tracey a. littrell, ba, dc, dacbr, daco, ccsplittrellradiology.com/images/phydia1/units/unit4/unit 4...
TRANSCRIPT

1
Eye Evaluation: Chapter 11
Tracey A. Littrell, BA, DC, DACBR, DACO, CCSP
Internal Eye
• Composed of three layers – Outer fibrous layer
• Sclera posteriorly and cornea anteriorly
– Middle layer • Choroid posteriorly and ciliary body/iris anteriorly
– Inner layer • Retina
Internal Eye (Cont.)
• Five major structures – Sclera – Cornea – Iris – Lens – Retina
Internal Eye (Cont.)
• Sclera – White of the eye – Avascular – Supports internal eye structures
• Cornea – Continuous with the sclera anteriorly – Clear – Sensory innervation for pain – Major part of the refractive power of the eye
Internal Eye (Cont.) • Uvea
– Iris, ciliary body, and choroids comprise the uveal tract
– The iris is a circular, contractile muscular disk containing pigment cells that produce the color of the eye
• Dilates/contracts to control amount of light traveling through the pupil to the retina
– The ciliary body produces the aqueous humor and contains the muscles controlling accommodation
– The choroid is a pigmented, richly vascular layer that supplies oxygen to the outer layer of the retina
Internal Eye (Cont.)
• Lens – A biconvex, transparent structure located
immediately behind the iris – Supported circumferentially by fibers arising
from the ciliary body • Contraction or relaxation of the ciliary body
changes its thickness – Changes in lens thickness allow images from
varied distances to be focused on the retina

2
Internal Eye (Cont.)
• Retina – Sensory network of the eye – Transforms light impulses into electrical
impulses, which are transmitted through: • Optic nerve • Optic tract • Optic radiation • Visual cortex • Consciousness in the cerebral cortex
Internal Eye (Cont.)
• Retina – Cortex interprets impulses as visual objects – Major landmarks of the retina include:
• Optic disc, from which the optic nerve originates, together with the central retinal artery and vein
• Macula, or fovea, is the site of central vision
Infants and Children
• Eye forms during the first 8 weeks of gestation – May become malformed due to maternal drug
ingestion or infection • Lacrimal drainage is complete at birth • By 2 to 3 weeks of age, the lacrimal gland
begins producing full volume of tears
Infants and Children (Cont.) • Vision development depends on nervous
system maturation and occurs over time – Term infants hyperopic [20/400] – Peripheral vision fully developed at birth – Central vision develops later – By 3 to 4 months of age, binocular vision
development is complete – By 6 months, vision has developed sufficiently so
that the infant can differentiate colors – The globe of the eye grows as the child’s head
and brain grow, and adult visual acuity is achieved at about 4 years of age
Pregnant Women • Hypersensitivity and changes in the refractory
power of the eye • Tears contain an increased level of lysozyme,
resulting in a greasy sensation and perhaps blurred vision for contact lens wearers
• Corneal edema/thickening occurs • Diabetic retinopathy may worsen • Intraocular pressure falls • Subconjunctival hemorrhages may occur/
resolve spontaneously
Older Adults
• The major physiologic eye change that occurs with aging is a progressive weakening of accommodation (focusing power) known as presbyopia
• Loss of lens clarity and cataract formation

3
The Visual Examination
• External eye inspection (least invasive) • Visual acuity: measured and recorded at
the beginning of the eye exam • Visual fields testing: detects and defines
important neurological or ocular disease • Pupillary exam: valuable clinical
information about disease processes • Ophthalmoscopy (most invasive) • Follow this order of exams
External eye exam
• Eyelids:
– should cover the top of the iris • Lacrimal gland
– Look for prominence of gland and excessive tearing
• Conjunctiva – Should be pink at the lid margins
• Sclera: – Should be white, without prominent blood vessels
• Cornea: – Should be clear
• Iris: – Should be same color without redness (minimal color
variation is okay) • Pupil:
– Shape, size, and responses – Should be equal size and PERRLA – Pupils are Equal, Round, Reactive to Light and
Accommodation
Visual acuity
• Equipment needed: Snellen or Sloan chart, pinhole occluder, near-vision card, color vision screening plates
• Measurement of visual acuity tests CN II (optic nerve) and is a test of central vision
• Very easy and quick to perform
Snellen chart
• Position the patient 20 feet away from the Snellen chart
• The chart should be placed at eye level (average) and should be well-lighted
• Each eye is tested individually, and by convention, we begin with the right eye
• A 3 x 5 card works well to occlude the other eye (doesn’t compress the eye)
• Testing should be performed with the patient wearing his or her distance glasses
Snellen chart • Ask the patient to read all of the letters on the smallest line he
or she can see clearly • After successful completion of one line, ask the patient to
identify as many letters as possible on the next smallest line • The visual acuity may be recorded in two manners (know both):
– the smallest line on which the patient can accurately identify more than one-half of the letters is the visual acuity, recorded as 20/that line’s number (20/25); additionally, record the number of letters missed on that same line (i.e. 20/25 -2 indicates 2 missed letters on that line)
– **** Or, record the number of the line seen with 100% accuracy and the number of letters correctly identified on the next line (i.e. 20/30 +3 indicates 3 correct letters on next line)
4
What do the numbers mean?
• 20/20 means that the patient can read at a distance of 20 feet a letter that was designed to be read at 20 feet
• 20/40 means that the patient can read at a distance of 20 feet a letter that was designed to be read at 40 feet
• Right eye = Oculus Dextra = O.D. • Left eye = Oculus Sinistra = O.S. • Both eyes = Oculus Uterque = O.U.
