thematic analysis of community proposals final … · tasmania medicare local social determinants...
TRANSCRIPT

TASMANIA MEDICARE LOCAL
Social Determinants of Health Project
THEMATIC ANALYSIS OF COMMUNITY
PROPOSALS
FINAL REPORT
Undertaken by the University of Tasmania, Centre for Rural Health on behalf of
Tasmania Medicare Local
September 2014

1
Copyright Citation
©This work is copyright. Apart from any use permitted under the Copyright Act 1968 no part may be reproduced without the permission of the authors
Suggested Citation
Auckland, S., Woodroffe, J., Allen, P. 2014. Tasmania Medicare Local Social Determinants of Health Project: Thematic Analysis of Community Proposals. University of Tasmania
Acknowledgements
The authors would like to thank Tasmania Medicare Local for their collaboration and for providing funding to undertake this report.
The authors would also like to acknowledge Mr Darren Grattidge for his graphic design contributions to the report, and Ms Alexandra King for her assistance with editing the report.
Contact Information
For further information please contact the authors:
Mr Stuart Auckland Centre for Rural Health School of Health Sciences University of Tasmania Locked Bag 1320 Launceston TAS 7250 Email: [email protected] Phone: (03) 6324 4035 Dr Jess Woodroffe Centre for Rural Health School of Health Sciences University of Tasmania Locked Bag 1320 Launceston TAS 7250 Email: [email protected] Phone: (03) 6324 4035 Dr Penny Allen Rural Clinical School School of Medicine University of Tasmania Private Bag 3513 Hospitals' Campus Burnie TAS 7320 Email: [email protected] Phone: (03) 6324 5020
Website for access
http://www.utas.edu.au/rural-health/

2
Table of Contents
__________________________________________________________________________________
ACKNOWLEDGEMENTS 1
TABLE OF CONTENTS 2
LIST OF TABLES AND FIGURES 3
GLOSSARY & ACRONYMS 4
1. EXECUTIVE SUMMARY 6
1.1 BACKGROUND TO THE PROJECT 6
1.2 THE THEMATIC ANALYSIS PROJECT 7
2. INTRODUCTION 10
2.1 BACKGROUND TO THE REPORT 10
2.2 NEED FOR FURTHER ANALYSIS OF THE SOCIAL DETERMINANTS OF HEALTH PROJECT PROPOSALS 12
3. PROJECT APPROACH & METHODOLOGY 14
3.1 PROJECT BRIEF AND SCOPE 14
3.2 AN INTEGRATED APPROACH TO THE ANALYSIS 15
3.3 STAGES OF THE ANALYSIS 17
4. FINDINGS 18
4.1 PROFILE OF PROPOSALS BY REGION AND COMMUNITY OF PRIORITY 18
4.2 PROFILE OF PROPOSALS BY TARGETED SOCIAL DETERMINANTS OF HEALTH 19
4.3 PROFILE OF PROPOSALS BY REGION, COMMUNITIES OF PRIORITY & SDOH TARGETED 21
4.5 UNDERSTANDING AND AWARENESS OF SOCIAL DETERMINANTS OF HEALTH 25
4.6 PROFILE OF PROPOSALS BY LEAD ORGANISATION, PARTNERING ORGANISATIONS, SECTOR AND EVIDENCE OF
GOVERNANCE AND PARTNERSHIPS STRUCTURES 29
4.7 PROPOSAL OUTCOMES AND SUSTAINABILITY ISSUES 33
5. CONCLUSION 36
REFERENCES 38
APPENDICES 39

3
List of Tables and Figures
_________________________________________________________________________________
TABLE 1: LOCATION OF SUCCESSFUL COP BY REGION ......................................................................................................... 7
TABLE 2: SUCCESSFUL COP, LEAD ORGANISATIONS AND TARGETED SDOH ............................................................................ 11
TABLE 3: EXAMPLES OF VARIABLES AND ASSOCIATED THEMES FOR APPROACHING ANALYSIS ...................................................... 15
TABLE 4: NUMBER OF PROPOSALS BY TASMANIAN REGION ................................................................................................ 18
TABLE 5: NUMBER OF PROPOSALS BY COMMUNITY OF PRIORITY (COP) ............................................................................... 19
TABLE 6: SOCIAL DETERMINANTS OF HEALTH AND NUMBER OF PROPOSALS ADDRESSING EACH DETERMINANT ............................. 20
TABLE 7: LEAD ORGANISATION OR PARTNERING ORGANISATION BY SECTOR ........................................................................... 30
FIGURE 1: COMMUNITIES OF PRIORITY AND TARGETED SOCIAL DETERMINANTS OF HEALTH ..................................................... 22
FIGURE 2: COMMUNITIES OF PRIORITY AND TARGETED SOCIAL DETERMINANTS OF HEALTH ..................................................... 23
FIGURE 3: COMMUNITIES OF PRIORITY AND TARGETED SOCIAL DETERMINANTS OF HEALTH IN THE ........................................... 24

4
Glossary & Acronyms
__________________________________________________________________________________
ABARE
The Australian Bureau of Agricultural and Resource Economics, ABARE, established in 1945, is an
Australian government economic research agency. It is also involved in commercial consultancy.
ABS
The Australian Bureau of Statistics (ABS) is Australia's national statistical agency. The ABS provides
key statistics on a wide range of economic, environmental and social issues.
Capacity Building
Capacity building is the process by which individuals, groups, organizations, institutions and societies
increase their abilities to perform core functions, solve problems, define and achieve objectives; and
understand and deal with their development needs in a broad context and in a sustainable manner.
Communities of Priority (CoP)
Communities of Priority are the 18 Local Government Areas (LGAs) that have been identified by
Tasmania Medical Local for the purposes of the Social Determinants of Health Project. These are
priority areas based on ABS data concerning social economic status, remoteness and capacity to
implement sustainable solutions.
Evidence based
Measurements or observational methods providing reliable and valid data across multiple
measurements, observations and studies.
Expression of Interest (EoI)
EoI refers to the Tasmania Medicare Local Social Determinants of Health ‘Expression of Interest’
process and Application Form, used by applicants in submitting their project proposals.
Local Government Area (LGA)
Local Government Areas (LGAs) are an ABS approximation of officially gazetted LGAs as defined by
each State and Territory (S/T) Local Government Department. An LGA is a spatial unit which
represents the whole geographical area of responsibility of an incorporated Local Government
Council. Tasmania has 29 Local Government Areas and Councils.
NAPLAN
National Assessment Program – Literacy and Numeracy (NAPLAN) is an annual assessment for
students in Years 3, 5, 7 and 9. NAPLAN tests the sorts of skills that are essential for every child to
progress through school and life, such as reading, writing, spelling and numeracy.
Place based approach
A collaborative process by which stakeholders address issues as they are experienced within a
geographic space, be it a neighbourhood or community.

5
Proposals
Refers to the 59 submissions or applications received in the EoI process.
SEIFA
Socio-Economic Indexes for Areas (SEIFA) is a product developed by the ABS that ranks areas in
Australia according to relative socio-economic advantage and disadvantage. The indexes are based
on information from the five-yearly Census and are assigned to areas, not to individuals. They
indicate the average socio-economic characteristics of the people, families, and households living in
the area. Common uses for SEIFA include determining areas that require funding and services and
research into the relationship between socio-economic disadvantage and various health and
educational outcomes.
Social Determinants of Health (SDoH)
The Social Determinants of Health are defined broadly as the conditions in which people are born,
grow, live, work and age. These circumstances are shaped by the distribution of money, power and
resources at a global, national and local level. The Social Determinants of Health are mostly
responsible for health inequities – the unfair and avoidable differences in health status seen within
and between countries (World Health Organisation 2014).
TML
Tasmania Medicare Local (TML) is a non-government, not-for-profit primary health care organisation
working to help coordinate and connect primary health care services for local communities. TML
aims to identify local health care needs, work to address any service gaps and make it easier for
Tasmanians to access the health services they need closer to home.

6
1. EXECUTIVE SUMMARY
__________________________________________________________________________________
1.1 Background to the Project
In 2013, as part of the Tasmanian Health Assistance Package (Schedule 33), Tasmania Medicare Local
(TML) program received funding from the Australian Government Department of Health for two
projects, aimed at improving the health of Tasmanians. These are the Risk Factor Project and the
Social Determinants of Health Project.
The Social Determinants of Health Project is both significant and unique because Tasmania Medicare
Local is the only Medicare Local nationally to receive substantial, long-term Australian Government
funding to manage a project that addresses social determinants of health at a local level.
The project aims to not only identify the major determinants of health in Tasmania, but also to
develop and implement strategies and activities to address them. It focuses on improving the health
of Tasmanians through addressing social determinants of health such as social status, health literacy,
housing, food, transport and education. It offers an exciting new opportunity to explore innovative
and evidence based approaches to addressing social determinants of health, through strong
partnerships with some of Tasmania’s most disadvantaged communities, and a commitment to
utilising place based approaches and capacity building strategies.
In developing a solid foundation for the project, TML undertook three stages of project planning
from July to December 2013. This involved: (1) conducting community and stakeholder consultations
across Tasmania; (2) running a visioning and priority-setting workshop with the project steering
group and team; and (3) investigating the literature, data and other policies and programs in place
across the state in the social determinants of health area. From this planning process, four key
themes were considered to be fundamental in implementing the project:
1. Undertaking a place-based approach to working with communities across the state;
2. Identifying “Communities of Priority” based on need and readiness;
3. Resourcing communities to assist them in identifying and addressing the social determinants
of health relevant to their circumstance; and
4. Building capacity within communities and across the state to harness sustainability beyond
the life of the project.
In developing this evidence based and place based approach to addressing the social determinants
of health, Tasmania Medicare Local identified 18 Communities of Priority (CoP) in Tasmania
according to their socio economic status, remoteness and capacity to implement sustainable
solutions. These included Break O’Day, Burnie, Brighton, Central Highlands, Devonport, Derwent
Valley, Dorset, Georgetown, Glenorchy, Glamorgan/Spring Bay, Huon Valley, Kentish, Launceston,
Sorell, Southern Midlands, Tasman, Waratah/Wynyard and the West Coast.
In February 2014, an Expression of Interest (EoI) process was implemented, inviting these
Communities of Priority to apply for funding. A key requirement of the EoI process was that

