translating research into practice: improving the ...sydney.edu.au/medicine/rehab/about/research...
TRANSCRIPT
31/07/2015
1
Translating research into practice: Improving the management of pain after spinal cord injury
1. John Walsh Centre for Rehabilitation Research,Kolling Institute for Medical Research, University of Sydney
2. State SCI Service, NSW Agency for Clinical Innovation
A/Professor James Middleton1,2, Dr Janet Long 1, and Lyndall Katte 1
Translating research into practice
2
Objectives
› To define Knowledge Translation (KT)
- Phases of KT
- Where implementation fits
› To define Implementation
- factors that contribute to success
- Stages
› To illustrate the stages with the SCI Pain Project

31/07/2015
2
Translating research into practice
• Overview of the Knowledge Translation Model
• The SCI Pain Project:
• Exploratory phase
• Developing the intervention
• Planning implementation strategy
• Implementation
• Evaluation
• Dissemination
• Sustainability
• Future plans3
Outline
Translating research into practice
4

31/07/2015
3
5
The Valley of Death: getting research into practice
Image by Mellor from Nature 453, 840-842 (2008)
6

31/07/2015
4
It’s hard
7
Effectiveness of professional behaviour change strategies from selected EPOC systematic reviews• 363 randomised trials• Mean absolute improvement in care / change in clinician behaviour
(e.g. prescribing) 3-12%
Defining Knowledge Translation and implementation
› “an ideal and an endeavour”
› Evidence from research put into practice
› Not an automatic process
Implementation
› systematic uptake of research
› Establish as routine practice
› Effectiveness and quality of health services
8
Knowledge translation
31/07/2015
5
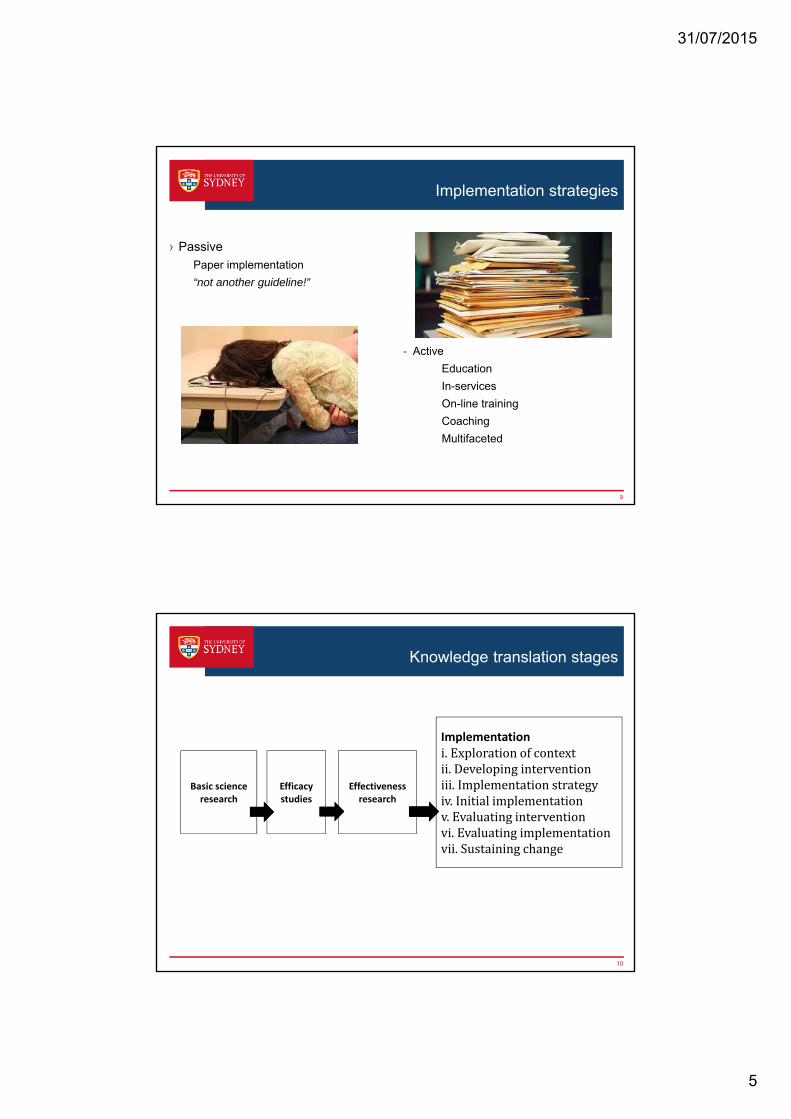
Implementation strategies
› Passive
Paper implementation
“not another guideline!”
- Active
Education
In-services
On-line training
Coaching
Multifaceted
9
10
Knowledge translation stages
Basic science research
Efficacy studies
Effectiveness research
Implementationi.Explorationofcontextii.Developinginterventioniii.Implementationstrategyiv.Initialimplementationv.Evaluatinginterventionvi.Evaluatingimplementationvii.Sustainingchange

