translating genomic findings into clinical practice- …€¦ · translating genomic findings into...
TRANSCRIPT
Translating genomic findings into clinical practice- MATCH-UP and
other efforts
Jonathan Rosenberg MD
Memorial Sloan Kettering
No progress in advanced UC in 20+ years
• Front-line chemotherapy remains platinum-based combinations
• No proven effective second-line agents – Vinflunine in Europe
– Optimism about immunotherapy based on MPDL3280a data
• Dramatic advances in understanding of the molecular pathophysiology UC may allow for improved patient selection and treatment outcomes
Advanced UC is a heterogeneous disease
• Multiple opportunities for targeted therapies, though each class of agents may only be useful for a minority of patients
• Unselected trials with targeted agents unlikely to yield positive results
• Therefore, would need to screen for activity in selected populations
• NCI MATCH trial is a multi-arm trial agnostic to histology with treatment based on mutations/amplifications/translocations
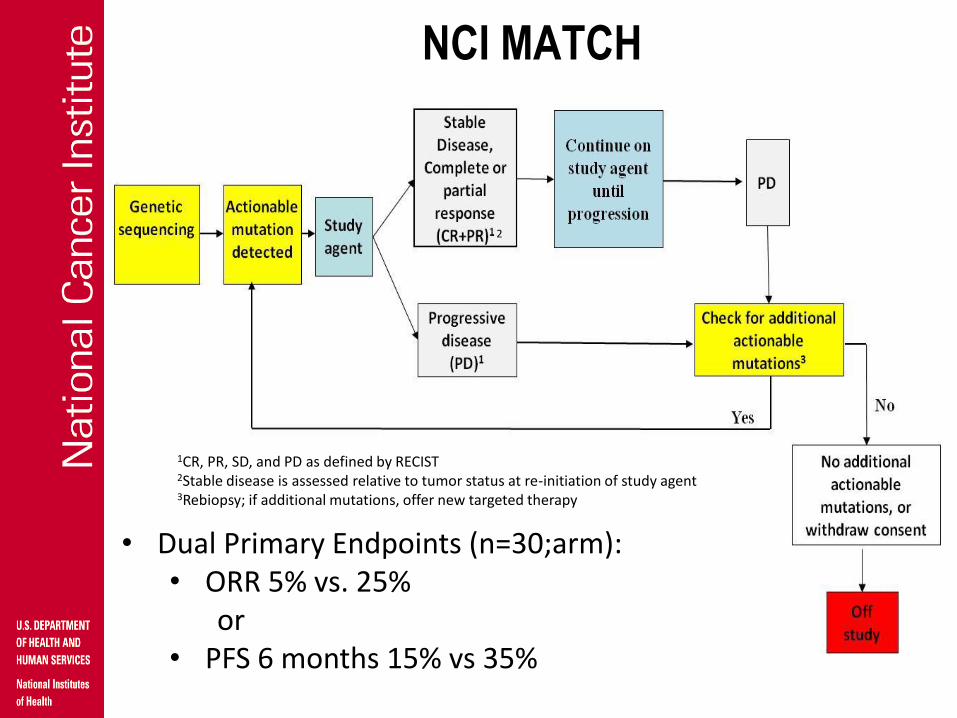
NCI MATCH
• Dual Primary Endpoints (n=30;arm): • ORR 5% vs. 25%
or • PFS 6 months 15% vs 35%
1CR, PR, SD, and PD as defined by RECIST
2Stable disease is assessed relative to tumor status at re-initiation of study agent
3Rebiopsy; if additional mutations, offer new targeted therapy
2
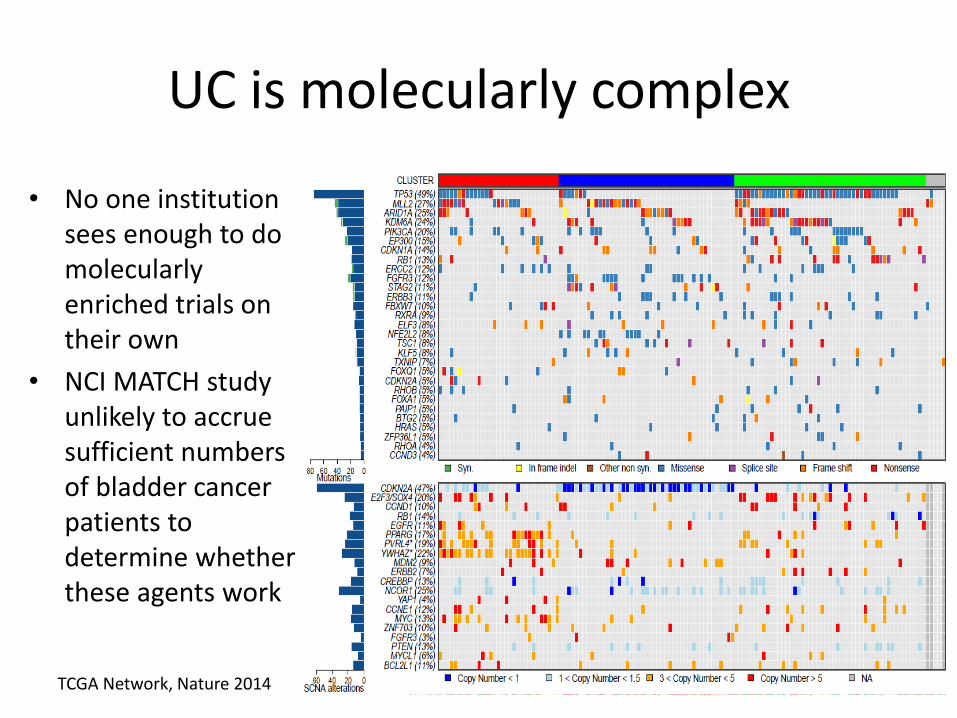
UC is molecularly complex
• No one institution sees enough to do molecularly enriched trials on their own
• NCI MATCH study unlikely to accrue sufficient numbers of bladder cancer patients to determine whether these agents work
TCGA Network, Nature 2014