7
applicants had to propose locally place based projects that: (1) addressed and/or had the potential
to impact on one or more of the social determinants of health; and (2) involved a partnership of
three or more organisations based in, providing an outreach service to or wishing to establish a
service in a Community of Priority.
In total, 59 proposals were received during the process from all 18 Communities of Priority. Eight
Communities of Priority from the North West, Northern and Southern regions of Tasmania were
successful in receiving ‘project development’ funding of $50,000 to progress their proposals to a
detailed project stage. Table 1 provides an overview of these CoPs by region.
Table 1: Location of Successful CoP by Region
North West Region Northern Region Southern Region
Waratah - Wynyard Launceston Derwent Valley
Burnie
Devonport (n=2) Brighton (n=2)
1.2 The Thematic Analysis Project In recognition of the scope and diversity of the 59 proposals and the need to undertake a more
detailed review of the information presented in them, Tasmania Medicare Local invited the
University of Tasmania Centre for Rural Health (CRH) to conduct a thematic and content analysis of
the proposals.
The thematic and content analysis applied an integrated approach to reviewing the proposals, and
incorporated quantitative and qualitative analysis and interpretive processes. The key aims of this
thematic analysis were to: better understand the Social Determinants of Health that were focussed
on, analyse the ways in which the proposals had approached the Social Determinants of Health at a
local level, note the evidence that was drawn on to demonstrate need, and synthesis the ways in
which applicants had conceptualised partnerships and models of governance, as well as their
understandings of sustainability, planning and social equity.
The information contained within all 59 proposals was comprehensive and diverse, with many
different approaches being proposed. The thematic analysis provided a valuable insight into the
understanding of, and approaches to, addressing Social Determinants of Health in each of the 18
Communities of Priority.
With respect to the Communities of Priority that were targeted by applicants in the EoI process, the
thematic and content analysis showed that 47.5 per cent (n=28) of proposals came from the
Southern region of Tasmania, 30.5 per cent (n=18) from the Northern region (n=18) and 22 per cent
(n=13) from the North West region.
A total of 225 organisations were listed as either lead organisations and/or partnering organisations.
The organisations were drawn from a range of different sectors including: not-for-profit
incorporated organisations and company organisations, Local Government Councils, Community
Neighbourhood Houses, rural health services, sporting groups, Universities, the business sector and

8
State Government Departments such as schools. Not surprisingly, the not-for-profit sector was
represented in 53 per cent of all proposals (n=119) as both lead organisation (n=35) or as a
partnering organisation (n=84). All the NGOs listed as either lead organisations or partnering
organisations were active in the population health or social services sectors.
A broad range of Social Determinants of Health were identified and targeted in the proposals. These
included: social status, health literacy, housing, transport, employment, education/training or skills
development, physical activity, food security/access to healthy food, prevention or treatment of
addiction, community connectedness or cohesion, family relationships or home life, financial or
economic security, mental health/psychological wellbeing, access to health and support services,
healthy ageing and other determinants such as migrant health. It should be noted that many
proposals, while nominating and acknowledging social determinants, also drew heavily on a broader
determinant of health framework, acknowledging issues such as physical environments and
infrastructure, ethnicity and culture, participation and inclusion, as well as others that influence
health and wellbeing.
There were six determinants of health that were most commonly identified as primary and
secondary targets for action within the proposals and across all Communities of Priority. These were:
(1) Social Status (61% of proposals), (2) Education, Training and Skills Development (52.5%), (3)
Health Literacy (47.5%), (4) Community Connectedness, Inclusion and Cohesion, (5) Employment
(39%) and (6) Food Security/Access to Healthy Food (30.5%).
The interpretative analysis of the proposals revealed that the EoI applicants had a reasonable
awareness and understanding of the SDoH concepts and that this awareness and understanding had
been gained from a broad range of sources but limited type of sources. However, there was little
evidence to suggest that a majority of the applicants had a deeper understanding of the SDoH as
they relate to the interplay between the local socio-economic and environmental factors that
influence the standard of health and wellbeing.
The concept of local place based approaches refers to action at a local level to influence change
through providing choice and control at the community level was generally well understood, with a
majority of applicants articulating strategies that would support a placed based approach. Less well
articulated was the understanding of how issues of access and equity would be addressed through
the proposed action on the SDoH.
The notion of inter-sectoral collaboration and representative governance structures was addressed
well in the proposals. There was evidence that there had been considerable effort by the lead
organisations to involve a diverse range of partnering organisations across multiple sectors. In over
70 per cent of the proposals, the composition of the partnership was informed by either prior
collaborative experiences or some other form of association such as working with the same
community. In the remaining proposals, the basis of the partnership appeared to be more
opportunistic, with lead organisations seeking to establish new strategic collaborations to address
the proposal objectives. It was unclear in some proposals as to what each partner would contribute
to the proposed works and therefore assessment of the adequacy of the governance of the
proposed partnership and ultimately its sustainability was indeterminate.

9
The issue of short and longer term impacts and sustainability of outputs was the least well-
articulated of the criteria included in the EoI process. With the exception of listing potential impacts,
the proposals on a whole, with few exceptions, did not explain what strategies would be employed
to ensure that the outputs from the projects would be sustained over an infinite time period.
In conclusion, valuable learnings can be drawn from both the EoI process and content of the
proposals that could inform future EoI processes. Despite the identified limitations, the EoI process
proved to be an effective approach for drawing together communities of interest to consider
innovative approaches to taking a place based approach to addressing the SDoH.
Mr Stuart Auckland, Dr Jess Woodroffe and Dr Penny Allen Report Authors – University of Tasmania

10
2. INTRODUCTION
__________________________________________________________________________________
2.1 Background to the Report
In 2013, as part of the Tasmanian Health Assistance Package (Schedule 33), Tasmania Medicare Local
(TML) program received funding from the Australian Government Department of Health for two
projects, aimed at improving the health of Tasmanians. These included a Risk Factors Project and a
Social Determinants of Health Project.
This Social Determinants of Health Project is both significant and unique because Tasmania Medicare
Local is the only Medicare Local nationally to receive substantial, long-term Australian Government
funding to manage a project that addresses Social Determinants of Health at a local level.
The project aims to not only identify the major determinants of health in Tasmania, but also to
develop and implement strategies and activities to address them. It focuses on improving the health
of Tasmanians through addressing Social Determinants of Health such as social status, health
literacy, housing, food, transport and education. It offers an exciting new opportunity to explore
innovative and evidence based approaches to addressing Social Determinants of Health, through
strong partnerships with some of Tasmania’s most disadvantaged communities, and a commitment
to utilising place based approaches and capacity building strategies.
The project also takes account of the social, cultural and institutional context of a region, its physical
geography and the knowledge of its residents, which are seen as central to developing solutions that
are both relevant and realistic for those communities.
In developing a solid evidence base for the project, TML undertook three stages of project planning
from July to December 2013. This involved: (1) conducting community and stakeholder consultations
across Tasmania; (2) running a visioning and priority-setting workshop with the project steering
group and team; and (3) investigating the literature, data and other policies and programs in place
across the state in the Social Determinants of Health area. From this planning process, four key
themes were identified as fundamental for implementing the project:
1. Undertaking a place-based approach to working with communities across the state;
2. Identifying “Communities of Priority” based on need and readiness;
3. Resourcing communities to assist them in identifying and addressing the Social Determinants
of Health relevant to their circumstance; and
4. Building capacity within communities and across the state to harness sustainability beyond
the life of the project.
In developing this evidence based and place based approach to addressing the Social Determinants
of Health, Tasmania Medicare Local identified 18 Communities of Priority (CoP) in Tasmania
according to their socio economic status, remoteness and capacity to implement sustainable
solutions. These included Break O’Day, Burnie, Brighton, Central Highlands, Devonport, Derwent

11
Valley, Dorset, Georgetown, Glenorchy, Glamorgan/Spring Bay, Huon Valley, Kentish, Launceston,
Sorell, Southern Midlands, Tasman, Waratah/Wynyard and the West Coast.
In February 2014, an Expression of Interest (EoI) process was implemented, inviting these
Communities of Priority to apply for funding via project proposals. A key requirement of the EoI
process was that applicants had to propose local, place based project proposals that (1) addressed
and/or has the potential to impacts on one or several of Social Determinants of Health; and (2)
involved a partnership of three or more organisations based in, providing an outreach service to or
wishing to establish a service in a Community of Priority.
Interested parties were provided with an information package and guidelines which contained
details of the rationale, scope and eligibility criteria associated with EoI process. In addition, regional
forums were provided by the funding body to potential applicants.
In total, 59 proposals were received collectively during the expression of interest process from all 18
Communities of Priority. Each of the 59 proposals was assessed resulting in a shortlist of potentially
successful proposals. Representatives from the shortlisted applicants were then invited to attend an
interview with TML project staff. Eight Communities of Priority from the North West, Northern and
Southern regions of Tasmania were successful in receiving ‘project development’ funding of $50,000
to progress their proposals to a detailed project stage. The successful CoPs and their respective lead
organisations/partnering organisations and targeted Social Determinants of Health are listed in Table
2 below.
Table 2: Successful CoP, lead organisations and targeted SDoH
Community of Priority
1Lead Organisation and Partners Targeted Social Determinant of Health
Waratah Wynyard 1The Smith Family Wynyard High School Table Cape Primary School Waratah-Wynyard Council
Education and social connectedness
Burnie 1Burnie Community House Centacare Heart Foundation Mission Australia TasTAFE
Training, employment, social connectedness, food access
Devonport 1Devonport City Council Devonport Community House Eastern Shore Community House Gateway Community Care
Training, employment, social connectedness, food access
Devonport 1Youth Family and Community Connections Don Medical Devonport City Council Wise Employment Eastern Shore Community House
Training, employment, social connectedness
1 Lead Organisation