31/07/2015
6
Early Stages of the KT continuum
11
› Efficacy studies
- Compile evidence for efficacy of intervention in controlled settings
- Laboratory work, animal models
- Randomised controlled trials
› Effectiveness studies
- Assessing evidence
- Compile evidence for intervention in "real world" settings
- Clinical trials
Stages of implementation
Explorationofcontext
Developingintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
12

31/07/2015
7
Active implementation
› Current practice
› Aims
› Strategies
› Acceptable
› The science
13
A collaboration between researchers and clinicians
Reasons why people might not change their behaviour when new processes are implemented
Knowledge
Do I understand what it is saying?
Skills
Do I know how to do this?
Social / professional role and identity
Who are they to tell me what to do?
Beliefs about capabilities
How hard / comfortable is it to do?
Theoretical Domains FrameworkMichie, Johnston, Abraham, et al (2005) Qual Saf Health Care 14:26-33
31/07/2015
8
Reasons why people might not change their behaviour when new processes are implemented
Beliefs about consequences
What is the cost/benefit to me or my clients of doing it?
Motivation and goals
How much do I want to do it?
Memory, attention and decision making
Will I remember to do it if it’s not part of my routine?
Environmental context and resources
Are there competing tasks / time constraints / equipment issues?
15
Theoretical Domains FrameworkMichie, Johnston, Abraham, et al (2005) Qual Saf Health Care 14:26-33
Reasons why people might not change their behaviour when new processes are implemented
Social influences
Are the clinicians I respect doing it too? Is the boss supportive?
Emotion
I messed up first time I did it. It was so humiliating
16
Theoretical Domains FrameworkMichie, Johnston, Abraham, et al (2005) Qual Saf Health Care 14:26-33

31/07/2015
9
How to measure implementation success?
17
› Feasibility - does it fit here?
› Acceptability: do people like it?
› Appropriateness: is it OK to do?
› Fidelity: it is being used properly?
› Adoption: are people actually using it?
What factors are associated with success?
18
Success 1. Preparing for change
2. Capacity — people
3. Capacity — setting
4. Types of implementation
5. Resources
6. Leverage
7. Enabling features
8. Sustainability
Obstacles • failure to prepare
• insufficient capacity
• resistance to change
“then care quality is at risk, and patient safety can be compromised.”
Braithwaite J, Marks D, Taylor N. (2014)
International Journal for Quality in Health Care. 2014 June 1, 2014;26(3):321-9.

31/07/2015
10
Resources
19
http://epoc.cochrane.org/
20
Resources
www.improvement academy.org

31/07/2015
11
21
Resources
www.improvement academy.org
Resources
22
http://nirn.fpg.unc.edu/
31/07/2015
12
Resources
23
http://implementation.fpg.unc.edu/
Resources
24
http://www.behaviourworksaustralia.org/resources/

31/07/2015
13
25
http://plus.mcmaster.ca/kt/
Resources
Stages of implementation
Explorationofcontext
Developingtheintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
26

31/07/2015
14
Exploratory Phase – Chronic Pain & SCI Project
› Online Survey- Clinicians- Consumers
› Focus Groups- Clinicians- Consumers
› Interviews
› Social media and print media- Spinal Cord Injuries Australia- ParaQuad NSW- Lifetime Care and Support
Authority
IDENTIFYING THE PROBLEM, UNDERSTANDING WHAT IS NEEDED
27
Do you feel adequately resourced to manage patients
with SCI and chronic pain?
Yes 18.87%
No 81.13%
How do people prefer to obtain Healthcare Information?
Resource type:
• Internet 74%
• Book 27%
• Flyers 25%
Healthcare Provider:
• GP 91%
• Spinal Specialist 72%
• Physio 58%
• OT 34%
• Massage Therapist 29%

