the$use$and$abuse$of$an/bio/cs$ during$pregnancy$ · infection and antibiotics in the aetiology,...
TRANSCRIPT

The Use and Abuse of An/bio/cs During Pregnancy
BSAC Spring Mee/ng, March 19th, 2015, RCP, London

The Abuse of An/bio/cs in Pregnancy
“The Major Obstetric Syndromes”!
• Preterm Birth!
• Preeclampsia!
• Stillbirth/small for gestational age!
Di Renzo GC. The Journal of Maternal-Fetal and Neonatal Medicine, August 2009; 22(8): 633–635 !

Infection and Antibiotics in the Aetiology, Prediction and Prevention of Spontaneous Early Preterm Labour and Preterm Birth!

The Cost of Preterm Birth !
• Babies born 22-26 weeks gestation!– 65% die in delivery room or in neonatal intensive care!
• Of the survivors at 2.5 years of age!– 50% disabled!
• 50% of these the disability is severe!
• At the age of 2.5 years !– Only 12-13% are alive and intact!
• Annual Cost of PTB in USA (IOM)- $26 billion!• UK cost of hospital re-admissions first 5-10 years!
– 20x more costly <28 vs >37 weeks !

Infection as a Cause of Spontaneous Early Preterm Labour (SPTL)!
• Bacterial products added to amnion cells in vitro results in a significant increase in PGE2 production !
– (Lamont et al, Lancet, 1985)!
• Between 26 and 34 wks GA, women in SPTL compared to women not in SPTL, are significantly more likely to have:!
– Abnormal vaginal flora (47% v 15%)!– Neonatal infection !– Chorioamnionitis (56% v 10%)!– (Lamont et al, BJOG, 1986)!
• Between 26 and 34 wks GA, women in SPTL compared to women not in SPTL, are significantly more likely to be colonised by high numbers Mycoplasmas and Ureaplasmas (18% v 0%)!
– (Lamont et al, J Med Microbiol, 1987)!

Late Miscarriage (<24w) and Early PTB (<34w) According to Grade of Vaginal Flora before 16 weeks!
16 weeks
16.7% 3.4%
Odds ratio = 5.35 (2.73 – 10.5) Relative risk = 3.12 (2.23 – 4.37) P-value = 0.000001
Hay PE, Lamont RF, Taylor-Robinson D et al, BMJ, 1994

It would appear logical to consider using antibiotics to
prevent PTB of infectious etiology!

The Problem with Antibiotic Studies
‘Different antibiotic studies have used different diagnostic methods, with different outcome parameters or differing definitions of success, to treat women of differing risks, with different susceptibilities and hence different host response, with different degrees of abnormal genital tract flora, at different gestational ages, using different antibiotics in different dose reg imens by d i f f e ren t r ou tes o f administration and not surprisingly DIFFERENT results’ Lamont 2001

Systematic Reviews/Meta-Analysis of Antibiotics used Prophylactically for the Prevention of PTB!
!!
2001 Guise! 2002 Koumans!
2003 Leitich! 2004 Klein!
2004 Riggs! 2005 Okun!
2006 Varma! 2007 Simcox!
2007 McDonald! 2008 Hutzal!
2008 Swadpanich! 2013 Brocklehurst!!
!Overall conclusions = antibiotics of no benefit!

So why the confusion?!
No Systematic review/meta-analysis has simultaneously addressed: • optimal choice of agent • optimal choice of patient • optimal choice of timing of administration

What is the best antibiotic?!

What is the best time to administer antibiotics?!

Which pregnant women should receive antibiotics?

Lamont RF, Nhan-Chang C-L, Sobel JD, Workowski K, Conde-Aguledo A, Romero R!Perinatology Research Branch, NICHD,NIH,DHHS!
Wayne State University, Detroit, MI!CDC, GA !
Am J Obstet Gynecol. 2011 Sep;205(3):177-90.

Hypothesis !
The conclusions of individual studies/systematic reviews/meta-analyses on the use of antibiotics used prophylactically for the prevention of PTB are flawed by the fact that undue reliance is placed on: !
i) Studies with suboptimal choice of antibiotics (mainly metronidazole)!ii) Used too late in pregnancy to influence outcome (23-27 weeks)!iii) In women whose risk of PTB was not due to BV!
(previous PTB, Low BMI, FFN, Ureaplasmas, GBS, TV, etc.) !Conversely, that antibiotics active against BV related organisms, used in
women whose risk of PTB is due to abnormal flora, and used early in pregnancy before irreversible inflammatory damage occurs, can reduce the rate of PTB !
! !!
Lamont et al, Am J Obstet Gynecol. 2011 Sep;205(3):177-90.

Preterm Birth 24-36 completed weeks of gestation
(5 Studies – Fixed Effects Model)!
Lamont et al, Am J Obstet Gynecol. 2011 Sep;205(3):177-90.

