treatment of acute myocardial infarction - summitmd.com · sge; 0802-3, 6 *available in 45% of...
TRANSCRIPT

Stephen G. Ellis, MDStephen G. Ellis, MDDirector, Sones Cardiac Catheterization LabsDirector, Sones Cardiac Catheterization Labs
Associate, Joseph J. Jacobs Center for Thrombosis and Arterial BAssociate, Joseph J. Jacobs Center for Thrombosis and Arterial BiologyiologyProfessor of Medicine, Ohio State UniversityProfessor of Medicine, Ohio State University
TTHEHE CCLEVELANDLEVELAND CCLINICLINIC FFOUNDATIONOUNDATION
Treatment ofTreatment ofAcute Myocardial Infarction Acute Myocardial Infarction
The FINESSE TrialThe FINESSE Trial
Miami, FloridaMiami, FloridaMay 6, 2003May 6, 2003

PathophysiologyPathophysiology: The Basics: The Basics
AMI RxAMI Rx
•• Five Five ““driversdrivers”” of mortality risk (age, of mortality risk (age, sBPsBP, Killip , Killip class, HR, MI location establish baseline risk)class, HR, MI location establish baseline risk)
•• ““Time is muscleTime is muscle””
•• TIMI 3 flow is goodTIMI 3 flow is good
•• TIMI 3 flow with microvascular perfusion is betterTIMI 3 flow with microvascular perfusion is better
SGE; 0802-3, 1

AMI RxAMI Rx
00--11 9.5%9.5% 13.0%13.0% 353522--33 8.2%8.2% 10.7%10.7% 252544--66 9.7%9.7% 11.5%11.5% 191977--1212 11.1%11.1% 12.7%12.7% 16161313--2424 10.0%10.0% 10.5%10.5% 55
Time is MuscleTime is Muscle
HoursHours FF CCfromfrom BenefitBenefit
OnsetOnset per 1000per 1000
Mortality 0Mortality 0--35d35d
FTT CollaborativeFTT CollaborativeGroup Lancet 1994Group Lancet 1994
SGE; 0802-3, 2

Acute MIAcute MIImportance of Importance of ““Door to NeedleDoor to Needle”” TimeTime
Cannon for NRMICannon for NRMI--2 Study, JACC 35:376A, 20002 Study, JACC 35:376A, 2000
28,624 33,867 11,616 10, 316N =
Door-to-Needle Time (min)28,624 33,867 11,616 10, 316N =
0 - 30 31 - 60 61 - 90 > 90
1.4
1.2
1.0
0.8
Door-to-Needle Time (min)
Adjusted Odds of DeathAdjusted Odds of Death
0 - 30 31 - 60 61 - 90 > 90
1.4
1.2
1.0
0.8
p = NS
p = 0.01
p = 0.0001
SGE; 0802-3, 3

Primary PCIPrimary PCIImportance of Door to Balloon TimeImportance of Door to Balloon Time
SGE; 1002-3, 1
25
15
5
0
20
10
25
15
5
0
30 Day Mortality (%)
>91N = 140
PTCA notperformed
N = 93
76 - 90N = 76
< 60N = 104
61 - 75N = 109
Time to PTCA (minutes)
30 Day Mortality (%)
>91N = 140
PTCA notperformed
N = 93
76 - 90N = 76
< 60N = 104
61 - 75N = 109
Time to PTCA (minutes)
20
10
p = 0.001
Berger for the GUSTO IIb Investigators, Circ 100:14, 1999Berger for the GUSTO IIb Investigators, Circ 100:14, 1999

Acute MIAcute MIPTCA vs LysisPTCA vs Lysis
SGE; 0802-3, 5
< 2 h< 2 h 2-4 h2-4 h > 4 h> 4 h
3.93.95.05.0 4.14.1
6.36.34.74.7
12.112.1
PP TT PP TT PP TT
30 Day Mortality30 Day Mortality
Timing of PresentationTiming of Presentation
Mortality/Time Mortality/Time InteractionInteraction
PCI: p=.90PCI: p=.90
Lytics: p=.0005Lytics: p=.0005
n=838(<2h), 1035 (2n=838(<2h), 1035 (2--4h), 612(<4h)4h), 612(<4h)↑↑ time time ∝∝ ↑↑ age, female gender, DM, age, female gender, DM, ↑↑HRHR
PCAT Collaborative GroupPCAT Collaborative Group

