top ten reasons god did not get tenured
DESCRIPTION
Top Ten Reasons God Did Not Get Tenured. 1. He had only one major publication. 2. It had no references. 3. It wasn't published in a refereed journal. 4. Some even doubt he wrote it himself. 5. It may be true that he created the world, but what has he done since then?. - PowerPoint PPT PresentationTRANSCRIPT
Top Ten Reasons God Did Not Get Tenured
1. He had only one major publication.
2. It had no references.
3. It wasn't published in a refereed journal.
4. Some even doubt he wrote it himself.
5. It may be true that he created the world, but what has he done since then?
Top Ten Reasons God Did Not Get Tenured
6. His cooperative efforts have been quite limited.
9. When one experiment went awry he tried to cover it up by drowning the subjects.
8. His office hours were infrequent and usually held on a mountaintop.
7. The scientific community has had a hard time replicating his results.
10. He never applied to the Ethics Board or IRB for permission to use human subjects.
Concussion in Sports-Neuropsychiatric Implications: Where we are, where we are going
1st International Conference on Translational MedicineNov. 3, 2010 Canberra, Australia
David BaronDirector, Global Center for Exercise, Psychiatry and SportUSCWPA
Goals and Objectives
Discuss Translational Process
Over view of Concussion in Sports
Translational Process
• Original concept– Bench to bedside
• Expanded to public health– Culture change
• Preclinical scientists> clinicians>policy makers(health and governmental)>educators
• Avoid State of the Shelf science– Blind man and the elephant phenomena
Concussion: Introduction
• An estimated 1.6- 3.8 million sports-related concussions occur annually in the United States
• 86,000- 134,000 of these concussions are sustained by high school students
• Acutely, concussions can cause a broad range of psychiatric defects, including depression, anxiety, and cognitive impairment
Concussion: Introduction
• Long term consequences of multiple concussions or multiple subconcussive blows are potentially more serious, with the deposition of tau deposits throughout the brain, and resultant early onset dementia and movement disorders
Definition of Concussion (International Consensus)
• A complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces
• Caused by direct blow to the head, face, neck, or elsewhere on the body with “impulsive” force transmitted to the head.
Definition of Concussion (International Consensus)
• Often rapid onset
• Often short-term impairment of neurologic function that resolves spontaneously
• May result in neuropathological changes, but acute clinical symptoms reflect functional disturbance rather than structural
Definition of Concussion (International Consensus)
• Results in graded set of clinical symptoms
• May or may not involve loss of consciousness
• Resolution of clinical and cognitive symptoms typically follows sequential course
Definition of Concussion (International Consensus)
• Small percentage of cases have prolonged post-concussive symptoms (10-20%)
• No abnormality found on standard structural neuroimaging (CT or standard MRI)
Classification of Concussion• At least 25 grading systems currently
in use
• Aimed at characterizing concussion severity and prognosis– And subsequently return to play
decisions
• No scientific agreement on which is best

International Conferences on Concussion in Sport- Issues addressed
• Definition• Classification• Evaluation• Management• Modifying Factors
– Factors that may alter evaluation and management
– Factors that predict prolonged or persistent symptoms
Is There any Consensus on Concussion?• 3 separate conferences in last 9
years aimed at reaching consensus of understanding and management of sports concussions
• Consensus decisions reached by votes from a panel of international concussion experts (Concussion in Sports Group or CISG)
Is There any Consensus on Concussion?
