the under-five mortality rate: the indispensable gauge of - unicef
TRANSCRIPT
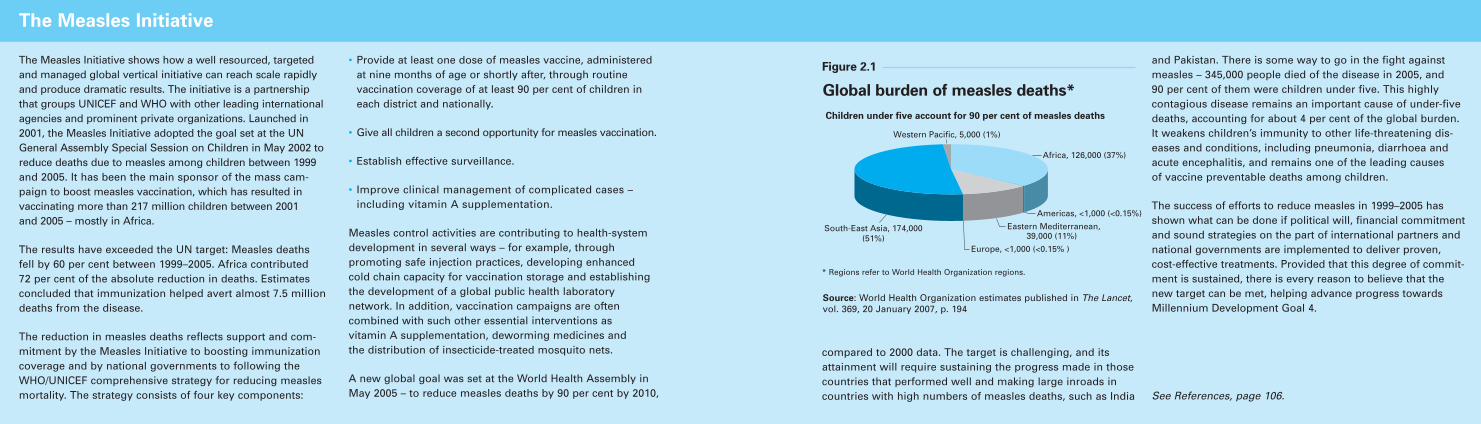
The report begins by examining thestate of child survival and primaryhealth care for children, with astrong emphasis on trends in childmortality. It then appraises the les-sons from failures and successes inchild survival over the past century.The centrepiece of the report looks atseveral of the most promisingapproaches – community partnerships,the continuum of care framework andhealth-system strengthening for out-comes – to reach those mothers, new-borns and children who are currentlyexcluded from essential interventions.By highlighting examples from coun-tries and districts where these havebeen successful, as well as exploringthe main challenges to their expan-sion, this report offers practical waysto jump-start progress.
Why child survival matters
Investing in the health of young children makes sense for a number
of reasons beyond the pain and suffering caused by even one child’sdeath. Depriving infants and youngchildren of basic health care anddenying them the nutrients neededfor growth and development setsthem up to fail in life. But when chil-dren are well nourished and cared forand provided with a safe and stimu-lating environment, they are morelikely to survive, to have less diseaseand fewer illnesses, and to fullydevelop thinking, language, emotion-al and social skills. When they enterschool, they are more likely to suc-ceed. And later in life, they have agreater chance of becoming creativeand productive members of society.
Investing in children is also wise froman economic perspective. Accordingto the World Bank, immunizationand vitamin A supplementation aretwo of the most cost-effective publichealth interventions available today.
Improving vitamin A status canstrengthen a child’s resistance to disease and decrease the likelihoodof childhood mortality.2 For only asmall sum, a child can be protectedfrom vitamin A deficiency and anumber of deadly diseases, includingdiphtheria, pertussis, tetanus, polio,measles, childhood tuberculosis, hepatitis B and Hib (Haemophilusinfluenzae type b), which is a majorcause of pneumonia and meningitis.3
Providing cotrimoxazole, a low-costantibiotic, to HIV-positive childrendramatically reduces mortality fromopportunistic infections.
Improvements in child health and sur-vival can also foster more balancedpopulation dynamics. When parentsare convinced that their children willsurvive, they are more likely to havefewer children and provide better careto those they do have – and countriescan invest more in each child.4
C H I L D S U R V I VA L : W H E R E W E S T A N D 3
walks of life – from religious leaders toGoodwill Ambassadors, from mayorsto Heads of State, from sports person-alities to parliamentarians, from pro-fessional associations to trade unions –to join the child survival and develop-ment movement.
Far from ploughing a lone furrow as it often did in the 1980s, UNICEFtoday is championing child survival aspart of a large community of concern.The partnerships that have developedduring the past two decades are prov-ing vital in tackling problems thatdemand more complex systemic andsociocultural changes than the earlyarchitects of the child survival revolu-tion realized. The State of the World’sChildren 2008 outlines the resultsborn from these partnerships, as wellas from the experiences and approach-es to child survival and health ofrecent decades.
2 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The under-five mortality rate, often known by itsacronym U5MR or simply as the child mortality rate,indicates the probability of dying between birth andexactly five years of age, expressed per 1,000 livebirths, if subject to current mortality rates. It has sever-al advantages as a barometer of child well-being ingeneral and child health in particular.
First, it measures an ‘outcome’ of the developmentprocess rather than an ‘input’, such as per capita calorie availability or the number of doctors per 1,000 population – all of which are means to an end.
Second, the U5MR is known to be the result of a wide variety of inputs: the nutritional status and the healthknowledge of mothers; the level of immunization andoral rehydration therapy; the availability of maternaland child health services (including prenatal care);income and food availability in the family; the avail-ability of safe drinking water and basic sanitation; and
the overall safety of the child’s environment, amongother factors.
Third, the U5MR is less susceptible to the fallacy of theaverage than, for example, per capita gross nationalincome (GNI per capita). This is because the naturalscale does not allow the children of the rich to be1,000 times as likely to survive, even if the human-made scale does permit them to have 1,000 times asmuch income. In other words, it is much more difficultfor a wealthy minority to affect a nation’s U5MR, and ittherefore presents a more accurate, if far from perfect,picture of the health status of the majority of children(and of society as a whole).
See References, page 104.
The under-five mortality rate: The indispensable gauge of child health
0.4
1.5
1.0
1.7
2.8
5.4
5.4
0.1
0.0 1.0 2.0 3.0 4.0 5.0 6.0
0.9
1.0
1.9
2.8
4.3
4.3
East Asia and Pacific
South Asia
Eastern and Southern Africa
West and Central Africa
Sub-Saharan Africa
Developing countries
World
Millions of under-fives
Millions of additionalchild deaths in 2015 if MDG 4 is notreached*
Millions of child livessaved in 2015 relative to 2006 if MDG 4 is reached**
The benefits of meeting Millennium Development Goal 4 –
and the cost of failing to reach the goal
* Number of additional deaths among children under age five that will occur in the year 2015 if current annual rates of reduction in the under-five mortality rate persist.
** Number of deaths among children under five that will be averted in the year 2015 alone, compared with the number of deaths in 2006, by reaching the MDG 4 target of a two-thirds reduction in the under-five mortality rate observed in 1990.
Source: UNICEF estimates based on data in Statistical Tables 1 and 10, pp. 114 and 150 of this report.
Figure 1.1
Maternal, newborn and under-five deaths and undernutritionhave a number of common structural and underlying causes,including:
• Poorly resourced, unresponsive and culturally inappropriate health and nutrition services.
• Food insecurity.
• Inadequate feeding practices.
• Lack of hygiene and access to safe water or adequate sanitation.
• Female illiteracy.
• Early pregnancy.
• Discrimination and exclusion of mothers and childrenfrom access to essential health and nutrition services andcommodities due to poverty and geographic or politicalmarginalization.
These factors result in millions of unnecessary deaths each year. Their wide-ranging nature and interrelatednessrequire them to be addressed at different levels – community, household, service provider, government and international – in an integrated manner to maximizeeffectiveness and reach.
The solutions to these impediments are well known, particularly those relating to the direct causes of maternal,neonatal and child deaths. The necessary interventionsinvolve the provision of packages of essential primary-health-care services for children across a continuum of carethat spans pregnancy, childbirth and after delivery, leadingto care for children in the crucial early years of life (seePanel, page 17, for a full definition of the continuum of care).
See References, page 104.
Underlying and structural causes of maternal and child mortality
The report begins by examining thestate of child survival and primaryhealth care for children, with astrong emphasis on trends in childmortality. It then appraises the les-sons from failures and successes inchild survival over the past century.The centrepiece of the report looks atseveral of the most promisingapproaches – community partnerships,the continuum of care framework andhealth-system strengthening for out-comes – to reach those mothers, new-borns and children who are currentlyexcluded from essential interventions.By highlighting examples from coun-tries and districts where these havebeen successful, as well as exploringthe main challenges to their expan-sion, this report offers practical waysto jump-start progress.
Why child survival matters
Investing in the health of young children makes sense for a number
of reasons beyond the pain and suffering caused by even one child’sdeath. Depriving infants and youngchildren of basic health care anddenying them the nutrients neededfor growth and development setsthem up to fail in life. But when chil-dren are well nourished and cared forand provided with a safe and stimu-lating environment, they are morelikely to survive, to have less diseaseand fewer illnesses, and to fullydevelop thinking, language, emotion-al and social skills. When they enterschool, they are more likely to suc-ceed. And later in life, they have agreater chance of becoming creativeand productive members of society.
Investing in children is also wise froman economic perspective. Accordingto the World Bank, immunizationand vitamin A supplementation aretwo of the most cost-effective publichealth interventions available today.
Improving vitamin A status canstrengthen a child’s resistance to disease and decrease the likelihoodof childhood mortality.2 For only asmall sum, a child can be protectedfrom vitamin A deficiency and anumber of deadly diseases, includingdiphtheria, pertussis, tetanus, polio,measles, childhood tuberculosis, hepatitis B and Hib (Haemophilusinfluenzae type b), which is a majorcause of pneumonia and meningitis.3
Providing cotrimoxazole, a low-costantibiotic, to HIV-positive childrendramatically reduces mortality fromopportunistic infections.
Improvements in child health and sur-vival can also foster more balancedpopulation dynamics. When parentsare convinced that their children willsurvive, they are more likely to havefewer children and provide better careto those they do have – and countriescan invest more in each child.4
C H I L D S U R V I VA L : W H E R E W E S T A N D 3
walks of life – from religious leaders toGoodwill Ambassadors, from mayorsto Heads of State, from sports person-alities to parliamentarians, from pro-fessional associations to trade unions –to join the child survival and develop-ment movement.
Far from ploughing a lone furrow as it often did in the 1980s, UNICEFtoday is championing child survival aspart of a large community of concern.The partnerships that have developedduring the past two decades are prov-ing vital in tackling problems thatdemand more complex systemic andsociocultural changes than the earlyarchitects of the child survival revolu-tion realized. The State of the World’sChildren 2008 outlines the resultsborn from these partnerships, as wellas from the experiences and approach-es to child survival and health ofrecent decades.
2 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The under-five mortality rate, often known by itsacronym U5MR or simply as the child mortality rate,indicates the probability of dying between birth andexactly five years of age, expressed per 1,000 livebirths, if subject to current mortality rates. It has sever-al advantages as a barometer of child well-being ingeneral and child health in particular.
First, it measures an ‘outcome’ of the developmentprocess rather than an ‘input’, such as per capita calorie availability or the number of doctors per 1,000 population – all of which are means to an end.
Second, the U5MR is known to be the result of a wide variety of inputs: the nutritional status and the healthknowledge of mothers; the level of immunization andoral rehydration therapy; the availability of maternaland child health services (including prenatal care);income and food availability in the family; the avail-ability of safe drinking water and basic sanitation; and
the overall safety of the child’s environment, amongother factors.
Third, the U5MR is less susceptible to the fallacy of theaverage than, for example, per capita gross nationalincome (GNI per capita). This is because the naturalscale does not allow the children of the rich to be1,000 times as likely to survive, even if the human-made scale does permit them to have 1,000 times asmuch income. In other words, it is much more difficultfor a wealthy minority to affect a nation’s U5MR, and ittherefore presents a more accurate, if far from perfect,picture of the health status of the majority of children(and of society as a whole).
See References, page 104.
The under-five mortality rate: The indispensable gauge of child health
0.4
1.5
1.0
1.7
2.8
5.4
5.4
0.1
0.0 1.0 2.0 3.0 4.0 5.0 6.0
0.9
1.0
1.9
2.8
4.3
4.3
East Asia and Pacific
South Asia
Eastern and Southern Africa
West and Central Africa
Sub-Saharan Africa
Developing countries
World
Millions of under-fives
Millions of additionalchild deaths in 2015 if MDG 4 is notreached*
Millions of child livessaved in 2015 relative to 2006 if MDG 4 is reached**
The benefits of meeting Millennium Development Goal 4 –
and the cost of failing to reach the goal
* Number of additional deaths among children under age five that will occur in the year 2015 if current annual rates of reduction in the under-five mortality rate persist.
** Number of deaths among children under five that will be averted in the year 2015 alone, compared with the number of deaths in 2006, by reaching the MDG 4 target of a two-thirds reduction in the under-five mortality rate observed in 1990.
Source: UNICEF estimates based on data in Statistical Tables 1 and 10, pp. 114 and 150 of this report.
Figure 1.1
Maternal, newborn and under-five deaths and undernutritionhave a number of common structural and underlying causes,including:
• Poorly resourced, unresponsive and culturally inappropriate health and nutrition services.
• Food insecurity.
• Inadequate feeding practices.
• Lack of hygiene and access to safe water or adequate sanitation.
• Female illiteracy.
• Early pregnancy.
• Discrimination and exclusion of mothers and childrenfrom access to essential health and nutrition services andcommodities due to poverty and geographic or politicalmarginalization.
These factors result in millions of unnecessary deaths each year. Their wide-ranging nature and interrelatednessrequire them to be addressed at different levels – community, household, service provider, government and international – in an integrated manner to maximizeeffectiveness and reach.
The solutions to these impediments are well known, particularly those relating to the direct causes of maternal,neonatal and child deaths. The necessary interventionsinvolve the provision of packages of essential primary-health-care services for children across a continuum of carethat spans pregnancy, childbirth and after delivery, leadingto care for children in the crucial early years of life (seePanel, page 17, for a full definition of the continuum of care).
See References, page 104.
Underlying and structural causes of maternal and child mortality
C H I L D S U R V I VA L : W H E R E W E S T A N D 54 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Until the mid to late 1990s, estimates of the number of childdeaths occurring during the neonatal period (the first monthof life) were drawn from rough historical data rather thanfrom specific surveys. More rigorous estimates for newborndeaths emerged in 1995 and 2000, as data from reliablehousehold surveys became available. Analysis of these data made it evident that previous estimates had seriouslyunderstated the scale of the problem. Although the globalneonatal mortality rate has decreased slightly since 1980,neonatal deaths have become proportionally much moresignificant because the reduction of neonatal mortality hasbeen slower than that of under-five mortality: Between 1980and 2000, deaths in the first month of life declined by aquarter, while deaths between one month and five yearsdeclined by a third.
The latest evidence is that 4 million babies die each year intheir first month of life, and up to half of these die in theirfirst 24 hours – a child is about 500 times more likely to die in the first day of life than at one month of age. Neonatal
mortality accounts for almost 40 per cent of all under-fivedeaths and for nearly 60 per cent of infant (under-one)deaths. The largest absolute number of newborn deathsoccurs in South Asia – India contributes a quarter of theworld total – but the highest national rates of neonatal mor-tality occur in sub-Saharan Africa. A common factor in thesedeaths is the health of the mother – each year more than500,000 women die in childbirth or from complications duringpregnancy, and babies whose mothers have died duringchildbirth have a much greater chance of dying in their firstyear than those whose mothers remain alive.
Even these figures understate the vast scale of the problemsthat affect child health during the neonatal period. For exam-ple, more than a million children who survive birth asphyxiaeach year go on to suffer such problems as cerebral palsy,learning difficulties and other disabilities. For every newbornbaby who dies, another 20 suffer birth injury, complicationsarising from preterm birth or other neonatal conditions.
Significant improvements in the early neonatal period willdepend on essential interventions for mothers and babiesbefore, during and immediately after birth. According to thelatest estimates for 2000–2006, at present in the developingworld, one quarter of pregnant women do not receive evena single visit from skilled health personnel (doctor, nurse,midwife); only 59 per cent of births take place with theassistance of a skilled attendant; and just over half takeplace in a health facility.
Averting neonatal deaths is pivotal to reducing child mortali-ty. The Lancet Neonatal Survival Series, published in 2005,estimated that 3 million of the 4 million deaths could be pre-vented each year if high coverage (90 per cent) is achievedfor a package of proven, cost-effective interventions that aredelivered through outreach, families and communities, andfacility-based clinical care across a continuum of neonatalcare (antenatal, intrapartum and postpartum). While increas-ing skilled care is essential, the Neonatal Survival Seriesunderlines the importance of interim solutions that can savealmost 40 per cent of newborn lives in community settings.Expanding programmes that prevent mother-to-child trans-mission of HIV is also crucial.
Actions required to save newborns include setting evidence-based, results-oriented plans at the national level with spe-cific strategies to reach the poorest, greater funding, agreedtargets for neonatal mortality reduction, and promotion ofgreater harmonization and accountability on the part ofstakeholders at the international level.
See References, page 104.
Newborn survival
44
40
48
26
44
20
15
18
4
Sub-Saharan Africa
Eastern and Southern Africa
West and Central Africa
Middle East and North Africa
South Asia
East Asia and Pacific
Latin America and Caribbean
CEE/CIS
Industrialized countries
Neonatal deaths per 1,000 live births0 10 20 30 40 50 60
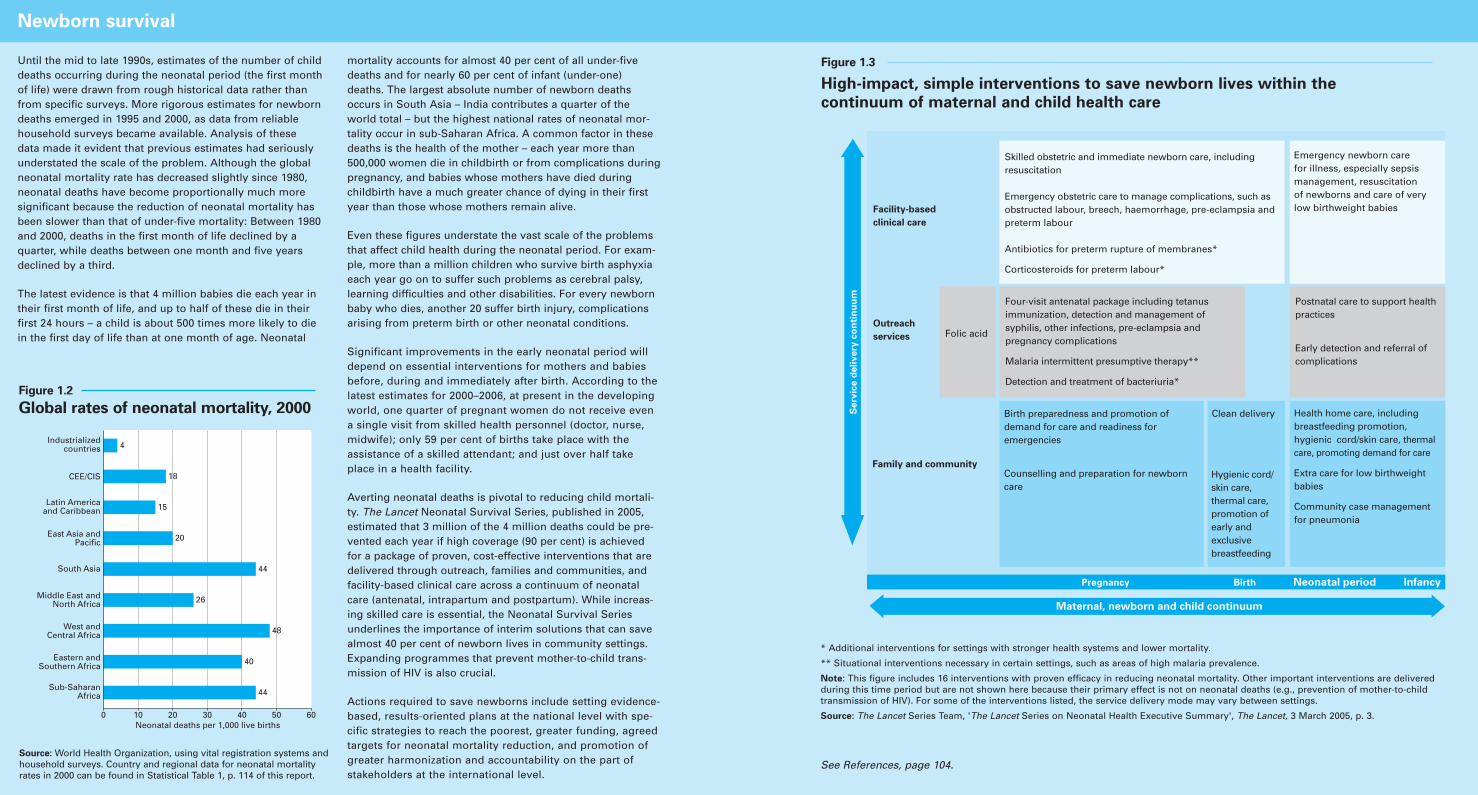
Figure 1.2
Global rates of neonatal mortality, 2000
Source: World Health Organization, using vital registration systems andhousehold surveys. Country and regional data for neonatal mortalityrates in 2000 can be found in Statistical Table 1, p. 114 of this report.
Infancy Neonatal periodBirth
Facility-based
clinical care
Outreach
services Folic acid
Family and community
Pregnancy
Skilled obstetric and immediate newborn care, including resuscitation
Emergency obstetric care to manage complications, such as obstructed labour, breech, haemorrhage, pre-eclampsia and preterm labour
Antibiotics for preterm rupture of membranes*
Corticosteroids for preterm labour*
Emergency newborn care for illness, especially sepsis management, resuscitation of newborns and care of very low birthweight babies
Four-visit antenatal package including tetanus immunization, detection and management of syphilis, other infections, pre-eclampsia and pregnancy complications
Malaria intermittent presumptive therapy**
Detection and treatment of bacteriuria*
Postnatal care to support health practices
Early detection and referral of complications
Birth preparedness and promotion of demand for care and readiness for emergencies
Counselling and preparation for newborn care
Clean delivery Health home care, including breastfeeding promotion, hygienic cord/skin care, thermal care, promoting demand for care
Extra care for low birthweight babies
Community case management for pneumonia
Maternal, newborn and child continuum
Se
rvic
e d
eli
ve
ry c
on
tin
uu
m
Hygienic cord/skin care, thermal care, promotion of early and exclusive breastfeeding
Figure 1.3
High-impact, simple interventions to save newborn lives within the
continuum of maternal and child health care
* Additional interventions for settings with stronger health systems and lower mortality.
** Situational interventions necessary in certain settings, such as areas of high malaria prevalence.
Note: This figure includes 16 interventions with proven efficacy in reducing neonatal mortality. Other important interventions are delivered during this time period but are not shown here because their primary effect is not on neonatal deaths (e.g., prevention of mother-to-child transmission of HIV). For some of the interventions listed, the service delivery mode may vary between settings.
Source: The Lancet Series Team, 'The Lancet Series on Neonatal Health Executive Summary', The Lancet, 3 March 2005, p. 3.
is insufficient to meet MDG 4 infull and on time.
Of most concern are the 27 countriesthat have registered scant progresssince 1990 or have an under-fivemortality rate that is stagnant orhigher than it was in 1990. Of the 46countries in sub-Saharan Africa, onlyCape Verde, Eritrea and Seychellesare on track to meet MDG 4, andnearly half the countries have regis-tered either no change or an increasein child mortality rates since 1990.The region as a whole only managedto reduce child mortality at an aver-age annual rate of 1 per cent from1990–2006, and double-digit reduc-tions will be needed during each of the remaining years if it is to meet MDG 4.5
Individual countries face differentchallenges in child survival, withoutdoubt some greater than others. Butthe notable achievements suggest thatgeography is no barrier to saving chil-dren’s lives. Perhaps most important,these gains are evident in some of theworld’s poorest countries and acrossthe developing regions, as illustratedin Figure 1.7. These gains suggest that remarkable progress is possible,despite such obstacles as geographiclocation or socio-economic disadvan-tage, when evidence, sound strategies,sufficient resources, political will andan orientation towards results areconsciously harnessed to improvechildren’s lives.
Furthermore, dramatic improvementsin child mortality and health can berapidly attained. Since 1990, morethan 60 countries have managed toreduce their under-five mortality rateby 50 per cent.
C H I L D S U R V I VA L : W H E R E W E S T A N D 98 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
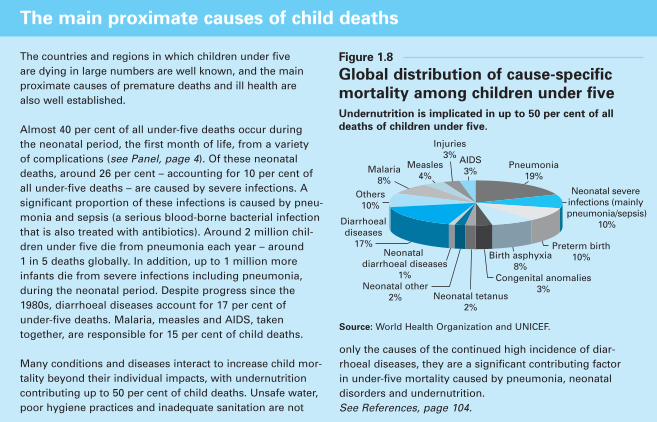
The countries and regions in which children under five are dying in large numbers are well known, and the mainproximate causes of premature deaths and ill health are also well established.
Almost 40 per cent of all under-five deaths occur during the neonatal period, the first month of life, from a variety of complications (see Panel, page 4). Of these neonataldeaths, around 26 per cent – accounting for 10 per cent ofall under-five deaths – are caused by severe infections. Asignificant proportion of these infections is caused by pneu-monia and sepsis (a serious blood-borne bacterial infectionthat is also treated with antibiotics). Around 2 million chil-dren under five die from pneumonia each year – around 1 in 5 deaths globally. In addition, up to 1 million moreinfants die from severe infections including pneumonia,during the neonatal period. Despite progress since the1980s, diarrhoeal diseases account for 17 per cent of under-five deaths. Malaria, measles and AIDS, taken together, are responsible for 15 per cent of child deaths.
Many conditions and diseases interact to increase child mor-tality beyond their individual impacts, with undernutritioncontributing up to 50 per cent of child deaths. Unsafe water,poor hygiene practices and inadequate sanitation are not
only the causes of the continued high incidence of diar-rhoeal diseases, they are a significant contributing factor in under-five mortality caused by pneumonia, neonatal disorders and undernutrition. See References, page 104.
The main proximate causes of child deaths
Pneumonia19%
Neonatal severe infections (mainly pneumonia/sepsis)
10%
Preterm birth10%Birth asphyxia
8%Congenital anomalies
3%Neonatal tetanus
2%
Neonatal other2%
Neonatal diarrhoeal diseases
1%
Diarrhoealdiseases
17%
Others10%
Malaria8%
Measles4%
Injuries3% AIDS
3%
Figure 1.8
Global distribution of cause-specific
mortality among children under five
Source: World Health Organization and UNICEF.
Undernutrition is implicated in up to 50 per cent of all
deaths of children under five.
Health and the Millennium Development Goals
Source: Adapted from World Health Organization, Health and the Millennium Development Goals,WHO, Geneva, 2005, p. 11.
Figure 1.9
GOAL 1Eradicate extreme poverty and hunger
GOAL 4Reduce child mortality
GOAL 5Improve maternalhealth
GOAL 6Combat HIV and AIDS, malaria and other diseases
GOAL 7Ensureenvironmental sustainability
GOAL 8Develop a global partnership for development
Target 2Halve, between 1990 and2015, the proportion of peo-ple who suffer from hunger
Target 5Reduce by two thirds,between 1990 and 2015, theunder-five mortality rate
Target 6Reduce by three quarters,between 1990 and 2015, thematernal mortality ratio
Target 7Halt and begin to reverse,by 2015, the spread of HIVand AIDS
Target 8Halt and begin to reverse, by 2015, the incidence ofmalaria and other majordiseases
Target 10Halve, by 2015, the propor-tion of people without sus-tainable access to safe drink-ing water and basic sanitation
Target 10By 2020, achieve a signifi-cant improvement in thelives of at least 100 millionslum dwellersTarget 17In cooperation with pharma-ceutical companies, provideaccess to affordable essentialdrugs in developing countries
Prevalence of underweight children under five
Proportion of population belowminimum level of dietary energyconsumption
Under-five mortality rate
Infant mortality rate
Proportion of one-year-olds immunized against measles
Maternal mortality ratio
Proportion of births attended byskilled health personnel
HIV prevalence among pregnantwomen aged 15–24
Condom use rate of the contra-ceptive prevalence rate
Ratio of school attendance oforphans to school attendance ofnon-orphans aged 10–14
Prevalence and death rates associated with malaria
Proportion of population in malaria-risk areas using effective malariaprevention and treatment measures
Prevalence and death rates associated with tuberculosis
Proportion of tuberculosis casesdetected and cured under DirectlyObserved Treatment Short-Course(DOTS)
Proportion of population usingan improved water source, urbanand rural
Proportion of population usingimproved sanitation, urban andrural
Proportion of population withaccess to affordable essentialdrugs on a sustainable basis
Goal Health Targets Health Indicators
Figure 1.7
Maldives
Timor-Leste
Bhutan
Nepal
Bangladesh
Eritrea
Haiti
Malawi
Samoa
Cape Verde
Comoros
Mozambique
Ethiopia
Solomon Islands
0 20 40 60 80 100
73
69
58
58
54
54
50
47
46
44
43
43
40
41
40
21
Lao PDR
Least developedcountries
Source: UNICEF, World Health Organization, United Nations Population Division and United Nations Statistics Divisions. Country and regional datacan be found in Statistical Tables 1 and 10, pages 114 and 150 of this report.
Almost one third of the 50 least developed countries have managed to reduce
their under-five mortality rates by 40 per cent or more since 1990
Leas
t d
evel
op
ed c
ou
ntr
y
Percentage reduction in U5MR, 1990–2006

Progress towards the other
health-related MDGs is mixed
Although advancements on all eightMillennium Development Goals areimportant to the survival and well-being of children, MDGs 1, 5, 6, 7and 8, as well as MDG 4, have targets that directly affect children’shealth. Progress in the areas targetedby these goals could have a dramaticeffect on the lives and prospects of children.
Enhancing nutritional status
(MDG 1)
Undernutrition is the main underlyingfactor for up to half of all deaths ofchildren under five. Improving nutri-tion and achieving MDG 1, whichaims to reduce poverty and hunger,would help avert child deaths fromdiarrhoea, pneumonia, malaria, HIVand measles, and it would reduceneonatal mortality. In other words,improving maternal and child nutritionis a prerequisite for achieving MDG 4.
The standard indicators used to meas-ure MDG 1, however, do not revealthe full extent of undernutritionamong children in the developingworld. One of the indicators focuseson hunger, as measured by the pro-portion of children under five whoare underweight. But that capturesonly one dimension of nutrition. A child may die from a weakenedimmune system when vitamin A islacking, for example, without beingapparently hungry or underweight.
Adequate nutrition needs to beginduring a mother’s pregnancy and con-tinue when a child is born. Immediateand exclusive breastfeeding is the bestsource of nutrition for a child, provid-ing physical warmth and strengthen-
ing immune systems. Micronutrientssuch as iron, vitamin A and iodinecan also have a profound impact on a child’s development and a mother’shealth. In cases of severe acute under-nutrition, specific therapeutic foodsare advised. Although these remediesare low-cost and highly effective, mil-lions of children and mothers still donot have access to or are not adoptingthem. More than 30 per cent ofhouseholds in the developing worlddo not consume iodized salt. Morethan 60 per cent of infants were notexclusively breastfed during the firstsix months of life, and 28 per centlacked full coverage (two doses) ofvitamin A supplementation in 2005.
Improving maternal health (MDG 5)
To reduce child mortality, improvingthe health of pregnant women andnew mothers is critical. More thanhalf a million women die each year
due to pregnancy-related causes, andmany more suffer debilitating long-term effects, such as fistula, thatcould be easily avoided through ade-quate maternal care. Furthermore,improving maternal health is vitallyimportant for a child’s prospects of survival. Evidence shows that amotherless child is more likely to die before reaching age two thaninfants whose mothers survive.6
Improving the health and nutritionof mothers-to-be and providing qual-ity reproductive health services arepivotal to addressing many underly-ing causes of child mortality. Poornutrition in women can result inpreterm births and babies with lowweight at birth. Visits to, or from, atrained health-care provider duringpregnancy can help avert early deliv-eries and neonatal tetanus, which is almost always fatal. A skilled
C H I L D S U R V I VA L : W H E R E W E S T A N D 1110 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Pneumonia kills more children than any other disease –more than AIDS, malaria and measles combined. It is amajor cause of child deaths in every region. Children with pneumonia may exhibit a wide range of symptoms,depending on age and cause of the infection. Commonsymptoms include rapid or difficult breathing, cough, fever,chills, headaches, loss of appetite and wheezing. In younginfants, severe cases of pneumonia can cause convulsions,hypothermia, lethargy and feeding problems.
In childhood, pneumonia and malaria have major overlapsin terms of symptoms, the requirements for their effectivemanagement and the feasibility of providing care in thecommunity. In effect, especially in very young children, itmay be impossible to tell whether a high fever, coughingand fast breathing is evidence of either pneumonia ormalaria, and in such cases children often receive treatmentfor both. Once a child develops pneumonia, a caregivermust recognize the symptoms and seek appropriate careimmediately.
Healthy children have natural defences that protect their lungs from the pathogens that cause pneumonia.Undernourished children, particularly those who are notexclusively breastfed or have inadequate zinc intake, orthose with compromised immune systems, run a higherrisk of developing pneumonia. Children suffering fromother illnesses, such as measles, or those living with HIV,are more likely to develop pneumonia. Environmental fac-tors, such as living in crowded homes and being exposedto parental smoking or indoor air pollution, may also play a role in increasing children’s susceptibility to pneumoniaand its consequences.
Prevention is as important as cure in reducing child deathsfrom pneumonia. The key preventive measures for childrenare adequate nutrition (including exclusive breastfeeding, vita-min A supplementation and zinc intake), reduced indoor airpollution and increased immunization rates with vaccines thathelp prevent children from developing infections that directlycause pneumonia, such as Haemophilus influenzae type b(Hib), and with those immunizations that prevent infectionsthat can lead to pneumonia as a complication (e.g., measlesand pertussis). Vaccines to protect against Streptococcuspneumoniae – the most common cause of severe pneumoniaamong children in the developing world – will be increasinglybecoming available for infants and young children.
