thriving in a changing environment · thriving in a changing environment ... specialty form” ......
TRANSCRIPT

Millenium Biltmore HotelLos Angeles, CA 90071
21st National AOA Category 1CME Sponsors Conference
January 8-10, 2015
Thriving in a Changing Environment
Sponsored by the American Osteopathic Association

21th National AOA Category 1 CME Sponsors Conference Millennium Biltmore Hotel
Los Angeles, CA 90071
Jan. 8-10, 2015
"Thriving in a Changing Environment"
Timothy Cheslock, DO W. Ashley Hood, DO Conference Chair Conference Co-Chair
Table of Contents Tab
Conference Agenda .................................................................................................................................. A Conference Faculty ................................................................................................................................... B Conference Attendees ............................................................................................................................. C Presentation of Materials The Emerging CME Environment ........................................................................................................ D Alejandro Aparicio, MD, Director, Division of Continuing Physician Professional Development, American Medical Association Understanding the AAFP, AMA PRA Category 1™ and AOA Credit Systems ............................ E Jeffrey S. Grove, DO, Chair, Council on CME, American Osteopathic Association Alejandro Aparicio, MD, Director, Division of Continuing Physician Professional Development, American Medical Association CME Update – AOA CME Guide and AOA Accreditation Requirements .................................... F Timothy Cheslock, DO, Member, Council on CME, American Osteopathic Association Delivery of Quality CME Programs – Panel: Needs Assessment ..................................................... G James E. Preston, DO, Vice Chair, Council on CME, American Osteopathic Association

Delivery of Quality CME Programs – Panel: Outcome Measures .................................................... H W. Ashley Hood, DO, Member, Council on CME, American Osteopathic Association Ed Williams, PhD, Executive Director of Louisiana Osteopathic Medical Association and Mississippi Osteopathic Medical Association Implications of Physician Payments Sunshine Act Final Rule ........................................................... I Ray Quintero, Vice President, Government Relations, American Osteopathic Association Washington Office How to Get a Perfect Score on Your Document Survey ................................................................... J W. Ashley Hood, DO, Member, Council on CME, American Osteopathic Association How to Properly Report CME Specialty Credits for your CME Programs Using the “Applicable Credits by Specialty Form” .......................................................................................................................................... K Stephen M. Scheinthal, DO, Chair, Bureau of Osteopathic Specialists, American Osteopathic Association
Delivering Quality Education via the Internet: Live, Virtual and Enduring Materials Joshua S. Coren, DO, MBA, Vice Chair & Associate Professor, Department of Family Medicine Rowan University School of Osteopathic Medicine ......................................................................................... L State Mandated CME Requirements for Relicensure - Panel ............................................................. M Nick Schilligo, MS, Associate Vice President, State Government Affairs, AOA Geraldine T. O’Shea, DO, President, AAOE & AOA Board Member Ronald R. Burns, DO, Past Chair, Florida Board of Osteopathic Medicine & AOA Board Member James Griffin, DO, Member, Rhode Island Board of Medical Licensure and Discipline .................................. N Materials of Interest Members of the AOA Council on CME Handbook of the Council on CME List of AOA Accredited Category 1 CME Sponsors AOA Accreditation Requirements for Category 1 CME Sponsors Continuing Medical Education – 2013-2015 Guide for Osteopathic Physicians AOA Specialty Credit Limitations – November 21 2014 AOA Category 1-A CME Credit for Outcomes Measurement for AOA Category 1 CME Programs Information JAOA – AOA Continuing Medical Education

21th National AOA Category 1 CME Sponsors Conference Millennium Biltmore Hotel
Los Angeles, CA 90071
Jan. 8-10, 2015
"Thriving in a Changing Environment"
Timothy Cheslock, DO W. Ashley Hood, DO Conference Chair Conference Co-Chair
Thursday, Jan. 8, 2015 – Emerald Ballroom
1:30 – 3:00 p.m. Registration CME Sponsors Conference – Emerald Galleria
3:00 – 3:15 p.m. Welcome
Jeffrey S. Grove, DO, Chair, Council on Continuing Medical Education Robert S. Juhasz, DO, President, American Osteopathic Association
3:15 – 4:00 p.m. The Emerging CME Environment
Alejandro Aparicio, MD, FACP, Director, Division of Continuing Physician Professional Development American Medical Association
4:00 – 4:45 p.m.
Understanding the AAFP, AMA PRA Category 1™ and AOA Credit Systems Jeffrey S. Grove, DO, Chair, Council on CME, American Osteopathic Association &
Alejandro Aparicio, MD, Director, Division of Continuing Physician Professional Development American Medical Association
4:45 – 5:00 p.m. Questions & Answers
5:00 – 5:30 p.m. CME Update – AOA CME Guide and AOA Accreditation Requirements
Timothy Cheslock, DO, Member, Council on CME, American Osteopathic Association
5:30 – 6:30 p.m. Welcome Reception – Crystal Ballroom
January 5, 2014
CME Sponsors Conference – Jan. 8-10, 2015 Program Agenda Page 2 of 3
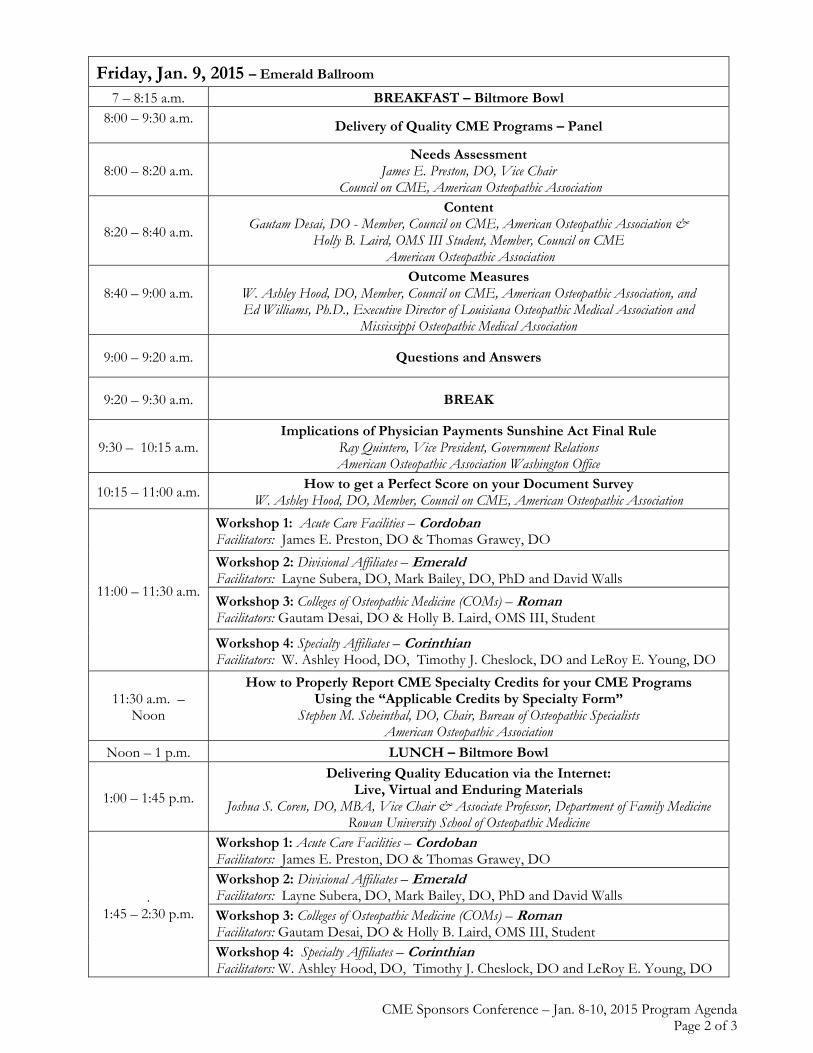
Friday, Jan. 9, 2015 – Emerald Ballroom 7 – 8:15 a.m. BREAKFAST – Biltmore Bowl
8:00 – 9:30 a.m.
Delivery of Quality CME Programs – Panel
8:00 – 8:20 a.m. Needs Assessment
James E. Preston, DO, Vice Chair Council on CME, American Osteopathic Association
8:20 – 8:40 a.m.
Content Gautam Desai, DO - Member, Council on CME, American Osteopathic Association &
Holly B. Laird, OMS III Student, Member, Council on CME American Osteopathic Association
8:40 – 9:00 a.m.
Outcome Measures W. Ashley Hood, DO, Member, Council on CME, American Osteopathic Association, and Ed Williams, Ph.D., Executive Director of Louisiana Osteopathic Medical Association and
Mississippi Osteopathic Medical Association
9:00 – 9:20 a.m. Questions and Answers
9:20 – 9:30 a.m. BREAK
9:30 – 10:15 a.m. Implications of Physician Payments Sunshine Act Final Rule
Ray Quintero, Vice President, Government Relations American Osteopathic Association Washington Office
10:15 – 11:00 a.m. How to get a Perfect Score on your Document Survey
W. Ashley Hood, DO, Member, Council on CME, American Osteopathic Association
11:00 – 11:30 a.m.
Workshop 1: Acute Care Facilities – Cordoban Facilitators: James E. Preston, DO & Thomas Grawey, DO
Workshop 2: Divisional Affiliates – Emerald Facilitators: Layne Subera, DO, Mark Bailey, DO, PhD and David Walls
Workshop 3: Colleges of Osteopathic Medicine (COMs) – Roman Facilitators: Gautam Desai, DO & Holly B. Laird, OMS III, Student
Workshop 4: Specialty Affiliates – Corinthian Facilitators: W. Ashley Hood, DO, Timothy J. Cheslock, DO and LeRoy E. Young, DO
11:30 a.m. – Noon
How to Properly Report CME Specialty Credits for your CME Programs Using the “Applicable Credits by Specialty Form”
Stephen M. Scheinthal, DO, Chair, Bureau of Osteopathic Specialists American Osteopathic Association
Noon – 1 p.m. LUNCH – Biltmore Bowl
1:00 – 1:45 p.m.
Delivering Quality Education via the Internet: Live, Virtual and Enduring Materials
Joshua S. Coren, DO, MBA, Vice Chair & Associate Professor, Department of Family Medicine Rowan University School of Osteopathic Medicine
. 1:45 – 2:30 p.m.
Workshop 1: Acute Care Facilities – Cordoban Facilitators: James E. Preston, DO & Thomas Grawey, DO Workshop 2: Divisional Affiliates – Emerald Facilitators: Layne Subera, DO, Mark Bailey, DO, PhD and David Walls Workshop 3: Colleges of Osteopathic Medicine (COMs) – Roman Facilitators: Gautam Desai, DO & Holly B. Laird, OMS III, Student Workshop 4: Specialty Affiliates – Corinthian Facilitators: W. Ashley Hood, DO, Timothy J. Cheslock, DO and LeRoy E. Young, DO
CME Sponsors Conference – Jan. 8-10, 2015 Program Agenda Page 3 of 3
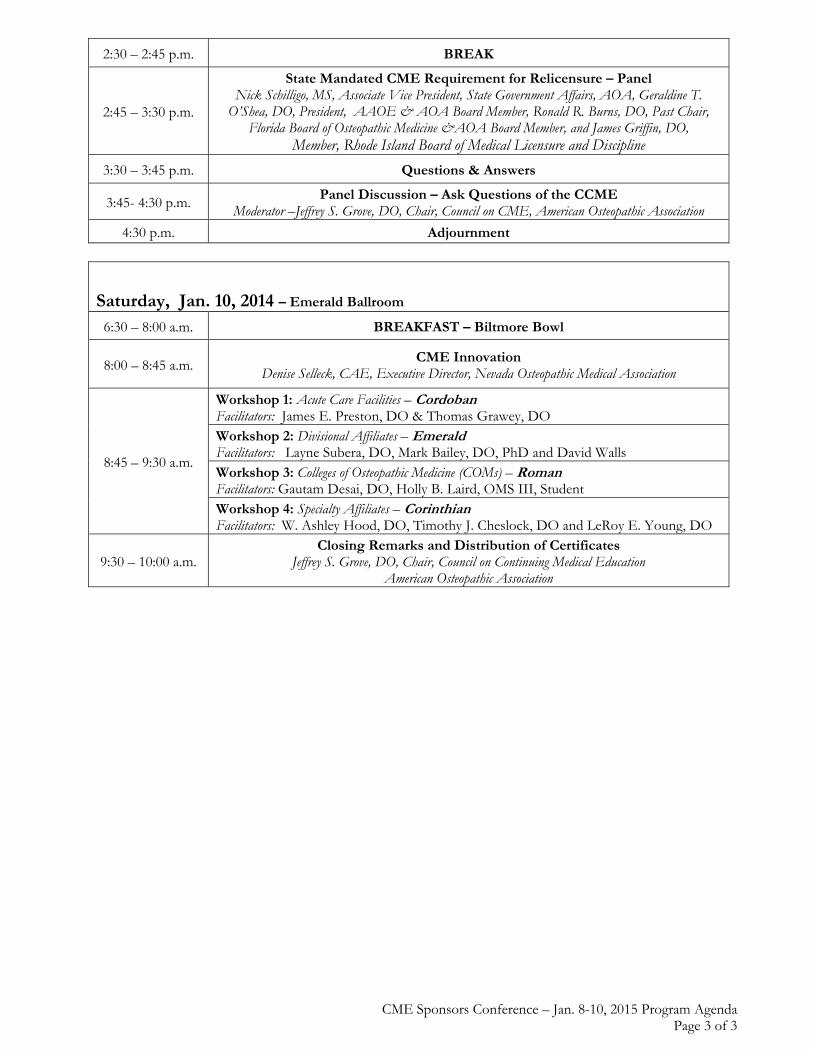
2:30 – 2:45 p.m. BREAK
2:45 – 3:30 p.m.
State Mandated CME Requirement for Relicensure – Panel Nick Schilligo, MS, Associate Vice President, State Government Affairs, AOA, Geraldine T.
O’Shea, DO, President, AAOE & AOA Board Member, Ronald R. Burns, DO, Past Chair, Florida Board of Osteopathic Medicine &AOA Board Member, and James Griffin, DO,
Member, Rhode Island Board of Medical Licensure and Discipline
3:30 – 3:45 p.m. Questions & Answers
3:45- 4:30 p.m. Panel Discussion – Ask Questions of the CCME
Moderator –Jeffrey S. Grove, DO, Chair, Council on CME, American Osteopathic Association
4:30 p.m. Adjournment
Saturday, Jan. 10, 2014 – Emerald Ballroom 6:30 – 8:00 a.m. BREAKFAST – Biltmore Bowl
8:00 – 8:45 a.m. CME Innovation
Denise Selleck, CAE, Executive Director, Nevada Osteopathic Medical Association
8:45 – 9:30 a.m.
Workshop 1: Acute Care Facilities – Cordoban Facilitators: James E. Preston, DO & Thomas Grawey, DO Workshop 2: Divisional Affiliates – Emerald Facilitators: Layne Subera, DO, Mark Bailey, DO, PhD and David Walls Workshop 3: Colleges of Osteopathic Medicine (COMs) – Roman Facilitators: Gautam Desai, DO, Holly B. Laird, OMS III, Student Workshop 4: Specialty Affiliates – Corinthian Facilitators: W. Ashley Hood, DO, Timothy J. Cheslock, DO and LeRoy E. Young, DO
9:30 – 10:00 a.m. Closing Remarks and Distribution of Certificates
Jeffrey S. Grove, DO, Chair, Council on Continuing Medical Education American Osteopathic Association

