treating type 2 diabetes: the oral diabetes drugs - abc news
TRANSCRIPT

Treating Type 2 Diabetes:
The OralDiabetes Drugs Comparing Effectiveness, Safety, and Price
®

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 3
Our Recommendations
2 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Six types of oral medicines (and 11 individual drugs) are now available to help the 21million people in the U.S. with type 2 diabetes control their blood sugar when diet andlifestyle change are not enough. Our evaluation of these medicines found the following:
n Newer drugs are no better. One older type of medicine, the sulfonylureas, and anolder drug named metformin work just as well as four newer classes. Indeed, sev-eral of the newer drugs are less effective than the older ones.
n Newer drugs are no safer. All diabetes pills have the potential to cause adverseeffects, both minor and serious. The drugs’ side effect “profiles” may be the mostimportant factor in your choice.
n Newer drugs are more expensive. The newer diabetes medicines cost many times morethan the older ones.
n Taking two diabetes drugs can improve blood sugar control. Many people with dia-betes do not get enough help from one drug. Two may be necessary. However, tak-ing two drugs can raise the risk of adverse effects and increase costs.
Taking effectiveness, safety, adverse effects, dosing, and cost into consideration, we havechosen the following as Consumer Reports Best Buy Drugs if your doctor and you havedecided that you need medicine to control your diabetes:
n Metformin – alone or in combination with glipizide or glimepiride
n Glipizide and Glipizide Sustained Release – alone or in combination with metformin
n Glimepiride – alone or in combination with metformin
These medicines are available as low-cost generics ($10 to $60). If you have been diag-nosed with diabetes, we recommend that you try metformin first unless your health sta-tus prevents it.
If metformin fails to bring your blood sugar into normal range, we recommend you addglipizide or glimepiride. Should either of those drugs cause problems, Actos (piogliti-zone) may be an option you and your doctor will want to consider. Actos and Avandia(rosiglitizone) have been heavily promoted to doctors and consumers, however, and havebeen over-prescribed.
This report was released and last updated in July 2007.

This report compares the effectiveness, safety, and cost of medicines usedto treat type 2 diabetes. It is part of a Consumers Union and ConsumerReports project to help you find safe, effective medicines that give you themost value for your health-care dollar. To learn more about the projectand other drugs we’ve evaluated for other diseases and conditions, go towww.CRBestBuyDrugs.org.
Type 2 diabetes is one of the most serious medical conditions affecting ournation today. The number of people who have it has been rising alarming-ly in recent years. That includes thousands of children and young adults.
Type 2 diabetes used to be referred to as “adult onset” diabetes. No longer.In recent years, the incidence among young people has exploded. Much ofthat surge has been linked to the dramatic increase in the last 20 years inthe number of young people who are overweight or obese and who arephysically inactive.
The statistics are sobering. An estimated 21 million people in the U.S. havediabetes, about 7 percent of the population. That’s up from 2.5 percent ofthe population in 1980. Despite the increase of the disease among theyoung, older people are still the largest age group affected: one in fivepeople aged 60 or over has diabetes. About 1.5 million people are newlydiagnosed every year.
But despite widespread attention to the diabetes “epidemic,” about one inthree people who have diabetes – some 7 million people – have not beendiagnosed and do not know they have it. Timely diagnosis is no assuranceeither: a third of the people who have been diagnosed with diabetes fail toreceive the medical care and medicines that research shows to be effective.
Why is diabetes of such concern? Studies conclusively show that diabetesmore than doubles the risk of developing and dying of heart disease andother problems. It is as potent a predictor and risk factor for heart diseaseand heart attack as cigarette smoking, high blood pressure, and uncon-trolled high cholesterol. When people with diabetes go untreated for years,the damage it causes almost guarantees a premature death from heart dis-ease.
Diabetes also significantly raises the risk of a host of other problems.These include: stroke, nerve damage (neuropathy), kidney damage; dam-age to the eye and blindness; liver disease, impotence, poor wound heal-ing, and susceptibility to infections that can fester and require amputa-tions of toes, a foot, or part of a leg.
In addition, people with diabetes are very likely to have other dangeroushealth conditions. One recent study found that 47 percent had two other
Welcome
Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 3

4 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
heart disease risk factors (such as smoking, high blood pressure, and highcholesterol) and 18 percent had three or more.
People with uncontrolled diabetes live an average eight years less thanpeople who do not have diabetes. At greatest risk of premature disabilityand death are: women (of all ethnic backgrounds), African Americans,Mexican Americans, American Indians, and the indigenous people ofAlaska.
Women have the same prevalence of diabetes as men, but recent studiesindicate they are much more likely to die from it. Minority group membersare both more prone to develop diabetes (due to genetic and environmen-tal factors) and to become disabled or die from it (due to multiple factorsbut also because they are less likely to get good care).
At the same time, it is important to note that all people with diabetes whoreceive proper and consistent care live good quality lives, and can workand function normally.
Type 1 and Type 2 Diabetes – The Difference
Confusion about diabetes is still widespread. What is it and what is the dif-ference between so-called type 1 and type 2?
Diabetes is a disease characterized by elevation of blood glucose (a sugar)caused by decreased production of the hormone insulin and/or increasedresistance to the action of insulin by certain cells. Insulin is produced inthe pancreas and plays a key role in regulating the level of glucose in yourblood. Glucose is the body’s main fuel, and is essentially the end productof eating any carbohydrates (pasta, bread, rice, grains, fruits, and vegeta-bles). Your digestive system breaks down all carbohydrates into glucose.Glucose then enters the blood stream. It also gets stored in the liver asglycogen, a precursor of glucose.
Insulin regulates both the movement of glucose into the body’s cells andthe breakdown in the liver of glycogen into glucose. Both actions are crit-ical to keeping blood sugar regular and normal.
In type 1 diabetes – usually diagnosed in childhood or the early teen years– the pancreas, over a relatively brief period of time, stops producinginsulin altogether. The onset of the disease is usually abrupt, with severesymptoms that require immediate attention. It is an “autoimmune” disease,which means that the part of the pancreas that produces insulin has beendestroyed by errant immune cells. People with type 1 diabetes must injectinsulin every day. About 1.5 to 2 million people in the U.S. have type 1diabetes.
In type 2 diabetes, the pancreas produces enough insulin, at least in theearly years that a person has the disease. But for reasons that are still notwell understood, the body’s cells become resistant or insensitive to it. To

compensate, the pancreas pumps out increasing amounts of insulin to nor-malize blood glucose levels. Over time – as long as a decade – this ever-increasing production becomes unsustainable, and the pancreas’ ability toproduce insulin declines.
As a result, the telltale marker – and problem – of diabetes emerges: bloodglucose, unable to enter the body’s cells, rises. That rise leads to symp-toms. And when the blood sugar reaches a certain high level it appears inthe urine and causes an increase in the daily volume of urine.
Elevated blood sugar puts a strain on almost every organ and many partsof the body.
Over years, it is particularly toxic to the body’s blood vessels; it causesthem to thicken. This leads especially to problems in the eyes and kidneys,the heart, and the blood circulation system. High blood sugar also dam-ages the nerves. Proper treatment that keeps blood sugar in the normalrange sharply reduces the risk of these complications.
Again, there are many ideas about the causes of type 2 diabetes, and theinsulin resistance that characterizes it. Studies show the disease has astrong genetic (hereditary) component. It runs in families. Another cause –or association – is also quite clear. That is overweight and obesity – due insome cases to a genetic propensity to overweight and obesity but in mostcases to overeating and lack of exercise. About 55 percent of people diag-nosed with diabetes in the U.S. are overweight or obese.
While recent media attention surrounding the diabetes epidemic hasfocused on its link to obesity, the statistic above also means that 45 per-cent of people with diabetes are not overweight.
Symptoms and Getting Tested
The symptoms of type 2 diabetes tend to develop gradually over time andinclude:
n Fatigue n Frequent urinationn Increased thirst and hunger n Blurred vision n Numbness in your hands and legsn Slow healing of wounds and sores
These symptoms can also be mild and/or intermittent for years. If youexperience any of them – and especially if you experience two or more,for even a few days – you should see a doctor immediately.
In the early stages of the disease, symptoms may well be non-existent.That’s unfortunate because the damage to organs occurs even in the
Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 5
absence of symptoms. For this reason, it’s important for people who maybe at risk of diabetes to get have their blood sugar levels checked regular-ly. Those at risk include:
n People with coronary artery disease, or vascular disease
n People who have high blood pressure
n People whose “bad” (LDL) cholesterol is elevated
n People who are overweight or obese
n Anyone with a parent or a sibling who has diabetes
n People who are Black Americans, Mexican or Latino Americans, AsianAmericans, Native Americans, Pacific Islanders, or Alaskan Natives
n Women who have had diabetes during pregnancy or a baby weighingmore than 9 pounds at birth
If you are in one of these groups and you have either never had a bloodsugar check or the last one was done a year or more ago, you should getyour blood sugar checked as soon as possible.
There is a disagreement in the medical community about whether alladults should have their blood sugar checked periodically. The AmericanDiabetes Association advises that everyone aged 45 and over have a bloodsugar test once every three years. But the highly-regarded U.S. PreventiveServices Task Force says not enough scientific evidence exists to indicatethat such broader screening has benefits or is worth the considerable cost.
We think the decision rests with you and your doctor and depends on anassessment of your overall health, risks, your weight, and family history.Some doctors are inclined to check the blood sugars of most people overage 45 or 50, especially if they are 10 or more pounds overweight. Otherdoctors may be more conservative.
Blood sugar tests are inexpensive and easy, though they may have to bedone a few times to yield a conclusive diagnosis. The most common oneis done after an overnight fast. If your blood sugar is 126 milligrams perdeciliter (mg/dl) or greater after being checked on two or three differentoccasions, you are considered to have diabetes. Another test assesses yourblood sugar at any time (not just after not eating for 8 or more hours). Ifyou have blood sugar levels of 200mg/dl or above on two or more occa-sions, you are considered to have diabetes.
Your doctor may also talk to you about a blood test known as “hemoglo-bin A1c” (pronounced hemoglobin “A,” “one,” “c,” and usually abbreviat-ed in print as HbA1c and often referred to by diabetes patients as “myA1c”). This is a commonly used test to evaluate blood sugar control aftertreatment is started. But your doctor may order this test at the time ofdiagnosis. There’s more about this measure in the next section.
6 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs

