treatment planning for the cyberknife treatment delivery ... · pdf filecomparison between...
TRANSCRIPT
© Accuray and/or its affiliates. All rights reserved.
Treatment Planning for the
CyberKnife® Treatment Delivery
System and InCiseTM Multileaf
Collimator:
a Literature Review
Lisa Goggin, PhD DABR
© Accuray and/or its affiliates. All rights reserved.
Disclosure
2
• I am an employee of Accuray® Incorporated

© Accuray and/or its affiliates. All rights reserved.
• Planning the Basics:
Comparison between InCiseTM MLC and Fixed/IrisTM for SBRT:
‒ Prostate
‒ Brain metastases
‒ Liver
• Focus on:
‒ Tumor size, shape, & location
• Expanding Treatment Possibilities:
‒ Conventional fractional
Overview
3
Reported User Experience
© Accuray and/or its affiliates. All rights reserved.
• Peer-reviewed publications
• Peer-reviewed conference submissions
• Search engines include PubMed, Google Scholar, individual
journal searches (Medical Physics, Red Journal, JACMP)
• Search terms include “InCise MLC” AND “CyberKnife” OR
“robotic”
• Abstracts/papers shared with us by users
Search Criteria
4

© Accuray and/or its affiliates. All rights reserved.
Prostate SBRT: MLC Compared to Fixed/IrisTM
5
Study N PTV vol
(cc)
MU
reduction
Tx time
reduction
InCiseTM MLC plan
outcomes
McGuinness
(2015)
5 33 – 85 37%
(p=0.01)
45%
(p=0.001)
gEUDMLC to bladder
lower by 25%
(p=0.005)
Kathriarachchi
(2016)
10 61 – 139 42%
(p=0.002)
40%*
(p=0.006)
GIMLC lower by 29%
(p=0.002)
Murai
(2017)
10 35 – 132 equiv. 19%**
(p=0.003)
rectal doseMLC: V50%,
V80%, V90% lower by
>30% (p<0.04)
Tomida
(2017)
10 n/a 27%
(p<0.05)
30%/20%**
F/I (p<0.05)
Bladder V50% lower by
30% (p<0.05)
Results
• *the time reported in the study included a 5 min set-up. The percentage time reduction recalculated without the set-up time for consistency with the other studies.
• **not known if set-up time is incorporated into the figures reported
• gEUD: generalized equivalent uniform dose, GI: gradient index, V50% volume receiving 50% of prescribed dose

© Accuray and/or its affiliates. All rights reserved.
Prostate SBRT: MLC Compared to Fixed/IrisTM
6
Figures
Average DVH from McGuinness et al.
demonstrating superior bladder
sparing with the InCiseTM MLC plans
Example from Kathriarachchi
et al. demonstrating the
steeper dose gradient with
the InCiseTM MLC
IrisTM InCiseTM MLC
McGuinness et al., JACMP 16, 2015
Kathriarachchi et al., JMP 41, 2016

© Accuray and/or its affiliates. All rights reserved.
Prostate SBRT: MLC Compared to Fixed/IrisTM
7
• McGuinness:‒ The “SBRT plans demonstrate superior performance for the CK-MLC
compared to the CyberKnife with circular collimators”.
• Kathriarachchi:‒ “the InCise™ MLC of CK M6™ was able to produce dosimetrically
comparable plans with the IRIS™ collimator for prostate SBRT.”
• Murai:‒ “MLC treatment is considered advantageous in cases with overlaps with
critical organs”
‒ “the MLC mode should be the first option in stereotactic body radiotherapy.”
• Tomida:‒ “In this study, the advantages of MLCs over other types of collimators in
robotic radiosurgery systems for prostrate SBRT treatment planning were clarified.”
Conclusions

© Accuray and/or its affiliates. All rights reserved.
Brain SBRT: MLC Compared to Fixed/IrisTM
8
Study N PTV vol
(cc)
MU
reduction
Tx time
reduction
InCiseTM MLC plan
outcomes
McGuinness
(2015)
5 7 – 70 67%
(p=0.085)
45%
(p=0.056)
- gEUDMLC to the
optical chiasm and
brainstem generally
lower (p>0.05)
- R50%(MLC) lower by
48% (p=0.05)
Jang
(2016)
25 0.09 - 47 58%
(p<0.05)
40%*
(p<0.05)
- 7% less conformal
(p=0.035)
Limoges
(2017)
10 3 - 34 37%
(p=n/a)
26%*
(p=n/a)
- GIMLC lower by 10%
(p=n/a)
Results
• *the time reported in the study included a 5 min set-up. The percentage time reduction recalculated without the set-up time for consistency with the other studies.
