ticagrelor vs prasugrel - oic.it · ticagrelor 6 8 10 12 cumulative incidence (%) 2 4 interaction...
TRANSCRIPT

1
Leonardo De Luca, M.D., Ph.D., F.A.C.C.
Department of Cardiovascular SciencesInterventional Cardiology UnitEuropean HospitalRome, [email protected]
9°MEETING CARDIOLUCCA
CONTROVERSIA D’AUTORE:QUALE TERAPIA ANTIAGGREGANTE NELLO STEMI?
Lucca, Auditorium S. Francesco28-30 Novembre 2013
Ticagrelor vsPrasugrel
1

Necessity is the mother of
invention
Plato
The Essence of Plato’s Philosophy

• Effective (in terms of recurrent ischemic events prevention) in the broad spectrum of STEMI pts
• Useful in Primary PCI (life-saving therapy in STEMI)
• Functional and safe in clinical practice
What do we Need from a New OAT in STEMI?

This analysis addresses the subgroup of patients with STE-ACS, defined as typical symptoms plus either persistent ST-elevation of 1 mV for 20 minutes in 2 contiguous leads and planned primary PCI (defined as PCI within the first 24 hours after symptom onset) or new or presumed-new left bundle-branch block (LBBB) and planned primary PCI. A sensitivity analysis also included patients with a discharge diagnosis of STEMI.
Who are STEMI Patients Enrolled in PLATO?
Steg PG et al, Circulation 2010;122:2131

p=0.98
p=0.93
p=0.10
p=0.67
%
PLATO STEMI Subgroup:Procedures
During index hospitalizationSteg PG, et al. Circulation. 2010;122:2131

Ticagrelor in PLATOSTEMI Subgroup
Steg PG, et al. Circulation. 2010;122:2131
N=7544P=0.07
0
Primary Efficacy Endpoint
2
4
8
12
6
10
0
ClopidogrelTicagrelor
6 8 10 12
Cum
ulat
ive
inci
denc
e (%
)
42
N=7544P=0.76
0
Plato Major Bleeding
2
4
8
10
6
0
Clopidogrel
Ticagrelor
6 8 10 12
Cum
ulat
ive
inci
denc
e (%
)
42
interaction P=0.29

1. Was the hypothesis specified a priori?2. Does the interaction test suggest a low likelihood that
chance explains the apparent subgroup effect?3. Is the size of the subgroup effect large?4. Is the interaction consistent across studies?5. Is there indirect evidence that supports the hypothesised
interaction (biological rationale)?
5 Criteria to Assess Credibility of Subgroup Analys esIs a Subgroup Effect Believable?
Sun X, et al. BMJ 2010;340:c117

pPCI
RISK
Death Rate Reduction in PLATO..Beyond Primary PCI
p=0.07 p=0.04
Steg PG, et al. Circulation 2010;122:2131Wallentin L, et al. N Engl J Med 2009;361:1045
� …of course, we cannot completely rule out the possibility it is a play of chance
� But consistent in ALL explored subgroups…
� …greater relative and absolute benefit than non-fatal endpoints…in a 18,000 pts study!

9
PLATO STE-ACS: Sensitivity analyses in patients diagnosed with STE-ACS/STEMI
CharacteristicInteraction
p valueHR (95% CI)
Ticagrelor better Clopidogrel better
0.5 1.0 2.00.2
Ticagrelor Clopidogrel
LBBB at presentation
Persistent STE at presentation
0.91
Diagnosis of STEMI at discharge only
14.5 14.5
8.9 10.4
8.4 12.5
Definition of STE-ACS/STEMI
0.89 (0.59–1.34)
0.87 (0.74–1.02)
0.67 (0.44–1.02)
720
6824
886
n
Primary efficacy endpoint at month 12 (%)
Steg PG et al, Circulation 2010;122:2131
As it was expected that some patients may not receive an initial diagnosis of STEMI, but may be diagnosed with STEMI upon discharge, sensitivity analyses were planned and performed to explore the consistency of the results using different definitions of the STE-ACS/STEMI population – in particular, analysing the group of patients with a diagnosis of STEMI at discharge only[Steg 2010:D,E]
• In addition to the 7544 patients with an initial diagnosis of STE-ACS (i.e. patients presenting with STE or LBBB), an additional 886 patients who received a diagnosis of STEMI upon discharge[Steg 2010:H]
• In the sensitivity analyses, the effect on the primary efficacy endpoint was similar for patients with STE at presentation, those with LBBB at presentation, and patients who had a diagnosis of STEMI at discharge only[Steg 2010:S]
Steg PG, et al. Circulation 2010;122:2131–2141.
9