Pinhole Occluder
• Tests for visual acuity improvement • If you have trouble reading something,
what do you do? • If the patient’s vision improves by reading
through a small hole in the 3 x 5 card, the patient likely needs a prescription correction
Near vision testing
• A Rosenbaum near vision card is standard
• You may use other text to evaluate (office papers, large newsprint, Reader’s Digest)
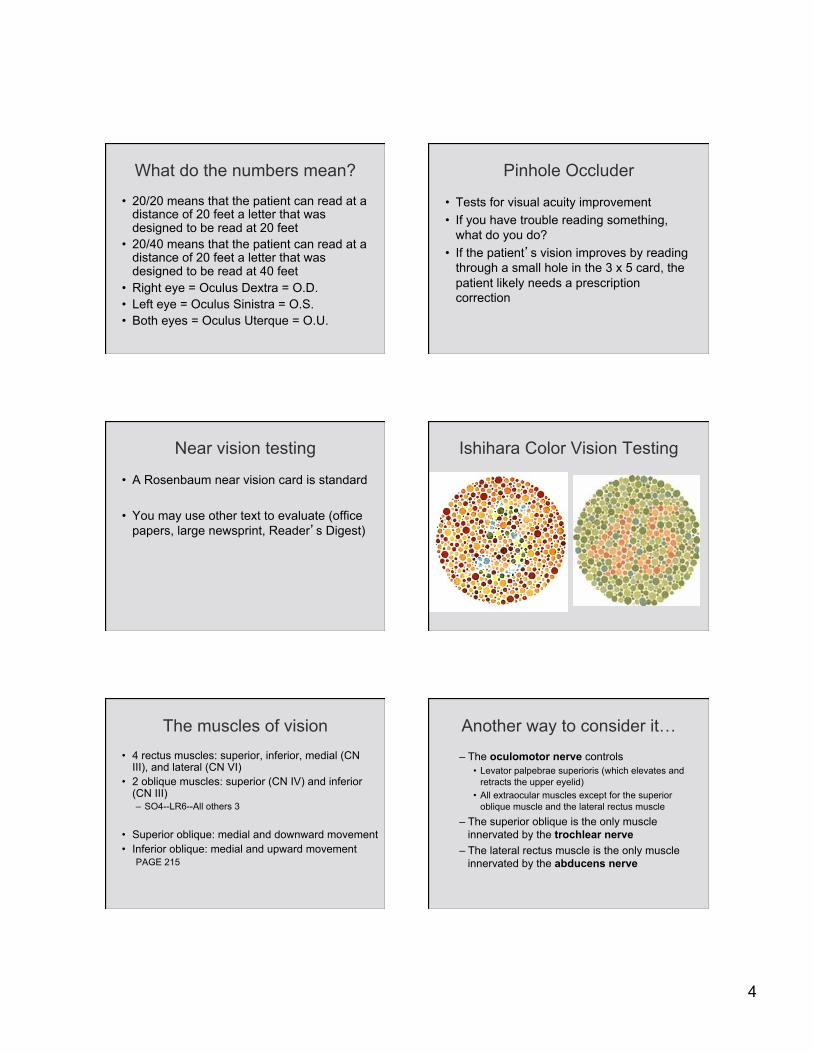
Ishihara Color Vision Testing
The muscles of vision • 4 rectus muscles: superior, inferior, medial (CN
III), and lateral (CN VI) • 2 oblique muscles: superior (CN IV) and inferior
(CN III) – SO4--LR6--All others 3
• Superior oblique: medial and downward movement • Inferior oblique: medial and upward movement
PAGE 215
– The oculomotor nerve controls • Levator palpebrae superioris (which elevates and
retracts the upper eyelid) • All extraocular muscles except for the superior
oblique muscle and the lateral rectus muscle – The superior oblique is the only muscle
innervated by the trochlear nerve – The lateral rectus muscle is the only muscle
innervated by the abducens nerve
Another way to consider it…
5
Cardinal fields/planes of gaze
• Sit (or stand) approximately 3 feet in front of the patient and hold a penlight or finger as a fixation point
• Ask the patient to follow the stimulus with his eyes only, without moving his head
• Draw a wide “H” pattern or asterisk • You are not testing accommodation (or
convergence), so move far enough away to allow binocular vision
Peripheral vision testing
• AKA: Visual fields testing, confrontation
• With peripheral fields testing, one can find previously undetected occipital strokes and optic chiasmal tumors (pituitary or suprasellar masses)
Peripheral vision testing
• Sit (or stand) 2 feet from patient and ask him or her to cover one eye with the palm of one hand or card while fixating on the examiner’s nose or opposite eye
• The examiner outstretches his or her hand and hold up 1, 2, or 5 fingers or a penlight (some definitive object) and moves from the periphery to centrally
• The patient reports when he or she can see the stimulus
• Confront in each quadrant of each eye • 60 nasally, 90 temporally, 50 superiorly, 70 inferiorly
Pupillary light reflexes/responses
• Accommodation/Near point reflex: – Convergence causes constriction of the pupils
Using a penlight: • Corneal light reflex/reflection:
– Shine the light at the nasal bridge. Ask patient to look at near object (not the light). If both eyes are aligned, the penlight will be reflected in both pupils equally
• Direct light reflex: – The pupil constricts with light stimulus
• Indirect light reflex/Consensual light reflex: – The opposite/contralateral pupil constricts with light
stimulus

6
Pupil abnormal responses • Physiological anisocoria: a normal variant
in 20%, characterized by a physiological difference in muscular tone between right and left pupils; does not change with illumination
• Pharmacologic dilation: sometimes unknowingly
• Horner’s syndrome: the pupil of the affected eye is smaller (miotic); patients also have ipsilateral ptosis and anhidrosis; difference varies with illumination
• Argyll Robertson pupils: constrict only in response to accommodation, but not in response to light; may be seen in tertiary syphillis, diabetics, alcoholics, neoplasms, infections; it is ALWAYS pathological
• Adie’s pupil: a tonic pupil that fails to constrict in response to BOTH light and accommodation; eventually it may constrict, but is sluggish; it is ALWAYS benign
Afferent pupillary defect
• AKA: Marcus Gunn pupil: has a normal efferent system, but an abnormal afferent pathway; using the “swinging flashlight test”, the affected eye will dilate in response to the light; on first stimulus, the Marcus Gunn pupil will constrict (normal), but poorly; optic neuritis is the most common cause, followed by asymmetric optic neuropathy, such as retinal lesion, artery occlusion
Causes of optic neuritis
• Demyelinating diseases (MS) • Infections: TB, HIV, Lyme’s disease,
Hepatitis B, Herpes, CMV • Sinus infections • Drugs • Radiation therapy

7
Ophthalmoscopic Examination
Equipment Overview • On/Off switch
– Optics: angled mirror allows compatible axes of both illumination and vision, reducing shadows
– Aperture: • Micro-spot: quick entry into undilated pupil • Small: excellent view of fundus in undilated pupil • Large: standard for dilated pupils • Slit or streak: useful to determine levels of lesions • Cobalt filter: used with fluorescein dye to evaluate small
lesions, corneal abrasions, foreign bodies • Red free filter: highlights hemorrhages
– Lens selection disc: • Some have -25 to +40 diopters • Allows for compensation of the patient’s and the
examiner’s vision • Allows examiner to focus on different portions of
the eye – Halogen light:
• Brighter than a regular penlight
– Brow rest: • Steadies the ophthalmoscope • Can be used with eyeglasses
Examining the eye • 1. Dim the lights in the room. This allows
the pupil to remain open. • 2. Examine the patient’s right eye with
your right eye and by holding the scope in your right hand. Stand slightly to the right of the patient.
