transfusion support in surgery
TRANSCRIPT

SPEAKER: DR. BARILIN PASSAH
TRANFUSION SUPPORT IN SURGERY &
MSBOS
1

Transfusion practice in surgery
Use of blood and blood components in elective surgery
Is inconsistent
Varies between hospitals, individual doctors and
between countries
Depends upon the diagnosis, different surgical
techniques, knowledge of the clinician on the use of
blood/blood components, availability of blood
Therefore each blood transfusion service should frame
its own guidelines for appropriate use of blood and
propagate them among the clinicians
2

Most elective surgery do not result in sufficient blood loss
to require blood transfusion
Careful assessment and management ↓ patient’s morbidity and mortality
Diagnosis, investigation and treatment of anaemia
Treatment of cardiorespiratory disorders
Detection of coagulation and platelet disorders
There is rarely justification for the use of preoperative blood transfusion simply to facilitate elective surgery
3

BLOOD SPARING STRATEGIES
Operative blood loss can be significantly reduced
Meticulous surgical techniques
Use of vasoconstrictors
Anaesthetic techniques
Use of antifibrinolytic drugs
Autologous blood donations
4

AUTOLOGOUS TRANSFUSION
The collection and subsequent reinfusion of the patient’s own blood or blood components
Advantages
Elimination of the risk of disease transmission
Elimination of alloimmunization
No risk of haemolytic, febrile and allergic reaction
Provides fully compatible blood in immunized patients and patients with rare blood group
Provision of blood in remote areas
Provision of blood to patients who refuse blood from homologous donors because of religious belief.
5

TYPES OF AUTOLOGOUS TRANSFUSION
1. Preoperative
2. Acute isovolemic or normovolemic haemodilution
(ANH)
3. Intraoperative blood salvage
4. Post operative blood salvage
Criteria for autologous donation
Written consent of the patient-donor
Age→ no minimum/maximum age limits
Weight→ blood drawn should be proportionate to
patient-donor weight (8-9ml/kg)
Haemoglobin→ >11gm/dl and Hct of 33%
6

Preoperative autologous donation
Patient’s blood is collected and stored prior to elective
surgery
Collection should be done
weekly or
at an interval of 4 days and last donation should be at
least 72 hours before surgery
Acute isovolemic or normovolemic haemodilution (ANH)
Predetermined volume of patient’s own blood is removed
before surgery (immediately before or shortly after
induction of anesthesia)
Simultaneously replaced with colloid/crystalloid solution7

Intraoperative blood salvage
Collection of shed blood from a body cavity/wound during
surgery and its subsequent reinfusion into the same
patient
Shed blood is processed by a number of machines (cell
savers) before transfusion the patient
Can provide the equivalent of 12 units of banked blood per
hour to massively bleeding patients
Post operative blood salvage
Collection of blood from surgical drains, followed by
reinfusion
Maximum amount of blood that can be reinfused is 1400ml8

INDICATIONS FOR AUTOLOGOUS TRANSFUSION
In elective surgery with resonable probability for
transfusion
Orthopedic surgery (joint eplacement)
Plastic and reconstructive surgery
Cardio-vascular surgery
Major abdominal surgery
Obstetrics and gynaecological patients having multiple
antibodies
9

MAXIMUM SURGICAL BLOOD ORDER SCHEDULE
(MSBOS)
List of surgical procedures with the number of units that will
be cross matched for each procedure
Careful audit of local surgical practice
Based on the transfusion patterns of each institute
Agreed upon by the surgeons, anesthesiologists, and
blood bank in charge
Recommended crossmatch to transfusion ratio (C:T) is 2:1
C:T ratio can be used to evaluate blood ordering practices
The ordering schedule is flexible depending on the
circumstances
10

PROCEDURE
The surgery schedule should be examined prior to
performing ordered cross matching
The patient’s order is compared with MSBOS
If the patient’s order meets the recommendations of
MSBOS, cross matching is done
If the order does not meet the recommendations, the
ordering physician should be consulted
11

