the the gynaecological examination pelvic aid diagnosis
TRANSCRIPT

Shri Gujarati Samaj Indore
SKRP Gujarati Homoeopathic Medical College Hospital & Research centreGuided BY : SUBMITTED
BY :DEEPTI GAUTAM3RD PROFF

THE GYNAECOLOGICAL EXAMINATION AND PELVIC AID DIAGNOSIS

CONTENTS
IntroductionGynecological historyGeneral examinationBreast examinationAbdominal examinationPelvic examination - Digital
and speculum examinationInvestigations

INTRODUCTION
Gynecological history coupled with a systemic examination would help in arriving at the correct diagnosis.
A good history taking ,alone can give a positive diagnosis without any physical examination.

•The examination should, in fact proceed with the provisional diagnosis in mind.•Patients privacy should be respected always .•A brief outline of history taking is given below:


GYNAECOLOGIACAL HISTORY
History should be taken in details.
If multiple symptoms are present, their chronological appearances are to be noted.
Enquiry should be made about the bowel habits and urinary troubles if any.

GYNAECOLOGIACAL HISTORY
MENSTRUAL HISTORY OBSTRETIC HISTORY PAST MEDICAL HISTORY PAST SURGICAL HISTORY FAMILY HISTORY PERSONAL HISTORY

MENSTRUAL HISTORY
Inquiry should be made about: First menarche(age of onset of first
menstrual period) Regularity of cycle Duration of period Length of the cycle Amount of bleeding excess is indicated
by clots and number of pads used. First day of last menstrual period(LMP)

OBSTRETIC HISTORY
If the patient had been previously pregnant then details should be noted.
Some times, the complaints may be related due to the pregnancy or lactation complications.

OBSTRETIC HISTORY
The details should be noted in following way
No. Date
Year &events
Pregnancy details
Labour details
Method of delivery
puerperium
Baby wt &sex birth asphyxia. duration of breast feeding, contraception
1
2

PAST MEDICAL HISTORY
The following disorder should be noted
SystemicMetabolicEndocrinal(diabetes, hepatitis,
hypertension)Sexual transmitted disorder

PAST SURGICAL HISTORY
This includesGeneral Obstetrical Gynecological surgeryNature of operation Bleeding or clotting complicationPost operative care Any histopathologiacal disorder

FAMILY HISTORY
It is of occasional value .Malignancy of breast,ovary,colon
are often related.Tubercular infection in family
can also give clue about pelvic tuberculosis

PERSONAL HISTORY
Occupation Marital status : widow, single,
married. If married then sexual history
should be taken.Contraceptive practice, if any,
should also be inquired.

EXAMINATION

GUIDELINES
Gynecological examination confirms presence of pathology suspected from the gynecological history.
Always explain to the patient the need and the nature of the proposed examination.
Obtain an informed verbal consent. The examiner (male or female) should be
accompanied by another female (chaperone).
Examination performed in a private setting, respecting patient's privacy at all times.
Patient should be covered at all times and only relevant parts of her anatomy exposed.

GENERAL AND SYSTEMIC EXAMINATION
BUILT: to obese or too thin. May be due to any endocrinopathy.
NUTRTION: average/ poorSTATURE: including development
of secondary sex characters.PALLOR JAUNDICE

OEDEMA OF LEGSTEETH GUMS AND TONSILSNECK: palpation of thyroid gland
and left Supraclavicular glands CARDIOVASCULAR AND
RESPIRATION SYSTEMS: any abnormality if present
PULSEBLOOD PRESSURE

GYNAECOLOGICAL EXAMINATION
BREAST EXAMINATIONABDOMINAL EXAMINATIONPELVIC EXAMINATION

BREAST EXAMINATION
Inspection with arms by her side
Inspection with arms Raised above Inspection with Hands at waist
Palpation of axillary node Palpation of Supraclavicular nodePalpation of Other half of breast

BREAST EXAMINATION
It should be routine examination in women above the age of 30
POSITION: patient reclining at 45 degrees with arms at the sides
INSPECTION – positions at rest, arms above head, on hips
1) Development and symmetry of breasts and nipples.
2) Reddening of skin, ulceration or dimpling (peau d'orange)
3) Retraction of nipple (CA breast) 4) Nipple discharge- blood, serous or
milky

PALPATION- palpate systematically for lumps with the flat part of the fingers, through all 4 quadrants. If present, describe the characteristics of the lump- location, size, shape, surface, edge, consistency and mobility in relation to deep and superficial structures.
Palpate the axillae for lymph nodes – describe if present

ABDOMINAL EXAMINATION
PREREQUISITE Bladder should be empty, if there is
history of chronic retention of urine, then do catheterisation.
The patient is to lie flat on table with thigh slightly flexed and abducted to make abdominal muscle relaxed.
The physician should stand on right side
Presence of female for the support of the patient

STEPS
INSPECTION: Assess for distension, scars (operative, traumatic or scarification), distended veins, striae, pubic hair distribution.
PALPATION: Palpate the abdomen systematically in all 9 regions
1) Superficial palpation- assess for tenderness, guarding and rebound tenderness
2) Deep palpation- assess any enlargement of intra-abdominal organs (uterus, liver, spleen etc) and for any abnormal masses.