21th National AOA Category 1 CME Sponsors Conference Millennium Biltmore Hotel
Los Angeles, CA 90071
Jan. 8-10, 2015
"Thriving in a Changing Environment"
Timothy Cheslock, DO W. Ashley Hood, DO Conference Chair Conference Co-Chair
Conference Faculty Jeffrey S. Grove, DO
A love of science and medicine runs in the family of Dr. Grove – his father, grandfather and uncle all practiced osteopathic family medicine. After completing his internship and family practice residency at Sun Coast Hospital in 1993, Dr. Grove joined Sun Coast Family Medical Associates. He is a board certified in family medicine with added certification in geriatrics. Dr. Grove is also board-certified and a Fellow of the American Board of Quality Assurance and Utilization Review Physicians. Graduated from Nova Southeastern University College of Osteopathic Medicine where he is a Past-President of the NSU-COM Alumni Association. He currently serves on the Board of Governors for the NSU Health Professions Division. He was selected to receive the 2004 Distinguished Alumni Achievement Award. He further was awarded the 2004 Alumni of the Year Award for the entire Nova Southeastern University. Active in the American College of Osteopathic Family Physicians, the youngest member ever to be elected to the National ACOFP Board of Governors being elected in March 2004. He was inaugurated as the 60th President in March 2013. He is a Past-President of the Florida Society ACOFP and currently serves as the Florida Society Delegate Chairman for the ACOFP Congress of Delegates. Dr. Grove received his “Fellow Award” from the ACOFP in 2002. In 2003 he was awarded “Physician of the Year” for the State of Florida. He was awarded the Distinguished Service Award in 2009. Has served on the American Osteopathic Association Bureau of State Government Affairs and continues to serve on the Council on Continuing Medical Education where he serves as Chairman. He is a member of the American Osteopathic Association House of Delegates for the State of Florida. Dr. Grove served as President of the Florida Osteopathic Medical Association from 2011- 2012. He also serves as a member of the state’s Legislative Committee. Locally, he completed two terms as President of the Pinellas County Osteopathic Medical Society.

Faculty to the 21th National AOA Category 1 CME Sponsors Conference Page 2
Dr. Grove was awarded “Physician of the Year” for Pinellas County in 2002 – 2003 and the “Distinguished Service Award” in 2007. He has served on the Board of Trustees for St. Paul’s School, a member of the Anona First United Methodist Church, and has two children, Garrett and Victoria. Robert S. Juhasz, DO,
An AOA board-certified internist from Concord Township, Ohio, is the 118th president of the AOA. Dr. Juhasz serves as president of Cleveland Clinic’s South Pointe Hospital in Warrensville Heights, Ohio, where he worked his way up from an after-school job as a dishwasher. “Out of all the positions I held at the hospital, I really enjoyed being an orderly because it was an opportunity to help patients meet their basic needs and I always felt the appreciation of not only the patients but their families as well,” says Dr. Juhasz. “Many of my mentors taught me that we could improve health care by treating patients the way we would want ourselves and our families to be treated. As AOA president, I want to ensure DOs have the resources they need to provide the best care for their patients.” One of his goals as president is to facilitate more osteopathic medical research, which, he says, would provide DOs fact-based research to communicate their distinctiveness to their patients, their colleagues and the world. Alejandro Aparicio, MD
Dr. Aparicio is the Director of Medical Education Programs at the American Medical Association, encompassing the Division of Continuing Physician Professional Development, which he led from 2004 until 2014. Prior to arriving at the AMA he was Director of Medical Education, Designated Institutional Official and Associate Medical Director at Advocate Illinois Masonic Medical Center. He is Board Certified in Internal Medicine and a Fellow of the American College of Physicians. In 2004 he was appointed by the President of the United States to the 2005 White House Conference on Aging Policy Committee and served as co-chair of its Health Care Subcommittee. Dr. Patricio co-chairs or serves on several committees at the University of Illinois at Chicago College of Medicine where he holds appointments as Clinical Assistant Professor of Medicine and Assistant Professor of Medical Education. He cared for patients in a multispecialty practice in the north side of Chicago for nearly 20 years and now continues to practice medicine as a volunteer physician at Community Health, a clinic which provides free health care to patients in need in the Chicago. Tim Cheslock, DO Doctor Cheslock is the Chair of the 21st CME Sponsors Conference, and Emergency Medicine Physician currently working at Waterman Hospital in Tavares, FL. He is a member of Florida Emergency Physicians. His undergraduate education was from King’s College in Wilkes-Barre PA as a Physician Assistant. After 7 years of clinical practice he returned to medical school. He graduated from Lake Erie College of Osteopathic Medicine in 2007 and completed an Emergency Medicine Residency at Saint Vincent Health Center in Erie, PA. He is board certified in Emergency Medicine by the AOBEM. Tim has been a member of the CCME for the last 9 years, currently serving as the Uniformed Services representative. He is a member of the ACOEP and serves on the EMS committee and is Chair of the Communications committee. He is currently a member of the FL Army National Guard with over 15 years of military service and completed a tour to Afghanistan in 2011. He and his wife Stephanie have two children, Abigail and Claire. In his free time he enjoys the outdoors and time with his family.
Faculty to the 21th National AOA Category 1 CME Sponsors Conference Page 3
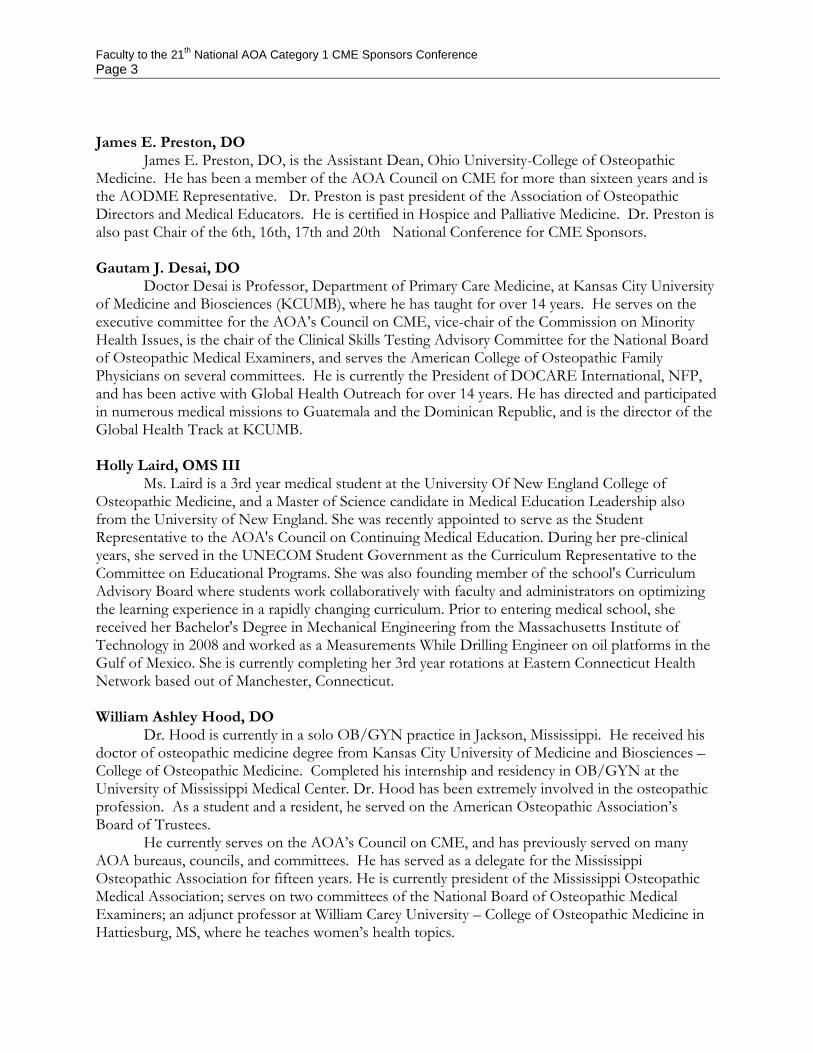
James E. Preston, DO
James E. Preston, DO, is the Assistant Dean, Ohio University-College of Osteopathic Medicine. He has been a member of the AOA Council on CME for more than sixteen years and is the AODME Representative. Dr. Preston is past president of the Association of Osteopathic Directors and Medical Educators. He is certified in Hospice and Palliative Medicine. Dr. Preston is also past Chair of the 6th, 16th, 17th and 20th National Conference for CME Sponsors.
Gautam J. Desai, DO
Doctor Desai is Professor, Department of Primary Care Medicine, at Kansas City University of Medicine and Biosciences (KCUMB), where he has taught for over 14 years. He serves on the executive committee for the AOA’s Council on CME, vice-chair of the Commission on Minority Health Issues, is the chair of the Clinical Skills Testing Advisory Committee for the National Board of Osteopathic Medical Examiners, and serves the American College of Osteopathic Family Physicians on several committees. He is currently the President of DOCARE International, NFP, and has been active with Global Health Outreach for over 14 years. He has directed and participated in numerous medical missions to Guatemala and the Dominican Republic, and is the director of the Global Health Track at KCUMB. Holly Laird, OMS III
Ms. Laird is a 3rd year medical student at the University Of New England College of Osteopathic Medicine, and a Master of Science candidate in Medical Education Leadership also from the University of New England. She was recently appointed to serve as the Student Representative to the AOA's Council on Continuing Medical Education. During her pre-clinical years, she served in the UNECOM Student Government as the Curriculum Representative to the Committee on Educational Programs. She was also founding member of the school's Curriculum Advisory Board where students work collaboratively with faculty and administrators on optimizing the learning experience in a rapidly changing curriculum. Prior to entering medical school, she received her Bachelor's Degree in Mechanical Engineering from the Massachusetts Institute of Technology in 2008 and worked as a Measurements While Drilling Engineer on oil platforms in the Gulf of Mexico. She is currently completing her 3rd year rotations at Eastern Connecticut Health Network based out of Manchester, Connecticut. William Ashley Hood, DO Dr. Hood is currently in a solo OB/GYN practice in Jackson, Mississippi. He received his doctor of osteopathic medicine degree from Kansas City University of Medicine and Biosciences – College of Osteopathic Medicine. Completed his internship and residency in OB/GYN at the University of Mississippi Medical Center. Dr. Hood has been extremely involved in the osteopathic profession. As a student and a resident, he served on the American Osteopathic Association’s Board of Trustees.
He currently serves on the AOA’s Council on CME, and has previously served on many AOA bureaus, councils, and committees. He has served as a delegate for the Mississippi Osteopathic Association for fifteen years. He is currently president of the Mississippi Osteopathic Medical Association; serves on two committees of the National Board of Osteopathic Medical Examiners; an adjunct professor at William Carey University – College of Osteopathic Medicine in Hattiesburg, MS, where he teaches women’s health topics.

