total cost of care - icsi.org · what defines total cost of care? • per member per month (pmpm)...
TRANSCRIPT
Total Cost of Care It’s Not Just For Primary Care Anymore
June 4, 2014 Scott R. Ketover, MD, AGAF
Dave Silvernale, CPA
What Defines Total Cost of Care?
• Per Member Per Month (pmpm) for attributed lives?
• Cost per visit / episode / treatment? • Volume utilization? • Conversion factor in fee for service? • Hospitalization / readmission / infection /
complication rates? • Out of pocket cost to the patient?

MNGI’s Participation in Total Cost of Care (TCOC)
1. Accountable Care Organizations 2. Measuring, Reporting and Paying for
Quality 3. Bundled Payment 4. Choosing Wisely Campaign 5. Engaging Specialists in TCOC

About Minnesota Gastroenterology, P.A.
• 68 Physicians – 20 Physician Extenders • 6 Core Offices in Twin Cities Metro Area including 5
Ambulatory Surgery Centers • Over 500 Employees • Single Specialty Gastroenterology including multiple
subspecialty programs • Fully integrated system with centralized billing, scheduling,
electronic health records, human resources, IT and quality functions
1) Multiple Accountable Care Organizations
• Allina Integrated Medical Network (AIM) • Fairview Health Network (FHN) • HealthEast Care Systems • Children’s Health Network • Specialists are involved with multiple networks –
system agnostic - while primary care is aligned with a single network (or none)
2) Measuring Reporting & Paying for Quality
Historical Definition of a “Good Physician” – Saw “a lot” of patients – Generated “a lot” of revenue – Had a “huge” backlog of patients – Had “many” charts on their desk – Kept a “busy” schedule – Had “very loyal” patients
Today’s “High Performing” Physician • Is available for an appointment within 7 days • Scores in the 80th percentile of CG-CAHPS for patient
satisfaction • Responds to every patient inquiry within 24 hours • Reports all test results within 24 hours • Completes all visit documentation and completes the billing
process before seeing the next patient • Publishes above the median scores on clinical measures
as developed by professional societies • Complies with at least 9 PQRS measures that demonstrate
quality

