the national ambulance productivity review with regards to creating an efficient estate that maximises operational performance
• Replace or refurbish properties and facilities with high backlog maintenance, poor functional suitability and utilisation or are approaching the end of their physical and economic life
• Ensure that there is a fit for purpose estate to support clinical hubs, remote triage, operational management and training delivery
• Undertake a review of the ‘support services estate’, including vehicle workshops, considering location, capacity, effectiveness and long term suitability
Fleet and Logistics
The primary aim of the Fleet and Logistics Strategy is to provide a safe and well equipped fleet that supports the Trust in delivering 24/7 emergency healthcare provision. Strategic intentions of this Strategy are to:• Consider and move towards the optimal vehicle ratio
(vehicle type and numbers) to support operational
22

delivery under the new national ambulance standards• Review the Trust’s vehicle replacement and
maintenance programme, including vehicle design and life cycle options, to ensure they remain fit for purpose and opportunities are realised in a timely manner
• Align future vehicle procurement against national direction
• Consider, and act upon as appropriate, the implications of the national ambulance productivity review with regards to creating efficient fleet and equipment policy that maximises operational performance and reduces variation
• Ensure Trust medical devices and other equipment meet the requirements of the user and where appropriate equipment is standardised, variation reduced there are fit for purpose maintenance and replacement cycles
• Provide an effective and efficient logistics system and process to ensure frontline individuals have the equipment and supplies when and where they require them
• Review the Trust’s stores provision and distribution operating models, to ensure they are fit for purpose and support efficient provision of consumables
• Review the Trust logistics operating model to ensure the operating model for stores and make ready are fit for purpose and support efficient provision of vehicles and equipment
Emergency Preparedness, Resilience and Response Strategy (EPRR)
The primary aim of the EPRR Strategy is to ensure the Trust continues to provide a resilient and responsive service to its patients. Strategic intentions of this Strategy are to:• Comply with the Civil Contingencies Act 2004, the
NHS England EPRR Framework and Core Standards and the requirements of the Care Quality Commission
• Develop a Trust wide understanding of the role of emergency preparedness, resilience and response providing direct support to wider A&E 999 operations as required supporting to the delivery of key
performance indicators and the A&E Operating Plan• Secure Commissioner’s commitment and support
to deliver a full robust emergency preparedness programme
• Comply with all internal and external requirements to agreed timescales
• Pursue operational efficiencies in collaboration with the Police, Fire and Rescue and other emergency services to improve performance, productivity and value for money and fulfilling our legal duties under the Policing and Crime Act 2017
• Ensure appropriate procedures are in place for the storage, retrieval and disposal of all emergency preparedness documents including adaptable emergency preparedness plans that incorporate lessons identified from emergency preparedness events and organisational restructures
• Undertake a training needs analysis of all Trust individuals, relevant to the arrangements contained within the plans and emerging risks and threats and deliver, and evaluate the resilience education and development programme once delivered
• Ensure appropriate operational emergency preparedness resources and equipment are in place with all geographical areas fully supported as per resilience requirements and needs
• Ensure all CBRN and hazardous material capabilities are supported geographically and risk assessed by the Trust and meet local and regional requirements, support national capabilities and support response, sustainability and recovery phases of all relevant incident types including event cover
• Ensure the Trust MTFA capabilities are supported geographically, are risk assessed by the Trust and meet local and regional requirements with fully trained and exercised MTFA individuals, resources and equipment
strategy2018/19 to 2020/21
Trust

FIN
AN
CIA
L P
LA
N
24
• The principles and objectives of the Finance Strategy • Financial change drivers • Sources of funding• Financial modelling
Financial Change Drivers
For the Trust and its services there are a number of elements that can influence the plan both in and across financial years. The key cost driver is pay at around 75% of total cost. Other non-pay cost drivers are driven by the Enabling Strategies and the level of required capital investment including within the Trust fleet, estates and technology. The financial plan will need to remain flexible to respond and mitigate changes across these elements.
Sources of funds
The source of funds to any change in cost drivers will be from the internal Cost Improvement Strategy or external funding.
Cost Improvement Strategy
The Trust has an internal governance process for the management and identification of the Cost Improvement Strategy. However one of the key elements in the identification of future cost improvements will be to implement the outputs from the Lord Carter Review on Operational Productivity, as led by NHS Improvement. One of these outputs will be the creation of a Model
Pay award, Incremental drift, Process changes
Pay award, Incremental drift, resource changes, Recruitment, agency
Pay award, Incremental drift, resource changes, Recruitment, Band 6 Paramedic, Structures, third parties
Support Pay
UCS Frontline Pay
A&E Frontline Pay
Salary recharges, events, commercial training
Tenders, Activity, Tariff, CQUIN
Activity, Marginal Rate, Tariff, CQUIN, HART income
Other Income
UCS Income
A&E Income
Third party use see A&E Frontline, Clinical Negligence Claims, Outsourcing e.g. Payroll, Occupational Health
CAD, Triage, Communications, Microsoft, Resilience, Maintenance, LIcence
Number of vehicles, activity levels, Compliance
Location of vehicles, Compliance, Lease vs. Buy
Vehicle number, design, mix, Fuel, vehicle insurance premiums, Lease vs. Buy, In-house vs. Outsource
Daily cash level
Capital plans - Fleet, Estates, IT, Medical, Asset Life
Other
ICT
Medical
Estates
Fleet
Public Dividend
Depreciation
INCOME
INC
OM
E A
ND
EX
PEN
DIT
UR
E
PAY
NON PAY
The financial plan over the life of this Strategy will be influenced by a number of factors:

strategy2018/19 to 2020/21
Trust
Ambulance Trust portal that will enable effective benchmarking against nationally agreed data sets across the sector.
This will capture a number of key thematic areas including: demand; response; operational response supported by compartments covering workforce, fleet and operational support. Potential headline metrics are (adjusted) ‘cost per call’, ‘cost per incident’ and ‘staff minutes assigned per incident’. These can then be split between pay and non-pay.
Commissioning Development
As part of the Ambulance Improvement Programme there is a national work stream focused on reducing variation in ambulance commissioning and service provision.
This will be achieved through the development of a consistent commissioning framework and
accompanying guidelines including a core 999 specification to support a more consistent model of ambulance commissioning and service provision. Once published the Trust will work with its local commissioners to implement these recommendations and refine the commissioning process.
Financial Modelling
NHS Improvement are in the process of developing an ambulance sector specific financial model, which will include demand and cost pressures specific to the ambulance provider sector for the period from 2017/18 to 2022/23. The Trust will maintain and utilise financial planning models to support its planning processes.

ST
RA
TE
GIC
RIS
KS
26
The Trust has undertaken a review of risks and has grouped them into eight new overarching themes that have been approved by the Trust’s Audit and Assurance Committee. The themes have been identified to enable an increased clarity, understanding and awareness of Trust risks among individuals and managers and to move to a position of increased ownership of risks. The identified risk themes (each of which have the related risks sitting within them) are presented in the image here.
Safety of care to patients
Strategic Risks
Financial Position
ReputationBusiness
Continuity
Failu
re to
M
eet R
egul
ator
y
Requ
irem
ents
Risks that can negatively affect the financial stability of the Trust both in year and longer term
Risks that arise from business continuity events that could affect the Trust’s ability to provide and maintain its services
Risks that could result in the Trust not meeting its core requirements as set out by regulation or law
Risks associated with adverse media or negative stakeholder engagement that can impact on the Trust’s reputation

One of the most significant strategic risks, and a risk to patient safety, remains the delivery of the national ambulance standards. The achievement of these standards remains challenging due to the gap in the Trust’s contractual position and in some cases the maturity of local urgent and emergency care systems; this creates an underlying risk to the safety of patients and creates the potential for patient harm. This potential for harm manifests in a number of different elements of the call cycle. This includes the triage process, the stacking of calls (including the clinical capacity to review extended response times) and the lack of resources available to respond to patients in a timely manner leading to a delayed response to patients. Whilst there will remain a risk to patient safety and therefore a risk of potential patient harm, the Trust continues to focus on ensuring that all possible actions are taken to mitigate, as far as possible, the impact of delays on patient outcome. Over the next three years, and with the procurement of the new risk platform, the focus will be on embedding risk within frontline operational areas. The aim will be for managers to access, influence and understand the risks to the organisation and therefore patients and a greater focus on ensuring actions, controls and risk are visible to the frontline. A fundamental part of the Trust’s Risk Management Strategy is to ensure that the quality of care is monitored and improved through a number of mechanisms; this includes the development of a proactive engagement process with our teams. The will continue to proactively identify, mitigate, monitor and review risks to governance of the organisation, and to the safety and wellbeing of its service users and our people.
strategy2018/19 to 2020/21
Trust
Strategic Risks
Safety and wellbeing of our People
Lack of available
workforce
Patie
nt h
arm
du
e to
del
ayed
re
spon
ses
Risks that the effect the quality of care provided to patients that can in turn impacts on patient safety and experience
Risks that impact on the
safety and wellbeing of
our people and teams
Risks that present workforce challenges in terms of
recruitment difficulties,
abstractions, vacancies and the
potential for a lack of appropriate
skills.
Risks that could impact on patients
as a result of delayed ambulance responses and clinician contact.

99
9
Choking.Chest pain.
Blacking out.
Blood loss.
Unwell?Unsure?Confused?
Need help?
Vomiting.Ear Pain.Stomach ache.
Back ache.
Diarrhoea.
Runny nose.
Painful cough.
Headache.
A&E or 999Emergencies only
Call 111out of hours
GP Surgery
Pharmacy
© South Western Ambulance Service NHS Foundation Trust 2018
If you would like a copy of this report in another format including braille, audio tape, total communications, large print, another language or any other format, please contact:
Email: [email protected] Telephone: 01392 261649 Fax: 01392 261560
Post: Marketing and Communications, South Western Ambulance Service NHS Foundation Trust, Abbey Court, Eagle Way, Exeter, Devon, EX2 7HY

Trust Public Board of Directors Meeting – 25 May 2018 Page 1 of 1
Trust Public Board Of Directors Date: 25 May 2018
Paper Title: Integrated Corporate Performance Report (ICPR)
Prepared by: Paul Quick, Performance Manager Jennie Kingston, Deputy Chief Executive/Executive Director of Finance
Presented by: Jennie Kingston, Deputy Chief Executive/Executive Director of Finance
Action: Information and Assurance
Recommendation:
Report presented for information, discussion and feedback.
Executive Summary:
To provide an overview of Trust performance and identified key performance metrics for the month of April 2018.

Page 1 of 8
Integrated Corporate Performance Report
April 2018

Page 2 of 8
Integrated Corporate Performance Report
Introduction 1.
The Integrated Corporate Performance Report (ICPR) includes: 1.1.
An Executive Summary - highlights the key areas of note and interest to the Trust Board. This summary includes details of any areas of significant exception where the Trust is either ‘off plan’ or below target, together with the key actions that are being taken to address under-performance;
A RAG rating Dashboard - summarises the RAG ratings of the key metrics monitored by the Trust. In order to promote consistency these are ordered according to the key headings contained within the A&E (999) Operating Plan;
An Information Pack – the comprehensive data set includes graphs and tables covering the full list of KPIs and metrics monitored by the Trust.
Ambulance Response Programme (ARP) 2.
New standards, indicators and measures have been introduced through the ARP for 2.1.publication in the NHSE Ambulance Quality Indicators. All ambulance trusts in England were required to commence reporting against the new standards by 30 November 2017.
Initially the standards proposed are to be used for monitoring purposes only to enable 2.2.ambulance trusts to update their operating models to deliver the new performance standards.
SWASFT implemented the new response time reporting standards required for ARP v2.3 2.3.with effect from 23 November 2017. This report therefore includes data in relation to the old metrics up to and including 22 November 2017 and reporting on the new metrics with effect from 23 November 2017. Further details on the new performance standards can be found in the Information Pack included with this report.
Following a successful period of reporting by all ambulance trusts in England a review of the 2.4.metrics was completed during April 2018 and a number of revisions to the current AQI guidance documentation are expected. Full details of these changes, including the revised guidance documentation are expected to be published during May 2018.
On receipt of the updated guidance the Trust will then be required to undertake a number of 2.5.internal process and reporting changes to comply with the updated metrics. Further updates will be included within this report once the final version of the guidance documentation has been released.
A&E (999) Performance 3. A&E Incident Numbers
A&E incident numbers in April 2018 were 1.24% higher than those reported in April 2017 3.1.but were 0.83% lower than the contracted volumes for April 2018.

Page 3 of 8
Whilst overall incident numbers were 1.24% above the volumes reported in April last year, 3.2.variance in the year on year movements between the CCG areas continues to be seen. In Somerset CCG incident numbers increased by 9.65%, were 4.52% higher in Swindon CCG and 3.96% higher in South Devon & Torbay CCG. In comparison activity in Bristol, North Somerset and South Gloucestershire CCG was 1.19% lower than the incident numbers reported in April 2017.
Activity levels during March 2018 increased during the periods of adverse weather, but 3.3.during April 2018 the weekly number of incidents returned to expected levels averaging 17,100 incidents per week. Whilst lower than the levels seen last month, it should be noted that the weekly incident numbers are still significantly higher than the numbers seen in Quarter 1 and Quarter 2 of 2017/18 when weekly activity was consistently below 17,000 incidents per week.
ARP Response Times Response times in April 2018 were above the national standards, however all response 3.4.
times showed improvements when compared to the response times reported in March 2018.
The summary of performance against the response time metrics on a weekly basis from 12 3.5.March 2018 to 13 May 2018 is included within the table below.
Week Commencing
National Standard 12 Mar 19 Mar 26 Mar 2 Apr 9 Apr 16 Apr 23 Apr 30 Apr 7 May
Category 1 Mean Response Time (Mins)
7 minutes
9 mins 19 secs
9 mins 12 secs
9 mins 01 secs
8 mins 58 secs
8 mins 39 secs
8 mins 14 secs
8 mins 10 secs
8 mins 24 secs
8 mins 17 secs
Category 1 90th Centile Response Time (Mins)
15 minutes
16 mins 52 secs
16 mins 51 secs
16 mins 30 secs
16 mins 43 secs
15 mins 37 secs
15 mins 02 secs
15 mins 26 secs
15 mins 44 secs
15 mins 39 secs
Category 2 Mean Response Time (Mins)
18 minutes
30 mins 07 secs
30 mins 35 secs
25 mins 31 secs
25 mins 51 secs
23 mins 47 secs
22 mins 39 secs
21 mins 01 secs
24 mins 53 secs
24 mins 49 secs
Category 2 90th Centile Response Time (Mins)
40 minutes
62 mins 58 secs
64 mins 37 secs
52 mins 31 secs
53 mins 23 secs
49 mins 04 secs
47 mins 21 secs
42 mins 54 secs
51 mins 30 secs
52 mins 06 secs

Page 4 of 8
During April and leading into May 2018 the Trust has seen improvements in the weekly 3.6.response times for the most serious patients (Category 1 and Category 2) as a result of actions taken under the Quality Performance Improvement Plans (QPIP) which commenced in Quarters 1 and 4 of 2017/18 . Further improvements are anticipated as a result of actions outlined in the Performance Improvement Plan (further details provided later in this report).
Mean Category 1 incident response times across the Trust show expected variation in the 3.7.month of April 2018, with the longest mean response time in Kernow CCG (10 mins 30 secs) compared to the shortest time of 6 mins 48 secs in Swindon CCG.
It is important to note that the Category 1 incidents represent around 6.5% of all incidents 3.8.received by the Trust (equating to around 160 to 170 incidents per day).
The ARP performance figures for ambulance trusts in England are included within the 3.9.Information Pack, the benchmarking for Category 1 Mean Response Times in April 2018 is included in the graph above for reference.
Whilst the Trust has seen improvements during April 2018, it remains in the lower quartile 3.10.for Category 1 Mean and other response time metrics. It is acknowledged that some of this national variance will be due to the extremely rural nature of the South West geography, the Trust has made contact with other ambulance trusts to identify any best practices which may assist in reducing the mean response times closer to the 7 minute response time target, in particular information on dispatch processes and systems.

Page 5 of 8
Actions to Deliver Performance Improvement 4.
To deliver performance improvements and where possible reduce the Trust response times 4.1.to all categories of incident the Trust has undertaken a three phase approach:
Phase One - Trust wide rota review to align rotas and fleet ratios to meet the new (increased) demand profiles and tackle inefficiencies. To ensure the right number of staff on duty at the right time in the right place.
Phase Two – Quality Performance Improvement Plans to improve patient safety and performance by maximising resource availability. To provide additional capacity to focus on a small number of high impact actions across the Trust.
Phase Three – Performance Improvement Plan – to address the performance gaps (after Phase 1 and 2) as per ORH analysis – commenced in February 2018 and scheduled to continue throughout 2018/19.
Phase One - Rota Review
The benefit of the rota changes (introduced during 2017/18) on performance will only be 4.2.fully realised when recruitment matches required establishment levels within each of the operational areas filling current vacancies within the rota patterns. Therefore recruitment to the funded establishment levels within each Division is seen as a key area of focus for the Trust. Details on the Trust forecast establishment position are included within the Information Pack accompanying this report.
Phase Two - Quality Performance Improvement Plan (QPIP) The Trust has developed an internal Quality Performance Improvement Plan (QPIP). The 4.3.
aim of the QPIP is to improve patient safety and performance by maximising resource availability. The QPIP contains a number of high impact actions to deliver efficiencies and increase productivity of Operational and Hub resources:
QPIP Phase 1 – commenced in September 2017 and identified a number of key areas of performance was completed in December 2017;
QPIP Phase 2 - focussed on further areas of performance and productivity improvements and commenced in Quarter 4 of 2017/18. QPIP2 identified a group of actions to deliver improvements in patient safety and performance by maximising resource availability. QPIP2 also included the launch of the Time to Care initiative. Time to Care is about working together to improve staff wellbeing and job satisfaction. Recognising that the demands faced by our staff on a daily basis are significant and growing, it is vital we improve the working environment in a way that sustains the delivery of safe and high quality services that provide benefits for staff, patients and the Trust;
QPIP Phase 3 – scheduled to be commence during May/June 2018 with a focus on delivering specific improvements in the ambulance Clinical Indicator metrics.
Phase Three - Performance Improvement Plan (PIP)
The Performance Improvement Plan (PIP) has been created to capture the key internal 4.4.actions being undertaken by the Trust to deliver changes that will either directly or indirectly impact on the Response Times to all categories of incidents within the next 12 months. These actions are then to be assessed to produce a performance improvement trajectory for Category 1 and Category 2 response times for the remainder of 2018/19.

Page 6 of 8
All the actions within the PIP are considered key to delivering the internal organisational, 4.5.process and delivery changes required to move from the current Response Time performance to delivering the optimum response times across the South West.
The PIP will not include items that are outside of the scope direct control (eg reduction in 4.6.NHS 111 activity to the ambulance service) and does not include any items included within the Trust Transition Plans that may require additional investment from NHS Commissioners.
Where possible the plan is focussed on those actions that deliver improvements in one of 4.7.the key areas impacting on Response Time performance:
Total Ambulance Incident Numbers; Call Answering; Call Coding and Allocation; Incident Outcomes (Hear & Treat, See & Treat, See & Convey); Call Cycle Times (Time to Scene, Time At Scene, Handover, Wrap Up); Operational Resource Hours Available.
It is acknowledged that there will be some actions where the direct impact on response 4.8.
times cannot be assessed but the action is deemed to be important to delivering improvements (eg staff engagement and wellbeing). These items will be included but no performance benefits will be assessed as part of the trajectory.
The performance improvement trajectory will be developed during May 2018 however it is 4.9.expected that a gap between the anticipated performance (even after these improvements) and the national performance standards will remain as identified in the resource modelling work undertaken by ORH during 2017/18. Commissioner Action Plan and Transition Plan
In addition to the Performance Improvement Plan the Trust is also committed to working 4.10.with NHS Commissioners to identify joint actions which can assist the Trust in delivering the required transformational changes to further improve Response Time performance to national standard levels.
These joint actions will be split into two areas: 4.11. Commissioner Actions – actions owned by NHS Commissioners to reduce
inappropriate demand on the ambulance service and reduce areas of operational pressure (eg reductions in handover delays at acute hospitals, assistance in recruitment and retention plans);
Transition Plan – actions jointly owned by SWASFT and NHS Commissioners to deliver transformational change. Some of these actions may subject to investment being provided by NHS Commissioners (eg additional resources).
NHS 111 Performance 5.
NHS 111 Call Answering performance during April 2018 was below the national target level 5.1.of 95%, but 89.60% of calls were answered within 60 seconds in Dorset (compared to

Page 7 of 8
81.89% in March 2018). Call abandonment rates however remained below (better than) the target level of 5% and were 2.40% in April 2018.
Whilst performance remains below the target levels, call answering performance are 5.2.consistently around 90% on a weekly basis, and is consistently higher (better) than the national average call answering performance amongst other NHS 111 service providers in England.
Week Commencing
National Standard 02/04/2018 09/04/2018 16/04/2018 23/04/2018 30/04/2018
% of Call Answered within 60 Seconds – National Average
95% 74.46% 86.93% 84.55% 88.79% 86.94%
% of Call Answered within 60 Seconds – NHS 111 Dorset
95% 90.13% 90.24% 88.76% 88.45% 86.27%
To deliver further improvements in call answering performance the Trust is undertaking a 5.3.full review of rotas for NHS 111 Call Takers and Clinicians during Quarter 1 of 2018/19. The review aims to deliver rotas to meet current demand patterns, including increased resilience during periods where current vacancies have created some weaknesses. The review will be undertaken in consultation with staff to develop the most appropriate rota patterns including a mix of full time and part time staff to meet the variable demand patterns within the service (including high levels of demand during evening and weekend periods).
GP Out of Hours Service Performance (GP OOH) 6.
The Quality Requirements relating to Urgent Treatment Centre appointments and Urgent 6.1.Home Visits remain the greatest challenge for the Dorset GP OOH service. The Trust has not been able to deliver these standards consistently although the patient numbers outside of the target are small.
In April 2018 the Dorset GP OOH service was non-compliant against the Urgent Treatment 6.2.Centre Appointments standard (88.121% compared to the target of 95%). The Trust missed the 2 hour target on 41 of the 345 cases in April, of which the majority are missed’ during the busier weekend periods. For Less Urgent Treatment Centre appointments the Trust was compliant with 98.35% of appointments completed within the 6 hour target (3.35% better than the 95% target).
The Trust was partially compliant for Urgent Home Visits in April 2018 with 416 of the 454 6.3.visits completed within the 2 hour urgent target (91.63% compared to the target of 95%). Whilst it is acknowledged that home visits are more difficult to target in view of the large geographical spread of a relatively low number of urgent incidents, operational managers continue to review appropriateness of the current profile of mobile resources.
For Less Urgent Visits in April 2018 the Trust achieved 96.84% of visits within 6 hours and 6.4.was therefore compliant against the 95% performance target.

Page 8 of 8
Urgent Care Centre (Tiverton) Performance 7.
The primary performance measure within this contract is the 4 hour waiting time standard. 7.1.In April 2018, 1,296 of 1,302 patients were seen within 4 hours giving performance of 99.54% against the 95% performance target. Performance above target levels has been delivered consistently since contract inception along with a local standard to triage patients within 15 minutes. In April 2018, 96.93% of patients were triaged in 15 minutes against a target of 95%.
Finance and Use of Resources 8.
The Trust is assessed by NHS Improvement against the Use of Resource Metric. Under the 8.1.
Use of Resource Metric the best score is 1 and the worse score is 4. As the Trust has not accepted its control total for 2018/19 the highest score the Trust can achieve is a 2.
The Trust delivered a Use of Resource Metric of 2 at the end of April 2018. The score of 2 is 8.2.
based on the Trust delivering against the control total derived by NHS Improvement from the Trust financial plan.
The financial information is based on the first month of the financial year and includes the 8.3.
actual and year end forecast position for the Trust against the 2018/19 Financial Plan: The Trust delivered a breakeven position at the end of April 2018; The position includes an under spend on basic pay relating to vacancies which
has been offset by the use of overtime, agency and third parties; The annual Cost Improvement target for 2018/19 is £7,500k and the Trust is
forecasting delivery but recognises a risk of £3,500k in relation to schemes that are non-recurrent in nature;
The Capital Plan for 2018/19 is £14,428k. The month one position shows an actual position of £384k compared to a plan of £100k (384%). This is due to timing of vehicle conversions ahead of plan;
The Trust cash position at the end of April 2018 is £19,147k compared to the plan of £22,524k. This variance relates to timing differences for increased levels of debtors and expenditure payments following year end;
The Trust year to date agency spend is £44k.
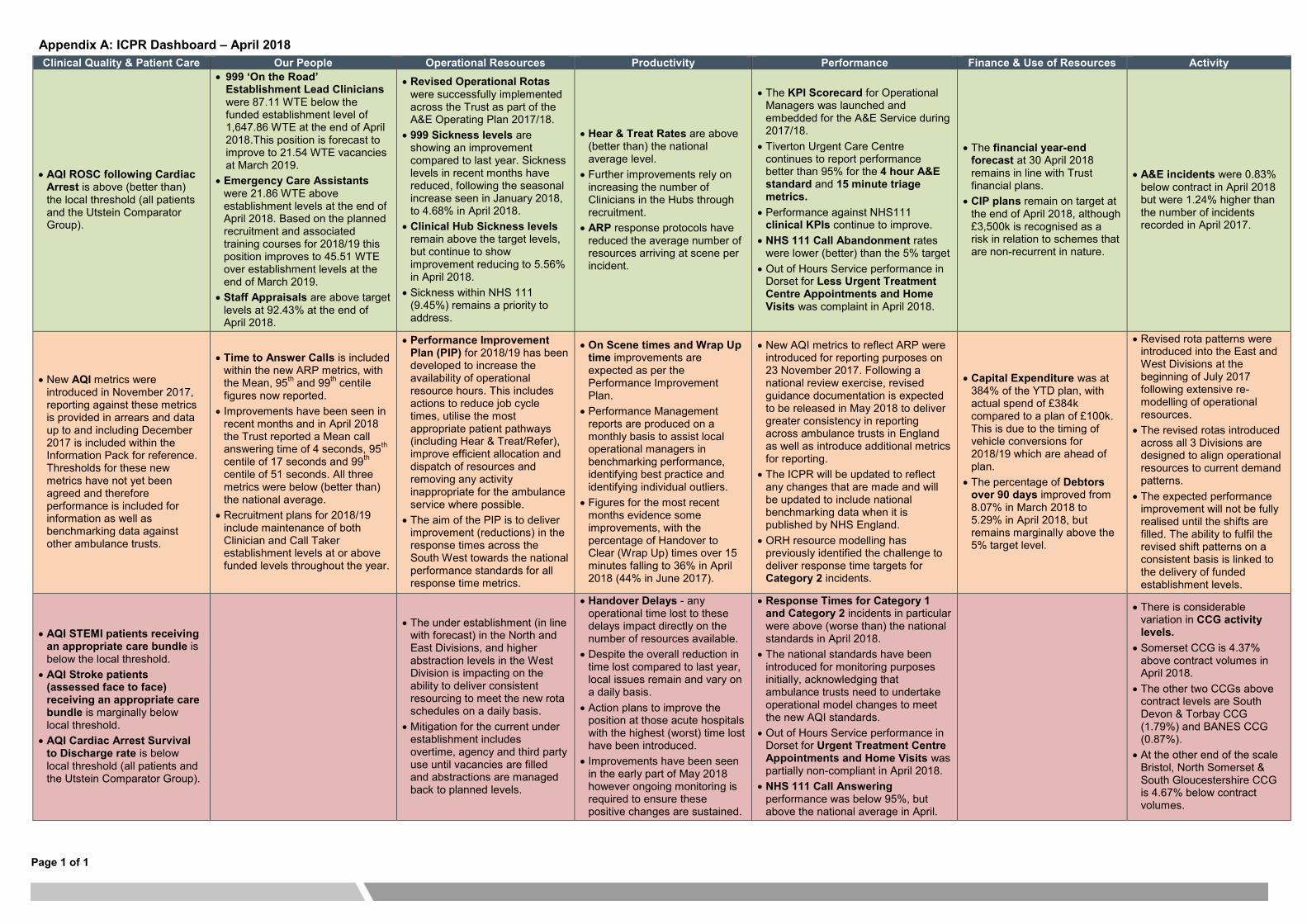
Page 1 of 1
Appendix A: ICPR Dashboard – April 2018
Clinical Quality & Patient Care Our People Operational Resources Productivity Performance Finance & Use of Resources Activity
AQI ROSC following Cardiac Arrest is above (better than) the local threshold (all patients and the Utstein Comparator Group).
999 ‘On the Road’ Establishment Lead Clinicians were 87.11 WTE below the funded establishment level of 1,647.86 WTE at the end of April 2018.This position is forecast to improve to 21.54 WTE vacancies at March 2019.
Emergency Care Assistants were 21.86 WTE above establishment levels at the end of April 2018. Based on the planned recruitment and associated training courses for 2018/19 this position improves to 45.51 WTE over establishment levels at the end of March 2019.
Staff Appraisals are above target levels at 92.43% at the end of April 2018.
Revised Operational Rotas were successfully implemented across the Trust as part of the A&E Operating Plan 2017/18.
999 Sickness levels are showing an improvement compared to last year. Sickness levels in recent months have reduced, following the seasonal increase seen in January 2018, to 4.68% in April 2018.
Clinical Hub Sickness levels remain above the target levels, but continue to show improvement reducing to 5.56% in April 2018.
Sickness within NHS 111 (9.45%) remains a priority to address.
Hear & Treat Rates are above (better than) the national average level.
Further improvements rely on increasing the number of Clinicians in the Hubs through recruitment.
ARP response protocols have reduced the average number of resources arriving at scene per incident.
The KPI Scorecard for Operational Managers was launched and embedded for the A&E Service during 2017/18.
Tiverton Urgent Care Centre continues to report performance better than 95% for the 4 hour A&E standard and 15 minute triage metrics.
Performance against NHS111 clinical KPIs continue to improve.
NHS 111 Call Abandonment rates were lower (better) than the 5% target
Out of Hours Service performance in Dorset for Less Urgent Treatment Centre Appointments and Home Visits was complaint in April 2018.
The financial year-end forecast at 30 April 2018 remains in line with Trust financial plans.
CIP plans remain on target at the end of April 2018, although £3,500k is recognised as a risk in relation to schemes that are non-recurrent in nature.
A&E incidents were 0.83% below contract in April 2018 but were 1.24% higher than the number of incidents recorded in April 2017.
New AQI metrics were introduced in November 2017, reporting against these metrics is provided in arrears and data up to and including December 2017 is included within the Information Pack for reference. Thresholds for these new metrics have not yet been agreed and therefore performance is included for information as well as benchmarking data against other ambulance trusts.
Time to Answer Calls is included within the new ARP metrics, with the Mean, 95th and 99th centile figures now reported.
Improvements have been seen in recent months and in April 2018 the Trust reported a Mean call answering time of 4 seconds, 95th centile of 17 seconds and 99th centile of 51 seconds. All three metrics were below (better than) the national average.
Recruitment plans for 2018/19 include maintenance of both Clinician and Call Taker establishment levels at or above funded levels throughout the year.
Performance Improvement Plan (PIP) for 2018/19 has been developed to increase the availability of operational resource hours. This includes actions to reduce job cycle times, utilise the most appropriate patient pathways (including Hear & Treat/Refer), improve efficient allocation and dispatch of resources and removing any activity inappropriate for the ambulance service where possible.
The aim of the PIP is to deliver improvement (reductions) in the response times across the South West towards the national performance standards for all response time metrics.
On Scene times and Wrap Up time improvements are expected as per the Performance Improvement Plan.
Performance Management reports are produced on a monthly basis to assist local operational managers in benchmarking performance, identifying best practice and identifying individual outliers.
Figures for the most recent months evidence some improvements, with the percentage of Handover to Clear (Wrap Up) times over 15 minutes falling to 36% in April 2018 (44% in June 2017).
New AQI metrics to reflect ARP were introduced for reporting purposes on 23 November 2017. Following a national review exercise, revised guidance documentation is expected to be released in May 2018 to deliver greater consistency in reporting across ambulance trusts in England as well as introduce additional metrics for reporting.
The ICPR will be updated to reflect any changes that are made and will be updated to include national benchmarking data when it is published by NHS England.
ORH resource modelling has previously identified the challenge to deliver response time targets for Category 2 incidents.
Capital Expenditure was at 384% of the YTD plan, with actual spend of £384k compared to a plan of £100k. This is due to the timing of vehicle conversions for 2018/19 which are ahead of plan.
The percentage of Debtors over 90 days improved from 8.07% in March 2018 to 5.29% in April 2018, but remains marginally above the 5% target level.
Revised rota patterns were introduced into the East and West Divisions at the beginning of July 2017 following extensive re-modelling of operational resources.
The revised rotas introduced across all 3 Divisions are designed to align operational resources to current demand patterns.
The expected performance improvement will not be fully realised until the shifts are filled. The ability to fulfil the revised shift patterns on a consistent basis is linked to the delivery of funded establishment levels.
AQI STEMI patients receiving an appropriate care bundle is below the local threshold.
AQI Stroke patients (assessed face to face) receiving an appropriate care bundle is marginally below local threshold.
AQI Cardiac Arrest Survival to Discharge rate is below local threshold (all patients and the Utstein Comparator Group).
The under establishment (in line with forecast) in the North and East Divisions, and higher abstraction levels in the West Division is impacting on the ability to deliver consistent resourcing to meet the new rota schedules on a daily basis.
Mitigation for the current under establishment includes overtime, agency and third party use until vacancies are filled and abstractions are managed back to planned levels.
Handover Delays - any operational time lost to these delays impact directly on the number of resources available.
Despite the overall reduction in time lost compared to last year, local issues remain and vary on a daily basis.
Action plans to improve the position at those acute hospitals with the highest (worst) time lost have been introduced.
Improvements have been seen in the early part of May 2018 however ongoing monitoring is required to ensure these positive changes are sustained.
Response Times for Category 1 and Category 2 incidents in particular were above (worse than) the national standards in April 2018.
The national standards have been introduced for monitoring purposes initially, acknowledging that ambulance trusts need to undertake operational model changes to meet the new AQI standards.
Out of Hours Service performance in Dorset for Urgent Treatment Centre Appointments and Home Visits was partially non-compliant in April 2018.
NHS 111 Call Answering performance was below 95%, but above the national average in April.
There is considerable variation in CCG activity levels.
Somerset CCG is 4.37% above contract volumes in April 2018.
The other two CCGs above contract levels are South Devon & Torbay CCG (1.79%) and BANES CCG (0.87%).
At the other end of the scale Bristol, North Somerset & South Gloucestershire CCG is 4.67% below contract volumes.

