translating injury surveillance to prevention: an update
TRANSCRIPT

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 1
Hazard(Edition No. 25)December 1995
Victorian InjurySurveillance SystemMonash UniversityAccident Research Centre
Translating injury surveillanceto prevention: an updateAs VISS is moving to a new system of data collection in 1996 it is timely to review our achievements over the past eightyears. This edition of Hazard highlights some VISS success stories and outlines some of the challenges that face us in1996 and beyond.
Erin CassellVirginia RoutleyJoan Ozanne-Smith
SummaryThe first edition of Hazard waspublished in July 1988, the year inwhich the Victorian InjurySurveillance System was established.The quarterly publication of Hazardis one of the major methods VISSuses to disseminate information. Theselection of topics for Hazard is basedon the relative severity, frequencyand the potential preventability ofinjury problems that emerge fromanalyses of VISS hospital emergencydepartment presentations data andreference to other relevant datasources.
Each Hazard edition includes thefindings from the data analysis on one
or more significant injury issues anda discussion of actions that need to betaken to reduce or eliminate thepotential for injury.
As background to this (the 25th)edition of Hazard, progress on all therecommendations to reduce injuriesmade in Hazard was reviewed. Thereview not only covered follow-upaction undertaken by VISS alone or incollaboration with other MonashUniversity Accident Research Centre(MUARC) projects but also includedsignificant action on VISSrecommendations taken by otherbodies. VISS intends to continuouslyupdate this review as an ongoingWorking Report.
This edition of Hazard highlightssome VISS success stories. It alsofocuses on injury issues where some
progress has been made by VISS andother bodies but where there is goodpotential for further gains. In theseareas a modest increase in human andfinancial resources applied to theproblem could be repaid by significantreductions in the number and/or theseverity of injuries.
Enclosed in this edition is a clientsurvey. In 1995 VISS received asmall grant from the VictorianHealth Promotion Foundation tosupport the implementation offindings from VISS data analysesand research. This grant includedfunds for a survey of VISS clientsand potential clients on their dataand other needs for progressing therecommendations for actionpublished in Hazard.
V.I.S.S.

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 2
IntroductionThe Victorian Injury SurveillanceSystem (VISS) was established in1988 to collect and analyse injurydata from hospital emergencydepartments and to disseminateinformation for the purposes of injuryprevention. VISS is currently fundedby the Victorian Health PromotionFoundation.
The size and nature of the datacollection has changed over thelifetime of VISS. It was initially acollection of child injuries reportedthrough the emergency department ofthe Royal Children’s Hospital underthe directorship of Associate ProfessorTerry Nolan. MUARC took overVISS management in 1990 anddeveloped the all age injury collection.By 1992 VISS had expanded to fivehospitals on seven campuses.
VISS is currently in transition fromthe manual collection of injury data inselected emergency departments to astatewide routine electronic collectionusing the National Minimum Dataset(Injury Surveillance).
VISS has also expanded to accessdata and information from a widerrange of sources so that a morecomplete picture of injury issues isobtained. The other sources frequentlyaccessed are the Australian Bureau ofStatistics (ABS), the Coroner’sFacilitation System (mortality) andthe Victorian Inpatient MinimumDataset.
There are currently 166,137 cases ofinjury on the VISS hospital emergencydepartment database. VISS data areused to identify injury problems,support research and, most import-antly, to underpin the development ofinjury prevention strategies andsupport their implementation andevaluation.
Media coverage of injury issues in Hazard - 1995 Table 1
Injury IssueNo. of media
requestsMedia coverage in 1995
Domestic violence
22 Print: AAP, Canberra Times, Herald Sun, IPA Review, Shepparton News, Sunday Herald Sun, Sydney Morning Herald, The Age, The Australian, The Independent Monthly, Warrnambool Standard, Waverley Gazette, Women's Day.Radio: ABC Sydney, SBS, Triple MTelevision: A Current Affair (Channel 9), GP (ABC TV)
Dog bites/attacks
12 Print: Fairfax Suburban Newspapers, Herald Sun, National Dog Magazine, Sunday Age, Sunday Herald Sun, Sterling MediaTelevision: A Current Affair (Channel 9), Burke's Backyard (Channel 9)
Horse related injuries
8 Print : Herald Sun, Warrnambool Standard, Weekly TimesRadio: Country Hour (ABC Radio)Television: Midday Show (Channel 9), Channel 9
Sports injuries 8 Print: Australian Golf Digest, Fairfax Newspaper Group, Herald Sun, Sunday Age, Sydney Morning HeraldRadio: 3BATelevision: Today Tonight (Channel 7)
Smoking related injuries
5 Print: AAP, Herald Sun, The AgeRadio: 3MP, 5DN
In-line skating injuries
3 Print: Shepparton NewsTelevision: The Today Show (Channel 9), News Channel Pay TV
Escalator-related injuries
3 Print: Australian Doctor, Parents (Australian Parenting Magazine), Herald Sun
Home injuries 3 Print: The AgeTelevision: Better Homes (Channel 7), Channel 7
Tractor-related injuries
2 Print: Herald Sun, Weekly TimesRadio: The Country Hour (ABC radio), Country Roundup (Ace Network)
Shopping trolley injuries
2Print: Herald Sun
Snake bites 2 Print: Sunday Herald SunTelevision: Burke's Backyard
Farm injuries 2 Print: Warrnambool Standard, Weekly Times
Chainsaw-related injuries
1Print: Gippsland Farmer

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 3
The latter is achieved by bringinghazards and potential solutions to theattention of the public and those whoshare the responsibility forsafeguarding Victorians - governmentdepartments and statutory authorities,manufacturers, retailers, insurers,consumer and injury preventiongroups, educators, researchers andspecialist medical practitioners.
The media play an important andresponsible role in reporting VISSdata and often follow up the injuryissues highlighted in Hazard. Table 1shows the media attention given toinjury issues in 1995 that are directlyattributable to the publication ofHazard. The issue that excited themost media attention was domesticviolence.
Over time, increasing emphasis hasbeen given by VISS to the vigorouspursuit of the implementation ofrecommendations based on VISS dataand available research.
VISS is a major program of MonashUniversity Accident Research Centre(MUARC) and Dr Joan Ozanne-Smith, a Senior Research Fellow withMUARC, is the Director of VISS.
Hazard 20 highlighted that carbonmonoxide poisoning from car exhaustswas a major means of suicide inVictoria, ranking second to hanging/strangulation. In 1994 carbonmonoxide gas was used by 98Victorians and 447 Australians(source-ABS microfiche data) tocommit suicide.
There is some research evidence whichsuggests that restricting access to themeans of suicide can contribute to afall in overall suicide rates. Forexample, a fall in suicides amongwomen in Australia occurred whenaccess to barbiturates was tightenedin the late 1960’s and in the U.K.when natural gas replaced coal gas.There is preliminary evidence thattighter firearm legislation in Victoriamay be having a similar beneficialeffect.
Cars built after 1986 have catalyticconverters fitted which convertharmful carbon monoxide gasemissions to carbon dioxide gas.However, ongoing surveillance of thetrend in suicides in Victoria andAustralia by VISS shows no clearevidence of a decline in the proportionof suicides from carbon monoxidepoisoning in recent times. In fact,Victorian Inpatient Morbidity dataindicate that hospital admissions forcarbon monoxide suicide attemptshave steadily increased from 15 in1989-90 to 56 in 1993-94.
Information from the VictorianInstitute of Forensic Medicine alsoconfirms that gassings are stilloccurring in post-1986 vehicles,probably because catalytic convertersdo not work efficiently at a cold start.
VISS therefore recommended theconsideration of other design
Progress on selected issuesPrevention of suicide - reducing car exhaust gas poisoning[reported in Hazard 11, June 92; Hazard 20, Sept 94]
Recommendations
• reduce access to the means of suicide, especially firearms and carbonmonoxide gas [Hazard 11, June 92]
• design modifications to motor vehicles to impede common methods ofcarbon monoxide poisoning, eg. modify/re-design car exhaust systems toreduce or eliminate carbon monoxide emission, and mandate these designchanges by incorporating them into the Australian Design Rules (ADRs)[Hazard 20, Sept 94]
• mandate, through changing ADRs, the incorporation of a sensing devicein motor vehicles which monitors carbon monoxide levels and shuts downthe motor when levels become life threatening [Hazard 20, Sept 94]
• improve motor engine designs and catalytic conversion techniques tocomplete the combustion process and thereby virtually eliminate carbonmonoxide emissions [Hazard 20, Sept 94]
• improve the identification and treatment of those who are most at risk ofsuicide [Hazard 11, June 92]

