the surgical patient & special patient populations concorde career college st210
TRANSCRIPT
The Surgical Patient & Special Patient
Populations
Concorde Career CollegeST210

List and differentiate between the preoperative duties of the circulator and the surgical technologist in the scrub role
Identify the biological needs of the patient and identify fundamental patient care elements used to meet these needs in the surgical environment
Objectives
Identify the psychological needs of the patient and identify fundamental patient care elements used to meet these needs in the surgical environment
Identify the social needs of the patient and identify fundamental patient care elements used to meet these needs in the surgical environment
Objectives
Identify the spiritual needs of the patient and identify fundamental patient care elements used to meet these needs in the surgical environment
Identify the cultural needs of the patient and identify fundamental patient care elements used to meet these needs in the surgical environment
Objectives

Objectives
Identify the needs of special patient populations (e.g., pediatric, geriatric, immunocompromised) and identify fundamental patient care elements used to meet those needs in the surgical environment

Team Members
Surgical Team Members

Team Members
Who are the surgical team members and what are their roles?

Needs of the Patient
Needs of the Patient

Needs of the Patient
Maslow’s Hierarchy of Needs

Needs of the Patient
Biological Needs (also called physical, physiologic)
Necessary for LifeOxygenNutrition (water, food)Regulation of body processes (sleep,
fluid balance, O2/CO2 exchange, temperature regulation, elimination of waste)
Needs of the Patient
Safety Needs
Perception that one’s environment is safe

Needs of the Patient
Love and Belonging Needs
Basic social needsTo be known and cared for as an
individualTo care for another (others)
Needs of the Patient
Prestige & Esteem Needs
Need to have a positive evaluation of oneself and others
Need to be respected and respect others

Needs of the Patient
Self Actualization
Need to fulfill what is believed to be one’s purpose
Needs of the Patient
Psychological Needs
Any need or activity related to the identification and understanding of oneself Fear Loss of security Family issues
Needs of the Patient
Social Needs
Any need or activity related to one’s identification or interaction with another individual or group
Needs of the Patient
Spiritual Needs
Any need or activity related to the identification and understanding of one’s place in an organized universe
Needs of the Patient
Cultural Needs
Every culture has different beliefs and value orientations
Cultural values will specify the way the patient thinks and feels about these values

Special Patient Populations
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
19
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
20
Patients with Special Needs
Surgical patients with special needs present various challenges
Unique physical and psychological needs
Surgical technologists must be aware of those needs
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
21
Special Needs Patients Unique physical & psychological needs
PediatricsImmunocompromisedPregnantDiabeticDisabledObeseGeriatric
Pediatrics
Developmental levels and Biological differences Neonate - birth to 28
days Infant – 1–18 months Toddler – 18-30
months Preschooler – 30 months to 5 years School age – 6-12
years Adolescent – 13-18 years
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
23
Monitoring the Pediatric Patient
Temperature Urine output
(collection bag/no catheter)
Cardiac function Intra-arterial
measurement Central Venous
Catheter Oxygenation
(ABG’s)