Appendix B:
Integrated Corporate Performance Report
Information Pack
April 2018
Integrated Corporate Performance Report 1

Category National Standard How long does the ambulance service have to make a decision?
7 minutes The earliest of:Mean response time The problem being identified;
An ambulance response being dispatched;15 minutes 30 seconds from the call being connected.
90th centile response time18 minutes The earliest of:
Mean response time The problem being identified; An ambulance response being dispatched;
40 minutes 240 seconds from the call being connected.90th centile response time
60 minutes The earliest of:Mean response time The problem being identified;
120 minutes An ambulance response being dispatched;90th centile response time 240 seconds from the call being connected.
The earliest of: The problem being identified;
180 minutes An ambulance response being dispatched;90th centile response time 240 seconds from the call being connected.
Ambulance Response Programme (ARP)
Category 1
Category 2
Category 3
Category 4
The Trust has participated in the Ambulance Response Programme (ARP) trial since April 2016. The Secretary of State for Health announced on 13 July 2017 that the three tests of ARP have been met as follows:
There is clear clinical consensus that the proposed changes will be beneficial to patient outcomes as a whole and will act to reduce overall clinical risk in the system;There is evidence from the analysis of existing data and pilots that the proposed changes will have the intended benefits and is safe for patients;There is an associated increase in operational efficiency. The aim is to reduce the average number of vehicles allocated to each 999 call and the ambulance utilisation rate.
Further information on the Ambulance Response Programme, the new ambulance standards and a copy of Sheffield University’s report on ARP can be found on the NHS England website: www.england.nhs.uk/urgent-emergency-care/arp/
NHS England has also developed a guide to the new Ambulance Standards, which outline the purpose of ARP and the new ambulance standards that have been introduced. A copy of this ‘easy read’ document can be found on the NHS England website: www.england.nhs.uk/publication/new-ambulance-standards-easy-read-document/
New standards, indicators and measures have been introduced through the ARP for publication in the NHS England Ambulance Quality Indicators (AQI). A technical guidance document issued in August 2017 (and updated in September 2017) has been developed to ensure that all aspects of ambulance performance are measured accurately and consistently. All ambulance trusts in England were required to commence reporting against the new standards by 30 November 2017.
Compliance against the new standards is expected from 1 April 2018. Until then the standards proposed are to be used for monitoring purposes only to enable ambulance trusts to update their operating models to deliver the new performance standards.
SWASFT implemented the new response time reporting standards required for ARP v2.3 with effect from 23 November 2017. This report therefore includes data in relation to the old metrics up to and including 22 November 2017 and reporting on the new metrics with effect from 23 November 2017.
The new performance standards against which the Trust will be monitored are outlined in the table below:
Integrated Corporate Performance Report 2

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
0:07:00 0:08:30 0:08:30
0:15:00 0:15:48 0:15:48
0:30:00 0:23:18 0:23:18
0:18:00 0:23:24 0:23:24
0:40:00 0:48:24 0:48:24
1:00:00 0:50:48 0:50:48
2:00:00 1:58:48 1:58:48
3:00:00 4:15:42 4:15:42
0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
0.03 0.03 0.03 0.03 0.03 0.03 0.03 0.03 0.03 0.03 0.03 0.03
0.08 0.08 0.08 0.08 0.08 0.08 0.08 0.08 0.08 0.08 0.08 0.08 0.08
0.13 0.13 0.13 0.13 0.13 0.13 0.13 0.13 0.13 0.13 0.13 0.13
ARP 2.3 Performance Metrics -Response Times
Category 1 Response Time - 90th Percentile (minutes)
Category 2 Response Time - Mean (minutes)
Category 2 Response Time - 90th Percentile (minutes)
Category 4 (999) Response Time - 90th Percentile (minutes)
Category 3 Response Time - 90th Percentile (minutes)
Category 1 Response Time - Mean (minutes)
Category 3 Response Time - Mean (minutes)
Category 1 (Transport) Response Time - 90th Percentile (minutes)
00:00
02:00
04:00
06:00
08:00
10:00
12:00
14:00
16:00
18:00
20:00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
ARP 2.3 - Category 1 Response Times (minutes)
0:00:00
0:15:00
0:30:00
0:45:00
1:00:00
1:15:00
1:30:00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
ARP 2.3 - Category 2 Response Times (minutes)
0:00:00
0:30:00
1:00:00
1:30:00
2:00:00
2:30:00
3:00:00
3:30:00
4:00:00
4:30:00
5:00:00
5:30:00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
ARP 2.3 - Category 4 (999) Response Times (minutes)
0:00:000:15:000:30:000:45:001:00:001:15:001:30:001:45:002:00:002:15:002:30:002:45:003:00:00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
ARP 2.3 - Category 3 Response Times (minutes)
Integrated Corporate Performance Report 3

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
0:08:12 0:08:120:07:24 0:07:240:07:54 0:07:540:08:42 0:08:420:10:30 0:10:300:09:00 0:09:000:08:54 0:08:540:08:12 0:08:120:06:48 0:06:480:09:00 0:09:00
0:07:00 0:08:30 0:08:30
0:16:06 0:16:060:13:00 0:13:000:13:48 0:13:480:16:06 0:16:060:19:30 0:19:300:17:24 0:17:240:16:48 0:16:480:15:00 0:15:000:11:12 0:11:120:16:36 0:16:36
0:15:00 0:15:48 0:15:48
Bristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
ARP 2.3 Performance Metrics - Category 1 Mean Response Times by CCG
ARP 2.3 Performance Metrics - Category 1 90th Percentile Response Times by CCG
Bath & North East Somerset CCGBristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
Bath & North East Somerset CCG
0:08:12
0:07:24
0:07:54
0:08:42
0:10:30
0:09:00
0:08:54
0:08:12
0:06:48
0:09:00
0:08:30
0:00:00 0:02:00 0:04:00 0:06:00 0:08:00 0:10:00 0:12:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 1 - Mean Response Times by CCG - Current Month
0:16:06
0:13:00
0:13:48
0:16:06
0:19:30
0:17:24
0:16:48
0:15:00
0:11:12
0:16:36
0:15:48
0:00:00 0:02:00 0:04:00 0:06:00 0:08:00 0:10:00 0:12:00 0:14:00 0:16:00 0:18:00 0:20:00 0:22:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 1 - 90th Percentile Response Times by CCG - Current Month
Integrated Corporate Performance Report 4
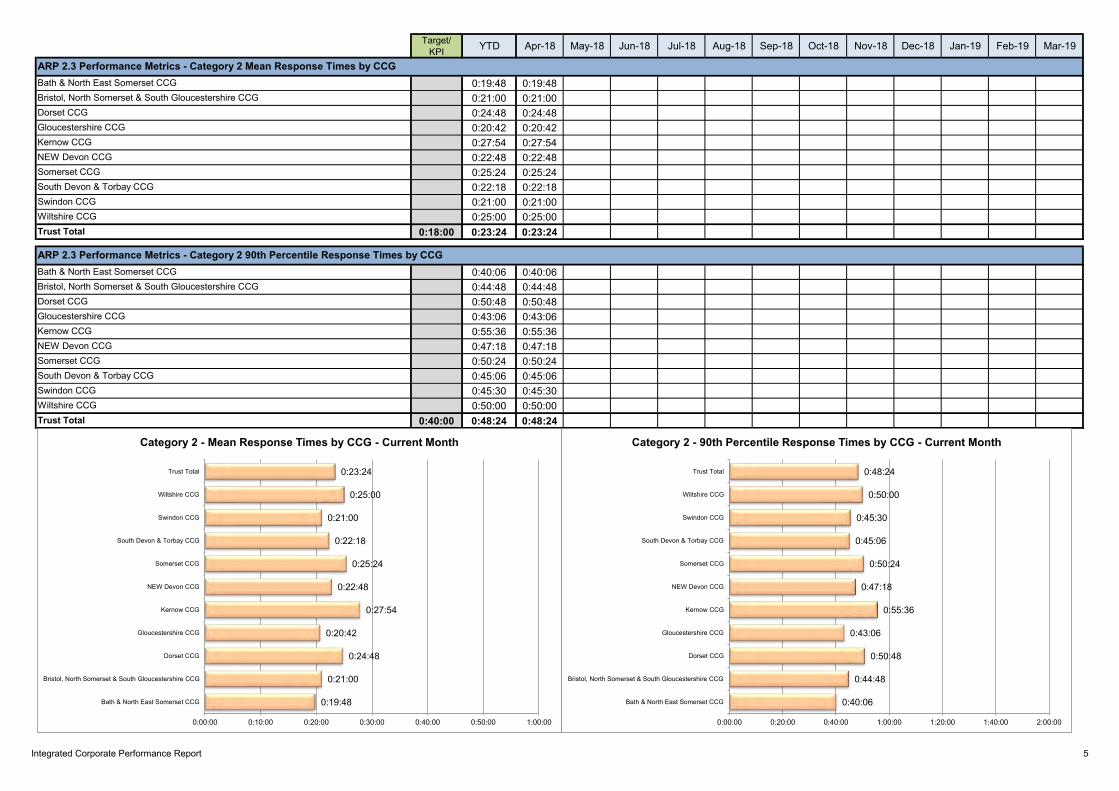
Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
0:19:48 0:19:480:21:00 0:21:000:24:48 0:24:480:20:42 0:20:420:27:54 0:27:540:22:48 0:22:480:25:24 0:25:240:22:18 0:22:180:21:00 0:21:000:25:00 0:25:00
0:18:00 0:23:24 0:23:24
0:40:06 0:40:060:44:48 0:44:480:50:48 0:50:480:43:06 0:43:060:55:36 0:55:360:47:18 0:47:180:50:24 0:50:240:45:06 0:45:060:45:30 0:45:300:50:00 0:50:00
0:40:00 0:48:24 0:48:24
Bristol, North Somerset & South Gloucestershire CCGDorset CCG
ARP 2.3 Performance Metrics - Category 2 Mean Response Times by CCGBath & North East Somerset CCGBristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCG
Swindon CCGWiltshire CCGTrust Total
Gloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCG
South Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
ARP 2.3 Performance Metrics - Category 2 90th Percentile Response Times by CCGBath & North East Somerset CCG
0:19:48
0:21:00
0:24:48
0:20:42
0:27:54
0:22:48
0:25:24
0:22:18
0:21:00
0:25:00
0:23:24
0:00:00 0:10:00 0:20:00 0:30:00 0:40:00 0:50:00 1:00:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 2 - Mean Response Times by CCG - Current Month
0:40:06
0:44:48
0:50:48
0:43:06
0:55:36
0:47:18
0:50:24
0:45:06
0:45:30
0:50:00
0:48:24
0:00:00 0:20:00 0:40:00 1:00:00 1:20:00 1:40:00 2:00:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 2 - 90th Percentile Response Times by CCG - Current Month
Integrated Corporate Performance Report 5

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
0:40:30 0:40:300:46:12 0:46:121:00:18 1:00:180:38:48 0:38:481:03:06 1:03:060:48:30 0:48:300:54:18 0:54:180:49:48 0:49:480:46:12 0:46:120:46:42 0:46:42
1:00:00 0:50:48 0:50:48
1:22:42 1:22:421:52:24 1:52:242:16:12 2:16:121:31:06 1:31:062:25:42 2:25:421:55:42 1:55:422:00:48 2:00:481:52:12 1:52:121:48:00 1:48:001:42:54 1:42:54
2:00:00 1:58:48 1:58:48
ARP 2.3 Performance Metrics - Category 3 Mean Response Times by CCGBath & North East Somerset CCGBristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
ARP 2.3 Performance Metrics - Category 3 90th Percentile Response Times by CCGBath & North East Somerset CCGBristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
0:19:48
0:21:00
0:24:48
0:20:42
0:27:54
0:22:48
0:25:24
0:22:18
0:21:00
0:25:00
0:23:24
0:00:00 0:10:00 0:20:00 0:30:00 0:40:00 0:50:00 1:00:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 3 - Mean Response Times by CCG - Current Month
0:40:06
0:44:48
0:50:48
0:43:06
0:55:36
0:47:18
0:50:24
0:45:06
0:45:30
0:50:00
0:48:24
0:00:00 0:20:00 0:40:00 1:00:00 1:20:00 1:40:00 2:00:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 3 - 90th Percentile Response Times by CCG - Current Month
Integrated Corporate Performance Report 6

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
0:40:30 0:40:300:46:12 0:46:121:00:18 1:00:180:38:48 0:38:481:03:06 1:03:060:48:30 0:48:300:54:18 0:54:180:49:48 0:49:480:46:12 0:46:120:46:42 0:46:42
3:00:00 0:50:48 0:50:48
1:22:42 1:22:421:52:24 1:52:242:16:12 2:16:121:31:06 1:31:062:25:42 2:25:421:55:42 1:55:422:00:48 2:00:481:52:12 1:52:121:48:00 1:48:001:42:54 1:42:54
0:30:00 1:58:48 1:58:48
ARP 2.3 Performance Metrics - Category 4 90th Percentile Response Times by CCGBath & North East Somerset CCGBristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
ARP 2.3 Performance Metrics - Category 1 (Transport) 90th Percentile Response Times by CCGBath & North East Somerset CCGBristol, North Somerset & South Gloucestershire CCGDorset CCGGloucestershire CCGKernow CCGNEW Devon CCGSomerset CCGSouth Devon & Torbay CCGSwindon CCGWiltshire CCGTrust Total
0:40:30
0:46:12
0:38:48
0:48:30
0:54:18
0:49:48
0:46:12
0:46:42
0:50:48
0:00:00 0:10:00 0:20:00 0:30:00 0:40:00 0:50:00 1:00:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 4 - 90th Percentile Response Times by CCG - Current Month
1:22:42
1:52:24
1:31:06
1:55:42
1:52:12
1:48:00
1:42:54
1:58:48
0:00:00 0:20:00 0:40:00 1:00:00 1:20:00 1:40:00 2:00:00
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Gloucestershire CCG
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Wiltshire CCG
Trust Total
Category 1 (T) - 90th Percentile Response Times by CCG - Current Month
Integrated Corporate Performance Report 7

Period National Average
East Midlands
East of England London North East North West South
CentralSouth East
CoastSouth
WesternWest
Midlands Yorkshire
Apr-18 0:07:38 0:08:36 0:08:06 0:06:52 0:05:53 0:07:51 0:06:35 0:07:24 0:08:32 0:06:50 0:08:02
Apr-18 0:13:26 0:15:39 0:14:44 0:11:15 0:10:05 0:13:24 0:11:50 0:13:45 0:15:50 0:12:04 0:13:44
Apr-18 0:22:14 0:39:42 0:24:02 0:19:26 0:14:48 0:21:17 0:18:31 0:19:36 0:23:17 0:14:03 0:20:23
Apr-18 0:20:15 0:31:57 0:22:43 0:16:54 0:17:09 0:23:38 0:14:13 0:16:08 0:23:25 0:11:23 0:21:39
Apr-18 0:41:42 1:08:06 0:47:23 0:33:16 0:34:56 0:51:59 0:27:46 0:30:17 0:48:24 0:20:24 0:45:53
Apr-18 0:49:37 1:07:22 0:57:48 0:47:14 0:51:50 0:59:18 0:43:48 1:04:25 0:50:50 0:25:38 0:54:00
Apr-18 1:55:52 2:41:18 2:17:03 1:49:47 2:01:38 2:21:50 1:40:08 2:32:34 1:58:50 0:55:17 2:05:16
Apr-18 2:43:12 2:01:50 2:47:28 2:05:08 1:52:32 2:56:37 2:33:04 4:10:57 4:15:42 1:32:40 2:44:53
Apr-18 44 43 34 65 30 54 37 44 50 48 28
Apr-18 82 73 59 135 59 106 71 91 103 55 50
Apr-18 6 3 3 6 2 10 5 15 4 2 3
Apr-18 31 4 6 39 8 70 9 97 17 4 9
Apr-18 91 49 51 139 25 133 63 204 51 31 54
Apr-18 5.2% 6.4% 6.3% 3.5% 5.1% 4.8% 6.2% 5.5% 5.8% 3.1% 6.5%
Apr-18 2.2 1.8 2.2 2.6 2.0 2.0 2.0 2.4 2.1 1.9 2.2
Apr-18 1.7 1.4 1.7 2.1 1.6 1.7 1.6 1.8 1.7 1.4 1.7
Apr-18 1.4 1.3 1.5 1.5 1.4 1.3 1.4 1.4 1.3 1.3 1.6
Apr-18 1.1 1.1 1.2 1.1 1.2 1.1 1.2 1.1 1.1 1.1 1.2
Apr-18 1.6 1.3 1.9 1.6 1.7 1.4 1.4 1.7 1.5 1.6 1.8
Apr-18 1.1 1.1 1.1 1.1 1.1 1.1 1.1 1.1 1.1 1.1 1.1
Apr-18 1.7 1.3 1.9 1.4 1.7 1.3 1.5 1.8 1.5 2.1 1.9
Apr-18 1.1 1.0 1.1 1.1 1.1 1.1 1.1 1.1 1.1 1.1 1.1
Call Answering - 95th Percentile Answer Time (Seconds)
Call Answering - 99th Percentile Answer Time (Seconds)
Mean Number of Ambulance Resources Allocated per Category 1 Incident
Mean Number of Ambulance Resources Arriving at Scene per Category 1 Incident
Mean Number of Ambulance Resources Allocated per Category 2 Incident
Mean Number of Ambulance Resources Arriving at Scene per Category 2 Incident
Mean Number of Ambulance Resources Allocated per Category 3 Incident
Mean Number of Ambulance Resources Arriving at Scene per Category 3 Incident
Mean Number of Ambulance Resources Allocated per Category 4 (999) Incident
Mean Number of Ambulance Resources Arriving at Scene per Category 4 (999) Incident
Mean Time To Identify Category 1 Incidents (where Category 1 incidents are identified with Nature of Call or Pre-Triage Questions) (Seconds)90th centile Time To Identify Category 1 Incidents (where Category 1 incidents are identified with Nature of Call or Pre-Triage Questions) (Seconds)
% of Calls Closed with Telephone Advice or Referral to Other Service
Ambulance Quality Indicators 2.3 Metrics - National BenchmarkingCategory 1 - Mean Response Time (Mins)
Category 1 - 90th Percentile Reponse Time (Mins)
Category 2 - Mean Response Time (Mins)
Category 2 - 90th Percentile Response Time (Mins)
Category 3 - 90th Percentrile Reponse Time (Mins)
Category 4 (999) - 90th Percentile Response Time (Mins)
Call Answering - Mean Answer Time (Seconds)
Category 1 (Transport) Response Time - 90th Percentile (minutes)
Category 3 Response Time - Mean (minutes)
0:07:38
0:08:36
0:08:06
0:06:52
0:05:53
0:07:51
0:06:35
0:07:24
0:08:32
0:06:50
0:08:02
0:00:00 0:02:00 0:04:00 0:06:00 0:08:00 0:10:00
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Category 1 - Mean Response (Mins)
0:13:26
0:15:39
0:14:44
0:11:15
0:10:05
0:13:24
0:11:50
0:13:45
0:15:50
0:12:04
0:13:44
0:00:00 0:05:00 0:10:00 0:15:00 0:20:00
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Category 1 - 90th Percentile Response (Mins)
0:20:15
0:31:57
0:22:43
0:16:54
0:17:09
0:23:38
0:14:13
0:16:08
0:23:25
0:11:23
0:21:39
0:00:00 0:10:00 0:20:00 0:30:00 0:40:00
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Category 2 - Mean Response (Mins)
0:41:42
1:08:06
0:47:23
0:33:16
0:34:56
0:51:59
0:27:46
0:30:17
0:48:24
0:20:24
0:45:53
0:00:00 0:20:00 0:40:00 1:00:00 1:20:00
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Category 2 - 90th Percentile Response (Mins)
Integrated Corporate Performance Report 8

1:55:52
2:41:18
2:17:03
1:49:47
2:01:38
2:21:50
1:40:08
2:32:34
1:58:50
0:55:17
2:05:16
0:00:00 1:00:00 2:00:00 3:00:00
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Category 3 - 90th Percentile Response (Mins)
2:43:12
2:01:50
2:47:28
2:05:08
1:52:32
2:56:37
2:33:04
4:10:57
4:15:42
1:32:40
2:44:53
0:00:00 1:00:00 2:00:00 3:00:00 4:00:00 5:00:00
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Category 4 (999) - 90th Percentile Response (Mins)
44
43
34
65
30
54
37
44
50
48
28
0 10 20 30 40 50 60 70
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Mean Time to Identify Cat 1 (NOC and PTQ)
82
73
59
135
59
106
71
91
103
55
50
0 20 40 60 80 100 120 140 160
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
90th Percentile Time to Identify Cat 1 (NOC and PTQ)
5.2%
6.4%
6.3%
3.5%
5.1%
4.8%
6.2%
5.5%
5.8%
3.1%
6.5%
0.0% 1.0% 2.0% 3.0% 4.0% 5.0% 6.0% 7.0%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
% Calls Closed with Tel Advice/Referral
6
3
3
6
2
10
5
15
4
2
3
0 2 4 6 8 10 12 14 16
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Mean Call Answer Time (Secs)
31
4
6
39
8
70
9
97
17
4
9
0 20 40 60 80 100 120
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
95th Percentile Call Answer Time (Secs)
91
49
51
139
25
133
63
204
51
31
54
0 50 100 150 200 250
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
99th Percentile Call Answer Time (Secs)
1.69
1.43
1.68
2.07
1.62
1.67
1.59
1.77
1.66
1.41
1.73
0.00 0.40 0.80 1.20 1.60 2.00 2.40
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Mean Number of Ambulance Resources Arriving at Scene (Cat 1 Incidents)
1.13
1.10
1.17
1.14
1.15
1.08
1.18
1.13
1.14
1.05
1.21
0.00 0.20 0.40 0.60 0.80 1.00 1.20 1.40
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Mean Number of Ambulance Resources Arriving at Scene (Cat 2 Incidents)
1.09
1.06
1.08
1.13
1.06
1.09
1.13
1.06
1.11
1.05
1.14
1.00 1.02 1.04 1.06 1.08 1.10 1.12 1.14 1.16
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Mean Number of Ambulance Resources Arriving at Scene (Cat 3 Incidents)
1.08
1.03
1.08
1.06
1.05
1.07
1.10
1.06
1.06
1.06
1.13
0.98 1.00 1.02 1.04 1.06 1.08 1.10 1.12 1.14
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Mean Number of Ambulance Resources Arriving at Scene (Cat 4 (999) Incidents)
Integrated Corporate Performance Report 9

Target/KPI
Rolling 12 Months Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17
n/a 3,805 359 277 308 343 314 293 339 312 282 301 318 359
24.00% 28.20% 25.91% 27.08% 31.82% 27.41% 27.07% 33.11% 31.86% 25.00% 30.14% 26.91% 27.04% 25.91%
n/a 580 49 42 50 37 41 58 53 53 36 46 53 62
45.00% 47.07% 46.94% 42.86% 50.00% 48.65% 36.59% 44.83% 54.72% 47.17% 52.78% 45.65% 47.17% 46.77%
n/a 3,684 353 272 302 335 300 284 327 301 274 282 302 352
9.00% 8.17% 8.22% 5.51% 9.27% 5.97% 7.67% 11.97% 10.70% 7.64% 9.12% 5.67% 6.95% 9.09%
n/a 552 48 41 48 36 39 55 51 49 35 40 51 59
27.00% 21.92% 27.08% 12.20% 29.17% 27.78% 12.82% 23.64% 21.57% 18.37% 25.71% 17.50% 19.61% 25.42%
n/a 2,537 239 180 210 220 196 211 216 227 234 197 196 211
84.00% 65.87% 67.36% 66.11% 60.95% 61.36% 61.73% 66.82% 69.44% 68.72% 66.24% 64.47% 65.31% 71.09%
n/a 325 147 178
n/a 259 121 138
tbc 02:21 02:25
tbc 03:24 03:17
n/a 10,808 968 857 931 837 924 921 861 993 812 885 958 861
97.00% 96.76% 96.28% 95.68% 96.89% 96.65% 94.70% 95.87% 95.01% 96.88% 95.32% 96.50% 96.76% 97.44%
n/a 956 956 Not yet available
tbc 01:20 01:20 Not yet available
tbc 01:16 Not yet available
tbc 01:59 Not yet available
n/a 582 582 Not yet available
tbc 02:50 Not yet available
tbc 00:35 Not yet available
tbc 04:10 Not yet available
n/a 68 956 Not yet available
tbc 00:53 Not yet available
tbc 00:43 Not yet available
tbc 01:29 Not yet available
Outcome from Stroke for Ambulance Patients - Number of stroke patients in SSNAP who had a CT scan
Outcome from Stroke for Ambulance Patients - Number of stroke patients in SSNAP who had thrombolysisOutcome from Stroke for Ambulance Patients - Mean time from arrival at hospital to thrombolysis for stroke patients in SSNAP who had thrombolysis (hours:minutes)
Ambulance Clinical Indicators
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at time of arrival at hospital (overall)
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at time of arrival at hospital (Utstein Comparator Group)
Outcome from Stroke for Ambulance Patients - % of suspected stroke or unresolved transient ischaemic attack pateints assessed face to face that received an appropriate diagnostic bundle
Outcome from Cardiac Arrest - Survival to Discharge - overall survival rate
Outcome from Cardiac Arrest - Survival to Discharge - Utstein Comparator Group survival rate
Outcome from Cardiac Arrest - Number of Patients who had resucitation commenced/continued by ambulance service following cardiac arrest
Outcome from Cardiac Arrest - Number of Patients who had resucitation commenced/continued by ambulance service following cardiac arrest (Utstein Comparator Group)
Outcome from Cardiac Arrest - Survival to Discharge - Number of patients who had resuscitation by ambulance service following cardiac arrest
Outcome from Cardiac Arrest - Survival to Discharge - Number of patients who had resuscitation by ambulance service following cardiac arrest (Utstein Comparator Group)
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - Number of patients with a pre-hospital diagnosis of suspected STEMI confirmed on ECG
Outcome from Stroke for Ambulance Patients - Number of suspected stroke or unresolved transient ischaemic attack pateints assessed face to face
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - Number of paitents directly admitted with an initial diagnosis of 'definite Myocardial Infarction' who had primary percutaneous coronary intervention (PPCI)
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - % of patients with a pre-hospital diagnosis of suspected STEMI confirmed on ECG receiving an appropriate care bundleOutcome from Acute ST-Elevation Myocardial Infarction (STEMI) - Number of paitents directly admitted with an initial diagnosis of 'definite Myocardial Infarction'
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - Mean time from call for help to catheter insertion for angiography for paitents directly admitted with an initial diagnosis of 'definite Myocardial Infarction' (hours:minutes)
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - 90the centile time from call for help to catheter insertion for angiography for paitents directly admitted with an initial diagnosis of 'definite Myocardial Infarction' (hours:minutes)
Outcome from Stroke for Ambulance Patients - Mean time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service (hours:minutes)
Outcome from Stroke for Ambulance Patients - 50th centile time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service (hours:minutes)
Outcome from Stroke for Ambulance Patients - 90th centile time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service (hours:minutes)
Outcome from Stroke for Ambulance Patients - Mean time from arrival at hospital to CT scan for stroke patients in SSNAP who had a CT scan (hours:minutes)Outcome from Stroke for Ambulance Patients - Median time from arrival at hospital to CT scan for stroke patients in SSNAP who had a CT scan (hours:minutes)Outcome from Stroke for Ambulance Patients - 90th centile time from arrival at hospital to CT scan for stroke patients in SSNAP who had a CT scan (hours:minutes)
Outcome from Stroke for Ambulance Patients - Median time from arrival at hospital to thrombolysis for stroke patients in SSNAP who had thrombolysis (hours:minutes)Outcome from Stroke for Ambulance Patients - 90th centile time from arrival at hospital to thrombolysis for stroke patients in SSNAP who had thrombolysis (hours:minutes)
Outcome from Stroke for Ambulance Patients - Number of patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service
Integrated Corporate Performance Report 10

0.01
As part of the Ambulance Response Programme review of Clinical Outcomes, new timelines measures have been introduced for STEMI and Stroke, superseding the previous measures.Full definitions can be found at www.england.nhs.uk/statistics/statistical-work-areas/ambulance-quality-indicatorsST-segment elevation myocardial infarction (STEMI)The Myocardial Ischaemia National Audit Project (MINAP) have supplied:• the count of patients transported by Ambulance Services in England with an initial diagnosis of “definite Myocardial Infarction”;• of those, how patient many had primary percutaneous coronary intervention (PPCI): inflation of a balloon inside a blood vessel to restore blood flow to the heart;• for those, the time (mean average, and 90th centile) from the call for an ambulance, until the insertion of a catheter into the blood vessels, to examine whether PPCI is clinically appropriate.StrokeThe FAST procedure helps assess whether someone has suffered a stroke:• Facial weakness: can the person smile? Has their mouth or eye drooped?• Arm weakness: can the person raise both arms?• Speech problems: can the person speak clearly and understand what you say?• Time to call 999 for an ambulance if you spot any one of these signs.The Ambulance Services of England have supplied the numbers of patients they transported that were either FAST positive, or had a provisional diagnosis of stroke; and of those, the time from the call for an ambulance, until arrival at hospital.Complementing that, the Stroke Sentinel National Audit Programme (SSNAP) have supplied:• the numbers of stroke patients who had a CT scan, and for those, the time from the hospital-recorded arrival to the CT scan;• the numbers who had thrombolysis (injection of drugs to dissolve a blood clot), and for those, the time from the hospital-recorded arrival time to thrombolysis.All times supplied for stroke indicators are mean average, median, and 90th centile.
0
50
100
150
200
250
300
350
400
0%
5%
10%
15%
20%
25%
30%
35%
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at Time of Arrival at Hospital
No. of Incidents Perf % Threshold
0
10
20
30
40
50
60
70
20%
25%
30%
35%
40%
45%
50%
55%
60%
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at Time of Arrival at Hospital
(Utstein Comparator Group)
No. of Incidents Perf % Threshold
0
50
100
150
200
250
300
350
400
0%
2%
4%
6%
8%
10%
12%
14%
Outcome from Cardiac Arrest - Surival to Discarge Rate (Overall)
No. of Incidents Perf % Threshold
0
10
20
30
40
50
60
70
0%
5%
10%
15%
20%
25%
30%
35%
Outcome from Cardiac Arrest - Surival to Discarge Rate (Utstein Comparator Group)
No. of Incidents Perf % Threshold
00:00
00:30
01:00
01:30
02:00
02:30
03:00
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - Mean time from call for help to catheter insertion for angiography for paitents directly admitted with an initial diagnosis of 'definite
Myocardial Infarction' (hours:minutes)
00:00
00:20
00:40
01:00
01:20
01:40
Outcome from Stroke for Ambulance Patients - Mean time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance
Service (hours:minutes)
0
50
100
150
200
250
300
0%10%20%30%40%50%60%70%80%90%
100%
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - % of patients with a pre-hospital diagnosis of
suspected STEMI confirmed on ECG receiving an appropriate care bundle
No. of Incidents Perf % Threshold
0
200
400
600
800
1,000
1,200
0%10%20%30%40%50%60%70%80%90%
100%
Outcome from Stroke for Ambulance Patients - % of suspected stroke or unresolved transient ischaemic attack pateints assessed face to face that received an appropriate
diagnostic bundle
No. of Incidents Perf % Threshold
00:00
00:30
01:00
01:30
02:00
02:30
03:00
Outcome from Stroke for Ambulance Patients - Mean time from arrival at hospital to CT scan for stroke patients in
SSNAP who had a CT scan (hours:minutes)
00:00
00:10
00:20
00:30
00:40
00:50
01:00
Outcome from Stroke for Ambulance Patients - Mean time from arrival at hospital to thrombolysis for stroke patients in SSNAP
who had thrombolysis (hours:minutes)
Integrated Corporate Performance Report 11

