third international pharmaceutical regulatory and ... · pdf filethird international...
TRANSCRIPT

Third International Pharmaceutical Regulatory
and Compliance Congress and Best Practices Forum
May 28 2009 Rome
Pre-conference I - International Compliance Program Basics
Dominique Laymand Sue EganSenior Director Compliance & Ethics EMEA Vice-President Compliance, ISMO
Bristol-Myers Squibb AstraZeneca

2
International Compliance Program Basics
• How can we maintain a robust Compliance Programme in the current difficult economic environment?
• How can we maintain a robust Compliance Programme in the changing internal environment of the pharmaceutical industry?
Let’s begin by taking a look at the external environment…
3
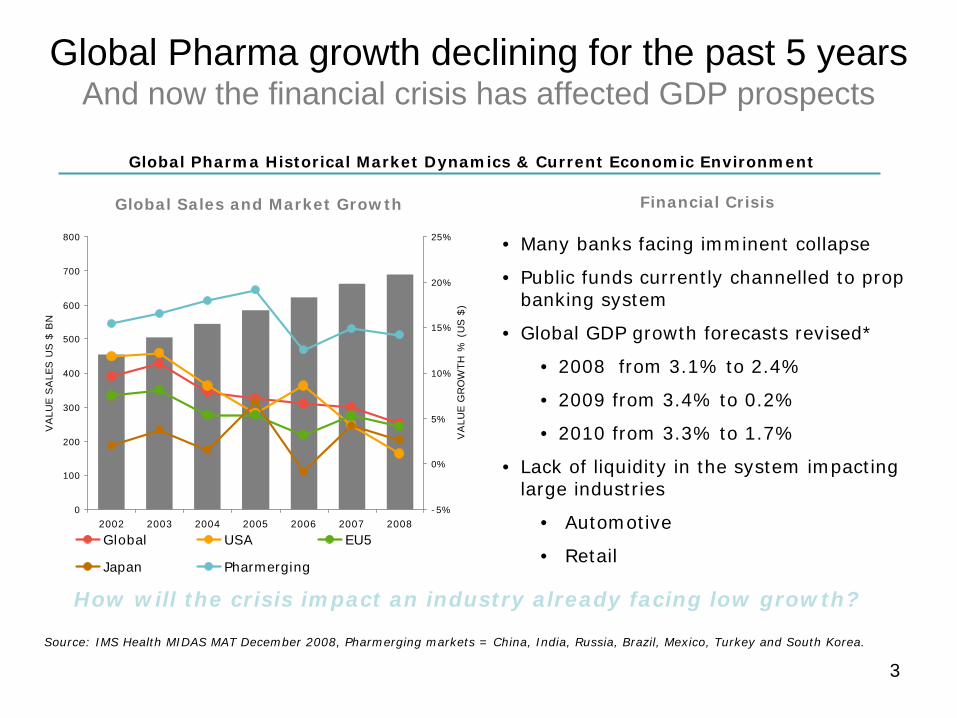
Global Pharma growth declining for the past 5 years And now the financial crisis has affected GDP prospects
0
100
200
300
400
500
600
700
800
2002 2003 2004 2005 2006 2007 2008
VA
LUE
SA
LES
US
$ B
N
-5%
0%
5%
10%
15%
20%
25%
VA
LUE
GR
OW
TH %
(U
S $
)
Global USA EU5
Japan Pharmerging
Source: IMS Health MIDAS MAT December 2008, Pharmerging markets = China, India, Russia, Brazil, Mexico, Turkey and South Korea.
Global Sales and Market Growth Financial Crisis
Global Pharma Historical Market Dynamics & Current Economic Environment
• Many banks facing imminent collapse
• Public funds currently channelled to prop banking system
• Global GDP growth forecasts revised*
• 2008 from 3.1% to 2.4%
• 2009 from 3.4% to 0.2%
• 2010 from 3.3% to 1.7%
• Lack of liquidity in the system impacting large industries
• Automotive
• Retail
How will the crisis impact an industry already facing low growth?