• 3. Ask the patient to look at a SPECIFIC distant point in the room. The pupil dilates when using far vision and fixating on a far point decreases fatigue on the patient’s eyes.
• 4. Turn the light on. Experienced examiners will begin with the light high, then lower the intensity for patient comfort. For practice, begin with the light at approximately 70-80% intensity. You will be able to practice the exam for longer periods without tiring your partner’s eyes.
• 5. Put the scope to your eye with your index finger on the lens selection wheel.
8
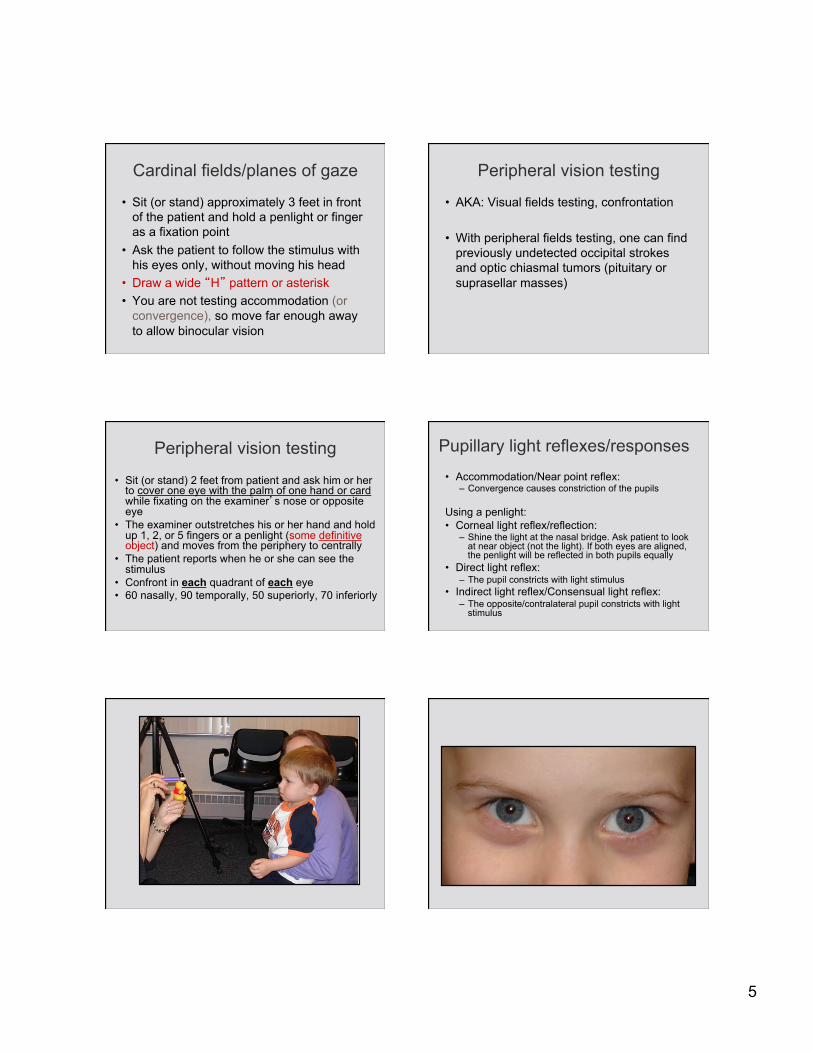
• 6. With the light about 6 inches and 25 degrees lateral (temporal) to the patient’s eye, look through the optic lens to view the patient’s pupil. Look for the red reflex, which indicates that you are appropriately viewing the retina (fundus).
• 7. Place your left hand on the patient’s forehead and lift the upper eyelid away from the iris with your thumb.
• 8. Move slowly towards the patient until the optic disc comes into view (keep the red reflex in view as you move closer).
• 9. Rotate the lens selector until the optic disc becomes clear. Patients who are myopic (near-sighted) will require the use of the “minus” lenses or red numbers. Patients who are hyperopic (far-sighted) will require the use of the “plus” lenses or green numbers.