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 4
modifications to cars to make carbonmonoxide emissions a less accessiblemeans of suicide. One intervention, acarbon monoxide sensing devicewhich turns off the engine when thecarbon monoxide reaches a dangerouslevel, has been assessed as costeffective in terms of lives saved. VISSalso made suggestions for engineereddesign changes to car exhaust systemsand these have been sent to experts inthe field for comment.
VISS circulated copies of Hazard 20,which highlights the problem andpossible solutions, to senior staff incar manufacturing companies,automotive bodies, governmentdepartments of transport, engineeringacademics and members of the varioussuicide prevention working partiesthat have been set up by governmentand other bodies. In December 1995updated and comprehensiveinformation was sent to these andother interested organisations seekingtheir co-operation and advice on howto progress action on the issue.
The national arm of the AustralianMedical Association (AMA) has alsopublicly stated its interest in pursuingthis suicide prevention initiative. In1995 the AMA wrote to Members ofParliament and automotive manu-facturers urging action and the AMA’sEthics, Science and Social IssuesCommittee and policy officer intendto pursue this matter in early 1996.
VISS has provided information on itsactivities to the AMA and offered tosupport the AMA’s efforts to restrictaccess to the means of suicide. In1996 VISS will continue to com-municate and co-operate with theAMA on this issue.
In late 1995 VISS established contactwith the Commonwealth Inter-departmental Working Group on
Youth Suicide, comprising theCommonwealth Department ofHuman Services and Health, theAttorney General’s Department andthe Commonwealth Department ofTransport, and the Youth SuicidePrevention Advisory Group, whichhas also been set up by theCommonwealth Department ofHuman Services and Health.
The latter has been established toprovide the Commonwealth withexpert and consumer advice on youthsuicide prevention activity. MUARC(through action by VISS) has beeninvited to be represented on a workinggroup of this committee which willexplore issues around access to themeans of suicide and possible optionsfor a national project or legislativeactivities.
Awareness raising among health andinjury professionals has also been partof the VISS implementation agenda.Information on the use of carbonmonoxide poisoning as a commonmeans of suicide was a majorcomponent of a paper presented at the1994 Public Health Association(PHA) Conference - ‘Non-trafficmotor vehicle injury’ (Routley V.).Posters on the topic have been acceptedfor the Third International Conferenceon Injury Prevention and Control tobe held in Melbourne in February1996 and the associated FourthInternational Conference on ProductSafety Research.
The challengeThe prevention of suicides is acomplex task and restriction of accessto the means of suicide is oneintervention where there appears tobe good potential to save lives. Since1991 suicides have surpassed motorvehicle traffic accidents as the majorcause of injury deaths in Australia
(Harrison & Cripps 1994; Harrison &Dolinis 1995). During 1996 VISSwill step up its efforts to bring togethera coalition of interested parties topush for action on the problem of carexhaust gassings and pursue theopportunities afforded to progress thisissue through its representative on theworking group of the CommonwealthYouth Suicide Prevention AdvisoryGroup.
Scalds prevention - hot drinks[reported in Hazard 3, June 1989;Hazard 11, June 92, Hazard 12September 1992]
Recommendations-hotdrinks
• develop new designs for cups,mugs, some electric kettles andcoffee makers which incor-porate the use of heavier materialand a lower centre of gravity toprevent tipping over [Hazard 3,June 1989]
• introduce a spill-resistant mugonto the Australian market[Hazard 12, Sept 92]
• educate carers to keep hot drinksout of reach of children and to useplacemats instead of tablecloths[Hazard 12, Sept 92]
• design kitchens to eliminatedangerous pathways between keywork areas, and kitchen bencheswith a rounded lip to catch spills[Hazard 12, Sept 92]
Follow-up action
• media: Herald Sun 1992,Montage April 1994, BaysideTimes April 1995, Colac HeraldJune 1995
• information requests: 18 generalscalds requests, including tworegarding spill-resistant mugs

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 5
Preventing hot drink scalds- spill resistant mugsIn 1992 VISS identified that the majorcause of scald injuries to children washot drinks being pulled or knockedonto young children. An updatedanalysis of all cases of child scalds onthe VISS database to June 1995 (Table2) reveals that this is still the case,39% of scald injuries to children agedunder 15 years are tea and coffeescalds.
For this reason VISS has concentratedmuch of its efforts on getting anattractive and well designed spillresistant tea/coffee mug onto theAustralian market. The availabilityof a safe, attractive spill-resistant mugwould facilitate the promotion of thiscountermeasure to child scalds toparents and carers of young children.It is especially important to safeguardone to two year olds as they are thehighest risk group for hot drink scalds.
The spill resistant mug was firstidentified as a promising counter-measure to child scalds in Hazard 12(Sept 1992). As shown in theaccompanying sketch, VISS considers
All of the products that were assessedhad some of the design characteristicsrequired but none appeared ideal, forexample, they had a wide base but nolid or had the safety features but weretoo large, too ugly or too expensive.
VISS subsequently approached anumber of Australian design and mugmanufacturing companies who wereall very helpful but their ultimateresponse was not encouraging. Thecost of developing prototypes andtooling up for production appearsprohibitive because of the smallvolume domestic market. NSWHealth experienced a similar reactionfrom the cup and mug manufacturersthey approached.
VISS also followed up a mug designthat was recently patented in the USA.An interesting design feature is thatthe mug can only be used if the lid isin place. The US health productcompany that sought the patent iscurrently at the stage of seekingfinance for tooling for production.VISS has supplied contacts for themanufacturer to follow up and willmeet the designer for discussions inFebruary 1996.
Scald injuries to children aged <15 years Table 2
Mechanism factor N %hot drinks - tea, coffee 672 39hot water - cooking 372 21
hot water - bath, tap, shower 241 14
hot water - other 104 6
cooking oil, fat 89 5
hot water - n/s 88 5
soup, gravy 81 4other 103 6
Total 1750 100%VISS data: RCH, WH, PANCH 1989-93,
LRH 4 years July 1991 to June 1995. Update of table in Hazard 12 September 1992.
Spill-resistant mug Figure 1
the essential features of a safe spillresistant mug to be a narrow mouth, awide, high friction base for maximumstability and a sip-through lid whichstays on (with minimum spillage)when the mug is in use or tipped over.
As a first step, VISS collected samplesof spill resistant mugs from companiesin Australia and the USA where theuse of this mug is promoted to coffeedrinking commuters (not a practicewe want to encourage amongAustralian drivers!).

