tightrope or slackline? the neuroscience of...
TRANSCRIPT
OpinionTightrope or Slackline? TheNeuroscience of PsychoactiveSubstancesPhilippe Coulon1,* and Ali Gorji2,3,*
Novel psychoactive substances flood worldwide markets faster than they canbe banned. Legislators struggle to find a balance between free availability,prescription systems, and criminalisation, while physicians try to balance risksand benefits of drug treatment and identify drug abuse – a tightrope walk.Classification of psychoactive substances is central to these decision-makingprocesses but existing classifications rely on unrelated, inconsistent, and shift-ing guidelines that categorise drugs by chemical structure, toxicity, or addictivepotency. We propose that a new categorisation of drugs based on neurobio-logical mechanisms of action may help to simplify the regulation of drug use,delivers a neurobiological context, and streamlines classification and futureregulatory directions. We provide guidelines to distinguish between drug abuseand treatment and to navigate the controversies over legalising or banningdrugs. Finally, we comment on the role neuroscientific research can play inthe future to solve imminent problems in this highly important field.
Psychoactive SubstancesThe treatment of psychological and neurological disorders with psychoactive substances has along history and can be traced back to ancient and medieval times [1–6]. The betel nut (Arecacatechu), for example, has been in use as a psychostimulant for over 10 000 years (for a reviewsee [7]). Compared with this long history, the effect of its primary active ingredient (arecoline, apartial agonist of muscarinic acetylcholine receptors) in improving learning in patients sufferingfrom Alzheimer's disease [8] is quite recent. Uses of psychoactive plants for their psychoactiveeffects or therapeutic properties have typically been regulated by cultural means instead of bylaw, for several centuries [9]. Most psychoactive substances have clinical uses in anaesthesia,analgesia, promoting sleep or wakefulness, or treating psychological or neurological disorders,but are used without medical indication for recreational purposes or in self-treatment to changethe state of consciousness, mood, or thinking processes. They are commonly divided by theirproperties into psychostimulants (‘uppers’, such as cocaine, amphetamines, and caffeine),sedatives/hypnotics/narcotics (‘downers’, such as opioids, ketamine, and benzodiazepines),and hallucinogens (‘all arounders’, such as LSD, mescaline, and bufotenin) [10].
In the past few decades, an international agreement emerged to confine psychoactive sub-stances exclusively to therapeutic or scientific uses. However, the range of psychoactivecompounds derived from plants or chemically synthesised is vast and ever increasing, compli-cating their regulation. The World Health Organization (WHO) issued a technical report [11] onthe implementation of the 1971 Convention on Psychotropic Substances [12] outlining thesubstances that should be banned due to their health or social impact. Similarly, in the UK theMisuse of Drugs Act 1971 was the tool to identify drugs that should be banned [13]: all
TrendsNovel psychoactive substances floodworldwide markets faster than legisla-tors can react. Existing drug classifica-tions rely on unrelated, inconsistent,and shifting guidelines that classifydrugs by chemical structure, harmful-ness, or their addictive potency.
Physicians balance risks and benefitsof drug treatments and identify drugabuse of an increasing number of sub-stances. Simultaneously, legislatorsstruggle to find a balance between freeavailability, prescription systems, andcriminalisation.
A new categorisation of psychoactivesubstances seems necessary. We sug-gest a simplified system based exclu-sively on neurobiological mechanisms ofaction. This may aid the regulation ofdrug use, delivers a neurobiological con-text for addictive potency and long-termhealth effects, and streamlines classifi-cation and future regulatory directions.
1Center for Integrative Brain Research,Seattle Children's Research Institute,Seattle, WA, USA2Epilepsy Research Center,Neurosurgery Department, NeurologyDepartment, Westfälische Wilhelms-Universität, Münster, Germany3Shefa Neuroscience ResearchCenter, Tehran, Iran
*Correspondence:[email protected],[email protected] (P. Coulon),[email protected] (A. Gorji).
Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7 http://dx.doi.org/10.1016/j.tips.2016.04.004 511© 2016 Elsevier Ltd. All rights reserved.
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.
substances may be banned ‘which are being or appear to them [the Advisory Council] likely to bemisused and of which the misuse is having or appears to them capable of having harmful effectssufficient to constitute a social problem’. The 1971 Act defined three classes of drugs, A throughC, in descending order of their potential for causing harm: class A includes heroin, cocaine(including crack), methadone, ecstasy, LSD, and magic mushrooms; class B includes amphet-amines, barbiturates, codeine, cannabis, cathinones (including mephedrone), and syntheticcannabinoids; and class C includes benzodiazepines, ketamine, anabolic steroids, andN-benzylpiperazine (BZP). Today, this listing and grouping raises some questions. Whilecannabis has been legalised in large parts of the world and its potential as a clinical drughas been revised over the past three decades [14], it is still listed in the same class asamphetamines and mephedrone and in a higher class than ketamine. Heroin, cocaine, andmethadone are listed in class A despite their highly varying degree of addictiveness and despitemethadone's successful use in the treatment of heroin addiction. While the original idea that theclass determines the penalty for offences is straightforward, the definition of classes listsindividual substances instead of underlying mechanisms and is thus not directly applicableto drugs that have been newly designed. The annual reports of the International NarcoticsControl Board [15] and the World Drug Reports issued by the United Nations Office on Drugsand Crime [16,17] indicate an alarming and unmanageable number of designer drugs knownas ‘legal highs’ flooding especially the European markets. In 2012 the European MonitoringCentre for Drugs and Drug Addiction detected 73 new substances on sale on Europeanmarkets, compared with 49 in 2011 [18]. In 2014 this number exceeded 100 new substancesfor the first time [19]. By December 2014, a total of 541 new psychoactive substances wereincluded in the UN World Drug Report [20]. Production and misuse of novel psychoactivesubstances, defined as substances not (yet) under international control, is on the rise worldwide,while the figures for ‘traditional’ drugs, such as heroin and cocaine stagnate [17]. Obviously,novel psychoactive substances emerge faster than they can be banned by legislation, and lawsenabling precautionary actions are considered. The New Zealand government, for instance,recently enacted legislation that requires evidence of low risk before new psychoactive drugscan be legally sold [21], a long-overdue reverse-onus clause. In this light, the Misuse of Drugs Act1971 seems outdated, insufficient, and misguiding. An alternative system should address andunify the following concepts: (i) categorise the drug's neurobiological mechanism; and (ii) rate itspotential for health and social damage. We therefore suggest that categorising known and futuredrugs of abuse should be based on the neurobiological mechanisms that are the cause of theirnegative impacts on health and society. We give an outline of the relevant topics of currentresearch in neuropsychopharmacology, including drug refinement potential, and discuss theimportance of future research for legal approaches to controlling psychoactive substances.