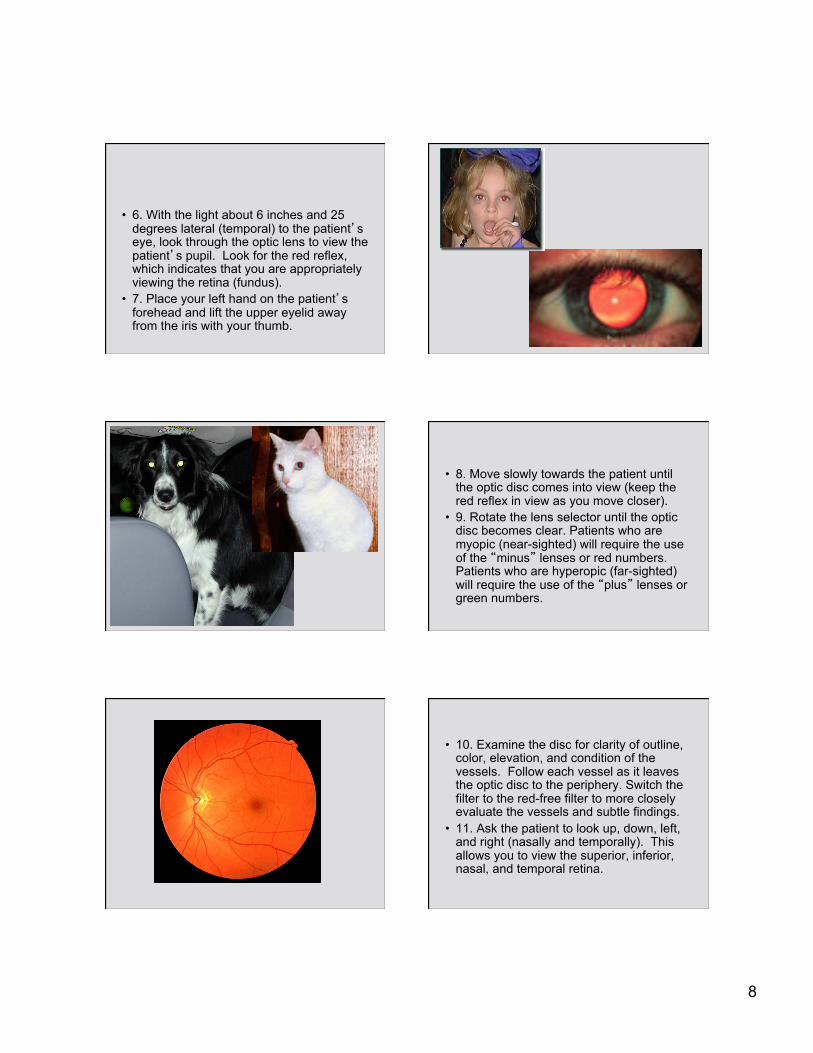
• 10. Examine the disc for clarity of outline, color, elevation, and condition of the vessels. Follow each vessel as it leaves the optic disc to the periphery. Switch the filter to the red-free filter to more closely evaluate the vessels and subtle findings.
• 11. Ask the patient to look up, down, left, and right (nasally and temporally). This allows you to view the superior, inferior, nasal, and temporal retina.
9
• 12. If the light reflected off the retina and the cornea interferes with your exam, switch to the cross-linear polarizing filter.
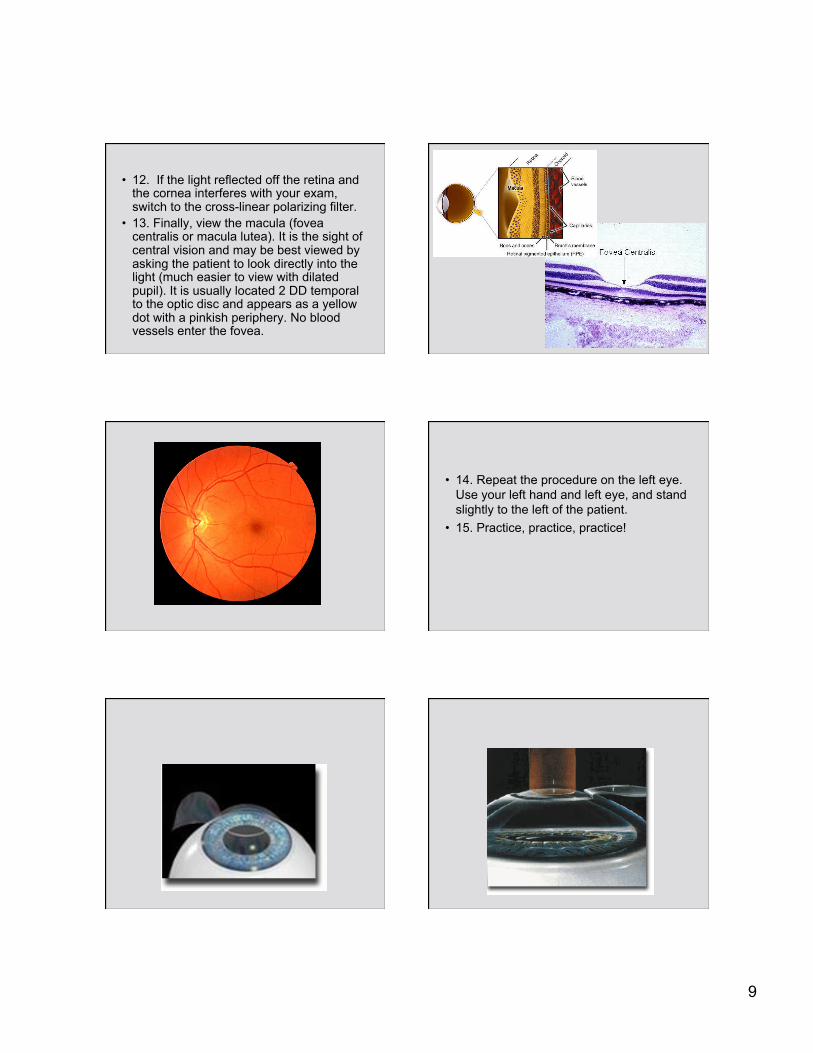
• 13. Finally, view the macula (fovea centralis or macula lutea). It is the sight of central vision and may be best viewed by asking the patient to look directly into the light (much easier to view with dilated pupil). It is usually located 2 DD temporal to the optic disc and appears as a yellow dot with a pinkish periphery. No blood vessels enter the fovea.
• 14. Repeat the procedure on the left eye. Use your left hand and left eye, and stand slightly to the left of the patient.
• 15. Practice, practice, practice!

