this presentation is the intellectual property of the...
TRANSCRIPT

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Deena E. Sutter, MD, FAAP
LtCol, USAF
Pediatric Infectious Disease Service
Brooke Army Medical Center
Deena E. Sutter, MD, FAAP has no
relevant financial relationships with
commercial interests to disclose.
Why Prenatal Screening for an
Infectious Disease?
Effective intervention for prevention
Effective intervention (pre- or post-natal) for treatment
If the incidence of disease is common enough that it is cost-effective
If transmission is common enough to warrant screening If significant sequelae are rare, though, it’s a problem
If there is high risk of severe effects if transmitted Preparing the parent
Elective termination
Ensure vaccination of mother post-partum

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Who makes the guidelines?
ACOG
ACIP/CDC
IDSA
USPSTF
USPHS
DoD/VA
AAP
AAFP
Surprise, surprise, they often have
different recommendations!
How about TORCH titers?
Cytomegalovirus Ab, IgM
Herpes simplex Ab, IgM
Rubella Ab, IgM
Toxoplasma Ab, IgM
False-positive rate for titers obtained
without specific clinical indication is high
Accurate diagnoses are rare with these
– JUST DON’T ORDER THEM!
Congenital/Perinatal Infections
Routine Testing Directed Testing
HIV*
Syphilis*
Hepatitis B*
Group B Strep
UA/Urine culture
CMV
Toxoplasma
Herpes Simplex
Parvovirus B19
Hepatitis C
HTLV
T cruzi (Chagas)
M tuberculosis
Test immediately and again in 3rd trimester if high-risk
High risk /non-immune
(variable)
•GC/Chlamydia*
•VZV
•Rubella

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Congenital/Perinatal Infections
Routine Testing Directed Testing
HIV*
Syphilis*
Hepatitis B*
Group B Strep
UA/Urine culture
CMV
Toxoplasma
Herpes Simplex
Parvovirus B19
Hepatitis C
HTLV
T cruzi (Chagas)
M tuberculosis
Test immediately and again in 3rd trimester if high-risk
High risk /non-immune
(variable)
•GC/Chlamydia*
•VZV
•Rubella
Serologic Assays
Antibody response as simple measure of immunity Not always best measure
○ Windows of IgG vs IgM presence highly variable
○ IgM may be cross-reactive (nonspecific)
LOTS of different types of serologic tests!
○ Sensitivity and specificity vary based on test
○ PPV and NPV related to overall prevalence of infection
Nonspecific screening assays may need specific/sensitive assays to follow (HIV, syphilis)
Some extremely complicated (toxoplasma)
Tests for Pathogens or Antigens
Viral or bacterial cultures – only a few of
the pathogens (GBS, HSV, CMV)
Nucleic acid testing (PCR, other) –
amniotic fluid, placenta, or fetal body
fluids/tissue
Occasionally ID from maternal or infant
blood
Antigen tests – HBSAg (blood), HSV or
VZV DFA (vesicles)

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Congenital/Perinatal Infections
Vaccine-Preventable
Routine Testing Directed Testing
HIV*
Syphilis*
Hepatitis B*
Group B Strep
UA/Urine culture
CMV
Toxoplasma
Herpes Simplex
Parvovirus B19
Hepatitis C
HTLV
T cruzi (Chagas)
M tuberculosis
Test immediately and again in 3rd trimester if high-risk
High risk /non-immune
(variable)
•GC/Chlamydia*
•VZV
•Rubella
Rubella “screening only”
No intervention
Rubella IgG – is mom immune?
>90% seroresponse to vaccine
○ Live-virus vaccine contraindicated in pregnancy
○ Goal to immunize women of childbearing age who
are not pregnant
Documentation of 1 or more doses is sufficient
evidence of immunity in pregnancy (CDC)
DoD guidelines recommend universal serology
○ Recommendation to avoid exposure (limited
evidence)
○ Immunization of susceptible women post-partum
Congenital Rubella Syndrome
99% decline after implementation of
vaccine in 1969
Few cases per year, essentially all
imported
Wkly Epidemiol Rec. 2010 Oct 15;85(42):413-8.
Controlling rubella and preventing congenital rubella
syndrome – global progress, 2009.