12
Launceston 1Ravenswood Neighbourhood House Ravenswood Child and Family Centre Ravenswood Heights Primary School Ravenswood Child Health and Parenting Service
Training, literacy, food access
Brighton 1Brighton Council Workskills Inc MONA Australian Red Cross
Housing, education, employment, social inclusion
Brighton 1Jordan River Service Inc Colony 47 Second Bite Local General Practitioner Centacare Evolve Workskills Inc
Training, employment, social connectedness, food access
Derwent Valley 1Derwent Valley Community House New Norfolk High School Derwent Valley Council Derwent Valley Real Action Forward Thinking (RAFT) Workskills Inc
Education, training employment, social connectedness
1 Lead Organisation
2.2 Need for Further Analysis of the Social Determinants of Health Project Proposals
In assessing the 59 submitted proposals, it was apparent to Tasmania Medicare Local that there
were further interpretations, knowledge and evidence contained in the proposals that could add
evidence to, and inform the Social Determinants of Health Project, including the design and
implementation of future project activity in Tasmania.
In recognition of the scope and diversity of all 59 proposals and the need to undertake a more
detailed review of the information presented in them, Tasmania Medicare Local invited the
University of Tasmania Centre for Rural Health (CRH) to conduct a thematic and content analysis of
the proposals.
This project has since been referred to as the Tasmania Medicare Local Thematic Analysis of
Community Submissions for Social Determinants of Health Project. The primary aim of the project
was to undertake a thematic analysis of the 59 proposals with a view to providing information about
the profile of proposal proponents and details about the scope of the proposals.
This report details and discusses the findings of this process, and acknowledges that the information
contained within all 59 proposals was comprehensive and diverse, with many different approaches
and responses to the expression of interest process being received.
The findings reveal the Social Determinants of Health that were focussed on, the ways in which the
proposals had approached identified Social Determinants of Health at a local level, the evidence that
was drawn on to demonstrate need, the ways in which applicants had conceptualised partnerships
and models of governance as well as their understanding and of sustainability, planning as well as
social equity. The thematic and content analysis provides valuable insight into the current

13
understanding of, and approaches to, addressing Social Determinants of Health in each of 18
Communities of Priority within Tasmania.
This report concludes with some recommendations for the funding body with respect to the
communication and feedback of the key findings from the project.

14
3. PROJECT APPROACH & METHODOLOGY
__________________________________________________________________________
3.1 Project Brief and Scope
In planning for, and undertaking this project, it should be acknowledged that the report authors
were given a broad activity brief by the funding agency, Tasmania Medicare Local. As detailed in the
introduction of this report, the primary aim of the project was to undertake a thematic analysis of
the 59 proposals, including those that were successful in receiving funding and those that were
unsuccessful, with a view to providing information about the profile of applicants and the scope of
the proposals. While the report authors were aware of which proposals were successful and which
were unsuccessful, this was not a central focus or point of comparative analysis in the thematic
analysis.
The EoI Application Form asked applicants to provide (mainly qualitative) responses to a number of
questions and criteria (see Appendix 1). These included information about the applicant’s region,
Community(ies) of Priority, partnering organisations, names of incorporated bodies, a broad outline
of their proposal including the targeted social determinant(s) of health, an outline of how they had
become aware of these targeted Social Determinants of Health, a description of what each
nominated organisation would contribute to the partnership, an outline of their approach to
governance arrangements and planning and development of their initiative, and the short and long
term outcomes that the initiative hoped to achieve.
The methodological approach and framework for the analysis needed to be quite flexible and
iterative, both because of the high number of proposals and because the report authors had not
been involved in the design and development of the Expression of Interest Application Form (e.g.
questions asked or criteria addressed, format etc). Once an initial analysis of the proposals had been
conducted, it was clear that the project required an integrated approach to managing, analysing and
interpreting the large amount of information contained in the proposals. The authors decided on a
mixed analytical framework for the analysis. This approach was approved by Tasmania Medical
Local, which provided an example of the types of themes and variables which they might expect to
see in the analysis (see Table 3 below).

15
Table 3: Examples of variables and associated themes for approaching analysis
Variables Themes
Organisations (lead
organisations and partners) • Sector
• Size
• Location
Partnerships • Resources
• Governance, roles and responsibilities
• Relationships history
• Collaboration
Project reach (geographic
and demographic) • Location of projects
• Target populations
Social determinants • Social determinant(s) targeted – primary
• Social determinants(s) targeted – secondary
Project activity • Approach
• Project activity/intervention
Policy and structural
outcomes • Policy change
• Structural change
• Systems and processes change
3.2 An Integrated Approach to the Analysis
An integrated and staged approach was used to collate, review and interpret all the information
contained in the 59 comprehensive proposals. An integrated approach to analysis essentially
involves the application of a number of techniques to interpret information. In this project, because
of the design of the Expressions of Interest Application Form, it was possible to manage and analyse
the proposal information at both a quantitative or descriptive level, as well as a thematic or more
detailed qualitative level, using the criteria in the proposals as a framework.
Quantitative Analysis
Information within the proposals that could be analysed through basic numerical description was
collated and entered into an SPPS data management software package. SPSS software assisted in
capturing frequencies within the data, such as counts and percentages of answers to relevant
questions (e.g. region of applicants, type of and number of collaborating organizations, number of
project partners, number of social determinants identified by frequency and region). This type of
information could not be reliably gathered through qualitative analysis alone. The findings from the
quantitative analysis were then used to present a clearer statistical picture of the proposals, to
identify and cross-check trends in responses, and to support the qualitative analysis process.
Qualitative Analysis
The Expression of Interest Application Form required applicants to respond in detail to a number of
predefined criteria (e.g. a broad outline of proposal, awareness and evidence of Social Determinants
of Health, responsibilities of partners and collaborating organisations, as well as initiative and
16
planning and development information). In collating and interpreting this information, it was
appropriate that the analysis be undertaken using a thematic and content approach.
Thematic analysis is a well-accepted approach to analysing and categorising qualitative data
collected in research. It represents some patterned response or meaning within the information or
data being looked at. A thematic analysis largely involves the identification of ideas, topics or
recurring patterns in written information (usually data collected in processes such as interviews,
focus groups or surveys). The process is often described as iterative or inductive because it involves
the building up of concepts and ideas rather than drawing on pre-conceived categories (Liamputtong
and Ezzy 2005). It further involves coding the data, which entails organizing and sorting sections of
written text into groups and segments (open codes) which are then examined to generate larger
themes and categories and their relationships.
The analysis of the qualitative results also drew on elements of content analysis – which does use
pre-established codes or categories for interpreting the data. Because of the prescriptive rather than
open-ended nature of the EOI process (e.g. structured criteria and questions and limited text boxes)
it was necessary to approach the analysis of the proposals using both techniques in order to most
validly interpret the 59 proposals.
Additionally, the process of the qualitative analysis was also framed by the definition of the Social
Determinants of Health. Our analysis of the 59 proposals considered them within the context of the
World Health Organisation’s definition of the Social Determinants of Health, as follows:
The circumstances, in which people are born, grow up, live, work and age, and the systems
put in place to deal with illness. These circumstances are in turn shaped by a wider set of
forces: economics, social policies, and politics. The determinants of health are mainly
responsible for health inequalities, the unfair and avoidable differences in health status
(WHO, 2014).
While these were not the primary focus of our analysis and review of the proposals, we also
recognised the wider determinants of health and wellbeing, including the social and economic
environment, the physical environment and people’s individual characteristics and behaviours which
have such a strong influence on health and wellbeing, both individually and collectively. In some of
the proposals, social determinants and broader determinants were inherently tied together in the
approach taken and information provided. Proposals that undertook this integrated approach were
not excluded from the analysis.

17
3.3 Stages of the Analysis
As detailed above, both qualitative and quantitative analysis techniques were used to examine the
59 proposals. A number of stages were applied to allow both descriptive and interpretive findings to
emerge, including:
1. Importing/collating each of the 59 proposals into a central electronic file.
2. Creating an SPPS data management spreadsheet, structured around the questions and
criteria in the Expression of Interest (EoI) Application Form (Appendix 1).
3. The creation of a number of Microsoft Word documents to store the qualitative responses
from all 59 proposals will be stored (e.g. each of the responses to the criteria which required
open or descriptive text and answers).
4. The use of SPSS to analyse the proposal responses by counts and frequencies.
5. Conducting ‘open coding’ of the qualitative responses to each EoI criteria by two of the
authors.
6. Cross-checking the open coding by both authors to ensure consistency and reliability in the
identification of qualitative themes and content.
7. The use of NVivo software where necessary to assist in more detailed interpretation of
themes and content in the proposals.
8. Engaging in further interpretation of the qualitative themes generated from the analysis
against SDoH frameworks and relevant documents.
9. Integrating the qualitative and quantitative data to generate the discussion,
recommendations and final report.
An integrated approach incorporating qualitative and quantitative analysis techniques was used to
review and analyse the proposals. The key aim of conducting this integrated analysis was to develop
a better understanding of the profile of applicants, the regions in which they were located, the
make-up of proposed partnerships, the Social Determinants of Health being focussed on, the ways in
which the proposals had approached targeted Social Determinants of Health at a local level, the
evidence that was drawn on to demonstrate need, the ways in which applicants had conceptualised
partnerships and models of governance, as well as their understanding of sustainability, planning
and social equity. These specific findings are presented in the next section of this report.