Since a large proportion of severe pneumonia cases in chil-dren of the developing world are bacterial in origin – most-ly Streptococcus pneumoniae or Haemophilus influenzae –they can be effectively treated using inexpensive antibioticsat home, provided that families and caregivers follow theadvice they receive and treat the child correctly, includingreturning for help as necessary. If these conditions are inplace, evidence from across the developing world suggeststhat community-based management of pneumonia can bevery effective. A meta-analysis of results from nine studiesin seven countries, including the United Republic of Tanzania,that investigated the impact of community-based casemanagement of pneumonia revealed substantial reductionsnot only in pneumonia mortality but in child mortality moregenerally. Trials resulted in a reduction of child mortality of26 per cent and a 37 per cent reduction in mortality frompneumonia.
See References, page 104.
Pneumonia: The forgotten killer of children
Figure 1.10
More than half of children under five with suspected pneumonia are taken to an
appropriate health provider
* Excludes China.
** Data refer to the mostrecent year available duringthe period specified.
Source: Demographic andHealth Surveys, MultipleIndicator Cluster Surveys andother national surveys.
40
66
62
64
56
Sub-Saharan Africa
Middle East and North Africa
South Asia
East Asia and Pacific*
Developingcountries/territories*
% of under-fives with suspected pneumonia taken to anappropriate health-care provider, 2000–2006,** various regions
0 10 20 30 40 50 60 70
26
0 5 10 15 20 25 30 35 40 45
5
7
14
17
28
42
Developingcountries/territories
CEE/CIS
Latin America andCaribbean
East Asia and Pacific
Middle East and NorthAfrica
Sub-Saharan Africa
South Asia
% of under-fives who are moderately or severely underweight, 2000–2006*
25
35Least developedcountries/territories
World
South Asia has the highest level of undernutrition among
the regions
*Data refer to the most recent year available during the period specified.
Source: Demographic and Health Surveys, Multiple Indicator Cluster Surveys, World HealthOrganization and UNICEF. Country and regional data can be found in Statistical Table 2, p. 118 ofthis report.
Figure 1.11
C H I L D S U R V I VA L : W H E R E W E S T A N D 17
and proven programmes, furtherscaling up is urgently required.
Priority 1: Focusing on countries
where the burden of child
mortality is highest
In 2003, concerned that progress onchild survival was behind schedule, agroup of technical experts workingon diverse aspects of child healthcame together for a workshop onchild survival in Bellagio, Italy,sponsored by the RockefellerFoundation. Later that year, theBellagio Child Survival Group pub-lished a series of articles on mater-nal, newborn and child survival andhealth in the British medical journal
The Lancet. Called The ChildSurvival series, the articles helped to spur awareness and called forimmediate action to translate knowl-edge into practice. The group’s workis now being continued by a newcoalition of scientists, policymakers,activists and health-programmemanagers participating in the Count-down to 2015: Tracking Progress in Maternal, Newborn and ChildMortality. The Countdown initiativeis sponsoring a series of conferencesthat began in December 2005 andwill take place approximately everytwo years until 2015 (the next onewill be held in April 2008 in CapeTown, South Africa).19
The Countdown gathers data on theprogress countries are making as theybroaden coverage of interventionsthat have proved effective in reducingthe deaths of children under five.Early on it was recognized thatalthough every region of the worldneeded to accelerate progress, coun-tries with the greatest number or the highest rates of under-five deathsshould be prioritized. To this end,Countdown to 2015 partners, includ-ing UNICEF, have identified 60 prior-ity countries for child survival initia-tives, based on two criteria: countrieswith more than 50,000 deaths of children under five and countries withan annual under-five mortality rate
16 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The 60 priority countries for child survival targeted by Countdown to 2015
Figure 1.17
Latin America/
Caribbean (3)
BrazilHaitiMexico
West/Central
Africa (22)
BeninBurkina FasoCameroonCentral African
Republic ChadCongoCongo, Dem. Rep.Côte d’IvoireEquatorial GuineaGabonGambiaGhanaGuineaGuinea-BissauLiberiaMaliMauritaniaNigerNigeriaSenegalSierra LeoneTogo
Middle East/
North Africa (5)
DjiboutiEgyptIraqSudanYemen
Eastern/Southern
Africa (16)
AngolaBotswanaBurundiEthiopiaKenyaMadagascarMalawiMozambiqueRwandaSomaliaSouth AfricaSwazilandTanzania, United
Republic ofUgandaZambiaZimbabwe
East Asia/
Pacific (6)
CambodiaChinaIndonesiaMyanmarPapua New GuineaPhilippines
CEE/CIS (3)
AzerbaijanTajikistan Turkmenistan
South Asia (5)
AfghanistanBangladeshIndiaNepalPakistan
Source: Countdown to 2015, Tracking Progress in Child Survival: The 2005 report, UNICEF Health Section, New York, 2006, p. 37.
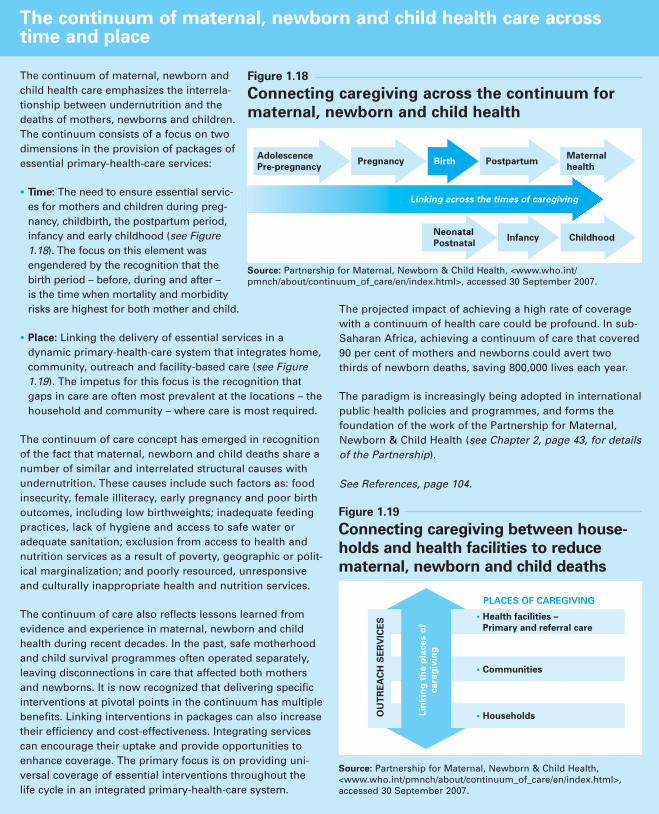
The continuum of maternal, newborn andchild health care emphasizes the interrela-tionship between undernutrition and thedeaths of mothers, newborns and children.The continuum consists of a focus on twodimensions in the provision of packages ofessential primary-health-care services:
• Time: The need to ensure essential servic-es for mothers and children during preg-nancy, childbirth, the postpartum period,infancy and early childhood (see Figure1.18). The focus on this element wasengendered by the recognition that thebirth period – before, during and after – is the time when mortality and morbidityrisks are highest for both mother and child.
• Place: Linking the delivery of essential services in adynamic primary-health-care system that integrates home,community, outreach and facility-based care (see Figure1.19). The impetus for this focus is the recognition thatgaps in care are often most prevalent at the locations – the household and community – where care is most required.
The continuum of care concept has emerged in recognitionof the fact that maternal, newborn and child deaths share anumber of similar and interrelated structural causes withundernutrition. These causes include such factors as: foodinsecurity, female illiteracy, early pregnancy and poor birthoutcomes, including low birthweights; inadequate feedingpractices, lack of hygiene and access to safe water or adequate sanitation; exclusion from access to health andnutrition services as a result of poverty, geographic or polit-ical marginalization; and poorly resourced, unresponsiveand culturally inappropriate health and nutrition services.
The continuum of care also reflects lessons learned fromevidence and experience in maternal, newborn and childhealth during recent decades. In the past, safe motherhoodand child survival programmes often operated separately,leaving disconnections in care that affected both mothersand newborns. It is now recognized that delivering specificinterventions at pivotal points in the continuum has multiplebenefits. Linking interventions in packages can also increasetheir efficiency and cost-effectiveness. Integrating servicescan encourage their uptake and provide opportunities toenhance coverage. The primary focus is on providing uni-versal coverage of essential interventions throughout thelife cycle in an integrated primary-health-care system.
The projected impact of achieving a high rate of coveragewith a continuum of health care could be profound. In sub-Saharan Africa, achieving a continuum of care that covered90 per cent of mothers and newborns could avert twothirds of newborn deaths, saving 800,000 lives each year.
The paradigm is increasingly being adopted in internationalpublic health policies and programmes, and forms thefoundation of the work of the Partnership for Maternal,Newborn & Child Health (see Chapter 2, page 43, for detailsof the Partnership).
See References, page 104.
The continuum of maternal, newborn and child health care acrosstime and place
Lin
kin
g t
he p
laces o
f
care
giv
ing
OU
TR
EA
CH
SE
RV
ICE
S • Health facilities –
Primary and referral care
• Communities
• Households
PLACES OF CAREGIVING
Figure 1.19
Connecting caregiving between house-
holds and health facilities to reduce
maternal, newborn and child deaths
Adolescence
Pre-pregnancyPregnancy
Linking across the times of caregiving
Maternal
healthPostpartumBirth
Neonatal
PostnatalChildhoodInfancy
Source: Partnership for Maternal, Newborn & Child Health, <www.who.int/pmnch/about/continuum_of_care/en/index.html>, accessed 30 September 2007.
Source: Partnership for Maternal, Newborn & Child Health,<www.who.int/pmnch/about/continuum_of_care/en/index.html>,accessed 30 September 2007.
Figure 1.18
Connecting caregiving across the continuum for
maternal, newborn and child health
Packaging and integrating proven,cost-effective interventions – forexample, immunization and vitaminA supplementation – is efficacious.It also ensures more comprehensivecare for the children served.Recently, a package of 16 proveninterventions was identified thatcould avert up to 72 per cent of all newborn deaths. These includetetanus toxoid immunization,skilled attendants at birth, access to obstetric care, immediate andexclusive breastfeeding, drying andkeeping newborns warm, access toresuscitation, if needed, special careof low-birthweight infants andtreatment of infection.21
The timing of these packaged inter-ventions can be crucial. More thanhalf of all maternal and newborndeaths occur at birth and during thefirst few days of life, but this is alsothe period when health coverage islowest. An effective continuum ofcare (see Panel, page 17) connectsessential maternal, newborn andchild health packages through preg-nancy, childbirth, postnatal and newborn periods, and into childhoodand adolescence. The advantage isthat each stage builds on the successof the previous stage. For example,providing integrated services to ado-lescent girls means fewer unintendedor poorly timed pregnancies. Visits to a health-care practitioner can prevent problems during pregnancyand make it more likely that mothers will get the appropriate care at birth.Skilled care before, during and imme-diately after birth reduces the risk of death or disability for both themother and the baby. Continued care for children supports their right to health.
An effective continuum of care alsoaddresses the gaps in care, whether inthe home, community, health centre orhospital. Babies with birth asphyxia,sepsis or complications from apreterm birth can die within hours or even minutes if appropriate care is not provided. Because more than60 million women in the developingworld deliver at home,22 it is criticalthat a skilled attendant be present atbirth with strong backup by a localhealth clinic or other first-level facili-ty and the hospital, should complica-tions arise. Quality of care at all ofthese levels is crucial.
Priority 3: Strengthening health
systems and community
partnerships
Delivering comprehensive health carefor children requires preventive meas-ures, as well as treatment of illness.Prevention typically requires behav-iour changes that start in the house-hold and can gain support throughthe community. Improvements innutrition, for example, are often theresult of better infant feeding prac-tices by mothers or other caregivers,whether through breastfeeding or,later, by providing a diversified dietthrough kitchen or community gar-dens. Such practices must be learnedby an individual and reinforced bythe community. Wells, pumps and toilets are important to good hygiene.But their effectiveness depends on acommunity primed to maintain themand to use them. Children must learnto wash their hands and practise goodhygiene, habits that are cultivated inthe home, in school and amongneighbours and friends.
As an integral part of the largerhealth system, community partner-
ships in primary health care canserve a dual function: activelyengaging community members ashealth workers and mobilizing thecommunity in support of improvedhealth practices. They can also stimulate demand for quality health services from governments.Community involvement fosterscommunity ownership. It can alsoadd vitality to a bureaucracy-ladenhealth system and is essential inreaching those who are the most iso-lated or excluded. As the followingchapters in this report will show,many countries, including some of the poorest in the world, haveimplemented successful community-based health programmes. The challenge now will be to learn from their experiences, take the programmes to scale and reach the millions of children whom thehealth system, so far, has passed by.
Creating a supportive
environment for child
survival strategies
Prospects for child survival are shapedby the institutional and environmentalcontext in which children and theirfamilies live. It comes as no surprise,for example, that infant and childmortality rates are highest in the poorest countries, among the mostimpoverished, isolated, uneducatedand marginalized districts and commu-nities, and in countries ravaged by civilstrife, weak governance and chronicunderinvestment in public health systems and physical infrastructure. Of the 11 countries where 20 per centor more of children die before age five– Afghanistan, Angola, Burkina Faso,Chad, the Democratic Republic of theCongo, Equatorial Guinea, Guinea-
C H I L D S U R V I VA L : W H E R E W E S T A N D 19
of at least 90 per 1,000 live births. In 2005, these 60 countries accountedfor 93 per cent of all deaths of chil-dren under five worldwide. Of these,only seven – Bangladesh, Brazil,Egypt, Indonesia, Mexico, Nepal andthe Philippines – are considered to beon track to meet MDG 4. In contrast,19 of the priority countries will needto achieve annual reductions of 10per cent or more per year to achievethe 2015 target.20
Priority 2: Providing a
continuum of care by packaging
interventions and delivering them
at key points in the life cycle
Astonishing results have beenachieved by some child health pro-grammes that target specific diseasesand conditions. These ‘vertical’ interventions, as they are known, areusually one-time events or disease-specific in nature, such as immuniza-tion campaigns covering one
disease. Lessons from the past,explored in greater detail in Chapter2, show that such programmes areill-suited to providing the more comprehensive and sustained carethat mothers, newborns and childrenneed. More recent experience sug-gests that even greater progress ispossible if these life-saving interven-tions were combined into ‘packages’of care and administered at keypoints in the life cycle.
18 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Meeting the health needs of children, women and familiespresents considerable challenges in peacetime. Thesechallenges are compounded many times during emergen-cies, natural or human-made. Yet delivery of health servic-es to populations in general and to children in particular isespecially critical in these contexts. In effect, a significantproportion of the children who are not currently beingreached through existing interventions live in countrieswhere the delivery of health services has been severelydisrupted. Between 1989 and 2000, 110 recorded conflictstook place; 103 of them were civil wars, many of them protracted, accompanied by institutional collapse and violence directed against civilians. At present, more than40 countries, 90 per cent of them low-income nations, aredealing with armed conflict. UNICEF’s Humanitarian ActionReport 2006 highlighted 29 emergency situations affectingchildren and women.
A complex emergency is defined broadly as a situation of armed conflict, population displacement and/or foodinsecurity with associated increases in mortality and mal-nutrition. Most of the major causes of child mortality incomplex emergencies are the same as the top killers ofchildren in general. They include measles, malaria, diar-rhoeal diseases, acute respiratory infections and malnutri-tion. These are often compounded by outbreaks of othercommunicable diseases, such as meningitis, and nutrition-al deficiencies that can contribute substantially to childmorbidity and mortality. The highest mortality rates inrefugee populations, for example, tend to occur amongchildren under five.
Child mortality rates are usually highest during the acuteearly phase of a complex emergency. By contrast, in post-
emergency settings, where children have remained in stablerefugee camps for prolonged periods, child mortality mightbe lower in the refugee population than among neighbour-ing resident children. Obstacles to the provision of healthcare to children in complex emergencies include limitedaccess, cultural barriers, insecurity, limitations in resourcessuch as drugs and supplies, and a lack of communicationamong the various organizations providing relief.
Community leadership and engagement is especially critical in these contexts. Contrary to the assumption thatcommunities in situations of crisis are fragile and tend tofragment under the stress of war, famine or mass disloca-tion, research increasingly suggests that some form ofcommunity mobilization is almost always possible and thatimportant elements of community remain intact and evengain in importance under conditions of stress. Evidencefrom Ethiopia, Malawi and Southern Sudan focusing onthe challenges of treating severe malnutrition in complexemergencies suggests that the success of an interventiondepends critically on involving key community figures(such as traditional leaders, teachers and communityhealth workers), as well as community organizations, vol-unteer networks and women’s organizations. In addition,involving traditional heath practitioners can be equallyimportant, because in many cases they are the first to beconsulted in health-seeking behaviour and can thereforeplay a critical role in identifying severely malnourishedchildren at an early stage.
See References, page 105.
Child health in complex emergencies
The challenge of reaching children incountries with such intractable prob-lems is daunting. Nevertheless, if thepolitical will is there, there are stepsthese countries can take to create asupportive environment for child survival and development.
Create laws to protect children
from violence, and see that they
are enforced
Data from countries in the Organi-sation for Economic Co-operationand Development (OECD) indicatethat among children under 18,infants less than a year old face thesecond-highest risk of dying by homi-
cide. The risk of death is about threetimes greater for children under onethan for those aged one to four, andthe younger the child, the more likelythat death will be caused by a closefamily member. Where deaths are notrecorded or investigated, the extentof fatal violence to children is notaccurately known and may becomeobscured by the generally high ratesof under-five mortality. It is assumedthat violence in one form or another– including neglect – may often playa part in infant and young childdeaths that are not recorded as homi-cides or perhaps not recorded at all.It is widely agreed that violence
against children by family membersresults in deaths far more often thanofficial records suggest.24
Forced marriage is another form of violence inflicted on children –and often socially condoned – withimplications for child survival.When girls give birth before theirbodies are fully developed, there is amuch higher risk of death for bothmother and child. Pregnancy-relateddeaths are the leading cause of mortality for girls 15–19 years oldworldwide, whether they are mar-ried or not.25 Those younger than 15 are five times more likely to
C H I L D S U R V I VA L : W H E R E W E S T A N D 21
Bissau, Liberia, Mali, Niger and SierraLeone23 – more than half have suffered a major armed conflict since 1989.Similarly, fragile states, characterizedby weak institutions with high levels of corruption, political instability anda shaky rule of law, are often inca-pable of providing basic services totheir citizens.
Institutional and environmental fac-tors can sometimes be the dominantfactor in child survival. In countrieswhere AIDS has reached epidemiclevels, for example, combating thesyndrome is the main challenge forchild survival. The scale and natureof the epidemic is such that allother interventions will prove
ineffective unless AIDS is addressed.Countries that suffer from foodinsecurity or are prone to droughtsare also at risk of having poorerchild survival outcomes. The inabil-ity to diversify diets leads to chronicmalnutrition for children, increasingtheir vulnerability to ill health and,ultimately, death.
20 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Empowering women, especially at the community level, is essential both to lowering the number of deaths amongchildren under five and to reaching MillenniumDevelopment Goal 5, which aims to reduce maternal mortality by three quarters by 2015. Yet the low status of women in many societies and their limited decision-making power within the household often present seriouschallenges to achieving significant progress in either area.Analysis of the data from recent Demographic and HealthSurveys in 30 countries, for example, suggests that inmany households, especially in South Asia and sub-Saharan Africa, women have little influence in health-related decisions in households, whether concerning theirown health or that of their children. In Burkina Faso, Maliand Nigeria, almost 75 per cent of women respondentsreported that husbands alone make decisions aboutwomen’s health care. In the two countries surveyed inSouth Asia, Bangladesh and Nepal, this ratio was around50 per cent.
This exclusion compromises the health and well-being ofall family members, particularly women and children, andis often linked to high maternal and child mortality rates –all five countries mentioned above are among the 60 select-ed as priority countries for child survival by the Countdownto 2015 (see Figure 1.17, page 16, for further details). The situation is often most severe in rural areas or in urbanslums, where women are largely illiterate and suffer fromsocio-cultural barriers to accessing health services, such asrestrictions on leaving their homes or on interacting withstrangers, and frequently do not have access to a healthcentre or a health clinic.
For example, in Afghanistan, women are prohibited from receiving health care at hospitals staffed exclusivelyby male health personnel, while cultural norms restrictwomen from working and receiving advanced medicaltraining.
A number of community health worker programmes thattrain primarily women have successfully circumvented gender-based barriers to utilization of health services. InBangladesh, the community health workers trained by BRACare married, middle-aged women, and their `doorstep’ healthservices allow women to circumvent purdah restrictions thatprevent them from leaving their homes to access health facili-ties on their own. In Pakistan, where in 1999 only about halfthe women of childbearing age were immunized againsttetanus, a campaign initiated by the Ministry of Health succeeded in raising that proportion to 80 per cent of a target group of 5 million women by relying on home visits by the Lady Health Workers, who were more acceptable towomen than male vaccinators.
Furthermore, interventions that have enhanced women’sempowerment and leadership at the community level havebeen equally important in improving the health status ofwomen and children. In Ghana, the prevalence of Guineaworm disease, which is spread by water and can incapacitatean infected person for months, required a comprehensive eradication campaign. Women volunteers, who were morefamiliar with the improved water sources than men, conduct-ed door-to-door surveillance, distributed filters, identifiedpotentially contaminated water supplies and provided com-munity education. As a result, incidence of the disease fell by36 per cent between 2002 and 2003. Similarly, in Puerto Rico,a programme to prevent dengue fever, carried out by WHOand the US Centers for Disease Control and Prevention,relied on community-nominated women to act as promoters.The women made house-to-house visits, interviewing headsof households and inspecting the premises for vector breed-ing sites. They also engaged in community-awareness activi-ties, including the creation of a dengue prevention exhibit atthe local supermarket. Through this strategy, 20 per cent ofhouseholds joined the campaign.
See References, page 105.
Empowering women to advance maternal, newborn and child health
Giving women a voice in making health-related decisions translates into better care for their children. Discussing health care at a meeting, India.
© U
NIC
EF/
HQ
06-2
640/
Tom
Pie
tras
ik
is about 20 per cent more likely tosurvive compared to a child born to a mother with no education; theodds increase to 80 per cent whenthe mother has obtained a second-ary education.32
Empowering women socially andeconomically can establish anotherpath towards improving child sur-vival. In many countries, women aredeprived of basic decision-makingresponsibilities, even concerning theirown health or that of their children.
It is also well known that whenwomen are in charge of householdfinances, they tend to spend a largerportion of the household budget onfood and other necessities for chil-dren. For these reasons, givingwomen the means to become moreeconomically self-reliant will likelyhave positive spin-offs for children.
Promote social equity
Because they are poor and disen-franchised, millions of women andchildren have been excluded from
progress in recent decades. The dis-parities in child survival prospectsbetween poor and better-off childrenare stark, not only among countriesbut within them. For example, inevery country where data are avail-able, children living in the poorest 20 per cent of households are farmore likely to die before their fifthbirthday than children living in therichest quintile of the population; insome countries the risk is up to fivetimes higher.33 Policy interventions toeliminate these inequalities – that is,
C H I L D S U R V I VA L : W H E R E W E S T A N D 23
die in childbirth than women intheir twenties.26 Their children arealso less likely to survive. If a moth-er is under 18, her baby’s chances ofdying during the first year of life are60 per cent higher than those of a baby born to a mother olderthan 19.27
In addition to laws that prohibit childmarriage and other forms of violenceagainst children, a policy of zero tolerance should be adopted by coun-tries seeking to create an environment
in which children can survive andthrive. Another essential form of protection is birth registration of allchildren. This legal acknowledgementof the child’s existence is often requiredto access essential services, such asvaccinations and vitamin A supple-mentation. It also establishes familyties where inheritance is an issue.28
Educate and empower women
The latest estimates indicate that,on average, almost 1 out of every 4 adults (defined here as those age
15 and over) is illiterate. Almosttwo thirds are women, according to the most recent data from theUNESCO Institute for Statistics.29
Research shows that less-educatedcaregivers generally have pooreraccess to information on basichealth care than their better-educatedpeers.30 This, in turn, can lead toill-informed decisions about whenand how to seek care for sick chil-dren.31 In contrast, evidence fromBangladesh shows that a child bornto a mother with primary education
22 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The right to a name and a nationality is well establishedby the Convention on the Rights of the Child, whichexplicitly calls in article 7 for the registration of a childimmediately after birth. Yet every year the births ofaround 51 million children go unregistered. These
children are almost always from poor, marginalized ordisplaced families or from countries where systems of registration are not functional, and the consequences for their health and well-being are often severe and long-lasting.
Birth registration: An important step towards accessing essential services
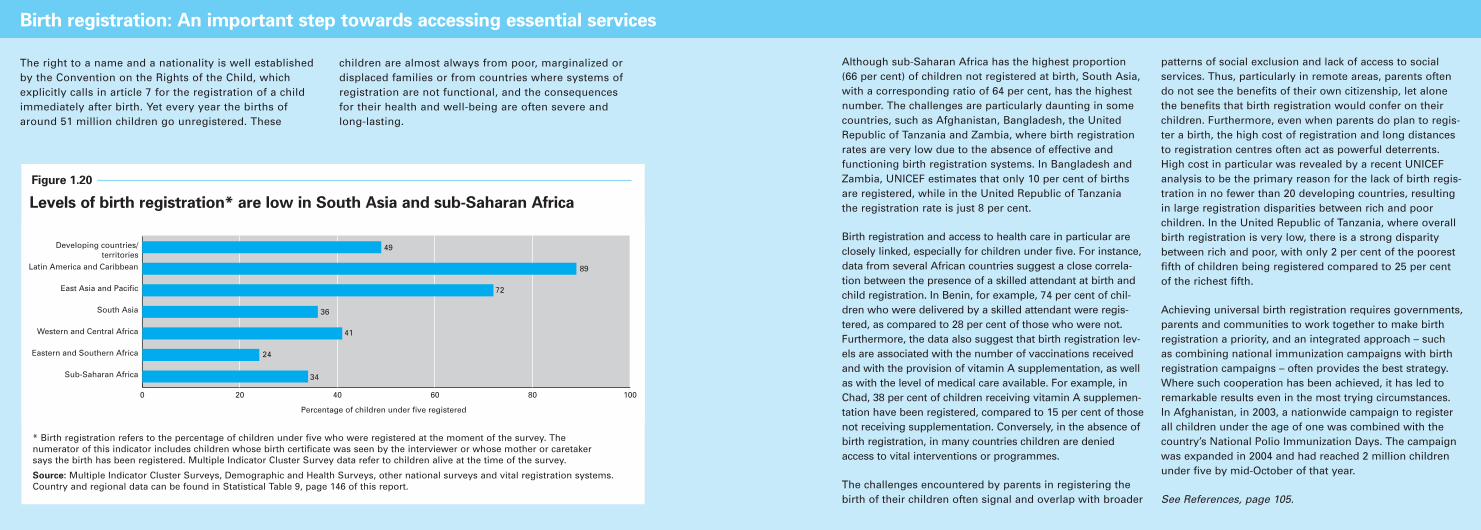
* Birth registration refers to the percentage of children under five who were registered at the moment of the survey. The numerator of this indicator includes children whose birth certificate was seen by the interviewer or whose mother or caretaker says the birth has been registered. Multiple Indicator Cluster Survey data refer to children alive at the time of the survey.
Source: Multiple Indicator Cluster Surveys, Demographic and Health Surveys, other national surveys and vital registration systems.Country and regional data can be found in Statistical Table 9, page 146 of this report.
Figure 1.20
34
41
36
72
89
24
49
Percentage of children under five registered
0 20 40 60 80 100
Developing countries/
Latin America and Caribbean
East Asia and Pacific
South Asia
Western and Central Africa
Eastern and Southern Africa
Sub-Saharan Africa
territories
Levels of birth registration* are low in South Asia and sub-Saharan Africa
Although sub-Saharan Africa has the highest proportion (66 per cent) of children not registered at birth, South Asia,with a corresponding ratio of 64 per cent, has the highestnumber. The challenges are particularly daunting in somecountries, such as Afghanistan, Bangladesh, the UnitedRepublic of Tanzania and Zambia, where birth registrationrates are very low due to the absence of effective and functioning birth registration systems. In Bangladesh andZambia, UNICEF estimates that only 10 per cent of birthsare registered, while in the United Republic of Tanzania the registration rate is just 8 per cent.
Birth registration and access to health care in particular areclosely linked, especially for children under five. For instance,data from several African countries suggest a close correla-tion between the presence of a skilled attendant at birth andchild registration. In Benin, for example, 74 per cent of chil-dren who were delivered by a skilled attendant were regis-tered, as compared to 28 per cent of those who were not.Furthermore, the data also suggest that birth registration lev-els are associated with the number of vaccinations receivedand with the provision of vitamin A supplementation, as wellas with the level of medical care available. For example, inChad, 38 per cent of children receiving vitamin A supplemen-tation have been registered, compared to 15 per cent of thosenot receiving supplementation. Conversely, in the absence ofbirth registration, in many countries children are deniedaccess to vital interventions or programmes.
The challenges encountered by parents in registering thebirth of their children often signal and overlap with broader
patterns of social exclusion and lack of access to socialservices. Thus, particularly in remote areas, parents oftendo not see the benefits of their own citizenship, let alonethe benefits that birth registration would confer on theirchildren. Furthermore, even when parents do plan to regis-ter a birth, the high cost of registration and long distancesto registration centres often act as powerful deterrents.High cost in particular was revealed by a recent UNICEFanalysis to be the primary reason for the lack of birth regis-tration in no fewer than 20 developing countries, resultingin large registration disparities between rich and poor children. In the United Republic of Tanzania, where overallbirth registration is very low, there is a strong disparitybetween rich and poor, with only 2 per cent of the poorestfifth of children being registered compared to 25 per cent of the richest fifth.
Achieving universal birth registration requires governments,parents and communities to work together to make birthregistration a priority, and an integrated approach – such as combining national immunization campaigns with birthregistration campaigns – often provides the best strategy.Where such cooperation has been achieved, it has led toremarkable results even in the most trying circumstances. In Afghanistan, in 2003, a nationwide campaign to registerall children under the age of one was combined with thecountry’s National Polio Immunization Days. The campaignwas expanded in 2004 and had reached 2 million childrenunder five by mid-October of that year.
See References, page 105.

bringing child mortality rates in thepoorest 80 per cent of the populationup to par with those of the richest 20 per cent – would have a dramaticeffect on the under-five mortality rate for a country as a whole.34
Worldwide, about 40 per cent ofunder-five deaths could be preventedin this way.35
Children are also excluded fromhealth services by discrimination,geographic isolation, low levels ofparental education, AIDS at epidemiclevels and complex emergencies, suchas armed conflict and natural disas-ters. Many children are affected bythese circumstances simultaneously,which further decreases the likeli-hood that life-saving interventionswill reach them.
Successful approaches used to tackle these inequities include pro-grammes that bring health interven-
tions to those who are hardest toreach. Subsidizing health care forthe poor and directing social mar-keting to those who have beenexcluded are other options. Perhapsmost crucial is ensuring that equityis a priority in the design of childsurvival interventions and deliverystrategies. Doing so will require a thorough knowledge of the situa-tion through the collection of survey data, which can also be used for education and advocacy.Regular monitoring must be insti-tuted along with mechanisms toensure accountability, both atnational and international levels.
Rising to the challenge of
providing a continuum of care
for mothers, newborns and
children
These are the types of challenges thathealth-care providers face in reaching
children currently excluded fromessential services. The main challengeto child survival no longer lies indetermining the proximate causes of or solutions to child mortality butin ensuring that the services and edu-cation required for these solutionsreach the most marginalized coun-tries and communities. As the rest of this report will show, many coun-tries, including some of the poorestin the world, have made significantstrides in reaching large numbers ofchildren and families with essentialservices. Effective scale-up, however,requires that we learn from the lessons of recent decades – with aparticular emphasis on strengtheningintegrated approaches to child healthat the community level.
C H I L D S U R V I VA L : W H E R E W E S T A N D 2524 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
by Ellen Johnson-Sirleaf, President of Liberia
According to the Women’s Commission for RefugeeWomen and Children, based in New York, a society’s treat-ment of children is a reflection of its worth. In the case ofpost-conflict Liberia, the country’s fate is inextricably tied tothe fate of its most vulnerable population. The survival ofchildren in Liberia is a fundamental underpinning of ourdevelopment agenda because it shapes how we progressas a nation.
The impact of conflict on the survival of Liberia’s children is stark: At 235 deaths per 1,000 live births, Liberia’s under-five mortality rate is the fifth highest in the world; its infantmortality is the third highest and maternal mortality thetwenty-first highest. Maternal mortality trends are animportant benchmark for achieving Millennium DevelopmentGoal 4 and other health-related MDG targets for childrenbecause maternal health bolsters child survival – and without a sound policy on women’s development andempowerment, children in any post-conflict situation willultimately be neglected reminders of a nation’s failures.
It is disconcerting that, despite all the improvements inmodern medicine, children under five in Liberia still perishbecause of malaria (18 per cent of total deaths), diarrhoeaand vaccine-preventable diseases, such as measles, neona-tal tetanus, diphtheria, whooping cough and acute respira-tory infections. Underlying these conditions are chronicmalnutrition and vitamin and mineral deficiencies, whichare common in children under five. Fifty-one per cent of the population is food insecure. HIV infection in pregnantwomen is estimated at 5.7 per cent in 2007 compared to 4 per cent in 2004 – another example of the impact of 15years of conflict and the structural problems in the econo-my that disadvantage women and girls.
Access to basic health care is improving, but coverage anddistribution remain inadequate, especially in the rural areas.The task of achieving universal access is enormous, owingto such devastating effects of armed conflict as the destruc-tion of health infrastructure, low availability of trainedhealth workers and low public sector resources for health.The Government of Liberia is making strenuous efforts tosignificantly reduce child morbidity and mortality by 2011. Anational health policy and plan of action leading to universalaccess have been developed and are being implemented,while a national strategy and plan to accelerate child sur-vival has been developed. A strategy and plan of action to
serve as the ‘road map’ to reducing maternal mortality areunder way. Peace has allowed immunization for young children and pregnant women to increase significantly.
The challenges remain, however.
Safe water, essential for survival, had been available in the large population centres, including Monrovia, Liberia’scapital, prior to the conflict, but most of the piped systemswere destroyed. Currently, other than Monrovia, where thepiped water system is being gradually rehabilitated, urbancentres are without access to pipe-borne water. Childrencannot survive, much less thrive, without safe, potabledrinking water, which stands at a low 32 per cent currentlyin Liberia.
