traitement médical du cancer de la prostate: la …...prof. karim fizazi, md, phd institut gustave...
TRANSCRIPT

Traitement médical du Cancer de la Prostate:
du désert à
la profusion
Prof. Karim Fizazi, MD, PhDInstitut Gustave Roussy
Villejuif, France

Disclosure
•
Participation in advisory
boards
or as a speaker for:Amgen, Astellas-Medivation, Astrazeneca, Bayer, BMS, Celgene, Dendreon, Exelixis, Ipsen, Janssen-Cougar, Keocyt, Millennium-
Takeda, Novartis, Sanofi-Aventis

Advanced prostate cancer: Natural history
(in the 2000s)
Local Treatment
PSA relapse (ADT)
Metastatic
Castrate-Resistant
Prostate Cancer
Castrate-resistant, M0
Metastatic
Hormone-Sensitive prostate cancer
Docetaxel
Zoledronate
ADT

A decade
of research in prostate cancer
2004-2009: No significant result
2010-2012:- Sipuleucel-T- Cabazitaxel- Denosumab- Abiraterone- Alpharadin- MDV 3100

Endocrine therapies
Testosterone
DNA
Cell division
TestisAdrenals
Autocrinesecretion
Castration(aLHRHor surgery)
Abiraterone
Abiraterone
Androgen Receptorinhibitors:-Bicalutamide-Enzalutamide(MDV 3100)

CYP17 blockade inhibits androgen synthesis
b

Abiraterone
acetate Phase III post-chemo
study design
Abiraterone
1000mg dailyPrednisone 5mg BID
n=797
Primary end point:
•
OS (HR 0.8)
Secondary end points:
•
TTPP
•
rPFS
•
PSA response
Efficacy end points (ITT)
Placebo dailyPrednisone 5mg BID
n=398
R
A
N
D
O
M
I
Z
E
D
2:1
•
1195 patients with progressive mCRPC
•
Failed 1 or 2 chemotherapy regimens, 1 of which contained docetaxel
Patients COU 301

COU-301: Abiraterone
prolongs survival in post-docetaxel
mCRPC
patients
Fizazi K, et al. Lancet Oncol. 2012;13:983–992.

Clinical benefit of abiraterone
October
2008 January
2010
Images courtesy of Dr Fizazi.

Abiraterone
in asymptomatic mCRPC: the COU-AA-302 Phase III study
•
Stratification by ECOG performance status 0 vs. 1Ryan C, et al. American Society of Clinical Oncology Congress
2012; Abstract LBA4518.
Patients•Progressive chemo-naïve mCRPC
•Asymptomatic or mildly symptomatic
Ran
do
mis
ati
on
1:1 Abiraterone acetate
+ prednisone (n = 546)
Placebo + prednisone (n = 542)
Co-primary endpoints•Radiographic progression-free survival
•Overall survival
Secondary•Time to opiate use (cancer-related pain)
•Time to initiation of chemotherapy
•Time to ECOG-PS deterioration
•Time to PSA progression

COU-AA-302: interim results•
Statistically significant radiographically-
evidenced progression-free survival (rPFS)
Ryan C, et al. ASCO 2012; Abstract LBA 4518.
Abiraterone
acetateControl
Data cut off: 20/12/2010
Abiraterone
acetatePlacebo
AA + PPL + P
HR 0.43 (95% CI: 0.35–0.52; P < 0.0001)

COU-AA-302: interim results
•
Overall survival
Data cut off: 20/12/2011
Abiraterone
acetateControl
HR 0.75 (95% CI: 0.61–0.93); P = 0.0097
Abiraterone
acetatePlacebo
Ryan C, et al. ASCO 2012; Abstract LBA 4518.