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 6
Another avenue of investigation thatwas implemented concurrently was afield assessment of consumer attitudeto a spill-resistant mug. In 1995 the7 Eleven spill-resistant mug wasmarket tested for VISS in a researchproject conducted by Carmelo Caputo,Peter Liodakis, Vicki Psihogios andLivia Rivera, students of MonashUniversity Medical School. Thisproject examined the effectivenessand acceptability of the spill resistantmug (donated by 7 Eleven) among agroup of 50 family day care workersemployed by the City of DandenongCouncil.
The researchers reported that thecaregivers responded positively. Theproduct was found to be acceptableand convenient to use but theresearchers recommended thatawareness raising education on scaldsprevention should accompany itsintroduction. The caregiverssuggested a number of changes interms of size, shape and material toimprove the mug’s consumer appealand safety.
These research findings were used torefine VISS design specifications fora spill resistant mug. VISS recentlyinterested a South Australian mugand lid manufacturing company inthe design and, possibly, themanufacture of the product. Thecompany is currently engaged inexploring the best design, in terms ofeffectiveness and aesthetics. Theirfirst concept sketches will besubmitted to VISS in January 1996.
The issue was raised nationally in apaper presented to the First NationalConference on Injury Prevention andControl held in Sydney in 1995(Commonwealth Department ofHuman services and Health 1995)and a paper on the researchunderpinning these developments has
been accepted for presentation to theFourth International Conference onProduct Safety Research to be held inCanberra in February 1996.
A VISS staff member is also co-ordinating the Spill-Resistant MugWorking Party of the VictorianPrevention of Child Injury Committee(established by the Department ofHealth and Community Services).
The challengeThe recent progress on thedevelopment of the design andprototype of a spill-resistant mug willinfluence the steps that will be takenin 1996. VISS intends to approachpotential sponsors if the prototypedesign satisfies VISS specifications.Kidsafe has indicated a strong interestin assisting in marketing the productwhen it becomes available.
More than three years have elapsedsince VISS identified scalds from cupsof tea and coffee as the major risk forthermal injury among young childrenand recommended the developmentof an acceptable spill resistant mug.In this period three hundred moreVictorian children have presented withscalds from hot cups of tea and coffeeto the four hospital emergencydepartments covered by VISS.
The time and persistent effort thatwere required to progress this Hazardrecommendation exemplifies the needfor more infrastructure and projectspecific funding to increase thecapacity of VISS to pursue interven-tions that arise from its researchfindings.
Burns prevention -cigarettes/lighters/matches[reported in Hazard 11, June 92;Hazard 12, Sept 92; Hazard 21,Dec 94]
Recommendations
• consider installing sprinklers ininstitutions housing elderlysmokers [Hazard 11, June 92]
• consider the introduction oflegislation for the mandatorymanufacture of low fire risk (selfextinguishing) cigarettes[Hazard 12, Sept 92; Hazard21, Dec 94 ]
• develop a low cost child-resistant cap for cigarettelighters and a child-resistantmatchbox (or import from USA.and U.K. respectively) andmandate their use in Australia[Hazard 12, Sept 92; Hazard21, Dec 94 ]
• support initiatives to reducesmoking [Hazard 21, Dec 94]
As reported in Hazard 12 and 21 burninjuries to children resulting fromplaying with cigarette lighters,although uncommon, are severe.Cigarette lighters were the cause of16% of the 31 smoking related deathsrecorded on the Victorian Coroner’sFacilitation System database duringthe period 1989/90 to 1991/92.Almost all of the cigarette lightercases involved a child under 5 yearsold playing with the lighter.
VISS Hospital EmergencyDepartment database shows that overhalf the children under five years whosuffer burns from cigarette lightersrequire admission to hospital.
Hazard 21 called for governments toregulate that all cigarette lighters on

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 7
sale in Australia should have child-resistant catches. To date there hasbeen no positive response from theCommonwealth or any Stategovernment, despite the introductionof this safer product onto theAustralian market.
Cricket, and to a lesser extent Bic,child resistant cigarette lighters arenow sold in major supermarket chains.Cricket lighters are currently promotedby Bryant and May through mediaadvertising and a lighter swap scheme.
At the suggestion of VISS, Kidsafehas arranged for a display pack of 25cigarette lighters to be donated byBryant and May to every Maternaland Child Health Centre in Victoria.These centres will promote a lighterswap scheme to parents of youngchildren as a means of raisingawareness of the availability of thisproduct among one of the highest riskgroups This promotion will exposesome 25,000 parents across Victoriato this safer product.
Similar exchange schemes operate atthe Child Safety Centre at the RoyalChildren’s Hospital (RCH),Melbourne and, for families whosechildren are fire lighters, through thePsychiatry Department of the RCH.
Despite the initiatives to educate theconsumer taken by Bryant and Mayand child injury prevention bodies,child resistant lighters currently makeup only four percent of the Australiancigarette lighter market share. Thispoor uptake by consumers indicatesthat more stringent measures arerequired.
The Cricket child resistant disposablelighter retails at more than double theprice of regular disposable lighters($1.95 v. 89-95 cents). Whileincreased production would reducethe cost of the child resistant lighter,
its higher price acts as a disincentivefor the wider implementation of thissafety measure.
Another burn prevention recommen-dation in Hazard 21 was the intro-duction of a child resistant matchboxsuch as Matchguard, which ismanufactured in the U.K.
Efforts by VISS to interest localmanufacturers in the production of asimilar product (designed to hold thestandard size Australian smallcardboard match box) have not beensuccessful. The high cost of toolingand low volume local market are againgiven by manufacturers as reasons fortheir lack of interest in manufacturingthis safety product.
The challengeMore active intervention by therelevant government authorities isrequired to decrease these burninjuries. Child resistant cigarettelighters are mandatory in the USAand Canada so there is a persuasiveprecedent for similar regulatory actionin Australia. The MelbourneMetropolitan Fire Brigade and otherfire prevention bodies are majorprotagonists for regulations in thisarea. VISS will continue its efforts tostimulate government regulatoryaction in 1996.
Child resistant Figure 2cigarette lighter
Child falls prevention -babywalkers[reported in Hazard 14, Mar 93 (homeinjuries); Hazard 16, Sept 93 (thesafety of babywalkers); Hazard 20,Sept 94 (an update)]
Recommendations
• impose an Australian productban on babywalkers or, lesspreferably, change the design toincorporate a broad base that iswider than household doorways[Hazard 14, Mar 93]
• raise public awareness of therisks associated with baby-walkers and the necessity ofstair guards and supervision[Hazard 16, Sept 93]
• encourage retailers to refuse tosell babywalkers [Hazard 16,Sept 93]
Follow-up action• media: The Sunday Age,
Townsville Bulletin, Herald-Sun, Sunday Herald Sun,Waverley Gazette, Channel 7,ABC Regional TV.
• information requests: nine,including invited submissionfrom the Federal Minister forConsumer Affairs.
• research study, based on VISSdata, on facial injuries sustainedby small children in babywalkers or prams.
• exposure data provided throughthe Australian Bureau ofStatistics (ABS) “Safety in theHome” survey conducted inMelbourne in November 1992enabled VISS to calculaterelative risk compared to othernursery items [Hazard 20, Sept94] which further supported theneed for a product ban orchanged design.

