to view the slides - american pharmacists association
TRANSCRIPT

Sticking With What Works: Helping Patients Adhere to
Medications
Daniel R. Touchette, PharmD, MA
Jessica Tilton, PharmD, BCACP University of Illinois at Chicago
College of Pharmacy
March 12, 2012

2 2
Supported by independent
educational grants from
Abbott Laboratories and Merck.

3 3
The American Pharmacists Association is accredited by the
Accreditation Council for Pharmacy Education as a provider of
continuing pharmacy education.
This activity, Sticking With What Works: Helping Patients Adhere to
Medications, is approved for 2.0 hours of CPE credit (0.2 CEUs). The ACPE
Universal Activity Number assigned by the accredited provider is 202-000-12-082-
H04-P for pharmacists and 202-000-12-082-H04-T for technicians. If you
participated in the live seminar of the same title held on Monday March 12, 2012 at
the APhA Annual Meeting and Exposition in New Orleans, LA you are NOT eligible
to receive CPE credit for this activity.
To obtain CPE credit for this activity, participants must view the slides and listen to
the audio for the activity then complete the online post test and evaluation by March
12, 2015. To complete the online post test and evaluation, participants must have a
valid Pharmacist.com user name and password. A Statement of Credit will be
automatically be generated upon achieving these requirements.
NOTE: no voucher code is needed when completing the online version of this
course

4 4
Disclosures
• Dr. Touchette has received grant funding from Medco Health
Solutions for research projects related to improving medication
adherence
• Dr. Tilton has received consulting fees from Medco Health
Solutions for presentations related to improving medication
adherence
5 5
Learning Objectives
• At the completion of this program, participants will be
able to:
– Describe causes and effects of medication nonadherence.
– Identify tools and strategies for assessing medication
adherence.
– Explain the relationship between medication adherence and
health care quality measures for the prevention and
treatment of diseases.
– Discuss strategies to overcome barriers to medication
adherence for patients including motivational interviewing.

6 6
Please note your answers to the self-assessment questions on a piece of
paper. The questions and answers will be reviewed at the end of the
presentation.
After 12 months of therapy, what
proportion of days do patients taking
lipid lowering medications have those
medications “on hand” (i.e. have
enough days supplied to cover)?
audience response
A. 15% 2
B. 30% 11
C. 60% 10
D. 80% 0

7 7
Which of the following is not a
tool for assessing medication
adherence?
audience response
A. Med Take 3
B. TIMER 6
C. Morisky 8-item index 5
D. AIMS 10

8 8
Assuming each fill in the figure
below is for 30 days, which of the
following is the correct calculation
for medication possession ratio?
audience response
A. 120 / 180 = 67% 9
B. 60 / 130 = 46% 1
C. 90 / 130 = 69% 6
D. 90 / 180 = 50%

9 9
Which of the following best
describes motivational
interviewing?
audience response
A. It is used to persuade patients to
implement healthful behaviors 3
B. It is a “tough love” approach
to behavior change 0
C. It is designed to stimulate a
patient’s intrinsic motivation to change 23

10 10
Which of the following
statements is false?
audience response
A. Patients’ adherence can be measure
by either proportion of days covered or
medication possession ratio 6
B. Motivational interviewing is most
useful when a patient is in the “action”
stage of change 17
C. Patients with asymptomatic
conditions are less likely to adhere
to their medications 3
D. Poor adherence is estimated to
result in $100 billion in avoidable
hospitalization costs 1

11 11
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer

12 12
Drugs don’t work in patients who don’t take them.
C. Everett Koop, M.D.

13 13
Adherence vs. Persistence
• Medication Adherence (Compliance):
– The extent to which patients take medications as
prescribed by their health care providers
– Compliance suggests patient passively following
directions
– Adherence implies an agreement
• Persistence
– Time of continuous therapy, demarcated by the time from
initiation to discontinuation of therapy
Osterberg et al. N Engl J Med 2005; 353: 487-97.
Cramer et al. Value Health 2007; 11: 44-47.
14 14
Patient Adherence to
Medications
• Poor adherence and persistence are serious issues
in healthcare
– Assessing lipid lowering medications in a Medicare cohort
(n=34,501)
• Patients had medications “on hand” (MPR) for only
60% of the time in the first year of therapy
• 34-39% had medications “on hand” for more than 80%
of the time (i.e. adherent)
• 29% of patients failed to fill prescriptions after 3
months
– Drugs with bothersome side effects may be filled less
frequently or discontinued more often
– Cost: $100 billion on avoidable hospitalizations
Benner JS et al. JAMA. 2002;288(4):455-61.
Osterberg et al. N Engl J Med 2005; 353: 487-97.

15 15
Clinical Impact of Poor
Adherence
Sokol MC, et al. Med Care. 2005;43(6):521-30.

16 16
Economic Impact of Poor
Adherence: Medication Costs
Sokol MC, et al. Med Care. 2005;43(6):521-30.