4
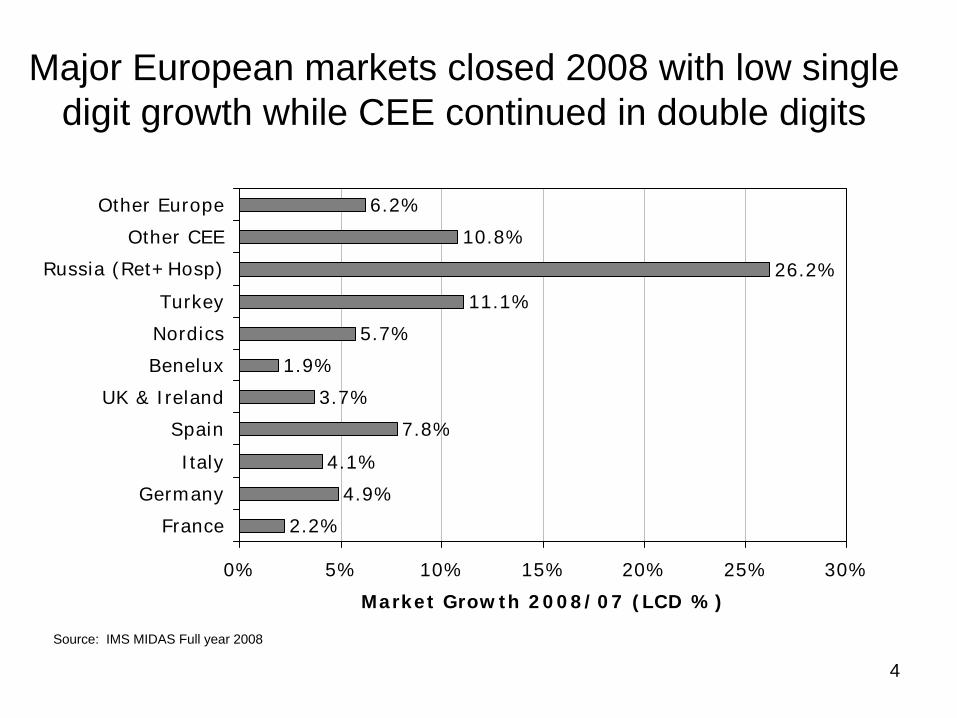
Major European markets closed 2008 with low single digit growth while CEE continued in double digits
2.2%
4.9%
4.1%
7.8%
3.7%
1.9%
5.7%
11.1%
26.2%
10.8%
6.2%
0% 5% 10% 15% 20% 25% 30%
France
Germany
Italy
Spain
UK & Ireland
Benelux
Nordics
Turkey
Russia (Ret+Hosp)
Other CEE
Other Europe
Market Growth 2008/07 (LCD %)
Source: IMS MIDAS Full year 2008
5
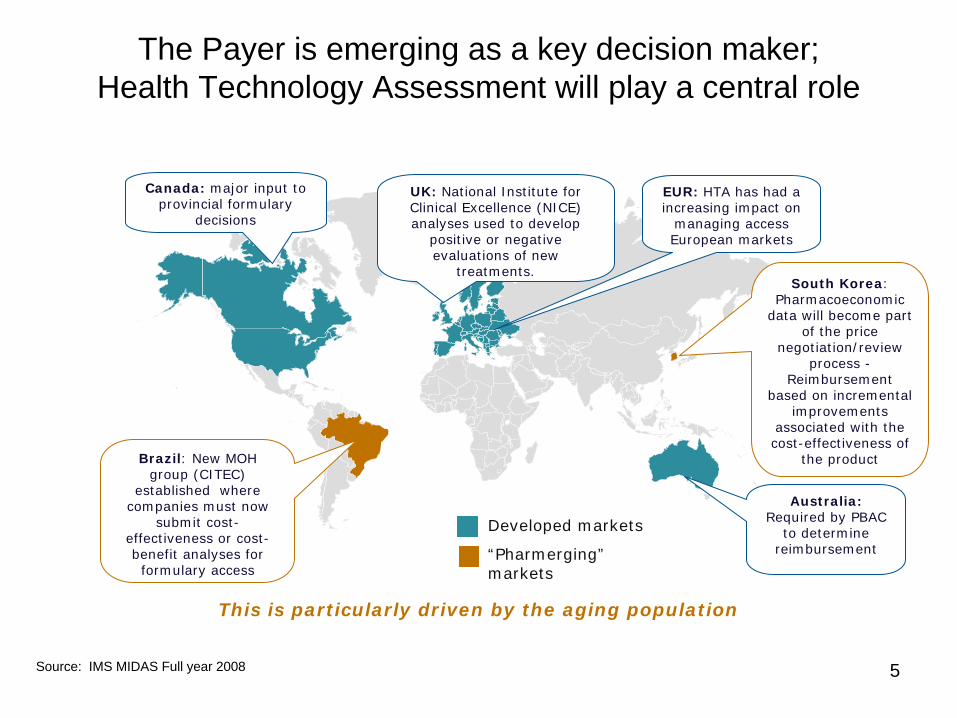
The Payer is emerging as a key decision maker; Health Technology Assessment will play a central role
This is particularly driven by the aging population
Canada: major input to provincial formulary
decisions
UK: National Institute for Clinical Excellence (NICE) analyses used to develop
positive or negative evaluations of new
treatments.