Describe any abnormal mass in terms of:
SIZE, SHAPE POSITION- MOBILITY- movable or fixed SURFACE - e.g. smooth or nodular CONSISTENCY - e.g. solid or cystic TENDERNESS (pain on palpation)

PERCUSSION: A pelvic tumor is usually dull and
resonance on flanks Assess for ascites using shifting
dullness and fluid thrill AUSCULTATION: Listen for bowel
sounds or for fetal heart rate in pregnancy.
Uterine soufflé can also be heard in pregnancy.

PELVIC EXAMINATION
This includes Inspection of external genitaliaVaginal examination
Inspection and palpation of cervix and vagina walls
Rectal examinationRectovaginal examination
Positions of patient during examination
Sims position Dorsal position Lithotomy position

Sims position

Dorsal position

Lithotomy position

INSPECTION OF VULVA
To note any : Anatomical abnormality starting form
pubic hair, clitoris, labia and perineum. Palpable pathology External urethral meatus and opening of
bartholin duct and character of hymen. To ask the patient to strain to elicit:
To see stress incontinence Genital prolapse
Lastly look for hemorrhoids

VAGINAL EXAMINATION
INSPECTION OF VAGINA AND CERVIX
Speculum examination
Digital examination
Bimanual examination

SPECULUM EXAMINATION
Most Preferably used.Advantages are:Cervical scrape cytology and
endocervical sampling can be taken for screening.
Cervical or vaginal discharge can be taken for bacteriological examination.

TWO TYPE OF SPECULUM IS USED
Sims's speculum Cusco’s valve

In dorsal position Cusco's valve is used, while in lateral – sim’s speculum.
Cervix is best seen by Cusco's valve
Vaginal fornices can only be seen by Cusco's valve while anterior wall of vagina can be seen by sim’s speculum.

DIGITAL EXAMINATION
Done by using gloved index finger lubricated with sterile lubricant.
In virgins done under anesthesia.To note
Palpation of any labial swelling Pressing of urethra from above down
ward to see any discharge escaping out.
Palpation of vaginal walls to detect any abnormality

Palpation of vaginal portion of cervix To note Direction-in anteroverted uterus ant. lip is
first felt & in retroverted position external-os or post. lip is felt.
Station-external-os is at level of ischial spine Texture- in nonpregnant stage firm. Shape- conical in multipara and cylindrical in
nullipara. Ext.os –smooth and round in nullipara and
dilated in parous Movement-painful or not Whether it bleeds or not

BIMANUAL EXAMINATION
Done by using gloved index finger lubricated with sterile lubricant.
Gloved right index and middle finger is inserted in to the vagina,if intortius is narrower then only one finger is used.
The left hand is placed on the hypogastrium well abdomen above the symphysis pubis so that the organs can be palpated.

BIMANUAL EXAMINATION
PALPATION OF UTERUSPALPATION OF UTERINE
APPENDAGESPOUCH OF DOUGLAS

PALPATION OF UTERUS
Note its position size shape consistency
and mobility Normally the uterus is anteverted,
pear shaped firm, freely mobile in al directions.

PALPATION OF UTERUS

PALPATION OF UTERUS

PALPATION OF UTERINE APPENDAGES
Normally uterine tube cannot be palpated.
Normal Ovary cannot be palpated. If palpated, it is mobile and sensitive
to manual pressure.

PALPATION OF UTERINE APPENDAGES

POUCH OF DOUGLAS
Normally faecal mass in rectosigmoid and the body of retroverted uterus is felt.