What is the current evidence for targeted therapy in UC
• Case reports to date:
– Iyer et al., Science- TSC1 and everolimus
– Wagle et al., Cancer Discovery- mTOR and everolimus
What are the targets?
• List of targets is long (fortunately) with several “low-hanging fruit”
– FGFR3
– PI3-kinase
– CDK4 pathway
– EGFR
– ERBB2
– Epigenetic regulatory pathways
FGFR3
• Mutations and fusions are rare in advanced UC
– Mutation 5-15%
– Fusion 3-5% using NGS
• FGFR3 targeted therapy: TKI258 (VEGFR and FGFR inhibitor) did not have activity in mutant tumors
– Flawed assay, flawed drug
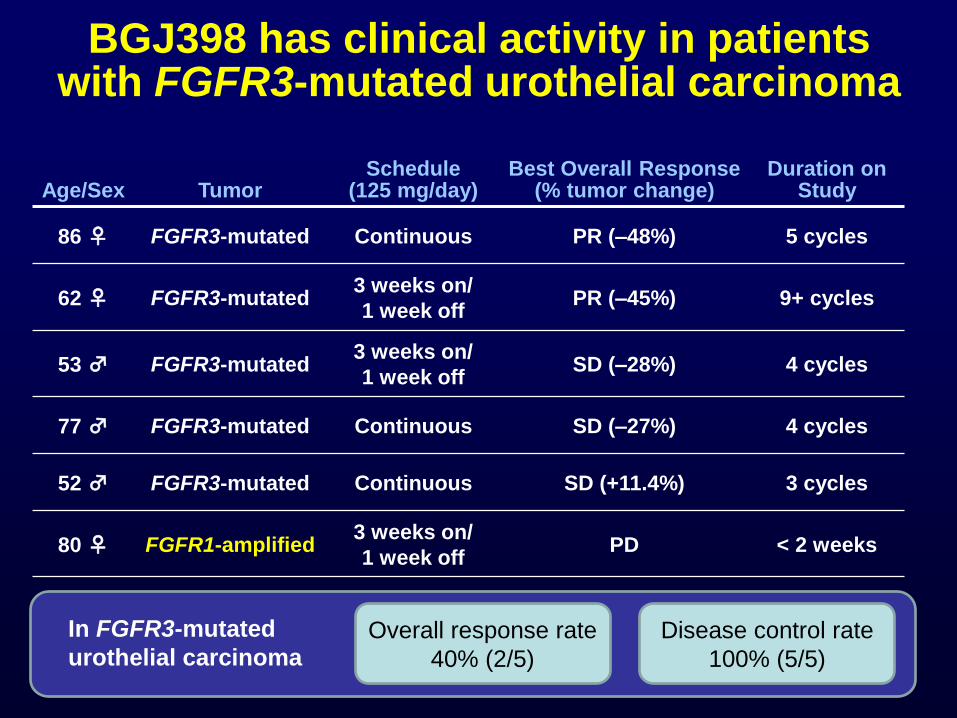
BGJ398 has clinical activity in patients with FGFR3-mutated urothelial carcinoma
Age/Sex Tumor Schedule
(125 mg/day) Best Overall Response
(% tumor change) Duration on
Study
86 ♀ FGFR3-mutated Continuous PR (–48%) 5 cycles
62 ♀ FGFR3-mutated 3 weeks on/
1 week off PR (–45%) 9+ cycles
53 ♂ FGFR3-mutated 3 weeks on/
1 week off SD (–28%) 4 cycles
77 ♂ FGFR3-mutated Continuous SD (–27%) 4 cycles
52 ♂ FGFR3-mutated Continuous SD (+11.4%) 3 cycles
80 ♀ FGFR1-amplified 3 weeks on/
1 week off PD < 2 weeks
In FGFR3-mutated
urothelial carcinoma Disease control rate
100% (5/5)
Overall response rate
40% (2/5)
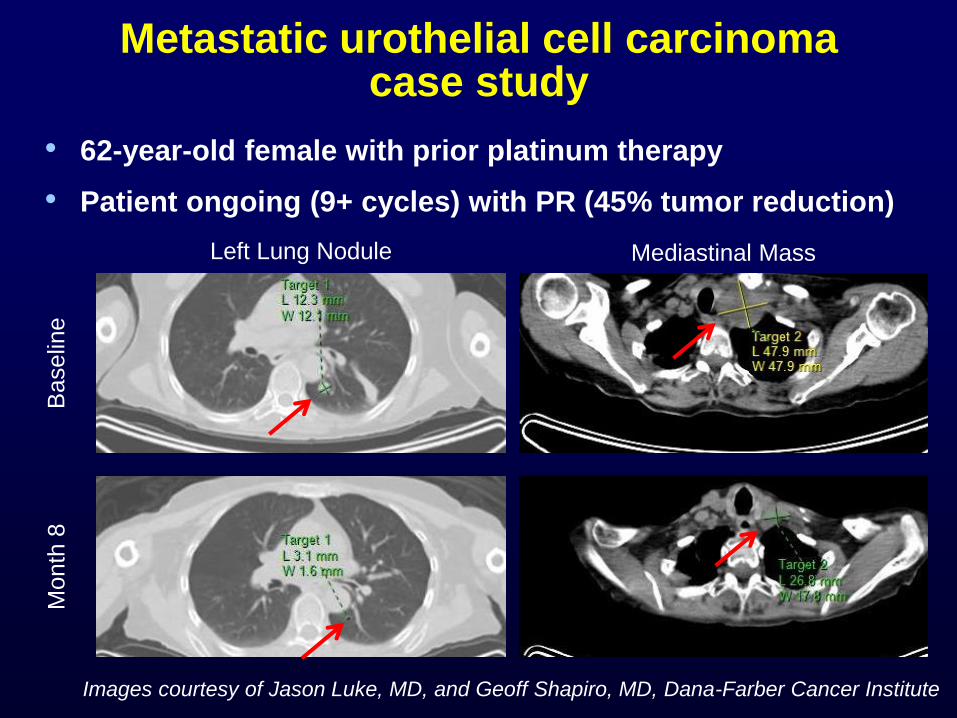
Metastatic urothelial cell carcinoma case study
• 62-year-old female with prior platinum therapy
• Patient ongoing (9+ cycles) with PR (45% tumor reduction)
Left Lung Nodule Mediastinal Mass
Baselin
e
Month
8
Images courtesy of Jason Luke, MD, and Geoff Shapiro, MD, Dana-Farber Cancer Institute
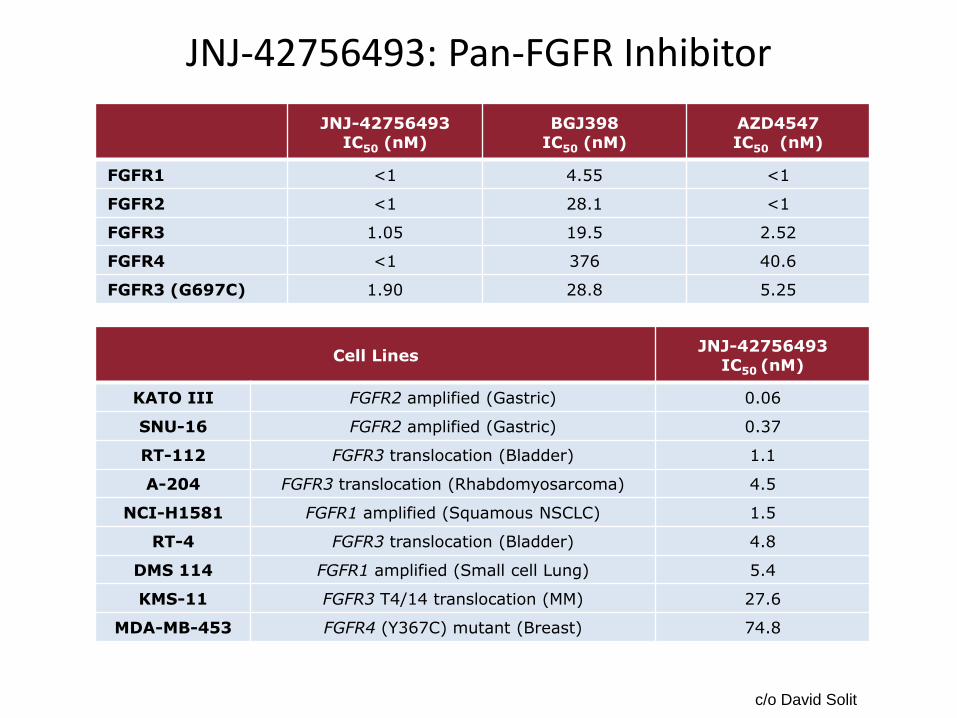
JNJ-42756493: Pan-FGFR Inhibitor
