total laparorobotic repair of abdominal aortic aneurysm with sac exclusion obliteration and...
TRANSCRIPT
1Section oUniversity of C
2Section ofMedicine, Chic
CorrespondSurgery and ES. Marylandhbassiou@surg
Ann Vasc SurgDOI: 10.1016/� Annals of VPublished onli
Total Laparorobotic Repair of AbdominalAortic Aneurysm with Sac ExclusionObliteration and Aortobifemoral Bypass
Timothy Wu,1 Jateen Prema,1 Gregory Zagaja,2 Arieh Shalhav,2
and Hisham S. Bassiouny,1 Chicago, Illinois
A 65-year-old man with coronary artery disease, hypertension, and peripheral vascular diseasewas found to have an asymptomatic abdominal aortic aneurysm (AAA) of 5.5 cm on surveillancefor his peripheral vascular disease. Cardiac stress testing demonstrated no evidence of myocar-dial ischemia, and he opted to undergo open repair of his aneurysm. Laparorobotic repair of theinfrarenal AAA using the da Vinci� robotic system was performed with an aortobifemoralbypass. We describe a novel technique for AAA exclusion using a cerclage method, whichgreatly facilitates repair of infrarenal AAAs using laparorobotic techniques. Laparorobotic repairof infrarenal AAA can be greatly facilitated by AAA sac exclusion and obliteration without theneed to ligate all lumbar arteries or to open the aneurysm. This virtually avoids blood lossfrom the sac and minimizes the possibility for open conversion as a result of poor visualization.Minimally invasive aortic intervention for aneurysmal disease using laparascopic methods hasbeen reported in the literature. Problems associated with this technique include a prolongedlearning curve and difficulty completing intracorporeal anastomoses. Robotic surgery providesan advantage over laparoscopic surgery in its ability to provide greater degrees of freedom ina relatively small field of view along with superior high-definition, three-dimensional visualization.To date, there have been no known reports of using robotic surgery in the United States as a solemethod for repair of AAA. We report our technique of combining robotic surgery with a novelprocedure for sac exclusion and obliteration to successfully repair AAA without the need foropening the aneurysm sac and endoaneurysmorrhaphy.
