thoracic radiographic anatomy
DESCRIPTION
Thoracic Radiographic Anatomy. Einav Shochat MS4 Visiting Medical Student. PA and Lateral Chest Radiograph. Lobar Anatomy. There are three lobes in the right lung and two in the left Lobes are divided into anatomic segments; each is supplied by its own bronchus and blood vessels. - PowerPoint PPT PresentationTRANSCRIPT
Thoracic Radiographic
AnatomyEinav Shochat MS4
Visiting Medical Student

PA and Lateral Chest Radiograph
Lobar Anatomy
There are three lobes in the right lung and two in the left
Lobes are divided into anatomic segments; each is supplied by its own bronchus and blood vessels
RUL RUL
RML
RML
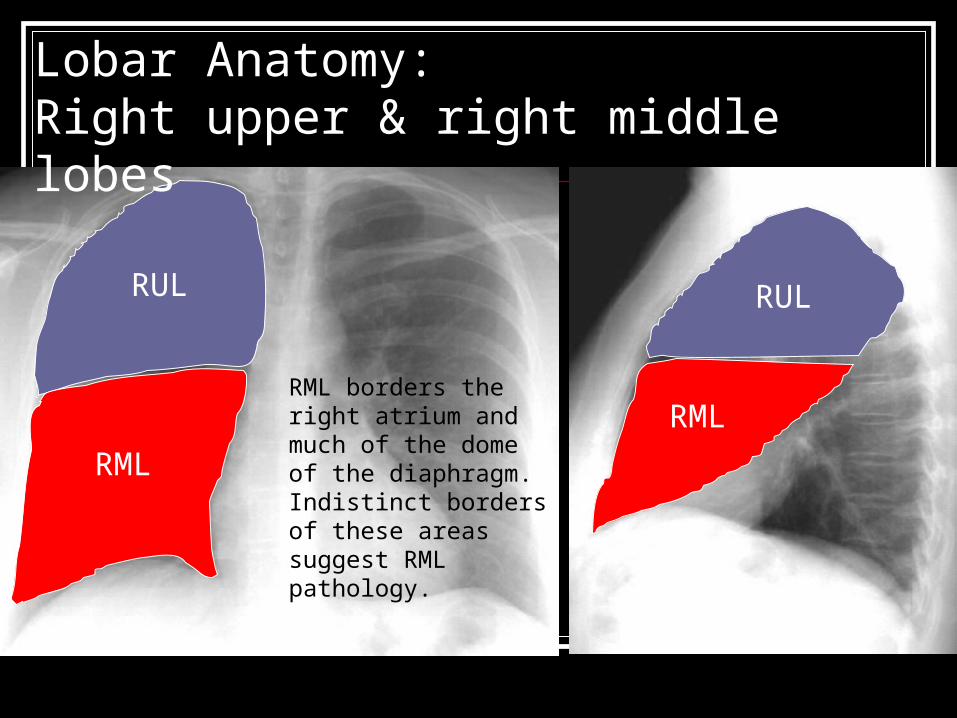
Lobar Anatomy: Right upper & right middle lobes
RML borders the right atrium and much of the dome of the diaphragm. Indistinct borders of these areas suggest RML pathology.
RLL
RLL
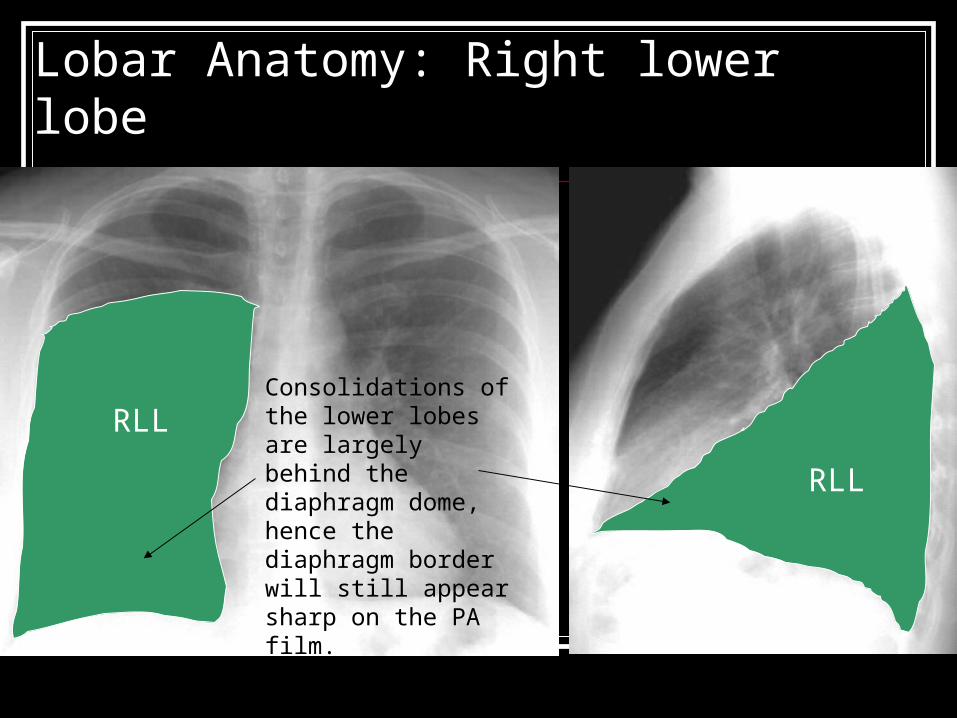
Lobar Anatomy: Right lower lobe
Consolidations of the lower lobes are largely behind the diaphragm dome, hence the diaphragm border will still appear sharp on the PA film.

LULLUL
Lobar Anatomy: Left upper lobe
LUL borders the left atrium, left ventricle and much of the dome of the diaphragm. Indistinct borders of these areas suggest LUL pathology.
LLL LLL
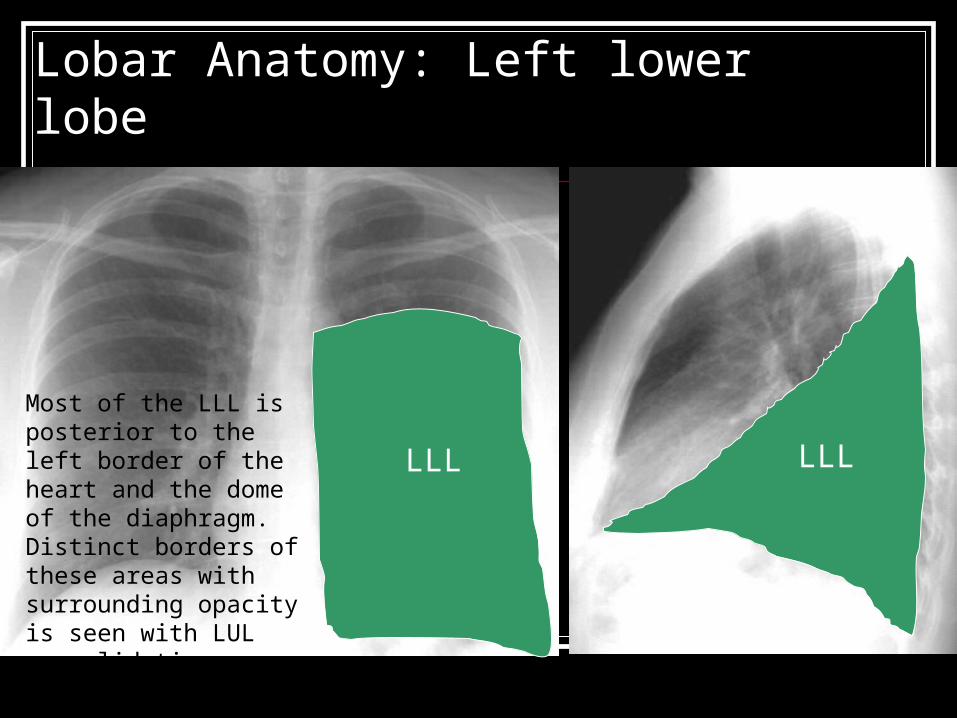
Lobar Anatomy: Left lower lobe
Most of the LLL is posterior to the left border of the heart and the dome of the diaphragm. Distinct borders of these areas with surrounding opacity is seen with LUL consolidations.

Can you find the source of this patient’s fever and cough?

