the burdenapps.searo.who.int/pds_docs/b0414.pdf · the global plan to stop tb and the regional...
TRANSCRIPT

The WHO South-East Asia Region covers Bangladesh, Bhutan, DPR Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor-Leste
1.5 billion people live in these eleven countries, including half of the world’s poor
Five countries – Bangladesh, India, Indonesia, Myanmar and Thailand – belong to the 22 countries globally with the highest burdens of TB
<1010 to 2425 to 4950 to 99100 to 299300 or moreNo Estimate
Global TB incidence rates
TB traps people in a vicious cycle of poverty and disease—in South-East Asia, the economic and social costs are staggering —
TB levies a cost of about US$ 4 billion every year
A TB patient loses on an average, three months’ wages
A death due to TB means a loss of 10-15 years of a household’s income
In India alone, 300 000 children drop out of school and
100 000 women are forced out of their homes every year due to TB
THE BURDEN
Five million people suffer from TB in the South-East Asia Region and over half a million die every year
Incidence rates per 100,000 pop
The boundaries shown on the above map do not imply official endorsement or acceptance by WHO


The Global Plan to Stop TB and the Regional Strategic Plan for TB Control 2006-2015, outline actions towards achieving the TB-related targets under the Millennium Development Goals—halting and reversing the incidence of TB by 2015.
Over the next 10 years in the South-East Asia Region, and towards reaching the MDGs, countries aim to:
Treat and cure 25 million TB patients, including those with HIV co-infection and drug-resistant TB; and thereby,
Save 5 million people from dying of TB
THE VISION
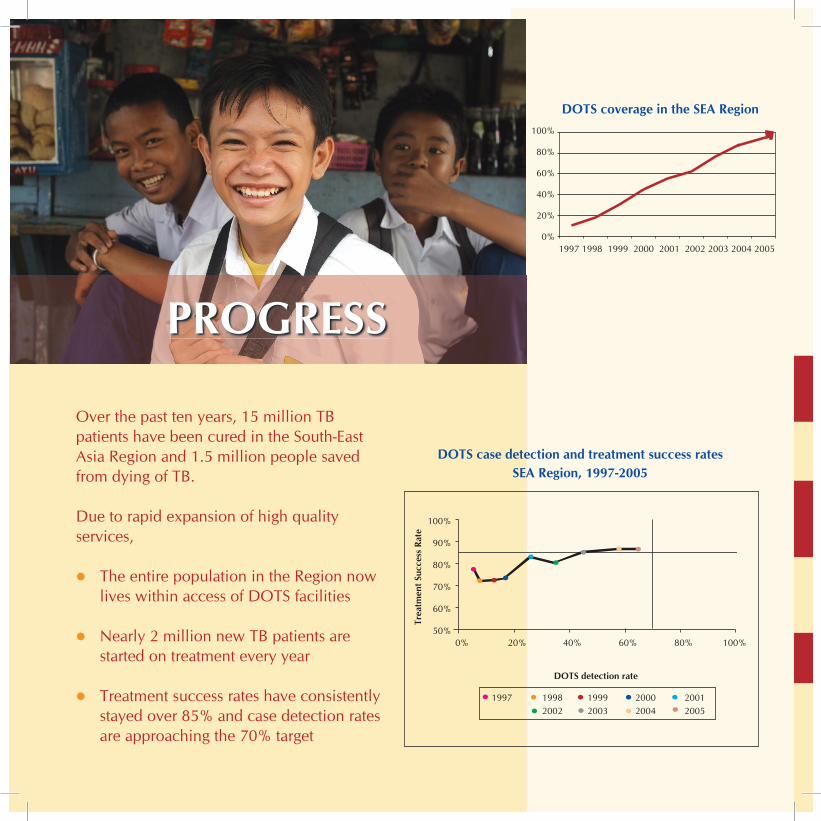
Over the past ten years, 15 million TB patients have been cured in the South-East Asia Region and 1.5 million people saved from dying of TB.