10
Eye pathologies • AV ratio • Cupping • Xanthelasma • Ptosis • Ectropion • Entropion • Hordeolum (acute) Chalazion (chronic) • Blepharitis-inflammation of lash follicles • Cataracts
• Glaucoma • Pterygium • Conjunctivitis/red eye • Senile hyaline plaque • Drusen bodies • Corneal ulcer • Band keratopathy • Corneal ulcer • Strabismus • Amblyopia • Optic atrophy • Retinoblastoma
• Coloboma • Nystagmus • Arcus cornealis • Corneal light reflex • Stye • Blue sclera • Viral conjunctivitis and preauricular node • Arcus senilis • Leukocoria
Arcus cornealis
• An opaque, grayish ring at the periphery of the cornea, just within the sclerocorneal junction
• Frequently occurs in the elderly • Results from fatty granules in, or hyaline
degeneration of, the lamellae and cells of the cornea
11
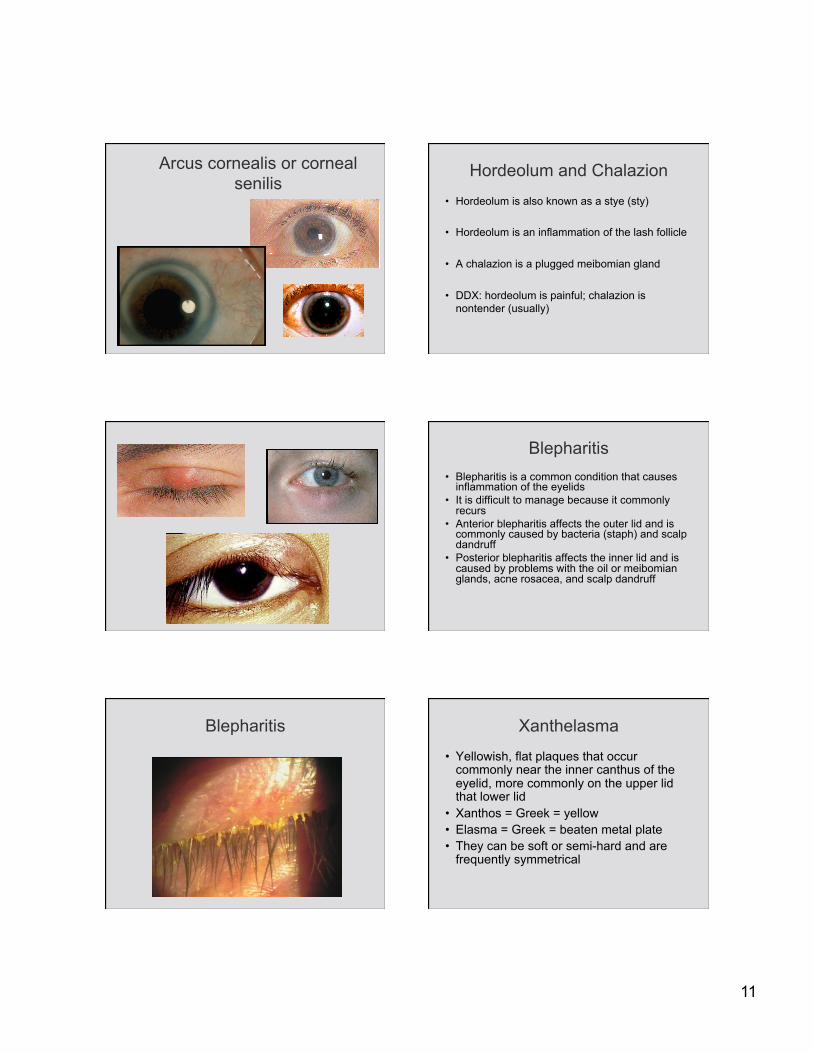
Arcus cornealis or corneal senilis
Hordeolum and Chalazion
• Hordeolum is also known as a stye (sty)
• Hordeolum is an inflammation of the lash follicle
• A chalazion is a plugged meibomian gland
• DDX: hordeolum is painful; chalazion is nontender (usually)
Blepharitis • Blepharitis is a common condition that causes
inflammation of the eyelids • It is difficult to manage because it commonly
recurs • Anterior blepharitis affects the outer lid and is
commonly caused by bacteria (staph) and scalp dandruff
• Posterior blepharitis affects the inner lid and is caused by problems with the oil or meibomian glands, acne rosacea, and scalp dandruff
Blepharitis Xanthelasma
• Yellowish, flat plaques that occur commonly near the inner canthus of the eyelid, more commonly on the upper lid that lower lid
• Xanthos = Greek = yellow • Elasma = Greek = beaten metal plate • They can be soft or semi-hard and are
frequently symmetrical

12
Xanthelasma
• 50% of these lesion occur with elevated plasma lipid levels
• Some occur with altered lipoprotein composition or structure such as lowered HDL levels
• They frequently occur in patients with Type II hyperlipidemia
Ectropion Entropion
Conjunctivitis
• Viral conjunctivitis is very common; the eyes feel gritty and discharge is possible
• Bacterial conjunctivitis causes yellow, sticky pus in the eyes; it is very common and highly contagious
• It is also known as… • Allergies and mechanical irritation also
cause conjunctivitis
Conjunctivitis

13
Pterygium/pinguecula
• Both are abnormal growths on the surface of the eyes
• A pinguecula does not typically interfere with sight and appears as a thickening lateral to the iris
• A pterygium may grow large enough to cover the iris and pupil and appears as a wedge-shaped growth lateral to the iris
• Both conditions are usually seen in warm, dry climates
Coloboma
Leukocoria
• “White reflex” instead of the red reflex • Indicates that something is either changing
the normal color of the retina (decreased blood supply) or that something is obstructing the normal reflex
• The most common cause is congenital cataract
• Retinoblastoma is the most serious cause of “white eye”

14
Leukocoria
Amblyopia
• Amblyopia is caused by any condition that affects normal use of the eyes and visual development
• There are three major causes of amblyopia: – Strabismus – Unequal focus – Cloudiness of the eye tissues (lens, cornea)
Normal retina

15
Diabetic retinopathy
• Diabetes, resulting in retinopathy, is the most common cause of blindness in individuals under the age of 65 (US)
• The duration of diabetes is the most important single risk factor with a 90% prevalence of retinopathy in those with the disease more than 15 years
• Early detection and treatment is currently the best hope of preservation of functional vision
Nonproliferative Diabetic Retinopathy (NDR)
• Most common form of diabetic retinopathy • After 20 years of diabetes, almost 100% of
patients with Type I and 60% of patients with Type II diabetes have some degree of retinopathy
• Clinical features: – Microaneurysm, hemorrhages, cotton wool
spots, exudates
Nonproliferative Diabetic Retinopathy (NPDR)
Proliferative Diabetic Retinopathy (PDR)
• Characterized by growth of new vessels on the surface of the retina
• Clinical features: – Progressive loss of vision – Fine to severe loops of new vessels that may grow on
the optic disk (neovascularization of the disk {NVD} or elsewhere {NVE})
– New vessels may leak and result in retinal edema – Risk factors: duration of diabetes, high cholesterol
and LDL, cigarette smoking, alcohol
Proliferative Diabetic Retinopathy (PDR)
Figure 11-45. Proliferative diabetic retinopathy. (Courtesy John W. Payne, MD, The Wilmer Ophthalmological Institute, The Johns Hopkins University and Hospital, Baltimore, MD.)