Period National Average
East Midlands
East of England London North East North West South
CentralSouth East
CoastSouth
WesternWest
Midlands Yorkshire
Apr-17 to Dec-17 29.97% 27.04% 31.53% 31.80% 30.11% 34.92% 32.01% 24.73% 28.21% 29.53% 28.64%
Apr-17 to Dec-17 51.32% 49.47% 60.70% 54.72% 55.91% 54.52% 46.91% 48.40% 47.15% 50.97% 47.79%
Apr-17 to Dec-17 9.20% 7.80% 9.03% 8.10% 8.97% 9.65% 15.26% 7.43% 8.31% 9.87% 10.81%
Apr-17 to Dec-17 27.84% 25.29% 30.74% 29.76% 35.71% 22.51% 33.55% 27.27% 21.45% 27.74% 28.75%
Apr-17 to Dec-17 76.56% 80.12% 91.29% 70.73% 90.66% 75.09% 79.86% 64.95% 66.19% 80.51% 79.87%
Dec-17 02:18 02:33 02:17 02:17 01:34 02:59 02:03 02:19 02:25 02:06 02:16
Dec-17 03:07 03:36 02:52 03:09 01:58 04:33 02:52 02:59 03:17 02:50 02:56
Apr-17 to Dec-17 97.13% 97.54% 99.62% 96.77% 98.66% 99.32% 98.51% 94.34% 96.14% 94.86% 98.37%
Nov-17 01:13 01:32 01:12 01:15 01:15 01:18 01:09 01:08 01:20 01:09 01:13
Nov-17 01:06 01:18 01:05 01:03 01:08 01:12 01:02 01:01 01:16 01:03 01:05
Nov-17 01:49 02:19 01:40 01:49 01:50 02:02 01:40 01:38 01:59 01:45 01:47
Nov-17 03:03 02:58 02:24 02:27 01:39 03:20 04:43 03:19 02:50 03:10 03:48
Nov-17 00:44 00:48 00:44 00:32 00:41 00:46 00:56 00:42 00:35 00:46 00:55
Nov-17 03:58 04:03 03:47 03:52 03:23 03:32 04:08 04:07 04:10 04:22 04:31
Nov-17 00:54 00:57 00:58 00:41 00:45 01:06 00:50 00:56 00:53 01:01 00:52
Nov-17 00:46 00:49 00:48 00:33 00:37 00:53 00:44 00:56 00:43 00:58 00:46
Nov-17 01:33 01:43 01:43 01:13 01:19 01:54 01:30 01:31 01:29 01:33 01:32
Outcome from Cardiac Arrest - Survival to Discharge - overall survival rate
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at time of arrival at hospital (overall)
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at time of arrival at hospital (Utstein Comparator Group)
Outcome from Stroke for Ambulance Patients - Median time from arrival at hospital to thrombolysis for stroke patients in SSNAP who had thrombolysis (hours:minutes)
Outcome from Stroke for Ambulance Patients - 90th centile time from arrival at hospital to thrombolysis for stroke patients in SSNAP who had thrombolysis (hours:minutes)
Outcome from Stroke for Ambulance Patients - Mean time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service (hours:minutes)
Outcome from Stroke for Ambulance Patients - 50th centile time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service (hours:minutes)
Outcome from Stroke for Ambulance Patients - 90th centile time from call to hospital arrival for patients either FAST positive, or with provisional daignosis of stroke transported by the Ambulance Service (hours:minutes)
Outcome from Stroke for Ambulance Patients - Mean time from arrival at hospital to CT scan for stroke patients in SSNAP who had a CT scan (hours:minutes)
Outcome from Stroke for Ambulance Patients - Median time from arrival at hospital to CT scan for stroke patients in SSNAP who had a CT scan (hours:minutes)
Outcome from Stroke for Ambulance Patients - 90th centile time from arrival at hospital to CT scan for stroke patients in SSNAP who had a CT scan (hours:minutes)
Ambulance Clinical Indicators - National Benchmarking
Outcome from Stroke for Ambulance Patients - Mean time from arrival at hospital to thrombolysis for stroke patients in SSNAP who had thrombolysis (hours:minutes)
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - % of patients with a pre-hospital diagnosis of suspected STEMI confirmed on ECG receiving an appropriate care bundle
Outcome from Cardiac Arrest - Survival to Discharge - Utstein Comparator Group survival rate
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - Mean time from call for help to catheter insertion for angiography for paitents directly admitted with an initial diagnosis of 'definite Myocardial Infarction' (hours:minutes)
Outcome from Acute ST-Elevation Myocardial Infarction (STEMI) - 90th centile time from call for help to catheter insertion for angiography for paitents directly admitted with an initial diagnosis of 'definite Myocardial Infarction' (hours:minutes)
Outcome from Stroke for Ambulance Patients - % of suspected stroke or unresolved transient ischaemic attack pateints assessed face to face that received an appropriate diagnostic bundle
Integrated Corporate Performance Report 12

29.97%
27.04%
31.53%
31.80%
30.11%
34.92%
32.01%
24.73%
28.21%
29.53%
28.64%
0% 5% 10% 15% 20% 25% 30% 35% 40%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at Time of Arrival at Hospital
51.32%
49.47%
60.70%
54.72%
55.91%
54.52%
46.91%
48.40%
47.15%
50.97%
47.79%
0% 10% 20% 30% 40% 50% 60% 70%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Cardiac Arrest - Return of Spontaneous Circulation at Time of Arrival at Hospital (Utstein Comparator
Group)
9.20%
7.80%
9.03%
8.10%
8.97%
9.65%
15.26%
7.43%
8.31%
9.87%
10.81%
0% 5% 10% 15% 20%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Cardiac Arrest - Surival to Discarge Rate (Overall)
27.84%
25.29%
30.74%
29.76%
35.71%
22.51%
33.55%
27.27%
21.45%
27.74%
28.75%
0% 5% 10% 15% 20% 25% 30% 35% 40%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Cardiac Arrest - Surival to Discarge Rate (Utstein Comparator Group)
76.56%
80.12%
91.29%
70.73%
90.66%
75.09%
79.86%
64.95%
66.19%
80.51%
79.87%
0% 20% 40% 60% 80% 100%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Acute STEMI - % of Patients Receiving an Appropriate Care Bundle
97.13%
97.54%
99.62%
96.77%
98.66%
99.32%
98.51%
94.34%
96.14%
94.86%
98.37%
90% 92% 94% 96% 98% 100% 102%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Stroke - % of Suspected Stroke or Unresolved Transient Ischaemic Attack Patients Assessed Face to Face Receiving an
Appropriate Diagnostic Bundle
02:18
02:33
02:17
02:17
01:34
02:59
02:03
02:19
02:25
02:06
02:16
0% 2% 4% 6% 8% 10% 12% 14%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Acute STEMI - Mean time from call for help to catheter insertion for angiography
01:13
01:32
01:12
01:15
01:15
01:18
01:09
01:08
01:20
01:09
01:13
0% 1% 2% 3% 4% 5% 6% 7%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Stoke - Meant time from call to hsopital arrival for patients either FAST positive or with provisional diagnosis of stroke transported
by ambulance service
03:03
02:58
02:24
02:27
01:39
03:20
04:43
03:19
02:50
03:10
03:48
0% 5% 10% 15% 20% 25%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Stroke - Mean time from arrival at hospital to CT scan
00:54
00:57
00:58
00:41
00:45
01:06
00:50
00:56
00:53
01:01
00:52
0% 1% 2% 3% 4% 5%
National Average
East Midlands
East of England
London
North East
North West
South Central
South East Coast
South Western
West Midlands
Yorkshire
Outcome from Stroke Patients - Mean time from arrival at hospital to thrombolysis
Integrated Corporate Performance Report 13

YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
71,880 71,880 75,799 72,745 78,118 74,734 71,872 77,303 74,796 81,305 77,855 67,924 74,798
72,194 72,194 75,978 74,395 76,765 74,725 74,755 78,201 76,112 86,526 79,505 71,625 80,605
73,088 73,088
1.24% 1.24%
73,703 73,703 77,171 75,608 78,335 76,419 75,289 78,483 76,896 86,255 79,804 71,620 80,240
-0.83% -0.83%
A&E Incident Numbers
Actual A&E Incident Numbers 2016/17
Actual A&E Incident Numbers 2018/19
Variance 2017/18 vs 2016/17
Contract A&E Incident Numbers 2018/19
Variance Actual vs Contract 2017/18
Actual A&E Incident Numbers 2017/18
55,000
60,000
65,000
70,000
75,000
80,000
85,000
90,000
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Incident Numbers
Actual A&E Incident Numbers 2016/17 Actual A&E Incident Numbers 2017/18
Actual A&E Incident Numbers 2018/19 Contract A&E Incident Numbers 2018/19
16,000
16,500
17,000
17,500
18,000
18,500
19,000
19,500
20,000
All Ambulance Incidents per Week
Bath & North East Somerset CCG
2,087 3% Bristol, North Somerset
& South Gloucestershire CCG
11,801 16%
Dorset CCG 11,298 15%
Gloucestershire CCG 7,252 10%
Kernow CCG 7,999 11%
NEW Devon CCG 12,287 17%
Somerset CCG 7,475 10%
South Devon & Torbay CCG 4,773 7%
Swindon CCG 2,568 4%
Wiltshire CCG 5,389 7%
Unknown CCG 159 0%
Ambulance Incidents by CCG Year to Date
Integrated Corporate Performance Report 14

YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
2,087 2,087
11,801 11,801
11,298 11,298
7,252 7,252
7,999 7,999
12,287 12,287
7,475 7,475
4,773 4,773
2,568 2,568
5,389 5,389
159 159
73,088 73,088
1.07% 1.07%
-1.19% -1.19%
1.06% 1.06%
0.28% 0.28%
-0.21% -0.21%
-0.19% -0.19%
9.65% 9.65%
3.96% 3.96%
4.52% 4.52%
-0.66% -0.66%
1.24% 1.24%
0.87% 0.87%
-4.67% -4.67%
-0.31% -0.31%
-2.58% -2.58%
-1.53% -1.53%
-0.74% -0.74%
4.37% 4.37%
1.79% 1.79%
-0.81% -0.81%
-2.66% -2.66%
-0.83% -0.83%
Trust Total
A&E Incident Numbers % Variance Actual vs Contract 2018/19
Kernow CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Wiltshire CCG
NEW Devon CCG
Somerset CCG
South Devon & Torbay CCG
Swindon CCG
Somerset CCG
Wiltshire CCG
Trust Total
Gloucestershire CCG
A&E Incident Numbers % Variance 2018/19 vs 2017/18
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Dorset CCG
Bath & North East Somerset CCG
Bristol, North Somerset & South Gloucestershire CCG
Swindon CCG
Wiltshire CCG
Trust Total
Gloucestershire CCG
Dorset CCG
Kernow CCG
South Devon & Torbay CCG
Swindon CCG
A&E Incident Numbers
Bath & North East Somerset CCG
Dorset CCG
Bristol, North Somerset & South Gloucestershire CCG
Gloucestershire CCG
Kernow CCG
Unknown CCG
NEW Devon CCG
Integrated Corporate Performance Report 15

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
9.76% 9.76%
35.17% 35.17%
5.73% 5.73%
49.35% 49.35%
44.92% 44.92%
50.65% 50.65%
YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Source of A&E Incidents
47,610 47,610
9,127 9,127
16,351 16,351
73,088 73,088
YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Category of Incidents
5,252 5,252
35,129 35,129
20,416 20,416
1,272 1,272
3,466 3,466
7,553 7,553
73,088 73,088 0 0 0 0 0 0 0 0 0 0 0
See & Treat %
See & Convey Non ED %
See & Convey ED %
NHS 111 Incidents
Total
Category 1
Category 2
Total
Category 3
Category 4 (999)
Category 4 (HCP)
Category 4 H
A&E Incident Outcomes
Hear & Treat %
Public Incidents
HCP Incidents
% of Incidents Resolved Without Any Conveyance (Non Conveyance)
% of Incidents Resolved Without Conveyance to ED (Non Conveyance to ED)
Public Incidents 65%
HCP Incidents 13%
NHS 111 Incidents
22%
Source of A&E Incidents (YTD) Hear & Treat %
10%
See & Treat % 35%
See & Convey Non ED %
6%
See & Convey ED %
49%
A&E Incident Outcomes (YTD) Category 1
7%
Category 2 48% Category 3
28%
Category 4 (999) 2%
Category 4 (HCP) 5%
Category 4 H 10%
Category of A&E Incidents (YTD)
Integrated Corporate Performance Report 16

YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
36,355 36,355 38,266 37,238 38,509 38,176 38,361 40,078 10,915 43,289 42,293 38,136 41,901
14,581 14,581 15,407 14,734 14,976 15,868 16,492 15,322 4,495 19,382 18,422 12,791 13,230
40.11% 40.11% 40.26% 39.57% 38.89% 41.57% 42.99% 38.23% 41.18% 44.77% 43.56% 33.54% 31.57%
2036:04 2036:04 2160:27 2107:43 2137:55 2326:41 2614:35 2353:20 685:11 3581:33 2888:03 2077:25 2362:35
67:52 67:52 69:41 70:15 68:57 75:03 87:09 75:54 22:50 115:32 93:09 74:11 76:12
39,657 39,657
10,898 10,898
27.48% 27.48%
1616:44 1616:44
53:53 53:53
36,438 36,438
13,202 13,202
36.23% 36.23%
2278:49 2278:49
75:57 75:57
Total Operational Resources Hours Lost to Handover Delays in Excess of 15 Minutes 2018/19
Average Operational Resources Hours Lost to Handover Delays in Excess of 15 Minutes per Day 2018/19
Handover to Clear Delays
Total Number of Handover to Clear Times Recorded at Acute Hospitals
Total Number of Handover to Clears in Excess of 15 Minutes
% of Handover to Clear Times in Excess of 15 Minutes
Handover Delays
Total Number of Handovers Reported at Acute Hospitals 2018/19
Total Number of Handovers in Excess of 15 Minutes 2018/19
% of Handovers in Excess of 15 Minutes 2018/19
Average Operational Resources Hours Lost to Handover Delays in Excess of 15 Minutes per Day 2017/18
Total Number of Handovers Reported at Acute Hospitals 2017/18
Total Number of Handovers in Excess of 15 Minutes 2017/18
% of Handovers in Excess of 15 Minutes 2017/18
Total Operational Resources Hours Lost to Handover Delays in Excess of 15 Minutes 2017/18
Total Operational Resources Hours Lost to Handover to Clear Delays in Excess of 15 Minutes
Average Operational Resources Hours Lost to Handover to Clear Delays in Excess of 15 Minutes per Day
0:00
24:00
48:00
72:00
96:00
120:00
144:00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Average Daily Operational Time Lost to Handover Delays at Hospitals in Excess of 15 Minutes
Average Operational Resources Hours Lost to Handover Delays in Excess of 15 Minutes per Day 2017/18
Average Operational Resources Hours Lost to Handover Delays in Excess of 15 Minutes per Day 2018/19
0:00
12:00
24:00
36:00
48:00
60:00
72:00
84:00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Average Daily Operational Time Lost to Handover to Clear Delays at Hospitals in Excess of 15 Minutes
Average Operational Resources Hours Lost to Handover to Clear Delays in Excess of 15 Minutes per Day
Integrated Corporate Performance Report 17

YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
2,638 2,638875 875
3,486 3,4861,391 1,3912,866 2,8662,235 2,2352,488 2,4881,297 1,2972,177 2,1772,098 2,0983,180 3,1802,659 2,6592,749 2,7491,148 1,1483,029 3,0292,464 2,464927 927
1,393 1,39339,100 39,100
YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
14:08 14:0809:50 09:4916:10 16:1011:10 11:0910:14 10:1309:47 09:4613:03 13:0213:01 13:0014:37 14:3714:19 14:1812:38 12:3812:54 12:5311:30 11:3010:13 10:1211:56 11:5511:26 11:2614:49 14:4809:21 09:2012:28 12:28
Royal Bournemouth Hospital
Royal Cornwall Hospital
Poole Hospital
Royal Devon & Exeter Hospital
Royal United Hospital Bath
Salisbury District Hospital
Southmead Hospital
Torbay Hospital
Weston General Hospital
Yeovil District Hospital
Total All Hospitals
Salisbury District Hospital
Southmead Hospital
Weston General Hospital
Yeovil District Hospital
Torbay Hospital
Total All Hospitals
Number of Handovers by Acute HospitalBristol Royal Infirmary
Cheltenham General Hospital
Derriford Hospital
Dorset County Hospital
Gloucester Royal Hospital
Great Western Hospital
Musgrove Park Hospital
North Devon District Hospital
Poole Hospital
Royal Bournemouth Hospital
Royal Cornwall Hospital
Bristol Royal Infirmary
Cheltenham General Hospital
Derriford Hospital
Dorset County Hospital
Gloucester Royal Hospital
Great Western Hospital
Musgrove Park Hospital
North Devon District Hospital
Royal Devon & Exeter Hospital
Royal United Hospital Bath
Average Handover Time per Incident (Mins:Sec)
Integrated Corporate Performance Report 18

YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Operational Resource Hours Lost to Handover Delays in Excess of 15 Minutes (Hours:Mins)147:26 147:2617:38 17:38
269:17 269:1752:50 52:5059:14 59:1451:18 51:18
106:19 106:1962:03 62:03
122:47 122:47136:44 136:44109:19 109:1974:48 74:4861:47 61:4728:56 28:56
112:52 112:52107:22 107:2258:46 58:4621:09 21:09
1600:43 1600:43
Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
90.00% 90.1% 90.1%
RAG Rating Green Green
90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
Other Metrics to be developed and included in future reports (when available):
Infection Prevention and Control Metrics (Quarterly)Training Compliance (Annual Development Day and Training Workbook completion compared to plan)
Bristol Royal Infirmary
Cheltenham General Hospital
North Devon District Hospital
Poole Hospital
Royal Bournemouth Hospital
Royal Cornwall Hospital
Yeovil District Hospital
Total All Hospitals
Southmead Hospital
Torbay Hospital
Weston General Hospital
Royal Devon & Exeter Hospital
Royal United Hospital Bath
Salisbury District Hospital
* The Information Governance Toolkit has been superseded by the Data Security and Protection Toolkit. The Trust is awaiting release of the new standards in relation to the revised toolkit (expected in July 2018). The Trust is therefore continuing to RAG rate itself as Green against the old Information Governance Toolkit standards based on the most recent toolkit submission, pending release of the revised standards. Once released the report will be updated to reflect the revised standards and the appropriate RAG rating against these standards.
Information Governance Toolkit Compliance *
Derriford Hospital
Dorset County Hospital
Gloucester Royal Hospital
Great Western Hospital
Vehicle deep cleaning compliance with schedule (A&E)
Other Performance Metrics
Musgrove Park Hospital
90.1%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Vehicle Deep Clean Compliance (A&E Vehicles)
Integrated Corporate Performance Report 19

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
10,365 10,365 8,881 7,345 8,349 8,150 7,778 8,194 7,757 12,474 9,226 8,134 10,381
9,532 9,532
-8% -8%
Out of Hours Patient Contacts
Dorset Out of Hours Patient Contacts - Actual 2017/18
Dorset Out of Hours Patient Contacts - Actual 2018/19 vs 2017/18
Dorset Out of Hours Patient Contacts - Actual 2018/19
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Dorset Out of Hours Patient Contacts
2017/18 2018/19
Integrated Corporate Performance Report 20

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
95.00% 90.06% 89.10% 88.87% 89.86% 91.63% 87.30% 91.77% 84.58% 92.14% 89.69% 92.21% 94.23% 89.47%
454 454
95.00% 91.63% 91.63%
95.00% 95.52% 94.13% 97.17% 97.45% 97.41% 97.16% 95.96% 92.67% 97.71% 90.34% 95.57% 98.93% 94.79%
1,107 1,107
95.00% 96.84% 96.84%Target Call 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Target Call 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%Target/
KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
95.00% 90.00% 91.86% 93.85% 93.37% 88.67% 86.96% 91.40% 85.50% 93.44% 84.52% 92.16% 90.75% 89.31%
345 345
95.00% 88.12% 88.12%
95.00% 97.56% 97.57% 98.16% 97.03% 98.22% 98.28% 98.64% 98.89% 98.87% 93.54% 98.66% 98.62% 96.16%
2,964 2,964
95.00% 98.35% 98.35%Target Call 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Target Call Answering 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Dorset - % of Urgent Home Visits Completed within 2 Hours - 2017/18
Dorset - % of Urgent Home Visits Completed within 2 Hours - 2018/19
Out of Hours - Home Visits - Urgent Completed within 2 Hours
Dorset - Number of Urgent Home Visits 2018/19
Out of Hours - Home Visits - Less Urgent Completed within 6 HoursDorset - % of Less Urgent Home Visits Completed within 6 Hours - 2017/18
Dorset - % of Less Urgent Treatment Centre Completed within 6 Hours - 20117/18
Dorset - % of Urgent Treatment Centre Completed within 2 Hours - 2016/17
Out of Hours - Treatment Centres - Urgent Completed within 2 Hours
Dorset - % of Less Urgent Treatment Centre Completed within 6 Hours - 2016/17
Dorset - Number of Less Urgent Treatment Centre Appointments 2017/18
Dorset - % of Urgent Treatment Centre Completed within 2 Hours - 20117/18
Dorset - Number of Urgent Treatment Cente Appointments 2017/18
Out of Hours - Treatment Centres - Less Urgent Completed within 6 Hours
Dorset - % of Less Urgent Home Visits Completed within 6 Hours - 2018/19
Dorset - Number of Less Urgent Home Visits 2018/19
050100150200250300350400450500
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Dorset Out of Hours - Urgent Home Visits Completed in 2 Hours
Dorset - Number of Urgent Home Visits 2018/19 % Completed in 2 Hours 2017/18 % Completed in 2 Hours 2018/19 Target
0
200
400
600
800
1,000
1,200
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Dorset Out of Hours - Less Urgent Home Visits Completed in 6 Hours
Dorset - Number of Less Urgent Home Visits 2018/19 % Completed in 6 Hours 2017/18
% Completed in 6 Hours 2018/19 Target
050100150200250300350400
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Dorset Out of Hours - Urgent Treatment Centre Appointments Completed in 2 Hours
Dorset - Number of Urgent Treatment Cente Appointments 2017/18 % Completed in 2 Hours 2016/17
% Completed in 2 Hours 2017/18 Target
0
500
1,000
1,500
2,000
2,500
3,000
3,500
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Dorset Out of Hours - Less Urgent Treatment Centre Appointments Completed in 6 Hours
Dorset - Number of Less Urgent Treatment Centre Appointments 2017/18 % Completed in 6 Hours 2016/17 % Completed in 6 Hours 2017/18 Target
Integrated Corporate Performance Report 21
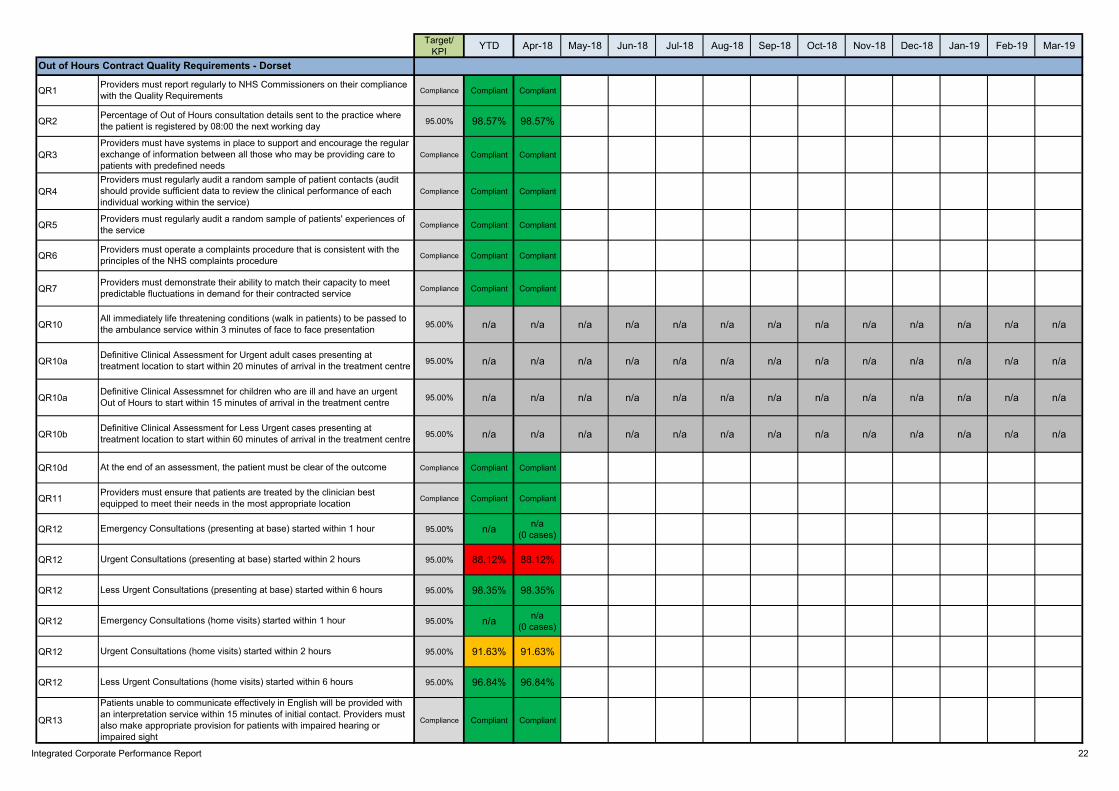
Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
QR1 Compliance Compliant Compliant
QR2 95.00% 98.57% 98.57%
QR3 Compliance Compliant Compliant
QR4 Compliance Compliant Compliant
QR5 Compliance Compliant Compliant
QR6 Compliance Compliant Compliant
QR7 Compliance Compliant Compliant
QR10 95.00% n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a
QR10a 95.00% n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a
QR10a 95.00% n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a
QR10b 95.00% n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a
QR10d Compliance Compliant Compliant
QR11 Compliance Compliant Compliant
QR12 95.00% n/a n/a(0 cases)
QR12 95.00% 88.12% 88.12%
QR12 95.00% 98.35% 98.35%
QR12 95.00% n/a n/a(0 cases)
QR12 95.00% 91.63% 91.63%
QR12 95.00% 96.84% 96.84%
QR13 Compliance Compliant Compliant
Patients unable to communicate effectively in English will be provided with an interpretation service within 15 minutes of initial contact. Providers must also make appropriate provision for patients with impaired hearing or impaired sight
Less Urgent Consultations (home visits) started within 6 hours
Urgent Consultations (home visits) started within 2 hours
Providers must demonstrate their ability to match their capacity to meet predictable fluctuations in demand for their contracted service
All immediately life threatening conditions (walk in patients) to be passed to the ambulance service within 3 minutes of face to face presentation
Definitive Clinical Assessment for Urgent adult cases presenting at treatment location to start within 20 minutes of arrival in the treatment centre
Definitive Clinical Assessmnet for children who are ill and have an urgent Out of Hours to start within 15 minutes of arrival in the treatment centre
Definitive Clinical Assessment for Less Urgent cases presenting at treatment location to start within 60 minutes of arrival in the treatment centre
At the end of an assessment, the patient must be clear of the outcome
Providers must ensure that patients are treated by the clinician best equipped to meet their needs in the most appropriate location
Emergency Consultations (presenting at base) started within 1 hour
Urgent Consultations (presenting at base) started within 2 hours
Providers must regularly audit a random sample of patients' experiences of the service
Providers must regularly audit a random sample of patient contacts (audit should provide sufficient data to review the clinical performance of each individual working within the service)
Providers must have systems in place to support and encourage the regular exchange of information between all those who may be providing care to patients with predefined needs
Percentage of Out of Hours consultation details sent to the practice where the patient is registered by 08:00 the next working day
Providers must report regularly to NHS Commissioners on their compliance with the Quality Requirements
Less Urgent Consultations (presenting at base) started within 6 hours
Emergency Consultations (home visits) started within 1 hour
Out of Hours Contract Quality Requirements - Dorset
Providers must operate a complaints procedure that is consistent with the principles of the NHS complaints procedure
Integrated Corporate Performance Report 22

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
21,983 21,983 20,523 18,111 19,981 19,456 18,061 19,380 18,303 25,842 20,939 18,558 24,648
21,683 21,683
23,852 23,852 24,954 22,660 23,175 24,523 22,740 21,503 21,017 29,322 24,610 19,992 23,003
-9.10% -9.10%
Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
95.00% 87.01% 88.95% 83.44% 87.88% 88.25% 89.46% 88.44% 85.37% 83.84% 84.39% 92.83% 90.88% 81.89%
95.00% 89.60% 89.60%Target Call 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
NHS 111 - Dorset Calls Offered - Actual 2018/19
NHS 111 - Dorset Calls Offered - Contract 2018/19
Percentage of Calls Offered - NHS 111 Dorset Actual vs Contract
NHS 111 Calls Offered
NHS 111 - Dorset - Percentage of Calls Answered in 60 Seconds 2018/19
NHS 111 - Dorset - Percentage of Calls Answered in 60 Seconds 2017/18
NHS 111 - Dorset Calls Offered - Actual 2017/18
NHS 111 Call Answering in 60 Seconds
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 Dorset Calls Offered
Actual 2017/18 Actual 2018/19 Contract 2018/19
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 Dorset - % of Calls Answered in 60 Seconds
% Answered in 60 Seconds 2017/18 % Answered in 60 Seconds 2018/19 Target Call Answering Performance %
Integrated Corporate Performance Report 23

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
QR1 Compliance Compliant Compliant
QR2 95.00% 97.41% 97.41%
QR3 Compliance Compliant Compliant
QR4 Compliance Partially Compliant
Partially Compliant
QR5 1.00% 0.78% 0.78%
QR6 Compliance Compliant Compliant
QR7 Compliance Partially Compliant
Partially Compliant
QR8a 5.00% 2.40% 2.40%
QR8b 95.00% 89.60% 89.60%
QR9a 95.00% 100.00% 100.00%
QR9b 95.00% 30.78% 30.78%
QR13 95.00% 100.00% 100.00%
QR14 Compliance Compliant Compliant
QR15 Compliance Compliant Compliant
Patients unable to communicate effectively in English will be provided with an interpretation service within 15 minutes of initial contact. Providers must also make appropriate provision for patients with impaired hearing or impaired sight
Providers must demonstrate the online completion of the annual assessment of the Information Governance Toolkit at level 2 or above and that this is audited on an annual basis by Internal Auditors using the national framework
Providers must demonstrate that they are complying with the Department of Health Information Governance SUI Guidance on reporting of Information Governance incidents appropriately.
Providers must report regularly to NHS Commissioners on their compliance with the Quality Requirements
All immediately life threatening conditions to be passed to the ambulance service within 3 minutes
Providers must send details of all consultations (including appropriate clinical information) to the practice where the patient is registered by 8.00 a.m. the next working day.
Calls to be answered within 60 seconds of the end of the introductory message
No more than 5% of calls abandoned before being answered
Providers must demonstrate their ability to match their capacity to meet predictable fluctuations in demand for their contracted service
Providers must operate a complaints procedure that is consistent with the principles of the NHS complaints procedure
Providers must regularly audit a random sample of patients' experiences of the service
Providers must regularly audit a random sample of patient contacts (audit should provide sufficient data to review the clinical performance of each individual working within the service)
Providers must have systems in place to support and encourage the regular exchange of information between all those who may be providing care to patients with predefined needs
Patient callbacks must be achieved within 10 minutes
NHS 111 Contract Quality Requirements - Dorset
Integrated Corporate Performance Report 24

NHS 111 Sitrep BenchmarkingTarget 05-Feb-18 12-Feb-18 19-Feb-18 26-Feb-18 05-Mar-18 12-Mar-18 19-Mar-18 26-Mar-18 02-Apr-18 09-Apr-18 16-Apr-18 23-Apr-18 30-Apr-18
95.00% 70.83% 67.26% 70.89% 66.66% 66.59% 71.65% 74.30% 76.74% 74.46% 86.93% 84.55% 88.79% 86.94%95.00% 88.40% 92.82% 92.70% 58.21% 83.52% 86.95% 87.73% 94.60% 90.13% 90.24% 88.76% 88.45% 86.27%95.00% 94.37% 92.82% 93.78% 91.07% 92.59% 94.62% 95.80% 96.23% 97.78% 96.98% 95.74% 98.21% 96.17%95.00% 51.25% 46.62% 42.03% 40.80% 38.69% 48.09% 43.36% 58.58% 60.17% 73.76% 72.80% 70.85% 67.47%
5.00% 6.33% 8.13% 6.95% 9.19% 7.93% 6.78% 5.86% 4.84% 5.38% 2.41% 3.18% 2.26% 2.49%5.00% 1.66% 0.99% 0.93% 11.45% 2.77% 2.12% 2.30% 0.79% 2.80% 1.94% 3.26% 1.89% 1.78%5.00% 11.98% 16.62% 16.81% 21.55% 18.44% 23.90% 18.06% 11.90% 11.41% 9.58% 7.39% 7.84% 7.57%5.00% 1.49% 0.99% 0.93% 1.69% 1.20% 1.02% 0.75% 0.52% 0.91% 0.41% 1.02% 0.25% 0.43%
40.90% 40.18% 40.85% 41.87% 41.37% 41.24% 41.95% 44.91% 44.50% 43.48% 43.76% 44.14% 44.33%44.66% 43.19% 46.54% 48.21% 48.37% 49.91% 47.73% 50.77% 47.94% 46.35% 47.44% 49.20% 48.50%68.69% 70.75% 66.85% 67.15% 67.03% 66.38% 63.16% 78.26% 65.95% 84.36% 78.42% 70.62% 83.90%17.07% 17.60% 20.68% 21.05% 21.77% 21.30% 23.29% 21.95% 24.20% 24.88% 25.75% 27.26% 27.09%
NHS 111 KPI Benchmarking - Weekly Sitrep Data - Call Backs in 10 Minutes95.00% 39.03% 37.56% 38.92% 39.53% 38.13% 39.81% 40.09% 45.10% 42.13% 39.57% 40.53% 43.25% 42.33%95.00% 43.56% 41.92% 36.86% 27.75% 38.15% 34.36% 37.95% 25.45% 24.06% 32.79% 34.93% 36.72% 33.76%95.00% 80.78% 76.65% 80.68% 74.20% 79.59% 87.83% 82.02% 81.91% 71.02% 86.36% 80.63% 74.40% 79.96%95.00% 15.56% 13.47% 19.26% 20.64% 19.19% 18.96% 17.52% 25.45% 19.29% 15.60% 23.90% 26.16% 22.83%
Percentage of Call Backs in 10 Minutes - DorsetPercentage of Call Backs in 10 Minutes - National HighestPercentage of Call Backs in 10 Minutes - National Lowest
Percentage of Call Backs Offered - National HighestPercentage of Call Backs Offered - National Lowest
Percentage of Call Backs in 10 Minutes - National Average
Percentage of Calls Answered in 60 Seconds - National Lowest
NHS 111 KPI Benchmarking - Weekly Sitrep Data - Call Abandonment
Percentage of Call Backs Offered - National AveragePercentage of Call Backs Offered - Dorset
NHS 111 KPI Benchmarking - Weekly Sitrep Data - % of Calls Answered or Dealt with by a Clinician
Percentage of Calls Abandoned - National AveragePercentage of Calls Abandoned - DorsetPercentage of Calls Abandoned - National HighestPercentage of Calls Abandoned - National Lowest
Percentage of Calls Answered in 60 Seconds - DorsetPercentage of Calls Answered in 60 Seconds - National Highest
NHS 111 KPI Benchmarking - Weekly Sitrep Data - Call AnsweringPercentage of Calls Answered in 60 Seconds - National Average
Week Commencing
30%
40%
50%
60%
70%
80%
90%
100%
05-Feb-18 12-Feb-18 19-Feb-18 26-Feb-18 05-Mar-18 12-Mar-18 19-Mar-18 26-Mar-18 02-Apr-18 09-Apr-18 16-Apr-18 23-Apr-18 30-Apr-18
Weekly National NHS 111 Sitrep - % Calls Answered in 60 Seconds
National Average Dorset Highest Lowest
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
05-Feb-18 12-Feb-18 19-Feb-18 26-Feb-18 05-Mar-18 12-Mar-18 19-Mar-18 26-Mar-18 02-Apr-18 09-Apr-18 16-Apr-18 23-Apr-18 30-Apr-18
Weekly National NHS 111 Sitrep - % of Calls Answered or Dealt with by a Clinician
National Average Dorset Highest Lowest
0%
5%
10%
15%
20%
25%
05-Feb-18 12-Feb-18 19-Feb-18 26-Feb-18 05-Mar-18 12-Mar-18 19-Mar-18 26-Mar-18 02-Apr-18 09-Apr-18 16-Apr-18 23-Apr-18 30-Apr-18
Weekly National NHS 111 Sitrep - % Calls Abandoned
National Average Dorset Highest Lowest
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
05-Feb-18 12-Feb-18 19-Feb-18 26-Feb-18 05-Mar-18 12-Mar-18 19-Mar-18 26-Mar-18 02-Apr-18 09-Apr-18 16-Apr-18 23-Apr-18 30-Apr-18
Weekly National NHS 111 Sitrep - % of Call Backs in 10 Minutes
National Average Dorset Highest Lowest
Integrated Corporate Performance Report 25

Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
1,321 1,321 1,436 1,320 1,401 1,205 1,238 1,208 1,173 1,163 1,193 1,105 1,287
1,419 1,419
1,425 1,425 1,356 1,405 1,392 1,392 1,343 1,274 1,235 1,212 1,240 1,177 1,505
-0.42% -0.42%
Target/KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
1,302 1,302
1,296 1,296
95.00% 99.54% 99.54%
1,302 1,302
1,262 1,262
95.00% 96.93% 96.93%Target Call 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Tiverton UCC - Number of Patients Seen within 4 Hours 2018/19
Tiverton UCC - % of Patients Seen within 4 Hours 2018/19
Tiverton UCC - Number of Cases 2018/19
Tiverton UCC - Number of Patients Triaged within 15 Minutes 2018/19
Tiverton UCC - % of Patients Triaged within 15 Minutes 2018/19
Tiverton UCC - Number of Cases 2018/19
Tiverton Urgent Care CentreTiverton Urgent Care Centre Activity - Actual 2017/18
Tiverton Urgent Care Centre Activity - Actual 2018/19
Tiverton Urgent Care Centre Activity - Contract Baseline 2018/19
Percentage Actual vs Contract - Tiverton Urgent Care Centre Activity
Tiverton Urgent Care Centre
1,419
0
200
400
600
800
1,000
1,200
1,400
1,600
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Tiverton Urgent Care Centre Activity
Actual 2018/19 Actual 2017/18 Contract 2018/19
0
200
400
600
800
1,000
1,200
1,400
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Tiverton Urgent Care Centre - % of Patients Seen Within 4 Hours 2018/19
Tiverton UCC - Number of Cases 2018/19 Tiverton UCC - % of Patients Seen within 4 Hours 2018/19 Target
0
200
400
600
800
1,000
1,200
1,400
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Tiverton Urgent Care Centre - % of Patients Seen Within 4 Hours 2018/19
Tiverton UCC - Number of Cases 2018/19 Tiverton UCC - % of Patients Triaged within 15 Minutes 2018/19 Target
Integrated Corporate Performance Report 26

Staff Metrics - Establishment and Staff TurnoverTrust Summary- Staff Metrics
Integrated Corporate Performance Report
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust Total Establishment - Actual WTE 3,966.58
Trust Total Establishment - Funded WTE 4,012.02
Variance -45.44
Vacancy % -1.1%
Support Services - Actual WTE 557.38
Support Services - Funded WTE 585.07
Variance -27.69
Vacancy % -4.7%
Trust Total Staff TurnoverApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Turnover % (excl redundancies) 13.06%
0
100
200
300
400
500
600
700
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Support Services Establishment
Support Services - Funded WTE Support Services - Actual WTE
3,000
3,200
3,400
3,600
3,800
4,000
4,200
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust Total Establishment
Trust Total Establishment - Funded WTE Trust Total Establishment - Actual WTE
13.06%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
18.00%
20.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust - Staff Turnover (exc Redundancies)
Turnover % (excl redundancies)
Integrated Corporate Performance Report 27

A&E Operations Establishment
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Lead Clinician - Actual WTE 1,717.14
Lead Clinician - Funded WTE 1,795.12
Variance -77.98
Vacancy % -4.3%
Emergency Care Assistants - Actual WTE 1,030.43
Emergency Care Assistants- Funded WTE 957.78
Variance 72.65
Vacancy % 7.6%
Total A&E Operations Establishment - Actual WTE 2,808.59
Total A&E Operations Establishment - Funded WTE 2,816.00
Variance -7.41
Vacancy % -0.3%
A&E Operations - TurnoverApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Turnover % (excl redundancies) 9.68%
Turnover % (Lead Clinician) 8.87%
Turnover % (Emergency Care Assistants) 11.17%
1,000.00
1,100.00
1,200.00
1,300.00
1,400.00
1,500.00
1,600.00
1,700.00
1,800.00
1,900.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations - Lead Clinician Establishment
Lead Clinician - Funded WTE Lead Clinician - Actual WTE
500.00
600.00
700.00
800.00
900.00
1,000.00
1,100.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations - Emergency Care Assistants Establishment
Emergency Care Assistants- Funded WTE Emergency Care Assistants - Actual WTE
8.87%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
18.00%
20.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations - Lead Clinician Turnover
Turnover % (Lead Clinician)
11.17%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
18.00%
20.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations - Emergency Care Assistants Turnover
Turnover % (Emergency Care Assistants)
Integrated Corporate Performance Report 28

A&E Clinical Hub Establishment
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Clinician- Actual WTE 72.13
Clinician - Funded WTE 74.00
Variance -1.87
Vacancy % -2.5%
Total A&E Clinical Hub Establishment - Actual WTE 420.86
Total A&E Clinical Hub Establishment - Funded WTE 414.89
Total Variance 5.97
Vacancy % 1.4%
A&E Clinical Hub - TurnoverApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Turnover % (excl redundancies) 25.96%
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Clinical Hub - Clinician Establishment
Clinician - Funded WTE Clinician- Actual WTE
200.00
250.00
300.00
350.00
400.00
450.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Clinical Hub - Total Establishment
Total A&E Clinical Hub Establishment - Funded WTE Total A&E Clinical Hub Establishment - Actual WTE
25.96%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Clinical Hub - Staff Turnover (exc Redundancies)
Turnover % (excl redundancies)
Integrated Corporate Performance Report 29

UCS - Out of Hours Establishment
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours Clinician - Actual WTE 29.00
UCS Out of Hours Clinician - Funded WTE 42.34
Variance -13.34
Vacancy % -31.5%
Total UCS Out of Hours Establishment - Actual WTE 90.62
Total UCS Out of Hours Establishment - Funded WTE 116.68
Variance -26.06
Vacancy % -22.3%
Out of Hours Service - Turnover (excl redundancies)
UCS Out of Hours - TurnoverApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Turnover % (excl redundancies) 17.30%
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours - Clinician Establishment
UCS Out of Hours Clinician - Funded WTE UCS Out of Hours Clinician - Actual WTE
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours - Total Establishment
Total UCS Out of Hours Establishment - Funded WTE Total UCS Out of Hours Establishment - Actual WTE
17.30%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Out of Hours Service Staff Turnover (excl redundancies)
Turnover % (excl redundancies)
Integrated Corporate Performance Report 30

UCS - NHS 111 Establishment
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 Clinician - Actual WTE 20.63
NHS 111 Clinician - Funded WTE 19.84
Variance 0.79
Vacancy % 4.0%
Total NHS 111 Establishment - Actual WTE 89.13
Total NHS 111 Establishment - Funded WTE 79.08
Variance 10.05
Vacancy % 12.7%
NHS 111 Service - Turnover (excl redundancies)
NHS 111 Service - TurnoverApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Turnover % (excl redundancies) 35.04%
0.00
5.00
10.00
15.00
20.00
25.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 - Clinician Establishment
NHS 111 Clinician - Funded WTE NHS 111 Clinician - Actual WTE
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 - Total Establishment
Total NHS 111 Establishment - Funded WTE Total NHS 111 Establishment - Actual WTE
35.04%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 Service Staff Turnover (excl redundancies)
Turnover % (excl redundancies)
Integrated Corporate Performance Report 31

Staff Metrics - Operational 'On the Road' Establishment ForecastThe Operational establishment position is also analysed based on the date when the staff become operationally available (ie when new staff become operationally active after initial training and induction periods)In order to produce this adjusted position a set of simple rules have been agreed between Operations and HR which are applied to the date that a new member of staff commences employment with the Trust: Lead Clinicians - 4 weeks after their commencement date Emergency Care Assistants - 8 weeks after their commencement date Clinical Hub Call Takers - 8 weeks after their commencment date Clinical Hub Clinicians - 4 weeks after their commencement dateThe position detailed in the tables below are based on the forecast establishment positon at the time of the report. All of the figures below are based on the date the staff become operationally available.West Division
Actual WTEApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Lead Clinician - Actual 'On the Road' WTE 553.26 550.99 548.71 546.43 544.15 540.88 539.60 537.32 535.05 531.76 534.49 548.71
Lead Clinician - Funded WTE 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14 561.14
Variance -7.88 -10.15 -12.43 -14.71 -16.99 -20.26 -21.54 -23.82 -26.09 -29.38 -26.65 -12.43
Vacancy % -1.4% -1.8% -2.2% -2.6% -3.0% -3.6% -3.8% -4.2% -4.6% -5.2% -4.7% -2.2%
Emergency Care Assistant - Actual 'On the Road' WTE 352.87 348.86 372.85 379.83 376.82 375.80 377.79 373.78 377.76 373.75 358.74 362.72
Emergency Care Assistant - Funded WTE 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87 340.87
Variance 12.00 7.99 31.98 38.96 35.95 34.93 36.92 32.91 36.89 32.88 17.87 21.85
Vacancy % 3.5% 2.3% 9.4% 11.4% 10.5% 10.2% 10.8% 9.7% 10.8% 9.6% 5.2% 6.4%
Total A&E Operations Establishment - Actual 'On the Road' WTE 906.13 899.85 921.56 926.26 920.97 916.68 917.39 911.10 912.81 905.51 893.23 911.43
Total A&E Operations Establishment - Funded WTE 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01 902.01
Variance 4.12 -2.16 19.55 24.25 18.96 14.67 15.38 9.09 10.80 3.50 -8.78 9.42
Vacancy % 0.5% -0.2% 2.2% 2.7% 2.1% 1.6% 1.7% 1.0% 1.2% 0.4% -1.0% 1.0%
East Division
Actual WTEApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Lead Clinician - Actual 'On the Road' WTE 430.12 428.28 428.45 429.61 432.78 427.95 452.11 474.28 484.45 479.61 487.78 486.94
Lead Clinician - Funded WTE 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52 472.52
Variance -42.40 -44.24 -44.07 -42.91 -39.74 -44.57 -20.41 1.76 11.93 7.09 15.26 14.42
Vacancy % -9.0% -9.4% -9.3% -9.1% -8.4% -9.4% -4.3% 0.4% 2.5% 1.5% 3.2% 3.1%
Emergency Care Assistant - Actual 'On the Road' WTE 273.59 270.81 288.03 285.25 283.46 285.68 284.90 282.12 279.33 276.55 272.77 277.99
Emergency Care Assistant - Funded WTE 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81 266.81
Variance 6.78 4.00 21.22 18.44 16.65 18.87 18.09 15.31 12.52 9.74 5.96 11.18
Vacancy % 2.5% 1.5% 8.0% 6.9% 6.2% 7.1% 6.8% 5.7% 4.7% 3.7% 2.2% 4.2%
Total A&E Operations Establishment - Actual 'On the Road' WTE 703.71 699.09 716.48 714.86 716.24 713.63 737.01 756.40 763.78 756.16 760.55 764.93
Total A&E Operations Establishment - Funded WTE 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33 739.33
Variance -35.62 -40.24 -22.85 -24.47 -23.09 -25.70 -2.32 17.07 24.45 16.83 21.22 25.60
Vacancy % -4.8% -5.4% -3.1% -3.3% -3.1% -3.5% -0.3% 2.3% 3.3% 2.3% 2.9% 3.5%
2018/19 Forecast WTE Based on Operational Assumptions
2018/19 Forecast WTE Based on Operational Assumptions
400
420
440
460
480
500
520
540
560
580
600
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
West Division - Lead Clinician Establishment
Lead Clinician - Actual 'On the Road' WTE Lead Clinician - Funded WTE
200
220
240
260
280
300
320
340
360
380
400
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
West Division - Emergency Care Assistant Establishment
Emergency Care Assistant - Actual 'On the Road' WTE Emergency Care Assistant - Funded WTE
300
320
340
360
380
400
420
440
460
480
500
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
East Division - Lead Clinician Establishment
Lead Clinician - Actual 'On the Road' WTE Lead Clinician - Funded WTE
120
140
160
180
200
220
240
260
280
300
320
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
East Division - Emergency Care Assistant Establishment
Emergency Care Assistant - Actual 'On the Road' WTE Emergency Care Assistant - Funded WTE
Integrated Corporate Performance Report 32

North Division
Actual WTEApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Lead Clinician - Actual 'On the Road' WTE 577.37 572.58 570.79 566.00 563.21 555.41 565.62 578.83 592.04 584.25 584.46 590.67
Lead Clinician - Funded WTE 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21 611.21
Variance -33.84 -38.63 -40.42 -45.21 -48.00 -55.80 -45.59 -32.38 -19.17 -26.96 -26.75 -20.54
Vacancy % -5.5% -6.3% -6.6% -7.4% -7.9% -9.1% -7.5% -5.3% -3.1% -4.4% -4.4% -3.4%
Emergency Care Assistant - Actual 'On the Road' WTE 353.16 348.70 376.24 371.78 380.31 389.85 389.39 384.93 384.47 380.01 359.04 362.58
Emergency Care Assistant - Funded WTE 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01 353.01
Variance 0.15 -4.31 23.23 18.77 27.30 36.84 36.38 31.92 31.46 27.00 6.03 9.57
Vacancy % 0.0% -1.2% 6.6% 5.3% 7.7% 10.4% 10.3% 9.0% 8.9% 7.6% 1.7% 2.7%
Total A&E Operations Establishment - Actual 'On the Road' WTE 930.53 921.28 947.03 937.78 943.52 945.26 955.01 963.76 976.51 964.26 943.50 953.25
Total A&E Operations Establishment - Funded WTE 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22 964.22
Variance -33.69 -42.94 -17.19 -26.44 -20.70 -18.96 -9.21 -0.46 12.29 0.04 -20.72 -10.97
Vacancy % -3.5% -4.5% -1.8% -2.7% -2.1% -2.0% -1.0% 0.0% 1.3% 0.0% -2.1% -1.1%
Clinical Hub
Actual WTEApr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Call Takers - Actual 'in The Room' WTE 150.50 152.96 159.43 157.89 157.35 157.82 156.28 157.74 156.21 159.67 152.13 156.60
Call takers - Funded WTE 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89 152.89
Variance -2.39 0.07 6.54 5.00 4.46 4.93 3.39 4.85 3.32 6.78 -0.76 3.71
Vacancy % -1.6% 0.0% 4.3% 3.3% 2.9% 3.2% 2.2% 3.2% 2.2% 4.4% -0.5% 2.4%
Clinician - Actual 'In The Room' WTE 71.73 72.07 74.51 74.95 74.39 73.83 74.27 73.71 74.15 74.59 75.03 75.47
Clinician - Funded WTE 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00 75.00
Variance -3.27 -2.93 -0.49 -0.05 -0.61 -1.17 -0.73 -1.29 -0.85 -0.41 0.03 0.47
Vacancy % -4.4% -3.9% -0.7% -0.1% -0.8% -1.6% -1.0% -1.7% -1.1% -0.5% 0.0% 0.6%
2018/19 Forecast WTE Based on Operational Assumptions
The Trust is currently forecasting a 2018/19 year end vacancy level of 7.07 WTE Lead Clinicians, however the above tables reflect the position for 'on the road' establishment available to undertake operational duties and therefore reports a slightly higher level of vanacy at the end of March 2019. All 7 new Lead Clinicians recruited from New Zealand have commenced duties with SWASFT, with the last 5 of these 7 scheduled to act as Lead Clinicians from June 2018. 234 applications have been received to date for the 2018/19 graduate campaign, 152 have so far been successful with their assessments, 9 are in review and 12 were unsuccessful. A further 41 are booked in for assessments between May and September 2018, the remaining 20 applicants withdrew. Mapping of the successful candidates is currently underway ahead of base offers being made in May 2018.The Trust is forecasting an over-establishment position at the end of March 2019 for Emergency Care Assistants, the Trust is currently reviewing the 2018/19 training plan to ensure total operational staff available continues to align with the required establishment numbers for frontline operaitonal delivery.
Recruitment of Clinicians for the Clinical Hub during 2017/18 was extremely successful with 28.96 WTE Clinicians joining the Trust. During Quarter 3 of 2017/18 a dedicated Clinical Hub recruitment website was created, alongside a creative advertising campaign for Clinicians across a range of online and offline media. There is a continuous NHS jobs advert running for Hub Clinicians.During 2018/19 work will continue with the Head of Clinical Hubs to develop an educational pathway for Clinicians to assist in recruitment and retention.Call Taker recruitment has been successful and is expected to maintain establishment at or above funded levels throughout 2018/19.Work is being progressed with the Head of Clinical Hubsto develop a 'model' Call Handler which will review the key attributes and experience required to be a highly performing Call Handler within the Hub environment. This work will shape the attraction and recruitment processes for Call Handlers during 2018/19.
2018/19 Forecast WTE Based on Operational Assumptions
420
440
460
480
500
520
540
560
580
600
620
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
North Division - Lead Clinician Establishment
Lead Clinician - Actual 'On the Road' WTE Lead Clinician - Funded WTE
180
200
220
240
260
280
300
320
340
360
380
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
North Division - Emergency Care Assistant Establishment
Emergency Care Assistant - Actual 'On the Road' WTE Emergency Care Assistant - Funded WTE
144
146
148
150
152
154
156
158
160
162
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Clinical Hub - Call Takers Establishment
Call Takers - Actual 'in The Room' WTE Call takers - Funded WTE
69
70
71
72
73
74
75
76
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Clinical Hub - Clinician Establishment
Clinician - Actual 'In The Room' WTE Clinician - Funded WTE
Integrated Corporate Performance Report 33

Staff Metrics - SicknessTrust Total Sickness Abstraction % Support Services Sickness Abstraction %
Integrated Corporate Performance Report
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust Total Long Term Sickness % 2.75%
Trust Total Short Term Sickness % 1.89%
Trust Total Sickness % 4.64%
Trust Total Sickness KPI 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Support Services Long Term Sickness % 1.52%
Support Services Short Term Sickness % 1.17%
Support Services Total Sickness % 2.69%
Support Services Sickness KPI 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
A&E Operational Sickness Abstraction % A&E Clinical Hub Sickness Abstraction %
A&E Operations Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations Long Term Sickness % 2.92%
A&E Operations Short Term Sickness % 1.76%
A&E Operations Total Sickness % 4.68%
A&E Sickness KPI 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
A&E Clinical Hub Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Clinical Hub Long Term Sickness % 2.56%
A&E Clinical Hub Short Term Sickness % 3.00%
A&E Clinical Hub Total Sickness % 5.56%
A&E Sickness KPI 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
2.92%
1.76%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations Sickness %
A&E Operations Long Term Sickness % A&E Operations Short Term Sickness % A&E Sickness KPI
2.56%
3.00%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Clinical Hub Sickness %
A&E Clinical Hub Long Term Sickness % A&E Clinical Hub Short Term Sickness % A&E Sickness KPI
1.52%
1.17%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Support ServicesSickness %
Support Services Long Term Sickness % Support Services Short Term Sickness % Support Services Sickness KPI
2.75%
1.89%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust Total Sickness %
Trust Total Long Term Sickness % Trust Total Short Term Sickness % Trust Total Sickness KPI
Integrated Corporate Performance Report 34

UCS Out of Hours Sickness Abstraction % NHS 111 Sickness Abstraction %
UCS Out of Hours Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours Long Term Sickness % 4.03%
UCS Out of Hours Short Term Sickness % 2.66%
UCS Out of Hours Total Sickness % 6.69%
UCS Out of Hours Sickness KPI 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
NHS 111 Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 Service Long Term Sickness % 5.11%
NHS 111 Service Short Term Sickness % 4.34%
NHS 111 Service Total Sickness % 9.45%
NHS 111 Service Sickness KPI 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
4.03%
2.66%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours Sickness %
UCS Out of Hours Long Term Sickness % UCS Out of Hours Short Term Sickness % UCS Out of Hours Sickness KPI
5.11%
4.34%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 Sickness %
NHS 111 Service Long Term Sickness % NHS 111 Service Short Term Sickness % NHS 111 Service Sickness KPI
Integrated Corporate Performance Report 35

Staff Metrics - Staff Appraisal Completion %
Integrated Corporate Performance Report
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust Total % Appraisals Completed 92.43%
Support Services % Appraisals Completed 92.75%
Appraisals Completion KPI 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations % Appraisals Completed 92.12%
A&E Clinical Hub % Appraisals Completed 93.21%
Appraisals Completion KPI 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
92.12%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Operations - Appraisals Completed %
A&E Operations % Appraisals Completed Appraisals Completion KPI
93.21%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
A&E Clinical Hub - Appraisals Completed %
A&E Clinical Hub % Appraisals Completed Appraisals Completion KPI
92.75%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Support Services Appraisals Completed %
Support Services % Appraisals Completed Appraisals Completion KPI
92.43%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Trust Total Appraisals Completed %
Trust Total % Appraisals Completed Appraisals Completion KPI
Integrated Corporate Performance Report 36

Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours % Appraisals Completed 95.35%
NHS 111 Service % Appraisals Completed 91.74%
Appraisals Completion KPI 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
95.35%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
UCS Out of Hours - Appraisals Completed %
UCS Out of Hours % Appraisals Completed Appraisals Completion KPI
91.74%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
NHS 111 - Appraisals Completed %
NHS 111 Service % Appraisals Completed Appraisals Completion KPI
Integrated Corporate Performance Report 37

A&E Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
81448
299
149
660274
120
Integrated Corporate Performance Report
20%36
13015
n/a75%33%
Serious Incidents Investigated and Presented to Panel
Adverse Incidents reported relating to medication administration, prescription and supply errors
Number of Adverse Incidents Reported
Of the Adverse Incidents Reported:
Number of Adverse Incidents Reported Relating to the Trust
Number of Adverse Incidents Reported Relating to external services
Number of Adverse Incidents Closed
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Central Alert System (CAS) received
Central Alert System Warnings (outside deadline)
Percentage of Serious Incident investigations completed within 60 working days
Serious Incidents Identified in Month
Serious Incidents Currently Under Investigation
Never Events' Identified in Month (included in Serious Incidents figure above)
Number of Moderate Incidents confirmed in Month
Number of Moderate Incidents Under Investigation
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this is possible) in accordance with the Duty of Candour
Percentage of Serious and Moderate Incidents where feedback has been completed within deadline, in accordance with Duty of Candour
448
81 0
50
100
150
200
250
300
350
400
450
500
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Reported
Number of Adverse Incidents Reported Adverse Incidents reported relating to medication administration, prescription and supply errors
274
0
50
100
150
200
250
300
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Outstanding
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
12
0 0
2
4
6
8
10
12
14
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Central Alert System (CAS)
Central Alert System (CAS) received Central Alert System Warnings (outside deadline)
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Serious Incidents Completed Within 60 Working Days
Percentage of Serious Incident investigations completed within 60 working days
3
0
1
1
2
2
3
3
4
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Identified in Month
Serious Incidents Identified in Month
13
0
2
4
6
8
10
12
14
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Currently Under Investigation
Serious Incidents Currently Under Investigation
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Confirmed in Month
Number of Moderate Incidents confirmed in Month
5
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Under Investigation
Number of Moderate Incidents Under Investigation
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Moderate Incidents Where Contact is Made in Accordance with Duty of Candour
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this ispossible) in accordance with the Duty of Candour
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Closed Moderate Incidents Investigated Within 35 Working Days
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
Integrated Corporate Performance Report 38

A&E Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
088
1244
5312787127
Data Not Yet Available
98
91
44
Safeguarding Referrals - it is a statutory duty for all organisations that work with children or vulnerable adults to share information, in a timely manner when abuse or neglect is identified or suspected.Any staff member who has a concern about a vulnerable child or adult will complete a safeguarding referral that is submitted to the SWASFT safeguarding hub. This referral is then triaged and sent out to the relevant agency according to need i.e adult or child social services, GP, Fire, Police, CQC, Named Nurse etc.
1,107
Number of Complaints Open (not resolved with the complainant and currently under investigation)
Number of Ombudsman referrals upheld
Number of Complaints Reported
Number of Complaints Closed (resolved with the Complainant and all investigations completed)
Number of Complaints Resolved (with the Complainant but internal investigation ongoing)
Number of Security Incidents Closed (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Safeguarding Referrals
The above figures can change on a daily basis as Complaints, Adverse Incidents and Serious Incidents are often recoded depending on the level of harm caused. Adverse Incidents, Moderate Incidents and Complaints can be deemed a Serious Incident and then downgraded to their original status, some complaints and plaudits get logged after the report is generated depending on where they are receive in the Trust.
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
Total PALS Reported
Total PALS Closed
Total PALS Currently ongoing
Compliments Received
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
88
0
10
20
30
40
50
60
70
80
90
100
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Reported
Number of Complaints Reported
53
0
10
20
30
40
50
60
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Outstanding
Number of Complaints Open (not resolved with the complainant and currently under investigation)
12
0
2
4
6
8
10
12
14
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Where The Complainant is Awaiting Feedback
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
98
0
20
40
60
80
100
120
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Reported
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
44
0
5
10
15
20
25
30
35
40
45
50
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Under Investigation
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
1,107
0
200
400
600
800
1,000
1,200
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Safeguarding Referrals
Number of Safeguarding Referrals
78
0
10
20
30
40
50
60
70
80
90
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Reported
Total PALS Reported
27
0
5
10
15
20
25
30
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Outstanding
Total PALS Currently ongoing
0 0
0
0
0
0
1
1
1
1
1
1
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Compliments Received
Compliments Received
Integrated Corporate Performance Report 39

Out of Hours Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
59
8
1
241
n/a101000
n/an/an/a
Serious Incidents Investigated and Presented to Panel
Serious Incidents Currently Under Investigation
Never Events' Identified in Month (included in Serious Incidents figure above)
Number of Moderate Incidents confirmed in Month
Number of Moderate Incidents Under Investigation
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this is possible) in accordance with the Duty of Candour
Percentage of Serious and Moderate Incidents where feedback has been completed within deadline, in accordance with Duty of Candour
Number of Adverse Incidents Closed
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Percentage of Serious Incident investigations completed within 60 working days
Adverse Incidents reported relating to medication administration, prescription and supply errors
Number of Adverse Incidents Reported
Of the Adverse Incidents Reported:
Number of Adverse Incidents Reported Relating to the Trust
Number of Adverse Incidents Reported Relating to external services
Serious Incidents Identified in Month
9
5
0
1
2
3
4
5
6
7
8
9
10
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Reported
Number of Adverse Incidents Reported Adverse Incidents reported relating to medication administration, prescription and supply errors
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Serious Incidents Completed Within 60 Working Days
Percentage of Serious Incident investigations completed within 60 working days
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Identified in Month
Serious Incidents Identified in Month
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Currently Under Investigation
Serious Incidents Currently Under Investigation
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Confirmed in Month
Number of Moderate Incidents confirmed in Month
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Under Investigation
Number of Moderate Incidents Under Investigation
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Moderate Incidents Where Contact is Made in Accordance with Duty of Candour
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this ispossible) in accordance with the Duty of Candour
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Closed Moderate Incidents Investigated Within 35 Working Days
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
41
0
5
10
15
20
25
30
35
40
45
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Outstanding
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Integrated Corporate Performance Report 40

Out of Hours Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
004012100
Data Not Yet Available
1
0
2
Safeguarding Referrals - it is a statutory duty for all organisations that work with children or vulnerable adults to share information, in a timely manner when abuse or neglect is identified or suspected.Any staff member who has a concern about a vulnerable child or adult will complete a safeguarding referral that is submitted to the SWASFT safeguarding hub. This referral is then triaged and sent out to the relevant agency according to need i.e adult or child social services, GP, Fire, Police, CQC, Named Nurse etc.
5
Number of Complaints Reported
Number of Complaints Closed (resolved with the Complainant and all investigations completed)
Number of Complaints Resolved (with the Complainant but internal investigation ongoing)
Number of Complaints Open (not resolved with the complainant and currently under investigation)
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
Number of Security Incidents Closed (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Safeguarding Referrals
The above figures can change on a daily basis as Complaints, Adverse Incidents and Serious Incidents are often recoded depending on the level of harm caused. Adverse Incidents, Moderate Incidents and Complaints can be deemed a Serious Incident and then downgraded to their original status, some complaints and plaudits get logged after the report is generated depending on where they are receive in the Trust.
Total PALS Reported
Total PALS Closed
Total PALS Currently ongoing
Compliments Received
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Ombudsman referrals upheld
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Reported
Number of Complaints Reported
1
0
0
0
1
1
1
1
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Outstanding
Number of Complaints Open (not resolved with the complainant and currently under investigation)
2
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Where The Complainant is Awaiting Feedback
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Reported
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
2
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Under Investigation
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
5
0
1
2
3
4
5
6
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Safeguarding Referrals
Number of Safeguarding Referrals
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Reported
Total PALS Reported
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Outstanding
Total PALS Currently ongoing
0 0
1
2
3
4
5
6
7
8
9
10
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Compliments Received
Compliments Received
Integrated Corporate Performance Report 41

NHS 111 Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
013
7
6
1715
n/a000000
n/an/an/aPercentage of Serious and Moderate Incidents where feedback has been completed within deadline, in accordance with Duty of Candour
Percentage of Serious Incident investigations completed within 60 working days
Adverse Incidents reported relating to medication administration, prescription and supply errors
Number of Adverse Incidents Reported
Of the Adverse Incidents Reported:
Number of Adverse Incidents Reported Relating to the Trust
Number of Adverse Incidents Reported Relating to external services
Number of Adverse Incidents Closed
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Serious Incidents Identified in Month
Serious Incidents Investigated and Presented to Panel
Serious Incidents Currently Under Investigation
Never Events' Identified in Month (included in Serious Incidents figure above)
Number of Moderate Incidents confirmed in Month
Number of Moderate Incidents Under Investigation
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this is possible) in accordance with the Duty of Candour
13
0 0
2
4
6
8
10
12
14
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Reported
Number of Adverse Incidents Reported Adverse Incidents reported relating to medication administration, prescription and supply errors
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Serious Incidents Completed Within 60 Working Days
Percentage of Serious Incident investigations completed within 60 working days
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Identified in Month
Serious Incidents Identified in Month
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Currently Under Investigation
Serious Incidents Currently Under Investigation
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Confirmed in Month
Number of Moderate Incidents confirmed in Month
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Under Investigation
Number of Moderate Incidents Under Investigation
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Moderate Incidents Where Contact is Made in Accordance with Duty of Candour
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this ispossible) in accordance with the Duty of Candour
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Closed Moderate Incidents Investigated Within 35 Working Days
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
15
0
2
4
6
8
10
12
14
16
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Outstanding
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Integrated Corporate Performance Report 42