What is Pre-Diabetes?
In the last decade, doctors and researchers have recognized that a largenumber of people in the U.S. have (fasting) blood sugar levels that areabove 110mg/dl (the upper limit of normal) but less than the 126mg/dlrequired for a diagnosis of diabetes. Namely, the most recent studies indi-cate that nearly 18 percent of the population – 54 million people – havewhat is called pre-diabetes, borderline diabetes, impaired fasting glucose,or impaired glucose tolerance.
What concerns doctors is that a growing body of research now shows thatpeople with pre-diabetes (a) are at very high risk of developing diabetesand (b) at elevated risk of heart disease and stroke even if their glucoselevel never rises above 125 mg/dl.
In the most recent analysis of this – published in June 2007 – people withpre-diabetes were found to have 2.5 times the risk of dying from heart dis-ease over a 5-year period compared to people without diabetes. The studywas of 10,428 people in Australia.
Such findings are leading many doctors to consider drug treatment forpeople with pre-diabetes. But most doctors agree, and good research backsit up, that dietary and lifestyle changes can be very effective for peoplewith pre-diabetes – before any medicines need to be prescribed.
This report does not specifically address treatment of pre-diabetes. If youare diagnosed with pre-diabetes we would urge you to talk with your doc-tor about ways to alter your diet and lifestyle, and lose weight if you needto under a program that you’ll stick to.
Lifestyle modifications have become a mainstay of treatment for peoplewith full-blown diabetes, too. Studies consistently show that lifestylechanges alone – and particularly losing weight – can prevent the compli-cations of diabetes. For some people, they eliminate or reduce the need fordrugs. The next section discusses this further.
Since many people with diabetes also have high blood pressure and/orhigh cholesterol, your doctor will aim to get those under control, too, withdiet and lifestyle changes and with medicines.
Oral diabetes medicines – pills you take by mouth – are thus just one treat-ment among several that doctors use to help people with diabetes and keepthem healthy. That said, they are a critical element of treatment.
Today, nine classes of drugs are available to treat type 2 diabetes. Thatincludes insulin and two other types of drugs that must be injected. Thatleaves six categories of pills. In this report we evaluate and compare allsix groups, and the drugs in them. We do not evaluate the injectable drugs,including the newest one, Byetta (exenatide). We also don’t compare treat-ment with insulin or the other injectible drugs with pills. And we do not
Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 7

8 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
analyze another new diabetes drug – Exubera, a form of insulin that canbe inhaled.
Note that even though most people prefer to avoid injections, insulin andother such drugs often become necessary if diet, exercise, and pills fail tokeep their blood sugar under control.
Like all drugs, the names of the six diabetes drug groups and the names ofthe individual medicines in those groups are not easy to pronounce orremember. We do our best to keep things simple but unfortunately we can’tavoid using the drug category names and the names of the individual drugs.
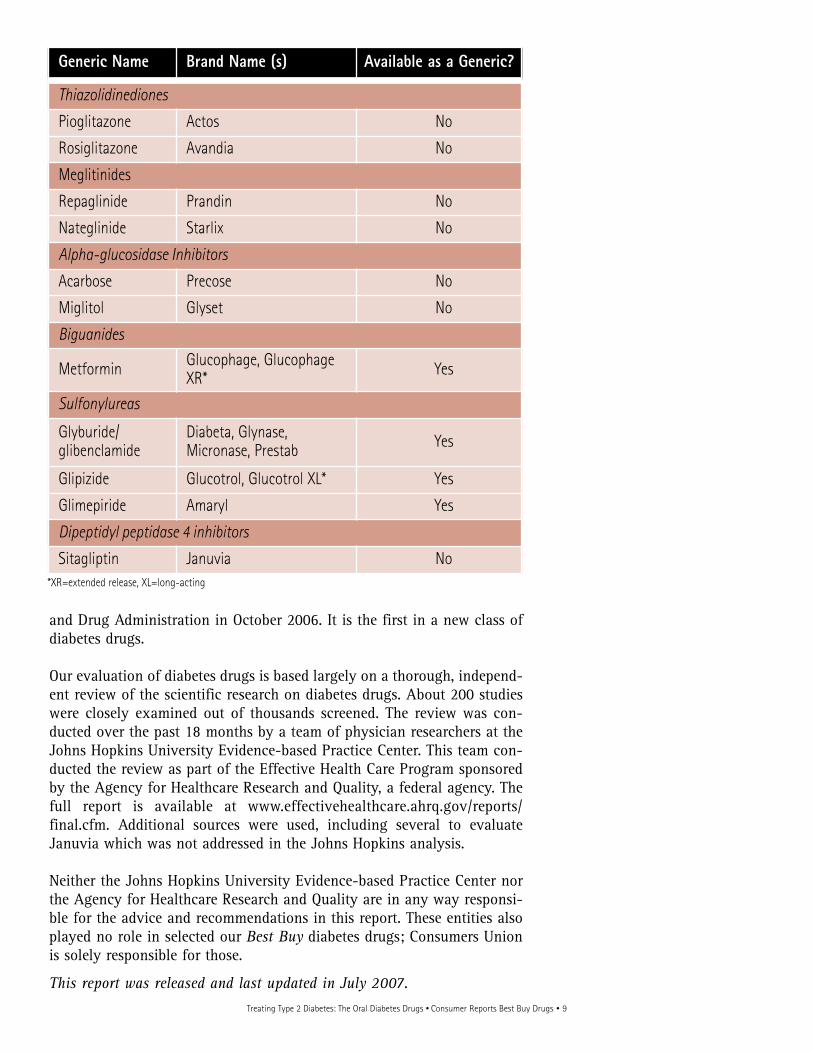
The first table below presents the groups of diabetes drugs, including thosenow available in combination form. The second table presents the individualdrugs, with their generic and brand names. In both, we indicate eitherwhether the class has a generic available or whether an individual drug isavailable in generic form. Generics are much less expensive and becomeavailable after a drug has been on the market for some 10 or more years.
As you can see, the sulfonylureas and metformin are older medicines nowavailable in generic form, while the thiazolidinediones, alpha-glucosidaseinhibitors, and meglitinides are newer. Januvia was approved by the Food
Type of Drug Individual Drugs (Brand and generic names) Available as a Generic?
Sulfonylureas
Brands: Amaryl, Diabeta,Glynase, Prestab, Glucotrol,Glucotrol XL, Micronase Generics: Glimepiride,Glipizide, Glyburide
Yes
Biguanides Brands: Glucophage,Glucophage XR, Generics: Metformin
Yes
Thiazolidinediones Actos, Avandia No
Alpha-glucosidaseinhibitors Precose, Glyset No
Meglitinides Prandin, Starlix No
Dipeptidyl pepti-dase 4 inhibitors Januvia No
Combinations ofsulfonylureas plusmetformin
Brands: Glucovance,Metaglip Generics: known by genericnames of the two drugs
Yes
OtherCombinations
ActosPlus Met, Avandaryl,Avandamet, Duetact,Janumet
No
Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 9
and Drug Administration in October 2006. It is the first in a new class ofdiabetes drugs.
Our evaluation of diabetes drugs is based largely on a thorough, independ-ent review of the scientific research on diabetes drugs. About 200 studieswere closely examined out of thousands screened. The review was con-ducted over the past 18 months by a team of physician researchers at theJohns Hopkins University Evidence-based Practice Center. This team con-ducted the review as part of the Effective Health Care Program sponsoredby the Agency for Healthcare Research and Quality, a federal agency. Thefull report is available at www.effectivehealthcare.ahrq.gov/reports/final.cfm. Additional sources were used, including several to evaluateJanuvia which was not addressed in the Johns Hopkins analysis.
Neither the Johns Hopkins University Evidence-based Practice Center northe Agency for Healthcare Research and Quality are in any way responsi-ble for the advice and recommendations in this report. These entities alsoplayed no role in selected our Best Buy diabetes drugs; Consumers Unionis solely responsible for those.
This report was released and last updated in July 2007.
Generic Name Brand Name (s) Available as a Generic?
Thiazolidinediones
Pioglitazone Actos No
Rosiglitazone Avandia No
Meglitinides
Repaglinide Prandin No
Nateglinide Starlix No
Alpha-glucosidase Inhibitors
Acarbose Precose No
Miglitol Glyset No
Biguanides
Metformin Glucophage, GlucophageXR* Yes
Sulfonylureas
Glyburide/glibenclamide
Diabeta, Glynase,Micronase, Prestab Yes
Glipizide Glucotrol, Glucotrol XL* Yes
Glimepiride Amaryl Yes
Dipeptidyl peptidase 4 inhibitors
Sitagliptin Januvia No*XR=extended release, XL=long-acting