16
Neovascularization and hemorrhage in PDR Cotton wool spots
• Small, yellowish areas of coloration in the retina • They occur because of swelling of the surface of
the retina (microinfarcts) • The swelling usually occurs because blood to
the retina has been impaired; in the absence of normal blood flow, the nerve fibers are injured
• Often the spots will disappear on their own, but will recur with further blood flow impediments
• Cotton wool spots are most commonly due to diabetes and high blood pressure
Cotton wool spots Microaneurysms
• The microaneurysm is often the earliest recognizable clinical sign of diabetic retinopathy
• They are seen as small, round, dark red dots on the retinal surface (not arising from visible vessels) that are less than the diameter of the optic veins
• They increase in number as the degree of retinal involvement progresses
Microaneurysms Hemorrhages
• Retinal hemorrhages have variable shapes, sometimes resembling bundles of straw, or may be round or flame-shaped
• They indicate an increasingly ischemic retina
• As the number of hemorrhages increases, the retinal vessels become more damaged and leaky, leading to exudation of fluid, lipid, and proteins
17
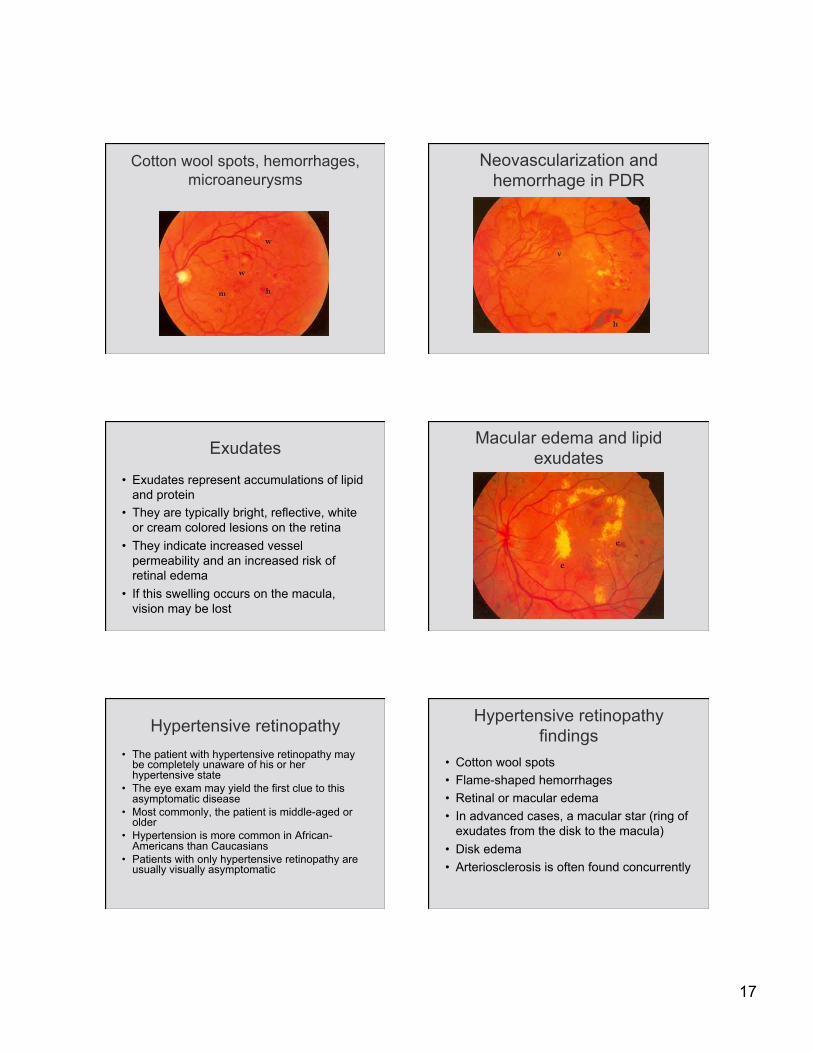
Cotton wool spots, hemorrhages, microaneurysms
Neovascularization and hemorrhage in PDR
Exudates
• Exudates represent accumulations of lipid and protein
• They are typically bright, reflective, white or cream colored lesions on the retina
• They indicate increased vessel permeability and an increased risk of retinal edema
• If this swelling occurs on the macula, vision may be lost
Macular edema and lipid exudates
Hypertensive retinopathy • The patient with hypertensive retinopathy may
be completely unaware of his or her hypertensive state
• The eye exam may yield the first clue to this asymptomatic disease
• Most commonly, the patient is middle-aged or older
• Hypertension is more common in African-Americans than Caucasians
• Patients with only hypertensive retinopathy are usually visually asymptomatic
Hypertensive retinopathy findings
• Cotton wool spots • Flame-shaped hemorrhages • Retinal or macular edema • In advanced cases, a macular star (ring of
exudates from the disk to the macula) • Disk edema • Arteriosclerosis is often found concurrently

18
Hypertensive retinopathy pathophysiology
• All the findings stem from the hypertension-induced changes in the retinal microvasculature
• Hypertension leads to a “laying down” of cholesterol into the tunica intima of medium and large arteries, leading to a decreased lumen size of these vessels and focal closure of the vessels
• This gives rise to the hemorrhages and cotton wool spots