Health and education are the pillars of any sound child sur-vival strategy. The two are opposite sides of the same coinand must be tackled simultaneously in Liberia to ensureMDG 4. Illiteracy is high in the population, estimated at 68 per cent (male 55 per cent and female 81 per cent); literacy and education, especially of girls, are closely asso-ciated with improved child survival rates. The 2006 Girls’Education Policy aims to provide education to all girls. Inorder to ensure child survival, girl children also need to be protected. The conflict left many young girls pregnant or already mothers. Special efforts are needed to protect adolescent girls from sexual exploitation and abuse, frompregnancy and AIDS, both to ensure they enjoy their ownrights to survival and to guarantee the rights of their children.
There needs to be renewed momentum around the issue of child survival, and Liberia is leading that clarion call. Wewant to ensure that our children move beyond survival andinto a phase of development that enables them to thriveand transform into productive citizens.
Child survival in post-conflict situations: Liberia’s challenges
and triumphs
designed. This experience providedimportant lessons for planning the1978 International Conference onPrimary Health Care that tookplace in Alma-Ata, Union of SovietSocialist Republics (now Almaty,Kazakhstan).
Early in the century, such countriesas Denmark, the Netherlands,Norway and Sweden managed toreduce maternal mortality veryquickly. The way in which skilledattendance at birth was organizedappears to have been the major fac-tor contributing to these gains. In thecase of these four countries, effortsfocused on providing professionalcare close to where women lived,mainly by enhancing the skills ofcommunity midwives.2
Mass disease control
campaigns: 1950–1977
By 1950, the population of theworld exceeded 2.5 billion, andglobal average life expectancy hadrisen to 47 years.
The 1950s, 1960s and 1970s wit-nessed a number of disease controlefforts, often termed ‘mass campaigns’or ‘disease-focused responses’. Theseefforts employed scientifically sound,epidemiologically proven interventionsthrough free-standing programmesdesigned to combat a specific diseaseor condition. Often characterized by clearly defined goals, they includ-ed time-delineated targets for eitherthe reduction or the eradication ofthe disease, using a specific technol-
ogy delivered by dedicated healthworkers.3
The most successful of these cam-paigns was the smallpox eradicationinitiative, which reported its lastcase of human-to-human transmis-sion in 1977. Other mass campaignshave been successful in eradicatingor substantially reducing such illnesses as Guinea worm disease, trachoma and yaws.
The success of the smallpox eradica-tion campaign was a key elementinforming the design of possibly themost successful preventive publichealth programme in history – theExpanded Programme on Immuni-zation (EPI), launched in 1974. EPIinitially aimed to vaccinate children
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 29
mostly consisted of facility-basedcare. Training of local staff startedwith nursing schools. Because of theoverwhelming workload, male andfemale nurses were soon runningmost peripheral services. District governments in some countries start-ed clinics and small district hospitals,but in most countries mission hospi-tals provided 50–80 per cent of hospital beds. Public health focusedon environmental protection, in particular on early efforts to providesafe water and improved sanitationfacilities in urban areas.
Health services in francophone and other European colonies wereuniquely different from those inanglophone countries, since the latter placed great emphasis on
the Grandes Endémies programme.In this, separate levels of a national network focused on a single disease,such as sleeping sickness, elephantia-sis, leprosy and other high-prevalenceconditions affecting the capacity to work. Mass care was provided by mobile units, often generouslyequipped with complete travellingfacilities. The rationale was that relying on outreach to treat patientsat mass gatherings was more effectivein reaching larger numbers of peoplethan investing in static facilities.Repetitive cycles of treatment focusedon simple curative interventions ratherthan on prevention and control.
As in Africa, the early Chinese hospitals were mainly established by missions. A national public health
system began in the 1920s withefforts to control the rapidly spread-ing pneumonic plague in the provinceof Manchuria.
An important historical footnote isthat the first published case study of successful community-based pri-mary health care concerns a projectof this period. The project tookplace in Ding Xian (formerly TingHsien), about 200 kilometres southof Beijing. In this province of abouthalf a million people, health carewas provided by health workerswho were the forerunners ofChina’s ‘barefoot doctors’. For aquarter of a century and for morethan a fifth of the world’s popula-tion, China had one of the mostequitable health systems ever
28 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The Measles Initiative shows how a well resourced, targetedand managed global vertical initiative can reach scale rapidlyand produce dramatic results. The initiative is a partnership that groups UNICEF and WHO with other leading internationalagencies and prominent private organizations. Launched in2001, the Measles Initiative adopted the goal set at the UNGeneral Assembly Special Session on Children in May 2002 toreduce deaths due to measles among children between 1999and 2005. It has been the main sponsor of the mass cam-paign to boost measles vaccination, which has resulted in vaccinating more than 217 million children between 2001 and 2005 – mostly in Africa.
The results have exceeded the UN target: Measles deaths fell by 60 per cent between 1999–2005. Africa contributed 72 per cent of the absolute reduction in deaths. Estimatesconcluded that immunization helped avert almost 7.5 milliondeaths from the disease.
The reduction in measles deaths reflects support and com-mitment by the Measles Initiative to boosting immunizationcoverage and by national governments to following theWHO/UNICEF comprehensive strategy for reducing measlesmortality. The strategy consists of four key components:
• Provide at least one dose of measles vaccine, administeredat nine months of age or shortly after, through routine vaccination coverage of at least 90 per cent of children ineach district and nationally.
• Give all children a second opportunity for measles vaccination.
• Establish effective surveillance.
• Improve clinical management of complicated cases –including vitamin A supplementation.
Measles control activities are contributing to health-systemdevelopment in several ways – for example, through promoting safe injection practices, developing enhanced cold chain capacity for vaccination storage and establishingthe development of a global public health laboratory network. In addition, vaccination campaigns are often combined with such other essential interventions as vitamin A supplementation, deworming medicines and the distribution of insecticide-treated mosquito nets.
A new global goal was set at the World Health Assembly inMay 2005 – to reduce measles deaths by 90 per cent by 2010,
The Measles Initiative
compared to 2000 data. The target is challenging, and itsattainment will require sustaining the progress made in thosecountries that performed well and making large inroads incountries with high numbers of measles deaths, such as India
and Pakistan. There is some way to go in the fight againstmeasles – 345,000 people died of the disease in 2005, and 90 per cent of them were children under five. This highly contagious disease remains an important cause of under-fivedeaths, accounting for about 4 per cent of the global burden.It weakens children’s immunity to other life-threatening dis-eases and conditions, including pneumonia, diarrhoea andacute encephalitis, and remains one of the leading causes of vaccine preventable deaths among children.
The success of efforts to reduce measles in 1999–2005 hasshown what can be done if political will, financial commitmentand sound strategies on the part of international partners andnational governments are implemented to deliver proven,cost-effective treatments. Provided that this degree of commit-ment is sustained, there is every reason to believe that thenew target can be met, helping advance progress towardsMillennium Development Goal 4.
See References, page 106.
Children under five account for 90 per cent of measles deaths
Western Pacific, 5,000 (1%)
Americas, <1,000 (<0.15%)
Eastern Mediterranean, 39,000 (11%)
Africa, 126,000 (37%)
South-East Asia, 174,000(51%)
Europe, <1,000 (<0.15% )
Figure 2.1
Global burden of measles deaths*
Source: World Health Organization estimates published in The Lancet,vol. 369, 20 January 2007, p. 194
* Regions refer to World Health Organization regions.
collaboration and integration in thegeneral health-delivery system.
A long-standing example of thegreater emphasis on integration dur-ing the 1990s is IMCI, the IntegratedManagement of Childhood Illness.Developed in 1992 by UNICEF andWHO, and employed in more than100 countries since then, IMCIadopts a broad, cross-cuttingapproach to case management ofchildhood illness, acknowledgingthat there is usually more than onecontributing cause.15 Indeed, inmany cases, sick children exhibitoverlapping symptoms of disease,complicating efforts to arrive at asingle diagnosis even in communitieswith adequate first-level examination
facilities, let alone those with morechallenging circumstances.
IMCI strategies have three pri-mary components, each of whichrequires adaptation to the countrycontext:
• Improving health worker perform-ance: This involves training healthworkers to assess symptoms ofdiseases, correct mapping of illnessto treatment, and provision ofappropriate treatment to childrenand information to the caregivers.Through provision of locallyadapted guidelines, health staff aretaught case management skills forfive major causes of childhoodmortality: acute respiratory
infections, especially pneumonia;diarrhoeal diseases; measles;malaria; and undernutrition.
• Improving health systems: Thiscomponent seeks to strengthenhealth systems for effective man-agement of childhood illnesses.Measures employed include sup-porting drug availability, enhancingsupervision, strengthening referraland deepening health informationsystems. Planning guides are pro-vided for managers at the districtand national levels.
• Improving community and familypractices: The final component isoften referred to as CommunityIntegrated Management of
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 33
the sharp fall in the global under-fivemortality rate, from 115 per 1,000live births in 1980 to 93 in 1990 – a reduction of 19 per cent over thecourse of the decade.
Focusing on integrated,
sector-wide approaches
and health systems: 1990s
Despite the gains of selective primaryhealth care, by the late 1980s, healthsystems in many developing countrieswere under severe stress. Populationgrowth, the debt crisis in many LatinAmerican and sub-Saharan Africancountries, and political and economictransition in the former Soviet Unionand Central and Eastern Europe werebut three of the contributing factors.
In response, a number of countriesembarked on efforts to reform deteri-orating, under-resourced health systems, raise their effectiveness, efficiency and financial viability, and increase their equity.
The Bamako Initiative
One such approach used by manycountries was the Bamako Initiative,which was launched in 1987 at theWorld Health Organization meeting ofAfrican health ministers in Bamako,Mali. This strategy focused on increas-ing access to primary health care andmeeting basic community needs insub-Saharan Africa by delivering anintegrated minimum health-care pack-age through health centres. A strongemphasis was placed on access to
drugs and regular contact betweenhealth-care providers and communi-ties. (See Panel, page 36, for furtherdetails on the Bamako Initiative.)
Integration
The emphasis on integrating essentialservices that was a central feature ofthe Bamako Initiative was to becomethe driving force of approaches in the1990s. Integrated approaches soughtto combine the merits of selective pri-mary care and primary health care.Like selective approaches, they placeda strong emphasis on providing a coregroup of cost-effective solutions in atimely way to address specific healthchallenges; like primary health care,they also focused attention on com-munity participation, intersectoral
32 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
National immunization days (NIDs) originated as one-daymass polio vaccination campaigns across the developingworld. NIDs, which still take place in many countries, aresupplementary and do not replace routine immunization.Their original aim was to prevent the spread of polio byimmunizing all children under the age of five, regardlessof their previous polio vaccination history.
The concept of setting aside a day for mass interventionson child health is not new. Successful trials of days took place in the 1980s in such places as Burkina Faso,Colombia and Turkey. More recently, active civil wars havebeen halted to provide days of tranquility that allow chil-dren to be safely vaccinated in such countries as Angola,Sierra Leone and Somalia. Mass vaccinations allow foreconomies of scale, as skilled professionals can supervisea cadre of volunteers, especially for oral polio vaccine,which does not require a needle and syringe.
Child health days have expanded the scope of interven-tions beyond polio immunization to include vitamin Asupplementation, and in the case of Zimbabwe, distribu-tion of insecticide-treated mosquito nets and otherimmunizations. Other countries that conduct similarevents include Nepal and Nigeria.
Nepal’s national vitamin A programme is particularlynoteworthy because it employs an existing network of female community health volunteers to deliver thesupplements. The programme is found to be highly cost-effective, with a cost per death averted estimated at US$327–$397, while the cost per disability-adjusted life year (DALY) gained was approximately US$11–$12. The programme was steadily expanded, from the origi-nal 32 priority districts to cover all 75 districts, in annualincrements of 8–10 districts over an eight-year period.Expansion was assisted by using national immunizationdays to advance coverage.
Integrating the delivery of a range of interventions in a single location and at a single point in time, childhealth days are efficient for both households andhealth service providers. Related concepts, such aschild health weeks, are enhancing the opportunities toreach a large number of usually excluded children withessential interventions.
See References, page 106.
National immunization days and child health days
During the 1990s, concerns escalated about the potentialpredominance of vertical approaches, which tend to cre-ate and utilize managerial, operational and logisticalstructures separate from those of the national health system to address disease control. These concerns con-tributed to the development of a new mode of healthfinancing: sector-wide approaches (SWAps). UnderSWAps, the major funding contributions for the healthsector support a single plan for sector policy, strategy andexpenditure backed by government leadership. Commonapproaches to health service delivery are adopted acrossthe sector, and government procedures increasingly con-trol the disbursement and accounting of funds.
SWAps were created for several purposes: to address thelimitations of project-based forms of donor assistance,ensure that overall health reform goals were met, reducelarge transaction costs for countries and establish gen-uine partnerships between donors and countries inwhich both had rights and responsibilities. SWAps are a dynamic process rather than an end point, and theydisplay considerable variation across countries. SWApshave led to greater dialogue and trust, a sharper focus on
a select number of key sector priorities and closer linksbetween policy and implementation. However, con-straints include an overemphasis on details in planningand the development of procedures; limited civil societyparticipation; weak performance management; and aslow shift from emphasizing donor coordination to considering service improvement and results.
At the end of the 1990s, in the context of the HeavilyIndebted Poor Countries Initiative implemented by theInternational Monetary Fund and the World Bank, thefocus on the health sector and financing reform in manylow-income countries broadened to include PovertyReduction Strategy Papers (PRSPs). Medium-term expenditure frameworks, the multi-annual public plan-ning instruments associated with PRSPs, are used to planfuture budget requirements for public services and toassess the resource implications of policy changes andnew programmes.
See References, page 106.
Health sector financing: Sector-wide approaches and the Heavily
Indebted Poor Countries Initiative
collaboration and integration in thegeneral health-delivery system.
A long-standing example of thegreater emphasis on integration dur-ing the 1990s is IMCI, the IntegratedManagement of Childhood Illness.Developed in 1992 by UNICEF andWHO, and employed in more than100 countries since then, IMCIadopts a broad, cross-cuttingapproach to case management ofchildhood illness, acknowledgingthat there is usually more than onecontributing cause.15 Indeed, inmany cases, sick children exhibitoverlapping symptoms of disease,complicating efforts to arrive at asingle diagnosis even in communitieswith adequate first-level examination
facilities, let alone those with morechallenging circumstances.
IMCI strategies have three pri-mary components, each of whichrequires adaptation to the countrycontext:
• Improving health worker perform-ance: This involves training healthworkers to assess symptoms ofdiseases, correct mapping of illnessto treatment, and provision ofappropriate treatment to childrenand information to the caregivers.Through provision of locallyadapted guidelines, health staff aretaught case management skills forfive major causes of childhoodmortality: acute respiratory
infections, especially pneumonia;diarrhoeal diseases; measles;malaria; and undernutrition.
• Improving health systems: Thiscomponent seeks to strengthenhealth systems for effective man-agement of childhood illnesses.Measures employed include sup-porting drug availability, enhancingsupervision, strengthening referraland deepening health informationsystems. Planning guides are pro-vided for managers at the districtand national levels.
• Improving community and familypractices: The final component isoften referred to as CommunityIntegrated Management of
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 33
the sharp fall in the global under-fivemortality rate, from 115 per 1,000live births in 1980 to 93 in 1990 – a reduction of 19 per cent over thecourse of the decade.
Focusing on integrated,
sector-wide approaches
and health systems: 1990s
Despite the gains of selective primaryhealth care, by the late 1980s, healthsystems in many developing countrieswere under severe stress. Populationgrowth, the debt crisis in many LatinAmerican and sub-Saharan Africancountries, and political and economictransition in the former Soviet Unionand Central and Eastern Europe werebut three of the contributing factors.
In response, a number of countriesembarked on efforts to reform deteri-orating, under-resourced health systems, raise their effectiveness, efficiency and financial viability, and increase their equity.
The Bamako Initiative
One such approach used by manycountries was the Bamako Initiative,which was launched in 1987 at theWorld Health Organization meeting ofAfrican health ministers in Bamako,Mali. This strategy focused on increas-ing access to primary health care andmeeting basic community needs insub-Saharan Africa by delivering anintegrated minimum health-care pack-age through health centres. A strongemphasis was placed on access to
drugs and regular contact betweenhealth-care providers and communi-ties. (See Panel, page 36, for furtherdetails on the Bamako Initiative.)
Integration
The emphasis on integrating essentialservices that was a central feature ofthe Bamako Initiative was to becomethe driving force of approaches in the1990s. Integrated approaches soughtto combine the merits of selective pri-mary care and primary health care.Like selective approaches, they placeda strong emphasis on providing a coregroup of cost-effective solutions in atimely way to address specific healthchallenges; like primary health care,they also focused attention on com-munity participation, intersectoral
32 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
National immunization days (NIDs) originated as one-daymass polio vaccination campaigns across the developingworld. NIDs, which still take place in many countries, aresupplementary and do not replace routine immunization.Their original aim was to prevent the spread of polio byimmunizing all children under the age of five, regardlessof their previous polio vaccination history.
The concept of setting aside a day for mass interventionson child health is not new. Successful trials of days took place in the 1980s in such places as Burkina Faso,Colombia and Turkey. More recently, active civil wars havebeen halted to provide days of tranquility that allow chil-dren to be safely vaccinated in such countries as Angola,Sierra Leone and Somalia. Mass vaccinations allow foreconomies of scale, as skilled professionals can supervisea cadre of volunteers, especially for oral polio vaccine,which does not require a needle and syringe.
Child health days have expanded the scope of interven-tions beyond polio immunization to include vitamin Asupplementation, and in the case of Zimbabwe, distribu-tion of insecticide-treated mosquito nets and otherimmunizations. Other countries that conduct similarevents include Nepal and Nigeria.
Nepal’s national vitamin A programme is particularlynoteworthy because it employs an existing network of female community health volunteers to deliver thesupplements. The programme is found to be highly cost-effective, with a cost per death averted estimated at US$327–$397, while the cost per disability-adjusted life year (DALY) gained was approximately US$11–$12. The programme was steadily expanded, from the origi-nal 32 priority districts to cover all 75 districts, in annualincrements of 8–10 districts over an eight-year period.Expansion was assisted by using national immunizationdays to advance coverage.
Integrating the delivery of a range of interventions in a single location and at a single point in time, childhealth days are efficient for both households andhealth service providers. Related concepts, such aschild health weeks, are enhancing the opportunities toreach a large number of usually excluded children withessential interventions.
See References, page 106.
National immunization days and child health days
During the 1990s, concerns escalated about the potentialpredominance of vertical approaches, which tend to cre-ate and utilize managerial, operational and logisticalstructures separate from those of the national health system to address disease control. These concerns con-tributed to the development of a new mode of healthfinancing: sector-wide approaches (SWAps). UnderSWAps, the major funding contributions for the healthsector support a single plan for sector policy, strategy andexpenditure backed by government leadership. Commonapproaches to health service delivery are adopted acrossthe sector, and government procedures increasingly con-trol the disbursement and accounting of funds.
SWAps were created for several purposes: to address thelimitations of project-based forms of donor assistance,ensure that overall health reform goals were met, reducelarge transaction costs for countries and establish gen-uine partnerships between donors and countries inwhich both had rights and responsibilities. SWAps are a dynamic process rather than an end point, and theydisplay considerable variation across countries. SWApshave led to greater dialogue and trust, a sharper focus on
a select number of key sector priorities and closer linksbetween policy and implementation. However, con-straints include an overemphasis on details in planningand the development of procedures; limited civil societyparticipation; weak performance management; and aslow shift from emphasizing donor coordination to considering service improvement and results.
At the end of the 1990s, in the context of the HeavilyIndebted Poor Countries Initiative implemented by theInternational Monetary Fund and the World Bank, thefocus on the health sector and financing reform in manylow-income countries broadened to include PovertyReduction Strategy Papers (PRSPs). Medium-term expenditure frameworks, the multi-annual public plan-ning instruments associated with PRSPs, are used to planfuture budget requirements for public services and toassess the resource implications of policy changes andnew programmes.
See References, page 106.
Health sector financing: Sector-wide approaches and the Heavily
Indebted Poor Countries Initiative
clearly defined roles for IMCI andother child health interventions, andthe need to critically analyse andaddress the system constraints.21
Stimulated by a series of studies onmaternal, newborn and child survivalpublished by The Lancet, integratedmodels of health care have beendeveloped within the context of thematernal, newborn and child healthcontinuum of care (see Chapter 1,page 17 for further details on thecontinuum of care and the partner-ship). In effect, the continuum of care concept expands IMCI toinclude integrated management of neonatal illness.22 Successful preliminary experience with the new approach, called the IntegratedManagement of Neonatal andChildhood Illnesses (IMNCI) hasbeen pioneered and fully implement-ed in India (see Panel above).
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 35
Childhood Illness (C-IMCI). It is based on the basic householdpractices for families and commu-nities outlined in the Panel inChapter 3, page 47.16
The integration of case managementseeks to protect children from, andoffer treatment for, all major diseases,not just one or two. It also empha-sizes adapting curative solutions tothe capacity and functions of localhealth systems, along with promotingdisease prevention by educatinghealth workers and caregivers on the importance of essential services.The role of parents and other primary
caregivers in detecting commonsymptoms of ill health, taking childrento health facilities and implementingsuch preventive measures as appro-priate feeding and hygiene practicesis critical.
Integrated Management ofChildhood Illness has been rigorous-ly evaluated since its inception in the mid-1990s. Several agencies –including WHO, UNICEF, the United Kingdom’s Department forInternational Development (DFID)and the United States Agency forInternational Development (USAID)– conducted multicountry evalua-
tions in the early 2000s. In 2004and 2005, UNICEF also reviewedthe community and family compo-nent (C-IMCI).17 Although initialresults were disappointing, mainlybecause of incomplete implementa-tion of the three core IMCI com-ponents, later results have demon-strated some notable successes.According to studies, IMCI casemanagement has enhanced the quality of health care delivered in first-level facilities, motivatedhealth workers and managers, andimproved health worker perform-ance. And it has been implementedat costs equivalent to or lower thanthose of existing services.18
Positive results for IMCI have beennoted in several countries in sub-Saharan Africa. A study conducted inrural districts of the United Republicof Tanzania, for example, found thatthose districts implementing a health-system-strengthening initiative andIMCI demonstrated a 13 per centgreater reduction in child mortalitythan control districts.19
Survey results in Malawi, SouthAfrica, the United Republic ofTanzania and Uganda indicated that wide-scale implementation of the C-IMCI strategy can result in sig-nificant improvement in some of thekey family practices, such as steps toimprove nutrition and early survival,disease prevention, home care or care-seeking for sick children, and provi-sion of a supportive environment forchild growth and development.20
Successes such as these have ledhealth policy experts to recommendthe development of national policiesbased on country priorities, with
34 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
© U
NIC
EF/
HQ
06-2
720/
She
hzad
Noo
rani
Approaches to the delivery of primary health care must be tailored to the needs andresources of each individual country and community. A nurse measures the blood pressureof a pregnant woman, Bangladesh.
Selective primary health care and trends in immunization
rates since 1980
Source: Data provided by Strategic Information Section, United Nations Children’s Fund.
0
10
20
30
40
50
60
70
80
90
1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006
% o
f o
ne-
year
-old
ch
ildre
n im
mu
niz
ed
Selective primary health
care takes root in the
form of GOBI (growth
monitoring, oral
rehydration therapy,
breastfeeding and
immunization.
GOBI and the Expanded
Programme on Immuniza-
tion contributed to rapid
advances in immunization
coverage in the 1980s.
After stagnating in the first half of the 1990s,
immunization coverage has been rising
slowly but steadily over the past 10 years.
Global DPT3 coverage
Global measles immunization coverage
Figure 2.2
During the 1990s, India experienced marked reduction inthe under-five mortality and infant mortality rates. Thesetrends were not been matched by declines in the rate ofneonatal deaths. By 2000, neonatal deaths were around two thirds of all infant deaths in the country, and around 45 per cent of under-five deaths. Close to half of neonataldeaths occur in the first week of life. Many of these deathscould be averted if parents recognized warning signs,undertook appropriate feeding practices or had access to skilled health workers and facility-based care.
In 2000, the Government of India adapted the IntegratedManagement of Childhood Illness (IMCI) strategy to focusgreater attention on neonatal care. The resulting approach,Integrated Management of Neonatal and ChildhoodIllnesses (IMNCI), modifies IMCI with specific actions takento promote neonatal health and survival. Like IMCI, IMNCIsupports three pillars for the effective delivery of essentialservices to neonates, infants and young children: strength-ening health-system infrastructure, enhancing the skills of
health workers and promoting community participation – allwith additional emphasis on neonatal health and survival.
In practice, IMNCI consists of three home visits in the first10 days after birth to promote best practices for the youngchild; a special provision at the village level for follow-up ofinfants with low birthweights; reinforcement of messagesthrough meetings of women’s groups and establishing alinkage between the village and the home; and assessmentof the child at local health facilities based on referral.
IMNCI is incorporated as part of the government’sReproductive and Child Health II programme, an integratedapproach to women’s health that aims to provide a continu-um of care from birth until adulthood. The additional costof adding the newborn component, mostly the home visits,is just US$0.10 per child.
See References, page 106.
Integrated Management of Neonatal and Childhood Illnesses in India

The Millennium Development
Goals and results-based
approaches: 2000 and beyond
By 2000, global life expectancy hadincreased from 47 years in the early1950s to around 65 years. However,many countries had failed to share inthe health gains that contributed tothis increase in longevity, and the AIDSpandemic threatened to reverse thegains in high-prevalence areas. Thisprompted the inclusion of three health-related goals in the eight MillenniumDevelopment Goals that were adoptedby 189 countries in 2000, with the target deadline of 2015 (See Figure 1.9, page 9, for the full list of thehealth-related MDGs and their associated indicators.)
As Chapter 1 explained, progresstowards the health-related MDGs hasbeen less rapid than the architects ofthe MDGs had hoped. There are seri-ous concerns that without a concert-ed, sustained drive to expand accessto essential interventions to the mil-lions of mothers and children whoare currently missing out, the goals,particularly in sub-Saharan Africa,will be missed by a wide margin.
In recent years, a number of high-levelmeetings have taken place to identifyopportunities for achieving the MDGs,explore best practices, make commit-ments to measurable results at thecountry level and support the pertinentinstitutional adjustments required atcountry, regional or global levels. A keyconcern of these meetings is progress insub-Saharan Africa, the region with thehighest rates of maternal, newborn andchild mortality and the one making the least progress towards the health-related Millennium Development
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 3736 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The Bamako Initiative, sponsored by UNICEF and WHOand adopted by African ministers of health in 1987, wasbased on the realization that, despite accepting in princi-ple the core tenets of comprehensive primary healthcare, by the late 1980s many countries – especially insub-Saharan Africa – were burdened by a lack ofresources and practical implementation strategies. In particular, many health facilities lacked the resources and supplies to function effectively. As a result, healthworkers were sometimes merely prescribing drugs to be bought from private outlets, often unlicensed and unsupervised, while many patients had lost confidence in the inefficient and under-resourced public health facili-ties. All of these developments threatened to reverse thegains of the 1980s. The core challenges were to promoteadditional donor investment, stop and reverse thedecline of government expenditure on social spending ingeneral and health in particular, and attract the moneyspent in the private and informal sectors back into thepublic system.
The Bamako Initiative aimed to increase access to pri-mary health care by raising the effectiveness, efficiency,financial viability and equity of health services. Bamakohealth centres implemented an integrated minimum-health-care package in order to meet basic communityhealth needs, focusing on access to drugs and regularcontact between health-care providers and communities.Based on the concept that communities should participatedirectly in the management and funding of essential drugsupplies, village committees engaged in all aspects ofhealth-facility management, with positive results for childhealth in West Africa in particular.
The purpose of community financing was to capture afraction of the funds households were already spendingin the informal sector and combine them with governmentand donor funding to revitalize health services andimprove their quality. The most effective interventionswere priced below private sector charges and cross-subsidized through higher markup and higher co-paymentson lower priority interventions. Immunization and oralrehydration therapy were supplied free of charge. Localcriteria for exempting the poor were established by thecommunities.
Although countries followed different paths in implement-ing the Bamako Initiative, in practice they had a commoncore objective: providing a basic package of integratedservices through revitalized health centres that employuser fees and community co-management of funds. A
number of common support structures were organizedaround this core agenda, including the supply of essentialdrugs, training and supervision, and monitoring.
‘Going to scale’ was a critical step in the implementationprocess. The pace of expansion varied depending on the availability of internal and external resources, localcapacity, the need to work at the speed of communityneeds and pressure from governments and donors. Most of the sub-Saharan countries that adopted theBamako Initiative employed some form of phased scaling up, and several countries – most notably Benin,Mali and Rwanda – achieved significant results.
In essence, implementing the Bamako Initiative was apolitical process that involved changing the prevailingpatterns of authority and power. Community participa-tion in the management and control of resources at the health-facility level was the main mechanism forensuring accountability of public health services to users. Health committees representing communitieswere able to hold monitoring sessions during which coverage targets, inputs and expenditures were set,reviewed, analysed and compared. It is estimated thatthe initiative improved the access, availability, afford-ability and use of health services in large parts of Africa, raised and sustained immunization coverage, and increased the use of services among children andwomen in the poorest fifth of the populace.
The Bamako Initiative was not without its limitations. Theapplication of user fees to poor households and the prin-ciples of cost recovery drew strong criticism, and thoughmany African countries adopted the approach, only in ahandful were initiatives scaled up. Even in those coun-tries where Bamako has been deemed a success, poorpeople viewed price as a barrier in the early 2000s, and alarge share did not use essential health services despiteexemptions and subsidies. The challenge that Benin,Guinea and Mali still face, along with other Africannations that adopted the Bamako Initiative, is to protectthe poorest and ensure that costs do not prevent accessto essential primary health-care services for poor andmarginalized communities.
See References, page 106.
The Bamako Initiative
THE INTEGRATED CASE MANAGEMENT PROCESS
OUTPATIENT HEALTH FACILITY
Check for DANGER SIGNS
• Convulsions • Lethargy/unconsciousness • Inability to drink/breastfeed
• Vomiting
Assess MAIN SYMPTOMS
• Cough/difficulty breathing • Diarrhoea
• Fever • Ear problems
Assess NUTRITION and
IMMUNIZATION STATUS and
POTENTIAL FEEDING PROBLEMS
Check for OTHER PROBLEMS
Home management
HOME
Caretaker is counselled on:• Home treatment(s)• Feeding and fluids
• When to return immediately• Follow-up
Urgent referral
OUTPATIENT
HEALTH FACILITY
• Pre-referral treatments• Advise parents
• Refer child
Treatment at outpatient
health facility
OUTPATIENT
HEALTH FACILITY
• Treat local infection• Give oral drugs
• Advise and teach caretaker• Follow up
REFERRAL FACILITY
• Emergency Triage andTreatment• Diagnosis• Treatment
• Monitoring and follow-up
CLASSIFY CONDITIONS and
IDENTIFY TREATMENT ACTIONS
Figure 2.3
IMCI case management in the outpatient health facility,
first-level referral facility and at home for the sick child
from age two months up to five years
Source: World Health Organization and United Nation Children’s Fund, Model Chapter for Textbooks: Integrated Management of Childhood Illness. WHO and UNICEF, Geneva and New York, 2001, p. 6.
Towards a unified framework
for ensuring health outcomes
for mothers, newborns and
children
In recent years, governments anddevelopment partners have renewedtheir commitment to achieving thehealth-related MDGs and ensuringthat their renewed resolve wouldtranslate effectively into joint orcoordinated regional strategies. Atthe same time, experts in maternal,newborn and child health are increas-ingly coalescing around a set ofstrategic principles based on the lessons of the past century. Theseprinciples are threefold, namely:
A renewed recognition of the princi-ples of primary health care, whichemphasize the primacy of family andcommunity partnership in the sur-vival, growth and development ofchildren.27 This has triggered arenewed interest in another principleof primary health care, namely theneed for community partnerships tosupport families in improving theircare practices for children and tohold health systems accountable for providing quality affordable services.(Chapter 3 examines communitypartnerships in support of maternal,newborn and child health and family-care practices.)
The ‘health systems development foroutcomes’ approach to health-servicedelivery combines the strengths ofselective/vertical and comprehensive/horizontal approaches. This newapproach is being adopted as theframework for scaling up cost-effectiveintervention packages and integratingthem into a continuum of care formothers, newborns and children. Itemphasizes the expansion of evidence-based, high-impact health, nutrition,HIV and AIDS, and water, sanitationand hygiene interventions and prac-tices, and underlines the importance ofremoving system-wide bottlenecks tohealth-care provision and usage. If
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 39
Goals. At the current pace, most of the 46 countries in sub-Saharan Africa– along with Sudan – will fail to meetmost of the MDGs. Current projec-tions indicate that sub-Saharan Africa’spoverty rate as measured by the pro-portion of people living on less than adollar a day will reach almost 40 per cent in 2015.23 In some countries,
under-five mortality rates have stagnat-ed or even reversed, and paediatricAIDS deaths continue to increase.
Despite this rather bleak outlook,there is hope from the experience ofother countries, whose targettedapproaches have brought about sig-nificant declines in under-five mortal-
ity rates.24 In recent years, severalcomprehensive reviews of evidence-based child survival interventionshave reaffirmed that existing low-cost interventions can avert up totwo thirds of under-five mortalityand over half of neonatal mortality.25
In addition, 88 up to 98 per cent ofmaternal deaths are preventable.26
38 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
According to one of its leading proponents, JaimeSepulveda of Mexico’s National Institute of Health, the diagonal approach is a “proactive, supply-driven provision of a set of highly cost-effective interventions on a large scale bridging health clinics and homes.”
Vertical interventions are often the starting point of diagonal approaches, with the caveat that the number ofthese interventions be expanded over time with supportfrom existing facilities and field workers. The diagonalapproach stresses the importance of integration andcoordination between vertical interventions, community-based initiatives and health facilities or extension services.It addresses a number of key issues by applying specificintervention priorities, including drug supply, facilityplanning, financing, human resources development,quality assurance and rational prescription.
In the 25 years from 1980–2005, Mexico implemented a number of successful vertical programmes that weresubsequently scaled up. These programmes targeteddiarrhoeal diseases (the distribution of oral rehydrationsalts and the Clean Water programme); vaccine preventa-ble diseases (national vaccination days, measles vaccina-tion campaigns, the Universal Vaccination Programme,national health weeks); vitamin A supplementation andanthelmintic therapy (national health weeks).
PROGRESA – a conditional cash transfer programmedesigned to engage the country’s poorest families – pro-vided financial incentives for improved health and nutri-tion practices, and for keeping children in school. Benefitsare contingent on regular attendance at health clinics thatsupply essential health and nutrition services. Food sup-plements are distributed to all children aged 6–23 monthsand underweight children aged 2–4 years in targetedhouseholds. The programme has been associated with a strong positive impact on children’s nutritional status.
A more comprehensive package covering the continu-um of maternal, neonatal and child health has beenintroduced since 2001, when the Ministry of Healthlaunched Arranque Parejo en la Vida (Equal Start inLife). This initiative promotes social and communityparticipation, strengthens and expands antenatal andneonatal care, and provides folic acid supplementationfor women, among other factors. It has reached a highlevel of coverage. Through Seguro Popular, a publichealth insurance initiative, maternal and child healthbecame entitlements.