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
24
Shock in the Pediatric Patient
Septic Shock• Caused by gram-negative bacteria• Intestinal perforation, UTI, URI
Hypovolemic Shock• Common cause: Dehydration• Treated by quick fluid and blood
replacement
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
25
Fluids & Electrolytes/Infection
Monitoring fluids & electrolytes
Infection• Monitoring• Antibiotics
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
26
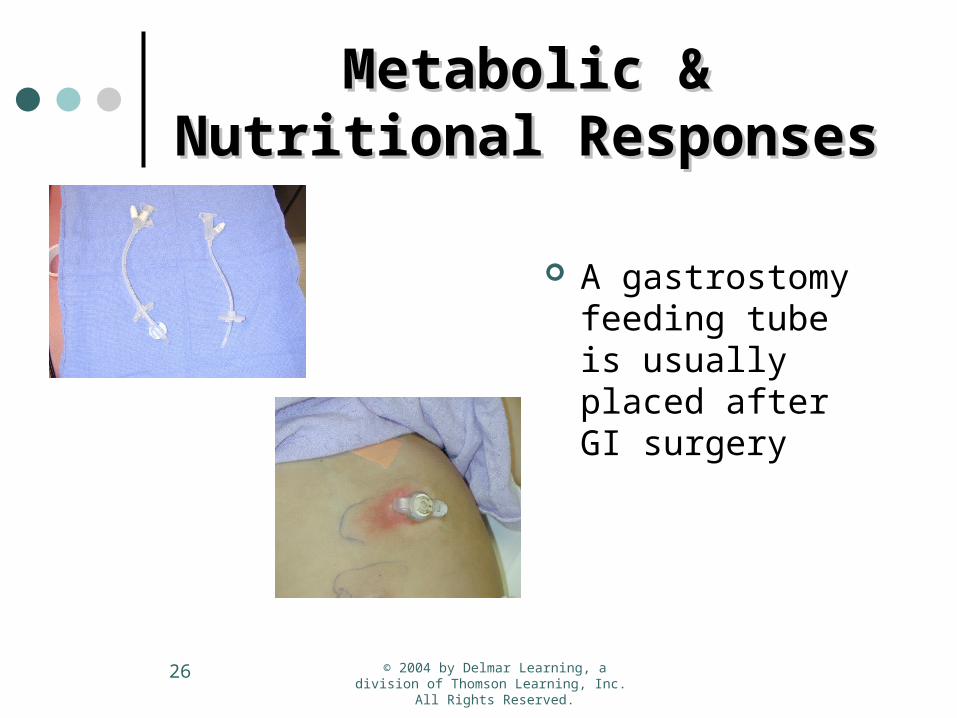
Metabolic & Nutritional Metabolic & Nutritional ResponsesResponses
A gastrostomy feeding tube is usually placed after GI surgery
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
27
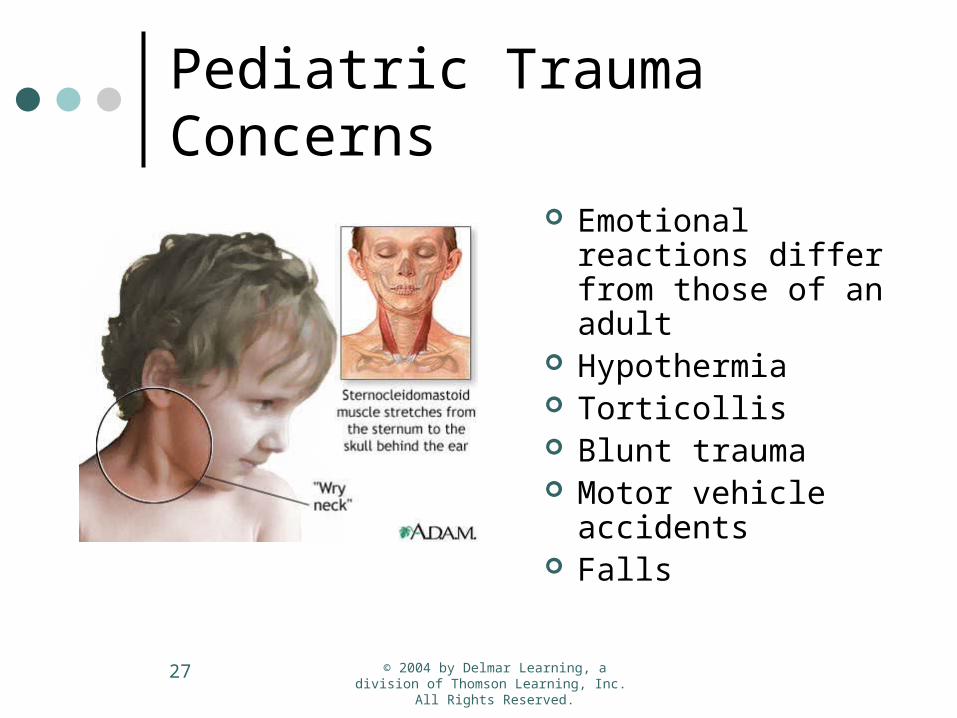
Pediatric Trauma Concerns
Emotional reactions differ from those of an adult
Hypothermia Torticollis Blunt trauma Motor vehicle
accidents Falls
Pediatrics
Accidents are the number one cause of death in children ages 1-15.
Approximately 20 million childhood injuries result in death or permanent disability annually
Obesity
Obesity – defined by BMI
•An adult who has a BMI between 25 and 29.9 is considered overweight.
•An adult who has a BMI of 30 or higher is considered obese.
Obesity Scale
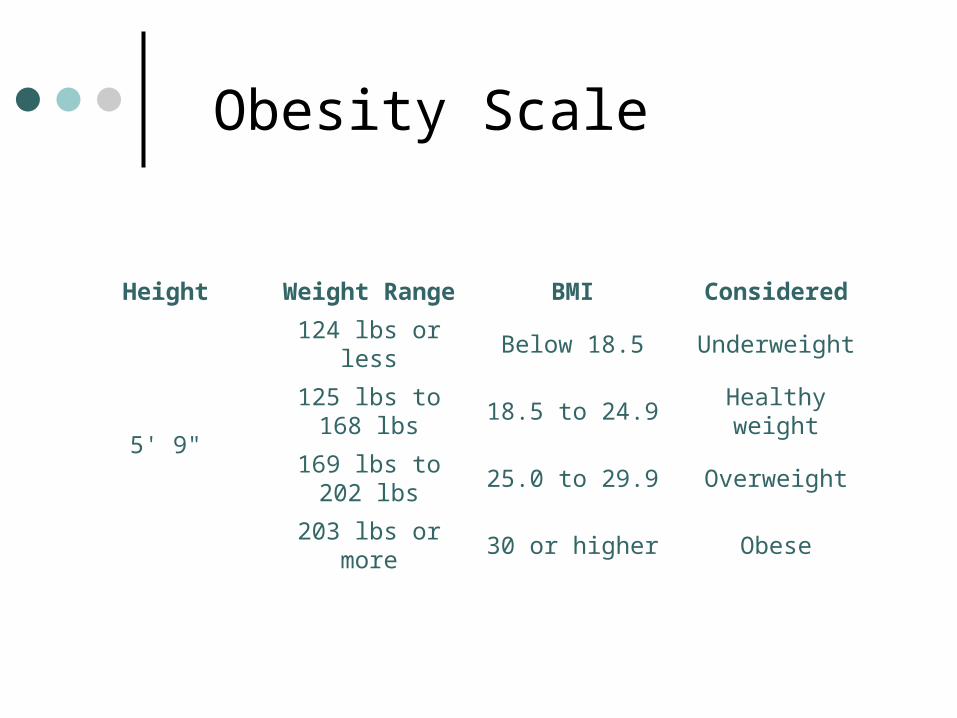
Height Weight Range BMI Considered
5' 9"
124 lbs or less Below 18.5 Underweight
125 lbs to 168 lbs
18.5 to 24.9 Healthy weight
169 lbs to 202 lbs
25.0 to 29.9 Overweight
203 lbs or more 30 or higher Obese