CASE REPORT
A 65-year-old man with coronary artery disease,
hypertension, and peripheral vascular disease pre-
sented with an incidentally found asymptomatic
abdominal aortic aneurysm (AAA) measuring
5.5 cm. The patient had a history of prior coronary
artery bypass surgery as well as bilateral iliac stents
f Vascular Surgery and Endovascular Therapy, Thehicago Pritzker School of Medicine, Chicago, IL.
Urology, The University of Chicago Pritzker School ofago, IL.
ence to: Hisham S. Bassiouny, MD, Section of Vascularndovascular Therapy, The University of Chicago, 5841
Avenue, MC 5028, Chicago, IL 60637, USA, E mail:ery.bsd.uchicago.edu
2009; 23: 686.e11 686.e16j.avsg.2009.02.005ascular Surgery Inc.ne: July 24, 2009
for his peripheral arterial disease. On physical
exam he had a palpable AAA with pedal pulses bilat-
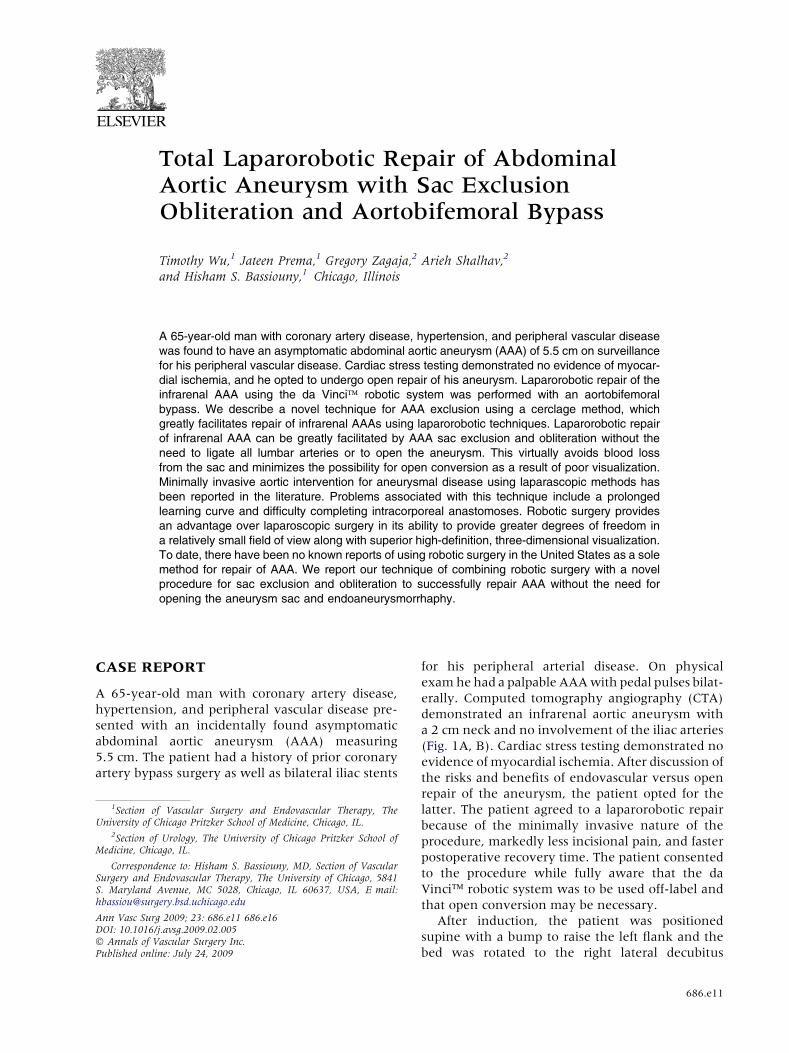
erally. Computed tomography angiography (CTA)
demonstrated an infrarenal aortic aneurysm with
a 2 cm neck and no involvement of the iliac arteries
(Fig. 1A, B). Cardiac stress testing demonstrated no
evidence of myocardial ischemia. After discussion of
the risks and benefits of endovascular versus open
repair of the aneurysm, the patient opted for the
latter. The patient agreed to a laparorobotic repair
because of the minimally invasive nature of the
procedure, markedly less incisional pain, and faster
postoperative recovery time. The patient consented
to the procedure while fully aware that the da
Vinci� robotic system was to be used off-label and
that open conversion may be necessary.
After induction, the patient was positioned
supine with a bump to raise the left flank and the
bed was rotated to the right lateral decubitus
686.e11
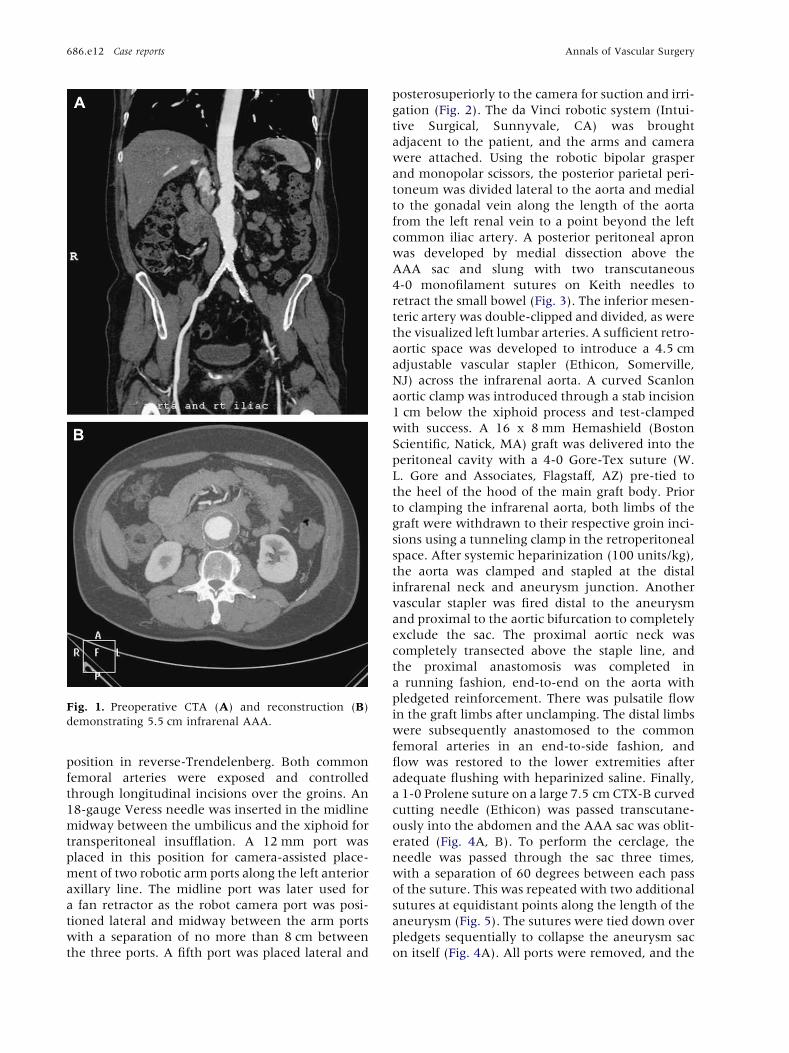