In part, the diagonal approach has emerged as aresult of research into Mexico’s health system and itsdevelopment during the past 25 years. Unlike otherapproaches, its genesis appears to have emerged as apractical response to the growing complexity of dis-ease profiles and the pressure faced by the country todevelop health interventions and systems that providequality services, are affordable, and reach the poorestand most marginalized populations.
Its implementation has led to Mexico being one ofonly seven countries on track to reach the MillenniumDevelopment Goals among the 60 nations selected in 2005 for priority attention by the Child SurvivalCountdown to 2015. The diagonal approach is nowformalized and being championed by Mexico’s formerMinister of Health, Julio Frenk, who considers that theframework should be integrated into a broader healthpolicy. It aims to bridge the dichotomies between horizontal and vertical approaches, intersectoral andsectoral policies, and national and international effortsby offering a ‘third way’ through which effective interventions become the drivers for health-systemdevelopment.
See References, page 106.
Diagonal approaches: The Mexican way
Actions at the macro level: Policies and
financingActions at the meso level:
Health system and other sectors
Achieve the
health-related
Millennium
Development Goals
1. Eradicate hunger
4. Reduce under-five mortality
5. Improve maternal health
6. Combat HIV andAIDS, malaria andother diseases
7. Ensureenvironmentalsustainability
Actions at the microlevel: Households and
communities
Family/
community-level care
Population-oriented
(outreach)services
Individual (clinical) care Procurement and supplies
Infrastructure and logistics
Social mobilization
Equitable financing
mechanisms
Training and supervision
Monitoring and information systems
Protect household
income
MDG1: Eradicateextreme poverty
MDG focused and
evidence based
National policies,strategies and plans
Poverty ReductionStrategy Papers(PRSPs)
Sector-wideapproaches(SWAps)
Budget support
Medium-termexpenditureframework (MTEF)
Target health,nutrition andpopulationoutcomes:Millennium
Development Goals
Conceptual framework for achieving health-related Millennium Development Goals
Figure 2.4
jointly scaled up and widely applied,these interventions are expected tohave a dual and synergistic impact not only on child survival but also onchildren’s growth and development.
This approach defies the long-standing dichotomy between verticalapproaches to achieve outcomes andintegrated approaches to strengthensystems, arguing that both aims canbe realized by adapting health systemsto achieve results. It also recognizesthat optimal child survival, growthand development are more likely to beachieved and sustained if preventivemeasures are available to future moth-ers (i.e., adolescent girls and youngwomen) before their children are bornand if they benefit from a continuumof care that is part of an evolving integrated approach to reproductive,maternal, newborn and child health.(Chapter 4 elaborates on how to takethese strategies to scale.)
Enhance ways of working at thenational and international levels, witha strong focus on coordination, har-monization and results. A new way ofworking for the global community isneeded to support countries in goingto scale with diagonal approaches toprimary health care. Harmonizationof the multitude of health-relatedglobal initiatives and partnerships,and of donor support to health-related MDGs, is pivotal to a unifiedparadigm. Other requisites include:
• Stronger support to developingcountries in national planning, pol-icy and budgeting frameworks forthe health-related MDGs.
• Aligning donors to support coun-tries’ own priorities and plans and
provide predictable long-term fund-ing for health-related MDGs.
• Strengthening health systems andother sectors for MDG outcomes.
• Improving the effectiveness andefficiency of multilateral support ina context of UN harmonization bystimulating a global collective senseof urgency for reaching the health-related MDGs.
• Changing institutional ways ofdoing business so as to achieve theMDGs; developing a more system-atic and robust approach to knowl-edge management and learning.
• Seizing the opportunity presentedby the renewed interest in healthoutcomes.
• Recognizing that the role playedby civil society and the private
sector will be critical for success.(Chapter 5 discusses this new wayof working.)
Figure 2.4 demonstrates the comple-mentarity of these new strategic princi-ples to achieve the health-relatedMillennium Development Goals. Itmakes clear that though the MDGswill be primarily determined at thehousehold and community level, theirattainment requires that families andcommunities receive support fromhealth systems and other sectors.Policies and financing at both globaland national levels are needed toenable health systems and other sectorsto support families and communitiesand ensure accountability for results.28
Building on the lessons learned
As this brief review has shown, thepublic health community is continu-ally learning and evolving. There is
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 4140 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
A more recent example of an integrated approach to pri-mary health care is the Accelerated Child Survival andDevelopment (ACSD) initiative, which was launched bynational governments in cooperation with UNICEF in Westand Central Africa and aims to reduce infant (under-one),under-five and maternal mortality rates. The programmeoriginated when the Canadian International DevelopmentAgency (CIDA) asked UNICEF to develop an innovativeproject that would reduce child mortality. It was initiated in2002 in four countries, covering 16 districts and 3 millionpeople. Since then, ACSD has grown rapidly and by 2004was targeting more than 16 million people in selected districts in 11 countries of West and Central Africa thathave high rates of under-five mortality. ACSD concentrateson three service-delivery strategies to augment coveragefor women and children:
• Community-based promotion of a package of family healthand nutrition practices, employing mostly volunteers.
• Outreach and campaigns to provide essential services andproducts, such as immunization, vitamin A, anthelmintictreatment and selected prenatal services.
• Facility-based delivery of an integrated minimum-care pack-age consisting of all the selected priority interventions.
These priority interventions are also organized around threeareas that build on the strengths of existing programmesand approaches:
• Antenatal Care plus (ANC+), which provides intermittentpreventive treatment of malaria during pregnancy, ironand folic acid supplementation, tetanus vaccine and pre-vention of mother-to-child transmission of HIV.
• Expanded Programme on Immunization plus (EPI+), whichincludes immunization, vitamin A supplementation anddeworming.
• Integrated Management of Childhood Illness plus (IMCI+),which covers promotion of insecticide-treated mosquitonets, oral rehydration therapy, antimalarial drugs, exclu-sive breastfeeding and complementary feeding.
The ‘three by three’ delivery and intervention framework issupported by cross-cutting strategies to address behaviour-al, institutional and environmental constraints. These strate-gies include:
• Advocacy, social mobilization and communication forbehavioural change.
• A results-based approach to service delivery at the community level.
• District-based monitoring and micro-planning.
• Integrated training.
• Improved supply systems.
Accelerated Child Survival and Development adopts anintegrative framework, building on existing interventionswith international and local partners. The programmestrongly emphasizes bringing the framework into themainstream of national policies and programmes, suchas health sector-wide approaches, poverty reductionstrategies and associated medium-term expenditureframeworks, basket funding and budget support. It alsoemphasizes building capacity at regional, district andcommunity levels.
ACSD has a strong community-based component and isconsidered a ‘behaviour-centred’ programme because themajority of interventions – such as utilizing insecticide-treated nets in communities where malaria is endemic,improving care of sick children and newborns, andencouraging breastfeeding and complementary feeding –promote behaviour change. ACSD also includes activeoutreach and mobile strategies that are essential toreaching the most remote areas.
Based on preliminary data presented by district healthteams in Ghana, this integrated approach, which includesimmunization, infant and young child feeding, integratedmanagement of childhood illness, and antenatal care, isalready having a positive impact on routine immunizationcoverage. Subsidized insecticide-treated mosquito netsare being distributed in conjunction with immunization-plus activities.
See References, page 106.
Accelerated Child Survival and Development in West Africa
© U
NIC
EF/
HQ
05-2
059/
Don
na D
eCes
are
Young children need adequate nutrition to have a healthy start in life. Eating a meal together, Honduras.

a need to focus on proven strategiestargeted towards relieving the majorcauses of child deaths, and to do soeffectively, interventions must be pro-vided within a continuum of care that engages communities andhouseholds, as well as outreach andfacility-based care. Health systemsmust be strengthened and expandedto support new initiatives, includingcommunity partnerships, and theymust be backed by strong nationaland international leadership and com-mitment. In addition, the many insti-tutions involved in maternal and childsurvival, health and nutrition mustwork together effectively.
One overarching principle that hasemerged from the review of sixdecades of approaches to child
survival and health is that no singleapproach is applicable in all circum-stances. The organization, deliveryand intervention orientation ofhealth-care services must be tailoredto meet the constraints of human and financial resources, the socio-economic context, the existing capac-ity of the health system and, finally,the urgency of achieving results.
Chapter 3, which highlights theimperative of developing health sys-tems to provide a continuum of qual-ity care and focuses on the benefits of employing community partner-ships in countries with weak health-system capacity, will show how theknowledge gleaned is being used. Theresults are often promising and some-times impressive, but much more can
be done – and there is a great dealmore to be learned – about scaling upthese approaches to reach the millionsof mothers, newborns and childrenwho currently live or die withoutaccess to quality health care.
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 4342 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The Partnership for Maternal, Newborn & Child Health(PMNCH), launched in September 2005, brings together 180 member maternal, newborn and child communities inan alliance to reduce mortality and morbidity. The PMNCHis the product of an alliance between the three leading partnerships on maternal, newborn and child health: thePartnership for Safe Motherhood and Newborn Health,hosted by WHO in Geneva; the Healthy Newborn Partnership,based at Save the Children USA; and the Child SurvivalPartnership, hosted by UNICEF in New York.
The partnership focuses on four key areas of work:
• Advocacy, its central mission, to raise the profile ofmaternal, newborn and child health on political agendasand press for more financial and other resources.
• Promotion and assessment of effective, evidence-based
interventions for scaling up, with a focus on reducinginequity in access to health care.
• Country support to include maternal, newborn and childhealth care in national development and investment
plans, strengthen health systems and improve equity in coverage.
• Monitoring and evaluation of coverage of priority inter-ventions, progress towards MDGs 4 and 5, and equity incoverage, to hold stakeholders accountable.
PMNCH members are divided into six constituency groups:academic and research institutions, health-care profession-als, UN agencies, non-governmental organizations, donorsand foundations, and governments.
The partnership aims to place at least 50 per cent of the 60 countries identified by Child Survival Countdown to2015 on track to achieve MDGs 4 and 5 by 2010. A definingprinciple of its work is to engender a continuum of care toaddress maternal, newborn and child care in an integratedmanner, across both time (pregnancy, birth, newborn andyoung child periods) and location (home, community andhealth facilities).
See References, page 106.
Partnership for Maternal, Newborn & Child Health
Elizabeth N. Mataka, United Nations Special Envoy of theSecretary-General for HIV/AIDS in Africa
It is disheartening to observe that nearly half of all adults liv-ing with HIV around the word are women. In sub-SaharanAfrica alone, out of the 23 million adults aged 15–49 andinfected with HIV, 13.1 million, or 57 per cent, are women. InZambia for example, women and girls are highly vulnerableto HIV and AIDS, and women aged 15–24 are three timesmore likely to be infected than males in the same age group.The toll that HIV has taken on women, especially those inAfrica, has been largely underestimated. Children have alsonot been spared from the effects of AIDS, and the impact isdevastating. It is estimated that at the end of 2006 there were2.3 million children less than 15 years old living with HIV.
Many children continue to lose parents as a result of AIDS,and this has led to an escalating number of orphans and vulnerable children, with predictions that by 2010 there willbe around 15.7 million children orphaned by AIDS in sub-Saharan Africa alone. Children suffer long before their par-ents die, especially girls, who may be drawn out of school tolook after sick parents, particularly their mothers. Childrenlose the opportunity for education and for the maximumdevelopment of their potential due to lack of support. Whenparents die, children may have to relocate – losing theirfriends, as well as the familiar surroundings and environmentthey are comfortable with. The real trauma suffered by thesechildren remains unknown because child counselling servicesare not developed in Africa. I would guess that emphasis hasbeen put on physical, visible needs to the neglect of the morecomplex and challenging psychological needs of children.
Children can no longer rely on the support of the traditionalextended family system, which provided care and support for the aged, orphans and any vulnerable and disadvantagedfamily member. This coping mechanism has been over-stretched by poverty and by the sheer numbers of children to be cared for, given the fact that AIDS affects the most productive family members in the prime of their productiveand reproductive lives. As a result, children have sometimesgone into homes that are already overstretched and wherethey are really not welcome. Some become homeless andhave to live on the streets of major capital cities in Africa.
All children need a roof over their heads, proper nutrition,parenting and support structures that will help in nurturingthem and giving them a renewed hope for the future.Without the education and socialization that parents andguardians provide, children cannot acquire the skills andknowledge they need to become fully productive adult
members of society. HIV and AIDS are leaving behind a generation of children being raised by grandparents, who in most cases also need support by virtue of their age.
The rates of infection among women and girls are a causefor deep concern, and when combined with the workloadthat women take on as well – in caring for AIDS patients,AIDS orphans and their own families – the situationbecomes untenable, especially in southern Africa.
The socio-economic status disparity between men andwomen has a great impact in fuelling the spread of HIV,among women and girls in particular. Cultural norms andearly marriages further increase the vulnerability of younggirls to infection. Poor communication around sex issueslimits their ability to negotiate safer practices and may forcewomen to remain in risky relationships. And socio-economicproblems may limit women’s access to counselling andtreatment. In this kind of set-up, women do not own proper-ty or have access to financial resources and are dependenton their husbands, fathers, brothers and sons for support.Without resources, women are susceptible to sexual vio-lence, and the threat of this violence also limits women’sability to protect themselves from HIV and AIDS.
The crisis is far from being over. African governments mustcommit to strengthening initiatives that increase capacities ofindividuals, especially women and children, to protect them-selves. Empowerment of women should no longer be dealtwith under the general heading of ‘Mainstreaming Gender inAll Aspects of Development’. Empowerment of women, aswell as support for orphans and vulnerable children, mustmove to the next level of well targeted, time-bound and wellfunded programmes with measurable results.
There is need for increased support of ‘beyond awareness’initiatives that focus on skills development, community-based health promotion, positive living, gender equity anduniversal access to prevention, care and treatment.
The ramifications of the AIDS pandemic are multiple andimpact negatively on every aspect of development. There is much to be done in Africa to ensure that the response iscommensurate to the human and financial challenges thatare posed by HIV and AIDS. There is a need for long-termsustained prevention, care and support programmes, and for consistent, predictable and sustained resource provision.There is also a need for the empowerment of women and forchange in cultural practices that discriminate against women.Long-term sustainable responses are essential and can onlybe achieved if all relevant stakeholders work together.
HIV and AIDS in Africa and its impact on women and children
a need to focus on proven strategiestargeted towards relieving the majorcauses of child deaths, and to do soeffectively, interventions must be pro-vided within a continuum of care that engages communities andhouseholds, as well as outreach andfacility-based care. Health systemsmust be strengthened and expandedto support new initiatives, includingcommunity partnerships, and theymust be backed by strong nationaland international leadership and com-mitment. In addition, the many insti-tutions involved in maternal and childsurvival, health and nutrition mustwork together effectively.
One overarching principle that hasemerged from the review of sixdecades of approaches to child
survival and health is that no singleapproach is applicable in all circum-stances. The organization, deliveryand intervention orientation ofhealth-care services must be tailoredto meet the constraints of human and financial resources, the socio-economic context, the existing capac-ity of the health system and, finally,the urgency of achieving results.
Chapter 3, which highlights theimperative of developing health sys-tems to provide a continuum of qual-ity care and focuses on the benefits of employing community partner-ships in countries with weak health-system capacity, will show how theknowledge gleaned is being used. Theresults are often promising and some-times impressive, but much more can
be done – and there is a great dealmore to be learned – about scaling upthese approaches to reach the millionsof mothers, newborns and childrenwho currently live or die withoutaccess to quality health care.
L E S S O N S L E A R N E D F R O M E V O L V I N G H E A L T H - C A R E S Y S T E M S A N D P R A C T I C E S 4342 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The Partnership for Maternal, Newborn & Child Health(PMNCH), launched in September 2005, brings together 180 member maternal, newborn and child communities inan alliance to reduce mortality and morbidity. The PMNCHis the product of an alliance between the three leading partnerships on maternal, newborn and child health: thePartnership for Safe Motherhood and Newborn Health,hosted by WHO in Geneva; the Healthy Newborn Partnership,based at Save the Children USA; and the Child SurvivalPartnership, hosted by UNICEF in New York.
The partnership focuses on four key areas of work:
• Advocacy, its central mission, to raise the profile ofmaternal, newborn and child health on political agendasand press for more financial and other resources.
• Promotion and assessment of effective, evidence-based
interventions for scaling up, with a focus on reducinginequity in access to health care.
• Country support to include maternal, newborn and childhealth care in national development and investment
plans, strengthen health systems and improve equity in coverage.
• Monitoring and evaluation of coverage of priority inter-ventions, progress towards MDGs 4 and 5, and equity incoverage, to hold stakeholders accountable.
PMNCH members are divided into six constituency groups:academic and research institutions, health-care profession-als, UN agencies, non-governmental organizations, donorsand foundations, and governments.
The partnership aims to place at least 50 per cent of the 60 countries identified by Child Survival Countdown to2015 on track to achieve MDGs 4 and 5 by 2010. A definingprinciple of its work is to engender a continuum of care toaddress maternal, newborn and child care in an integratedmanner, across both time (pregnancy, birth, newborn andyoung child periods) and location (home, community andhealth facilities).
See References, page 106.
Partnership for Maternal, Newborn & Child Health
Elizabeth N. Mataka, United Nations Special Envoy of theSecretary-General for HIV/AIDS in Africa
It is disheartening to observe that nearly half of all adults liv-ing with HIV around the word are women. In sub-SaharanAfrica alone, out of the 23 million adults aged 15–49 andinfected with HIV, 13.1 million, or 57 per cent, are women. InZambia for example, women and girls are highly vulnerableto HIV and AIDS, and women aged 15–24 are three timesmore likely to be infected than males in the same age group.The toll that HIV has taken on women, especially those inAfrica, has been largely underestimated. Children have alsonot been spared from the effects of AIDS, and the impact isdevastating. It is estimated that at the end of 2006 there were2.3 million children less than 15 years old living with HIV.
Many children continue to lose parents as a result of AIDS,and this has led to an escalating number of orphans and vulnerable children, with predictions that by 2010 there willbe around 15.7 million children orphaned by AIDS in sub-Saharan Africa alone. Children suffer long before their par-ents die, especially girls, who may be drawn out of school tolook after sick parents, particularly their mothers. Childrenlose the opportunity for education and for the maximumdevelopment of their potential due to lack of support. Whenparents die, children may have to relocate – losing theirfriends, as well as the familiar surroundings and environmentthey are comfortable with. The real trauma suffered by thesechildren remains unknown because child counselling servicesare not developed in Africa. I would guess that emphasis hasbeen put on physical, visible needs to the neglect of the morecomplex and challenging psychological needs of children.
Children can no longer rely on the support of the traditionalextended family system, which provided care and support for the aged, orphans and any vulnerable and disadvantagedfamily member. This coping mechanism has been over-stretched by poverty and by the sheer numbers of children to be cared for, given the fact that AIDS affects the most productive family members in the prime of their productiveand reproductive lives. As a result, children have sometimesgone into homes that are already overstretched and wherethey are really not welcome. Some become homeless andhave to live on the streets of major capital cities in Africa.
All children need a roof over their heads, proper nutrition,parenting and support structures that will help in nurturingthem and giving them a renewed hope for the future.Without the education and socialization that parents andguardians provide, children cannot acquire the skills andknowledge they need to become fully productive adult
members of society. HIV and AIDS are leaving behind a generation of children being raised by grandparents, who in most cases also need support by virtue of their age.
The rates of infection among women and girls are a causefor deep concern, and when combined with the workloadthat women take on as well – in caring for AIDS patients,AIDS orphans and their own families – the situationbecomes untenable, especially in southern Africa.
The socio-economic status disparity between men andwomen has a great impact in fuelling the spread of HIV,among women and girls in particular. Cultural norms andearly marriages further increase the vulnerability of younggirls to infection. Poor communication around sex issueslimits their ability to negotiate safer practices and may forcewomen to remain in risky relationships. And socio-economicproblems may limit women’s access to counselling andtreatment. In this kind of set-up, women do not own proper-ty or have access to financial resources and are dependenton their husbands, fathers, brothers and sons for support.Without resources, women are susceptible to sexual vio-lence, and the threat of this violence also limits women’sability to protect themselves from HIV and AIDS.
The crisis is far from being over. African governments mustcommit to strengthening initiatives that increase capacities ofindividuals, especially women and children, to protect them-selves. Empowerment of women should no longer be dealtwith under the general heading of ‘Mainstreaming Gender inAll Aspects of Development’. Empowerment of women, aswell as support for orphans and vulnerable children, mustmove to the next level of well targeted, time-bound and wellfunded programmes with measurable results.
There is need for increased support of ‘beyond awareness’initiatives that focus on skills development, community-based health promotion, positive living, gender equity anduniversal access to prevention, care and treatment.
The ramifications of the AIDS pandemic are multiple andimpact negatively on every aspect of development. There is much to be done in Africa to ensure that the response iscommensurate to the human and financial challenges thatare posed by HIV and AIDS. There is a need for long-termsustained prevention, care and support programmes, and for consistent, predictable and sustained resource provision.There is also a need for the empowerment of women and forchange in cultural practices that discriminate against women.Long-term sustainable responses are essential and can onlybe achieved if all relevant stakeholders work together.
HIV and AIDS in Africa and its impact on women and children
programmes and ‘learning bydoing’, it is far easier than trying todisaggregate the elements that didnot work in a community-basedprogramme from the contextual fac-tors. Consequently, while the panelon page 48 lists several of the com-mon challenges to community part-
nerships in primary health care, thechapter will concentrate mostly onidentifying and explaining the com-mon tenets of successful initiatives.
Success factors drawn from evidenceand experience are identified as followsand summarized below. They include:
• Cohesive, inclusive communityorganization and participation.
• Support and incentives for community health workers.
• Adequate programme supervisionand support.
C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 47
A number of agencies, including UNICEF and WHO, haveagreed on 12 key household practices for neonates andinfants that can help to promote child survival, health andnutrition in communities:
• Exclusive breastfeeding: Exclusive breastfeeding from birthto six months. (Mothers found to be HIV-positive requirecounselling about possible alternatives to breastfeeding.)
• Complementary feeding: Starting at about six months old,feeding children energy- and nutrient-rich complementaryfoods while continuing to breastfeed for at least two yearscould prevent more than 10 per cent of deaths from diar-rhoea and acute respiratory infections, particularly pneumo-nia; and increase resistance to measles and other illnesses.
• Micronutrient supplementation: Improving the intake of vitamin A through diet or supplements in communitieswhere it is deficient could reduce mortality among childrenaged 6 months to five years by 20 per cent.
• Hygiene: Better hygiene practices, particularly hand washing with soap (or ashes) and the safe disposal ofexcreta could reduce the incidence of diarrhoea by 35 per cent.
• Immunization: Vaccination against measles for childrenunder age one could prevent most of the measles-relateddeaths each year. Caregivers should make sure childrencomplete a full course of immunizations (bacille Calmette-Guérin; diphtheria, pertussis and tetanus vaccine; oral poliovaccine; and measles vaccine) before their first birthday.
• Malaria prevention: The use of insecticide-treated mosquitonets in households in malaria-endemic areas could lowermalaria-related child deaths by as much as 23 per cent.
• Psychosocial care and development: Promote mental andsocial development by responding to a child’s need forcare and by talking, playing and providing a stimulatingenvironment.
• Feeding and fluids for sick children: Continue to feed andoffer more fluids, including breast milk, to children whenthey are sick.
• Home treatment: Give sick children appropriate hometreatment for infections.
• Care seeking: Recognize when sick children need treat-ment outside the home, and seek care from appropriateproviders.
• Appropriate practices: Follow the health worker’s adviceabout treatment, follow-up and referral.
• Antenatal care: Every pregnant woman should have adequate antenatal care. This includes having at least fourantenatal visits with an appropriate health-care providerand receiving the recommended doses of tetanus toxoidvaccination. The mother also deserves support from herfamily and community in seeking care at the time of delivery and during the postpartum and lactation period.
Further important practices that protect children include:providing appropriate care for those who are affected byHIV and AIDS, especially orphans and vulnerable children;protecting children from injury and accident, abuse andneglect; and involving fathers in the care of their children.
Many of these practices can be undertaken by communityhealth workers or by community members themselves,given the appropriate support and distribution of productsand services. The direct involvement of the community isperhaps most appropriate for those aspects of health careand nutrition that most closely affect members on a dailybasis. These include infant and young child feeding, othercaring practices, and water and sanitation.
See References, page 107.
Basic practices for community-based health-care interventions
Based on this broad definition ofcommunity, community partnershipsare approaches and strategies thatseek to actively engage communitymembers in their own health careand well-being, along with those oftheir children and other dependants.
Community partnerships in maternal,newborn and child health are rich indiversity. Some are small-scale, involv-ing only a few thousand or even a fewhundred people; other initiatives, suchas the Brazilian community healthworkers network or the Lady HealthWorkers programme in Pakistan,encompass thousands of workers covering millions of children andwomen. Some programmes emphasizesupply-side elements, such as serviceprovision through community healthworkers, while others focus more ondemand-side initiatives to mobilizesocial demand for accountability andresults from governments. Some com-munity health worker initiatives relyon voluntary participation, while oth-
ers include payment in kind, in part or in cash. Some community-basedprogrammes are nationally supportedand integrated into sector-wide poli-cies and the broader health system,while others have yet to be fully orpartially incorporated.5
The multiplicity of programmes andapproaches to community participationin health care reflects, in part at least,the diversity of communities. Eachone has its own social characteristics,organizational structure and links withother groups. To be effective, pro-grammes and approaches directedtowards communities must thereforeadapt to the local needs and contextand be owned by the community.
Adaptation of strategies for individ-ual settings is a complex processbecause communities, like countriesand regions, are often heterogeneousentities. Not only are there markeddifferences between communities in aparticular country or district, there
are likely to be disparities withinthem as well. Members of communi-ties may share common heritage andinterests and experience similar dep-rivations, discrimination and disem-powerment, but different memberswill have specific needs, concerns and expectations regarding healthcare. Communities are likely to comprise powerful individuals withthe potential to help or hinder ahealth programme, depending ontheir viewpoint or interests.
Despite these variations, evidence andobservation allow for the identificationof common factors in community-based approaches to health care andnutrition. An overarching aim is that community-based programmesincrease the potential of the localpopulation to access health servicesand interventions. In addition, theyare perceived as having the potentialto accelerate advances in behaviourchange, care practices and care seek-ing, and to empower communitiesand households to demand qualityservices.6 Other common aspects of community-based approaches to health care and nutrition are illustrated in the panel on page 48.
Success factors in community
partnerships
Several factors are commonly foundin successful community-basedapproaches. Implementation in anysetting depends on the local context.Identifying successful factors is notonly a positive way of assessing
46 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Supporting pregnant women throughcommunity outreach enhances care forboth mother and child. HIV counselling forpregnant women at a local health centre,the Democratic Republic of the Congo.
© U
NIC
EF/
HQ
05-2
186/
Gia
com
o P
irozz
i

Organization alone is not sufficientto bring lasting change. To be trulyeffective and universal in scope, com-munity participation must be sociallyinclusive. Given that communities areoften heterogeneous in compositionand structure, establishing a sociallyinclusive community partnership maybe challenging. Long-held patterns ofexclusion and discrimination by gen-der, religion, ethnicity or disabilitycan impede the reach of interven-tions. Divisions among communitymembers may also be rooted in morerecent events and circumstances, suchas civil strife and the stigma attachedto HIV and AIDS.8
Even when communities haverespected, socially inclusive organ-izations, their participation in programmes is not automatic.Advocacy and communication arerequired to allow community organi-zations to state their preferences andneeds for health care, nutrition, andwater and sanitation services. Once a programme is launched and imple-mented, community members need to see that it is progressing towardstheir stated objectives, both individu-ally and collectively. As programmesprogress, their ongoing relevanceshould also be regularly assessed.9
Programmes that limit communityparticipation to implementation runthe risk of weak local ownership,with the result that participationwill be tentative and tenuous.10
Periodic meetings of communityorganizations involved with commu-nity programmes are an importantcomponent of participation. At thesemeetings, the results and evidencecan be discussed as part of planning,monitoring and evaluation.
Support and incentives for
community health workers
Community health workers areestablished as an integral part ofcommunity-based programmes, serv-ing as a bridge between professionalhealth staff and the community, andhelping communities identify andaddress their own health needs.
Community health workers are gen-erally the main agents of community-based treatment, education andcounselling, usually through house-hold visits. They also attend localhealth facilities, obtain and dispensesupplies of drugs and other essentialproducts, participate in communitymeetings and fulfil their responsibili-ties in programme management.Other duties often include attendinglocal district and regional meetingsfor training and feedback, and repre-
senting the community in dialoguewith other communities and govern-ment health personnel.
Because they can reach vulnerablechildren who may otherwise lackaccess to basic health services, community health workers have beenparticularly effective in improvingchild survival outcomes at projectlevel in countries as diverse asEcuador, Ethiopia, Colombia andNepal. Successful scale-up effortsacross the developing world confirmthe potential of community healthworkers to deliver equitable healthservices to children living in remoteareas and to help fill the unmetdemand for regular health services incountries with weak health systems.
Efforts to scale up communityhealth worker programmes,
C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 49
© U
NIC
EF/
HQ
07-0
463/
Chr
istin
e N
esbi
tt
Village leaders can be strong advocates for promoting essential health interventions withincommunities. A district chief vaccinates his son against polio, Nigeria.
• Effective referral systems to facility-based care.
• Cooperation and coordination withother programmes and sectors.
• Secure financing.
• Integration with district andnational programmes and policies.
Each of these tenets is briefly summa-rized in the following pages.
Cohesive, inclusive community
organization and participation
Cohesive, inclusive organization is a fundamental feature of success-ful community partnerships.Communities function under established norms and practices that are often deeply entrenched insocial, religious or cultural heritage.Programmes that respect this her-itage have been found to be amongthe most successful community-based approaches to health care
and nutrition. In Asia, for example,the large-scale initiatives under-taken in Bangladesh (BRAC), India(Jamkhed and others), Pakistan(Lady Health Workers) and othercountries have been led by localorganizations – often women’sgroups. These groups have built onthe established structures withincommunities that extend to otherareas of development, includingeducation and credit, as well as health.7
48 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Overarching aim
• Reduce maternal, newborn and child mortality and morbidity.
Objectives
• Improve access to basic preventive and curative services.
• Foster direct and more frequent contact between healthworkers and caregivers, mothers and children.
• Encourage sustainable behaviour change.
• Support caring practices.
• Stimulate social mobilization by the community todemand better services and accountability.
Central features
• Health care and nutrition activities take place outside formal health facilities.
• Community health workers, often volunteers or part-timeworkers, are frequently key participants in dispensingessential services and promoting better caring practices.
• Training, support and supervision for community healthworkers are common features of programmes.
• There is often a central point within the geographicalvicinity for the delivery of services or home visits.
• A community organization supports the programme andcontributes not only administration and implementation,but often design and evaluation as well.
• Other aspects of primary health care – especially waterand sanitation, and agricultural interventions – are part ofthe programme.
Additional features common to some, but not
all, community partnerships
• Referral to facility-based care.
• Support from outreach workers.
• Integration of the programmes into the wider health sector.
• Integration into national development programmes andpolicies.
• Measures to strengthen the supportive environment, e.g,gender equality initiatives.
Common constraints on community partnerships
• Lack of community health workers to deliver quality services.
• Inadequate coordination of diverse participants.
• Insufficient funding for community-based activities.
• Irregular supply of drugs and commodities.
• Poor support and supervision of community health workers.
• Entrenched traditional childcare practices.
• Low economic status of women.
See References, page 107.
Common aspects and challenges of community partnerships in
health and nutrition
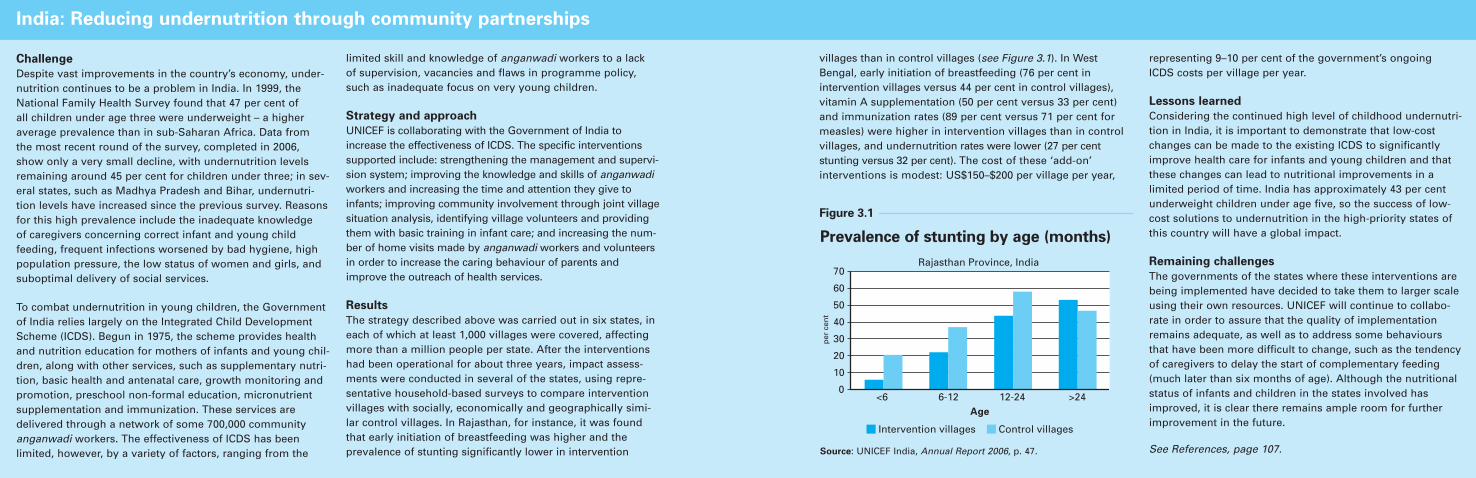
The incentives required to retain andmotivate community health workersare not necessarily monetary. Thedisappointing results of evaluationsof post Alma-Ata large-scale trainingand deployment of community healthworkers underscore the fact thatsound programme management andrefresher training are more effica-cious at sustaining workers’ effective-ness than initial training. Active com-munity participation and support is avital element of successful and sus-tainable community health workerprogrammes throughout the world. In the Philippines, for example,health workers at the barangay level,the smallest political unit in the
country, have become a significantdriving force behind improved childsurvival. This success has beenencouraged by the Barangay HealthWorkers’ Benefits and Incentives Act of 1995, which includes suchprovisions as subsistence allowances,career enrichment and special train-ing programmes, and preferentialaccess to loans. Similarly, in Ceara,Brazil, a programme using a decen-tralized approach that allows com-munity health workers to earn a substantial monthly income (twicethe local average) has led to dramaticimprovements in child health, includ-ing a 32 per cent reduction in child mortality.13
Adequate programme supervision
and support
Supervision and support systems forcommunity partnerships in primaryhealth care can diminish the communi-ty health workers’ sense of isolationand help sustain interest and motiva-tion, reducing the risk of attrition.Skilled health workers based in, orclosely linked to, health facilities gen-erally undertake the supervisory func-tion, which can add to their alreadyheavy workloads. Supervisors them-selves require training to acquire theappropriate skills for oversight of com-munity-based programmes. Resourceconstraints – human, financial or orga-nizational – can limit the breadth and
C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 51
addressed in greater depth inChapter 4, can face obstacles andbottlenecks. In fact, just being ableto maintain adequate participantnumbers and structure is often oneof the greatest challenges. Existingprogrammes, regardless of theirscale, grapple with poor training,inadequate supervision, lack of sup-plies and poor relationships with thecommunities they intend to serve.Attrition rates in community healthworker programmes are often high.One review, for example, foundattrition rates of 30 per cent overnine months in Senegal and 50 percent over two years in Nigeria.Similar challenges have been identi-
fied in India, Sri Lanka and theUnited Republic of Tanzania.11
Attrition is related to multiple fac-tors. Fulfilling the responsibilities ofa community health worker takestime and financial resources, andmay involve significant opportunitycosts. Community health workers,particularly those who are volunteersor paid in kind or part, may haveobligations to meet and requireincome to support their families. If the demands on their time andresources prove overwhelming, thereis a risk they will not function effec-tively as health workers or will dropout of community partnerships.
