transition clinics - an update. andrew symes clinical nurse specialist royal free london nhs...
TRANSCRIPT

Transition Clinics - an update.
Andrew SymesClinical Nurse Specialist
Royal Free London NHS Foundation TrustOctober 2012

Overview
• About us: Centre for Immunodeficiency• Why transition?• What we’re doing• Patient & parent feedback: qualitative and
quantitative• Conclusions & the future

Centre for Immunodeficiency
• Partnership between Great Ormond Street Hospital (GOSH) and Royal Free Hospital (RFH)
• Around 850 PID patients between two centres
• Over 400 on IV or SC replacement therapy
• Increasing post bone marrow transplant (BMT) population

Why Transition?
“Transition is the purposeful, planned movement of adolescents and young adults with chronic physical and medical conditions from child-centred to adult-orientated health care systems”
(Blum et al, 1993)
“A painful passage o’er a restless flood”
(William Cowper, 1731-1800)
• Need for transition recognised by many professional associations and patient groups (RCN, DoH, RCP etc)
• Some disciplines more established than others: diabetes, cystic fibrosis, epilepsy
• PID patients need good transition like anyone else. No specific current literature to direct best practice (Tuchman et al, 2008)

Why Transition?
• Increased survival rates of complex chronic conditions means greater awareness and need (Sawyer et al 1997)
• Absence of established pathway can lead to decreased compliance and have adverse effect on patient health (Dovey-Pearce et al, 2005)
• Agreement of need between sites and first clinic in May 2009
In The Beginning…
• Unsure of who was doing what• Poor clinic preparation• Lack of information to patients• Inadequate follow-up• High in goodwill, low in organisation!

Transition 2.0
• Protocol (finally) agreed November 2011• Algorithm developed• Basic timeline• Referral templates depending on type of patient• Responsibilities clearer

Transition Algorithm
Checklist for Initial Adolescent and Family Discussion (14-16 yrs)
• Diagnosis• Treatment• Consultant/transition coordinator• Explanation and expectations of move to adult centre • Assess level of understanding regarding condition• Assess level of understanding regarding treatment and medication• Discussion of family planning issues where relevant (genetics) • Opportunity to ask questions regarding transfer to adult centre
(patient and family/carers)• Areas to be addressed before last transition clinic visit• Psychology input included

Last Appointment at GOSH• RFH nurse, doctor and psychologist present• Visible id and introductions – full room can be intimidating• Explain why we are here• In-depth history from patient and parent/carer• Gently reinforced that patient now more in control• Psychologist to explain service and offer appointment• Differences between equipment and delivery arrangements
explained – pumps & needles• Telephone and email details exchanged• Agree date of first appointment at RFH

Transfer Letter Requirements for Immunology Patients from GOSH to RFH (16-18 yrs)
• Diagnosis, with genetic details if available and date• Medication including previous immunosuppressive and chemo
drugs• Lab values including at diagnoses/before treatment initiation and
current• Dates and copies of recent lung function, CT chest etc• Family history where relevant• IVIg or SCIg dose/frequency details• Comment on compliance or relevant social history• Infection history including particular bugs found

Transfer Letter Requirements for Immunology Patients from GOSH to RFH (16-18 yrs)
• Vaccination history• Date of onset of symptoms• Which diagnoses are still active and which are previous
history/resolved• Known allergies • Previously failed therapeutic approaches• Previously successful therapeutic approaches which are currently
not needed• Family history• Contact numbers on patient, or parents/carer if needed

Transfer Letter Requirements for Post BMT Patients from GOSH to RFH (16–18 yrs)
• Diagnosis, with genetic details if available and date• Conditioning regimen• Donor type (Haplo/MUD/Sibling/Cord)• Acute or chronic GVHD• Chimerism• Engraftment & immune reconstitution• Medication including previous immunosuppressive, chemo drugs &
prophylaxis• Post transplant growth: growth, endocrine assessment & re-
vaccination• Lab values including at diagnoses/before treatment initiation and
current

Transfer Letter Requirements for Post BMT Patients from GOSH to RFH (16–18 yrs)
• Dates and copies of recent lung function, CT chest etc• Family history where relevant• IVIg or SCIg dose/frequency details• Comment on compliance or relevant social history• Infection history including particular bugs/viruses found• Which diagnoses are still active and which are previous
history/resolved• Known Allergies • Previously failed therapeutic approaches• Previously successful therapeutic approaches which are currently
not needed• Family history• Contact numbers on patient, or parents/carer if needed

Other responsibilities• Copy of referral letter to both attending RFH nurse & doctor• GOSH to continue prescribing until patient has first appointment at
RFH• One person identified as first contact for patient if any problems
(usually RFH nurse)• Referral to home delivery company made after first RFH visit• Same nurse & doctor must be present at first RFH clinic
appointment to provide continuity

Questionnaire
• 23 patients transitioned at time of sending• 20 eligible for questionnaire (2 moved away, 1
died) • Separate questionnaire for patients and parents• Qualitative & quantitative• 5 replies from patients, 6 from parents (no
surprise!)