Due to rapid expansion of high quality services,
The entire population in the Region now lives within access of DOTS facilities
Nearly 2 million new TB patients are started on treatment every year
Treatment success rates have consistently stayed over 85% and case detection rates are approaching the 70% target
PROGRESS
DOTS case detection and treatment success rates SEA Region, 1997-2005
100%
90%
80%
70%
60%
50%
Trea
tmen
t Suc
cess
Rat
e
DOTS detection rate
0% 20% 40% 60% 80% 100%
1997 1998 1999 2000 2001 2002 2003 2004 2005
DOTS coverage in the SEA Region100%
80%
60%
40%
20%
0%1997 1998 1999 2000 2001 2002 2003 2004 2005
CHALLENGESThe need to extend quality services to find and successfully treat all TB patients who have not yet been reached
Improving access to quality laboratory services as well as drugs and support for patients until they are cured, to prevent multi-drug resistance (MDR-TB)
HIV-associated TB and anti-TB drug resistance which threaten to reverse hard-won gains in TB control
Establishing close collaboration between TB and HIV/AIDS control programmes to address the needs of patients dually affected, through a patient-friendly “one-stop-shop” approach, and treating those with drug resistant TB
Limited public and private partnerships
Involving all health care providers, other ministries and departments, NGOs, business, industry and civil society at large, to ensure an equitable access to TB services
DOTS coverage in the SEA Region
1997 1998 1999 2000 2001 2002 2003 2004 2005
CHALLENGESIgnorance, stigma and misconceptions leading to poor community utilization of available services
Sustaining communication and social mobilization approaches adapted to local situations, so that people use and help themselves to use services already in place
Overstretched national health systems with limited infrastructure, scarcity of skilled staff
Developing and better managing staffing and financing for health, effectively integrating and streamlining services, through innovative approaches
Insufficient resources particularly in the longer term—the sustainability of TB control in the Region is at risk
Leveraging regional resources, complemented by external resources, to ensure human, financial and operational capacity, until we begin to reverse the epidemic

Sustaining and enhancing DOTS to reach all TB patients, improving case detection and treatment success rates
Ensuring quality diagnostics and universal access to treatment for all TB patients, while simultaneously evaluating and monitoring programme performance and impact
Establishing interventions to address HIV-associated TB and drug-resistant TB