31/07/2015
15
Setting Clinical Standards & Planning for Implementation
KNOWLEDGE CREATION
‘Discovery’ research (basic, applied)
Knowledge Synthesis (scoping, evidence mapping, systematic reviews)
Stakeholder Dialogues (harness expertise, offer different perspectives, collectively problem-solve)
mobilize ‘Community of Practice’
Further research
Develop Clinical
Practice GuidelinesNO
IMPLEMENTATION PLANNING Audit Current Practice Identify Evidence-Practice Gaps Determine Health Drivers
IMPLEMENTATION STRATEGY
AGREED STANDARDS OF PRACTICE Ready for Implementation
› Applies collective problem solving to important issues
› Defines the key challenges through consultation with key stakeholders to understand the issues and complexities.
› Synthesises information from publications and further expert consultation into briefing document.
› Convenes stakeholder dialogues to:- connect the relevant information with people who can make
change happen (clinicians, researchers, people with SCI, advocacy organisations, managers, policy-makers, funding agencies)
- Harness expertise, gathering views, experiences and tacit knowledge that key stakeholders bring to the issues at hand
- motivate and inspire dialogue participants by bringing them together to address a common challenge.
› Supporting improvements by preparing dialogue summary
National Trauma Research Institute (NTRI) Forum Model
www.ntriforum.org.au

31/07/2015
16
› NTRI Forum held 20 August, 2013 (N=19)- Researchers, clinicians, consumer, service
providers, govt funding and advocacy organisations
› Context - current SCI projects in NSW & Canada, national & state-wide pain management initiatives, resources/information to underpin implementation
› Aim to develop a shared understanding of currentstandards, practice, and barriers & facilitators of optimal management of chronic pain in SCI, and
› Consider how this information can inform change strategies to optimise clinical practice.
SCI Pain Stakeholder Dialogue
NTRI Forum Model for KT
Bragge, Piccenna & Gruen, 2012
32

31/07/2015
17
› SCI Pain algorithms (Siddall & Middleton, 2006)› National Pain Strategy (co-ordinated interdisciplinary assessment & management)
› NSW ACI Pain Mgt Network reviewed Models of Care- ‘stepped care’ to screening & triage, promote active
engagement & self-management by patient; multi-disciplinary, comprehensive, integrated & system-wide (Conway & Higgins, 2011)
› SCI KMN Canada 3-round Delphi survey to prioritise implementation targets (89 → 12 → 7 practices)
› International SCI Pain Basic Dataset version 2.0 (Widerström-Noga et al, 2013)
› Updated Pain Classification (Bryce et al, 2012)
Pain Forum – Contextual Issues
Treatment Algorithm for Nociceptive SCI Pain
34
PAINLocated in a region of normal sensation
Dull, aching painRelated to posture, activity, movement
Somatic tenderness
Vague, poorly localised,cramping, intermittent
pain in thorax, abdomenRelated to visceral function
Antibiotics
Cystoscopy Lithotripsy
Disempaction
Adjust bowel aperients &
routine
Oral baclofenTizanidineDiazepam
NOCICEPTIVE
VISCERALMUSCULOSKELETAL
AcetaminophenNSAIDs
Botulinum toxin (if focal spasm)
Intrathecalbaclofen
ColonoscopyBowel transit
studies
Transanalirrigation
Colostomy
Treat muscle imbalance, exercise Postural reeducation, seatingRetrain transfer techniques
Address wheelchair biomechanicsActivity pacing & modificationEnvironmental modifications
NEUROPATHIC(see Figure 4)
-Nociceptive pain
indirectly related or unrelated to SCI, such as
dysreflexicheadache, pressure areas, migraine
Electric shock, shooting, squeezing, burning pain
Segmental pattern,located at NLI and/or
within 3 dermatomes, or involves cauda equina
Electric shock, shooting, squeezing, burning pain
Located more than 3dermatomes below NLI(but may include them)
BELOW-LEVELNEUROPATHIC
AT-LEVELNEUROPATHIC
OTHERNOCICEPTIVE
- - -
Related to repetitive movement
Local tenderness, pain on stretching,resisted movement
Neck or back painKyphus / scoliosis
Worsens during dayRelieved by lying
Possible trigger pts
POOR POSTURE & MECHANICS
“OVERUSE SYNDROME”
Increased muscle tone
MUSCLE SPASM
-- Fever, frequency, urine leakage, debris,
blood, spasms, ADWCC, urinalysis,
MCS, ultrasound, CT
Constipation, diarrhoea, bloatingWorse after meal,
Improved by evacuationImpacted on AXR
Pounding headache,sweating, flushing, blurred vision, etc
Elevated blood pressure (>20mmHg)
-PSEUDOBOWELOBSTRUCTION
INFECTION,CALCULUS
AUTONOMICDYSREFLEXIA
--
-
Tramadol“Strong” opioids
Located in a region of impaired sensation
Spinal fusion
Signs of instability on examination
Structural changes evident on imaging
FRACTUREDISLOCATION
-Exclude pathology, such as peptic ulcer,
gall stones, etc on ultrasound, CT scan, endoscopy
-
-
Identify and treat cause
Identify and treat cause
BP lowering drugs
Further investigation
-
+++++
++ +++ + +
ALL - ASSESS AND TREAT PSYCHOSOCIAL & ENVIRONMENTAL CONTRIBUTORS - POOR PACING, UNHELPFUL COGNITIONS, MOOD DYSFUNCTION (e.g. CBT, Anxiolytics, Antidepressants)
- --
+ -
Siddall PJ, Middleton JW. Pain following spinal cord injury. In: ISCoS textbook on comprehensive management of spinal cord injuries, Chhabra HS (Ed.). Wolters Kluwer, New Delhi pp825-848 (2015).
31/07/2015
18
Guideline Summary from KMN Delphi Survey
Final Recommendations identified for implementation
› INTERDISCIPLINARY TREATMENT & ASSESSMENT:
› Treat in an interdisciplinary fashion guided by comprehensive assessment (Source: PVA)
› Full text of relevant recommendations:
- “Because chronic pain related to musculoskeletal disorders is a complex, multidimensional clinical problem, consider the use of an interdisciplinary approach to assessment and treatment planning. Begin treatment with a careful assessment of the following: aetiology, pain intensity, functional capacities, psychosocial distress associated with the condition.” [PVA, p.460]25
- “Treat chronic pain and associated symptomatology in an interdisciplinary fashion and incorporate multiple modalities based on the constellation of symptoms revealed by the comprehensive assessment.”[PVA, p. 461]25
Very strong support for this recommendation. (Grade of Recommendation-A; Clinical/epidemiologic evidence–1; Ergonomic evidence–NA, Panel opinion-Strong)
35
Wolfe D, Hsieh J, Kras-Dupuis A, et al. Online Delphi to Identify Targets for Best Practice Implementation and Associated Performance Measures Interdependence 2012. Vancouver, BC; 2012.
› 12 SCI Rehabilitation Facilities with onsite Pain Management Services (Craven et al, 2012)- 75% adequate waiting time, 58% services sufficient
- <30% use standardised assessments or validated tools (eg. VAS, BPI, DN-4, etc)
- 25% follow documented standards of care or CPG!
› Priority to overcome regional disparity
- Best practice indicators include: extent of inter-disciplinary care, collaborativeness of inter-facility & regional chronic pain programs, timeliness of PM care, standardisation of assessment & outcome tools, integration pharmacological & non-pharmacological treatment pathways, and improved patient education.
Canadian Environmental Scan
Craven C, Verrier M, Balioussis C, et al. Rehabilitation environmental scan atlas: Capturing capacity in Canadian SCI Rehabilitation. Vancouver: Rick Hansen Institute, 2012.