c/o David Solit
JNJ-42756493
IC50 (nM) BGJ398
IC50 (nM) AZD4547 IC50 (nM)
FGFR1 <1 4.55 <1
FGFR2 <1 28.1 <1
FGFR3 1.05 19.5 2.52
FGFR4 <1 376 40.6
FGFR3 (G697C) 1.90 28.8 5.25
Cell Lines JNJ-42756493
IC50 (nM)
KATO III FGFR2 amplified (Gastric) 0.06
SNU-16 FGFR2 amplified (Gastric) 0.37
RT-112 FGFR3 translocation (Bladder) 1.1
A-204 FGFR3 translocation (Rhabdomyosarcoma) 4.5
NCI-H1581 FGFR1 amplified (Squamous NSCLC) 1.5
RT-4 FGFR3 translocation (Bladder) 4.8
DMS 114 FGFR1 amplified (Small cell Lung) 5.4
KMS-11 FGFR3 T4/14 translocation (MM) 27.6
MDA-MB-453 FGFR4 (Y367C) mutant (Breast) 74.8

Clinical Activities of JNJ-42756493 in Patients with FGFR Aberration in Tumor Treated at ≥ 6mg Dose
1
1 – Intrahepatic Cholangiocarcinoma: FGFR translocation
2 – Breast Cancer: FGF amp
3 – Adrenal Carcinoma: FGFR translocation
4 – NSCLC: FGFR amp
5 – Breast Cancer: FGFR amp
6 – NSCLC: FGF amp
7 – Urothelial CA: FGFR translocation
8 – GBM: FGFR translocation
9 – Urothelial CA: FGFR translocation
1
2 5 3 4 6 7* 9* 8*
6 mg daily 9 mg daily 12 mg daily 12 mg 7 on/7 off
*Ongoing
c/o David Solit

Epigenetic Regulatory Mutations in UC
• Truncating (inactivating) mutations are enriched in genes involved in epigenetic regulation
• MLL2, ARID1A, KDM6A, and EP300 are all significantly mutated in bladder cancer
– MLL3, MLL, CREBBP, CHD7, and SRCAP all were mutated in > 10% of samples, although did not reach statistical significance
• 76% of tumors have at least one inactivating mutation in epigenetic regulatory genes and 41% had two mutations
• Exploration of epigenetic-modifying therapy is warranted
Targeting histone acetyltransferases (HAT’s)