Faculty to the 21th National AOA Category 1 CME Sponsors Conference Page 4
Also serves as a preceptor for osteopathic medical students during their third and fourth year. Serves on many hospital committees at River Oaks Hospital in Jackson, Mississippi and spoken for various organizations on issues of women’s health. Ed Williams, PhD
Doctor Williams earned his BS from Louisiana Tech University followed by the MS and PhD degrees from Texas A & M University. He taught undergraduate and graduate level zoology in the Department of Biological Sciences at Delta State University in Cleveland, MS for 28 years before retiring in 2004. While there, Ed served as Chief Pre-Health Advisor and Chair of the Department. He advised many students into osteopathic medical schools during his academic career and has continued that effort since retirement. After retiring in 2004, Dr. Williams became the first full-time Executive Director of the then non-operational Louisiana Osteopathic Medical Association – a position he still holds today. He also began working for the Mississippi Osteopathic Medical Association as its Director of Education in 2007 and has served as its Executive Director since 2009. Ray Quintero
Ray Quintero currently serves as Vice President of Government Relations at the American Osteopathic Association (AOA) in Washington, DC. In this capacity he oversees the AOA’s diverse government relations operation, which includes the legislative, regulatory, advocacy, and political operations of the organization. Prior to his current position, he was the AOA’s Director of Government Relations from 2012-2013, Deputy Director of Government Relations from 2011-2012, and Director of Congressional Affairs from 2006-2008. During his tenure he has led the association’s efforts on many issues, including Medicare physician payment, medical liability reform, graduate medical education, delivery system reform, and efforts to implement new delivery models for physicians under both public and private systems. He has also represented the American College of Osteopathic Family Physicians (ACOFP) as their Director of Government Relations. Quintero is well versed in the diverse issues of health care policy. He is actively engaged in numerous multi-stakeholder coalitions aimed at improving our nation’s health care delivery and financing systems, and is involved in health care workforce discussions. He previously held government relations positions at Merck Pharmaceuticals and the Blue Cross Blue Shield Association. Quintero was also Vice President of Strategic Alliances at 720 Strategies where he provided grassroots consultation to a variety of health care clients. He began his career in health care government relations as a lobbyist in the Health and Life Sciences practice of B&D Consulting. Stephen M. Scheinthal, DO
Stephen M. Scheinthal, DO, dFACN, earned his bachelor’s degree from Brandeis University in Waltham, MA. He completed his Doctor of Osteopathy degree from the University of Medicine and Dentistry of New Jersey-School of Osteopathic Medicine (UMDNJ-SOM) in Stratford, New Jersey, where he completed his internship, psychiatry residency, and a geriatric psychiatry fellowship. Presently he is the Associate Director and Chief, Geriatric Behavioral Health at New Jersey Institute for Successful Aging – Rowan University School of Osteopathic Medicine, where he provides outpatient and long-term care services to the elderly. He is a distinguished Fellow of the American College of Osteopathic Neurology and Psychiatry and the College of Physicians of Philadelphia. He is the recipient of a Geriatric Academic Career Award from the Health Resources Service Administration and is a member of the first Costin Institute class. Doctor Scheinthal currently serves as the Chair of the AOA - Bureau of Osteopathic Specialists.
Faculty to the 21th National AOA Category 1 CME Sponsors Conference Page 5
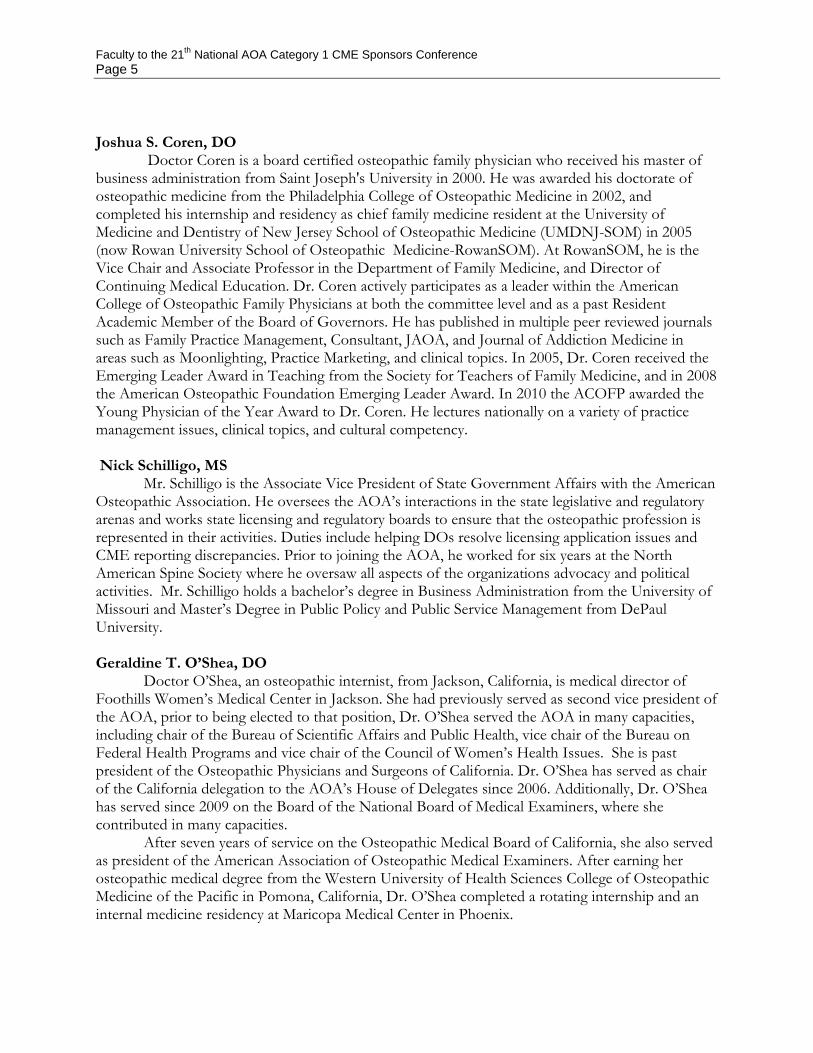
Joshua S. Coren, DO
Doctor Coren is a board certified osteopathic family physician who received his master of business administration from Saint Joseph's University in 2000. He was awarded his doctorate of osteopathic medicine from the Philadelphia College of Osteopathic Medicine in 2002, and completed his internship and residency as chief family medicine resident at the University of Medicine and Dentistry of New Jersey School of Osteopathic Medicine (UMDNJ-SOM) in 2005 (now Rowan University School of Osteopathic Medicine-RowanSOM). At RowanSOM, he is the Vice Chair and Associate Professor in the Department of Family Medicine, and Director of Continuing Medical Education. Dr. Coren actively participates as a leader within the American College of Osteopathic Family Physicians at both the committee level and as a past Resident Academic Member of the Board of Governors. He has published in multiple peer reviewed journals such as Family Practice Management, Consultant, JAOA, and Journal of Addiction Medicine in areas such as Moonlighting, Practice Marketing, and clinical topics. In 2005, Dr. Coren received the Emerging Leader Award in Teaching from the Society for Teachers of Family Medicine, and in 2008 the American Osteopathic Foundation Emerging Leader Award. In 2010 the ACOFP awarded the Young Physician of the Year Award to Dr. Coren. He lectures nationally on a variety of practice management issues, clinical topics, and cultural competency. Nick Schilligo, MS
Mr. Schilligo is the Associate Vice President of State Government Affairs with the American Osteopathic Association. He oversees the AOA’s interactions in the state legislative and regulatory arenas and works state licensing and regulatory boards to ensure that the osteopathic profession is represented in their activities. Duties include helping DOs resolve licensing application issues and CME reporting discrepancies. Prior to joining the AOA, he worked for six years at the North American Spine Society where he oversaw all aspects of the organizations advocacy and political activities. Mr. Schilligo holds a bachelor’s degree in Business Administration from the University of Missouri and Master’s Degree in Public Policy and Public Service Management from DePaul University. Geraldine T. O’Shea, DO
Doctor O’Shea, an osteopathic internist, from Jackson, California, is medical director of Foothills Women’s Medical Center in Jackson. She had previously served as second vice president of the AOA, prior to being elected to that position, Dr. O’Shea served the AOA in many capacities, including chair of the Bureau of Scientific Affairs and Public Health, vice chair of the Bureau on Federal Health Programs and vice chair of the Council of Women’s Health Issues. She is past president of the Osteopathic Physicians and Surgeons of California. Dr. O’Shea has served as chair of the California delegation to the AOA’s House of Delegates since 2006. Additionally, Dr. O’Shea has served since 2009 on the Board of the National Board of Medical Examiners, where she contributed in many capacities.
After seven years of service on the Osteopathic Medical Board of California, she also served as president of the American Association of Osteopathic Medical Examiners. After earning her osteopathic medical degree from the Western University of Health Sciences College of Osteopathic Medicine of the Pacific in Pomona, California, Dr. O’Shea completed a rotating internship and an internal medicine residency at Maricopa Medical Center in Phoenix.

Faculty to the 21th National AOA Category 1 CME Sponsors Conference Page 6
Ronald R. Burns, DO
An AOA board-certified family physician, Dr. Burns serves on the board of the National Board of Osteopathic Medical Examiners and is a member of the American College of Osteopathic Family Physicians. He has also served the Florida Osteopathic Medical Association (FOMA) in many capacities, including being president from 2004-2005. Dr. Burns has been an active member of the AOA Board of Trustees since 2007. He served as chair of the Department of Business Affairs and received FOMA’s Physician of the Year award in 2002, as well as its Distinguished Service Award in 2007.
Dr. Burns completed his osteopathic medicine degree from what is now the Ohio University Heritage College of Osteopathic Medicine in Athens. Following completion of his degree, he completed his postdoctoral medical training at the Doctors Hospital of Stark County in Massillon, Ohio, and the Florida Hospital – East Orlando James Griffin, DO
Doctor Griffin received his DO degree from the University of Health Sciences; College of Osteopathic Medicine in Kansas City, MO, completed a rotating Osteopathic Internship at Union Hospital in Union, NJ and residencies programs in Internal Medicine and Anesthesiology at Albany Medical Center in Albany, NY. He is currently in private practice anesthesiology at South County Hospital in Wakefield, RI and serving his third term on the Rhode Island Board of Medical Licensure & Discipline. He is a member of the AAOE, the AOA Bureau of State Government Affairs Committee, the Federation of State Medical Boards Ethics, and Professionalism Committee. Denise Selleck, CAE
Denise Selleck, CAE is currently responsible for daily management of programs, assets and staff of the Nevada Osteopathic Medical Association. She is a full time lobbyist for ongoing legislative agenda. Ms. Selleck develops, administers and designs continuing medical education programs. She serves as liaison with local, state and national organizations. She also serves on the American Osteopathic Association Counsel on Continuing Education for 3- years. Ms. Selleck is a Certified Association Executive since January 2007. Her current memberships include the American Osteopathic Sate Executive Directors, the American Society of Association Executives and the Nevada Society of Association Executives. Ms. Selleck's interests are gardening, travel, hiking/kayaking and her dog.

1
21th National AOA Category 1 CME Sponsors Conference Millennium Biltmore Hotel
Los Angeles, CA 90071
Jan. 8-10, 2015
"Thriving in a Changing Environment"
ATTENDANCE
Mark Bailey, DO, PhD Member, CCME John Becher, DO AOA President-Elect Chris Bowles Missouri Association of Osteo Phys & Surgeons William Burke, DO, FACOFP Chair, Dept of Educ Affairs, AOA BOT Timothy Cheslock, DO Member, CCME Joshua Coren, DO, MBA Kennedy University Hospital Gautam Desai, DO Member, CCME Stephen Eddy, DO, MPH Oklahoma State University
Thomas Grawey, DO Member, CCME Jeffrey Grove, DO Chair, Council on CME W. Ashley Hood, DO Member, CCME Robert S. Juhasz, DO AOA President Holly Laird, OMS III Member, CCME Geraldine O'Shea, DO Vice-Chair, Dept of Educ Affairs, AOA BOT James Preston, DO Vice Chair, CCME Delores Rodgers Secretary, CCME Layne Subera, DO Member, CCME

2
David Walls, DO Member, CCME Ed Williams, PhD Louisiana Osteopathic Medical Association LeRoy Young, DO, RPH Member, CCME Alejandro Aparicio, MD American Medical Association Robert Burns, DO AOA Board of Trustees Ray Quintero AOA Washington Office Steven Scheinthal, DO Chair, AOA Bureau of Osteopathic Specialists Nick Schilligo, MS American Osteopathic Association Denise Selleck, CAE Nevada Osteopathic Medical Association Pouya Bahrami, DO Essential Medicine Clinic Debra L. Bailey, CMP AOCOO-HNS Steven Barag, DO, FACOFP ACOFP-CA Jessica Bartolone Affinity Medical Center Donna Barton South Pointe Hospital Jan Baum, MA A. T. Still University
Karl Baur, CMP, CGMP Osteopathic Physicians and Surgeons of California Lisa J. Belliveau Pinellas County Osteopathic Medical Society Greg Bergman, DO South Carolina Osteopathic Medical Association Lisa Bohen Carson City Hospital Robert Boorstein, DO Health & Wellness Medicine Brian Bowles Missouri Association of Osteo Phys & Surgeons Devin Anna Bradford Tennessee Osteopathic Medical Association Jo Brogus Rocky Vista University Melissa Budd Michigan Osteopathic Association Jon Burdzy, DO Southwest Florida Osteopathic Medical Association Cyndi Canning Oklahoma State University-COM Sara Carson MSU College of Osteopathic Medicine Brenda Chezek Kansas City University of Medicine and Biosciences Kara Classens Munson Medical Center

3
Samantha Clinton Campbell University, School of Osteopathic Medicine Jennifer Colwell American College of Osteopathic Surgeons Valbona Cook, B.A. St. John Providence Macomb-Oakland Hospital Ashleigh Day Tucson Osteopathic Medical Foundation Meghan Dipiazza MSU College of Osteopathic Medicine Brenda Dohman Chicago College of Osteopathic Medicine Dennis Dowling, MA, DO, FAAO NBOME Tom Drabek, MPA Sparrow Hospital Sidney Dunn The Cranial Academy, Inc. Jeff Ehmke Capital Region Medical Center Karen Ehmke Capital Region Medical Center Bernadette Emig Memorial Hospital Robert Fernandez, DO, MPH Westchester General Hospital Walter Flesner III, D.O. District XI, F.O. M. A. Andrew Floyd, CMP-HC FSACOFP
Aleesa Foltz UPMC Horizon Suzanne Frederick Utah Osteopathic Association Celia Freeman, MBA Pacific Northwest University of Health Sciences Cathy Galligan American Osteopathic Association Mary Garcia Michigan Osteopathic Neuropsychiatric Society Bernice Garrison Saint Joseph's Hospital/NPHS Brent Gear, DO, FACEP, FACOEP American Society of Bariatric Physicians Susan Gonzalez Nova Southeastern University Heather Gray Community Hospital Andrew Gruber Idaho Osteopathic Association Elizabeth Harano Association of Osteopathic Directors and Medical Educators Maria Harris Virginia Osteopathic Medical Association Maria Harris Edward Via College of Osteopathic Medicine Courtney Haxton Osteopathic Founders Foundation

4
Leslie Herman UNT Health Science Center Esther Hewlett-Crewes Philadelphia College of Osteopathic Medicine, GA Gretchen Higbee Mclaren Macomb Holly Huddleston Georgia Osteopathic Medical Assn Colleen Jensen Minnesota Osteopathic Medical Society Andrea Jerabek American College of Osteopathic Emergency Physicians Sherry Jimenez, EdD Marian University COM Marie Kadavy Oklahoma Osteopathic Association Victoria Kaprielian, MD Campbell University, School of Osteopathic Medicine Kristen Kennedy American College of Osteopathic Emergency Physicians Georgiaetta Klebba Capital Region Medical Center Joan Kulikowski American College of Osteopathic Family Physicians Anna Lamb, DO Western New York Osteopathic Medical Society Mario Lanni, DSc Pennsylvania Osteopathic Medical Association (POMA Foundation)
Jeffrey LeBoeuf, CAE AOCOPM Beth Ann Levendoski Osteopathy's Promise to Children Alicia Lund, MBA Westchester General Hospital Leslie Lynch OhioHealth Doctors Hospital Gina L. Maraio, DO Beauty of Wellness Peggy Mariucci McLaren Greater Lansing Deb Marti Cleveland Clinic Sherry McAuliffe American Osteopathic Association Steven R. McLaren, DO Kaiser West Los Angeles Leah McWilliams Iowa Osteopathic Medical Association Teresa Mersereau, BEd, MBA, CCMEP Mercy St. Vincent Medical Center Linda Miller Philadelphia College of Osteopathic Medicine Ryan Miller Oklahoma State University College of Osteopathic Medicine Cassandra Mills Henry Ford Macomb Hospitals Beverly Minock Oklahoma State University-COM

5
Eric Nicastro Lake Erie College of Osteopathic Medicine Michael Oliverio, DO NYS-ACOFP Linda Pavina AOAPRM Cindy Penkala, CMM, CMPE, CMSCS AOIA Joy Potter New Hampshire Osteopathic Association Rose Ann Prince CAMC Health Education and Research Institute Crystal Probasco Fairfield Medical Center David Rechlin, DO Samaritan Medical Center Phyllis Ring, MBA Denver Osteopathic Foundation Rose Ann Prince CAMC Health Education and Research Institute Rob Robinson Oklahoma State University-COM Vanessa Ross, CMP, CCMEP Des Moines University Jill Sanders, DO Vermont State Assn. of Osteopathic Physicians & Surgeons Cole Schulte, MHA Des Peres Hospital Vicki Shuman West Virginia School of Osteoapthic Medicine
Michael Steelman, DO Heart of Lancaster Regional Medical Center Lisa Stella McLaren-Macomb Nicole Struck Tucson Osteopathic Medical Foundation Amy Taylor UH Regional Hospitals Amy Tillou Broward Health Kathy Tobasko, CPMSM Western Reserve Hospital Marilyn Tracy Millcreek Community Hospital Nina Vidmer American Osteopathic Academy of Addiction Medicine Kirsten Waarala, DO Garden City Hospital Sherrie Warner American Academy of Osteopathy Janet Weigel Arizona Osteopathic Medical Association Diane West Crozer-Keystone Health System Adrienne White-Faines American Osteopathic Association Jamie Wilcox, GME Samaritan Medical Center Stephanie Wilson AOCPMR