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Cohen & Powderly: Infectious Diseases, 3rd ed.
Congenital Varicella
Rare development of congenital varicella
even when pregnant women infected
Rates of natural disease decreased with
vaccine (90-95% response) – congenital
infection even more rare
Of more concern – severe varicella in infants
exposed perinatally or preterm infants
without maternal immunity
VZV – screening, with potential
intervention in case of exposure Obtain test if proof of immunity does not exist IgG negative - vaccinate after delivery
Birth before 1980 NOT an accepted proof of immunity
Most women of childbearing age - screening if immunization records not available
Varizig – (IND hyperimmune globulin) If suspected infection = immunoglobulin for mom
For neonates with maternal symptoms 5 days prior to or 2 days post-delivery
Neonates with presumed lack of maternal antibody and post-natal exposure

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Hepatitis B Immunization of high-risk groups 1980’s-1990’s
1999 - Universal immunization of all infants
recommended
Hepatitis B
Rates of congenital infection have fallen dramatically since vaccination (first high-risk, then universal) was implemented
From 1990 to 2004, reported incidence of hepatitis B in children declined 96% (from 3.0/100,000 to 0.16/100,000)
All women are screened with Hepatitis B surface antigen (HBSAg) Not surface antibody – this is an indicator of
prior immunization, or recovery from natural infection
Hepatitis B serologies
Interpretation HBSAb HBSAg Anti-HBc HBeAg
Susceptible –
unimmunized
or
nonresponder
- - - -
Immunized,
Immune+ - - -
Prior infection,
Immune, not
infectious
+ - + -
Chronic carrier,
infectious- + + -
Chronic carrier,
highly
infectious
- + + +

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
CDC, 2006
Hepatitis B
If HBSAg is positive
Additional serologic evaluation, liver function
tests, DNA PCR
○ Determination whether she is a chronic carrier
(low viral load, HBSAg+/HBcAb+) or at
highest risk for transmission (high viral load
with HBeAg)
Infants born to HBSAg mothers should all
receive HB vaccine AND HBIG within 12
hours of birth
Hepatitis B
90% of perinatal infections
can be prevented with
appropriate screening and
prophylaxis
Up to 90% of infants
born to HBSAg and
HBeAg+ mothers will
be infected
90% of infants
infected
congenitally will
be chronically
infected
Acute infection will
resolve in 90% of
adults who are
infected

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
(Often confusing test results)
Congenital/Perinatal Infections
Routine Testing Directed Testing
HIV*
Syphilis*
Hepatitis B*
Group B Strep
UA/Urine culture
CMV
Toxoplasma
Herpes Simplex
Parvovirus B19
Hepatitis C
HTLV
T cruzi (Chagas)
M tuberculosis
Test immediately and again in 3rd trimester if high-risk
High risk /non-immune
(variable)
•GC/Chlamydia*
•VZV
•Rubella
Congenital CMV BY FAR the most common congenital
infection in the US
Estimated 40,000 cases per year (out of approximately 4 million births per year = 1% of all live births)○ Primary infection in non-immune women
○ Young women with toddlers, daycare workers
90-95% asymptomatic○ Development of SN hearing loss
possible in asymptomatic
○ Routine screening NOT indicated Efficacy of gancyclovir in asymptomatic or
mildly symptomatic still unclear
Toxicity – neutropenia, central line placement

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Congenital CMV – Labs
Prenatal
Mom with febrile illness +/- rash
And/or infant with abnormalities on
ultrasound
○ Maternal CMV IgM
○ High-avidity IgG assays
○ Amniotic fluid culture (60% sensitive) or PCR
(near 100%)
○ Fetal blood (cordocentesis) – less sensitive
Congenital CMV – Labs
Postnatal
Viral culture – gold standard
○ Urine, saliva, tissue
○ May take 2 or more weeks, but high sensitivity (90%+)
○ Modifications such as shell vial or microtiter plate with IF Abs for quicker results
PCR
○ Highly sensitive Blood, urine, CSF, saliva, tissue
Quantitative PCR from blood
- Varying data on prognostic value of viral load
Congenital CMV – Labs
Serologic assays for newborn
IgM – relatively insensitive (60-80%)
IgG - persistence past 3-4 months may be
helpful in late dx
After 2 weeks of life, any positive test
(PCR, culture, IgM) could be post-natal
infection
Viral shedding for months is common

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Congenital Toxoplasmosis
Toxoplasma
gondii
Parasite –
protozoan
Zoonosis – cats
(oocysts),
undercooked meat
(tissue cysts)
Incidence of 1-
10/10,000 in US
Kliegman: Nelson Textbook of Pediatrics, 18th ed.
Classic triad:
-Hydrocephalus
-Intracranial calcifications
-Chorioretinitis
Like CMV, many asymptomatic 80% of women infected in
last few weeks of pregnancy transmit
○ Almost all subclinical
○ Risk for late ophtho findings
Diagnostic Methods
Traditionally, based on clinical suspicion and suggesting laboratory findings
Elevated CSF protein, mononuclear pleocytosis
Histologic evidence (often from autopsy or placenta)
Culture methods – mouse innoculation or tissue culture
PCR assays
Have replaced most culture diagnostics
○ Highly sensitive
CSF, placenta, amniotic fluid, other tissues
Neonatal parasitemia varies (15-75%) depending on disease presentation