1010
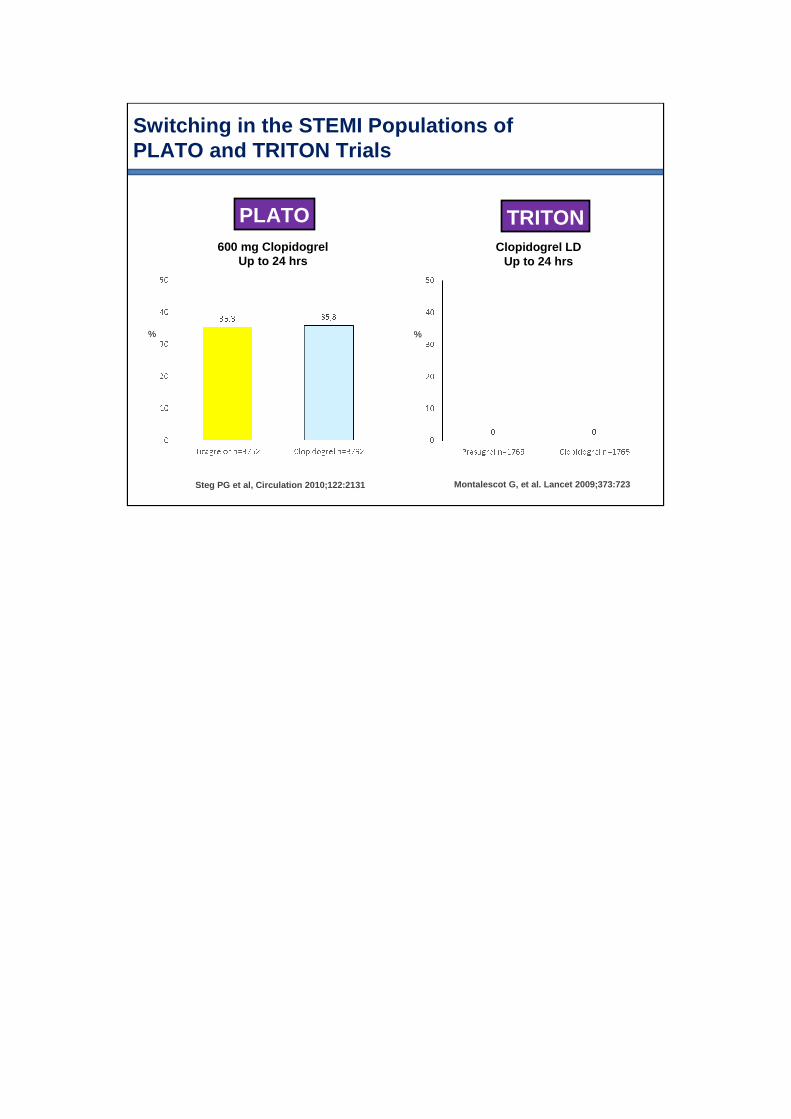
Switching in the STEMI Populations of PLATO and TRITON Trials
PLATO TRITON
Steg PG et al, Circulation 2010;122:2131 Montalescot G, et al. Lancet 2009;373:723
%
600 mg ClopidogrelUp to 24 hrs
%
Clopidogrel LDUp to 24 hrs

This presentation is provided as background training for speakers
PLATO was not designed or powered to demonstrate the efficacy or safety of BRILINTA compared with clopidogrel in specific subgroups. Subgroup analyses were performed to evaluate consistency of results in different cohorts. Analyses must be interpreted cautiously, as differences can reflect the play of chance among a large number of analyses. Some subgroups were based on post-randomized determinations
•Any information contained in this presentation that is not contained in a promotional slide deck must not be shared proactively during speaker programs
Information from this presentation that is consistent with the Prescribing Information for BRILINTA may be shared in a specific response to an unsolicited question from the audience
12
12
STEMI With Planned PCI in the PLATOEfficacy – Clopidogrel Loading Dose
Steg et al. Circulation. 2010;122:2131