The sustainability of communityhealth worker programmes dependson creating a package of incentivesthat is sufficiently attractive to prevent attrition. These packageswill vary among settings, reflectingthe different functions communityhealth workers undertake in differ-ent communities. But all need tofocus on priorities that include compensating community healthworkers for lost economic opportu-nities; providing adequate supervi-sion and peer support; offering personal growth and developmentopportunities; and creating a strong support system within thecommunity.12
50 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Challenge
Despite vast improvements in the country’s economy, under-nutrition continues to be a problem in India. In 1999, theNational Family Health Survey found that 47 per cent of all children under age three were underweight – a higheraverage prevalence than in sub-Saharan Africa. Data from the most recent round of the survey, completed in 2006,show only a very small decline, with undernutrition levelsremaining around 45 per cent for children under three; in sev-eral states, such as Madhya Pradesh and Bihar, undernutri-tion levels have increased since the previous survey. Reasonsfor this high prevalence include the inadequate knowledge of caregivers concerning correct infant and young child feeding, frequent infections worsened by bad hygiene, highpopulation pressure, the low status of women and girls, andsuboptimal delivery of social services.
To combat undernutrition in young children, the Governmentof India relies largely on the Integrated Child DevelopmentScheme (ICDS). Begun in 1975, the scheme provides healthand nutrition education for mothers of infants and young chil-dren, along with other services, such as supplementary nutri-tion, basic health and antenatal care, growth monitoring andpromotion, preschool non-formal education, micronutrientsupplementation and immunization. These services are delivered through a network of some 700,000 communityanganwadi workers. The effectiveness of ICDS has been limited, however, by a variety of factors, ranging from the
limited skill and knowledge of anganwadi workers to a lack of supervision, vacancies and flaws in programme policy,such as inadequate focus on very young children.
Strategy and approach
UNICEF is collaborating with the Government of India toincrease the effectiveness of ICDS. The specific interventionssupported include: strengthening the management and supervi-sion system; improving the knowledge and skills of anganwadiworkers and increasing the time and attention they give toinfants; improving community involvement through joint villagesituation analysis, identifying village volunteers and providingthem with basic training in infant care; and increasing the num-ber of home visits made by anganwadi workers and volunteersin order to increase the caring behaviour of parents andimprove the outreach of health services.
Results
The strategy described above was carried out in six states, ineach of which at least 1,000 villages were covered, affectingmore than a million people per state. After the interventionshad been operational for about three years, impact assess-ments were conducted in several of the states, using repre-sentative household-based surveys to compare interventionvillages with socially, economically and geographically simi-lar control villages. In Rajasthan, for instance, it was foundthat early initiation of breastfeeding was higher and theprevalence of stunting significantly lower in intervention
villages than in control villages (see Figure 3.1). In WestBengal, early initiation of breastfeeding (76 per cent in intervention villages versus 44 per cent in control villages),vitamin A supplementation (50 per cent versus 33 per cent)and immunization rates (89 per cent versus 71 per cent formeasles) were higher in intervention villages than in controlvillages, and undernutrition rates were lower (27 per cent stunting versus 32 per cent). The cost of these ‘add-on’ interventions is modest: US$150–$200 per village per year,
representing 9–10 per cent of the government’s ongoing ICDS costs per village per year.
Lessons learned
Considering the continued high level of childhood undernutri-tion in India, it is important to demonstrate that low-costchanges can be made to the existing ICDS to significantlyimprove health care for infants and young children and thatthese changes can lead to nutritional improvements in a limited period of time. India has approximately 43 per centunderweight children under age five, so the success of low-cost solutions to undernutrition in the high-priority states ofthis country will have a global impact.
Remaining challenges
The governments of the states where these interventions arebeing implemented have decided to take them to larger scaleusing their own resources. UNICEF will continue to collabo-rate in order to assure that the quality of implementationremains adequate, as well as to address some behavioursthat have been more difficult to change, such as the tendencyof caregivers to delay the start of complementary feeding(much later than six months of age). Although the nutritionalstatus of infants and children in the states involved hasimproved, it is clear there remains ample room for furtherimprovement in the future.
See References, page 107.
Prevalence of stunting by age (months)
Source: UNICEF India, Annual Report 2006, p. 47.
Rajasthan Province, India70
<6
Intervention villages Control villages
6-12Age
12-24 >24
60
50
40
30
20
10
0
per
cen
t
Figure 3.1
India: Reducing undernutrition through community partnerships
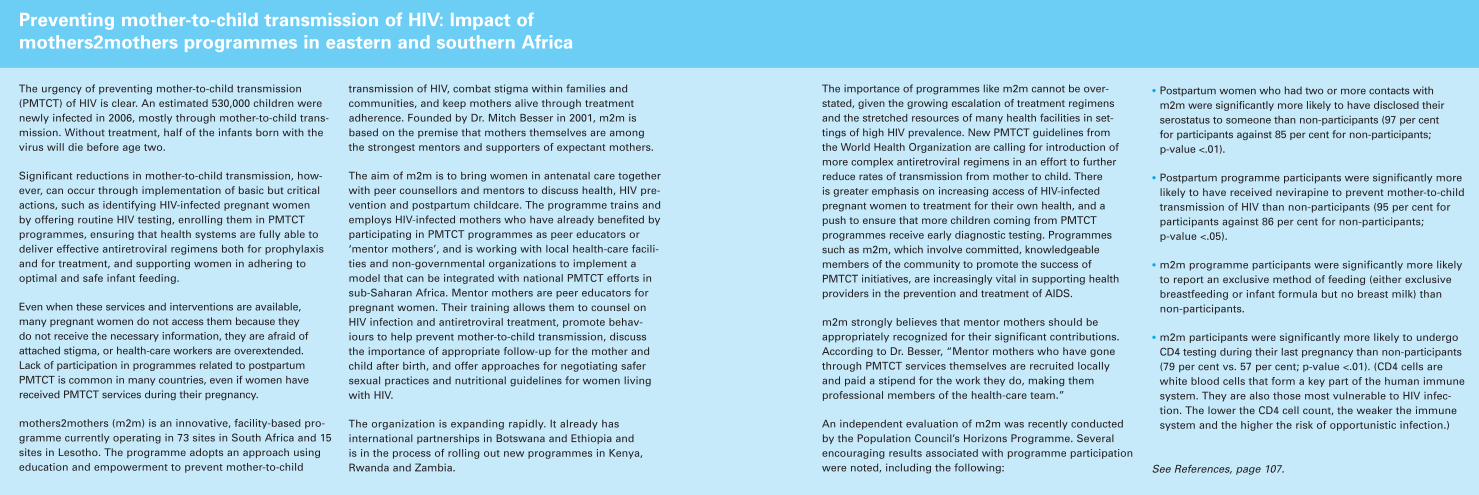
health workers and preparations arein place for transportation to andfrom both locations.
Supervision should not be limitedto the official health authorities,however, and community organiza-tions have a role in oversight ofhealth workers and programmeoutcomes. In principles widelyaccepted by practitioners, it is recommended that the communitybe involved in the initial selectionof health workers, and that healthworkers accept community mem-bers’ participation in identifyingpriorities and planning projects.14
Effective referral systems
Effective referral systems are anessential complement to successfulcommunity-based programmes toensure a continuum of care (seeChapter 4). Hospitals provideservices that cannot be safely replicated elsewhere, such asCaesarian sections and other emergency obstetric care. How-ever, in the poorest countries withthe highest maternal and childmortality rates, health-careresources are often limited andaccess to referral hospitals fre-quently low. In these situations,millions of children can be assisted
very rapidly by scaling up ofproven, cost-effective interventionsin primary health care, particularlythose that are community-based.
At the same time, there is a need toinvest in strengthening district healthsystems to provide basic referral care and to support expansion ofessential primary-health-care servic-es. Community health workers haveproved to be effective in managingmany serious childhood illnesses, suchas diarrhoea, malaria, acute undernu-trition and pneumonia; supervisionand access to referral servicesstrengthen the quality of this activity.
C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 53
depth of training, leaving both supervi-sors and community health workers ata considerable disadvantage in imple-menting and managing programmes.Visits by supervisors to communities,in particular, are important for on-sitetraining and learning by doing forboth parties, but these visits are fre-quently compromised by constraintson financial resources or by poortransportation infrastructure.
Efficient administration of communi-ty programmes aids evaluation, andmonitoring can help ensure that coverage is as universal as possible.Records of patients, treatments and
outcomes should be kept up to date,and regular meetings should be held to build cooperative relation-ships between health workers andsupervisors and to inform pro-gramme assessment and modifica-tion. Employing technology, such as computer-based databases, emailand cellphones, can streamline theprocess of information gathering and dissemination while freeing timefor workers and supervisors to visitcommunities and households andmeet together.
Other types of support to programmesinclude logistics, supplies and equip-
ment. Community health workersrequire sufficient tools, including training and products, to be able to dotheir job and maintain their standingin the community. The previously citedevaluations of large-scale communityhealth worker programmes undertakenin the 1980s show that when thesetools and products – especially drugs –are inappropriate or not resuppliedregularly, the effectiveness of healthworkers is compromised. When communities are located far fromsupporting health facilities, evidenceshows that programmes are moreeffective if there is a clear schedule ofvisits by supervisors and community
52 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The urgency of preventing mother-to-child transmission(PMTCT) of HIV is clear. An estimated 530,000 children werenewly infected in 2006, mostly through mother-to-child trans-mission. Without treatment, half of the infants born with thevirus will die before age two.
Significant reductions in mother-to-child transmission, how-ever, can occur through implementation of basic but criticalactions, such as identifying HIV-infected pregnant women by offering routine HIV testing, enrolling them in PMTCT programmes, ensuring that health systems are fully able todeliver effective antiretroviral regimens both for prophylaxisand for treatment, and supporting women in adhering to optimal and safe infant feeding.
Even when these services and interventions are available, many pregnant women do not access them because they do not receive the necessary information, they are afraid ofattached stigma, or health-care workers are overextended. Lack of participation in programmes related to postpartumPMTCT is common in many countries, even if women havereceived PMTCT services during their pregnancy.
mothers2mothers (m2m) is an innovative, facility-based pro-gramme currently operating in 73 sites in South Africa and 15sites in Lesotho. The programme adopts an approach usingeducation and empowerment to prevent mother-to-child
transmission of HIV, combat stigma within families and communities, and keep mothers alive through treatmentadherence. Founded by Dr. Mitch Besser in 2001, m2m isbased on the premise that mothers themselves are amongthe strongest mentors and supporters of expectant mothers.
The aim of m2m is to bring women in antenatal care togetherwith peer counsellors and mentors to discuss health, HIV pre-vention and postpartum childcare. The programme trains andemploys HIV-infected mothers who have already benefited byparticipating in PMTCT programmes as peer educators or‘mentor mothers’, and is working with local health-care facili-ties and non-governmental organizations to implement amodel that can be integrated with national PMTCT efforts insub-Saharan Africa. Mentor mothers are peer educators forpregnant women. Their training allows them to counsel onHIV infection and antiretroviral treatment, promote behav-iours to help prevent mother-to-child transmission, discussthe importance of appropriate follow-up for the mother andchild after birth, and offer approaches for negotiating safersexual practices and nutritional guidelines for women livingwith HIV.
The organization is expanding rapidly. It already has international partnerships in Botswana and Ethiopia and is in the process of rolling out new programmes in Kenya,Rwanda and Zambia.
Preventing mother-to-child transmission of HIV: Impact of
mothers2mothers programmes in eastern and southern Africa
The importance of programmes like m2m cannot be over-stated, given the growing escalation of treatment regimensand the stretched resources of many health facilities in set-tings of high HIV prevalence. New PMTCT guidelines fromthe World Health Organization are calling for introduction ofmore complex antiretroviral regimens in an effort to furtherreduce rates of transmission from mother to child. There is greater emphasis on increasing access of HIV-infectedpregnant women to treatment for their own health, and apush to ensure that more children coming from PMTCTprogrammes receive early diagnostic testing. Programmessuch as m2m, which involve committed, knowledgeablemembers of the community to promote the success ofPMTCT initiatives, are increasingly vital in supporting healthproviders in the prevention and treatment of AIDS.
m2m strongly believes that mentor mothers should beappropriately recognized for their significant contributions.According to Dr. Besser, “Mentor mothers who have gonethrough PMTCT services themselves are recruited locallyand paid a stipend for the work they do, making them professional members of the health-care team.”
An independent evaluation of m2m was recently conductedby the Population Council’s Horizons Programme. Severalencouraging results associated with programme participationwere noted, including the following:
• Postpartum women who had two or more contacts with m2m were significantly more likely to have disclosed theirserostatus to someone than non-participants (97 per cent for participants against 85 per cent for non-participants; p-value <.01).
• Postpartum programme participants were significantly morelikely to have received nevirapine to prevent mother-to-childtransmission of HIV than non-participants (95 per cent forparticipants against 86 per cent for non-participants; p-value <.05).
• m2m programme participants were significantly more likelyto report an exclusive method of feeding (either exclusivebreastfeeding or infant formula but no breast milk) thannon-participants.
• m2m participants were significantly more likely to undergoCD4 testing during their last pregnancy than non-participants(79 per cent vs. 57 per cent; p-value <.01). (CD4 cells arewhite blood cells that form a key part of the human immunesystem. They are also those most vulnerable to HIV infec-tion. The lower the CD4 cell count, the weaker the immunesystem and the higher the risk of opportunistic infection.)
See References, page 107.
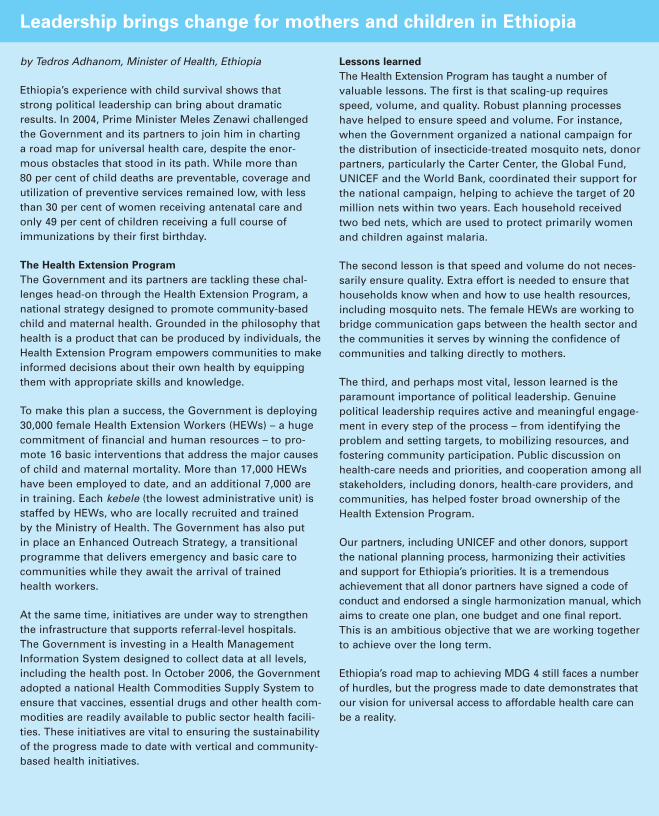
Community health workers have beenless effective in identifying and man-aging complications during childbirth.Reducing maternal mortality there-fore requires the scaling up of skilledattendance at birth with referral sys-tems for emergency obstetric care.
District health systems also serve as a focal point for public health programme coordination, integratingdirect care for patients with popula-tion-based campaigns and supervisionand coordination of community-based care and other lower levelhealth services. At higher referral lev-els (regional or national hospitals)this role is often broadened to includesuch functions as training and
research, and technical support andquality assurance for lower levels.
An essential component of an effectivereferral system is good communicationbetween the community programmeparticipants and facility-based staff.Reinforcing points made in the previ-ous sections, referral hospitals shouldengage with community programmes,provide strong support for communityhealth workers and spend a significantproportion of time providing advicethrough person-to-person contact or other modes of communication.Upgrading information and commu-nications technology can facilitatedialogue and referral, even in low-income countries.15
Coordination and cooperation with
other essential services and sectors
Just as referral systems are essentialto support and coordinate activitiesat the community level, cooperationand communication between pro-grammes at the district level andintersectoral collaboration are alsoimportant. Coordination with otherhealth services can take many forms.The possible benefits are multiple,including the sharing of new ideas,training, resources and evaluationskills; and early warning, manage-ment and containment of disease outbreaks.16
In Cambodia, for example, non-governmental organizations share
C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 5554 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Positive behavioural changes in the household and community lead to improvements in maternal, newborn and child health. A communityhealth worker demonstrates the use of water-treatment supplies, Indonesia.
© U
NIC
EF/
HQ
06-1
855/
Josh
Est
ey
by Tedros Adhanom, Minister of Health, Ethiopia
Ethiopia’s experience with child survival shows thatstrong political leadership can bring about dramaticresults. In 2004, Prime Minister Meles Zenawi challengedthe Government and its partners to join him in charting a road map for universal health care, despite the enor-mous obstacles that stood in its path. While more than 80 per cent of child deaths are preventable, coverage andutilization of preventive services remained low, with lessthan 30 per cent of women receiving antenatal care andonly 49 per cent of children receiving a full course ofimmunizations by their first birthday.
The Health Extension Program
The Government and its partners are tackling these chal-lenges head-on through the Health Extension Program, anational strategy designed to promote community-basedchild and maternal health. Grounded in the philosophy thathealth is a product that can be produced by individuals, theHealth Extension Program empowers communities to makeinformed decisions about their own health by equippingthem with appropriate skills and knowledge.
To make this plan a success, the Government is deploying30,000 female Health Extension Workers (HEWs) – a hugecommitment of financial and human resources – to pro-mote 16 basic interventions that address the major causesof child and maternal mortality. More than 17,000 HEWshave been employed to date, and an additional 7,000 arein training. Each kebele (the lowest administrative unit) isstaffed by HEWs, who are locally recruited and trained by the Ministry of Health. The Government has also put in place an Enhanced Outreach Strategy, a transitional programme that delivers emergency and basic care tocommunities while they await the arrival of trained health workers.
At the same time, initiatives are under way to strengthenthe infrastructure that supports referral-level hospitals. The Government is investing in a Health ManagementInformation System designed to collect data at all levels,including the health post. In October 2006, the Governmentadopted a national Health Commodities Supply System toensure that vaccines, essential drugs and other health com-modities are readily available to public sector health facili-ties. These initiatives are vital to ensuring the sustainabilityof the progress made to date with vertical and community-based health initiatives.
Lessons learned
The Health Extension Program has taught a number of valuable lessons. The first is that scaling-up requiresspeed, volume, and quality. Robust planning processeshave helped to ensure speed and volume. For instance,when the Government organized a national campaign forthe distribution of insecticide-treated mosquito nets, donorpartners, particularly the Carter Center, the Global Fund,UNICEF and the World Bank, coordinated their support forthe national campaign, helping to achieve the target of 20million nets within two years. Each household receivedtwo bed nets, which are used to protect primarily womenand children against malaria.
The second lesson is that speed and volume do not neces-sarily ensure quality. Extra effort is needed to ensure thathouseholds know when and how to use health resources,including mosquito nets. The female HEWs are working tobridge communication gaps between the health sector andthe communities it serves by winning the confidence ofcommunities and talking directly to mothers.
The third, and perhaps most vital, lesson learned is theparamount importance of political leadership. Genuinepolitical leadership requires active and meaningful engage-ment in every step of the process – from identifying theproblem and setting targets, to mobilizing resources, andfostering community participation. Public discussion onhealth-care needs and priorities, and cooperation among allstakeholders, including donors, health-care providers, andcommunities, has helped foster broad ownership of theHealth Extension Program.
Our partners, including UNICEF and other donors, supportthe national planning process, harmonizing their activitiesand support for Ethiopia’s priorities. It is a tremendousachievement that all donor partners have signed a code ofconduct and endorsed a single harmonization manual, whichaims to create one plan, one budget and one final report.This is an ambitious objective that we are working togetherto achieve over the long term.
Ethiopia’s road map to achieving MDG 4 still faces a numberof hurdles, but the progress made to date demonstrates thatour vision for universal access to affordable health care canbe a reality.
Leadership brings change for mothers and children in Ethiopia

C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 59
National strategies must give priorityattention to the removal of obstaclesto effective scaling up and implemen-tation at different levels of the healthsystems (see Chapter 4 for furtherdetails on measures to address bottle-necks in health-service delivery). Wellknown bottlenecks include irregularimmunization sessions, negativeexperiences with the health system,distance to health centres and lack of information. At the family andcommunity level, effective coverageof primary-health-care services isoften impeded by lack of basicaffordable supplies, low demand and other fundamental challenges,such as mosquito nets not beingtreated with insecticide.23
Both the short-term, disease-specificinitiatives – increasingly supportedby new international donor partner-
ships – and longer-term, health-sector development programmes are likely to continue to coexist.Sufficient human and financialresources must be invested in bothsets of initiatives to produce sustain-able gains for child health. Donor-driven, disease-specific partnershipsshould consider adapting theirapproaches into multisectoral frame-works that align with national healthpriorities, with equitable benefits forthe whole national health system.24
The ultimate responsibility for ensur-ing children’s rights to health andnutrition lies with national govern-ments in partnership with civil socie-ty. Governments have an importantrole in developing and implementingpolicies to lower the barriers to pri-mary health care, in improving thequality and efficiency of service
providers and in increasing publicaccountability. At the same time,health policies must be accountableto the communities and districts theyserve. Governments and health sys-tems must be closely attuned to theneeds and interests of the population.Developing effective, child-focusedhealth policies and building stronginstitutions between communities and health systems is critical; in mostcountries, increases in health expen-ditures will need to be accompaniedby substantial improvements in the policy environment to achievesignificant progress towards thehealth-related MillenniumDevelopment Goals.25
Finding the appropriate mix of
solutions for enhanced health
and nutrition outcomes
Each developing country has aunique mix of opportunities for, and constraints on, the developmentof its health system, owing to differ-ing levels of economic progress, environmental and institutional cir-cumstances, political situation andcurrent health-system capacity. As a result, there is no universally applicable method of fosteringimprovement. Some may find thattheir greatest challenge lies not in scaling up community-basedapproaches to essential health-carepackages nationwide, but in strength-ening and expanding service deliverythrough facility-based programmes,decentralizing health services, andaddressing non-communicable diseases and conditions, such as diabetes and obesity.26
For low-income countries, particu-larly those where large proportions
58 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Community-based programmes are strengthened when there is access to facility-basedcare. A health worker prepares a solution of oral rehydration salts, Eritrea.
© U
NIC
EF/
HQ
97-1
086/
Gia
com
o P
irozz
i
Context and challenge: Mozambique is one of the world’spoorest countries, with gross national income per capita ofjust US$340 in 2006 and an under-five mortality rate of 138deaths per 1,000 live births. Life expectancy at birth is just42 years, more than 40 per cent of children under five aresuffering from moderate or severe stunting, and only onethird of the population is using adequate sanitation facili-ties. Access to essential health-care services is limited, with23 per cent of infants lacking a measles vaccine. Only 10per cent of children sleep under a mosquito net (treated oruntreated). And almost two thirds of the population live in rural areas, where only 1 in every 4 has access to animproved source of drinking water.
The challenge was to deliver an effective community-based child survival programme to rural communities with poor physical and environmental health infrastruc-ture, and verify that the community programme con-tributed to mortality reduction.
Approach: The Chokwe Ministry of Health and World Reliefpartnership project in operation during 1999–2003 used the ‘Care Group’ approach to implement a child survivalprogramme that aimed to address three elements ofCommunity Integrated Management of Childhood Illness (C-IMCI):
• Improved partnerships between the health system andthe community.
• Increased accessible care for community-based providers.
• Promotion of essential household practices for child health.
The Care Group approach trains community educatorsthrough group interaction. One volunteer Women’s HealthEducator provides peer-to-peer health education to 15 sur-rounding households, and 10 Women Health Educatorsform a Care Group that meets once a month with a paidsupervisor. During monthly Care Group meetings, a healthfield staff member or a Women’s Health Educator supervi-sor presents health messages about child survival andwomen’s health. The Care Group members then practisetraining with each other, sharing the information presented.Before the next Care Group meeting, each volunteer isresponsible for visiting the households under her jurisdic-tion to relay the messages she has just learned.
The child survival programme was designed to be compre-hensive, integrating breastfeeding, complementary feed-
ing, use of oral rehydration therapy and insecticide-treatedmosquito nets. The programme strengthened referral tolocal health facilities and case management of common illnesses at the facilities.
Partnerships with UNICEF and the International Committeeof the Red Cross facilitated the provision of free insecti-cide-treated nets, vaccines and vitamin A supplements.Close cooperation with village health committees and localpastors provided support for the volunteers in carrying outhealth promotion and community mobilization for such asactivities as distribution of insecticide-treated mosquitonets and conducting immunization campaigns.
Results: The project also implemented a community-basedvital registration and health information system throughthe 2,300 community volunteers who collected data onbirths, deaths and childhood illnesses every month. Thesedata were aggregated during the monthly meetings and the registers sent to health posts operated by communityproviders, or socorristas, who were trained by the districtMinistry of Health. The collated information was sent backto local village health committees, health centres and theMinistry of Health.
Data from the community-based vital registration andhealth information system showed a 66 per cent reductionin infant mortality and a 62 per cent reduction in under-fivemortality. To check the reliability of these findings, an inde-pendent mortality assessment was carried out by experi-enced researchers using a pregnancy history survey basedon standard methodologies applied in the Demographicand Health Survey. This mortality survey found reductionsof 49 per cent and 42 per cent in infant mortality and under-five mortality, respectively.
These results demonstrated the effectiveness of theCommunity IMCI and validated the fact that communityhealth workers can collect reliable health data for monitor-ing mortality.
See References, page 107.
Mozambique: Reducing under-five mortality through
a community-based programme
FocusOn
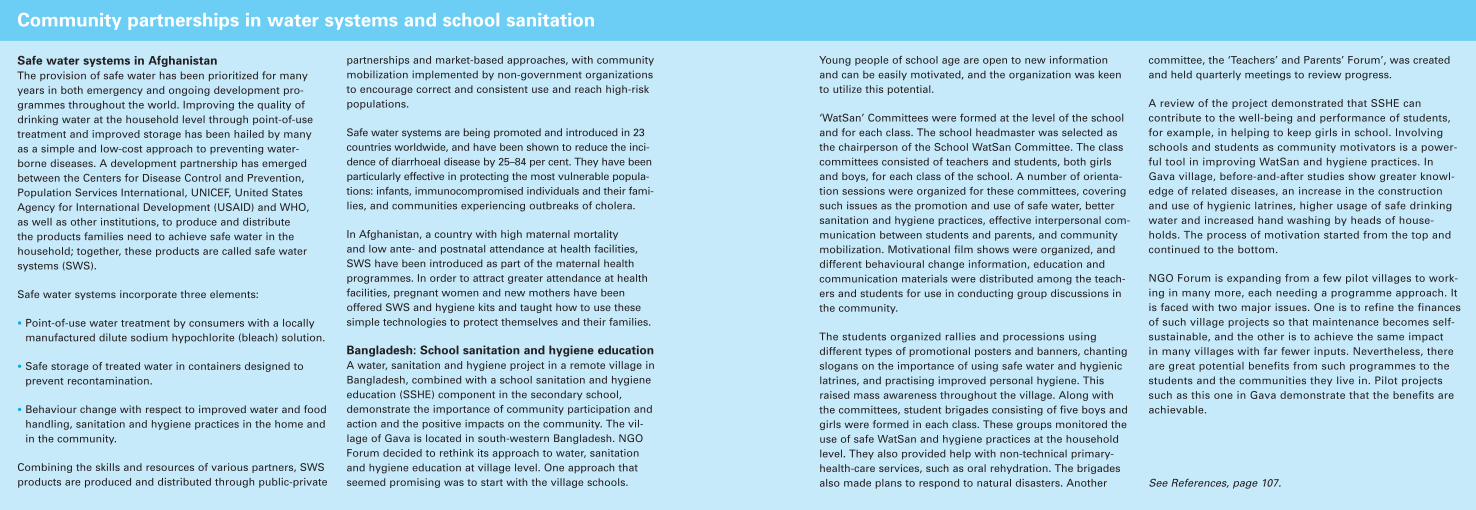
community partnerships must beconducted in conjunction with effortsto overcome system-wide bottlenecksin facility-based maternal and childhealth and nutrition services, andaddress other behavioural, institu-tional and environmental constraints.
The next chapter focuses on scalingup community partnerships in health,nutrition and environmental healthcare. Although many of the argumentscited are perhaps most applicable tolow-income countries and marginal-ized or impoverished communities,
much of the discourse is also relevantto countries and communities in lesschallenged circumstances.
C O M M U N I T Y P A R T N E R S H I P S I N P R I M A R Y H E A L T H C A R E 61
of mothers and children remainexcluded from facility-based pro-grammes, and whose health systemcapacity has been undermined byyears of underinvestment and mis-management, weak governance,mass migration of professionalhealth workers, complex emergenciesor the AIDS epidemic, determiningthe best strategy is neither straight-forward nor without risks. In suchcountries, an important and perhapsoverriding consideration is feasibili-ty, under the guise of the followingquestion: What is the most appropri-
ate, cost-effective, timely and sus-tainable strategy for improvingmaternal, newborn and child sur-vival and health and increasing cov-erage of essential services and com-modities, given the current strengthof a country’s health, nutrition andenvironmental health systems?27
The feasibility paradigm aims toaddress the urgent needs of the poorest and most marginalized soci-eties – where maternal, newborn andchild mortality rates are highest –that are most lacking in basic preven-
tive services, such as immunizationand access to drugs and emergencycare. In countries with relativelyweak health, nutrition and water and sanitation systems and low health-system capacity, community-basedapproaches that rely less on healthfacilities and outreach services canhelp expand coverage of essentialservices, products and practices –particularly if basic preventive servi-ces such as immunizations are alreadyin place.28 It must be stressed, however, that in order to underpinsustainability, the expansion of
60 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Safe water systems in Afghanistan
The provision of safe water has been prioritized for manyyears in both emergency and ongoing development pro-grammes throughout the world. Improving the quality ofdrinking water at the household level through point-of-usetreatment and improved storage has been hailed by manyas a simple and low-cost approach to preventing water-borne diseases. A development partnership has emergedbetween the Centers for Disease Control and Prevention,Population Services International, UNICEF, United StatesAgency for International Development (USAID) and WHO,as well as other institutions, to produce and distribute the products families need to achieve safe water in thehousehold; together, these products are called safe watersystems (SWS).
Safe water systems incorporate three elements:
• Point-of-use water treatment by consumers with a locallymanufactured dilute sodium hypochlorite (bleach) solution.
• Safe storage of treated water in containers designed to prevent recontamination.
• Behaviour change with respect to improved water and foodhandling, sanitation and hygiene practices in the home andin the community.
Combining the skills and resources of various partners, SWSproducts are produced and distributed through public-private
partnerships and market-based approaches, with communitymobilization implemented by non-government organizationsto encourage correct and consistent use and reach high-riskpopulations.
Safe water systems are being promoted and introduced in 23countries worldwide, and have been shown to reduce the inci-dence of diarrhoeal disease by 25–84 per cent. They have beenparticularly effective in protecting the most vulnerable popula-tions: infants, immunocompromised individuals and their fami-lies, and communities experiencing outbreaks of cholera.
In Afghanistan, a country with high maternal mortality and low ante- and postnatal attendance at health facilities,SWS have been introduced as part of the maternal health programmes. In order to attract greater attendance at healthfacilities, pregnant women and new mothers have beenoffered SWS and hygiene kits and taught how to use thesesimple technologies to protect themselves and their families.
Bangladesh: School sanitation and hygiene education
A water, sanitation and hygiene project in a remote village inBangladesh, combined with a school sanitation and hygieneeducation (SSHE) component in the secondary school,demonstrate the importance of community participation andaction and the positive impacts on the community. The vil-lage of Gava is located in south-western Bangladesh. NGOForum decided to rethink its approach to water, sanitationand hygiene education at village level. One approach thatseemed promising was to start with the village schools.
Community partnerships in water systems and school sanitation
Young people of school age are open to new information and can be easily motivated, and the organization was keento utilize this potential.
‘WatSan’ Committees were formed at the level of the schooland for each class. The school headmaster was selected asthe chairperson of the School WatSan Committee. The classcommittees consisted of teachers and students, both girlsand boys, for each class of the school. A number of orienta-tion sessions were organized for these committees, coveringsuch issues as the promotion and use of safe water, bettersanitation and hygiene practices, effective interpersonal com-munication between students and parents, and communitymobilization. Motivational film shows were organized, anddifferent behavioural change information, education andcommunication materials were distributed among the teach-ers and students for use in conducting group discussions inthe community.
The students organized rallies and processions using different types of promotional posters and banners, chantingslogans on the importance of using safe water and hygieniclatrines, and practising improved personal hygiene. Thisraised mass awareness throughout the village. Along withthe committees, student brigades consisting of five boys andgirls were formed in each class. These groups monitored theuse of safe WatSan and hygiene practices at the householdlevel. They also provided help with non-technical primary-health-care services, such as oral rehydration. The brigadesalso made plans to respond to natural disasters. Another
committee, the ‘Teachers’ and Parents’ Forum’, was createdand held quarterly meetings to review progress.