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
31
Care of Obese PatientsCare of Obese Patients
Patient whose body weight is 100 pounds greater than ideal weight
Physiological disease conditions related to obesity• Myocardial hypertrophy• Coronary artery disease• Hypertension & vascular changes of the kidneys• Varicose veins and edema• Pulmonary Functions• Liver & Gallbladder Disease• Diabetes• Osteoarthritis• Pituitary abnormalities
Gastric Bypass Gastric Bypass (Bariatric Surgery)(Bariatric Surgery)
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
33
What is Morbid Obesity?
Morbid Obesity is a serious disease process, in which the accumulation of fatty tissue on the body becomes excessive, and interferes with, or injures the other bodily organs, causing serious and life-threatening health problems, which are called co-morbidities.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
34
Indications
Gastric bypass surgery is recommended only for patients who are morbidly obese. Usually more than 100 pounds overweight, these individuals have major health problems related to their weight.
The Body Mass Index BMI is typically used to identify surgery candidates with a cut-off of 40 being used by most surgeons. BMI’s down to 35 are typically permitted if the individual has other serious health issues.
Gastric bypass is overwhelmingly successful, with many patients losing over 100 pounds within the first 18 months following surgery. Gastric bypass surgery should always be accompanied by an exercise regimen.
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
35
Today, there are several surgical Today, there are several surgical procedures used for achieving procedures used for achieving weight loss. The most common are:weight loss. The most common are:
: Roux-en-Y gastric bypass Lap-Band
Gastric Bypass Surgery
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
36
Comparison between the Lap-Band
& Gastric Bypass procedures Lap-Band
Less invasive Outpatient surgery Reversible Adjustable No rearrangement of
anatomy Slower weight loss Not endorsed by NIH Less well studied in US More follow-up required More dietary
compliance required
Gastric Bypass
More invasive Inpatient surgery Not easily reversible Not adjustable Anatomy rearranged Faster weight loss Endorsed by NIH Well studied in US Less follow-up required Less dietary compliance
required
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
37
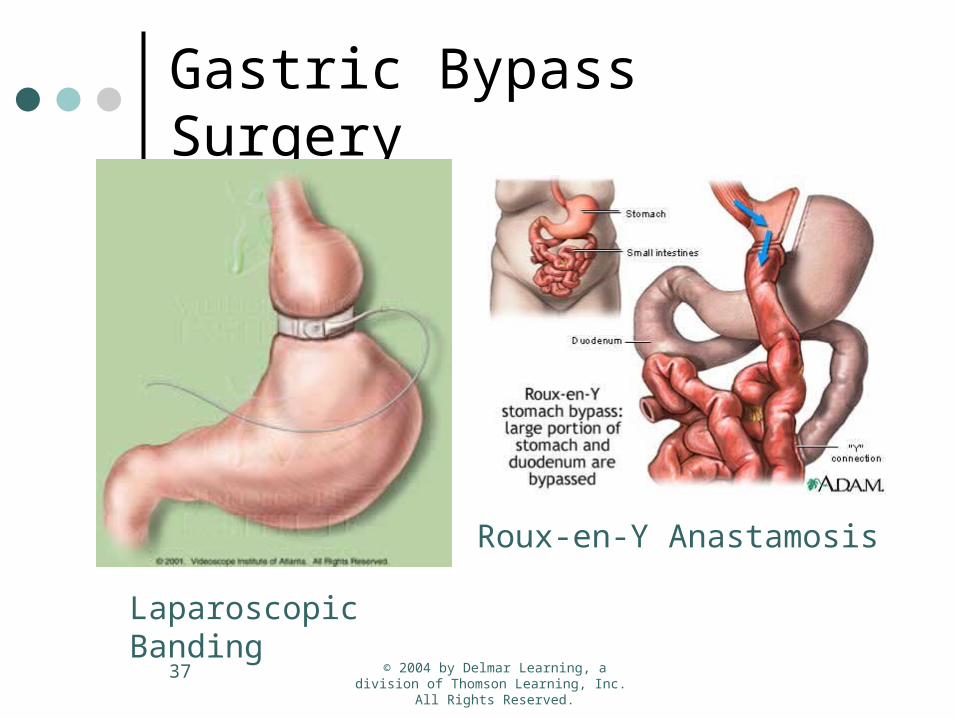
Gastric Bypass Surgery
Laparoscopic Banding
Roux-en-Y Anastamosis