• The mechanism is not fully understood, but it may be related to hypertension-induced increase in the ICP (intracranial pressure)
Hypertensive retinopathy
Hypertensive retinopathy Hypertensive retinopathy
AV ratio and AV nicking
• Remember that the normal arteriovenous ratio is 3:5 to 2:3
• The site of the crossing, the arteriole and vein share a common adventitial sheath
• Vascular sclerosis causes compression of the underlying lumen, resulting in “AV nicking” or a tapering of a venule (“skips”)
• The most common reason for AV nicking is prolonged systemic hypertension
19
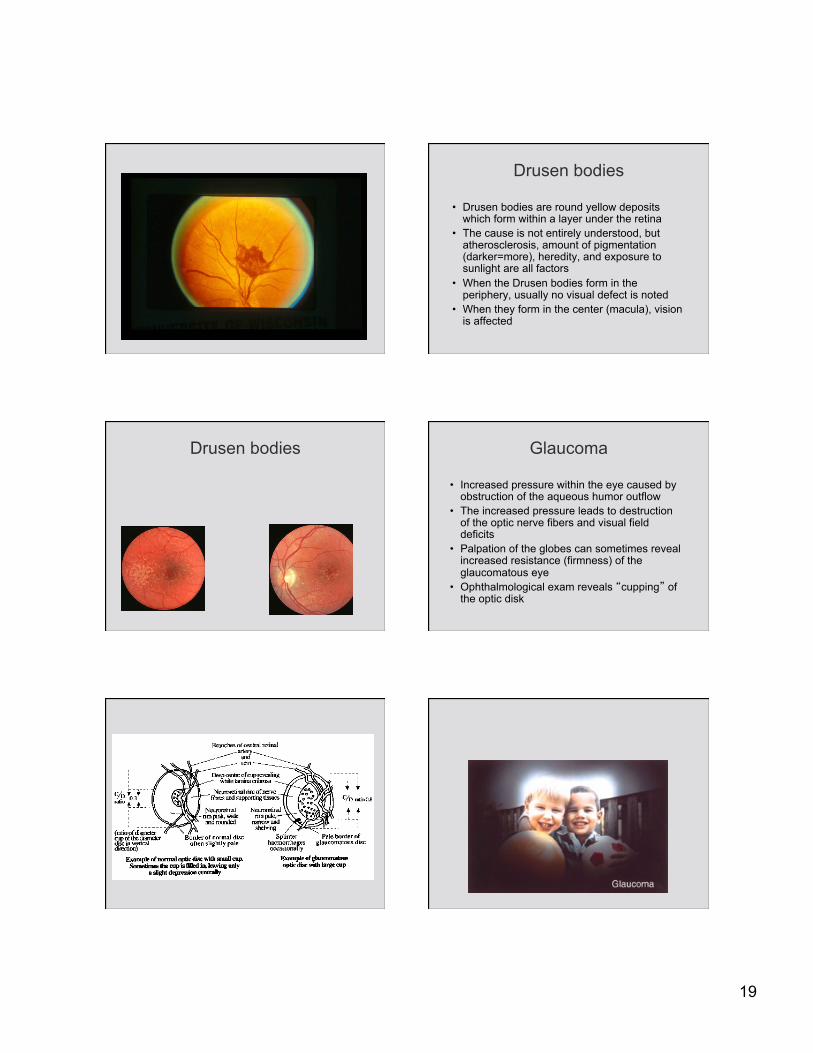
Drusen bodies
• Drusen bodies are round yellow deposits which form within a layer under the retina
• The cause is not entirely understood, but atherosclerosis, amount of pigmentation (darker=more), heredity, and exposure to sunlight are all factors
• When the Drusen bodies form in the periphery, usually no visual defect is noted
• When they form in the center (macula), vision is affected
Drusen bodies Glaucoma
• Increased pressure within the eye caused by obstruction of the aqueous humor outflow
• The increased pressure leads to destruction of the optic nerve fibers and visual field deficits
• Palpation of the globes can sometimes reveal increased resistance (firmness) of the glaucomatous eye
• Ophthalmological exam reveals “cupping” of the optic disk
20
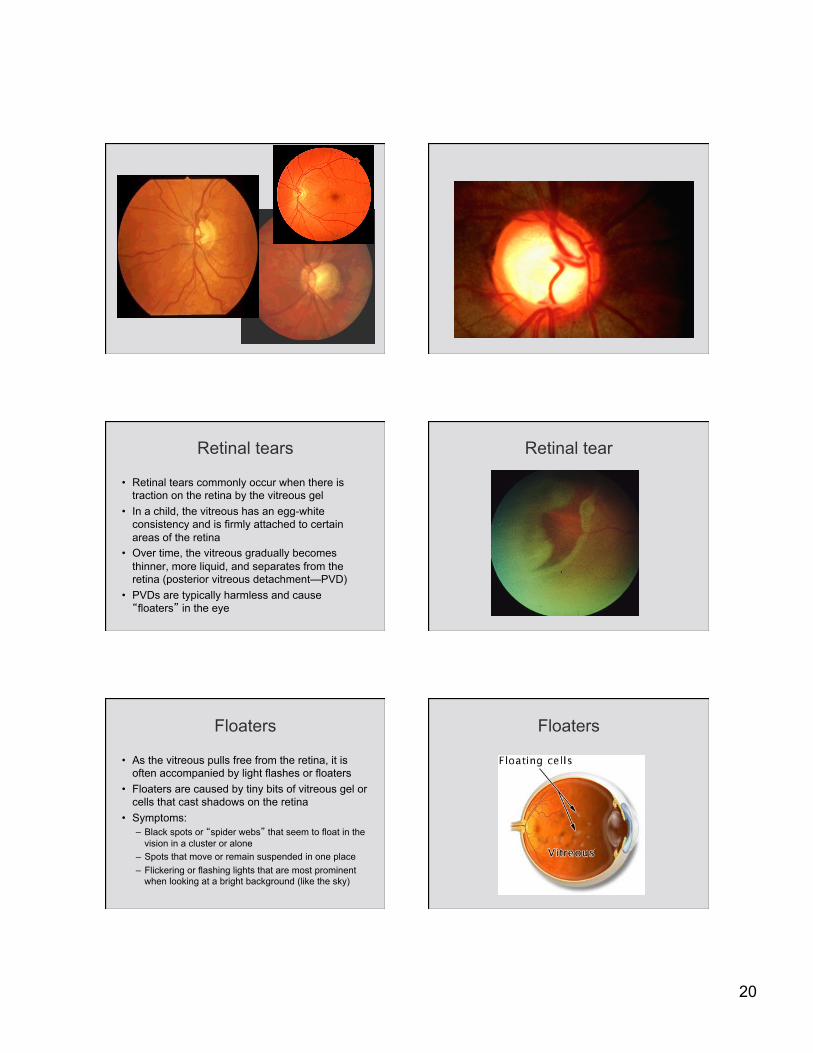
Retinal tears
• Retinal tears commonly occur when there is traction on the retina by the vitreous gel
• In a child, the vitreous has an egg-white consistency and is firmly attached to certain areas of the retina
• Over time, the vitreous gradually becomes thinner, more liquid, and separates from the retina (posterior vitreous detachment—PVD)
• PVDs are typically harmless and cause “floaters” in the eye
Retinal tear
Floaters
• As the vitreous pulls free from the retina, it is often accompanied by light flashes or floaters
• Floaters are caused by tiny bits of vitreous gel or cells that cast shadows on the retina
• Symptoms: – Black spots or “spider webs” that seem to float in the
vision in a cluster or alone – Spots that move or remain suspended in one place – Flickering or flashing lights that are most prominent
when looking at a bright background (like the sky)
Floaters

21
Retinal detachment
• A retinal detachment occurs when the retina’s sensory and pigment layers separate
• Retinal detachment is considered an ocular emergency because it can cause permanent visual damage
• It occurs most commonly in middle-aged and elderly
3 types of retinal detachment