NHS 111 Service Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
021010000
Data Not Yet Available
1
0
2
Safeguarding Referrals - it is a statutory duty for all organisations that work with children or vulnerable adults to share information, in a timely manner when abuse or neglect is identified or suspected.Any staff member who has a concern about a vulnerable child or adult will complete a safeguarding referral that is submitted to the SWASFT safeguarding hub. This referral is then triaged and sent out to the relevant agency according to need i.e adult or child social services, GP, Fire, Police, CQC, Named Nurse etc.
133
Number of Ombudsman referrals upheld
Number of Complaints Reported
The above figures can change on a daily basis as Complaints, Adverse Incidents and Serious Incidents are often recoded depending on the level of harm caused. Adverse Incidents, Moderate Incidents and Complaints can be deemed a Serious Incident and then downgraded to their original status, some complaints and plaudits get logged after the report is generated depending on where they are receive in the Trust.
Number of Complaints Resolved (with the Complainant but internal investigation ongoing)
Number of Complaints Open (not resolved with the complainant and currently under investigation)
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
Total PALS Reported
Total PALS Closed
Total PALS Currently ongoing
Compliments Received
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Security Incidents Closed (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Safeguarding Referrals
Number of Complaints Closed (resolved with the Complainant and all investigations completed)
2
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Reported
Number of Complaints Reported
1
0
0
0
1
1
1
1
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Outstanding
Number of Complaints Open (not resolved with the complainant and currently under investigation)
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Where The Complainant is Awaiting Feedback
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Reported
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
2
0
1
2
3
4
5
6
7
8
9
10
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Under Investigation
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
133
0
20
40
60
80
100
120
140
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Safeguarding Referrals
Number of Safeguarding Referrals
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Reported
Total PALS Reported
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Outstanding
Total PALS Currently ongoing
0 0
1
2
3
4
5
6
7
8
9
10
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Compliments Received
Compliments Received
Integrated Corporate Performance Report 43

Tiverton Urgent Care Centre Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
00
0
0
00
n/a000000
n/an/an/a
Number of Moderate Incidents confirmed in Month
Number of Moderate Incidents Under Investigation
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this is possible) in accordance with the Duty of Candour
Percentage of Serious and Moderate Incidents where feedback has been completed within deadline, in accordance with Duty of Candour
Never Events' Identified in Month (included in Serious Incidents figure above)
Serious Incidents Investigated and Presented to Panel
Serious Incidents Currently Under Investigation
Adverse Incidents reported relating to medication administration, prescription and supply errors
Number of Adverse Incidents Reported
Number of Adverse Incidents Reported Relating to the Trust
Number of Adverse Incidents Reported Relating to external services
Number of Adverse Incidents Closed
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Percentage of Serious Incident investigations completed within 60 working days
Serious Incidents Identified in Month
0 0 0
1
2
3
4
5
6
7
8
9
10
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Reported
Number of Adverse Incidents Reported Adverse Incidents reported relating to medication administration, prescription and supply errors
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Serious Incidents Completed Within 60 Working Days
Percentage of Serious Incident investigations completed within 60 working days
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Identified in Month
Serious Incidents Identified in Month
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Serious Incidents Currently Under Investigation
Serious Incidents Currently Under Investigation
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Confirmed in Month
Number of Moderate Incidents confirmed in Month
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Moderate Incidents Under Investigation
Number of Moderate Incidents Under Investigation
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Moderate Incidents Where Contact is Made in Accordance with Duty of Candour
Percentage of Moderate Incidents where contact has been made with the patient or relative (where this ispossible) in accordance with the Duty of Candour
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
% of Closed Moderate Incidents Investigated Within 35 Working Days
Percentage of Moderate Incidents closed in the month which were investigated within 35 working days
0 0
0
0
0
0
1
1
1
1
1
1
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Adverse Incidents Outstanding
Number of Adverse Incidents Currently Under Investigation (as of last day of month)
Integrated Corporate Performance Report 44

Tiverton Urgent Care Centre Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
010000000
Data Not Yet Available
0
0
0
Safeguarding Referrals - it is a statutory duty for all organisations that work with children or vulnerable adults to share information, in a timely manner when abuse or neglect is identified or suspected.Any staff member who has a concern about a vulnerable child or adult will complete a safeguarding referral that is submitted to the SWASFT safeguarding hub. This referral is then triaged and sent out to the relevant agency according to need i.e adult or child social services, GP, Fire, Police, CQC, Named Nurse etc.
5Number of Safeguarding Referrals
The above figures can change on a daily basis as Complaints, Adverse Incidents and Serious Incidents are often recoded depending on the level of harm caused. Adverse Incidents, Moderate Incidents and Complaints can be deemed a Serious Incident and then downgraded to their original status, some complaints and plaudits get logged after the report is generated depending on where they are receive in the Trust.
Total PALS Closed
Total PALS Currently ongoing
Compliments Received
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Security Incidents Closed (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
Number of Complaints Reported
Number of Complaints Closed (resolved with the Complainant and all investigations completed)
Number of Complaints Resolved (with the Complainant but internal investigation ongoing)
Number of Complaints Open (not resolved with the complainant and currently under investigation)
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
Total PALS Reported
Number of Ombudsman referrals upheld
1
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Reported
Number of Complaints Reported
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Outstanding
Number of Complaints Open (not resolved with the complainant and currently under investigation)
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Complaints Where The Complainant is Awaiting Feedback
Number of Complaints where an investigation has been returned but the complainant is still awaiting feedback.
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Reported
Number of Security Incidents Reported (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Security Incidents Under Investigation
Number of Security Incidents Currently Under Investigation (SIRS)(A&E Activity, Control, Operations, Fleet, Admin, Education & Training and Patient Safety Incidents)
5
0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Safeguarding Referrals
Number of Safeguarding Referrals
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Reported
Total PALS Reported
0 0
1
2
3
4
5
6
7
8
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of PALS Outstanding
Total PALS Currently ongoing
0 0
1
2
3
4
5
6
7
8
9
10
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Compliments Received
Compliments Received
Integrated Corporate Performance Report 45

South Western Ambulance Service NHS Foundation Trust Financial Performance - Summary Dashboard
Better Payment Practice Code KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Q1 Q2 Q3 Q4 On Target Of Concern
Action Required
Better Payment Practice Code NHS (Value) % 95% 99.87% 99.87% 99.87% >95% <95%
Better Payment Practice Code NHS (Volume) % 95% 94.87% 94.87% 94.87% >95% <95%
Better Payment Practice Code Non NHS (Value) % 95% 98.57% 98.57% 98.57% >95% <95%
Better Payment Practice Code Non NHS (Volume) % 95% 98.72% 98.72% 98.72% >95% <95%
Other Key Financial Metrics KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Q1 Q2 Q3 Q4 On Target Of Concern
Action Required
Debtors >90 Days Past Due as a % of Total Debtor Balances 5.00% 5.29% 5.29% 5.29% <5% >5%
Creditors >90 Days Past Due as a % of Total Creditor Balances
5.00% 0.14% 0.14% 0.14% <5% >5%
Capital Expenditure as a % of Plan (Min)(YTD position reported each month)
85.00% 384% 384% 384% >85% <85%
Cost Improvement Programme (CIP) as a % of Plan(YTD position reported each month)
85.00% 100% 100% 100% >85% <85%
Single Oversight Framework - Use of Resources KPI YTD Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Q1 Q2 Q3 Q4
Capital Service Cover 5.95 5.95 5.95
Capital Service Cover Metric Score 1.00 1.00 1.00
Liquidity 10.58 10.58 10.58
Liquidity Metric Socre 1.00 1.00 1.00
I&E Margin (%) 0.00% 0.00% 0.00%
I&E Metric Score 2.00 2.00 2.00
Variance in I&E Margin as % of Plan 0.00% 0.00% 0.00%
Variance in I&E Margin Metric Score 1.00 1.00 1.00
Agency Spend Variance to Cap (YTD) -88.50% -88.50% -88.50%
Agency Metric Score 1.00 1.00 1.00
Use of Resources Metric 2.00 2.00 2.00
The Capital Plan for 2018/19 is £14,428k. The month one position shows an actual position of £384k compared to a plan of £100k (384%). This is due to timing of vehicle conversions ahead of plan.Comments:
Integrated Corporate Performance Report 46

South Western Ambulance Service NHS Foundation Trust Financial Performance - Statement of Comprehensive Income
Statement of Comprehensive Income Actual Budget Variance Actual Budget VariancePeriod Ending 30/04/2018Month 1
£'000 £'000 £'000 £'000 £'000 £'000Income:
A&E Income (16,409) (16,377) (32) (196,902) (196,522) (380)UCS Income (1,067) (980) (87) (12,766) (11,761) (1,005) 3
PTS Income (2) (2) - (25) (25) - HART Income (555) (555) - (6,661) (6,659) (2)Other Income (1,255) (1,039) (215) (15,699) (12,500) (3,199) 3
Total Income (19,287) (18,953) (334) (232,053) (227,467) (4,585)Expenditure:
Employee Benefits (Pay) 14,308 14,414 (106) 1,2 172,257 172,975 (718) 1,2
Drugs 42 43 (2) 708 522 187 Medical 442 372 70 4,979 4,460 520 ICT 598 542 56 6,998 6,505 494 Estates 742 581 161 7,160 6,980 180 Fleet Expenses 376 351 25 4,582 4,215 368 Fuel 502 550 (48) 5,976 6,605 (629)Vehicle Insurance 171 187 (16) 2,086 2,244 (158)Vehicle Leasing 73 56 17 873 673 200 Education & Training 15 65 (50) 870 783 87 Other 852 567 285 1 10,938 6,807 4,131 1
Total Operating Expenses 18,120 17,728 391 217,429 212,768 4,661 3
EBITDA (1,167) (1,225) 57 (14,624) (14,699) 75 EBITDA % 6.05% 6.46% 6.30% 6.46%
Profit/Loss on Asset Disposal (8) - (8) (8) - (8)Depreciation 986 1,019 (33) 12,205 12,226 (21)Impairments
Total Operating (Surplus)/Deficit (189) (206) 17 (2,427) (2,473) 46
Total Interest Receivable (10) (8) (2) (113) (96) (17)Total Interest Payable 11 9 2 102 110 (8)PDC Dividend 188 205 (17) 2,438 2,460 (22)Net (Surplus)/Deficit - - - - - -
Comments:1 Use of third parties offset vacancies in A&E; 2 Use of overtime and bank to offset vacancies3 Other income above plan offset by additional expenduiture
Year to Date Forecast
Integrated Corporate Performance Report 47

South Western Ambulance Service NHS Foundation Trust Financial Performance - Statement of Financial Position
31-Mar-18Statement of Financial Position Actual Actual Budget Variance Actual Budget Variance
Period Ending 30/04/2018Month 1
£'000 £'000 £'000 £'000 £'000 £'000 £'000Non-Current Assets
Property, Plant & Equipment & Intangible Assets, Net 89,663 89,062 88,756 306 1 92,587 92,565 22 Trade & Other Receivables Non-Current 162 155 159 (4) 78 - 78
Total Non-Current Assets 89,825 89,217 88,915 302 92,665 92,565 100 Current Assets
Inventories 2,030 2,056 2,050 6 2,000 2,000 - NHS Trade Receivables, Current 1,510 3,227 1,400 1,827 2 1,900 1,900 - Non NHS Trade Receivables, Current 1,059 1,079 800 279 2 550 550 - Other Receivables, Current 878 956 997 (41) 1,171 1,188 (17)Prepayments, Current, Non-PFI related 2,906 3,277 3,476 (199) 3 2,747 2,747 - Other Financial Assets, Current 725 1,213 725 488 4 129 129 - Cash and Cash Equivalents 23,364 19,147 22,524 (3,377) 5 17,551 17,616 (65)
Current Assets 32,472 30,955 31,972 (1,017) 26,048 26,130 (82)Non Current Assets Held for Sale - - - - - Total Current Assets 32,472 30,955 31,972 (1,017) 26,048 26,130 (82)TOTAL ASSETS 122,297 120,172 120,887 (715) 118,713 118,695 18
Current Liabilities - - Deferred Income (484) (508) (886) 378 (747) (747) - NHS Trade Payables (655) (443) (250) (193) 6 (225) (225) - Non-NHS Trade Payables (3,857) (2,492) (3,500) 1,008 6 (2,225) (2,225) - Capital Accruals (1,695) (1,472) (100) (1,372) 7 (1,212) (1,221) 9 Other Liabilities (6,090) (6,226) (6,000) (226) (6,090) (6,090) - Borrowings (439) (439) (439) - (439) (439) - Other Financial Liabilities (8,315) (7,910) (9,018) 1,108 8 (9,273) (9,273) - PDC Dividend Payable, Current - (182) (201) 19 - - - Provisions for Liabilities and Charges (3,056) (3,044) (3,037) (7) (649) (642) (7)
Total Current Liabilities (24,591) (22,716) (23,431) 715 (20,860) (20,862) 2 Net Current Assets/(Liabilities) 7,881 8,239 8,541 (302) 5,188 5,268 (80)
TOTAL ASSETS LESS CURRENT LIABILITIES 97,706 97,456 97,456 - 97,853 97,833 20 Non-Current Liabilities
Finance Leases, Non-Current (617) (617) (617) - (617) (617) - Long Term Borrowings (862) (862) (862) - (434) (434) - Other Financial Liabilities, Non-Current - - - - - - - Provisions, Non-Current (4,039) (3,788) (3,790) 2 (3,913) (3,895) (18)Trade and Other Payables, Non-Current - - - - - - -
Total Non-Current Liabilities (5,518) (5,267) (5,269) 2 (4,964) (4,946) (18)TOTAL ASSETS EMPLOYED 92,188 92,189 92,187 2 92,889 92,887 2
Represented ByPublic Dividend Capital (43,025) (43,025) (43,025) - 43,025 43,025 - Income & Expenditure Account (37,183) (37,225) (37,218) (7) 9 37,608 37,601 7 Revaluation Reserve (11,980) (11,939) (11,944) 5 10 12,256 12,261 (5)
TOTAL TAXPAYERS EQUITY (92,188) (92,189) (92,187) (2) 92,889 92,887 2
Comments:1 Property, Plant and Equipment - 2017/18 Capital ahead of plan £284k, depreciation £21k behind plan, sale of vehicles (£0k) = (£305k)2 Trade Receivables - ahead of plan due to Gloucester CCG A&E contract not paid for April (paid May), outstanding Air Ambulance invoices and salary overpayments invoices.3 Prepayments - behind plan due to insurance below budget.4 Other Financial Assets - Salary recharge, Band 6 funding and Salisbury incident.5 Cash - Receivables, Other Assets, Capital & Other liabilities ahead of plan £1,239k, Prepayments, Trade Payables, Financial liabilities and Deferred income more than plan £2,102k = £3,341k6 Trade Payables - less than plan, more creditors paid than planned for year end.7 Capital & capital accruals new vehicles bought earlier than plan to arrive by June 2018.8 Other Financial Liabilities - Less accruals than plan for 3rd party transport, overtime, agancy, utilities and estates.9 Income & Expenditure:- £6k more excess depreciation than plan due to £2,000k revaluation of assets March 2018
10 Revaluation Reserve:- £6k more excess depreciation than plan due to £2,000k revaluation of assets March 2018
Year to Date Forecast
Integrated Corporate Performance Report 48

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 3
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Standing Financial Instructions
Prepared by: Marty McAuley, Trust Secretary
Presented by: Marty McAuley, Trust Secretary
Action: Approval
Recommendation:
The Board of Directors is asked to approve the: Introduction of Government Procurement Cards Delegation to the Deputy Chief Executive/Executive Director of
Finance to approve individual card holders Proposed amendments to the SFIs
Executive Summary:
The Trust would like to introduce Government Procurement Cards to be used by some Senior Managers in the command structure during serious or major incidents. The paper requests that the Board approve the introduction of Government Procurement Cards and delegates authority to the Deputy Chief Executive/Executive Director of Finance to approve individual card holders. The Trust SFIs would need to be amended to approve this and the two proposed amendments are included for approval.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 3
Standing Financial Instructions 1. Standing Financial Instructions 1.1 The Standing Financial Instructions (SFIs) of the Trust detail the financial responsibilities,
policies and procedures to be adopted by the Trust. 1.2 They are designed to ensure that the Trust’s financial transactions are carried out in
accordance with the law, the Regulatory Framework and the guidance and best practice advice issued by the Independent Regulator in order to achieve probity, accuracy, economy, efficiency and effectiveness in all financial matters concerning the Trust.
2. Government Procurement Cards 2.1 The Trust has identified that it would be useful for some Senior Managers within the
command structure to be issued with Government Procurement Cards, that allow them to make purchases on behalf of the Trust, during a serious or major incident.
2.2 These cards will only be used when a serious or major incident has been declared and
there are set criteria as to what they can be used for and when. The Finance Team will have a number of checks and audit each card for appropriate use.
2.3 The Executive Directors group has identified a group of Senior Managers in the command
structure who would benefit from these cards. 2.4 The Trust’s governance arrangements need to be robust but not restrictive and the
proposal would mean that we would not have to return for Board approval each time a new card were to be issued.
2.5 The SFIs will need to be amended to give authority for these cards to be issued. 2.6 The Board is asked to approve the introduction of the Government Procurement Cards
and delegate authority to the Deputy Chief Executive /Executive Director of Finance to approve each individual named cardholder on an individual basis.
3. Proposed amendment to the Standing Financial Instructions 3.1 There are two sections that will be amended to reflect the changes and these are
proposed below:
(1) Section 3.3 Responsibilities of the Deputy Chief Executive /Executive Director of Finance
It is the responsibility of the Deputy Chief Executive /Executive Director of Finance to approve each Government Procurement Card that the Trust issues and ensure Managers receive the appropriate guidance on its use

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 3
(2) Section 12.2.6 - Government Procurement Cards
12.2.6.1 Government Procurement Cards will be made available to a list of Senior Managers in the command structure for the purpose of ad-hoc purchases and payment during major or serious incident.
12.2.6.2 Managers issued with cards must ensure that they comply fully with any guidance issued by the Deputy Chief Executive/Executive Director of Finance regarding the card.
4. Recommendation 4.1 The Board of Directors is asked to approve the:
Introduction of Government Procurement Cards Delegation to the Deputy Chief Executive/Executive Director of Finance to approve
individual card holders Proposed amendments to the SFIs
Marty McAuley Trust Secretary

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 10
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: NHS Improvement Self-Certifications
Prepared by: Marty McAuley, Trust Secretary
Presented by: Jenny Winslade, Executive Director of Nursing and Quality
Action: Approval
Recommendation:
The Trust Board of Directors is asked to approve: The self-certification declarations required The Corporate Governance Statement
Executive Summary:
This paper seeks approval for the self-certifications of the Board against three license conditions. The Board is recommended to confirm its compliance with all three statements. These conditions are: Condition G63 – providers must certify that the Board has taken all precautions necessary to comply with the license, NHS Acts and NHS constitution. Condition C0S7(3) – Providers providing commissioner requested service (CRS) must certify that they have a reasonable expectation that the required resources will be available to deliver the designated service. Condition FT4(8) - Providers must certify compliance with required governance standards and objectives. For this condition, the Trust must also seek Board approval for its corporate governance statement which must be produced at the end of each financial year showing compliance with this license condition (see Annex A). In a change of process this year, the self-certifications do not need to be submitted to NHS Improvement but there are set timescales for approval and a requirement to publish some of the self-certifications.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 10
NHS Improvement Self-certifications 1.1 NHS Foundation Trusts are required to self-certify whether or not they have complied with
the conditions of the NHS provider licence (which itself includes requirements to comply with the National Health Service Act 2006, the Health and Social Care Act 2008, the Health Act 2009, and the Health and Social Care Act 2012, and have regard to the NHS Constitution), have the required resources available if providing commissioner requested services, and have complied with governance requirements.
1.2 In a change to the arrangements this year, the Trust will not be required to submit the
declarations to NHS Improvement. 1.3 Despite this change the self-certification must be signed off by the Board of Directors.
Each statement is approved through a confirmed/not confirmed marking system. 1.4 The G6/CoS7 declarations are required to be made by the 31 May 2018, whilst the FT4 is
required by 30 June 2018. 1.5 The Trust will be required to publish its G6 self-certification declaration and the Trust must
make a corporate governance statement from its compliance against FT4. This is Annex A of the report.
1.6 The Trust needs to self-certify the following three conditions from the NHS Provider
license. Having reviewed the guidance the Trust is recommended to declare confirmed for all three declarations. This is appropriate for the 2017/18 year and consistent with our position in previous years.
No Condition Declaration Recommended status
1 G6 The provider has taken all precautions necessary to comply with the licence, NHS Acts and NHS Constitution
Confirmed
2 FT4 The provider has complied with required governance arrangements Confirmed
3 CoS7
If providing commissioner requested services, the provider has a reasonable expectation that required resources will be available to deliver the designated service
Confirmed

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 10
2. Self Certification 1: Condition G6: Systems for Compliance with License Conditions
Self-Certificate Declaration Recommendation – Confirmed 2.1 Condition G6(2) requires NHS Foundation Trusts to have processes and systems that (a)
identify risks to compliance and (b) take reasonable mitigating actions to prevent those risks and a failure to comply from occurring. Providers must annually review whether these processes and systems are effective.
2.2 The Trust Board of Directors is committed to ensuring that effective risk management is an
integral part of its management approach, underpinning all activities. At each Board meeting, the Risk Register and Board Assurance Framework is received which details the key corporate risks which could lead to the Trust not achieving its corporate objectives or compliance.
2.3 The Audit and Assurance Committee develop an Internal Audit Plan designed to test the
robustness of the controls we have in place. As part of the process to identify risk, regular risk assessments were undertaken throughout the year and reported to the Audit and Assurance Committee as well as the Quality Committee as appropriate.
2.4 The Trust has previously had a Regulatory Consolidated Action Plan (RCAP). This set out
the actions required in order for the Trust to address compliance and regulatory issues but as these have all been completed and closed, it has evolved to become an annual Quality Improvement Plan.
2.5 In March 2016, the Trust was placed under investigation with NHSI. In May 2017 the NHSI
investigation was also closed with no formal action taken. The nine informal actions were completed and closed in 2017/18.
2.6 The Trust achieved and maintained a single oversight framework (SOF) score of 2 since
the introduction of the SOF. 2.7 In 2017/18 the Trust commissioned KPMG to deliver its Well Led Governance Review.
The conclusion of KPMG was that the Trust has a large number of effective processes and controls in place to support compliance with the governance framework but noted some areas of improvement that the Trust has been working to deliver.
2.8 Through regular NHSI and CQC relationship meetings, the Trust is able to have open and
honest dialogue about key issues that affect the Trust and seek appropriate support and guidance. This has ensured that there has been no breaches of the license conditions and allows any risks to be effectively managed.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 4 of 10
3. Self-certification 2: Condition CoS7 - commissioner requested services (CRS) Self-Certificate Declaration Recommendation – Confirmed 3.1 Commissioners had a time limited window in which to designate services as CRS. This
had to be formally agreed with the Trust and NHSI and reflected in contracts by 1 April 2016.
3.2 Whilst the Trust took part in discussions with Commissioners, the formal position remains
that none of our services are designated as CRS. However, the Trust considers all of our services (999, OOH and 111) to be a CRS due to the principles of CRS (to ensure continuity of services) and we are self-certifying in this spirit.
3.3 The Trust has an Operating Plan in place, approved by the Trust Board of Directors. 3.4 A 2 year signed contract is in place for A&E services and there are also signed contracts in
place for the Urgent Care Services delivered. Regular contract meetings addressing both performance and quality are in place with Commissioners.
4. Self-Certification 3: Condition FT4 – Governance Arrangements 4.1 The Trust Board oversees a robust culture of appropriate governance, scrutiny and
challenge and this is reflected in the self-certifications statements below. The Board is effective with good engagement from the Executive and Non-Executive Members and demonstrable evidence of action as a unitary board.
4.2 The Board has an effective committee management structure that has been further
strengthened by the Chair with the introduction of a new People and Culture Committee. 4.3 Board Assurance and Risk Management remains a constant feature at each Board
meeting, with an ICPR that provides a strong assurance base for Trust performance. 4.4 The Trust also undertook its Well Led Governance Review with a robust conclusion from
KPMG to support the Trust’s governance arrangements.
Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 5 of 10
4.5 Statement 1: The Board is satisfied that the Trust applies those principles, systems and standards of good governance which reasonably would be regarded as appropriate for a supplier of health care services to the NHS.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
confirmed No risk or further action required
Key Sources of Assurance: The Trust has undertaken a Well Led Governance Review led by KPMG NHSI investigation closed with no governance concerns found NHSI informal actions have been delivered and closed Significant level of assurance from key internal audit reports
4.6 Statement 2: The Board has regard to such guidance on corporate governance as may be
issued from time to time.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
confirmed No risk or further action required
Key Sources of Assurance: Developed a new Fit and Proper Person Policy Extension of Freedom to Speak Up guidance and Peer Support Network Duty of Candour adherence and monitoring Significant Internal Audit Assurance around corporate governance processes
4.7 Statement 3: The Board is satisfied that the Trust implements:
(a) Effective Board and committee structures; (b) Clear responsibilities for its Board, for committee reports to the Board and for staff
reporting to the Board and those committees; (c) Clear reporting lines and accountabilities throughout its organisation.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
confirmed No risk or further action required Key Sources of Assurance:
Introduction of New Ways of Working document for the Board Strategic Direction Working Group introduced Each committee reviewed for effectiveness and terms of reference reviewed Development of a new People and Culture Committee
Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 6 of 10
4.8 Statement 4. The Board is satisfied that the Trust effectively implements systems and/or processes: (a) To ensure compliance with the Licensee’s duty to operate efficiently, economically
and effectively; (b) For timely and effective scrutiny and oversight by the Board of the Licensee’s
operations; (c) To ensure compliance with healthcare standards binding on the Licensee including
but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and Statutory Regulators of Healthcare Professions;
(d) For effective financial decision making management and control (including but not restricted to appropriate systems and/or processes to ensure the Licensee’s ability to continue as a going concern);
(e) To obtain and disseminate accurate, comprehensive and timely and up to date information for Board and Committee decision-making;
(f) To identify and manage (including but not restricted to managing through forward plans) material risks to compliance with the conditions of its license;
(g) To generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery;
(h) To ensure compliance with all applicable legal requirements.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
Confirmed No risk or further action required Sources of Assurance:
Trust Annual Governance Statement is open and transparent and is accompanied by a Head of Internal Audit Opinion offering significant assurance and External Audit opinion
Integrated Corporate Performance Report (ICPR) presented at each Board meeting
Risk management processes established with Quality Risk Assurance Group (QRAG) and Audit and Assurance Committee and Board
Effective board and committee structure, with a cycles of business in place and each Committee provides assurance reports through to the Board
Trust Constitution and Code of Governance compliance monitored by Trust Secretary and Audit and Assurance Committee
4.9 Statement 5. The Board is satisfied that the systems and/or processes referred to in
paragraph 4 (above) should include but not be restricted to systems and or processes to ensure: (a) That there is sufficient capability at Board level to provide effective organisational
leadership on the quality of care provided; (b) That the Board’s planning and decision making processes take timely and
appropriate account of quality of care considerations;

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 7 of 10
(c) The collection of accurate, comprehensive and up to date information on quality of care;
(d) That the Board receives and takes into account accurate, comprehensive and up to date information on quality of care;
(e) That the Trust, including its Board, actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources;
(f) That there is clear accountability for quality of care throughout the Trust including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
confirmed No risk or further action required Sources of Assurance:
Board capacity has been increased with the appointment of an additional Executive Director appointment
Introduction of a new approach to Equality Quality Impact Assessment (EQIA) and annual quality improvement plan as part of our approach to quality
Quality Committee meets quarterly with a focus and remit for quality issues and is responsible for the monitoring of the development of the Quality Strategy
Patient Safety and Experience and Engagement report presented at the Quality Committee, Board and Council of Governor meeting. Also hear from patients directly who have used the service.
4.10 Statement 6. The Board is satisfied that there are systems to ensure that the Trust
has personnel on the Board, reporting to the Board and within the rest of the organisation who are sufficient in number and appropriately qualified to ensure compliance with its NHS provider license.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
confirmed No risk or further action required Sources of Assurance
Stability and continuity of leadership from Chief Executive and Chairman Membership of Executive Director team balanced with established and new
members, including the new post of Executive Director of Operations created New appointments of two NEDs with second terms of office for three NEDs Development of an Associate Non-Executive Director role Operational restructure of senior management and support services review People and Culture Committee established

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 8 of 10
4.11 Section 151 (2) of the Health and Social Care Act also requires us to declare that we have taken appropriate steps to equip the Governors with the skills and knowledge that they require. This is not a formal license condition but it is a requirement that we make the declaration.
Proposed declaration
Risks and mitigating action (comments will be added to the submission)
Confirmed No risk or further action required Sources of Assurance
Governwell training provided by NHS Providers, scoped by Trust Secretary and Lead Governor
Two development workshops to support Governor knowledge Trust Induction for new Governors delivered Governor sub group looking at training requirements Governors are routinely asked what training they want and it is delivered Local and national opportunities to network and share best practice
5. Corporate Governance Statement 5.1 The Trust is also required to produce a corporate governance statement by and on behalf
of its Board confirming compliance with the FT4 – NHS foundation trust governance arrangement condition. This statement is taken directly from the license condition requirements and shown in Annex A.
6. Recommendation The Board of Directors is asked to approve
The self-certifications statements The Annual Corporate Governance Statement
Marty McAuley Trust Secretary

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 9 of 10
Annex A - Corporate Governance Statement
1. The Board is satisfied that the Trust applies those principles, systems and standards of good governance which reasonably would be regarded as appropriate for a supplier of health care services to the NHS.
2. The Board has regard to such guidance on corporate governance as may be issued from
time to time.
3. The Board is satisfied that the Trust implements: (a) Effective Board and committee structures; (b) Clear responsibilities for its Board, for committee reports to the Board and for staff
reporting to the Board and those committees; (c) Clear reporting lines and accountabilities throughout its organisation.
4. The Board is satisfied that the Trust effectively implements systems and/or processes:
(a) To ensure compliance with the Licensee’s duty to operate efficiently, economically and effectively;
(b) For timely and effective scrutiny and oversight by the Board of the Licensee’s operations;
(c) To ensure compliance with healthcare standards binding on the Licensee including but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and statutory regulators of healthcare professions;
(d) For effective financial decision making management and control (including but not restricted to appropriate systems and/or processes to ensure the Licensee’s ability to continue as a going concern);
(e) To obtain and disseminate accurate, comprehensive and timely and up to date information for Board and Committee decision-making;
(f) To identify and manage (including but not restricted to managing through forward plans) material risks to compliance with the conditions of its license;
(g) To generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery;
(h) To ensure compliance with all applicable legal requirements.
5. The Board is satisfied that the systems and/or processes referred to in paragraph 4 (above)should include but not be restricted to systems and or processes to ensure: (a) That there is sufficient capability at Board level to provide effective organisational
leadership on the quality of care provided; (b) That the Board’s planning and decision making processes take timely and
appropriate account of quality of care considerations; (c) The collection of accurate, comprehensive and up to date information on quality of
care; (d) That the Board receives and takes into account accurate, comprehensive and up to
date information on quality of care;

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 10 of 10
(e) That the Trust, including its Board, actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources;
(f) That there is clear accountability for quality of care throughout the Trust including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
6. The Board is satisfied that there are systems to ensure that the Trust has personnel on the
Board, reporting to the Board and within the rest of the organisation who are sufficient in number and appropriately qualified to ensure compliance with its NHS provider license.
7. The Board is satisfied that during the financial year most recently ended the Licensee has
provided the necessary training to its Governors, as required in s151(5) of the Health and Social Care Act, to ensure they are equipped with the skills and knowledge they need to undertake their role.
Trust Board of Directors South Western Ambulance Service NHS Foundation Trust

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 1 of 4
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: NHS Improvement Activity Update
Prepared by: Rachel Tozer, Acting Planning Manager
Presented by: Jennie Kingston, Deputy Chief Executive / Executive Director of Finance
Action: Assurance
Recommendation:
The Board of Directors is asked to take assurance from the information provided.
Executive Summary:
The purpose of this report is to provide the Board of Directors with: An update on key correspondence from NHS Improvement; Assurance of compliance with deadlines set for information returns and
ad hoc submission requirements.

