totally laparoscopic abdominal wall reconstruction: lessons learned and results of a short-term...
TRANSCRIPT
ORIGINAL ARTICLE
Totally laparoscopic abdominal wall reconstruction: lessonslearned and results of a short-term follow-up
A. Moazzez • R. J. Mason • A. Darehzereshki •
N. Katkhouda
Received: 11 February 2012 / Accepted: 28 July 2013 / Published online: 9 August 2013
� Springer-Verlag France 2013
Abstract
Purpose Totally Laparoscopic Abdominal Wall Recon-
struction (TLAWR) combines the laparoscopic component
separation and the laparoscopic ventral hernia repair, with
the purpose of further increasing the benefits of a mini-
mally invasive procedure. However, neither the patient
selection criteria nor the long-term results of this technique
have been reported. Our objective is to discuss our expe-
rience with five patients who received a TLAWR.
Methods All patients with a midline incisional hernia
who underwent a TLAWR from September 2008 to
October 2009 were retrospectively reviewed for early and
late postoperative complications.
Results A total of five patients underwent the procedure,
with a mean age of 48.6 ± 7.9 years. The mean length of
stay was 9.2 ± 5.4 days, and follow-up was 12.3 ±
6.8 months. The mean defect size was 175.8 ± 56.2 cm2.
There were no early or late wound complications. Two
patients had an early respiratory complication, and one
patient developed a port site hernia and small bowel
obstruction early after procedure, which required a re-
operation. Three patients (60 %) experienced a recurrence.
Possible risk factors for recurrence include previous failed
hernia repair, loss of domain, large hernias and close
proximity to bony structures.
Conclusions Although TLAWR is feasible and improves
wound complications, it may be associated with higher
recurrence. Appropriate patient selection is imperative in
order for the patient to benefit from this technique.
Keywords Totally laparoscopic abdominal wall
reconstruction � Laparoscopic component separation �Hernia repair � Laparoscopic hernia repair
Introduction
In 1990, Ramirez et al. [1] reported the technique of
component separation (CST) by medializing the bilateral
rectus abdominis muscles, which allowed for an autologous
tissue reconstruction of the central abdominal wall without
the use of prosthetic materials. However, this technique
required extensive tissue dissection and was associated
with high rates of wound complications ranging from 30 to
40 % [2, 3]. In an attempt to overcome these complica-
tions, less invasive modifications of CST have been
developed, all with the goal of preserving the periumbilical
perforators [3–7]. Lowe et al. [3] described the endoscopic
technique of CST in 2000, which was associated with a
significantly lower wound complication rate. This tech-
nique has been gradually adopted by surgeons and in
addition has now been combined with a laparoscopic her-
nia repair; namely, a Totally Laparoscopic Abdominal
Wall Reconstruction (TLAWR) to further increase the
benefits from a totally laparoscopic procedure. Although
the short-term result of this technique was promising, there
is sparse published literature evaluating the long-term
outcomes.
The results of available case series of TLAWR have
reported no recurrence rates or wound complications by
12 months after the procedure [8, 9]. In this article, we
report our experience with a case series of five patients who
A. Moazzez (&)
Harbor-UCLA Medical Center, Torrance, CA, USA
e-mail: [email protected]
R. J. Mason � A. Darehzereshki � N. Katkhouda
University of Southern California, Los Angeles, CA, USA
123
Hernia (2013) 17:633–638
DOI 10.1007/s10029-013-1145-0

underwent a TLAWR for an abdominal wall hernia, and
will discuss the outcomes, patient selection criteria and
potential pitfalls in the management of this group.
Materials and methods
After approval by the Institutional Review Board of the
University of Southern California, all patients with a midline
incisional hernia, who underwent a TLAWR at LAC ? USC
Medical Center during a time period between September
2008 and October 2009, were retrospectively reviewed.