Responses: quantitative
• 100% male responses!• 40% on immunoglobulin replacement, 40% not,
20% blank• 40% had BMT, 60% not• 60% of patients knew who was present at the
clinic compared with 100% of parents• 20% of patients would have like the opportunity
to talk away from their parents

Responses: quantitative• Comparable average score between patients and parents (8.5 &
8.8) when asked if they found the clinic helpful (1 = not at all helpful, 10 = very helpful)
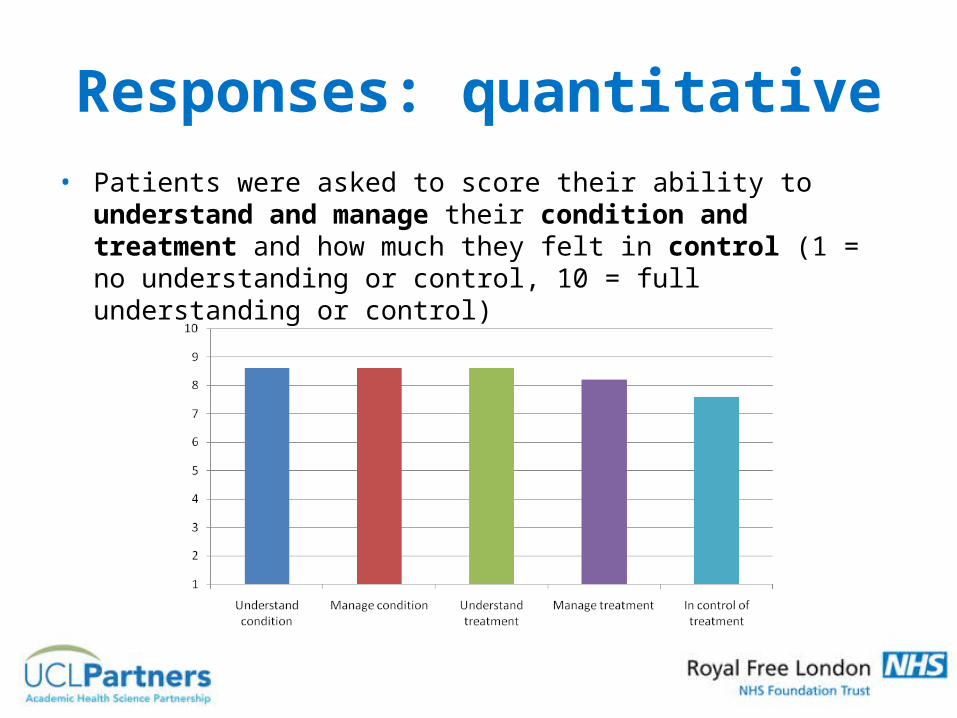
Responses: quantitative• Patients were asked to score their ability to understand and
manage their condition and treatment and how much they felt in control (1 = no understanding or control, 10 = full understanding or control)

Responses: quantitative• When asked to score how worried, scared and confused patients
were (1 = not at all, 10 = very) both before and after their transition, the collective average score reduced from 3.2 to 2.8, with the highest reduction being confusion (3.6 to 2.6)
Responses: qualitative• Please use 5-10 words to describe yourself:
“Positive, worried, creative, healthy, unsure, sporty, social, fun, friendly, likes to work, worried about my future, laid-back, ambitious, caring.”

Responses: qualitative• Both patients and parents had positive comments when asked
what was helpful about the process:– Meeting the new team in advance and knowing there was a
good handover– Reassurance that they could contact their new immunology
nurse– Knowing who they would be coming to see– To talk through things that would be different

Responses: qualitative• Some found parts of the process less helpful:
– The new doctor was not prepared and Mum had to tell him everything about me when I was young
– Not having enough information about my son, me having to update them
– Would have liked a map of the new hospital and surrounding car parks
– They did not talk about their hospital services and their appointments system
Responses: qualitative
• Apart from one parent who did not have a separate (dermatology) appointment arranged for their son, no patient or parent felt let down by something we had promised and not delivered

Responses: qualitative• When asked to suggest ways in which the transition process could
be improved patients mentioned, amongst other things:
– Doctors need to be more informed– More contact by the adult service– A leaflet or booklet about the RFH team ahead of the visit

Responses: qualitative• Whilst parents thought:
– Could be more organised– Process should be quicker– Helpful to know more about how the infusion equipment was
going to differ– Could be made to feel more welcome by reception staff– Son could have been asked more about his “thoughts and
feelings”

Conclusions & the future…• Transition process worthwhile• Formalise documentation • Greater clarity for patients• Get the basics right• More written information – transition booklet and questionnaire• Recent addition of adult psychologist• Give questionnaire at last clinic to ensure better audit response• Transition clinic at adult centre?

Thanks to• Clare Malcomson• Sarita Workman• Mari Campbell• Bodo Grimbacher• Helen Baxendale• Suranjith Seneviratne • James Thaventhiram• Alison Jones• Graham Davies• Marie-Louise Chiew
References• Blum R, Haydock P & Gallay L. Moving into Adulthood for Youth with
Disabilities and Serious Health Concerns. Network on Transitions to Adulthood Policy Brief, July 2005, Issue 26.
• Dovey-Pearce G, Hurrell R, May C, Walker C, Doherty Y. Young adults’ (16-25 years) suggestions for providing developmentally appropriate diabetes services: a qualitative study. Health Soc Care Community. 2005 Sep; 13(5):409-19.
• Tuchman LK, Slap GB, Britto MT. Transition to Adult Care: experiences and expectations of adolescents with a chronic illness. Childcare, Health and Development. 2008, Sept; 34(5): 557-63
• Adolescent transition care: Guidance for nursing staff. Royal College of Nursing. 2004
• Transition: moving on well. A good practice guide for health professionals and their partners on transition planning for young people with complex health needs or a disability. Department of Health. 2008