10 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
The six types of diabetes medicines work in differentways. But they all: (a) lower blood sugar levels; (b)help improve the body’s use of glucose; (c) decreasethe symptoms of high blood sugar; (d) help keep peo-ple with diabetes functioning normally; and (e) mayhelp prevent the complications, organ-damagingeffects, and premature death that diabetes can cause.
The complexity of the way the different diabetesdrugs work defies simple explanation. But it’s usefulto know the basics.
n The sulfonylureas and meglitinides increase thesecretion of insulin by the pancreas.
n Metformin inhibits glucose production by theliver and decreases insulin resistance.
n The alpha-glucosidase inhibitors delay absorp-tion of glucose by the intestine.
n The thiazolidinediones decrease insulin resist-ance.
n Januvia promotes the release of insulin from thepancreas.
Since the drugs work in different ways, they aresometimes used in combination to enhance the effec-tiveness of treatment. Indeed, 25 to 50 percent of
What Are the Oral Diabetes Medicines and Who Needs Them? people with diabetes who start taking a drug will needanother type of drug (or insulin) within six years.
The plain fact is that most people with type 2 dia-betes will eventually need to take medicine to keeptheir blood sugar controlled. But all will also need toalter their diets and lifestyles as well – losing weightif needed, dietary changes (such as cutting back oncarbohydrates), quitting smoking, and becomingmore physically active.
Evidence strongly supports the additive effect of thetwo – drugs and lifestyle changes. But many studiesalso show conclusively that many people with dia-betes can lower their blood sugar levels almost asmuch with modest lifestyle changes alone as withmedicines, especially in the early stages of the disease.
Thus, given that (a) all the diabetes drugs have thepotential to cause adverse effects and (b) lifestylechanges have benefits to your health beyond con-trolling blood sugar, most doctors will recommendyou try diet and lifestyle first – before you try a drug.
Many people with diabetes, however, also have highblood pressure and/or elevated cholesterol, or havebeen diagnosed with coronary artery or vascular dis-ease. If you are in this category, your doctor may

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 11
prescribe a diabetes drug when you are diagnosed,along with diet and lifestyle changes and classes indiabetes self-management.
Indeed, so many people with diabetes have otherconditions and heart disease risk factors that doctorsoften treat them as “multi-disease” patients whosecare and drugs must be managed particularly close-ly. Because heart disease risks factors, including dia-betes, take a cumulative toll, medical groups andphysician organizations have set aggressive goals forpeople with diabetes who have multiple conditions.Table 1 above presents these.
Treatment with lifestyle changes and drugs hasshort-term, medium-term, and long-term goals. Inthe short-term, it aims to get your fasting blood glu-cose below 110mg/dl (below 100mg/dl is better) andto eliminate or significantly reduce your symptoms.
In the medium and long-term, it aims to get yourHbA1c measure down below a certain level, and keepit there.
As mentioned already, the HbA1c test is the one yourdoctor will use to track treatment success (or failure).It measures glucose levels chemically bound to
hemoglobin, a protein carried by red blood cells. Thecurrent recommended goal for HbA1c is expressed asa percentage. If you have diabetes, the magic num-ber is 7 percent. Below that is good. Above it is notgood. (Technically anything above 6 percent is con-sidered abnormal. So some doctors would rather seeyour HbA1c be 6.5 percent or lower.)
Many studies show that an HbA1c level below 7 per-cent is associated with a lower risk of diabetes com-plications and premature death. However, important-ly for this report, most studies of the oral diabetesdrugs have only looked at the effects on HbA1c for ayear or less.
Another medium-term and long-term goal of treat-ment is to make sure you are free of the well-knowndiabetes complications as time goes on. This takesconstant monitoring. Indeed, the intensity of careneeded by most people with diabetes is such thatexperts advise all to be cared for in formal diabetesprograms.
Part of the purpose of such programs is to track thedrugs you are taking and at what dose. Your doctorsand caregivers will recommend changes if yourblood sugar is not controlled. In fact, many doctors
Table 1. Goals for People with Diabetes
Measures Recommended Goal
Blood Sugar
Fasting blood glucose Below 110mg/dl (Below 100 is better)
Post-meal (2-hour) blood glucose Below 180mg/dl (Below 140 or so is better)
HemoglobinA1c (HbA1c) Below 7% (Below 6.5% is better)
Cholesterol
Total cholesterol Below 200mg/dl
LDL (“bad” cholesterol) Below 100 mg/dl (below 75 is better)
HDL (“good” cholesterol) Above 40mg/dl for men and 50 mg/dl for women
Triglycerides Below 150 mg/dl
Blood pressure Below 130/80 mmHgSources: American Diabetes Association; American Association of Clinical Endocrinologists; International Diabetes Federation; National Cholesterol Education Program;Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Definitions: LDL= low-density lipoprotein cholesterol; HDL= high-density lipoprotein cholesterol; mg = milligrams; dl=deciliter of blood; mmHg = millimeters mercury.

12 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Side Effects of Diabetes Drugs
Most of the side effects listed here ease over time orstop when the medication is discontinued. However, afew can be permanent in certain people.
Commonn Hypoglycemia or low blood sugar (usually minor if
caught in time but can be serious or fatal if not
treated; symptoms include profuse sweating,
tremor, shakiness, dizziness, hunger. When serious,
includes mental confusion, coma, and a rare risk of
stroke or death)
n Weight gain
n Gastrointestinal side effects (abdominal pain, nau-
sea, vomiting, diarrhea, gassiness, and bloating)
n Edema (fluid in legs and ankles)
n Increase in “bad” cholesterol (LDL)
Uncommon n Congestive heart failure
n Anemia (low red blood cell counts)
n Allergic reactions
Very Raren Thrombocytopenia (low blood platelet counts)
n Lactic acidosis (build up of acid in the blood)
n Leucopenia (low white blood cell counts)
n Macular edema (eye problems)
n Liver disease/liver failure
will encourage you to adjust the doses of your med-icines based on the blood sugar readings you takeyourself.
If you have good health insurance, diabetes self-management programs are usually accessible. Suchprograms (which can be expensive) usually include adietician or nutritionist, exercise experts, and doctorsthat specialize in diabetes care (endocrinologists).
The team may also include a cardiologist, neurolo-gist, ophthalmologist, kidney expert, and a foot spe-cialist. You will also get training in self-glucosemonitoring and other self-care.
A conscientious primary care doctor whose practicehas support staff with diabetes training can do just asgood a job at managing people with the disease as aformal program. People without insurance or thosewith inadequate coverage should find such a doctorsince they have limited access to formal diabetes pro-grams.
Safety and Side Effects
All the diabetes medicines can have adverse effects.Those vary from drug class to drug class and medi-cine to medicine. Generally, the risks posed by dia-betes drugs are not an impediment to using them ifyou truly need one. That is, for most people, the ben-efits of the drugs clearly outweigh the risks.
Even so, adverse side effects can keep people fromtaking their diabetes pills. On average, 10 to 20 per-cent of people with diabetes stop taking their pillsdue to side effects. Significant side effects occur inabout 1 of every 100 people taking diabetes pills.
Most notably, some diabetes drugs can cause lowblood sugar, or hypoglycemia. This is a vexing sideeffect and one that often leads doctors to prescribeone diabetes drug over another. The symptoms ofhypoglycemia are listed in the box to the left.Unfortunately, some people do not have minorsymptoms to warn them that their blood sugar is get-ting dangerously low. That is one reason your doctorwill emphasize to you that you must check yourblood sugar regularly.
The other big, worrisome side effect of some of thediabetes drugs is weight gain, or difficulty losingweight. Since many people with diabetes are tryingto lose weight, this side effect can be particularlyfrustrating.
The box on this page gives a general run down of theside effects linked to diabetes drugs. The potentialside effects of each drug are discussed at more lengthin the next section, which also compares the drugsacross a range of criteria (including their cost) andpresents our Best Buys choices.