– 1st International Conference on Concussion in Sport, Vienna 2001
– 2nd International Conference on Concussion in Sport, Prague 2004
– 3rd International Conference on Concussion in Sport held in Zurich, November 2008
Classification of Concussion
• The international Concussion in Sports Group (CISG) does not endorse any single grading system
• Concussion severity can only be determined in retrospect:– After all concussion symptoms clear– After neurological examination normal– After cognitive function returns to
baseline

Concussion Laws
Concussion Laws
• In October 2007, under pressure from congress and media NFL made dramatic changes in its handling of concussion– For the first time acknowledged that
concussions lead to long-term problems
– Return to play decisions made only by a independent neurologists
– Resignation of NFL Concussion Committee’s 2 co-chairmen
Concussion Laws
• In May 2009, the state of Washington passed a new bill called the Lystedt Law– Requires any youth showing signs of a
concussion be examined and cleared by a licensed health care provider before being allowed to return to play
Concussion Laws
– Named after Zackery Lystedt, a young athlete permanently disabled after sustaining a concussion in 2006, and prematurely returning to the game
Chronic Traumatic Encephalopathy
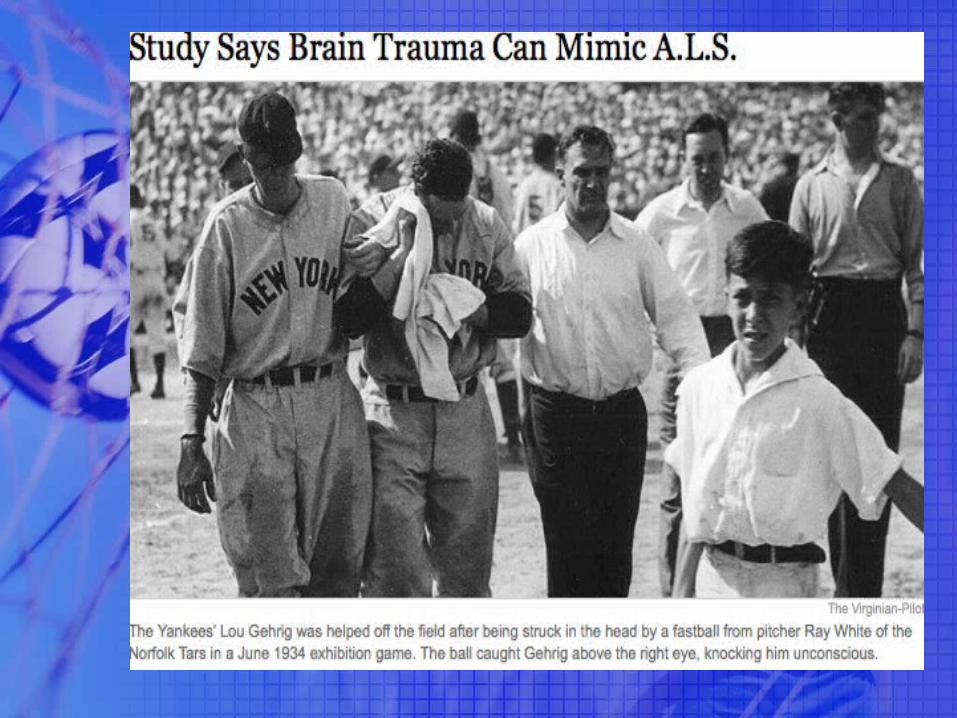
ALS or CTE?
• Doctors at Veterans Affairs Medical Center in Bedford, MA and Boston University School of Medicine recently discovered by autopsy that 2 NFL players and 1 boxer diagnosed with ALS really had a variant of CTE
• Similar findings in deceased soldiers previously diagnosed with ALS
Chronic Traumatic Encephalopathy (CTE)• First described by Dr. Harrison
Stanford Martland, a pathologist, in 1928 (“punch drunk syndrome”)
• Later called “Dementia Pugilistica”, and more recently, “Chronic Traumatic Encephalopathy”
• An estimated 17% of retired professional boxers will develop chronic traumatic encephalopathy
Chronic Traumatic Encephalopathy• Highest incidence in boxers and NFL
linemen, although cases have been described in a soccer player, wrestler, epileptics, head bangers, and domestic abuse victims
Chronic Traumatic Encephalopathy