Categorisation of Psychoactive Substances Based on NeurobiologicalMechanismsHow should psychoactive substances be categorised, especially concerning their potential toharm human health? The WHO ‘plays the role of a scientific arbiter on “scientific and medical”aspects in the classification of controlled substances under the international drug controltreaties’ [22] but their Expert Committee addresses wider responsibilities in a broader publichealth approach. To cover the whole range of psychoactive substances and to consider afundamentally new approach to drug classifications, these committees will require additionalresources and expertise from research. Research in the past three to four decades hasadvanced to such an extent that a fundamentally new approach to drug classification is required.We suggest that a simplified drug classification may be helpful. This may be achieved by dividingthe basic mechanisms of action into just two hazard groups.
Group I includes substances that are highly addictive, strongly hallucinogenic, and/or causedelusional states of mind (non compos mentis) in combination with a high potential for long-term
512 Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.
changes in chemical synaptic transmission. High addictiveness is ultimately expressed in‘substance seeking’ [7] and is a result of a drug's pharmacodynamics, pharmacokinetics,and metabolic compatibility. Research on the neurobiology of addiction has shown thatsubstance seeking of most drugs of abuse is caused by activation of the mesolimbic dopa-minergic system, the orbitofrontal cortex, and the extended amygdala [23–28]. In addition, somehighly addictive substances, such as cocaine and heroin, modify the activity of the endogenousopioid system and produce adaptive alterations that play crucial roles in their harmful effects [29].The transition to addiction and chronic drug seeking involves neuroplasticity in all of the abovestructures, most likely begins with a cascade of neuroadaptations, and finally causes alterationsof intracellular messenger pathways, transcription factors, and immediate early gene expressionin reward circuits [30]. If a drug mimics a neurotransmitter in a reward system but has a higheraffinity than the physiological transmitter, it becomes potentially detrimental to the physiologicalfunction of these neuronal networks, as is the case for heroin (opioid receptors), barbiturates(GABAA receptors), and some hallucinogens (LSD, bufotenin, 5-HT receptors). Receptor affinitywas proposed as a tool for the classification of psychoactive drugs over 30 years ago [31] andsuch ‘affinity profiles’ were found to permit a clinically meaningful classification of psychoactivedrugs and to be useful in the assessment of newly synthesised compounds at an early stage ofdrug development. Taken together, these factors determine our group I: neuroplasticity ofreward circuitry (dopaminergic system) to cause substance seeking, high receptor affinitycausing detrimental adaptations in physiological signalling and function, and delusional cognitivestates (serotonergic signalling, GABAergic signalling).
Group II includes drugs that may also have a potential for long-term changes in chemicalsynaptic transmission but which lack immediately hazardous effects. Changes in neuroplasticityare mostly in serotonergic and/or noradrenergic pathways and the drugs cause little or nosubstance seeking, have only modulatory effects on physiological signalling, do not causereduced consciousness (in regular doses required to cause the desired effect), and have noacutely toxic effects.
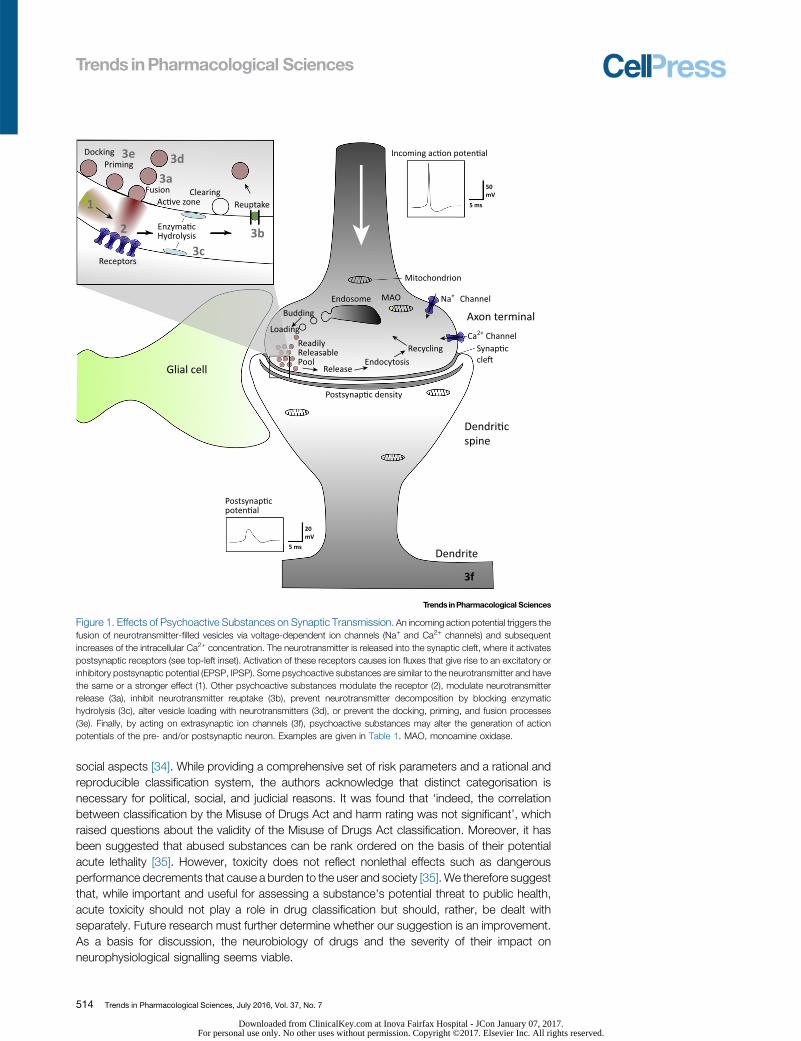
We categorise each mechanism of action of psychoactive substances (Figure 1) as group I orgroup II (Table 1). Psychoactive substances have diverse mechanisms and, in a simplified view,all mechanisms eventually impact chemical synaptic transmission, although extrasynaptic ionchannels seem to play a much larger role than previously assumed (see next section). Examplesof the most common mechanisms of action on the subcellular, cellular, and neuronal networklevels can be found in Table 1 and their mechanisms are illustrated in Figure 1.