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
38
The Procedure…
The patient is placed in the supineposition and trocars are placed appropriately.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
39
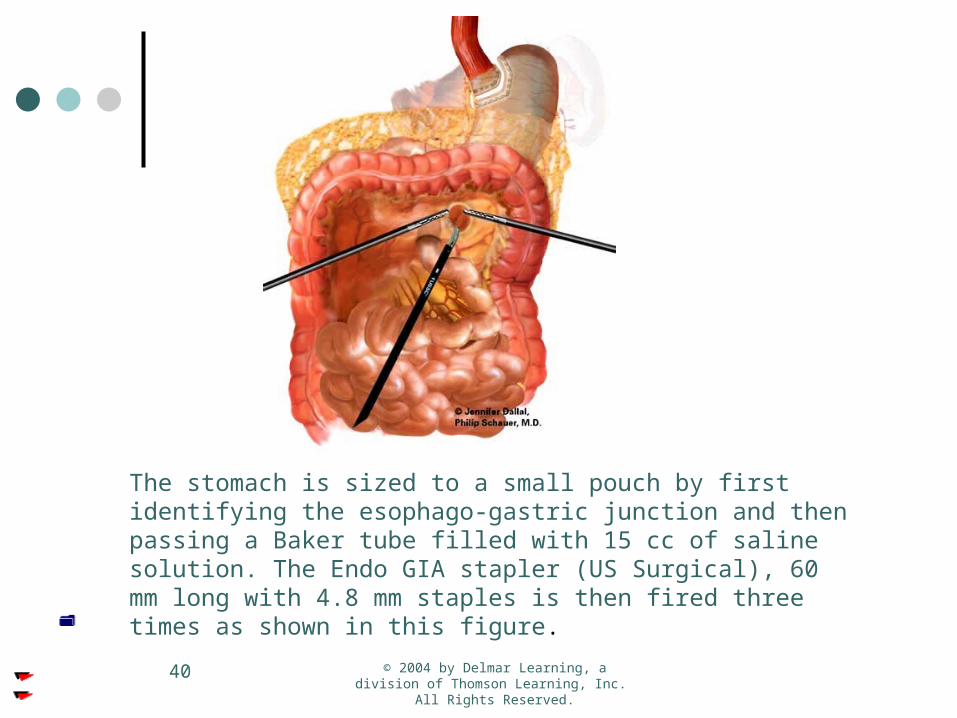
The stomach is sized to a small pouch by first identifying the esophago -gastric junction and then passing a Baker tube filled with 15 cc of saline solution. The Endo GIA stapler (US Surgical), 60 mm long with 4.8 mm staples is then fired three times as shown in this figure.
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
40
The stomach is sized to a small pouch by first identifying the esophago-gastric junction and then passing a Baker tube filled with 15 cc of saline solution. The Endo GIA stapler (US Surgical), 60 mm long with 4.8 mm staples is then fired three times as shown in this figure.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
41
In order to create the Roux-limb, the jejunum is divided 15 cm beyond the ligament of Treitz by using an Endo GIA II stapler (US Surgical), 45 mm long with 3.5 mm staples. In addition the mesentery is also divided with a Endo GIA II stapler, but this time using the vascular load (45 mm length, 2.0 mm staples). This maneuver will facilitate mobilization of the small intestine through the mesocolon. A rubber drain is sutured to the jejunum to help with the pulling.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
42
The Roux-limb is measured according to the patient BMI (Body Mass Index) and can range from 75 to 200 cm in length. Notice that the laparoscopic grasper is used as a ruler.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
43
An end-to-side anastomosis between the proximal jejunum and the roux limb is created by firing two Endo GIA II staplers. The enterotomy is closed using another load of staples. The mesentery
is also closed to prevent bowel entrapment (internal hernias).