18
4. FINDINGS
__________________________________________________________________________________
This section of the report presents the key findings and themes generated from the analysis of the
Expression of Interest proposals. Where appropriate, this section draws on descriptive statistical
data and figures, as well as examples of qualitative quotes from proposals.
4.1 Profile of Proposals by Region and Community of Priority
In total, 59 proposals were received by TML in response to the Expression of Interest Social
Determinants of Health Proposal process.
Proposals were received from all three regions of Tasmania (North West, Northern and Southern)
and from all 18 local government geographic areas identified as Communities of Priority within these
regions. While all Communities of Priority were represented, there was considerable variation in the
number of proposals received from (a) these communities and (b) the regions in which they are
located.
Table 4 below shows the number of EoI proposals received by each greater geographical region of
Tasmania.
Table 4: Number of proposals by Tasmanian region
Region of Tasmania Number of proposals
within region % of total proposals state-wide
North West 13 22
Northern 18 31
Southern 28 48
Table 5 below shows the number of EoI proposals received by each of the Communities of Priority
within the three Tasmanian regions. As shown, there were five CoPs in the North West Region of
Tasmania, five in the Northern Region and eight in the Southern Region.
It should be noted that there were some proposals which had a broader scope than just one CoP
(e.g. Burnie and Devonport) or which took a regional approach (e.g. Cradle Coast Authority
geographic catchment). There are therefore some CoPs which have been recorded as focus locations
more than once.

19
Table 5: Number of proposals by Community of Priority (CoP)
Region of Tasmania Community of Priority (CoP)
Number of proposals with CoP as focus location/shared focus
location *
North West Region
Burnie 6
Devonport 5
Waratah/Wynyard 2
Kentish 2
West Coast 1
Northern Region
Launceston 12
Dorset 3
Glamorgan/Spring Bay 3
Break O'Day 3
George Town 2
Southern Region
Glenorchy 10
Derwent Valley 7
Huon Valley 4
Southern Midlands 4
Brighton 4
Sorell 3
Tasman 2
Central Highlands 2
As shown in the Table 4 and 5, the analysis of the proposals indicated that the Communities of
Priority in which proposed activities would occur varied between each of the three regions.
Most CoP were referenced as target communities in multiple proposals, with Launceston (n=12) and
Glenorchy (n=10) identified the most times across all regions. The least targeted CoP in the
proposals were the West Coast (n=1), George Town (n=2), Tasman (n=2) and Central Highlands
(n=2).
4.2 Profile of Proposals by Targeted Social Determinants of Health
The Expression of Interest process requested that proposals provide a broad outline of their
targeted Social Determinants of Health. While this was approached qualitatively in a diversity of
ways by applicants, and reflected both broad and specific understandings of Social Determinants of
Health (see Section 4.5 below), it was possible to analyse and quantify the social determinants being
targeted.
In total, 22 individual determinants of health were identified within 98.3 per cent of the proposals as
primary or secondary targeted determinants. For the purpose of the analysis, these determinants
were grouped into 16 individual groupings (Table 6). Only one proposal did not clearly identify or
focus on a social determinant of health that could be used validly in the broader analysis.
20
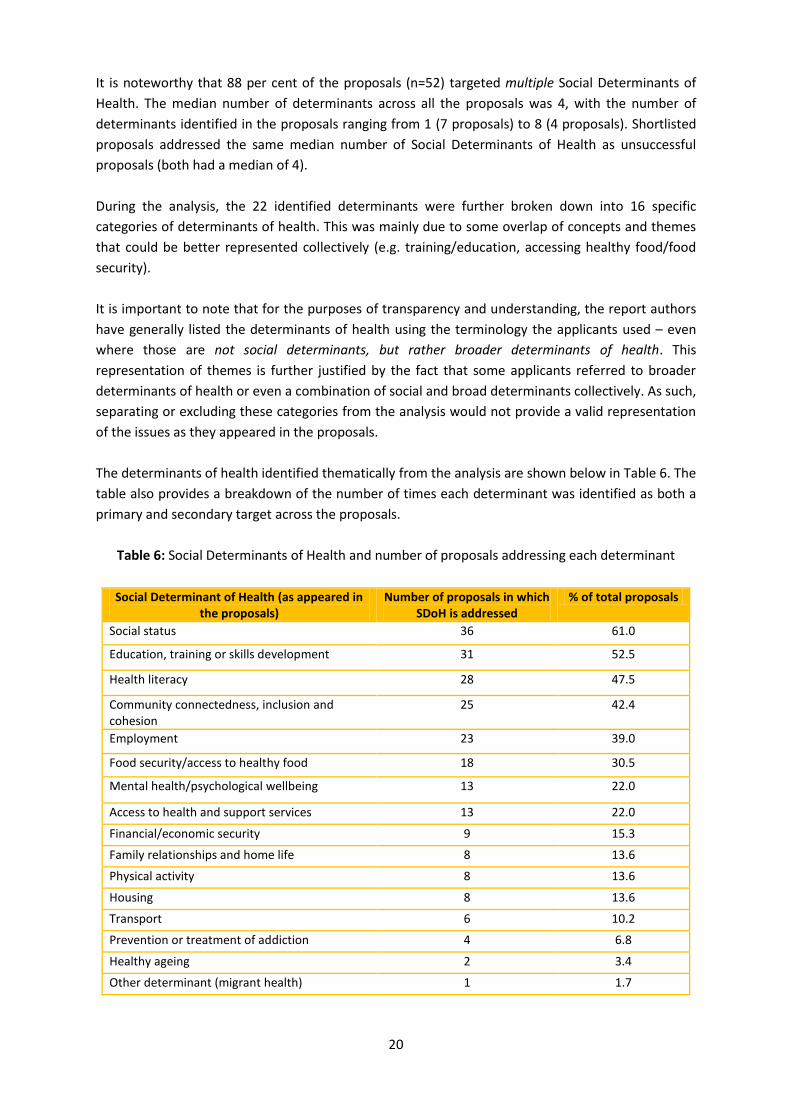
It is noteworthy that 88 per cent of the proposals (n=52) targeted multiple Social Determinants of
Health. The median number of determinants across all the proposals was 4, with the number of
determinants identified in the proposals ranging from 1 (7 proposals) to 8 (4 proposals). Shortlisted
proposals addressed the same median number of Social Determinants of Health as unsuccessful
proposals (both had a median of 4).
During the analysis, the 22 identified determinants were further broken down into 16 specific
categories of determinants of health. This was mainly due to some overlap of concepts and themes
that could be better represented collectively (e.g. training/education, accessing healthy food/food
security).
It is important to note that for the purposes of transparency and understanding, the report authors
have generally listed the determinants of health using the terminology the applicants used – even
where those are not social determinants, but rather broader determinants of health. This
representation of themes is further justified by the fact that some applicants referred to broader
determinants of health or even a combination of social and broad determinants collectively. As such,
separating or excluding these categories from the analysis would not provide a valid representation
of the issues as they appeared in the proposals.
The determinants of health identified thematically from the analysis are shown below in Table 6. The
table also provides a breakdown of the number of times each determinant was identified as both a
primary and secondary target across the proposals.
Table 6: Social Determinants of Health and number of proposals addressing each determinant
Social Determinant of Health (as appeared in the proposals)
Number of proposals in which SDoH is addressed
% of total proposals
Social status 36 61.0
Education, training or skills development 31 52.5
Health literacy 28 47.5
Community connectedness, inclusion and cohesion
25 42.4
Employment 23 39.0
Food security/access to healthy food 18 30.5
Mental health/psychological wellbeing 13 22.0
Access to health and support services 13 22.0
Financial/economic security 9 15.3
Family relationships and home life 8 13.6
Physical activity 8 13.6
Housing 8 13.6
Transport 6 10.2
Prevention or treatment of addiction 4 6.8
Healthy ageing 2 3.4
Other determinant (migrant health) 1 1.7

21
As reported in Table 6, six determinants of health were most commonly identified as primary and
secondary targets for action across all Communities of Priority. These were: (1) Social Status (61% of
proposals), (2) Education, Training and Skills Development (52.5%), (3) Health Literacy (47.5%), (4)
Community Connectedness, Inclusion and Cohesion, (5) Employment (39%) and (6) Food
Security/Access to Healthy Food (30.5%).
4.3 Profile of Proposals by Region, Communities of Priority & SDoH targeted
In order to develop a profile of the different Social Determinants of Health being targeted and their
CoPs, maps were generated from the data shown in Tables 2, 3, and 5. Figures 1 – 3 below provide a
visual representation of the Social Determinants of Health (primary and secondary) that were
identified in the proposals, highlighted by the Community of Priority and by region. The number of
and type of SDoH varied both within and between the three regions. On a regional basis, the
Southern region had the most number of CoPs (n=8), whilst the Northwest and Northern regions
both had five CoPs respectively. The most number of SDoH addressed in a proposal from a single
CoP was Burnie (n=13), followed by Launceston (n=12). The least number of SDoH addressed in a
proposal from a CoP was the West Coast (n=1), followed by Sorell (n=2), which addressed social
status, and community connectedness and cohesion.