Facilitated PCI for AMIFacilitated PCI for AMIMight Time to Reperfusion be Less Important Might Time to Reperfusion be Less Important for PCI than for Fibrinolysis?for PCI than for Fibrinolysis?
NN 666666 11351135 ——SxSx→→ER (hr)ER (hr) 1.31.3 1.51.5 .55.55ER ER →→reperfusion (hr)reperfusion (hr) 3.03.0 2.12.1 <.001<.001Ant MI %Ant MI % 4040 3636 NSNSPeak CKPeak CK--MBMB 187187 164164 .003.00330 day mortality (%)30 day mortality (%) 7.67.6 8.18.1 NSNS∆∆ acute acute →→ 6 mo6 mo +2.7+2.7 +3.8+3.8 NSNS
LVEF*LVEF*
4 referral hosp4 referral hosp44--34 miles distance34 miles distance TransferredTransferred
NotNotTransferredTransferred PP
SGE; 0802-3, 6
**available in 45% of patientsavailable in 45% of patients Brodie, AJC '02Brodie, AJC '02
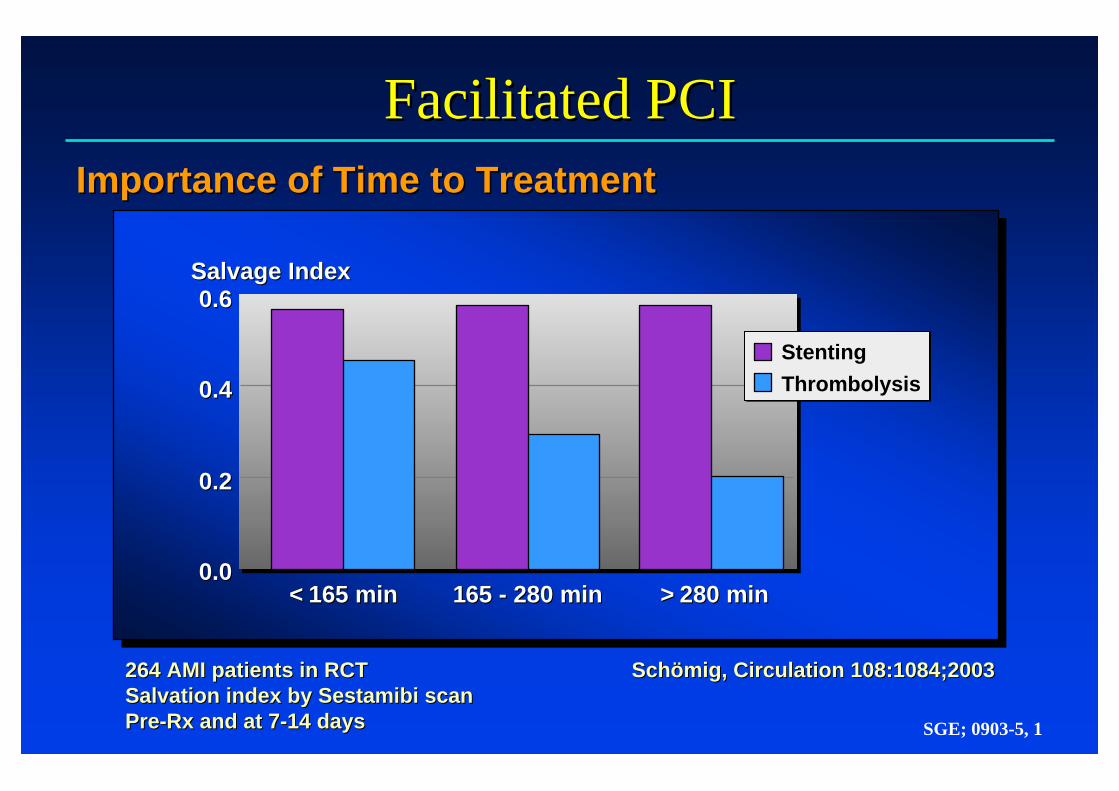
Importance of Time to TreatmentImportance of Time to Treatment
Facilitated PCIFacilitated PCI
SGE; 0903-5, 1
264 AMI patients in RCT264 AMI patients in RCTSalvation index by Sestamibi scanSalvation index by Sestamibi scanPrePre--Rx and at 7Rx and at 7--14 days14 days
SchSchöömigmig, Circulation 108:1084;2003, Circulation 108:1084;2003
0.60.6
0.40.4
0.20.2
0.00.0<< 116655 mmiinn
Salvage IndexSalvage Index
116655 -- 228800 mmiinn >> 228800 mmiinn
StentingThrombolysis