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
44
Close up view of the enteroenterostomy

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
45
The Roux-limb is now advanced trough the mesocolic window (retrocolic and retrogastric) near the transected stomach.
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
46
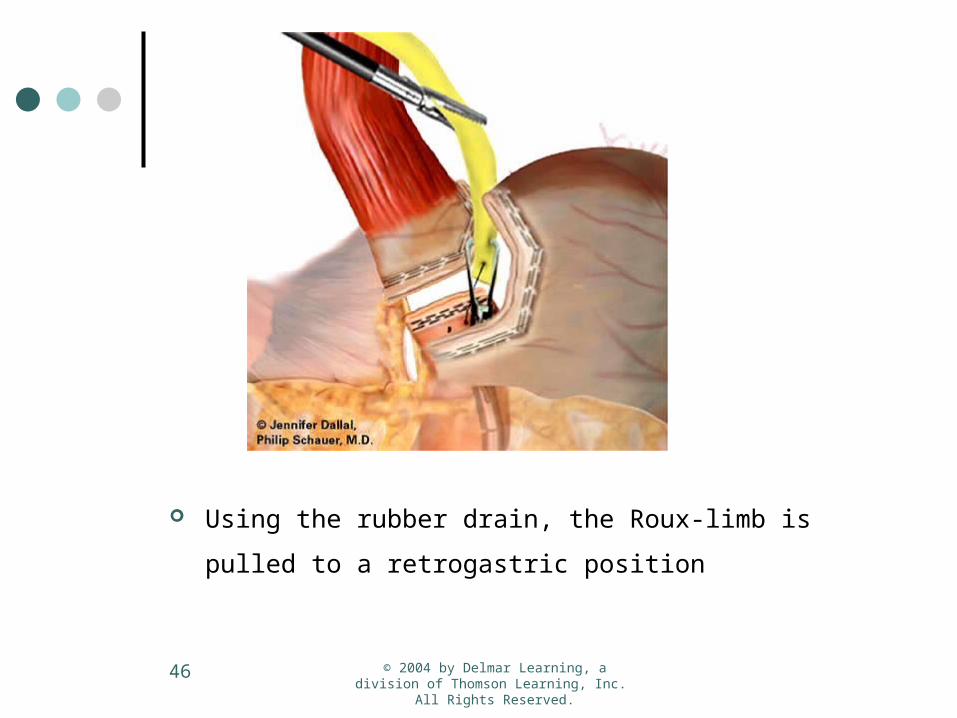
Using the rubber drain, the Roux-limb is pulled to a
retrogastric position

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
47
Following an enterotomy an anastomosis between the gastric pouch and the Roux-limb is created by firing a Endo GIA II.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
48
The enterotomy is stapled shut with another load of Endo GIA II. The anastomosis is secured by placing an extra row of stitches. The gastrojejunostomy and the enterotomy site are tested for leakage by applying insufflation through an nasogastric tube (or endoscope) and submerging the area
in irrigation solution.