Today’s “High Performing” Physician
• Has the lowest severity adjusted pmpm Total Cost of Care based on attributed lives during the rolling 4 quarters ending 9 months ago.
• Utilizes the latest technology to communicate with patients, referring physicians, office staff and administration
• Has a sunny disposition and treats patients, referring MD’s, office staff and administration with the utmost respect and compassion in order to promote a healthy workplace
Why?
• To Demonstrate and Improve Quality
• To Achieve the Triple Aim – Improving the patient experience of care – Improving the health of populations; and – Reducing the per capita cost of health care
• To Reduce Total Cost of Care
How does MNGI motivate MD’s to embrace performance measurement?
• $’s and Data • In 2008 MNGI implemented a Physician Pay for
Performance Program (P4P) – Objectives
• Recognize and Reward Effort • Improve Quality • Differentiate ourselves in the market • Improve patient satisfaction and outcomes • Lower Total Cost of Care
– Pool of $’s available to physicians for exceeding benchmarks established by the group
2010 – Same as 2009
2008 – Biopsy results signed off
within 4 days – Timely submission of billing – Withdrawal time for
Colonoscopy
2009 – Biopsy results signed off within
4 days – Timely submission of billing – Withdrawal time for
Colonoscopy – E-mail read timely – Meeting attendance
MNGI P4P Through the Years
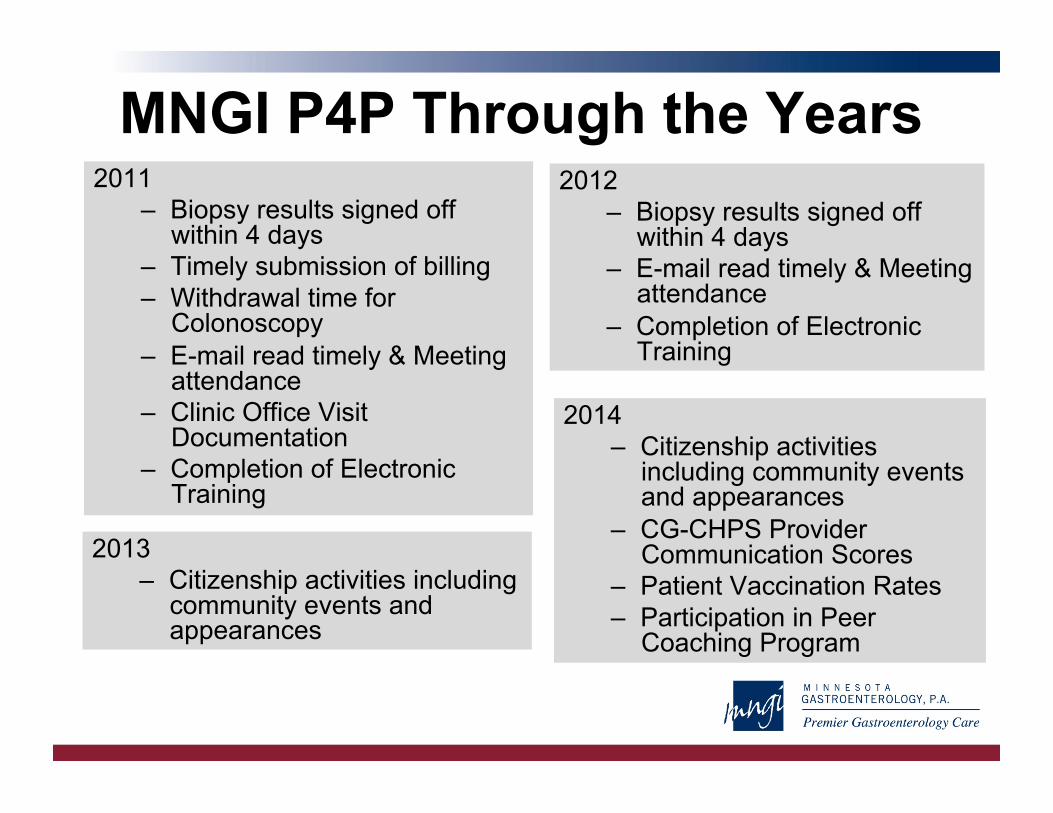
MNGI P4P Through the Years 2011
– Biopsy results signed off within 4 days
– Timely submission of billing – Withdrawal time for
Colonoscopy – E-mail read timely & Meeting
attendance – Clinic Office Visit
Documentation – Completion of Electronic
Training
2012 – Biopsy results signed off
within 4 days – E-mail read timely & Meeting
attendance – Completion of Electronic
Training
2014 – Citizenship activities
including community events and appearances
– CG-CHPS Provider Communication Scores
– Patient Vaccination Rates – Participation in Peer
Coaching Program
2013 – Citizenship activities including
community events and appearances
What Have We Learned? • If you can’t measure it you can’t improve it - Drucker
• Lot’s of discussion about what is quality • Does it matter if it is clinical quality or operational
efficiency or patient satisfaction/outcomes or TCOC?
• 90% of measures are met • Transparency of data was more effective than
monetary reward • Has it improved TCOC?

3) Bundled Payment Pay One Price Colonoscopy
How did we get here? – Material price variation based on place of service
and physician – Multiple bills from multiple providers and facilities
(up to 5) – Variation in insurance benefits and out of pocket
expense to patients based on screening benefits – Unwillingness by health plans to steer patients
and to administer payment and benefits outside of fee for service environment
©Minnesota Gastroenterology, PA

The Best Fit for Bundled Payment • Treatment or Procedure with a limited amount of variation in
resources used, but material variation in price. • Definable to a single encounter or series of encounters with
a recognized beginning and end • Relatively high volume of low cost services or a low volume
of high cost procedures • Elective/non urgent services that allow for direction of care • Alternative locations where the service can be performed
(Hospital/ASC/Clinic) • Potential use of mid level providers / group visits /
telemedicine / protocol driven care to reduce number of physician visits
©Minnesota Gastroenterology, PA

Who has the Incentive to Control Cost? • Health Plans? – actual claims passed through to
employers either by being self funded or increasing premiums the follow year
• Patients? – If cancer screenings require no out of pocket, why do
they care where they go? – Once the co-pay/coinsurance is paid and/or deductible
has been reached, care is “free” – Will the exchanges put control of the health care $’s with
the patient? • Federal or State Programs? – Zero sum game; just
reduce the conversion factor for all services • Employers - Currently the greatest incentive to control
costs ©Minnesota Gastroenterology, PA
Let’s Make a Deal! 1. Patients
– Looking for guaranteed out of pocket expense – Willingness to go to a recommended provider
2. Self Funded Employers – Looking to control costs by steering patients to high value – Looking to control costs by avoiding catastrophic events
3. Provider Groups – Having strong partnerships with all parties that are
involved in the delivery of the service – Willing to accept some risk and compete on the total
package
©Minnesota Gastroenterology, PA
MNGI’s Pay One Price Colonoscopy - What’s Included -
• Pre Procedure Assessment (scheduling intake) • Prep Kit • Professional (physician) charges • Facility (ASC) charges • Pathology Services (if required, prof & tech) • Sedation charges • 14 day professional service guarantee • Adherence to nationally recognized follow up surveillance
guidelines • Fixed Fee - One bill sent directly to the employer – No
intermediaries ©Minnesota Gastroenterology, PA