Preterm Birth 24-36 completed weeks of gestation
(5 Studies – Fixed Effects Model)!
Lamont et al, Am J Obstet Gynecol. 2011 Sep;205(3):177-90.

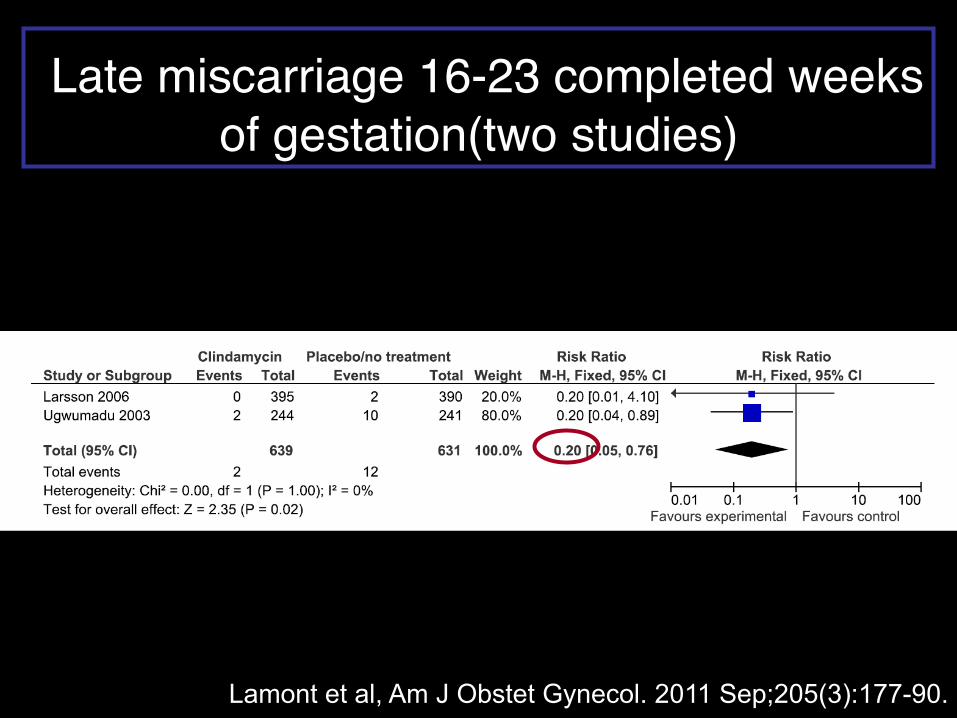
Late miscarriage 16-23 completed weeks of gestation(two studies) !
Lamont et al, Am J Obstet Gynecol. 2011 Sep;205(3):177-90.
Late miscarriage 16-23 completed weeks of gestation(two studies)!
Lamont et al, Am J Obstet Gynecol. 2011 Sep;205(3):177-90.

Conclusions!
• The appropriate antibiotics!– (clindamycin)!
• Given to the appropriate women !– (those with objective evidence of abnormal genital tract
flora)!• At the appropriate time in pregnancy to prevent infection
and inflammatory tissue damage!– (<22 weeks)!
• Significantly reduces the risk of LM (80%) & PTB (40%)!
Lamont et al, Am J Obstet Gynecol. 2011 Sep;205(3):177-90.

“The Right Antibiotics in the Right Women at the Right Time”!

Percep/on

Percep/on

What is the Current Extent of An/bio/c Usage?

Extent of Antibiotic Use in Pregnancy:the Who, What, Where, Why, When?!
Antibiotics!
Who?! What?!
When?! Where?!
Why?!
Self/OTC!
Hospital Dr!
GP!
Ist trimester !
2nd trimester!
In labour!3rd trimester!Hospital! Community!
Antibacterial!
Antiviral! Antifungal!
UTI!
URTI! PPROM! GBS!
Vulvovaginal candidiasis!
CS prophylaxis!

The Extent of An/bio/c use in Pregnancy
• Largely unknown • Nordic countries (registries)
– Not at single substance level/not all an/microbials – Short /me span/change in drug use over /me – Regional data – Lack demographic data
• Worldwide studies – Maternal recall of drug use – Small popula/on sample size
• Best Es/mate – An/bio/cs cons/tute 80% of drugs in pregnancy – 20-‐25% at least one prescribed an/bio/c in pregnancy (penicillins)

Extent of Antibiotic Use in Pregnancy!
BJOG. 2014. 121: 988-96 !

The Use of Antibiotics in a Population Based Cohort Study of Danish Pregnant Women
2000-2010!• Registry Based!
– Danish Medical Birth Registry!– Danish National Patient Registry!– Registry of Medicinal Product Statistics!
• Filled prescriptions for 4 main ATC groups (community based)!– Systemic antibacterials!– Systemic antimycotics!– Systemic antivirals!– Intravaginal antibiotics!
• Association with demographic variables and trends in antibiotic use over time (11 years)!
BJOG. 2014. Jul;121(8):988-96.! !

