trans-optics and refraction
DESCRIPTION
TRANS-Optics and RefractionTRANSCRIPT
Pag
e1 b
y IC
EM
AN
Bas
tin
en
Legend: ** NOTES
Refraction
Definition
• Physics: change in the direction of a wave due to change in its transmission medium
• Bending of a light wave as it enters a medium where its speed is different
• Medicine: clinical test in which a phoropter/loose lenses may be used to determine the eye’s refractive error and the best corrective lenses to be described
**The amount on bending depends on the indices of refraction of the 2 media and is quantitatvely described in Snell’s law
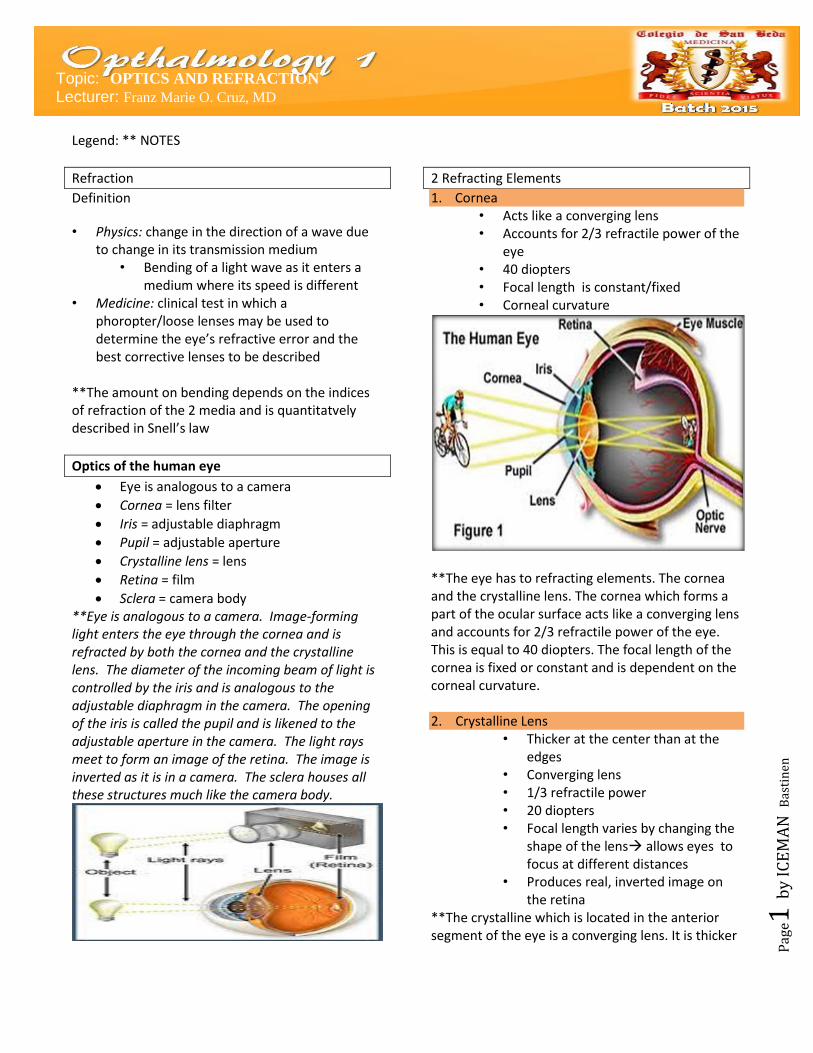
Optics of the human eye
Eye is analogous to a camera
Cornea = lens filter
Iris = adjustable diaphragm
Pupil = adjustable aperture
Crystalline lens = lens
Retina = film
Sclera = camera body **Eye is analogous to a camera. Image-forming light enters the eye through the cornea and is refracted by both the cornea and the crystalline lens. The diameter of the incoming beam of light is controlled by the iris and is analogous to the adjustable diaphragm in the camera. The opening of the iris is called the pupil and is likened to the adjustable aperture in the camera. The light rays meet to form an image of the retina. The image is inverted as it is in a camera. The sclera houses all these structures much like the camera body.
2 Refracting Elements
1. Cornea • Acts like a converging lens • Accounts for 2/3 refractile power of the
eye • 40 diopters • Focal length is constant/fixed • Corneal curvature
**The eye has to refracting elements. The cornea and the crystalline lens. The cornea which forms a part of the ocular surface acts like a converging lens and accounts for 2/3 refractile power of the eye. This is equal to 40 diopters. The focal length of the cornea is fixed or constant and is dependent on the corneal curvature. 2. Crystalline Lens
• Thicker at the center than at the edges
• Converging lens • 1/3 refractile power • 20 diopters • Focal length varies by changing the
shape of the lens allows eyes to focus at different distances
• Produces real, inverted image on the retina
**The crystalline which is located in the anterior segment of the eye is a converging lens. It is thicker
Topic: OPTICS AND REFRACTION Lecturer: Franz Marie O. Cruz, MD