31/07/2015
19
› Care highly variable/adherence to identified standards higher in specialist/inpatient centres compared with outpatient and community-based settings
› Lack of access to tertiary centres with expertise, compounded by geographical and travel issues
› Barriers in primary practice include lack of knowledge, limited time and funding, and shortfalls in workforcevolume/training, especially in rural and remote areas
› Facilitators include fostering ‘hub and spoke’ model of education/ capacity building, CDSM models
› Use of formal, standardised assessment tools and management plans, develop case studies / scenarios as an educational strategy
Pain Forum – Key Issues
The SCI Pain Clinical Standards
1. People with SCI should be screened for pain prior to discharge from the spinal cord injury unit
2. If pain is found, assessment will be done using a SCI-validated tool to establish a baseline record of pain history
3. Standard terminology will be used to describe pain, consistent with the International SCI Pain Basic Data Set and the International Spinal Cord Injury Pain Classification
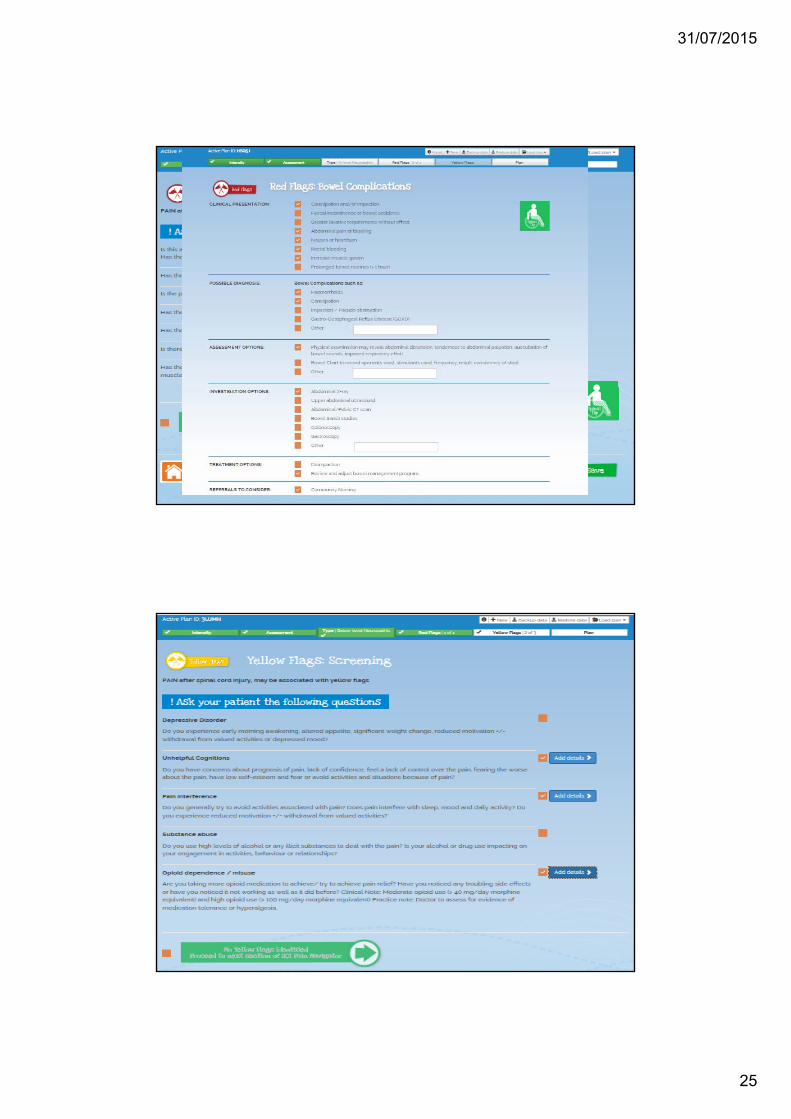
4a). Red flags are to be ruled out for any new or changing pain and managed accordingly if present
4b). Yellow flags will be ruled out for any pain and when identified, managed accordingly
5. A multidisciplinary approach is used to management.38