Patients’ data were collected through review of charts and
clinic notes. All postoperative clinic evaluations were per-
formed by a surgeon. Demographic and perioperative data
including age, gender, body mass index (BMI, calculated as
weight in kilograms divided by height in meters squared),
number of previous abdominal surgeries and hernia repairs,
as well as defect size were recorded in a Microsoft Excel
database. Early and late complications were reviewed. The
descriptive data were calculated using Microsoft Excel.
Surgical technique
We have previously described our technique [10]. In
summary, the technique consists of four steps: 1. Laparo-
scopic bilateral component separation, 2. Laparoscopic
lysis of adhesions, 3. Approximation of rectus muscles, and
4. Intraperitoneal mesh placement. After receiving naso-
gastric tube, Foley catheterization, and preoperative anti-
biotics, patients were placed in the supine position with
both arms extended. Important anatomical landmarks,
including the costal margin, the anterior superior iliac
spine, the hernia margins, and the lateral border of rectus
abdominis were identified and marked on both sides.
First incision was made in a transverse fashion in front of
the 11th rib. The fascia of the external oblique was opened
and its muscle fibers were separated until the internal
oblique muscle was visualized. The space between the
external and internal oblique muscles was then, first bluntly
and then using a SpacemakerTM Balloon Dissector (Covi-
dien, Norwalk, CT) dissected. The correct placement of the
balloon was confirmed by direct vision of the internal
oblique muscle inferiorly, the external oblique superiorly
and the semilunaris line on the medial side. This trocar was
then removed, and a balloon trocar was replaced. The
insufflation pressure was maintained at 15 mmHg. A 5- or
10-mm trocar was then placed under direct vision in the
lateral abdominal wall, at the level of mid-axillary line.
Using a laparoscopic scissors, the external oblique fascia
was divided about 1–2 cm lateral to the semilunaris line and
extended inferiorly toward the inguinal ligament. At this
point, another 5- or 10-mm port was placed, and incision of
the fascia continued superiorly about 5 cm above the costal
margin until the pectoralis major muscle fibers were visu-
alized. This was performed on both sides.
One of the subcostal ports was introduced into the
abdomen under direct vision and the peritoneal cavity was
insufflated. Other trocars were added as needed. All
adhesions were meticulously taken down. Once the hernia
was completely free of adhesions, the hernia defect was
measured and a piece of mesh was measured so that it
covers the defect with an overlap of at least 5 cm. An
overlap of 7–10 cm was considered, if the end of hernia
defect was close to the xiphoid process or pubic bone.
At the next step, the rectus muscles on both sides were
approximated using multiple non-absorbable figure-of-
eight sutures through the fascia. Through a stab incision in
midline, a Prolene #1 suture was passed through the fascia
about 1–1.5 cm lateral to the edge using a suture passer.
The suture passer was then introduced back through the
fascia on the other side and at the same level, and the free
end of the suture was retrieved. This was done one more
time through the same stab incision to complete a figure-of-
eight suture. The needed number of sutures to completely
approximate the rectus muscles was placed through mul-
tiple midline stab incisions and a Rummel tourniquet
technique was used to keep the sutures under tension and to
bring the fascia edges closer together, as the other sutures
were placed. After completion of placement of these
sutures, they were all pulled at the same time to ensure that
the fascial edges can be approximated. Then the mesh was
introduced into the abdominal cavity and the transfascial
sutures were passed through the abdominal wall using a
suture passer. Next, the intra-abdominal pressure was
lowered to 5–8 mmHg, and the midline sutures were tied in
place to close the defect. Approximation of the fascial
edges along the whole length of the hernia defect was
accomplished in all five cases. Then the transfascial sutures
were tied and mesh was further secured to the abdominal
wall using a combination of tackers and fibrin sealant
(Tisseel�, Baxter Bio-surgery, Deerfield, IL). All port sites
that were accessed using open technique were closed with
sutures. Four patients received Proceed� mesh (Ethicon
Inc. Somerville, NJ, USA), and one received Parietex�
(Covidien, Norwalk, CT, USA).