Pag
e2 b
y IC
EM
AN
Bas
tin
en
at the center than at its edges. It accounts for 1/3 of the refractile power of the eye and this is approximately equal to 20 diopters. Unlike the cornea, the focal length of the lens varies. This is achieved by changing the shape of the lens and this allows the eye to focus at different distances. A person with no refractive error can see clearing at distance and near. The 2 converging lens system of the eye produces images that are real and inverted on the retina. Pupil
- Central opening of the iris - Diameter of the pupil changes with ambient
light - Bigger pupil diameter in the dark - Smaller pupil diameter in bright
light - Smaller pupil reduces spherical aberration
(causes image blur)
Accommodation
• Process by which the eye changes in optical power to maintain clear image of an object as its distance varies
• Part of the near reflex triad: convergence and pupillary miosis
• During accommodation, the ciliary body contracts slackening of the zonule fibers lens assumes a spherical shape lens becomes more positive allows eye to have a focused image of near object
**This is a diagramatic explanation on how changes in the shape of the lens allow for clear distance and close vision. Light rays from a distance object are parallel when they reach the eye, so you do not need much refraction or converging power to bring them to a focus on the retina. On the other hand, light rays from a near object diverges and you need more refraction to focus properly
Refraction
Emmetropia When parallel light rays are focused sharply on the retina Ametropia When the eye is unable to bring parallel light rays from a distant object into focus on the retina
Ciliary body is relaxed, lens zonules are taut, Lens is flat
Ciliary body contracts, Lens zonules are relaxed, Lens assumes a spherical shape

Pag
e3 b
y IC
EM
AN
Bas
tin
en
**An eye is emmetropic when its converging lens system is able to focus parallel light rights on the retina resulting to a clear image. On the other hand, ametropia is defined when the eye is …. The focal point may fall in front or behind the retina. This results to a blurry image.
Ametropia
Types of Refractive Errors: 1. Hyperopia 2. Myopia 3. Astigmatism 4. Presbyopia
Incidence of Refractive Errors: • 2.3 billion people worldwide suffer
from poor vision due to refractive errors
• 670 million have uncorrected or inadequately corrected refractive errors
• 90% reside in rural areas and low-income countries
• One of 5 priority eye diseases of “Vision 2020: Right to Sight” program (WHO)
**There are 4 types of refractive errors. Refractive Errors affects an estimate of 2.3 billion worldwide. Of this, 670 million have uncorrected or inadequately corrected refractive errors. 90% reside in rural areas and low-income countries. Because of this, WHO has named errors of refraction as one of its 5 priority diseases in its advocacy to eliminate avoidable blindness globally by year 2020 Determinants of Refractive Errors:
1. Corneal curvature 2. Axial length – length of the eyeball 3. Loss of accommodation
**There are 3 determinants of refractive errors: the corneal curvature, axial length of the eye of the length of the eyeball from the cornea to the retina and age-related decline in accommodation. 1. Hyperopia Far-sightedness
• Causes: - Insufficient convergence power (lens or
cornea) to focus light rays on the retina - Short eyeballs
• Rays focus posterior to the retina • Present in babies and young children;
outgrown as they get older and the eyeball gets longer
• Corrected by a plus (convergent) spherical lens
**Hyperopia or farsightedness results from insufficient convergence power of the eye to focus the light rays on the retina. This occurs in people with short eyeballs. The rays focus posterior to the retina. Hyperopia is normally present in babies and

