true-ahf - cardiorentis · true-ahf investigating ularitide: the first prospective phase iii...
TRANSCRIPT

TRUE-AHFInvestigating ularitide:the first prospective Phase III mortality trial in acute heart failure
Study Chair: Milton Packer, MD
www.cardiorentis.com

TRUE-AHFTRial of Ularitide’s Efficacy and safety in patients with Acute Heart Failure
The TRUE-AHF trial is a phase III, multicenter, ran-domized, double-blind, placebo-controlled trial to evaluate the efficacy and safety of Ularitide (Urodi-
latin) intravenous infusion in addition to conventional therapy in patients suffering from acute decompensated heart failure in addition to conventional therapy.
* Investigational drug; limited by United States law to
investigational use only.
2
Study Status
The study is currently recruiting subjects in over 190 clinical sites in over 22 countries: Germany, France, Finland, Italy, Switzerland, Netherlands, Spain, Hungary, Poland, Czech Rep., Estonia, Turkey, Romania, Serbia, Latvia, Lithuania, USA, Canada, Colombia, Argentina, Chile, Brazil. Additional countries are currently being explored.
3
Study Overview
Primary Efficacy Endpoint; There are two co-primary end-points. Coprimary efficacy endpoint 1 evaluates changes in a hierarchical clinical composite comprising patient global assessment using a 7-point scale of symptomatic impro-vement, lack of improvement, or worsening; persistent or worsening heart failure (HF) requiring initiation or intensifi-cation of IV therapy, circulatory or ventilatory mechanical support, surgical intervention, ultrafi ltration, hemofi ltration or dialysis; and all-cause mortality. Assessment of the clini-cal composite will be performed at 6 hour (h), 24h and 48h after start of IV ularitide infusion. Patients will be classified as
“improved” if the patients are moderately or markedly im-proved at all 3 time points (at 6h, 24h and 48h) and do not fulfill criteria for “worse” during the first 48 hours following the start of the study drug infusion. Patients will be classified as “worse” if (during the 48h) they die; experience persistent or worsening HF requiring a pre-specified intervention at any time during the first 48h; or experienced moderate or marked worsening of their global assessment at any of the 3 time points (at 6h, 24h or 48h). Co-primary efficacy end-point 2 evaluates cardiovascular mortality during follow-up after randomization, for the entire duration of the trial.
Key Inclusion Criteria:1) Males and females aged 18 to 85 years.2) Unplanned hospitalization or emergency department
visit for ADHF. Acute HF is defined as including all of the following:a) Dyspnea at rest in a recumbent sitting position (30 to
45 degrees), which has worsened within the past week.b) Radiological evidence of HF on a chest X-ray.c) BNP >500 pg/mL or NT-pro BNP >2000 pg/mL.
3) Ability to start infusion of the study drug within 12h after initial clinical assessment performed by a physician at the emergencyroom/hospital with symptoms of ADHF.
4) Ability to reliably carry out self-assessment of symptoms.5) Systolic blood pressure (SBP) ≥116 mmHg ≤ 180 mmHg.
6) Persisting dyspnea at rest despite standard background therapy for ADHF (as determined by the Investigator) which must include IV furosemide (or equivalent diuretic) at ≥ 40 mg (or its equivalent) at any time after start of emergency services (ambulance, emergency depart-ment, or hospital). At the time of randomization, the pa-tient must still be symptomatic. In addition, the patient should not have received an IV bolus of a diuretic for at least 2h prior to randomization, and the infusion rates of ongoing IV infusions must not have been increased or decreased for at least 2h prior to randomization.
7) Ability to understand the purpose and risks of the study and provide signed and dated informed consent and au-thorization to use protected health information (in accord-ance with national and local privacy regulations).
Ularitide i.v., 15ng/kg/min (n = 1,076)
48h study drug infusion Post-infusion/Post-discharge evaluations
0 6h 24h 48h 60h 72h 120h 30 days 60 days 90 days ... end of study
Aim and Study Design
Cardiovascular reshospitalization until day 180 & cardiovascular mortality for the entire duration of the trial
Placebo i.v. (n = 1,076)
Estimated no. patients: 2,152
Randomization (n = 2,152 patients); Hospitalized patients with AHF
Ularitide for Injection*
Ularitide is the chemically synthesized form of urodilatin, a human, 32-amino acid natriuretic peptide that is pro-duced in the kidneys and found primarily in urine and in very low concentrations in blood plasma.
Under physiologic conditions the endogenous peptide functions purely as an intrarenal paracrine factor. It in-duces natriuresis and diuresis by binding to the natri-uretic peptide receptor in the cortical and inner medullary collecting duct, thereby increasing intracellular levels of cyclic guanosine monophosphate (cGMP).
Broader systemic effects as a potent vasodilatatory agent are achieved when the synthetic peptide Ularitide is infused into the circulation.