Results
Five patients (four male and one female) underwent a
TLAWR with mesh during the study period. The mean age
was 48.6 ± 7.9 years, and the mean BMI was 29.71 ± 3.4.
Two patients had previous history of hernia repair. All
defects were located in the midline, and the mean defect
size was 175.8 ± 56.2 cm2. Table 1 summarizes the
634 Hernia (2013) 17:633–638
123
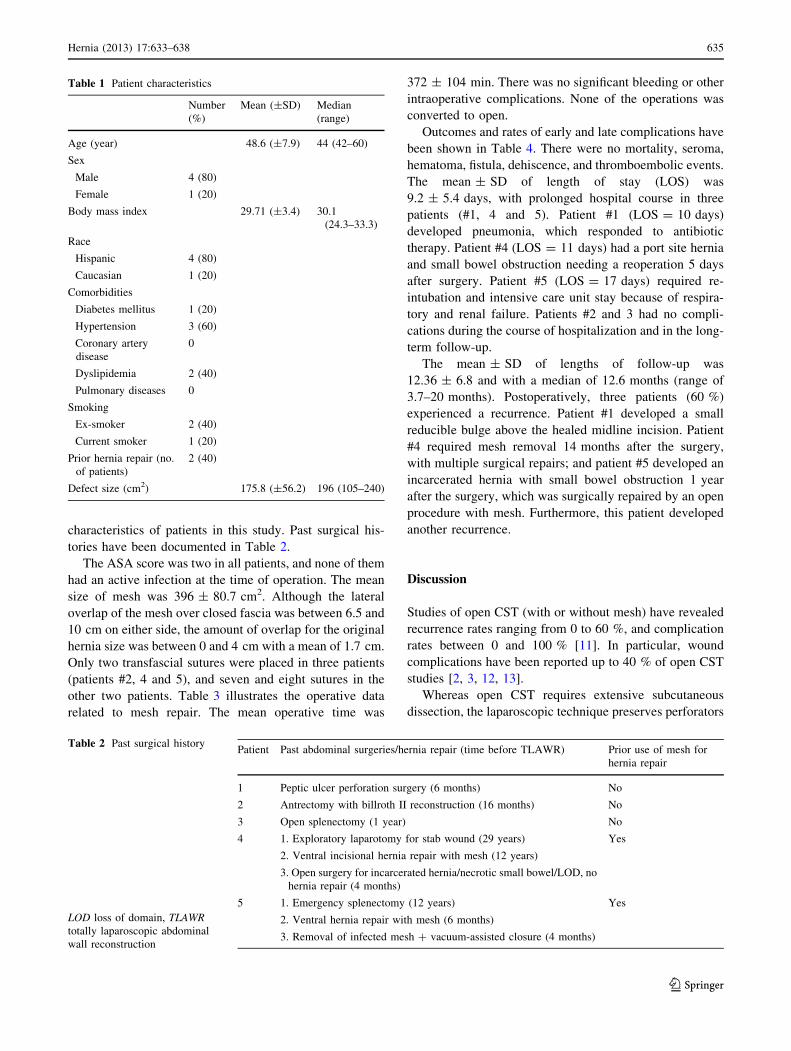
characteristics of patients in this study. Past surgical his-
tories have been documented in Table 2.