• CREBBP and EP300 are histone and non-histone acetyltransferases – Acetylate chromatin – Acetylate multiple transcription factors to either
activate (p53) or inactivate (e.g. BCL6) them
• Preclinical data suggest tumors harboring inactivating mutations or deletions in CREBBP and/or EP300 may be sensitive to HDAC inhibition
• TCGA reported approximately 29% of patients with urothelial carcinoma harbor these alterations
Pasqualucci et al, Nature, 2011 TCGA, Nature, 2014
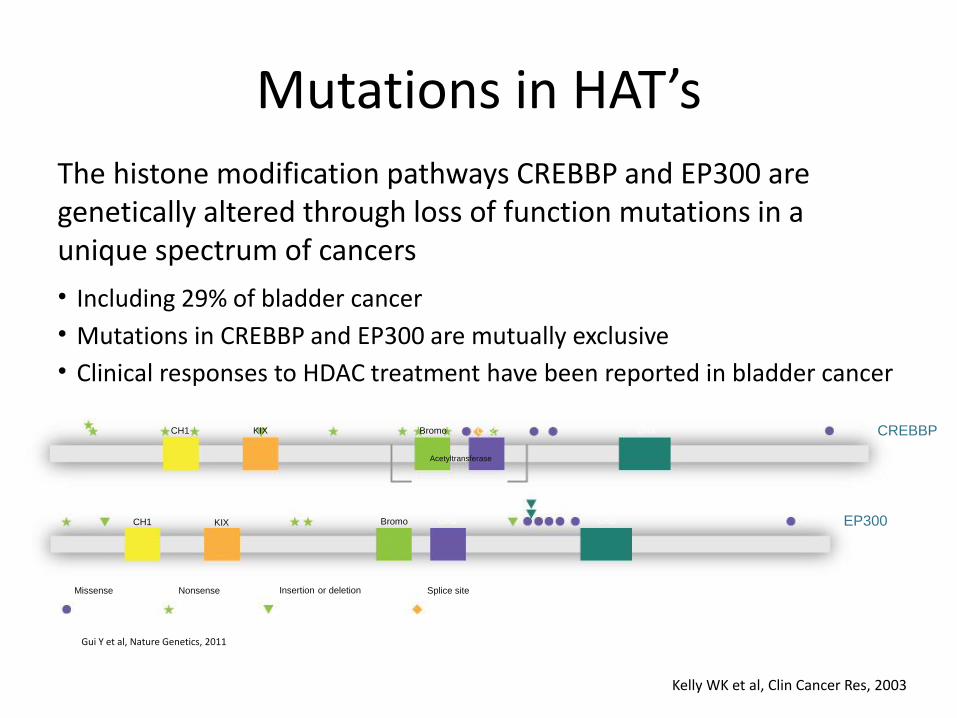
Mutations in HAT’s
The histone modification pathways CREBBP and EP300 are genetically altered through loss of function mutations in a unique spectrum of cancers
• Including 29% of bladder cancer
• Mutations in CREBBP and EP300 are mutually exclusive
• Clinical responses to HDAC treatment have been reported in bladder cancer
Gui Y et al, Nature Genetics, 2011
CH1 KIX Bromo CH2 CH3 CREBBP
Acetyltransferase
EP300 Bromo KIX CH1
Splice site Insertion or deletion Nonsense Missense
CH2 CH3
Kelly WK et al, Clin Cancer Res, 2003
Mocetinostat (aka MGCD0103)
• Oral HDAC inhibitor selective for isoforms 1, 2, 3, and 11
• Evaluation of over 30 mutant cell lines and 20 xenograft tumor models showed those with CREBBP or EP300 mutations are highly responsive to mocetinostat
• Single arm, Phase 2 trial planned – previously treated, locally advanced, unresectable or
metastatic urothelial carcinoma harboring inactivating mutations or deletions of the genes CREBBP and/or EP300
Eligibility
• Tumor gene sequencing for eligibility – Foundation Medicine as central laboratory