Fig. 1. Preoperative CTA (A) and reconstruction (B)
demonstrating 5.5 cm infrarenal AAA.
686.e12 Case reports Annals of Vascular Surgery
position in reverse-Trendelenberg. Both common
femoral arteries were exposed and controlled
through longitudinal incisions over the groins. An
18-gauge Veress needle was inserted in the midline
midway between the umbilicus and the xiphoid for
transperitoneal insufflation. A 12 mm port was
placed in this position for camera-assisted place-
ment of two robotic arm ports along the left anterior
axillary line. The midline port was later used for
a fan retractor as the robot camera port was posi-
tioned lateral and midway between the arm ports
with a separation of no more than 8 cm between
the three ports. A fifth port was placed lateral and
posterosuperiorly to the camera for suction and irri-
gation (Fig. 2). The da Vinci robotic system (Intui-
tive Surgical, Sunnyvale, CA) was brought
adjacent to the patient, and the arms and camera
were attached. Using the robotic bipolar grasper
and monopolar scissors, the posterior parietal peri-
toneum was divided lateral to the aorta and medial
to the gonadal vein along the length of the aorta
from the left renal vein to a point beyond the left
common iliac artery. A posterior peritoneal apron
was developed by medial dissection above the
AAA sac and slung with two transcutaneous
4-0 monofilament sutures on Keith needles to
retract the small bowel (Fig. 3). The inferior mesen-
teric artery was double-clipped and divided, as were
the visualized left lumbar arteries. A sufficient retro-
aortic space was developed to introduce a 4.5 cm
adjustable vascular stapler (Ethicon, Somerville,
NJ) across the infrarenal aorta. A curved Scanlon
aortic clamp was introduced through a stab incision
1 cm below the xiphoid process and test-clamped
with success. A 16 x 8 mm Hemashield (Boston
Scientific, Natick, MA) graft was delivered into the
peritoneal cavity with a 4-0 Gore-Tex suture (W.