The ASA score was two in all patients, and none of them
had an active infection at the time of operation. The mean
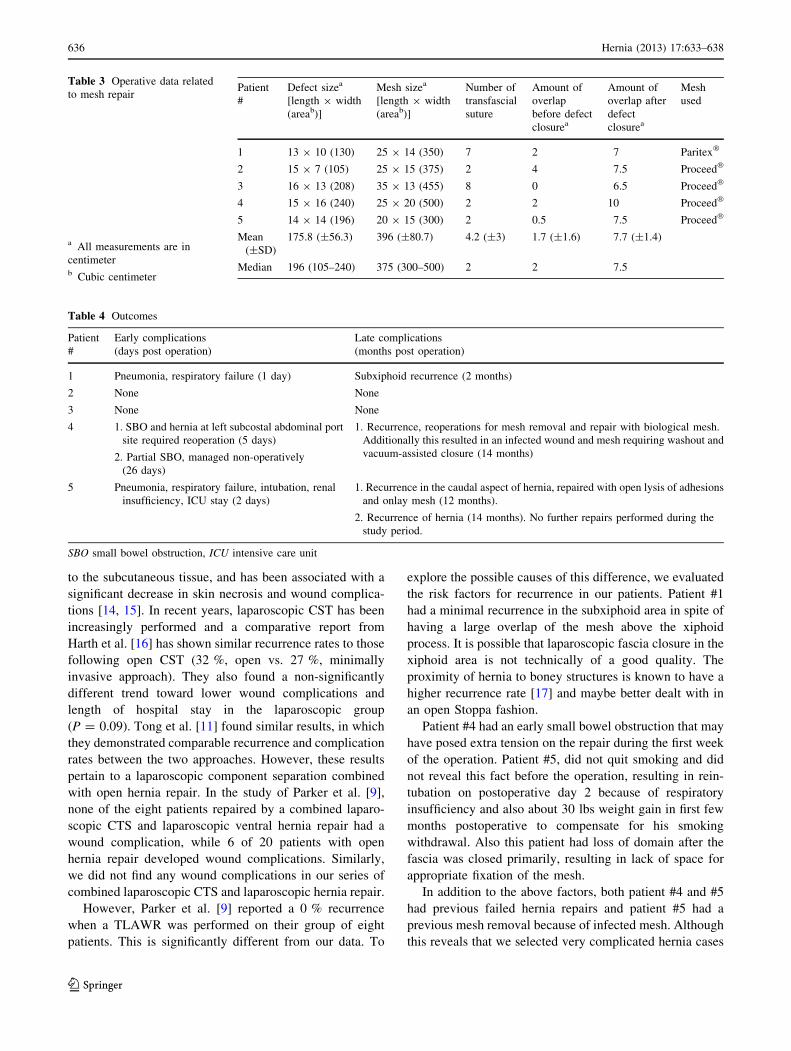
size of mesh was 396 ± 80.7 cm2. Although the lateral
overlap of the mesh over closed fascia was between 6.5 and
10 cm on either side, the amount of overlap for the original
hernia size was between 0 and 4 cm with a mean of 1.7 cm.
Only two transfascial sutures were placed in three patients
(patients #2, 4 and 5), and seven and eight sutures in the
other two patients. Table 3 illustrates the operative data
related to mesh repair. The mean operative time was
372 ± 104 min. There was no significant bleeding or other
intraoperative complications. None of the operations was
converted to open.
Outcomes and rates of early and late complications have
been shown in Table 4. There were no mortality, seroma,
hematoma, fistula, dehiscence, and thromboembolic events.
The mean ± SD of length of stay (LOS) was
9.2 ± 5.4 days, with prolonged hospital course in three
patients (#1, 4 and 5). Patient #1 (LOS = 10 days)
developed pneumonia, which responded to antibiotic
therapy. Patient #4 (LOS = 11 days) had a port site hernia
and small bowel obstruction needing a reoperation 5 days
after surgery. Patient #5 (LOS = 17 days) required re-
intubation and intensive care unit stay because of respira-
tory and renal failure. Patients #2 and 3 had no compli-
cations during the course of hospitalization and in the long-
term follow-up.
The mean ± SD of lengths of follow-up was
12.36 ± 6.8 and with a median of 12.6 months (range of
3.7–20 months). Postoperatively, three patients (60 %)
experienced a recurrence. Patient #1 developed a small
reducible bulge above the healed midline incision. Patient
#4 required mesh removal 14 months after the surgery,
with multiple surgical repairs; and patient #5 developed an
incarcerated hernia with small bowel obstruction 1 year
after the surgery, which was surgically repaired by an open
procedure with mesh. Furthermore, this patient developed
another recurrence.