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 8
Babywalkers are an injury hazard. InVictoria each year there is a risk that1 in every 192 babywalkers will causea significant injury resulting in ahospital emergency departmentpresentation to a child less than oneyear of age. Babywalkers have beenshown to be of no benefit to the baby,in fact there is evidence that their usemay hinder child development.
VISS and other Australian andoverseas data have consistently shownthat babywalker use is associated withserious injury, for example, stairwayfalls and burns. In the US in 1993babywalkers were associated with25,000 hospital emergency depart-ment presentations among childrenaged 5-15 months and the deaths of11 children in the period from 1989through 1993 (Murray 1995).
VISS has maintained continuouspressure on Commonwealth and StateConsumer Affairs bodies to havebabywalkers banned, or, lesspreferably, the Australian standardrevised (as was done in Canada) todemand a broader and more stablebase. This latter approach to theproblem would limit the mobility ofbabies using babywalkers, preventingthem getting through doorways. TheFederal Bureau of Consumer Affairs(FBCA) has declined to place aproduct ban on babywalkers citinglegal impediments as it is the use,rather than the product itself, that isunsafe.
However, in 1995 the Federal Ministerfor Consumer Affairs, The Hon.Jeannette McHugh wrote to 350retailers of babywalkers asking themto voluntarily withdraw this product.This action was influenced by thedecision of the Myer group ofdepartment stores to withdrawbabywalkers from sale following
earlier adverse media reportsgenerated by VISS.
The Minister’s action through theFederal Bureau of Consumer Affairsand the media attention given to theissue as a result of reports in threeissues of Hazard appear to have had abeneficial effect in Victoria.
A VISS survey of 13 major retailoutlets in a cross section of Melbournesuburbs in November 1995 found thatother major general retail chains(Target, K-Mart and Toys R Us) hadwithdrawn babywalkers from sale“because they were unsafe ordangerous”, as had some specialistnursery furniture retailers.
Two of the five specialist nurseryfurniture retailers that still soldbabywalkers reported that they onlystocked models which they perceivedto have special safety features (forexample, models with eight wheels
and a high padded back or wheels thatcan be locked). The retailers regardedthese models as comparatively safe,indicating that they also had someawareness of the injury issue.
The issue has been raised by VISS inconference papers given at the SecondWorld Conference on Injury Control,Atlanta USA, 1993; the Public HealthAssociation Seminar ‘The Health ofMothers and Children’, Melbourne1993; the Children’s NurseryFurniture Seminar, Royal Children’sHospital, Melbourne, 1994; and theHealth and Community ServicesConference, ‘Healthy Families,Healthy Children’, Melbourne, 1994.
The challengeIn 1996 VISS will continue to workwith other child injury preventionagencies to pressure the FederalBureau of Consumer Affairs to reviewits position and place a product ban onbabywalkers.
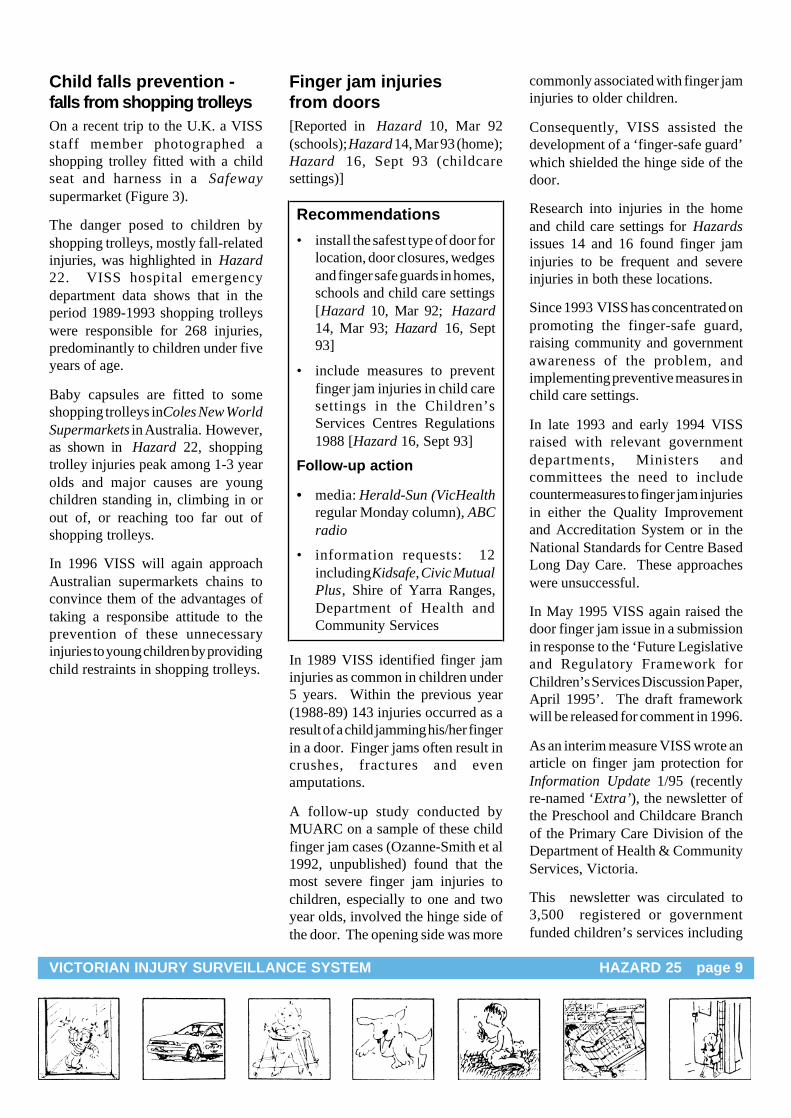
Shopping trolley fitted with child seat Figure 3
VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 9
Child falls prevention -falls from shopping trolleysOn a recent trip to the U.K. a VISSstaff member photographed ashopping trolley fitted with a childseat and harness in a Safewaysupermarket (Figure 3).
The danger posed to children byshopping trolleys, mostly fall-relatedinjuries, was highlighted in Hazard22. VISS hospital emergencydepartment data shows that in theperiod 1989-1993 shopping trolleyswere responsible for 268 injuries,predominantly to children under fiveyears of age.
Baby capsules are fitted to someshopping trolleys in Coles New WorldSupermarkets in Australia. However,as shown in Hazard 22, shoppingtrolley injuries peak among 1-3 yearolds and major causes are youngchildren standing in, climbing in orout of, or reaching too far out ofshopping trolleys.
In 1996 VISS will again approachAustralian supermarkets chains toconvince them of the advantages oftaking a responsibe attitude to theprevention of these unnecessaryinjuries to young children by providingchild restraints in shopping trolleys.
commonly associated with finger jaminjuries to older children.
Consequently, VISS assisted thedevelopment of a ‘finger-safe guard’which shielded the hinge side of thedoor.
Research into injuries in the homeand child care settings for Hazardsissues 14 and 16 found finger jaminjuries to be frequent and severeinjuries in both these locations.
Since 1993 VISS has concentrated onpromoting the finger-safe guard,raising community and governmentawareness of the problem, andimplementing preventive measures inchild care settings.
In late 1993 and early 1994 VISSraised with relevant governmentdepartments, Ministers andcommittees the need to includecountermeasures to finger jam injuriesin either the Quality Improvementand Accreditation System or in theNational Standards for Centre BasedLong Day Care. These approacheswere unsuccessful.
In May 1995 VISS again raised thedoor finger jam issue in a submissionin response to the ‘Future Legislativeand Regulatory Framework forChildren’s Services Discussion Paper,April 1995’. The draft frameworkwill be released for comment in 1996.
As an interim measure VISS wrote anarticle on finger jam protection forInformation Update 1/95 (recentlyre-named ‘Extra’), the newsletter ofthe Preschool and Childcare Branchof the Primary Care Division of theDepartment of Health & CommunityServices, Victoria.
This newsletter was circulated to3,500 registered or governmentfunded children’s services including
Finger jam injuriesfrom doors[Reported in Hazard 10, Mar 92(schools); Hazard 14, Mar 93 (home);Hazard 16, Sept 93 (childcaresettings)]
Recommendations
• install the safest type of door forlocation, door closures, wedgesand finger safe guards in homes,schools and child care settings[Hazard 10, Mar 92; Hazard14, Mar 93; Hazard 16, Sept93]
• include measures to preventfinger jam injuries in child caresettings in the Children’sServices Centres Regulations1988 [Hazard 16, Sept 93]
Follow-up action
• media: Herald-Sun (VicHealthregular Monday column), ABCradio
• information requests: 12including Kidsafe, Civic MutualPlus, Shire of Yarra Ranges,Department of Health andCommunity Services
In 1989 VISS identified finger jaminjuries as common in children under5 years. Within the previous year(1988-89) 143 injuries occurred as aresult of a child jamming his/her fingerin a door. Finger jams often result incrushes, fractures and evenamputations.
A follow-up study conducted byMUARC on a sample of these childfinger jam cases (Ozanne-Smith et al1992, unpublished) found that themost severe finger jam injuries tochildren, especially to one and twoyear olds, involved the hinge side ofthe door. The opening side was more