Results!• 987,973 pregnancies Denmark (2000-2010)!• 38.9% births received ≥1antibiotic treatment during
pregnancy!• Systemic antibacterials most frequent (33.4%)!
– Increased from 28.4% - 37% (2000-2010)!– Pivmecillinam 6.3% - 19.5% (2000-2010)!
• Demographics:!– Obesity (OR=1.5; 95% CI=1.47-1.56)!– Young age (OR=1.35; 95% CI=1.30-1.39)!– Low education (OR=1.37; 95% CI=1.35-1.39)!
Broe A, Pottegård A, Lamont RF, Jørgensen JS, Damkier P. The Increasing Use of Antibiotics in Pregnancy from 2000-2010: Prevalence, Timing, Category and
Demographics. !BJOG. 2014 Jul;121(8):988-96.!

Safety of An/microbials in Pregnancy
• Reluctance to perform safety studies (cost and ethical considera/ons) • Knowledge extrapolated from
– Animal studies – Anecdotal reports – Case-‐control studies relying on maternal recall
• Physiological adapta/ons alters pharmacokine/cs – Intravascular/extravascular volumes – Increased GFR and clearance – Placental passage rate limi/ng factor
• Changes with gesta/onal age • Drug characteris/cs (Mol wt; protein binding; fat solubility)
• Teratogenicity • An/microbial resistance • Atopy and allergy
Lamont et al., Safety of An/microbial Treatment During Pregnancy:
A Current Review of Resistance, Immunomodula/on and Teratogenicity.
Expert Opin Drug Saf. 2014. Dec;13 (12):1569-‐81

Teratogenesis • An/bacterial
• Penicillins • Cephalosporins • Macrolides • Lincosamides • Sulfonamides • Nitrofurantoin • Quinolones • Aminoglycosides • Tetracyclines • Metronidazole • Chloramphenicol
• An/virals • An/fungals
Lamont et al., Safety of An/microbial Treatment During Pregnancy:
A Current Review of Resistance, Immunomodula/on and Teratogenicity.
Expert Opin Drug Saf. 2014. Dec;13 (12):1569-‐81

An/microbial Resistance
• 2013 CDC: – ≥ 2,000,000 suffer from an/bio/c resistance • > 23,000 die as a result
• US Gain Act, 2012 • (Genera/ng An/bio/c Innova/on Now) • (FDA Safety and Innova/on Act)
Is Bacterial Vaginosis an Important Condition?!
US FDA Gain Act, 2012 (Generating Antibiotic Innovation Now)

Atopic Disease • Syndrome of hypersensi/vity/allergic triad
– Allergic lung disease (asthma) – Allergic derma//s (eczema) – Allergic rhini/s (Hay fever)
• Gene-‐environmental interac/on – 60% monozygo/c concordance
• Hygiene Hypothesis – Geographic and chronological increase in prevalence – Decreased exposure to infec/ons in childhood/an/bio/cs
• Biological model – neonatal gut microbiome • Failure of matura/on of immune response • Gut microflora in atopic children is different to controls • Neomune Project
– Danish Council for Strategic Research – Early milk and microbiota to s/mulate later immunity – hip://neomune.ku.dk/about/

Who Will Come to our Rescue and Make Us Understand?!

Human Microbiome Project (HMP)!

HMP Background!
• Human Genome Project • 100,000 genes predicted • 23,000 protein-coding genes found
• Human Supra-organism • Human genome+ bacterial microbiome • Bacterial cells 10x human somatic cells • Human microbiome = collective genome of symbionts • Bacterial genome provides traits that humans did not need to evolve • Human Genome + Microbiome > 1,000,000 genes
• NIH investing $100,000,000 roadmap for medical research

i) Molecular microbiologists ii) Bio-informatics & Computational statisticians BJOG, 2011. Apr;118(5):533-49.!

Summary!• Antibiotics should only be used when absolutely necessary during pregnancy.!• The long-term safety record of commonly used antibiotics is supported, but reliance on
these has led to a growing resistance problem.!– More evidence is needed to establish the safety of lesser used antibiotics to provide alternative treatments.!
• A growing body of evidence links antibiotic exposure in utero to atopic disease and alterations in the neonatal gut microbiome are thought to play a role. !
– More research needs to be done in this area to establish and explain this association.!
• Best estimate (underestimate): 40% pregnant women use antibiotics!– Teratogenicity: vigilence!– Safest: 1st line choice!– Dose, duration, frequency: minimum required!
• New devolopments!– Agents (GAIN Act)!– Diagnostics (BV panel)!– Microbiology (Human Microbiome Project)!– Probiotics/Prebiotics/Synbiotics!– Biofilms!

Thank you for your aien/on

hip://nocogo2015.dk

One size fits all