Discussion
Studies of open CST (with or without mesh) have revealed
recurrence rates ranging from 0 to 60 %, and complication
rates between 0 and 100 % [11]. In particular, wound
complications have been reported up to 40 % of open CST
studies [2, 3, 12, 13].
Whereas open CST requires extensive subcutaneous
dissection, the laparoscopic technique preserves perforators
Table 1 Patient characteristics
Number
(%)
Mean (±SD) Median
(range)
Age (year) 48.6 (±7.9) 44 (42–60)
Sex
Male 4 (80)
Female 1 (20)
Body mass index 29.71 (±3.4) 30.1
(24.3–33.3)
Race
Hispanic 4 (80)
Caucasian 1 (20)
Comorbidities
Diabetes mellitus 1 (20)
Hypertension 3 (60)
Coronary artery
disease
0
Dyslipidemia 2 (40)
Pulmonary diseases 0
Smoking
Ex-smoker 2 (40)
Current smoker 1 (20)
Prior hernia repair (no.
of patients)
2 (40)
Defect size (cm2) 175.8 (±56.2) 196 (105–240)
Table 2 Past surgical history
LOD loss of domain, TLAWR
totally laparoscopic abdominal
wall reconstruction
Patient Past abdominal surgeries/hernia repair (time before TLAWR) Prior use of mesh for
hernia repair
1 Peptic ulcer perforation surgery (6 months) No
2 Antrectomy with billroth II reconstruction (16 months) No
3 Open splenectomy (1 year) No
4 1. Exploratory laparotomy for stab wound (29 years)
2. Ventral incisional hernia repair with mesh (12 years)
3. Open surgery for incarcerated hernia/necrotic small bowel/LOD, no
hernia repair (4 months)
Yes
5 1. Emergency splenectomy (12 years)
2. Ventral hernia repair with mesh (6 months)
3. Removal of infected mesh ? vacuum-assisted closure (4 months)
Yes
Hernia (2013) 17:633–638 635
123
to the subcutaneous tissue, and has been associated with a
significant decrease in skin necrosis and wound complica-
tions [14, 15]. In recent years, laparoscopic CST has been
increasingly performed and a comparative report from
Harth et al. [16] has shown similar recurrence rates to those
following open CST (32 %, open vs. 27 %, minimally
invasive approach). They also found a non-significantly
different trend toward lower wound complications and
length of hospital stay in the laparoscopic group
(P = 0.09). Tong et al. [11] found similar results, in which
they demonstrated comparable recurrence and complication
rates between the two approaches. However, these results
pertain to a laparoscopic component separation combined
with open hernia repair. In the study of Parker et al. [9],
none of the eight patients repaired by a combined laparo-
scopic CTS and laparoscopic ventral hernia repair had a
wound complication, while 6 of 20 patients with open
hernia repair developed wound complications. Similarly,
we did not find any wound complications in our series of
combined laparoscopic CTS and laparoscopic hernia repair.
However, Parker et al. [9] reported a 0 % recurrence
when a TLAWR was performed on their group of eight
patients. This is significantly different from our data. To
explore the possible causes of this difference, we evaluated
the risk factors for recurrence in our patients. Patient #1
had a minimal recurrence in the subxiphoid area in spite of
having a large overlap of the mesh above the xiphoid
process. It is possible that laparoscopic fascia closure in the
xiphoid area is not technically of a good quality. The
proximity of hernia to boney structures is known to have a
higher recurrence rate [17] and maybe better dealt with in
an open Stoppa fashion.
Patient #4 had an early small bowel obstruction that may
have posed extra tension on the repair during the first week
of the operation. Patient #5, did not quit smoking and did
not reveal this fact before the operation, resulting in rein-
tubation on postoperative day 2 because of respiratory
insufficiency and also about 30 lbs weight gain in first few
months postoperative to compensate for his smoking
withdrawal. Also this patient had loss of domain after the
fascia was closed primarily, resulting in lack of space for
appropriate fixation of the mesh.