Jointly implementing HIV/AIDS and TB prevention, treatment, care and support for those dually affected, and providing quality diagnosis and treatment with second-line drugs for those with drug-resistant TB
KEY STRATEGIES

Costs for TB control activities National TB Programmes
KEY STRATEGIESForging partnerships to ensure equitable access to an essential standard of care to all TB patients
Consolidating existing partnerships with all stakeholders including all providers, attracting new partners and engaging communities and patients to extend an equitable access to services
Contributing to health systems strengthening
Developing and better managing human and other key resources, and contributing to health systems development through integrated and innovative approaches
SUPPORT TO COUNTRIES WHO Regional and Country offices assist National TB Control Programmes with —
13%6%
12%
10%
10%
5% 5%
36%
3%
Policy, Planning, Coordination and Resource Mobilization
Advocacy, Communication and Social Mobilization
Surveillance, Monitoring and Evaluation
Addressing MDR-TB and TB/HIV
Strengthening Laboratory Networks
Establishing Private and Public Partnerships
Ensuring Effective Drug Procurement and Supply Management
Research
Operational Costs
TOTAL BUDGET 2006-2007: US$ 28 MILLION
REGIONAL OFFICE
WHO Support in the Region
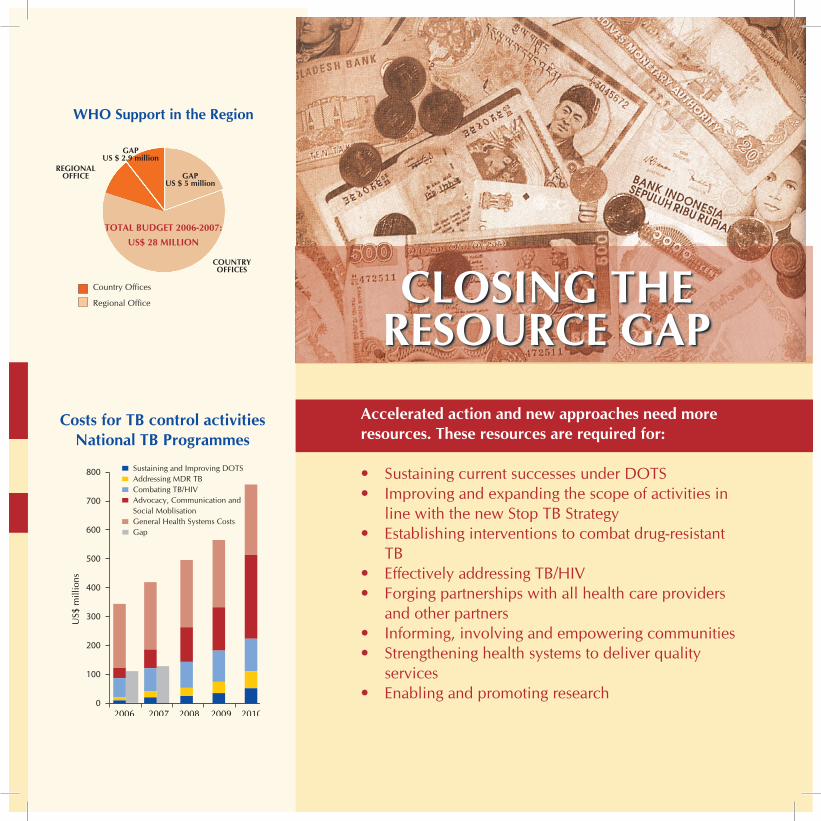
Costs for TB control activities National TB Programmes
CLOSING THE RESOURCE GAP
Accelerated action and new approaches need more resources. These resources are required for: • Sustaining current successes under DOTS • Improving and expanding the scope of activities in
line with the new Stop TB Strategy • Establishing interventions to combat drug-resistant
TB • Effectively addressing TB/HIV • Forging partnerships with all health care providers
and other partners• Informing, involving and empowering communities • Strengthening health systems to deliver quality
services • Enabling and promoting research
2006 2007 2008 2009 2010
US$
mill
ions
Sustaining and Improving DOTSAddressing MDR TBCombating TB/HIVAdvocacy, Communication andSocial MoblisationGeneral Health Systems CostsGap
0
100
200
300
400
500
600
700
800
TOTAL BUDGET 2006-2007: US$ 28 MILLION
GAPUS $ 5 million
GAPUS $ 2.9 million
REGIONAL OFFICE
COUNTRYOFFICES
Country Offices
Regional Office
WHO Support in the Region
"
SRI LANKA
TIMOR L’ESTE
MALDIVES
NEPAL
INDIA
BHUTAN
MYANMAR
THAILAND
INDONESIA
BANGLADESH
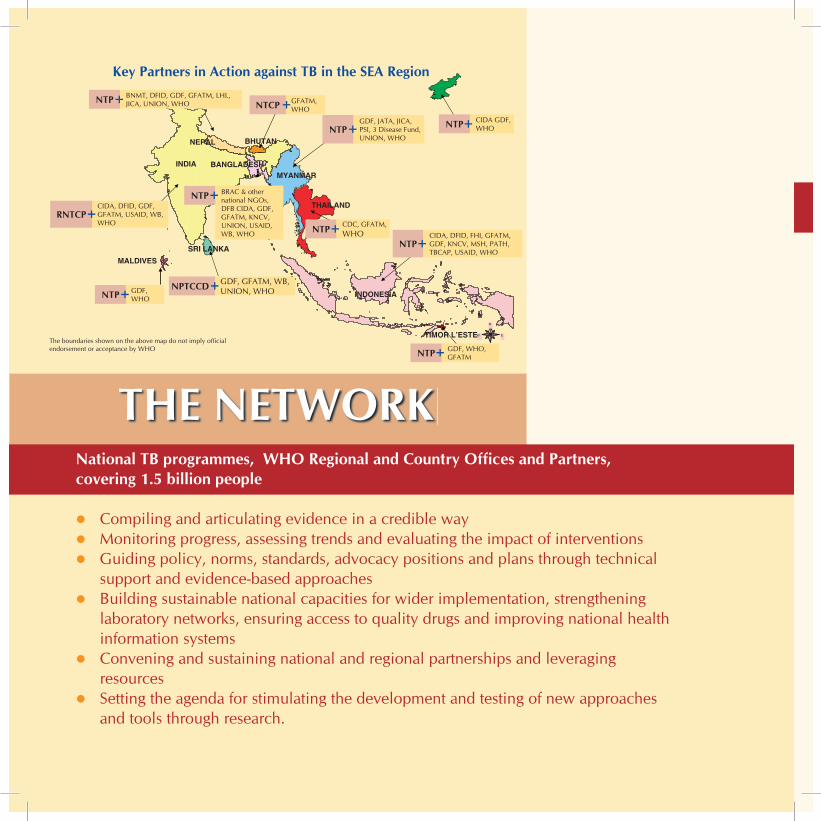
Key Partners in Action against TB in the SEA Region
National TB programmes, WHO Regional and Country Offices and Partners, covering 1.5 billion people
