thrombolysis – what can i do when it goes wrong? complications – recognition & management dr...
TRANSCRIPT

Thrombolysis – What can I do when it goes wrong?
Complications – recognition & management
Dr L Sekaran
Consultant Stroke Physician
Clinical Lead, Beds, Herts & Milton Keynes Stroke Network
14-03-2013
This is an example of an opening slide. Please use other photos if you wish

1930 – discovery of antibiotics1950 – double helix of DNA1970 – an extremely aggressive cancer of melanoma
Events above contributed to the development of thrombolytic agent
CLOT BUSTERS!! - DISCOVERY OFTHROMBOLYTIC THERAPY FOR HEART
ATTACK& STROKE


Alteplase / recombinant tissue plasminogen activator, rtPAUseful Facts
Selective localised fibrinolysis – fibrin dependant activation TPA within the clot. – minimal systemic effects
Fibrinogen – levels decrease 60% at 4 hours, reverts to 80% at 24 hrs
Plasminogen –levels decrease 70% at 4 hrs, reverts to 80% at 24 hrs
Alpha antiplasmin – levels decerease 35% at 4 hrs and reverts to 80% at 24 hours
Clearence of rtPA – 50% in 5 minutes, 80% in 10 mts, completely in 40 mts
Antibody to rtPA - <0.5% patients transiently, NO sustained formation of antibodies
rtPA readministartion in stroke – no data available

Thrombolysis - A lot can go wrongIntracranial bleeding – infarct, normal parenchyma
Brain oedema
ERIS – early recurrent Ischemic strokes
Oro-lingual facial angio-neurotic oedema
Anaphylaxis
Fat / Cholesterol embolism
Systemic bleeding – GI, urological, ENT etc
Reperfusion arrhythmias

Symptomatic ICH
Studies Placebo rtPA P-value
NINDS 3.5% 7.9% 0.006
ECASS II 0.2% 2.4% 0.008
ECASS III 2.2% 5.3% 0.023
SITS-MOST 0.2% 1.9% 0.022
IST-3 1.0% 7.0% 0.0001
ECASS III definition – Symptomatic cerebral haemorrhage was defined as any blood in the brain or intracranially associated with a clinical deterioration of ≥ 4 points of the NIHSS for which the haemorrhage has been identified as the dominating cause of the neurologic deterioration. ECASS II definition – Any intracranial bleed and 4 points or more worsening on the NIHSS score from baseline or the lowest value in the first 7 days, or any haemorrhage leading to death. NINDS definition – A haemorrhage was considered symptomatic if it was not seen on a previous CT scan and there had subsequently been either a suspicion of haemorrhage or any decline in neurologic status. To detect intracranial haemorrhage, CT scans were required at 24 hours and 7 to 10 days after the onset of stroke and when clinical finding suggested haemorrhage. SITS-MOST definition – Local or remote parenchymal haematoma type 2 on the 22- to 36-hour post-treatment imaging scan, combined with a neurologic deterioration of 4 points or more on the NIHSS from baseline, or from the lowest NIHSS value between baseline and 24 hours, or leading to death.
Intracranial bleeding – infarct, normal parenchyma
Actilyse info leaflet from Boehringer-Ingelheim ltd ,NSW, Australia 25/10/2012, IST-3 Lancet 2012;
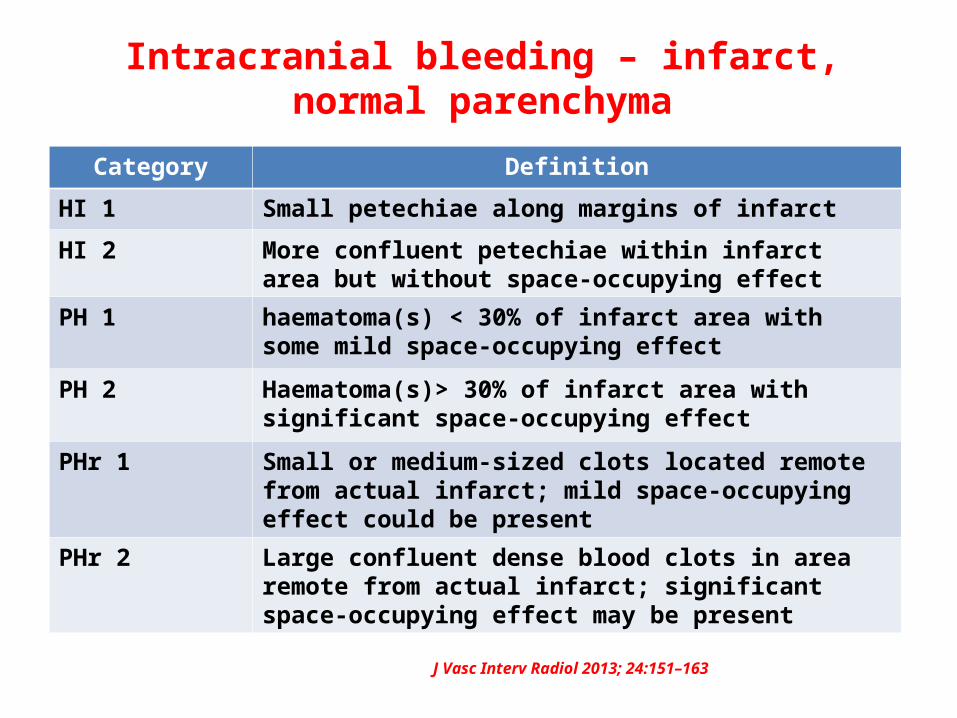
Category Definition
HI 1 Small petechiae along margins of infarct
HI 2 More confluent petechiae within infarct area but without space-occupying effect
PH 1 haematoma(s) < 30% of infarct area with some mild space-occupying effect
PH 2 Haematoma(s)> 30% of infarct area with significant space-occupying effect
PHr 1 Small or medium-sized clots located remote from actual infarct; mild space-occupying effect could be present
PHr 2 Large confluent dense blood clots in area remote from actual infarct; significant space-occupying effect may be present
Intracranial bleeding – infarct, normal parenchyma
J Vasc Interv Radiol 2013; 24:151–163