EXAMPLE OF MSBOS
General surgery
Obstetrics/gynaecology
12
Procedure Units
Breast biopsy T/S
Colon resection 2
Exploratomy laparotomy T/S
Gastectomy 2
Procedure Units
Abdomino-perineal repair T/S
Cesarean section T/S
Dilation and curettage T/S
Hysterectomy ,laparoscopic T/S
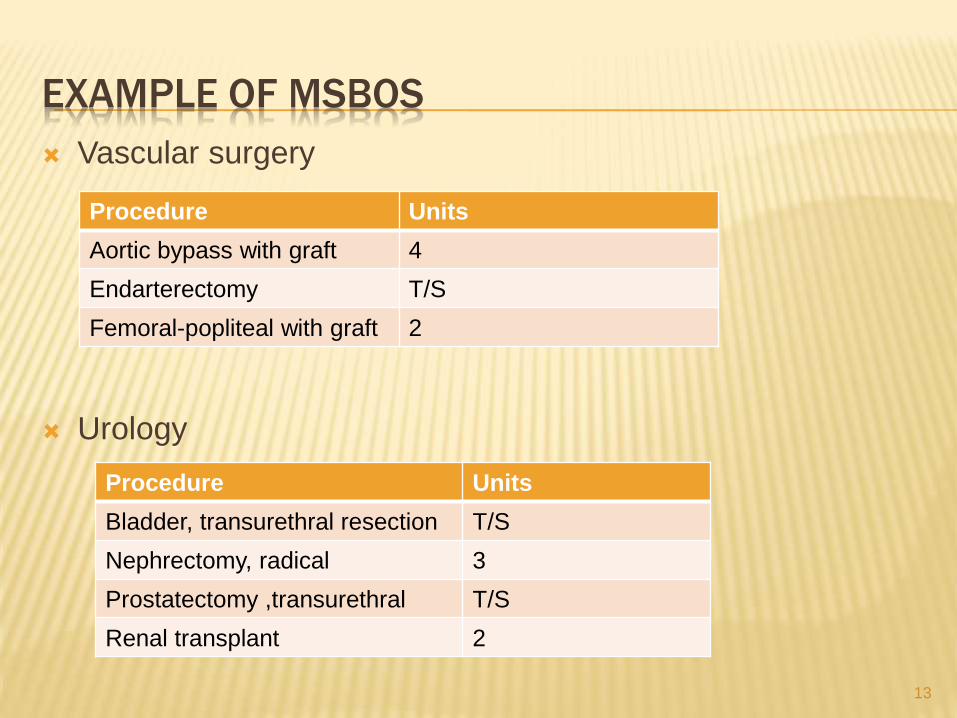
EXAMPLE OF MSBOS
Vascular surgery
Urology
13
Procedure Units
Aortic bypass with graft 4
Endarterectomy T/S
Femoral-popliteal with graft 2
Procedure Units
Bladder, transurethral resection T/S
Nephrectomy, radical 3
Prostatectomy ,transurethral T/S
Renal transplant 2

BLOOD TRANSFUSION IN ACUTE BLOOD LOSS
Decision to transfuse PRBC
The Hb concentration prior to hemorrhage
The extent of haemorrhage
The presence of other conditions which may alter the
physiologic response to acute blood loss
Loss of <15% blood volume→ minimal symptoms
15% to 30%→ tachycardia
30% to 40%→ increased signs of shock
>40%→ severe shock
14

RED CELL TRANSFUSION GUIDELINES
Acute blood loss:
Hb :
>10 gm/dl→ RBCs rarely needed
<6 gm/dl →usually needed
6-10gm/dl→ RBC need depends on other factors
15
Loss of blood Replacement fluid
<20% blood volume none
20-30% blood volume Crystalloids/colloids
30-40% blood volume Red cells and crystalloids
> 40% of blood loss Red cells and crystalloids
TRANSFUSION SUPPORT IN BURN PATIENTS
Acutely burned patient
↓ erythrocyte function
Consumptive coagulopathy
Immunosupression
↓ red cell synthesis
Careful monitoring of coagulation status and correction of
coagulapathies is important
Administration of fresh frozen plasma, cryoprecipitate and
platelets may be required
16

Several interventions may minimize transfusion
requirements in burn patients
Administration of erythropoietin
Use of conservative strategies during burn wound
excision
Use of topical hemostatic agents during burn excision
and grafting
Early excision of wound prior to bacterial infection
Minimizing blood draws
17

ANAEMIA AND SURGERY
Presence of anaemia indicates an underlying pathology
exists which needs to be treated
Compensatory response to anaemia may not always be
sufficient to maintain oxygenation during surgery
Reduction in the oxygen carrying capacity due to
surgical blood loss
Cardiorespiratory depressant effects of anaesthetic
agents
Adequate Hb must be ensured preoperatively to ↓ blood
transfusion during surgery
18

ANAEMIA AND SURGERY
Causes of anaemia:
Nutritional deficiencies of iron and folate
Parasitic and helminthic infestations
Anaemia should be screened and treated in elective
surgical patients and surgery should be postponed till
Hb is adequate
Haemoglobin level as a transfusion trigger→7-8 gm/dl in a well compensated and healthy individual for minor surgery
19

Higher haemoglobin levels in:
Inadequate compensation for anaemia and oxygen supply to the tissues
angina, ↑ dyspnoea, dependent edema, cardiac failure
Cardiorespiratory diseases which limits the ability to compensate ↓ oxygen supply
ischaemic heart disease or obstructive airway disease
Major surgery or anticipated significant blood loss (>10ml/kg)
20

SURGERY AND COAGULATION DISORDERS
Coagulation and platelet disorders can be classified as
Acquired coagulation disorders arising as a result of
disease or drug therapy
Liver diseases
Aspirin-induced platelet dysfunction
Disseminated intravascular coagulation
Congenital coagulation disorders
Hemophilia A or B
von Willebrand disease
21