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 13
The good news is that the diabetes drugs have beencompared to each other in many good studies, andsome of the drugs have been used for years andhelped millions of people. The bad news is thatmost of the careful studies have not tracked peo-ple, or the long-term effects of the drugs, overmany years. Most followed people for just a yearor less.
Even so, the studies help clarify the benefits andadverse effects of the drugs, and signal typical andexpected effects among a group of people with dia-betes. But very importantly, such studies do notreveal how a specific person with diabetes willrespond to a particular drug. Only your doctor andyou can decide precisely which drug or drug combi-nation is best for you given your health status,weight, other medical needs, and the severity of yourdiabetes.
Tables 2, 3 and 4 on pages 16 to 20 summarize thecomparative evidence on the diabetes drugs. Thetables reflect an evaluation of the results from morethan 200 studies. Table 2 presents summary evidenceof the various classes of drugs. Table 3 is more spe-cific, with detailed information on the individualdrugs. As such, Table 3 takes a bit more time to fig-ure out. But it contains information unique to thisreport and which may be valuable for your treatmentdecision.
Table 4 presents a run-down of the pros and cons ofeach class of diabetes. The tables contain materialthat is duplicative. On balance, though, they giveyou three ways of assessing the important differ-ences among the diabetes drugs.
Our evaluation leads to the following overall conclu-sions:
n The newer drugs are no better. The thiazolidine-diones, meglitinides, alpha-glucosidase inhibitors,and dipeptidyl peptidase 4 inhibitors (all morerecently developed) are no more effective than thesulfonylureas and metformin (which have beenaround for decades). In fact, three of the newermedicines – acarbose, miglitol, and nateglinide –decrease HbA1c less than the other drugs.
n The newer drugs are no safer. As discussed in theprevious section and presented in Tables 2, 3 and4, all diabetes pills have the potential to causeadverse effects – both minor and serious.
n Metformin emerges as a superior diabetes drugbased on the available evidence. This medicinelowers HbA1c the same amount or more thanother drugs, does not cause weight gain, decreas-es low-density lipoprotein (LDL) and triglyc-erides, and appears to have the safest profilewhen comparing serious side effects in peoplewho do not have kidney, liver, or heart disease.As further discussed below, however, metformincan not be taken by everyone.
n Taking two diabetes drugs has a positive additiveeffect on reducing HbA1c. This is a major plus formany people with diabetes whose blood glucoseis not well controlled by a single drug. Thedownside is that taking two drugs poses a higherrisk of side effects. If lower doses of each drugare used in combination, the added risk of sideeffects can be reduced.
n The newer drugs are more expensive. The neweroral diabetes medicines cost many times morethan the older ones. (See Table 5.)
As mentioned earlier, the diabetes drugs have dis-tinctly different “safety profiles.” It’s this that maydrive your and your doctor’s decision – for initialand on-going treatment.
For example, the evidence clearly shows that the sul-fonylureas pose a higher risk of hypoglycemia thanmetformin or the thiazolidinediones (Avandia andActos). Between 9 and 22 percent of people takingone of the sulfonylurea drugs can expect to have anepisode of potentially dangerous low blood sugar,compared to zero to 7 percent taking metformin, forexample.
The risk of hypoglycemia is about the same for thesulfonylureas and repaglinide, but two recent stud-ies suggest that repaglinide may cause less hypo-glycemia in the elderly or in people who skipmeals.
Choosing an Oral Diabetes Medicine – Our Picks

14 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
One of the newer classes of drugs poses an elevatedrisk of heart failure. Evidence overwhelmingly indi-cates that the thiazolidinediones (Avandia andActos) pose a 1.5 to 2 times increased risk of conges-tive heart failure compared to other diabetes medi-cines. Between 1 and 3 in a 100 people without ahistory of heart disease will develop the condition.In contrast, metformin and the sulfonylureas do notraise the risk of heart failure in any significant waycompared to the general risk of this conditionamong people with diabetes, which is higher thannormal.
Because of the mounting evidence on this link, inMay 2007 the FDA requested that the manufactur-ers of Actos and Avandia put a high-profile “blackbox” warning about the risk of heart failure onthe labels for the two drugs. If you are taking oneof these medicines and have swelling of any partof your body, sudden weight gain, or breathingproblems, you should contact your doctor imme-diately.
In addition, Avandia has also recently been associat-ed with a possibly higher risk of heart attack. In astudy that received widespread media attention inthe spring of 2007, Avandia was associated with a 43percent greater risk of heart attack compared to otherdiabetes pills (though the absolute risk was still a rel-atively low 1 to 3 in a 100 for people who had dia-betes but no heart disease).
Notably, however, other studies comparing Avandiawith other diabetes drugs or placebo have not foundsuch a risk, and the type of study used to make theconnection has limitations. The upshot is that moreresearch is needed and no definitive conclusions canyet be reached about heart attack risks posed byAvandia.
If your doctor prescribes Avandia, we join othergroups (including the American DiabetesAssociation, American Heart Association, andAmerican College of Cardiology) in urging you totalk to him or her about the risks and benefits andthe appropriateness of this choice. If in addition todiabetes, you have multiple risk factors for heart dis-ease, we would advise against Avandia until furtherstudies clarify whether it poses any heightened riskof heart attack.
Avandia also has been recently associated with anincreased risk of fractures of the wrist and arm inwomen. This unexpected finding is being furtherinvestigated and needs confirmation.
As good as it looks in other ways, metformin hasbeen associated with rare occurrences of lactic acido-sis – the build up of lactic acid in the blood, whichcan lead to severe consequences. This rare riskappears to exist mostly for diabetics who also havemoderate kidney disease and/or heart failure. As aresult, such patients should not be prescribed met-formin.
Minor but annoying side effects may also play a rolein your choice of a diabetes medicine. For example,gastrointestinal side effects – including bloating, gas,nausea, and diarrhea – are more frequent with met-formin and particularly with acarbose than the otherdrugs.
Our Picks and Recommendations
Taking effectiveness, safety, side effects, dosing, andcost into consideration, we have chosen the follow-ing as Consumer Reports Best Buy Drugs if your doc-tor has decided that you need medicine to controlyour diabetes:
n Metformin – alone or in combination with glip-izide or glimepiride
n Glipizide and Glipizide Sustained Release – aloneor in combination with metformin
n Glimepiride – alone or in combination with met-formin
All these medicines are available as low-cost gener-ics, either alone or in combination. (See Table 5.) Inrecent years, a strong medical consensus hasemerged in the U.S., Europe, and Australia that mostnewly diagnosed people with diabetes who need amedicine should first be prescribed metformin alone.
Based on the systematic evaluation of diabetes drugsthat forms the basis for this report, we concur withthat advice: metformin first, unless your health sta-tus prevents it. If metformin fails to bring your blood