22
Figure 1: Communities of Priority and Targeted Social Determinants of Health in the North West Region of Tasmania

23
Figure 2: Communities of Priority and Targeted Social Determinants of Health
in the Northern Region of Tasmania

24
Figure 3: Communities of Priority and Targeted Social Determinants of Health in the Southern Region of Tasmania
25
4.5 Understanding and Awareness of Social Determinants of Health
The Expression of Interest process asked applicants to detail how they had become aware of the
issues surrounding the Social Determinants of Health identified in their proposal. The analysis of this
information revealed some considerable differences in the ways in which the applicants understood,
and demonstrated awareness of, the Social Determinants of Health in their targeted Communities of
Priority. It also showed disparities in the way applicants detailed their understanding of how the
SDoH interact with, and upon, not only the health but the social, economic and environmental fabric
of their respective communities.
Three key themes were produced from the analysis of the awareness of applicants with regards to
SDoH in their CoP(s). These were: (1) general awareness and understanding of the Social
Determinants of Health, including use of evidence based approaches; (2) adoption of place based
approaches; and (3) considerations of social equity and access.
General Awareness, Evidence and Understanding of Social Determinants of Health
Overall, the proposals revealed that the applicants had a reasonable awareness and understanding
of the SDoH. However, there was inconsistency in the ways in which SDoH were defined and
contextualised within both general and local contexts.
A clear awareness of the SDoH was most evident in proposals that articulated an understanding that
health was influenced by the interplay of a range of social, economic, environmental, political and
cultural factors rather than simply the provision of health services, or as expressed in one proposal,
“as the relationship between people, place and health”. This perspective is captured in the following
extracts from two proposals:
Health starts at homes, communities, schools and workplaces not just with health care
services which may be viewed as having limited influence on the SDoH (Southern Region
proposal)
Such a strong relationship between health and life outcomes for children and the socio-
economic circumstances in which they live (Northern Region proposal)
There were, however, a number of proposals that did not clearly articulate a strong understanding
or awareness of SDoH. For example, some proposals focused on a particular risk factor or health
issue/behaviour (e.g. bullying, obesity, abuse, teen pregnancy) and thus failed to clearly articulate
the links between the risk factor/issue and the broader social determinants that could be addressed
at a local or regional level to make an impact on these conditions. It should be noted that many
proposals, while nominating and acknowledging social determinants, also drew heavily on a broader
determinant of health framework by acknowledging issues such as physical environments and
infrastructure, ethnicity and culture, participation and inclusion, as well as others that influence
health and wellbeing.

26
At a basic or general level, very few of the applicants provided or reiterated a conceptual definition
of the Social Determinants of Health, or referenced additional documents that might be expected to
be seen in an outline of a project proposal addressing such issues.
In most cases, the proposals referred to material provided in the Tasmania Medicare Local (TML)
Expression of Interest (EoI) brief, as well as to material provided in the regional forums offered to
the potential applicants. However, only a small number of proposals referenced or contextualised
their proposals by referring to literature and resources indexed in the supporting documentation to
the EoI proposal provided by TML. Such resources included references to the World Health
Organisation (WHO), Social Determinants of Health Alliance documents, resources of the Tasmanian
Council of Social Services, as well as reports released by the Tasmanian State Government including
State of Health Reports and relevant strategies.
To this end, awareness and understanding was best gauged with regards to the types of evidence
that applicants referred to within their proposals to demonstrate not only their understanding of
SDoH but also their awareness of SDoH at a localised level. The types of evidence that were most
commonly drawn on in the proposals to demonstrate how applicants had become aware of SDoH in
their CoP(s) included Census and ABS Data, ABARE and NAPLAN data. These statistics were mostly
quoted and some proposals did extrapolate this data to a local level to support the case for action
around particular SDoH, but this was not generally not well articulated.
Several proposals contained details about how an understanding about SDoH was gained through
less conventional sources such as the media or from particular programs such as Bridges Out of
Poverty which reference the SDoH as an approach to addressing intergenerational poverty.
Other sources of evidence that were cited to support their knowledge and understanding of SDoH
within particular COPs included the evaluation of the Healthy Community Initiative, Kids First
reports, program specific evaluations and reports, local surveys and forums and community
assessments. However, more often than not, these reports were not specifically named or included
as a reference.
Over half of the proposals reported anecdotal observations as evidence informing their knowledge
and understanding of SDoH in their Community/(ies) of Priority. This was often from the perspective
of the lead organisation/partnering organisation as either a community based organisation or
government service provider providing programs or support to their community, and therefore
these organisations were seen as key sources of knowledge. Examples of extracts from the proposals
citing the importance of anecdotal evidence included:
We have awareness and understanding of the Social Determinants of Health obtained
through work with clients, research and evaluations we have conducted (Southern Region
proposal)
Evidence gained FROM listening to people’s actual experiences and life outcomes over time
(North West Region proposal)

27
… have learned about SDOH in our area through running a program about preventive health
and realising the link between historical trauma and the SDoH (Southern Region proposal)
We have regular and ongoing conversations with our community which inform what we need
to respond to... (Northern Region proposal)
The use of anecdotal evidence to support the proposals was often a valid approach because some
proposals acknowledged that, apart from baseline data such as ABS statistics, very little evidence in
fact existed at the local level to support their proposal. Ten proposals included an ‘evidence scoping
component’ (e.g. community health needs assessment, environmental scans or community
consultations), in which they proposed to conduct research to inform their anecdotal observations
and/or build on existing evidence about the SDoH in their targeted CoPs.
The scope of the proposed projects also varied considerably, with some proposals focusing on
addressing particular health or social issues, whilst other proposals focused on addressing one or
more SDoH. This wide variation in scope suggested that a number of the applicants had difficulty
making the distinction between a health risk factor or social issue and an SDoH. Where multiple
SDoH were being addressed, most applicants were able to clearly articulate linkages between the
targeted determinants. This was evidenced by them highlighting the interconnectedness of issues
that impact on the health and wellbeing of communities, and outlining how action towards
addressing one particular SDoH influenced the health and wellbeing of the community through
impacting on other determinants.
Adoption of place based approaches
Importantly, a number of proposals highlighted an understanding of the importance of place based
approaches in addressing the Social Determinants of Health. This was evident in proposals that
made reference to some of the guiding principles, philosophies and resources for place based
approaches.
Place based approaches are defined as approaches through which stakeholders engage in a
collaborative process to address issues as they are experienced within a geographic space, such as a
neighbourhood or community (DHHS 2012). Place based approaches have shown to be effective for
influencing the SDoH because they take into account the unique needs of the project location,
involve and engage stakeholders in decision making processes and seize opportunities, particularly
local skills and resources.
The analysis revealed a mix of approaches to addressing the Social Determinants of Health using a
place based approach. While most proposals concentrated on a single Community of Priority and
engaged with how SDoH could be addressed across that community through different activities and
outreach, some actually focused on specific geographic neighbourhoods within a CoP. For example,
a number of proposals (n=4) focused on the suburb of Ravenswood which is located within the wider
CoP of Launceston. At least two proposals concentrated on a number of CoPs (e.g. Devonport and
Burnie), while others engaged with the notion of a place based approach within a greater regional
context (e.g. the whole Cradle Coast region). Evidently, the approach to place was, in many cases,

28
directly relevant to the SDoH that were being focussed on. For example, a regional approach to
employment or a neighbourhood specific approach to food security.
The importance of adopting a place based approach was evident in proposals which highlighted the
value of tapping into the local communities’ natural and human resources to address issues at a local
level. These proposals argued for local solutions tailored to specific community needs, focusing on
where people live, work and play as being critical for addressing the underlying causes of poor
health. One proposal described the process as “picture building” or conducting an environmental
scan to provide information on the local economy such as closure of businesses, truancy levels,
closure of local services or availability of fresh fruit and vegetables. The importance of place is best
captured in the following extracts from two of the proposals:
We need to examine why individuals/communities are missing out, because they might live in
a household where no one work, they are not safe at home, they have lots of time off school,
there is no access to a computer or the internet at home, there is no one to read to them and
they cannot take part in sport or activities because there is no public transport or driving
costs too much… (Northern Region proposal)
Providing place based approaches to the underlying causes of health inequalities that
provide support and empowerment for individuals that can help them to make healthier
choices (Southern Region proposal)
Employing a place based approach at an operational level of service delivery, ten proposals
recognised the importance of service coordination being focussed on the Community of Priority in
order to address the SDoH in those localities. As such, a number of these proposals acknowledged
that, rather than developing additional programs and services, more sustained changes to address
Social Determinants of Health such as education, employment, food security etc. could be made by
services collaborating and tailoring their services to better meet collective local needs. For example,
one proposal stated:
We have experience and understanding of the importance of operating in a place based
model in order to affect change – restructuring service delivery to this place based approach
(Northern Region proposal).
A handful of proposals argued that achieving the best possible outcomes for the SDoH would involve
a balance of realigning existing programs and services together with, and through, the creation of
new place based approaches that more closely link the SDoH to health outcomes. Other proposals
considered the funding an opportunity to trial new ways of working that embraced place based
approaches to addressing the underlying causes of health inequities. In one proposal, the approach
was based on applying program models that had ‘worked’ in other regions and could be applied to a
new context. The proposed place based approaches had a strong focus on capacity building through
providing support and empowerment for individuals to enable them to make healthier choices.

29
Consideration of access and equity
Less evident in all the 59 proposals were details of how the applicants considered issues of access
and equity in both the design and implementation of proposed project activities. For example, there
was limited application or reference to the use of equity measurement tools such as health equity
impact assessment methodologies which are often applied to projects addressing the SDoH.
Issues of equity were best considered in proposals that aimed to address barriers to social change or
improve access or affordability. Consideration of issues of equity was most evident in proposals that
addressed the determinants of education, transport and food. Principles of equity were also
expressed in some proposals through the concepts of empowerment, leadership and capacity
building. The following extract from a proposal that addressed education as a SDoH provides an
example of how the concept of social equity was considered:
Social equity is addressed through the provision of health literacy education for those who
might not otherwise receive it delivered in a creative and engaging manner utilizing the
powerful medium of music and the arts, along with active engagement in a powerful
intervention that has the capacity to impact positive social change and significantly influence
population health outcomes (Southern Region proposal)
4.6 Profile of Proposals by Lead Organisation, Partnering Organisations, Sector and
Evidence of Governance and Partnerships Structures
This section reports on the findings of the analysis of the proposals with respect to the sectors from
which the organisations were drawn. It further discusses the qualitative themes that emerged from
the proposals relating to governance, partnerships and capacity to address Social Determinants of
Health.
Profile of Proposals by Lead Organisation, Sector and Partners
In total, 225 organisations were represented in the 59 submitted proposals, as either lead
organisations or partnering organisations. Only 25 per cent of these organisations (n=57) were
registered for GST.
A number of organisations and sectors (e.g. local governments or NGOs) were nominated as lead or
partnering organisations in multiple proposals within specific regions. Some state-wide organisations
were listed as lead organisations across all regions and in several CoPs.
With respect to the breakdown of proposals by sector, the analysis showed that there was a
diversity of organisations represented in the EoI proposals. Table 7 below shows a breakdown of the
lead and partnering organisations by sector.