17 17
Economic Impact of Poor
Adherence: Total Costs
Sokol MC, et al. Med Care. 2005;43(6):521-30.

18 18
• Analysis of 1705 Medicaid patients with type 2
diabetes
– 37% of patients were adherent (MPR > 80%)
– Adherent patients had
• Lower risk for hospitalizations (OR = 0.80)
• Lower risk for ED visit (OR = 0.71)
• 15% lower total medical costs
• 12% lower hyperlipidemia medical costs
Predictors of Higher
Healthcare Costs
Wu et al. Ann Pharmacother. 2011 45(3): 342-349.

19 19
Work-related Economic Impact
of Poor Adherence
• Retrospective, observational study (n=2112)
• New episode of treatment with
antidepressant
– Characterized as “adherent” or “non-adherent”
according to HEDIS criteria
– Acute phase: 84/114 days
– Continuation phase: 180/231 days
Burton WN et al. Am J Manag Care. 2007;13(2):105-12.

20 20
Work-related Economic Impact
of Adherence
Burton WN et al. Am J Manag Care. 2007;13(2):105-12.
21 21
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer

22 22
Identified Predictors of
Nonadherence
• Presence of barriers to care or medications
• Cost of medication, copayment
• Treatment complexity
• Psychological problems / depression
• Cognitive impairment
• Asymptomatic disease
• Inadequate follow-up / discharge planning
• Side effects of medication
• Lack of belief in treatment benefit
• Lack of insight into illness
• Poor provider-patient relationship
• Missed appointments
McDonald HP et al. JAMA. 2002;288(22):2868-79.
Gherman A et al. Diabetes Educat. 2011; 37(3): 392-408.
Gellad WF et al. Am J Geriatr Pharmacother. 2011; 9: 11-23.

23 23
Impact of Medication Choice
on Adherence
0
0.5
1
1.5
2
2.5
3
Multiple Thiazides Betablock
Other CCB ACEInhib
RR
fo
r A
dh
eren
ce
Monane. AJH 1997;38(2):303-12.
24 24
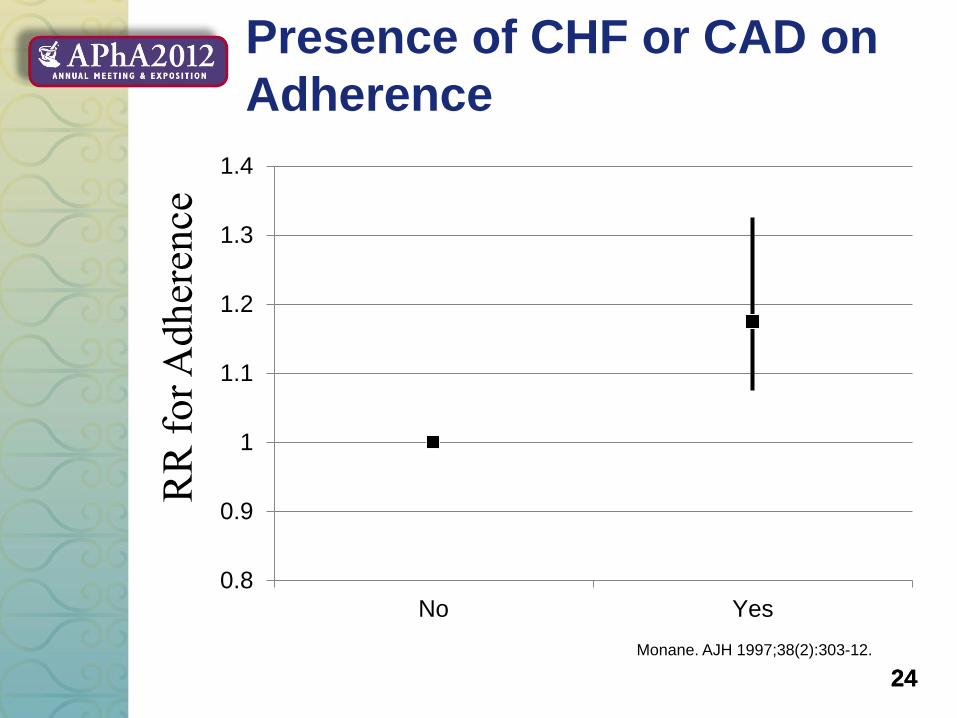
Presence of CHF or CAD on
Adherence
0.8
0.9
1
1.1
1.2
1.3
1.4
No Yes
RR
fo
r A
dh
eren
ce
Monane. AJH 1997;38(2):303-12.

25 25
Impact of Number of Pharmacies
Used on Adherence
0
0.2
0.4
0.6
0.8
1
1.2
One More than one
RR
fo
r A
dh
eren
ce
Monane. AJH 1997;38(2):303-12.