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 15
glucose into normal range, you may need a seconddrug. Most commonly that should be one of twoother Best Buys we have chosen above. Should eitherof those trigger hypoglycemia, Actos may be anoption you and your doctor will want to consider.
If you are unable to take metformin or do not tolerateit well, you face a choice of one of the sulfonylureasor a newer medicine. Despite the elevated risk ofhypoglycemia, we recommend trying glipizine orglimepiride. If either of those triggers hypoglycemia,talk with your doctor about Actos. If glipizide,glimepiride, or Actos alone fail to bring your bloodglucose into control and keep your HbA1c below 7percent, your doctor will likely recommend a seconddrug.
If upon initial diagnosis your glucose and HbA1c arequite high, you may be prescribed a combination oftwo drugs at the beginning of treatment – usuallymetformin plus a sulfonylurea. Another optionwould be metformin plus Actos.
Avandia may still be a viable option for some people.But as indicated above, its present disadvantagescompel a clear rationale for its choice, either as asolo treatment or in combination with another drug.If your doctor prescribes Avandia as the first drug
you take after diagnosis, you should question thatdecision. There are some clinical circumstances inwhich this would be a wise choice, but only for asmall percentage of people.
Unfortunately, Actos and Avandia have been heavilypromoted to doctors and consumers in the U.S. As aresult, both drugs have been over-prescribed to peo-ple who should instead be taking metformin and/or asulfonylurea. Both drugs have been marketed specif-ically to minorities as well, but there is no good evi-dence that any diabetes medicine is more effective orsafer in African-Americans and Hispanic orAmerican Indian patients than in others.
Januvia is a promising new addition to the diabetesmedicine cabinet. But it has not yet been well stud-ied. It is not as effective at lowering blood glucoseand HbA1c as other diabetes drugs, but it has notbeen linked to date with weight gain or hypo-glycemia either - a plus. Until it has been better stud-ied and prescribed more broadly over a longer peri-od, we would not advise it as a first-line drug. It isalso expensive.
Finally, as a reminder, if your diabetes is not con-trolled by pills, you may have to take insulin or oneof the other drugs available by injection only.

Source: Bolen S., et al, Comparative Effectiveness and Safety of Oral Diabetes Medications for Adults with Type 2 Diabetes.http://www.effectivehealthcare.ahrq.gov
Definitions: “No difference” means that adequate or good studies have been done and when considered as a whole have found no difference between thesetwo categories of drugs. “Not enough evidence” means not enough studies have been done, or the studies that have been done are not good enough towarrant a judgment about any differences between these two classes of drugs.
1. For repaglinide only. 2. Pioglitizone (Actos) decreased triglycerides while rosiglitizone (Avandia) increased triglycerides; thus, Actos showed similar effects to the sulfonylureas
while Avandia was worse than the sulfonylureas. But no direct comparisons were available to draw firm conclusions. 3. Pioglitizone (Actos) was better than metformin while rosiglitizone (Avandia) was worse.
16 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Table 2. Summary of Comparative Effectiveness of Diabetes Drugs
Outcome Sulfonylureas vs.Metformin
Sulfonylureas vsThiazolidinediones
Sufonylureas vs. Meglitinide1
Metformin vs. Thiazolidinediones
Hemoglobin A1c No difference No difference No difference No difference
Weight Metformin better No difference No difference Metformin better
Blood Pressure No difference No difference Not enough evidence No difference
LDL (bad) cholesterol Metformin better Sulfonylureas better No difference Metformin better
HDL (good)cholesterol No difference Thiazolidinediones better No difference
Thiazolidinedionesbetter
Triglycerides Metformin better No difference2 No difference One thiazolidinedione
better3
Risk of Hypoglycemia Metformin better Thiazolidinediones better No difference No difference
Risk of GI problems Sulfonylureas better Not enough evidence Not enough evidence Thiazolidinediones
better
Risk of Congestive Heart Failure No difference Sulfonylureas better Not enough evidence Metformin better
Risk of Anemia Not enough evidence Sulfonylureas better Not enough evidence Metformin better
Risk of Edema (fluidbuild-up) Not enough evidence Sulfonylureas better Not enough evidence Metformin better

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 17
Table 3. Effects of Diabetes Drugs on Specific Measures
A down arrow (t) means a decrease or decline; an up arrow (s) means increase; and a diamond (u) means nomeaningful effect or change. IE = Insufficient Evidence. Brand names are not given for drugs available as generics.
AveragepointreductionHbA1c (percent)
Averagepointchange inbloodpressure(mmHg)
Averageabsolutechange inLDLcholesterol(mg/dL)
Averageabsolutechange inHDLcholesterol(mg/dL)
Averageabsolute change inTriglycerides(mg/dL)
Risk ofHypo-glycemia(% ofpeople)1
Averagechange inweight (lbs)
Sulfonylureas
Glyburide t 1.3-1.8 u u u t 10-20 10-22% s 5-10
Glipizide t 1.3-1.8 u u u t 10-20 10-15% s 5-10
Glimepiride t 1.3-1.8 u u u t 10-20 9-14% s 5-10
Biguanides
Metformin t 0.9-1.4 u s 5-7 u t 15-25 0-7% u
Thiazolidinediones
Pioglitazone(Actos)
t 0.8-1.2 u s 8-12 s 5 t 35-45 0-3% s 5-10
Rosiglitazone(Avandia)
t 0.9-1.4 u s 12-15 s 3 s 10-20 4-11% s 5-10
Meglitinides
Repaglinide(Prandin)
t 0.8-2.0 IE2 u u t 10-15 11-32% s 5-10
Nateglinide(Starlix)
t 0.3-0.8 IE IE IE IE 13%3 IE
Alpha-glucosidase inhibitors
Acarbose4
(Precose)t 0.6-0.9 IE u u t 10-15 0-5% u
Miglitol4
(Glyset)t 0.4-0.9 IE IE IE IE IE IE
Dipeptidyl peptidase 4 inhibitor
Sitagliptin5
(Januvia) t 0.6-0.8 IE u u u Low u

18 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Table 3. Effects of Diabetes Drugs on Specific Measures (continued)
A down arrow (t) means a decrease or decline; an up arrow (s) means increase; and a diamond (u) means nomeaningful effect or change. IE = Insufficient Evidence. Brand names are not given for drugs available as generics.
AveragepointreductionHbA1c (percent)
Averagepointchange inbloodpressure(mmHg)
Averageabsolutechange inLDLcholesterol(mg/dL)
Averageabsolutechange inHDLcholesterol(mg/dL)
Averageabsolute change inTriglycerides(mg/dL)
Risk ofHypo-glycemia(% ofpeople)1
Averagechange inweight (lbs)
Selected Combinations
Metformin +sulfonylurea(Glucovance,Metaglip)
t 1.7-2.3 IE t 5-7 u t 20-40 14-28% s 5-10
Metformin +rosiglitazone(Avandamet)
t 1.3-2.0 IE s 12-15 s 3 u 0-7% s 5-10
Sulfonylurea +rosiglitazone(Avandaryl)
t 1.7-2.3 IE s 10-12 s 3 u 18-30% s 5-10
Source: Bolen S., et al, Comparative Effectiveness and Safety of Oral Diabetes Medications for Adults with Type 2 Diabetes.http://www.effectivehealthcare.ahrq.gov
Definitions/Key: u No meaningful change; t Significant decrease; s Significant increase; IE=insufficient data; lbs=pounds; mg/dl=milligrams perdeciliter of blood; mmHg=millimeters mercury; HbA1c=hemoglobin A1c; LDL=low-density lipoprotein cholesterol; HDL= high-density lipoprotein choles-terol.
1. Results mostly come from short-duration studies lasting 3 months to 1 year. There are only a few studies longer than one year which show slightly high-er rates of hypoglycemia but similar comparative results.
2. IE = insufficient evidence for this drug on this measure to reach any meaningful conclusions. 3. Results based on one short-term study (<1 year). 4. Results are based on data from a systematic review plus a large randomized study. 5. Preliminary data based on product label and a monograph by the Veteran’s Administration’s national pharmacy service.