30
Table 7: Lead organisation or partnering organisation by sector
Lead organisation Number of times listed as lead organisation
Number of times listed as partnering organisation
Not-for-profit incorporated organisations *36 108
Local Government/Councils 10 28
Community/Neighbourhood houses 6 20
Rural health services 3 8
State Government agencies (including schools) 4 37
Businesses 1 24
*Includes both not-for-profit incorporated and business organisations
As shown in Table 7, it is perhaps not surprising that the not-for-profit sector (comprising both not -
for-profit incorporated and not-for-profit business organisations) was represented in 53 per cent of
all proposals (n=119), as either lead organisation (n=35) or as a partnering organisation (n=107).
Local Government/Councils within the individual Communities of Priority were the second most
represented sector in the proposals (17%) and were nominated as both lead organisation (n=10) and
as partnering organisation (n=28).
The business sector was the least nominated sector as lead organisation, with only one EoI proposal
being led by a business organisation. Interestingly, the business sector was more heavily represented
as partnering organisation than as lead organisation; they were nominated as a partner in 24
proposals.
Whilst the spread of organisations listed in the proposals was extensive (n=225), it is important to
note that a number of organisation were listed as either lead organisation or as partnering
organisation on multiple proposals. The maximum number of proposals in which a single
organisation was listed as lead organisation was three.
With respect to organisational size, it was difficult to gauge this type of information from the
received proposals. While some proposals briefly outlined this information in their description of
their organisation or in what they proposed to bring to a nominated partnership, there were obvious
differences in the size and resources of some of the not-for-profit organisations. Additionally,
because of the place based approach to a particular community, most applicants concentrated on
their role, resourcing and size within these specific geographic areas rather than presenting a
generalised overview of their organisation at a state or national level (St Vincent de Paul was one of
the few organisations that provided this information).

31
Capacity to Deliver: Understandings and Evidence of Governance Structures, Partnerships Capacity
and Connectedness with Community
The Expression of Interest Application Form asked applicants to address two questions by providing
open qualitative comments. These were: “Describe what each organisation contributes to the
project partnership” (Criterion 2); and “How will you approach governance arrangements for the
project?” (Criterion 3).
The research literature on effective approaches to addressing the SDoH highlights the importance of
collaborative working relationships between government agencies and other relevant organisations
in delivering services and programs, acknowledging the interrelatedness of key social and economic
determinants across multiple life domains (Osborne, K, et al. 2013).
The analysis of these combined criteria across all the proposals therefore enabled the report authors
to generate themes relating to the capacity of applicants to undertake work around the SDoH, based
on the capacity and strength of their proposed partnerships and their commitment to community
connectedness. The analysis retrieved two main themes which were considered to be key measures
in assessing the capacity of the applicants to successfully undertake their proposed project activities.
These elements are:
a. Proposed governance structures, assessed in terms of the appropriateness of the
governance model in terms of representation, to achieve the aims and objectives of
the proposed activities, and the capacity of the proposed governance structure to
influence or impact on the target SDoH.
b. Level of community connectedness as evidenced by the level of input or
involvement by the target community in the governance processes. This element is
of particular importance when assessing the capacity to establish new approaches
that embrace place based approaches to underlying causes of poor health.
(a) Governance Structures
With respect to governance structures, the thematic analysis showed that the applicants had given
significant consideration to the establishment of collaborative structures and approaches. Overall,
the proposals showed that the lead organisations had made considerable efforts to involve a diverse
range of partnering organisations across multiple sectors. In one or two proposals, collaborations
were not limited to agencies or organisations operating at a regional or State level but included
interstate partners.
In over half the proposals, the composition of the partnership was informed by a history of prior
collaborative experiences. The basis of the partnerships varied between those that proposed to put
in place agreements to work together, to partnerships that entailed arrangements to share assets,
resources, staff and programs. In some cases, the partnership arrangements were supported by
formal governance structures such as the extension of Memoranda of Understanding (MOUs), and
Advisory Boards or Steering Committees. Table 8 below outlines the main types of governance
structures referenced in the proposals. The table also indicates the number of proposals that made
reference to the employment of a Project Officer and external consultants to assist with the
implementation of the project development phase.

32
Table 8: Types of governance structure and positions represented in the proposals
Governance type n (%)
Advisory board/steering committee* 45 (76.3)
Project Officer 26 (44.1)
Overseen by existing advisory board 21 (35.6)
Formal agreement (e.g. MOU, ToR, etc.) 18 (30.5)
Risk register 2 (3.4)
External Project Consultants 2 (3.4)
Governance not clearly specified 1
In three proposals, the capacity and strength of the partnerships was be achieved by implementing
specific collaborative models such as the ‘Collective Impact Model’, the ‘Thrive Tasmanian
Community Model of Health and Wellbeing’ and the ‘The Family Partnership Model’. Extracts from
some proposals which reflect stronger understandings of partnerships and governance included:
A shared vision for social change that includes common understanding of the problem and
joint approaches for solving problems through agreed actions (Northern Region proposal)
Use of family sensitive community reference groups which would also include local service
providers and families would add value (Southern Region proposal)
In the remaining proposals, the basis of the composition of the partnership appeared to be more
opportunistic, with lead organisations seeking to establish new strategic collaborations to address
the project objectives. The proposals were detailed in listing the contribution that each partner
would make to the collaboration, although there was some duplication of knowledge, skills and
expertise suggesting some of the collaborative structures could potentially be more streamlined.
There were a number of occasions where a single organisation was a partner on more than one
proposal. Whilst this was clearly acceptable within the EOI funding guidelines, there was a lack of
clarity as to how the organisation may be adequately resourced or could contribute to, or add value,
to the proposed place based approach, particularly in situations where the particular organisation
had no prior involvement or connection with the target community.
(b) Community Connectedness and Engagement
In regard to community connectedness as a measure of capacity and readiness for action, the
literature on SDoH highlights the importance of community input into defining and addressing the
impacts of the SDoH on the health and well-being of the local community, through combining better
public policy and enhanced community capacity (Harpur, S. 2011).
The importance of ensuring high levels of community connectedness was clearly articulated in the
vast majority of the proposals. Strategies for connecting with local communities included:
community health needs assessments (CHNA), forums and workshops. A number of proponents saw
this as a process of validating proposed works as well as engaging directly with communities about
SDoH and involving community members in the project governance (e.g. representation on project
groups or governing boards).

33
Additionally, over half of the proposals referred to the importance of engaging with communities,
although there was variation in the level of detail that was offered as to how this may occur. Below
are two extracts from the proposals relating to this theme:
Collaborative approaches where community is the “bread and butter” partner (Southern
Region proposal)
Importance of our strong history of building capacity and development in our local
communities (North West Region proposal)
With regard to achieving community connectedness and engagement, detail was less evident on
how this was to be strategically achieved. The proposals that did not highlight strategies to engage
local communities argued that strong connections with the community already existed and that
structures were in place that organisations could utilise to further connect to the community. Key
differences existed between proposals as to when engagement with the community should occur,
with some applicants indicating that the project team would seek community input in the planning
phase, whilst other applicants proposed an “as and when required” approach to engagement.
4.7 Proposal Outcomes and Sustainability Issues
A major aim of the EoI process was to generate initiatives that reflect the communities’ commitment
to focus on and address the SDoH at the local level. This could be achieved through supporting the
establishment or delivery of services and resources that would make a longer term difference to the
health and wellbeing of the target community. Whilst acknowledging changes to the health and
wellbeing of a target community may not be easily measured or attributed to a single intervention
such as the implementation of a proposed SDoH project, it is important to consider how the
proposed outcomes of the project could be sustained. The Expression of Interest process asked
applicants to describe what short and long term outcomes the initiative hoped to achieve. The
analysis of these answers was informed by the overarching interpretive theme of sustainability.
Based on the analysis, the report authors define sustainability as the ability or capacity of the
proposed initiative and respective outcomes to be sustained over an infinite period.
The concept of sustainability was addressed to varying degrees as part of the applicant’s response to
the question relating to the potential short and longer term outcomes that the initiative hoped to
achieve. Whilst virtually all the proposals provided a degree of clarity around what the proponents
perceived to be the short and longer term outcomes from the proposed initiatives, the proposals
were less clear on what strategies would be employed to ensure the sustainability of proposed
outcomes. This criteria was the weakest component of all the proposals, with many applicants
struggling to look at outcomes in a systematic way, largely because (as some noted in their
proposals) it was difficult to measure.
It was apparent that a number of the applicants had not considered the issue of sustainability when
providing information on the longer term outcomes. This may have been partly due to the fact that
the EoI guidelines did not specifically request information on how the initiatives and their respective
outcomes could be sustained. The absence of any direct reference to sustainability was picked up in