Can you find the source of this patient’s fever and cough?
Left LowerLobe
pneumonia
Note the abnormal opacification of the lower vertebrae in the lateral view. Normally there is less soft tissue around the inferior thoracic vertebrae making them appear darker than the more superior vertebrae. See next slide for comparison.
Distinct borders
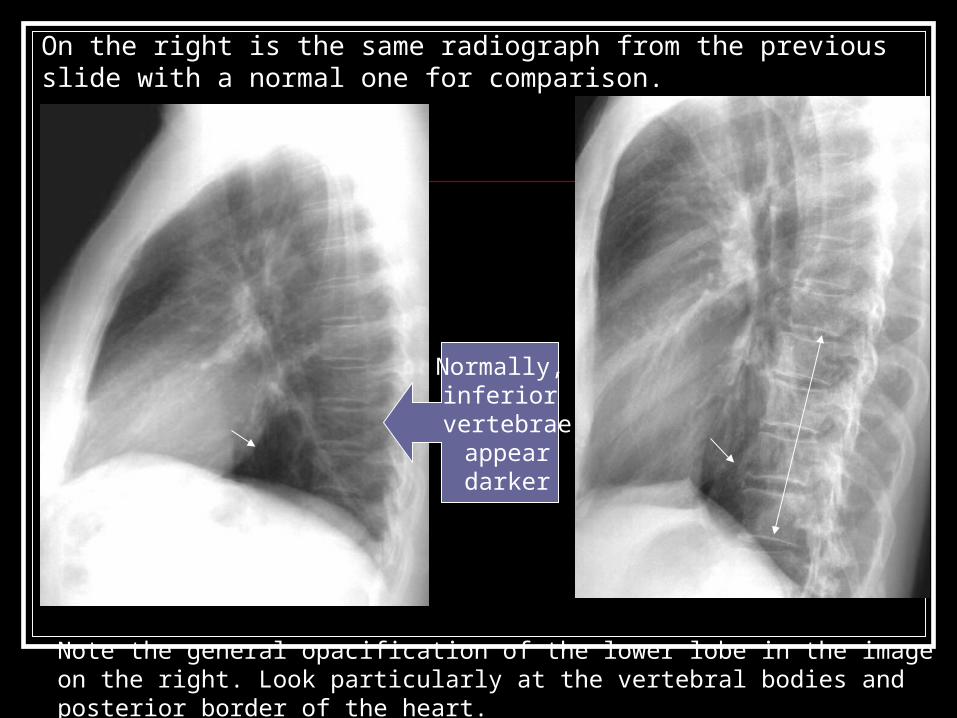
On the right is the same radiograph from the previous slide with a normal one for comparison.
Normally,inferior
vertebrae appear darker
Note the general opacification of the lower lobe in the image on the right. Look particularly at the vertebral bodies and posterior border of the heart.
Lobar Anatomy The lobes of the lungs are lined by visceral
pleura, which normally is not visualized except along the interlobar fissures
Fissure anatomy may have many anatomic variations and may not be complete
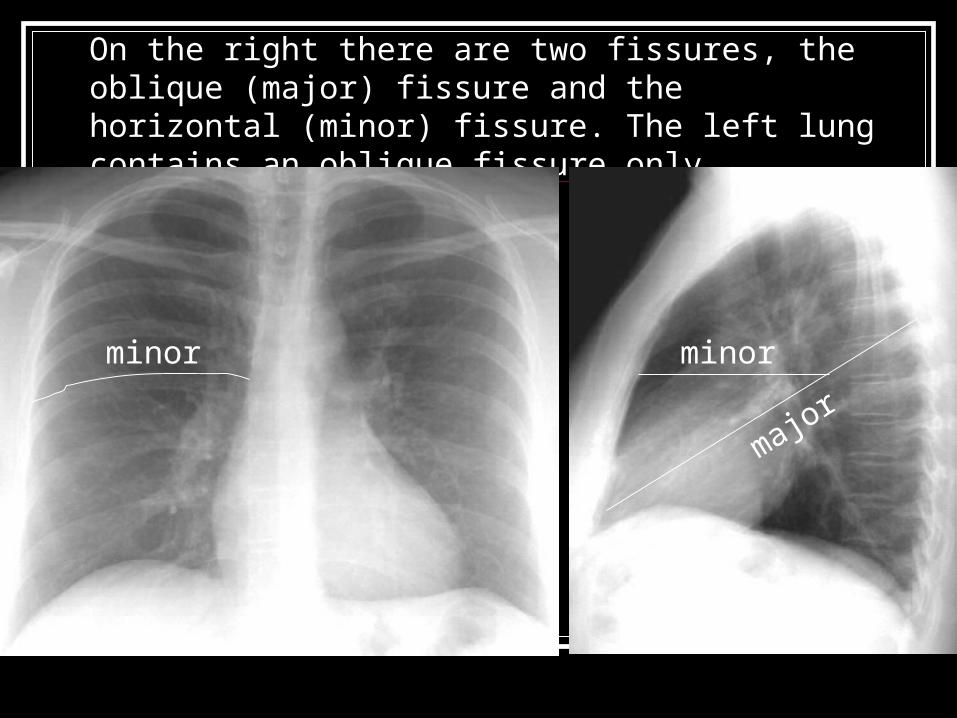
On the right there are two fissures, the oblique (major) fissure and the horizontal (minor) fissure. The left lung contains an oblique fissure only.
minor
major
minor
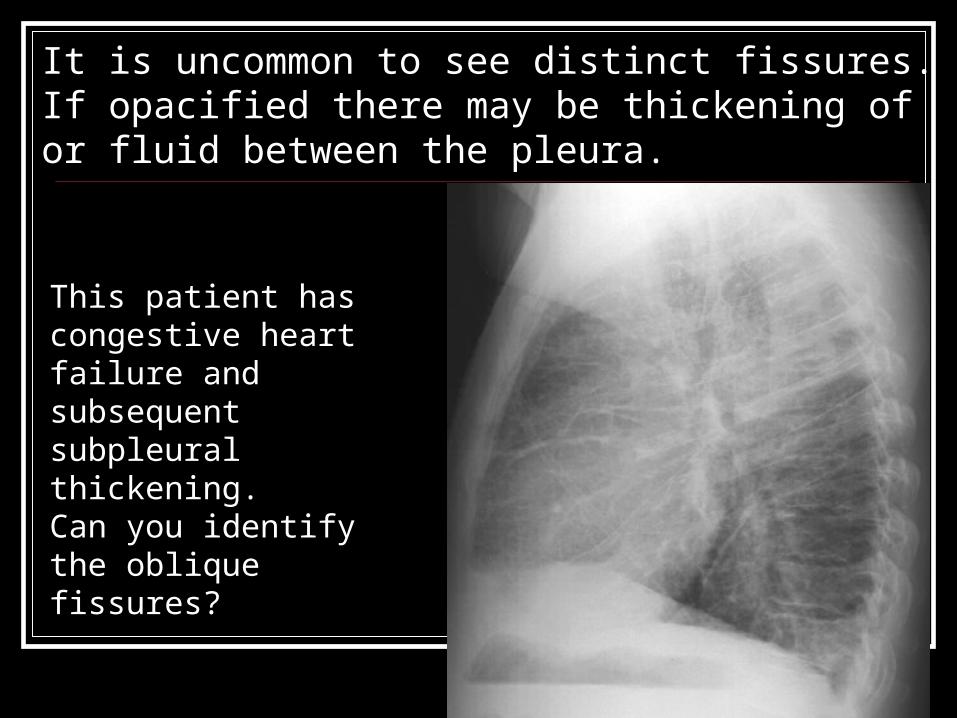
It is uncommon to see distinct fissures. If opacified there may be thickening of or fluid between the pleura.
This patient has congestive heart failure and subsequent subpleural thickening. Can you identify the oblique fissures?
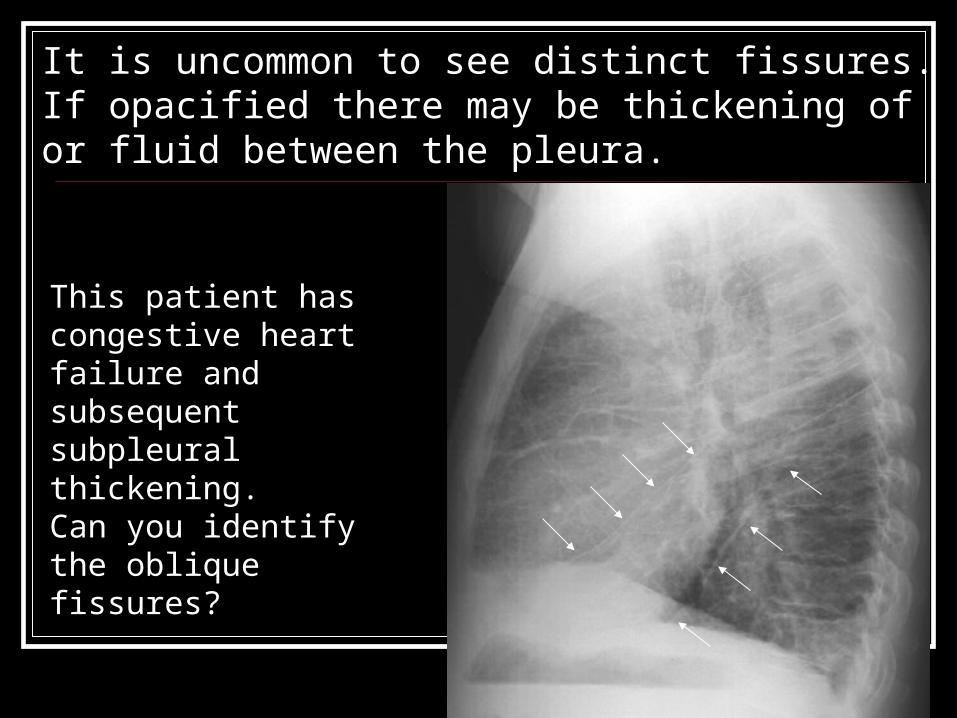
It is uncommon to see distinct fissures. If opacified there may be thickening of or fluid between the pleura.
This patient has congestive heart failure and subsequent subpleural thickening. Can you identify the oblique fissures?