AFFIRM: A Phase 3 Trial of MDV3100 vs. Placebo in Post-Chemotherapy
Treated CRPC
Clinicaltrials.gov
identifier: NCT00974311
R
A
N
D
O
M
I
Z
E
D
2:1
R
A
N
D
O
M
I
Z
E
D
2:1
Primary Endpoint:
Overall Survival
MDV3100160 mg daily
n = 800
MDV3100160 mg daily
n = 800
Placebon = 399Placebon = 399
Patient Population:
1199 patients with progressive CRPC
Failed docetaxel chemotherapy
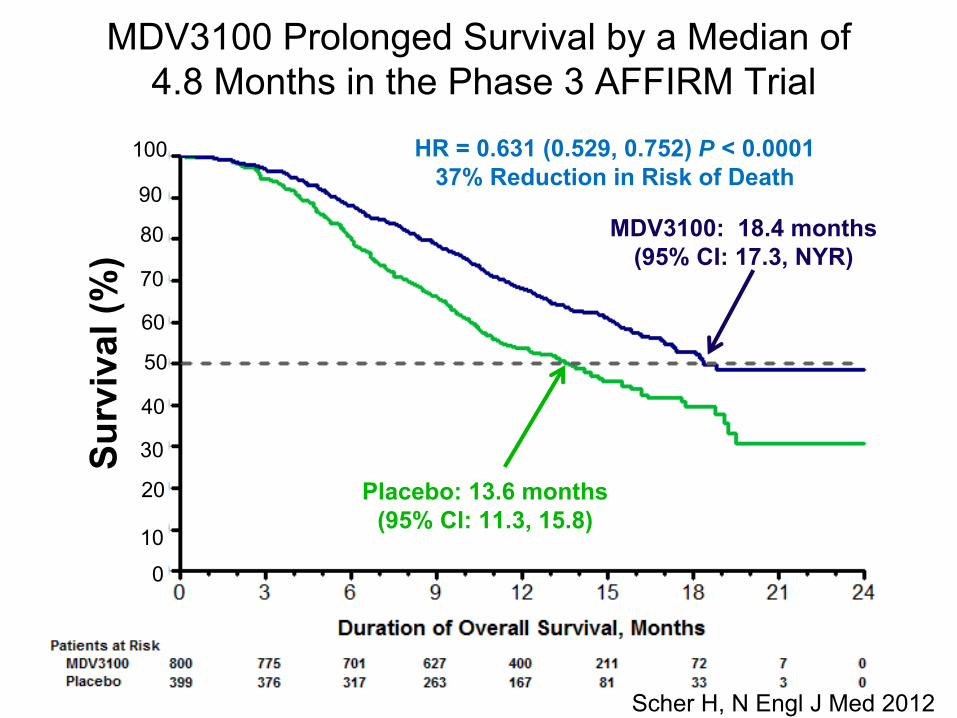
MDV3100 Prolonged Survival by a Median of 4.8 Months in the Phase 3 AFFIRM Trial
HR = 0.631 (0.529, 0.752) P < 0.000137% Reduction in Risk of Death
MDV3100: 18.4 months (95% CI: 17.3, NYR)
Placebo: 13.6 months (95% CI: 11.3, 15.8)
Surv
ival
(%)
100
80
60
40
20
90
50
30
0
10
70
Scher H, N Engl
J Med 2012

Taxanes for CRPC
•
Well-established
drug in Oncology
•
Main toxicity:–
Peripheral
neurotoxicity
–
Nail
Toxicity
•
Crosses the blood-brain barrier
in vivo
(humans?)•
Active in some
docetaxel-resistant models
•
Main toxicity:–
Hemato
(G-CSF)
–
Diarrhea
Docetaxel Cabazitaxel

Cabazitaxel in Second-line CRPC TROPIC Phase III Study
R
A
N
D
O
M
I
Z
E
Mitoxantrone
12mg/m2 q3w
Prednisone 10mg qd
mHRPCProgressionafter TXT
Cabazitaxel
25mg/m2 q3w
Prednisone
10mg qd
360 pts
360 pts
R
A
N
D
O
M
I
Z
E
Stratification factor :ECOG PS (0,1 vs
2)Mesurable/non_mesurable
Primary Endpoint:Overall survival
Secondary Endpoint:PSA response, PSA progression, PFS, RR, Pain progression, Safety, PK of cabazitaxel
Enrolment closed: 745/720 ptsHypothesis: 25% Reduction in the risk of deathor median OS=10.67 months for cabazitaxel
vs
8 months511 events, duration 36 months