26 26
Reasons for Poor Medication
Adherence
External:
System and Health
Barriers
Cognitive
Factors
Internal:
Behavioral Factors
and Beliefs
Touchette. Pharmacotherapy 2010 30(5): 425-427.
27 27
System and Health Related
Barriers
• Lack of coverage
• Complicated drug coverage
• High out-of-pocket costs
• Presence of depression
• Complicated regimen
• Drug adverse events
• Complicated or poorly
worded directions
Touchette. Pharmacotherapy 2010 30(5): 425-427.

28 28
Behavioral Factors and Beliefs
Ways people
evaluate
drug therapy
Drug taking
Drug therapy
and identity
Touchette. Pharmacotherapy 2010 30(5): 425-427.

29 29
Behavioral Factors and Beliefs
• Social support and interaction
• Busy schedule
• Poor patient-provider
relationship
• Beliefs about condition
• Beliefs about Western
medicine
• Beliefs about specific
medicine
Touchette. Pharmacotherapy 2010 30(5): 425-427.

30 30
Cognitive Factors
• Poor memory
• Difficulty understanding
directions / health literacy
• Ability to follow directions /
self-efficacy
• Physical limitations
Touchette. Pharmacotherapy 2010 30(5): 425-427.

31 31
Patient Adherence to
Medications
• Poor adherence and persistence are impacted by
healthcare beliefs
– 4076 South Carolina Medicaid recipients 18 yo or over
• Overall, MPR was approximately 58%
– White patients: 61%
– Black patients: 55%
$0
$500
$1,000
$1,500
$2,000
$2,500
Mean DrugCosts
MeanHospitalCosts
Black Patients
White Patients
Dickson et al. Ethnic Dis 2008; 18: 204-209.

32 32
• Black patients more likely to perceive high blood
pressure as being “very serious” or “serious”
– So why lower adherence?
• Possible reasons for differences in adherence are
– Perception that medications are harmful and ineffective
• Non-Caucasian patients receive lower-cost
medications
• May experience more side effects
– Belief that hypertension and high blood pressure are
different disease models
– “Scare tactics” don’t work
– Patient-provider trust may not be established
– Increased comorbidities
Patient Adherence to
Medications
Bosworth et al. Am J Med 2006; 119: 70.e9-70.e15.
Ogedegbe et al. Ethn Dis 2004; 14: 3 -12.
Lukoschek. J Health Care Poor Underserved 2003; 14: 566-587.

33 33
Assessing Adherence:
Methods
• Pharmacy records and claims data
• Patient interviews
– Patient estimates of adherence
• Pill counts
• Biological assays
• Weight of topical medications
• Electronic monitoring
34 34
Assessing Adherence:
Tools
• Raehl’s Med Take Interview
• TIMER DRP identification tool
• Morisky adherence index

35 35
MedTake
• Patient interview assessing:
– Demographics
– Medical history
– Medication history
– Current medication review
• Prescription
– Pillboxes or calendar boxes
– Notes from physician regarding changes to dosing
or directions (e.g. warfarin)
• OTC
• Herbal
– Recent medication changes
– Patients asked to open container and simulate taking the
drug
Raehl. Pharmacotherapy 2002; 22(10): 1239-48.

36 36
MedTake
Drug
Name,
dose, SIG
Subject’s
description
of how
he/she takes
the drug
Dose
(1, 0)
Indication
(1, 0)
Food, water
coingestion
(1, 0)
Regimen
(1, 0)
Score
(=total / 4)
Metoprolol
50mg
1 twice
daily
50mg
1 pt
No idea
0 pts
Water
1 pt
1 at 9am
1 at 6pm
1 pt
3 pts
(75%)
1 = correct, 0 = incorrect Raehl. Pharmacotherapy 2002; 22(10): 1239-48.

37 37
TIMER
• Designed for identifying and assessing DRPs
• Regarding adherence:
– Four questions
– Three recommendations
• Questions are worded in non-threatening way
– Give patient “permission” to have less than perfect
adherence
– Patient more likely to be open and honest