Pag
e4 b
y IC
EM
AN
Bas
tin
en
young children but they as a rule outgrow them as they get older and the eyeball gets longer. In hyperopia, you would a plus or convergent spherical lens to bring the focal point to the retina. 2. Myopia Near-sightedness
• Causes: - Excessive convergence power (lens or
cornea) to focus light rays on the retina - Long eyeballs
• Rays focus anterior to the retina • Genetically-inherited • Develops in children between the ages 8-
12, progresses during teenage years, stabilizes by age 20
• Corrected by a minus (divergent) spherical lens
3. Astigmatism • Cornea and crystalline lens may not
have the same radius of curvature in all meridians
• More than 1 focal points • Results in distortion of vision at all
distances • Corrected by a cylindrical lens
4. Presbyopia • Progressive loss of accommodative
ability of the crystalline lens caused by the natural process of aging (beginning at the age of 40 y/o)
• Progressive hardening of the lens, loss of ability to change its shape
• Difficulty with near visual work such as
reading, “eye strain” • Occurs in the presence of myopia,
hyperopia and astigmatism • Remedied optically with plus spherical
lens **Patients complain that they’re arms are not long enough
**When we measure visual acuity, we take visual acuity at distance and visual acuity at near. These are just reminders when taking the visual acuity. One eye at a time, the other eye, non-tested eye has to be fully occluded. Uncorrected/corrected VA
Well-lighted chart Appropriate distance One eye at a time Uncorrected/corrected/ pinhole VA Proper labeling
Well-lighted room Appropriate distance Wear reading glasses Proper labeling

Pag
e5 b
y IC
EM
AN
Bas
tin
en
the pinhole, Jaeger chart held 14 inches away, wear reading glasses
Refractive Errors
Prescription of Lenses
**Corrective eye surgeries Correction of Refractive Errors 1. Spectacle correction: monofocal vs bifocal vs
trifocal 2. Contact Lenses 3. Refractive Surgeries A. Corrective corneal surgeries i. Corneal incisions a. Radial keratotomy b.Limbal relaxing incisions ii. Corneal ablative surgeries a. Photorefractive keratectomy (PRK) b. Laser-in-situ-keratomileusis (LASIK) c. Femtosecond LASIK (Intralase) B. Lens surgeries i. Cataract surgery ii Clear Lens extraction iii. Phakic intraocular lens implantation **There are several ways to correct refractive errors. The simplest and cheapest ways are thru the prescription of spectacles or glasses or contact lenses. 1. Spectacle correction: monofocal vs bifocal vs trifocal/multifocal
2. Contact Lenses: spherical vs toric **Corrective glasses can be monofocal, bifocal or trifocal. Monofocal glasses corrects for one distance only, and its usually for far. Most if not all of you who wears glasses will have monofocal correction. Bifocal means there are 2 segments for correction at 2 distances. Toric contact lenses has a treated or ballasted are such that it lies at a certain way or angle on the cornea and doesn’t rotate allowing it to correct the astigmatism. 3. Refractive Surgeries Corrective corneal surgeries
A. Corneal incisions i. Radial Keratotomy ii. Limbal relaxing incisions iii. Partial thickness peripheral incisions

Pag
e6 b
y IC
EM
AN
Bas
tin
en
b. Corneal ablative surgeries i. PRK-Photorefractive Keratectomy ii. LASIK iii. Femtosecond LASIK
Lens Surgeries
i. Cataract Surgery with implantation of intraocular lens
ii. Clear Lens Surgery + IOL implantation iii. Phakic IOL
Intraocular Lenses
i. Monofocal • Monofocals are set to provide best corrected
vision at near, intermediate or far distances. • Most people who choose monofocals have their
IOLs set for distance vision and use reading glasses for near activities. On the other hand, a person whose IOLs were set to correct near vision would need glasses to see distant objects clearly.
ii. Toric • This is a monofocal IOL with astigmatism
correction built into the lens. iii. Multifocal • These newer IOL types reduce or eliminate the
need for glasses or contact lenses.
• In the multifocal type, a series of focal zones or rings is designed into the IOL. Depending on where incoming light focuses through the zones, the person may be able to see both near and distant objects clearly.
• The design of the accommodative lens allows certain eye muscles to move the IOL forward and backward, changing the focus

Pag
e7 b
y IC
EM
AN
Bas
tin
en
much as it would with a natural lens, allowing near and distance vision.
• The ability to read and perform other tasks without glasses varies from person to person but is generally best when multifocal or accommodative IOLs are placed in both eyes.
• It usually takes 6 to 12 weeks after surgery on the second eye for the brain to adapt and vision improvement to be complete with either of these IOL types.
iv. Multifocal +Toric v. Phakic IOL • a special kind of intraocular lens that is
implanted surgically into the eye to correct myopia (nearsightedness). They are called "phakic" because the eye's natural lens is left untouched. This is in contrast to intraocular lenses that are implanted into eyes after the eye's natural lens has been removed during cataract surgery.
• Phakic intraocular lenses are indicated for patients with high refractive errors when the usual laser options for surgical correction (LASIK and PRK) are contraindicated