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 19
Table 4. Advantages and Disadvantages of the Diabetes Drugs
Advantages: Disadvantages:
The sulfonylureas (glyburide, glimepiride, glipizide)
- Fast onset of action - No effect on blood pressure - No effect on LDL cholesterol- Convenient dosing- Low cost
- Weight gain (5 to 10 pounds on average)- Heightened risk of hypoglycemia - Glyburide has slightly higher risk of hypoglycemia com-
pared with glimepiride and glipizide
Metformin
- Low risk of hypoglycemia - Not linked to weight gain - Good effect on LDL cholesterol - Good effect on triglycerides- No ill effect on blood pressure- Low cost
- Higher risk of GI side effects (nausea and diarrhea)- Can not be taken by people with diabetes who have mod-
erate kidney disease or heart failure because of risk of lac-tic acid build-up
- Less convenient dosing
The alpha-glucosidase inhibitors (acarbose, miglitol)
- Slightly lower risk of hypoglycemia compared to sul-fonylureas
- Not associated with weight gain - Decreases triglycerides - No adverse effects on cholesterol
- Less effective than most other diabetes pills in loweringHbA1c
- Higher risk of GI side effects than other diabetes pillsexcept metformin
- Inconvenient dosing - High cost
The thiazolidinediones (Actos, Avandia)
- Low risk of hypoglycemia- Slight increase in “good” (HDL) cholesterol - Actos linked to decreased triglycerides - Convenient dosing
- Higher risk of heart failure- Weight gain (5 to 10 pounds) - Link to higher risk of edema (fluid build-up)- Link to higher risk of anemia - Increase in “bad” (LDL) cholesterol- Avandia linked to increased triglycerides and possibly
(not yet confirmed) higher risk of heart attack - Slower onset of action - Rare risk of liver problems; required monitoring - High cost

20 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Table 4. Advantages and Disadvantages of the Diabetes Drugs
Advantages: Disadvantages:
The meglitinides (nateglinide, repaglinide)
- No bad effect on cholesterol - Rapid onset of action
- Repaglinide associated with risk of hypoglycemia andweight gain similar to the sulfonylureas
- Nateglinide has less effect on HbA1c- Inconvenient dosing- High cost
Januvia (sitagliptin)*
- Apparent low risk of hypoglycemia - Few known side effects (but new drug)- No weight gain - Convenient dosing
- Reduces HbA1c less than several other diabetes drugs- May only be valuable as second drug if needed until
more research is conducted; initial treatment use only ifunable to take other diabetes drugs
- Less data on potential side effects compared to olderdrugs
- High cost
* This is a new drug approved in October 2006. There is less research and experience with it than with other diabetes medicines. In addition, no studieshave followed patients taking it for longer than one year.
Sources: (1) Bolen S., et al, Comparative Effectiveness and Safety of Oral Diabetes Medications for Adults with Type 2 Diabetes. http://www.effectivehealth-care.ahrq.gov; (2)“Oral hypoglycemics in the treatment of type 2 diabetes”; Therapeutic Insights – American Medical Association (June 2007); Januvialabeling and available material

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 21
Table 5: Cost of Diabetes Drugs
Generic Name and Dose
Brand Name (or Generic)
Number of Pills (Per day)1 Total Daily Dose1 Average Monthly
Cost2
Glyburide 5 mg tablet Generic One 5 mg $12
Glyburide 5 mg tablet Micronase One 5 mg $41
Glyburide 5 mg tablet Diabeta One 5 mg $31
Glyburide 5 mg tablet+ 2.5 mg tablet
Generic One 7.5 mg $23
Glyburide 5 mg tablet+ 2.5 mg tablet
Micronase One 7.5 mg $69
Glyburide 5 mg tablet+ 2.5 mg tablet
Diabeta One 7.5 mg -
Glyburide 5 mg tablet Generic Two 10 mg $39
Glyburide 5 mg tablet Micronase Two 10 mg $81
Glyburide 5 mg tablet Diabeta Two 10 mg $62
Glyburide micronized3 mg tablet
Glynase One 3 mg $42
Glyburide micronized3 mg tablet
Generic One 3 mg $12
Glyburide micronized6 mg tablet
Glynase One 6 mg $66
Glyburide micronized6 mg tablet
Generic One 6 mg $19
Glyburide micronized6 mg tablet +1.5 mg tablet
Glynase One 7.5 mg $89
Glyburide micronized6 mg tablet +1.5 mg tablet
Generic One 7.5 mg $29
Glipizide 5 mg tablet Glucotrol One 5 mg $22
Glipizide 5 mg tablet Generic One 5 mg $9
Glipizide 10 mg tablet Glucotrol One 10 mg $34
Glipizide 10 mg tablet Generic One 10 mg $11

22 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Table 5: Cost of Diabetes Drugs (continued)
Generic Name and Dose
Brand Name (or Generic)
Number of Pills (Per day)1 Total Daily Dose1 Average Monthly
Cost2
Glipizide 10 mg tablet Glucotrol Two 20 mg $68
Glipizide 10 mg tablet Generic Two 20 mg $22
Glipizide 5 mg tablet,sustained release
Glucotrol One 5 mg $22
Glipizide 5 mg tablet,sustained release
Generic One 5 mg $14 to $17
Glipizide 5 mg + 2.5mg tablets, sustained release
Glucotrol One 7.5 mg $43
Glipizide 5 mg + 2.5mg tablets, sustained release
Generic One 7.5 mg $28
Glipizide 10 mg tablet, sustained release
Glucotrol One 10 mg $39
Glipizide 10 mg tablet, sustained release
Generic One 10 mg $23 to $29
Glipizide 10 mg + 5tablets, SustainedRelease
Glucotrol One 15 mg $61
Glipizide 10 mg + 5tablets, sustained release
Generic One 15 mg $43
Glipizide 10 mgtablets, sustained release
Glucotrol Two 20 mg $78
Glipizide 10 mgtablets, sustained release
Generic Two 20 mg $46 to $58
Glimepiride 1 mgtablet
Amaryl One 1 mg $20
Glimepiride 1 mgtablet
Generic One 1 mg $12
Glimepiride 2 mgtablet
Amaryl One 2 mg $29

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 23
Table 5: Cost of Diabetes Drugs (continued)
Generic Name and Dose
Brand Name (or Generic)
Number of Pills (Per day)1 Total Daily Dose1 Average Monthly
Cost2
Glimepiride 2 mg tablet
Generic One 2 mg $18
Glimepiride 4 mg tablet
Amaryl One 4 mg $51
Glimepiride 4 mg tablet
Generic One 4 mg $27
Metformin 500 mg tablet
Glucophage Three 1500 mg $102
Metformin 500 mg tablet
Generic Three 1500 mg $38
Metformin 1000 mg tablet
Glucophage Two 2000 mg $134
Metformin 1000 mg tablet
Generic Two 2000 mg $45
Metformin 1000 and500 mg tablets
Glucophage Three 2550 mg $168
Metformin 1000 and500 mg tablets
Generic Three 2500 mg $58
Metformin 850 mg tablet
Glucophage Three 2550 mg $167
Metformin 850 mg tablet
Generic Three 2550 mg $60
Sitagliptin 100 mg tablet
Januvial One 100 mg $208
Sitagliptin 50 mg tablet
Januvia One 50 mg $201
Pioglitazone 15 mg tablet
Actos One 15 mg $142
Pioglitazone 30 mg tablet
Actos One 30 mg $221
Pioglitazone 45 mg tablet
Actos One 45 mg $241
Rosiglitazone 2 mg tablet
Avandia Two 4 mg $180

24 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Table 5: Cost of Diabetes Drugs (continued)
Generic Name and Dose
Brand Name(or Generic)
Number of Pills (Per day)1 Total Daily Dose1 Average Monthly
Cost2
Rosiglitazone 4 mgtablet
Avandia One 4 mg $131
Rosiglitazone 4 mgtablet
Avandia Two 8 mg $262
Rosiglitazone 8 mgtablet
Avandia One 8 mg $233
Repaglinide 1 mgtablet
Prandin Three 3 mg $162
Repaglinide 1 mg and0.5 mg tablet
Prandin Three 4.5 mg $321
Repaglinide 2 mgtablet
Prandin Three 6 mg $156
Nateglinide 60 mgtablet
Starlix Three 180 mg $157
Nateglinide 120 mgtablet
Starlix Three 460 mg $162
Acarbose 50 mg tablet Precose Three 150 mg $106
Acarbose 50 mg plus25 mg tablets
Precose Three 225 mg $210
Acarbose 100 mgtablet
Precose Three 300 mg $124
Miglitol 50 mg tablet Glyset Three 150 mg $99
Miglitol 50 mg plus25 mg tablets
Glyset Three 225 mg $195
Miglitol 100 mg tablet Glyset Three 300 mg $113
Metformin+glipizide250 mg/2.5 mg
Metaglip Two 250/2.5-500/5 mg $71
Metformin+glipizide250 mg/2.5 mg
Generic Two 500/5 mg $57
Metformin+glipizide500 mg/2.5 mg
Metaglip Two 1000/5 mg $78
Metformin+glipizide500 mg/2.5 mg
Generic Two 1000/5 mg $63