Multitude subsists
simultaneously with
the one.
Plato
The Essence of Plato’s Philosophy

ACS
STEMI
Sample Size Calculation and p Values
p for Interaction
SUBGROUP
PLATO
ACS
STEMI
Sample Size Calculation and p Values

NSTE-ACS
STEMI30% of total
TRITON TIMI-38
Sample Size Calculation and p Values
p Valuefor Superiority
COHORT

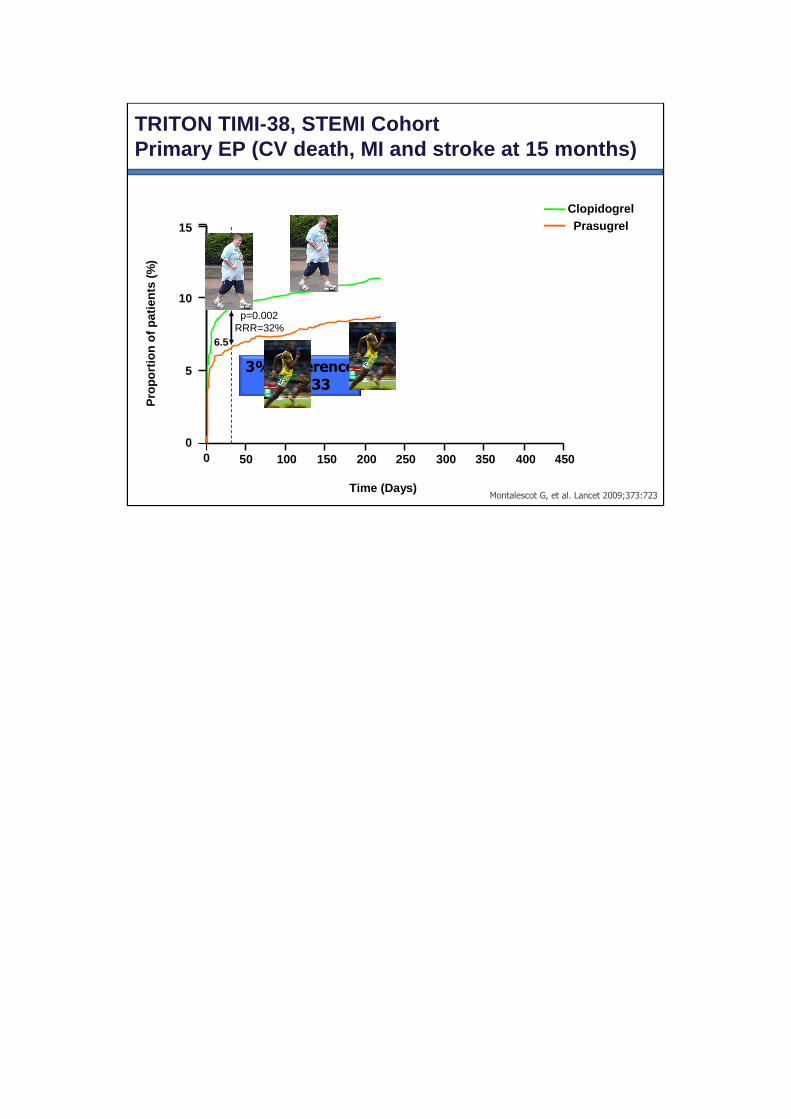
TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0p=0.02
ClopidogrelPrasugrel
N=3534