AMIAMIEffect of Time to PCI on 6 Month MortalityEffect of Time to PCI on 6 Month Mortality
AntoniucciAntoniucci, AJC 89:1248 , AJC 89:1248 ‘‘0202+ age < 70 yrs, non+ age < 70 yrs, non--ant MI, HR <100ant MI, HR <100
Low RiskLow Risk High RiskHigh Risk
< 2< 2 2-42-4 4-64-6 > 6> 600
55
1010
1515
2020PercentPercent
HoursHours
1.6 1.3 1.30.0
P=NS
< 2< 2 2-42-4 4-64-6 > 6> 600
55
1010
1515
2020PercentPercent
HoursHours
4.87.9
12.911.5
P=0.04
N=394N=394 N=942N=942
SGE; 0703-1, 01

PTCA vs. Lytics for AMIPTCA vs. Lytics for AMI
GrinesGrines, NEJM 1996, NEJM 1996
Impact of TIMI 3 Flow on MortalityImpact of TIMI 3 Flow on Mortality
GUSTO Study of Thrombolysis1. Occluded arteries (all patients)2. Patients given subcutaneous SK and heparin3. Patients given intravenous SK and heparin4. Patients given SK plus t-PA5. Patients given accel t-PA
GUSTO Study of Thrombolysis1. Occluded arteries (all patients)2. Patients given subcutaneous SK and heparin3. Patients given intravenous SK and heparin4. Patients given SK plus t-PA5. Patients given accel t-PA
Studies of Primary PTCA6. GUSTO IIb7. PAMI - 18. PAR9. PAMI - 2
Studies of Primary PTCA6. GUSTO IIb7. PAMI - 18. PAR9. PAMI - 2
Patients with TIMI Grade 3 Flow (%)
12
3
45
6
7
8
9
0 20 40 60 80 1000
2
4
6
8
10Death (%)
0
2
4
6
8
10
0 20 40 60 80 100Patients with TIMI Grade 3 Flow (%)
Death (%)
SGE; 0802-3, 8

Facilitated PCI for AMIFacilitated PCI for AMIImportance of TIMI 3 Flow Pre PCIImportance of TIMI 3 Flow Pre PCI
NN 19521952 375375 ——Age (yr)Age (yr) 60 60 ±± 1212 60 60 ±± 1313 NSNSSxSx→→Angio (min)Angio (min) 261 261 ±± 275275 264 264 ±± 200200 NSNSKillip 2Killip 2--3 (%)3 (%) 11.611.6 7.07.0 .009.009LAD infarct (%)LAD infarct (%) 3939 3939 NSNSBaseline EFBaseline EF 53 53 ±±1111 57 57 ±±1010 .003.003Final TIMI 3 (%)Final TIMI 3 (%) 91.491.4 98.198.1 <.001<.0016 mo mortality (%)6 mo mortality (%) 4.24.2 0.50.5 <.001<.001
PAMI TrialsPAMI Trials TIMI 0TIMI 0--22PrePre
TIMI 3TIMI 3PrePre PP
SGE; 0802-3, 9
Stone, Circ 104:636 '01Stone, Circ 104:636 '01

AMIAMIOn Site Lysis vs Transfer On Site Lysis vs Transfer →→ PCIPCI
Keeley, Lancet 361:13 Keeley, Lancet 361:13 ‘‘0303AIR PAMI, CAPTIM, DANAMIAIR PAMI, CAPTIM, DANAMI--2, PRAGUE2, PRAGUE--22
Frequency (%)Frequency (%)2020
1515
1010
55
00DeathDeath NonNon--fatalfatal
MIMITotalTotal
StrokeStrokeHaemorrhagicHaemorrhagic
StrokeStrokeDeath, NonDeath, Non--fatalfatal
ReinfarctionReinfarctionor Strokeor Stroke
PTCA (n=1466)Thrombolytic therapy (n=1443)
P=0.057 P<0.0001 P<0.049 P=0.25
P<0.0001
SGE; 0703-1, 02

Acute MIAcute MI
•• Speed reperfusion therapySpeed reperfusion therapy
•• Improve microvascular flowImprove microvascular flow
•• Explore novel methods to lessen Explore novel methods to lessen ““reperfusion injuryreperfusion injury”” and / or repopulate and / or repopulate lost myocardiumlost myocardium
Remaining Needs in 2004Remaining Needs in 2004
SGE; 0802-3, 19