38 38
TIMER
1. Everyone forgets to take their medicines. How
often does this happen to you?
2. Everyone says that they miss a dose of their
medication or adjust it to suit their own needs.
How often do you do this? Why?
3. Has your physician told you to change how you
take any of your medications?
4. Has your physician told you to stop taking any of
your medications?
Lee et al. Am J Pharm Ed 2009; 73(3): Article 52.
39 39
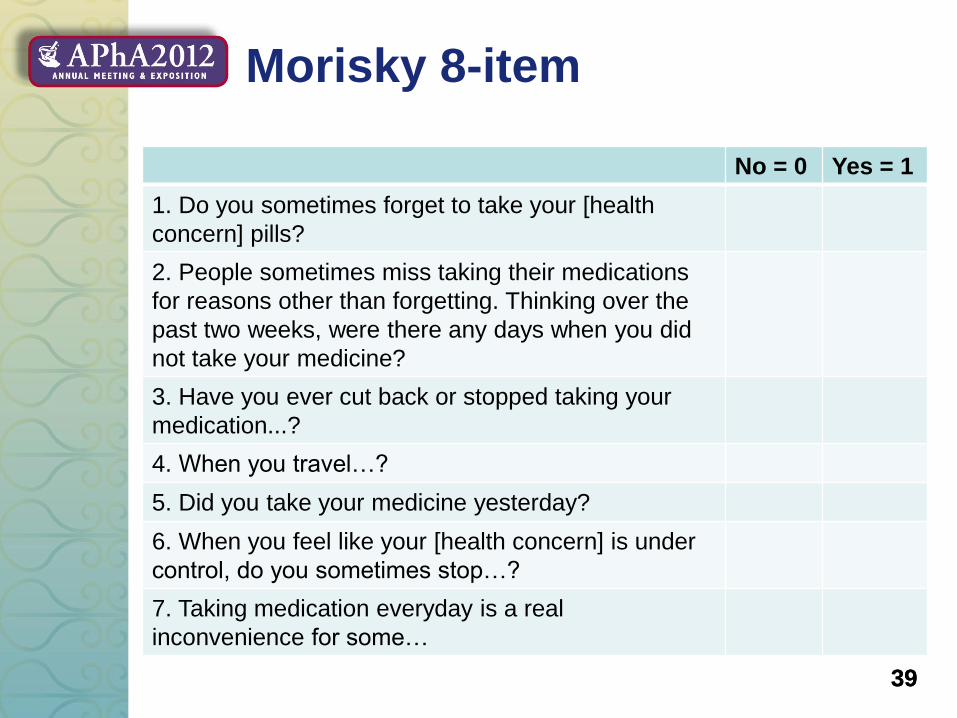
Morisky 8-item
No = 0 Yes = 1
1. Do you sometimes forget to take your [health
concern] pills?
2. People sometimes miss taking their medications
for reasons other than forgetting. Thinking over the
past two weeks, were there any days when you did
not take your medicine?
3. Have you ever cut back or stopped taking your
medication...?
4. When you travel…?
5. Did you take your medicine yesterday?
6. When you feel like your [health concern] is under
control, do you sometimes stop…?
7. Taking medication everyday is a real
inconvenience for some…

40 40
Morisky 8-item
8. How often do you have difficulty remembering to
take all your medications?
Never/rarely
Once in a while
Sometimes
Usually
All the time
Morisky et al. J Clin Hypertens 2008; 10(5):348-354

41 41
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer
42 42
Addressing Medication
Adherence
Number one predictor of a patient’s medication adherence is if they believe they have a healthcare provider that
cares about them
-Bruce Berger, PhD

43 43
Tools and Strategies for
Addressing Adherence Issues
• Cognitive Factors • Poor memory
• Difficulty understanding directions / health literacy
• Ability to follow directions / self-efficacy
• Physical limitations
• Possible Adherence Solutions – Count out doses in advance
– Keep a checklist
– Use a beeping alarm
– Put dosage time in daily planner
– Arrange for privacy
– Keep a diary
– Leave notes and reminders
– Establish and use support network

44 44
Tools and Strategies for
Addressing Adherence Issues
• System and Health • Lack of coverage
• Complicated drug coverage
• High out-of-pocket costs
• Presence of depression
• Complicated regimen
• Drug adverse events
• Complicated or poorly worded directions
• Possible Adherence Solutions • Patient assistance programs
• Sample
• $4 generics
• Talking with doctor
• Discuss with patient what is will work for them
45 45
Tools and Strategies for
Addressing Adherence Issues
• Behavioral Factors and Beliefs • Social support and interaction
• Busy schedule
• Beliefs about condition
• Beliefs about Western medicine
• Beliefs about specific medicine
• Poor patient-provider relationship
• Possible Adherence Solutions • Educate family and caregivers
• Work with patient’s life to help identify a regimen for them
to remember
• Educate the patient-verbal and written
• Motivational Interviewing

46 46
They speak of my drinking, but never of my thirst.
-Scottish Proverb

47 47
Addressing Adherence
• Typical Challenges
– Communication is NOT patient-centered
– The pharmacist is trying to save the patient
– Labeling the patient
– Dictate behavior change
• Build a pharmacist-patient relationship
• Use Motivational Interviewing (MI)

48 48
What is Motivational
Interviewing?
Patient-centered, evidenced-based
counseling approach that is
specifically designed to enhance
motivation to change among
patients not ready to change
Miller, W.R., Rollnick, S., Motivational Interviewing , 2nd
edition. NY: The Guilford Press, 2002.