References: Mitrovic V, Seferovic P, Simeunovic D, et al. Haemodynamic and clinical effects of Ularitide in
decompensated heart failure.European Heart Journal 2006;27:2823–2832

Subject Identification
PHASE IIIProtocol Pathway ULA01 – TRUE-AHF
Key Inclusion Criteria
Ò Unplanned hospitalization or ER visit for ADHF Ò Dyspnea at rest Ò Radiological evidence of HF on chest X-Ray Ò BNP > 500 pg/mL or NT-pro BNP > 2000 pg/mL Ò Ability to start infusion of the study drug within 12 hrs after initial clinical assessment (ER/hospital)
Ò Ability to reliably carry out self-assessment of symptoms
Ò Systolic blood pressure (SBP) ≥ 116 ≤ 180 mmHg Ò Received IV furosemide ≥ 40 mg (or its equivalent)
4
Key Exclusion Criteria
Ò Suspected acute mechanical cause of ADHF Ò Clinical diagnosis of ACS Ò Planned PCI or CABG within 5 days of randomization Ò Treatment with nesiritide within last 30 days Ò Treatment with dobutamine at a dose > 5 μg/kg/min or use of drugs for support of blood pressure
Ò Treatment with levosimendan, milrinone, or PDE inhibitor within last 7 days
Ò Temperature ≥ 38°C Ò Suspected infections including pneumonia and acute hepatitis
Ò Known vasculitis, active infective endocarditis Ò Acute or chronic respiratory disorder or primary pulmonary hypertension that may interfere with the ability to interpret dyspnea assessment
Ò Serum creatinine > 2.5 mg/dL Ò Anemia (hemoglobin < 9 g/dL or a hematocrit < 25%)
Ò Any previous exposure to Ularitide
Acute Decompensated Heart Failure
ER (Cardiologists/Intensivists)Study
Timeline
Consent
Screening Exams
Randomization
X-Ray; BNP/NT-proBNP; Labs; ECG
Consent to study
Patient randomized
Targeted T < 6 hours(Tmax < 12 hours)The targeted time to Ularitide (TTU) is below 6 hours after the first physician assessment; treatment must be started within 12 hours of initial assessment (ER/Hospital)
6hMax.12 hours
Prospective, Treatment*,Randomized,Double-Blind
*Treatment will be administered
on top of standard treatment
Ularitide, IV 15ng/kg/min
48 hours
Placebo, IV
Final assessment at 120 hours or hospitaldischarge, whichever comes first
Follow-UpVisit D30, then phone follow-ups to assess cardiovascular hospitalisation and death
Day 30, 60, 90,180, every 90
days until EOS
Disclaimer: Patient pathways are tools and not intended to replace the protocol. For a complete overview of the inclusion and
exclusion criteria please refer to the protocol.5
Challenges for Recruitment
Ò Close collaboration between ER and cardiologist Ò Time to treatment window Targeted Time to Ularitide (TTU) < 6 hours, Tmax < 12 hours
Ò Trained personnel 24/7 availability
Primary Efficacy EndpointHierarchical Composite
Ò Death Ò Worsening HF requiring intervention Ò Patient Global Assessment Ò Cardiovascular Mortality
2152 subjects randomized Ularitide : Placebo = 1 : 13d-Model of Ularitide
6
Study Design
Patients with ADHF who meet all inclusion and exclusioncriteria will be randomized on a 1:1 basis to continuous IV infusion of either ularitide 15 ng/kg BW/min or matching placebo for 48 h. In addition, patients may receive all appropriate therapy that may include vaso-dilatory, inotropic, and diuretic support as clinically indi-cated. However, use of nesiritide, levosimendan, milrinone, or any other phosphodiesterase inhibitor is not allowed during the first 72 h following the start of the infusion.
All timepoints refer to the start of the study drug infu-sion at the timepoint called “0 hours” (t0). Co-primary efficacy endpoint 1 will be assessed at 6 h, 24 h and 48
h from the start of infusion Co-primary efficacy endpoint 2 evaluates cardiovascular mortality during follow-up af-ter randomization, for the entire duration of the trial.
Safety parameters will be assessed during the index hospitalization and adverse events (AEs) and serious ad-verse events (SAEs) will be evaluated until Day 30 after the start of therapy. All patients will be assessed through a study visit at Day 30 and phone call follow-ups at Day 60, Day 90 and Day 180 for the occurrence of cardiovas-cular rehospitalization and allcause mortality. After Day 180, patients will be contacted every 3 months until the end of the study, in order to assess all-cause mortality.
Independent Committees
All outcomes associated with the primary endpoints will be adjudicated by an independent Clinical Events Committee (CEC). In addition, all cardiovascular hospi-talizations and deaths recorded during the 180-day follow-up period will be adjudicated.