31/07/2015
20
Stages of implementation
Explorationofcontext
Developingtheintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
39
Consumer Resources
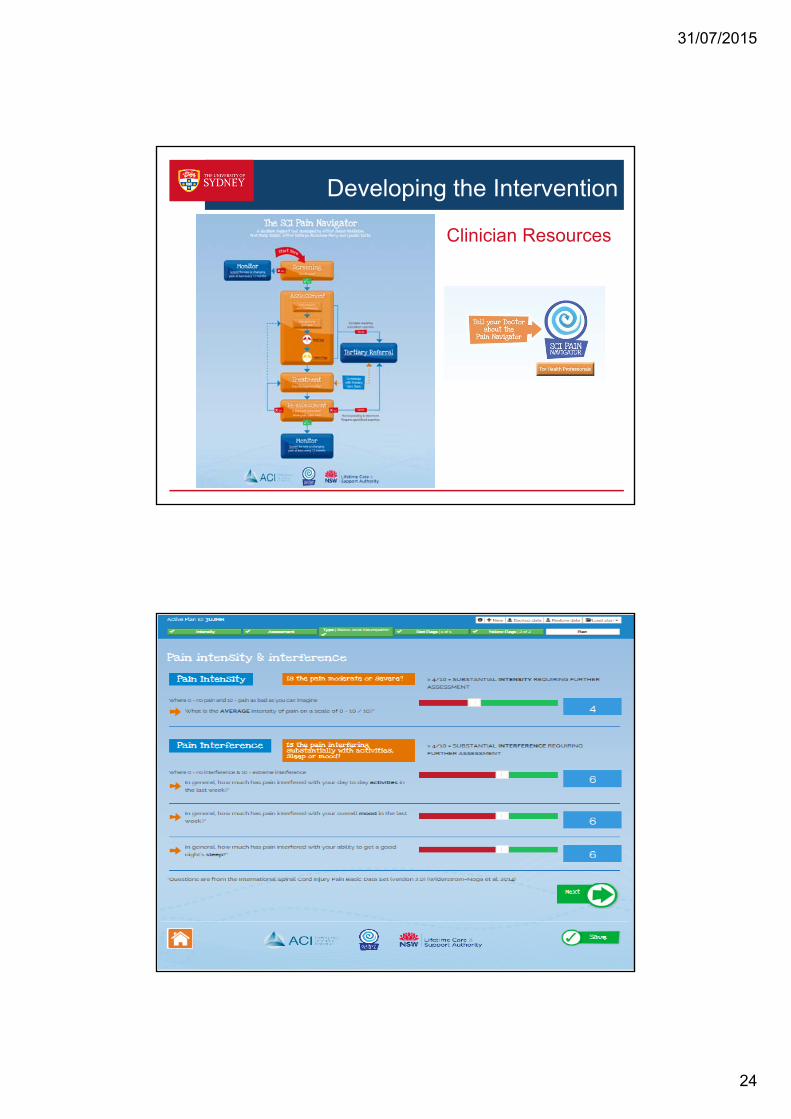
Developing The Intervention -Resources
http://www.aci.health.nsw.gov.au/chronic-pain/spinal-cord-injury-pain