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 2 of 4
NHS Improvement Activity Update 1. Introduction
1.1. The purpose of this report is to provide the Board of Directors with:
An update on key correspondence from NHS Improvement (NHSI); and Assurance of compliance with deadlines set for information returns and ad hoc
submission requirements. 2. Letters/Correspondence with NHSI
2.1. The table overleaf sets out correspondence with/from NHSI since the last update to the Board. File Ref: 03 April 2018: Local Clinical Excellence Award (LCEA) Schemes and Junior Doctors Contract 2016 Letter from Spencer Prosser, Regional Director of Finance South - NHSI Letter requesting information on Local Clinical Excellence Award (LCEA) Schemes. Some trusts stopped or substantially reduce investment in LCEA; this resulted in a legal challenge from the BMA against the Department of Health and Social Care which has now been settled. A nil return was made to the template, as this does not apply to the Trust. The letter also requested Trust’s notify NHSI if the organisation has incurred unexpected additional costs relating to the new contract for Junior Doctors. No return was submitted.
NHSI.1
18 April 2018: 2018/19 Planning Round Letter from Ian Dalton CBE, Chief Executive – NHSI Letter issued to all NHS Foundation Trusts relating to concerns that some Trust’s do not have sufficiently robust plans. All Trusts were asked to review their plans before the 30 April deadline, with reference to: ‘the activity levels you will deliver; the financial position you will sustain; and the performance levels you genuinely expect to deliver, highlighting any gaps against national planning requirements.’ The Trust’s plan was suitably robust, and did not receive significant challenge from the local NHSI team when submitted.
NHSI.2
20 April 2018: Notification of Indicative Sustainability and Transformation Fund (STF) Value Letters from Elizabeth O’Mahony, Chief Financial Officer – NHSI Two letters about STF incentive and bonus scheme. The first details the arrangements for the scheme for 17/18. The second letter is individual to the Trust and confirms that it is not entitled to STF income as it has not accepted the control total.
NHSI.3

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 3 of 4
File Ref: 3 May 2018: Consultancy Spend Approval Process Letter from Jeremy Marlow, Executive Director Operational Productivity, Stephen Hay Executive Director Regulation/Deputy Chief Executive and Kathy Mclean Executive Medical Director/Chief Operating Officer Letter reminding Trust’s to comply with the management consultancy spend limits and process. If required these are handled by the Executive Director of HR and OD.
NHSI.4
NHSI Investigation Update
2.2. As previously updated, following the closure of their investigation NHSI set out nine informal actions that NHSI deem are the most appropriate in supporting the Trust to address the specific issues raised over the NHS 111 service. Provider Review Meetings (PRM) were set up for the remainder of the financial year at which the Trust will provide ongoing assurance to NHSI. These meetings have now been renamed as Integrated Delivery Meetings (IDM)
2.3. At the February PRM NHSI verbally confirmed closure of the final informal action. However, they advised they would seek assurance on progress against the Trust’s Management Action Plan, developed following the Well Led Review, up to June 2018 when the last action is due for completion.
2.4. Since the last Board update one IDM was held on the 17 April 2018. IDMs review Trust performance, quality measures, financial performance and other updates as required throughout the year. This meeting included discussions relating to the 2017/18 financial position, the 2018/19 Operating Plan, the 2018/19 A&E Contract and the ARP Spring Review. NHSI were updated on executive appointments, CQC inspection, operations restructure and recruitment, and the impact of the Salisbury incident. The next meeting is due to be held on the 5 June 2018.
3. Submissions
3.1. The following submissions have been made to NHSI since the last Board update. Where a deadline was provided all were delivered either before or on the deadline: Standard Reporting The Month 12 2017/18 key data return on 17 April 2018 The Month 12 2017/18 financial and workforce monitoring returns, including Trust
Accounts Consolidation Schedules, on the 24 April 2018; Final 2018/19 Operating Plan and associated documents on 30 April 2018; Handover Delay information for the months of March and April 2018; Weekly agency returns reporting any instances where the Trust has exceeded the price
cap and/or secured agency staff via off-framework agreements; Updates for incidents that are due to go to inquest shortly and any instances a

Trust Public Board of Directors Meeting – Friday 25 May 2018 Page 4 of 4
Prevention of Future Deaths Report has been issued to the Trust; Paramedic Re-Banding and NQP Assurance Template on 23 March 2018 and 23 April
2018; Notifications and updates for complaints currently being investigated by the
Parliamentary Health Service Ombudsman; Notification of incidents that have received media interest along with the Trust’s
response.
Ad Hoc/Other Nil return for the LCEA Return Emergency Operations Centre (EOC) data return to the National Operational
Productivity Team; Response to questions relating to the Draft Operating Plan; Response to CQUIN reserve query for 18/19 contract; Update on decontamination teams relating to the Salisbury Incident; Sharing papers linked to the Integrated Delivery Meeting (previously known as the
Provider Review Meeting) held in March 2018;
4. Recommendation The Board of Directors is asked to take assurance from the information provided. Rachel Tozer, Acting Planning Manager

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 5
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: General Data Protection Regulation (GDPR) Update
Prepared by: Tineke Dixon, IM&T Programme Manager
Presented by: Martin Roe, Interim Director of IM&T
Action: Assurance
Recommendation:
The Trust Board of Directors is asked to note the progress on GDPR and to be assured that following the GDPR Project the Trust is compliant as of 25 May 2018.
Executive Summary:
This paper updates the Trust Board on the current status of the General Data Protection regulation (GDPR) and the work undertaken to meet compliance for 25th May 2018 when the regulation comes into force. The Trust is 94% compliant which is in the low risk categorisation and many dimensions are within the 75%-100% compliance standard of best practice. This paper also presents for assurance the key policies and risks and their impact on the organisation.

Trust Public Board of Directors – Friday 25 May 2018 Page 2 of 5
GDPR Update 1 Introduction
1.1 This paper updates the Trust Board on the current status of the General Data Protection
regulation (GDPR) and the work undertaken to meet compliance for 25th May 2018 when the regulation comes into force.
1.2 As part of the implementation phase of the project a number of policies required substantial
updates. 2 Summary GDPR progress 2.1 The Project has been working to remain on track and to progress towards compliance.
However, it is recognised that the Trust has had a number of competing high priority activities that have delayed responses in some areas and plans have been adjusted accordingly.
2.2 The Assurance Heat Map in the GDPR Highlight report shown below shows where our level
of compliance is of 25th May 2018. From the spider map and the table you can see that our overall compliance is 94% and identifies the Trust as low risk for GDPR compliance. Where 75-100% represents best practice. The areas remaining in the “needs minor improvement” sector have action plans in place to bring them into the best practice by the end of June 2018. The key areas will be set out below. Assurance Heat Map
2.3 The steps to compliance include:-
Collecting the information assets and data flows from all areas of the Trust to form the
baseline of our understanding.
Cat Description Score ICO1 Corporate awareness 100% ICO2 Data we hold and process 100% ICO3 Privacy information 75% ICO4 Individual's rights 86% ICO5 Subject Access Requests (SAR) 93% ICO6 Lawful basis for processing 100% ICO7 Consent 100% ICO8 Data on children 100% ICO9 Data breaches 100% ICO10 Privacy Impact Assessments (DPIA) 100% ICO11 Data Protection Officer (DPO) 100% ICO12 Processing by 3rd parties 75%

Trust Public Board of Directors – Friday 25 May 2018 Page 3 of 5
Risks are then analysed and ways of working developed to mitigate unacceptable risk and renew policies and processes to manage our data in a compliant way.
The final step is to implement and evidence our compliance. This is the stage we are in now.
2.4 We are now compliant in all areas; however there is ongoing work in some dimensions to fully assure the implementation. ICO3 and ICO12 are areas that are yet to complete their implementation due to delays in the previous steps.
2.5 Data Flows were circulated to the business in February with the expectation of completion by the end of March. However, some of these were not completed in some areas until 14th May 2018. The project was RAG rated as Amber because of this, however, intensive work in the past two weeks has progressed this to compliance just ahead of the go-live date and the project is now Green.
2.6 Key items that are outstanding include ICO3 and ICO4 which require policy approvals will be
sought from the Audit and Assurance Committee.
2.7 The other requirement (ICO12) for us to seek assurance from external bodies and suppliers has been difficult and we have not had all of the responses returned yet. A further piece of work may follow as to how we respond to non-compliant data processing and contracts.
2.8 Several of the dimensions required the confirmation of the Trust’s agreed roles and
responsibilities; these are set out below for information.
Role Description Responsibility Person Caldicott Guardian
Senior health professional responsible for person identifiable health information held in the Trust
Executive Medical Director
Dr Andy Smith
Data Protection Officer (DPO)
Senior Information practitioner responsible for ensuring Trust compliance with GDPR, data protection strategy and implementation
DPAS Nigel Gooding
Senior Information Risk Officer (SIRO)
Board level accountability for information risks
Executive Director of IM&T
Martin Roe (interim)
3 Privacy notices
3.1 The Trust has developed two privacy notice: one for patients and one for employees.
3.2 The Patient Privacy Notice that explains to patients the purposes for which we collect their
data and how we use it. It also outlines their rights to see what we hold about them (Subject Access Requests) and in some cases have data deleted.
3.3 The Privacy Notice for Employees covers similar information to the Privacy Notice for Patients, except in the context of a staff member. Clearly the purposes are different, and so are data subjects rights in this case. This policy also includes other stakeholders such as volunteers, Non-Executive Directors and Governors.

Trust Public Board of Directors – Friday 25 May 2018 Page 4 of 5
3.4 Both Privacy Notices were developed from the Data Flows and our understanding of what data we collect and how we use it. These are living documents and will be regularly reviewed if there are new data flows that we need to declare. These are presented to the Trust board for information
4 Policies 4.1 The Trust will be developing a Data Protection Officer (DPO) Policy sets out the roles and
requirements of the DPO. The Policy highlights the mechanism for incident reporting, data privacy impact assessments (DPIA), and advice and guidance intrinsic to the role of the DPO. This will be presented to Audit and Assurance Committee for approval.
4.2 There are a number of other policies that require review in the light of GDPR that have been
signed off by other mechanisms. These are set out in the table below.
Document Type Owner Content Approval Route
Information Asset Management Policy
Policy Kevin Pointer / Nigel Peirce
Information Asset Management IG Group, Audit & Assurance for info
Corporate Records Management Policy
Policy Kevin Pointer Records Management of Corporate Documents
Directors /SLT
Data Privacy Impact Assessment SOP IG04
SOP Kevin Pointer Data Privacy Impact Assessment Completion Process
IG Group
SWASFT Access & Disclosure of Personal & Sensitive Information Policy
Policy Kevin Pointer General guidance for review and access to personal / sensitive information
Directors / SLT
Subject Access Request SOP
SOP Kevin Pointer Subject Access Request Completion Process
IG Group
Incident Reporting Policy Policy Caroline Brown / Vanessa Williams
IG SIRI Reporting (Sections 8, 9) IG Group, Audit & Assurance for info
Keeping information private and confidential - a guide for staff
Leaflet Kevin Pointer Staff Awareness Leaflet HR Management/ IG Group
Information Risk Assessment IGO5
SOP Kevin Pointer Risk assessment for IG to identify associated risks for Information Assets
IG Group
IM&T Security Policy Policy Nigel Pierce Information Security and BD, DR Audit and Assurance
Use of IM&T Services Policy
Policy Rob White Incident Reporting Process (Section 6)
IM Managers Mtg, Directors/SLT
Complaints Policy Policy Donna Bamford Consent and Verification of ID (Section 7)
Quality Committee

Trust Public Board of Directors – Friday 25 May 2018 Page 5 of 5
5 Risks
5.1 The delivery of the GDPR “project” has its own risk register. The key risk remaining to the
project is Changes to contracts that contain data security clauses need to be amended. This
includes MOUs and Information Sharing Agreements with public bodies where we share personal information (3x4=12);
5.2 In addition to the project risks we have identified two risks for the Corporate Risk Register in
relation to data security and data breaches and the potential consequences under GDPR. Composite IG risks : Potential non-compliance with IG and Information security
requirements through the loss of paper based records, technical solutions to protect personal information, non-compliance with the process for completion and delivery of records and information requests
Potential non-compliance with GDPR and action to be taken by Information Commissioners Office with financial and reputational impact. Or claims against the Trust by data subjects for inappropriate use of personal data.
5.3 Action plans to change the business process to reduce or avoid the risks may be required by
the DPO and these will be addressed with the Information Asset Owner. 6 Recommendation 6.1 The Trust Board of Directors is asked to note the progress on GDPR and to be assured that
following the GDPR Project the Trust is compliant with GDPR as of 25 May 2018. Tineke Dixon Programme Manager

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 26
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: Joint Board Assurance and Risk Report
Prepared by: Emma Murgatroyd, Quality Support Manager Vanessa Williams, Head of Quality
Presented by: Jenny Winslade, Executive Director of Nursing and Quality
Action: Assurance
Recommendation:
The Board of Directors is asked to take assurance from the information provided.
Executive Summary:
There are 49 current risks on the Corporate and Directors Risk Register.
There is one risk which has a current risk rating of 25; Incident Stacking (A&E)
There are seven risks that have a current risk rating of 20. These are:
ARP Performance Targets Major IT Service Failure Service Changes and the Impact on the Ambulance Service Reputation Commissioner Affordability External Impact on Finance Strategy 999 Clinical Call Audit Compliance
A deep dive has taken place for the eight risks which have current scores of 25 and 20. The Internal Audit review of the BAF recommended that the Board of Directors receive a deep dive on risks that sit below the highest level risks on a rotational basis. For the May 2018 BAF the additional risk included for review is ‘GDPR Compliance’.

Trust Public Board of Directors – Friday 25 May 2018 Page 2 of 26
Joint Board Assurance and Risk Report 1. Introduction 1.1 The purpose of the joint Risk and Board Assurance report is to enable the Board of
Directors to have meaningful discussions about the management of key strategic risks that could impact upon the achievement of long term, strategic priorities. The report will continually evolve and will require regular review and update in order for its content, and the framing of strategic risks, to remain live.
1.2 This report is composed of two parts which taken together should enable the Board to take
assurance from the range of activities undertaken and the evidence provided. The two key parts are the Corporate and Directors Risk Register – The Trust’s Governance and Risk Strategy sets out the process for the management of the risk registers. The Quality Risk Assurance Group (QRAG) is responsible for reviewing the content of the risk registers, quality assuring and proposing changes to risks. The combined risk register is presented for information. The content and format of the risk register is currently being reviewed in light of the procurement of the new risk platform which is due to be implemented by the end of the financial year.
1.4 Board Assurance Framework – The BAF provides a simple but comprehensive method for
the effective and focused management of the principle risks to meeting the strategic objectives of the Trust and provide a structure for the evidence to support the Annual Governance Statement. The highest rated risks from the Corporate Risk Register have been explored in more detail for the Board of Directors to be able to gain the assurance that they require that the risks are being effectively managed.
1.5 A review of the Corporate and Directors Risk Register took place ahead of the move from the previous Excel based Risk Register to the Trust’s new online Pentana Risk Management system. This piece of work was aimed at refining the Risk Register as well as making the monitoring and the challenging of assurance of risks more efficient and easier. This report reflects the current, reworked risks. A meeting took place with the chair of the Audit and Assurance Committee to discuss reporting arrangements where it was agreed that the Board will receive a report in the new format at its July meeting.
1.6 The scoring matrix for risk and assurance is in Appendix A of this report.
2. Summary 2.1 There are 49 current risks on the Corporate and Directors Risk Register. Appendix B
provides a summary of the current corporate level ‘red’ risks, i.e. those scoring 15 – 25.

Trust Public Board of Directors – Friday 25 May 2018 Page 3 of 26
2.2 The previous ‘Call Audit 999’ risk (risk score of 16) has been split into Clinical and Non-
Clinical due to the different challenges experienced between the two systems for call audit in achieving call audit compliance. ‘999 Clinical Call Audit Compliance’ has been scored as 20 (Consequence: Serious (4), Likelihood: Almost Certain (5)). ‘999 Non-Clinical Call Audit Compliance’ has been scored as 16 (Consequence: Serious (4), Likelihood: Likely (4)). Risk Assessments have been completed for both risks and these were reviewed at the Quality Risk Assurance Group on 09 May 2018.
2.3 There are eight risks that have a current score of either 25 or 20. These are:
Risk Current Forecast Incident Stacking (A&E) 25 15
Reputation 20 20
Commissioner Affordability 20 20
External Impact on Finance Strategy 20 20 ARP Performance Targets 20 15 Major IT Service Failure 20 15 Service Changes and the Impact on the Ambulance Service 20 12
999 Clinical Call Audit Compliance 20 12 2.4 Since the Risk Register was last presented to the Board of Directors the ‘TUPE – Litigation’
risk has been removed as this is now an issue rather than a risk.
Date Total Scored at
15 – 25 Scored at 10
– 12 Scored at
Less than 9
January 2017 66 37 29 0
March 2017 70 39 28 3
May 2017 67 37 29 1
July 2017 56 28 28 0
September 2017 58 31 25 2
November 2017 56 31 25 0
January 2018 56 32 22 2
March 2018 56 34 21 1
May 2018 48 30 17 2

Trust Public Board of Directors – Friday 25 May 2018 Page 4 of 26
2.5 The ‘Resilience – Business Continuity’ risk has been reduced from a risk score of 12 (Likelihood: Possible (3), Consequence: Serious (4)) to 9 (Likelihood: Possible (3), Consequence: Moderate (3)) as confirmed by the Director of Operational Services due to the progress made under the Business Continuity Plan and the exercises which have been undertaken.
2.6 A deep dive has taken place for the eight risks which have a current score of 25 or 20. The
Internal Audit review of the BAF recommended that the Board of Directors receive a deep dive on risks that sit below the highest level risks on a rotational basis. For the March 2018 BAF the risk included for review is ‘GDPR Compliance’.
2.7 Risks based on current and forecast scores are below. The forecast scores are in the
process of being reviewed with individual directorate risk leads;.
Current Score Number of Risks Forecast score Number of Risks 25 1 20 3 20 7 16 1 16 12 15 11
15 10 12 11
12 13 10 4 10 4 9 6
9 1 8 9
8 1 6 2 6 - 5 -
5 - 4 2
0 - 3 -
2 -

Trust Public Board of Directors – Friday 25 May 2018 Page 5 of 26
3. Corporate Risk Register Mapping Against the Strategic Goals
Strategic Goal 1: Every Patient Matters (36 risks) Risk description Current Forecast
Incident Stacking (A&E) 25 15 999 Clinical Call Audit Compliance 20 12 Major IT Service Failure 20 15 ARP Performance Targets 20 15 Service Changes and the Impact on the Ambulance Service 20 12 Reputation 20 20 OOH Resourcing and Performance 16 12 111 Resourcing and Performance 16 12 Restraint 16 9 Management of Controlled and Non Controlled Medicines 16 8 Infection Control Compliance 16 12 Locating Patients 16 12 Changes in Activity 16 16 Impact of REAP Levels, and Summer, Winter and Peak Pressures 16 8 Submission of Safeguarding Referrals via EPCR 16 4 Investigation Delays 16 12 Inability to Answer 999 Calls 16 15 999 Non-Clinical Call Audit Compliance 16 12 Timely Complaint Response 15 9 C3 Split Brain – Assurance of Resilience 15 15 Operational Resources (A&E) 15 10 Impact of STPs and other National change programs 15 15 Terrorist Activity 15 15 Pollution Regulation Activity 15 10 Clinical Alerts (Warning Markers) – A&E 15 8 Handover Delays at Hospital – Impact on Patient Safety and Resource Availability 15 15
Safeguarding Compliance 12 9 Serious Incident Process 12 8 Regional Care Plan Strategy 12 6 Information Governance and Security Requirements 12 6 Provision of Welfare Calls within the 999 Clinical Hubs 12 8 Frequent Caller Record Management 12 8 Care Quality Commission 10 10 Patient Clinical Records 10 8

Trust Public Board of Directors – Friday 25 May 2018 Page 6 of 26
Vehicle Security 10 10 Resilience – Business Continuity 9 9
Strategic Goal 2: Every Team Member Matters (2 risks)
Risk description Current Forecast Potential Loss of the Dorset NHS 111, OOH, and SPoA Contract 12 12 Health and Safety – Strategic Oversight 10 8
4. Heat Map Overview of May 2018 Risk Register
4.1 The heat map has been populated using all 49 risks contained within the Corporate and Directors Risk Register.
May 2018 – CURRENT SCORE
Strategic Goal 3: Every Pound Matters (11 risks) Risk description Current Forecast
Commissioner Affordability 20 20 External Impact on Finance Strategy 20 20 Financial Position (Operations Directorate) 15 15 Cost Improvement Strategy 15 15 Impact of IR35 12 12 Procurement Compliance 12 12 Service Line Development Project Creep 12 12 NHS Transition Network 12 9 NHS Mail 12 9 Off Payroll Arrangements 12 8 GDPR Compliance 8 4
Rare Unlikely Possible Likely Almost Certain
Negligible Low
Moderate 1 6 1
Serious 1 7 12 3 Very
Serious 4 9 4 1

Trust Public Board of Directors – Friday 25 May 2018 Page 7 of 26
May 2018 – FORECAST SCORE
Rare Unlikely Possible Likely Almost Certain
Negligible
Low 1
Moderate 2 6 2
Serious 2 8 10 1 1 Very
Serious 4 10 2

Trust Public Board of Directors – Friday 25 May 2018 Page 8 of 26
5. Board Assurance – Deep Dive: Incident Stacking (A&E) Date added: April 2016 Risk Owner: Executive Director of Operations Executive Summary Overarching Risk Area: Patient Harm (Delayed Responses) The risk of stacking calls within the 999 Clinical Hubs which could impact patient safety, patient experience, staff morale and performance. This risk is currently scored as 25 (Consequence: Very Serious (5), Likelihood: Almost Certain (5) as of 05 March 2018 – previously scored as 20). Key controls in place include the introduction of a number of Clinical Hub SOPs to support triage, Welfare Calls etc., the use of GPs within the Hubs for advice and assistance, appointment of Operational Support Officers and the use of RRVs for face to face welfare checks. Key actions required to further mitigate this risk include recruitment to Clinical Hub clinician vacancies, recruitment of additional Call Handlers, a Clinical Hub restructure and a rewrite of the Ambulance Quality Indicator guidance. Confirmation of full establishment of Clinical Hub clinicians and additional Call Handlers is required to provide further assurance. Risk Description Stacking of Cat 2, Cat 3 and 4 calls due to the availability of resources and/or high demand could affect patient safety, patient experience, staff morale and performance.
Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score V. Serious
5 Almost Certain
5 25 Serious 5
Possible 3 15
Rationale for current score Quality Performance Reputation HR Health and Safety
Rationale for forecast score Quality Performance Reputation HR Health and Safety
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 3 2 9 - STRONG

Trust Public Board of Directors – Friday 25 May 2018 Page 9 of 26
History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 20 20 20 20 20 20 20 20 20 20 25 25
Forecast 10 10 10 10 10 10 10 15 15 15 15 15 History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 9 9 9 9 9 9 9 9 9 9 9 9 Controls in place
Demand Management Plan in place; A suite of SOPs is in place – including the Welfare SOP – to manage patients in the call queue; Clinical Supervisors’ constant review of the call queue; Robust plans in place to reach clinical establishment in the Hub.
Assurance Source Evidence of Assurance ICPR and performance reporting to Board of Directors Board minutes Patient Safety reports to Quality Committee Record of reports Reports to IQPMG at Commissioner meetings Commissioner minutes Duty Performance Manager monitors stack and escalates as appropriate to Gold Commander
Live web reporting Record of reports Gaps in assurance
Increased number of DCAs required; Hub clinician rota review.
Actions to be taken to close the gap Single Escalation Framework document to be produced (combining the previous Demand Management Plan and
REAP document)– deadline: 30 June 2018; Development of Performance Improvement Plan (PIP) – deadline: 31 May 2018; Development of Achieving National Standards through Investment and Transformation – deadline: 31 July 2018; Hub Clinician recruitment plan implemented and in progress – deadline: 14 September 2018; Ongoing review and monitoring of resourcing within the Clinical Hubs – deadline: 14 September 2018.

Trust Public Board of Directors – Friday 25 May 2018 Page 10 of 26
6. Board Assurance – Deep Dive: Reputation Date added: April 2016 Risk Owner: Chief Executive Executive Summary Overarching Risk Area: Reputation The risk of potential damage to the Trust’s reputation could lead to a loss of confidence by patients, commissioners, stakeholders and staff. This risk is currently scored as 20 (Consequence: Serious (4), Likelihood: Almost Certain (5)). Key controls are a proactive and robust communications and engagement plan and ongoing liaison with the National Ambulance Communications Group (NACOM). Key actions required to further mitigate this risk are to undertake a review and update of the communications and engagement plan and the completion of an annual review of stakeholder activity. The Trust cannot provide any assurance related to unplanned or unknown external factors. Risk Description The potential for adverse reputation which could lead to a loss of confidence of patients, commissioners, stakeholders and staff.
Risk Score – CURRENT Risk Score – FORECAST Consequence Likelihood Risk Score Consequence Likelihood Risk Score
Serious 4
Almost Certain
5 20 Serious
4 Possible
3 20
Rationale for current score Quality Reputation HR
Rationale for forecast score Quality Reputation HR
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
1 2 3 2 8 - MODERATE
History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018

Trust Public Board of Directors – Friday 25 May 2018 Page 11 of 26
Current 12 20 12 12 20 20 20 20 20 20 20 20
Forecast 8 12 12 12 12 12 12 20 20 20 20 20 History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - 8 8 8 8 8 8 8 8 Controls in place
Proactive Communications and Engagement plan in place (which includes FOI forward view, Regular reminders issued to staff via internal communication channels on ways to raise concerns internally and maintaining a close working relationship with the Patient Experience and Claims & Inquests teams who highlight any potential media cases, etc.);
Ongoing liaison with National Ambulance Communications Group (NACOM) which enables agreed national lines and early warnings.
Assurance Source Evidence of Assurance Patient Surveys Survey Responses Friends and Family Test FFT Score Reports to the Board of Directors Reports Kantar media monitoring Kantar access Gaps in assurance
Unplanned or unknown external factors Communications team resourcing
Actions to be taken to close the gap
Review and update of Communications and Engagement Plan – deadline 26/07/2018; Annual review of stakeholder activity – deadline 01/03/2019

Trust Public Board of Directors – Friday 25 May 2018 Page 12 of 26
7. Board Assurance – Deep Dive: Service Changes and the Impact on the Ambulance Service
Date added: May 2017 Risk Owner: Executive Director of Operations Executive Summary Overarching Risk Area: Patient Harm (Delayed Responses) The risks presented to the Trust by changes to the Health Service. This risk is currently scored as 20 (Consequence: Serious (4), Likelihood: Almost Certain (5)). Key controls include engagement with STPs and the Strategic Partnership Board, ORH modelling and impact of service change methodology. Key actions required to further mitigate this risk include negotiations for additional funding relating to service change, the production of a service development map and contract negotiations. Any decisions made regarding changes in healthcare provision across the Trust’s patch will ultimately be made external to the Trust, however additional assurance can be sought via the Trust applying for additional funding. Risk Description Changes to Health Services (as a result of service change arising from a change in location of services, a change in the journey time, a change in the volume of incidents or other activity, changes in patient pathways etc.) will impact on the Trust including the availability of resources to respond safely, patient journey times (affecting patient safety and experience), staff experience, performance and finances.
Risk Score – CURRENT Risk Score – FORECAST Consequence Likelihood Risk Score Consequence Likelihood Risk Score
Serious 4
Almost Certain 5 20 Serious
4 Possible
3 12
Rationale for current score Quality Reputation Performance Financial HR
Rationale for forecast score Quality Reputation Performance Financial HR
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 3 3 2 10 – STRONG

Trust Public Board of Directors – Friday 25 May 2018 Page 13 of 26
History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - 20 20 20 20 20 20
Forecast - - - - - - 12 12 12 12 12 12 History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - 10 10 10 10 10 10 Controls in place
Methodology developed for estimating and assessing the impact of service change; Ongoing communications with Commissioners regarding service changes; Principles of service change agreed.
Assurance Source Evidence of Assurance Regular updates on STP plans and meetings provided to the Executive Directors / SLT by Planning & Performance Team
Updates and meeting papers
Service Change Map produced and submitted to SPB Service Change Map SPB (Strategic Partnership Board) first meeting July 2017. Process for agreeing service change ratified at this meeting. Meetings bi-monthly for 2017/18.
Meeting Minutes
CQUIN quarterly submissions - Commissioners receive these quarterly updates as this is linked to a CQUIN worth £924k in 17/18
CQUIN quarterly submissions
Gaps in assurance
Any decisions made regarding changes in healthcare provision across the Trusts geography will ultimately be made external to the Trust;
The need to negotiate for additional funding. Actions to be taken to close the gap
Clinical Directorate to continue to monitor service change using their methodology for estimating and assessing the impact of service change – deadline: 29 March 2019;
Continue communications with Commissioners regarding service changes – deadline: 29 March 2019; Continue to attend and feed into the Strategic Partnership Board – deadline: 29 March 2019.

Trust Public Board of Directors – Friday 25 May 2018 Page 14 of 26
8. Board Assurance – Deep Dive: ARP Performance Targets Date added: March 2018 Risk Owner: Executive Director of Operations Executive Summary Overarching Risk Area: Patient Harm (Delayed Responses) The potential risk of not achieving and sustaining ARP performance targets – this risk is currently scored as 20 (Consequence: Very Serious (5), Likelihood: Likely (4)). Key controls in place include actions undertaken as part of the Quality Performance Improvement Plan (QPIP), the introduction of new rotas within Operations and the Clinical Hubs and robust Executive Director and Operational Senior Manager monitoring of performance, establishment, delayed calls, hospital handovers and the A&E Operating Plan. Key actions required to further mitigate this risk include the development of new web reports to enable review of performance against the new standards, discussion and agreement to be made regarding the future configuration of specialist functions (i.e. Air Operations, HART etc.) within the Hub, recruitment of additional call handlers and Clinical Hub clinicians. Assurance of the full implementation of the 2017/18 Operating Plan and a review of the proportion of patients being categorised as CAT1 and CAT2 is required as this is an area of concern. Risk Description The potential for not achieving and sustaining ARP performance targets which could impact on patient safety, patient experience, staff experience, the Trust's reputation and financial position and the Single Oversight Framework. Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score
V Serious 5
Likely 4 20 V. Serious
5 Possible
3 15
Rationale for current score Quality Reputational Regulatory Performance Financial Business Continuity
Rationale for forecast score Quality Reputational Regulatory Performance Financial Business Continuity

Trust Public Board of Directors – Friday 25 May 2018 Page 15 of 26
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 3 2 9 – STRONG History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 20 20 20 20 20 20 20 20 20 20 20 20
Forecast 10 10 10 10 10 10 10 15 15 15 15 15
History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 9 9 9 9 9 9 9 9 9 9 9 9 Controls in place
Extended Delay Review Process; ORH Modelling Dataset; Performance Assurance Meeting (PAM).
Assurance Source Evidence of Assurance Monthly reports to IQPMG Minutes ICPR report for Trust Board Board minutes Reports to NHSI Record of reports Weekly performance report to Executive Directors Record of reports Monthly performance report to SLT Records of meetings Live web reports Record of reports Weekly meetings with Deputy CEO/Executive Director of Finance, Planning and Performance to monitor and Progress QPIP Records of meetings
Gaps in assurance
Full implementation of Operating Plan; Increased number of DCAs required.
Actions to be taken to close the gap
Demand Management Plan to be reviewed – deadline: 30 April 2018; Development of Performance Improvement Plan (PIP) – deadline 31 May 2018; Performance Assurance Meeting led by the Deputy Chief Executive/Executive Director of Finance –
deadline: 30 July 2018; ORH Remodeling – deadline: 31 August 2018.

Trust Public Board of Directors – Friday 25 May 2018 Page 16 of 26
9. Board Assurance – Deep Dive: Commissioner Affordability Date added: 26 April 2016 Risk Owner: Deputy Chief Executive/Executive Director of Finance Executive Summary Overarching Risk Area: Financial Position The risks presented to the Trust by its ability to mitigate the gap in funding within its contracts. This risk is currently scored as 20 (Consequence: Very Serious (5), Likelihood: Likely (4)). Key controls are: contracts, operational modelling, Financial plan and a Cost Improvement Plan in place, managing MAVIS to affordable levels and negotiation of a 2 year contract. Key actions in place to be undertaken include ongoing participation in STPs, establishment of an ongoing engagement in a Strategic Partnership Board with Commissioners and ongoing monitoring. Further assurance is required in order to quantify all risks based on the updates on recent guidance and changes in assumptions and the costs. This will be an ongoing process which will need to be part of the in-year management of financial risks in 2018/19. Risk Description The ability of the Trust to mitigate the gap in funding within the contracts as part of contract negotiations. Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score
V. Serious 5
Likely 4 20 V. Serious
5 Likely
4 20
Rationale for current score Quality Performance Financial HR
Rationale for forecast score Quality Performance Financial HR
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 3 2 9 – STRONG

Trust Public Board of Directors – Friday 25 May 2018 Page 17 of 26
History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 20 20 20 20 20 20 20 20 20 20 20 20
Forecast 15 15 15 15 20 20 20 20 20 20 20 20
History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 9 9 9 9 9 9 9 9 9 9 9 9 Controls in place
Contracts in place with Commissioners; Operational Modelling undertaken by ORH; Trust Financial Plan including Cost Improvement Plan approved by the Trust Board of Directors.
Assurance Source Evidence of Assurance MEAP Gaps in assurance
Identification of all risks based on the updates on recent guidance and changes in assumptions and costs. This will be an ongoing process which will need to be part of the in-year management of financial risks.
Actions to be taken to close the gap
A&E modelling of resource, performance and demand profiling being undertaken – deadline: 29 March 2019; Participation in STP process – deadline: 29 March 2019;

Trust Public Board of Directors – Friday 25 May 2018 Page 18 of 26
10. Board Assurance – Deep Dive: External Impact on Finance Strategy Date added: 24 August 2017 Risk Owner: Deputy Chief Executive/Executive Director of Finance Executive Summary Overarching Risk Area: Financial Position The risk of legislative, contractual or regulatory changes made by government bodies which impact on the Trust’s Finance Strategy. This risk is currently scored as 20 (Consequence: Very Serious (5), Likelihood: Likely (4)). Key controls in place include support from NHS Improvement, good relationships with Commissioners, recruitment planning, professional advisors in place, A&E Contract in place and Finance Directorate review of financial decisions made by external organisations. Key actions in place to mitigate this risk include ongoing liaison with NHS Improvement, use of professional advice when needed, the completion and presentation of a Brexit Risk Assessment to the Audit and Assurance Committee and a review of inflation on budget setting. Risk Description Legislative, contractual or regulatory changes made by government bodies that impact on the Finance Strategy of the Trust. Likelihood score increased due to increased external financial pressures, e.g. pay award, national funding decisions, etc. Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score
V. Serious 5
Likely 4 20 V. Serious
5 Likely
4 20
Rationale for current score Financial HR
Rationale for forecast score
Financial HR
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 3 2 9 – STRONG
History of the risk

Trust Public Board of Directors – Friday 25 May 2018 Page 19 of 26
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - - 15 15 20 20 20
Forecast - - - - - - - - 20 20 20 20
History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - - 9 9 9 9 9 Controls in place
Internal Employment Law expertise; Finance, and where necessary professional advisors, review financial decisions by external organisations; Contact in place with Commissioners; Procurement contracts based on multi-year arrangements where possible; Support from NHS Improvement who also set the tariff inflation within contracts to consider the impact of
elements such as the National set pay award. Assurance Source Evidence of Assurance Gaps in assurance
Actions to be taken to close the gap Review procurement contracts and the financial impact of inflation by the Finance Team – deadline: 31 July
2018; Establishment of risk specific teams – deadline: 24 September 2018; Ongoing monitoring of risk – deadline: 01 October 2018; Ongoing liaison with NHS Improvement – deadline: 29 October 2018.