An independent Data and Safety Monitoring Board (DSMB) will monitor all efficacy and safety outcomes, but will be able to recommend early termination of the trial for benefit only for a favorable effect of treatment on cardiovascular mortality.
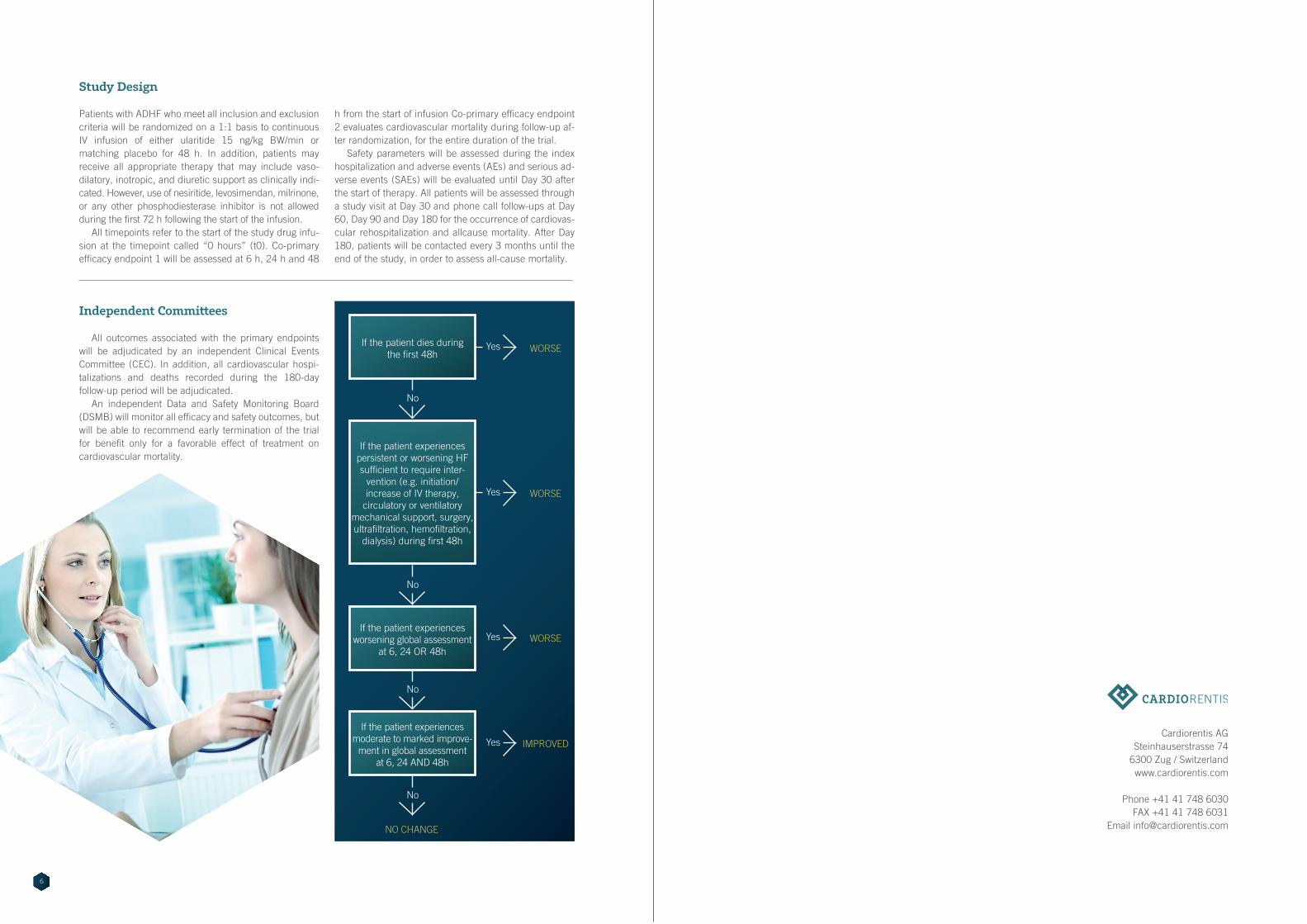
If the patient dies during the first 48h
If the patient experiences persistent or worsening HF sufficient to require inter-
vention (e.g. initiation/ increase of IV therapy,
circulatory or ventilatory mechanical support, surgery, ultrafiltration, hemofiltration,
dialysis) during first 48h
If the patient experiences worsening global assessment
at 6, 24 OR 48h
If the patient experiences moderate to marked improve-
ment in global assessment at 6, 24 AND 48h
No
WORSEYes
No
No
No
WORSEYes
WORSEYes
IMPROVEDYes
NO CHANGE
Cardiorentis AGSteinhauserstrasse 74
6300 Zug / Switzerlandwww.cardiorentis.com
Phone +41 41 748 6030FAX +41 41 748 6031
Email [email protected]

www.cardiorentis.com