49 49
Why use Motivational
Interviewing?
• Understand patient’s frame of reference
• Express acceptance & affirmation
– No face loss
• Spirit is “unconditional acceptance”
– Love, caring and collaboration
• Monitor patient's degree of readiness to
change
• Affirm patient's freedom of choice & self-
direction Rollnick, Mason, Butler. Health Behavior
Change. A Guide for Practitioners. Churchill
Livingstone: Elsevier, 1999. Print
50 50
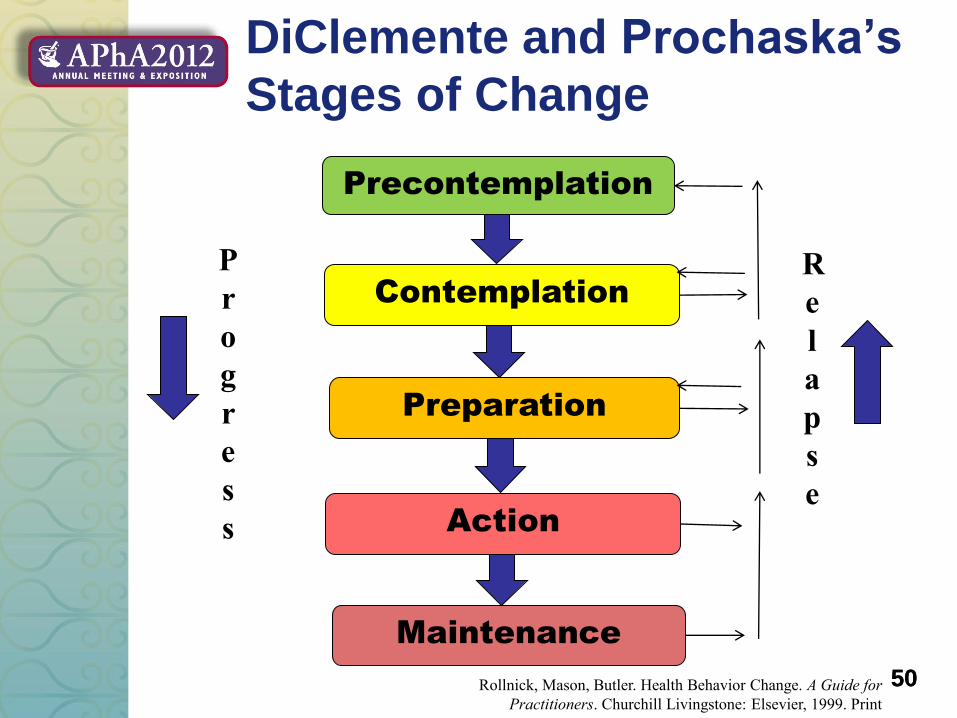
DiClemente and Prochaska’s
Stages of Change
Precontemplation
Contemplation
Preparation
Action
Maintenance
P
r
o
g
r
e
s
s
R
e
l
a
p
s
e
Rollnick, Mason, Butler. Health Behavior Change. A Guide for
Practitioners. Churchill Livingstone: Elsevier, 1999. Print

51 51
Motivational Interviewing
Principles
• Decisional Balance – PharmD’s job is to tell the patient the risks of not changing
their behavior…not to “fix” them.
– Tilt balance towards favor of benefit by asking how the risks would affect their life.
– PharmD can inform them, but not make them change.
Rollnick, Mason, Butler. Health Behavior Change. A
Guide for Practitioners. Churchill Livingstone: Elsevier,
1999. Print

52 52
Motivational Interviewing
Principles
• Resistance
– 2 types
• Issue: “I’m not ready to take my insulin, I’m fine.”
• Relational: “I told you; I’m just not ready to take my
insulin!”
– Pharmacist’s role is to reduce resistance by
rolling with it….explore don’t explain
– DO NOT PERSUADE!
Rollnick, Mason, Butler. Health Behavior
Change. A Guide for Practitioners. Churchill
Livingstone: Elsevier, 1999. Print

53 53
Motivational Interviewing
Principles
• Do you dance or wrestle with your
patients?
Rollnick and Miller, 2001
54 54
Motivational Interviewing
Principles
• Express empathy
– Skillful, reflective listening
– Ambivalence is normal
Rollnick, Mason, Butler. Health Behavior
Change. A Guide for Practitioners. Churchill
Livingstone: Elsevier, 1999. Print

55 55
Motivational Interviewing
Principles
• Support self-efficacy
– The patient’s belief in the possibility of change is an
important motivator
– The pharmacist’s belief in the patient’s ability to change
becomes a self-fulfilling prophecy
Rollnick, Mason, Butler. Health Behavior
Change. A Guide for Practitioners.
Churchill Livingstone: Elsevier, 1999. Print
56 56
Motivational Interviewing
Principles
• Develop discrepancy
– This should come from the patient rather than the
pharmacist
– Change is motivated by a perceived discrepancy between
the patient’s current behavior and their personal goals and
values
Rollnick, Mason, Butler. Health Behavior Change. A
Guide for Practitioners. Churchill Livingstone:
Elsevier, 1999. Print

57 57
Motivational Interviewing
Tools
• What if scenarios – “What would it look like if….”
• The envelope – “What would the message inside this envelope have to
say for you to….”
• Insurance card – “Can I tell you what concerns me?”