In previous suggestions, a medical purpose for a psychoactive drug has been proposed as abasis for drug classifications: Substances with no ‘accepted’ medical use were considered themost dangerous. However, heroin, for instance, was clinically used as an analgesic, coughsuppressant, and antidiarrhoeal and would not have been a class I controlled drug according toclassification systems relying on accepted medical use [12,13,32]. Opiates in general have ahigh therapeutic potential and their clinical use has greatly reduced suffering. Vice versa,cannabis is still a class I drug according to this schedule, although today its medical use asan analgesic for chronic pain is widely accepted. Thus, accepted medical use does not seem aviable criterion, since it requires knowledge of a medical indication and comparison withalternatives (which may or may not exist) and may change drastically with new research.Moreover, it has been suggested that, when utilised and administered by competent medicalpersonnel, psychoactive agents offer relief for psychopathological suffering [33], which iscertainly a viable medical use. Genetic, biological, social, and cultural factors influence theeffects of a substance on a person and the outcome of substance use [22] and no classificationsystem can take all of these factors into account. Later suggestions of classification systemsincluded approaches to rationally assess the harm of substances in physical, dependence, and
Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7 513
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.
social aspects [34]. While providing a comprehensive set of risk parameters and a rational andreproducible classification system, the authors acknowledge that distinct categorisation isnecessary for political, social, and judicial reasons. It was found that ‘indeed, the correlationbetween classification by the Misuse of Drugs Act and harm rating was not significant’, whichraised questions about the validity of the Misuse of Drugs Act classification. Moreover, it hasbeen suggested that abused substances can be rank ordered on the basis of their potentialacute lethality [35]. However, toxicity does not reflect nonlethal effects such as dangerousperformance decrements that cause a burden to the user and society [35]. We therefore suggestthat, while important and useful for assessing a substance's potential threat to public health,acute toxicity should not play a role in drug classification but should, rather, be dealt withseparately. Future research must further determine whether our suggestion is an improvement.As a basis for discussion, the neurobiology of drugs and the severity of their impact onneurophysiological signalling seems viable.
DockingPriming
Fusion ClearingAc�ve zone Reuptake
Incoming ac�on poten�al
Mitochondrion
Endosome MAO Na+
Ca2+
Channel
ChannelSynap�ccle�
RecyclingEndocytosis
Postsynap�c density
Release
ReadilyReleasablePool
Budding
LoadingAxon terminal
Dendri�cspine
Dendrite
3f
Postsynap�cpoten�al
50mV
20mV
5 ms
5 ms
Enzyma�cHydrolysis
Glial cell
Receptors
3e 3d3a
3b3c
1
2
Figure 1. Effects of Psychoactive Substances on Synaptic Transmission. An incoming action potential triggers thefusion of neurotransmitter-filled vesicles via voltage-dependent ion channels (Na+ and Ca2+ channels) and subsequentincreases of the intracellular Ca2+ concentration. The neurotransmitter is released into the synaptic cleft, where it activatespostsynaptic receptors (see top-left inset). Activation of these receptors causes ion fluxes that give rise to an excitatory orinhibitory postsynaptic potential (EPSP, IPSP). Some psychoactive substances are similar to the neurotransmitter and havethe same or a stronger effect (1). Other psychoactive substances modulate the receptor (2), modulate neurotransmitterrelease (3a), inhibit neurotransmitter reuptake (3b), prevent neurotransmitter decomposition by blocking enzymatichydrolysis (3c), alter vesicle loading with neurotransmitters (3d), or prevent the docking, priming, and fusion processes(3e). Finally, by acting on extrasynaptic ion channels (3f), psychoactive substances may alter the generation of actionpotentials of the pre- and/or postsynaptic neuron. Examples are given in Table 1. MAO, monoamine oxidase.
514 Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.
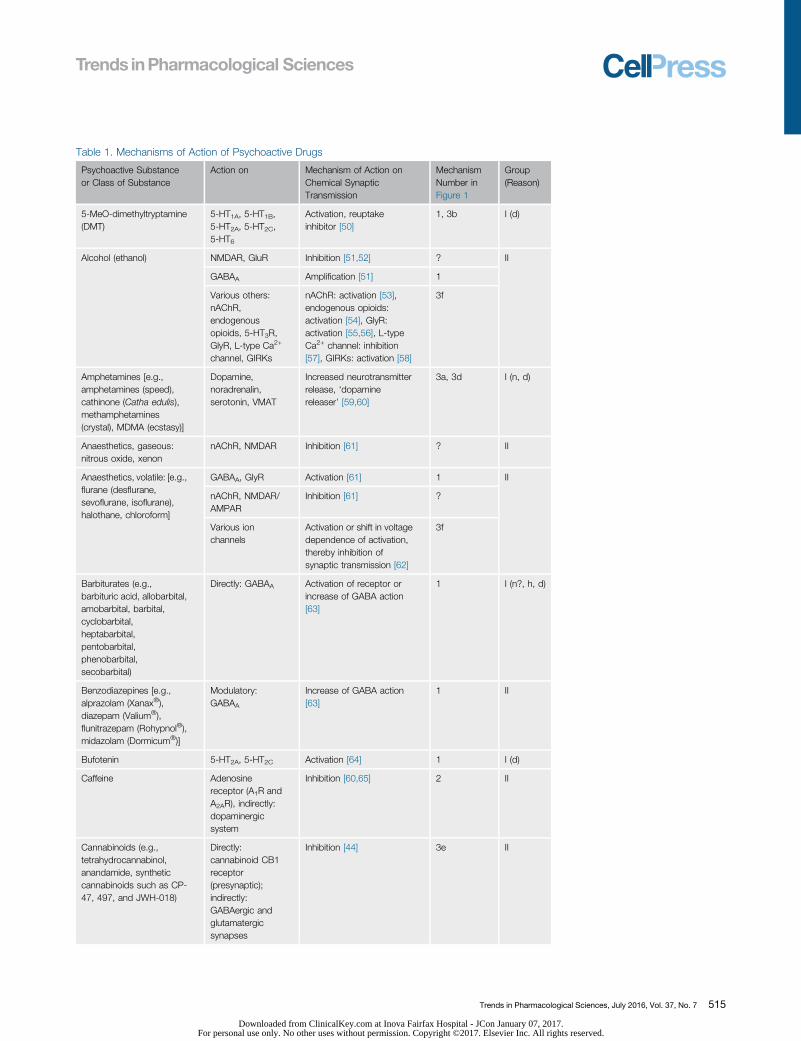
Table 1. Mechanisms of Action of Psychoactive Drugs
Psychoactive Substanceor Class of Substance
Action on Mechanism of Action onChemical SynapticTransmission
MechanismNumber inFigure 1
Group(Reason)
5-MeO-dimethyltryptamine(DMT)
5-HT1A, 5-HT1B,5-HT2A, 5-HT2C,5-HT6
Activation, reuptakeinhibitor [50]
1, 3b I (d)
Alcohol (ethanol) NMDAR, GluR Inhibition [51,52] ? II
GABAA Amplification [51] 1
Various others:nAChR,endogenousopioids, 5-HT3R,GlyR, L-type Ca2+
channel, GIRKs
nAChR: activation [53],endogenous opioids:activation [54], GlyR:activation [55,56], L-typeCa2+ channel: inhibition[57], GIRKs: activation [58]
3f
Amphetamines [e.g.,amphetamines (speed),cathinone (Catha edulis),methamphetamines(crystal), MDMA (ecstasy)]
Dopamine,noradrenalin,serotonin, VMAT
Increased neurotransmitterrelease, ‘dopaminereleaser’ [59,60]
3a, 3d I (n, d)
Anaesthetics, gaseous:nitrous oxide, xenon
nAChR, NMDAR Inhibition [61] ? II
Anaesthetics, volatile: [e.g.,flurane (desflurane,sevoflurane, isoflurane),halothane, chloroform]
GABAA, GlyR Activation [61] 1 II
nAChR, NMDAR/AMPAR
Inhibition [61] ?