6
Missy Windon Alabama Osteopathic Medical Association Shelley Wood American Osteopathic College of Dermatology Amanda Yochum Western University of Health Sciences, COMP Kelly Zarwell UNT Health Science Center

MILLENNIUM BILTMORE HOTEL, LOS ANGELES, CALIFORNIA. JANUARY 8, 2015
The Emerging CME EnvironmentAOA's 21st National CME Sponsors Conference

© 2014 American Medical Association. All rights reserved.
Contact information
Alejandro Aparicio, MD, FACPDirector, Medical Education ProgramsAmerican Medical AssociationClinical Assistant Professor of Medicine and
Assistant Professor of Medical EducationUniversity of Illinois at Chicago College of Medicine
AMA Plaza330 N. Wabash Ave., Suite 39300Chicago, IL [email protected]
2

© 2014 American Medical Association. All rights reserved.
Disclosures
• I have no financial relationships to commercial interests to disclose and this presentation does not include any clinical topics
• I am a full time employee (ten years) and a 28 year member of the AMA
3

© 2014 American Medical Association. All rights reserved.
Learning objectives
At the end of this presentation participants will be able to:
• Summarize the evolution of formal CME in the US
• Describe the current trends and forces impacting CME
• Discuss, based on current trends and forces, a likely future for CME
4

A Brief History of (CME) Time (with apologies to Stephen Hawking)
5

Or How We Got Here
6
© 2014 American Medical Association. All rights reserved.
American Academy of Family Physicians
• AAFP began content review of individual activities and its specialty specific credit in 1947
• Two types of credit:
AAFP Prescribed Credit
AAFP Elective Credit
http://www.aafp.org/online/en/home/cme/cmea/cmeapplying.html
7

© 2014 American Medical Association. All rights reserved.
American Medical Association
The Physician Recognition Award and the credit system were created in 1968
AMA PRA Category 1 Credit™• Certified activities by state accredited or nationally accredited CME
providers under the ACCME accreditation system• Individual learning activities certified for credit directly by the AMAAMA PRA Category 2 Credit™• Educational activities not certified for Category 1 Credit but claimed for
credit by individual physicians
8

© 2014 American Medical Association. All rights reserved.
American Osteopathic Association
• AOA began content review of individual activities, specialty-specific institutional accreditation, and specialty-specific credit in 1973
• Four types of credit:
1-A, 1-B, 2-A, and 2-B
www.do-online.org
9

© 2014 American Medical Association. All rights reserved.
CME and the AMA Code of Ethics
A physician shall continue to study, apply, and advance scientific knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues, and the public, obtain consultation, and use the talents of other health professionals when indicated.
One of the nine Principles of medical ethics
AMA Code of Ethics
10

© 2014 American Medical Association. All rights reserved.
Ethical guidance to physicians related to CME
Opinion 9.011 – Continuing Medical Educationhttp://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion9011.page
Opinion 9.0115 - Financial Relationships with Industry in CME http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion90115.page
Opinion 8.061 - Gifts to Physicians from Industryhttp://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion8061.page
11
© 2014 American Medical Association. All rights reserved.
Some CME credit requirements in the US
Voluntary recognition awards – AMA PRA, others
Specialty Societies – Mandated by some for membership
Hospitals – Mandated by accrediting bodies
Specialty boards – Mandated to maintain specialty certification
Licensing boards – Mandated to maintain license to practice in vast majority of states
12

© 2014 American Medical Association. All rights reserved.
Evolution of credit in the US
From time based to value based
From credit for participation to credit for accomplishment
13

Forces currently impacting CME
14

© 2014 American Medical Association. All rights reserved.
Professional Forces
• MOC/OCC
15

© 2014 American Medical Association. All rights reserved.
The four parts of MOC Part I: Professionalism and Professional Standing• Behave in a professional manner • Act in the patients’ best interest • Hold a valid, unrestricted medical license Part II: Lifelong Learning and Self-Assessment• Participate in high quality, unbiased educational and self-assessment activities
determined by each Member Board Part III: Assessment of Knowledge, Judgment, and Skills• Pass a written examination and other evaluations Part IV: Improvement in Medical Practice• Engage in ongoing assessment and improvement activities to improve patient outcomes • Demonstrate use of evidence and best practices compared to peers and national
benchmarks
http://www.abms.org/board-certification/a-trusted-credential/assessed-through-a-four-part-framework/
16

© 2014 American Medical Association. All rights reserved.
Updated MOC Standards – Part I Standards –Professionalism and Professional Standing
PPS-1: Each ABMS Member Board will identify and convey that Board’s professionalism expectations to its diplomates and will incorporate professionalism learning and assessment activities into its Program for MOC. PPS-2: Each ABMS Member Board will establish and maintain a process that provides former diplomates an opportunity to regain board certification. PPS-3: Each ABMS Member Board will have a process in place to consider the circumstances of an action taken against a diplomate’s license by a State Medical Board or other determination of unprofessional conduct by an appropriate authority and to respond appropriately.
17

© 2014 American Medical Association. All rights reserved.
Updated MOC Standards – Part II Standards –Lifelong Learning and Self-Assessment
LLS-1: Each ABMS Member Board will establish requirements for LLS and document that diplomates are meeting the learning and self-assessment requirements. ABMS Member Boards’ requirements should address currently relevant medical knowledge and other competencies in the specialty and ongoing advances relevant to the applicable specialty, and should include a requirement that LLS activities be free of commercial bias and control of a commercial interest. ABMS Member Boards should work to ensure that diplomates have access to tools for identifying and learning about advances relevant to the specialty and for identifying professional practice gaps in the specialty and in their own clinical practices. ABMS Member Boards should document that LLS activities are of high quality.
18

© 2014 American Medical Association. All rights reserved.
Updated MOC Standards – Part IV Standards –Improvement in Medical Practice
IMP-1: Each ABMS Member Board will incorporate practice assessment and improvement activities into its Program for MOC requirements throughout diplomates’ careers. Each ABMS Member Board’s Program for MOC will incorporate ways in which diplomates may engage in specialty-relevant, performance-in-practice assessment followed by improvement activities when practice gaps are identified.
IMP-2: Each ABMS Member Board should encourage diplomateinvolvement in performance improvement activities within the context of the health care team and system of practice, and in alignment with other care-related quality improvement programs.
19

© 2014 American Medical Association. All rights reserved.
Professional Forces
• MOC/OCC
• Need for better self assessment tools which are certified for credit and promote self-directed learning
20

© 2014 American Medical Association. All rights reserved.
Definition of Self-Directed Learning
Hammond and Collins definition:• “A process in which learners take the initiative, with the support
and collaboration of others, for increasing self- and social-awareness; critically analyzing and reflecting on their situation; diagnosing their learning needs with specific reference to competencies they have helped identify; formulating socially and personally relevant learning goals; identifying human and material resources for learning; choosing and implementing appropriate learning strategies; and reflecting on and evaluating their learning.
Hammond M, Collins R. SDL: Critical Practice. New York, NY: Nichols/GP Publishing; 1991

© 2014 American Medical Association. All rights reserved.
Professional Forces
• MOC/OCC• Need for better self assessment tools which are certified for credit• Emphasis on competencies at the undergraduate, graduate and
practicing physician level• Increased emphasis on faculty development as the pace of change
in medical education increases at all levels• Increased body of evidence on the value of CME based on research
of learning and improvement through formal CME, including new formats, informing educational design
22
© 2014 American Medical Association. All rights reserved.
Regulatory Forces
• Maintenance of Licensure
23

© 2014 American Medical Association. All rights reserved.
Maintenance of Licensure Framework
1. Reflective Self Assessment (What improvements can I make?) Reflective self‐evaluation, self‐assessment and practice assessment and appropriate educational or improvement activities.
2. Assessment of Knowledge and Skills (What do I need to know and be able to do?)
Physicians must demonstrate the knowledge, skills and abilities necessary to provide safe, effective patient care, based on the general competencies model.
3. Performance in Practice (How am I doing?) Assess their performance in practice and guide improvement.
24

© 2014 American Medical Association. All rights reserved.
Regulatory Forces
• Maintenance of Licensure
• Open Payments – impact on physicians and on industry (commercial support, personal COIs, and public perception)
25

© 2014 American Medical Association. All rights reserved.
Open payments revisions (10/31/14)
Where industry does not select or directly pay the CME speaker nor provide the CME provider with a list of suggested speakers, the transfer is not reportable as an indirect transfer even if industry learns the identity of the speakers/participants subsequently.
https://s3.amazonaws.com/public-inspection.federalregister.gov/2014-26183.pdf
26

© 2014 American Medical Association. All rights reserved.
Open Payments (page 595)
27
If an applicable manufacturer or applicable GPO provides funding to support a continuing education event but does not require, instruct, direct, or otherwise cause the continuing education event provider to provide the payment or other transfer or value in whole or in part to a covered recipient, the applicable manufacturer or applicable GPO is not required to report the payment or other transfer of value. The payment is not reportable regardless if the applicable manufacturer or applicable GPO learns the identity of the covered recipient during the reporting year or by the end of the second quarter of the following reporting year because the payment or other transfer of value did not meet the definition of an indirect payment. This approach is also consistent with our statement at (78 FR 9490), where we explained that “if an applicable manufacturer provided an unrestricted donation to a physician professional organization to use at the organization’s discretion, and the organization chose to use the donation to make grants to physicians, those grants would not constitute ‘indirect payments’ because the applicable manufacturer did not require, instruct, or direct the organization to use the donation for grants to physicians.” Therefore, because such payments are not indirect payments, we do not need to create an additional exclusion specific to continuing education indirect payments by modifying the indirect payment exclusion at §403.904(i)(1).

© 2014 American Medical Association. All rights reserved.
Trends in industry funding of CME in the US
• Decreased industry funding (ACCME system providers only)2007 - $1,248,924,872 (approx. 47%)2010 - $846,182,6682011 - $752,406,638*2012 - $674,747,116* 2012 - $659,953,563* (approx. 26%)
*New way of reporting commercial support: monetary value of in-kind commercial support excluded starting in 2012
28

© 2014 American Medical Association. All rights reserved.
Regulatory Forces
• Maintenance of Licensure
• Open Payments – impact on physicians and on industry (commercial support, personal COIs, and public perception)
• Pay for Performance (MOC)
• Joint Commission medical staff requirements including Ongoing Professional Practice Evaluation (OPPE) or Focused Professional Practice Evaluation (FPPE)
29

© 2014 American Medical Association. All rights reserved.
Other forces
• Emphasis on Continuous Quality Improvement/Performance Improvement (“CQI without education is just a Pavlovianexercise.” Don Moore, PhD, SACME Fall conference 11/4/14)
• Emphasis on evidence based care and evidence based medicine
• Emphasis on Team based learning and Interprofessionaleducation
30

© 2014 American Medical Association. All rights reserved.
Other forces (cont.)
• New technologies such as branching logic as additional tools to increase/improve learning.
• Integration of education into the electronic health records
• Better integration of registries into the electronic health records
• AAFP/AOA/AMA close working relationship in the field of CME
• The need to find ways for physicians to meet the multitude of requirements (learning and improving, MOC, OCC, MOL, Joint Commission, etc.) without needless duplication of effort.
31

The future?
32

© 2014 American Medical Association. All rights reserved.
It is hard to predict the future before it happens
• Continued decrease in industry funding of CME
• Increased reliance in institutional and physician support for CME
• Further decrease in the number of CME providers
• Need to base changes to the credit systems and accreditation process on evidence/research/pilots
33

© 2014 American Medical Association. All rights reserved.
It is hard to predict the future before it happens
• Increased integration of CME and PI
• Increased integration of the competencies into CME
• Increased integration of health disparities and patient safety issues into CME
• Increased demonstration on the part of the credit systems not just of the quality of the education but also the achievement of the learning objective by the learners
34
© 2014 American Medical Association. All rights reserved.
Continuing Medical Education
• An educational need
• A professional responsibility
• An Ethical Imperative
35

© 2014 American Medical Association. All rights reserved.

MILLENNIUM BILTMORE HOTEL, LOS ANGELES, CALIFORNIA. JANUARY 8, 2015
Understanding the AMA PRA Credit System AOA's 21st National CME Sponsors Conference

© 2014 American Medical Association. All rights reserved.
Contact information
Alejandro Aparicio, MD, FACPDirector, Medical Education ProgramsAmerican Medical AssociationClinical Assistant Professor of Medicine and
Assistant Professor of Medical EducationUniversity of Illinois at Chicago College of Medicine
AMA Plaza330 N. Wabash Ave., Suite 39300Chicago, IL [email protected]
2

© 2014 American Medical Association. All rights reserved.
Disclosures
• I have no financial relationships to commercial interests to disclose and this presentation does not include any clinical topics
• I am a full time employee (ten years) and a 28 year member of the AMA
3

© 2014 American Medical Association. All rights reserved.
Learning objectives
At the end of this presentation participants will be able to:
• Summarize the history of the AMA Physician Recognition Award and the CME credit system created to support it;
• Compare and contrast AMA PRA Category 1 Credit™ and AMA PRA Category 2 Credit™;
• Compare and contrast provider credit, direct credit and international credit conversions;
• Describe the different learning formats that can be certified for AMA PRA Category 1 Credit™.
4

The AMA Physician Recognition Award Credit System
5

© 2014 American Medical Association. All rights reserved.
The AMA’s Physician Recognition Award
The AMA established the PRA in 1968 as a way to encourage and recognize physicians that devoted 50 hours a year to CME. The credit system was developed to describe activities that would be accepted to meet the requirements. It has continued to evolve under the direction of the AMA Council on Medical Education
www.ama-assn.org/go/prabooklet
6

© 2014 American Medical Association. All rights reserved.
AMA’s Definition of CME
The AMA House of Delegates has defined continuing medical education as follows:
CME consists of educational activities which serve to maintain, develop, or increase the knowledge, skills, and professional performance and relationships that a physician uses to provide services for patients, the public or the profession.
7

© 2014 American Medical Association. All rights reserved.
AMA CME credit
AMA PRA Category 1 Credit™
• Certified activities by state accredited or nationally accredited CME providers under the ACCME accreditation system
• Individual learning activities certified for credit directly by the AMA
AMA PRA Category 2 Credit™
• Educational activities not certified for Category 1 Credit but claimed for credit by individual physicians
8

© 2014 American Medical Association. All rights reserved.
Certified CME
Certified CME is defined as:
• 1. Nonpromotional learning activities certified for credit prior to the activity by an organization authorized by the credit system owner, or
• 2. Nonpromotional learning activities for which the credit system owner directly awards credit
9

© 2014 American Medical Association. All rights reserved.
CME: An ethical imperative
A physician shall continue to study, apply, and advance scientific knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues, and the public, obtain consultation, and use the talents of other health professionals when indicated.
One of the nine Principles of medical ethicsAMA Code of Ethics
10

© 2014 American Medical Association. All rights reserved.
Ethical guidance to physicians related to CME
Opinion 9.011 – Continuing Medical Educationhttp://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion9011.page
Opinion 9.0115 - Financial Relationships with Industry in CME http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion90115.page
Opinion 8.061 - Gifts to Physicians from Industryhttp://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion8061.page
11

