trauma in relation to psychosis and hospital experiences in secure settings katherine berry, sarah...
TRANSCRIPT

Trauma in relation to psychosis and Trauma in relation to psychosis and hospital experiences in secure settingshospital experiences in secure settings
Katherine Berry, Sarah Ford,
Lorna-Jellicoe Jones and Gillian Haddock
University of Manchester
Lancashire Care NHS Foundation Trust

Background Background Well-established that psychosis and
hospitalisation can be distressing (e.g. Centofanti et al., 2005; Robins et al., 2005).
These experiences conceptualised as events that could trigger PTSD (Mueser et al., 2010).
PTSD in psychosis associated with a range of worse outcomes (e.g. Mueser et al., 2002).
Rates of psychosis- or hospital-related PTSD range from 11-67%.

Background Background Past 30 years has seen the closure of long-stay
institutions, but significant numbers still reside for long periods in secure settings (Schizophrenia Commission, 2012).
This population have high levels of symptoms and risk (Berry & Drake, 2010). Therefore possibly high rates of psychosis- or hospital-related PTSD.
Secure populations also typically have histories of interpersonal trauma and attachment difficulties (Berry & Drake, 2010).

Background Background Well-established that past trauma can increase
vulnerability to PTSD following subsequent trauma (e.g. Brewin et al., 2000).
Some evidence for the role of past trauma in psychosis-related and hospital-related PTSD (e.g. Centofanti et al., 2005).
Other moderating or mediating factors are equally important in the development of PTSD in the general literature (Brewin et al., 2000).
But these have been less well researched in the context of psychosis-related and hospital-related PTSD.

Background Background Earlier experiences of trauma are associated with
insecure attachment styles in adulthood (e.g. Berry et al., 2009).
Evidence of associations between insecure attachment and PTSD in people with psychosis and substance misuse (Picken et al., 2010), but no research looking specifically at psychosis- or hospital-related PTSD.
Recovery from psychosis has been associated with attachment style (e.g. Tait et al., 2004).

Background Background
Internal secure base which enables integration and processing of experiences of psychosis (Birchwood, 2003).
McGlashan et al (1976):
Integration – flexible thinking style which incorporates psychosis into everyday experience.
Sealing over – psychosis appraised as threatening and therefore recall avoided.

Background Background
Jackson et al’s (2004) first episode study found sealers were more likely to avoid intrusions. No relationship between recovery style and PTSD caseness, but only 9 sealers.
Mueser et al’s (2010) first episode study found those with PTSD syndrome had a more integrative coping style than those who did not.
Although sealing over may be adaptive in the short-term, it is associated with worse outcomes longer term (McGlashan, 1987).

Aims and hypotheses Aims and hypotheses To investigate rates of psychosis-related and PTSD-related psychosis in long-stay secure settings.
To investigate potential moderators or mediators of PTSD symptoms. We predicted:
- Positive correlations between trauma history and PTSD.
- Positive correlations between insecure attachment and PTSD.
- More secure attachments and more PTSD symptoms in those with an integrative recovery style compared to those with a sealing over recovery style.

MethodMethod
Measures- PANSS (Kay et al., 1987)- Impact of Event Scale-Revised (Weiss & Marmar,
1997)- Trauma History Questionnaire (Green, 1996)- Psychiatric Experiences Questionnaire (Cusack et
al., 2005)- Psychosis Attachment Measure (Berry et al., 2008)- Recovery Style Questionnaire (Drayton et al., 1998)

Adult attachment dimensions
High levels of attachment anxiety- negative self-image- an overly demanding interpersonal style- fear of rejection- tendency to exaggerate or be overwhelmed by negative affect
High levels of attachment avoidance- negative image of others- interpersonal hostility - social withdrawal - defensive minimisation of affect and importance of social relationships

MethodMethod
Participants and procedure- 50 patients recruited from low-secure and
medium-secure sites in the North West. - Diagnoses of schizophrenia or related
disorders, 18 years + and inpatients for at least one month.
- Assessment measures completed as part of a structured interview.
ResultsResults
• 24% met criteria for psychosis-related PTSD.
• 18% met criteria for hospital-related PTSD.
• 30% met criteria for psychosis-related or hospital related PTSD.