• To determine eligibility at sites without a qualifying local lab
• To retrospectively confirm cases initially enrolled based on local lab result
– Local sequencing lab may determine eligibility if agreement on assay capability to detect target alterations and certified by CLIA and CAP
– Gene sequencing well before the need for second-line treatment is encouraged, e.g., during first-line platinum-based regimen
MATCH-UP: Molecular allocation trial to choose
therapy for metastatic urothelial carcinoma following platinum-
based chemotherapy
Why a bladder “basket” trial
• NCI-MATCH unlikely to have enough bladder patients to develop a true signal
• Context often matters-
– B-Raf colon cancer vs melanoma
• Proof of concept for multiple agents
– Efficient use of patients and resources
• Screening sample size based on the rarest “basket”
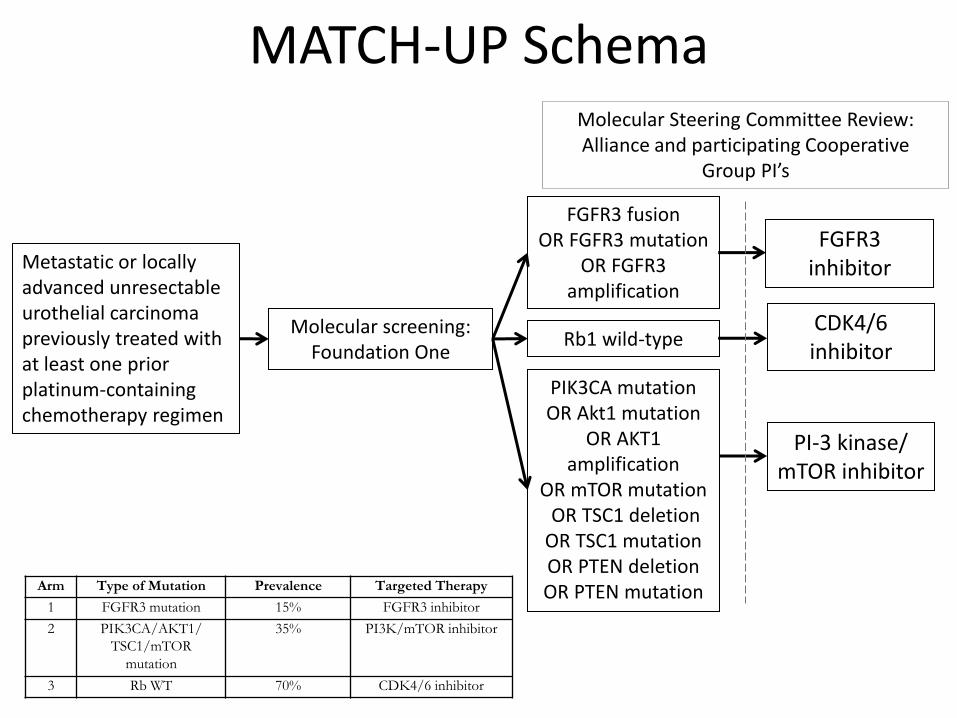
MATCH-UP Schema
Arm Type of Mutation Prevalence Targeted Therapy
1 FGFR3 mutation 15% FGFR3 inhibitor
2 PIK3CA/AKT1/
TSC1/mTOR
mutation
35% PI3K/mTOR inhibitor
3 Rb WT 70% CDK4/6 inhibitor
Molecular screening: Foundation One
PIK3CA mutation OR Akt1 mutation
OR AKT1 amplification
OR mTOR mutation OR TSC1 deletion OR TSC1 mutation OR PTEN deletion OR PTEN mutation
FGFR3 fusion OR FGFR3 mutation
OR FGFR3 amplification
Rb1 wild-type
PI-3 kinase/ mTOR inhibitor
FGFR3 inhibitor
CDK4/6 inhibitor
Molecular Steering Committee Review: Alliance and participating Cooperative
Group PI’s
Metastatic or locally advanced unresectable urothelial carcinoma previously treated with at least one prior platinum-containing chemotherapy regimen
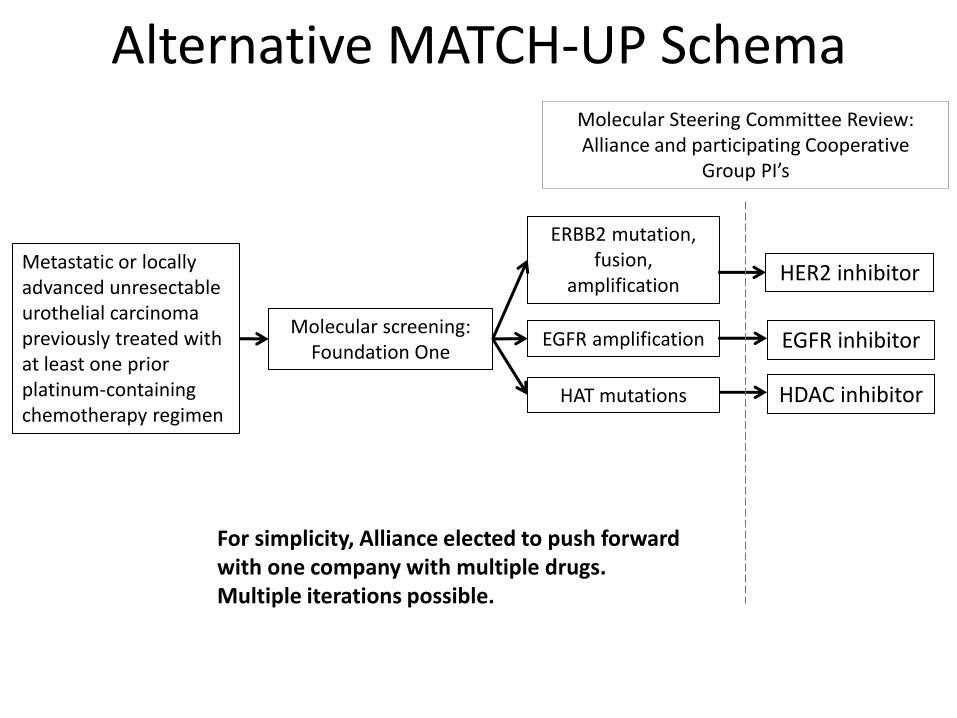