Various ionchannels
Activation or shift in voltagedependence of activation,thereby inhibition ofsynaptic transmission [62]
3f
Barbiturates (e.g.,barbituric acid, allobarbital,amobarbital, barbital,cyclobarbital,heptabarbital,pentobarbital,phenobarbital,secobarbital)
Directly: GABAA Activation of receptor orincrease of GABA action[63]
1 I (n?, h, d)
Benzodiazepines [e.g.,alprazolam (Xanax®),diazepam (Valium®),flunitrazepam (Rohypnol®),midazolam (Dormicum®)]
Modulatory:GABAA
Increase of GABA action[63]
1 II
Bufotenin 5-HT2A, 5-HT2C Activation [64] 1 I (d)
Caffeine Adenosinereceptor (A1R andA2AR), indirectly:dopaminergicsystem
Inhibition [60,65] 2 II
Cannabinoids (e.g.,tetrahydrocannabinol,anandamide, syntheticcannabinoids such as CP-47, 497, and JWH-018)
Directly:cannabinoid CB1receptor(presynaptic);indirectly:GABAergic andglutamatergicsynapses
Inhibition [44] 3e II
Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7 515
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.
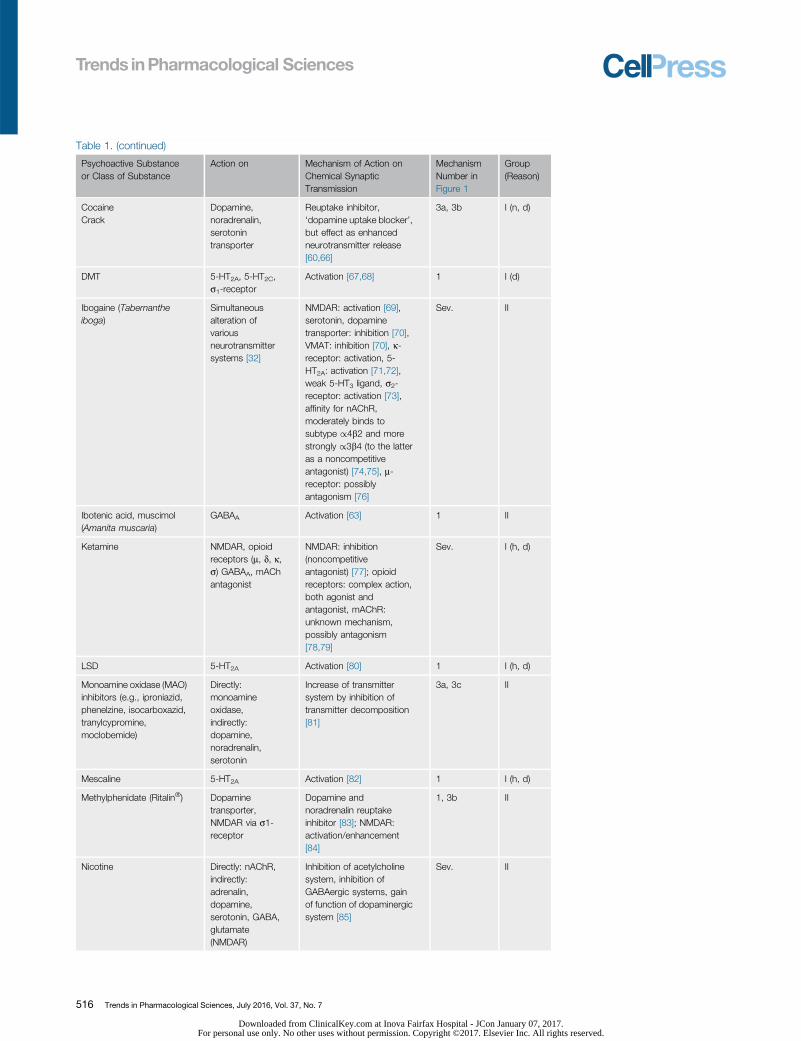
Table 1. (continued)
Psychoactive Substanceor Class of Substance
Action on Mechanism of Action onChemical SynapticTransmission
MechanismNumber inFigure 1
Group(Reason)
CocaineCrack
Dopamine,noradrenalin,serotonintransporter
Reuptake inhibitor,‘dopamine uptake blocker’,but effect as enhancedneurotransmitter release[60,66]
3a, 3b I (n, d)
DMT 5-HT2A, 5-HT2C,s1-receptor
Activation [67,68] 1 I (d)
Ibogaine (Tabernantheiboga)
Simultaneousalteration ofvariousneurotransmittersystems [32]
NMDAR: activation [69],serotonin, dopaminetransporter: inhibition [70],VMAT: inhibition [70], k-receptor: activation, 5-HT2A: activation [71,72],weak 5-HT3 ligand, s2-receptor: activation [73],affinity for nAChR,moderately binds tosubtype /4b2 and morestrongly /3b4 (to the latteras a noncompetitiveantagonist) [74,75], m-receptor: possiblyantagonism [76]
Sev. II
Ibotenic acid, muscimol(Amanita muscaria)
GABAA Activation [63] 1 II
Ketamine NMDAR, opioidreceptors (m, d, k,s) GABAA, mAChantagonist
NMDAR: inhibition(noncompetitiveantagonist) [77]; opioidreceptors: complex action,both agonist andantagonist, mAChR:unknown mechanism,possibly antagonism[78,79]
Sev. I (h, d)
LSD 5-HT2A Activation [80] 1 I (h, d)
Monoamine oxidase (MAO)inhibitors (e.g., iproniazid,phenelzine, isocarboxazid,tranylcypromine,moclobemide)
Directly:monoamineoxidase,indirectly:dopamine,noradrenalin,serotonin
Increase of transmittersystem by inhibition oftransmitter decomposition[81]
3a, 3c II
Mescaline 5-HT2A Activation [82] 1 I (h, d)
Methylphenidate (Ritalin®) Dopaminetransporter,NMDAR via s1-receptor
Dopamine andnoradrenalin reuptakeinhibitor [83]; NMDAR:activation/enhancement[84]
1, 3b II
Nicotine Directly: nAChR,indirectly:adrenalin,dopamine,serotonin, GABA,glutamate(NMDAR)
Inhibition of acetylcholinesystem, inhibition ofGABAergic systems, gainof function of dopaminergicsystem [85]
Sev. II
516 Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.