• **not known if set-up time is incorporated into the figures reported
• gEUD: generalized equivalent uniform dose, GI: gradient index=V50%RxIDL/VRxIDL, R50%=V50%RxIDL/PTV
(Publication/Presentation)
© Accuray and/or its affiliates. All rights reserved.
Brain SBRT: MLC Compared to Fixed/IrisTM
9
• McGuinness:‒ The “SBRT plans demonstrate superior performance for the CK-MLC
compared to the CyberKnife with circular collimators”.
• Jang:‒ “The present study showed that the delivery of intracranial SRS using the
InCise1 MLC was dosimetrically feasible…However, small targets (size < 7.6 mm × 7.5 mm) might not be good candidates for MLC-based planning. Overall, the InCise1 MLC is a useful delivery modality for cases in which delivery time is a limiting factor or for multitarget cases”
• Limoges:‒ “The use of the InCise MLC for Cyberknife stereotactic radiotherapy
allows a significant reduction of MU and treatment time compared to Iris collimator while maintaining a high degree of conformality and a steep dose gradient.”
Conclusions

© Accuray and/or its affiliates. All rights reserved.
Liver SBRT: MLC Compared to Fixed/IrisTM
10
Study N PTV (cc)
Equiv diam*
(cm)
MU
reduction
Tx time
reduction
InCiseTM MLC plan
outcomes
Murai
(2017)
10 26 – 283
3.6 – 8.1
69%
(p=0.002)
37%**
(p=0.001)
- Dmax(MLC): stomach,
esophagus, spinal cord
reduced by >30%
(p>0.5)
Doro
(2017)
27 25.7 – 643
3.7-10.7
16%
(p=0.02)
23%**
(p<0.001)
- GIMLC lower by 15%
(p<0.001)
- Bowelmean lower by
54% (p=0.002)
Limoges
(2017)
10 59 - 387
4.8 - 9
-8%
(p=n/a)
17%***
(p=n/a)
- GIMLC lower by 15%
(p=n/a)
Results
• *diameter of equivalent sphere, calculated from the volume for this presentation **not known if set-up time is incorporated into the figures reported
• ***the time reported in the study included a 15 min set-up. The percentage time reduction recalculated without the set-up time for consistency with the other studies.
• GI: gradient index, Dmax: maximum dose
(Publication/Presentation)

© Accuray and/or its affiliates. All rights reserved.
Liver SBRT: MLC Compared to Fixed/IrisTM
11
• Murai:‒ “MLC treatment is considered advantageous in cases with overlaps with
critical organs”
‒ “the MLC mode should be the first option in stereotactic body radiotherapy.”
• Doro:‒ “The results demonstrate that MLC is a good alternative to IRIS for
CyberKnife Liver SBRT”
• Limoges:‒ “The use of the InCise MLC for Cyberknife stereotactic radiotherapy
allows a significant reduction of MU and treatment time compared to Iris collimator while maintaining a high degree of conformality and a steep dose gradient.”
Conclusions
© Accuray and/or its affiliates. All rights reserved.