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 10
childcare, preschool and occasionalcare centres, school-age services, peakbodies and interested associations.
Civic Mutual Plus, the insurer of 98%of Victorian Local Government Areas(LGAs) included finger jam protectionin their March 1995 Risk ManagementManual update. Their attention wasdrawn to the issue by media reports ofVISS findings published in Hazardand the information used in thismanual update was largely from VISS.
In terms of implementation, in 1995the Shire of Yarra Ranges was awardeda grant of $10 000 by the VictorianDepartment of Health and CommunityServices to reduce finger jam injuriesamong children in their own homesand child care settings.
The Shire incorporated informationfrom VISS on the prevention of fingerjam injuries, including the use of doorguards, in their training program fornew child care workers and raisedawareness of the issue among thegeneral public during Children’s Week1995. The Shire will produce aneducational video on the topic in 1996.
Kidsafe has included VISSinformation on finger jam injuries inits leaflet on outdoor safety in pre-school centres to be distributed in1996.
Sales of this door hinge finger jamprotective device have increased at anaccelerated rate during 1995. Salesalmost doubled from 338 in the secondquarter of the year to 640 in the thirdquarter.
This jump in sales can be attributed toa number of factors: the RiskManagement Manual update; asuccessful litigation case which drewattention to the issue; greaterawareness through VISS input into
the media and a Department of Health& Community Services publication;and the promotion work undertakenby the Child Safety Centre at theRoyal Children’s Hospital amongchild care bodies seeking governmentaccreditation.
During 1995 VISS encouraged aneducational toy shop Hop, Step andJump to stock finger safe guards asthe number of sale outlets for theproduct was very limited.
A recent development is theestablishment by the VictorianPrevention of Child Injury Committeeof the Finger Jam Prevention WorkingParty. Its brief is to examine theissues surrounding finger jam injuries,develop prevention strategies andmake recommendations on theirimplementation. VISS is representedon this working party.
The challengeIn 1996 VISS will continue its effortsto increase community awareness ofthis issue and push for the use ofproducts which prevent door fingerjams in homes, child care settings,kindergartens and schools through itswork for the Victorian Prevention ofInjury Committee and other avenues.
Community awareness (and sales) ofthe finger-safe guard will need toincrease dramatically for this measureto have any significant impact on thefinger jam injury problem.
Prevention of needlestickinjuries[reported in Hazard 17, Sept 93(workplace)]
Recommendations
• use disposable syringes [Hazard17, Sept 93]
• develop and promote the use ofsafer products eg. pliable andpuncture resistant gloves, lowcost retractable needles andother devices such as rubbersheath removers that minimisecontact with a sharp [Hazard17, Sept 93]
• educate health care staff aboutcurrent recommendations oninfection control practices andways to reduce exposure[Hazard 17, Sept 93]
• immunise hospital staff againstHepatitis B [Hazard 17, Sept93]
Accidental needlestick injuries are aserious concern because of the risk ofblood-borne transmission of HepatitisB and C and HIV. There were 225needlestick injuries reported on theVISS hospital emergency presenta-tions database in the period 1991-1992. Injured workers were pre-dominantly registered nurses, medicalpractitioners, State enrolled nursesand cleaners.
Hazard 17 recommended an holisticapproach to this problem whichincludes education of healthcareworkers and the development andpromotion of safer products.
A company that has taken thisapproach and invested heavily inresearch and development of safety-engineered products and educationprograms to minimise the risk from

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 11
hypodermic products is BectonDickinson, the world’s largestmanufacturer of needles and syringes.
As shown in the Figure 4, theB-DSafety Lok Syringe is fittedwith a sliding shield that locks overthe needle and an indicator whichturns red to green to confirm that theshield is in place and safe for disposal.This syringe is suitable for widespreadgeneral use in place of standarddisposable syringes. However, thehigher cost-per-item (currently morethan double the cost of a standarddisposable syringe) is a barrier to use,although the cost differential isshrinking as the volume of productionincreases.
Another of the company’s productsthat has the potential to significantly
reduce needlestick injuries in hospitalsettings is the Interlink IV AccessSystem (co-promoted with BaxterHealthcare). This intravenous therapysystem introduces an advanced designinjection site and safe blunt cannulato replace conventional needles. Iteliminates up to 80% of the sharpsteel needles formerly used forintravenous administration.
While many hospitals have intro-duced needleless systems for theadministration of anaesthetics,Victoria appear to be lagging behindother States in adopting hospital-wideneedleless systems. From theinformation supplied to VISS in late1995, sixteen NSW hospitals haveintroduced a hospital-wide system,while the Maroondah Hospital is theonly Victorian hospital to do so.
The B-DSafety Lok Syringe Figure 4
ReferencesChalmers D. “Prevention of armfractures in playground falls. Do wehave the answers?” in Proceedingsfrom The First National Conferenceon Injury Prevention and Control heldon 27-28 February 1995, Sydney,NSW. Commonwealth Departmentof Human Services and Health .AGPS, 1995.
Harrison JE, Cripps RA (editors).Injury in Australia: an epidemiologicalreview. Canberra, AGPS, 1994(Chapter 10).
Harrison JE, Dolinis J. InjuryMortality Australia 1993. AustralianInjury Prevention Bulletin 10, August1995.
Murray T. “US pediatricians urgerecall, ban on baby walkers”. InjuryPrevention 1995;1: 149-151.
Ozanne-Smith J et al. “Finger jaminjuries to children in doors” in Childaccident and injury preventionresearch in other than road accidents(unpublished). Monash UniversityAccident Research Centre. 1992.
Victorian Injury Surveillance SystemHazard Volume 1, Editions 1 to 10,Injury data and prevention. MonashUniversity Accident Research Centre.March 1993.
Victorian Injury Surveillance SystemHazard Volume 2, Editions 11 to 20,Injury data and prevention. MonashUniversity Accident Research Centre.February 1995.
Victorian Injury Surveillance System“Smoking-related injuries” in HazardEdition 21, Domestic Violence.Monash University AccidentResearch Centre. December 1994.
Victorian Injury Surveillance SystemHazard Edition 22, Product relatedinjury - a selection (domesticarchitectural glass and shopping trolleysinjuries). Monash University AccidentResearch Centre. March 1995.
B-D is a registered trademark of Becton Dickinson & CompanyInterLink is a registered trademark of Baxter Healthcare