Acute MIAcute MI
•• ~20% US patients live > 60 min from cath lab~20% US patients live > 60 min from cath lab
•• 20%20%--90% African, Asian, Canadian, European, 90% African, Asian, Canadian, European, Pacific region and South American patients live Pacific region and South American patients live >60 min from cath lab>60 min from cath lab
•• Not all cath labs offer 24/7 PCINot all cath labs offer 24/7 PCI
Therefore, need for early pharmacologic reperfusionTherefore, need for early pharmacologic reperfusion
Access to Reperfusion TherapyAccess to Reperfusion Therapy
SGE; 0802-3, 20

t-PAt-PA PIPI
3.03.0 2.62.6
t-PAt-PA PIPI
3.63.6 3.33.3
PACTPACTAMI RxAMI Rx
N=606N=606
Eligible acute infarct patientsEligible acute infarct patients
ASA, IV heparinASA, IV heparin
RandomizedRandomized
Immediate angiographyImmediate angiography
FollowFollow--up angiogram at 5up angiogram at 5--7 days7 days
rTrT--PAPA50mg bolus50mg bolus
TIMI 3TIMI 3
Second bolusSecond bolusof Study Drug of Study Drug
PlaceboPlacebobolusbolus
TIMI 0,1,2TIMI 0,1,2
Immediate Immediate AngioplastyAngioplasty
MortalityMortality ReRe--MIMI30 Day30 Day
p=.81 p=.80
Ross, JACC 34: 1954 Ross, JACC 34: 1954 ‘‘9999
Follow up LVEFTIMI 3 Flow 62±11%*
Pre/Post PCITIMI 3 Flow 58±13%
Post PCI onlyNo TIMI 3 Flow 54±14%
Follow up LVEFFollow up LVEFTIMI 3 FlowTIMI 3 Flow 6262±±11%*11%*
Pre/Post PCIPre/Post PCITIMI 3 FlowTIMI 3 Flow 5858±±13%13%
Post PCI onlyPost PCI onlyNo TIMI 3 FlowNo TIMI 3 Flow 5454±±14%14%
**p=0.004 vs p=0.004 vs TIMI 3 post onlyTIMI 3 post only SGE; 0802-3, 21

Acute MIAcute MIPlatelet Activation by FibrinolyticsPlatelet Activation by Fibrinolytics
Rudd and Rudd and LoscalzoLoscalzo, , CircResCircRes ‘‘9090Rabbit model, .05mM ADP as agonistRabbit model, .05mM ADP as agonist
Normalized Maximal Aggregation RateNormalized Maximal Aggregation Rate
Time (min)Time (min)00 5050 100100 150150 200200 250250
1.51.5
1.01.0
0.50.5
t-PASK
SGE; 0802-3, 22

30 min30 min 60 min60 min 90 min 90 min 120 min120 min 240 min240 min
PercentPercent
34 3748
5764
73 73 8087 89
LyticsCombo
Fascilitated Fascilitated PCIPCITiming of ST Resolution >50%Timing of ST Resolution >50%
KrucoffKrucoff, ACC , ACC ‘‘0303
TimeTime
P=.34
P=.03
P=.02P=.06
P=.30
SGE; 0403SGE; 0403--6, 16, 1IMPACTIMPACT--AMI, PARADIGM, GUSTO V, INTEGRITI (n=654)AMI, PARADIGM, GUSTO V, INTEGRITI (n=654)

Facilitated PCI for AMIFacilitated PCI for AMIADMIRAL / Effect of Time of Administration ADMIRAL / Effect of Time of Administration of Abciximab on 24 hr LVEFof Abciximab on 24 hr LVEF
Mobile ICU or ERMobile ICU or ER CCU or Cath LabCCU or Cath Lab OverallOverall00
2525
5050
7575
100100PercentPercent
5347
55 53 54 51
AbciximabPlacebo
P=.05 P=.23 P=.05
SGE; 0802-3, 23

Acute MIAcute MIGUSTO VGUSTO V
* * including ICH in > 75yrs 2.1 v 1.1% p=0.07including ICH in > 75yrs 2.1 v 1.1% p=0.07 Lancet 357: 1905 Lancet 357: 1905 ‘‘0101
•• 16,588 pts ST16,588 pts ST↑↑MIMI
•• RPA vs halfRPA vs half--dosedoseRPA + abciximabRPA + abciximab
•• Heparin to aPTT Heparin to aPTT 5050--70sec70sec
RPA: RPA: 5000+1000u/hr5000+1000u/hrRPA+Abc: RPA+Abc: 60u/kg+7u/kg/hr60u/kg+7u/kg/hr
•• 30 day outcomes30 day outcomes DeathDeath ReMIReMI Major BleedingMajor Bleeding00
22
44
66
88
1010PercentPercent
5.9 5.6
3.52.3
0.51.1
RPARPA+Abc
P=0.45
P<0.001
P<0.001*
SGE; 0802-3, 14