Results Results Hypothesis: Associations between previous trauma
and psychosis-related or hospital-related PTSD
Psychosis-related PTSD
Hospital-related
PTSD
Total number of previous traumas
.19 (.186) .23 (.108)
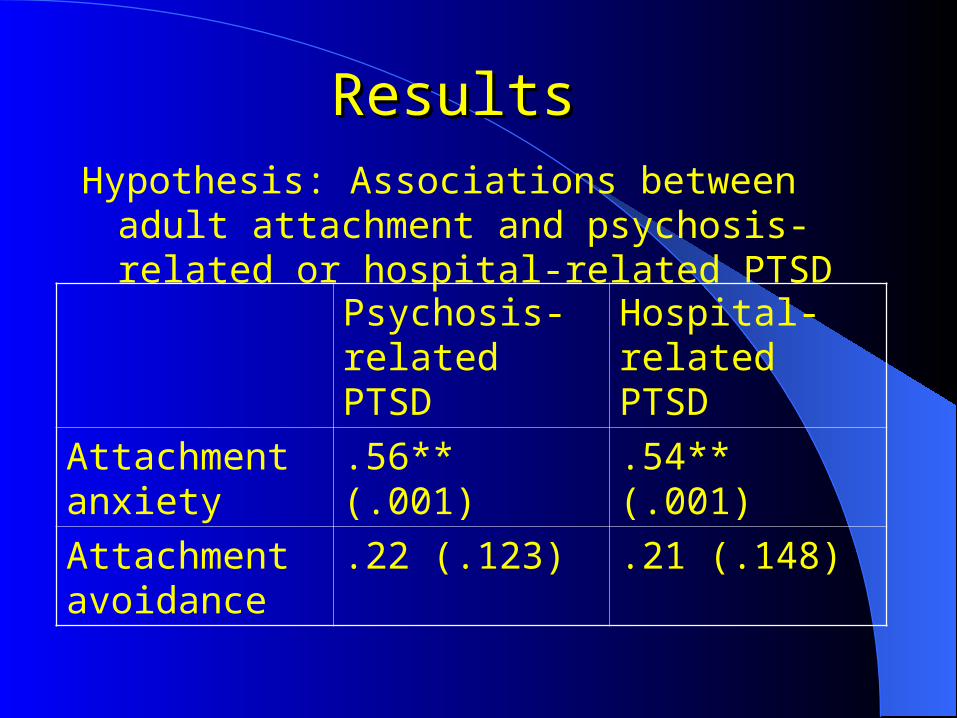
Results Results Hypothesis: Associations between adult attachment
and psychosis-related or hospital-related PTSD
Psychosis-related PTSD
Hospital-related PTSD
Attachment anxiety
.56** (.001) .54** (.001)
Attachment avoidance
.22 (.123) .21 (.148)

Results Results Hypothesis: Integrators will have lower levels of
attachment anxiety and avoidance, but more PTSD symptoms
Integrators
(n = 40)
Sealers
(n = 10)
Attachment Anxiety
.68 (.54) .58 (.23)
Attachment Avoidance
1.25 (.45) 1.49 (.65)
Psychosis-related PTSD
21.30 (17) 17.80 (12.81)
Hospital-related PTSD
15.20 (12.37) 19.60 (12.56)

Summary and discussionSummary and discussion
The 30% rate of PTSD are lower than expected. Participants may have habituated to symptoms and
hospital experiences over time or actively developed ways of coping.
No significant associations between previous trauma and psychosis-related or hospital-related PTSD.
Mixed evidence of associations in the literature, with studies with smaller samples or less sensitive measures not finding effects (e.g. Beattie et al., 2009; Tarrier et al., 2007).
PTSD literature suggests other factors may also be important.

Summary and discussionSummary and discussion
Attachment anxiety characterised by negative self-image and a tendency to be overwhelmed be overwhelmed by affect may be vulnerability factor for PTSD.
However, evidence to suggest that the defensive coping style associated with avoidant attachment can also breakdown under extreme distress (Mikulincer et al., 1993).
No significant differences between integrators and sealers in terms of attachment or PTSD, but consistent with previous research we found relatively few sealers (e.g. Jackson et al., 2004).

Selection of caveatsSelection of caveats
Rates of PTSD or trauma over or underestimated due to sample selection or reporting biases.
Reduced power due to small numbers, particularly a problem in analyses involving recovery style.
Cross-sectional design, so cannot ascertain the direction of relationships or rule out third variables.

Future implications Future implications
Adds to growing literature on the distressing nature of psychosis and the iatrogenic effects of treatment.
Highlights the need to routinely assess people’s reactions to their experiences and screen for PTSD.
Some evidence that PTSD in the context of psychosis can be treated with CBT (Mueser & Rosenberg, 2008).

Future implications Future implications
CBT should be routinely offered to those who want to engage and therapists should recognise the traumatic nature of psychosis.
Although there have been reforms in mental health care, these findings highlight a need to do more.
Findings of associations between attachment and PTSD, highlight the importance of considering attachment patterns in treatment, particularly given evidence that insecure attachments can have an adverse effect on therapy (e.g. Mallinckrodt et al., 2010).