This analysis addresses the subgroup of patients with STE-ACS, defined as typical symptoms plus either persistent ST-elevation of 1 mV for 20 minutes in 2 contiguous leads and planned primary PCI (defined as PCI within the first 24 hours after symptom onset) or new or presumed-new left bundle-branch block (LBBB) and planned primary PCI. A sensitivity analysis also included patients with a discharge diagnosis of STEMI.
Not All STEMI Patients Are Alike
Steg PG et al, Circulation 2010;122:2131
We divided participants into two strata:(1)those enrolled within 12 h of onset of symptoms (primary PCI); and (2) those enrolled between 12 h and 14 days after symptom onset (secondary PCI).
Patients undergoing secondary PCI included those who had recurrent ischaemia after initial management or those whose treating doctor chose to pursue an invasivestrategy as part of routine management, even without recurrent ischaemia
Montalescot G, et al. Lancet 2009;373:723
PLATO
TRITON TIMI-38

Ioannidis JP, et al. Am Heart J 2007;154:1065
Death
Is PCI for Late Reperfusion after STEMI Useful?

Primary PCI n=2,438
“Secondary” PCI n=1,044
Clopidogrel Prasugrel Clopidogrel Prasugrel
30 Days
1o – CV death/MI/stroke 8.2% 6.6% 12.3% 6.4%
2o – CV death/MI/UTVR 7.4% 6.8% 12.1% 6.6%
Non-CABG TIMI major bleed 1.5% 1.2% 1.0% 0.5%
15 Months
1o – CV death/MI/stroke 11.6% 10.2% 14.1% 9.6%
2o – CV death/MI/UTVR 11.2% 9.9% 13.9% 9.0%
Non-CABG TIMI major bleed 1.9% 3.1% 2.5% 0.9%
Outcomes in TRITON STEMI Cohort
P = NS
P = NS
P =NS
P = NS
P = NS
P = NS
P = 0.0008
P = 0.0016
P = NS
P = 0.0154
P = 0.009
P = NS
20

Spontaneous (type 1) MIProcedural-Related (types 4-5) MI
Effect of Prasugrel on Spontaneous and Procedural MI in the TRITON TIMI-38
Morrow DA, et al. Circulation. 2009;119:2758
By design of the trial, the majority of periprocedu ral events occurred with revascularization procedur es for the qualifying event performed at the time of randomiza tion. In contrast, the
majority of spontaneous (type 1) MIs occurred after 30 days.
Which K-M curves resemble STEMI curves?

Spontaneous (type 1) MIProcedural-Related (types 4-5) MI
Effect of Prasugrel on Spontaneous and Procedural MI in the TRITON TIMI-38
Morrow DA, et al. Circulation. 2009;119:2758
By design of the trial, the majority of periprocedu ral events occurred with revascularization procedur es for the qualifying event performed at the time of randomiza tion. In contrast, the
majority of spontaneous (type 1) MIs occurred after 30 days.
Which K-M curves resemble STEMI curves?

Long-Term CV Mortality After Procedure-Related or Spontaneous MI in ACS
A Collaborative Analysis of Individual Patient Data From the FRISC, ICTUS, and RITA-3 Trials
Damman P, et al. Circulation. 2012;125:568