Here there is fluid trapped between the pleura within the fissures.
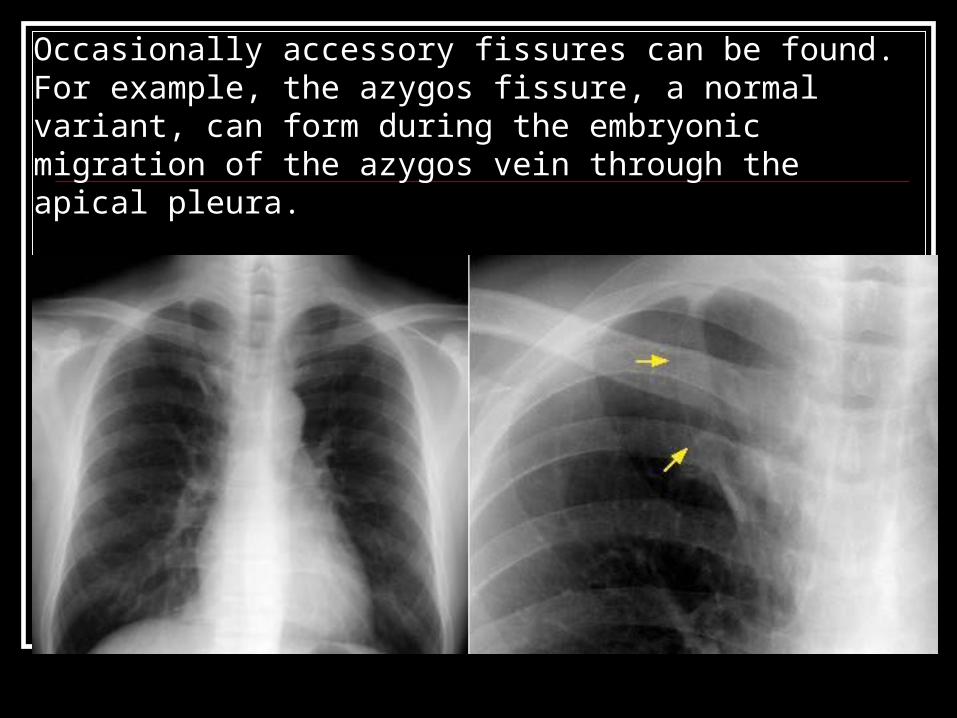
Occasionally accessory fissures can be found. For example, the azygos fissure, a normal variant, can form during the embryonic migration of the azygos vein through the apical pleura.
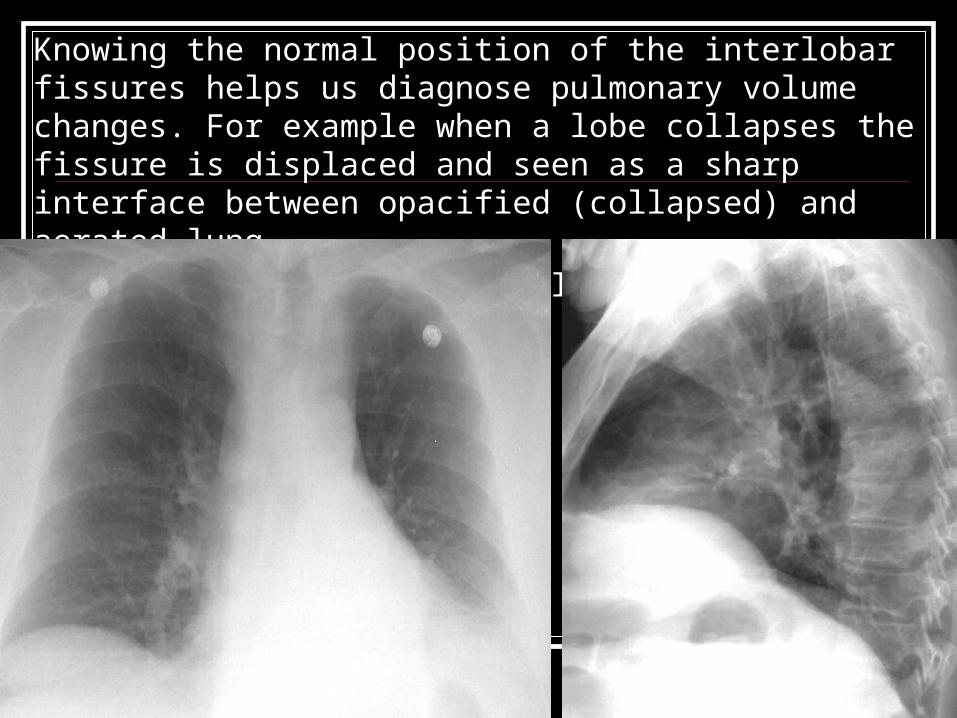
Knowing the normal position of the interlobar fissures helps us diagnose pulmonary volume changes. For example when a lobe collapses the fissure is displaced and seen as a sharp interface between opacified (collapsed) and aerated lung.
Can you identify the pleural lining of the collapse lung?
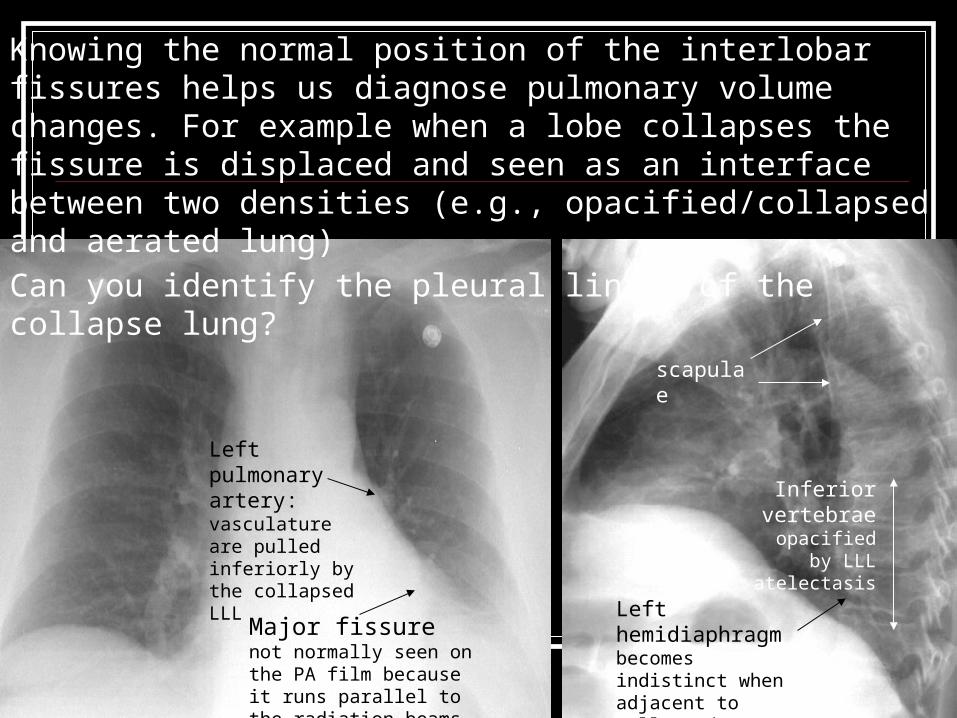
scapulae
Major fissure not normally seen on the PA film because it runs parallel to the radiation beams
Knowing the normal position of the interlobar fissures helps us diagnose pulmonary volume changes. For example when a lobe collapses the fissure is displaced and seen as an interface between two densities (e.g., opacified/collapsed and aerated lung)
Can you identify the pleural lining of the collapse lung?
Left hemidiaphragm becomes indistinct when adjacent to collapsed LLL
Inferior vertebrae
opacified by LLL atelectasis
Left pulmonary artery: vasculature are pulled inferiorly by the collapsed LLL

What’s happened here?

What’s happened here?
Right upper lobe collapse

We can use the pleura to identify whether a mass is within the lung parenchyma or in the extrapleural space. Is this mass intrapleural or extrapleural? How can you tell?
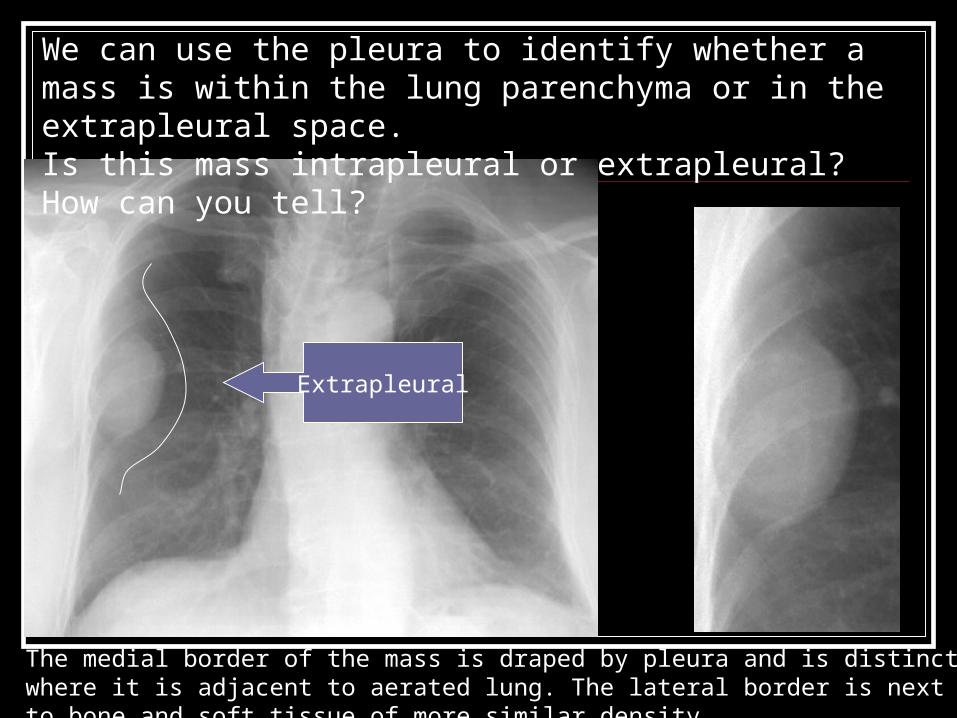
We can use the pleura to identify whether a mass is within the lung parenchyma or in the extrapleural space. Is this mass intrapleural or extrapleural? How can you tell?
Extrapleural
The medial border of the mass is draped by pleura and is distinct where it is adjacent to aerated lung. The lateral border is next to bone and soft tissue of more similar density.