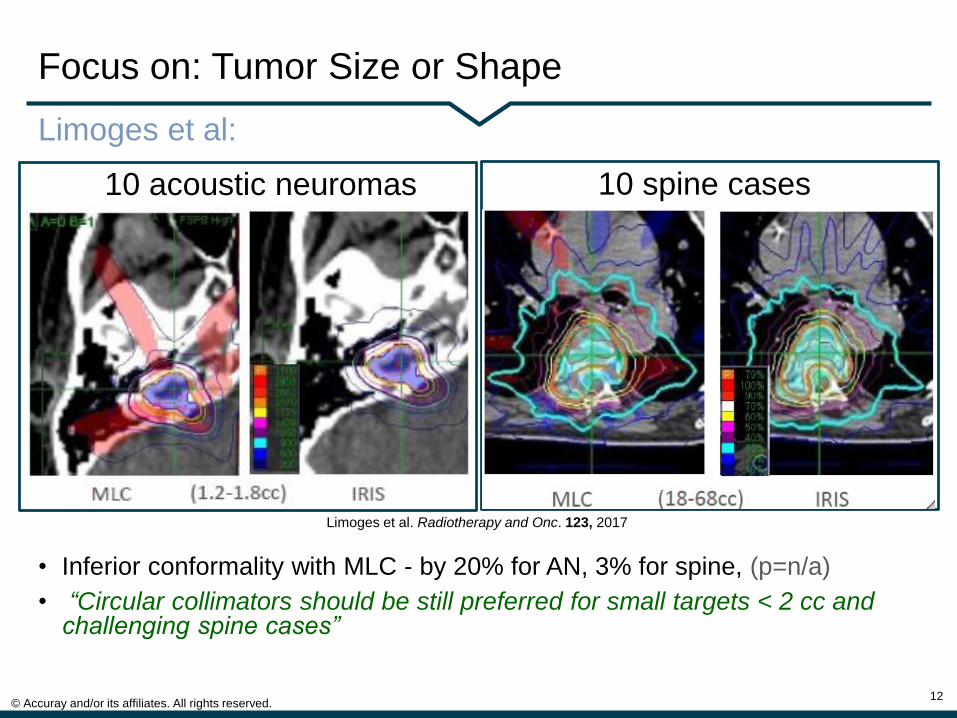
Focus on: Tumor Size or Shape
12
10 acoustic neuromas
Limoges et al:
10 spine cases
• Inferior conformality with MLC - by 20% for AN, 3% for spine, (p=n/a)
• “Circular collimators should be still preferred for small targets < 2 cc and challenging spine cases”
Limoges et al. Radiotherapy and Onc. 123, 2017

© Accuray and/or its affiliates. All rights reserved.
Focus on: Tumor Size
13
Murai et al• Contoured spherical PTVs: 1, 3, 5, 7 cm (0.5-180 cc)
• Compared plans for circular collimators and MLC
• Assumed no critical organs
“…unless the priority of
conformity is higher than
that of any other factors,
the MLC mode is
recommended.”
Murai et al. J Radiat Res. 2017
MLCF/I
© Accuray and/or its affiliates. All rights reserved.
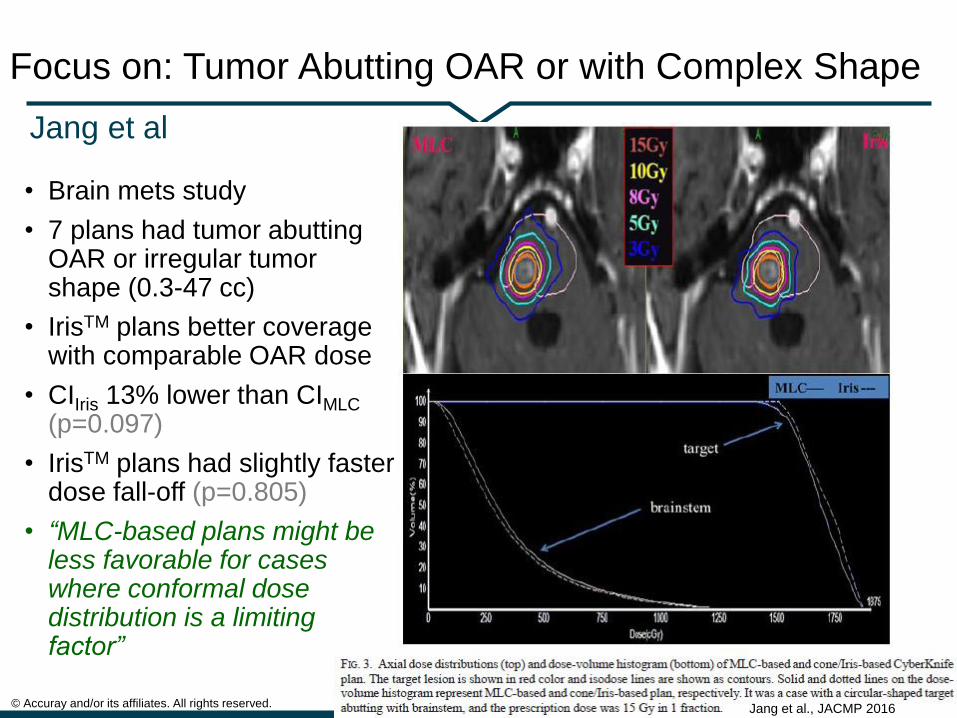
Focus on: Tumor Abutting OAR or with Complex Shape
14
• Brain mets study
• 7 plans had tumor abutting OAR or irregular tumorshape (0.3-47 cc)
• IrisTM plans better coverage with comparable OAR dose
• CIIris 13% lower than CIMLC
(p=0.097)
• IrisTM plans had slightly faster dose fall-off (p=0.805)
• “MLC-based plans might be less favorable for cases where conformal dose distribution is a limiting factor”
Jang et al
Jang et al., JACMP 2016
© Accuray and/or its affiliates. All rights reserved.