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
49
Lifetime Commitment
Undergoing a gastric bypass requires patients to commit to a new lifestyle. They will no longer be able to eat large portions of food at one sitting, nor will they be able to eat foods high in sugar or fat, which often result in dumping syndrome, an unpleasant feeling of faintness caused by the sudden absorption of these foods in the shortened digestive tract. Due to the limited amount patients can take in at any one time, they must constantly drink small amounts of water or risk dehydration.
The operation while highly successful does have a morbidity rate of approximately 2% overall. 1% having immediate complications and death another 1% will commonly have post operative complications that lead to death within one month of surgery. This can be mitigated by compliance with the surgeon's post operative plan and using a Doctor who has performed more then 200 procedures.
However it should be noted that a full 25% of people undergoing this operation will have some form of post operative complication either requiring a further procedure or change in habits.
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
50
Diabetes Mellitus
Type I (IDDM)Insulin dependent: The pancreas
produces little or no insulin
Type II (NIDDM)Non insulin dependent: The pancreas
produces different amounts of insulin

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
51
Care of Diabetic Patients
Insulin and glucose must be monitored
IV access Avoid metabolic crisis Antiembolic stockings required Postoperative compression boots
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
52
Complications Associated with Diabetes
Infection Dehydration Poor circulation Myocardial Infarction Delayed wound healing Control of blood sugar Neuropathic skeletal disease Neurogenic bladder Retinopathy Coronary Artery Disease Thrombophlebitis Tachycardia
Pregancy
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
54
The Pregnant Surgical Patient
Surgical procedures in first trimester avoided
Anesthesia Abdominal organs displaced from
normal position Physiological assessment is difficult
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
55
Fetal SurgeryFetal Surgery
ImmunocompromisedPatients
HIV+ Multiple sclerosis Lupus erythematosus Rheumatoid arthritis Transplant recipients Steroid use
(Cushing’s syndrome) Patient undergoing
radiation or chemotherapy

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
57
Care of Care of Immunocompromised Immunocompromised
PatientsPatients
Additional personnel to move patient Possible difficult intubation IV placement is difficult Grounding pad placement could be
difficult

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
58
Surgical Intervention Surgical Intervention RequiredRequired
Peritonitis secondary to cytomegaloviris
Non-Hodgkin’s lymphoma of GI tract Kaposi’s sarcoma of the GI tract Mycobacterial infection of
retroperitoneum or spleen HIV/AIDS (splenomegaly,
diagnostic biopsies)

Disabled Patients

Geriatrics
Biological differences
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
61
Geriatric PatientsGeriatric Patients
Usually over the age of 65 Chronic debilitation Decreased physiologic status Visual impairments Hearing impairments

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
62
Other Special Needs Other Special Needs PatientsPatients
Hearing impaired Visually impaired Physically disabled

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
63
Trauma PatientsTrauma Patients
“Golden Hour” Trauma Centers
• Level I• Level II• Level III• Level IV
Blunt Trauma Penetrating Trauma

© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
64
Trauma Scoring Trauma Scoring
Eye Opening Response Spontaneous--open with
blinking at baseline 4 points To verbal stimuli, command,
speech 3 points To pain only (not applied to
face) 2 points No response 1 point
Verbal Response Oriented 5 points Confused conversation, but
able to answer questions 4 points
Inappropriate words 3 points Incomprehensible speech 2
points No response 1 point
Motor Response Obeys commands for movement 6
points Purposeful movement to painful
stimulus 5 points Withdraws in response to pain 4
points Flexion in response to pain
(decorticate posturing) 3 points Extension response in response to
pain (decerebrate posturing) 2 points
No response 1 point Categorization:
Coma: No eye opening, no ability to follow commands, no word verbalizations (3-8)
Head Injury Classification:Severe Head Injury----GCS score of 8 or lessModerate Head Injury----GCS score of 9 to 12Mild Head Injury----GCS score of 13 to 15
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
65
Preservation of EvidencePreservation of Evidence
Violent crime items must be preserved for law enforcement
Physical evidence must be handled carefully
Facility policy must be strictly followed
© 2004 by Delmar Learning, a division of Thomson Learning, Inc. All Rights Reserved.
66
Other Considerations for the Trauma Patient
Hypothermia Infection Preparation of the case
The EndThe End