L. Gore and Associates, Flagstaff, AZ) pre-tied to
the heel of the hood of the main graft body. Prior
to clamping the infrarenal aorta, both limbs of the
graft were withdrawn to their respective groin inci-
sions using a tunneling clamp in the retroperitoneal
space. After systemic heparinization (100 units/kg),
the aorta was clamped and stapled at the distal
infrarenal neck and aneurysm junction. Another
vascular stapler was fired distal to the aneurysm
and proximal to the aortic bifurcation to completely
exclude the sac. The proximal aortic neck was
completely transected above the staple line, and
the proximal anastomosis was completed in
a running fashion, end-to-end on the aorta with
pledgeted reinforcement. There was pulsatile flow
in the graft limbs after unclamping. The distal limbs
were subsequently anastomosed to the common
femoral arteries in an end-to-side fashion, and
flow was restored to the lower extremities after
adequate flushing with heparinized saline. Finally,
a 1-0 Prolene suture on a large 7.5 cm CTX-B curved
cutting needle (Ethicon) was passed transcutane-
ously into the abdomen and the AAA sac was oblit-
erated (Fig. 4A, B). To perform the cerclage, the
needle was passed through the sac three times,
with a separation of 60 degrees between each pass
of the suture. This was repeated with two additional
sutures at equidistant points along the length of the
aneurysm (Fig. 5). The sutures were tied down over
pledgets sequentially to collapse the aneurysm sac
on itself (Fig. 4A). All ports were removed, and the
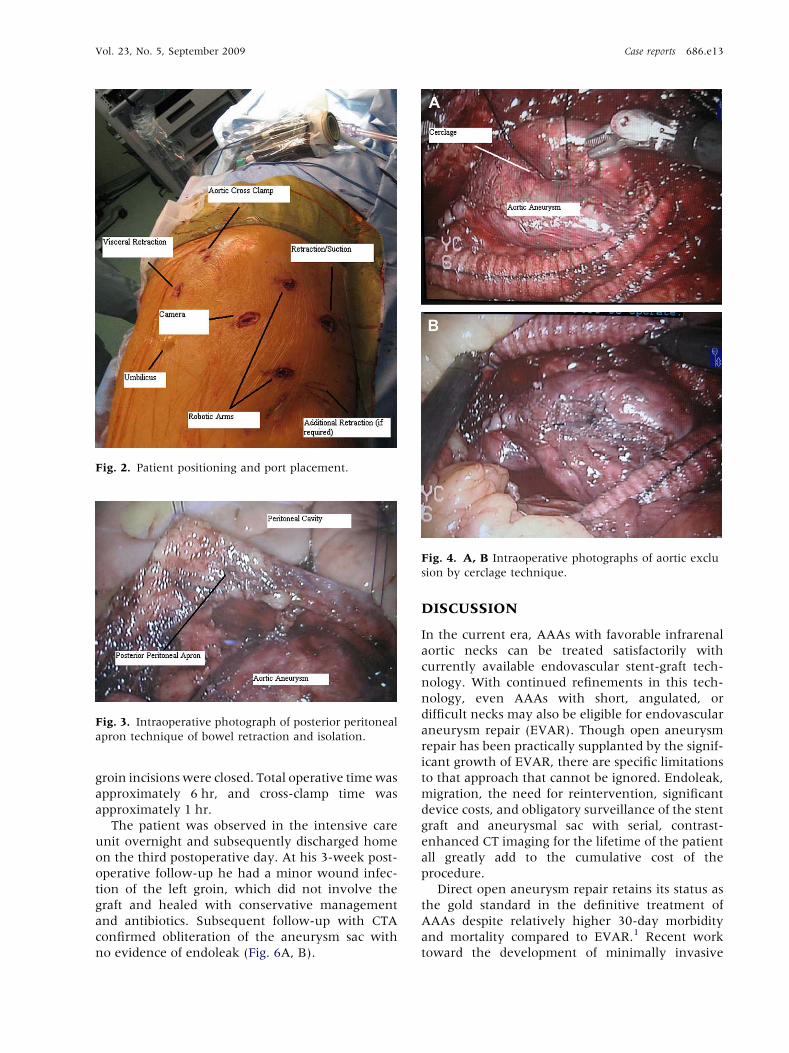
Fig. 2. Patient positioning and port placement.
Fig. 3. Intraoperative photograph of posterior peritoneal
apron technique of bowel retraction and isolation.
Fig. 4. A, B Intraoperative photographs of aortic exclu
sion by cerclage technique.
Vol. 23, No. 5, September 2009 Case reports 686.e13
groin incisions were closed. Total operative time was
approximately 6 hr, and cross-clamp time was
approximately 1 hr.
The patient was observed in the intensive care
unit overnight and subsequently discharged home
on the third postoperative day. At his 3-week post-
operative follow-up he had a minor wound infec-
tion of the left groin, which did not involve the
graft and healed with conservative management
and antibiotics. Subsequent follow-up with CTA
confirmed obliteration of the aneurysm sac with
no evidence of endoleak (Fig. 6A, B).