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 25
Table 5: Cost of Diabetes Drugs (continued)
Generic Nameand Dose
Brand Name(or Generic)
Number of Pills (Per day)1 Total Daily Dose1 Average Monthly
Cost2
Metformin+glipizide500 mg/5 mg
Metaglip Two 1000/10 mg $79
Metformin+glipizide500 mg/5 mg
Generic Two 1000/10 mg $62
Metformin+glyburide250 mg/1.25 mg
Glucovance Two 500/2.5 mg $72
Metformin+glyburide250 mg/1.25 mg
Generic Two 500/2.5 mg $44
Metformin+glyburide500 mg/2.5 mg
Glucovance Two 1000/5 mg $86
Metformin+glyburide500 mg/2.5 mg
Generic Two 1000/5 mg $47
Metformin+glyburide500 mg/5 mg6 Glucovance Three 1500/15 mg $129
Metformin+glyburide500 mg/5 mg6 Generic Three 1500/15 mg $71
Pioglitazone+metformin 15mg/850 tablet
Actoplus Met One 850/15 mg $105
Pioglitazone+metformin 15mg/500 tablet
Actoplus Met Two 1000/30 mg $206
Pioglitazone+metformin 15mg/850 tablet
Actoplus Met Two 1500/45 mg $210
Rosiglitazone+glimepiride 4mg/1 mg tablet
Avandaryl One 4/1 mg $144
Rosiglitazone+glimepiride 4mg/2 mg tablet
Avandaryl One 4/2 mg $150
Rosiglitazone+glimepiride 4mg/4 mg tablet
Avandaryl One 4/4 mg $148
Rosiglitazone+glimepiride 4mg/8 mg tablet
Avandaryl One 4/4 mg $148

26 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Table 5: Cost of Diabetes Drugs (continued)
Generic Name and Dose
Brand Name(or Generic)
Number of Pills (Per day)1 Total Daily Dose1 Average Monthly
Cost2
Rosiglitazone+metformin 1 mg/500 mg
Avandamet Two 2/1000 mg $83
Rosiglitazone +metformin 1 mg/500 mg
Avandamet Two 4/1000 mg $152
Rosiglitazone +metformin 2 mg/500 mg
Avandamet Two 4/2000 mg $161
Rosiglitazone +metformin 4 mg/1000 mg
Avandamet Two 8/2000 mg $262
Sitagliptin +metformin 50/500
Janumet Two 100/1000 $106
Sitagliptin +metformin 50/1000
Janumet Two 100/1000 $104
1. As commonly or usually recommended. 2. Prices reflect nationwide retail average for May 2007, rounded to the nearest dollar. Information derived by Consumer Reports Best Buy Drugs from data provided byWolters Kluwer Health, Pharmaceutical Audit Suite.

Best Buy Drug Recommendations
Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 27
Talking With Your DoctorIt's important for you to know that the information we present in this report is not meant to substitute for a doctor'sjudgment. But we hope it will help your doctor and you arrive at a decision about which diabetes drug and at whatdose is best for you.
Bear in mind that many people are reluctant to discuss the cost of medicines with their doctors and that studies showdoctors do not routinely take price into account when prescribing medicines. Unless you bring it up, your doctors mayassume that cost is not a factor for you.
Many people (including many physicians) also believe that newer drugs are always or almost always better. While that'sa natural assumption to make, the fact is that it's not true. Studies consistently show that many older medicines areas good as, and in some cases better than, newer medicines. Think of them as "tried and true," particularly when itcomes to their safety record. Newer drugs have not yet met the test of time, and unexpected problems can and docrop up once they hit the market.
Of course, some newer prescription drugs are indeed more effective and safer. Talk with your doctor about the plusesand minuses of newer versus older medicines, including generic drugs.
Prescription medicines go "generic" when a company's patents on a drug lapse, usually after about 12 to 15 years. Atthat point, other companies can make and sell the drug.
Generics are almost always much less expensive than newer brand name medicines, but they are not lesser qualitydrugs. Indeed, most generics remain useful medicines even many years after first being marketed. That is why todayabout half of all prescriptions in the U.S. are for generics.
Another important issue to talk with your doctor about is keeping a record of the drugs you are taking. There are sev-eral reasons for this:
First, if you see several doctors, they may not always tell each other which drugs have been prescribed for you.
Second, it is very common for doctors today to prescribe several medicines for you before finding one that works wellor best, mostly because people vary in their response to prescription drugs.
Third, more and more people today take several prescription medications, nonprescription drugs and supplements allat the same time. Many of these interact in ways that can be very dangerous.
And fourth, the names of prescription drugs—both generic and brand—are often hard to pronounce and remember.
For all these reasons, it's important to keep a list of the drugs you are taking, both prescription and nonprescriptionand including dietary supplements.
Always be sure, too, that you understand the dose of the medicine being prescribed for you and how many pills youare expected to take each day. Your doctor should tell you this information. When you fill a prescription at the phar-macy, or if you get it by mail, you may want to check to see that the dose and the number of pills per day on the pillbottle match the amounts that your doctor told you.

28 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
Our evaluation is based in large part on an independ-ent review of the scientific evidence on the effective-ness, safety, and adverse effects of the oral diabetesmedicines conducted by the Johns Hopkins University-evidence based Practice Center under contract number290-02-0018 with the Agency for Healthcare Researchand Quality. This analysis reviewed hundreds of stud-ies, including those conducted by the drugs’ manufac-turers. A synopsis of the results of this analysis, writ-ten by the researchers at Johns Hopkins, forms thebasis for portions of this report.
However, no statement in this report should be con-strued as the official position of the Johns HopkinsEvidence-based Practice Center, the Agency forHealthcare Research and Quality, or the U.S.Department of Health and Human Services. In par-ticular, none of those entities played any role in ourselection of the Best Buy diabetes drugs. ConsumersUnion and Consumer Reports Best Buy Drugs is sole-ly responsible for those, and for all other specificadvice and recommendations in this report.
Additional sources were also used in writing thisreport. Those include:
n An analysis of selected classes of diabetes drugsconducted by the Drug Effectiveness ReviewProject (DERP), a 15-state initiative to evaluatethe comparative effectiveness and safety of hun-dreds of prescription drugs
n The results of three recent reviews of oral dia-betes drugs by the Cochrane Collaboration
n An American Medical Association monographon the oral diabetes drugs
n Diabetes: Treatment Options Report, an April2006 publication released by the CaliforniaHealthCare Foundation and prepared by theUniversity of California, Davis Center for HealthServices Research in Primary Care
n A Veteran’s Administration monograph on dia-betes drugs
n Recent guidelines issued by the American DiabetesAssociation and American College of Cardiology
n Selected recent articles in peer-reviewed journals(See References)
The prescription drug costs we site were obtainedfrom a healthcare information company that tracksthe sales of prescription drugs in the U.S. Prices for adrug can vary quite widely, even within a single cityor town. All the prices in this report are nationalaverages based on sales of prescription drugs in retailoutlets. They reflect the cash price paid for a month'ssupply of each drug in May 2007.
Consumers Union and Consumer Reports selected theBest Buy Drugs using the following criteria. The drughad to:
n Be as effective or more effective than other oraldiabetes medicines
n Have a safety record equal to or better than otherdiabetes medicines
n Cost roughly the same or less than other diabetesmedicines
The Consumers Reports Best Buy Drugs methodologyis described in more detail in the methods section atwww.CRBestBuyDrugs.org.
How We Conducted Our Review of the Diabetes Drugs

Treating Type 2 Diabetes: The Oral Diabetes Drugs • Consumer Reports Best Buy Drugs • 29
Sharing this ReportThis copyrighted report can be freely downloaded, reprinted and disseminated for individual noncommercial usewithout permission from Consumers Union or Consumer Reports® magazine as long as it clearly attributed toConsumer Reports Best Buy Drugs.® We encourage its wide dissemination as well, for the purpose of informingconsumers. However, Consumers Union does not authorize the use of its name or materials for commercial, mar-keting, or promotional purposes. Any organization interested in broader distribution of this report should contactWendy Wintman at [email protected]. Consumer Reports Best Buy Drugs® is a trademarked property ofConsumers Union. All quotes from the material should site Consumer Reports Best Buy Drugs ® as the source.
© Consumers Union 2007
Consumers Union, publisher of Consumer Reports® magazine, is an independent and nonprofit organization whosemission since 1936 has been to provide consumers with unbiased information on goods and services and to cre-ate a fair marketplace. Its website is www.consumer.org. The magazine's website is www.consumerreports.org.
Consumer Reports Best Buy Drugs® is a public education project administered by Consumers Union. Two outsidesources of generous funding made the project possible. They are a major grant from the Engelberg Foundation, aprivate philanthropy, and a supporting grant from the National Library of Medicine, part of the National Institutesof Health. A more detailed explanation of the project is available at www.CRBestBuyDrugs.org.
We followed a rigorous editorial process to ensure that the information in this report and on the Consumer ReportsBest Buy Drugs website is accurate and describes generally accepted clinical practices. If we find, or are alerted to,an error, we will correct it as quickly as possible. However, Consumer Reports and its authors, editors, publishers,licensors and any suppliers cannot be responsible for medical errors or omissions, or any consequences from theuse of the information on this site. Please refer to our user agreement at www.CRBestBuyDrugs.org for furtherinformation.
Consumer Reports Best Buy Drugs should not be viewed as a substitute for a consultation with a medical or healthprofessional. This report and the information on www.CRBestBuyDrugs.org are provided to enhance your commu-nication with your doctor, rather than to replace it.
About Us