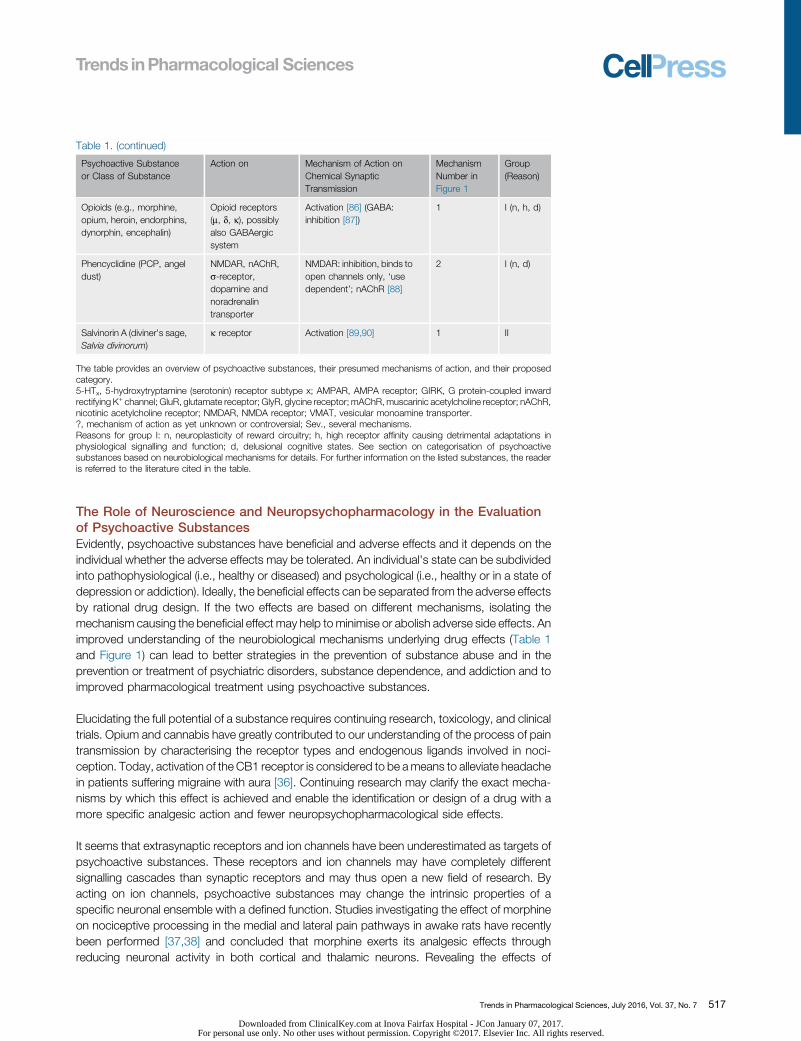
The Role of Neuroscience and Neuropsychopharmacology in the Evaluationof Psychoactive SubstancesEvidently, psychoactive substances have beneficial and adverse effects and it depends on theindividual whether the adverse effects may be tolerated. An individual's state can be subdividedinto pathophysiological (i.e., healthy or diseased) and psychological (i.e., healthy or in a state ofdepression or addiction). Ideally, the beneficial effects can be separated from the adverse effectsby rational drug design. If the two effects are based on different mechanisms, isolating themechanism causing the beneficial effect may help to minimise or abolish adverse side effects. Animproved understanding of the neurobiological mechanisms underlying drug effects (Table 1and Figure 1) can lead to better strategies in the prevention of substance abuse and in theprevention or treatment of psychiatric disorders, substance dependence, and addiction and toimproved pharmacological treatment using psychoactive substances.
Elucidating the full potential of a substance requires continuing research, toxicology, and clinicaltrials. Opium and cannabis have greatly contributed to our understanding of the process of paintransmission by characterising the receptor types and endogenous ligands involved in noci-ception. Today, activation of the CB1 receptor is considered to be a means to alleviate headachein patients suffering migraine with aura [36]. Continuing research may clarify the exact mecha-nisms by which this effect is achieved and enable the identification or design of a drug with amore specific analgesic action and fewer neuropsychopharmacological side effects.
It seems that extrasynaptic receptors and ion channels have been underestimated as targets ofpsychoactive substances. These receptors and ion channels may have completely differentsignalling cascades than synaptic receptors and may thus open a new field of research. Byacting on ion channels, psychoactive substances may change the intrinsic properties of aspecific neuronal ensemble with a defined function. Studies investigating the effect of morphineon nociceptive processing in the medial and lateral pain pathways in awake rats have recentlybeen performed [37,38] and concluded that morphine exerts its analgesic effects throughreducing neuronal activity in both cortical and thalamic neurons. Revealing the effects of
Table 1. (continued)
Psychoactive Substanceor Class of Substance
Action on Mechanism of Action onChemical SynapticTransmission
MechanismNumber inFigure 1
Group(Reason)
Opioids (e.g., morphine,opium, heroin, endorphins,dynorphin, encephalin)
Opioid receptors(m, d, k), possiblyalso GABAergicsystem
Activation [86] (GABA:inhibition [87])
1 I (n, h, d)
Phencyclidine (PCP, angeldust)
NMDAR, nAChR,s-receptor,dopamine andnoradrenalintransporter
NMDAR: inhibition, binds toopen channels only, ‘usedependent’; nAChR [88]
2 I (n, d)
Salvinorin A (diviner's sage,Salvia divinorum)
k receptor Activation [89,90] 1 II
The table provides an overview of psychoactive substances, their presumed mechanisms of action, and their proposedcategory.5-HTx, 5-hydroxytryptamine (serotonin) receptor subtype x; AMPAR, AMPA receptor; GIRK, G protein-coupled inwardrectifying K+ channel; GluR, glutamate receptor; GlyR, glycine receptor; mAChR, muscarinic acetylcholine receptor; nAChR,nicotinic acetylcholine receptor; NMDAR, NMDA receptor; VMAT, vesicular monoamine transporter.?, mechanism of action as yet unknown or controversial; Sev., several mechanisms.Reasons for group I: n, neuroplasticity of reward circuitry; h, high receptor affinity causing detrimental adaptations inphysiological signalling and function; d, delusional cognitive states. See section on categorisation of psychoactivesubstances based on neurobiological mechanisms for details. For further information on the listed substances, the readeris referred to the literature cited in the table.
Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7 517
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.

morphine on individual neurons and their intrinsic properties, identifying the neuronal populationsthat respond to opioid treatment, and ultimately understanding the role of the neuronal networksthese neurons form in the CNS could open new pathways for pain treatment via supraspinalmechanisms of analgesia and could possibly aid in understanding and treating substancedependence. For example, the K+-conducting ion channels known as “M-channels” (KV 7.2and 7.3), are known to stabilise the membrane potential, thereby controlling neuronal excitability[39–41], and have recently been shown to produce effective analgesia [41]. Currents throughGABAA receptors may also occur at extrasynaptic sites. In contrast to phasic inhibition bysynaptic release, this so-called tonic inhibition is produced by the activation of high-affinityreceptors by ambient GABA at extrasynaptic sites [42,43]. Baclofen's clinical action, in particularin the treatment of alcohol dependence and withdrawal, may be due to GABAB-mediatedenhancement of tonic GABAA currents throughout the brain [42], an action it shares with ethanolbut without the latter's addictive potency. These examples demonstrate that research in thesefields can yield tremendous advances for therapies and treatments. Moreover, knowledge of allof the mechanisms of action of a psychoactive substance can be crucial for their classification.For example, D-9-tetrahydrocannabinol (THC), the active compound in cannabis, mimics aneurotransmitter, and in this is similar to opiates. However, opiate signalling causes downstreammodifications of the dopaminergic reward circuitry. Cannabis, by contrast, mimics anandamide,which activates the CB-1 receptor, inhibits calcium channels in the presynaptic membrane, andultimately leads to a reduced neurotransmitter release [44].