DISCUSSION
In the current era, AAAs with favorable infrarenal
aortic necks can be treated satisfactorily with
currently available endovascular stent-graft tech-
nology. With continued refinements in this tech-
nology, even AAAs with short, angulated, or
difficult necks may also be eligible for endovascular
aneurysm repair (EVAR). Though open aneurysm
repair has been practically supplanted by the signif-
icant growth of EVAR, there are specific limitations
to that approach that cannot be ignored. Endoleak,
migration, the need for reintervention, significant
device costs, and obligatory surveillance of the stent
graft and aneurysmal sac with serial, contrast-
enhanced CT imaging for the lifetime of the patient
all greatly add to the cumulative cost of the
procedure.
Direct open aneurysm repair retains its status as
the gold standard in the definitive treatment of
AAAs despite relatively higher 30-day morbidity
and mortality compared to EVAR.1 Recent work
toward the development of minimally invasive
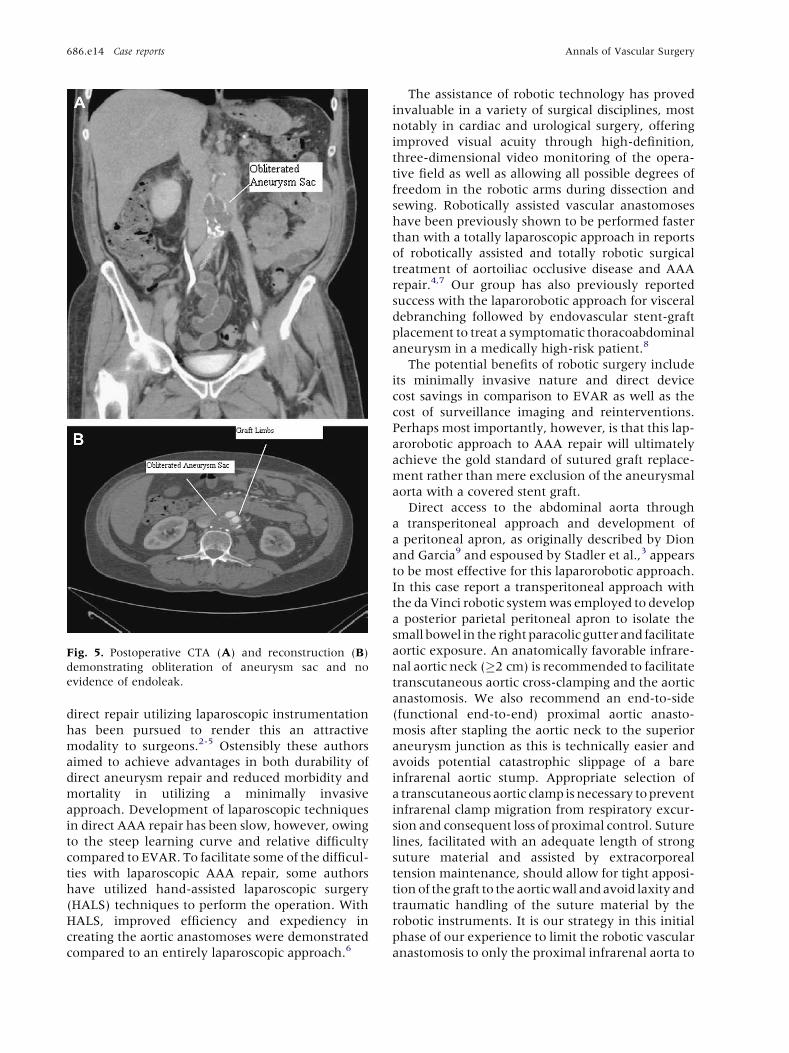
Fig. 5. Postoperative CTA (A) and reconstruction (B)
demonstrating obliteration of aneurysm sac and no
evidence of endoleak.