AMA CME credit awarded by accredited providers
12

© 2014 American Medical Association. All rights reserved.
AMA core requirements for an AMA PRA Category 1 Credit™ activity
• Conform to the AMA’s definition of CME.
• Address demonstrated educational needs.
• Communicate to prospective participants a clearly identified educational purpose and/or objectives in advance of participation in the activity.
13

© 2014 American Medical Association. All rights reserved.
Core requirements (continued)
• Be designed using AMA approved learning formats and learning methodologies appropriate to the activity’s educational purpose and/or objectives; credit must be based on AMA guidelines for the type of learning format used.
• Present content appropriate in depth and scope for the intended physician audience.
• Be planned in accordance with the relevant AMA Council on Ethical and Judicial Affairs opinions and the ACCME Standards for Commercial SupportSM, and be nonpromotional in nature.
14
© 2014 American Medical Association. All rights reserved.
Core requirements (continued)
• Evaluate the effectiveness in achieving its educational purpose and/or objectives.
• Document credits claimed by physicians for a minimum of six years.
• Be certified for AMA PRA Category 1 Credit™ in advance of the activity; i.e. an activity may not be retroactively approved for credit.
• Include the AMA Credit Designation Statement in any activity materials that reference CME credit with the exception of “save the date” or similar notices.
15
© 2014 American Medical Association. All rights reserved.
AMA Credit Designation Statement
The following AMA Credit Designation Statement must be included in relevant announcement and activity materials:
The [name of accredited CME provider] designates this [learning format] for a maximum of [number of credits] AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
16

© 2014 American Medical Association. All rights reserved.
AMA PRA Category I Credit™ approved Learning Formats for use by accredited providers
1. Live activity*
2. Enduring material*
3. Journal-based CME activity*
4. Test-item writing activity
5. Manuscript review activity
6. PI CME activity*
7. Internet Point of Care activity*
17

© 2014 American Medical Association. All rights reserved.
Live Activity
Occurs at a specific time as scheduled by the accredited CME provider
Includes Courses, Regularly scheduled conferences, Live internet, Simulation workshops and Journal clubs
Credit calculation is based on time that physician participates; 60 minutes = 1 AMA PRA Category 1 Credit™ (credit can be claimed in quarter-hour increments or 0.25 credits)
18

© 2014 American Medical Association. All rights reserved.
Enduring Material
Activity that endures over a specified time
Includes print, audio, (tapes, podcasts, CDs) video or internet materials (archived webinars)
Credit calculation based on time it takes average target audience to complete; 60 minutes = 1 AMA PRA Category 1 Credit™
19
© 2014 American Medical Association. All rights reserved.
Enduring Material
• Provide clear instructions to learner on completion of activity
• Provide bibliographic sources for further study
• Provide an assessment of learner that measures achievement of purpose/objectives with minimum performance level required for credit– Rationale: Brings consistency to what is already a frequent
practice; strengthens confidence that physicians have assimilated the content and met the objectives.
20

© 2014 American Medical Association. All rights reserved.
Journal-based CME
Article, within a peer-reviewed professional journal, certified for credit prior to publication
– Peer-reviewed article– Provide an assessment of learner that measures
achievement of purpose/objectives with minimum performance level required for credit
• Rationale - Brings consistency to what is already a frequent practice; strengthens confidence that physicians have assimilated the content and met the objectives.
– Individual articles are certified for 1 AMA PRA Category 1 Credit™ (not time-based)
21

© 2014 American Medical Association. All rights reserved.
Test Item Writing
Physicians learn through contributions to development of high-stakes examinations or certain peer-reviewed self-assessment activities
Be developed only for:• NBME examinations• ABMS member board certification examinations• National specialty society peer-reviewed, published, self-
assessment examinations
22

© 2014 American Medical Association. All rights reserved.
Test Item Writing
Depth and scope that requires review of literature and evidence base
Includes participation in a group peer review process
Completion of process certified for 10 AMA PRA Category 1 Credits™ (not time-based)
23

© 2014 American Medical Association. All rights reserved.
Manuscript Review
• Physicians learn through the critical review of an assigned journal manuscript
• Reviewed article must be submitted to a journal indexed in MEDLINE
• Manuscript must be original article requiring multiple reviewers
24
© 2014 American Medical Association. All rights reserved.
Manuscript Review
Depth and scope that requires review of literature and evidence base
Credit only awarded for acceptable reviews• Rationale - Provides consistency that credit is awarded to
physicians that fully participate in activity in a meaningful way
Certified for 3 AMA PRA Category 1 Credits™ (not time-based)
25

© 2014 American Medical Association. All rights reserved.
Performance Improvement CME (PI CME)
• Three stage learning model approved for AMA PRA Category 1 Credit™, September 2004, as a result of pilot study done in collaboration with the American Academy of Family Physicians (AAFP) and other stakeholders
• Structured long-term process developed by an accredited CME provider in which evidence-based measures and quality improvement (QI) interventions, not traditionally thought of as CME, are used to change physician performance
26

© 2014 American Medical Association. All rights reserved.
Stage A - Learning from current practice performance assessment
• Assess current practice using identified evidenced based performance measures, either through chart reviews, record reviews, or other appropriate data sources
• Participating physicians are actively involved in data analysis to determine causes of variations
• Identify appropriate intervention(s)
27

© 2014 American Medical Association. All rights reserved.
Stage B - Learning from the application of PI to patient care
• Implement interventions based on results of Stage A, using suitable tracking tools
• Participating physicians should receive guidance on appropriate parameters for applying the intervention(s)
28
© 2014 American Medical Association. All rights reserved.
Stage C - Learning from the evaluation of the PI effort
• Re-assess and reflect on performance in practice measured after implementation of interventions in Stage B by comparing to the assessment done in Stage A
• Summarize any practice, process and/or outcomes changes that resulted from conducting the PI CME activity
29

© 2014 American Medical Association. All rights reserved.
Credit awarded for PI CME
• Twenty AMA PRA Category 1 Credits™ for completion of all three stages.
• Five credits for each of the first two stages, 20 credits for completing all three stages in order.
• Credit is based on participation in the 3 stages and not based on time.
30

© 2014 American Medical Association. All rights reserved.
Internet Point of Care (PoC)
• Structured activity in which physician engages in self-directed, online learning, using vetted databases, on topics relevant to patient care
– 3 stage learning cycle must be completed1. Review clinical question2. Identify relevant sources3. Describe application to practice
– Certified for 0.5 AMA PRA Category 1 Credit™ for completion of each cycle
31

AMA CME credit awarded directly by the AMA
32

© 2014 American Medical Association. All rights reserved.
AMA PRA Category I Credit™ awarded directly by the AMA as owners of the credit system
• Preparing and presenting an original presentation at a live activity certified for AMA PRA Category 1 Credit™
• Publishing (lead author) a peer-reviewed article in a journal indexed in MEDLINE (10 credits)
• Preparing a poster presentation (first author) included in the abstracts of an activity certified for AMA PRA Category 1 Credit™ (5 credits)
• Obtaining a medically related advance degree (25 credits)• Completing an ABMS board certification or MOC© process (60 credits)• Participation in an ACGME approved residency or fellowship (20 credits per
year)
33

© 2014 American Medical Association. All rights reserved.
International activities
• Union of European Medical Specialists (conversion of credit)
• Royal College of Physicians and Surgeons of Canada (conversion of credit)
• International Conference Recognition Program (certified for credit by the AMA as owner of the CME credit system)
34

AMA CME credit self reported by physicians
35

© 2014 American Medical Association. All rights reserved.
AMA PRA Category 2 Credit™
Educational activities not certified for AMA PRA Category 1 Credit™ but claimed for credit by individual physicians. Examples of learning activities that might meet the requirements for AMA PRA Category 2 Credit™ include, but are not limited to: • Participation in activities that have not been certified for AMA PRA Category 1 Credit™ • Teaching physicians, residents, medical students or other health professionals • Unstructured online searching and learning (i.e., not Internet PoC) • Reading authoritative medical literature • Consultation with peers and medical experts
36

© 2014 American Medical Association. All rights reserved.
AMA PRA Category 2 Credit™
• Small group discussions
• Self assessment activities
• Medical writing
• Preceptorship participation
• Research
• Peer review and quality assurance participation
37

Additional Resources
38

© 2014 American Medical Association. All rights reserved.
AMA on line resources
•Direct AMA PRA questions to [email protected]
•AMA PRA credit system www.ama-assn.org/go/pra and www.ama-assn.org/go/prabooklet
•AMA Division of Continuing Physician Professional Developmentwww.ama-assn.org/go/cppd
•Resources for physicianswww.ama-assn.org/go/cme
•Information for CME providerswww.ama-assn.org/go/cmeprovider
•AMA MedEd Update – sign up via:http://www.ama-assn.org/ama/pub/news/subscribe-newsletters.page
39

© 2014 American Medical Association. All rights reserved.
CME UPDATE 2013-2015 CYCLE
Tim Cheslock, DO FACOEP
Member, CCME


Objectives
• Understand the changes to the 2013-2015 CME Guide for AOA Members
• Updates regarding the AOA Board of Trustees Action for 2014
• Review the Accreditation Guidelines for AOA Category 1A Sponsors

The Basics
• The CME requirement for AOA members remains 120 hours for the 3 year cycle
• 30 Category 1A credits are required
• 90 credits may be earned in any category
• AOA boarded members are required to earn 50 credits in their primary specialty
• CME requirements are also state specific. Check with your state licensing board for current requirements

2013-2015 CME Cycle
So, What’s new for
2013-2015?

Category 1A
• Definition:
• AOA Category 1-A credits will be granted to attendees for formal educational programs designed to enhance clinical competence and improve patient care. These programs must be sponsored by an AOA accredited Category 1 CME sponsor and are limited to:
• A. Formal Osteopathic CME
• Consisting of formal face-to-face programs that meet the Category 1 quality guidelines, faculty requirements, and which are sponsored by AOA-accredited Category 1 CME sponsors.
• Topics may be related to any of the seven (7) Core Competencies listed below, as the core competencies have been recognized throughout the continuum of osteopathic education as essential and critical to the development and maintenance of osteopathic physicians overall education.

What are the core competencies?
• Osteopathic Philosophy/ Osteopathic Manipulative Medicine
• Medical Knowledge
• Patient Care
• Interpersonal and Communication Skills
• Professionalism
• Practice Based Learning and Improvement
• Systems Based Practice

How will this change the face of CME?
• Broad based range of topics that were not previously eligible for CME.
• Activities that were previously part of the educational process but were not viewed as CME can now be included.
• Makes the needs assessment process more streamlined.

Streamlining Needs Assessment
• Needs Assessment must be submitted for each program.
• The needs assessment must cover each topic of the program
• Must be current for the field
• At least one evidence based reference

Streamlining Needs Assessment
• Exempt include the following:
• OMT/OPP- State that it is “Part of the profession” in documentation
• Core Competencies that are non-clinical (Professionalism, Communications, System Based Practice, etc) – State Core “Competency, required for specialty.” Cite the applicable core competency
• Faculty Development Programs
• State Requirements such as Risk Management
• Board preparation courses based on pass rate/board scores

Other CME Updates
• Standardized Life Support Courses
• Limited to a total of 8 Category 1A credits per three year cycle. All additional credit will be Category 1B.
• 1A credit is only applicable to live, in person activity. For Online courses, only the skills verification portion is eligible for 1A.
2014 CME Resolutions
• B4 Mid year Meeting: DO’s attending the Annual CCME Sponsor Conference will be eligible for Category 1A CME credit for their attendance.
• This is not applicable to members of the CCME committee.

2014 CME Resolutions
• B6 Mid year Meeting: Accrediting AOA CME Sponsors outside of currently eligible sponsors
• After review by the CCME at the OCT 2013 meeting, it was determined that current needs are being met and 9 new hospitals had been accredited over a six month period.
• There is not enough data to suggest further expansion outside of the current eligibility standards is necessary at this time. CCME will continue to monitor this based on member feedback.

2014 CME Resolutions
• B9 2014 Mid year Meeting: Needs Assessment for Category 1A and 1B programs.
• A needs assessment is required when seeking approval for any Category 1A or 1B program. Current language states the needs assessment is only needed when seeking pre-approval.
• Resolution clarifies the requirement and removes the “pre”- approval stipulation. If preapproval is not sought for a program, advertisement must strictly adhere to section 5.5 of the CME manual in regards to anticipated approval of credits.

2014 CME Resolutions
• B1: Annual Programming Requirement
• Purpose was to clarify the minimum programming requirement needed in order to maintain status as a CME sponsor. Previous language stated a minimum of 3 hrsannually per cycle.
• The resolution now states that a minimum of 3 hours per accreditation cycle will be the new requirement.

2014 CME Resolutions
• B2- A/2014: Standardized Life Support Courses.
• A maximum of 8 Category 1A credits may be granted for standardized life support classes over the three year CME cycle.
• Credits beyond the 1A threshold hours earned can be logged as 1B or 2A as appropriate.

2014 CME Resolutions
• B5 – A/2014: Random site visits for CME Sponsors
• This resolution approves the process for random CME site visits as required by the EPRCC III recommendations.
• Details of this process can be found in Appendix E of the CME Sponsors Manual

New CME Report
• The Physician CME Report has a new look

Small Sub-Specialties
• AOA members who are in a specialty or sub-specialty of less than 300 certificate holders are eligible to submit ACCME Category 1 credits, up to 15 per 3 year cycle to partially fulfill their Category 1A requirement.
• The member must be an AOA member, be AOA or ABMS certified in a specialty currently on the eligible list. The current roster is available at osteopathic.org.

Preceptoring Credits
• Osteopathic Physicians who precept osteopathic residents or students are eligible for Category 1B credit, regardless of the physicians institutional affiliation.
• Category 1A for didactic teaching in Osteopathic residencies must be submitted by Category 1 CME Sponsoring COM or hospital CME Department.

Accreditation
• New eligible applicants must complete an initial packet for review.
• Initial accreditation is awarded based on this review by the AOA Division of CME
• Attendance at a CME Sponsors Conference is mandatory for new sponsors.
• Accreditation is from 1 to 3 years based on points from the document survey

Accreditation
• In order to maintain accreditation Sponsors must
• Conduct at least one 3 hour program per cycle.
• Pay applicable fees to the AOA
• Respond to requests for document surveys
• Attend CME Sponsors conference at least once during the accreditation cycle.