AMI Treatment LessonsAMI Treatment LessonsFINESSEFINESSE
Early RxEarly Rx TIMI 3TIMI 3 MicrovascMicrovascIC StreptokinaseIC Streptokinase –– +/ +/ –– ––IV StreptokinaseIV Streptokinase ++ +/ +/ –– ––IV tIV t--PA PA →→ 3rd gen. lytics3rd gen. lytics ++ ++ ––Primary PTCAPrimary PTCA –– ++++ ––Primary StentPrimary Stent –– ++++ ––Lytics, Lytics, llbllb//llla llla + 1+ 1°°stents stents ++++ ++++ +/+/--Lytics, Lytics, llbllb//lllallla + 1+ 1°° stents + EPD/RI blockersstents + EPD/RI blockers ++++ ++++ ?+?+
Historical ProgressionHistorical Progression
SGE; 0802-3, 24
Early RxEarly Rx
MicrovascularMicrovascularFlowFlow
TIMI 3 FlowTIMI 3 Flow
PlateletsPlateletsWBC/Reperfusion InjuryWBC/Reperfusion InjuryDebrisDebris
EPD=Emboli Protection Device EPD=Emboli Protection Device RI=Reperfusion InjuryRI=Reperfusion Injury

Cath lab availableCath lab available< 60 minutes< 60 minutes
abciximab + PCI abciximab + PCI
Cath lab delayCath lab delay> 4 hours or not available> 4 hours or not available
ReteplaseReteplase
AMIpresentation
Cath lab availabilityCath lab availabilityuncertain or delay ofuncertain or delay of> 60 min, < 4 hours> 60 min, < 4 hours
Options for Treating AMI PatientsOptions for Treating AMI Patients
Triage
SGE; 0802-3, 29

Facilitated PCI for AMIFacilitated PCI for AMI
MI < 6 hrs and cath likely in 1MI < 6 hrs and cath likely in 1--4 hrs4 hrsExclude low risk (age <60 yrs and localized IMI)Exclude low risk (age <60 yrs and localized IMI)
FINESSE Protocol DesignFINESSE Protocol Design
Heparin 40Heparin 40µµ/kg (70/kg (70µµ/kg in placebo group)/kg in placebo group)or Enoxaparin 30 mg IV + 0.3 mg/kg SCor Enoxaparin 30 mg IV + 0.3 mg/kg SC
90 day Death, Stroke90 day Death, StrokeRehospitalization Rehospitalization for CHF, Late VFfor CHF, Late VF
Cath Cath ±± PCIPCICath Cath ±± PCIPCI Cath Cath ±± PCIPCI(with Abciximab)(with Abciximab)
AbciximabAbciximabASAPASAP
PlaceboPlaceboASAPASAP
RPA (5 + 5U)*RPA (5 + 5U)*AbciximabAbciximabASAPASAP
N = 3000N = 3000*5U only for age >75 yrs*5U only for age >75 yrs
SGE; 0802-3, 25

Fascilitated Fascilitated PCIPCIBRAVE TrialBRAVE Trial Outcomes Combination Abciximb P
only
TIMI 3 flow pre PCI (%) 40 18 <.001
Final infarct size (%) 13 11.5 0.81
Death at 30 days (%) 1.6 1.6 NS
Death/MI at 30 days 2.4 1.6 NS
30 day death, MI, 3.2 1.6 0.66
stroke (%)
Major bleeding (%) 5.6 1.6 0.16
N=253 pts. withSTEMI < 12 hrs.
Randomized to• Abciximab X 12 hrs. or• RPA 5U X 2+ abciximab
1o endpoint: infarct size
Kastrati, AHA ‘03

Facilitated PCI for AMIFacilitated PCI for AMI
•• Inadequate dataInadequate data
•• Consider for large MI and transfer delayConsider for large MI and transfer delay
•• Use 1/2 dose lytics (possibly 1/4 dose lytics for Use 1/2 dose lytics (possibly 1/4 dose lytics for elderly or higher risk for hemorrhagic CVA); elderly or higher risk for hemorrhagic CVA); use low dose UFH/LMWHuse low dose UFH/LMWH
Current Status (5/04)Current Status (5/04)
SGE; 0802-3, 27