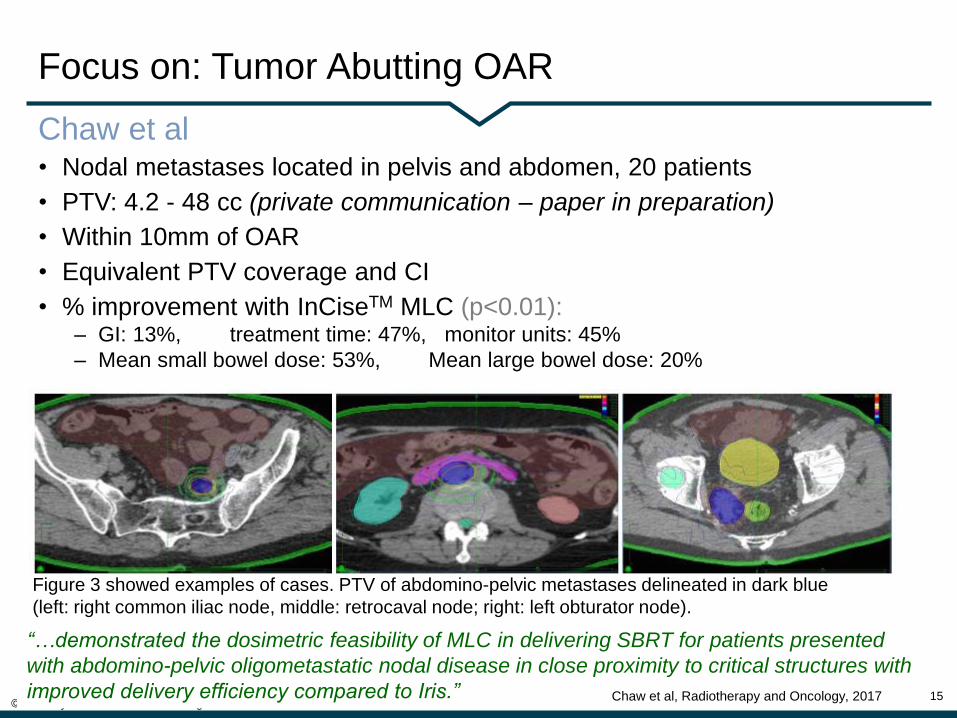
Focus on: Tumor Abutting OAR
15
Figure 3 showed examples of cases. PTV of abdomino-pelvic metastases delineated in dark blue
(left: right common iliac node, middle: retrocaval node; right: left obturator node).
• Nodal metastases located in pelvis and abdomen, 20 patients
• PTV: 4.2 - 48 cc (private communication – paper in preparation)
• Within 10mm of OAR
• Equivalent PTV coverage and CI
• % improvement with InCiseTM MLC (p<0.01):‒ GI: 13%, treatment time: 47%, monitor units: 45%
‒ Mean small bowel dose: 53%, Mean large bowel dose: 20%
Chaw et al
“…demonstrated the dosimetric feasibility of MLC in delivering SBRT for patients presented
with abdomino-pelvic oligometastatic nodal disease in close proximity to critical structures with
improved delivery efficiency compared to Iris.” Chaw et al, Radiotherapy and Oncology, 2017

© Accuray and/or its affiliates. All rights reserved.