%
Periprocedural MI at 30 Daysin the STEMI Cohort of the TRITON TIMI-38
25
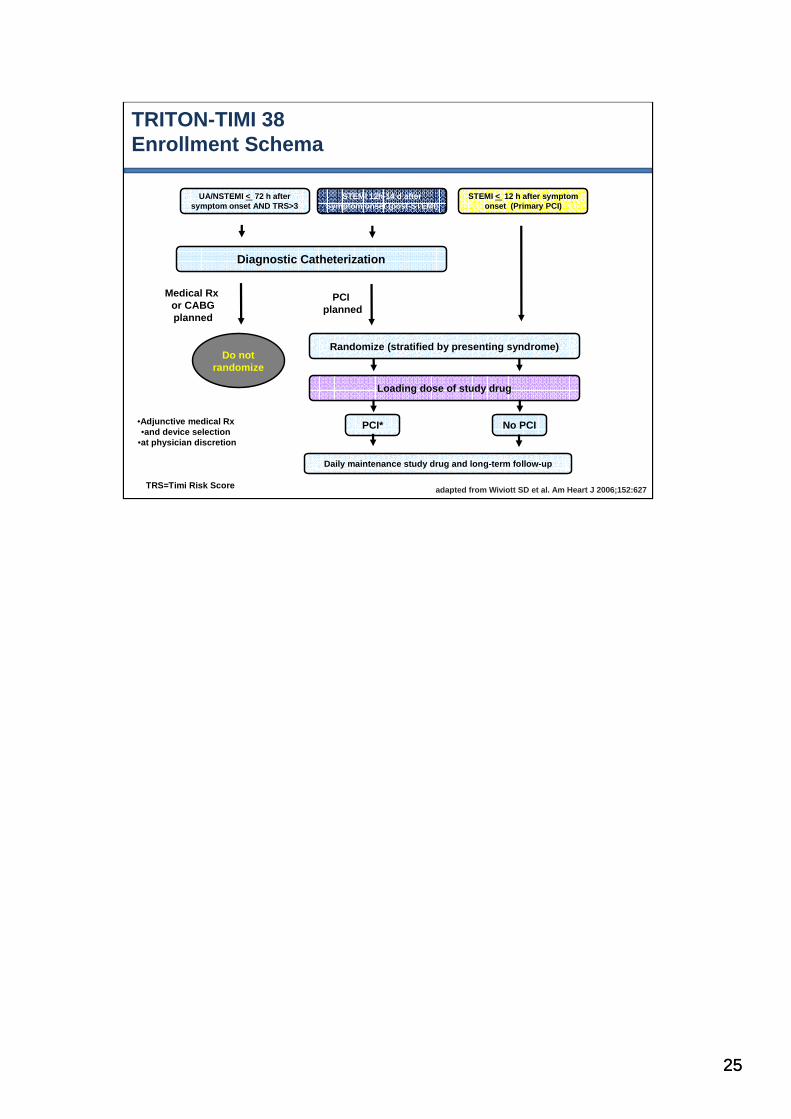
TRITON-TIMI 38 Enrollment Schema
adapted from Wiviott SD et al. Am Heart J 2006;152:62 7TRS=Timi Risk Score
UA/NSTEMI < 72 h after symptom onset AND TRS>3
STEMI 12h-14 d afterSymptom onset (post-STEMI)
STEMI < 12 h after symptom onset (Primary PCI)
Diagnostic Catheterization
Randomize (stratified by presenting syndrome)
Loading dose of study drug
PCI* No PCI
Daily maintenance study drug and long-term follow-u p
Do not randomize
PCI planned
Medical Rx or CABGplanned
•Adjunctive medical Rx •and device selection
•at physician discretion
25

26
TRITON-TIMI 38 Enrollment Schema
adapted from Wiviott SD et al. Am Heart J 2006;152:62 7TRS=Timi Risk Score
UA/NSTEMI < 72 h after symptom onset AND TRS>3
STEMI 12h-14 d afterSymptom onset (post-STEMI)
STEMI < 12 h after symptom onset (Primary PCI)
Diagnostic Catheterization
Randomize (stratified by presenting syndrome)
Loading dose of study drug
PCI* No PCI
Daily maintenance study drug and long-term follow-u p
Do not randomize
PCI planned
Medical Rx or CABGplanned
•Adjunctive medical Rx •and device selection
•at physician discretion
26

TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
2.6% Difference
NNT: 38
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0
p=0.02RRR=21%
ClopidogrelPrasugrel
3% Difference
NNT: 33
p=0.002RRR=32%

TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
2.6% Difference
NNT: 38
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0
p=0.02RRR=21%
ClopidogrelPrasugrel
3% Difference
NNT: 33
p=0.002RRR=32%
TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
3% Difference
NNT: 332.6% Difference
NNT: 38
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0
p=0.02RRR=21%
p=0.002RRR=32%
ClopidogrelPrasugrel

TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
3% Difference
NNT: 332.6% Difference
NNT: 38
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0
p=0.02RRR=21%
p=0.002RRR=32%
ClopidogrelPrasugrel

TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
3% Difference
NNT: 332.6% Difference
NNT: 38
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0
p=0.02RRR=21%
p=0.002RRR=32%
ClopidogrelPrasugrel