Alternative MATCH-UP Schema
Molecular screening: Foundation One
HAT mutations
ERBB2 mutation, fusion,
amplification
EGFR amplification
HDAC inhibitor
HER2 inhibitor
EGFR inhibitor
Molecular Steering Committee Review: Alliance and participating Cooperative
Group PI’s
Metastatic or locally advanced unresectable urothelial carcinoma previously treated with at least one prior platinum-containing chemotherapy regimen
For simplicity, Alliance elected to push forward with one company with multiple drugs. Multiple iterations possible.
Identification of eligible patients
• FoundationOne test- committed to study – Centralized
– CLIA certified
– Used to dealing with obtaining tissue from multiple sites
– Turnaround time is reasonable
– Willing to collaborate and return additional information beyond traditional report
• BIQSFP funding to be requested as integral biomarker
Design
• Parallel two stage phase II studies • Co-primary endpoints:
– % progression-free survival (PFS) at 3 month – ORR at 3 months
• The historical control PFS rate at 3 months for this patient population (chemotherapy refractory urothelial carcinoma) is estimated to be 40%.
• Historical ORR for chemotherapy is 15% • Study is looking for improvement of 20% in the
proportion free from progression and/or ORR with each mutation-targeted therapy
Choueiri et al. JCO 2011
Sample size • Need approximately 53 patients for each treatment arms
using the phase II generalized enrichment design for approximately 5% type I error and at 84% power
• Need to screen based on the lowest frequency alteration
– FGFR3 ~15% prevalence
– To enroll 53 FGFR3 mutant patients, need to screen 354 patients