In addition to the above factors, both patient #4 and #5
had previous failed hernia repairs and patient #5 had a
previous mesh removal because of infected mesh. Although
this reveals that we selected very complicated hernia cases
Table 3 Operative data related
to mesh repair
a All measurements are in
centimeterb Cubic centimeter
Patient
#
Defect sizea
[length 9 width
(areab)]
Mesh sizea
[length 9 width
(areab)]
Number of
transfascial
suture
Amount of
overlap
before defect
closurea
Amount of
overlap after
defect
closurea
Mesh
used
1 13 9 10 (130) 25 9 14 (350) 7 2 7 Paritex�
2 15 9 7 (105) 25 9 15 (375) 2 4 7.5 Proceed�
3 16 9 13 (208) 35 9 13 (455) 8 0 6.5 Proceed�
4 15 9 16 (240) 25 9 20 (500) 2 2 10 Proceed�
5 14 9 14 (196) 20 9 15 (300) 2 0.5 7.5 Proceed�
Mean
(±SD)
175.8 (±56.3) 396 (±80.7) 4.2 (±3) 1.7 (±1.6) 7.7 (±1.4)
Median 196 (105–240) 375 (300–500) 2 2 7.5
Table 4 Outcomes
Patient
#
Early complications
(days post operation)
Late complications
(months post operation)
1 Pneumonia, respiratory failure (1 day) Subxiphoid recurrence (2 months)
2 None None
3 None None
4 1. SBO and hernia at left subcostal abdominal port
site required reoperation (5 days)
2. Partial SBO, managed non-operatively
(26 days)
1. Recurrence, reoperations for mesh removal and repair with biological mesh.
Additionally this resulted in an infected wound and mesh requiring washout and
vacuum-assisted closure (14 months)
5 Pneumonia, respiratory failure, intubation, renal
insufficiency, ICU stay (2 days)
1. Recurrence in the caudal aspect of hernia, repaired with open lysis of adhesions
and onlay mesh (12 months).
2. Recurrence of hernia (14 months). No further repairs performed during the
study period.
SBO small bowel obstruction, ICU intensive care unit
636 Hernia (2013) 17:633–638
123

in the later part of our experience, this also signifies that
complicated patients with previous failed hernia repair,
previous mesh removal or a history of infected mesh should
possibly be treated with an open ventral hernia repair.
It is also important to note that laparoscopic closure of
fascia does not allow for a good evaluation of the edges of
the fascia and its viability. So, whenever there is doubt
about the healthiness of fascia edges, i.e., previous failed
hernia repairs, previous mesh placements/removals, previ-
ous mesh or wound infections, it may be preferable to repair
the hernia in an open fashion. This allows for the possibility
to evaluate the fascia edges and debride it as necessary.
Other possible general factors contributing to recurrence
in our series could be the lack of sufficient mesh overlap,
lack of enough number of transfascial sutures, later failure
of midline fascia closure because of extra tension on the
edges of the fascia, ischemia of fascial edges or inadequate
fascial bites with suture. Factors related to mesh are also of
significant importance. For example, mesh shrinkage could
have contributed to recurrences, as meshes used in this
study can contract from 15 to 30 % [18]. Macroporous
versus microporous nature of the mesh can be another
related factor; however, all of our recurrences happened at
the periphery of the mesh and not the center, which may
indicate that mesh shrinkage played a more important role
in recurrences compared to the size of the pores of the mesh.
We suggest that to decrease the risk of recurrence when
the mesh is placed intraperitoneally, the overlap of the
mesh should be added to the original size of the hernia
before closure of the fascia. In other words, for example, if
the hernia width is 10 cm, the mesh width should be at
least 20 cm (i.e., 5 cm on either side of a 10 cm hernia
defect) and not 10 cm (5 cm overlap assuming the defect
size is 0 when it is closed primarily). In our series, the
amount of overlap considering the original hernia size was
only 0–4 cm and we believe that this was an important
factor for high recurrence rate seen in our series.