A review of the project demonstrated that SSHE can contribute to the well-being and performance of students,for example, in helping to keep girls in school. Involvingschools and students as community motivators is a power-ful tool in improving WatSan and hygiene practices. InGava village, before-and-after studies show greater knowl-edge of related diseases, an increase in the constructionand use of hygienic latrines, higher usage of safe drinkingwater and increased hand washing by heads of house-holds. The process of motivation started from the top andcontinued to the bottom.
NGO Forum is expanding from a few pilot villages to work-ing in many more, each needing a programme approach. Itis faced with two major issues. One is to refine the financesof such village projects so that maintenance becomes self-sustainable, and the other is to achieve the same impact in many villages with far fewer inputs. Nevertheless, thereare great potential benefits from such programmes to thestudents and the communities they live in. Pilot projectssuch as this one in Gava demonstrate that the benefits areachievable.
See References, page 107.
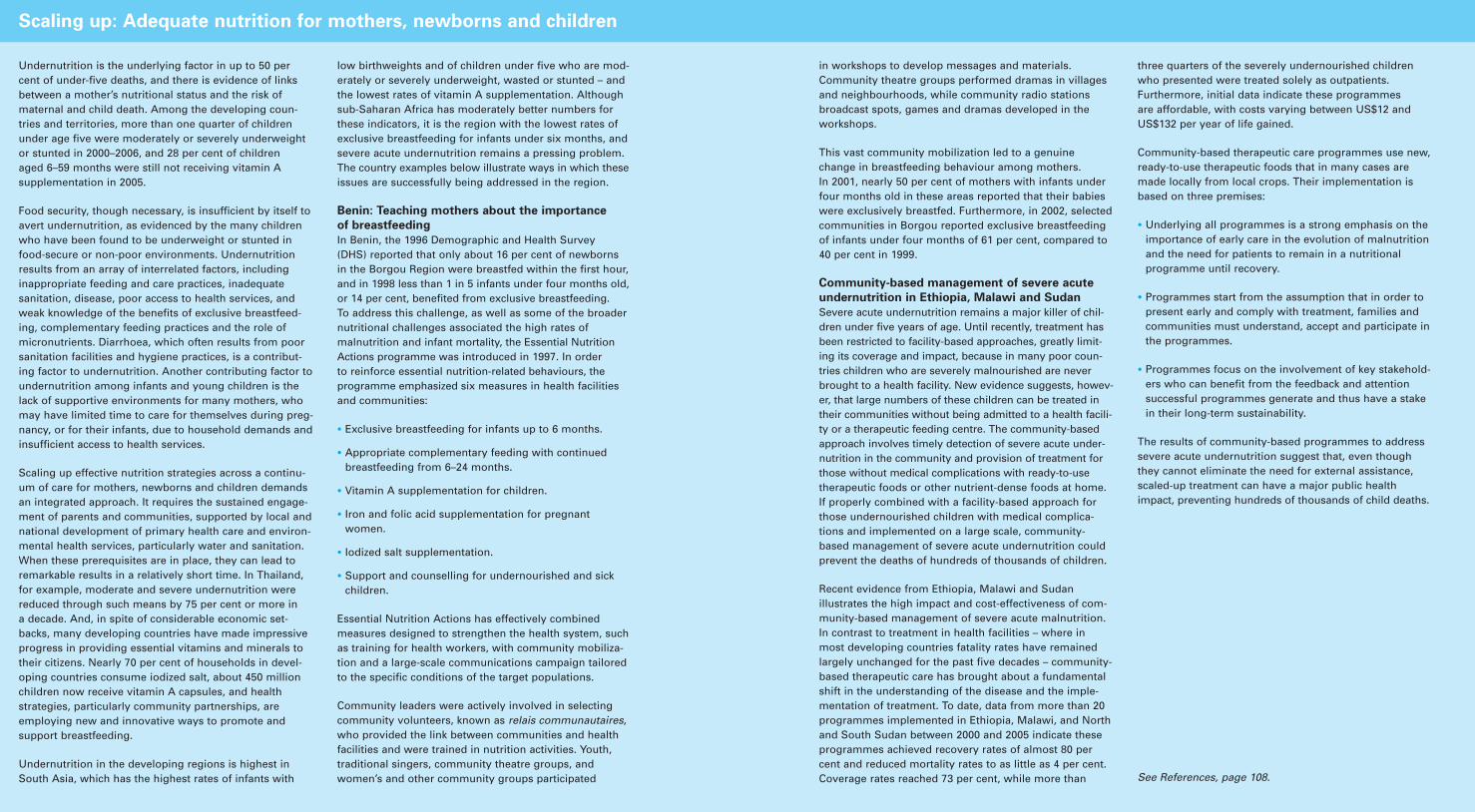
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 6766 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Undernutrition is the underlying factor in up to 50 percent of under-five deaths, and there is evidence of linksbetween a mother’s nutritional status and the risk ofmaternal and child death. Among the developing coun-tries and territories, more than one quarter of childrenunder age five were moderately or severely underweightor stunted in 2000–2006, and 28 per cent of children aged 6–59 months were still not receiving vitamin A supplementation in 2005.
Food security, though necessary, is insufficient by itself toavert undernutrition, as evidenced by the many childrenwho have been found to be underweight or stunted infood-secure or non-poor environments. Undernutritionresults from an array of interrelated factors, includinginappropriate feeding and care practices, inadequate sanitation, disease, poor access to health services, andweak knowledge of the benefits of exclusive breastfeed-ing, complementary feeding practices and the role ofmicronutrients. Diarrhoea, which often results from poorsanitation facilities and hygiene practices, is a contribut-ing factor to undernutrition. Another contributing factor toundernutrition among infants and young children is thelack of supportive environments for many mothers, whomay have limited time to care for themselves during preg-nancy, or for their infants, due to household demands andinsufficient access to health services.
Scaling up effective nutrition strategies across a continu-um of care for mothers, newborns and children demandsan integrated approach. It requires the sustained engage-ment of parents and communities, supported by local andnational development of primary health care and environ-mental health services, particularly water and sanitation.When these prerequisites are in place, they can lead toremarkable results in a relatively short time. In Thailand,for example, moderate and severe undernutrition werereduced through such means by 75 per cent or more in a decade. And, in spite of considerable economic set-backs, many developing countries have made impressiveprogress in providing essential vitamins and minerals totheir citizens. Nearly 70 per cent of households in devel-oping countries consume iodized salt, about 450 millionchildren now receive vitamin A capsules, and healthstrategies, particularly community partnerships, areemploying new and innovative ways to promote and support breastfeeding.
Undernutrition in the developing regions is highest inSouth Asia, which has the highest rates of infants with
low birthweights and of children under five who are mod-erately or severely underweight, wasted or stunted – andthe lowest rates of vitamin A supplementation. Althoughsub-Saharan Africa has moderately better numbers forthese indicators, it is the region with the lowest rates ofexclusive breastfeeding for infants under six months, andsevere acute undernutrition remains a pressing problem.The country examples below illustrate ways in which theseissues are successfully being addressed in the region.
Benin: Teaching mothers about the importance
of breastfeeding
In Benin, the 1996 Demographic and Health Survey (DHS) reported that only about 16 per cent of newborns in the Borgou Region were breastfed within the first hour,and in 1998 less than 1 in 5 infants under four months old,or 14 per cent, benefited from exclusive breastfeeding.To address this challenge, as well as some of the broadernutritional challenges associated the high rates of malnutrition and infant mortality, the Essential NutritionActions programme was introduced in 1997. In order to reinforce essential nutrition-related behaviours, the programme emphasized six measures in health facilities and communities:
• Exclusive breastfeeding for infants up to 6 months.
• Appropriate complementary feeding with continuedbreastfeeding from 6–24 months.
• Vitamin A supplementation for children.
• Iron and folic acid supplementation for pregnantwomen.
• Iodized salt supplementation.
• Support and counselling for undernourished and sickchildren.
Essential Nutrition Actions has effectively combinedmeasures designed to strengthen the health system, suchas training for health workers, with community mobiliza-tion and a large-scale communications campaign tailoredto the specific conditions of the target populations.
Community leaders were actively involved in selectingcommunity volunteers, known as relais communautaires,who provided the link between communities and healthfacilities and were trained in nutrition activities. Youth,traditional singers, community theatre groups, andwomen’s and other community groups participated
Scaling up: Adequate nutrition for mothers, newborns and children
in workshops to develop messages and materials.Community theatre groups performed dramas in villagesand neighbourhoods, while community radio stationsbroadcast spots, games and dramas developed in theworkshops.
This vast community mobilization led to a genuinechange in breastfeeding behaviour among mothers. In 2001, nearly 50 per cent of mothers with infants underfour months old in these areas reported that their babieswere exclusively breastfed. Furthermore, in 2002, selectedcommunities in Borgou reported exclusive breastfeedingof infants under four months of 61 per cent, compared to40 per cent in 1999.
Community-based management of severe acute
undernutrition in Ethiopia, Malawi and Sudan
Severe acute undernutrition remains a major killer of chil-dren under five years of age. Until recently, treatment hasbeen restricted to facility-based approaches, greatly limit-ing its coverage and impact, because in many poor coun-tries children who are severely malnourished are neverbrought to a health facility. New evidence suggests, howev-er, that large numbers of these children can be treated intheir communities without being admitted to a health facili-ty or a therapeutic feeding centre. The community-basedapproach involves timely detection of severe acute under-nutrition in the community and provision of treatment forthose without medical complications with ready-to-usetherapeutic foods or other nutrient-dense foods at home.If properly combined with a facility-based approach forthose undernourished children with medical complica-tions and implemented on a large scale, community-based management of severe acute undernutrition couldprevent the deaths of hundreds of thousands of children.
Recent evidence from Ethiopia, Malawi and Sudan illustrates the high impact and cost-effectiveness of com-munity-based management of severe acute malnutrition.In contrast to treatment in health facilities – where inmost developing countries fatality rates have remainedlargely unchanged for the past five decades – community-based therapeutic care has brought about a fundamentalshift in the understanding of the disease and the imple-mentation of treatment. To date, data from more than 20programmes implemented in Ethiopia, Malawi, and Northand South Sudan between 2000 and 2005 indicate theseprogrammes achieved recovery rates of almost 80 percent and reduced mortality rates to as little as 4 per cent.Coverage rates reached 73 per cent, while more than
three quarters of the severely undernourished childrenwho presented were treated solely as outpatients.Furthermore, initial data indicate these programmes are affordable, with costs varying between US$12 andUS$132 per year of life gained.
Community-based therapeutic care programmes use new,ready-to-use therapeutic foods that in many cases aremade locally from local crops. Their implementation isbased on three premises:
• Underlying all programmes is a strong emphasis on theimportance of early care in the evolution of malnutritionand the need for patients to remain in a nutritional programme until recovery.
• Programmes start from the assumption that in order topresent early and comply with treatment, families andcommunities must understand, accept and participate inthe programmes.
• Programmes focus on the involvement of key stakehold-ers who can benefit from the feedback and attentionsuccessful programmes generate and thus have a stakein their long-term sustainability.
The results of community-based programmes to addresssevere acute undernutrition suggest that, even thoughthey cannot eliminate the need for external assistance,scaled-up treatment can have a major public healthimpact, preventing hundreds of thousands of child deaths.
See References, page 108.
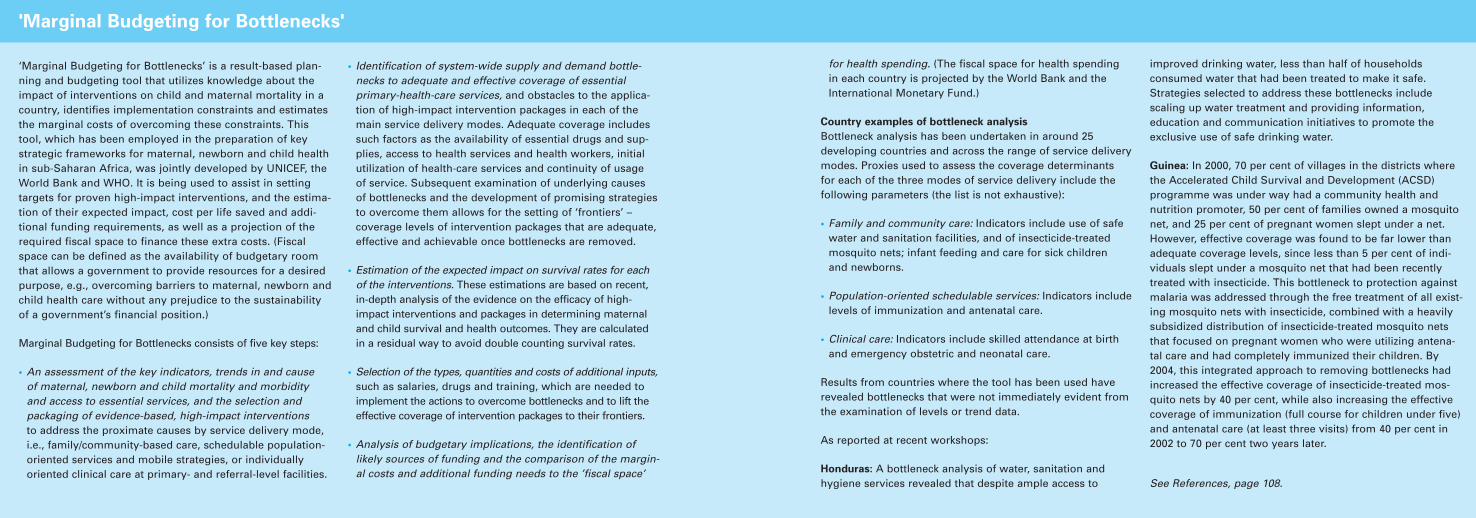
for countries with low health-systemcapacity are as follows:
Phase one: The initial phasefocuses on reducing by half system-wide bottlenecks for fami-ly/community-based care andpopulation-oriented outreachservices, fostering demand forquality clinical services and pro-viding a minimum package ofhigh impact, low-cost interven-tions that can be implementedgiven the current policy, humanresources and capacity conditions.
Operational strategies include the training and deployment ofcommunity health and nutritionpromoters for improved familycare practices. The minimumpackage of interventions typicallyincludes the following components:
• Antimalaria interventions
• Nutrition
• Hygiene promotion
• Immunization complemented
by measles mortality reductioncampaigns
• Integrated Management ofNeonatal and Childhood Illnesses
• Skilled delivery and newborn care and emergency obstetric care
• HIV and AIDS prevention andtreatment
• Facility-based care
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 71
operating was one third to one halfof the average under-five mortalityrate in the control districts.13
Phase in intervention packages
and strengthen health systems
It is increasingly recognized thatactions to scale up packages of inter-ventions may need to be phased,depending on such contingencies as budget availability, logistical con-straints, technical capacity or socio-economic and cultural factors. Whilesome interventions may be rapidlyexpanded, others will require a longer
time frame. Scaling up minimum pack-ages of essential interventions forms akey component of the new strategies,with the aim of achieving specific coverage targets. Intervention packagesare being prepared to meet theseagreed targets through the three coreservice delivery modes discussed previ-ously, delivered in three phases.14
A phased approach to health servicedelivery will allow each country todefine and implement an initial package of interventions that canthen be expanded over time. Both
the packaging and the delivery of the priority interventions will depend on the country’s health-system capacity. The gradual removalof bottlenecks will facilitate theexpansion of service delivery –including in situations of complexemergencies. Since the packagedapproach is results-oriented, theimplementation of priority interven-tions at scale can be planned andmonitored in a phased manner.
The three phases recommended forexpanding service delivery coverage
70 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
‘Marginal Budgeting for Bottlenecks’ is a result-based plan-ning and budgeting tool that utilizes knowledge about theimpact of interventions on child and maternal mortality in acountry, identifies implementation constraints and estimatesthe marginal costs of overcoming these constraints. Thistool, which has been employed in the preparation of keystrategic frameworks for maternal, newborn and child healthin sub-Saharan Africa, was jointly developed by UNICEF, theWorld Bank and WHO. It is being used to assist in setting targets for proven high-impact interventions, and the estima-tion of their expected impact, cost per life saved and addi-tional funding requirements, as well as a projection of therequired fiscal space to finance these extra costs. (Fiscalspace can be defined as the availability of budgetary roomthat allows a government to provide resources for a desiredpurpose, e.g., overcoming barriers to maternal, newborn andchild health care without any prejudice to the sustainabilityof a government’s financial position.)
Marginal Budgeting for Bottlenecks consists of five key steps:
• An assessment of the key indicators, trends in and cause of maternal, newborn and child mortality and morbidity and access to essential services, and the selection and packaging of evidence-based, high-impact interventionsto address the proximate causes by service delivery mode,i.e., family/community-based care, schedulable population-oriented services and mobile strategies, or individually oriented clinical care at primary- and referral-level facilities.
• Identification of system-wide supply and demand bottle-necks to adequate and effective coverage of essential primary-health-care services, and obstacles to the applica-tion of high-impact intervention packages in each of themain service delivery modes. Adequate coverage includessuch factors as the availability of essential drugs and sup-plies, access to health services and health workers, initialutilization of health-care services and continuity of usage of service. Subsequent examination of underlying causes of bottlenecks and the development of promising strategiesto overcome them allows for the setting of ‘frontiers’ – coverage levels of intervention packages that are adequate,effective and achievable once bottlenecks are removed.
• Estimation of the expected impact on survival rates for eachof the interventions. These estimations are based on recent,in-depth analysis of the evidence on the efficacy of high-impact interventions and packages in determining maternaland child survival and health outcomes. They are calculated in a residual way to avoid double counting survival rates.
• Selection of the types, quantities and costs of additional inputs,such as salaries, drugs and training, which are needed toimplement the actions to overcome bottlenecks and to lift theeffective coverage of intervention packages to their frontiers.
• Analysis of budgetary implications, the identification of likely sources of funding and the comparison of the margin-al costs and additional funding needs to the ’fiscal space’
'Marginal Budgeting for Bottlenecks'
for health spending. (The fiscal space for health spending in each country is projected by the World Bank and theInternational Monetary Fund.)
Country examples of bottleneck analysis
Bottleneck analysis has been undertaken in around 25 developing countries and across the range of service deliverymodes. Proxies used to assess the coverage determinants for each of the three modes of service delivery include thefollowing parameters (the list is not exhaustive):
• Family and community care: Indicators include use of safewater and sanitation facilities, and of insecticide-treatedmosquito nets; infant feeding and care for sick children and newborns.
• Population-oriented schedulable services: Indicators includelevels of immunization and antenatal care.
• Clinical care: Indicators include skilled attendance at birthand emergency obstetric and neonatal care.
Results from countries where the tool has been used haverevealed bottlenecks that were not immediately evident fromthe examination of levels or trend data.
As reported at recent workshops:
Honduras: A bottleneck analysis of water, sanitation andhygiene services revealed that despite ample access to
improved drinking water, less than half of households consumed water that had been treated to make it safe.Strategies selected to address these bottlenecks include scaling up water treatment and providing information, education and communication initiatives to promote theexclusive use of safe drinking water.
Guinea: In 2000, 70 per cent of villages in the districts wherethe Accelerated Child Survival and Development (ACSD) programme was under way had a community health and nutrition promoter, 50 per cent of families owned a mosquitonet, and 25 per cent of pregnant women slept under a net.However, effective coverage was found to be far lower thanadequate coverage levels, since less than 5 per cent of indi-viduals slept under a mosquito net that had been recentlytreated with insecticide. This bottleneck to protection againstmalaria was addressed through the free treatment of all exist-ing mosquito nets with insecticide, combined with a heavilysubsidized distribution of insecticide-treated mosquito netsthat focused on pregnant women who were utilizing antena-tal care and had completely immunized their children. By2004, this integrated approach to removing bottlenecks hadincreased the effective coverage of insecticide-treated mos-quito nets by 40 per cent, while also increasing the effectivecoverage of immunization (full course for children under five)and antenatal care (at least three visits) from 40 per cent in2002 to 70 per cent two years later.
See References, page 108.
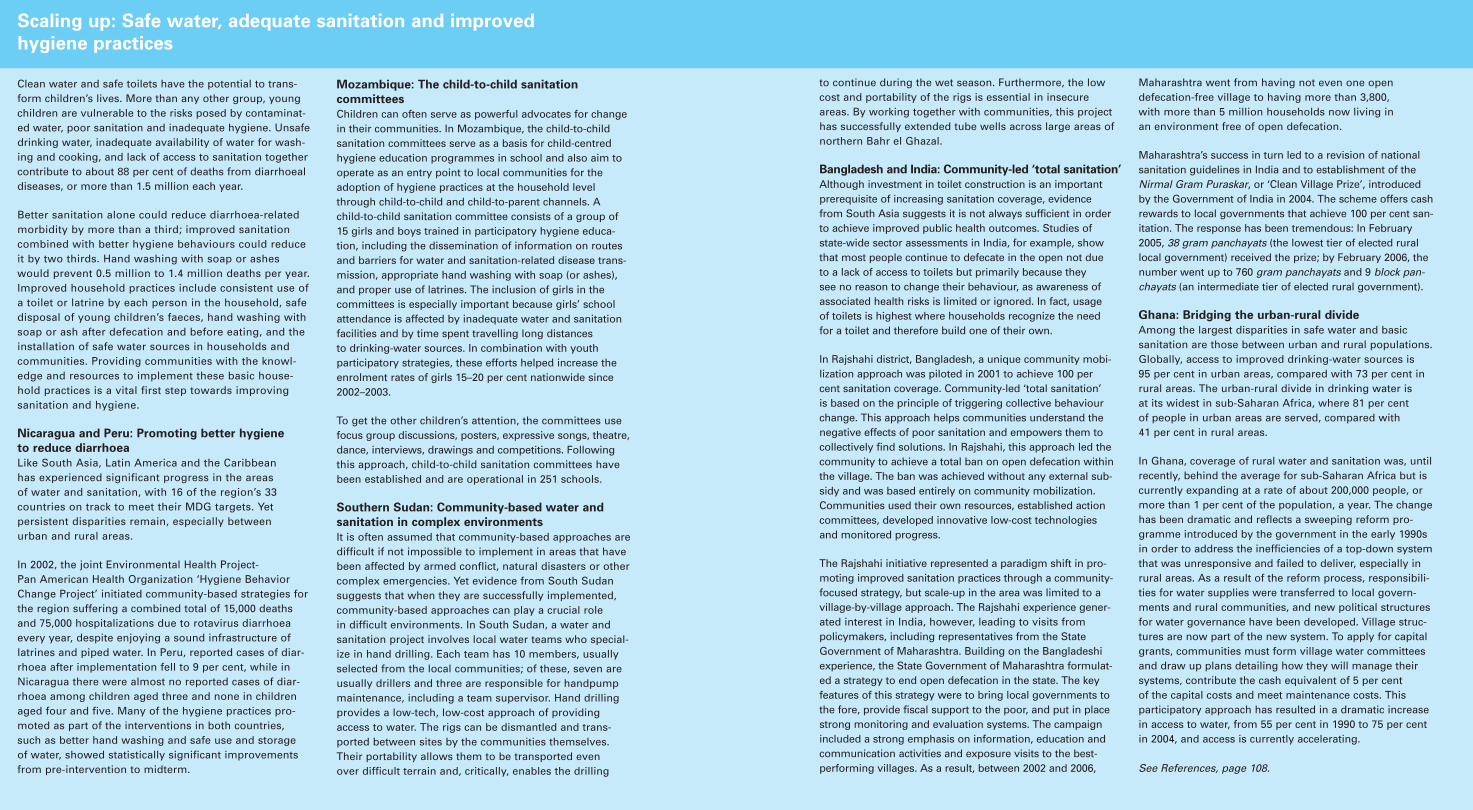
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 7574 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Clean water and safe toilets have the potential to trans-form children’s lives. More than any other group, young children are vulnerable to the risks posed by contaminat-ed water, poor sanitation and inadequate hygiene. Unsafedrinking water, inadequate availability of water for wash-ing and cooking, and lack of access to sanitation togethercontribute to about 88 per cent of deaths from diarrhoealdiseases, or more than 1.5 million each year.
Better sanitation alone could reduce diarrhoea-relatedmorbidity by more than a third; improved sanitationcombined with better hygiene behaviours could reduceit by two thirds. Hand washing with soap or asheswould prevent 0.5 million to 1.4 million deaths per year.Improved household practices include consistent use ofa toilet or latrine by each person in the household, safedisposal of young children’s faeces, hand washing withsoap or ash after defecation and before eating, and theinstallation of safe water sources in households andcommunities. Providing communities with the knowl-edge and resources to implement these basic house-hold practices is a vital first step towards improvingsanitation and hygiene.
Nicaragua and Peru: Promoting better hygiene
to reduce diarrhoea
Like South Asia, Latin America and the Caribbean has experienced significant progress in the areas of water and sanitation, with 16 of the region’s 33 countries on track to meet their MDG targets. Yet persistent disparities remain, especially between urban and rural areas.
In 2002, the joint Environmental Health Project-Pan American Health Organization ‘Hygiene BehaviorChange Project’ initiated community-based strategies forthe region suffering a combined total of 15,000 deathsand 75,000 hospitalizations due to rotavirus diarrhoeaevery year, despite enjoying a sound infrastructure oflatrines and piped water. In Peru, reported cases of diar-rhoea after implementation fell to 9 per cent, while inNicaragua there were almost no reported cases of diar-rhoea among children aged three and none in childrenaged four and five. Many of the hygiene practices pro-moted as part of the interventions in both countries, such as better hand washing and safe use and storage of water, showed statistically significant improvementsfrom pre-intervention to midterm.
Mozambique: The child-to-child sanitation
committees
Children can often serve as powerful advocates for changein their communities. In Mozambique, the child-to-childsanitation committees serve as a basis for child-centredhygiene education programmes in school and also aim tooperate as an entry point to local communities for theadoption of hygiene practices at the household levelthrough child-to-child and child-to-parent channels. A child-to-child sanitation committee consists of a group of15 girls and boys trained in participatory hygiene educa-tion, including the dissemination of information on routesand barriers for water and sanitation-related disease trans-mission, appropriate hand washing with soap (or ashes),and proper use of latrines. The inclusion of girls in thecommittees is especially important because girls’ schoolattendance is affected by inadequate water and sanitationfacilities and by time spent travelling long distances to drinking-water sources. In combination with youth participatory strategies, these efforts helped increase theenrolment rates of girls 15–20 per cent nationwide since2002–2003.
To get the other children’s attention, the committees usefocus group discussions, posters, expressive songs, theatre,dance, interviews, drawings and competitions. Followingthis approach, child-to-child sanitation committees havebeen established and are operational in 251 schools.
Southern Sudan: Community-based water and
sanitation in complex environments
It is often assumed that community-based approaches aredifficult if not impossible to implement in areas that havebeen affected by armed conflict, natural disasters or othercomplex emergencies. Yet evidence from South Sudansuggests that when they are successfully implemented,community-based approaches can play a crucial role in difficult environments. In South Sudan, a water andsanitation project involves local water teams who special-ize in hand drilling. Each team has 10 members, usuallyselected from the local communities; of these, seven areusually drillers and three are responsible for handpumpmaintenance, including a team supervisor. Hand drillingprovides a low-tech, low-cost approach of providingaccess to water. The rigs can be dismantled and trans-ported between sites by the communities themselves.Their portability allows them to be transported even over difficult terrain and, critically, enables the drilling
Scaling up: Safe water, adequate sanitation and improved
hygiene practices
to continue during the wet season. Furthermore, the lowcost and portability of the rigs is essential in insecureareas. By working together with communities, this projecthas successfully extended tube wells across large areas ofnorthern Bahr el Ghazal.
Bangladesh and India: Community-led ‘total sanitation’
Although investment in toilet construction is an importantprerequisite of increasing sanitation coverage, evidencefrom South Asia suggests it is not always sufficient in orderto achieve improved public health outcomes. Studies ofstate-wide sector assessments in India, for example, showthat most people continue to defecate in the open not dueto a lack of access to toilets but primarily because they see no reason to change their behaviour, as awareness ofassociated health risks is limited or ignored. In fact, usageof toilets is highest where households recognize the needfor a toilet and therefore build one of their own.
In Rajshahi district, Bangladesh, a unique community mobi-lization approach was piloted in 2001 to achieve 100 percent sanitation coverage. Community-led ‘total sanitation’ is based on the principle of triggering collective behaviourchange. This approach helps communities understand thenegative effects of poor sanitation and empowers them tocollectively find solutions. In Rajshahi, this approach led thecommunity to achieve a total ban on open defecation withinthe village. The ban was achieved without any external sub-sidy and was based entirely on community mobilization.Communities used their own resources, established actioncommittees, developed innovative low-cost technologiesand monitored progress.
The Rajshahi initiative represented a paradigm shift in pro-moting improved sanitation practices through a community-focused strategy, but scale-up in the area was limited to avillage-by-village approach. The Rajshahi experience gener-ated interest in India, however, leading to visits from policymakers, including representatives from the StateGovernment of Maharashtra. Building on the Bangladeshiexperience, the State Government of Maharashtra formulat-ed a strategy to end open defecation in the state. The keyfeatures of this strategy were to bring local governments tothe fore, provide fiscal support to the poor, and put in placestrong monitoring and evaluation systems. The campaignincluded a strong emphasis on information, education andcommunication activities and exposure visits to the best-performing villages. As a result, between 2002 and 2006,
Maharashtra went from having not even one open defecation-free village to having more than 3,800, with more than 5 million households now living in an environment free of open defecation.
Maharashtra’s success in turn led to a revision of nationalsanitation guidelines in India and to establishment of theNirmal Gram Puraskar, or ‘Clean Village Prize’, introducedby the Government of India in 2004. The scheme offers cashrewards to local governments that achieve 100 per cent san-itation. The response has been tremendous: In February2005, 38 gram panchayats (the lowest tier of elected rurallocal government) received the prize; by February 2006, thenumber went up to 760 gram panchayats and 9 block pan-chayats (an intermediate tier of elected rural government).
Ghana: Bridging the urban-rural divide
Among the largest disparities in safe water and basic sanitation are those between urban and rural populations.Globally, access to improved drinking-water sources is 95 per cent in urban areas, compared with 73 per cent inrural areas. The urban-rural divide in drinking water is at its widest in sub-Saharan Africa, where 81 per cent of people in urban areas are served, compared with 41 per cent in rural areas.
In Ghana, coverage of rural water and sanitation was, untilrecently, behind the average for sub-Saharan Africa but iscurrently expanding at a rate of about 200,000 people, ormore than 1 per cent of the population, a year. The changehas been dramatic and reflects a sweeping reform pro-gramme introduced by the government in the early 1990sin order to address the inefficiencies of a top-down systemthat was unresponsive and failed to deliver, especially inrural areas. As a result of the reform process, responsibili-ties for water supplies were transferred to local govern-ments and rural communities, and new political structuresfor water governance have been developed. Village struc-tures are now part of the new system. To apply for capitalgrants, communities must form village water committeesand draw up plans detailing how they will manage theirsystems, contribute the cash equivalent of 5 per cent of the capital costs and meet maintenance costs. This participatory approach has resulted in a dramatic increasein access to water, from 55 per cent in 1990 to 75 per centin 2004, and access is currently accelerating.
See References, page 108.
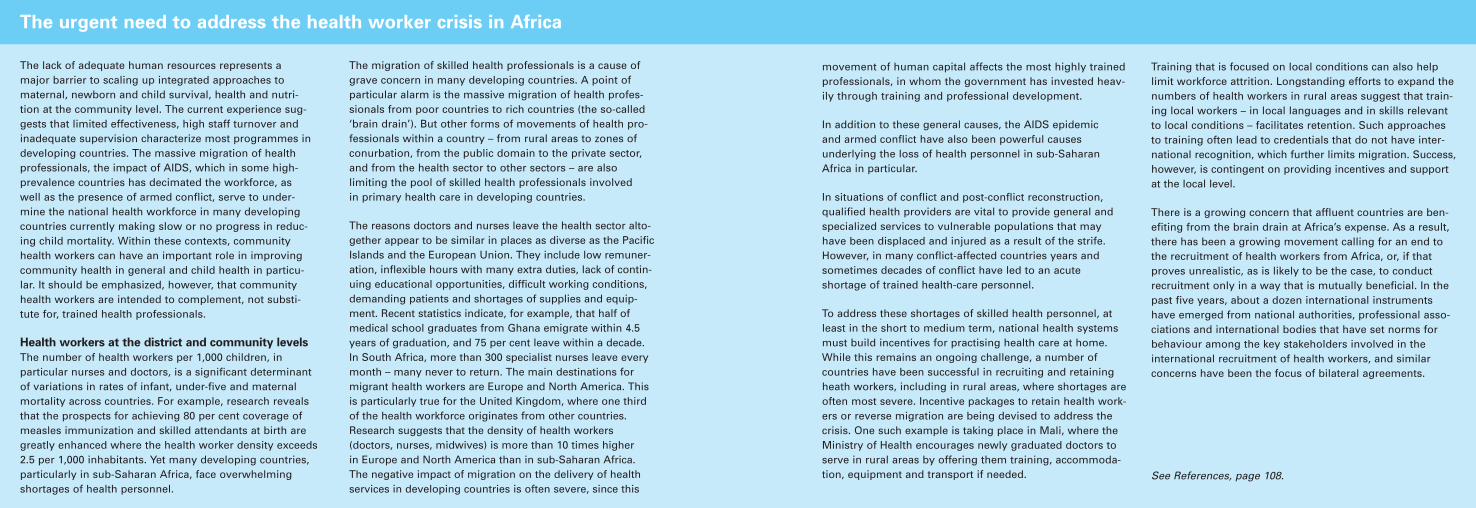
tres, family practices or equivalentdecentralized structures, backed byreferral hospitals. Where districtshave become stable and viable structures, they have demostratednotable results, even under situationsof complex emergencies, as in theDemocratic Republic of the Congoand Guinea. Similarly, Mali hasbroadened its health-centre networksand services for mothers andchildren.21 In countries where decen-tralization has been accompanied byreforms of public administration,there has been significant progresswithin a few years. Examples include
Mozambique, Rwanda and Uganda,all countries that experienced manyyears of conflict and economic col-lapse but have since made significantprogress in reforming governmentinstitutions and performance, includ-ing their health systems.22
In recent decades, evidence on the performance of district health systems has grown. However, the evidence base is still relatively small,the study coverage is inconsistent,and the approaches advocated bypractitioners do not enjoy the samelevel of consensus and visibility
within the scientific community asthose on essential interventions.
Work on the district approach todelivering the continuum of mater-nal, newborn and child health carerequires a new impetus and morerigorous systematization. In particu-lar, a key focus of research should be on the reorientation of nationalhealth systems to create the condi-tions in which district health andnutrition systems providing a contin-uum of care can thrive. Systematicanalysis and case studies from coun-tries that have tried this approach
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 77
These countries are also consolidatingtheir bottlenecks, startegies, expectedhealth outcomes and additional fund-ing needs into ‘investment cases’ toleverage political and financial supportfor their national plans.