686.e14 Case reports Annals of Vascular Surgery
direct repair utilizing laparoscopic instrumentation
has been pursued to render this an attractive
modality to surgeons.2-5 Ostensibly these authors
aimed to achieve advantages in both durability of
direct aneurysm repair and reduced morbidity and
mortality in utilizing a minimally invasive
approach. Development of laparoscopic techniques
in direct AAA repair has been slow, however, owing
to the steep learning curve and relative difficulty
compared to EVAR. To facilitate some of the difficul-
ties with laparoscopic AAA repair, some authors
have utilized hand-assisted laparoscopic surgery
(HALS) techniques to perform the operation. With
HALS, improved efficiency and expediency in
creating the aortic anastomoses were demonstrated
compared to an entirely laparoscopic approach.6
The assistance of robotic technology has proved
invaluable in a variety of surgical disciplines, most
notably in cardiac and urological surgery, offering
improved visual acuity through high-definition,
three-dimensional video monitoring of the opera-
tive field as well as allowing all possible degrees of
freedom in the robotic arms during dissection and
sewing. Robotically assisted vascular anastomoses
have been previously shown to be performed faster
than with a totally laparoscopic approach in reports
of robotically assisted and totally robotic surgical
treatment of aortoiliac occlusive disease and AAA
repair.4,7 Our group has also previously reported
success with the laparorobotic approach for visceral
debranching followed by endovascular stent-graft
placement to treat a symptomatic thoracoabdominal
aneurysm in a medically high-risk patient.8
The potential benefits of robotic surgery include
its minimally invasive nature and direct device
cost savings in comparison to EVAR as well as the
cost of surveillance imaging and reinterventions.
Perhaps most importantly, however, is that this lap-
arorobotic approach to AAA repair will ultimately
achieve the gold standard of sutured graft replace-
ment rather than mere exclusion of the aneurysmal
aorta with a covered stent graft.
Direct access to the abdominal aorta through
a transperitoneal approach and development of
a peritoneal apron, as originally described by Dion
and Garcia9 and espoused by Stadler et al.,3 appears
to be most effective for this laparorobotic approach.
In this case report a transperitoneal approach with
the da Vinci robotic system was employed to develop
a posterior parietal peritoneal apron to isolate the
small bowel in the right paracolic gutter and facilitate
aortic exposure. An anatomically favorable infrare-
nal aortic neck (�2 cm) is recommended to facilitate
transcutaneous aortic cross-clamping and the aortic
anastomosis. We also recommend an end-to-side
(functional end-to-end) proximal aortic anasto-
mosis after stapling the aortic neck to the superior
aneurysm junction as this is technically easier and
avoids potential catastrophic slippage of a bare
infrarenal aortic stump. Appropriate selection of
a transcutaneous aortic clamp is necessary to prevent
infrarenal clamp migration from respiratory excur-
sion and consequent loss of proximal control. Suture
lines, facilitated with an adequate length of strong
suture material and assisted by extracorporeal
tension maintenance, should allow for tight apposi-
tion of the graft to the aortic wall and avoid laxity and
traumatic handling of the suture material by the
robotic instruments. It is our strategy in this initial
phase of our experience to limit the robotic vascular
anastomosis to only the proximal infrarenal aorta to

Fig. 6. Schema of aneurysm exclusion in robotic AAA
repair. This diagram shows a modified approach to
robotic AAA repair. Endovascular placement of bilateral
iliac occluders or the cerclage technique can function to
exclude the aneurysm completely.
Vol. 23, No. 5, September 2009 Case reports 686.e15
minimize operative and limb ischemia time and
potentially risky dissection of the iliac vessels. Hence,
the rationale for aortobifemoral reconstruction in
this case is to quickly restore lower extremity perfu-
sion. As with any operative technique in its relative
infancy, development and advancement of this
approach must be made with the safety of the patient
of ultimate concern. Conversion to an open direct
repair is mandatory for excessive blood loss or oper-
ative time over a predetermined threshold.