34
one proposal, with the proponent proposing that evidence of sustainability should be made a key
determinant as to whether funding for a specific proposal should proceed.
Although not always explicit, the theme of sustainability was implicit in a number of the proposals.
Four key themes and strategies relating to sustainability emerged from the responses to the
question relating to the short and long term outcomes. The four key sustainability strategies were:
(1) integration of proposed activities into existing programs/services; (2) restructuring existing
services/programs with a focus on enhancing sustainability through training initiatives; (3)
embedding sustainability in the design of new programs/services instigated by the proposed
initiative; and (4) supporting the creation of specific employment sectors such as the establishment
of social enterprises.
(1) Integration of proposed activities into existing programs/services
A common theme within approximately half of the 59 proposals was application of “value adding”,
based around designing the proposed initiative as a platform to build on to, or leverage off, existing
services and programs delivered by the applicants in the target community. The assumption was
that the existing programs and services were already wholly or partially addressing the aims and
objectives of the SDoH project, and with additional resources delivered through the SDoH project,
the outputs could be further enhanced. It was also claimed that this approach would have the added
benefit of making better use of existing community structures and networks associated with the
existing services and programs.
(2) Restructuring existing services/programs
The second most common strategy to build sustainability was restructuring or remodelling existing
services and programs through incorporating elements of cultural and social change, leading
towards more sustainable outcomes from the proposed activities. Advocates for this approach saw it
as an opportunity to build principles of resilience into the project through the delivery of educational
and training opportunities. The following extract from one of the proposals illustrates this point:
Work towards putting a longer term vision in place as to what the project will achieve. Focus
on the bigger picture and changing the culture and perspective of some parts of our
community through education, achievement and aspiration (North West Region proposal)
This type of strategy, based on restructuring existing services and approaches within a CoP, was
particularly common in proposals that addressed food access as a Social Determinant of Health.
These proposals acknowledged the plethora of community based food initiatives that are currently
operating but saw the project as an opportunity to rethink how these initiatives operate, with a view
to taking a more sustainable approach to the programs, as highlighted in the following statements:
Focus on creating a model of sustainable food systems that benefit economic, social and
environmental needs of the community (North West Region proposal)
Change the way the current systems work in local food supply (towards a more sustainable
model) (Southern Region proposal)

35
Building a level of flexibility into existing projects through creating space to accommodate emerging
needs was also seen as a potential route to improved sustainability.
(3) Embedding sustainability in the design of new programs/services
A number of proposals focused on the opportunity presented by the SDoH Project to design new
programs and services within which strategies for sustainability would be embedded. These
proposals referenced a number of strategies linked to the proposed initiatives that the applicants
believed delivered a degree of sustainability. Examples of these strategies included: the creation of
programs with a strong outreach focus, design of initiatives that incorporated employment
pathways for the target community through adoption of accredited skills and training courses
leading to the attainment of qualifications, designing activities in such a way that they can be
replicated in communities outside the target community, and exploring ways different sectors can
be directly involved in the initiative, such as long term sponsorship from the business sector.
The point of difference for sustainability strategies related to the timing of the intervention, with
some applicants suggesting that they be built into the planning and implementation phase, whilst
other applicants suggested that strategies for sustainability should be considered once the key
proposed project activities have been implemented and proven to be successful.
(4) Creation of specific employment initiatives
Whilst the creation of employment initiatives through skills development or training programs
reflects both an outcome and a strategy for sustainability, it has been included as a key marker of
sustainability as it was referred to as a sustainability strategy in a significant number of proposals.
Of particular note are references to the creation of specific employment opportunities through the
establishment of social enterprises. Social enterprises were seen as a vehicle for ensuring
sustainability of the proposed project outcomes. Social enterprise provides opportunities for
innovation, employment, skills development and income generation, all of which are key elements
of a sustainable strategy. This point is reflected in the following extract from one of the proposals:
…social enterprise to help sustain the project into the future and provide real life skills in
business… (Southern Region proposal)
Whilst most proposals focused on employment opportunities, the creation of social enterprise
encompasses not only employment opportunities but also contributes to the social capital of the
local community, a key contributor to sustainable communities.
Establish a Community Strategic Action Plan and activity work plan to ensure that all the
activities met the identified SDoH (Southern Region proposal)
Partner organisations that provide a road map for working in and with local communities to
achieve change, this is known as the ‘platform model’ which involves 6 stages: raising
awareness, harnessing support, establishing partnerships, learning, developing an outcome
based plan, implementation and review (Southern Region proposal)

36
5. CONCLUSION
__________________________________________________________________________________
The Social Determinants of Health Project was shaped by a comprehensive process that included
considerable community and stakeholder consultation and review of SDoH programs and policy. The
inclusion of the EoI process was an outcome of this consultation and was aimed at identifying locally
place based projects that: (1) addressed and/or had the potential to impact on one or more of the
Social Determinants of Health; and (2) involved a partnership of three or more organisations based
in, providing an outreach service to or wishing to establish a service in a Community of Priority.
The Expression of Interest process resulted in 59 proposals from all 18 Communities of Priority in
Tasmania. This report has provided a thematic overview of these proposals.
The analysis revealed that the EoI process achieved considerable organisational reach, with a total of
225 organisations listed as either lead organisation and/or partnering organisation in the proposals.
Importantly, these organisations were drawn from a broad cross section of industries and sectors
across Tasmania and interstate, with interests in a range of Social Determinants of Health.
The assistance provided to potential applicants by the TML, such as the regional forums and the EoI
proposal support documentation provided to applicants, was clearly valuable in helping applicants
complete the EoI process. This was evidenced by the number of occasions that one or both of the
support processes was referenced by the applicants as a key source of information about the SDoH
project. Whilst this process may have provided valuable information about the SDoH, it may have
also shaped the different determinants and range of determinants that were selected by applicants.
It is worth noting that four of the top five determinants selected by applicants were listed as
examples of SDoH in the EoI Guidelines document provided to applicants. It is recommended that in
future SDoH proposal processes, support documentation may not need to be quite so detailed in
terms of identifying specific determinants that applicants may wish to consider addressing in their
proposals, or alternatively a greater justification for those choices could be detailed.
The Application Form asks the applicant to indicate how they became aware of the issues around the
SDoH. The responses overwhelmingly identified the variety of sources from which information about
SDoH was accessed. As this information, in most cases, was not contextualised in the proposals it
was difficult to ascertain whether the applicants had a firm understanding of the SDoH. This was
evidenced by some applicants confusing a social issue e.g. bullying, obesity or child abuse, with the
SDoH. The EOI process may have benefitted from the inclusion of a criterion that provided an
opportunity for the applicants to better articulate their understanding of the SDoH.
The concept of local place based approaches was generally well understood, with a majority of
proposals articulating strategies that would support a place based approach. Some of these
strategies included proposing approaches that: reflected the unique needs of the target location,
embedding processes to engage local stakeholders in decision making, drawing together assets and
knowledge through shared ownership, and aiming to change behaviours or norms in a specific
location.

37
The notion of inter-sectoral collaboration and representative governance structures was addressed
well in the proposals. There was evidence that there had been considerable effort by the lead
organisations to involve a diverse range of partnering organisations across multiple sectors. In over
half the proposals, the composition of the partnership was informed by prior collaborative
experiences. In the remaining proposals, the basis of the partnership appeared to be more
opportunistic, with lead organisations seeking to establish new strategic collaborations to address
the proposal’s objectives. However, it was unclear in some proposals as to what each partner would
contribute to the collaborations.
The issue of short and longer term impacts and sustainability of outcomes was the least well-
articulated of the EoI proposal criteria. A number of proposals referred to a third party that would
take responsibility for ensuring that the longer term impacts of the proposal would be realised
without providing clear evidence as to how this may work. Information on how applicants could
measure whether the proposed short or longer impacts had been achieved was scant, suggesting
that many of the proposed longer term impacts were visionary statements rather than statements of
impact. Evidence on how the impacts would be sustained was also not apparent, aside from some
innovative approaches such as the establishment of accredited courses, career pathways or the
development of social enterprises. It is recommended that the criterion relating to short and long
term outcomes include reference to sustainability and in particular how the proposed project
outcomes could be sustained beyond the funding life of the project.
The issue of using an ‘equity lens’ to develop and implement activities to identify priority areas and
achieve fairness in the distribution of resources was not well addressed in any of the proposals. As
ensuring equity is an accepted principle in addressing the SDoH, the report authors recommend that
a criterion be included which relates to achieving equity in the distribution of resources and sharing
of the benefits of project outcomes.
This report has provided further analysis and information regarding the scope and content of all the
proposals received by TML. The report authors recommend that the funding body extend key
findings from this report to all EoI applicants by conducting workshops in each region, which would
give applicants an opportunity to have the findings of the thematic analysis presented. The authors
also suggest that there could be some minor refinements or amendments to the EoI Application
Form which may assist in future processes of this kind.
In conclusion, valuable learnings can be drawn from both the EoI process and the content of the
proposals, which could inform future EoI processes. Despite the identified limitations, the EoI
process proved to be an effective approach for drawing together Communities of Priority to develop
innovative initiatives which take a place based approach to addressing the SDoH.