Strengthen health systems at the
district level
Strengthening health systems remainsa daunting and complex task, espe-cially in many of countries that aremaking insufficient progress towardsthe health-related MDGs. The decen-tralization of health systems and anincreasing focus on the district level
can be seen as an effective vehicle for delivering primary health care tomarginalized children and families atthe community level.18 But decentral-ization is not without risks: It canhave unintended consequences, suchas deepening existing inequalities incommunities, based on factors suchas poverty, gender, language and ethnicity.19 Furthermore, even wheredecentralization efforts have been successful, experience suggests thattransforming an administrative dis-trict into a functional health systemtakes time. In 2000, for example,only 13 of Niger’s district hospitals
were equipped to perform aCaesarean section. Only 17 of the 53 district hospitals in Burkina Fasohad appropriate facilities 10 yearsafter districts had been established;moreover, only 5 of those 17 hospi-tals had the three doctors required to ensure continuity of care through-out the year.20
Nevertheless, the experience of decen-tralization during the past decadesuggests that, on balance, health dis-tricts remain a rational way for gov-ernments to roll out primary healthcare through networks of health cen-
76 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The lack of adequate human resources represents amajor barrier to scaling up integrated approaches tomaternal, newborn and child survival, health and nutri-tion at the community level. The current experience sug-gests that limited effectiveness, high staff turnover andinadequate supervision characterize most programmes indeveloping countries. The massive migration of healthprofessionals, the impact of AIDS, which in some high-prevalence countries has decimated the workforce, aswell as the presence of armed conflict, serve to under-mine the national health workforce in many developingcountries currently making slow or no progress in reduc-ing child mortality. Within these contexts, communityhealth workers can have an important role in improvingcommunity health in general and child health in particu-lar. It should be emphasized, however, that communityhealth workers are intended to complement, not substi-tute for, trained health professionals.
Health workers at the district and community levels
The number of health workers per 1,000 children, in particular nurses and doctors, is a significant determinantof variations in rates of infant, under-five and maternalmortality across countries. For example, research revealsthat the prospects for achieving 80 per cent coverage ofmeasles immunization and skilled attendants at birth aregreatly enhanced where the health worker density exceeds2.5 per 1,000 inhabitants. Yet many developing countries,particularly in sub-Saharan Africa, face overwhelmingshortages of health personnel.
The migration of skilled health professionals is a cause ofgrave concern in many developing countries. A point ofparticular alarm is the massive migration of health profes-sionals from poor countries to rich countries (the so-called‘brain drain’). But other forms of movements of health pro-fessionals within a country – from rural areas to zones ofconurbation, from the public domain to the private sector,and from the health sector to other sectors – are also limiting the pool of skilled health professionals involved in primary health care in developing countries.
The reasons doctors and nurses leave the health sector alto-gether appear to be similar in places as diverse as the PacificIslands and the European Union. They include low remuner-ation, inflexible hours with many extra duties, lack of contin-uing educational opportunities, difficult working conditions,demanding patients and shortages of supplies and equip-ment. Recent statistics indicate, for example, that half ofmedical school graduates from Ghana emigrate within 4.5years of graduation, and 75 per cent leave within a decade.In South Africa, more than 300 specialist nurses leave everymonth – many never to return. The main destinations formigrant health workers are Europe and North America. Thisis particularly true for the United Kingdom, where one thirdof the health workforce originates from other countries.Research suggests that the density of health workers (doctors, nurses, midwives) is more than 10 times higher in Europe and North America than in sub-Saharan Africa. The negative impact of migration on the delivery of health services in developing countries is often severe, since this
The urgent need to address the health worker crisis in Africa
movement of human capital affects the most highly trainedprofessionals, in whom the government has invested heav-ily through training and professional development.
In addition to these general causes, the AIDS epidemicand armed conflict have also been powerful causesunderlying the loss of health personnel in sub-SaharanAfrica in particular.
In situations of conflict and post-conflict reconstruction,qualified health providers are vital to provide general andspecialized services to vulnerable populations that mayhave been displaced and injured as a result of the strife.However, in many conflict-affected countries years andsometimes decades of conflict have led to an acute shortage of trained health-care personnel.
To address these shortages of skilled health personnel, atleast in the short to medium term, national health systemsmust build incentives for practising health care at home.While this remains an ongoing challenge, a number ofcountries have been successful in recruiting and retainingheath workers, including in rural areas, where shortages areoften most severe. Incentive packages to retain health work-ers or reverse migration are being devised to address thecrisis. One such example is taking place in Mali, where theMinistry of Health encourages newly graduated doctors toserve in rural areas by offering them training, accommoda-tion, equipment and transport if needed.
Training that is focused on local conditions can also helplimit workforce attrition. Longstanding efforts to expand thenumbers of health workers in rural areas suggest that train-ing local workers – in local languages and in skills relevantto local conditions – facilitates retention. Such approachesto training often lead to credentials that do not have inter-national recognition, which further limits migration. Success,however, is contingent on providing incentives and supportat the local level.
There is a growing concern that affluent countries are ben-efiting from the brain drain at Africa’s expense. As a result,there has been a growing movement calling for an end tothe recruitment of health workers from Africa, or, if thatproves unrealistic, as is likely to be the case, to conductrecruitment only in a way that is mutually beneficial. In thepast five years, about a dozen international instrumentshave emerged from national authorities, professional asso-ciations and international bodies that have set norms forbehaviour among the key stakeholders involved in theinternational recruitment of health workers, and similarconcerns have been the focus of bilateral agreements.
See References, page 108.
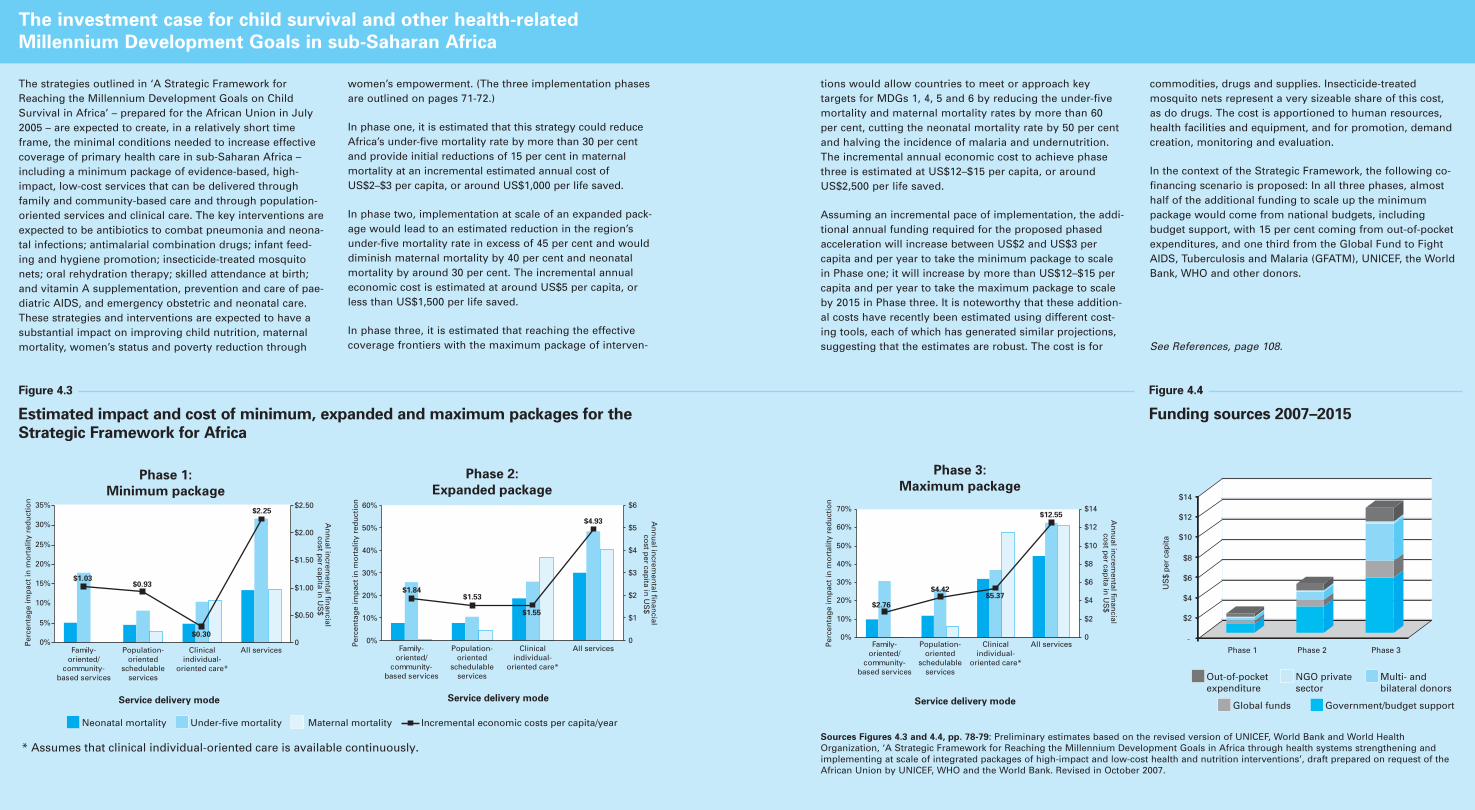
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 7978 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The strategies outlined in ‘A Strategic Framework forReaching the Millennium Development Goals on ChildSurvival in Africa’ – prepared for the African Union in July2005 – are expected to create, in a relatively short timeframe, the minimal conditions needed to increase effectivecoverage of primary health care in sub-Saharan Africa –including a minimum package of evidence-based, high-impact, low-cost services that can be delivered throughfamily and community-based care and through population-oriented services and clinical care. The key interventions areexpected to be antibiotics to combat pneumonia and neona-tal infections; antimalarial combination drugs; infant feed-ing and hygiene promotion; insecticide-treated mosquitonets; oral rehydration therapy; skilled attendance at birth;and vitamin A supplementation, prevention and care of pae-diatric AIDS, and emergency obstetric and neonatal care.These strategies and interventions are expected to have asubstantial impact on improving child nutrition, maternalmortality, women’s status and poverty reduction through
women’s empowerment. (The three implementation phasesare outlined on pages 71-72.)
In phase one, it is estimated that this strategy could reduceAfrica’s under-five mortality rate by more than 30 per centand provide initial reductions of 15 per cent in maternalmortality at an incremental estimated annual cost ofUS$2–$3 per capita, or around US$1,000 per life saved.
In phase two, implementation at scale of an expanded pack-age would lead to an estimated reduction in the region’sunder-five mortality rate in excess of 45 per cent and woulddiminish maternal mortality by 40 per cent and neonatalmortality by around 30 per cent. The incremental annualeconomic cost is estimated at around US$5 per capita, orless than US$1,500 per life saved.
In phase three, it is estimated that reaching the effectivecoverage frontiers with the maximum package of interven-
The investment case for child survival and other health-related
Millennium Development Goals in sub-Saharan Africa
tions would allow countries to meet or approach key targets for MDGs 1, 4, 5 and 6 by reducing the under-fivemortality and maternal mortality rates by more than 60 per cent, cutting the neonatal mortality rate by 50 per centand halving the incidence of malaria and undernutrition.The incremental annual economic cost to achieve phasethree is estimated at US$12–$15 per capita, or aroundUS$2,500 per life saved.
Assuming an incremental pace of implementation, the addi-tional annual funding required for the proposed phasedacceleration will increase between US$2 and US$3 per capita and per year to take the minimum package to scalein Phase one; it will increase by more than US$12–$15 percapita and per year to take the maximum package to scaleby 2015 in Phase three. It is noteworthy that these addition-al costs have recently been estimated using different cost-ing tools, each of which has generated similar projections,suggesting that the estimates are robust. The cost is for
commodities, drugs and supplies. Insecticide-treated mosquito nets represent a very sizeable share of this cost,as do drugs. The cost is apportioned to human resources,health facilities and equipment, and for promotion, demandcreation, monitoring and evaluation.
In the context of the Strategic Framework, the following co-financing scenario is proposed: In all three phases, almosthalf of the additional funding to scale up the minimumpackage would come from national budgets, includingbudget support, with 15 per cent coming from out-of-pocketexpenditures, and one third from the Global Fund to FightAIDS, Tuberculosis and Malaria (GFATM), UNICEF, the WorldBank, WHO and other donors.
See References, page 108.
* Assumes that clinical individual-oriented care is available continuously.
Phase 1:
Minimum package
$2.25
$1.03$0.93
$0.300%
5%
10%
15%
20%
25%
30%
35%
Family-oriented/
community-based services
Population-oriented
schedulableservices
Clinicalindividual-
oriented care*
All services Family-oriented/
community-based services
Population-oriented
schedulableservices
Clinicalindividual-
oriented care*
All services Family-oriented/
community-based services
Population-oriented
schedulableservices
Clinicalindividual-
oriented care*
All services
Service delivery mode
Per
cen
tag
e im
pac
t in
mo
rtal
ity
red
uct
ion
An
nu
al increm
ental fin
ancial
cost p
er capita in
US
$
An
nu
al increm
ental fin
ancial
cost p
er capita in
US
$
An
nu
al increm
ental fin
ancial
cost p
er capita in
US
$
0
$0.50
$1.00
$1.50
$2.00
$2.50
Phase 2:
Expanded package
$4.93
$1.55
$1.53$1.84
0%
10%
20%
30%
40%
50%
60%
Service delivery mode
Per
cen
tag
e im
pac
t in
mo
rtal
ity
red
uct
ion
Per
cen
tag
e im
pac
t in
mo
rtal
ity
red
uct
ion
0
$1
$2
$3
$4
$5
$6
Neonatal mortality Under-five mortality Maternal mortality Incremental economic costs per capita/year
Phase 3:
Maximum package
$12.55
$2.76
$4.42$5.37
0%
10%
20%
30%
40%
50%
60%
70%
Service delivery mode
0
$2
$4
$6
$8
$10
$12
$14
-
$2
$4
$6
$8
$10
US
$ pe
r ca
pita
$12
$14
Phase 1 Phase 2 Phase 3
Out-of-pocketexpenditure
NGO private sector
Multi- and bilateral donors
Global funds Government/budget support
Funding sources 2007–2015
Figure 4.4
Estimated impact and cost of minimum, expanded and maximum packages for the
Strategic Framework for Africa
Figure 4.3
Sources Figures 4.3 and 4.4, pp. 78-79: Preliminary estimates based on the revised version of UNICEF, World Bank and World HealthOrganization, ‘A Strategic Framework for Reaching the Millennium Development Goals in Africa through health systems strengthening andimplementing at scale of integrated packages of high-impact and low-cost health and nutrition interventions’, draft prepared on request of theAfrican Union by UNICEF, WHO and the World Bank. Revised in October 2007.
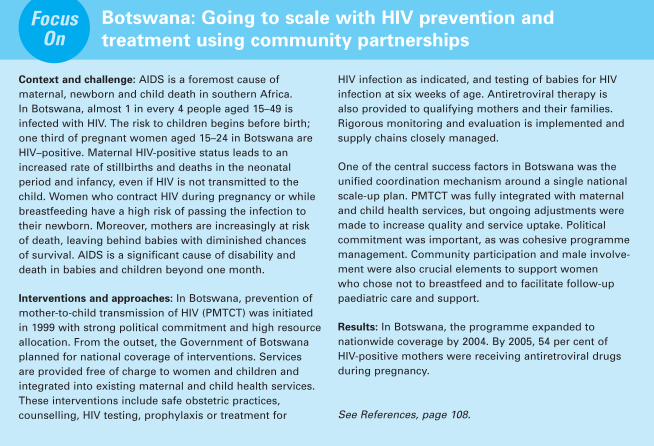
low levels of execution and effec-tiveness of disease control pro-grammes are observed. Absent orweak control of government overthe behaviour of health serviceproviders, and of beneficiaries ofhealth services over the use of public funds, undermine effectiveimplementation.23
Recent international health partner-ships propose to leverage greaterresources for scaling up for theMDGs. These initiatives seek a focuson results and a clear link betweenresources allocated and health out-comes. Doing this requires strength-ening health systems as a means ofachieving development outcomes –
both directly and by influencing otherdonors – and call for greater coher-ence in the health aid architecture.24
There is a growing agreement about the importance of supportingrobust sectoral plans, and about the desirability of ensuring full coher-ence with existing efforts on healthsystems strengthening. Key issuesrelated to these new initiativesinclude development and quality of scaling-up plans, monitoringprocesses and selection of countries,as well as flow and management of funds.25
In this context, a consensus is emerging on five principles for aid:
• Rewarding performance in a predictable way through compacts.
• Aligning development assistance tocountry systems.
• Results-based financing.
• Establishing benchmarks and out-come indicators for health-systemsdevelopment.
• Developing innovative and equitable financing strategies.
Rewarding performance in a
predictable way through compacts
Along with the renewed emphasis onresults, there is an emerging consensus
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 81
could yield important insights intothe ways that current policy process-es function and might be improved.Some significant problems – such asbuilding institutional capacity andobtaining strategic intelligence forsteering and monitoring resourceflows and health-system perform-ance – are already well recognizedby practitioners.
It is clear that there is much work to be done in gathering evidence andknowledge on ways to build capaci-ties for policy formation, regulationand steering that can inform gover-
nance of the health sector as a whole,as well as the organization of a con-tinuum of maternal, newborn andchild care at the district level.
III. Improving the quality and
consistency of financing for
strengthening health systems
Finding the money to finance healthcare is a significant obstacle to scaling up in low-income countries,where health-care sectors alreadyface huge budget shortfalls. Policiesdetermining government health-financing can have a profound effecton health outcomes for children and women, through subsidizing or taxing critical services affectingmaternal, newborn and child sur-vival, health and nutrition or by supporting equitable cost-sharingmechanisms.
Adequate financing of the health sector, in addition to fighting specificdiseases, is imperative for effective,sustainable scale-up. The less thanoptimal outcomes from earlier andcurrent support to the health sectorhave largely been attributed to several factors, namely:
A lack of evidence and country-basedbudgeting for health outcomes. Giventhe predominance of disease-specificinitiatives, national strategies formaternal, newborn and child healthoften do not give sufficient attentionto a multi-sectoral approach toachieving health outcomes, removingsystemic bottlenecks to service deliv-ery or adequately budgeting forhealth strategies – including the costs of removing bottlenecks to thesupply of and demand for primaryhealth-care services.
Slow progress and weak alignment tocountry processes and harmoniza-tion. Linkages between the healthsector and broader developmentprocesses at country level (public sector and budget reform, povertyreduction strategies, macroeconomicand fiscal planning, etc.) oftenremain tenuous in low-income countries. Monitoring systems fortracking resource flows, progress and outcomes are often largely inade-quate, and there is limited progress in translating global commitments onaid effectiveness into concrete actionat country level – most particularly in relation to the provision of pre-dictable long-term financing and the reduction of fragmented aid leading to high transaction costs, in line with the Paris Declaration on Harmonization and AidEffectiveness.
Insufficient focus of funding inaddressing obstacles to strengthen-ing health systems. Despite anincreasing commitment by the global community to health goals,countries still experience criticalshortages in funding to build uptheir health systems – includingfinancing for producing and retain-ing key human resources, providingincentives for performance, buildingprocurement and logistics systemsand facilitating transfers to poorerhouseholds to address demand-sideobstacles to better health. As moreand more funds are mobilized forspecific diseases such as HIV, anincreased imbalance is oftenobserved at country level, withhealth service delivery and financingmechanisms required to absorb thefunds made available for special initiatives often absent. As a result,
80 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Context and challenge: AIDS is a foremost cause of maternal, newborn and child death in southern Africa. In Botswana, almost 1 in every 4 people aged 15–49 isinfected with HIV. The risk to children begins before birth;one third of pregnant women aged 15–24 in Botswana areHIV–positive. Maternal HIV-positive status leads to anincreased rate of stillbirths and deaths in the neonatal period and infancy, even if HIV is not transmitted to thechild. Women who contract HIV during pregnancy or whilebreastfeeding have a high risk of passing the infection totheir newborn. Moreover, mothers are increasingly at riskof death, leaving behind babies with diminished chances of survival. AIDS is a significant cause of disability anddeath in babies and children beyond one month.
Interventions and approaches: In Botswana, prevention ofmother-to-child transmission of HIV (PMTCT) was initiated in 1999 with strong political commitment and high resourceallocation. From the outset, the Government of Botswanaplanned for national coverage of interventions. Services are provided free of charge to women and children andintegrated into existing maternal and child health services.These interventions include safe obstetric practices, counselling, HIV testing, prophylaxis or treatment for
HIV infection as indicated, and testing of babies for HIVinfection at six weeks of age. Antiretroviral therapy is also provided to qualifying mothers and their families.Rigorous monitoring and evaluation is implemented andsupply chains closely managed.
One of the central success factors in Botswana was the unified coordination mechanism around a single nationalscale-up plan. PMTCT was fully integrated with maternaland child health services, but ongoing adjustments weremade to increase quality and service uptake. Political commitment was important, as was cohesive programmemanagement. Community participation and male involve-ment were also crucial elements to support women who chose not to breastfeed and to facilitate follow-up paediatric care and support.
Results: In Botswana, the programme expanded to nationwide coverage by 2004. By 2005, 54 per cent of HIV-positive mothers were receiving antiretroviral drugsduring pregnancy.
See References, page 108.
Botswana: Going to scale with HIV prevention and
treatment using community partnershipsFocus
OnThe shortage of health workers in develop-ing countries must be addressed in nationalplans to reverse its negative impact on thehealth of mothers, newborns and children.A health worker examines a child at theregional centre for AIDS prevention and protection, Russian Federation.
© U
NIC
EF/
HQ
04-0
689/
Gia
com
o P
irozz
i
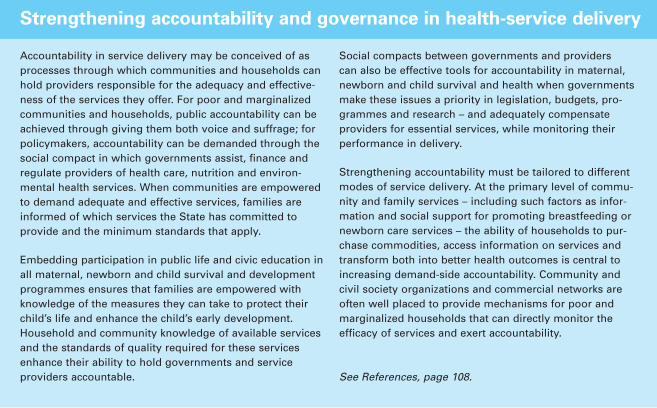
Results-based financing offers severaladvantages over traditional, input-based approaches, including:
• An emphasis on achieving outputsand outcomes relatively quicklywithin a well defined time period.
• Incentives for performance at key junctures in the service delivery chain.
• Addresses important funding gaps,provides governments with flexiblefinancing to counterbalance fund-ing distortions and gives them theopportunity to focus on priorities,such as targeting the poor.
• By design, results-based financingis essentially a monitoring and
evaluation tool, built on a measur-able and targeted strategy thatrequires baseline, target andprogress data at the relevant levels.Consequently, results-based effortswill allow regular review of suc-cesses, shortfalls and bottlenecks,enabling midstream adjustments to implementation plans.
• In addition, it supports a broader-range of solutions to health pro-blems beyond those that are official-ly under the control of the healthsector, such as improving roads,water supplies and sanitation.
• Perhaps most importantly, resultsbased financing creates an opportu-nity to consolidate fragmented aid,thereby reducing high transaction
costs to countries. This can beaccomplished through results-basedfinancing arrangements that focuson outputs to which many donorscan simultaneously contribute.27
Establishing benchmarks
and outcome indicators for
health-system development
Indicators associated with the health-related MDGs can serve as appropri-ate tracers or proxy measures for theperformance of health systems. Newinitiatives plan to provide support to governments to achieve agreed outcomes in selected target areasthrough results-based financing,establishing appropriate incentiveframeworks. The objective is toachieve defined output targets forcoverage of services that are strongly
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 83
that resources should be allocated onthe basis of such criteria as: need(based on such factors as populationsize, poverty levels and current stateof national health) and peformance(health outcomes and capacity toabsorb funds effectively). Performancewould be related to key results andpolicy measures agreed at the countrylevel in a ‘compact’ that builds onexisting results-oriented frameworks,such as those developed by theEuropean Commission, World Bankand African Development Bank and bilateral donors.26
These compacts constitute mutualagreements between developingcountries and donors based onaccountabilities and meeting per-formance criteria by recipients and provision of predictable financ-ing by donors.
Aligning development assistance
to country systems
Alignment of disbursement andimplementation to country systems is pivotal to enhancing aid effective-ness. In countries with fiduciary environments (public financial management and procurement) thatare considered adequate overall by multilateral and bilateral donors and jointly monitored by partnersthrough the public expenditure andfinancial accountability mechanism,funding for effective scale-up couldflow as sector budget support – pro-viding incremental funding for theimplementation of the health-sectorcomponent of the national budget, aswell as related activities. Monitoringthe effectiveness of these funds wouldbe integrated into the monitoring ofthe existing general and sector budgetsupport. A similar mechanism could
be used in countries with sector-wideapproaches and basket fund mecha-nisms, complementing existing evaluation methods.
There is a growing consensus thatresources for the health sector shouldbe channelled through institutionsthat aim to provide universal cover-age, rather than through projects andprogrammes. Maternal, newborn andchild health services must be part ofthe basket of core health interven-tions that are covered in any benefitpackage funded through these institu-tions. Enhancing resources spent onmaternal, newborn and child healthmay require trade-offs in governmentexpenditures, either within the healthbudget itself or within the nationalbudget. Such trade-offs need to benegotiated in the context of the overall macroeconomic environment,which can allow for incremental sector spending if health-care require-ments are well argued. At the coun-try level, resources also need to bemobilized outside of the public sectorthrough the involvement of the private sector, civil society organiza-tions, communities and households.
Results-based financing
One of the key areas supported by thenew scaling-up initiatives is results-based financing. This is an importantcomplement to existing funding flowsand a potentially promising approachto surmounting existing obstacles with-in health systems to achieve health,nutrition and population results.Recent experiences in Afghanistan,Argentina, Cambodia and Rwanda(see Panel, page 84, on performance-based financing in Rwanda) haveshown positive results, and more rigor-ous evaluation for the latter is planned.
82 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Accountability in service delivery may be conceived of asprocesses through which communities and households canhold providers responsible for the adequacy and effective-ness of the services they offer. For poor and marginalizedcommunities and households, public accountability can beachieved through giving them both voice and suffrage; forpolicymakers, accountability can be demanded through thesocial compact in which governments assist, finance andregulate providers of health care, nutrition and environ-mental health services. When communities are empoweredto demand adequate and effective services, families areinformed of which services the State has committed to provide and the minimum standards that apply.
Embedding participation in public life and civic education inall maternal, newborn and child survival and developmentprogrammes ensures that families are empowered withknowledge of the measures they can take to protect theirchild’s life and enhance the child’s early development.Household and community knowledge of available servicesand the standards of quality required for these servicesenhance their ability to hold governments and serviceproviders accountable.
Social compacts between governments and providers can also be effective tools for accountability in maternal,newborn and child survival and health when governmentsmake these issues a priority in legislation, budgets, pro-grammes and research – and adequately compensateproviders for essential services, while monitoring their performance in delivery.
Strengthening accountability must be tailored to differentmodes of service delivery. At the primary level of commu-nity and family services – including such factors as infor-mation and social support for promoting breastfeeding ornewborn care services – the ability of households to pur-chase commodities, access information on services andtransform both into better health outcomes is central toincreasing demand-side accountability. Community andcivil society organizations and commercial networks areoften well placed to provide mechanisms for poor and marginalized households that can directly monitor the efficacy of services and exert accountability.
See References, page 108.
Strengthening accountability and governance in health-service delivery
Enhanced political commitment and adequate financing by governments are necessary toguarantee access to the continuum of care for mothers, newborns and children. A childholds his baby sister, Guatemala.
© U
NIC
EF/
HQ
05-1
876/
Don
na D
eCes
are
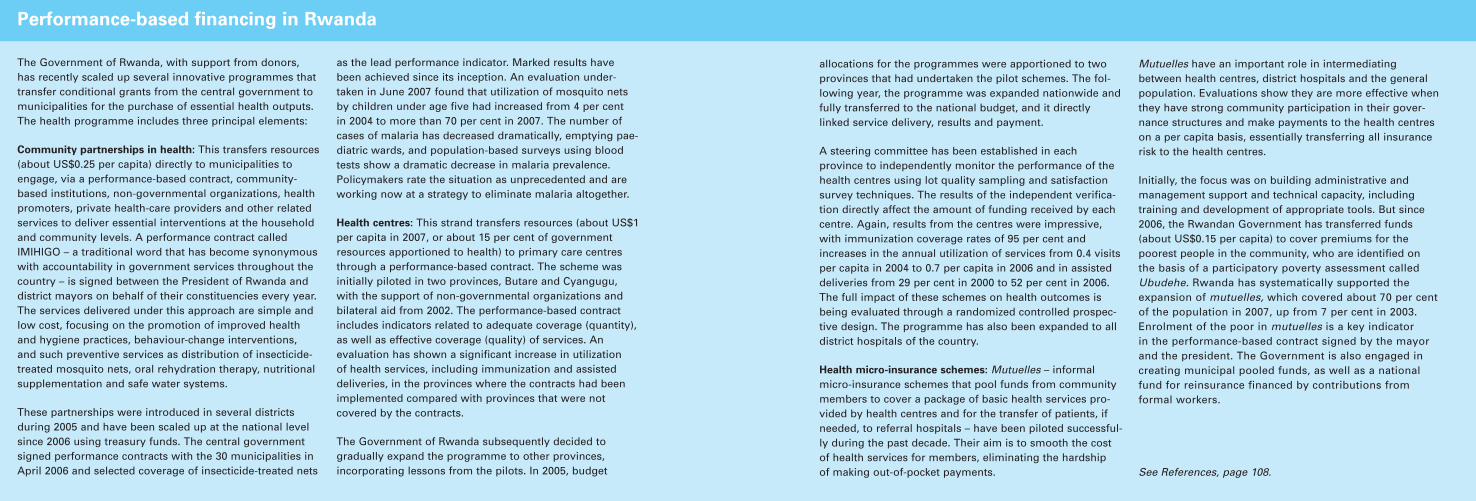
While the Strategic Framework suggests that it is possible to fill thegap between present levels and near-universal coverage by 2015, it alsoshows that scaling up interventionswill not be possible without massivelyincreasing investment in maternal,newborn and child health.29
Moving towards universal access to acontinuum of quality maternal, new-born and child health care, however,is not merely a question of findingmoney to expand the supply of serv-ices or to pay providers. Reachingthe health-related MDGs will require
that financing strategies focus onovercoming financial barriers towomen and children’s access to serv-ices and give users predictable protec-tion against the financial hardshipthat may result from paying for care.
This has important implications.Calls for the immediate and univer-sal elimination of user fees forhealth-care services may prove over-ly simplistic or unrealistic. Policydecisions regarding user fees shouldbe addressed within the broadercontext of the health sector budgetand the national budgetary frame-
work. Over time, user fees may bephased out in favour of prepaymentand pooling schemes, on conditionthat this is accompanied, from itsinception, by structural changes toensure the long-term sustainabilityof health financing.
IV. Obtaining national political
commitment
Given the level of resources requiredto ensure access to quality primaryhealth-care services and financial pro-tection, scaling up is as much a politi-cal challenge as it is a technical one.
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 85
correlated with positive maternal,newborn and child health and sur-vival outcomes – for example: theproportion of deliveries in an accred-ited facility; immunization coverageof three doses of diphtheria, tetanustoxoid and pertussis vaccine; or coverage of insecticide-treated mosquito nets in malaria-endemicareas. These outputs and targetswould be selected based on the riskfactors contributing to mortality andmorbidity for each country.
Key outcome indicators can be set invarious forms. These parameters can
measure either direct outputs, such asthe absolute number of childrenimmunized; coverage, such as thepercentage of the target populationvaccinated, by antigen, in a definedcatchment area; or trends, such asincreases in the number of childrenvaccinated or coverage levelsachieved over time. A set of coreindicators can also be defined for all projects to allow for some cross-country comparison and learning.Countries could also include addi-tional indicators that monitor impor-tant elements of their maternal, childand newborn health programmes.
Developing innovative and
equitable financing strategies
Investment in human resources andhealth-system strengthening requiressignificant resources. Countries wheredonor support plays a critical role infunding these programmes cannotplan for long-term activities unlessfinancing is secure. Yet, researchtracking donor assistance to maternal,newborn and child health found thatthe 60 priority countries that accountfor more than 90 per cent of childdeaths received only US$1.4 billion in official development assistance in2004, or just US$3.10 per child.28
84 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
The Government of Rwanda, with support from donors, has recently scaled up several innovative programmes thattransfer conditional grants from the central government tomunicipalities for the purchase of essential health outputs.The health programme includes three principal elements:
Community partnerships in health: This transfers resources(about US$0.25 per capita) directly to municipalities toengage, via a performance-based contract, community-based institutions, non-governmental organizations, healthpromoters, private health-care providers and other relatedservices to deliver essential interventions at the householdand community levels. A performance contract called IMIHIGO – a traditional word that has become synonymouswith accountability in government services throughout thecountry – is signed between the President of Rwanda anddistrict mayors on behalf of their constituencies every year.The services delivered under this approach are simple andlow cost, focusing on the promotion of improved healthand hygiene practices, behaviour-change interventions, and such preventive services as distribution of insecticide-treated mosquito nets, oral rehydration therapy, nutritionalsupplementation and safe water systems.
These partnerships were introduced in several districts during 2005 and have been scaled up at the national levelsince 2006 using treasury funds. The central governmentsigned performance contracts with the 30 municipalities inApril 2006 and selected coverage of insecticide-treated nets
as the lead performance indicator. Marked results havebeen achieved since its inception. An evaluation under-taken in June 2007 found that utilization of mosquito netsby children under age five had increased from 4 per cent in 2004 to more than 70 per cent in 2007. The number ofcases of malaria has decreased dramatically, emptying pae-diatric wards, and population-based surveys using bloodtests show a dramatic decrease in malaria prevalence.Policymakers rate the situation as unprecedented and areworking now at a strategy to eliminate malaria altogether.
Health centres: This strand transfers resources (about US$1per capita in 2007, or about 15 per cent of governmentresources apportioned to health) to primary care centresthrough a performance-based contract. The scheme was initially piloted in two provinces, Butare and Cyangugu,with the support of non-governmental organizations andbilateral aid from 2002. The performance-based contractincludes indicators related to adequate coverage (quantity),as well as effective coverage (quality) of services. An evaluation has shown a significant increase in utilization of health services, including immunization and assisteddeliveries, in the provinces where the contracts had beenimplemented compared with provinces that were not covered by the contracts.
The Government of Rwanda subsequently decided to gradually expand the programme to other provinces, incorporating lessons from the pilots. In 2005, budget
Performance-based financing in Rwanda
allocations for the programmes were apportioned to twoprovinces that had undertaken the pilot schemes. The fol-lowing year, the programme was expanded nationwide andfully transferred to the national budget, and it directlylinked service delivery, results and payment.