The pleura is often involved in inflammatory and traumatic insults to the chest. These may result in areas of thickening or distortion of the pleural lining, which may be appreciated in the normally sharp costophrenic & cardiophrenic angles/sulci.
Lateral costophrenic angle
Lateral costophrenic angle
Posterior costophrenic angle
Cardiophrenic angle

Pleural effusions can be identified by: blunting of the lateral and posterior costophrenic sulci, a meniscus sign, opacification of a hemithorax, and/or fluid in the fissures.
Small free-flowing pleural effusions are best identified on the lateral radiograph as this view captures the most dependent region of the thoracic cavity, the posterior costophrenic angles.

Mediastinum Many structures can be identified within
the mediastium; we will start with the heart and blood vessels…

How many structures can you identify?

LV
RV
SVCAortic pulmonary recess
Left
Aortic arch
Aor
ta
RA
pulmonary
artery
LA
Right pulmonary
artery
Right pulmonary artery(lower lobe)
Vascular pedicle

How many structures can you identify?
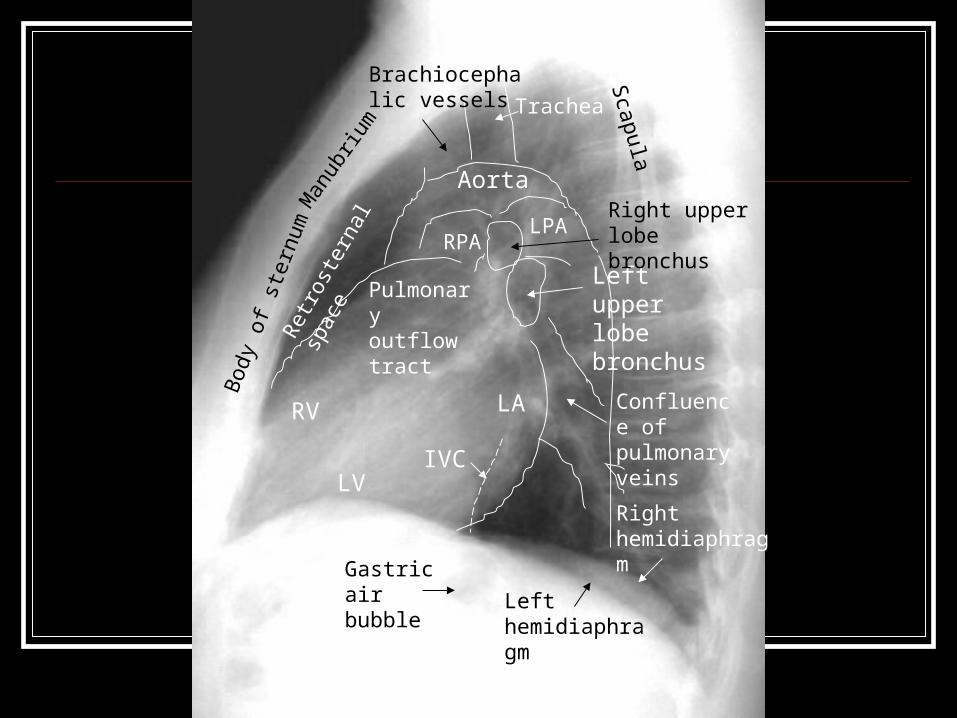
Gastric air bubble
Left upper lobe bronchus
IVC
Right hemidiaphragm
LV
LARV
Pulmonary outflow tract
AortaRight upper lobe bronchusRPA
LPA
Confluence of pulmonary veins
Brachiocephalic vessels Trachea
Left hemidiaphragm
Scapula
Man
ubriu
m
Bod
y of
ste
rnum
Ret
rost
erna
l spa
ce

Which valve has been replaced?

Which valve has been replaced?
Aortic valveNote the orientation of the valve perpendicular to the plane of the PA film.

Which valve has been replaced?
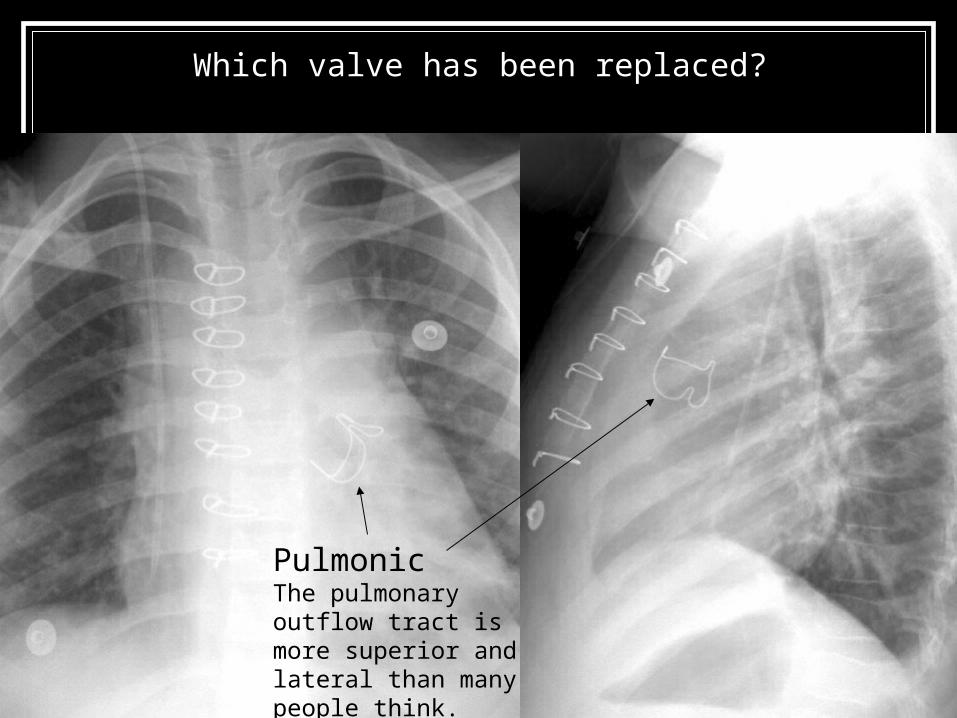
Which valve has been replaced?
PulmonicThe pulmonary outflow tract is more superior and lateral than many people think.

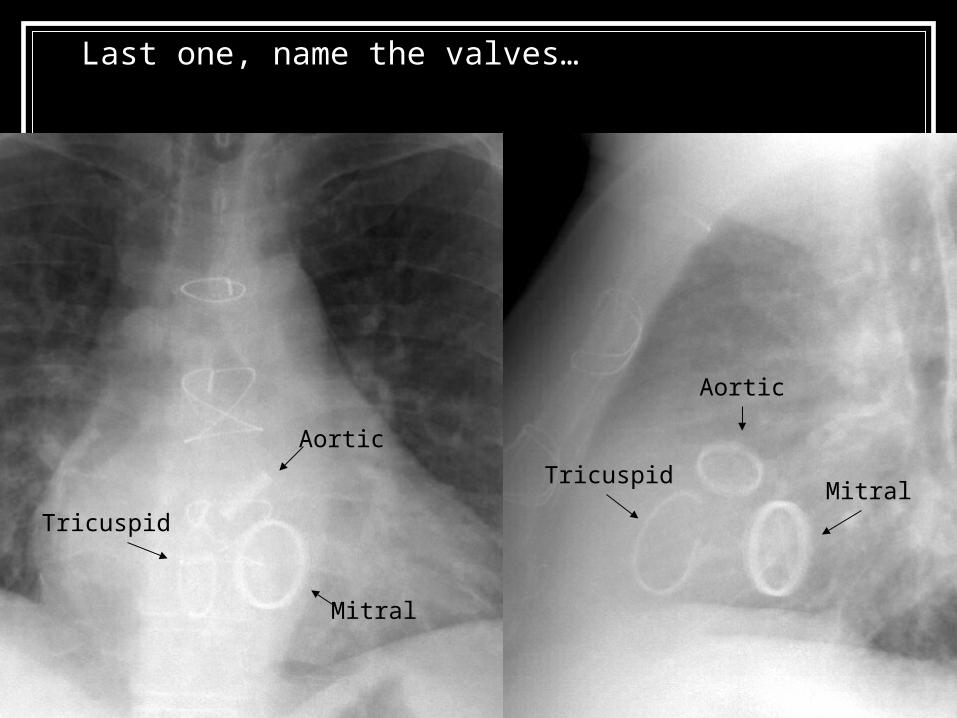
Last one, name the valves…
Last one, name the valves…
Aortic
Tricuspid
Mitral
TricuspidMitral
Aortic

The Vascular Pedicle Found in the superior mediastinum. Right and left margins are normally formed by the
superior vena cava and the descending portion of the aortic arch, respectively.
A widened vascular pedicle can have several etiologies including elevated intravascular volume, aortic trauma, or pericardial effusion.