Conventional Fractionation with CyberKnife® System InCiseTM MLC
16
Study N PTV vol
(cc)
Prescription
isodose line
(%)
Reduction
in R50%
CyberKnife
MLC Tx
time
Increase
in MU
whole
pelvis
5 426-761 86 29%
(p=0.0007)
24.8 mins 3x
intracranial 5 46-219 92 28%
(p=0.16)
19 mins 1.4x
McGuinness et al
• Same margins used for CyberKnife® System and linac planning
• CyberKnife prescription isodose line within 2-3% of conventional linac
• Equivalent conformity, dose to OARs
• Reasonable treatment time – 4 of 5 IC plans < 20 mins
• Plan quality and efficiency drop when max 2D target projection exceeds the maximum field size – whole pelvis plans.
• CyberKnife® System with InCise MLC, “in select clinical cases, might be a potential alternative for standard fractionated treatments ”
© Accuray and/or its affiliates. All rights reserved.
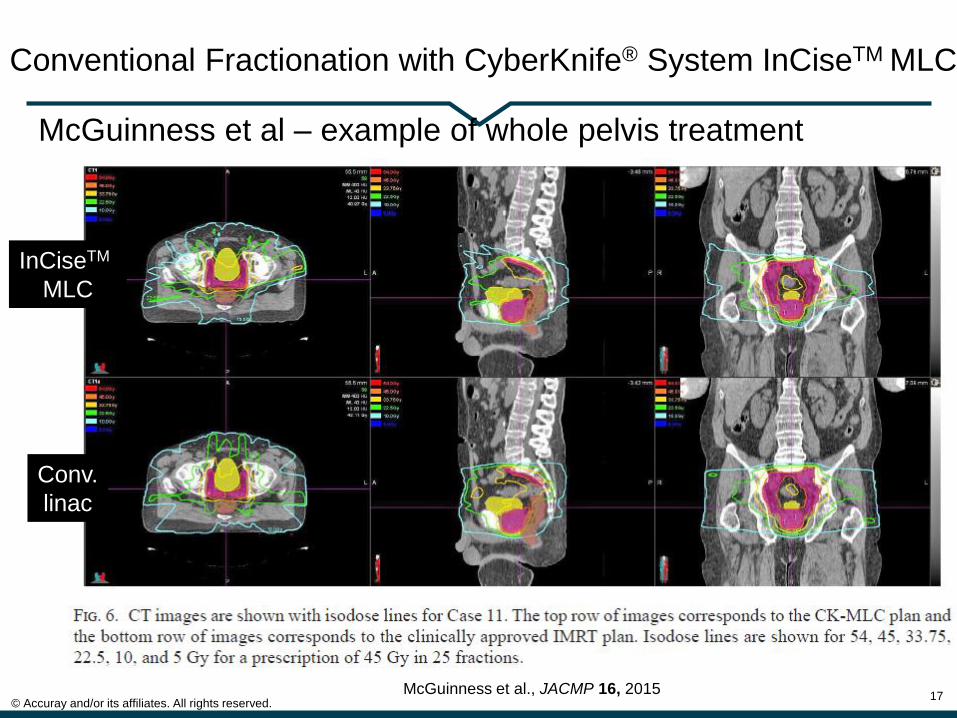
Conventional Fractionation with CyberKnife® System InCiseTM MLC
17
McGuinness et al – example of whole pelvis treatment
InCiseTM
MLC
Conv.
linac
McGuinness et al., JACMP 16, 2015
© Accuray and/or its affiliates. All rights reserved.