• Most common type occurs when there is a break in the sensory layer of the retina, and fluid seeps underneath, causing the layers of the retina to separate
• Those who are very nearsighted (eye globes are longer, causing the retina to be thinner), have undergone eye surgery (not Lasik or RK), or have experienced a serious eye injury are more susceptible
• 2nd most common type of retinal detachment occurs when strands of vitreous or scar tissue create traction on the retina, pulling it loose
• Patients with diabetes are more likely to experience this type
• 3rd most common type of retinal detachment occurs when fluid collects underneath the layers of the retina, causing it to separate
• This type usually occurs in conjunction with another disease that affects the eyes
Retinal detachment Retinal detachment
22
Retinal detachment Signs and symptoms of retinal detachment
• Light flashes • “Wavy” or “watery” vision • Veil or curtain obstructing vision • Shower of floaters that resemble spots, bugs, or
spider webs • Sudden decrease of vision
• It is critical that you refer the patient to an ophthalmologist immediately for care to improve the chances for vision preservation
Papilledema • Papilledema is an optic disk swelling secondary
to elevated intracranial pressure (ICP) • In contrast to other causes of optic disk
swellings, vision is usually well preserved with acute papilledema
• It almost always presents as a bilateral phenomenon and may develop over hours to weeks
• The term should not be used to describe underlying infectious, infiltrative, or inflammatory etiologies
Papilledema
• The disk swelling in papilledema is the result of axoplasmic flow stasis with intra-axonal edema in the optic disk area
• The subarachnoid space of the brain is continuous with the optic nerve sheath
• Hence, as the CSF pressure increases, the pressure is transmitted to the optic nerve
• The optic nerve sheath acts as a tourniquet to impede axoplasmic transport
• This leads to a swelling of the nerve head
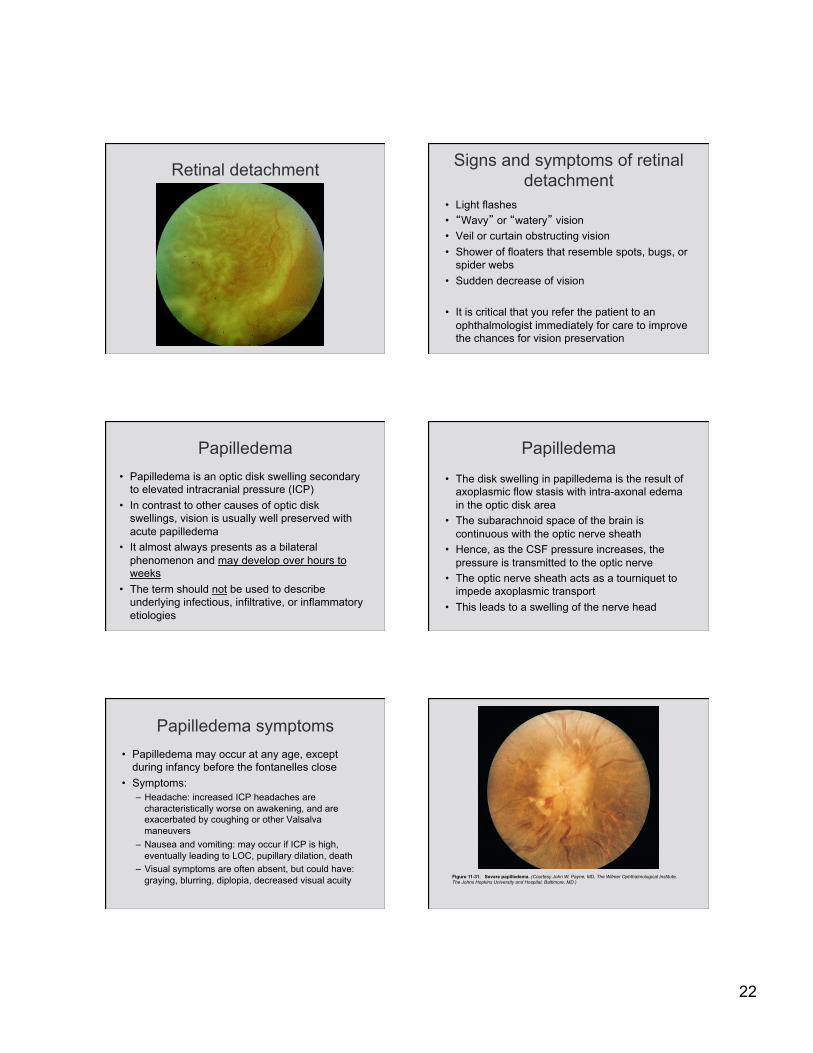
Papilledema symptoms • Papilledema may occur at any age, except
during infancy before the fontanelles close • Symptoms:
– Headache: increased ICP headaches are characteristically worse on awakening, and are exacerbated by coughing or other Valsalva maneuvers
– Nausea and vomiting: may occur if ICP is high, eventually leading to LOC, pupillary dilation, death
– Visual symptoms are often absent, but could have: graying, blurring, diplopia, decreased visual acuity Figure 11-31. Severe papilledema. (Courtesy John W. Payne, MD, The Wilmer Ophthalmological Institute,
The Johns Hopkins University and Hospital, Baltimore, MD.)

23
Papilledema Papilledema
Papilledema