How Much Does a Colonoscopy Cost?
A) $10,000 B) $1,925 C) $1,950 D) $0 E) All of the Above

Same Procedure 3 Different Billing Scenarios

Initial Success / Future Plans • Pilot program with one employer group studied
29 patients with great results • Expanded to four self funded employers (two
with on site clinics) • Savings to employer is calculated to be roughly
$1,000 per procedure compared to their average cost
• In discussion with health plans – they are hearing about it in the press
• Collaborating with other specialists to provide a broader menu of bundles to employers
©Minnesota Gastroenterology, PA
Choosing Wisely American Gastroenterology Association (AGA)
1. For pharmacological treatment of patients with gastroesophageal reflux disease (GERD), long-term acid suppression therapy (proton pump inhibitors or histamine2 receptor antagonists) should be titrated to the lowest effective dose needed to achieve therapeutic goals.
2. Do not repeat colorectal cancer screening (by any method) for 10 years after a high-quality colonoscopy is negative in average-risk individuals.
3. Do not repeat colonoscopy for at least five years for patients who have one or two small (< 1 cm) adenomatous polyps, without high-grade dysplasia, completely removed via a high-quality colonoscopy.
4. For a patient who is diagnosed with Barrett’s esophagus, who has undergone a second endoscopy that confirms the absence of dysplasia on biopsy, a follow-up surveillance examination should not be performed in less than three years as per published guidelines.
5. For a patient with functional abdominal pain syndrome (as per ROME III criteria) computed tomography (CT) scans should not be repeated unless there is a major change in clinical findings or symptoms.
Choosing Wisely MNGI’s Initiatives
• Measuring our compliance with the recommendation for a 10 year follow up after a normal colonoscopy (AGA recommendation #2)
• Conducted a limited (50 patient) review of 5 year follow up, and evaluating how to measure our compliance with this measure
• Quality committee is evaluating how to increase information available to MNGI MDs and Staff to promote Choosing Wisely materials
5) Engaging Specialists in TCOC
• How many specialists know how they rank in TCOC against local and national peers?
• How many specialists know the top things they could do to lower their TCOC as defined by: – The Health Plan – The Referring MD – The Patient
Engaging Specialists in TCOC - Key Questions -
• Is the data available or possible to obtain at the specialist level?
• Will the health plans, government payers, or primary care physicians steer patients to practices with lower TCOC?
• Will employers design plan benefits to provide incentive for employees to chose based on TCOC?
• Will patients choose specialists based on TCOC?

Engaging Specialists in TCOC
• Role of the Health Plans – Report monthly to every practice a TCOC measure,
including results by provider and episode of treatment – Implement plan design that steers patients to providers
with lower TCOC. – Promote and pay for visits that don’t require face to face
physician patient encounters if it proves to lower the office visits needed
– Reward development and adherence of treatment protocols
Role of the Policy Makers
• Simplify the billing process by dramatically consolidating the # of codes (CPT) and reducing documentation requirement – Will ICD 10 improve TCOC?
• Promote bundled services – Stark and Anti-Kickback regulations promote the creation
of additional entities each of them battling for their share of the $’s
– 1 Visit = 1 Bill – 1 Treatment = 1 Cost
Role of the Health System
• Publish the TCOC for treatment by all specialties
• Provide incentives to primary MD’s to use the lowest cost and highest quality specialists rather than the “Health System First” approach
Role of the Patient
• Select a health plan based on that plans success for controlling cost (is that just the premium?)
• Utilize a primary care provider that promoted and published the lowest TCOC
• Ask to be referred to the doctor with has the best outcomes and lowest cost
• Demand quality, service, responsiveness, safe and proven outcomes
Role of the Specialist • Utilize Evidenced Based Medicine and proven best practice • Develop clinical pathways and protocols that involve
primary, inpatient and follow up care • Utilize programs that reduce 1:1 physician patient visits
– Telemedicine – E-consults – Group Teaching – E-tools
• Utilize the most cost effective location for care (site of service) – PCP – Ambulatory Surgery Center – Hospital

Additional ICSI Resources ICSI website: www.icsi.org
Choosing Wisely® Minnesota:http://consumerhealthchoices.org/choosing-wisely-minnesota/
Healthcare Affordability Page: https://www.icsi.org/health_initiatives/health_care_affordability/
Affordability Video: https://www.icsi.org/health_initiatives/health_care_affordability/ (Video courtesy of Twin Ci2es Public Television (tpt), The Bush Founda2on, and ICSI)
Email: [email protected]