throwing athlete rehabilitation · lateral scapular slidetest superior angle t2/ scapular spinet4/...
TRANSCRIPT

Throwing Athlete Rehabilitation
Brett Schulz LAT/CMSSSport and Spine Physical Therapy

Disclosure
No conflicts to disclose

Throwing Athlete DilemmaThe shoulder must have enough range of motion to allow excessive ER and enough stability to prevent humeral subluxation. There must be a balance between mobility and functional stability.

Muscles acting on scapula Scapulothoracic groupRhomboid majorRhomboid minorLevator scapulaTrapeziusSerratus anterior
Scapulohumeral groupSubscapularisSupraspinatusInfraspinatusTeres MinorTeres MajorDeltoid
Thoracohumeral groupPectoralis MajorLatissimus Dorsi
Extrinsic MusclesCoracobrachialsTricepsBicepsOmohyoid

Scapulothoracic rotationUpward scapular rotators Downward scapular rotators
Upper trapeziusLower trapeziusSerratus anterior
Levator scapulaPectoralis MinorRhomboids
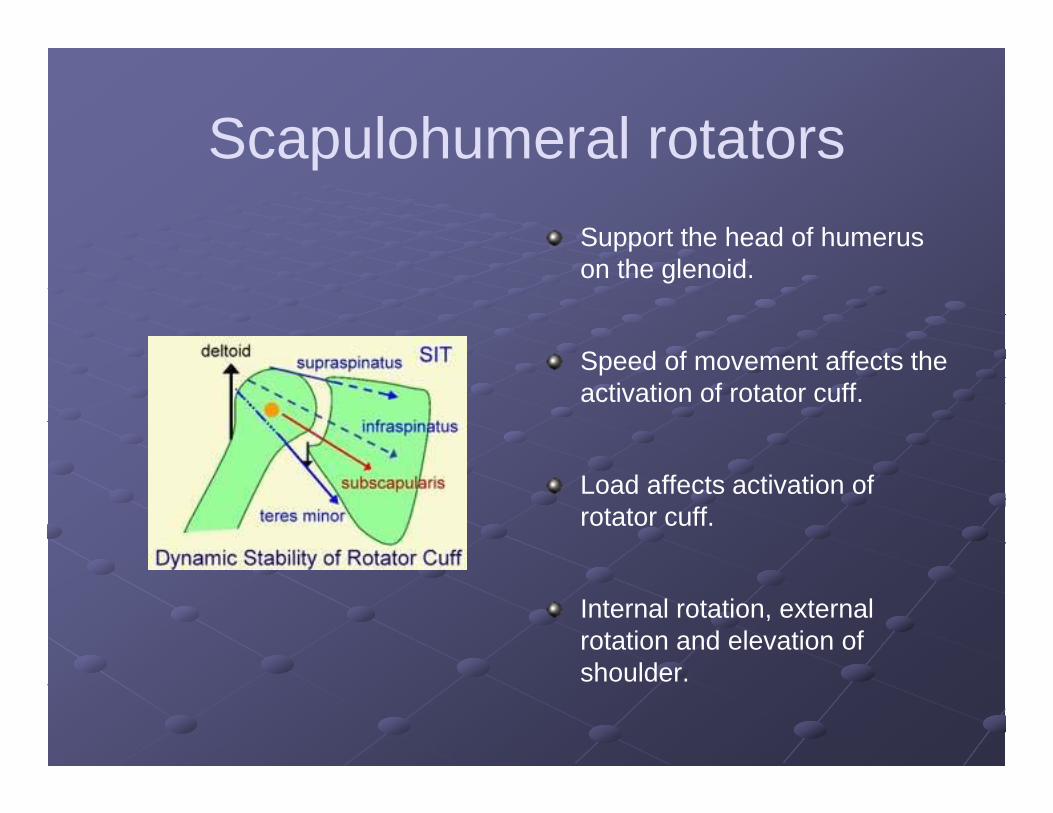
Scapulohumeral rotatorsSupport the head of humerus on the glenoid.
Speed of movement affects the activation of rotator cuff.
Load affects activation of rotator cuff.
Internal rotation, external rotation and elevation of shoulder.