EUR: HTA has had a increasing impact on
managing access European markets
Australia: Required by PBAC
to determine reimbursement
Brazil: New MOH group (CITEC)
established where companies must now
submit cost- effectiveness or cost- benefit analyses for formulary access
South Korea: Pharmacoeconomic
data will become part of the price
negotiation/review process -
Reimbursement based on incremental
improvements associated with the cost-effectiveness of
the product
Developed markets
“Pharmerging” markets
Source: IMS MIDAS Full year 2008

6
Payers are increasingly fragmented within key markets, as decision making becomes increasingly ‘localised’
UK: PCTs power & influence varies resulting in divergent prescribing behaviour & implementation of national guidelines
France: Recent health reforms decentralisation process will create Agences Regionales de Sante (ARS) and consolidate control over both primary & hospital care. Potential impact is more control over GP prescribing & increased efficiency
Italy: Regional governments taken on increasing healthcare financing responsibility. North-South affluence divide reflected in Lombardy seeking increased responsibilities, whilst Lazio & Sicily struggle with huge deficits and central government disciplinary pacts.
Spain: Decentralised healthcare in 2002 to 17 autonomous regions. Over half of spending in 4 key regions Andalusia (16.4%), Catalonia (15.5%), Valencia (2.9%) and Madrid (10.6%). The 17 regions all pursue variable policies but reference pricing is now nationwide.
Source: IMS Health Consulting
France
Spain
UK
Italy
German y
Germany: Contracting with the different sick funds has increased regional variability. Regional sick funds are partnering with corps to issue treatment guidance with preferred therapy, becoming key decision makers.
Local managed care (style) influence develops in Europe
7
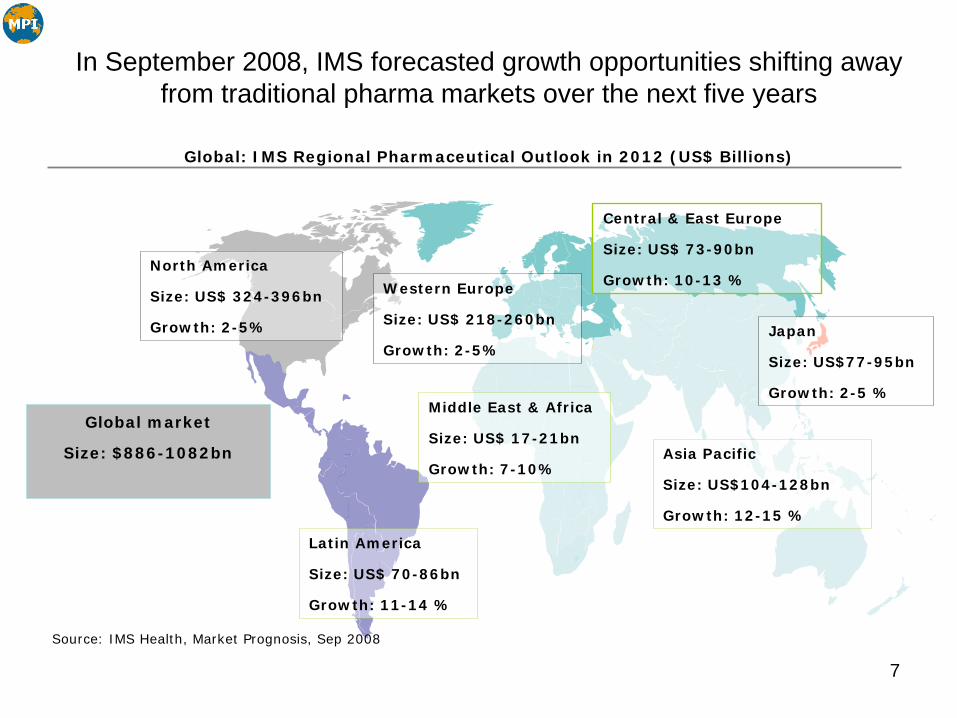
In September 2008, IMS forecasted growth opportunities shifting away from traditional pharma markets over the next five years
Japan
Size: US$77-95bn
Growth: 2-5 %
North America
Size: US$ 324-396bn
Growth: 2-5%
Global market
Size: $886-1082bn
Source: IMS Health, Market Prognosis, Sep 2008
Western Europe
Size: US$ 218-260bn
Growth: 2-5%
Latin America
Size: US$ 70-86bn
Growth: 11-14 %
Central & East Europe
Size: US$ 73-90bn
Growth: 10-13 %
Middle East & Africa
Size: US$ 17-21bn
Growth: 7-10%Asia Pacific
Size: US$104-128bn
Growth: 12-15 %
Global: IMS Regional Pharmaceutical Outlook in 2012 (US$ Billions)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Indi
a
Mex
ico*
Bra
zil
US
Chi
na
Rus
sia
Can
ada
S.