Faculty Requirements
• Currently, programs submitted for Category 1A credit must have 50% osteopathic presenters/hours. The 30% pilot project has ended and was not approved by the BOE.
• At least 50% of the presenters are osteopathic physicians; or MD's, PhD's, and other professionals with graduate degrees who hold a full-time paid faculty appointment at a college of osteopathic medicine; or AOA staff or AOA component society who hold a graduate degree and clinical COM faculty or OGME core faculty.
Sponsor Eligibility
• AOA accredited colleges of osteopathic medicine;
• AOA affiliated Specialty Colleges;
• AOA Non-practice Affiliates, College of Osteopathic Medicine Alumni Groups, and Osteopathic Philanthropic Organizations (Foundations);
• AOA affiliated Divisional societies,
• Branch Campuses (All Branch Campuses must independently apply to be recognized as an AOA Category 1 CME Sponsor effective January 1, 2013.),
• Healthcare Facilities that are HFAP-Accredited and/or have AOA-approved training programs and,
• Healthcare Facilities that are in states/regions where AOA CME opportunities are not available or available on a limited basis.

Questions????
• All information for CME can be found on the osteopathic.org website under CME
• Delores Rodgers at Client and Member Services can be reached at [email protected]

Needs Assessments and Core Competencies
James E. Preston, D.O.AOA Council of ContinuingMedical EducationJanuary 2015

RES. NO. 38 – M/09 – Page 1
SUBJECT: NEEDS ASSESSMENT, PRE APPROVAL OF CME PROGRAMS FOR
AOA CATEGORY 1-A OR CATEGORY 1-B CREDIT
SUBMITTED BY: Bureau of Osteopathic Education / Council on Continuing Medical
Education
REFERRED TO: Reference Committee 4
1 WHEREAS, the Needs Assessment is the systematic effort to address the competence and
2 performance “gaps” of physicians that underlie deficits in the quality of healthcare,
3 with this in mind, the Needs Assessment will include (1) matching the scope of the
4 learner’s practice, (2) designing activities that will link to practice-based needs and (3)
5 being able to measure the change in the physician’s competence, performance and
6 patient outcome; and
7 WHEREAS, quality CME programs should focus on the determined needs of the physicians
8 as assessed by proven methods of needs assessment such as (1) medical audit, (2)
9 pre-test item analysis, (3) self-assessment, and (4) questionnaire; now, therefore, be it
10 RESOLVED, that effective January JULY 1, 2009 all AOA Category 1 CME Sponsors
11 requesting pre approval for a formal program (Category 1A or Category 1-B credit)
12 must provide written documentation of their needs assessment as tied to the
13 program objectives at the time of the request for approval.
ACTION TAKEN __APPROVED_AS AMENDED (LINE 10)__________________
DATE _____3/1/09______________________________

Needs Assessments
Questions for your CME Committee WHO is your audience?◦ Specialists, generalists, or combination
WHAT do they WANT to learn?◦ Physician surveys◦ Conversations/Peer Discussions
WHAT do they NEED to learn?◦ Hospital/Med Literature Statistics◦ Local Health Department Statistics

Needs Assessments
HOW is the best way to teach them?◦ Lecture, small group, combination, or online
WHERE is the best place for them to learn?◦ Lecture Hall, classroom, breakout rooms
CREATE OBJECTIVES you want covered◦ CME Committee should control the direction
of the speaker’s information. You know the KNOWLEDGE GAPS!!!

LINK TO CORE COMPETENCIES
This CME Committee activity takes the information that your audience needs and links it to the required areas of professional development as established by the accreditation agencies of the AOA and ACGME. This activity provides the continuity of medical education from medical school throughout the learner’s medical practice until retirement.

Just What Are Core Competencies?
AOA and ACGME standards for learner performance in graduate medical education.
A fundamental knowledge, ability of expertise in specific subject areas or skill sets in the field of medicine.
Concept being embraced by JCAHO, specialty college certification, and FSMB for CME content and outcomes measures
Strongly encouraged by AOA CCME.

How are Core Competencies utilized in Graduate Medical Education? Core competencies drive the didactic and
clinical curriculum. All core competencies must have multiple
assessment modalities. Graduating physicians must be documented as
“competent” in each of the core competencies/skill sets.
Competency is attested by Program Director at conclusion of training program.

How should CME Sponsors Utilize the Core Competencies? During the needs assessment process and
outcomes measures process, assign core competencies as indicated.
Core competencies will assist the CME sponsor in justifying programs and improving outcomes measures.
Core competencies will demonstrate that your CME Committee has completed a needs assessment process.

What is the Best Way to Start Implementing Core Competencies? Familiarize your CME Committee about
core competencies. Add core competency assignment to your
needs assessment process. Add core competency to your CME Activity
Checklist
We have included sample handouts that demonstrate the incorporation of core competencies into your CME process.

CORE COMPETENCY 1OSTEOPATHIC PHILOSOPHY AND
OSTEOPATHIC MANIPULATIVE MEDICINE• Practitioners are expected to demonstrate
and apply knowledge of accepted standards in Osteopathic Manipulative Treatment (OMT) appropriate to their specialty. The educational goal is to train a skilled and competent osteopathic practitioner who remains dedicated to life-long learning and to practice habits in osteopathic philosophy and manipulative medicine.

CORE COMPENTENCY 1OSTEOPATHIC PHILOSOPHY AND OSTEOPATHIC MANIPULATIVE MEDICINE
CME Applications: Any OMM Lecture/Workshop. A lecture which highlights the
osteopathic “holistic” approach to a clinical issue.
Any lecture which adds OMM into the list of applicable therapies.

CORE COMPENTENCY 2
MEDICAL KNOWLEDGE• Practitioners are expected to
demonstrate and apply knowledge of accepted standards of clinical medicine in their respective specialty area, remain current with new developments in medicine, and participate in life-long learning activities, including research.

CORE COMPETENCY 2MEDICAL KNOWLEDGE
CME Applications: Any CME activity highlighting a new
medication/skill/procedure. Any CME activity which emphasizes
current research.

CORE COMPETENCY 3
PATIENT CARE• Practitioners must demonstrate the ability
to effectively treat patients, provide medical care that incorporates the osteopathic philosophy, patient empathy, awareness of behavioral issues, the incorporation of preventive medicine and health promotion.

CORE COMPETENCY 3PATIENT CARE
CME Applications: CME programs that involve preventive
health concepts/innovations. CME programs that include the
psychological/emotional support of the patient.

CORE COMPETENCY 4
INTERPERSONAL AND COMMUNICATION SKILLS
• Practitioners are expected to demonstrate interpersonal and communication skills that enable them to establish and maintain professional relationships with patients, families and other members of health care teams.

CORE COMPETENCY 4INTERPERSONAL AND COMMUNICATION SKILLS
CME Applications: CME activities that involve physician
audience interaction. CME activities that highlight
communication challenges in the doctor-patient relationship.

CORE COMPETENCY 5PROFESSIONALISM• Practitioners are expected to uphold the
Osteopathic Oath in the conduct of their professional activities that promote advocacy of patient welfare, adherence to ethical principles, collaboration with health professionals, life-long learning and sensitivity to a diverse patient population. Practitioners should be cognizant of their own physical and mental health in order to care effectively for patients.
CORE COMPETENCY 5PROFESSIONALISM
CME Applications: CME programs centered around risk
issues, medical ethics, medical-legal issues. CME programs that include discussion of
physician impairment and state medical board issues.

CORE COMPETENCY 6
PRACTICE-BASED LEARNING AND IMPROVEMENT
• Practitioners must demonstrate the ability to critically evaluate their methods of clinical practice, integrate evidence-based medicine into patient care, show an understanding of research methods and improve patient care practices.

CORE COMPETENCY 6PRACTICE-BASED LEARNING AND IMPROVEMENT
CME Applications: CME activities which highlight “best
practices” or improved clinical pathways. CME activities that demonstrate
evidence-based methodology.

CORE COMPETENCY 7
SYSTEM-BASED PRACTICE• Practitioners are expected to
demonstrate an understanding of health care delivery systems, provide effective and qualitative patient care within the system and practice cost-effective medicine.

CORE COMPETENCY 7SYSTEM-BASED PRACTICE
CME Applications: CME programs that include methods for
patient care quality assessment. CME programs that include utilization of
public health systems and adjunctive community healthcare modalities.

SAMPLE CME ACTIVITY CHECKLIST

CME NEEDS ASSESSMENT

AOA CME Sponsor’s Conference Millennium Biltmore Hotel
Los Angeles, CA
January 8-10, 2014
Outcome Measurement
W. Ashley Hood, DO AOA Council on CME, Member
Ed Williams, PhD Mississippi and Louisiana Osteopathic Medical Associations, Executive Director

Learning Objectives
• Discuss the importance of measuring outcomes.
• Understand the AOA Council on CME accreditation standards and the awarding of CME credits related to outcomes measures.
• Be able to implement various options to measure outcomes related to a CME program.
• Utilize outcomes measures to build your needs assessment.

Outcomes Measurement
How do we KNOW that what we are doing is working?

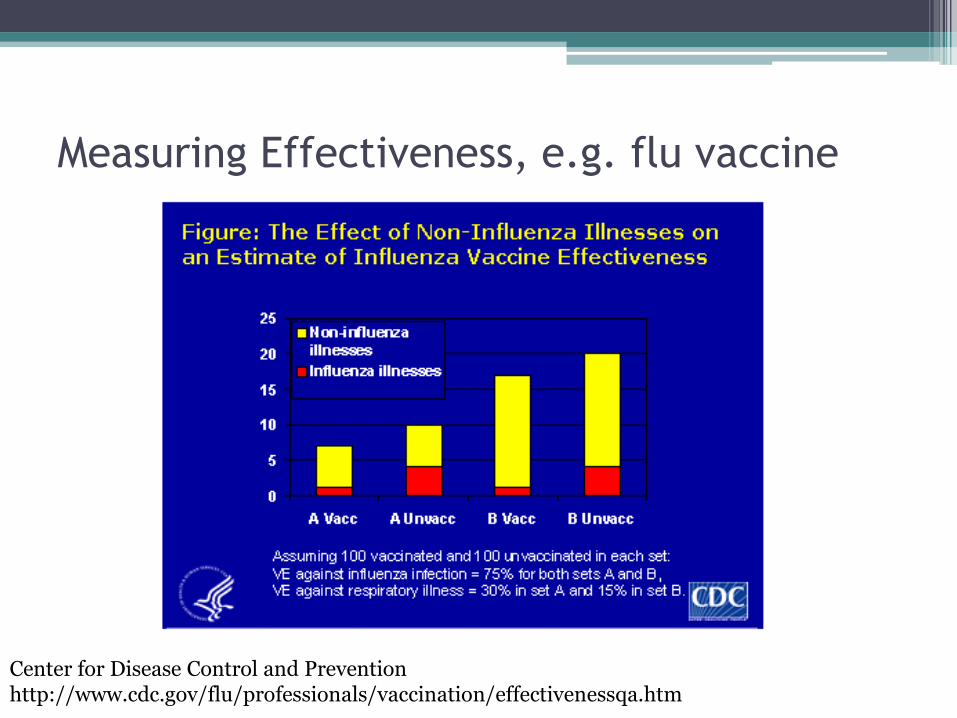
Measuring Effectiveness, e.g. flu vaccine
Center for Disease Control and Prevention http://www.cdc.gov/flu/professionals/vaccination/effectivenessqa.htm

AOA Accreditation Manual for CME
Sponsors
• Outcome Measurement: The tabulation, calculation or recording of activity or effort that can be expressed in a quantitative or qualitative manner (when attempting to measure shifts or progress toward desired levels of quality).

Outcomes continuum
Patient Education Update
http://www.patienteducationupdate.com/2005-05-01/article7.asp

Focus on Outcomes Measures
CME providers structure the
learning activity so that the physician’s
current performance is measured or
evaluated.
Physicians take what is learned in
structured CME program and then
evaluate how he/she may apply it in the
practice setting.
CME providers ask the physician to
re‐assess performance in the
practice setting through various
tools and activities.

CME credits
• Required that one CME program must be
outcomes based in CME Cycle 2013‐2015
• There is no program fee for recording outcomes measurement CME credit.
CME credits
• 1 Cat I-A hour for every 10 hours of original CME program (up to 3 hours):
▫ Round down to nearest 10 hours of credit.
Less than 10 hour CME program can still offer 1 credit.
26 hour CME program could offer ADDITIONAL 2 hours of Cat 1-A credit for completing the outcomes measurement exercise.

CME credits
• 1 Cat I-A hour for every 10 hours of original CME program (up to 3 hours):
▫ The participant successfully completes an outcomes questionnaire.
▫ At least 30 days from the last day of the initial CME program, but no more than 90 days.
▫ Even though it is only required for 1 CME event per CME cycle, this is a great way to optimize CME credits for your members.

How to Perform Outcomes Measurement
• Post Activity: Surveys/Tests/Emails/Attestation (Level 5 Outcomes Measurement – MOORE’s) • Looking for Performance Based Change • Examples:
▫ Self-Test of questions related to original CME event. ▫ Physicians asked to commit (in writing) changes that they plan to
make as a result of CME activity over next 1‐3 months. ▫ The CME sponsor emails physician participants and asks if they
have fully, partially, or were unable to implement changes they intended to make.
▫ Data is self‐reported and serves as a surrogate marker that is indicative of actual change.
▫ This exercise can be used to further drive the Needs Assessment.

MOMA’s CME Programming Model
“How it Works”

Moore’s 7 Levels of Outcomes Measurement
1. Attendance
2. Satisfaction
3. Learning
4. Competence
5. Performance
6. Patient Health
7. Community Health
Easy but of least value
Difficult but of
most value

1. Gather Attestation & Evaluation responses. Use as:
▫ Feedback for Levels 1 (Attendance), 2 (Satisfaction), and 3 (Learning).
▫ Feedback for Level 5 (Performance): Ask provider: Will you change practice behavior?
How we KNOW what we do WORKS!

Example: MOMA CME Evaluation Form
Tuesday, 4:15-5:15pm – Session D: Hood - Contraceptive Options, Benefits, and Risks Rate each evaluator: 1(P) 2(W) 3(A) 4(G) 5(E) N/A
•Presenter met educational objectives
•Presenter offered interactive opportunities
•Content level and delivery appropriate for this topic
•Will change/improve my practice skills & judgment
•Added to my confidence/ability to treat patients
•Relevance to my practice & patients
•Need for additional CME on this topic and related topics
•Comments:

2a. Employ Real-time Pre- and Post- Testing using paper or ARS. Use as:
▫ Feedback for Level 3 (Learning).
▫ Did attendees learn the key takeaways from the presentation?
▫ Example PPT slide from Dr. Hood
How we KNOW what we do WORKS!

PRE-TEST #3
• What is the incidence of regret in a
patient younger than 30 yo that has
a permanent sterility procedure?
A. 10%
B. 20% ******
C. 25%
D. 30%
E. 35%

2b. Employ hands-on training and test out by demonstration. Use as:
▫ Feedback for Levels 3 (Learning), 4 (Competence), and 5 (Performance).
▫ Ask attendees to demonstrate key takeaways from the presentation?
▫ Examples: Workshops on OMT, sutures, dermatoscope use, or charts
How we KNOW what we do WORKS!

3. Employ 30-90 day electronic OA surveys. Use as:
▫ Feedback for Levels 3 (Learning), 4 Competence, and 5 (Performance):
▫ Ask:
Content retention questions
Practice behavior questions
Grant-specific questions for reporting
Was information learned, retained, and put to use through practice change?
How we KNOW what we do WORKS!