Compiling and articulating evidence in a credible way Monitoring progress, assessing trends and evaluating the impact of interventions Guiding policy, norms, standards, advocacy positions and plans through technical
support and evidence-based approaches Building sustainable national capacities for wider implementation, strengthening
laboratory networks, ensuring access to quality drugs and improving national health information systems
Convening and sustaining national and regional partnerships and leveraging resources
Setting the agenda for stimulating the development and testing of new approaches and tools through research.
THE NETWORK
RNTCPCIDA, DFID, GDF, GFATM, USAID, WB, WHO
NTP BNMT, DFID, GDF, GFATM, LHL, JICA, UNION, WHO NTCP GFATM,
WHO
NTPGDF, JATA, JICA, PSI, 3 Disease Fund, UNION, WHO
NTP BRAC & other national NGOs, DFB CIDA, GDF, GFATM, KNCV, UNION, USAID, WB, WHO
NPTCCD GDF, GFATM, WB, UNION, WHONTP GDF,
WHO
NTP CDC, GFATM, WHO
NTPCIDA, DFID, FHI, GFATM, GDF, KNCV, MSH, PATH, TBCAP, USAID, WHO
NTP CIDA GDF, WHO
NTP GDF, WHO, GFATM
The boundaries shown on the above map do not imply official endorsement or acceptance by WHO
TOWARDS A WORLD FREE OF TB
Private involvement in delivering TB services: The Mahavir Hospital, a private hospital in Hyderabad, India, successfully piloted a private partnership programme in collaboration with the government, to expand DOTS within the city through private medical practitioners. This initiative led the way for establishing wider model private and public partnerships for TB care.
National partnerships for wider sustainability: A wide social movement (Gerdunas) involving several organizations and groups has been established in Indonesia, creating TB awareness and broadening the national resource base for TB services. National partnerships of this kind will help sustain efforts in the years to come.
Realizing the potential in South-East Asia: South-East Asia is a manufacturing hub, already a major supplier of first-line anti-TB drugs to the Global Drug Facility. The pharmaceutical sector in the Region offers great potential for research and development as well as for manufacturing new and more effective tools for diagnosis and treatment.
Community-based TB Care: Women community volunteers, the shastho shebikas of BRAC in Bangladesh, demonstrated success of TB programmes in poor settings, and among unorganized groups with minimal resources. Today, several countries have established community-based models for TB care.
We can succeed! A number of innovative and successful interventions by governments, NGOs and the private sector have already inspired wider replication