Kor
ea
Ital
y*
Fran
ce
Japa
n
Spa
in
Ger
man
y
UK**
Turk
ey*
% S
HARE
OF
PHARM
A S
PEN
DIN
G
% out of pocket % other private % public
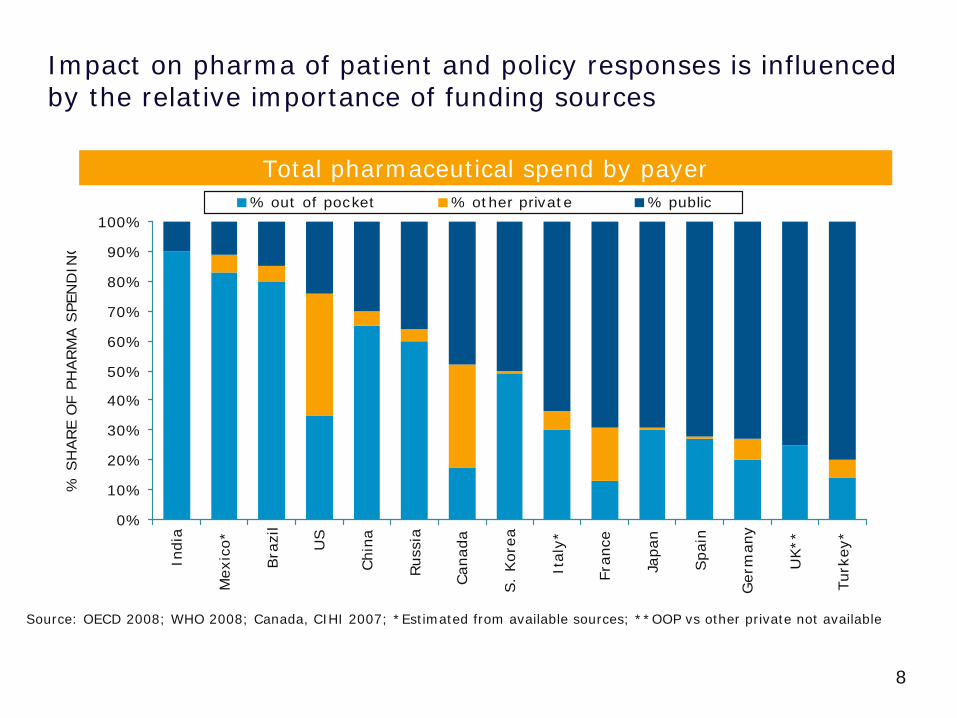
Impact on pharma of patient and policy responses is influenced by the relative importance of funding sources
Source: OECD 2008; WHO 2008; Canada, CIHI 2007; *Estimated from available sources; **OOP vs other private not available
Total pharmaceutical spend by payer
8
9
Pharmaceutical Companies – Internal environment
• Evolution of organisations in response to the external environment by reducing costs, streamlining internal structures, etc…
• Key components for maintaining a robust Compliance Programme as a business enabler through the approaches of 2 companies:
– BMS approach Slides 10 and 11– AstraZeneca approach Slides 12 and 13

10
Office of Compliance & Ethics
MISSION STATEMENTTo establish an effective Compliance & Ethics program that ensures a culture of integrity enabling BMS to conduct its global business with the highest ethical standards, in full compliance with all applicable laws and regulations and our own Pledge and the Standards of Business Conducts & Ethics.