Example: MOMA 30-90 Day OA Survey
Three component question types: (1) General Outcome Assessment of Conference Participation on Practice Behavior (4 questions)
(2) Post-Test on Specific CME Content (10 questions drawn\from presentations), and
(3) Grant: TEAM-A Management of Atrial Fibrillation
Post-Test (7 questions on practice behavior and 7 post-test content specific questions from the live TEAM-A Atrial Fibrillation CME activity). “Results of this survey will be aggregated for reporting/evaluation purposes and used by the MOMA Seminar Program Planning Committee in review of the meeting and future program planning.”

Examples: MOMA 30-90 Day OA Survey
(1). General Outcome Assessment of Conference Participation on Practice Behavior
1. “Overall, the CME presentations had positive impact on my abilities/practice? (Yes), (No), (N/A)”
2. “Overall, the CME presentations improved my skills & judgment relative to topics covered. (Yes), (No), (N/A)”
3. “Overall, the CME presentations added to my confidence/ability to treat patients relative to topics covered. (Yes), (No), (N/A)”
4. “I have made some change(s) in practice behavior as a result of the content delivered? (Yes), (No), (N/A)”

Examples: MOMA 30-90 Day OA Survey
(2)Post-Test on Specific CME Content (10 questions drawn from presentations)
1. “Which of the following diabetes medications do not need to be dose adjusted due to renal dysfunction? (a) Trajenta (b) Onglyza (c) Januvia (d) Nesina”
2. Collagenase produced by Clostridium histolyticum is the newest form of non-surgical treatment used for which of the following: (a) impingement syndrome (b) Dupuytren’s contracture (c) retinal detachment (d) rheumatoid arthritis”
Examples: MOMA 30-90 Day OA Survey
(3) Grant: TEAM-A Management of Atrial Fibrillation (7 questions on practice behavior and 7 questions on specific content from the live TEAM-A Atrial Fibrillation CME activity).
1. “As a result of participation in the TEAM A AFIB CME program, I have increased the compliance rate of my patients receiving anticoagulant therapy. (Yes), (NO), (N/A)”
2. “The HAS-BLED threshold score at which a patient is considered to be at a high risk for bleeding events is: (1), (2), (3), (4):

MOMA’s CME Programming Model “IT WORKS”

Agenda
Overview - Physician Payments Sunshine Act Final Rule
Reporting - Open Payments System
Physician Participation
Year One Reporting Issues
CME Changes - 2015 Medicare Physician Fee Schedule
Resources for Physicians

OverviewThe Physician Payments Sunshine Act is a provision intended to make financial relationships between health
care providers and manufacturers more transparent.Summary The provision requires drug and device manufacturers to report any
payments or gifts provided to physicians and teaching hospitals.
– Manufacturers covered by Medicare, Medicaid, or the Children’sHealth Insurance Program will have to report payments ortransfers of other items of value.
The provision further mandates that manufacturers and grouppurchasing organizations disclose all physician ownership andinvestment interests.
Violators would face civil money penalties, capped at $150,000annually for failing to report, and $1 million for knowingly failing toreport.

AOA’s Position• The AOA believes that collaboration between health care
professionals, scientists, and industry is an important part“life-long learning” and the education continuum.
• We support full transparency in interactions betweenphysicians and industry, and we do not believe that theserelationships are harmful or contrary to the public’s bestinterest.
• We believe these collaborative relationships play an importantrole in medical innovation, which ultimately leads to betterhealth care outcomes and improves the quality of patientcare.

ReportingAll payments to physicians of at least $10.00 or any
combination of payments exceeding $100.00. Payments include gifts, consulting fees, speaking fees, food and
beverages, travel, and research payments.
Physician ownership interest in GPOs & manufacturers.
Once the data has been submitted, CMS: Aggregates submissions at the individual physician and teaching
hospital level
Provides a 45-day period to confidentially review and, ifnecessary, dispute the data
Makes the data available on a publicly available website

Reporting - Open Payments System
• The CMS Open Payments system houses all data on payments and transfers of value made by pharmaceutical companies to physicians and teaching hospitals.
• On June 1, CMS opened its registration process so physicians and teaching hospitals could review the data reported by manufacturers before public release.
• Public reporting began on September 30.
Registration is voluntary, but necessary if you want the ability to review and dispute data reported about you.

Physician ParticipationFirst Set of Data – October 1, 2014 4.4 million reported payments
$3.5 billion in value
Attributable to 546,000 individual physicians andnearly 1,360 teaching hospitals
26,000 physicians were registered in the Open Payments System
4.8 percent physician participation

Year One Reporting Issues
CMS announced that 33 percent of all payments were notpublished in 2014. This represented $1.1 billion of a $3.5 billioncomplete data set.
• The AOA's greatest concern with the $1.1 billion of undisclosed datais that CMS has yet to announce whether these reports willeventually be available for physician review before being published.
• Some physicians impacted might already be registered in the OpenPayments System, and are still unable to see their data.
• Manufacturers and group purchasing organizations can request adelay in the publication of this data for up to four years.

Original CME Language
The original definition for direct compensation for serving as afaculty or as a speaker for a medical education program includedboth accredited and non accredited CME.
Exemption if all of the following conditions are met: The program meets the accreditation or certification requirements and standards
of the AOA, ACCME, AMA, AAFP, or ADA CERP
The applicable manufacturer does not select the covered recipient speaker nordoes it provide the third party vendor with a distinct, identifiable set of individualsto be considered as speakers for the accredited or certified continuing educationprogram
The applicable manufacturer does not directly pay the covered recipient speaker.

CME Changes 2015 Medicare Physician Fee Schedule Final Rule
Eliminates a provision of the Sunshine Act that exemptedmanufacturers from reporting payments for speakers at certifiedcontinuing medical education (CME) programs.
According to CMS, unrestricted grants or payments from industry tosupport CME or other educational activities were in fact already notrequired to be reported.

A communications campaign to expand understanding aboutthe value of physician-industry interactions
Partners for Healthy Dialogues
Goals» Partner with stakeholders, including physician and patient groups,
to create and communicate a narrative that illustrates the benefits of interactions between biopharmaceutical/medical technology companies and physicians
» Collaborate with physician organizations to provide resources that will help physicians feel comfortable and confident discussing transparency and why interactions with biopharmaceutical/medical technology companies are important to their patients’ health and well-being
» Equip patients with context and resources to help them better understand publicly reported information and what interactions between industry and physicians mean to patient care and medical innovation

Program MaterialsWebsite & Blog, Dialogues+ Videos & YouTube Page
Fact Sheets & Pocket Cards

Discussion
Grassroots Advocacy Network (GOAL) advocacy.osteopathic.org
DO Day On Capitol HillMarch 5, 2015
Department of Government Relations(202) 414-0140

AOA CME SPONSOR’S CONFERENCEMillennium Biltmore Hotel - Los Angeles, CAJanuary 8-10, 2014

AOA CMEDOCUMENT SURVEYW. Ashley Hood, DO, AOA Council on CME, MemberJanuary 8-10, 2014

Now…. It’s my turn

AOA CME Document Survey
Learning Objectives Review steps of AOA CME Documents Survey Discussion of scoring system for accreditation

AOA Document Survey
What is the Document Survey? Prior to the end of a CME sponsor’s term of accreditation, the AOA Division of CME will
review a listing of CME programs and select an appropriate program(s) for review. The AOA will then notify the sponsoring organization of the program(s) chosen for review
via certified mail and will ask the organization to submit the required information within thirty working days of notification.
The requested information will be reviewed by the AOA Division of CME and the results of this review will be forwarded to the Council on CME to determine the accreditation status of the applying organization at the next CCME meeting.
If the Council determines that serious quality problems exist, the Council has the option of notifying the sponsoring organization that it must respond to the cited deficiencies with a plan of corrective action. Organizations will be notified of the need to submit missing documentation and will be given 10-working days to submit missing information before any points are taken away.
Failure to submit the required documentation, or failure to respond to deficiencies within the 30-working days may result in an on-site visit and survey and/or the initiation of procedures that would lead to the loss of AOA Category 1 CME Sponsor Accreditation status.
If an organization requests an extension of more than 40 days, only up to 2 years of accreditation will be awarded.

“Accreditation with Commendation”
A CME Sponsor who passes the document survey with a perfect score of 100 points and submits an outcomes measurement survey will be identified as holding “Accreditation with Commendation” as a Level 3 Accreditation Status.

Document Survey Checklist
1. A description of the needs assessment process and procedure used indetermining the content and topic of the program (include any supportingdocuments). (MAJOR‐8)
2. A copy of the CME program brochure or agenda distributed toparticipants at the CME program. (MINOR‐4)
3. Copies of all program participants’ (speakers and moderators inchronological order) curriculum vitae or biosketch defining theirqualifications for involvement in the CME program. (MAJOR‐8) Partial credit is awarded based on the percentage of CVs and biosketches
provided during the document survey review. (E.g., 5 CVs provided from a totalof 10 speakers yields 4 points) All fractions are rounded down.
(Less than 50% ‐ 0) (50% ‐ 4) (90% ‐ 8)

Document Survey Checklist
4. A copy of each speaker’s signed Disclosure Declaration Statement inchronological order. (MAJOR‐8) Partial credit is awarded based on the percentage of the disclosure statements provided
during the document survey.(Less than 90% ‐ 0) (90% ‐ 4) (100% -8)
5. A copy of the CME credits requested by the AOA‐accredited sponsorfor each participating physician in accordance with the attestationdocument. (MINOR‐4)
6. A copy of the program administration evaluation document and thetotal number of evaluation documents returned by conferenceregistrants. Provide two copies of the program evaluation documentsthat were returned by conference attendees. (MINOR‐4)

Document Survey

Document Survey Checklist
7. A statement indicating the total number of registrants, and the number of attestation forms returned by conference participants. (MAJOR‐8) Partial credit is awarded.
(25% ‐ 2) (50% ‐ 4) (95% ‐ 8)
8. A statement reflecting the distribution of program evaluation documents(i.e.: The beginning of the program, random survey, etc.) (MINOR‐4)
9. A policy statement on managing grievances relative to the returned program administration and evaluation document(s). (MINOR‐4)
10. A copy of the program outcomes questionnaire and the total number of outcomes questionnaire documents returned by conference registrants. Provide two copies of the outcomes questionnaire documents that were returned by conference attendees. (MINOR‐4) within 90 days after the program

Document Survey Checklist
11A. Provide needs assessment per program topic. (MAJOR‐12) Partial credit is awarded.
(25% ‐2) (50% ‐ 4) (75% ‐6) (95%‐ 12)
11B. A statement relative to how topics and/or speakers were selected in
direct response to needs assessment procedures. (MINOR‐4)

Document Survey

Document Survey Checklist
12. If the program was commercially supported, the following additional items must be submitted: A) A copy of the formal written agreement between the AOA CME Sponsor and each
Commercial Supporter reflecting that activity (program) is educational and not promotional. (MAJOR‐8 ) Partial credit is awarded. (Less than 90 %‐ 0) (90% ‐ 4) (100% - 8)
B) Proof that commercial support is appropriately acknowledged in program brochures (submit brochures, flyers, etc. indicating such). (MINOR‐4)
C) A brief statement regarding all funding arrangements, include how funds received from commercial supporters were expended, how speakers were paid, i.e., if speakers were directly funded by a third party agent (someone besides the AOA CME sponsor/provider), attach copy of the funding arrangement between the CME sponsor and the third party agent.(MAJOR‐8 ) Partial credit is awarded. (Less than 90% ‐ 0) (90% ‐ 4) (100% - 8)
D) A statement indicating how disclosure of potential conflict of interest regarding each speaker was given to the participants. (MAJOR‐8) Partial credit is awarded. (Less than 90% ‐ 0) (90% ‐ 4) (100% - 8)

Document Survey Checklist
TOTAL SCORE = 100

Scoring Key
< 60 points on the document survey - accreditation is withdrawn
60 to 69 points on the document survey is awarded 1‐year accreditation with required attendance at the next CME sponsors conference
70 – 79 points on the document survey is awarded 1‐year accreditation
80 – 94 points on the document survey is awarded 2‐year accreditation
95 points or better on the document survey is awarded 3‐year accreditation
100 points perfect score on the document survey, including an outcomes measurement data will be awarded Level 3 Accreditation with Commendation.

Conclusions
The purpose of the AOA Document Survey is to standardize QUALITY OSTEOPATHIC CME across all AOA CME Sponsors.
The survey is to used as a tool to build your next quality osteopathic CME program.
Plan multiple CME programs with your CME planning committee!! Use your Needs Assessments and your Document Survey
tools. Call for help! Share good practices!!

QUESTIONS

Specialty Credit for Category 1A CME Sponsors
CME SPONSORS CONFERENCE
Stephen Scheinthal, DOFriday, January 9, 2014

Learning Objectives
After this presentation, you will:
• Understand the specialty credit requirement for maintenance of AOA board certification.
• Know how to submit specialty credits and how to respond to member inquiries.
• Be informed about recent changes to specialty credit requirements for AOA board certification.

Specialty Credit
• BOS has been aware that there is confusion
• Have met with CCME to resolve issue
• Felt need for action at Nov. 2014 meeting
• Specialty Credit is an important part of OCC

Osteopathic Continuous Certification
• Component 1: Unrestricted Licensure
• Component 2: Lifelong Learning/CME• Component 3: Cognitive Assessment
• Component 4: Practice Performance Assessment and Improvement
• Component 5: Continuous AOA Membership

OCC Component 2
Lifelong Learning
– Minimum of 120 credits of CME during each three-year cycle (two boards require 150 credits)
– Minimum of 50 specialty credits must be in the specialty area of certification
• As applicable, 25% of specialty credits must be in each CAQ subspecialty focus area

30 1-A Credits
CAQ Specialty
CME Credits (as applicable)
50 Specialty
CME Credits
AOA CME Requirements120 CME Credits

Qualified Specialty Credit
• Speaker must be certified in the specialty being presented (or be otherwise qualified)
• Topic must be of interest to DOs certified in the specialty for which specialty credit is sought

Specialty Credit Roster
• Submit Roster of Specialty CME with Roster of Attendance
• Physicians can appeal – CME will provide a form for individual requests


Recent Changes
• Removed caps on specialty CME for:– State Society Seminars
– Acute Care Hospital Programs
– COM Seminars
– Osteopathic Foundation Seminars
• Task Force established to review specialty CME as a whole

Questions / Concerns?
For questions on the OCC process, please contact your specialty certifying board. The AOA Division of
Certification can help you as well.
AOA Division of Certification(800) 621-1773, ext. 8266

Delivering Live CMEs OnlineROWAN UNIVERSITY SCHOOL OF OSTEOPATHIC MEDICINE
JOSHUA S. COREN, D.O. , MBA, FACOFP
VICE CHAIR AND ASSOCIATE PROFESSOR, FAMILY MEDICINE

Learning Objectives
Demonstrate an example of an online CME program for a live audience
Examine resources to enable the creation of an online CME program
Outline basic logistical set‐up of an online CME program

The Training Gap (The Formula) Balancing effective pain management
+ Ensuring patient safety + Increasing prevalence of addiction
+ Increasing drug use disorders=
Complex and often misunderstood challenge in medical care.