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 12
Issu
es in
Brie
f
Issu
eP
reve
ntio
n of
dom
estic
arc
hite
ctu
ral
gla
ss in
jurie
sIn
jurie
s as
soci
ated
with
rol
lerb
lad
ing
Dur
ing
the
per
iod
1989
to
1993
the
re w
ere
862
arc
hite
ctu
ral g
lass
inju
ries
re
cord
ed o
n th
e V
ISS
hos
pita
l em
erge
ncy
dep
artm
ent
data
base
. M
ost o
f th
em o
ccur
red
in t
he h
om
e an
d in
volv
ed g
lass
doo
rs a
nd
win
dow
s.
Rol
lerb
ladi
ng in
juri
es h
ave
ris
en
fro
m n
o re
cord
ed c
ases
in V
ISS
pa
rtic
ipa
ting
hos
pita
ls in
198
9 to
113
cas
es in
19
92 a
nd 1
47
case
s in
199
3.
Nea
rly h
alf o
f rol
lerb
ladi
ng in
juri
es r
ecor
ded
in 1
993
we
re w
rist i
njur
ies,
80
%
The
inju
red
wer
e p
redo
min
ant
ly m
ale
and
in th
e yo
ung
er a
ge g
roup
s (u
nder
5
year
old
s fo
r ch
ildre
n a
nd 2
0-24
yea
r ol
ds fo
r ad
ults
age
d >
15 y
ears
).
frac
ture
s.
Ele
ven
per
cent
wer
e he
ad in
jurie
s.
Th
e 10
-14
yea
r ol
d ag
e gr
oup
is m
ost a
t ris
k an
d in
juri
es o
ccur
mos
t of
ten
on
foo
tpat
hs a
nd p
ublic
T
he v
ast
maj
ority
of
the
inju
ries
we
re la
cera
tions
to t
he u
ppe
r lim
bs a
nd
face
.ro
ads.
A
sm
all f
ollo
w-u
p st
udy
in 1
992
sho
we
d th
at r
olle
rbla
ding
inju
ries
occu
rred
whe
n u
sers
wer
e le
arni
ng o
r w
hen
expe
rien
ced
rolle
rbla
ders
we
re
tryi
ng n
ew
stu
nts
(m
ost o
f the
inju
red
wer
e no
t we
arin
g w
rist g
uard
s).
Haz
ard
cov
erag
eE
diti
ons:
7,
June
19
90;
14,
Mar
93;
16
, S
ept 9
3; 2
2,
Mar
95
Ed
ition
: 15
, Ju
l 93
Key
re
com
men
datio
ns*
incl
ude
the
198
9 r
evis
ion
of t
he A
ustr
alia
n S
tand
ard
(A
S 1
288)
on
"Gla
ss
in B
uild
ings
- S
ele
ctio
n a
nd I
nsta
llatio
n"
in V
icto
ria's
bu
ildin
g c
ode
whi
ch
requ
ires
safe
ty g
lazi
ng m
ater
ials
in s
ome
resi
dent
ial s
itua
tions
* c
reat
e ar
eas
for
rolle
rbla
ding
sep
arat
ed f
rom
tra
ffic
and
ped
est
rians
and
en
cou
rage
initi
al t
rain
ing
in a
pro
tect
ed e
nvir
onm
ent
[Haz
ard
15]
* c
hild
ren
und
er 5
yea
rs o
ld s
hou
ld n
ot u
se r
olle
rbla
des
[Haz
ard
15]
whe
re a
nnea
led
gla
ss w
as
prev
ious
ly a
ccep
tabl
e [H
azar
d 7]
* r
epla
ce a
nne
ale
d gl
ass
with
saf
ety
gla
ss w
hene
ver
glas
s is
re
plac
ed
in
* p
rom
ote
the
use
of s
afet
y e
quip
me
nt (
hel
met
s, w
rist
pro
tect
ors,
kn
ee a
nd
elbo
w g
uard
s) [H
azar
d 15
]ex
istin
g ho
mes
[H
azar
d 22
]*
red
uce
the
pric
e le
vel d
iffer
entia
l bet
we
en s
afet
y a
nd a
nnea
led
glas
s [ H
azar
d 22
] *
pro
mot
e th
e a
pplic
atio
n o
f spe
cial
pla
stic
film
, ba
rs, r
ails
or
war
ning
st
icke
rs o
n ex
istin
g ha
zard
ous
glas
s [H
azar
d 7
& 2
2]
* r
olle
rbla
de h
ire
outle
ts s
houl
d al
so h
ire o
ut p
rote
ctiv
e e
quip
men
t; h
irers
an
d se
llers
sho
uld
giv
e ad
vice
on
fittin
g o
f rol
lerb
lade
s, o
ffer
initi
al t
uitio
n an
d re
com
men
d t
he u
se o
f sa
fety
eq
uipm
ent
[Haz
ard
15]
Med
ia fo
llow
-up
* G
lass
Aus
tral
ia (
trad
e jo
urna
l)*
She
ppar
ton
New
s; T
he A
ge; T
he T
oday
Sho
w (
Cha
nne
l 9);
Aus
tral
ian
Jour
nal o
f Pae
diat
rics
and
Chi
ld H
ealth
; Kid
safe
Mag
azin
e.
Info
rmat
ion
requ
ests
* e
igh
t inc
ludi
ng O
'Brie
n's
Gla
ss*
fou
r in
clu
ding
Dep
artm
ent
of O
rtho
pae
dics
(R
oyal
Chi
ldre
n's
Hos
pita
l)
Fur
ther
act
ion
* r
esea
rch
stu
dy
by D
rs N
olan
and
Co
urt (
Roy
al C
hild
ren
Hos
pita
l) on
a
sam
ple
of c
hild
ren
inju
red
by d
omes
tic g
lass
[Haz
ard
7]*
CS
IRO
co
ndu
cted
a s
tud
y to
de
term
ine
the
na
ture
of
the
dom
estic
gla
ss
invo
lved
in in
jurie
s [H
azar
d 7]
* r
esea
rch
use
d as
Cas
e S
tudy
in R
epo
rt t
o th
e A
ustr
alia
n C
ons
um
er's
C
ounc
il (1
993
) (S
afe
ty in
the
Mak
ing
Pro
duc
t S
afe
ty f
or t
he Y
ear
200
0 -
Mol
ler,
J.
199
4)
Impl
emen
tatio
n*
Vic
toria
ado
pte
d th
e 19
89 r
evis
ion
to t
he "
Gla
ss in
Bui
ldin
gs"
Sta
nda
rd
into
its
build
ing
code
, ope
ratio
nal f
rom
Ap
ril 1
991
for
new
hou
ses
and
ho
use
s un
derg
oin
g re
nova
tion
[Haz
ard
7]
* M
UA
RC
ha
s pr
epar
ed
a re
sear
ch p
ropo
sal t
o ex
amin
e th
e e
ffect
ive
ness
of
wris
t gu
ard
s an
d in
vest
igat
e th
eir
wea
ring
rat
e b
y ro
llerb
lad
ers.
Fut
ure
chal
leng
es*
mo
nito
r th
e e
ffec
tive
ness
of t
he r
evi
sed
Aus
tra
lian
Sta
nda
rd a
nd B
uild
ing
code
req
uire
men
t as
an
inju
ry p
reve
ntio
n m
easu
re
* p
rom
ote
the
use
of s
afet
y g
lass
whe
n d
ome
stic
gla
ss is
be
ing
repl
ace
d
* r
esea
rch
the
use
and
effe
ctiv
ene
ss o
f pro
tect
ive
equ
ipm
ent
esp
ecia
lly
wris
t gu
ard
s*
sur
vey
hire
out
lets
to
det
erm
ine
curr
ent p
ract
ice
reg
ardi
ng s
afet
y to
ho
use
hold
ers
, gla
zier
s a
nd in
sura
nce
com
pan
ies,
with
att
entio
n to
re
duci
ng t
he p
rice
diffe
rent
ial
* a
s an
inte
rim
mea
sure
pro
mot
e th
e a
pplic
atio
n o
f spe
cial
pla
stic
film
, ba
rs, r
ails
an
d/or
war
ning
stic
kers
on
exis
ting
haza
rdo
us g
lass
educ
atio
n an
d m
easu
res
* in
vest
iga
te w
heth
er
safe
ty s
trat
egie
s ar
e pr
omot
ed/
impl
emen
ted
by t
he
rolle
rbla
der
s' a
ssoc
iatio
n