Intracranial bleeding – infarct, normal parenchyma
Predictors of risk of haemorrhage Hypertension
Chronic atrial fibrillation
Increasing age Increased blood glucose
High NIHSS score
Overweight Early ischaemic change on CT scan
Profound cerebral blood volume reduction Large perfusion/diffusion abnormalities (diffusion volume ≥100ml) Early blood-brain barrier disruption on FLAIR imaging sequences Leukoaraiosis of the deep white matter
Intracranial bleeding – infarct, normal parenchyma
Management;
Stop the infusion – repeat CT, fibrinogen levels, bleeding profile
Platelet infusion,
FFP, Cryoprecipitate 1 unit / 10 kg ( replace fibrinogen )
Antifibrinolytic agent – trenexamic acid 5 gm bolus IV over 15-30 mts

PH 1 HT1 HT2 PH2
PH2

63 yr M pre and post TX scans with Lt side weakness 04-02-2013 & 05-02-2013
PHr 1

Brain Oedema
Brain oedema after Thrombolysis;
Forced Reperfusion injury of already damaged tissue
Less common than after conventional treatment
More severe
Cerebrovasc Dis 1998;8:166–171

Brain Oedema
Management;
Discuss with Neurosurgery
HemicraniectomyAge - 60, time <48 hrs, infarct volume 50% MCA territory, reasonable life expectancy, NIHSS >15
Dexamethasone IV
Hypertonic solutions – IV Mannitol, IV 3% Normal saline

Post -Thrombolysis Brain oedema


During admission:
Day 2: noted to be drowsy, responding but keeping eyes shut
Day 3: intermittently seems alert and drowsy
Day 4: ‘very sleepy’
Day 5: GCS noted to be 10/15 by NS, 14/15 on Drs r/v. Rpt CT r/q
Later in day 5: GCS 12/15 Discussed with RF hospital and transferred

During RF admission:
Day 5: transferred
Day 6: right decompressive craniectomy, taken to ITU post-op
Day 7: extubated, GCS 11/15
Day 8: on ward, continuing dense left hemiplegia
Day 14: transferred back to L&D, GCS 13-14/15

An early Assessment of a TIA case

An early Assessment of a TIA case

Early Recurrent Ischemic Stroke
Rare – 0.6%
IST-3 – 1%
Due to emboli from cardiac / aortic
Usually within the first few hours
Further deterioration after thrombolysis
Neuro-observations / Neurocritical care
Circulation. 2006;114:237-241 IST-3, Lancet ;May 23, 2012DOI:10.1016/S0140-6736(12)60768-5

08-01-2013 14.29 hrs weakness of all 4 limbs and GCS was E-1, M-1, V-1
Intubated & ventilated

09-01-2013 11.49 MRI Brain scans

Oro-lingual angio-neurotic edema
Rare 0.02% after Tx in MI1-5% after Tx in Stroke
Histamine, bradykinin mediated
More common in those who are already on ACEI, less so on ARBs/hereditary complement deficiencies.
Increases C3a, C4a, C5a, C2Increases Bradykinin
Unilateral angioedema - Insular cortex in sympathetic and parasymp. Regulation – autonomic dysregulation leading to angioedema on the hemiparetic side CMAJ,2000;162(9);1281-1284

Oro-lingual angio edema
Management;
Stop infusion
Stop ACEI / ARBs
IV hydrocortisone 100-200 mg
IV diphenhydramine 50 mg
IV Ranitidine 50 mg
Other;RashUrticariaLaryngeal edema
- Respond to above treatment
JNNP,2010;81;1079

AnaphylaxisRare
Anti alteplase antibodies
Transient
Not seen sustained levels
Management;
As for angioedema
Early anaesthetic evaluation, intubation, tracheostomy
Adrenaline avoided unless really required

Fat / Cholesterol embolism
Uncommon after thrombolysisMay be not recognised
Petechial rashSoB, hypoxiaTachycardiaLivedo reticularis
J Emer Trauma shock; 2009; 2(1);29-33
MRI – imaging modality, T2WI
Management;Supportive measuresHigh flow O2IV AlbuminVentilation if needed

Systemic Bleeding
Pre Tx CT Post Tx CT, bleeding PR Caecal Ca

Reperfusion Arrhythmias
Atrial fibrillation
Ventricular arrhythmias
Bradycardia / Heart Blocks
Majority can be managed in Hyperacute Stroke Units

Alteplase – rtPA – useful facts
Intracranial bleeding – infarct / normal parenchyma – devastating in some cases
Brain oedema – fatal in some cases
ERIS – early recurrent Ischemic strokes – rare 0.6 -1.0%
Oro-lingual facial angio-neurotic oedema – 1-5%
Anaphylaxis – uncommon but be prepared
Fat / Cholesterol embolism – unrecognised in this setting
Systemic bleeding – GI, urological, ENT etc
Reperfusion arrhythmias