58 58
Motivational Interviewing
Skills
• Get permission
• Open-ended questions
• Reflective listening
• Summarizing

59 59
MI Flow Basics
• Develop a relationship – Create a rapport
– Develop an atmosphere that is safe for the patient
• Non-defensive
• Can talk openly and honestly without being judged
– This will help make the patient open their thinking
Rollnick, Mason, Butler. Health Behavior Change.
A Guide for Practitioners. Churchill Livingstone:
Elsevier, 1999. Print

60 60
MI Flow Basics
• Develop a relationship – Express empathy
• Skillful, reflective listening
– Support self-efficacy
• The patient’s belief in the possibility of change is an important motivator
• The patient is responsible for choosing to change and carry it out
• The pharmacist’s belief in the patient’s ability to change becomes a self-fulfilling prophecy
Rollnick, Mason, Butler. Health Behavior
Change. A Guide for Practitioners. Churchill
Livingstone: Elsevier, 1999. Print

61 61
MI Flow Basics
• Evaluate the patient’s reasoning
– Recognize the patient’s core issues
– Reflect and empathize with core issues
– Examine the reasoning behind each issue
– Address the weakness in each point of faulty
reasoning
– Encourage the pt to draw a new conclusion
Rollnick, Mason, Butler. Health Behavior Change. A
Guide for Practitioners. Churchill Livingstone:
Elsevier, 1999. Print

62 62
MI Flow Basics
• Use reflective listening to give clear evidence that
you have heard the patient’s issue
– Feeling + content + reasons
– Avoid: “I understand that….”

63 63
MI Flow Basics
Reflective listening to identify the core issue:
Pt: “It’s really hard to remember take my medication every morning. I am too busy trying to get the kids and my husband dressed and fed before they leave for the day.”
PharmD: “It sounds like your mornings can be really hectic and stressful, which does allow time for you to take your medication.”
64 64
MI Flow Basics
Reflective Listening to support self-efficacy and empathy:
Pt: “I’m shocked that my lipids didn’t come down a lot more b/c I’ve lost weight…..I’ve been really watching what I’m eating.”
PharmD: “It’s great that you’ve been able to lose weight. Tell me how you’ve managed to do that.”

65 65
MI Flow Basics
• Need to make sure there is a transition from
evaluating their reasoning to informing the patient.
• Patients can misunderstand questions as
accusatory
• Need to create a direct connection back to the
shared understanding of the patient’s issue.

66 66
MI Flow Basics
Example of transition:
Pt: “I don’t think I need to take my Lipitor anymore, my cholesterol is fine and I’ve heard it can harm my liver and cause muscle pain.”
PharmD: “It sounds like you’re wondering whether you still need to take your Lipitor because your cholesterol has been controlled and the medication could cause side effects. In order for me to address your concern about the medicine, may I ask you some questions?”
Pt: Sure.

67 67
MI Flow Basics
• Explore the patient’s reasoning
• Identify influences in the patient’s line of reasoning
68 68
MI Flow Basics
• Address line of reasoning – Add new information
– Correct misinformation
– Address understated statements
• “I feel fine.”
– Personalize benefits/losses
– Create discrepancies
– “Insurance Card”

69 69
MI Flow Basics
• Have patient make a conclusion
– Don’t pressure the patient
• “That’s why we want you to…”
– Implying only one conclusion
• “Would you be willing to try…”
– This is a yes or no question
• “What are your thoughts about this information?”
• “How do think this information applies to you?”

70 70
MI Flow Basics
• Have patient make a conclusion
– Goal is to avoid creating relational resistance
– Want to assist the patient in make their own argument for
change
– If they aren’t ready, back off
71 71
MI Flow Basics
• Gauge willingness, readiness and confidence to change
– Reinforce change talk and any changed conclusions
– Examine what the patient is willing and ready to do
Example
PharmD: “Cutting back on your fruit juice intake will help reduce your blood sugars. How do you think you can go about cutting back?”
Rollnick, Mason, Butler. Health Behavior
Change. A Guide for Practitioners. Churchill
Livingstone: Elsevier, 1999. Print

72 72
MI Flow Basics
• Close the deal
– Summarize patient’s line of reasoning
– Express desire to help the patient in reach their
goal
– Acknowledge self-efficacy of any change
suggested by the patient
– Identify future interactions with the patient

73 73
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer

74 74
Case Video

75 75
Case
MB is a 49 year old Caucasian female for who you
are performing a comprehensive medication review.
PMH:
DM
HTN
Medications:
• Metformin 1000 mg, 1 tab po twice daily.
• Aspirin 81 mg, 1 tab po daily.
• Carvedilol 25 mg, 1 tab po twice daily.
• Enalapril 20 mg, 1 tab po twice daily.
• Amlodipine 10 mg, 1 tab po daily.
• Hydrochlorothiazide 25 mg, 1 tab po daily.

76 76
Case
Upon further review and assessing how she is taking her medication, the patient states that she hasn’t filled carvedilol, enalapril, amlodipine, or hydrochlorothiazide for over two months.
She states that her life has been very stressful, taking care of 3 teenagers. She also states that she isn’t able to afford all of her medication and has been taking them only once in a while but has now run out.
You ask permission to discuss her adherence issues.