Concluding RemarksAlcohol, hypnotics, sedatives, opioids, cannabis, cocaine, amphetamines, and hallucinogensare among the most frequently used and abused psychoactive substances. Antidepressantsand neurocognitive enhancers should perhaps also be counted in this group. Research hascontributed considerably to explaining the mechanisms of action of these substances byelucidating the physiological or pathophysiological basis of the respective mental states, byinvestigating the effects of these substances on neurons or neuronal networks, and by investi-gating adverse effects, substance tolerance, and addiction as well as the health and socialimpact. In summary, research in neuropsychopharmacology can provide tremendous advancesin treatment strategies and in our general understanding of brain function.
Unfortunately, funding largely concentrates on potential new drugs. Once a drug is available andsold, interest in public or commercial funding for research on alternative uses or improvementsseems to diminish. Providing sufficient funds for basic, non-commercial research in neuro-psychopharmacology is thus of primary interest (see Outstanding Questions). Since anyresearch on these substances requires their availability, a solid framework must be in placeto establish free access to substances for basic neuroscientific research. This may leave publicbanning of hazardous substances unaffected, but which substances or mechanisms of actionare to be banned, and which substances may be freely available, cannot be decided without thebackground knowledge provided by neuroscientific research. The existing framework providedby, for example, the Misuse of Drugs Act seems outdated and in need of an update. Wetherefore propose that a characterisation of psychoactive substances based on neurobiologicalmechanisms should be taken into consideration. This may simplify the regulation of drug use,delivers a neurobiological context for addictive potency and long-term health effects, and thusprovides a means of staying ahead of drug design by streamlining regulatory directions.
Alongside judicial intricacies and social controversies, it has become increasingly difficult forphysicians to calculate the risks and to balance the possible positive and negative outcomes ofdrug treatment. It increasingly resembles a tightrope or slackline walk: jurisdiction must find abalance between banning, the prescription systems, and free availability; physicians have todistinguish between drug treatment and drug abuse. On the one hand, it is often argued that
Outstanding QuestionsWhich substances or mechanisms ofaction are to be banned and which sub-stances should be freely available? Thenew categorisation we suggest here canbe a first step only and is intended as abasis for future discussions. A completeand comprehensive retooling requires abroad consensus among the scientificcommunity across fields.
What is the optimal balance betweentreatment with potential drugs of abuse(to reduce suffering) and drug addiction(increased suffering)? Does a prescrip-tion system provide adequate control?
What is the origin of addiction? What isthe genetic basis of drug addiction?Answering these questions can com-plete the transition from a social prob-lem to a medical problem and fromdisdain to sympathy.
Can new and improved treatmentstrategies be developed for psycholog-ical and physiological disorders basedon the neurobiological mechanisms ofaction of novel psychoactive substan-ces? How can research in drug refine-ment and alternative uses of existingsubstances be improved and betterfunded?
518 Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.

omission to ban or to legalise a substance may suggest that it is harmless. On the other hand,judicial bans are already in place for numerous substances but seem to be ineffective inpreventing abuse. Legislation has the duty to protect from harm, and this involves protectionof an individual from hazardous substances. Moreover, addiction and its associated criminalactivity have always posed threats to individuals and to society. Nevertheless, criminalisation ofself-harm is neither a morally acceptable nor an effective measure for controlling psychoactivesubstances.
What differentiates the legally available drugs from illicit drugs? It is argued that alcohol isinherently no less dangerous than illicit drugs, and dependence on nicotine in tobacco causesmore deaths and health problems than dependence on any other psychoactive substance [22].Tobacco ranks ninth in mortality and morbidity in countries with high mortality and third incountries with low mortality [45]. In 2002, 5500 billion cigarettes were manufactured andconsumed by 1.2 billion smokers in the world [46]. The annual per capita consumption ofalcohol is well above 10 l of pure ethanol in Western and Central Europe and just under 10 l inNorth America and Australia [47]. Tobacco smoking and drinking alcohol cause the majority ofdrug-related medical problems. It seems hypocrisy to issue a general ban on drugs and excludethe ones that are most widely used and cause by far the most medical and, in the case of alcohol,social problems. The absolute numbers of both deaths and life-years lost are far larger for legalsubstances [16,48] than for the illicit opiates, cocaine, and amphetamines combined. However,there are far fewer illegal drug users than there are users of alcohol and tobacco. Thus, whentaking into account the total number of users, the amount and severity of abuse-relatedproblems are comparably low for these drugs. While, on average, 18–19 life-years were lostfor users of opiates, cocaine, and amphetamines, it was 5 years for users of tobacco and 2 yearsfor alcohol [16,48,49]. It seems that ‘life-years lost’ may serve as a viable criterion for categorisingsubstances. These numbers, however, take decades to determine [49].
Recent events and developments have shown that it is essential to continue research to improvethe therapeutic risk balance and to identify possible drug effects, even years after licensing orthousands of years after the first reports of recreational use or abuse. Continuing efforts to findnovel mechanisms of psychoactive substances and to investigate already-licensed drugs notonly allows the expansion of therapeutic strategies but also helps to reduce risks and potentiallysaves lives. Improving our knowledge regarding the basic mechanisms of action of psychoactivesubstances may also allow reduction of the abuse potential by drug refinement and improve ourfundamental research strategies.
AcknowledgmentsThe authors thank Erwin-Josef Speckmann, Peter Mullen, Thomas Budde, Carole E. Landisman, and Anna Ventura for
helpful comments and discussion.