Cabazitaxel
vs
Mitoxantrone: Overall Survival
MP CBZP
Median OS (months) 12.7 15.1
Hazard ratio 0.72
95% CI 0.61–0.84
P-value <.0001
Median FU: 13.7 mo
MTX+PREDCBZ+PREDPr
opor
tion
of O
vera
llSu
rviv
al
0
10
20
30
40
50
60
70
80
90
100
0 6 12 18 24 30
377378
300321
188231
6790
1128
14
Number
at
RiskMTX + PREDCBZ + PRED
28% risk of death reduction
Time (months)
De Bono et al., Lancet 2010;376:1147-54

Is prostate cancer a chemosensitive neoplasm?
•
High response
rate
(>50%) in first-line•
Benefit
in OS in first-line (Docetaxel)
•
Second-line
chemotherapy
with demonstrated
activity
(Cabazitaxel)
•
Chemotherapy improves
PFS/OS when used
in the localized
setting
to prevent
relapse
YES
YES
YES: OS !
First answer
in 2014?

Sipuleucel-T: Autologous
APCs
cultured with
antigen
fusion protein
(PAP)

Sipuleucel-T autologous
vaccine: Overall Survival
0 6 12 18 24 30 36 42 48 54 60 660
25
50
75
100
Perc
ent S
urvi
val
Survival (Months)
p
= 0.032 (Cox model)HR = 0.78
[95% CI: 0.61, 0.98]
Sipuleucel-T (n = 341) vs
Placebo (n=171)Median OS: 25.8 vs
21.7 months
Kantoff PW, NEJM 2010, 363: 411-22Small EJ, J Clin Oncol 2009; 24: 3089-94

The “vicious cycle” of bone metastases
BoneRANK
RANKL
Bone Resorption
Osteoclast
Prostate cancer cells
Ca2+
Growth Factors (TGF-IGFs, FGFs,
PDGFs, BMPs)
Cytokines and Growth Factors (ET-1, IL-6, IL-8, TNF-
, PTHrP, etc)
Adapted from Roodman
GD. N Engl J Med. 2004;350:1655-64.
RA
NK
L
Direct effectson tumor?
Osteoblastlineage

Targeting
RANK-L: Proof of concept
OPG
RANKL
CTR CTROSB+ 2b
OSB+ 2a
OSB + LNCaP
OSB+ PC3
Fizazi et al., Clin Cancer Res 2003;9:2587–2597Fizazi et al., J Clin Oncol 2009; 27: 1564-71
RANK-L overexpressedby osteoblasts
in bone metastases
Positive randomized Phase II: Denosumabdecreases uNTx (biomarker for osteolysis)

Phase III trial of Denosumab in bone metastases from castrate-
resistant prostate cancer (103)
Denosumab
120 mg SC andPlacebo IV* every 4 weeks
Zoledronic
acid 4 mg IV* andPlacebo SC every 4 weeks
Castration-resistant prostate cancer and bone metastases
Key Inclusion
Current or prior intravenous bisphosphonate
administration
Key Exclusion
+ Supplemental Calcium and Vitamin D
SRE
n= 1901 patients

Denosumab: Time to First SRE
Zoledronic
Acid 951 733 544 407 299 207 140 93 64 47
Denosumab 950 758 582 472 361 259 168 115 70 39
Subjects at risk:
0
1.00
Prop
ortio
n of
Sub
ject
s W
ithou
t SR
E
0 3 6 9 12 15 18 21 24 27
0.25
0.50
0.75
KM Estimate of
Median MonthsDenosumabZoledronic
acid
20.717.1
HR 0.82 (95% CI: 0.71, 0.95) P = 0.0002 (Non-inferiority)
P = 0.008 (Superiority)
Study Month
18% Risk Reduction
Fizazi et al. Lancet 2011; 377: 811-822