Vascular pedicle
Aortic arch
Superior vena cava
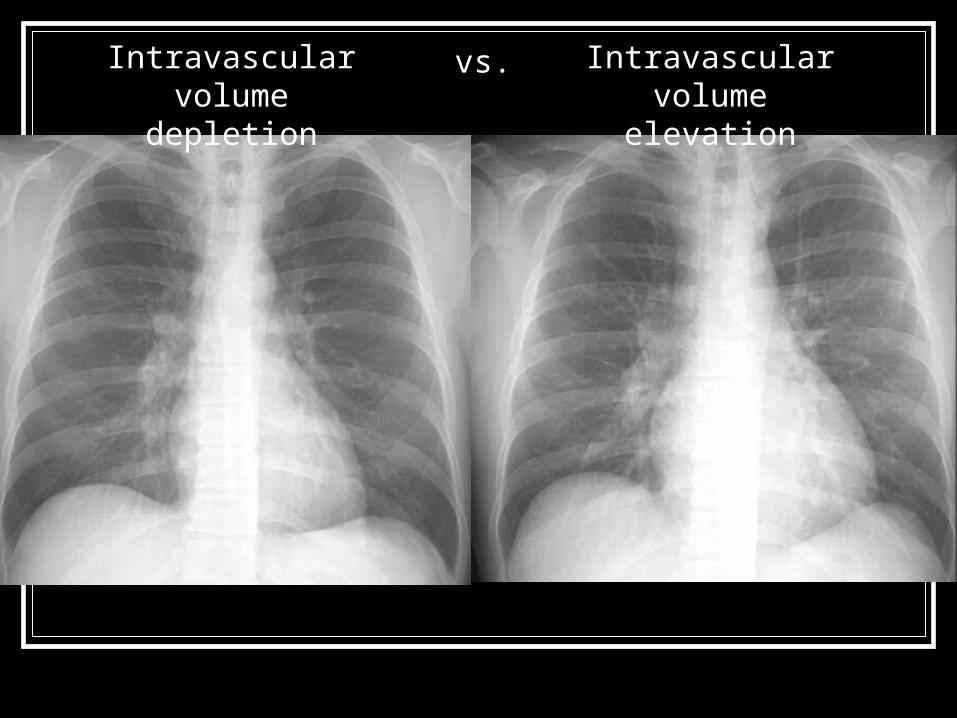
Intravascular volume depletion
Intravascular volume elevation
vs.

Vascular pedicleVascular
pedicle
Intravascular volume depletion
Intravascular volume elevation
Intravascular volume elevation resulting in an expanded SVC should not be mistaken for hematoma, which would have a less distinct border and more opacified appearance.
vs.
Superior vena cava
AortaSuperior vena cava
Aorta

Trauma patient with an aortic transection
Note the vascular pedicle’s “fuzzy”, opacified right border.

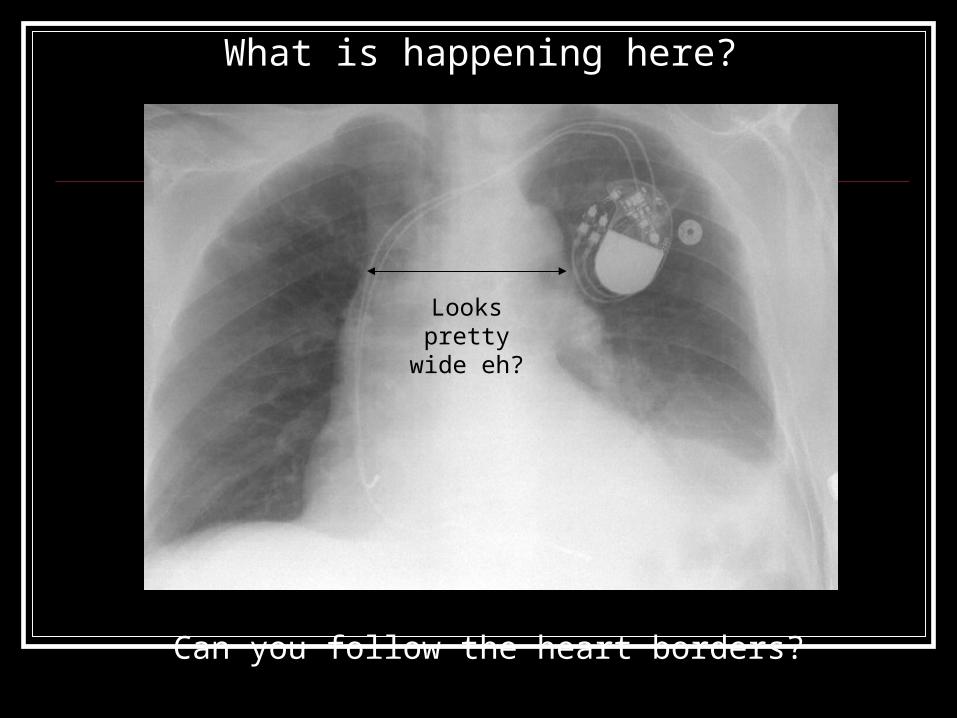
What is happening here?
What is happening here?
Looks pretty wide eh?
Can you follow the heart borders?

What is happening here?
The wide vascular pedicle here results from a pericardial effusion
The pacemaker wires roughly outline the right atrium border
If you look closely you can make out the superior pericardial border
The left heart border can be seen within the effusion
effusioneffusion
Comparing this with older films can also help make the diagnosis.

Pulmonary Airways & Vasculature The lungs on the normal chest radiograph
are made by pulmonary vessels, the bronchi are normally not seen.
This is because: Pulmonary vessels are blood-filled with density
similar to water. Bronchi are filled with air and normally have thin
walls that do not provide contrast to aerated lungs.
Pulmonary Airways & Vasculature When lung parenchyma fill with water or
inflammatory material: Water-density vessels become less distinct. Air-filled bronchi can be seen as “air
bronchograms”. If airways are obstructed (e.g., tumor) they may fill
with fluid and no “air bronchograms” will be appreciated.

How do these two radiographs differ?
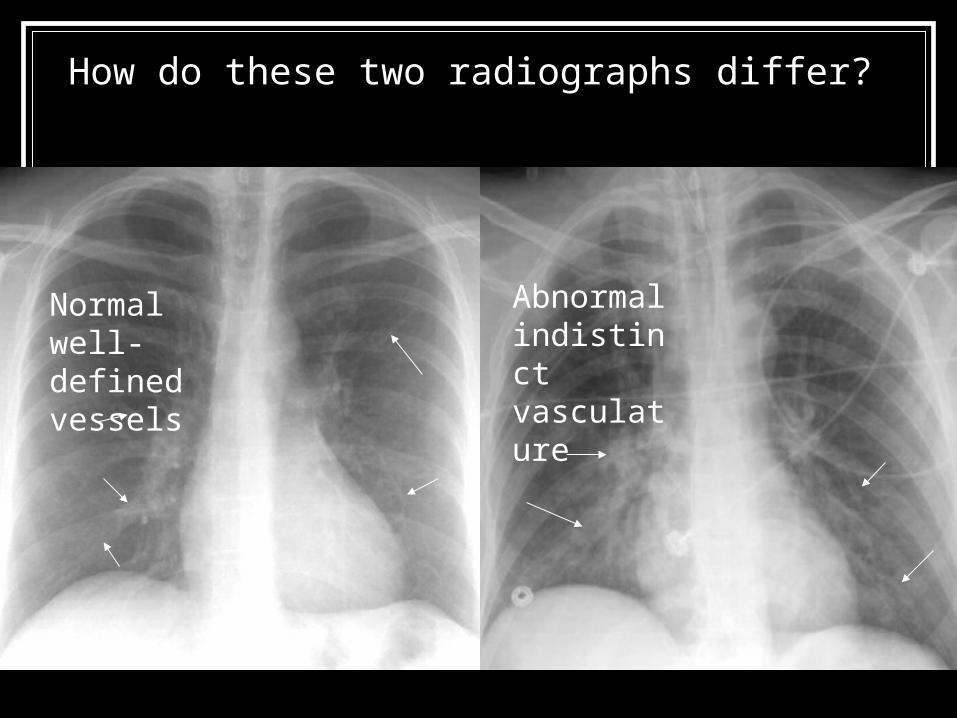
How do these two radiographs differ?
Normal well-defined vessels
Abnormal indistinct vasculature