References1. Gorji, A. (2003) Pharmacological treatment of headache using
traditional Persian medicine. Trends Pharmacol. Sci. 24, 331–334
2. Vakili, N. and Gorji, A. (2006) Psychiatry and psychology in medi-eval Persia. J. Clin. Psychiatry 67, 1862–1869
3. Gorji, A. and Khaleghi Ghadiri, M. (2002) History of headache inmedieval Persian medicine. Lancet Neurol. 1, 510–515
4. Koulivand, P.H. et al. (2013) Lavender and the nervous system.Evid. Based Complement. Altern. Med. 2013, 681304
5. Gorji, A. and Khaleghi Ghadiri, M. (2001) History of epilepsyin medieval Iranian medicine. Neurosci. Biobehav. Rev. 25,455–461
6. Mahdizadeh, S. et al. (2015) Avicenna's Canon of Medicine: areview of analgesics and anti-inflammatory substances. AvicennaJ. Phytomed. 5, 182–202
7. Sullivan, R.J. and Hagen, E.H. (2002) Psychotropic substance-seeking: evolutionary pathology or adaptation? Addiction 97,389–400
8. Soncrant, T. et al. (1993) Memory improvement without toxicityduring chronic, low dose intravenous arecoline in Alzheimer'sdisease. Psychopharmacology. (Berl.) 112, 421–427
9. Tupper, K. and Labate, B. (2014) Ayahuasca, psychedelic studiesand health sciences: the politics of knowledge and inquiry into anAmazonian plant brew. Curr. Drug Abuse Rev. 7, 71–80
10. Alberts, A. and Mullen, P. (2011) Psychoaktive Pflanzen, Pilze undTiere, Franckh-Kosmos. (in German)
11. World Health Organization (1981) Assessment of Public Healthand Social Problems Associated with the Use of PsychotropicDrugs – Report of the, WHO., Expert Committee on
Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7 519
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.

Implementation of the Convention on Psychotropic Substances.1971, World Health Organization
12. Khan, I. (1979) Convention on psychotropic substances, 1971.The role and responsibilities of the World Health Organization.Prog. Neuropsychopharmacol. 3, 11–14
13. Advisory Council on the Misuse of Drugs (1971) Misuse of DrugsAct 1971, ACMD
14. Sharma, P. et al. (2012) Chemistry, metabolism, and toxicology ofcannabis: clinical implications. Iran. J. Psychiatry 7, 149–156
15. International Narcotics Control Board (2013) Report of the Inter-national Narcotics Control Board 2012, United Nations
16. United Nations Office on Drugs and Crime (2012) World DrugReport 2012, United Nations
17. United Nations Office on Drugs and Crime (2013) World DrugReport 2013, United Nations
18. European Monitoring Centre for Drugs and Drug Addiction (2013)European Drug Report 2013, EMCDDA
19. European Monitoring Centre for Drugs and Drug Addiction (2015)European Drug, Report., Trends and Developments 2015,EMCDDA
20. United Nations Office on Drugs and Crime (2015) UN World DrugReport, United Nations
21. Schep, L.J. et al. (2014) Regulating new psychoactive drugs:innovation leading to compromise. BMJ 349, g5085
22. World Health Organization (2004) Neuroscience of psychoactivesubstance use and dependence. Addiction 99, 1361–1362
23. Büttner, A. (2011) Review: the neuropathology of drug abuse.Neuropathol. Appl. Neurobiol. 37, 118–134
24. Hyman, S.E. et al. (2006) Neural mechanisms of addiction: the roleof reward-related learning and memory. Annu. Rev. Neurosci. 29,565–598
25. Koob, G.F. and Nestler, E.J. (1997) The neurobiology of drugaddiction. J. Neuropsychiatry Clin. Neurosci. 9, 482–497
26. Koob, G.F. (2000) Neurobiology of addiction. Toward the devel-opment of new therapies. Ann. N. Y. Acad. Sci. 909, 170–185
27. Leshner, A.I. and Koob, G.F. (1999) Drugs of abuse and the brain.Proc. Assoc. Am. Physicians 111, 99–108
28. Nestler, E.J. (2004) Molecular mechanisms of drug addiction.Neuropharmacology 47 (Suppl.), 24–32
29. Noble, F. et al. (2015) The opioid receptors as targets for drugabuse medication. Br. J. Pharmacol. 172, 3964–3979
30. Koob, G.F. and Volkow, N.D. (2010) Neurocircuitry of addiction.Neuropsychopharmacology 35, 217–238
31. Closse, A. et al. (1984) Classification of drugs according to recep-tor binding profiles. Naunyn Schmiedebergs Arch. Pharmacol.327, 95–101
32. United Nations Conference for the Adoption of a Single Conven-tion on Narcotic Drugs (1962) The single convention on narcoticdrugs. United Nations 16, 776
33. Woolley, B.H. (1982) An approach to drug classification. AMCAPJ. 8, 13–18
34. Nutt, D. et al. (2007) Development of a rational scale to assess theharm of drugs of potential misuse. Lancet 369, 1047–1053
35. Gable, R.S. (2004) Comparison of acute lethal toxicity of com-monly abused psychoactive substances. Addiction 99, 686–696
36. Kazemi, H. et al. (2012) Effect of cannabinoid receptor activationon spreading depression. Iran. J. Basic Med. Sci. 15, 926–936
37. Su, Y. et al. (2012) The effects of morphine on basal neuronalactivities in the lateral and medial pain pathways. Neurosci. Lett.525, 173–178
38. Wang, J-Y. et al. (2009) Morphine modulation of pain processing inmedial and lateral pain pathways. Mol. Pain 5, 60
39. Tatulian, L. et al. (2001) Activation of expressed KCNQ potassiumcurrents and native neuronal M-type potassium currents by theanti-convulsant drug retigabine. J. Neurosci. 21, 5535–5545
40. Brown, D.A. and Passmore, G.M. (2009) Neural KCNQ (Kv7)channels. Br. J. Pharmacol. 156, 1185–1195
41. Cerina, M. et al. (2015) Thalamic Kv7 channels: pharmacologicalproperties and activity control during noxious signal processing.Br. J. Pharmacol. 172, 3126–3140
42. Connelly, W.M. et al. (2013) GABAB receptors regulate extrasy-naptic GABAA receptors. J. Neurosci. 33, 3780–3785
43. Farrant, M. and Nusser, Z. (2005) Variations on an inhibitorytheme: phasic and tonic activation of GABAA receptors. Nat.Rev. Neurosci. 6, 215–229
44. Piomelli, D. (2003) The molecular logic of endocannabinoid sig-nalling. Nat. Rev. Neurosci. 4, 873–884
45. Uchtenhagen, A. (2004) Substance use problems in developingcountries. Bull. World Health Organ. 82, 641–642
46. Mackay, J. and Eriksen, M. (2002) The Tobacco Atlas, WorldHealth Organization
47. Rehm, J. et al. (2003) Alcohol as a risk factor for global burden ofdisease. Eur. Addict. Res. 9, 157–164
48. World Health Organization (2002) The World Health Report, WorldHealth Organization