30 • Consumer Reports Best Buy Drugs • Treating Type 2 Diabetes: The Oral Diabetes Drugs
References1. Bolen S., et al, Comparative Effectiveness and Safety of Oral Diabetes Medications
for Adults with Type 2 Diabetes. (July 2007) Report sponsored by the Agency forHealthcare Research and Quality. Available at: www.effectivehealthcare.ahrq.gov/reports/final.cfm.
2. Bolen S., et al, “Systematic review: comparative effectiveness and safety of oralmedications for type 2 diabetes mellitus,” Ann. of Int. Med. (September 18, 2007);Web published in advance of print publication, July 16, 2007. Available atwww.annals.org/cgi/content/full/ 0000605-200709180-00178V1.
3. “Standards of Medical Care in Diabetes–2007,” American Diabetes AssociationPosition Statement. Diabetes Care 2007 30: S4-S41.
4. Cutler, E.D. and Prescott, P., Diabetes: Treatment Options Report (April 2006)Reports prepared for the California HealthCare Foundation. www.chcf.org
5. Oral Hypoglycemics in the Treatment of Type 2 Diabetes, American MedicalAssociation Therapeutic Insights (June 2007).
6. American Diabetes Association: Diagnosis and Classification of Diabetes Mellitus.Diabetes Care 2007 30: S42-47.
7. All About Diabetes, American Diabetes Association. Accessed July 2, 2007.http://www.diabetes.org/about-diabetes.jsp.
8. Guidelines for Clinical Practice for the Management of Diabetes Mellitus, AmericanAssociation of Clinical Endocrinologists, American College of Endocrinology, TheAmerican Association of Clinical Endocrinologists Medical (May/June 2007).Available at www.aace.com/pub/pdf/guidelines/DMGuidelines2007.pdf.
9. National PBM Drug Monograph – Sitagliptin (Januvia), (November 2006); Veteran’sAdministration Pharmacy Benefit Management Strategic Health Care Group.Available at www.pbm.va.gov/monograph/sitagliptin.pdf.
10. Diabetes Overview, National Diabetes Information Clearinghouse. Accessed June22, 2007. www.diabetes.niddk.nih.gov/dm/pubs/overview/index.htm.
11. Drugs for Diabetes – Treatment Guidelines, The Medical Letter (August 2005) Vol. 3,Issue 36.
12. National Diabetes Fact Sheet – U.S. 2005, Centers for Disease Control andPrevention. Accessed June 22. www.cdc.gov/diabetes.
13. Nathan, D. “Finding new treatments for diabetes – how many, how fast, howgood,” N Engl J Med (February 1, 2007): Vol. 356, No 5, pages 437-440
14. Gregg, E.W. et al, “Mortality trends in men and women with diabetes, 1971-2000,”Annals of Internal Med. (June 18, 2007) Published online; print version datedAugust 7, 2007; Vol. 147, No. 3.
15. Burnet, D.L. et al, “Preventing diabetes in the clinical setting,” J. Gen Int. Med. (2006)Vol. 21, pages 84-93
16. Franco, O.H. et al, “Associations of diabetes mellitus with total life expectancy andlife expectancy with and without cardiovascular disease,” Arch. Internal Med.(June 11, 2007) Vol. 167, pages 1145-1151
17. Barr, E.L. et al, “Risk of cardiovascular and all-cause mortality in individuals withdiabetes mellitus, impaired fasting glucose and impaired glucose tolerance,” TheAustralian Diabetes, Obesity, and Lifestyle Study. Circulation (July 10, 2007). Vol.116.
18. Hampton, T., “Diabetes drugs tied to fractures in women,” JAMA (April 18, 2007):Vol. 297, No. 15, page 1645.
19. Mitka, M., “Report quantifies diabetes complications,” JAMA (June 6, 2007): Vol.297, No 21, pages 2337-2338.
20. Dabelea, D. et al, “Incidence of diabetes in youth in the United States,” JAMA (June27, 2007): Vol. 297, No 24, pages 2716-2724.
21. Amori, R.E. et al, “Efficacy and safety of incretin therapy in type 2 diabetes – sys-tematic review and meta-analysis,” JAMA (July 11, 2007): Vol. 298, No. 2, pages194-206
22. “Sitagliptin/Metformin (Janumet) for Type 2 Diabetes,” The Medical Letter on Drugsand Therapeutics (June 4, 2007): Vol. 49, Issue 1262, page 1.
23. “Intensive blood-glucose control with sulphonylureas or insulin compared withconventional treatment and risk of complications in patients with type 2 diabetes,”The UK Prospective Diabetes Study Group.” Lancet (1998): Vo. 352 (9131), pages837-853.
24. “A randomized trial of efficacy of early addition of metformin in sulfonylurea-treated type 2 diabetes.” The UK Prospective Diabetes Study Group. Diabetes Care(1998): Vol 21 (1), pages 87-92.
25. “Third Report of the National Cholesterol Education Program (NCEP) Expert Panelon Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (AdultTreatment Panel III),” Circulation (2002): Vol. 106(25), pages 3143-3421.
26. “Global guidelines for type 2 diabetes: recommendations for standard, compre-hensive, and minimal care. Diabetes Med (2006); Vol. 23(6), pages 579-593.
27. Chobanian, A.V. et al, “The Seventh Report of the Joint National Committee onPrevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC7 Report.” JAMA (2003): Vol. 289(19), pages 2560-2572.
28. Holman R.R., et al, “A randomized double-blind trial of acarbose in type 2 diabetesshows improved glycemic control over 3 years,” (The UK Prospective DiabetesStudy). Diabetes Care (1999): Vol. 22(6), pages 960-964.
29. Inzucchi S.E., et al, “Oral antihyperglycemic therapy for type 2 diabetes: scientificreview,” JAMA (2002): Vol. 287(3), pages 360-372.
30. Salpeter S., et al, “Risk of fatal and nonfatal lactic acidosis with metformin use intype 2 diabetes mellitus,” Cochrane Database Sys. Rev. (2006)(1).
31. Van de Laar F.A., et al, “Alpha-glucosidase inhibitors for people with impaired glu-cose tolerance or impaired fasting blood glucose.” Cochrane Database Syst. Rev.(2006)(4).
32. Nesto R.W., et al. “Thiazolidinedione use, fluid retention, and congestive heart fail-ure: A consensus statement from the American Heart Association and AmericanDiabetes Association.” Circulation (December 9, 2003): Vol.108, pages 2941-2948.
33. Nissen S.E., et al, “Effect of rosiglitazone on the risk of myocardial infarction anddeath from cardiovascular causes,” N Engl J Med (2007) Vol. 356, pages 2457-2471.
34. Kahn S.E., et al., “ADOPT Study Group: Glycemic durability of rosiglitazone, met-formin, or glyburide monotherapy.” N Engl J Med. (2006): Vol. 355, pages 2427-2443.
35. Home P.D., et al, “Rosiglitazone evaluated for cardiovascular outcomes – an inter-im analysis, “ N Engl J Med. (2007)
36. Goldstein B.J. et al, “Effect of initial combination therapy with sitagliptin, a dipep-tidyl peptidase-4 inhibitor, and metformin on glycemic control in patients withtype 2 diabetes. Diabetes Care. (May 7, 2007) (E-pub ahead of print)
37. Dormandy JA, et al. Secondary prevention of macrovascular events in patientswith type 2 diabetes in the PROactive Study – a randomised controlled trial.”Lancet (2005): Vol. 366 (9493), pages 1279-89.
38. Papa G., et al, “Safety of type 2 diabetes treatment with repaglinide comparedwith glibenclamide in elderly people: a randomized, open-label, two-period, cross-over trial.” Diabetes Care (2006): Vol. 29, pages 1918-1920.
39. Damsbo, P. et al, “A double-blind randomized comparison of meal-related glycemiccontrol by repaglinide and glyburide in well-controlled type 2 diabetic patients,”Diabetes Care (1999): Vol.22, pages 789-94.
40. Vijan, S. et al, “Estimated benefits of glycemic control in microvascular complica-tions in type 2 diabetes,” Ann Intern Med (1997): Vol. 127, pages 788-795
41. Stettler. C. et al, “Glycemic control and macrovascular disease in types 1 and 2 dia-betes mellitus: meta-analysis of randomized trials,” Am Heart J. (2006): Vol. 152,pages 27-38.