Because of the preoperative loss of domain in patients #
4 and 5, and loss of working space after closure of the
fascia, we were not able to place extra transfascial sutures
in addition to those placed previously in these patients. Not
only is placement of the appropriate number of transfascial
sutures necessary to transfer the tension from fascia to the
mesh and to secure the mesh to the fascia, but it should
also be performed prior to tying of the figure-of-eight
sutures. We also believe that increased tension could lead
to the necrosis of the fascia at the suture site putting the
patient at increased risk for recurrence. History of previous
recurrence and mesh repair (40 %) are other factors that
could have contributed to recurrence in two of the three
patients with complications. Another interesting finding
was association of early complications and risk of recur-
rence (Table 4). All the recurrences happened in patients,
who had an early complication. This again may be an
indicator of importance of patient selection for TLAWR.
Another explanation for the difference between our data
and Parker’s data [9] is the nature of the follow-up. All of
our patients were evaluated for recurrence postoperatively
by a surgeon. However, in Parkers series, follow-up was
performed telephonically, which may have resulted in an
underestimation of the recurrence rate because of the
patients’ inability to evaluate a hernia recurrence.
Ultimately, the minimally invasive abdominal wall
reconstruction may be beneficial in selected patients with
midline incisional hernia, who based on surgeon’s opinion
will need a component separation in addition to the hernia
repair. Based on our limited experience in this case series,
we suggest the following selection criteria for TLAWR:
1. Surgical expertise in performing TLAWR
2. Midsize hernia defects (8–12 cm). (However, if
approximation of the rectus muscles cannot be
achieved easily, fascial closure should be converted
to open fashion.)
3. Midline hernias away from the xiphoid process and the
pubic bone
4. None of the following contraindications:
a. Prior failed hernia repair
b. Prior use of mesh or if the mesh needs to be
removed
c. Obese patients whose abdominal contour may
prevent an accurate placement of fascial closure
sutures
d. Loss of domain
e. Need for a concomitant procedure that requires an
open approach or if there is a risk of contamination
f. Need for skin debridement because of presence of
skin graft or skin ulcer.
Our study is limited by the small number of cases
(n = 5) and uncontrolled retrospective nature of the study.
Also the pattern of recurrence is indicative of an aggressive
patient selection after the third patient. The reported fol-
low-up of patients in our case series occurred over a
3.7–20 month period. Longer follow-up of each patient is
needed to fully assess the hernia recurrence.
Conclusion
Based on our experience with this small number of cases,
we believe that although a TLAWR improves wound
complications, it may not be a preferred technique in cases
of very large hernia or defects closed to bony structures.
Moreover, previous history of failed hernia repair or loss of
domain places the patient at increased risk of recurrence. In
Hernia (2013) 17:633–638 637
123

this group of high risk patients, probably a different
approach (such as a combination of laparoscopic compo-
nent separation and open hernia repair), which can maxi-
mize the outcome benefits, including a lower recurrence
risk should be chosen. Patient selection plays a very
important role to have an acceptable result. It is important
to emphasize that there is only a very limited number of
patients with abdominal wall hernias, who may meet this
stringent selection criteria and as a result may benefit from
TLAWR. Otherwise, while the patient may benefit from
less wound complications, they may end up having a
recurrence or more severe complications.
Conflict of interest A.M, R.M, A.D and N.K declares no conflict of
interest that directly relates to this study.