49. Smyth, B. et al. (2007) Years of potential life lost among heroinaddicts 33 years after treatment. Prev. Med. 44, 369–374
50. Halberstadt, A. et al. (2008) Modification of the effects of 5-methoxy-N, N-dimethyltryptamine on exploratory behavior in ratsby monoamine oxidase inhibitors. Psychopharmacology (Berl.)201, 55–66
51. Deitrich, R.A. et al. (1989) Mechanism of action of ethanol: initialcentral nervous system actions. Pharmacol. Rev. 41, 489–537
52. Möykkynen, T. and Korpi, E. (2012) Acute effects of ethanol onglutamate receptors. Basic Clin. Pharmacol. Toxicol. 111, 4–13
53. Narahashi, T. et al. (1999) Neuronal nicotinic acetylcholinereceptors: a new target site of ethanol. Neurochem. Int. 35,131–141
54. McIntosh, C. and Chick, J. (2004) Alcohol and the nervous system.J. Neurol. Neurosurg. Psychiatry 75, iii16–iii21
55. Mihic, S.J. (1999) Acute effects of ethanol on GABAA and glycinereceptor function. Neurochem. Int. 35, 115–123
56. Mihic, S.J. et al. (1997) Sites of alcohol and volatile anaestheticaction on GABAA and glycine receptors. Nature 389, 385–389
57. Wang, X. et al. (1994) Ethanol directly modulates gating of adihydropyridine-sensitive Ca2+ channel in neurohypophysial ter-minals. J. Neurosci. 14, 5453–5460
58. Kobayashi, T. et al. (1999) Ethanol opens G-protein-activatedinwardly rectifying K+ channels. Nat. Neurosci. 2, 1091–1097
59. Elliott, J.M. and Beveridge, T.J.R. (2005) Psychostimulants andmonoamine transporters: upsetting the balance. Curr. Opin. Phar-macol. 5, 94–100
60. Ferré, S. (2008) An update on the mechanisms of the psychos-timulant effects of caffeine. J. Neurochem. 105, 1067–1079
61. Campagna, J.A. et al. (2003) Mechanisms of actions of inhaledanesthetics. N. Engl. J. Med. 348, 2110–2124
62. Budde, T. et al. (2008) Reciprocal modulation of I (h) and I (TASK) inthalamocortical relay neurons by halothane. Pflugers Arch. 456,1061–1073
63. Macdonald, R.L. and Olsen, R.W. (1994) GABAA receptor chan-nels. Annu. Rev. Neurosci. 17, 569
64. McBride, M.C. (2000) Bufotenine: toward an understanding ofpossible psychoactive mechanisms. J. Psychoactive Drugs 32,321–331
65. Basheer, R. et al. (2004) Adenosine and sleep–wake regulation.Prog. Neurobiol. 73, 379–396
66. Torres, G.E. et al. (2003) Plasma membrane monoamine trans-porters: structure, regulation and function. Nat. Rev. Neurosci. 4,13–25
67. Fontanilla, D. et al. (2009) The hallucinogen N, N-dimethyltrypta-mine (DMT) is an endogenous s-1 receptor regulator. Science323, 934–937
68. Smith, R.L. et al. (1998) Agonist properties of N, N-dimethyltryp-tamine at serotonin 5-HT2A and 5-HT2C receptors. Pharmacol.Biochem. Behav. 61, 323–330
69. Popik, P. et al. (1994) The putative anti-addictive drug ibogaine is acompetitive inhibitor of [3H]MK-801 binding to the NMDA receptorcomplex. Psychopharmacology (Berl.) 114, 672–674
70. Popik, P. and Skolnick, P. (1998) Pharmacology of ibogaine andibogaine-related alkaloids. Alkaloids 52, 197–231
520 Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.

71. Glick, S.D. et al. (1999) (�)-18-Methoxycoronaridine: a novel ibogaalkaloid congener having potential anti-addictive efficacy. CNSDrug Rev. 5, 27–42
72. Szumlinski, K.K. et al. (2000) The potential anti-addictive agent,18-methoxycoronaridine, blocks the sensitized locomotor anddopamine responses produced by repeated morphine treatment.Brain Res. 864, 13–23
73. Mach, R.H. et al. (1995) Ibogaine possesses a selective affinity fors 2 receptors. Life Sci. 57, PL57–PL62
74. Glick, S.D. et al. (2002) Antagonism of /3b4 nicotinic receptors asa strategy to reduce opioid and stimulant self-administration. Eur.J. Pharmacol. 438, 99–105
75. Schneider, A.S. et al. (1996) Ibogaine selectively inhibits nicotinicreceptor-mediated catecholamine release. Eur. J. Pharmacol.317, R1–R2
76. Antonio, T. et al. (2013) Effect of iboga alkaloids on m-opioidreceptor-coupled G protein activation. PLoS ONE 8, 1–18
77. Orser, B.A. et al. (1997) Multiple mechanisms of ketamine blockadeof N-methyl-D-aspartate receptors. Anesthesiology 86, 903–917
78. Bergman, S.A. (1999) Ketamine: review of its pharmacology andits use in pediatric anesthesia. Anesth. Prog. 46, 10–20
79. Hirota, K. and Lambert, D.G. (1996) Ketamine: its mechanism(s) ofaction and unusual clinical uses. Br. J. Anaesth. 77, 441–444
80. Backstrom, J.R. et al. (1999) Agonist-directed signaling of serotonin5-HT2C receptors: differences between serotonin and lysergic aciddiethylamide (LSD). Neuropsychopharmacology 21, 77S-81S
81. Yamada, M. and Yasuhara, H. (2004) Clinical pharmacology ofMAO inhibitors: safety and future. Neurotoxicology 25, 215–221
82. Aghajanian, G.K. and Marek, G.J. (1999) Serotonin and halluci-nogens. Neuropsychopharmacology 21, 16S-23S
83. Kuczenski, R. and Segal, D.S. (1997) Effects of methylphenidateon extracellular dopamine, serotonin, and norepinephrine: com-parison with amphetamine. J. Neurochem. 68, 2032–2037
84. Zhang, C-L. et al. (2012) Methylphenidate enhances NMDA-receptor response in medial prefrontal cortex via s-1 receptor:a novel mechanism for methylphenidate action. PLoS ONE 7,e51910
85. Mansvelder, H.D. and McGehee, D.S. (2002) Cellular and synapticmechanisms of nicotine addiction. J. Neurobiol. 53, 606–617
86. Pasternak, G.W. (2004) Multiple opiate receptors: déjà vu all overagain. Neuropharmacology 47, 312–323
87. Kalyuzhny, A.E. et al. (2000) Opioid- and GABAA-receptors are co-expressed by neurons in rat brain. Neuroreport 11, 2625–2628
88. Morris, B.J. et al. (2005) PCP: from pharmacology to modellingschizophrenia. Curr. Opin. Pharmacol. 5, 101–106
89. Chavkin, C. et al. (2004) Salvinorin A, an active component of thehallucinogenic sage Salvia divinorum is a highly efficacious k-opioid receptor agonist: structural and functional considerations.J. Pharmacol. Exp. Ther. 308, 1197–1203
90. Roth, B.L. et al. (2002) Salvinorin A: a potent naturally occurringnonnitrogenous kappa opioid selective agonist. Proc. Natl. Acad.Sci. U.S.A. 99, 11934–11939
Trends in Pharmacological Sciences, July 2016, Vol. 37, No. 7 521
Downloaded from ClinicalKey.com at Inova Fairfax Hospital - JCon January 07, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.