• May result from single concussion, although more frequently results from repeated concussions or subconcussive blows
• Can present upon retirement or years later
Chronic Traumatic Encephalopathy
• Common presenting symptoms include:– memory loss– irritability– outbursts of aggressive or violent behavior– confusion– speech abnormalities– cognitive decline/dementia– gait abnormalities
Chronic Traumatic Encephalopathy• Often times there is a mood
disturbance as well:– depression (often with suicidal
ideation)– bipolarity
• Often accompanied by psychosis in the form of paranoid ideation
• Often times culminates in suicidal behavior
Chronic Traumatic Encephalopathy• Microscopic Pathology: neuronal loss
and gliosis with Tau deposition• Hippocampus, entorhinal cortex→ memory
disturbances • Amygdala→ mood disorders• Frontal and Temporal cortices→
dysexecutive symptoms, cognitive deficits• Substantia nigra→ parkinsonism• Brainstem white matter tracts (including
cerebellar tracts)→ Ataxia, gait abnormalities
Chronic Traumatic Encephalopathy• Gross brain pathology (may or may
not have)– Reduction in brain weight– Enlargement of lateral and 3rd ventricles– Thinning of Corpus callosum– Cavum septum pellucidum with
fenestrations– Scarring and neuronal loss of cerebellar
tonsils
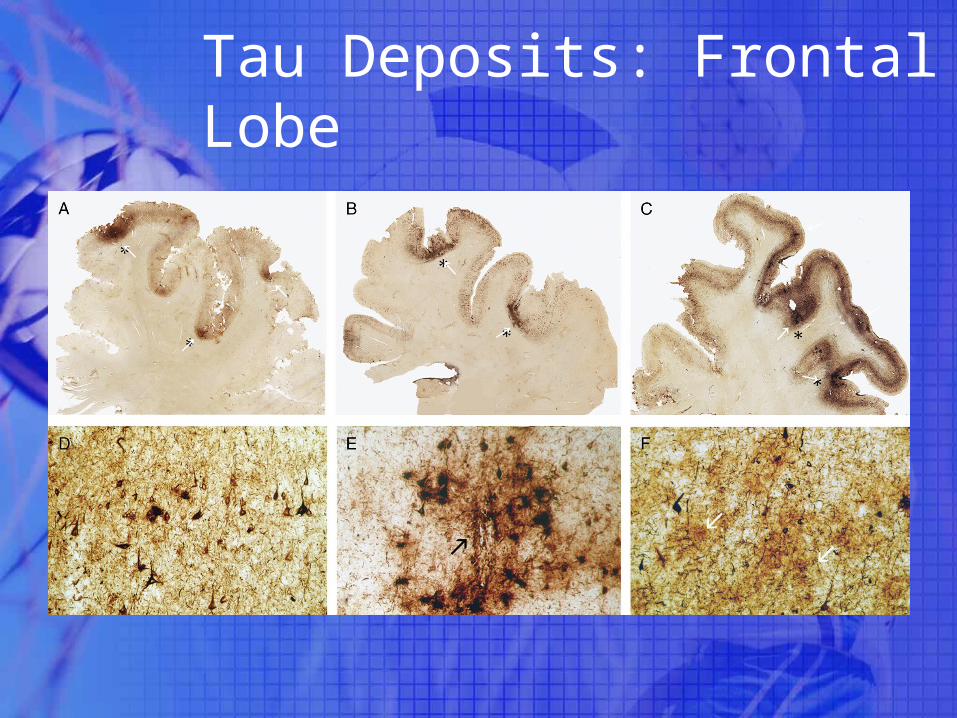
Tau Deposits: Frontal Lobe
↙
↙
↙
↙
↙
↙
↙
↙
↙
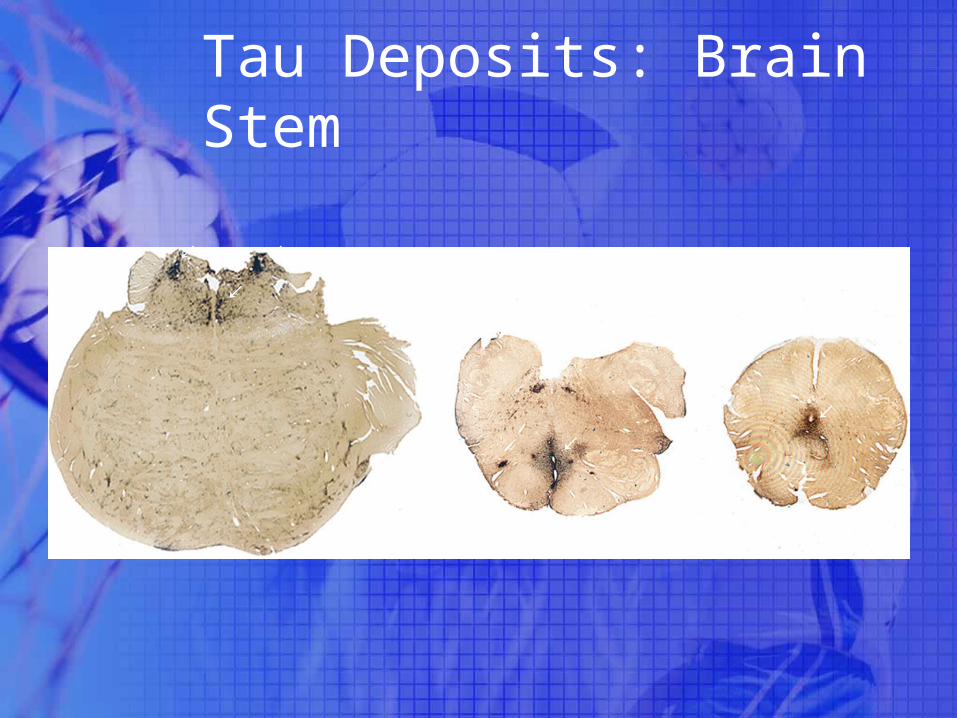
Tau Deposits: Brain Stem
↙ ↙
↙
↙
↙
↙
Pathophysiology
• No existing animal or experimental models (not fully elucidated)
• Impaired neurotransmission– Excessive release of excitatory
neurotransmitter glutamate• Neurotoxicity• Opening of ion channels, leading to
dysregulation of ions in the brain
Pathophysiology
• Dysregulation of ions– Causes strain on ion pumps
• Leads to increased energy demand
• Hypermetabolic state– Larger than normal amounts of glucose
consumed
• Reduction of cerebral blood flow– Combined with hypermetabolic state,
results in “energy crisis”

Translational issues
• Need better longitudinal data on consequences of multiple sub-clinical concussions
• Need to change culture in collision sports-acknowledge the long term risks
• Data needed from pitch to bench