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Serologic assays
Primary method of diagnosis
Numerous methods employed
Sabin-Feldman dye test, Complement fixation,
IHA, Agglutination, IFA, various ELISA assays
Most labs employ conventional ELISA
○ SHOULD NOT BE USED TO DIAGNOSE
MATERNAL OR FETAL INFECTION - High rates
of false-positive IgM
IgM double sandwich ELISA
Immunosorbent Agglutination Assay
(ISAGA)
IgM, IgA, IgE
Testing in the United States
Palo Alto –
Toxoplasma serology laboratory
www.pamf.org
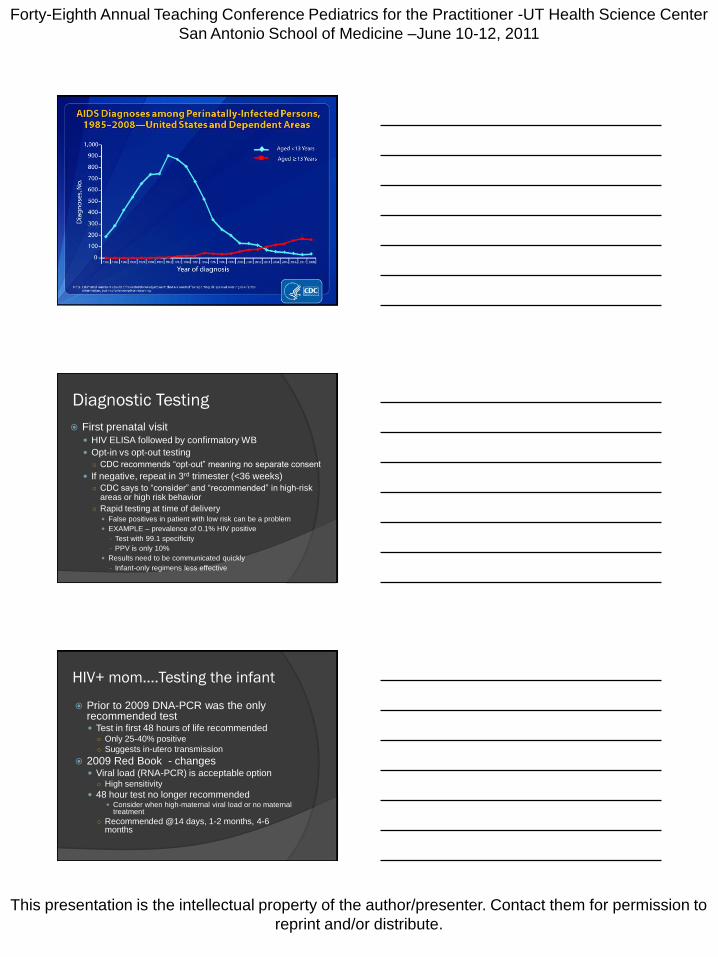
HIV
1994 - PACTG-076
Transmission reduced from 25.5% to 8.3%
with ZDV-only regimen in mother and infant
Since then - dramatic progress in ART –
most women already on 3-drug HAART
Undetectable viral load and no other risk
factors – risk likely 1-2% or less
Today – estimated 100-300 infants
infected annually
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Diagnostic Testing
First prenatal visit
HIV ELISA followed by confirmatory WB
Opt-in vs opt-out testing
○ CDC recommends “opt-out” meaning no separate consent
If negative, repeat in 3rd trimester (<36 weeks)
○ CDC says to “consider” and “recommended” in high-risk areas or high risk behavior
○ Rapid testing at time of delivery False positives in patient with low risk can be a problem
EXAMPLE – prevalence of 0.1% HIV positive
- Test with 99.1 specificity
- PPV is only 10%
Results need to be communicated quickly
- Infant-only regimens less effective
HIV+ mom….Testing the infant
Prior to 2009 DNA-PCR was the only recommended test Test in first 48 hours of life recommended
○ Only 25-40% positive
○ Suggests in-utero transmission
2009 Red Book - changes Viral load (RNA-PCR) is acceptable option
○ High sensitivity
48 hour test no longer recommended Consider when high-maternal viral load or no maternal
treatment
○ Recommended @14 days, 1-2 months, 4-6 months