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 13
Issu
eP
lay
equi
pmen
t-re
late
d in
jury
D
og b
ites
The
re w
ere
4,23
7 ca
ses
of p
lay
equi
pmen
t-re
late
d in
jury
to
child
ren
unde
r 15
yea
rs o
f age
rep
orte
d by
VIS
S p
artic
ipat
ing
hosp
itals
in th
e pe
riod
1989
-93
. T
he 5
-9 y
ear
age
grou
p w
as m
ost a
t ris
k of
thes
e in
jurie
s. I
njur
ies
In t
he f
ive
year
per
iod
1989
to 1
993,
109
3 ch
ildre
n pr
esen
ted
to V
ISS
pa
rtic
ipat
ing
hosp
itals
with
dog
bite
s, 2
6% o
f th
ese
case
s w
ere
adm
itted
to
hosp
ital.
Chi
ldre
n un
der
5 ye
ars,
par
ticul
arly
todd
lers
, wer
e m
ost a
t ris
k .
mos
tly o
ccur
red
in s
choo
l pla
ygro
unds
and
oth
er c
hild
care
set
tings
(47
%),
fo
llow
ed b
y pr
ivat
e ho
mes
(18
%)
and
publ
ic a
nd p
rivat
e or
com
mer
cial
pl
aygr
ound
s an
d am
usem
ent
area
s (1
7%).
O
ver
80%
of
inju
ries
resu
lted
Out
door
s at
hom
e w
as th
e m
ost
freq
uent
loca
tion
for
child
dog
bite
inju
ries
(54%
of c
ases
). I
n th
e th
ree
year
per
iod
1991
-94,
ther
e w
ere
516
adul
t ca
ses
of d
og b
ite in
jury
rep
orte
d in
the
VIS
S d
atab
ase.
from
falls
. M
onke
y ba
rs, s
lides
or
slid
ing
boar
ds,
swin
gs a
nd s
win
g se
ts
wer
e th
e pi
eces
of
play
equ
ipm
ent
mos
t fre
quen
tly in
volv
ed in
inju
ries
to
Haz
ard
cov
erag
eE
ditio
ns: 2
, Dec
88
(joy
whe
els)
; 3, J
uly
1989
; 4, N
ov 1
989;
10
, Mar
92
(sch
ools
);14
, Mar
93
(hom
e in
jurie
s);
16, S
ept 9
3 (c
hild
car
e se
tting
s)E
ditio
ns: 3
, Jul
y 19
89; 4
, Nov
89;
12
, Sep
t 92;
18
, Mar
ch 9
4 (w
ork-
rela
ted)
Key
re
com
men
datio
ns*
add
ress
des
ign
fact
ors
that
are
ass
ocia
ted
with
pla
y eq
uipm
ent i
njur
ies
incl
udin
g he
ight
of e
quip
men
t, sa
fety
rai
ls, s
ize
and
dist
ance
bet
wee
n ba
rs,
stab
ility
and
layo
ut o
f equ
ipm
ent a
nd r
evis
e A
ustr
alia
n S
tand
ards
* p
rom
ote
the
deve
lopm
ent o
f a
radi
ator
cap
tha
t has
a s
afet
y va
lve
and
devi
ces
such
as
mag
netic
def
lect
ors
whi
ch d
efle
ct th
e bo
iling
rad
iato
r w
ater
/ste
am d
ownw
ards
to p
rote
ct t
he m
otor
ist o
r m
echa
nic
[ Haz
ard
20]
[Haz
ard
3, 1
4, 1
6]*
inst
all a
nd m
aint
ain
effe
ctiv
e im
pact
abs
orbi
ng u
nder
surf
acin
g to
the
reco
mm
ende
d de
pth
of 2
00m
m (
com
mun
ity p
layg
roun
ds 2
50m
m)
* d
evel
op a
rad
iato
r ca
p w
hich
can
not b
e re
mov
ed if
the
wat
er te
mpe
ratu
re
is a
bove
a d
esig
nate
d te
mpe
ratu
re o
r pr
essu
re [ H
azar
d 1
2 &
20]
* pr
omot
e th
ese
safe
ty r
ules
to m
otor
ists
: wai
t for
the
vehi
cle
radi
ator
cap
[Haz
ard
3, 1
4, 1
6]*
atte
nd to
the
desi
gn, m
aint
enan
ce a
nd c
onfo
rman
ce to
the
new
Aus
tral
ian
Sta
ndar
d (A
S 2
155)
, whe
n av
aila
ble,
for
play
equ
ipm
ent a
nd u
nder
surf
acin
g in
all
prim
ary
scho
ols,
chi
ld c
are
sett
ings
(in
clud
e
to c
ool d
own
befo
re to
uchi
ng; r
elea
se to
the
first
clic
k an
d re
mov
e ca
p if
th
ere
is n
o pr
essu
re [ H
azar
d 2
0]
conf
orm
ance
in C
hild
ren'
s S
ervi
ces
Cen
tres
Reg
ulat
ion
Med
iafo
llow
-up
Her
ald-
Sun
, Ade
laid
e A
dver
tiser
, A
BC
rad
io, H
eral
d-S
un, T
he S
unda
y A
ge,
60 M
inut
esIn
form
atio
n re
ques
tsP
layg
roun
ds -
fiv
e in
clud
ing
The
Pla
ygro
unds
and
Rec
reat
ion
Ass
ocia
tion
of
Vic
toria
, S
hire
of B
ulla
Saf
e Li
ving
Pro
gram
, in
divi
dual
loca
l gov
ernm
ent
coun
cils
Sch
ool p
lay
area
s -
23 in
clud
ing
Out
door
Edu
catio
n D
epar
tmen
t, S
hire
of
Bul
la S
afe
Livi
ng P
rogr
am, L
atro
be V
alle
y B
ette
r H
ealth
Pro
gram
, Q
ueen
slan
d C
ounc
il of
Par
ents
and
Citi
zens
; pro
pose
d S
choo
lsaf
e p
rogr
amF
urth
er a
ctio
n*
Pla
ygro
und
and
Rec
reat
ion
Ass
ocia
tion
of V
icto
ria fo
llow
-up
stud
y of
pl
aygr
ound
inju
ries
iden
tifie
d by
VIS
S, i
nclu
ding
site
inve
stig
atio
ns a
nd
inte
rvie
ws
with
vic
tims/
care
rs p
ublis
hed
with
rec
omm
enda
tions
[ Haz
ard
10
* V
ISS
atte
mpt
s to
con
tact
the
man
ufac
ture
r of
mag
netic
def
lect
ors
wer
e un
succ
essf
ul -
the
pro
duct
is n
o lo
nger
on
the
mar
ket
Mar
92]
Impl
emen
tatio
n*
nin
e jo
y w
heel
s re
mov
ed fr
om p
layg
roun
ds b
y S
t Kild
a C
ounc
il ov
er a
th
ree
mon
th p
erio
d fo
llow
ing
VIS
S r
epor
t[Haz
ard
2, D
ec 8
8]*
the
1982
Aus
tral
ian
Sta
ndar
d ha
s be
en u
nder
rev
iew
by
a S
tand
ards
Aus
tral
ia C
omm
ittee
sin
ce 1
986
but
no a
gree
men
t on
revi
sion
s ha
s be
en
reac
hed
to d
ate
* S
tand
ards
Aus
tralia
is c
urre
ntly
con
side
ring
the
adop
tion
of th
e N
SW
K
idsa
fe G
uide
lines
on
Saf
e P
layg
roun
dsF
utur
e C
halle
nges
* fu
rthe
r re
sear
ch to
con
firm
and
ref
ine
findi
ngs
repo
rted
at
the
Firs
t N
atio
nal C
onfe
renc
e on
Inju
ry P
reve
ntio
n an
d C
ontr
ol 1
995
by D
r D
avid
C
halm
ers
(Inj
ury
Pre
vent
ion
Res
earc
h U
nit,
NZ
) re
gard
ing
fall
heig
hts
and
* id
entif
y th
e re
spon
sibl
e au
thor
ity w
ho s
houl
d ta
ke u
p th
e is
sue
of n
on-
traf
fic m
otor
veh
icle
rel
ated
inju
ries
incl
udin
g ca
r ra
diat
or s
cald
s
play
grou
nd e
quip
men
t inj
ury
(i.e.
that
falls
from
hei
ghts
in e
xces
s of
1.5
m
etre
s w
ere
over
four
tim
es m
ore
likel
y to
res
ult
in in
jury
tha
n fa
lls fr
om 1
.5
met
res
or le
ss)
* a
ctio
n to
bre
ak th
e im
pass
e th
at h
as d
evel
oped
ove
r th
e in
trod
uctio
n of
a
revi
sed
Sta
ndar
d fo
r pl
aygr
ound
s w
hich
incl
udes
und
ersu
rfac
ing