Trust Public Board of Directors – Friday 25 May 2018 Page 20 of 26
11. Board Assurance – Deep Dive: Major IT Service Failure Date added: February 2007 Risk Owner: Executive Director of IM&T Executive Summary Overarching Risk Area: Business Continuity The risk of potential major IT service failures which could lead to business continuity issues and could impact on the Clinical Hubs, radios, mobile data or telephony. This risk is currently scored as 20 (Consequence: Very Serious (5), Likelihood: Likely (4)). Key controls in place are the regular backing up of all IT systems, Business Continuity plans in place, third party maintenance contracts in place for Gold/Platinum assets and regular patching and updating of software. Key actions required to further mitigate this risk include moving to virtual telephony, development of service management processes, decommissioning of NHS Pathways for 999, the deployment of new firewalls and enhanced maintenance for Status Servers. Outstanding assurance required includes a systems upgrade, confirmation of new firewalls deployment and a Digital Strategy review. Risk Description A Major ICT service failure, which cannot be redressed via the Trust hardware/software maintenance contracts or a Cyber Security issue which allowed a vulnerability to be exploited, which could impact on the Clinical Hubs, Telephony and/or Radio or Mobile data may lead to a potential business continuity risk (including access to resources) in A&E, UCS or support services. Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score
V. Serious 5
Likely 4 20 V. Serious
5 Possible
3 15
Rationale for current score Quality Business Continuity Finance Performance Regulatory Reputation HR
Rationale for forecast score Quality Business Continuity Finance Performance Regulatory Reputation HR

Trust Public Board of Directors – Friday 25 May 2018 Page 21 of 26
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 3 2 9 - STRONG
History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 15 15 15 15 15 15 20 20 20 20 20 20
Forecast 12 12 12 12 12 12 12 15 15 15 15 15
History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current 9 9 9 9 9 9 9 9 9 9 9 9 Controls in place
‘One Domain’ project; Business Continuity Plans; Generators and Uninterrupted Power Systems (UPS); Gold ICT systems such as AirWave, CAD, etc.; Third party maintenance contracts are in place for Gold/Platinum assets i.e. Cisco Maintenance etc.
Assurance Source Evidence of Assurance Internal Audit report on business continuity Final Report Monthly Project Board meetings for IM&T projects. Minutes of meeting Reports to Audit and Assurance Committee Reports and minutes Internal Audit Report on Cyber Security Final Report Gaps in assurance
Systems upgrade; Deployment of new Firewalls; Digital Strategy review.
Actions to be taken to close the gap
Work plans to keep all Gold systems up to date – deadline: 30 May 2018; Decommission of old domains/migration to the SWAST domain is ongoing – deadline: 01 November 2018; Standardisation of remote access solutions and deployment of new secure portal – deadline: 31 December
2018; Deployment of various monitoring/alerting tools – Cisco Prime, Meraki, SolarWinds etc. – deadline: 01 April
2019.

Trust Public Board of Directors – Friday 25 May 2018 Page 22 of 26
12. Board Assurance – Deep Dive: 999 Clinical Call Audit Compliance Date added: May 2018 Risk Owner: Executive Director of Operations Executive Summary Overarching Risk Area: Quality – Safety of Care to Patients The risk not being able to meet clinical call audit compliance within the 999 Clinical Hubs. This risk is currently scored as 20 (Consequence: Serious (4), Likelihood: Almost Certain (5)). Key controls in place include the implementation of personal action plans for underperforming staff with closer monitoring, audit feedback is given to staff in a timely manner and extended 999 Clinical Audit with an increase in Clinical Team Leader staffing levels. A number of actions are being taken to attempt to make quick improvements to clinician call audit compliance. Key actions required to further mitigate this risk include the production of an Options paper, offering overtime to auditors and members of the 999 audit pool and the production and implementation of an improvement trajectory aiming to achieve compliance by 01 October 2018. Risk Description
Failure to meet 999 clinical call audit compliance which could compromise patient safety and the requirements of the licence. The potential impact could be: • The potential for the advice provided to be sub optimal; • The possibility that the quality of a member of staff’s performance may not be identified and therefore not addressed; within a timely manner with a risk to people; • A breach of the licencing requirements could compromise the Trust's position and reputation.
Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score Serious
4 Almost Certain
5 20 V. Serious 5
Possible 3 12
Rationale for current score Quality Performance Reputational Regulatory HR
Rationale for forecast score Quality Performance Reputational Regulatory HR
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 2 2 8 - MODERATE

Trust Public Board of Directors – Friday 25 May 2018 Page 23 of 26
History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - - - - - - 20
Forecast - - - - - - - - - - - 12 History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - - - - - - 8 Controls in place
All A&E Hub audits are fed back to staff in a timely manner, where possible during the staff member’s next working shift;
Audits undertaken for all A&E Hub complaints and serious incidents to ensure that any performance issues are identified;
Extended A&E Clinical Audit with increase in Clinical Team Leader staffing levels (increased time allocated to Clinical Audit and increased use of Peer Audit);
Risk assessment updated with associated actions; Under performing staff within A&E Hub have personal action plans devised with associated closer
monitoring. Assurance Source Evidence of Assurance Call Abandonment data is included within the AQI section of the ICPR which is presented to the Board of Directors, available to commissioners and is published online
Minutes of Board Record of Reports
ICPR is available to Commissioners, is published on line and includes AQIs.
ICPR
Clinical Hub Call Answering Action Plan reported to the HOPs/HODs Huddle
Meeting minutes Record of reports
Gaps in assurance
Numbers of clinicians within the Clinical Hub Improvement trajectory
Actions to be taken to close the gap
Focused efforts on Clinician recruitment – ongoing action; Introduce a 999 Audit Policy – deadline 31 May 2018; Implement new MPDS Governance Framework – deadline: 29 June 2018; Options paper to be produced during Q1 which sets out issues around call auditing – deadline: 29 June
2018; Overtime offered to auditors and members of audit pool in A&E hub to increase number of A&E audits
undertaken – deadline: 29 June 2018; Introduce levelling from Clinical Auditors – deadline: 19 July 2018; Obtain approval of an Option from the Improvement Plan – deadline: 13 May 2018; Produce an Improvement Plan Options Paper – deadline – 13 May 2018; Produce an improvement trajectory with timescales – deadline: 20 May 2018.

Trust Public Board of Directors – Friday 25 May 2018 Page 24 of 26
13. Board Assurance – Deep Dive: GDPR Compliance Date added: 10 September 2017 Risk Owner: Executive Director of IM&T Executive Summary Overarching Risk Area: Regulatory Requirements The risks of non-compliance with the GDPR (General Data Protection Regulation) which could result in financial penalties or reputational damage from published regulatory remedial action including warnings, reprimands and inspections. GDPR is due to come into effect on 25 May 2018 and the risk of non-compliance was previously scored as 15 (Likelihood: Possible (3), Consequence: Very Serious (5)). The risk has recently been reviewed due to the significant amount of progress made and the assurance that SWASFT will be 94% compliant by 25 May 2018. The risk of non-compliance is therefore currently scored as 8 (Likelihood: Unlikely (2), Consequence: Serious (4)). Key controls for this risk include the completion of a review of policies and completion of reviews of Data Flows, Information Asset Registers and Data Risk Registers. In addition, regular GDPR Project Plan and Checkpoint meetings are in place. The key actions are the engagement and communications across the Trust for Data Flows, Information Asset Register (IAR) and awareness, the appointment of a Data Protection Officer (DPO) and the Data Privacy Advisory Service (DPAS) to support SWASFT’s compliance journey and the development of Privacy Notices. Risk Description Non-compliance with the GDPR (General Data Protection Regulation) which could result in financial penalties or reputational damage from published regulatory remedial action including warnings, reprimands and inspections. Risk Score – CURRENT Risk Score – FORECAST
Consequence Likelihood Risk Score Consequence Likelihood Risk Score
Serious 4
Unlikely 2 8 Serious
4 Rare
1 4
Rationale for current score Quality Regulatory HR Financial Business Continuity
Rationale for forecast score Quality Regulatory HR Financial Business Continuity

Trust Public Board of Directors – Friday 25 May 2018 Page 25 of 26
Overall Assurance Score
How much assurance
Basis for assurance
Timeliness Rigour Assurance Score
2 2 3 3 10 – STRONG History of the risk
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - - - 15 15 15 8
Forecast - - - - - - - - 5 5 5 4
History of the assurance
Score July 2016
Sept 2016
Nov 2016
Jan 2017
Mar 2017
May 2017
July 2017
Sept 2017
Nov 2017
Jan 2018
Mar 2018
May 2018
Current - - - - - - - - 10 10 10 10 Controls in place
Management responsibilities; Information Governance Group; Incident Reporting System; IG Policies; IG requirement as part of tender submissions; Data Protection responsibilities communicated; Data Flows; Corporate and Clinical Records Management Policies as well as a Retention Schedule; Information Governance training and education programme; GDPR Project management including Checkpoint meetings; Engagement of DPAS to support compliance journey.
Assurance Source Evidence of Assurance
Checkpoint Meeting Privacy Notices Data Risk Register DPO appointment Policies and SOPS DPAS approval
Minutes from meetings including Assurance Heat Map
Privacy notes published DPAS approval Policy sign off process Communications plan
Gaps in assurance
Information Asset Management Policy, Incident Reporting Policy and Access & Disclosure Policy are written and will be presented to the Audit & Assurance Committee for approval on 14 June 2018.
External providers and supplier contracts, MOUs and ISAs need to be reviewed, GDPR compliance status to be recorded. Further work is required to ensure that the Trust is able to assure itself that non-contractual MOUs and ISAs with other public bodies are stored using a robust system.
Actions to be taken to close the gap
Consent Policy – Audit and Assurance Committee 14/06/18; Data Breach Policy – Audit and Assurance Committee 14/06/18;

Trust Public Board of Directors – Friday 25 May 2018 Page 26 of 26
GDPR Communications – Complete and ongoing; Privacy notice and Information leaflets regarding GPDR compliance – Complete and ongoing; Policy and Strategy compliance with GDPR – Audit and Assurance Committee 14/06/18; Suppliers contracts GDPR compliance – To be completed June 2018;
16. Recommendation 16.1 The Board of Directors is asked to take assurance from the information provided. Emma Murgatroyd Vanessa Williams Quality Support Manager Head of Quality

Appendix A – Risk Scoring Consequence score Severity Descriptors
1 2 3 4 5 Negligible Low Moderate Serious Very Serious
Likelihood score 1 2 3 4 5 Descriptor Rare Unlikely Possible Likely Almost
Certain
Rare Unlikely Possible Likely Almost Certain
Negligible 1 2 3 4 5
Low 2 4 6 8 10
Moderate 3 6 9 12 15
Serious 4 8 12 16 20
Very Serious 5 10 15 20 25
Assurance scoring How much Full 3 Partial 2 Minimal 1 Basis External Verification 3 Internal Verification 2 Self- Assessment 1 Timeliness Within last 3 months 3 3 and 9 months 2 9+ months 1 Rigour Strong 3 Moderate 2 Weak 1
Score Level of assurance
0 – 5 Weak – very limited reliance
6 - 8 Moderate – limited reliance
9 - 12 Strong – strongly relied upon

1
Board of Directors Corporate and Directors Risk Register Generated on: 17 May 2018 Risk Score 25 Title Description Control Risk Score Current Risk
Matrix Action Title
Incident Stacking (A&E) Stacking of Cat 2, Cat 3 and 4 calls due to the availability of resources and/or high demand could affect patient safety, patient experience, staff morale and performance.
Robust plans in place to reach Clinical establishment in the Hubs 25
Single Escalation Framework document to be produced (combining the previous Demand Management Plan and REAP document)
A suite of SOPs in place - including the Welfare SOP - to manage patients in the call queue
Development of Achieving National Standards Through Investment and Transformation (ANITA)
Clinical Supervisors' constant review of the call queue
Development of Performance Improvement Plan (PIP)
Demand Management Plan in place Hub Clinician recruitment plan implemented and in progress
Ongoing review and monitoring of resourcing within the Clinical Hubs
Risks Scoring 20 Title Description Control Risk Score Current Risk
Matrix Action Title

2
Title Description Control Risk Score Current Risk Matrix
Action Title
Reputation Potential for adverse reputation which could lead to a loss of confidence by patients, commissioners, stakeholders and staff.
Communications and Engagement Plan 20
Annual Review of Stakeholder Activity
Ongoing liaison with National Ambulance Communications Group (NACOM)
Review and update Communications and Engagement Plan
ARP Performance Targets The potential for not achieving and sustaining ARP performance targets which could impact on patient safety, patient experience, staff experience, the Trust's reputation and financial position and the Single Oversight Framework.
ORH Modelling Dataset
20
Assurance piece led by the Deputy Chief Executive/Executive Director of Finance
Extended Delay Review Process Demand Management Plan to be reviewed
Performance Assurance Meeting (PAM)
Development of Performance Improvement Plan (PIP)
ORH Remodelling
Service Change and the impact on the Ambulance Service
Changes to Health Services (as a result of service change arising from a change in location of services, a change in the journey time, a change in the volume of incidents or other activity, changes in patient pathways etc.) will impact on the Trust including the availability of resources to respond safely, patient journey times (affecting patient safety and experience), staff experience, performance and finances.
Ongoing communications with Commissioners regarding service changes 20
Clinical Directorate to continue to monitor service change using their methodology for estimating and assessing the impact of service change
Principles of service change agreed Continue communications with Commissioners regarding service changes
Methodology developed for estimating and assessing the impact of service change
Continue to attend and feed into the Strategic Partnership Board
External Impact on Finance Strategy
Legislative, contractual or regulatory changes made by government bodies that impact on the Finance Strategy of the Trust.
Contract in place with Commissioners
20
Establishment of risk specific teams
Support from NHS Improvement who also set the tariff inflation within contracts to consider the impact of elements such as the national set pay
Ongoing liaison with NHS Improvement and other professional advisors where necessary

3
Title Description Control Risk Score Current Risk Matrix
Action Title
award Finance, and where necessary professional advisors, review financial decisions by external organisations
Ongoing monitoring of risk
Procurement contracts based on multi-year agreements where possible
Review procurement contracts and the financial impact of inflation by the finance team
Internal Employment Law expertise Commissioner Affordability The ability of the Trust to
mitigate the gap in funding within the contracts as part of contract negotiations
Trust Financial Plan including Cost Improvement Plan approved by Trust Board of Directors 20
A&E modelling of resource, performance and demand profiling being undertaken
Operational modelling undertaken by ORH
Implementation of Trust Operating Plan 2018/19
Contract in place with Commissioners Participation in STP process
Strategic Partnership Board with Commissioners and Finance and Information Group established
Major IT Service Failure A Major ICT service failure, which cannot be redressed via the Trust hardware/software maintenance contracts or a Cyber Security issue which has the potential to impact on the Clinical hubs, Telephony and/or Radio or Mobile data may lead to a potential business continuity risk (including access to resources) in A&E, UCS or support services.
Third party maintenance contracts are in place for Gold / Platinum assets i.e. Cisco Maintenance 20
Decommission of old domains/migration to the SWAST domain, is ongoing
Gold ICT systems such as Air Wave, CAD, etc.
Deployment of various monitoring/alerting tools - Cisco Prime, Meraki, SolarWinds
Generators and Uninterrupted Power Systems (UPS) systems
Standardisation of remote access solutions and deployment of a new secure portal
Business Continuity Plans Work plans to keep all Gold systems up to date
"One Domain" project
999 Clinical Call Audit Compliance
Failure to meet 999 clinical call audit compliance which could compromise patient safety and the requirements of the licence.
Extended A&E Clinical Audit with increase in Clinical Team Leader staffing levels (increased time allocated to Clinical Audit and increased use of Peer Audit
20
Focused efforts on Clinician recruitment

4
Title Description Control Risk Score Current Risk Matrix
Action Title
Audits undertaken for all A&E Hub complaints and serious incidents to ensure that any performance issues are identified
Introduce a 999 Audit Policy
All A&E Hub audits feedback to staff in a timely manner
Introduce Levelling for Clinical Auditors
Under performing staff within A&E Hub have personal action plans devised with associated closer monitoring
Implement new MPDS Governance Framework
Risk assessment updated with associated actions
Options paper to be produced during Q1 which sets out issues around call auditing
Overtime offered to auditors and members of audit pool in A&E hub to increase number of A&E audits undertaken
Produce an Improvement Plan Options Paper
Produce an improvement trajectory with timescales
Risks Scoring 16 Title Description Control Risk Score Current Risk
Matrix Action Title

5
Title Description Control Risk Score Current Risk Matrix
Action Title
Inability to Answer 999 Calls
Inability to Answer 999 (Emergency and Health Care Professional) Calls can lead to patients waiting, potentially affecting their safety
Demand Management Plan in place
16
Ongoing recruitment campaign to reach and then maintain 999 Call Taker establishment
Monthly formal establishment review meetings held between the Executive Director of Operations, the Head of Operations - Clinical Hubs and HR which include a 12 month forward view
Demand Management Plan to be reviewed
Call Answering Action Plan in place 999 Non-Clinical Call Audit Compliance
Failure to meet non-clinical call audit compliance in 999 could compromise patient safety and the requirements of the licence.
Audits undertaken for all A&E Hub complaints and serious incidents to ensure that any performance issues are identified
16
Auditors to attend the Academy’s Navigator Conference
All A&E Hub audits feedback to staff in a timely manner, where possible during the staff member’s next working shift
Auditors to work in both Clinical Hubs to build working relationships and consistency
Under performing staff within A&E Hub have personal action plans devised with associated closer monitoring
Identify additional funding to staff the non-clinical audit team
Risk assessment updated with associated actions
Introduce a Trust-wide Audit Policy
Implement new MPDS Governance Framework
Options paper to be produced during Q1 which sets out issues around call auditing
Overtime offered to auditors and members of audit pool in A&E hub to increase number of A&E audits undertaken
Recruit to Clinical Team Leader vacancies within A&E Hub which will increase supervision of EMAs

6
Title Description Control Risk Score Current Risk Matrix
Action Title
Review Non-Clinical Call Audit Compliance Risk Assessment
Schedule bi-monthly Levelling Meetings
Investigation Delays Delays in investigation of complaints, serious, moderate and adverse incidents, claims and inquests could result in poor patient and staff experience and breaches of regulations, national and contractual requirements.
Quality Leads in place and trained
16
Implementation of organisational change process relating to Quality structure
Investigation training delivered to Operational and Investigation Officers
Provision of further training to OOs
Investigation Guide updated and circulated
KPI Individual Scorecard Complaints Policy
Submission of Safeguarding Referrals via EPCR
The potential for safeguarding referrals not to be received by the Safeguarding Team via EPCR as a result of: staff not emailing the referral; network connections preventing emails from being transmitted.
Weekly monitoring of referral process and weekly call with Executive Director of Nursing and Quality to review weekly position and any potential risks
16
Continue daily cross checking exercise
Senior Safeguarding Support undertakes daily cross checking exercise with Clinical Records team
EPCR safeguarding referral form to be re-designed and implemented to remove email facility.
Procedure for emailing referrals cascaded to staff via the LDOs and OOs
Further updates to EPCR required
Head of Safeguarding provided additional guidance to staff regarding how to submit quality referrals
Reinforce correct email process through Safeguarding training
Head of Safeguarding to continue to meet with EPCR project lead
Reminders issued to advise staff to notify Safeguarding service if confirmation email not received
Impact of REAP Levels, and Summer, Winter and
Increased REAP levels as a result of under-performance
Escalatory Process in place (REAP)
16
Development of strategic winter plan (complete)

7
Title Description Control Risk Score Current Risk Matrix
Action Title
Peak pressures against national performance indicators leading to; •over activity against contract ; •slippage to training programme deliveries and other work streams, including cancellation of priority meetings dependent on REAP levels, winter pressures and weather; •increased demand on thre core services; •impact on delivery of business plans; •impact on resilience within the Trust.
Performance management arrangements in place
Meeting with all A&E Delivery Boards to establish working arrangements and escalation plans
Winter and Escalation Steering Group established
Monthly meetings of Winter & Escalation Steering Group
REAP and Demand Management Plans in place
Ongoing discussions with Commissioners at IQPMG meetings to review activity and demand profile in each CCG area and agree actions to mitigate increase in demand including the review of alternative pathways
Daily conference calls Review of escalation arrangements (Escalation Framework)
Changes in Activity Changes in daily and hourly spread call volumes and incident numbers has the potential to impacting on the Trust's ability to respond with potential consequences for patient care and experience, performance and staff experience. This relates to both hub and frontline operations.
Demand Management Plan in place
16
A set of rotas which can be flexed for known periods (e.g. winter, Easter) are to be developed to move the Trust' resourcing to a more sensitive approach based on activity during the year
Rotas flexed for known busy periods Demand Management Plan to be reviewed
Development of Performance Improvement Plan (PIP)
Locating Patients Gazetteer updates not taking place in a timely manner could result in resources being dispatched to an incorrect location.
Map books available on vehicles
16
Audit electronic sat Nav maps on all vehicles
Address Base Premium replaced Address Base
Planning to start to migrate to the latest version of NGIS mapping
200 Thorcom units purchased Review process and resources required for database
TerraFix is up to date

8
Title Description Control Risk Score Current Risk Matrix
Action Title
C3 Patch has brought the gazetteer up to date
C3 Map Tile Updates Restraint Application of restraint by
ambulance staff which has the potential to result in patient harm and/or harm to staff.
Mental Health Guideline available to support staff in understanding of mental health and mental capacity 16
Consideration of the provision of mental health support with the placement of mental health professionals in the Clinical Hub
Restraint Policy available which clearly sets when restraint can and cannot be applied
Provide greater support to staff through education (included in TNA)
De-escalation techniques taught during conflict resolution training
Restraint training included within 2018-19 Development Day Proposal - awaiting confirmation from Directors that this proposal has been agreed and funding appropriately identified
Further guidance available on Mental health page of Intranet
Work with regional and national Police partners to develop agreed response to requests for support at incidents requiring restraint. Regional protocol completed
Staff advised to seek police support in provision of restraint when appropriate
Application of chemical restraint restricted to those staff trained in application and specifically authorized by Executive Medical Director
Mental health conveyance review completed
De-escalation techniques taught during conflict resolution training
Infection Control Compliance
Risk of not being compliant with Hygiene Code,
Comprehensive Infection Prevention and Control Policy in place 16
IPC update to be provided to all frontline staff during the 2018-19

9
Title Description Control Risk Score Current Risk Matrix
Action Title
including compliance with Level 1 and 2 training requirements.
development day
Annual Infection Prevention and Control Action Plan
LDR reporting development underway with co-operation of education department
Mandatory Training Workbook for staff Management of Controlled and Non Controlled Medicines
Potential breach of legislation in relation to the management of controlled drugs and medicines in relation to: •mandatory requisitions; • issue and returns; and •inconsistent application of medicines management systems and processes.
Medicines Management Policy implemented throughout the Trust 16
All localities to be required to implement new medicines system without modifications
Full time dedicated Pharmaceutical Advisor/Responsible Officer for Controlled Drugs
Consideration of development of ECS solution to support electronic medicines management through the Digital Strategy - to implement if approved
Storage of controlled drugs standardised to restrict access to staff without authority to possess
Roll out of system to specialist units to bring all staff into the same system
Medicines Governance Group monitors implementation of policy by reviewing Adverse Incident reports, progress reports and audit reports
Update process for medicines management audits at stations to enhance robustness
Implementation of Medicines Management module for Adastra to provide electronic support in UCS
New drug bags issued to all staff to ensure that only registered clinicians can access LSCDs and CDs
Drugs held in a secure cabinet with robust process for access control
Annual station inspection programme implemented to provide assurance that all locations are fully compliant with medicines management

10
Title Description Control Risk Score Current Risk Matrix
Action Title
111 Resourcing and Performance
The potential inability to meet 111 performance as a result of demand and/or resource issues could result in • A failure to meet performance national standards for call answering (95% within 60 seconds); • Increased numbers of calls being abandoned and extended waiting times for a clinical call back; • Increased 111 call transfers to 999 or Emergency Departments.
Recruitment plan in place to reach and maintain NHS 111 establishment 16
Demand Management Plan to be reviewed
Staffing modelling completed and plan in place to ensure that staff in the floor matches the modelling
Ongoing recruitment plan to recruit to and maintain NHS 111 establishment.
Escalation process and Demand Management Plan in place
Call Back SOP in place to manage volume and safety
OOH Resourcing and Performance
The inability to meet OOH performance could result in: • The failure to achieve the contractual KPIs for Home Visiting and Treatment Centre (base) consultations; • A delay in calling a patient could impact on the quality of the service offered, patient safety and experience, staff morale and reputation. This is exacerbated by the difficulty in recruiting GPs.
Meetings held with UCS clinicians and Clinical Working Group Plan in place; 16
Advanced Nurse Practitioner development and recruitment programme;
Comfort Calling SOP in place; Agency staff recruitment in accordance with procurement guidelines;
Risk assessment of clinical staffing; Clinical Working Groups in place; Local Consultative Committee held monthly for UCS service line;
Continue use of UCS Specialist Paramedics;
111 Clinical Cover close to establishment levels;
Continued engagement with staff to understand the risks and concerns;
Clinical Team Leaders (CTLs) manage the clinical queue during periods of high demand, ensuring that cases are prioritised in clinical order;
Further GP engagement - additional recruitment taking place and regular meetings are being held with GPs;
Delays on the clinical queue are escalated through the Trust’s normal Escalation processes to Operational and Tactical commanders to agree appropriate mitigation to secure the
Implementation of incentivised shifts where appropriate;

11
Title Description Control Risk Score Current Risk Matrix
Action Title
safety of patients; Centralisation of the Resource Operations Centre (ROC) and GRS implemented across Trust;
Improve joint working with District Nurses;
Workforce plan; Recruitment continues for all clinical groups;
Recruitment Plan in place; Rota review pending. GP Lead and Nurse Leads in place; UCS Business meeting with Terms of Reference to include monitoring of targets;
Rota review pending; New senior Management structure in place;
Business Continuity Plan in place; Out of Hours Triage Delay Risk Assessment re-reviewed at QRAG in September 2017.

12
Risks Scoring 15 Title Description Control Risk Score Current Risk
Matrix Action Title
Financial Position (Operations Directorate)
Potential adverse financial variances the A&E Service line impacting on the overall financial position of the Trust. Possible variance due to commissioner affordability, increased cost pressures, ability to identify recurrent cost improvements and increases in demand
Budget arrangements in place
15
Budget setting
Dedicated management accountants Financial Modelling
Escalation Process in place (Financial) Identification of CIP schemes
Ongoing contract negotiations with Commissioners
Pollution Regulation Compliance
Potential breach of Pollution regulations which could affect public health, Trust reputation and financials.
Oil tanks and equipment regularly inspected and maintained by approved contractor 15
All staff to receive training/guidance on spill response
Spill kits on site Develop programme to review and potentially replace aging underground storage tanks
Annual leakage test of fuel tanks below ground
Drainage survey to be undertaken at all sites
Waste Management Policy in place Site specific risk assessments to be carried out and communicated on each site containing fuel and oil storage
Pollution action plan Tender exercise including regular maintenance and servicing plan for interceptors
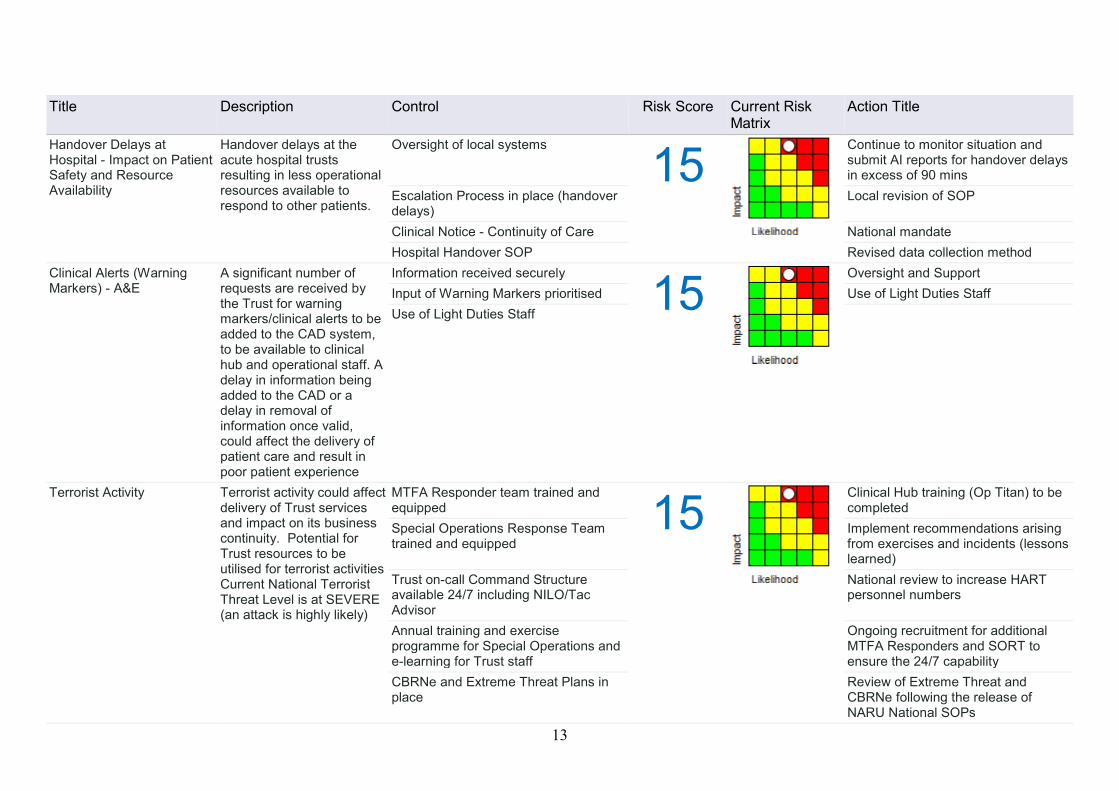
13
Title Description Control Risk Score Current Risk Matrix
Action Title
Handover Delays at Hospital - Impact on Patient Safety and Resource Availability
Handover delays at the acute hospital trusts resulting in less operational resources available to respond to other patients.
Oversight of local systems
15
Continue to monitor situation and submit AI reports for handover delays in excess of 90 mins
Escalation Process in place (handover delays)
Local revision of SOP
Clinical Notice - Continuity of Care National mandate
Hospital Handover SOP Revised data collection method
Clinical Alerts (Warning Markers) - A&E
A significant number of requests are received by the Trust for warning markers/clinical alerts to be added to the CAD system, to be available to clinical hub and operational staff. A delay in information being added to the CAD or a delay in removal of information once valid, could affect the delivery of patient care and result in poor patient experience
Information received securely
15
Oversight and Support Input of Warning Markers prioritised Use of Light Duties Staff Use of Light Duties Staff
Terrorist Activity Terrorist activity could affect delivery of Trust services and impact on its business continuity. Potential for Trust resources to be utilised for terrorist activities Current National Terrorist Threat Level is at SEVERE (an attack is highly likely)
MTFA Responder team trained and equipped 15
Clinical Hub training (Op Titan) to be completed
Special Operations Response Team trained and equipped
Implement recommendations arising from exercises and incidents (lessons learned)
Trust on-call Command Structure available 24/7 including NILO/Tac Advisor
National review to increase HART personnel numbers
Annual training and exercise programme for Special Operations and e-learning for Trust staff
Ongoing recruitment for additional MTFA Responders and SORT to ensure the 24/7 capability
CBRNe and Extreme Threat Plans in place
Review of Extreme Threat and CBRNe following the release of NARU National SOPs

14
Title Description Control Risk Score Current Risk Matrix
Action Title
Impact of STPs and other National change programs
Potential organisational changes in the Trust area such as STP, Devolution and other national programmes. Impact maybe financial, resources or corporate operations of the organisation. (Risk replaces devolution and changing commissioner arrangements risks)
Engagement with STPs
15
A&E modelling of resource and demand undertaken
CQUIN work programme Risk assessment to be completed
Ongoing engagement with Clinical Commissioning Groups
Review of Carter implications
Representation at Contract meetings Single A&E Contract 2 year Financial Framework agreed Trust has good working relationship with CSU
Engagement with Ambulance Improvement Program
Map of service changes presented to Board of Directors
Cost Improvement Strategy Non achievement of the 5 year cost improvement strategy targets could result in:- • lack of investment in service infrastructure; • a trigger of downside scenarios; • compromised delivery of national targets; • non delivery of Financial Plan.
Strict controls on costs and monitoring of budgets 15
Delivery of enabling strategies
Downside scenario planning identified Implementation of A&E Operating Plan
Governance framework in place Implementation of MEAP or CEAP
Finance Committee monitor CIS at each meeting
Monitoring of implementation plans
Implementation plans developed with clear accountability identified and implemented
Monthly monitoring against NHSI Operational Plan
Recognition Agreement in place and ongoing dialogue with Staffside
Review of Carter implications
Workforce Planning aligned to CIS programmes
Undertake review of operational remodelling
Quality Impact Assessments to be signed off for each CIP
Cost Improvement Strategy

15
Title Description Control Risk Score Current Risk Matrix
Action Title
Operational Resources (A&E)
Not enough operational resources available (core and other) to meet demand.
Centralisation of ROC and GRS
15
Implementation of robust recruitment plan
Workforce Plan ORH Remodelling
Provision of staff by third parties, agencies, bank and overtime
Payment of incentivised shifts
Weekly RMG meetings Undertake Culture Review
Demand Management Plan Ongoing recruitment
C3 Split Brain - Assurance of resilience
Uncertainty around the effectiveness of the C3 Split Brain system as a result of the system not being tested which could affect business continuity arrangements of the CAD.
Solar Winds
15
Business continuity arrangements
Business continuity arrangements Business continuity exercise
Real time duplication on CAD database Review Working Practices, SOPs and training
Timely Complaint Response
Delays in acknowledging and responding to complaints from patients and relatives; and potential for limited learning opportunities as a result of: •An increase in the number of complaints being received impacting on the capacity of the Patient Experience team; •The time taken by Investigating Officers to investigate complaints.
Investigation training delivered to Operational and Investigation Officers 15
Heads of Operations to review time available to Operational Officers to investigate complaints
Complaints Policy Review Patient Experience team structure when appropriate, i.e. during recruitment for any vacancies
Multiskilled staff within Patient Experience team
Level 3 complaint actions monitored by Patient Experience team;
Complaints response trajectory