References
1. Ramirez OM, Ruas E, Dellon AL (1990) ‘‘Components separa-
tion’’ method for closure of abdominal-wall defects: an anatomic
and clinical study. Plast Reconstr Surg 86:519–526
2. de Vries Reilingh TS, van Goor H, Rosman C, Bemelmans MH,
de Jong D, van Nieuwenhoven EJ et al (2003) ‘‘Components
separation technique’’ for the repair of large abdominal wall
hernias. J Am Coll Surg 196:32–37
3. Lowe JB, Garza JR, Bowman JL, Rohrich RJ, Strodel WE (2000)
Endoscopically assisted ‘‘components separation’’ for closure of
abdominal wall defects. Plast Reconstr Surg 105:720–729
4. Maas SM, de Vries RS, van Goor H, de Jong D, Bleichrodt RP
(2002) Endoscopically assisted ‘‘components separation tech-
nique’’ for the repair of complicated ventral hernias. J Am Coll
Surg 194:388–390
5. Rosen MJ, Williams C, Jin J, McGee MF, Schomisch S, Marks J
et al (2007) Laparoscopic versus open-component separation: a
comparative analysis in a porcine model. Am J Surg 194:385–389
6. Milburn ML, Shah PK, Friedman EB, Roth JS, Bochicchio GV,
Gorbaty B et al (2007) Laparoscopically assisted components
separation technique for ventral incisional hernia repair. Hernia
11:157–161
7. Baghai M, Ramshaw BJ, Smith CD, Fearing N, Bachman S,
Ramaswamy A (2009) Technique of laparoscopic ventral hernia
repair can be modified to successfully repair large defects in
patients with loss of domain. Surg Innov 16:38–45
8. Malik K, Bowers SP, Smith CD, Asbun H, Preissler S (2009) A
case series of laparoscopic components separation and rectus
medialization with laparoscopic ventral hernia repair. J Laparo-
endosc Adv Surg Tech A 19:607–610
9. Parker M, Bray JM, Pfluke JM, Asbun HJ, Smith CD, Bowers SP
(2011) Preliminary experience and development of an algorithm
for the optimal use of the laparoscopic component separation
technique for myofascial advancement during ventral incisional
hernia repair. J Laparoendosc Adv Surg Tech A 21:405–410
10. Moazzez A, Mason RJ, Katkhouda N (2010) A new technique for
minimally invasive abdominal wall reconstruction of complex
incisional hernias: totally laparoscopic component separation and
incisional hernia repair. Surg Technol Int 20:185–191
11. Tong WM, Hope W, Overby DW, Hultman CS (2011) Com-
parison of outcome after mesh-only repair, laparoscopic compo-
nent separation, and open component separation. Ann Plast Surg
66:551–556
12. Lowe JB 3rd, Lowe JB, Baty JD, Garza JR (2003) Risks asso-
ciated with ‘‘components separation’’ for closure of complex
abdominal wall defects. Plast Reconstr Surg 111:1276–1283
13. Gonzalez R, Rehnke RD, Ramaswamy A, Smith CD, Clarke JM,
Ramshaw BJ (2005) Components separation technique and lap-
aroscopic approach: a review of two evolving strategies for
ventral hernia repair. Am Surg 71:598–605
14. Clarke JM (2010) Incisional hernia repair by fascial component
separation: results in 128 cases and evolution of technique. Am J
Surg 200:2–8
15. Saulis AS, Dumanian GA (2002) Periumbilical rectus abdominis
perforator preservation significantly reduces superficial wound
complications in ‘‘separation of parts’’ hernia repairs. Plast
Reconstr Surg 109:2275–2280
16. Harth KC, Rosen MJ (2010) Endoscopic versus open component
separation in complex abdominal wall reconstruction. Am J Surg
199:342–346
17. Morales-Conde S (2004) Laparoscopic ventral hernia repair:
advances and limitations. Semin Laparos Surg 11:191–200
18. Pierce RA, Perrone JM, Nimeri A, Sexton JA, Walcutt J, Frisella
MM, Matthews BD (2009) 120-day comparative analysis of
adhesion grade and quantity, mesh contraction, and tissue
response to a novel omega-3 fatty acid bio-absorbable barrier
macroporous mesh after intraperitoneal placement. Surg Innov
16:46–54
638 Hernia (2013) 17:633–638
123