In the normal chest radiograph only airways within the mediastinum are apparent.
Trachea
Left mainstem bronchus
TracheaRight mainstem bronchus
Left mainstem bronchus
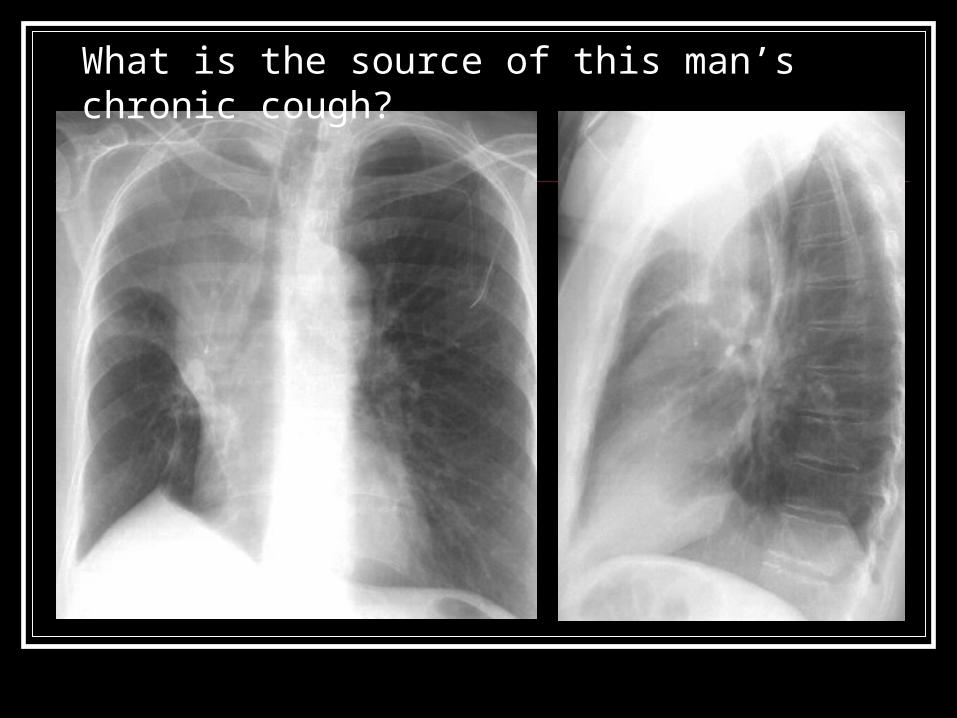
What is the source of this man’s chronic cough?
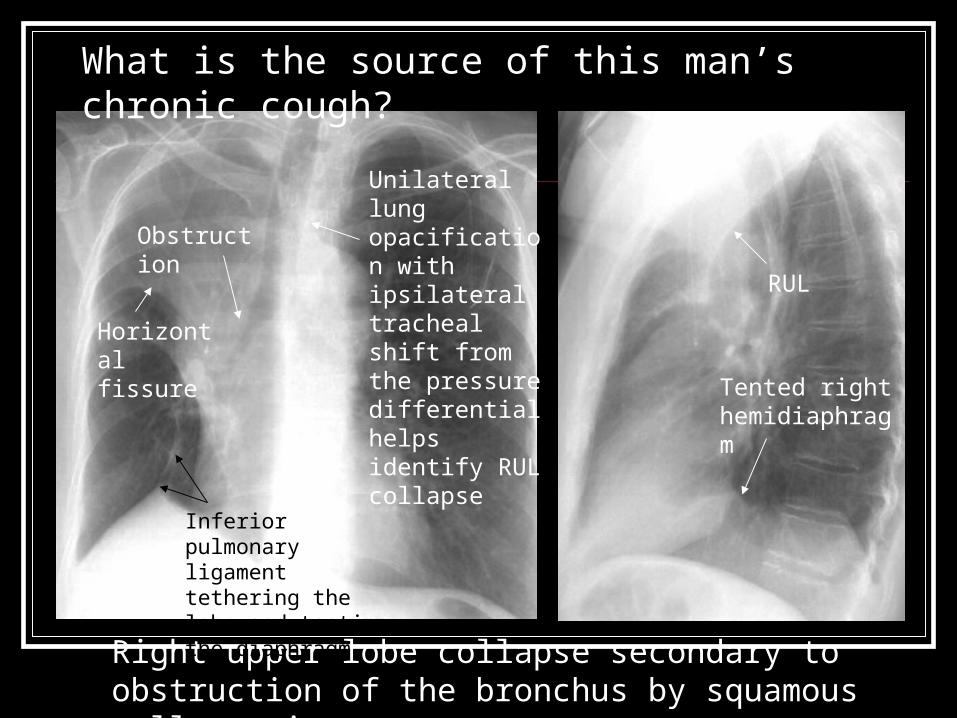
What is the source of this man’s chronic cough?
Right upper lobe collapse secondary to obstruction of the bronchus by squamous cell carcinoma.
Unilateral lung opacification with ipsilateral tracheal shift from the pressure differential helps identify RUL collapse
Obstruction
Horizontal fissure
Inferior pulmonary ligament tethering the lobe and tenting the diaphragm
Tented right hemidiaphragm
RUL
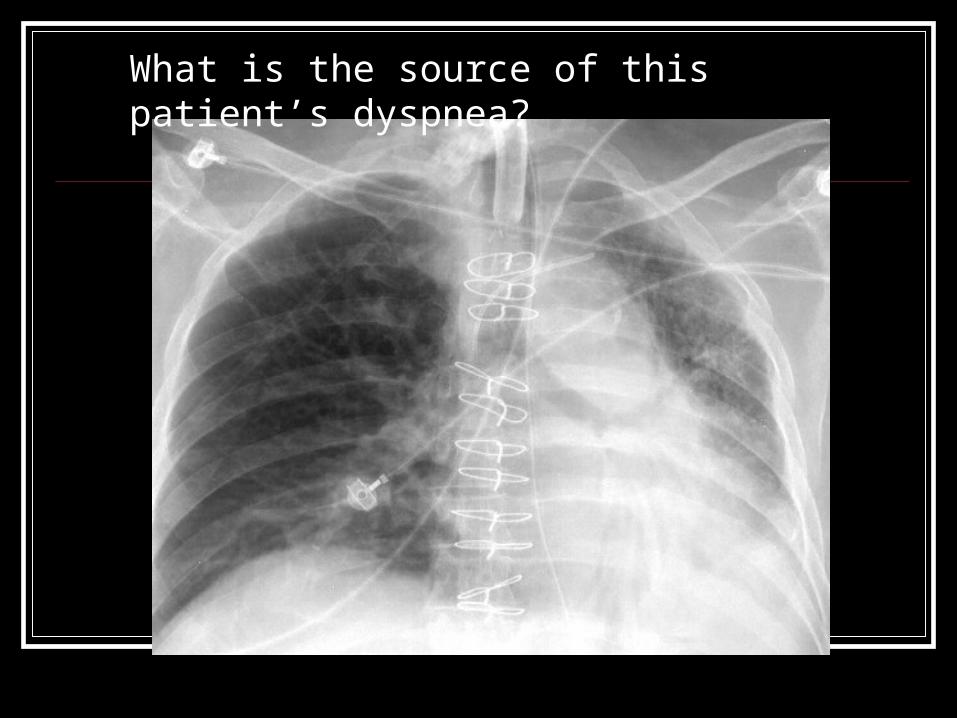
What is the source of this patient’s dyspnea?
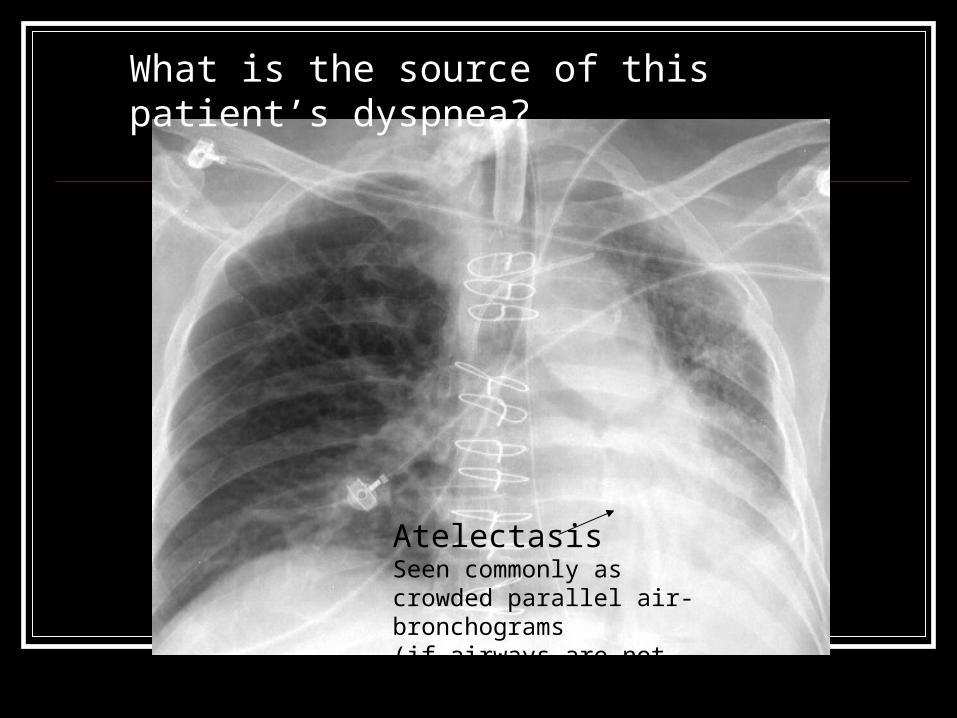
What is the source of this patient’s dyspnea?
Atelectasis Seen commonly as crowded parallel air-bronchograms (if airways are not obstructed)

What is abnormal here?

What is abnormal here? The patient has Sarcoidosis.
Think about lymphadenopathy when opacities obscure the aortic pulmonary recess (PA) or surrounding the left distal main bronchus (on the lateral)
Bronchus lumen is obscured
Lateral border of the SVC is obscured by lymphadenopathy

Other Mediastinal Structures Esophagus Thyroid Thymus Lymph nodes
These are generally not seen unless there is pathology
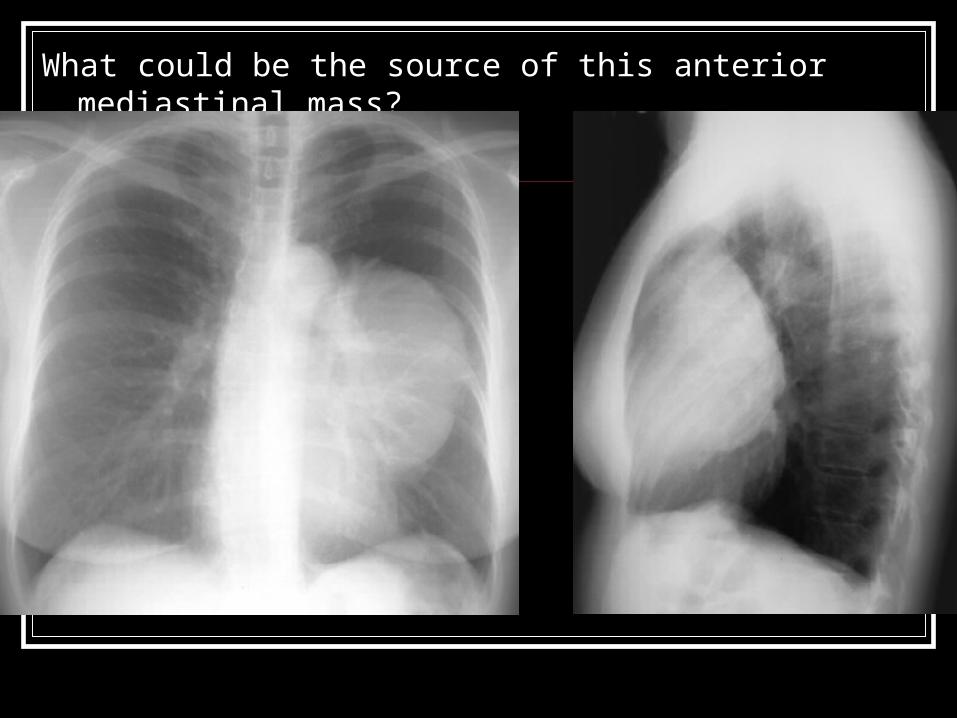
What could be the source of this anterior mediastinal mass?