0
1
2
3
4
5
6
7
8
9
%
Spinal cord compression
Preventing the onset of the worst enemy:
Placebo Zoledronicacid
Dmab
103 trialZA pivotal
trial
8% 4% 2.7%
Zoledronicacid
Denosumab
(120 mg Q4W) is not approved in the EU for use in patients with
advanced cancer to delay SREs. Denosumab
is investigational in that setting Saad, et al. J Natl Cancer Inst 2004;96:879–82; Fizazi et al. Lancet 2011; 377: 811-822

Radiopharmaceuticals: α
versus β-emitters
α-emitter:Radium-223
α-particles:2 neutrons + 2 protonsRelative mass: 7000
β-emitters:Strontium-89Samarium-153
β-particles:1 electronRelative mass: 1

Cell killing
and marrow
penetration: Two
advantages
of α-emitters
Large molecule+
High Linear
Energy
Transfer
More DNA double-strand
breaksIn (cancer) cells
Low
marrow
penetration
(≤100 μm )
Limited hematological
toxicity

TREATMENT
6 injections at 4-week intervals
Radium-223 (50 kBq/kg) + Best standard of care
Radium-223 (50 kBq/kg) + Best standard of care
Placebo (saline) + Best standard of care
Placebo (saline) + Best standard of care
RA
N D
O M I
ZE
D
2:1
N = 922
PATIENTS
•
Confirmed symptomatic CRPC
•
≥
2 bone metastases
•
No known visceral metastases
•
Post-
docetaxel
or unfit for docetaxel
•
Confirmed symptomatic CRPC
•
≥
2 bone metastases
•
No known visceral metastases
•
Post-
docetaxel
or unfit for docetaxel
ALSYMPCA (ALpharadin
in SYMptomatic Prostate CAncer) Phase III Study Design
Clinicaltrials.gov
identifier: NCT00699751.
•
Total ALP: < 220 U/L vs
≥
220 U/L
•
Bisphosphonate
use: Yes vs
No
•
Prior docetaxel: Yes vs
No
•
Total ALP: < 220 U/L vs
≥
220 U/L•
Bisphosphonate
use: Yes vs
No•
Prior docetaxel: Yes vs
No
STRATIFICATION
Planned follow-up is 3 years

Radium-223 Phase III trial (ALSYMPCA): Overall Survival
Radium-223, n = 614Median OS: 14.9 months
Placebo, n = 307Median OS: 11.3 months
HR = 0.69595% CI, 0.581, 0.832
P = 0.00007
Month 0 3 6 9 12 15 18 21 24 27 30 33 36 39
Radium-223 614 578 504 369 274 178 105 60 41 18 7 1 0 0
Placebo 307 288 228 157 103 67 39 24 14 7 4 2 1 0
0
10
20
30
40
50
60
70
80
90
100
%
n=921
Parker C, ASCO 2012

Systemic
treatment
for CRPC in 2012-2013
Local Treatment
PSA relapse (ADT)
Metastatic
Castrate-Resistant
Prostate Cancer
Castrate-resistant, M0
Metastatic
Hormone-Sensitive prostate cancer
Docetaxel
Zoledronate
Cabazitaxel
Denosumab
AbirateroneAbiraterone EnzalutamideRadium 223
Continuous
ADT
ADT

The cornucopia
of new drugs for CRPC
•
Endocrine agents–
Abiraterone
–
Enzalutamide•
Immunotherapy–
Sipuleucel-T
•
Chemotherapy–
Cabazitaxel
•
Bone-targeting
agents–
Denosumab
–
Alpharadin
The cornucopia
of new drugsfor CRPC in the future
•
Endocrine agents–
ODM 201
(ESMO 12)
–
ARN 509
(ASCO 12)–
Orteronel
•
Immunotherapy–
Ipilimumab
(2013?)
–
Prostvac–
Tasquinimod
•
Bone-targeting
agents–
Cabozantinib
(ASCO 12)
–
Dasatinib (2013?)•
HSP-targeting
drugs
–
OGX 011, OGX 427