38
References
__________________________________________________________________________________
Department of Health and Human Services (2012). Place Based Approaches to Health and Wellbeing
Issues Paper. DHHS. Tasmania
Harpur, S. 2011. A Healthy Tasmania: Setting New Directions for Health and Wellbeing. Action on
Social Determinants of Health: Case Studies from Australia. La Trobe University pp35 -46.
Liamputtong and Ezzy (2005) Qualitative Research Methods: Oxford University Press. South
Melbourne.
Osborne, K,. Baum, F,. Brown, L, (2013). Issues Paper no. 7 produced for the Closing the Gap
Clearinghouse
Tasmania Medicare Local (2013). Guidelines Expression of Interest Social Determinant of Health
Proposal. TML
WHO Commission on Social Determinants of Health (2007). Achieving health equity: From root
causes to fair outcomes. Geneva. WHO
WHO Commission on Social Determinants of Health. Social Determinants of Health - The Solid Facts.
Geneva. WHO, http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf

39
Appendices
__________________________________________________________________________________
T
Tasmania Medicare Local Limited ABN 47 082 572 629
Application Form
Expression of Interest
Social Determinants of Health
Proposal

40
Social Determinants of Health Proposal EXPRESSION OF INTEREST APPLICATION FORM
APPLICATIONS CLOSE: 5pm Monday 31 March 2014
EMAIL in Word or PDF format to: [email protected]
OR POST TO: Tasmania Medicare Local
PO Box 358 Ulverstone, Tasmania 7315
Background Tasmania Medicare Local (TML) is seeking Expressions of Interest (EOI) for proposals from
eligible communities and organisations for the Social Determinants of Health (SDoH)
Strategy.
The SDoH Strategy has been funded through the Australian Government Department of
Health to assist communities in Tasmania to improve the health status of residents by
reducing inequalities in health impacted by social determinants. These are generally
described as the conditions in which people are born, grow, live, work and age, including the
health system.
Funding will be made available to eligible communities to address social determinants of
health. These may include:
Social status
Health literacy
Housing
Education and employment
Transport and
Food security as well as
Other significant social determinants.
Eligible communities
The SDoH Strategy has identified 18 Tasmanian local government geographic areas as Communities of Priority using a range of ABS data and consultation which highlighted:
Socio economic status
Remoteness
Capacity to implement sustainable solutions. Communities include:

41
Northern region – Break O’Day, Dorset, George Town, Glamorgan/Spring Bay,
Launceston
North west region – Burnie, Devonport, Kentish, Waratah/Wynyard, West Coast
Southern region – Brighton, Central Highlands, Derwent Valley, Glenorchy, Huon
Valley, Sorell, Southern Midlands, Tasman.
TML encourages joint applications from smaller/ neighbouring communities in different local
government area.
Information on the selection of Communities of Priority can be found in the Social
Determinants of Health Proposal information pack on the TML website:
www.tasmedicarelocal.com.au
Eligible partners
Proposals from Communities of Priority must be in partnership and should include at least
three partners. Partners may:
Be based in a Community of Priority
Provide (an outreach) service to a Community of Priority
Wish to establish a service in a Community of Priority.
At least one of the partners should be based in the Community of Priority where the project
will be implemented. A not-for-profit or company organisation must be the fund-holder.
Eligible partners include:
Not-for-profit incorporated organisations
Not-for-profit company organisations
Local councils
Community/neighbourhood houses
Rural health services
State government agencies including schools and
Businesses.
TML encourages proposals from partnerships that include community groups.
More information on eligible partners can be found in the Expressions of Interest: Social
Determinants of Health Proposal information pack which can be found on the TML website:
www.tasmedicarelocal.com.au
Proposals
Proposals that have the potential to impact on social determinants of health will be
considered for Project Development funding. Proposals might be directed for example
towards:
Making housing affordable, safe and secure
Skilling and supporting people into work
Engaging with education and sustaining lifelong learning
Creating optimal early childhood development conditions

42
Increasing transport options for vulnerable populations
Making nutritious food accessible and affordable
Reducing the impact of poverty.
Key considerations
Proposals may build on an existing program or service or be directed towards a new
initiative that is:
Place-based
Addresses a community’s(ies’) prioritised needs
Achievable, targeted and timely
Able to build community capacity and
Able to support change beyond the life of the project funding period.
Proposals should also take into consideration:
Improving health equity and social outcomes
Demonstrating innovation and collaboration
Reducing inefficiency and fragmentation
Strengthening outreach and access
Providing effective governance
Providing resources in-kind.
More information on the SDoH Strategy, social determinants of health resources and
Communities of Priority can be found in the Social Determinants of Health Proposal
information pack on the TML website: www.tasmedicarelocal.com.au
Interested communities are encouraged to discuss their proposals with a TML Social
Determinants of Health Coordinator prior to submitting proposals.
Funding available
Phase 1 Project Development: $50,000
Funding will be provided to successful applicants who have submitted an Expression of
Interest – Social Determinants of Health Proposal application form. This funding is to
progress proposals to Project Development stage which includes the development of a
detailed project plan.
Funding of $50,000 may be used towards administration and operating costs and may
include (for example):
Salaries
Office expenses
Community consultation
Needs assessments or research
Consultancy fees

43
Transport/accommodation and
Other associated costs.
Project Development plans must be completed for assessment by TML by the end of August
2014. TML SDoH Coordinators will be available to provide Project Development information
and support.
Phase 2 Project Implementation: Up to $300,000
Funding up to $300,000 will be made available to successful applicants who have submitted
a Project Development plan. This funding will be for Project Implementation and will be
proportional to the activities outlined in the project plan. Project implementation will be from 1
November 2014 to 30 April 2016.
Capital works projects are not eligible for funding.
Information Briefing Sessions Pre-proposal information briefing sessions will be held around the state to assist interested
organisations understand the Expression of Interest process and decide whether they wish
to submit a proposal. Tasmania Medicare Local Social Determinants of Health Coordinators
will be available to provide information and answer questions.
To register for an information session please phone 6425 0800 or email [email protected]
Briefing Session Dates and Locations Hobart: Thursday 13 February 2014 Launceston: Monday 17 February 2014 Burnie: Tuesday 18 February 2014 Bicheno: Thursday 20 February 2014
Assessment process
As part of the assessment process, all applicants (representatives of partnering
organisations) will be invited to meet with representatives of TML’s Social Determinants of
Health Strategy assessment panel to discuss their proposal. Meetings will be held in regional
locations in the week beginning 7 April 2014 and all applicants will be notified dates, times
and locations.
Assessments of EOIs will be conducted in April and applicants will be notified by 30 April
2014.

44
Submitting Expressions of Interest
The Expression of Interest: Social Determinants of Health Proposal application form must be
completed and emailed as an attachment in either MS Word or PDF format to:
All applications will be acknowledged in writing after the closing date.

45
Part 2
Social Determinants of Health Proposal EXPRESSION OF INTEREST APPLICATION FORM
Applications must be received by 5pm on Monday 31 March 2014. Please submit the completed application form by email to: [email protected] or post to: Tasmania Medicare Local PO Box 358 Ulverstone, Tasmania 7315 Your answers should not necessarily be limited to the size of the text boxes below. However, please keep responses to the minimum necessary to provide sufficient detail in the response.
APPLICANT DETAILS
REGION NORTH NORTH-WEST SOUTH
COMMUNITY(IES) OF PRIORITY
(Local Government Geographic Area)
PARTNERING
ORGANISATIONS
(Minimum of 3)
NAME OF INCORPORATED BODY WHERE FUNDS WILL BE LODGED
ABN REGISTERED FOR GST
AUTHORISED OFFICERTO SIGN LETTER OF OFFER/GRANT DEED
NAME
POSITION
ADDRESS POSTCODE
EMAIL PHONE

46
KEY CONTACT FOR PARTNERING ORGANISATION 1:
NAME
POSITION
ADDRESS POSTCODE
EMAIL PHONE
KEY CONTACT FOR PARTNERING ORGANISATION 2:
NAME
POSITION
ADDRESS POSTCODE
EMAIL PHONE
KEY CONTACT FOR PARTNERING ORGANISATION 3:
NAME
POSITION
ADDRESS POSTCODE
EMAIL PHONE
KEY CONTACT FOR ADDITIONAL PARTNERS/ORGANISATIONS:
NAME
POSITION
ADDRESS POSTCODE
EMAIL PHONE

47
GENERAL INFORMATION
For general information to assist you to complete the application please refer to the
Expressions of Interest: Social Determinants of Health Proposal information pack.
The information pack can be found at www.tasmedicarelocal.com.au
It is strongly recommended that applicants contact a Tasmania Medicare Local Social
Determinants of Health (SDoH) Coordinator prior to lodging an Expression of Interest.
Information sessions for eligible communities will be held across the state in February 2014:
(see page 4 of this document for details).
Community Contact
Break O’Day, Dorset, George Town,
Glamorgan/Spring Bay, Launceston,
Glenorchy, Huon Valley, Sorell,
Tasman
Wendy French
t: 6331 9296
Burnie, Devonport, Kentish,
Waratah/Wynyard, West Coast,
Central Highlands, Derwent Valley,
Southern Midlands, Brighton
Nicki Fletcher
t: 6425 0800
Please note: Suggestions in italics are included only as a guide to addressing criterion.
Answers must be limited to the boxes provided.
DESCRIPTION
Please provide a broad outline of your proposal
(Refer to your community(ies)areas of concern around social determinants of health)
SELECTION CRITERIA

48
Criterion 1
How have you become aware of the issues around social determinants
of health mentioned in your proposal?
(Refer to any previous community consultation, observations, reports,
projects, data, needs analyses)
Criterion 2
Describe what each organisation contributes to the project partnership.
(Experience in and across sectors, connections to community, expertise in
targeted area)
Criterion 3
How will you approach governance arrangements for the project?
(Refer to developing a governance structure, advisory groups, project
leadership, management, communication)
.
Criterion 4
How will you approach the planning and development of the initiative?
(Refer to engaging stakeholders, identifying community priorities, developing a
common agenda, identifying programs and services)
Criterion 5
What short- and long-term outcomes does the initiative hope to
achieve?
(Refer to community priorities for social determinants of health, improving
access and equity, improving service delivery)
Please add any other relevant information about your community, partners or
proposal
(Optional)
.

49
Checklist Applicants have:
Read the Social Determinants of Health Proposal information pack
Attended a pre-proposal Information Session
Spoken with a Social Determinants of Health Coordinator
Completed Applicant Details
Addressed the Criterion
Retained pages 1 to 4 for future reference
Saved pages 5 to 11 as an MS Word document or PDF
APPLICATIONS CLOSE: 5pm Monday 31 March 2014
EMAIL in Word or PDF format to: [email protected]
OR POST TO: Tasmania Medicare Local
PO Box 358 Ulverstone, Tasmania 7315