In our approach the lumbar arteries are not
ligated within the sac as this is left intact to maintain
operative exposure and to minimize blood loss. We
instead clip the left lumbar arteries with titanium
surgical clips. While there may be a theoretical risk
of continued pressurization of the aneurysm sac by
the remaining, patent lumbar arteries and, with
that, a risk of expansion of the sac and subsequent
rupture, this risk has been reported to be 4 7%
with EVAR.10 The cerclage approach to aneurysm
exclusion obliterates the sac lumen, which theoret-
ically promotes sac thrombosis and any significant
endoleak from residual lumbar arteries. The patient
described in this case has undergone several surveil-
lance CT scans postoperatively, and at 1 year there is
evidence of complete obliteration of the aneurysm
sac, with no evidence of endoleak. We describe
distal exclusion of the aneurysm sac in this case by
use of a vascular stapler; however, additional
adjuncts for iliac occlusion can be used, such as
intravascular occlusion devices introduced in
a retrograde fashion from the femoral anastomosis
and stapling of the inferior mesenteric artery if
necessary.
CONCLUSION
The described technique for repair of an infrarenal
AAA with the da Vinci robotic system offers the
possibility of aortic repair without violating the
aneurysm sac. The aneurysm sac is obliterated by
a cerclage technique which, though previously
unpublished, has proven effective, as evidenced by
complete AAA sac obliteration at 1 year on CT
imaging. This case was performed using the da Vinci
robotic system as an off-label device as it is currently
not approved by the Food and Drug Administration
(FDA) for aortic reconstruction. An investigational
device exemption for peripheral and aortic recon-
struction is currently under review by the FDA. Lap-
arorobotic AAA repair by exclusion and
aortobifemoral bypass has the potential to evolve
into a viable, minimally invasive alternative to
open repair which offers a durable reconstruction
for infrarenal AAA.
REFERENCES
1. Blankensteijn JD, de Jong SE, Prinssen M, et al. Two year
outcomes after conventional or endovascular repair of abdom
inal aortic aneurysms. N. Engl. J. Med. 352:2398 2405.
2. Dion YM, Griselli F, Douville Y, Langis P. Early and mid
term results of totally laparoscopic surgery for aortoiliac

686.e16 Case reports Annals of Vascular Surgery
disease: lessons learned. Surg. Laparosc. Endosc. Percutan.
Tech. 14:328 334.
3. Stadler P, Sebesta P, Vitasek P, Matous P, El Samman K. A
modified technique of transperitoneal direct approach for
totally laparoscopic aortoiliac surgery. Eur. J. Vasc. Endo
vasc. Surg. 32:266 269.
4. Kolvenbach R, Ceshire N, Pinte L, DaSilva L, Delinga O, Kas
per AS. Laparoscopy assisted aneurysm resection as a mini
mally invasive alternative in patients unsuitable for
endovascular surgery. J. Vasc. Surg. 34:216 221.
5. Stadler P, Dvoracek L, Vitasek P, Matous P. Is robotic surgery
appropriate for vascular procedures? Report of 100 aortoiliac
cases. Eur. J. Vasc. Endovasc. Surg. 36:401 404.
6. Kolvenbach R, Schwierz E, Wasilljew S, Miloud A, Puerschel
A, Pinter L. Total laparoscopically and robotically assisted
aortic aneurysm surgery: a critical evaluation. J. Vasc.
Surg. 39:771 776.
7. Stadler P, Matous P, Vitasek P, Spacek M. Robot assisted
aortoiliac reconstruction: a review of 30 cases. J. Vasc.
Surg. 44:915 919.
8. Wahlgren CM, Skelly C, Shalhav A, Bassiouny H. Hybrid lap
arorobotic debranching and endovascular repair of thora
coabdominal aortic aneurysm. Ann. Vasc. Surg. 22:285 289.
9. Dion YM, Gracia C. A new technique for laparoscopic aorto
bifemoral grafting in occlusive aortoiliac disease. J. Vasc.
Surg. 26:685 692.
10. Darling RC, Ozsvath BB, Chang PB, et al. The incidence,
natural history, and outcome of secondary intervention for
persistent collateral flow in the excluded abdominal aortic
aneurysm. J. Vasc. Surg. 30:968 976.