– This will be sufficient to accrue the other arms
– Inflate screening sample by 20% to account for ineligibility and subsequent screen failures
– Therefore, screening population will be 425 patients
Statistics (continued)
• If an arm fails, will re-evaluate mutation selection criteria and possible re-open or add an arm.
• A similar two-stage design will be adopted for the replacement arm and the decision rule remains the same.
– However, this will affect the overall type I error for this phase II clinical trial (inflated to more than 15%).
MATCH-UP Status
• Concept with sponsor, pending decision
• Next steps- finalizing correlatives, BIQSFP funding, CTEP submission
Challenges to implement personalized medicine trials
• Archival tumor is often quite remote from current disease burden, and many cytotoxics intervene
– Currently, not feasible to use metastatic biopsies for NGS screening on large scale (do-able at selected institutions).
– Biopsy of metastatic sites for mutation analysis is not yet SOC in UC
• Heterogeneity will be a problem- whether it will be universally a problem is unknown
• Co-occuring alterations may drive resistance (de novo and acquired)
• How will new FDA regulation of laboratory tests influence this process?
– How interchangeable are assays?
Conclusions
• Clinical trials selecting for UC subpopulations are rolling out based on TCGA and other data
• So far: PI3K/mTOR, FGFR3, RB WT, ERBB2/EGFR, and HAT mutations
• Rational combinations are next step once these initial “screens” for anticancer activity are complete – Hopefully additive or synergistic activity, and not
toxicity