The Training GapOften overlooked…
Both pain and addiction management can be frustrating aspects of clinical care due to
◦Lack of provider training ◦Legal concerns◦Time constraints in patient care.

The Training Gap
On one hand patients may hide their
use of controlled substances from
providers; on the other hand, patients
disclosing true pain may not be
receiving appropriate medical care.
The Training Gap
Addiction is the number one cause of preventable illness and death in the US
&At the same time a chronic pain management burden which outweighs many common chronic care diseases including diabetes and heart disease combined.
360⁰ FeedbackCalibrating Pain and Addiction ManagementDefine pain as a chronic care condition.
Explain the etiologies of addiction and challenges of recovery from a patient’s viewpoint.
Identify the basic principles of opioid maintenance and refer patients misusing opioids to methadone and buprenorphine treatment.
Develop effective strategies for health care quality to prevent diversion and addiction while meeting the needs of patients with pain.
Construct integrative and multidisciplinary approaches to care for patients with chronic pain or addiction.

Faculty
3 Pain Management Specialists2 Addiction Specialists1 Clinical Psychology Doctorate

Live CME PresentationsCME presentations are given by speakers in the school auditorium at a podium with a desktop computer with their presentation.
The image on the computer screen is projected onto the larger screens in the auditorium for the live audience to view.

Presentation Recording and DeliveryAt RowanSOM, the live CME presentation is also:
Being recorded, as it is given, to a local hard drive

Presentation Recording and DeliveryAt RowanSOM, the live CME presentation is also:
Recorded as it is being given to a local hard drive
Being Broadcast as it is given to online attendees
The Equipment UsedEverything can be done with just ONE laptop.
The live presentation.
The recording of the live presentation.
The broadcast online.

Live Presentation RecordingAt RowanSOM, we have a dedicated lecture capture system. All of our recorded presentations are sent to a dedicated server. If you do not have a lecture capture system, the same type of recording can be accomplished with a screen capture software. Pricing for the software can beunder $200.00.

Live Presentation BroadcastFor streaming broadcast of live events and presentations. Costs can be about $500 per year for one license with no limit on broadcasts and allows you to:
1. Capture video from many sources 2. Produce live during broadcast 3. Stream your presentation LIVE

CME Q & AAn Email question submission system was put into place. For any online or live attendee, there is an option to submit questions to an email address. In our case, we use a dedicated email address: [email protected]. (There are a number of free email options if you do not have a dedicated email.) The questions are all received by the CME administrator who has access to the question email and the questions received are triaged to the appropriate speaker. Questions can be responded to in real‐time during the CME event or after the event.

CME Pre‐Test & Post‐TestThe CMEs also have participants take a pre‐test before the CME presentation and a post‐test right after the CME. Participants are able to do both on the day of the CME. The post‐test must be taken to receive the 1A credit and a score of 70% or better is required. The online participants are sent electronic versions of the pre‐test and post‐test via a survey/polling application.

CME AdministrationThe CME administration is handled by one individual who does everything from attendee registration to creating and sending out the pre and post‐tests as well as duties needed for attendee attestation and accreditation. There is IT support provided on the day of the CME in the form of one IT technician to set up all equipment and to be available in the event there are technical issues.

SummaryThe CME presentation process does necessarily not require a lot of resources.
Online broadcast of CME presentations are possible using one laptop and some low‐cost software applications.
The cost of an adequate laptop, microphone and software would be approximately $2,000 ‐$2,500.
Live CMEs award 1A credit and the recorded CME awards 1B credit.

The End

State Mandated CMERequirements for
Relicensure
Nicholas A. Schilligo, MSAssociate Vice PresidentState Government AffairsAmerican Osteopathic Association

CME Mandates
Relicensure Requirement
Remain Up to Date with Advancements
Assure Competency
Protect the Public

Significant Variation
• Colorado, Indiana, Montana, and South Dakota
• New York
• Everyone Else

The Varying Requirements
• Number of Credits/Hours
• Type of CME – (AOA vs. AMA)
– Category 1, 1-A, 2, etc..
• Subject Specific
• Length of Term
Trends in CME Mandates
• Addressing public health concerns
• Promoting changes in health care delivery

Addressing Public Health Concerns
Infectious Disease
AIDS/HIV
Suicide
Child and Dependent Adult Abuse
Prescription Drug Abuse

Promoting Changes inHealth Care Delivery
Massachusetts: Certifying Proficiency in Electronic Health Records

AOA PositionH278-A/04 MANDATORY CME COURSE REQUIREMENTS
The American Osteopathic Association opposes any federal attempts to impose any specific continuing medical education (CME) course requirements and will assist any component societies in opposing additional specific CME course requirements. 2004; reaffirmed 2009

AOA Resources
• US Licensure Summaryhttp://www.osteopathic.org/inside-aoa/development/licensure/Pages/us-licensure.aspx
• AOA Staff– [email protected]
– (312) 202-8185

Thank You!

State Mandated CME Requirements for RelicensureThe Rhode Island Experience

Current Rhode Island CME requirements Physicians are required to document to the Board of Medical Licensure
and Discipline that they have earned a minimum of forty (40) hours of AMA PRA Category 1 credit or American Osteopathic Association Category 1a continuing medical education credits.
CMEs on Public Health Topics At least 2 hours of continuing medical education shall be earned on
topics of current concern as determined by the director of the Rhode Island Department of Health. Current topics include:
Risk Management Opioid pain management / chronic pain management End of life / palliative care Infection control

Historical context Mid‐late 1980’s heightened concern about blood borne pathogens
Lack of uniformity in precautions among health care workers
Series of high profile instances of patient to practitioner and practitioner to patient transmissions

State law enacted in the mid 1990’s requiring 2 hours of CME in bloodborne pathogens
Acceptance of the standards for Universal Precautions and a better understanding of HIV transmission were issues leading the discussion
A better understanding and adoption of these precautions would help protect practitioners and their patients

Initial CME mandates were directed at HIV, Hepatitis C, needle sticks, etc.However, the mandated courses were repetitive and didn’t pertain to all specialties and practicesOther topics were introduced based on relevant public health priorities at the time

How were these added?
6.2.1 Said continuing medical education shall include a minimum of two (2) hours from a list of topics related to current public health needs, which list shall be developed by the Director in consultation with and as approved by the appropriate medical or osteopathic society. The list shall be available to physicians as of 1 July of each even‐numbered year. (emphasis added)

RI approved topics Universal precautions/infection control Bioterrorism End of life/palliative care OSHA Risk management Ethics Pain management
Problems with mandated topics Looks good, legislators and regulators feel like they are doing something to address priorities in health care delivery
Efficacy of these mandates in doubt No objective measures of change in practice Once added, difficult to remove

Medical society pushback
Rhode Island Medical Society Council Meeting of Monday, April 2, 2012
“It is RIMS and AMA policy to oppose content‐specific CME mandates in principle. “
Responsibility for setting standards of CME should be that of the medical profession, not legislators and regulators.
Notably, the RI BMLD has not experienced problems with individual licensees contesting or having difficulty meeting these requirements.

Documenting CME in Rhode Island 6.4 It shall be the sole responsibility of the individual physician to obtain documentation from the approved sponsoring or co‐sponsoring organizations, agencies or other, of his or her participation in a learning experience and the number of dated credits earned. (emphasis added)
6.4.1 Those documents must be safeguarded, for a period of three (3) years, by the physician for review by the Board if required. Only a summary list of those documents, not the documents themselves, shall be submitted with the application for renewal of the certification. (emphasis added)

Future plans Review the list of topics of current concern Consider removing risk management and adding topic of addiction
Directed CME better addressed through MOC/OCC?

Page 1
21th National AOA Category 1 CME Sponsors Conference Millennium Biltmore Hotel
Los Angeles, CA 90071
Jan. 8-10, 2015
"Thriving in a Changing Environment"
Timothy Cheslock, DO W. Ashley Hood, DO Conference Chair Conference Co-Chair
Please evaluate this educational activity as a whole by filling in the appropriate box: Excellent Good Fair Poor A. Usefulness
B. Quality
C. Facilities/Management
D. Registration
E. Environment
F. Audiovisuals
G. Food & Beverage
FACULTY EVALUATIONS: Please rate the activity for each faculty member listed: DAY 1: Thursday, Jan. 8, 2015 The Emerging CME Environment Alejandro Aparicio, MD, FACP, Director, Division. Of Continuing Physician Professional Development, American Medical Association Objectives:
1. Summarize the evolution of formal CME in the US. 2. Describe the current trends and forces impacting CME. 3. Discuss, based on current trends and forces, a likely future for CME.
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly

Page 2
Understanding the AAFP, AMA PRA Category 1™ and AOA Credit Systems Jeffrey S. Grove, DO, Chair, Council on CME, American Osteopathic Association & Alejandro Aparicio, MD, Director, Division of Continuing Physician Professional Development, American Medical Association Aparicio’s Objectives:
1. Summarize the history of the AMA Physician Recognition Award and the CME credit system created to support it.
2. Compare and contrast AMA PRA Category 1 Credit™ and AMA PRA Category 2 Credit™. 3. Compare and contrast provider credit, direct credit and international credit conversions. 4. Describe the different learning formats that can be certified for AMA PRA Category 1 Credit™.
Grove’s Objectives: 1. Discuss the AAFP, AMA PRA Category 1 Credit™ and AOA credit systems. 2. Compare and contrast the requirements for designating and awarding the different types of credit. 3. Determine when each type of credit may be appropriate for the activities you produce.
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly CME Update – AOA CME Guide and AOA Accreditation Requirements Timothy Cheslock, DO, Member, Council on CME, American Osteopathic Association Objectives:
1. Understand the changes to the 2013-2015 CME Guide for AOA Members. 2. Updates regarding the AOA Board of Trustees Action for 2014. 3. Review of the Accreditation Guidelines for AOA Category 1-A Sponsors.
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly DAY 2: Friday, Jan. 9, 2015 Needs Assessment James E. Preston, DO, Vice Chair Council on CME, American Osteopathic Association Objectives:
1. Attendee will be able to recognize the justification for Needs Assessments in their CME programs. 2. Attendee will discover the different types of Needs and how to prioritize them for medical practice
improvement purposes. 3. Attendee will learn how to link their CME Committee Needs Assessments to AOA Competencies to
facilitate learner medical practice improvement. Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly Content Gautam Desai, DO - Member, Council on CME, American Osteopathic Association & Holly B. Laird, OMS III Student Member, Council on CME, American Osteopathic Association Objectives:
1. Learn about different formats of CME delivery. 2. Realize the advantages to having a non-traditional CME program. 3. Understand the needs of a younger generation of learners.

Page 3
Excellent Good Fair Poor Content of presentation Were the objectives met? Ability to convey the subject matter clearly Outcome Measures W. Ashley Hood, DO, Member, Council on CME, American Osteopathic Association & Ed Williams, Ph.D., Executive Director of Louisiana Osteopathic Medical Association and Mississippi Osteopathic Medical Association Objectives:
1. Discuss the importance of measuring outcomes. 2. Understand the AOA Council on CME accreditation standards and the awarding of CME credits
related to outcomes measures. 3. Be able to implement various options to measure outcomes related to a CME program. 4. Utilize outcomes measures to build your needs assessment.
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly Implications of Physician Payments Sunshine Act Final Rule Ray Quintero, Vice President, Government Relations, American Osteopathic Association Washington Office Objectives:
1. Describe the function of the Open Payments System. 2. Detail issues related to physician participation in the September release of data. 3. How was CME impacted by the 2015 Medicare Physician Fee Schedule?
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly How to get a Perfect Score on your Document Survey W. Ashley Hood, DO, Member, Council on CME, American Osteopathic Association Objectives:
1. Review steps of AOA CME Documents Survey. 2. Discussion of scoring system for accreditation. 3. Be able to create your next CME event based on the document survey.
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly How to Properly Report CME Specialty Credits for Your CME Programs Using the “Applicable Credits by Specialty Form” Stephen M. Scheinthal, DO, Chair, Bureau of Osteopathic Specialists, American Osteopathic Association. Objectives:
1. Understand the specialty credit requirement for maintenance of AOA board certification. 2. Learn how to submit specialty credits and how to respond to member inquiries. 3. Learn about recent changes to specialty credit requirements for AOA board certification.
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly

Page 4
Delivering Quality Education via the Internet: Live, Virtual and Enduring Materials Joshua S. Coren, DO, MBA, Vice Chair & Associate Professor, Department of Family Medicine, Rowan University School of Osteopathic Medicine Objectives:
1. Demonstrate an example of an online CME program that can be conducted to a live audience. 2. Examine resources to enable the creation of an online CME program. 3. Outline basic logistical set-up of an online CME program..
Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly State Mandated CME Requirement for Relicensure – Panel Discussion Nick Schilligo, MS, Associate Vice President, State Government Affairs, American Osteopathic Association Geraldine T. O’Shea, DO, President, AAOE & AOA Board Member, Ronald R. Burns, DO, Past Chair, Florida Board of Osteopathic Medicine &AOA Board Member, and James Griffin, DO, Member, Rhode Island Board of Medical Licensure and Discipline Objectives:
1. Provide an overview of state CME requirements for relicensure. 2. Discuss national trend of states addressing public health concerns by mandating certain subject
specific CME. 3. Educate on state specific examples of CME mandates for relicensure; state requirements as they
relate to these mandates—live in person, number of credits, subjects, etc.. Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly Panel Discussion – Ask Questions of the CCME Moderator –Jeffrey S. Grove, DO, Chair, Council on CME, American Osteopathic Association Objectives:
1. Discussion of the AOA CME Program. 2. Awarding CME credits for different types of activities. 3. Discussion – any and all questions relating to the AOA CME program and accreditation
requirements. Excellent Good Fair Poor
Content of presentation Were the objectives met? Ability to convey the subject matter clearly DAY 3: Saturday, Jan. 10, 2015 CME Innovation Denise Selleck, CAE, Executive Director, Nevada Osteopathic Medical Association Objectives: 1. Learners will share innovations they have incorporated over the last year. 2. Learners will review the design of programs they offer and identify one area for improvement. 3. Learners will evaluate their programs and determine if innovation or change will increase effectiveness. Excellent Good Fair Poor Content of presentation Were the objectives met? Ability to convey the subject matter clearly

Page 5
General comments:
A. Suggested topics and/or presenters you would like for the 2016 CME Sponsors Conference:
B. Please enter additional comments here and on the back side of this sheet:
C. Would you participate in on-line modules as a substitute/replacement of the CME Sponsors
Conference?
Yes___ No___
PLEASE GIVE THIS FORM TO CONFERENCE STAFF BEFORE YOU LEAVE.
THANK YOU!