31/07/2015
21
Introduction to SCI & Chronic Pain
› Pain is common after SCI
› There are a number of different types of pain that occur after SCI
› Learn how to talk about your pain
› Identify SCI Red flags
Understanding Pain After SCI
› Pain is due to primary trauma, nervous system response and secondary changes to the nervous system
› Introduction to pain gates
› What happens to pain gates after SCI
› Explanation of neuropathic pain mechanisms after SCI
› You can re–train the brain to feel less pain – even after spinal cord injury

31/07/2015
22
SCI Pain, Physical Activity & Exercise
› It is important to be physically active after spinal cord injury
› Be aware of risks of shoulder overuse
› Physical activity can actually help to reduce the pain
› Use pain management principles; set goals, pace yourself and devise a graded activity program for best results
SCI Pain Nutrition & Lifestyle
› A balanced and nutritious diet can help to
• increase your energy
• reduce your pain
› Aim for a selection of fresh vegetables and fruit, whole-grains and lean protein choices
› Monitor your bowel program if on medication for pain that can cause constipation
› Healthy food choices are easier than you think!
› Links to nutrition resources

31/07/2015
23
SCI Pain & Medications› Different types of medications are used to treat different types
of pain after SCI
› It is important to match appropriate pain medication with pain type
› It is important to have a plan to review efficacy of medication
› Weigh up the benefit (pain reduction/increased function) against the side effects to help guide future planning
Pain and Thoughts
› Thoughts and feelings can influence the pain experience
› You can re-train the brain to reduce the impact of pain on your life
› Techniques include a combination of:
• Managing your thoughts • De-sensitisation• Distraction• Meditation / Relaxation• Goal setting• Graded activity & pacing • Flare up plan• Sleep strategies
“Everyone has a different way to copewith the pain. I used a lot of meditation early on and desensitisation. Now I have taught myself to play guitar, and when I
play it is like a meditation for me.”
31/07/2015
24
Developing the Intervention
Clinician Resources
31/07/2015
25

31/07/2015
26
PAIN MANAGEMENT - PHYSICAL
• Goal Setting• Exercise• Strengthening• Stretching• Fitness/Conditioning• Pacing• Graded Activity Plan• Flare Up Plan• Upper limb preservation

31/07/2015
27
PAIN MANAGEMENT - PSCYCHOLOGICAL
• Dealing with unhelpful thoughts
• Relaxation / Meditation
• Desensitisation
• Hypnosis
• Dealing with flare ups
• Pacing
• Goal setting
PAIN MANAGEMENT PLAN
• Pain Assessment
• Pain Features and Types
• SCI Specific Red Flags
• Yellow Flags
• Medical Management
• Physical Management
• Psychological Management
• Referrals
• Re-Assessment
• Resources

31/07/2015
28
Stages of implementation
Explorationofcontext
Developingtheintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
55
Planning the strategy
1. Spinal Rehabilitation units
Patients with a new injury on discharge from the unit going home / into residential care
2. Community Health Centres
56
SITES
Clients accessing their community nursing or allied health services
3. Tier 2 pain clinics (Regional outpatient pain services)Clients referred for specialist pain management

31/07/2015
29
Planning the strategy
• Estimated clients with a SCI seen per year
• Community Health Centres: <15 per year
• Tier 2 pain clinics: 0-5 per year
• Spinal Rehab units: 30-80 per year
57
NUMBERS
Planning the strategy
• To improve the process of pain assessment and management in clients with spinal cord injury (SCI) through the use of a decision support tool and web-based resources: increasing the number of people with SCI screened for pain and if pain is present, having a comprehensive assessment and management plan documented.
• To determine the acceptability, adoption, appropriateness, feasibility, fidelity and sustainability of the tools and resources.
58
Project objectives

31/07/2015
30
Planning the strategy
59
KNOWLEDGE: spinal cord injury chronic pain educational resources
ENVIRONMENTAL CONTEXT AND RESOURCES: access to the website
MEMORY, ATTENTION, DECISION MAKING: checklists, other documents
SKILLS: coaching on the SCI Pain Navigator, gaining experience
Planning for known barriers:
Retrospective audits of files for last 12 months
60