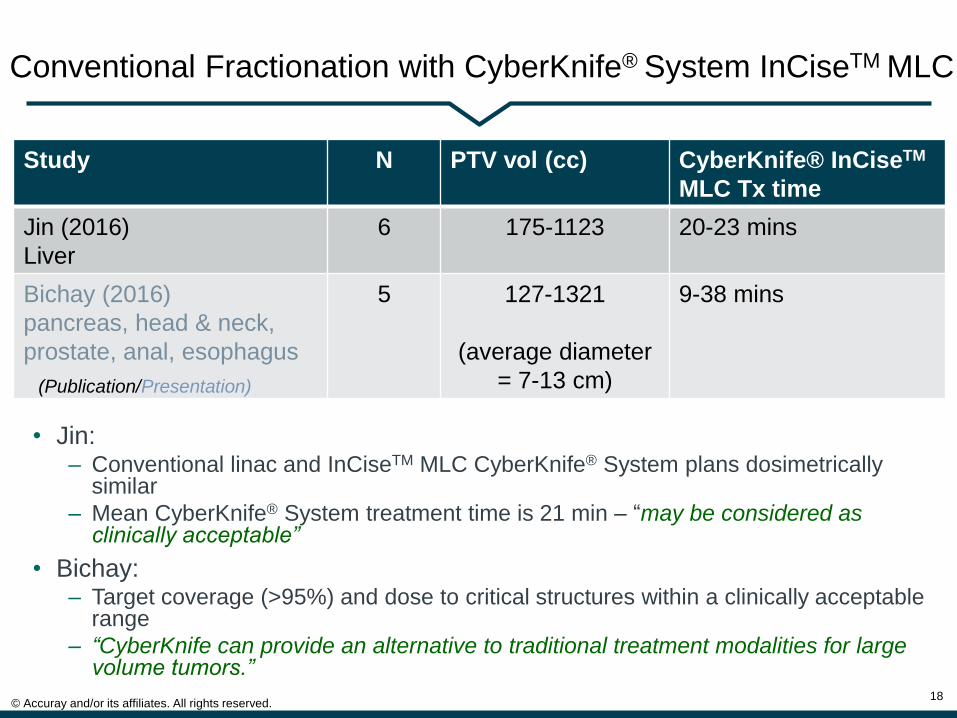
Conventional Fractionation with CyberKnife® System InCiseTM MLC
18
Study N PTV vol (cc) CyberKnife® InCiseTM
MLC Tx time
Jin (2016)
Liver
6 175-1123 20-23 mins
Bichay (2016)
pancreas, head & neck,
prostate, anal, esophagus
5 127-1321
(average diameter
= 7-13 cm)
9-38 mins
• Jin: ‒ Conventional linac and InCiseTM MLC CyberKnife® System plans dosimetrically
similar
‒ Mean CyberKnife® System treatment time is 21 min – “may be considered as clinically acceptable”
• Bichay:‒ Target coverage (>95%) and dose to critical structures within a clinically acceptable
range
‒ “CyberKnife can provide an alternative to traditional treatment modalities for large volume tumors.”
(Publication/Presentation)

© Accuray and/or its affiliates. All rights reserved.
• Prostate
‒ Feng J, Yang J, Lamond J, Lavere N, Laciano R, Ding W, Arrigo S, Brady L. A DosimetricComparison of Robotic Prostatic Radiosugery Using Multi- Leaf Collimation Vs Circular Collimators. Medical Physics, 2014 Jun; 41(6), 223
‒ Fahimian B, Soltys S, Xing L, Gibbs I, Chang S, Wang, L. Evaluation of MLC-Based Robotic Radiotherapy. Medical Physics, 2013, 40(6) 344
• Breast
‒ Goggin LM, Descovich M, McGuinness C, Shiao S, Pouliot J, Park C. Dosimetric comparison between 3-dimensional conformal and robotic SBRT treatment plans for accelerated partial breast radiotherapy. Technology in cancer research & treatment. 2016 Jun; 15(3): 437-45.
‒ Ding C, Timmerman R, Jiang S, Rahimi A. The Comparison of Robotic Partial Breast Stereotactic Irradiation Using MLC Vs. Iris Cone. Medical Physics, 2016 Jun; 43(6), 3613.
‒ Fahimian B, Soltys S, Xing L, Gibbs I, Chang S, Wang, L. Evaluation of MLC-Based Robotic Radiotherapy. Medical Physics, 2013, 40(6) 344
• Peri-orbit carcinoma
‒ Fahimian B, Soltys S, Xing L, Gibbs I, Chang S, Wang, L. Evaluation of MLC-Based Robotic Radiotherapy. Medical Physics, 2013, 40(6) 344
• Ventricular Tachycardia
‒ Wang L, Fahimian B, Soltys SG, Zei P, Lo A, Gardner EA, Maguire PJ, Loo Jr BW. Stereotactic Arrhythmia Radioablation(STAR) of Ventricular Tachycardia: A Treatment Planning Study. Cureus, 2016 Jul; 8(7), e694
• Prone Treatments
‒ Ahn KS, Cho JH, Keum KC. Dosimetric Evaluation of MLC and Fixed Cone for Patients in the Prone Position with CyberKnife. Radiotherapy and Oncology. 2017 May; 123 S1:S456.