What could be the source of this anterior mediastinal mass?
Ddx: Lymphoma/leukemia, germ cell tumors (e.g., teratoma), thymic mass (e.g., thymoma, cyst), enlarged thyroid, vascular (e.g., hematoma, aortic aneurysm).
This patient has a thymoma.
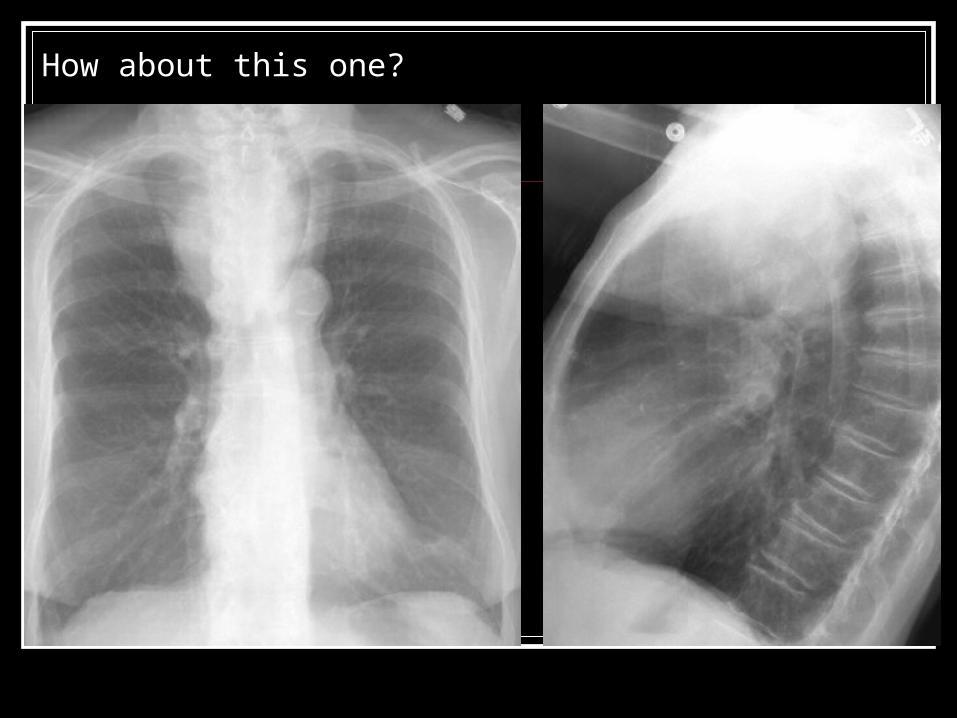
How about this one?

How about this one?
This patient has a an enlarged thyroid gland.

Extrapulmonary Structures Diaphragm Stomach/gastric bubble Liver, spleen Bones: clavicles, ribs, scapulae, spine Other soft tissues
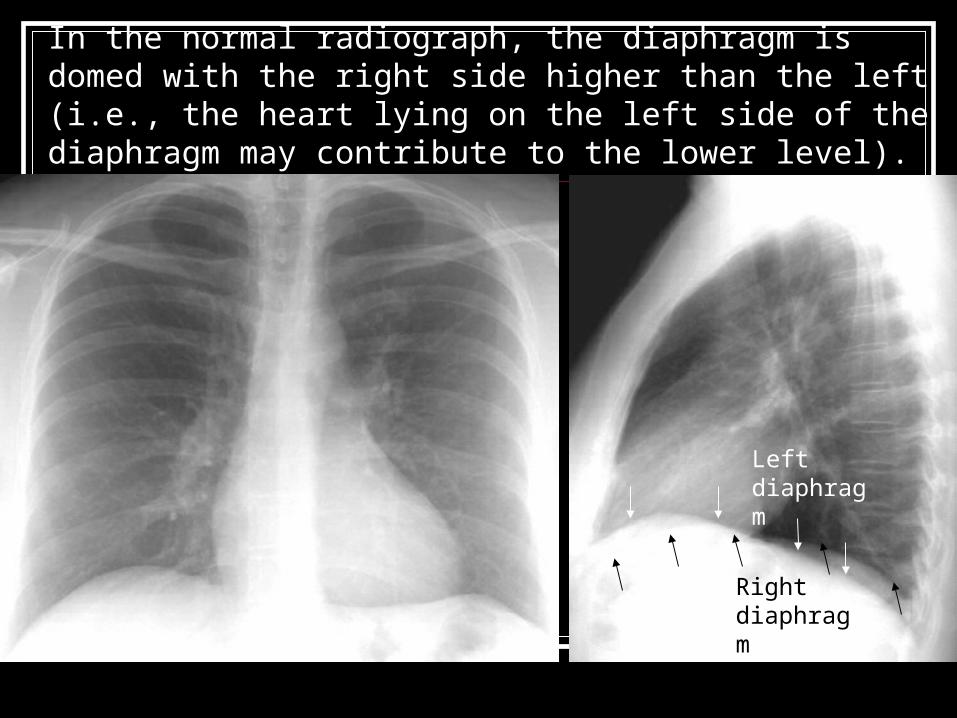
In the normal radiograph, the diaphragm is domed with the right side higher than the left (i.e., the heart lying on the left side of the diaphragm may contribute to the lower level).
Right diaphragm
Left diaphragm

Elevated intrathoracic pressures (e.g., hyperinflation from obstructive lung disease, tension pneumothorax) will flatten the diaphragm.
Flat
Flattened
Not many structures left, so let’s just quiz…
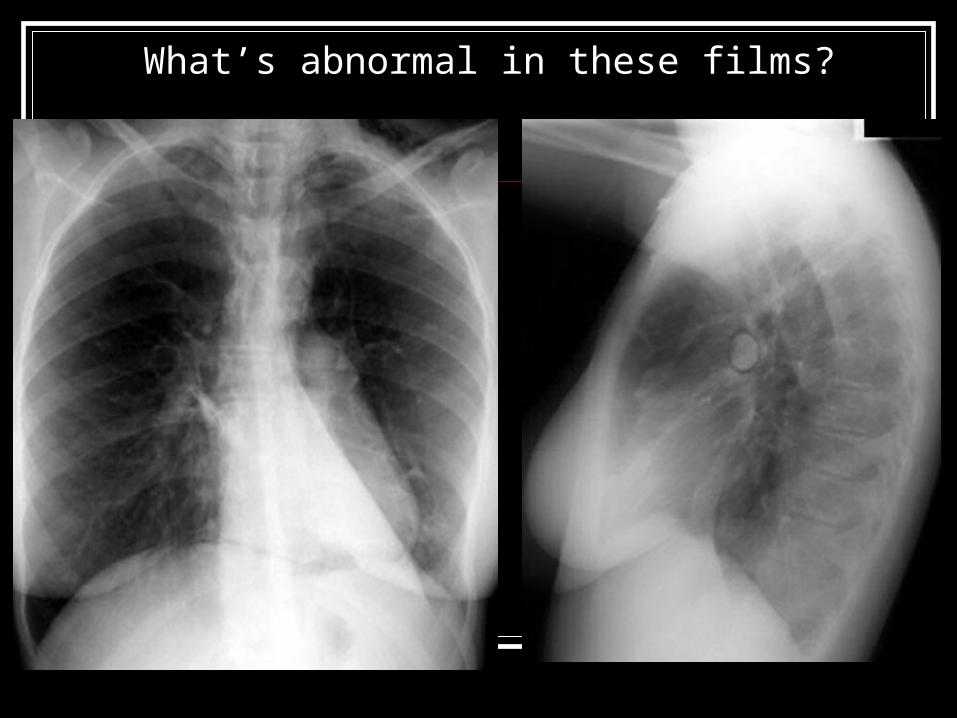
What’s abnormal in these films?

What’s abnormal in these films?
The lucent stripe along the inferior heart border, crossing midline is called a “continuous diaphragm” sign and is indicative of pneumomediastinum.
Notice the air around the left and right pulmonary arteries.
LLL atelectasis
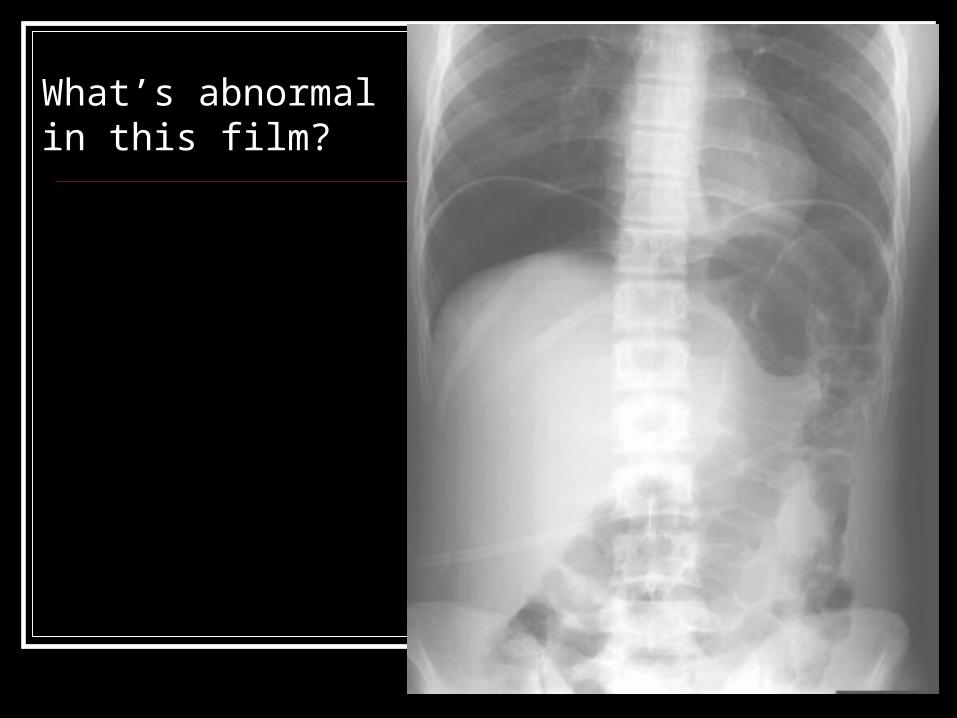
What’s abnormal in this film?