31/07/2015
31
Pain Clinic #1 Process map
Pain Clinic #1 Process map

31/07/2015
32
Pain clinic audit
63
Standard 2 If pain is present,
assessment will be
done using a SCI‐
validated tool, to
establish a baseline and
record of pain history
No Initial Pain intensity scores
only
Interference recorded but
not scored or compared
well over time
0123456789
Jan Mar Apr Sept Nov
Pain intensity
Pain interference
Pain clinic audit
64
Standard 4 a) Red flags are to be ruled out for
any new or changing pain and
managed accordingly if present
b) Yellow flags will be ruled out for
any pain and when identified,
managed accordingly
No
Yes
Reliance on GPs to
pick up problems
Not systematic
Difference between
the professions
Clinical Standards SCI Pain Project Y/N Comments

31/07/2015
33
Pain Clinic #2 Process map
Pain Clinic #2 Process map
31/07/2015
34
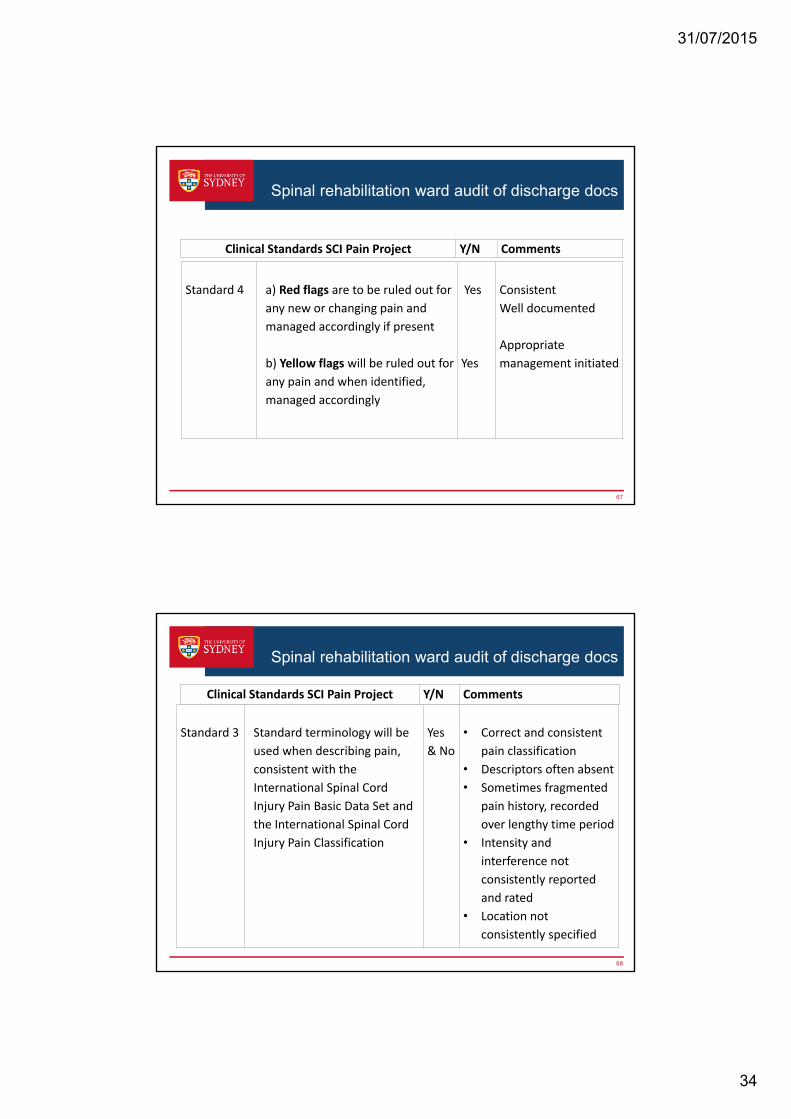
Spinal rehabilitation ward audit of discharge docs
67
Standard 4 a) Red flags are to be ruled out for
any new or changing pain and
managed accordingly if present
b) Yellow flags will be ruled out for
any pain and when identified,
managed accordingly
Yes
Yes
Consistent
Well documented
Appropriate
management initiated
Clinical Standards SCI Pain Project Y/N Comments
Spinal rehabilitation ward audit of discharge docs
68
Standard 3 Standard terminology will be
used when describing pain,
consistent with the
International Spinal Cord
Injury Pain Basic Data Set and
the International Spinal Cord
Injury Pain Classification
Yes
& No
• Correct and consistent
pain classification
• Descriptors often absent
• Sometimes fragmented
pain history, recorded
over lengthy time period
• Intensity and
interference not
consistently reported
and rated
• Location not
consistently specified
Clinical Standards SCI Pain Project Y/N Comments