A steering committee has been established in eachprovince to independently monitor the performance of thehealth centres using lot quality sampling and satisfactionsurvey techniques. The results of the independent verifica-tion directly affect the amount of funding received by eachcentre. Again, results from the centres were impressive,with immunization coverage rates of 95 per cent andincreases in the annual utilization of services from 0.4 visitsper capita in 2004 to 0.7 per capita in 2006 and in assisteddeliveries from 29 per cent in 2000 to 52 per cent in 2006.The full impact of these schemes on health outcomes isbeing evaluated through a randomized controlled prospec-tive design. The programme has also been expanded to alldistrict hospitals of the country.
Health micro-insurance schemes: Mutuelles – informalmicro-insurance schemes that pool funds from communitymembers to cover a package of basic health services pro-vided by health centres and for the transfer of patients, ifneeded, to referral hospitals – have been piloted successful-ly during the past decade. Their aim is to smooth the costof health services for members, eliminating the hardship of making out-of-pocket payments.
Mutuelles have an important role in intermediatingbetween health centres, district hospitals and the generalpopulation. Evaluations show they are more effective whenthey have strong community participation in their gover-nance structures and make payments to the health centreson a per capita basis, essentially transferring all insurancerisk to the health centres.
Initially, the focus was on building administrative and management support and technical capacity, includingtraining and development of appropriate tools. But since2006, the Rwandan Government has transferred funds(about US$0.15 per capita) to cover premiums for the poorest people in the community, who are identified on the basis of a participatory poverty assessment calledUbudehe. Rwanda has systematically supported theexpansion of mutuelles, which covered about 70 per centof the population in 2007, up from 7 per cent in 2003.Enrolment of the poor in mutuelles is a key indicator in the performance-based contract signed by the mayorand the president. The Government is also engaged increating municipal pooled funds, as well as a nationalfund for reinsurance financed by contributions from formal workers.
See References, page 108.
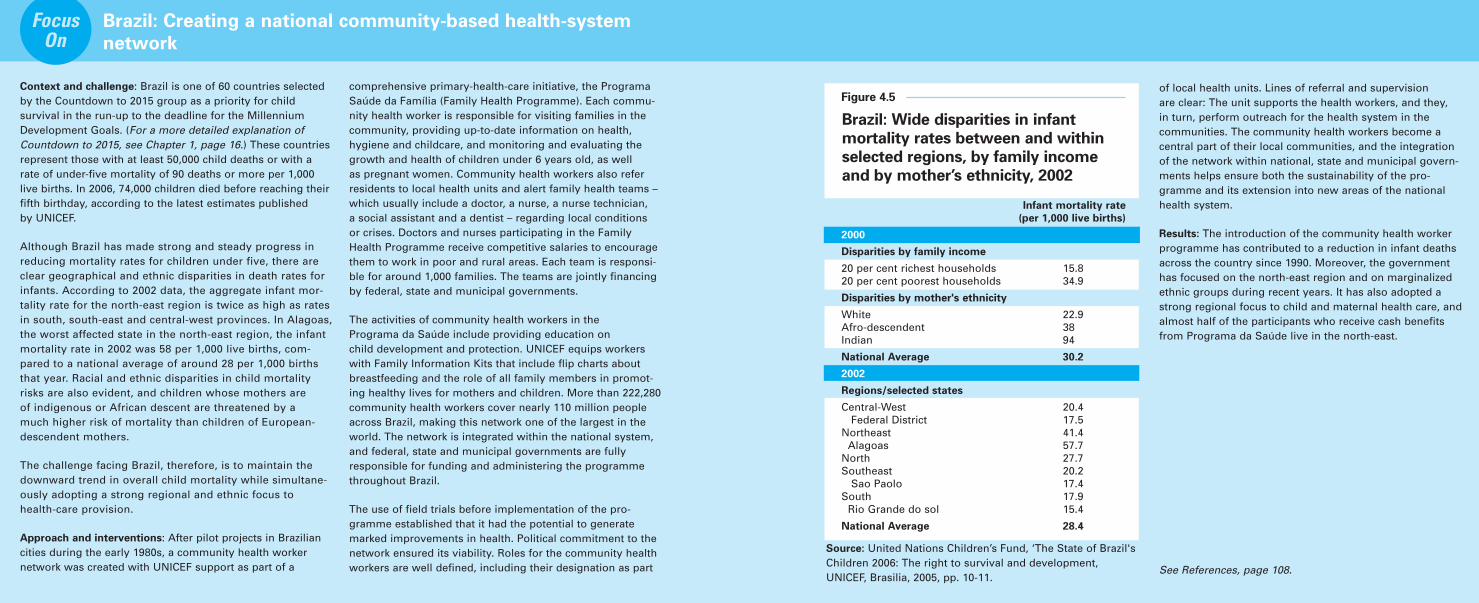
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 87
in conjunction with improvementsin living conditions and the status of women.
• Prioritizing broad social safetynets that ensured equitableaccess to health, nutrition andeducation, making health and nutrition services widelyavailable.
• Reducing barriers to key servicesand providing primary and second-ary schooling to all children.
Even in some of the poorest coun-tries in Latin America, where economic crises, institutional defi-ciencies and wide socio-economicdisparities continue to hinderadvances, there has been marked
progress towards generalized accessto quality health care.
Country ownership and public sectorleadership can vastly increase theprospects for successful scaling up.Time and again, it has been shownthat when governments take the leadand are committed to expanding suc-cessful pilot and small-scale projects,
Sustained improvements in mater-nal, newborn and child health will necessitate long-term commit-ments that go well beyond thepolitical lifespan of many decisionmakers. Countries including Brazil,Sri Lanka and Thailand have rooted their impressive results in a step-by-step extension ofhealth-system coverage and nutri-
tion services over many years.During recent decades, LatinAmerica’s performance in enhanc-ing health-service coverage, despite periodic economic crises,institutional deficiencies and wide socio-economic disparities,has been noteworthy. All of the countries mentioned wentthrough several distinct phases:
• Building up a cadre of professio-nal health workers as the foundation.
• Developing an accessible networkof community-based, primary andreferral-level services.
• Consolidating advances by im-proving the quality of care, all
86 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
Context and challenge: Brazil is one of 60 countries selectedby the Countdown to 2015 group as a priority for child survival in the run-up to the deadline for the MillenniumDevelopment Goals. (For a more detailed explanation ofCountdown to 2015, see Chapter 1, page 16.) These countriesrepresent those with at least 50,000 child deaths or with arate of under-five mortality of 90 deaths or more per 1,000live births. In 2006, 74,000 children died before reaching theirfifth birthday, according to the latest estimates published by UNICEF.
Although Brazil has made strong and steady progress inreducing mortality rates for children under five, there areclear geographical and ethnic disparities in death rates forinfants. According to 2002 data, the aggregate infant mor-tality rate for the north-east region is twice as high as ratesin south, south-east and central-west provinces. In Alagoas,the worst affected state in the north-east region, the infantmortality rate in 2002 was 58 per 1,000 live births, com-pared to a national average of around 28 per 1,000 birthsthat year. Racial and ethnic disparities in child mortalityrisks are also evident, and children whose mothers are of indigenous or African descent are threatened by a much higher risk of mortality than children of European-descendent mothers.
The challenge facing Brazil, therefore, is to maintain thedownward trend in overall child mortality while simultane-ously adopting a strong regional and ethnic focus tohealth-care provision.
Approach and interventions: After pilot projects in Braziliancities during the early 1980s, a community health worker network was created with UNICEF support as part of a
comprehensive primary-health-care initiative, the ProgramaSaúde da Família (Family Health Programme). Each commu-nity health worker is responsible for visiting families in thecommunity, providing up-to-date information on health,hygiene and childcare, and monitoring and evaluating thegrowth and health of children under 6 years old, as well as pregnant women. Community health workers also refer residents to local health units and alert family health teams –which usually include a doctor, a nurse, a nurse technician, a social assistant and a dentist – regarding local conditions or crises. Doctors and nurses participating in the FamilyHealth Programme receive competitive salaries to encouragethem to work in poor and rural areas. Each team is responsi-ble for around 1,000 families. The teams are jointly financingby federal, state and municipal governments.
The activities of community health workers in the Programa da Saúde include providing education on child development and protection. UNICEF equips workerswith Family Information Kits that include flip charts aboutbreastfeeding and the role of all family members in promot-ing healthy lives for mothers and children. More than 222,280community health workers cover nearly 110 million peopleacross Brazil, making this network one of the largest in theworld. The network is integrated within the national system,and federal, state and municipal governments are fullyresponsible for funding and administering the programmethroughout Brazil.
The use of field trials before implementation of the pro-gramme established that it had the potential to generatemarked improvements in health. Political commitment to thenetwork ensured its viability. Roles for the community healthworkers are well defined, including their designation as part
of local health units. Lines of referral and supervision are clear: The unit supports the health workers, and they, in turn, perform outreach for the health system in the communities. The community health workers become acentral part of their local communities, and the integrationof the network within national, state and municipal govern-ments helps ensure both the sustainability of the pro-gramme and its extension into new areas of the nationalhealth system.
Results: The introduction of the community health workerprogramme has contributed to a reduction in infant deathsacross the country since 1990. Moreover, the governmenthas focused on the north-east region and on marginalizedethnic groups during recent years. It has also adopted astrong regional focus to child and maternal health care, and almost half of the participants who receive cash benefitsfrom Programa da Saúde live in the north-east.
See References, page 108.
Brazil: Creating a national community-based health-system
network
FocusOn
Brazil: Wide disparities in infant
mortality rates between and within
selected regions, by family income
and by mother’s ethnicity, 2002
Figure 4.5
Infant mortality rate
(per 1,000 live births)
2000
Disparities by family income
20 per cent richest households 15.820 per cent poorest households 34.9
Disparities by mother's ethnicity
White 22.9Afro-descendent 38Indian 94
National Average 30.2
2002
Regions/selected states
Central-West 20.4Federal District 17.5
Northeast 41.4Alagoas 57.7
North 27.7Southeast 20.2
Sao Paolo 17.4South 17.9
Rio Grande do sol 15.4
National Average 28.4
Source: United Nations Children’s Fund, ‘The State of Brazil'sChildren 2006: The right to survival and development,UNICEF, Brasilia, 2005, pp. 10-11.
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 89
of children unprotected from iodinedeficiency, the leading cause of preventable intellectual impairmentin the world. Iodine deficiency disorders can be prevented with a single teaspoon of iodine spreadover a lifetime. The challenge wasto raise public awareness of thevital importance of iodized salt,especially in salt-producing regionswhere local residents resisted theidea of paying for salt.
With political support from provin-cial governors, rigorous monitoring
and enforcement of iodized salt regu-lations, as well as a nationwide pub-lic health campaign that used posterson buses, newspaper editorials andtelevision documentaries to informconsumers and create demand forfortified salt, adequately iodized saltreached 90 per cent of the house-holds around 2005, up from 51 per cent around 1995.30
Addressing the political dimension in creating sustainable continuumsof quality care requires more thancompelling technical arguments.
It also necessitates a broad under-standing of the constraints andopportunities for fostering willand commitment among key political players.
Politicians may need to be convin-ced that actions in support of the continuum of care satisfy severalexpedient criteria, including that they:
• Demonstrate visible and tangibleresults within a relatively shorttime frame.
these initiatives can rapidly gainnationwide coverage. Brazil’s commu-nity health worker programme (seePanel page 86) and the Bolsa Familiainitiative, Mexico’s health, nutritionand education programme, PROGRE-SA, and Seguro Popular de Saludhealth insurance scheme, Indonesia’scommunity health workers andEgypt’s oral rehydration initiatives,along with many other examples,show the potential for scale-up whengovernments are willing to commiteven scarce funding to health andsocial welfare programmes.
Ownership is more than just funding,however. Governments must also becommitted to creating and sustainingthe required technical and adminis-tration capacity. Support at each levelof health-system administration –federal, provincial and district – isrequired to coordinate and supervisethe expansion. Sustainability issuesmust also be addressed at the nation-al level, and the programme fullyendorsed by the political system –including the legislature – to ensurethat it outlasts political transitionsand changes.
Governments can provide thecapacity and will to creating anational network based on commu-nity health. When this has hap-pened, the results are often signifi-cant. In the case of China, forexample, the Government set itselfa tremendous challenge with thelaunch of the National IodineDeficiency Disorders EliminationProgram, a strategy for ensuring anationwide supply of commerciallymarketed iodized salt and promot-ing universal compliance. At thattime, China had the highest number
88 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
In New York, 19 July 2007, global health leaders from eightinternational organizations met informally to discuss ways of strengthening their collaboration to achieve better healthoutcomes in developing countries. Capitalizing on the recentappointments of several leaders, the objective of the meetingwas to review progress made during recent years, assess cur-rent trends and future challenges for global health, and agreeto collective action, in the context of current opportunities.Several key commitments were recommended, including:
• Stimulate a global collective sense of urgency for reach-
ing the health-related MDGs. Participants agreed that,despite important advances in health care for mothers,newborns and children in some countries and for someindicators, the international community – in partnershipwith national governments – must accelerate and intensi-fy efforts dramatically in order to reach all of the health-related Millennium Development Goals. The eight organi-zations represented have an important role in stimulatingthis action. Participants agreed to hold themselvesaccountable for providing the necessary support to countries to reach the goals and to accelerate action at all levels within each of their own organizations.
Action: The global health leaders agreed to catalyse a greatersense of urgency in their own organizations and support itthrough budgetary and human resources decisions.
• Modify institutional ways of doing business. Achieving thehealth-related MDGs will require increased collaboration
and teamwork. Emphasis was placed on clarifying the coreresponsibilities of each agency; the need for a coordinatedinter-agency approach to providing high-quality, demand-driven technical assistance; and implementation of a collec-tively supported and robust monitoring and evaluation system. Such approaches need to build on existing struc-tures and programmes at the global, regional and countrylevels. Each of the organizations agreed to evaluate theirpersonnel, training programmes and incentives structureto reflect this new, collaborative way of doing business,
recognizing that new skills will need to be developed, particularly at the country level. The development of aframework for mutual accountability would ensure moreclarity on roles, responsibilities and milestones, and a system for monitoring commitments.
Action: The global health leaders agreed to work together tobetter define their individual and collective accountabilitiesfor better and faster results.
• Foster a more systematic and robust approach to knowl-
edge management and learning. Given the significant newinvestments in global health, opportunities are available to capture knowledge and lessons learned in health pro-grammes. The participants emphasized the opportunity toconduct more systematic mapping of the health sector at thecountry level, including the role played by the private sector.
Action: The global health leaders agreed to explore meansto systematically capture knowledge gained in health
A new way of working together for multilateral institutions
programmes and to develop a more robust and coordinat-ed approach to knowledge management in general. Finally, the group agreed to pool resources when theirorganizations conduct mapping exercises and health sector assessments.
• Recognition of the important opportunity presented by
the renewed interest in health systems. Participants wel-comed the commitment to the health-related MDGs as articulated in several new global initiatives being developedaround health-system strengthening. Such support is wellaligned with the priorities of the participating organizations.There was strong agreement for adopting a ‘systems foroutcomes’ approach whereby strengthening would be evaluated by its ability to deliver against health outcomes.In addition, the group recognized the key brokering role ofthe UN agencies in bridging the need for accountability andcountries’ desires to lead their own development processes.The urgent need for benchmarking health system perform-ance was emphasized. Finally, with the growing number ofstakeholders working in global health, the need for closeralignment around an overarching health-sector strategy atthe country level was emphasized. In this regard, the globalhealth leaders discussed the experience of programmingfor HIV and AIDS, which may offer learning opportunities.
Action: The global health leaders agreed to engage emergingglobal initiatives in a coordinated manner to ensure theirorganizations effectively support countries through fundingand/or technical and policy assistance. In addition, WHO and
the World Bank committed to fast-track the benchmarking ofhealth system performance.
• Recognition that the role of civil society and the private
sector will be critical for success. The private sector hasseveral roles to fulfil in delivering health services, in financ-ing health care and in bringing new technologies to market.Innovations can help accelerate progress, whether they aretechnologically driven or new programme models, such as micro-venture and performance-based financing. Non-governmental organizations have a long history ofdelivering services in developing countries, and their fieldexperience is a source of important lessons. Support todeveloping countries in reaching the health-related MDGswill require strengthening integrated delivery systemsacross the public and private sectors, and creating opportu-nities for private sector involvement and investment.
Action: The global health leaders expressed their commit-ment to involve the private sector and civil society more systematically as the work on the health-related MDGsexpands at global, regional and country levels.
The group has agreed to monitor progress towards achieving the commitments made at this meeting.
See References, page 108.
to meet the MDGs, particularly insub-Saharan Africa, do not enjoypolitical or economic stability. Undersuch circumstances, it is important to mobilize all forms of effectiveleadership in society, whether at thenational level where broad sectoral
decisions are made or at various sub-national levels (provincial, district)where the interaction with communi-ties takes place.
In contrast to the extensive knowl-edge of the technical and contextual
interventions required to improvematernal, newborn and child health,there is less known on how politicalcommitment to a result-orientedapproach to health services deliveryis both effected and sustained, partic-ular in settings of low health systems
STRENGTHENING COMMUNITY PARTNERSHIPS , THE CONTINUUM OF CARE , AND HEALTH SYSTEMS 91
• Are affordable and cost-effective at scale.
• Fit within existing structures and hierarchies and have the support of professional groups and lobbies.
These political considerations arelikely to constrain some of the tech-nical choices that advocates of thecontinuum prefer, but unless suchpolitical concerns are acknowledgedand addressed, the strategies theypromote are unlikely to succeed.
Stability, in political and macro-economic terms, and sound budget-ing are prerequisites for mobilizingthe institutional, human and financialresources required to strength healthsystems and nutrition services. Many of the countries struggling
90 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
by Paul Farmer and Jim Yong Kim
With 20 years of experience in rural Haiti introducing modern medical care to millions who had not previouslyenjoyed it, we now know many of the requirements for asuccessful health-care programme in areas devastated bydisease and poverty. To provide primary care alongsidespecialized treatment for infectious disease, while promot-ing women’s and children’s health, community health-careworkers must be trained and mobilized to prevent illnessand to deliver quality health care. With recent expansion to Lesotho, Malawi and Rwanda, we now see that many ofthe lessons learned in Haiti are universal in improving thehealth of children and adults worldwide.
In each of the settings in which Partners In Health works,our goal is to ‘do whatever it takes’ to improve the healthand well-being of those we serve, almost all of whom livein poverty. In each setting, we have learned that healthproblems do not occur in isolation from other basicneeds, such as adequate nutrition, clean water, sanita-tion, housing and primary education. We have alsolearned that non-governmental organizations cannotwork in isolation but must collaborate with members ofthe communities served and with local health authoritiesto strengthen public health so that future generationsmay come to regard these services as rights rather than privileges.
This rights-based, community-based approach to
promoting health leads to a clear vision regarding
the health of children
In Haiti, Lesotho, Malawi and Rwanda, Partners In Health –in collaboration with local communities and a wide rangeof partner organizations, including the Clinton Foundation,ministries of health, UNICEF and the François-XavierBagnoud Center for Health and Human Rights – has
identified five key components for a comprehensive,community-based child survival programme.
First, we work with public health authorities to roll outthe interventions shown to be crucial to improved childsurvival. These include expanded vaccination campaigns;vitamin A distribution; the use of oral rehydration salts totreat diarrhoeal disease and safe-water programmes toprevent it; an aggressive programme for prevention ofmother-to-child transmission of HIV; malaria preventionwith mosquito nets, backed by improved community-based and clinical care; nutritional assistance for childrensuffering from or at risk of malnutrition; and the provi-sion of high-quality in-patient and ambulatory paediatricservices for those children who do fall ill. Currently, weare working with the Government of Rwanda and otherpartners to show how an integrated package of key childsurvival interventions, including prevention of mother-to-child transmission of HIV, can be rapidly deployed underthe Government’s strengthened rural-health-care model.With support from the international Joint LearningInitiative on Children and HIV/AIDS, a cross-sectoral,interdisciplinary exercise in collaboration between lead-ing practitioners, policymakers and scholars, practitionersscaling up child survival interventions in rural districtsare sharing innovations and results through a collabora-tive network that will enable them to improve servicequality, even as they reach greater numbers of childrenand families in previously underserved areas.
Second, since the health and well-being of mothers arekey determinants of child survival, our efforts promoteintegrated maternal and child health. Our work on behalfof children is linked to efforts on behalf of their mothersand other family members through family planning pro-grammes, prenatal care and modern obstetrics as part of women’s health programmes, efforts to promote adultliteracy and poverty alleviation in general.
Human rights, community-based health care and child survival
Third, we initiate and/or strengthen paediatric AIDS prevention and control programmes. As part of an upcom-ing campaign, and in the manner outlined above, we arelaunching a major paediatric AIDS initiative in Rwanda inconcert with the Clinton Foundation and Rwandan healthofficials and providers. This initiative will establish a nation-al centre of excellence for paediatric AIDS care. Qualitypaediatric services will be linked to community-based carefor children with HIV and also to prevention efforts withinprimary and secondary schools in rural Rwanda.
Fourth, we need to launch operational research and train-ing programmes designed to improve the quality of careafforded to rural children. Such research will examine theprogrammatic features of successful efforts to preventHIV transmission from mother to child; the diagnosis andmanagement of HIV among infants; paediatric tuberculo-sis diagnosis and care; the role of community healthworkers in improving care for chronic paediatric condi-tions, including AIDS and tuberculosis, and in preventing,diagnosing and providing home-based treatment for suchcommon ailments as malaria and diarrhoea; and assess-ing the impact of social interventions, including thosedesigned to curb food insecurity and illiteracy, on thehealth and well-being of children worldwide.
Fifth, we work to advance these efforts in tandem withthose designed to promote the basic rights, in particular,the social and economic rights, of the child. The Partners In Health Program on Social and Economic Rights(POSER) disseminates, through tangible projects andthrough advocacy, a rights-based model of poverty allevi-ation, using access to health care as a means of meetingand working with the poorest children and families in thecommunities we serve. POSER backs education, agricul-ture, housing and water projects to guarantee basicsocial and economic rights for every child and every family. If we know that hunger and malnutrition are the
underlying cause of millions of child deaths each year – and we do – then we must face up to the challenge of pre-scribing food as an essential medicine for immunizationand paediatric care. Similarly, if studies show that educa-tion reduces the risk of infection with HIV – as they do –then we must be prepared to invest in access to schoolingas a potent and cost-effective element in our formulary forcombating HIV and other diseases of poverty.
We now know that without a community-based, compre-hensive strategy, efforts to treat children – and subsequent-ly mothers, fathers and siblings – fail to provide the desiredoutcomes. Working in conjunction with ministries of health,international institutions and other non-profit organizations,we are committed to stemming the tide of childhood deathand disease in the areas we serve. From experience in Haitiand now around the world, we know that community-basedservices to improve health and reduce poverty, linked,when necessary, to excellent clinical resources, offer thehighest standard of care in the world today and the key toimproving child survival.
Drs. Paul Farmer and Jim Yong Kim are co-founders ofPartners In Health, an international health and social justiceorganization that works in Haiti, Lesotho, Malawi, Peru, theRussian Federation, Rwanda and the United States. PaulFarmer is the Presley Professor of Medical Anthropology atHarvard University and an attending physician at Brighamand Women’s Hospital in Boston. Jim Yong Kim is Chair ofthe Department of Social Medicine at Harvard MedicalSchool, Chief of the Division of Social Medicine and HealthInequalities at Brigham and Women's Hospital, Director ofthe François-Xavier Bagnoud Center for Health and HumanRights and a former director of the World HealthOrganization’s HIV/AIDS Department.
industrialized nations pledged todouble their aid to Africa by 2010.Yet, as of mid-2007, there is littleadvance in this direction.11 Africancountries, too, have been remiss indemonstrating their commitment to their own children. In the AbujaDeclaration, adopted at theOrganization of African Unity’s special summit on AIDS in 2001,African leaders included a commit-ment to devote 15 per cent of theirnational budgets to health. Yet sixyears later, only a few countries have managed to do so.12
The resources are available to meet the health-related MDGs. Theworld is richer than it has ever been.Financial flows to developing coun-tries are at record levels, in terms ofprivate debt inflows, foreign directinvestment, portfolio equity andremittances. And yet, while officialdevelopment assistance has doubledsince 2000, its increase has laggedmarginally behind other financialflows (see Figure 5.1, page 99).Donors have yet to make good ontheir promise to increase assistance to Africa and will need to step upefforts markedly in the coming years.
Make maternal, newborn and
child survival a global imperative
Many have heard the cry for childand maternal survival. Since the earlyyears of the child survival revolution,global partnerships for health, oftenfinanced through private sources,have proliferated and reinvigoratedthe field: including, for example, the Flour Fortification Initiative, the Global Alliance for ImprovedNutrition, the GAVI Alliance, thePartnership for Maternal, Newborn& Child Health, Roll Back Malaria
and the Special Programme forResearch and Training in TropicalDiseases, among many others.
As a consequence of these and otheralliances, public attention to globalhealth issues is at an all-time high.Research and development sponsoredby these partnerships are beginningto yield results, with 25 drugs, 8microbicides and 50 vaccines in thepipeline to address diseases predomi-nantly affecting the poor. A numberof these partnerships have provedremarkably effective in offering communities free or reduced-costmedicines whose quality is assured,along with vaccines. Others areimproving national policymaking and supporting institutional reforms.Still others are contributing to theestablishment of norms and stan-dards in treatment protocols.13
Yet, in their single-mindedness toproduce results, it has been arguedthat global partnerships are oftendonor- and commodity-driven ratherthan country- and people-centred.Moreover, a frequent focus on singlediseases has sometimes meant anover-reliance on vertical interven-tions and insufficient emphasis onintegrating services and strengthen-ing national health systems.14 Themessage that has been widely heard– and heeded – is that developingcountries must take the lead and‘own’ the solutions to their healthproblems. This will require greaterharmonization and alignment withdeveloping countries’ own priorities,systems and procedures. Indeed, thiswas the position adopted in the ParisDeclaration on Aid Effectiveness inMarch 2005, which is providing aframework through which donor
U N I T I N G F O R C H I L D S U R V I VA L 101
In sub-Saharan Africa, where the situ-ation of young children is most dire,UNICEF, WHO and the World Bankcollaborated in 2006 on an analysisof what it would cost to reduce childmortality there (see Panel, Chapter 4,page 78). By scaling up the existinginterventions highlighted in thisreport, deaths of children under fivecould be reduced by 35 per cent by
2009 at an additional cost of aboutUS$2.50 per capita (or about US$800per life saved). To fully achieve MDG4, a reduction in under-five mortalityby two thirds by 2015, would requireadditional strengthening of Africa’shealth systems, as well as the intro-duction of new interventions, such as vaccines against rotavirus andpneumococcal infections. The analy-
sis found that it is entirely feasible tosave the lives of more than 5 millionchildren and nearly 200,000 mothersa year. What would saving these livescost? An additional US$10 per capitaper year (or less than US$2,000 perlife saved).10
At the 2005 G8 Summit inGleneagles, Scotland, the major
100 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
“It is not because countries are poor that they cannotafford good health information; it is because they arepoor that they cannot afford to be without it.” – HealthMetrics Network, World Health Organization
Sound information is central to public health decisions,informing policy, programmes, budgets and evaluationsand forming the basis of accountability for governmentsto their commitments and to their citizens. In many devel-oping countries, however, underinvestment in healthinformation systems has left gaps in data collection, dis-semination and analysis. With health challenges on therise and the deadline for the health-related MillenniumDevelopment Goals drawing ever closer, fulfilling thedemand for sound information is imperative.
Before the mid-1990s, critical gaps in data hindered accurate and effective analysis for making such publichealth decisions. For example, only 38 developing coun-tries had data on whether undernutrition rates amongchildren were rising or falling – a basic indicator of childhealth and well-being. To help fill these important datagaps and to facilitate monitoring of the 1990 WorldSummit for Children goals, UNICEF initiated the MultipleIndicator Cluster Surveys (MICS) in 1995. MICS aredesigned to provide quantitative data on a wide range oftopics, including child health and nutrition, child protec-tion, education, HIV and AIDS, and maternal health.
Since 1995, nearly 200 MICS have been conducted inapproximately 100 countries and territories. The currentround of surveys, implemented in more than 50 countriesduring 2005–2006, provides data for 21 of 53 MDG sub-indicators. Together with the Demographic and HealthSurveys, a complementary initiative sponsored by theUnited States Agency for International Development
(USAID) with which data are harmonized, this is thelargest single source of information for MDG monitoring.
Monitoring progress towards the Millennium Develop-ment Goals has also stimulated the formation of a seriesof interagency groups that address specific technical andmethodological issues, including standardizing indicatorsand monitoring tools, building statistical capacity at thecountry level, developing joint estimates and harmonizingmonitoring work between partners. These groups focuson such areas as under-five and maternal mortality, waterand sanitation, immunization, malaria, and HIV and AIDS.
There is also an urgent need to improve overall data systems at the national level so they may more reliablyreport robust and timely data that can be used for inform-ing public health decisions. This is a long-term effort, andthe World Health Organization and the Health MetricsNetwork (HMN), among others, are working closely withcountries and other initiatives to improve health informa-tion systems. Specifically, the objective is to develop acomprehensive system that would incorporate all the multiple subsystems and data sources that, taken together,contribute to generating health information: surveys, vitalregistration, censuses, disease surveillance and response,service statistics, health management information, financialdata and resource tracking. The development of such acomprehensive system would require enhanced coordina-tion and cooperation between countries and internationalpartners, working together based on one harmonized planfor a unified system. This comprehensive data systemwould thereby reduce duplication, fragmentation andoverlap in data collection and reporting.
See References, page 108.
Strengthening data collection and monitoring for public health
decisions
Partnerships and renewed commitment on the part of all stakeholders are required to realizethe health needs of all mothers, newborns and children. A health worker discusses immu-nization with a mother, United Republic of Tanzania.
© U
NIC
EF/
HQ
00-0
001/
Gia
com
o P
irozz
i
The challenge is to build on theprogress achieved across the developing world in preventive interventions delivered by outreachservices, particularly in recent years.Expanded interventions delivered by outreach – notably expandedimmunization programmes,enhanced distribution of insecticide-treated mosquito nets, greater distri-bution of oral rehydration therapyand a broadening of vitamin A supplementation – have enhancedthe input side of the child and mater-nal health balance sheet. Analysis ofthese results, together with theenhanced frequency of data collec-tion, promises to show a markedimpact on child and maternal sur-vival outcomes in the coming years.
Notwithstanding the many initia-tives, programmes and policies that have proliferated since the firstyear of the new millennium, theopportunity to reduce deaths amongchildren under five has never been clearer. What needs to be done forprogress in child survival is clear.When it needs to be done, and whoneeds to be involved is also clear.The need to be united – in bothword and deed – to ensure the rightof mothers, newborns and childrento quality primary health care isclearest of all.
The challenge is, therefore, to shakeoff any cynicism and lethargy andput aside the broken promises of thepast. At the midpoint between the
inauguration of the MDGs in 2000and their target date for fulfilmentin 2015, much has already beenachieved. The basis for action – data,research, evaluation – is already wellestablished. It is time to rally behindthe goals of maternal, newborn and child survival and health withrenewed energy and sharper vision,and to position these goals at theheart of the international agenda tofulfil the tenets of social justice andhonour the sanctity of life.
The means are at hand. It is now aquestion of will and of action – forthere is no enterprise more noble, orreward more precious than saving the life of a child.
U N I T I N G F O R C H I L D S U R V I VA L 103
and developing country partnershipscan fully exploit their potential.
So, where does the world find itselftoday, just past the midway point to the target date for achieving theMillennium Development Goals? Onbalance, half of the world’s regionsare on track to meet MDG 4 andreduce child mortality rates by twothirds between 1990 and 2015. Thisis without doubt an unprecedentedscenario, reflecting advances inmaternal and child health in the
past century and the commitment of both donors and national govern-ments to unite to ensure that chil-dren survive and thrive.
Many developing countries and several regions have managed tomake great strides in reducing childmortality, and a few have managedto reduce mortality rates to levelsapproaching those in some indus-trialized countries, despite having far lower levels of per capita income.Three regions – Latin America and
the Caribbean, East Asia and thePacific, and Central and EasternEurope and the Commonwealth ofIndependent States (CEE/CIS) – havereduced child mortality substantiallysince 1960, despite bouts of economicand political instability. This successprovides a source of hope that child mortality rates will continue to decline at an even faster rate globally if ways can be found toenhance access to quality care formothers, newborns and children inthe developing world.
102 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 8
by Melinda French Gates, Co-chair, Bill & Melinda Gates Foundation
When Bill and I meet people in the developing countrieswe visit, it’s easy to see what we have in common withthem, in spite of our different circumstances. Like us, theyhave hopes for the future. They have parents who lovethem and children who need them. They have intellectualcuriosity, an entrepreneurial spirit and a determination tomake life better for themselves and their children.
I am especially moved by the mothers I meet. They inviteme into their homes, and we sit on the floor, often onopposite sides of a small mat, talking. I have young chil-dren myself, and I try to put myself in their position. Whatwould I do if I were on the other side of the mat? Whatwould I want for my children?
If I were a pregnant mother in Bangladesh, I would want a skilled attendant who knew how to help me deliver mybaby safely. If I were a young mother in India, I would wantto know the facts: that breastfeeding instead of using for-mula is one of the best ways to save my newborn fromcholera. If I were a mother in Malawi and my daughter gotsick with diarrhoea, I would hope that she could get theelectrolytes she needed before it was too late.
Those would be my hopes, my dreams, my wishes. But formany, they are not the reality of their daily lives. The realityis this: In 2006, 9.7 million children died before they turnedfive – most from easily preventable or treatable causes.
In some countries I’ve visited, mothers don’t give theirchildren names for weeks or even months because theydon’t want to start caring about them. The chance thattheir children will die in those first weeks is just too high.When I hear such stories, I am jolted back to my side ofthe mat. How can such widespread tragedy be so com-mon in the developing world?
On my side of the mat, when my kids are sick, they get antibiotics. On the other side of the mat, when their children get sick, they may be receiving a death sentence. Those of us in wealthy countries must try to put ourselves on the other side of the mat.
Fortunately, the story is starting to change. Governmentsaround the world are doing more for children’s health.Efforts to treat and prevent the world’s most devastatingdiseases are improving the lives of millions of children.
To keep this momentum going, we must remember thatthese mothers love their children just as much as we loveours. We must see that these children have boundlesspotential. And we must help them realize their potentialby bringing more governments, more businesses andmore individuals to this work – to unite for maternal, newborn and child survival and health. When we do, allmothers will have a chance to see their children grow uphappy and strong, and all children will have a chance tomake their dreams come true.
The other side of the mat: Uniting for maternal, newborn and child
survival and health