16
Risks Scoring 12 Title Description Control Risk Score Current Risk
Matrix Action Title
Frequent Caller Record Management
Should the Trust have an ineffective frequent caller record management process this would affect the Trust's duty to protect vulnerable adults resulting in a breach of safeguarding legislation.
Frequent Caller Policy and Process in place; 12
Procurement of a new Sequel Database
Standard Microsoft Product back-up; Communication and planning within team;
Administration support.
Provision of Welfare Calls within the 999 Clinical Hubs
Potential for inability to provide welfare call-backs for patients who are awaiting an operational response
Welfare Call SOP
12
Hub Demand Management Plan Review
Allocation of Welfare Calls Monitor Effectiveness of Welfare Call SOP
Exit Advice Reduce On Scene Times
Public Awareness Review of Clinical Supervisor Rota
Impact of IR35 The impact on the organisation’s resources, finances and service delivery in respect of the sessional GPs following the updated IR35 and employment status on line tool.
Proactive contact with GPs and LMCs
12
Continued engagement with GPs
Ongoing liaison with Commissioners Mitigation of associated cost pressures including negotiation with Commissioners;
Safe levels of staffing and rota identified for 999 clinical hub and Urgent Care Services;
Resourcing reviewed constantly by Operations Manager.
FAQs developed and published; Timely response to queries from GPs
New option for Bank Status for GPs agreed by Trust Board and contracts issued;
Dissemination of contracts including indemnity arrangements.
Business Continuity Plans
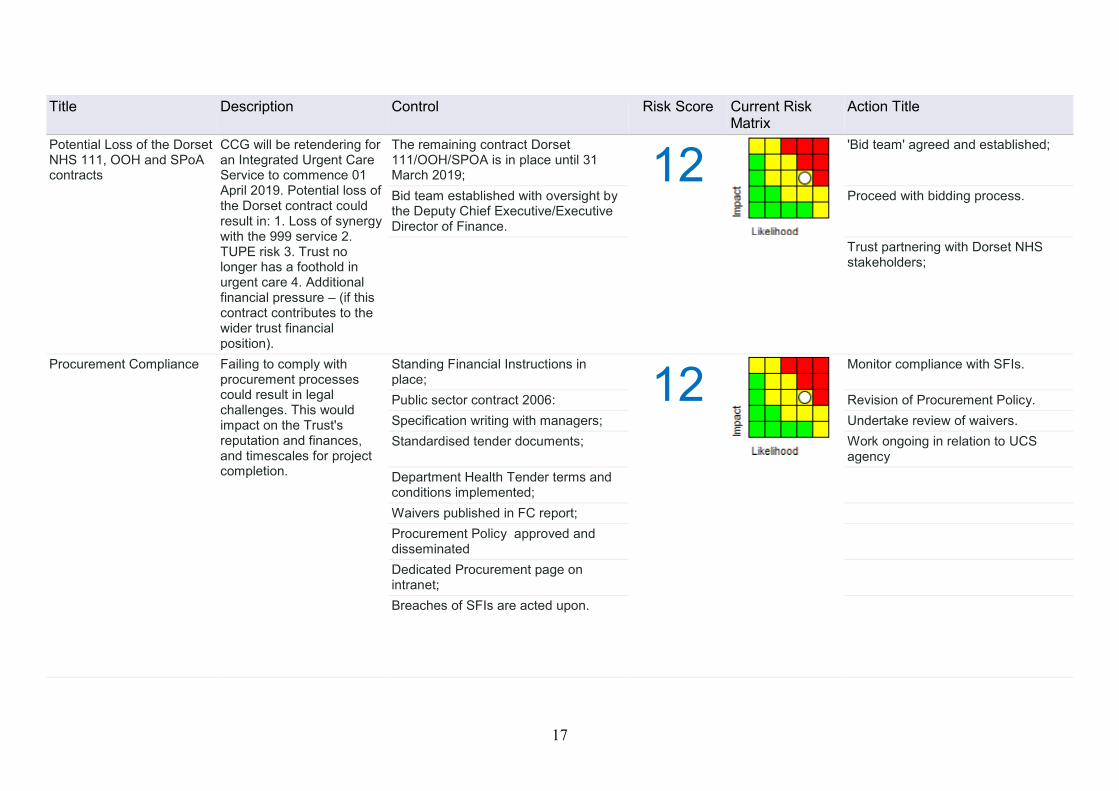
17
Title Description Control Risk Score Current Risk Matrix
Action Title
Potential Loss of the Dorset NHS 111, OOH and SPoA contracts
CCG will be retendering for an Integrated Urgent Care Service to commence 01 April 2019. Potential loss of the Dorset contract could result in: 1. Loss of synergy with the 999 service 2. TUPE risk 3. Trust no longer has a foothold in urgent care 4. Additional financial pressure – (if this contract contributes to the wider trust financial position).
The remaining contract Dorset 111/OOH/SPOA is in place until 31 March 2019; 12
'Bid team' agreed and established;
Bid team established with oversight by the Deputy Chief Executive/Executive Director of Finance.
Proceed with bidding process.
Trust partnering with Dorset NHS stakeholders;
Procurement Compliance Failing to comply with procurement processes could result in legal challenges. This would impact on the Trust's reputation and finances, and timescales for project completion.
Standing Financial Instructions in place; 12
Monitor compliance with SFIs.
Public sector contract 2006: Revision of Procurement Policy. Specification writing with managers; Undertake review of waivers. Standardised tender documents; Work ongoing in relation to UCS
agency
Department Health Tender terms and conditions implemented;
Waivers published in FC report; Procurement Policy approved and disseminated
Dedicated Procurement page on intranet;
Breaches of SFIs are acted upon.

18
Title Description Control Risk Score Current Risk Matrix
Action Title
Off Payroll Arrangements Procurement issues associated with legislation regarding Off Payment arrangements
Ongoing monitoring of agency and consultant spend 12
Decisions to authorise off payment arrangements only to be made by Executive Directors.
Review of implications of IR35 undertaken.
Robust governance register to be developed.
Service Line Development Project Creep
The potential for services to expand the scope and responsibilities which compromises the Trust Financial position. This may include the risk of change in banding within Agenda for change or undertaking additional work outside the original scope of contracts.
Use of tenders
12
Ongoing review of roles
Business cases reviewed by Directors group
Review of functions by Corporate Programmes Manager.
Financial issues included within project risk registers as appropriate.
Review of service models
Job Matching Review Process Service line management roles
Commissioning Managers in place Programme Boards for each Project
Information Governance and Security Requirements
Potential non-compliance with Information Governance and Information Security Requirements as a result of: the potential loss or theft of paperwork containing personal information; failure to follow appropriate technical solutions to protect personal/confidential information; information being out of date, incomplete, inaccurate or deleted; non-compliance with the process for completion and delivery of
Maintain Information Governance training and education programme 12
Changes to be made to Corporate marking scheme.
Clinical Records Management Policy sets out process for PCRs
Implement actions arising from Internal Audit review of Data Integrity
Corporate Records Management Policy Include issue within IG communications plan and consider the use of posters, aide memoires, etc.
Data flows mapped and risk assessed. IT Security Incident SOP to be produced.
Regular monitoring of adverse incidents.
Monitor implementation of revised Data Quality checking process and provide report to IASG;
SOP on Secure Transfers of Information available on IG Directorate page of the Intranet and promoted in the Bulletin;
Ongoing completion and submission of data quality checks;

19
Title Description Control Risk Score Current Risk Matrix
Action Title
records; increased information request workload within IG impacting on ability to deliver toolkit requirements; and withdrawal of current online IG training solution from 31/12/2016 with no confirmed date for replacement.
Monitoring the use of emails by IT and auto alert on any key words in emails sent insecurely;
Use of IM&T Services Policy; Information Security Plan; Data Quality Policy Information Assurance Steering Group; Monthly data quality checks completed and submitted to the Information Management team;
Data Quality Lead appointed Outcome of internal audit review was 'green' with no recommendations
ECS rolled out across Trust. Regional Care Plan Strategy
Lack of Regional Care Plan Strategy resulting in different approaches by individual CCGs and STPs to care records impacting on the ability to use different systems.
Care Record Working Group established; 12
Agree strategy;
Promotion of Summary Care Record; Communications underway with Local Area Team and CCGs;
Ongoing monitoring of Enhanced Summary Care Record;
Implement actions arising from Care Record Working Group;
National Information Board (NIB) assessment complete;
Joining Up Your Information (JUYI) Dorset Care Record;
Draft 5 year plan feeding into STPs. Monitor initiatives taking place across region, e.g. Connecting Care and Connecting Care Programmes;
Monitor STPs and local activity plans; Participate in IT local delivery plans. Reconcile IT local delivery plans with
Sustainability and Transformation Plans (STPs);

20
Title Description Control Risk Score Current Risk Matrix
Action Title
NHS Transition Network Transition from N3 Network to the N3 Transition Network with a potential to affect Trust finances from 2018/19 and unknown technical impact. Central funding to decrease to 75% in 2018/19 and 50% in 2019/20.
Regular meetings with NHS Digital and the BT / N3 team 12
Mitigate year on year funding reduction from NHS Digital.
Paper to Directors Group advising of issues;
Monitor situation, there is currently insufficient information available from NHS Digital to create and robust plans and/or Business case to seek additional funding to mitigate any potential issues;
NHS Mail Potential for limited options in relation to the choice of email system due to decision not yet being made. This could have financial and resource implications.
New Trust wide email system built on new SWAST domain; 12
Directors paper regarding strategic direction and choices being developed.
Trajectory in place to migrate email accounts to new domain;
Risk assessment to be reviewed;
Serious Incident Process Potential for non-compliance with the National Serious Incident Framework due to: •insufficient capacity within the Patient Safety team; •limited capacity/resilience for Quality Leads to investigate serious incidents; •Investigating Officers capacity; •an increase in the number of potential SIs being reviewed.
Quality Leads in place and trained
12
Implementation of revised Quality Lead structure
Serious and Moderate Harm Incident Policy which is informed by the updated National Framework
Ongoing utilisation of clinical staff on light duties to provide assistance within Patient Safety team;
Root Cause Analysis training for Investigating Officers. Further updates have been provided, most recently January 2018.
Regular communication regarding serious incidents and actions with CSU Patient Safety lead
Safeguarding Compliance Risk of potential for non-compliance with Safeguarding requirements: •an increase in the number
Extension to secondment of additional post within the Safeguarding team; 12
Business Case to be presented to the Executive Directors Group regarding the future structure of the Safeguarding team (complete).

21
Title Description Control Risk Score Current Risk Matrix
Action Title
of referrals and quality of referrals received affecting capacity and potentially patient safety, this may be a consequence of reporting via the EPCR and the additional training; •insufficient resources within the Safeguarding team to maintain the current high standard of reporting and management for all referrals,
Safeguarding referrals processed in accordance with RAG rating;
Further updates to EPCR required Urgently - Escalated to Director Group;
IT system in place involving an email being sent to staff advising that the referral has been submitted;
Head of Safeguarding provided additional guidance to staff regarding how to submit quality referrals;
Weekly monitoring of referral process and weekly call with Executive Director of Nursing and Quality to review weekly position and any potential risks;
Reminders issued to advise staff to notify Safeguarding service if confirmation email not received;
Risk assessment re-visited; Internal audit review completed.

22
Risks Scoring 10 Title Description Control Risk Score Current Risk
Matrix Action Title
Vehicle Security Lack of security of Trust vehicles could impact upon patient, public and staff safety, Trust performance and financials.
Vehicle locking arrangements in place
10
HSSM to continue to raise awareness of security issues and precautions as and when required
Vehicle tracking devices Resilience team to continue to raise awareness of security issues and precautions as and when required
Process for selling Trust vehicles Local Security Management Specialists in post
CCTV Management Process Patient Clinical Records Non completion of clinical
records by ambulance clinicians affecting continuity of care and the Trust's ability to evidence care provided. In addition, the ability to locate clinical records required by coroner, police, claimants, complainants could affect the ability of the Trust to defend a claim or provide information for investigations and could result in reputational and financial consequences.
Management of Clinical Records Policy; 10
Clinical Dashboard pilot - including consideration of the introduction of a non-record completion measurement (KPI etc.) to support clinical staff.
Clinical record review at station level; Data quality dashboard to provide a high level view of record keeping;
Record completion included within training programmes;
Development and dissemination of awareness and training materials;
HCPC registration process requires good record keeping;
Development of a tool to support OMs to identify and review cases where a record should be present but not available;
Centralised audit of record completion; Managers conduct timely audit of incidents where no record has been completed, results should be logged
Ongoing annual audit; Review Clinical Hub Stop Definitions; Access to ECS restricted to certain groups with robust procedures and policies in place to support access to clinical records and data;
Revised Management of Clinical Records Policy to be presented to the Quality Committee;
Regular system and process audits completed and shared with the information Governance Group as well as other departmental managers and staff;
TNA to be developed;
Centralised audit of record completion

23
Title Description Control Risk Score Current Risk Matrix
Action Title
Health and Safety - Strategic Oversight
Potential for a lack of Corporate Senior Management and Board Ownership of Health and Safety Risks and Responsibilities. .
Executive Director and Non-Executive Director with responsibility for health and safety 10
Additional IOSH Managing Training to be provided to 2nd cohort of managers
Health and Safety Strategy in place with associated policies
Peer review to be completed using the HSE Audit Form
Leading Safely Training Health and Safety Committee in place Bi Monthly Health and Safety Reports to Trust Board of Directors and People and Culture Committee cumulating in an Annual Report
Care Quality Commission Failure to achieve compliance with the requirements of the Care Quality Commission registration could result in a loss of reputation, and impact upon regulators interaction with the Trust
CQC Relationship meetings take place regularly; 10
Enhanced staff engagement by Chief Executive, Directors Group and Non-Executive Directors to gain staff feedback;
Internal Audit Report of Compliance with 4 CQC regulations each year, CQC Compliance is also considered when specific work streams are audited;
Project Plan formulated and is to be delivered to ensure preparedness for inspections.
Monitoring of Serious Incidents; Implementation of QIP; Direct staff engagement; Quality Improvement Plan progress
and exception reports to QPB, SLT, Quality Committee and Board;
Quality Improvement Plan monitored by Quality Programme Board
Quality Programme Board in place to give renewed focus and monitor preparation for inspections
Implementation of new CQC quarterly monitoring report
Quality Strategy CQC Leads from each Directorate appointed;
Quality Support Manager appointed Deputy Director of Nursing and Quality appointed.

24
Risk Scoring 9 Title Description Control Risk Score Current Risk
Matrix Action Title
Resilience - Business Continuity
The potential inability to respond to major service disruption because BCPs have not been tested to ensure effectiveness which could impact on continuity of service, patient safety and experience, and staff morale.
Business Continuity lead appointed and working with departments to develop plans 9
C3 Split Brain BC exercise to be undertaken.
Business Continuity monthly progress dashboard reviewed by Directors Group
Ensure representatives from all key functions attend Business Continuity Steering Groups;
Clinical Hub Duty Managers trained in new Fall Back arrangements
Exercise Waterwell to be undertaken in 999 Clinical Hubs
Implementation of SWASFT5 (business continuity awareness campaign)
Ongoing review of Business Continuity Plans and maturity;
Regular generator testing now takes place
Revision and formulation of planning against best practice guidance from the National Business Continuity Institute
All actions arising from internal audit report have been implemented;
Updated pocket action cards disseminated to Hub staff regarding fall back procedures;
Business Continuity Policy ICT BCP reviewed and integrated with departmental BCPs
Test Business Continuity Plans yearly against ISO 22301 Standard

Trust Public Board of Directors – Friday 25 May 2018 Page 1 of 1
Trust Public Board of Directors Date: Friday 25 May 2018
Paper Title: KPMG Well Led Governance Review Action Plan
Prepared by: Marty McAuley, Trust Secretary
Presented by: Marty McAuley, Trust Secretary
Action: Approval
Recommendation: The Trust Board of Directors is asked to note the progress with the delivery of the action plan and close the actions presented as complete.
Executive Summary:
The Trust Board of Directors commissioned a well-led governance review. An action plan has been developed to respond to the five medium and six low level recommendations contained within the report. It was agreed that the Trust Board of Directors will monitor progress against the plan and it will be reported at each meeting until the Board is satisfied that all actions have been completed and the plan can be closed. At the Board meeting in March 2018 the Board approved that four actions had been completed and were formally closed. Action 1 - Split of agenda between public and private session at Board
meetings Action 5 – Freedom to Speak Up Guardian Action 8 - Board Action 10 - Meeting management
The Board of Directors are asked to close the following three actions having taken assurance that they have been completed: Action 2 - Forward looking performance and risk information Action 3 - Formalization of station visit feedback to Board/committees Action 6 - Staff survey responses The following four actions remain in progress, an update has been given for assurance: Action 4 - Developing and articulating strategic priorities Action 7 – Board development programme Action 9 – Improving the diversity of the Board and Governors Action 11 – Risk Management A further update will be provided to the Board of Directors in July 2018.

No. Risk Recommendation Management response Lead Deadline Comments
1 M
Split of agenda between public and private session at Board
meeting
We noted certain items within the private session of the Board
that arguably could have been included within the public
session e.g. finance overview, serious incidents report. With a
continued focus on increased transparency, the Board should
challenge the private agenda at the end of each meeting to
ensure all items that are not commercial or otherwise sensitive
should in future be included within the public domain.
A new agenda item to be added to confidential board
agenda titled - transparency of paper review. This will
give the Board the opportunity to discuss any papers that
could have been held in the public session.
Confidential Board agendas will also have their coversheet
amended so that reports that are sent to the confidential
board will have the justification for it as part of the report.
Trust Secretary will also undertake a review as part of the
Board cycle of Business preparation, which will see the
draft 2018/19 Board cycle of business presented for
approval at the January 2018 Board.
Finance Committee assurance report already moved to
public domain.
Marty
McAuley
Trust
Secretary
31-Mar-18
New agenda item added to each Confidential Board agenda -
transparency review to challenge the information received in the
confidential session.
For 2018-19 the Corporate Committee templates have been updated
and the justification for why the paper is being taken in the
confidential session has been added.
Review of the cycle of business has been conducted and changes have
been made to the cycle of business.
Finance committee now reports in public and confidential session.
ACTION COMPLETE
2 M
Forward looking performance and risk information
We noted that the performance reporting was predominantly
backward looking and whilst it included comparisons to other
ambulance trusts, it did not show any future expected
trajectories. This makes it hard to understand Board
expectations on what the accepted Trust target level of
performance is (rather than just the National target), the
actions being taken, and the expected length of time for
performance to revert to target.
We recommend that forward trajectories for quarter and year
end performance are included within the performance
reporting pack, and will share examples where relevant. In
addition the Trust should align its performance report with its
strategy to enable better monitoring of achievement against
strategic goals.
Some items have already been updated such as in the
ICPR information pack we now have an establishment
forward look. This has been in place since November
2017.
The Performance Manager will undertake a review of the
ICPR and see where further opportunities to offer a
trajectory exists. If any changes are to be made they will
be incorporated into the current month where possible
but all changes will be added to the ICPR for April 2018
which will be produced in May 2018. The ICPR is received
by the Board each month.
The Executive Director lead for each Committee, the Chair
of each Committee and the Trust Secretary will proactively
review each agenda to ensure that they are forward
looking.
Paul Quick
Performance
Manager
31-May-18
Establishment forecasts are now embedded within the ICPR report
and updated on a monthly basis.
A&E Contract activity levels for 2018/19 have been profiled based on
historic activity patterns and therefore reflect a monthly activity
forecast for the A&E Service for 2018/19. These forecasts are built at
CCG level and therefore enable granular analysis for activity variances
where these are identified.
Financial forecast positions continue to be included in the ICPR with a
forecast year end position for the key metrics.
The Trust will continue to review and consider where other
opportunities exist and will undertake an annual review of the ICPR.
ACTION PROPOSED AS COMPLETE

No. Risk Recommendation Management response Lead Deadline Comments
3 L
Formalisation of station visit feedback to Board/committees
Positively each NED is allocated a geographical location within
the Trust and as per the role requirements set out in the New
Ways of Working document is expected to undertake regular
visits to stations and hubs. Such visits are an invaluable way of
gaining insight into frontline services and to triangulate
evidence presented in reports to board and committee
meetings. They can also be used to escalate issues of concern.
NEDs have commented that they find the visits helpful, but the
current feedback mechanism from visits is informal and
inconsistent. The Trust may be missing opportunities to use the
feedback to take actions or ensure continuous improvement.
The Trust should develop a formal mechanism to record
outcomes or issues from a station visit and to ensure these are
reported and actions taken. This could be adapted from existing
good practice such as the NHS 15 Steps Challenge framework
used for ward walk-arounds which provides a toolkit and an
aide memoire to inform visits.
A board to floor type approach will be developed for the
NEDs with an agreed governance framework for its
completion. This will see a mixture of formal and informal
station visits. The framework will be developed from the
NHS 15 steps challenge.
Sign off of the framework will be at the Quality Committee
on 14 February 2017 and will be monitored by the Trust
Secretary with accountability through the Trust Chairman
via the NED appraisals.
Feedback from station visits will be fed back to the Board
through Board Seminar on a standing agenda item and
the New Ways of Working version 5 will incorporate these
changes.
Marty
McAuley
Trust
Secretary
14-Feb-18
Based on NHS England guidance the 15 steps, the Trust has developed
two new proformas - (1) Board Member Station Visits and (2) Board
Member Third Manning Observation and Reflection Forms.
The forms have been reviewed and approved by the Qulaity
Committee on 23 April 2018. They have been issued to the Board
Memnbers for use at all station viisits and observation sessions
undertaken.
Station visit feedback has been added to all Board Seminar agendas
and Board Seminars have been reformatted to enable a greater
number of station visits to be undertaken.
New ways of working version 5 has incorporated the revised approach
to station visits and rthe recording of feedback.
ACTION PROPOSED AS COMPLETE
4 M
Developing and articulating strategic priorities
The Trust should develop an engagement plan that:
•Helps commissioners and other external stakeholders
understand the likely implications of the ARP and what this
means for future service performance management;
•Involves commissioners and other stakeholders in dialogue
about the Trust’s overall ambition and its developing strategic
plan;
•Clarifies roles and responsibilities of executive and non-
executive board members in engaging with key stakeholders
including prioritising and allocating key partner contacts to
relevant board members.
The Trust is in the process of refreshing its strategy with
Board approval planned for March 2018. As a result of
the new strategy, a new Trust wide Communications and
Engagement Strategy will be developed. This will cover
the roll out of ARP, Commissioner engagement around
our strategic intentions and our public engagement
programme on our strategy. This will be approved in May
2018 at the Trust Public Board of Directors.
The board role in stakeholder engagement will also
feature in the refreshed communication and engagement
strategy but will also form part of the new ways of
working version 5.
Claire Warner
Head of
Comms
31-May-18
Comprehensive communication and engagement plans are developed
to support all strategic corporate projects, such as ARP.
Delivery of the engagement plan to support the new Trust Strategy is
nearing completion (see attached).
Following approval of the Trust Strategy 2018-2021, a new Trust
Communication and Engagement Strategy is in development and will
consolidate the engagement work of several directorates and
encompass engagement with all audiences, from patients and the
public to commissioners and key stakeholders.
This will include the Board’s role in
stakeholder engagement. A final draft will be available for review and
comment by 31 May 2018.
ACTION IN PROGRESS

No. Risk Recommendation Management response Lead Deadline Comments
5 L
Freedom to Speak Up (FTSU) guardian
The Trust’s Freedom to Speak Up (FTSU) guardian is currently a
NED with a medical background. We interviewed the FTSU
guardian and discussed the role and how it works. The post
holder has had several contacts and is currently following up on
some issues, which can be quite operational.
Best practice suggests that the FTSU guardian works best when
the role is undertaken by an employee with operational
experience. The Trust should consider how its current model fits
with the role of the NED and what other support such as
Champions could be implemented to strengthen the role and
promote openness and transparency across the Trust.
The FTSU Guardian, Venessa James, Deputy Director of HR
Clare Melbourne and Trust Secretary Marty McAuley are
to meet and develop a guardian arrangement that:
* Builds on Venessa's recommendations from November
2017 board report
* Strengthens the existing good practice in the Trust and
aligns to national direction of travel
* Reflects the significant assurance from recent internal
audit report and its recommendations
* Venessa is an ambassador and not a single Guardian.
Approval for this will be through the Trust Public Board of
Directors on 29 March 2018.
Marty
McAuley
Trust
Secretary
Clare
Melbourne
Deputy
Director of HR
and OD
31-Mar-18
FTSU Guardian arrangements have been discussed by the Board at
Seminar in February 2018. The arrangements have been strengthened
and the revised model was presented and approved in March 2018.
Trust Secretary appointed as Freedom to Speak Up Guardian, Venessa
James is the NED Lead, HR support and the Peer Support Network will
also act as Guardians. This scheme is also being rolled out further.
ACTION COMPLETE
6 L
Staff survey responses
The Trust’s most recent annual staff surveying 2016 showed a
number of improvements over the previous year.
Commissioners praised the Trust on the results of its staff
survey and the Trust's staff engagement score at 3.57 (out of 5)
was above average compared to similar trusts.
Despite a positive set of results when compared to other
ambulance trusts, results in absolute terms were low. For
example, only a third of staff views were represented by the
survey. One of the most improved areas from the previous
survey was the action taken by the Trust to ensure well-being.
While this is to be congratulated, only 35% of respondents
agreed and only 29% said their manager involved them in
important decisions.
Though comparison with other trusts provides context, the
Trust should be ambitious to significantly improve results in the
future, particularly in the poorest performing departments such
as the Hubs.
The Trust encourages all staff to respond and has seen an
increase in the most recent survey in its response (up on
the last two years) but accept this is still only 41% of our
total workforce. In order to support completion of the
staff survey this year, regular bulletin updates were
provided as well as the incentive of being entered into a
draw to win one of three i-pads.
We do have challenges in relation to our geography and
the nature of roles within the service which mean staff are
less able to access the survey while on shift, however this
year we were able to ensure the survey was accessible via
the e-PCR allowing crews the opportunity to complete the
survey even while working remotely.
Each year results are analysed and the HR team work with
managers to develop action plans to support key areas
including the least favourable results as well as
encouraging and supporting best practice that has been
highlighted through the survey. We will be able to
evaluate the success of these measures in March 2018
when the results of the survey are known.
Clare
Melbourne
Deputy
Director of HR
and OD
31-May-18
The Board received the findings from the Staff Survey in March 2018
and further analysis in Seminar in April 2018.
The Council of Governors also received a presentation from the
Executive Director of People and Culture in April 2018 on the staff
survey, its results and our learning.
ACTION PROPOSED AS COMPLETE

No. Risk Recommendation Management response Lead Deadline Comments
7 M
Board Development Programme
The Trust does not have a formal or published Board
Development Plan in place.
The Trust Board has a number of new NEDs and EDs, so the
development of a formal programme to identify and then
programme in relevant development activities would be helpful
to ensure effectiveness of board operations.
The Trust will create a Board Development Plan for
2018/19. This will include all of the activities that the
Trust currently undertakes but is not captured in a single
plan, as well as new initiatives. It will build on the
foundations set by the Trust Chairman in the New Ways of
Working document.
The Board development Plan will be led by the Trust
Chairman but jointly owned with the Chief Executive, with
support from the Trust Secretary. It will be approved by
the whole Board in March 2018.
The Plan will incorporate the development seminars,
appraisal schemes, training and development
opportunities, mandatory training as well as the work
currently being scoped by the Chairman and Chief
Executive regarding 360 degree feedback and support
available from external company to facilitate the board
development opportunities.
Marty
McAuley
Trust
Secretary
31-Mar-18
Further work is needed to support the Board Development
Programme.
An in house diagnostic tool is being developed led by the Executive
Director of People and Culture and supported by the Trust Secretary.
External support for the development and facilitation is being
considered with the NHS Leadership Academy involvement being
explored.
Further development opportunities have been identified and will be
incorporated into the development plan - this will include the use of
Board Seminar time.
ACTION IN PROGRESS
8 L
Board
Although the Board was well chaired and good challenge was
observed, the Trust has scope to improve governance further
through:
•Avoiding duplication through expecting assurance at Board for
detailed papers that have already received assurance at a sub-
committee. For example QIP, patient experience, and patient
safety had already received assurance at a previous Quality
Committee
•Increasing transparency by including more items, such as
financial reports in the public part of the Board.
Duplication is minimal except where there are key
statutory duties such as Health and Safety.
Sometimes a Committee will receive a detailed report in
Committee and a highlight report or assurance will go to
full Board.
The Trust Secretary will review any areas of potential
duplication when the cycles of business for 2018/19 are
created and approved.
Marty
McAuley
Trust
Secretary
31-Mar-18
All Committee and Board papers have been reviewed and there is no
duplication. Statutory duties are sometimes dual reported to a Board
and a Committee but the focus of the information is different.
ACTION COMPLETE

No. Risk Recommendation Management response Lead Deadline Comments
9 L
Improving diversity of the Board and Governors
There is scope to improve diversity in terms of age profile of the
Trust’s Governors, which is skewed in favour of older
participants.
In order to better match the population that SWASFT covers the
Trust should develop opportunities for younger people to sit on
the Board or become governors. This could be done by linking
to other organisations in the region that have already
established ‘Young Ambassador’ or Youth Board type schemes,
or by offering ‘associate’ non-executive positions to younger
people to introduce them to the role of a NED.
The Trust Secretary will speak to Membership Managers
of local acute Trusts and see who has established Youth
Ambassador type roles. These Ambassadors can be
invited to SWASFT COG and SWASFT Board Meetings so
we can provide them with further experience whilst
learning how the roles could work for us.
Proposal for the establishment of the scheme and the
governance framework to be presented to the July 2018
Council of Governors and Board Meetings.
People and Workforce Committee will also look at where
there are opportunities to engage with our staff and
volunteers.
Marty
McAuley
Trust
Secretary
31-Jul-18
Proposal for the establishment of the scheme and the governance
framework to be presented to the July 2018 Council of Governors and
Board Meetings.
ACTION IN PROGRESS
10 L
Meeting management
The meetings we observed were generally well managed.
However, we identified a number of areas where this could be
further enhanced or strengthened.
Although the majority of meetings we observed ran to time, the
Trust does not include indicative timings on its agenda for each
item. It is good practice to set indicative times to guide
discussion and to ensure that issues of most importance are
afforded the most time on the agenda.
At two meetings we noted that the committee chair did not
take the opportunity to agree with the meeting items that
should be escalated to the board.
The Trust should ensure that:
•It provides indicative discussion times on each meeting agenda
item;
•Committee chairs clarify what action has been agreed for each
paper presented e.g. assurance, information, approval etc.
•Committee chairs should agree with meeting participants the
items requiring escalation to the board.
Indicative timings have been added to all Committee
agendas going forward, as it already is with the Board.
These are indicative and the Board will continue any
debate that has merit regardless of the time allocated.
Expectation on Committee Chairs to be re-iterated
through the appraisal process and the new ways of
working version 5 with regard to recapping when an
action is approved or assurance taken.
The agendas for all committee have been strengthened
already so each item has its purpose for presentation
noted.
Marty
McAuley
Trust
Secretary
31-Mar-18
Indicative timings have been added to all Committee agendas going
forward, as it already is with the Board.
Expectation on Committee Chairs has been built into the appraisal
process and the new ways of working version 5.
The agendas for all committee have been strengthened already so
each item has its purpose for presentation noted.
ACTION COMPLETE

No. Risk Recommendation Management response Lead Deadline Comments
11 M
Risk register
The Trust board regularly reviews its risk register and we can
evidence changes made as a result of that review. Many
aspects of the Risk register are in line with good practice. For
example we note that it is linked to strategic goals and has
forecast ratings post action.
However a target rating is not set for each risk, forecast ratings
are often set for long periods but not achieved and a number of
risks have remained on the register for a considerable time i.e.
since 2012. The use of the risk register as an effective
monitoring and reporting tool could be enhanced by:
•Including a target rating against each risk;
•Ensuring that forecast ratings are realistic, and are regularly
reviewed to ensure they remain realistic and relevant; and
•Reviewing longstanding risks to ensure that mitigating actions
or controls are having an impact.
The QRAG has already made a process change so that
whenever a risk is reviewed, a review date is captured and
not the date the risk was added to the risk register. If the
context of a risk changes it will be closed and reopened as
a new risk. Our previous process would see an
amendment hence some risks looking like they have been
on the system for years.
The Trust has procured a new risk platform which will be
launched in March 2018. Prior to its implementation the
QRAG are reviewing all risks that the Trust currently has
on its risk register and will be ensuring:
* All risks will have a target score
* Actions, controls and targets will be realistic and
relevant and regularly monitored through the QRAG
* Automated review triggers will be set to ensure that no
risk is left for a period of time without review .
Vanessa
Williams
Head of
Quality
30-Jun-18
The risk platform was presented to the Board of Directors in April
2018. Following feedback at the Board, a meeting is being arranged
with the Chair of the Audit and Assurance Committee to discuss the
content of future reports.
Work is ongoing with directorate leads to review individual risks,
controls and actions which includes a scoring mechanism to measure
effectiveness.
ACTION IN PROGRESS