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 14
- INDEX -Subject Edition PagesBabywalkers, update .................................................................................................................. 16,20........................... 1-4,12-13Bunkbeds ......................................................................................................................................... 11 ....................................... 12Bicycles
- Bicyle related injuries ......................................................................................................... 6 ...................................... 1-8- Cyclist head injury study ................................................................................................... 2, ......................................... 2- Cyclist head injury study updates ............................................................................... 7,8,10 ................................. 8,13,9
Burns- Scalds ................................................................................................................................... 3 ...................................... 1-4- Burns prevention ............................................................................................................... 12 .................................... 1-11
Chainsaw injuries ............................................................................................................................ 22 .................................. 13-17Child care settings ........................................................................................................................... 16 .................................... 5-11Data base use, interpretation & example of form ............................................................................ 2 ...................................... 2-5Deaths from injury (Victoria) ......................................................................................................... 11 .................................... 1-11Dishwasher machine detergents - Update ...................................................................................... 18 ....................................... 11Dogs
- Dog related injuries ............................................................................................................. 3 ...................................... 5-6- Dog bite injuries ................................................................................................................ 12 ....................................... 12
Domestic architectural glass ........................................................................................................7,22............................. 9-10,2-5Domestic Violence .......................................................................................................................... 21 ...................................... 1-9Drownings/near drownings
- Immersions .......................................................................................................................... 2 ......................................... 3- Pool fencing leglislation, update ..................................................................................... 2,7 ...................................... 3,7- Drownings & near-drownings at home ............................................................................... 5 ...................................... 1-4
Escalator and elevator injuries ....................................................................................................... 24 .................................... 9-13Exercise bicycles, update ............................................................................................................... 5,9 ...............................6,13-14Home injuries .................................................................................................................................. 14 .................................... 1-16Horse related injuries ...................................................................................................................7,23............................. 1-6,1-13Infants - injuries in the first year of life ........................................................................................... 8 .................................... 7-12Intentional injuries .......................................................................................................................... 13 .................................... 6-11Latrobe Valley
- The first three months ......................................................................................................... 9 .................................... 9-13- Latrobe Valley injuries .................................................................................. * March 1992 ...................................... 1-8- Injury surveillance & prevention in the L. V. ..................................................... *Feb 1994 .................................... 1-14
Lawn mower injuries ...................................................................................................................... 22 ...................................... 5-9Martial arts ...................................................................................................................................... 11 ....................................... 12Motor vehicle related injuries, non-traffic ..................................................................................... 20 ...................................... 1-9Needlestick injuries......................................................................................................................... 11 ....................................... 12Older people, injuries among.......................................................................................................... 19 .................................... 1-13Off-street parking areas .................................................................................................................. 20 .................................. 10-11Playground equipment ...................................................................................................................... 3 ...................................... 7-9Poisons
- Child resistant closures ....................................................................................................... 2 ......................................... 3- Drug safety and poisons control ......................................................................................... 4 ...................................... 1-9- Dishwasher detergent, update ........................................................................................10,6................................. 9-10,9
Roller Blades ................................................................................................................................... 15 .................................. 11-13School injuries................................................................................................................................. 10 ...................................... 1-8Shopping trolley injuries................................................................................................................. 22 .................................. 10-12Skateboard injuries............................................................................................................................ 2 ...................................... 1-2Smoking Related injuries ................................................................................................................ 21 .................................. 10-12Sports
- Sports related injuries.......................................................................................................... 8 ...................................... 1-6- The 5 most common sports ................................................................................................. 9 ...................................... 1-8- Adult sports injury............................................................................................................. 15 .................................... 1-10
Tractor injuries ................................................................................................................................ 24 ...................................... 1-8Trampolines..................................................................................................................................... 13 ...................................... 1-5VISS: early overview ........................................................................................................................ 1 ...................................... 1-5VISS: how it works ........................................................................................................................... 1 ...................................... 6-8Work Related Injuries ................................................................................................................ 17,18........................... 1-13,1-10
* Special edition

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 15
Editorial BoardProfessor Peter Vulcan, Monash University Accident Research Centre
Dr Joan Ozanne-Smith, Monash University Accident Research Centre
Assoc. Professor Terry Nolan, Department of Paediatrics, Melbourne University
Mr. Jerry Moller , National Injury Surveillance Unit
VISS StaffDirector: Dr Joan Ozanne-Smith
Co-ordinators: Virginia RoutleyGraeme Watt
Research Assistant: Karen Ashby
Administrative Assistant: Christine Chesterman
Data Processor: Julia Palmer Latrobe Regional Hospital
Associate Director: Dr Terry Nolan(Child Injuries)
GeneralAcknowledgementsParticipating HospitalsLatrobe Regional Hospital (Traralgon and Moe)
The contributions to the collection of VISS data by the director and staff of theEmergency Departments of these hospitals, other particpating clinicians, MedicalRecords Departments, and ward staff are all gratefully acknowledged. Thesurveillance system could not exist without their help and co-operation.
Coronial ServicesAccess to coronial data and links with the development of the Coronial Service’sstatistical database are valued by VISS.
National Injury Surveillance UnitThe advice and technical back-up provided by NISU is of fundamental importanceto VISS.
How toAccess VISSData:VISS collects and tabulates informa-tion on injury problems in order tolead to the development of preventionstrategies and their implementation.VISS analyses are publicly availablefor teaching, research and preventionpurposes. Requests for informationshould be directed to the VISS Co-ordinators or the Director bycontacting them at the VISS office.
VISS is located at:Building 70Accident Research CentreMonash UniversityWellington RoadClayton, Victoria, 3168
Postal address:
As above
Phone:
Reception (03) 9905 1808
Co-ordinators (03) 9905 1805(03) 9905 1815
Director (03) 9905 1810
Fax (03) 9905 1809

VICTORIAN INJURY SURVEILLANCE SYSTEM HAZARD 25 page 16
VISS is a project of the Monash University Accident Research Centre.
Hazard was produced by the Victorian Injury Surveillance Systemwith the layout assistance of Glenda Cairns, Monash University Accident Research Centre.Illustrations by Jocelyn Bell, Education Resource Centre, Royal Children’s Hospital and
Ann James, Books Illustrated.
ISSN-1320-0593
Printed by Sands and McDougall Printing Pty. Ltd., North Melbourne
Project Funded byVictorian Health Promotion Foundation