What’s abnormal in this film?
Normally the only air we see under the diaphragm is in the gastric bubble and bowels. Subdiaphragmatic free air is indicative of perforated viscus.
Free air

What’s abnormal in this film?

What’s abnormal in this film?
Hiatal hernia
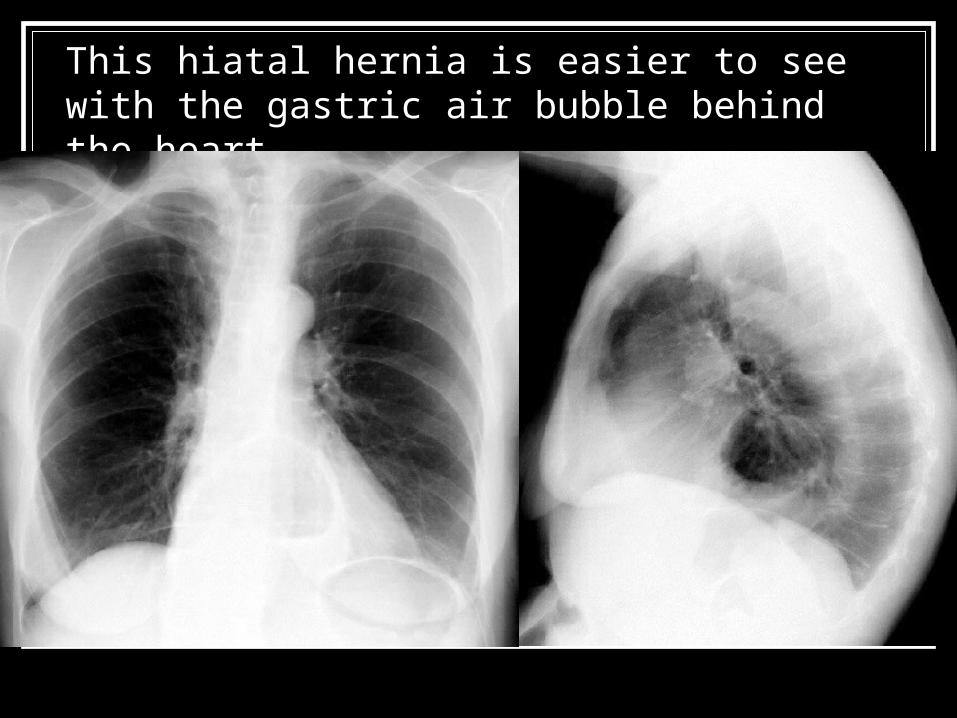
This hiatal hernia is easier to see with the gastric air bubble behind the heart.

What’s abnormal in this film?

What’s abnormal in this film?
Gastric bubble, bad sign
Ruptured diaphragm
Tracheal deviation
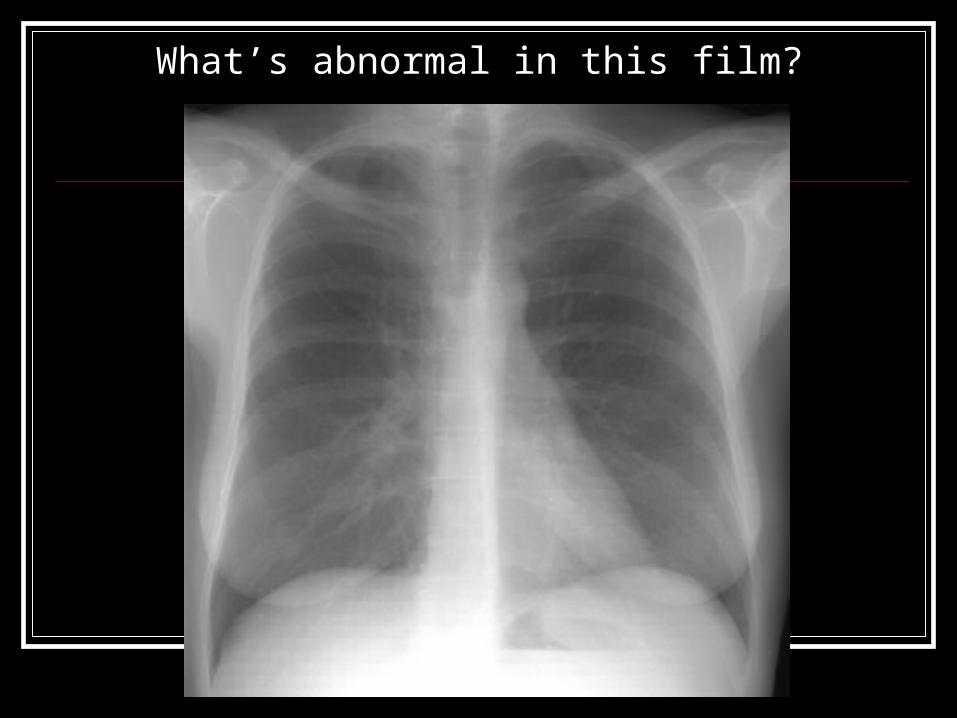
What’s abnormal in this film?
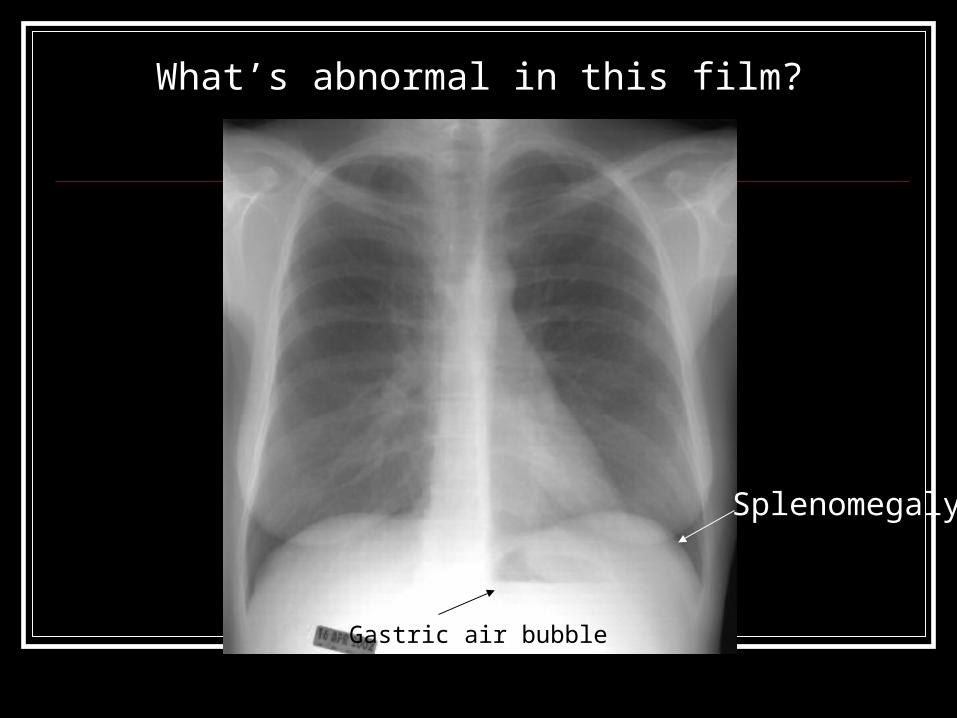
What’s abnormal in this film?
Splenomegaly
Gastric air bubble

What’s abnormal in this film?
Gastric air bubble

What’s abnormal in this film?
Gastric air bubble
Ouch

Which patient needs a chest tube?
Gastric air bubble

Which patient needs a chest tube?
Gastric air bubble
Skin fold lateral border
Pneumothorax
Scapula medial border
To decide whether a line in the lung represents the scapula, a skin fold or a pneumothorax consider the density difference between the two sides of the line. A pneumothorax will have a sharp line with air density (equal density) on both sides. Skin or scapula will have a line with air on one side and more opaque tissue on the other.

What’s abnormal in this film?

What’s abnormal in this film?
The patient is rotated slightly causing the “heel effect”, the relative over exposure of one hemithorax compared to the other caused by uneven radiation. Looking at the relative exposure of the extrathoracic soft tissues can help identify the “heel effect”.
Nothing
The left lung appears more opacified but it is the result of uneven radiation.
References: Collins J, Stern EJ. Chest Radiology, the
Essentials. Lippincott, Williams & Wilkins. 1999. Dafner RH. Clinical Radiology, the Essentials. 2nd
Ed. Lippincott, Williams & Wilkins. 1999. Freindlich IM, Bragg DG. A Radiologic Approach
to Diseases of the Chest. 2nd Ed. Williams & Wilkins. 1997.