SURGERY AND COAGULATION DISORDERS
It is important to enquire about history
Any abnormal bleeding tendency in the patient or
his/her family
Drug intake→ aspirin, NSAIDS
To prevent excessive blood loss
Diagnosis and treatment of coagulation disorders prior to any surgical procedures
Stopping intake of drugs which interfere with platelet function 10 days before surgery
INR should be less than 2 before surgery commences
22

BLOOD TRANSFUSION IN OPEN HEART SURGERY
Blood/blood components important supportive therapy
↓ requirement of blood
Preoperatively
Autologous predonation of whole blood
Pheresis of platelets
Erythropoietin
Intraoperatively
Rigourous surgical techniques
Pre-CPB normovolemic hemodilution
Retransfusion of pump blood
23

Cell saver or ultrafiltration of pump blood
Drug therapy
Antifibrinolytic agents
Post operatively
Shed mediastinal blood transfusion
FFP
24

BLOOD TRANSFUSION IN LIVER TRANSPLANTATION
Orthotopic liver transplantation (OLT) involves the
removal of the native diseased liver and replacing it with a
healthy liver from the donor in the same anatomic location
Extensive, complex and technically demanding
Associated with extensive bleeding→ multiple vascular
transections and anastomoses
25

MECHANISM OF BLEEDING IN LIVER TRANSPLANTATION
High vascularity of the liver
End stage liver diseases
associated with portal hypertension→ risk factor for massive hemorrhage
Components of the haemostatic system may be abnormal
Chronic liver diseases → associated with anaemia and thrombocytopenia
Surgical and technical factors
26

ALTERATIONS TO HAEMOSTATIC SYSTEM IN LIVER DISEASES
Thrombocytopenia
Platelet function defects
Enhanced production of nitric oxide and prostacyclin
Low levels of of factor II, V, VII, IX, X and XI
Vitamin K deficiency
Low levels of a2-antiplasmin and factor XIII
dysfibrinogenemia
27

BLOOD TRANSFUSION IN RENAL TRANSPLANTATION
Blood transfusion has a beneficial effect on renal graft
survival
May result in the development of HLA antibodies which
are detected at the time of pre-transplant cross
matching
May cause immunosupression due to enhancement of
suppressor T cell activity
Rapid improvement of immunosupressive therapy suggest
no difference in graft survival between transfused and non
transufused organ recipients
28

BLOOD MANAGEMENT IN OBSTETRICS AND
GYNECOLOGY
Uterine hemorrhage is normal and expected
500ml during vaginal delivery
1000ml for cesarean section
↑ 30-40% intravascular volume
↑ 20-30% red cell mass
Immediate contraction of the uterus after childbirth results in
autotransfusion of maternal blood previously sequestered in
the uterine walls
Hypercoagulable state → clotting factors function at their
maximum immediately following deliveris
29

INDICATION FOR TRANSFUSION IN PREGNANCY
1. Duration of pregnancy <36 weeks
Hb ≤ 5gm/dl with or without signs of cardiac failure/hypoxia
Hb 5-7gm/dl in the presence of
Cardiac failure or clinical evidence of hypoxia
Pneumonia or any other serious bacterial infection
Malaria
Pre-existing heart disease not related to anemia
30

2. 36 weeks or more
Hb 6gm/dl or less
Hb 6-8gm/dl in the presence of
Cardiac failure or clinical evidence of hypoxia
Pneumonia or any other serious bacterial infection
Malaria
Pre-existing heart disease not related to anemia
31

3. Planned elective cesarean section and there is a history
of
3. Antepartum Haemorrhage
4. Postpartum Haemorrhage
5. Previous CS
32

MASSIVE TRANSFUSION
Transfusion of whole blood equal to or exceeding the
person’s blood volume with 24 hours
Transfusion of 10 units of whole blood or 20 units PRBC in
24 hours
Replacement of more than 50% blood volume in 3-4 hours
in an adult
Priorities in massive blood loss
Restoring and maintaining adequate blood volume
Maintaining sufficient oxygen carrying capacity
Securing haemostasis
33

Haematological investigations in massive transfusion
Investigation Target value
Hb/HCT
Platelet count
PT
PTT
Fibrinogen
Hb 10gm/dl, Hct 0.32
> 50 X 109 /L
<1.5 X control
<1.5 X control
>0.8 gm/L
34

FFP TRANSFUSION
Supplementation of FFP should be considered after one
blood volume is lost
4-5 units FFP should be given to an adult patient
Thereafter 4 units FFP should be given for every 6 units
of red cells
Coagulation factors should be maintain above the critical
level
35

PLATELET TRANSFUSION
Necessary after 2 volumes of blood loss
Recent guidelines advocates the use of red cells, plasma
and platelets in1:1:1 ratio to massively bleeding patients
Laboratory parameters along with clinical considerations
should be used for effective management
36

37

REFERENCES
1. Spiess B D, Spence R K, Shander A.Perioperative
transfusion medicine. 2ND edition
2. Makroo R.N . Principles and practice of transfusion
medicine. 1st edition
3. Saran R K. Transfusion medicine technical manual. 2nd
edition
4. Technical manual. AABB. 17th edition
5. WHO manual. Clinical use of blood.
38