TRITON TIMI-38, STEMI CohortPrimary EP (CV death, MI and stroke at 15 months)
3% Difference
NNT: 332.6% Difference
NNT: 38
Montalescot G, et al. Lancet 2009;373:723Time (Days)
5
10
15
00 50 100 150 200 250 300 350 400 450
Pro
port
ion
of p
atie
nts
(%)
9.5
6.5
12.4
10.0
p=0.02RRR=21%
p=0.002RRR=32%
ClopidogrelPrasugrel
Is Triton Supporting the Need for Prolonged Prasugrel in STEMI ???
TRITON TIMI-38, STEMI CohortDo We Need a Fair Comparison with Clopidogrel?
TRITON TIMI-38, STEMI CohortDo We Need a Fair Comparison with Clopidogrel?
There is a solution to
every problem:
your solution, my solution
and the right solution
Plato
The Essence of Plato’s Philosophy

The STEMIWorld

The STEMIWorld
Thrombolysis/Rescue PCI/Pharmacoinvasive
Primary PCI
Secondary PCIConservative RxCABG
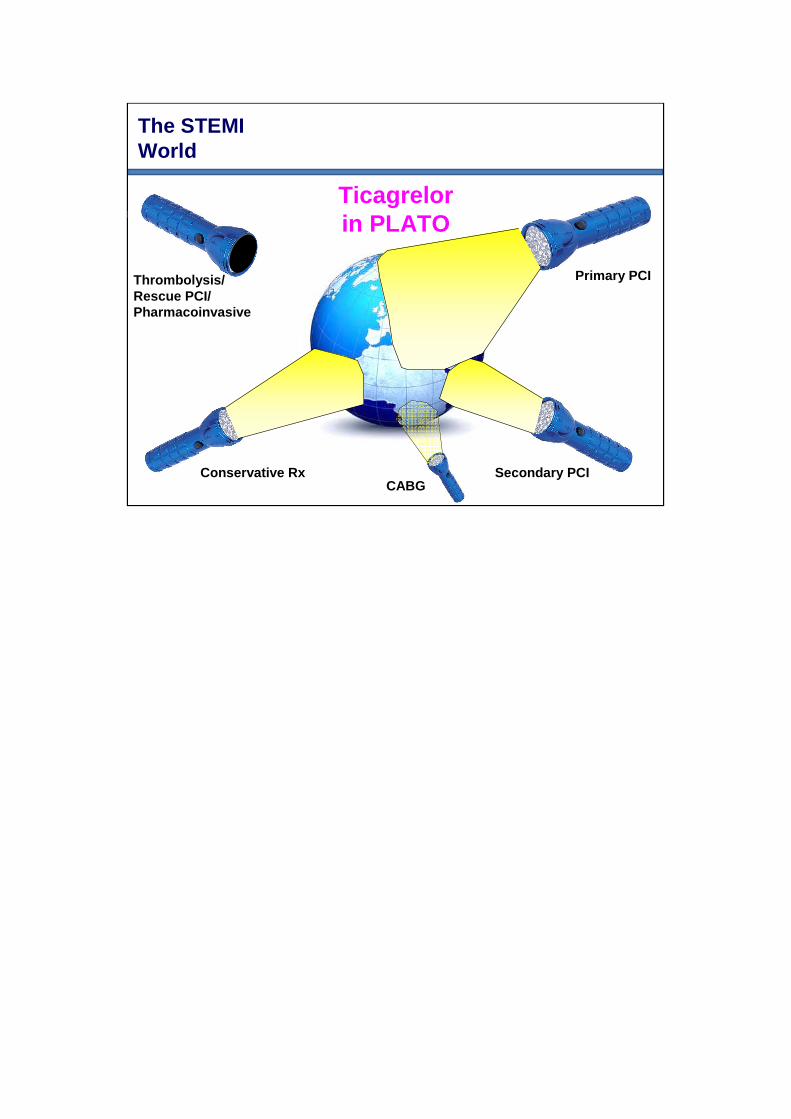
The STEMIWorld
Primary PCI
Secondary PCIConservative Rx
Ticagrelorin PLATO
Thrombolysis/Rescue PCI/Pharmacoinvasive
CABG

The STEMIWorld
Primary PCI
Secondary PCIConservative Rx
Prasugrelin TRITON
Thrombolysis/Rescue PCI/Pharmacoinvasive
CABG

TicagrelorPrasugrel
Clopidogrel
OAT in STEMI