Additional MLC planning studies
19
(Publication/Presentation)
© Accuray and/or its affiliates. All rights reserved.
Summary
20
• InCiseTM MLC plans are dosimetrically equivalent or superior to CyberKnife® System plans with circular collimators for prostate, brain, liver.
• InCise™ MLC plans are more efficient than CyberKnife® System plans with circular collimators for prostate, brain, liver.
• Circular collimators may provide superior plans for small and irregularly-shaped tumors abutting an OAR
• Conventional fractionation on CyberKnife® System is feasible with the MLC

© Accuray and/or its affiliates. All rights reserved.
References
21
• McGuinness CM, Gottschalk AR, Lessard E, Nakamura JL, Pinnaduwage D, PouliotJ, Sims C, Descovich M. Investigating the clinical advantages of a robotic linacequipped with a multileaf collimator in the treatment of brain and prostate cancer patients. Journal of Applied Clinical Medical Physics. 2015 Sep 8;16(5).
• Kathriarachchi V, Shang C, Evans G, Leventouri T, Kalantzis G. Dosimetric and radiobiological comparison of CyberKnife M6™ InCise multileaf collimator over IRIS™ variable collimator in prostate stereotactic body radiation therapy. Journal of medical physics/Association of Medical Physicists of India. 2016 Apr;41(2):135.
• Murai T, Hattori Y, Sugie C, Iwata H, Iwabuchi M and Shibamoto Y. Comparison of multileaf collimator and conventional circular collimator systems in Cyberknife stereotactic radiotherapy. J Radiat Res. 2017 Feb 13:1-8. doi: 10.1093/jrr/rrw130. [Epub ahead of print]
• Tomida M, Kamomae T, Suzuki J, Ohashi Y, Itoh Y, Oguchi H, Okuda T. Clinical usefulness of MLCs in robotic radiosurgery systems for prostate SBRT. Journal of Applied Clinical Medical Physics. 2017 Jun, doi: 10.1002/acm2.12128. [Epub ahead of print]
• Jang SY, Lalonde R, Ozhasoglu C, Burton S, Heron D, and Huq MS. Dosimetriccomparison between cone/Iris-based and InCise MLC-based CyberKnife plans for single and multiple brain metastases. J Appl Clin Med Phys. 2016 Sep;17(5):1-16.
(Publication/Presentation)
© Accuray and/or its affiliates. All rights reserved.
References
22
• Limoges C, Bellec J, Delaby N, Perdrieux M, Jouyaux F, Nouhaud E, Lecouillard L, Chajon E, DeCrevoisier R, Le Prisé E, Lafond C. Evaluation of the new InCise MLC for Cyberknife stereotactic radiotherapy. Radiotherapy and Oncology. 2017 May; 123 S1:S444.
• Doro R, Masi L, Di Cataldo V, Cipressi S, Bonucci I, Loi M, Livi L. Investigating the advantages of CyberKnife M6 MLC over Iris collimator for Liver SBRT plans.Radiotherapy and Oncology. 2017 May; 123 S1:S834–S835.
• Chaw C L, VanAs N J, Khoo V S. Cyberknife Iris based versus InCise based plans for 20 cases of prostate oligonodal metastases. Radiotherapy and Oncology. 2017 May; 123 S1:S834.
• Jin L, Price RA, Wang L, Meyer J, Fan JJ, Ma CM. Dosimetric and delivery efficiency investigation for treating hepatic lesions with a MLC-equipped robotic radiosurgery–radiotherapy combined system. Medical physics. 2016 Feb 1;43(2):727-33.
• Bichay T, Mayville A. CyberKnife with MLC for Treatment of Large Volume Tumors: A Feasibility Study. Medical Physics. 2016 June; 43(6):3587.
(Publication/Presentation)

© Accuray and/or its affiliates. All rights reserved.
Thank You
23Part #