77 77
Case
• What is the patient’s reason(s) for nonadherence to
her medications?
– Stress and cost
• What questions should we ask about her
nonadherence?
– Tell me your understanding about why you are taking
these medications?
– Tell me what you know about HTN and DM?
– How do you feel when you don’t take your medications
and how do you feel when you do take all of your
medications?
– What are your healthcare goals?
78 78
Case
• Patient’s responses
– Tell me your understanding about why you are taking
these medications?
• “For high blood pressure and diabetes.”
– Tell me what you know about HTN and DM?
• “I don’t know, I feel fine….my doctor said they can
cause bad things to happen if I don’t take my
medication.”

79 79
Case
• Patient’s responses continued
– How do you feel when you don’t take your medications
and how do you feel when you do take all of your
medications?
• “I feel fine if I don’t take my medications, but get really
dizzy when I take all of them.”
– What are your healthcare goals?
• “To feel good and not have the bad things happen
because of my diabetes and blood pressure.”

80 80
Case
• What additional barriers did we discover about her
nonadherence?
– Lack of belief in treatment benefit
– Lack of insight into illness
– Side effects - dizziness

81 81
Case
• What tools can we use to address her adherence?
– Motivational interviewing
• Assess motivation to change – probably preparation to
action phase
– Education
• About diabetes and hypertension
• About medications
– Establish and use support network, if possible
– Evaluate how much she can afford each month
– Involve her physician
• Evaluate if all medications are necessary if she takes them – dizziness
– Follow-up!

82 82
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer

83 83
Chronic Care Model
Community Health Systems
Self
Management
Support
Delivery
System
Design
Decision
Support
Clinical
Information
Improved Outcomes
Informed,
Activated
Patient
Prepared,
Proactive
Practice Team
Adapted from http://www.improvingchroniccare.org/index.php?p=the_chronic_care_model&s=2.

84 84
Chronic Care Model
Community Health Systems
Self
Management
Support
Delivery
System
Design
Decision
Support
Clinical
Information
Improved Outcomes
Informed,
Activated
Patient
Prepared,
Proactive
Practice Team
85 85
Self Management Support
• Motivational interviewing
• Information / education
– Medication education
– Disease state educator
• Improve patient self-efficacy

86 86
Delivery System Design
• Help patient navigate complex health system
– Follow-up liaison - continuity of care
– Ensure medications can be obtained by the patient based
on cost and/or formulary
– Prior approvals
• Suggest improvements to work flow
– Create collaborative agreements or standing orders
• Break down barriers to patients receiving care
– Be an active part of ACO/Medical Home

87 87
Decision Support
• General Provider Education
– Keep nurses and physicians up to date on medication
literature and on-going trials
• Patient-specific Recommendations
– Therapy recommendations
– Drug monitoring recommendations
– Prevent adverse drug events
– Prevent drug interactions
88 88
Clinical Information
• Generate New Information to Improve Care
– Medication reconciliation
• Provide Timely Information / Review and Interpret
Literature
– Drug information center
– Clinical practice

89 89
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer

90 90
Quality Measures for
Programs
• Measure adherence using prescription claims data
– Medication Possession Ratio (MPR)
– Proportion of Days Covered (PDC)
– Adjustment for hospitalization
• Issues:
– Cash generic medications
– Lag in claims
– Multiple drugs
– Drug switching
– Overlapping fills
– Non-persistent patients
– Prescriptions returned to stock
– 90-day fills
– Can have over 100% adherence (MPR)

91 91
Medication Possession Ratio
• Number of days medication supplied in a given
interval
• Numerator is the sum of the days supplied from the
first fill in period to the second last fill in the period
• Denominator is date of the last fill minus the date of
the first fill
Days supplied in the period
Days in the period =

92 92
Medication Possession Ratio
Claim 1
Claim 2
Claim 3
Claim 4
Claim 5
Study Period Begins Study Period Ends
Day 1-30 Day 31-60 Day 61-90 Day 91-120 Day 121-150 Day 151-180
4 x 30
150 = = MPR 80%

93 93
Medication Possession Ratio
• Multiple drugs (dual or triple therapy)
Days supplied in the period / number of drugs
Days in the period =
• If the days in period are different for each
medications:
– Average the MPR for all medications for a condition

94 94
Medication Possession Ratio
Claim 1
Claim 2
Claim 3
Claim 4
Claim 5
Claim 1
Claim 2
Claim 3
Claim 4
Study Period Begins Study Period Ends
Day 1-30 Day 31-60 Day 61-90 Day 91-120 Day 121-150 Day 151-180
(3 x 30)
150 = = MPR2 60%
MPR1 = 80%
MPR = (80% + 60%) / 2 = 70%