31/07/2015
35
Stages of implementation
Explorationofcontext
Developingtheintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
69
Coaching with case studies
70
Bryce TN, Biering-Sørensen F, Finnerup NB, Cardenas DD, Defrin R, Ivan E, Lundeberg T, Norrbrink C, Richards JS, Siddall P,
Stripling T, Treede RD, Waxman SG, Widerström-Noga E, Yezierski RP, Dijkers M. (2012) International Spinal Cord Injury Pain (ISCIP) Classification: Part 2. Initial validation using vignettes. Spinal Cord, 50, 6, pp. 404-12
31/07/2015
36
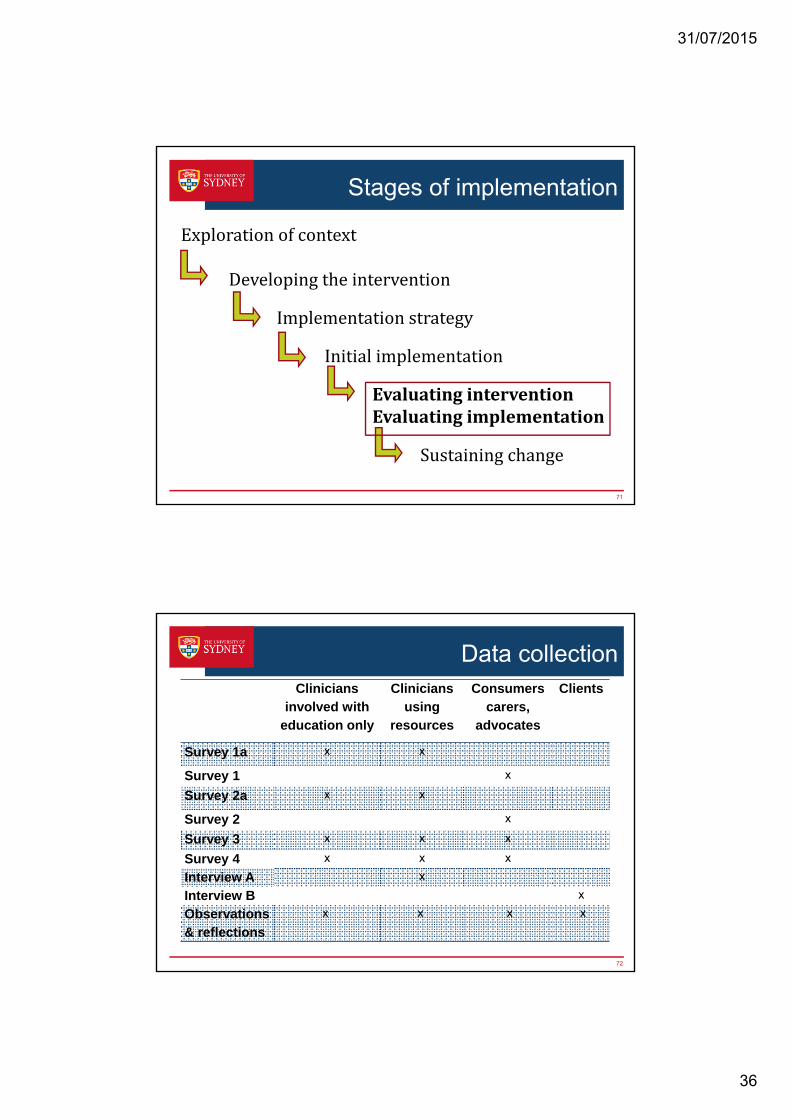
Stages of implementation
Explorationofcontext
Developingtheintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
71
Data collection
72
Clinicians involved with
education only
Clinicians using
resources
Consumers carers,
advocates
Clients
Survey 1a x x
Survey 1 x
Survey 2a x x
Survey 2 x
Survey 3 x x x
Survey 4 x x x
Interview A x
Interview B x
Observations& reflections
x x x x

31/07/2015
37
Measuring implementation success
73
Accept-ability
Adoption Feasibility Fidelity Appropriate-
ness
Survey 1 x x x
Survey 2, 3 x x x x
Interview A x x x x x
File audit x x x x
Survey 4 x x x x x
Website
Usage
x
Tool Usage x
Interview B x x x x
Prospective audits of files for next 12 months
74
31/07/2015
38
Stages of implementation
Explorationofcontext
Developingtheintervention
Implementationstrategy
Initialimplementation
EvaluatinginterventionEvaluatingimplementation
Sustainingchange
75
Thank you to our sponsors and research partners
Office of Health and Medical Research
NSW Agency for Clinical Innovation (ACI)
National Trauma Research Institute (NTRI)
Lifetime Care and Support Authority (LTCSA)
NSW Health clinicians and managers
ParaQuad NSW, Spinal Cord Injuries Australia
76