The Rotator Cuff Muscles: SITS
Supraspinatus ABD Infraspinatus ER
Teres minor ER Supscapularis IR
Depress humeral head against glenoid to allow full abduction

So…what causes shoulder pain?
Impingement
Labrum and biceps pathology
A-C joint pathology
Rotator Cuff Injury
InstabilityAmong other things…

Clinical ExamHistory
Single eventRepetitive overloadInstability Does it feel like it’s going to come
out?Catching/Locking
Sport or OccupationPrevious injury/surgery/fx to elbow, wrist, neck, arm, back, knee, anklePrevious treatment
PainAcute ChronicWeaknessAbnormality

Initial Evaluation-ObjectiveElbow/Shoulder ROMTrunk ROM-Thoracic/Lumbar Rotational movement
45° bilaterally should be minimum Flexion/Extension
Important for follow-throughHip ROM Rotational Mobility:
IR= 30°± 5°ER=45°± 7°

Initial Evaluation-Objective(cont.)
Strength Shoulder/Scapular Strength-All planes
Pain or crepitation w/ resisted motion?Assessment at neutral and 90/90 position ER/IR
IR: 35-40% stronger than ER Elbow/Wrist strength Core strength/Stability
VERY important in mechanics Hip/Knee Strength
Base is EVERYTHINGRotational Hip Strength
Special Tests Hawkins-Kennedy, O’Brien’s, Speed’s, etc.

Treatment Phases
Acute Phase Diminish pain and inflammation
Modalities as appropriate-ice,ionto,etc.Mobilization-manual/self stretchModification of activities
Limiting throwing and certain exercisesStretching exercises- with limitation of IR
GIRD-Glenohumeral Internal Rotation DeficitDiagnosed by more than 20-25° loss of IR when compared to other side- Posterior capsule tightness?
Limitation in horizontal adductionSupine Horz. Add w/ IR(Hawkins)

Clinical DiagnosisWhen evaluating an over head
athlete for shoulder or elbow pain it is pertinent to look at the entire kinetic chain.
Faulty biomechanics can produce shoulder and elbow pain which may lead many patients into a rehabilitation setting to seek care to solve this problem.

Scapulothoracic Nerves
1.Spinal Accessory
2.Long Thoracic
3.Dorsal Scapular
1.Trapezius –depression and lateral translation2.Serratus- superior and medial translation3.Rhomboids-depression and lateral translation

Causes of Scapular Dyskinesis
1.Postural2.Nerve3.Lack of muscular/capsular flexibility or
contracture4.Muscular weakness5.Proprioceptive Dysfunction

Learning to throw with proper form…

Special testScapular retraction testPatient is asked to retract both
scapula’s to hold an isometric contraction for 10-15 seconds. Reports of pain with burning in the rhomboid region suggests paresis.
Scapular assistance testUseful in determining if poor
scapular control weakness in the serratus or lower trapezius musculature as a cause for impingement. Examiner will assist patient by pushing laterally and upward on the inferior scapular border to simulate serratus and trapezius. A positive test is indicated by a decrease or abolishment of impingement symptoms.

Lateral Scapular SlideTestsuperior angle T2/ scapular spineT4/ inferior angleT7,8

Inclinometer Test
Testing at rest, 60,90, 120 degrees.From Abduction and flexion at 40 degreesFrom root of scapular spine and posterior lateral acromion.
90 degrees should have about 25 degrees of upward rotation.

Pitch CycleWhen looking at the pitch cycle as a kinetic chain the body can be split up into four segments (1)the hips (2)trunk/core (3)shoulder (4) the arm and ball.These segments must produce what is called angular velocity. Each segment has it’s contribution in this cycle where the hips will rotate first, followed by the trunk, then followed by the shoulder in which the velocity gained from each segment produces momentum to propel the baseball.

Balance PointGluteus mediusQuadsHip mobilityCore strength

Exercise Level 1
Hip AbductionClamHip slides- 4 waysHip hikesTubing squatsCore single/dbl leg extension add upper extremitiesTorso rotations

Exercise level 2
Hip Internal rotationFire HydrantAdvanced ClamLateral Step upSingle leg bridgeDying BugBall touch

Exercise Level 3
Bosu or Tramp balance “T”Single leg Bridge4 way kicksLateral tubing Monster WalksSingle leg chair rise

Exercise Level 4
Torso rotationsSB Single leg balanceSB Alternate arm/legSingle leg STAR

Y-T-W

Exercise
Serratus TrapeziusUpper/Lower
ABC’sSLA scaptionFull canWhizzer
90/90 IR/ERD2Side lying ER
Dynamic wall stabsBall walk outsPush up plusWall dribble

External Rotation
65-67% activation of Infraspinatus occurs in side-lying position. 25% more effective with towel roll.

Prone Series

Throwing Special Drills
Wall DrillProtects thrower from getting too much horizontal abduction in cocking phase.
Towel snapBall Touch from balance point to opposite leg throw
Decel Plyo Toss

Questions?