95 95
Proportion of Days Covered
• Similar to MPR for a single medication
– Values range from 0 to 1
• Conservative estimate of medication adherence
compared to MPR for multiple medications
– A day is counted if ALL MEDICATIONS are available on
that day
Days drugs are available
Days in the period =
96 96
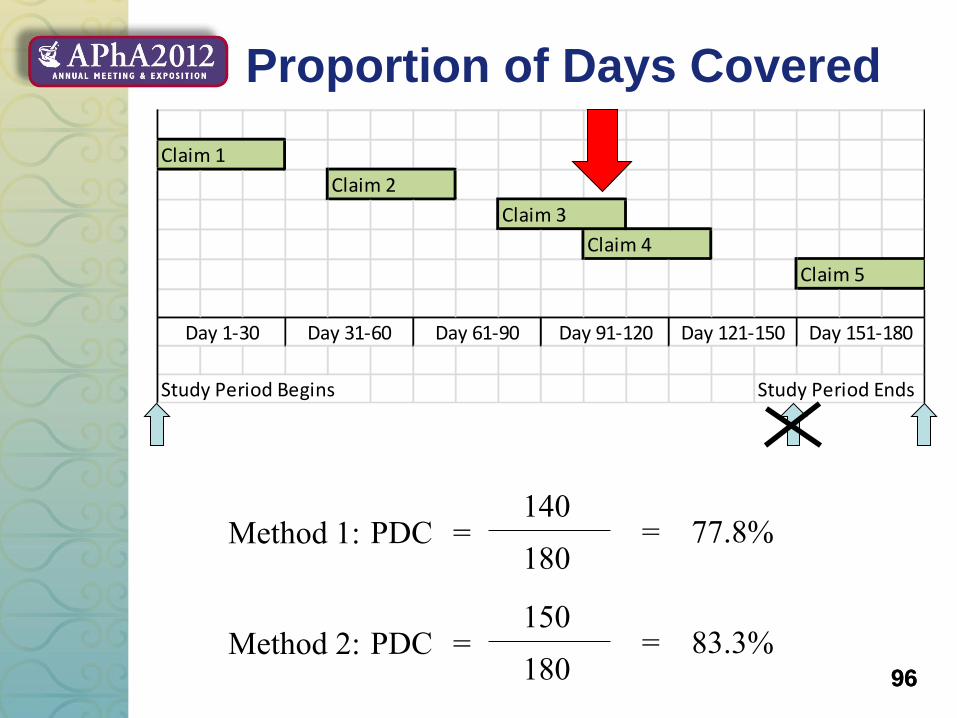
Proportion of Days Covered
Claim 1
Claim 2
Claim 3
Claim 4
Claim 5
Study Period Begins Study Period Ends
Day 1-30 Day 31-60 Day 61-90 Day 91-120 Day 121-150 Day 151-180
140
180 = = PDC 77.8% Method 1:
150
180 = = PDC 83.3% Method 2:

97 97
MPR vs. PDC for Multiple
Medications
Claim 1
Claim 2
Claim 3
Claim 4
Claim 5
Claim 1
Claim 2
Claim 3
Claim 4
Study Period Begins Study Period Ends
Day 1-30 Day 31-60 Day 61-90 Day 91-120 Day 121-150 Day 151-180
90
180 = = PDC 50%
MPR = 70%

98 98
Index
• Medication Adherence and Impact on Health
• Tools and Strategies for Assessing Adherence
• Tools and Strategies for Addressing Adherence
Issues
• Case Studies
• Pharmacists Roles in Improving Adherence
• Medication Adherence and Quality Measures
• Question and Answer

99 99
Key Points
• Nonadherence can increase healthcare costs,
decrease patient productivity and quality of life
• Nonadherence happens for a multitude of reasons
• Nonadherence must be managed on an individual
basis
• Nonadherence requires a patient-centered
approach
• Pharmacists have the resources to identifying the
root cause of the patient’s nonadherence and how
to address those issues

100 100
After 12 months of therapy, what
proportion of days do patients taking
lipid lowering medications have those
medications “on hand” (i.e. have
enough days supplied to cover)?
audience response
A. 15% 0
B. 30% 1
C. 60% 13
D. 80% 8

101 101
Which of the following is not a
tool for assessing medication
adherence?
audience response
A. Med Take 2
B. TIMER 1
C. Morisky 8-item index 0
D. AIMS 25

102 102
Assuming each fill in the figure
below is for 30 days, which of the
following is the correct calculation
for medication possession ratio?
audience response
A. 120 / 180 = 67% 7
B. 60 / 130 = 46% 3
C. 90 / 130 = 69% 14
D. 90 / 180 = 50% 2
103 103
Which of the following best
describes motivational
interviewing?
audience response
A. It is used to persuade patients
to implement healthful behaviors 1
B. It is a “tough love” approach
to behavior change 0
C. It is designed to stimulate a
patient’s intrinsic motivation to change 27
104 104
Which of the following
statements is false?
audience response
A. Patients’ adherence can
be measured by either proportion
of days covered or medication
possession ratio 0
B. Motivational interviewing is most
useful when a patient is in the “action”
stage of change 23
C. Patients with asymptomatic conditions
are less likely to adhere to their medications 2
D. Poor adherence is estimated to result
in $100 billion in avoidable hospitalization costs 0