BMS Approach
10

11
EMEA Business Compliance & Ethics Governance Model Overview
Business strategy and Risk-based ApproachFocused on Accountability
Collaborative working process with Finance Control and Legal Functions
EMEA BusinessControl Program
EMEA BusinessCompliance & Ethics
Program
EMEA Compliance & Ethics Governance Model
Contribution to Productivity Transformationand Continuous Improvement by:
4A standardized approach on core activities4A focus on innovative and new projects
4Continuous assessment of processes in terms of controls and compliance efficiency with the objective of working in a safe environment while removing bureaucracy
BMS Approach
Compliance Programme Basics
Having clear, written rulesAppointing an LCO and Local Compliance CommitteeCarrying out effective training so people know what the rules arePeople carrying out their duties with the rules in mindMonitoring activities detect non-compliance with the rulesPeople having the confidence and appropriate mechanisms to report problems positivelyReasons for non-compliance are analysed and appropriate actions taken, for example
– Rules are clarified / updated– Re-training– Bonus impact– Warning (verbal / written)– Dismissal(Based on OIG (Office of Inspector General) – 7 Elements of Compliance)
13
AZ Approach
13
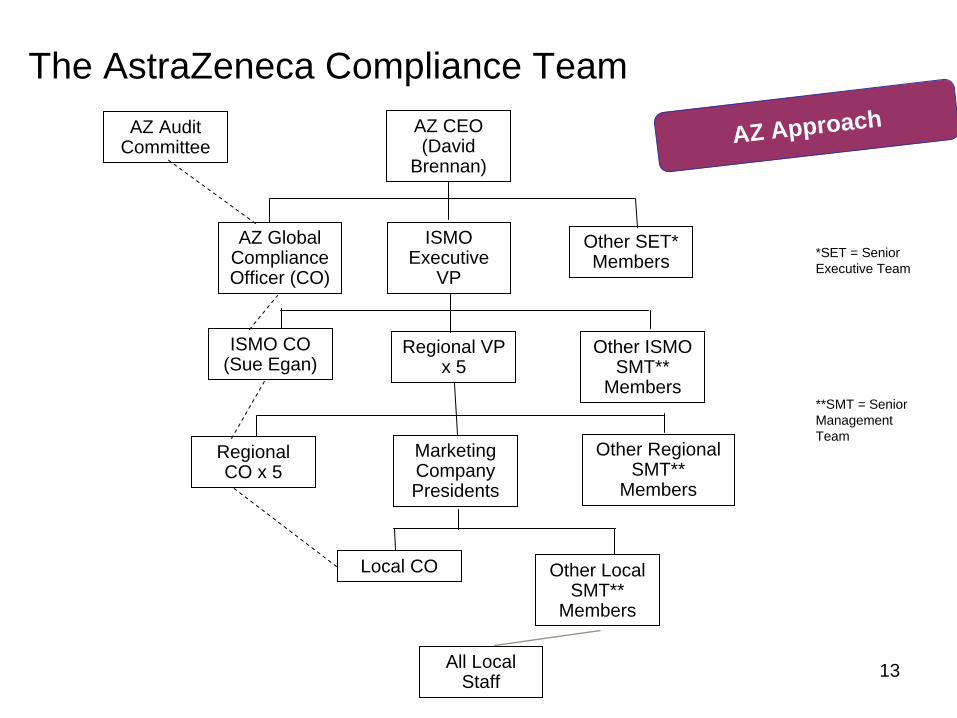
The AstraZeneca Compliance TeamAZ CEO (David
Brennan)
ISMO Executive
VP
AZ Global Compliance Officer (CO)
Other SET* Members
Regional VP x 5
Other ISMO SMT**
Members
ISMO CO (Sue Egan)
Regional CO x 5
Other Regional SMT**
Members
Marketing Company Presidents
Other Local SMT**
Members
Local CO
All Local Staff
AZ Approach
*SET = Senior Executive Team
**SMT = Senior Management Team
AZ Audit Committee
14
Examples of what can go wrong
• Too few people in compliance roles• Decentralised compliance programme• Over centralised compliance programme• Insufficient in-depth monitoring• Ineffective audit programme• Line managers not taking responsibility• Culture and language barriers• Resistance to change• Others
15
Discussion
• What works for other companies?• What changes are you seeing internally?• What impact will these changes have on
our Compliance Programmes?• Are you seeing a shift in the types of
incidents reported in your companies?• Do you have any questions for us?