Indications of mass felt of bimanual examination
Uterine tumor: Uterus is not separated from mass Movements of mass felt per
abdominally transmitted to the cervix.
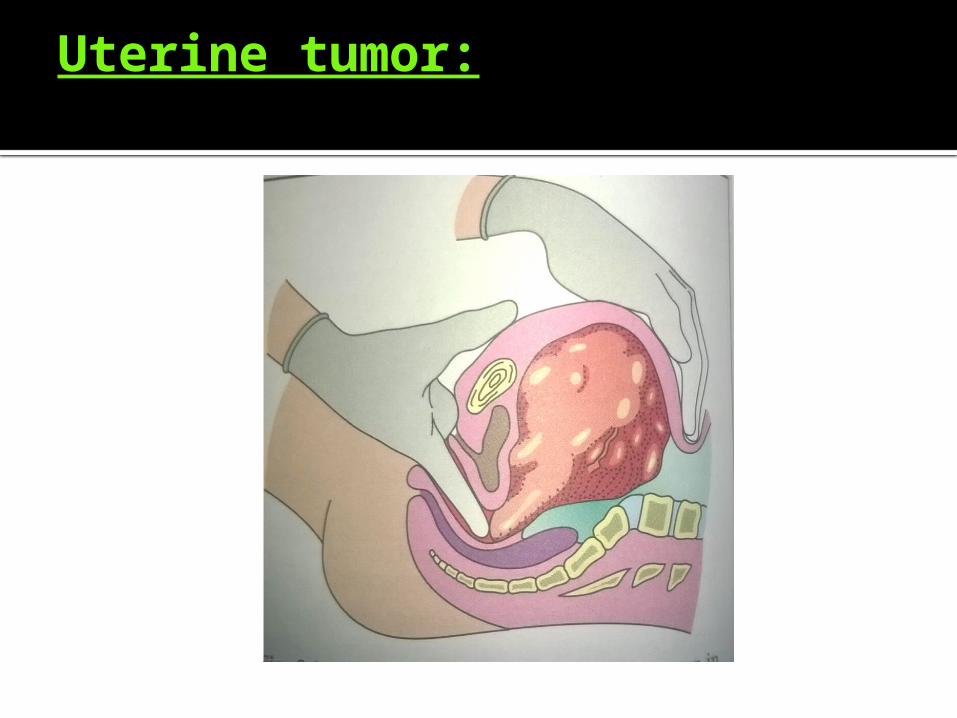
Uterine tumor:
Adnexal mass: uterus is separated from mass Movements of mass are not
transmitted to the cervix.


RECTAL EXAMINATIONORRECTOVAGINAL EXAMINATION

RECTAL EXAMINATION
Indication for rectal examination: Children or in adult virgins. Painful vaginal examination Ca of cervix Abnormal findings in pouch of
Douglas during bimanual examination
Artesia of vagina Patient having rectal symptoms

RECTAL EXAMINATION

RECTOVAGINAL EXAMINATION
In this procedure, gloved index finger is introduced n vagina and middle finger is introduced in rectum
Helps in determining whether the lesion is in bowel or between rectum and vagina .

RECTOVAGINAL EXAMINATION

DIAGNOSTIC PROCEDURE
Blood values Urine Urethral discharge Vaginal or cervical discharge: done
by Cusco's bivalve speculum

BLOOD VALUES
Hemoglobin estimation: in cases of excessive bleeding.
TLC & DLC, ESR Platelet count in cases of puberty
menorrhagia.
:diagnosis of pelvic inflammation
URINE EXAMINATION
For the presence of protein sugar pus cell casts are done .
In the presence of excessive of vaginal discharge midstream urine is taken
Culture &drug sensitivity test: Midstream collection Catheter collection Suprapubic bladder puncture

EXAMINATION OF CERVICAL MUCUS
Bacteriological study: Cusco's bivalve speculum is inserted
without lubricant sample is taken via sterile cotton sterile swab and sent for culture.

EXAMINATION OF CERVICAL MUCUS
Hormonal status: cervical secretion is dependent on
hormones estrogen and progesterone the influence of these hormones helps in detection of time of ovulation.
Normal Ph of cervical mucus during ovulation is about 6.8-7.4.

Fern test
Cervical mucus shows characteristic fern pattern formation.
The ferning disappears completely after 21st day .

Presence of ferning even after the 21st day indicates anovulation and its absence gives evidence of ovulation.

INVESTIGATIONs
Colposcopy
X-ray Ct scan Ultrasoun
d MRI

X ray
Uses Can be helpful in locating IUCDs,
benign tumors etc.

Ct scan
Bilateral ovarian cystic masses

INVESTIGATIONs
ENDOSCOPY
Culdocentesis Laparoscopy Hysteroscopy Salpingoscopy
COLPOSCOPY
Done by colposcope. Use: magnify the surface
epithelium of the vaginal part of the cervix including entire transformation zone

COLPOSCOPY

CULDOCENTESIS
Aspiration of peritoneal fluid from pouch of doulas.

LAPAROSCOPY
Visualization of peritoneal cavity by means of a fiber optic endoscope.

HYSTEROSCOPY
Visualization of endometrial cavity by means of a fiber optic telescope

SALAPINGOSCOPY
Visualisation of uterine tubes.FIMBRIA
TELESCOPE
UTERINE TUBE

END OF PRESENTATION
FOR LISTENING