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
HIV-1 Exclusion in Infants
Presumptive exclusion*
2 negative virologic tests
(2+ weeks and 4+
weeks)
1 negative virologic test
after 4 weeks
HIV Ab after 6 months
Definitive exclusion
2 negative tests (1+
months and 4+ months)
2 negative HIV Ab tests
after 6 months
No clinical or other lab
evidence of
immunodeficiency or HIV
*If presumptive exclusion, PCP prophylaxis no
longer indicated at 4-6 weeks
Infant with Unknown Maternal
Status
Foreign adoptees
Infants of mothers without documented
prenatal testing, or possible seroconversion
after testing in 1st trimester
HIV-1 Ab with reflex Western Blot – if > 6m
Positive WB after 18 months diagnostic
Syphilis
“We’re calling from Ft Hood. We have a
mom and a baby with positive RPRs,
and we don’t know what workup to do.”

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Congenital Syphilis Rates from 1-100/100,000 live births
Dramatic decrease since late 1980’s
;
www.marchofdimes.com
Congenital Syphilis
Culture (rabbit infectivity test), darkfield
microscopy, PCR not widely available
Nearly all diagnostic labs are serological
Combination of non-treponemal (screening)
and treponemal testing
Comparison of maternal and infant titers

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Remember
RPR/VDRL are non-treponemal antibodies
Antibodies to cardiolipin
Titers reflective of disease activity
○ False positives with connective tissue disease,
other infections
○ + RPR in mom with + treponemal Ab = syphilis
Treponemal tests
FTA-ABS, TP-PA, Syphilis IgG (ELISA)
Usually positive for life
Adequate Maternal Therapy Penicillin G (IM Benzathine, 2.4m U x 1 or x 3)
>30 days prior to delivery
4-fold decrease in RPR titer
Must be documented!
If above are not met, full workup of infant (CSF studies, CBC, long bone films) required If workup negative – 50K U/kg Benzathine PenG IM x 1
If infant has with RPR 4x > maternal RPR and/or clinical signs of syphilis Evaluate with LP, CBC, other tests “as indicated”
Treat – PenG 100-150K U/kg/day x 10 days or procaine 50K U/kg/day x 10days
If infant RPR less than 4x maternal, treatment adequate 50K U/kg Benzathine PCN x 1
May defer therapy if able to follow infant closely with RPRs
Follow the Flowchart!
Red Book®: 2009 Report
of the Committee on
Infectious Diseases - 28th
Ed.
Long: Principles
and Practice of
Pediatric Infectious
Diseases, 3rd ed.;

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Perinatal HSV
1/3,000 to 1/20,000 live births
Not usually “congenital” – disease
occurs around time of delivery
Ascending infection or during vaginal
delivery
Approximately 30-50% of women with
primary transmission vs 1-2% of women
with recurrence (seropositive)
75% of perinatal HSV – no maternal history
Perinatal HSV
Routine screening NOT indicated
60% of women of childbearing age have HSV-1 and 23% have HSV-2 antibodies
Serology rarely helpful unless indicates acute maternal infection at time of delivery
○ Need clinical suspicion (genital lesions, febrile illness, new sexual partner)
○ Most seroconversions are asymptomatic
Viral shedding in patients even when symptomatic – PCR/culture not indicated but may be useful if genital lesions present

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Workup of Infant with HSV+ Mother
Surface cultures (12-24 hours of life) Skin (lesions), conjunctivae, rectum, urine,
oropharynx
HSV culture – gold standard○ Cell culture - 48-72h, stained with fluorescent Abs
PCR of CSF or blood (do not send surface swabs for PCR)○ CSF 75-90% sensitive, may need to repeat if
negative but evidence of CNS disease
○ Serum PCR – 40-70% sensitive – more likely in disseminated HSV
Serologies usually not helpful
Vesicles – DFA less sensitive than culture○ Tzank smear – insensitive
In utero (3%)
Disseminated infection
20-30%
Delivery 1 week
CNS disease
30%
2 weeks
SEM disease
30-40%
4 weeks3 weeks
Timeline of Perinatal HSV Infection
Manifestations
•Most patients will have workup days to weeks post-delivery
•Surface cultures not indicated, CSF studies ALWAYS
indicated, plus virologic/antigen testing of lesions, LFTs, CBC
Summary
Testing for perinatal or congenital
infections can be tricky
Need to know the incidence of disease
The epidemiology of transmission
Which labs are indicated, and which are not
If labs results are available which were not
indicated – know the significance!
AAP Red Book is always a good starting
place

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.